HIV, HBV, AND HCV POSTEXPOSURE MANAGEMENT FOR HEALTHCARE WORKERS. Weerawat Manosuthi Bamrasnaradura Infectious Diseases Institute
|
|
|
- Janel Barrett
- 5 years ago
- Views:
Transcription
1 HIV, HBV, AND HCV POSTEXPOSURE MANAGEMENT FOR HEALTHCARE WORKERS Weerawat Manosuthi Bamrasnaradura Infectious Diseases Institute
2 Outline Case scenario of HIV postexposure prophylaxis Risks of and how to manage postexposure prophylaxis Current HIV PEP guideline US PHS 2013 New York guideline 2012 Thai guideline 2010 HBV and HCV postexposure mannagement


3
4 Case presentation 1 Male paramedic splashed with large volume of bloody amniotic fluid onto open ulcers on his arm. He has DM II, HT, DLP, GERD, CKD, peripheral neuropathy. Source is HIV+ without any treatment during this pregnancy. Paramedic started on AZT, 3TC, and lopinavir/rtv. Two days later, he complains of overwhelming nausea and vomiting.
5 Case 2: 32 Year-old Nurse 11 Jan 15: Her left finger got stuck with a needle #18 used to draw blood from a patient. Visibly bloody superficial stick was found. This source patient is a HIV-infected patient with a history of multiple ARV regimens (NRTIs, NNRTIs, PIs). Year Regimens Viral load RAMs 2001 d4t, 3TC, EFV VL < AZT, 3TC, EFV VL < AZT, 3TC, LPV/r VL 76,800 RT: 103N, 190A 2011 VL 99,500 RT: 103N, 138K 2013 TDF, 3TC, LPV/r VL 318,000 RT: 138A Nov 14 VL 519,000 She was admitted with pneumonia and MAC infection. Her current ARV regimen was TDF, 3TC, LPV/r. She had a recent history of virologic failure with HIV RNA of 519,000 copies/ml and genotypic resistance showed NNRTI RAMs without NRTIs and PIs.
6 AK , 32 Year-old Nurse 11 Jan 15: Her left finger got stuck with a needle #18 used to draw blood from a patient Visibly bloody AZT, 3TC, superficial EFV stick was VL <50 found. This source 2010 patient is AZT, a 3TC, HIV-infected LPV/r patient VL 76,800 with a history RT: of 103N, multiple 190A ARV regimens(nrtis, NNRTIs, PIs). Year Regimens Viral load RAMs 2001 d4t, 3TC, EFV VL < VL 99,500 RT: 103N, 138K He was 2013 admitted with TDF, pneumonia 3TC, LPV/r and MAC infection. VL 318,000 His current ARV RT: regimen 138A was TDF, 3TC, LPV/r. He had Nov a 14 recent history of virologic failure with VL HIV 519,000 RNA of 519,000 copies/ml and genotypic resistance showed NNRTI RAMs without NRTIs and PIs. What would you manage this expose person? Would you prescribe NRTI drugs in this expose person? 1. I would 2. I would not What third agent should be given?
7 AK , 32 Year-old Nurse 11 Jan 15: Her left finger got stuck with a needle #18 used to draw blood from a patient. Visibly bloody superficial stick was found. This source patient is a HIV-infected patient with a history of multiple ARV regimen (NRTIs, NNRTIs, PIs). She was admitted with pneumonia and MAC infection. Her current ARV regimen was TDF, 3TC, LPV/r. She had a recent history of virologic failure with HIV RNA of 519,000 copies/ml and genotypic resistance showed NNRTI RAMs without NRTIs and PIs. TDF/FTC, Raltegravir, DRV/r was given.
8 AK , 32 Year-old Nurse 22 Jan 15: She developed petechial rashes at trunk and extremities without fever. CBC showed HCT 40%, WBC 4,900, N56%, L34%, Mo7%, Eo2%, Ba1%, plt 210,000. ALT was 88U/L and Cr was 0.68 mg/dl. How to manage this event? A. Continue PEP regimen B. Discontinue PEP regimen C. Modify PEP regimen D. Others
9 AK , 32 Year-old Nurse 22 Jan 15: She developed petechial rashes at trunk and extremities without fever. CBC showed HCT 40%, WBC 4,900, N56%, L34%, Mo7%, Eo2%, Ba1%, plt 210,000. ALT was 88U/L and Cr was 0.68 mg/dl. How to manage this event?
10 Postexposure Prophylaxis Occupational exposure - Percutaneous exposure - Mucous membrane exposure - Non-intacted skin Non-occupational exposure - Sexual exposure - Intravenous drug user
11 Who is the most frequently reported occupational acquired HIV infection? 1. Nurses 2. Physicians 3. Lab technicians 4. House keepers

12 Occupational Acquired HIV infection Do A, et al. Infect Control Hosp Epidemiol 2003;24:86-96.
13 Accidental Injuries in BIDI On exposed person analysis, 7.5% (3 of 40), 2.9% (1 of 34), 0% were positive for HBsAg, Anti-HCV and Anti-HIV, respectively. Seven of 45 (15.5%) events were severe exposures. 24 % (22of 45) of staffs initiated HIV PEP. 16 % initiated within 1 hour after exposure and half of them continued HIV PEP until 4 weeks. 53% (24 of 45) of staffs had previous history of HBV vaccination.
14 Postexposure Management Step Management 1 Exposure site management 2 Exposure reporting 3 Evaluation of transmission risk 4 Counseling 5 Consideration of PEP 6 Follow-up
15 Exposure Site Management Wound and skin: washed with soap and water Mucous membrane: flushed with water No evidence of benefit for: Application of antiseptics or disinfectants Squeezing ( milking ) puncture sites Avoid use of bleach and other agents caustic to skin
16 Postexposure Management Step Management 1 Exposure site management 2 Exposure reporting (1-4) 3 Evaluation of transmission risk 4 Counseling 5 Consideration of PEP 6 Follow-up
17 Exposure Report 1 (1) Details of procedure being performed Date and time of exposure Where and how exposure occurred Type and brand of device How and when in course of handling device (2) Details of exposure Type and amount of fluid, severity of exposure Percutaneous: depth of injury whether fluid was injected Skin or mucous membrane: estimated volume of material, condition of skin
18 Exposure Report 2 (3) Details of exposure source Source of material contained HBV, HCV or HIV? If HIV-infected: stage of disease, history of ARV, viral load, ARV resistance (4) Details of exposed person Anti HIV, Anti HBV, Anti HCV status Hepatitis B vaccination & vaccine response
19 Postexposure Management Step Management 1 Exposure site management 2 Exposure reporting 3 Evaluation of transmission risk 4 Counseling 5 Consideration of PEP 6 Follow-up
20 Evaluation of Transmission Risk 3 Type of HIV transmission Risk of transmission per exposure event Blood transfusion 0.95 Perinatal exposure 0.13 Needle stick (0.3%, 95%CI %) Unprotected receptive anal intercourse Needle sharing Unprotected receptive vaginal intercourse Mucous membrane exposure (0.09%, 95%CI %) Unprotected insertive vaginal intercourse Ingestion of human milk
21 Blood Potential fluid Body fluid containing visible blood CSF Pleural fluid Semen, Vg secretion Synovial fluid Pleural fluid Peritoneal fluid Non Potential fluid Feces Sweat Nasal secretion Tears Saliva Urine Sputum Vomitus Pericardial fluid Amniotic fluid Human bite Direct contact

22 Factors APPENDIX D. Associated LOGISTIC REGRESSION with ANALYSIS Transmission OF RISK FACTORS FOR HIV after INFECTION AFTER PERCUTANEOUS EXPOSURE TO HIV-INFECTED BLOOD Percutaneous Exposure Logistic Regression Analysis of Risk Factors for HIV Infection After Percutaneous Exposure to HIV-Infected Blood Risk Factor US Cases a All Cases b Adjusted odds ratio (95% CI) c Deep injury 16.1 ( ) Visible blood on device 5.2 ( ) Procedure involving needle in artery or vein 5.1 ( ) Terminal illness in source patient d 6.4 ( ) Postexposure use of zidovudine 0.2 ( ) Reprinted from Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure: Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med 1997;337: [PubMed] a All risk factors were significant (P < 0.02). b All risk factors were significant (P < 0.01). c Odds ratios are for the odds of seroconversion after exposure in workers with the risk factor as compared with those without it. d Terminal illness was defined as disease leading to the death of the source patient from AIDS within two months after the health care worker s exposure. NEJM 1997; 337: Postgrad Med J 2003,79:324-8.
23 Average Risk for Transmission of HIV, HBV, and HCV after Needle stick Source Risk HBV HBeAg+ HBeAg- 22.0% % 1.0% - 6.0% HCV+ 1.8% HIV+ 0.3%
24 Postexposure Management Step Management 1 Exposure site management 2 Exposure reporting 3 Evaluation of transmission risk 4 Counseling 5 Consideration of PEP 6 Follow-up
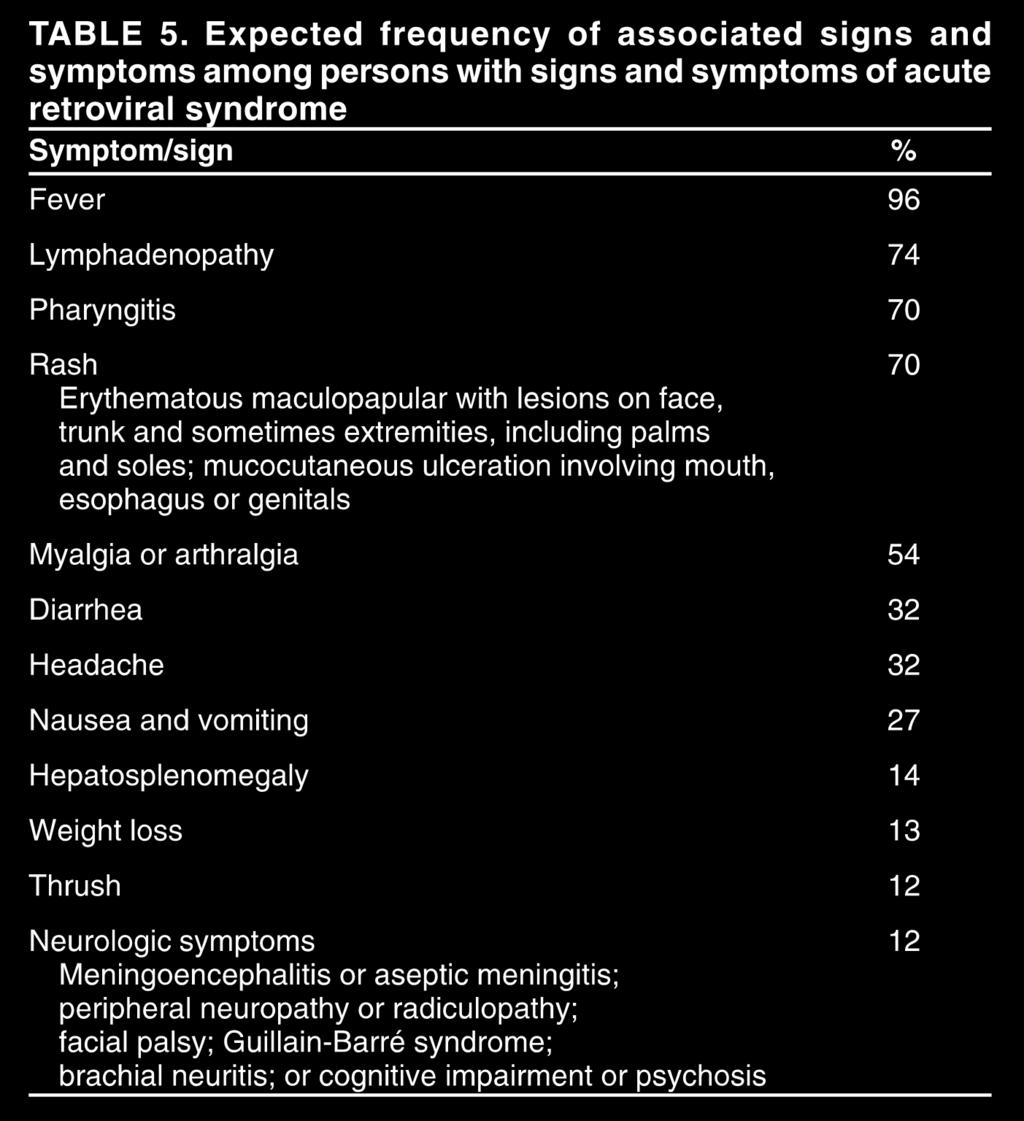
25 HIV Postexposure Counseling 1. Possible side effects of PEP drugs 2. Possible drug interactions 3. Adherence 4. Signs and symptoms of acute HIV infection Fever, rash, flu-like illness 5. Prevention of secondary transmission Sexual abstinence or condom use No blood/tissue donation Transmission and PEP drug risks if breastfeeding No work restriction indicated
26
27 Postexposure Management Step Management 1 Exposure site management 2 Exposure reporting 3 Evaluation of transmission risk 4 Counseling 5 Consideration of PEP 6 Follow-up
28 Considerations When Using PEP Risk of Transmission PEP Risk of Adverse Effects
29 Initiation of HIV PEP If indicated, start PEP as soon as possible after exposure Regard as an urgent medical concern Hours rather than days Interval after which PEP is no longer likely to be effective in humans is unknown Initiating PEP days or weeks after an exposure might be considered if warranted for increased risk exposure

30
31 Animal Studies of PEP: Prevention of SIV in macaques with Tenofovir Initiation / duration % Protected 24h / 28d 100% 48h / 28d 50% 72h / 28d 50% 24h / 10d 75% 24h / 3d 0% Tsai et al, J Virol, 1998;72:4265 Tsai et al, J Virol 1998;72:4265.

32 Thai Guideline 2010 Prefered basic regimens Alternative basic regimens Expanded regimens AZT/3TC d4t/3tc PI: LPV/r, IDV/r, ATV/r, SQV/r TDF/3TC ddi/3tc NNRTI: EFV TDF/FTC Thai Guideline 2014 ส ตรยาต านไวร ส A TDF + 3TC/FTC + Lopinavir/r หมายเหต B C TDF + 3TC/FTC + Rilpivirine TDF + 3TC/FTC + Atazanavir/r TDF +3TC/FTC + Raltegravir ปร กษาแพทย ผ เช ยวชาญด านโรคต ดเช อก อนเร มยา AZT แทน TDF ในส ตร A หร อ B ในบ คลากรท ม GFR < 60

33

34 Figure 1. PEP Following Occupational Exposure Two-drug regimen is not recommended. New York Guideline
35 Recommended Regimen for HIV PEP Table 3 Recommended Regimen for HIV PEP Following Occupational Exposure a Tenofovir b 300 mg PO qd + Emtricitabine b,c 200 mg PO qd Plus AZT is no longer recommended. Raltegravir d 400 mg PO bid a When the source is known to be HIV-infected, past and current ART experience, viral load data, and genotypic or phenotypic resistance data (if available) may indicate the use of an alternative PEP regimen. Consult with a clinician experienced in managing PEP. See Tables 4 and 5. b The dosing of tenofovir and emtricitabine/lamivudine should be adjusted in patients with baseline creatinine clearance <50 ml/min (see Appendix A for dosing recommendations). Tenofovir should be used with caution in exposed workers with renal insufficiency or who are taking concomitant nephrotoxic medications. Fixed-dose combinations should not be used in patients who need dose adjustment due to renal failure. c Lamivudine 300 mg PO qd may be substituted for emtricitabine. However, a fixed-dose combination is available when tenofovir is used with emtricitabine (Truvada 1 PO qd). d The dosing of raltegravir should be adjusted when co-administered with rifampin (see Appendix A for dosing recommendations). A. Duration of PEP Regimen New York Guideline
36 Preferred Alternative PEP Regimens New York Guideline
37 Antiretroviral Drugs to Avoid Drugs to avoid Efavirenz Nevirapine Abacavir Stavudine and Didanosine Nelfinavir and Indinavir CCR5 co-receptor antagonists Reasons - CNS side effects are common - Complicating the need to provide a first dose at any time of the day - Should be avoided in pregnant women - Substantial efavirenz resistance - Severe hepatotoxicity - Hypersensitivity reactions - Possibility of toxicities -Poorly tolerated - Lack of activity against potential CXCR4 tropic virus New York Guideline

38 US PHS Guideline 2013 Infection Control Hospital Epidimiology 2013;34:
39 US PHS Guideline 2013 Infection Control Hospital Epidimiology 2013;34:
40 US PHS Guideline 2013 Infection Control Hospital Epidimiology 2013;34:


41 Drug-drug Interactions!
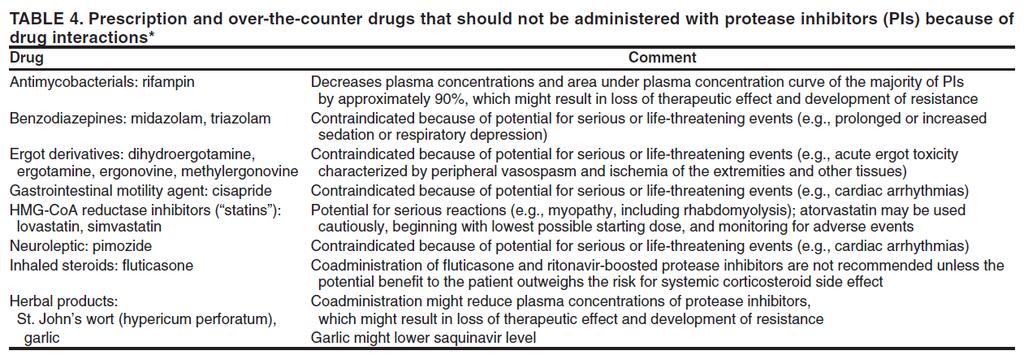

42 Drug-drug interactions
43 Consideration of PEP PEP during pregnancy Efavirenz is NOT recommended during pregnancy because of possible teratogenicity? Cases of fatal lactic acidosis in pregnant women treated with d4t and ddi reported Indinavir should not be given shortly before delivery because of hyperbilirubinemia


44
45 Primary HIV Infection: Common Signs & Symptoms fever 86 lethargy 74 myalgias rash headache pharyngitis adenopathy N = 160 patients with PHI in Geneva, Seattle and Sydney % of patients Vanhems P et al. AIDS 2000; 14:
46 Primary HIV Infection: Other Signs & Symptoms aseptic meningitis 24 oral ulcers 15 genital ulcers 10 thrombocytopenia 45 leukopenia 40 transaminitis % of patients Kahn JO, Walker BD. N Engl J Med. 1998;339:33-39.
47 Postexposure Management Exposure site management Exposure reporting Evaluation of transmission risk Counseling Consideration of PEP Follow-up

48 New York 2012: How to Follow-up New York Guideline
49 US PHS 2013: How to Follow-up Infection Control Hospital Epidimiology 2013;34:
50 Thai 2014: How to Follow-up
51 Postexposure Management Step Management 1 Exposure site management 2 Exposure reporting 3 Evaluation of transmission risk 4 Counseling 5 Consideration of PEP 6 Follow-up
52 Summary of PEP Recommendation Thai 2014 US PHS 2013 New York 2012 Time to initiate PEP < 72 hrs ASAP, <72 hrs Prefer <2 hrs, < 36 hrs Preferred PEP Alternative PEP LPV/r ATV/r RPV RAL EFV TDF/FTC TDF /3TC AZT/3TC RAL TDF/FTC RAL TDF/FTC RAL DRV/r ATV/r LPV/r ETR RPV TDF/FTC TDF/3TC AZT/3TC AZT/FTC DRV/r ATV/r FPV/r TDF/FTC
53 Summary of HIV Test Recommendation Baseline Wk 4 Wk 6 Wk 12 Wk 16 Wk 24 Wk 48 US PHS 2013* X X X X* X** New York 2012 X X X X** Thai 2014 X X X X** WHO 2007 X X X X** *Only wk 0, 6, 16 if use 4 th gen combination HIV p24 Ag-HIV Ab test **In case of HCV co-infection
54 Occupational exposure to HBV

55 HBV and HCV Transmission Risk after Needle stick Compared to HIV Source Risk HBV HBeAg+ HBeAg- 22.0% % 1.0% - 6.0% HCV+ 1.8% HIV+ 0.3%
56 HBV Postexposure Management Management depends on: Source hepatitis B surface antigen status Whether exposed person vaccinated Whether exposed person has immunity
57 Recommended PEP for Exposure to HBV Vaccination and Ab response status of exposed workers Source HBs Ag positive Treatment Source HBs Ag negative Source unknown or not available for testing Unvaccinated/Nonimmune HBIG 1 and initiate HB vaccine series Initiate HB vaccine series Initiate HB vaccine series Previously vaccinated - Known responder No treatment No treatment No treatment - Known nonresponder HBIG 0.06 ml/kg IM HBIG 1 and initiate revaccination or HBIG 2 No treatment If known high risk source, treat as if source were HBsAg+
58 Recommended PEP for Exposure to HBV Vaccination and Ab response status of exposed workers Previously vaccinated but Ab response unknown Source HBs Ag positive Treatment Source HBs Ag negative Source unknown or not available for testing Single vaccine dose No treatment No treatment unless high-risk source; if high-risk source, treat as if source were HBsAg positive If still undergoing vaccination HBIG 1; complete series Complete series Complete series
59 Efficacy of HBV PEP Regimen Multiple doses of HBIG alone when 1st dose initiated within 1 week Hepatitis B vaccine series alone Combination of HBIG and vaccine series * Estimated for adults, based on perinatal data Prevention of HBV Infection 70-75% 70-75% 85-95% MMWR Recomm Rep. 2003;52(RR-01):1-36. BeasleyRP, et al. Hepatology. 1983;3:
60 Follow-up HBV Testing of Exposed Person Perform follow-up anti-hbs testing in healthcare personnel who receive hepatitis B vaccine Test for anti-hbs 1-2 months after last dose Anti-HBs response to vaccine cannot be ascertained if HBIG received in the previous 3-4 months
61 Occupational exposure to HCV
62 Occupational Transmission of HCV Inefficiently transmitted by occupational exposures Average incidence 1.8% (range 0-7%) following percutaneous exposure from HCV-positive source Case reports of transmission from blood splash to mucous membrane Prevalence 1-2% among healthcare personnel Lower than among adults in the general population 10 times lower than for HBV infection
63 Interpretation of Hepatitis C Test Anti-HCV screening test results (EIA) HCV RNA (PCR) Nonreactive Nonreactive Not infected with HCV Comments Nonreactive Positive Active HCV infection; test subject is likely immune compromised. Reactive Negative 1. Resolved infection 2. Active infection. Single negative HCV RNA result does not rule out active infection. Follow-up HCV RNA test needed in > 6 months 3. False positive EIA test Reactive Positive Active HCV infection. Adapted from MMWR 2003;52(No. RR-3):11.
64 Hepatitis C Post-Exposure Management According to Baseline Test Results Clinical Scenario Source patient: HCV-antibody - neg Source patient: Unavailable or refuses testing Source patient: HCV-antibody - pos and HCV RNA - neg (A single negative HCV RNA result does not exclude active infection) Source patient: Both HCV antibody and HCV RNA - pos and Exposed worker is HCV-antibody negative Exposed worker: Both HCV antibody and HCV RNA - pos Follow-Up No further testing or follow-up is necessary for source patient or the exposed worker Exposed worker: Follow-up HCV antibody at 3 and 6 months Manage the exposed worker as if the source patient has chronic hepatitis C Source patient: Counsel and manage as chronic hepatitis C regardless of status of exposed worker Exposed worker: Follow up as outlined in Post-Exposure Follow-Up for HCV Counsel and manage as chronic hepatitis C
65 Postexposure Prophylaxis and Follow-up for HCV Not recommended after exposure immunoglobulin not effective no data on use of antivirals (e.g., interferon), and may be effective only with established infection antivirals not FDA approved for this setting For individuals exposed to hepatitis C-infected source patients Follow-up with HCV RNA is recommended in addition to HCV antibody testing Because HCV RNA testing can identify acute infection within 2 weeks of exposure Antibody test can be delayed up to several months after acute infection % Seroconversion with ELISA antibody Time after exposure 50% 9 weeks 80% 15 weeks 97% 6 months
66 Follow-up of HCV-Exposed HCP HCV Ab LFT HCV RNA Baseline (source HCV+ or unknown) X X 1 month X If source HCV + 3 months X X X 6 months X X X Increase in ALT in 1st 24 wks X
67 Case presentation 1 Male paramedic splashed with large volume of bloody amniotic fluid onto open ulcers on his arm. He has DM II, HT, DLP, GERD, CKD, peripheral neuropathy. Source is HIV+ without any treatment during this pregnancy. Paramedic started on AZT, 3TC, and lopinavir/rtv. Two days later, he complains of overwhelming nausea and vomiting.
68 Case 2: 32 Year-old Nurse 11 Jan 15: Her left finger got stuck with a needle #18 used to draw blood from a patient. Visibly bloody superficial stick was found. This source patient is a HIV-infected patient with a history of multiple ARV regimens (NRTIs, NNRTIs, PIs). Year Regimens Viral load RAMs 2001 d4t, 3TC, EFV VL < AZT, 3TC, EFV VL < AZT, 3TC, LPV/r VL 76,800 RT: 103N, 190A 2011 VL 99,500 RT: 103N, 138K 2013 TDF, 3TC, LPV/r VL 318,000 RT: 138A Nov 14 VL 519,000 She was admitted with pneumonia and MAC infection. Her current ARV regimen was TDF, 3TC, LPV/r. She had a recent history of virologic failure with HIV RNA of 519,000 copies/ml and genotypic resistance showed NNRTI RAMs without NRTIs and PIs.
69 AK , 32 Year-old Nurse 11 Jan 15: Her left finger got stuck with a needle #18 used to draw blood from a patient Visibly bloody AZT, 3TC, superficial EFV stick was VL <50 found. This source 2010 patient is AZT, a 3TC, HIV-infected LPV/r patient VL 76,800 with a history RT: of 103N, multiple 190A ARV regimens(nrtis, NNRTIs, PIs). Year Regimens Viral load RAMs 2001 d4t, 3TC, EFV VL < VL 99,500 RT: 103N, 138K He was 2013 admitted with TDF, pneumonia 3TC, LPV/r and MAC infection. VL 318,000 His current ARV RT: regimen 138A was TDF, 3TC, LPV/r. He had Nov a 14 recent history of virologic failure with VL HIV 519,000 RNA of 519,000 copies/ml and genotypic resistance showed NNRTI RAMs without NRTIs and PIs. What would you manage this expose person? Would you prescribe NRTI drugs in this expose person? 1. I would 2. I would not What third agent should be given?
70 AK , 32 Year-old Nurse 11 Jan 15: Her left finger got stuck with a needle #18 used to draw blood from a patient. Visibly bloody superficial stick was found. This source patient is a HIV-infected patient with a history of multiple ARV regimen (NRTIs, NNRTIs, PIs). She was admitted with pneumonia and MAC infection. Her current ARV regimen was TDF, 3TC, LPV/r. She had a recent history of virologic failure with HIV RNA of 519,000 copies/ml and genotypic resistance showed NNRTI RAMs without NRTIs and PIs. TDF/FTC, Raltegravir, DRV/r was given.
71 AK , 32 Year-old Nurse 22 Jan 15: She developed petechial rashes at trunk and extremities without fever. CBC showed HCT 40%, WBC 4,900, N56%, L34%, Mo7%, Eo2%, Ba1%, plt 210,000. ALT was 88U/L and Cr was 0.68 mg/dl. How to manage this event? A. Continue PEP regimen B. Discontinue PEP regimen C. Modify PEP regimen D. Others

72 AK , 32 Year-old Nurse 22 Jan 15: She developed petechial rashes at trunk and extremities without fever. CBC showed HCT 40%, WBC 4,900, N56%, L34%, Mo7%, Eo2%, Ba1%, plt 210,000. ALT was 88U/L and Cr was 0.68 mg/dl. How to manage this event?
73 Outline Case scenario of HIV postexposure prophylaxis Risks of and how to manage postexposure prophylaxis Current HIV PEP guideline US PHS 2013 New York guideline 2012 Thai guideline 2010 HBV and HCV postexposure mannagement
74 THANK YOU
Blood-Borne Pathogens and Post-Exposure Prophylaxis
 Blood-Borne Pathogens and Post-Exposure Prophylaxis Christopher Behrens MD Northwest Association of Occupational and Environmental Medicine October 2017 with thanks to Shireesha Dhanireddy MD Disclosures
Blood-Borne Pathogens and Post-Exposure Prophylaxis Christopher Behrens MD Northwest Association of Occupational and Environmental Medicine October 2017 with thanks to Shireesha Dhanireddy MD Disclosures
To provide the guidelines for the management of healthcare workers who have had an occupational exposure to blood and/or body fluids.
 TITLE/DESCRIPTION: MANAGEMENT OF OCCUPATIONAL EXPOSURE TO HBV, HCV, and HIV INDEX NUMBER: EFFECTIVE DATE: APPLIES TO: ISSUING AUTHORITY: 01/01/2009 01/01/2013 All GCC Countries GULF COOPERATION COUNCIL
TITLE/DESCRIPTION: MANAGEMENT OF OCCUPATIONAL EXPOSURE TO HBV, HCV, and HIV INDEX NUMBER: EFFECTIVE DATE: APPLIES TO: ISSUING AUTHORITY: 01/01/2009 01/01/2013 All GCC Countries GULF COOPERATION COUNCIL
EXPOSURE (HIV/HEPATITIS) BLOOD & BODY FLUIDS
 BLOOD & BODY FLUIDS") Page(s): 1 of 11 PURPOSE To set a standardized procedure to ensure that employees are evaluated in a consistent and timely manner.. POLICY A. The treatment of Team Member exposure to bloodborne pathogens
Page(s): 1 of 11 PURPOSE To set a standardized procedure to ensure that employees are evaluated in a consistent and timely manner.. POLICY A. The treatment of Team Member exposure to bloodborne pathogens
One of your office personnel
 Doug Campos-Outcalt, MD, MPA Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix HIV postexposure prophylaxis: Who should get it? CORRESPONDENCE Doug Campos-Outcalt,
Doug Campos-Outcalt, MD, MPA Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix HIV postexposure prophylaxis: Who should get it? CORRESPONDENCE Doug Campos-Outcalt,
Management of Workplace Exposure to Blood-borne Pathogens
 Management of Workplace Exposure to Blood-borne Pathogens 11/22/2017 Management of Workplace Exposure to Blood-borne Pathogens BY SOLYMOLE KURUVILLA, PHD, RN, ACNP-BC DIRECTOR, OCCUPATIONAL HEALTH SERVICES
Management of Workplace Exposure to Blood-borne Pathogens 11/22/2017 Management of Workplace Exposure to Blood-borne Pathogens BY SOLYMOLE KURUVILLA, PHD, RN, ACNP-BC DIRECTOR, OCCUPATIONAL HEALTH SERVICES
Occupational HIV exposures are crisis situations demanding immediate, decisive action. Henderson, 2001
 Post-Exposure Care: A Balancing Act Alice C. Thornton, MD Southeast AIDS Training & Education Center Kentucky Local Performance Site University of Kentucky October 24, 2009 Objectives Review the goals
Post-Exposure Care: A Balancing Act Alice C. Thornton, MD Southeast AIDS Training & Education Center Kentucky Local Performance Site University of Kentucky October 24, 2009 Objectives Review the goals
Bloodborne Pathogens Across the Continuum of Care Sue Sebazco, Arlington, Texas A Webber Training Teleclass
 Bloodborne Pathogens Across the Continuum of Care Objectives Sue Sebazco, RN, BS, CIC Infection Control/Employee Health Director Arlington, TX Pittsburg Mercy Health System skrystofiak@mercy.pmhs.org Define
Bloodborne Pathogens Across the Continuum of Care Objectives Sue Sebazco, RN, BS, CIC Infection Control/Employee Health Director Arlington, TX Pittsburg Mercy Health System skrystofiak@mercy.pmhs.org Define
Post-Exposure Prophylaxis Review for International Visitors
 Post-Exposure Prophylaxis Review for International Visitors Case Presentation 27 yo nurse presents to Urgent Care for a needlestick 2 days ago from a diabetic lancet. Source patient (SP): 35 yo male known
Post-Exposure Prophylaxis Review for International Visitors Case Presentation 27 yo nurse presents to Urgent Care for a needlestick 2 days ago from a diabetic lancet. Source patient (SP): 35 yo male known
Exposure. What Healthcare Personnel Need to Know
 Information from the Centers for Disease Control and Prevention National Center for Infectious Diseases Divison of Healthcare Quality Promotion and Division of Viral Hepatitis For additional brochures
Information from the Centers for Disease Control and Prevention National Center for Infectious Diseases Divison of Healthcare Quality Promotion and Division of Viral Hepatitis For additional brochures
HIV prophylaxis for health care providers. Dr. A. K. M. Humayon Kabir Assistant Professor Department of Medicine Dhaka Medical College Hospital
 HIV prophylaxis for health care providers. Dr. A. K. M. Humayon Kabir Assistant Professor Department of Medicine Dhaka Medical College Hospital HIV continues to be a major global public health issue, Approximately
HIV prophylaxis for health care providers. Dr. A. K. M. Humayon Kabir Assistant Professor Department of Medicine Dhaka Medical College Hospital HIV continues to be a major global public health issue, Approximately
Clinical Education Initiative OCCUPATIONAL POST- EXPOSURE PROPHYLAXIS. Antonio E. Urbina, MD
 Clinical Education Initiative Support@ceitraining.org OCCUPATIONAL POST- EXPOSURE PROPHYLAXIS Antonio E. Urbina, MD 5/22/2013 Occupational Post-Exposure Prophylaxis [Video Transcript] 00:00:15 - [Tony]
Clinical Education Initiative Support@ceitraining.org OCCUPATIONAL POST- EXPOSURE PROPHYLAXIS Antonio E. Urbina, MD 5/22/2013 Occupational Post-Exposure Prophylaxis [Video Transcript] 00:00:15 - [Tony]
HIV and PEP. LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED
 HIV and PEP LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED Disclaimer The views expressed in this presentation are those of the speaker and do not reflect the official policy of the Department
HIV and PEP LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED Disclaimer The views expressed in this presentation are those of the speaker and do not reflect the official policy of the Department
Bloodborne Pathogens: Recognition and Treatment 2011
 Bloodborne Pathogens: Recognition and Treatment 2011 Occupational Health Services at The Summit Rita M. Lopez, APRN-BC, MSN 751-4189 rlopez@krmc.org OBJECTIVES DEFINE Bloodborne Pathogen Exposure WHO must
Bloodborne Pathogens: Recognition and Treatment 2011 Occupational Health Services at The Summit Rita M. Lopez, APRN-BC, MSN 751-4189 rlopez@krmc.org OBJECTIVES DEFINE Bloodborne Pathogen Exposure WHO must
/AIDS HIV/ HIV Overview. Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program
 /AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
/AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
Needlestick and Splash Exposure Flow Chart Page 1 Clinical Practice Guidelines
 Needlestick and Splash Exposure Flow Chart Page 1 If ANY student experiences a needlestick or splash exposure ANY time of day/night, they need to page #11709 which will be forwarded to: (**in the event
Needlestick and Splash Exposure Flow Chart Page 1 If ANY student experiences a needlestick or splash exposure ANY time of day/night, they need to page #11709 which will be forwarded to: (**in the event
Post Exposure Prophylaxis (PEP)
") Post Exposure Prophylaxis (PEP) Occupational exposure Occupational exposure refers to exposure to potential blood-borne infections (HIV, HBV and HCV) that may occur in healthcare settings during performance
Post Exposure Prophylaxis (PEP) Occupational exposure Occupational exposure refers to exposure to potential blood-borne infections (HIV, HBV and HCV) that may occur in healthcare settings during performance
HIV Overview. Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program
 HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Non-occupational HIV Post Exposure Prophylaxis (npep)
") Mountain West AIDS Education and Training Center Non-occupational HIV Post Exposure Prophylaxis (npep) Robert Harrington, M.D. This presentation is intended for educational use only, and does not in any
Mountain West AIDS Education and Training Center Non-occupational HIV Post Exposure Prophylaxis (npep) Robert Harrington, M.D. This presentation is intended for educational use only, and does not in any
SIV/SHIV Exposure Medical Response Guidance for the University of Wisconsin-Madison
 SIV/SHIV SIV/SHIV Exposure Medical Response Guidance for the University of Wisconsin-Madison 1.0 Instructions: Information in this guidance is meant to inform both laboratory staff and health professionals
SIV/SHIV SIV/SHIV Exposure Medical Response Guidance for the University of Wisconsin-Madison 1.0 Instructions: Information in this guidance is meant to inform both laboratory staff and health professionals
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV
 POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
MUSC Occupational Bloodborne Pathogen Protocol Off Campus Procedure Packet. Instructions for Employees/Students:
 MUSC Occupational Bloodborne Pathogen Protocol Off Campus Procedure Packet MUSC has established these protocols in accordance with the OSHA Bloodborne Pathogen Standard and Center for Disease Control recommendations
MUSC Occupational Bloodborne Pathogen Protocol Off Campus Procedure Packet MUSC has established these protocols in accordance with the OSHA Bloodborne Pathogen Standard and Center for Disease Control recommendations
43. Guidelines on Needle stick Injury
 43. Guidelines on Needle stick Injury The following information is abstracted from the South African Department of Health guidelines entitled: Management of Occupational Exposure to the Human Immunodeficiency
43. Guidelines on Needle stick Injury The following information is abstracted from the South African Department of Health guidelines entitled: Management of Occupational Exposure to the Human Immunodeficiency
HIV Management Update 2015
 9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Guidelines for Post- Exposure Prophylaxis for HAV, HBV, HCV & HIV
 Guidelines for Post- Exposure Prophylaxis for HAV, HBV, HCV & HIV By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties An exposure that might place health
Guidelines for Post- Exposure Prophylaxis for HAV, HBV, HCV & HIV By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties An exposure that might place health
INITIAL EVALUATION AND MANAGEMENT FOLLOWING EXPOSURE TO BLOOD OR BODY FLUIDS
 Page 1 of 11 Original Date of Issue: June 1991 Reviewed 2/96 5/97 11/98 11/99 5/01 5/02 12/05 Revised 9/95 5/97 5/00 7/02 3/06 6/08 6/10 The following are the procedures to be followed when a person sustains
Page 1 of 11 Original Date of Issue: June 1991 Reviewed 2/96 5/97 11/98 11/99 5/01 5/02 12/05 Revised 9/95 5/97 5/00 7/02 3/06 6/08 6/10 The following are the procedures to be followed when a person sustains
Revised April WGH ER #5 Hospital Rd. Whitehorse Phone: (867) Outside of Whitehorse: Local Community Health Centre/Clinic/ER
 Outside of Whitehorse: Local Community Health Centre/Clinic/ER") Where to access care Who to consult and when Please consult whenever questions arise on how to proceed with postexposure management and when exposure is beyond the scope of guidelines. Blood and Body Fluid
Where to access care Who to consult and when Please consult whenever questions arise on how to proceed with postexposure management and when exposure is beyond the scope of guidelines. Blood and Body Fluid
Outline. A 41 Year-old Male COMMON PITFALLS IN HIV/AIDS MANAGEMENT: A CASE-BASED APPROACH. Q1: What anti-fungal regimen would you start?
 Outline COMMON PITFALLS IN HIV/AIDS MANAGEMENT: A CASE-BASED APPROACH Considerations for antiretroviral use in patients with coinfections Concerning and how to manage drug-drug interactions ARV-other drugs
Outline COMMON PITFALLS IN HIV/AIDS MANAGEMENT: A CASE-BASED APPROACH Considerations for antiretroviral use in patients with coinfections Concerning and how to manage drug-drug interactions ARV-other drugs
FAMILY HIV CENTER NJ CARES SANE
 HIV, Hepatitis B & C Postexposure Prophylaxis for Sexual Assault Victims Update for Case Managers Susan Burrows-Clark, RN, MSN, CNS, C. 10/17/11 Antiretroviral Postexposure Prophylaxis After Sexual, Injection-Drug
HIV, Hepatitis B & C Postexposure Prophylaxis for Sexual Assault Victims Update for Case Managers Susan Burrows-Clark, RN, MSN, CNS, C. 10/17/11 Antiretroviral Postexposure Prophylaxis After Sexual, Injection-Drug
Exposure. Blood. Department of Health & Human Services
 Exposure to Blood What Health-Care Workers Need to Know Department of Health & Human Services OCCUPATIONAL EXPOSURES TO BLOOD Introduction Health-care workers are at risk for occupational exposure to bloodborne
Exposure to Blood What Health-Care Workers Need to Know Department of Health & Human Services OCCUPATIONAL EXPOSURES TO BLOOD Introduction Health-care workers are at risk for occupational exposure to bloodborne
Post-Sexual Exposure Prophylaxis (npep)
") Projeto Praça Onze Universidade Federal do Rio de Janeiro Post-Sexual Exposure Prophylaxis (npep) Mauro Schechter Principal Investigator, Projeto Praça Onze Professor of Infectious Diseases Universidade
Projeto Praça Onze Universidade Federal do Rio de Janeiro Post-Sexual Exposure Prophylaxis (npep) Mauro Schechter Principal Investigator, Projeto Praça Onze Professor of Infectious Diseases Universidade
determine need but regimen does not change based on risk factor ED medicine attending meets
 HIV PEP Guidelines after Sexual Assault Harborview Medical Center January 2015 Initial risk assessment and discussion with patient about risk and PEP is by clinician who does exam (SANE, Ob-Gyn resident,
HIV PEP Guidelines after Sexual Assault Harborview Medical Center January 2015 Initial risk assessment and discussion with patient about risk and PEP is by clinician who does exam (SANE, Ob-Gyn resident,
Antonio E. Urbina, M.D. Associate Medical Director Center for Comprehensive Care, West 17 th Street Clinic St. Luke s Roosevelt Hospital DISCLOSURES
 PROPHYLAXISFOLLOWINGHIV, HEPB ANDC EXPOSURES: WHAT SNEW Antonio E. Urbina, M.D. Associate Medical Director Center for Comprehensive Care, West 17 th Street Clinic St. Luke s Roosevelt Hospital DISCLOSURES
PROPHYLAXISFOLLOWINGHIV, HEPB ANDC EXPOSURES: WHAT SNEW Antonio E. Urbina, M.D. Associate Medical Director Center for Comprehensive Care, West 17 th Street Clinic St. Luke s Roosevelt Hospital DISCLOSURES
Bloodbourne Pathogens (BBP) Occupational Post-Exposure Chemophrophylaxis
 Occupational Post-Exposure Chemophrophylaxis") Bloodbourne Pathogens (BBP) Audience: All personnel in the. Purpose: The purpose of this document is to establish UTMB policy for the initiation of prophylaxis after occupational exposure to the human
Bloodbourne Pathogens (BBP) Audience: All personnel in the. Purpose: The purpose of this document is to establish UTMB policy for the initiation of prophylaxis after occupational exposure to the human
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
0% 0% 0% Parasite. 2. RNA-virus. RNA-virus
 HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
HIV Occupational Transmission and Exposure. Marsh Gelbart 2010
 HIV Occupational Transmission and Exposure Marsh Gelbart 2010 Rationale for Post Exposure Prophylaxis (PEP) It was estimated that the risk for HIV transmission after percutaneous exposures involving larger
HIV Occupational Transmission and Exposure Marsh Gelbart 2010 Rationale for Post Exposure Prophylaxis (PEP) It was estimated that the risk for HIV transmission after percutaneous exposures involving larger
Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP)
") Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) For Healthcare Providers About Emtricitabine/Tenofovir Disoproxil
Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) For Healthcare Providers About Emtricitabine/Tenofovir Disoproxil
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
Blood/Body Fluid Exposure Option
 Introduction: Transmission of bloodborne pathogens [e.g., Hepatitis B virus (HBV), Hepatitis C virus (HBC), Human Immunodeficiency Virus (HIV)] from patients to healthcare workers (HCW) is an important
Introduction: Transmission of bloodborne pathogens [e.g., Hepatitis B virus (HBV), Hepatitis C virus (HBC), Human Immunodeficiency Virus (HIV)] from patients to healthcare workers (HCW) is an important
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
Bloodborne Pathogens Exposure Procedure
 Bloodborne Pathogens Exposure Procedure Background: Bloodborne pathogens are infectious microorganisms present in blood that can cause disease in humans. These pathogens include, but are not limited to,
Bloodborne Pathogens Exposure Procedure Background: Bloodborne pathogens are infectious microorganisms present in blood that can cause disease in humans. These pathogens include, but are not limited to,
Exposures at Non-MUSC Clinical Sites
 BLOOD BORNE PATHOGEN EXPOSURE CHECKLIST Exposures at Non-MUSC Clinical Sites (Students on clinical rotations at Roper Hospital, Trident Hospital, Affiliated Local Clinical Sites, Out of Town Clinical Sites,
BLOOD BORNE PATHOGEN EXPOSURE CHECKLIST Exposures at Non-MUSC Clinical Sites (Students on clinical rotations at Roper Hospital, Trident Hospital, Affiliated Local Clinical Sites, Out of Town Clinical Sites,
Jennifer Adams, MD Denver Health. September 28, 2010
 Jennifer Adams, MD Denver Health General Internal Medicine dii and HIV Primary Care September 28, 2010 HIV for PCP s PCP s often think they don t need to know much about HIV: it s managed by specialists
Jennifer Adams, MD Denver Health General Internal Medicine dii and HIV Primary Care September 28, 2010 HIV for PCP s PCP s often think they don t need to know much about HIV: it s managed by specialists
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
Occupational and Non- Occupational HIV Post-exposure Prophylaxis
 Occupational and Non- Occupational HIV Post-exposure Prophylaxis Amy V. Kindrick, MD, MPH National Clinicians Post-Exposure Prophylaxis Hotline (PEPline) University of California, San Francisco San Francisco
Occupational and Non- Occupational HIV Post-exposure Prophylaxis Amy V. Kindrick, MD, MPH National Clinicians Post-Exposure Prophylaxis Hotline (PEPline) University of California, San Francisco San Francisco
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
An International Antiviral Society-USA
 Doug Campos-Outcalt, MD, MPA University of Arizona, Phoenix dougco@email.arizona. edu A look at new guidelines for HIV treatment and prevention Start antiretroviral therapy as soon as possible after HIV
Doug Campos-Outcalt, MD, MPA University of Arizona, Phoenix dougco@email.arizona. edu A look at new guidelines for HIV treatment and prevention Start antiretroviral therapy as soon as possible after HIV
HIV Update Objectives. Epidemiology. Epidemiology, Transmission and Natural History. Transmission Risk by Exposure. Transmission 9/29/2014
 Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
Important Safety Information About TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication. For Healthcare Providers
 Indication. For Healthcare Providers") Important Safety Information About TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication For Healthcare Providers About TRUVADA for a PrEP Indication INDICATION AND PRESCRIBING CONSIDERATIONS TRUVADA,
Important Safety Information About TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication For Healthcare Providers About TRUVADA for a PrEP Indication INDICATION AND PRESCRIBING CONSIDERATIONS TRUVADA,
PREP IN PRIMARY CARE TRACY SALAMEH RN, BSN, ACRN HIV CLINICAL SPECIALIST DAKOTA AIDS EDUCATION AND TRAINING CENTER
 PREP IN PRIMARY CARE TRACY SALAMEH RN, BSN, ACRN HIV CLINICAL SPECIALIST DAKOTA AIDS EDUCATION AND TRAINING CENTER THE NEED FOR CONTINUED HIV PREVENTION Estimated new HIV infections in the US for the most
PREP IN PRIMARY CARE TRACY SALAMEH RN, BSN, ACRN HIV CLINICAL SPECIALIST DAKOTA AIDS EDUCATION AND TRAINING CENTER THE NEED FOR CONTINUED HIV PREVENTION Estimated new HIV infections in the US for the most
Obstetric Complications in HIV-Infected Women. Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School
 Obstetric Complications in HIV-Infected Women Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School Obstetric Complications and HIV Obstetric complications are not increased in
Obstetric Complications in HIV-Infected Women Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School Obstetric Complications and HIV Obstetric complications are not increased in
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
PrEP for HIV Prevention. Adult Clinical Guideline from the New York State Department of Health AIDS Institute
 PrEP for HIV Prevention Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the PrEP Guideline Raise awareness of PrEP among healthcare
PrEP for HIV Prevention Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the PrEP Guideline Raise awareness of PrEP among healthcare
STUDENT EXPOSURE TO BLOOD OR OTHER POTENTIALLY INFECTIOUS MATERIALS
 STUDENT EXPOSURE TO BLOOD OR OTHER POTENTIALLY INFECTIOUS MATERIALS (See Bloodborne Pathogen Worksheet and Post Exposure Prophylaxis consent immediately following this policy ) 1. Student must report immediately
STUDENT EXPOSURE TO BLOOD OR OTHER POTENTIALLY INFECTIOUS MATERIALS (See Bloodborne Pathogen Worksheet and Post Exposure Prophylaxis consent immediately following this policy ) 1. Student must report immediately
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
Clinical skills building - HIV drug resistance
 Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES?
 WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
I. HIV Epidemiology. HIV Infection A Primer. Objectives. Disclosures 7/18/2014
 Objectives HIV Infection A Primer Discuss the worldwide and domestic epidemiology of HIV infection Review HIV Biology Review HIV Transmission and Prevention Review HIV diagnosis Describe the approaches
Objectives HIV Infection A Primer Discuss the worldwide and domestic epidemiology of HIV infection Review HIV Biology Review HIV Transmission and Prevention Review HIV diagnosis Describe the approaches
Postexposure prophylaxis (PEP)
") Postexposure Prophylaxis Against Human Immunodeficiency Virus MICHAEL A. TOLLE, MD, MPH, and HEIDI L. SCHWARZWALD, MD, MPH, Baylor College of Medicine, Houston, Texas Family physicians often encounter
Postexposure Prophylaxis Against Human Immunodeficiency Virus MICHAEL A. TOLLE, MD, MPH, and HEIDI L. SCHWARZWALD, MD, MPH, Baylor College of Medicine, Houston, Texas Family physicians often encounter
01.02 Blood Borne Pathogens (BBP) Occupational Post Exposure Management
 Occupational Post Exposure Management") 01.02 Blood Borne Pathogens (BBP) Occupational Post Exposure Purpose Audience Policy Definitions Establish protocol for management of occupational exposures to blood or potentially infectious materials.
01.02 Blood Borne Pathogens (BBP) Occupational Post Exposure Purpose Audience Policy Definitions Establish protocol for management of occupational exposures to blood or potentially infectious materials.
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course
 Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Module 1: HIV epidemiology, transmission and prevention
 Session 2 Module goals Module 1 Participants will be able to: -offer an insight into the epidemiological situation in the country and worldwide -present the HIV transmission modes and the broad approaches
Session 2 Module goals Module 1 Participants will be able to: -offer an insight into the epidemiological situation in the country and worldwide -present the HIV transmission modes and the broad approaches
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
Post exposure prophylaxis following exposure to HIV. Paul Benn Mortimer Market Centre, Camden PCT HIVPA study day Tuesday 18 th November 2008 SOAS
 Post exposure prophylaxis following exposure to HIV Paul Benn Mortimer Market Centre, Camden PCT HIVPA study day Tuesday 18 th November 2008 SOAS Overview Hypothesis PEP? Awareness & uptake PEP/PEPSE Ensuring
Post exposure prophylaxis following exposure to HIV Paul Benn Mortimer Market Centre, Camden PCT HIVPA study day Tuesday 18 th November 2008 SOAS Overview Hypothesis PEP? Awareness & uptake PEP/PEPSE Ensuring
HIV basics. Katya Calvo Medical Director of Antimicrobial Stewardship
 HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HEPATITIS B INFECTION and Pregnancy. Caesar Mensah Communicable Diseases & Infection Control Specialist, UK June 2011
 HEPATITIS B INFECTION and Pregnancy Caesar Mensah Communicable Diseases & Infection Control Specialist, UK June 2011 HEPATITIS B 26/07/2011 What is Hepatitis B? It is inflammation (infection) of the liver
HEPATITIS B INFECTION and Pregnancy Caesar Mensah Communicable Diseases & Infection Control Specialist, UK June 2011 HEPATITIS B 26/07/2011 What is Hepatitis B? It is inflammation (infection) of the liver
Pre and Post Exposure Prophylaxis. Laila AL Dabal MD FRCP MSc Infectious Diseases Unit Dubai Health Authority 15 March 2018
 Pre and Post Exposure Prophylaxis Laila AL Dabal MD FRCP MSc Infectious Diseases Unit Dubai Health Authority 15 March 2018 Indications for Pre and Post Exposure Prophylaxis: occupational and non-occupational
Pre and Post Exposure Prophylaxis Laila AL Dabal MD FRCP MSc Infectious Diseases Unit Dubai Health Authority 15 March 2018 Indications for Pre and Post Exposure Prophylaxis: occupational and non-occupational
Decision Analysis Example
 Decision Analysis Example after Occupational Exposure to Infection after Needlestick Injury Direct inoculation into blood vessels Cutaneous dendritic (Langerhans) cells Delay from injury to infection Initial
Decision Analysis Example after Occupational Exposure to Infection after Needlestick Injury Direct inoculation into blood vessels Cutaneous dendritic (Langerhans) cells Delay from injury to infection Initial
Overview of HIV. LTC Paige Waterman
 Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION. Jason E. Vercher, PA-C, AAHIVM
 NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION Jason E. Vercher, PA-C, AAHIVM Disclosures No disclosures to report Learning Objectives q Identify Individuals who would benefit from non-occupational
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION Jason E. Vercher, PA-C, AAHIVM Disclosures No disclosures to report Learning Objectives q Identify Individuals who would benefit from non-occupational
Structured Treatment Interruption in HIV Positive Patients. Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007
 Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
AMERICAN ACADEMY OF PEDIATRICS. Guidance for the Clinician in Rendering Pediatric Care. Peter L. Havens, MD, and the Committee on Pediatric AIDS
 AMERICAN ACADEMY OF PEDIATRICS CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care Peter L. Havens, MD, and the Committee on Pediatric AIDS Postexposure Prophylaxis in Children and Adolescents
AMERICAN ACADEMY OF PEDIATRICS CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care Peter L. Havens, MD, and the Committee on Pediatric AIDS Postexposure Prophylaxis in Children and Adolescents
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
Clinical management of non-occupational and occupational exposure to blood borne pathogens. - A Pocket Reference -
 Pocket P.E.P. Clinical management of non-occupational and occupational eposure to blood borne pathogens Development Team: Deborah Yoong, PharmD 1 1, 2, 3 Kevin Gough, MD, MEd 1 Positive Care Clinic, Toronto,
Pocket P.E.P. Clinical management of non-occupational and occupational eposure to blood borne pathogens Development Team: Deborah Yoong, PharmD 1 1, 2, 3 Kevin Gough, MD, MEd 1 Positive Care Clinic, Toronto,
Guidance for management of exposure events where there is a risk of transmission of blood borne viruses
 Guidance for management of exposure events where there is a risk of transmission of blood borne viruses (HIV, Hepatitis B and Hepatitis C) in the community SUMMARY Where a child is thought to have had
Guidance for management of exposure events where there is a risk of transmission of blood borne viruses (HIV, Hepatitis B and Hepatitis C) in the community SUMMARY Where a child is thought to have had
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Definitions. Appendix A
 Definitions Appendix A 1. Blood means human blood, human blood components, and products made from human blood. 2. Bloodborne Pathogens means pathogenic microorganisms that are present in human blood and
Definitions Appendix A 1. Blood means human blood, human blood components, and products made from human blood. 2. Bloodborne Pathogens means pathogenic microorganisms that are present in human blood and
TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication. Training Guide for Healthcare Providers
 Indication. Training Guide for Healthcare Providers") TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication Training Guide for Healthcare Providers About TRUVADA for a PrEP indication to reduce the risk of sexually acquired HIV-1 infection in high-risk
TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication Training Guide for Healthcare Providers About TRUVADA for a PrEP indication to reduce the risk of sexually acquired HIV-1 infection in high-risk
Management of sharps injuries in the healthcare setting
 Link to this article online for CPD/CME credits Management of sharps injuries in the healthcare setting Anna Riddell, 1 Ioana Kennedy, 2 C Y William Tong 1 3 1 Department of Infection, Barts Health NHS
Link to this article online for CPD/CME credits Management of sharps injuries in the healthcare setting Anna Riddell, 1 Ioana Kennedy, 2 C Y William Tong 1 3 1 Department of Infection, Barts Health NHS
Malaysian Consensus Guidelines on Antiretroviral Therapy Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh
 Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
European AIDS Clinical Society (EACS) Guidelines for the Clinical Management and Treatment of HIV Infected Adults in Europe
 Guidelines for the Clinical Management and Treatment of HIV Infected Adults in Europe") European AIDS Clinical Society (EACS) Guidelines for the Clinical Management and Treatment of HIV Infected Adults in Europe PANEL MEMBERS Nathan Clumeck, Treasurer Chair, Brussels, Belgium Anton Pozniak,
European AIDS Clinical Society (EACS) Guidelines for the Clinical Management and Treatment of HIV Infected Adults in Europe PANEL MEMBERS Nathan Clumeck, Treasurer Chair, Brussels, Belgium Anton Pozniak,
01.02 Blood Borne Pathogens (BBP) Occupational Post Exposure Prophylaxis
 Occupational Post Exposure Prophylaxis") 01.02 Blood Borne Pathogens (BBP) Occupational Post Exposure Purpose Audience Establish protocol for management of occupational exposures to blood or potentially infectious materials. All employees of
01.02 Blood Borne Pathogens (BBP) Occupational Post Exposure Purpose Audience Establish protocol for management of occupational exposures to blood or potentially infectious materials. All employees of
PEDIATRIC EMERGENCY DEPARTMENT CLINICAL GUIDELINE: NON- OCCUPATIONAL EXPOSURE TO BLOOD-BORNE PATHOGENS (HIV, Hepatitis B, AND Hepatitis C)
") General Definition: Blood-borne pathogens are infectious agents that can be transmitted through contact with blood or certain other body fluids. The primary pathogens are HIV, Hepatitis B, and C. Before
General Definition: Blood-borne pathogens are infectious agents that can be transmitted through contact with blood or certain other body fluids. The primary pathogens are HIV, Hepatitis B, and C. Before
Pediatric HIV Update NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers
 Training Guide for Healthcare Providers") Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers About emtricitabine/tenofovir disoproxil fumarate for HIV-1 PrEP
Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers About emtricitabine/tenofovir disoproxil fumarate for HIV-1 PrEP
Commonly Asked Questions About Chronic Hepatitis C
 Commonly Asked Questions About Chronic Hepatitis C From the American College of Gastroenterology 1. How common is the hepatitis C virus? The hepatitis C virus is the most common cause of chronic viral
Commonly Asked Questions About Chronic Hepatitis C From the American College of Gastroenterology 1. How common is the hepatitis C virus? The hepatitis C virus is the most common cause of chronic viral
What s New. In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group
 What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
TRANSMISSION OF BLOODBORNE PATHOGENS: HIV,HBV,HCV. Dr Daniel Kimani HIV Prevention Medical Transmission CDC, Kenya.
 TRANSMISSION OF BLOODBORNE PATHOGENS: HIV,HBV,HCV Dr Daniel Kimani HIV Prevention Medical Transmission CDC, Kenya. Nevada Hepatitis C Outbreak Tied to Las Vegas Clinic. Thousands Now At Risk for Hepatitis,
TRANSMISSION OF BLOODBORNE PATHOGENS: HIV,HBV,HCV Dr Daniel Kimani HIV Prevention Medical Transmission CDC, Kenya. Nevada Hepatitis C Outbreak Tied to Las Vegas Clinic. Thousands Now At Risk for Hepatitis,
Management of NRTI Resistance
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Management of NRTI Resistance David Spach, MD Principal Investigator, NW AETC Professor of Medicine, Division of Infectious Diseases University of Washington
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Management of NRTI Resistance David Spach, MD Principal Investigator, NW AETC Professor of Medicine, Division of Infectious Diseases University of Washington
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort
 Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,