An Update On HIV Pharmacotherapy. Gonzalo M.L. Bearman MD,MPH Assistant Professor of Medicine Associate Hospital Epidemiologist
|
|
|
- Flora Ford
- 6 years ago
- Views:
Transcription

1 An Update On HIV Pharmacotherapy Gonzalo M.L. Bearman MD,MPH Assistant Professor of Medicine Associate Hospital Epidemiologist
2 Outline Review HIV epidemiology HIV natural history Viral Dynamic and three compartment model of HIV infection Current Antiretrovirals ucleoside/ucleotide Analogs RTI PI Fusion Inhibitors Once daily dosing Highlight important toxicities and drug interactions DHHS guidelines for the use of antiretrovirals Treatment failure Compliance and barriers to adherence
3
4 atural History of HIV Infection I Pantaleo EJM 1993;328:327
5 Viral Dynamics -- Summary 10 billion new virions created and cleared daily 200 million CD4 cells destroyed daily (twice the rate of replacement by the hematopoietic system) Ho et al, ature 1995;373:123

6 MACS cohort, Mellors,et al. Ann Intern Med 1997;126:946
7 Antiretroviral Therapy: 2004
8 Antiretroviral Drugs: 2004 nucleoside RTIs zidovudine (ZDV) didanosine (ddi) zalcitabine (ddc) stavudine (d4t) lamivudine (3TC) abacavir (ABC) emtricitabine (FTC) RTIs nevirapine (VP) delavirdine (DLV) efavirenz (EFV) nucleotide RTIs tenofovir (TFV) protease inhibitors saquinavir (SQV) ritonavir (RTV) indinavir (IDV) nelfinavir (FV) amprenavir (APV) lopinavir/r (LPV/r) atazanavir (ATV) fusion inhibitors enfuvirtide (T-20)
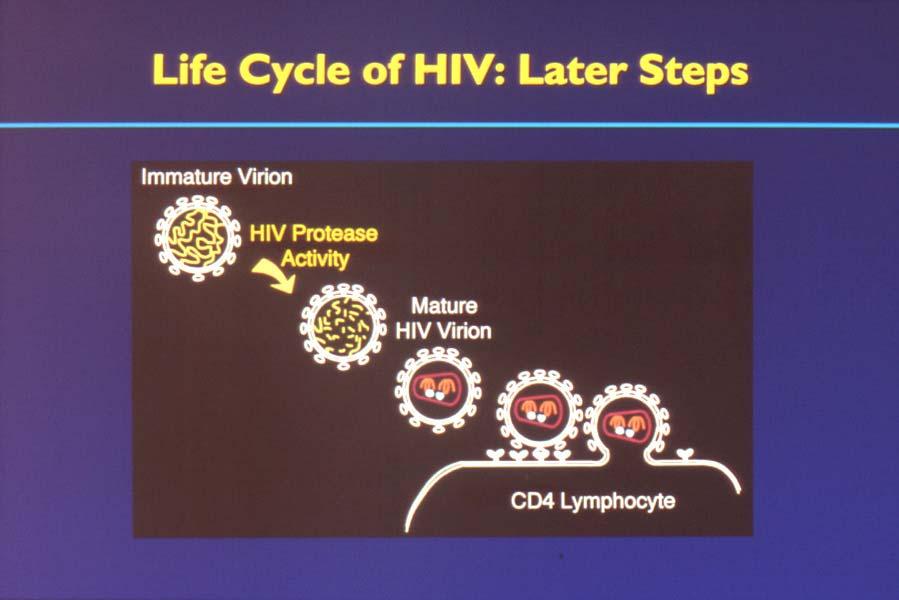
9 Life Cycle of HIV DS dna COMPLEX

10 Life Cycle of HIV reverse transcriptase inhibitors DS dna COMPLEX protease inhibitors entry inhibitors
11 H 2 H 2 O O H H CH 3 H adenosine O H cytosine H 2 H guanine O H thymine O O HO H didanosine (ddi) O H 2 O HO zalcitabine (ddc) HO H 2 H abacavir (ABC) HO H 3 O O H O CH 3 zidovudine (ZDV) H 2 CH 3 H 3 C O O CH 3 O O O P O O O CH 3 O O CH 3 O H 2 O HO S lamivudine (3TC) O H 2 O HO S F O H 2 HO O H 2 amdoxovir (DAPD) HO O O H O CH 3 stavudine (d4t) tenofovir (TDF) emtricitabine (FTC)
12 ucleoside/tide Analogs: Toxicity zidovudine GI, anemia, leukopenia, myositis didanosine P, pancreatitis,, diarrhea zalcitabine P, aphthous ulcers stavudine P lamivudine, emtricitabine (uncommon) abacavir GI, hypersensitivity reaction, rash tenofovir (uncommon) nucleosides as a class lactic acidosis with hepatic steatosis DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
13 ucleoside/tide Analogs: Toxicity Lactic Acidosis/hepatic steatosis Chronic compensated hyperlactatemia Incidence of severe, decompensated lactic acidosis with hepatomegaly and steatosis is rare 1.3 cases/1,000 person years of RTI exposure Must correlate blood lactate level with clinical presentation Treatment Cessation of HAART Supportive management
14 ewer formulations and once daily dosing. Didanosine EC- once daily dosing Stavudine XR-once daily dosing Lamivudine-300 mg po qd evirapine-400 mg po qd Atazanavir-400mg po qd Tenofovir-300 mg po qd Emtricitabine- 200mg po qd
15 ew nucleoside RTI Emtricitabine (Emtriva) One Capsule, Once daily 200mg po qd Chemically structure similar to Epivir (3TC) Clinical trials suggest that efficacy is similar to Epivir in treatment naive patients Likely not effective on lamivudine resistant virus Clinical activity against hepatitis B virus. Common side effects include headache, diarrhea, nausea and rash
16 ucleoside/tide Analogs: Selected Drug Interactions ZDV and ganciclovir: leukopenia ZDV and ribavirin: : antagonism in vitro ZDV and d4t: antagonism, decreased CD 4 ddi, ddc,, d4t: P-causing agents ddi and other pancreatitis-causing causing agents ddi and d4t: methadone decreases levels ddi and tenofovir: : increased ddi levels tenofovir and atazanavir: : decreased atazanavir levels must boost 300mg of atazanavir with 100mg of ritonavir DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
17 Structures of RTI - VP, DLV, EFV nevirapine (VP) efavirenz (EFV) delavirdine (DLV)
18 RTI: Toxicity Rash Majority are mild to moderate in severity, occuring within the first several weeks of therapy Most are confined to cutaneous reactions only- do not involve mucous membranes. VP 7%, DLV 4%, EFV 2% require discontinuation Stevens-Johnson syndrome reported Hepatic transaminase elevations VP (EFV, DLV) evirapine 400mg po qd Greater incidence of hepatoxicity than 200 mg po bid dosing CS symptoms (~50%) -- EFV Teratogenicity in monkeys -- EFV DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
19 RTI: Selected Drug Interactions CYP 3A4 effects (VP + EFV inducers; DLV inhibitor): rifampin/( /(rifabutin), ketoconazole, anticonvulsants, simvastatin/lovastatin lovastatin, astemizole/tefenadine tefenadine, midazolam/triazolam triazolam, ergotamines VP, EFV decrease methadone levels RTI-PI interactions VP decreases SQV, IDV, LPV DLV increases SQV, IDV EFV decreases SQV, IDV, APV, LPV Efavirenz decreases atazanavir: : must boost 300mg of atazanavir with 100mg of ritonavir DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
20
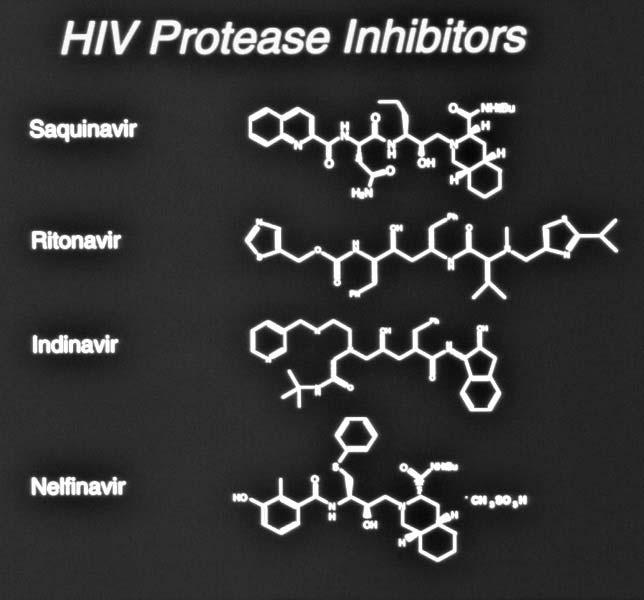
21
22 HIV Protease Inhibitors (2) amprenavir (APV) lopinavir (LPV) atazanavir (ATV)
23 PI: Toxicity SQV: GI RTV: GI, circumoral paresthesias IDV: nephrolithiasis,, incr. indirect bilirubin FV: diarrhea APV: GI, rash LPV: GI, diarrhea ATV: increased indirect bilirubin PIs as a class: increased hepatic transaminases, hyperglycemia, lipodystrophy and lipidemia, increased bleeding in hemophiliacs DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
24 ew PI formulation: fosamprenavir Lexiva: fosamprenavir prodrug of agenerase (amprenavir) Likely will not be effective in patients who are resistant to agenerase For PI experienced patient 700 mg fosamprenavir and 100mg ritonavir bid Advantage over amprenavir Easier dosing Decreased incidence of nausea, diarrhea, abdominal pain and rash
25 ew PI: Atazanavir Indicated both for PI naïve and PI experienced patients Once daily dosing; preferably taken with food to increase absorption Dosing PI naive: 400mg po qd PI experienced:300mg atazanavir/100mg norvir Boosted 300mg atazanavir/100mg norvir when administered with either efavirenz or tenofovir Side effects Increased indirect bilirubin May not increase triglycerides and LDL as do other protease inhibitors Impact on lipodystrophy and CAD not well known yet
26 PI: Selected Drug Interactions CYP 3A4 effects (RTV>>other PIs): rifampin/( /(rifabutin), ketoconazole,, anticonvulsants, simvastatin/lovastatin lovastatin, astemizole/tefenadine tefenadine, midazolam/triazolam triazolam, ergotamines,, St. John s Wort RTV increases levels of other PIs (1.5-40X) RTV, FV, APV lower oral contraceptive levels APV lowers methadone levels DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
27 Fuzeon:enfuvirtide enfuvirtide (T-20) Enfuvirtide (T-20) ew Category Fusion Inhibitors/entry inhibitors Indication Fuzeon binds to gp41 protein thus preventing viral binding and entry into T-cellsT For HAART experienced patient with resistant virus Injectable formulation with bid dosing Side effects: Skin irritation at injection site is most common Fatigue, insomnia and peripheral neuropathy
28
29 Combination Therapy: 3 vs. 2 Study ACTG 320 (=1156) Hammer, EJM 1997 Merck 035 (=97) Gulick, EJM 1997 Regimens ZDV/3TC vs. ZDV/3TC/IDV ZDV/3TC vs. IDV vs. ZDV/3TC/IDV Results (1 yr f/u) 3-drugs reduced AIDS/death by ~50% 3-drugs: ~80% HIV RA <500 cps/ml (compared to 30-45%) Agouron 511 (=297) Saag,, AIDS 2001 ZDV/3TC vs. ZDV/3TC/FV 3-drugs: ~75% HIV RA <400 cps/ml (compared to 37%) Combination Combination three three drug drug management management (HAART) (HAART) is is the the standard standard of of care care

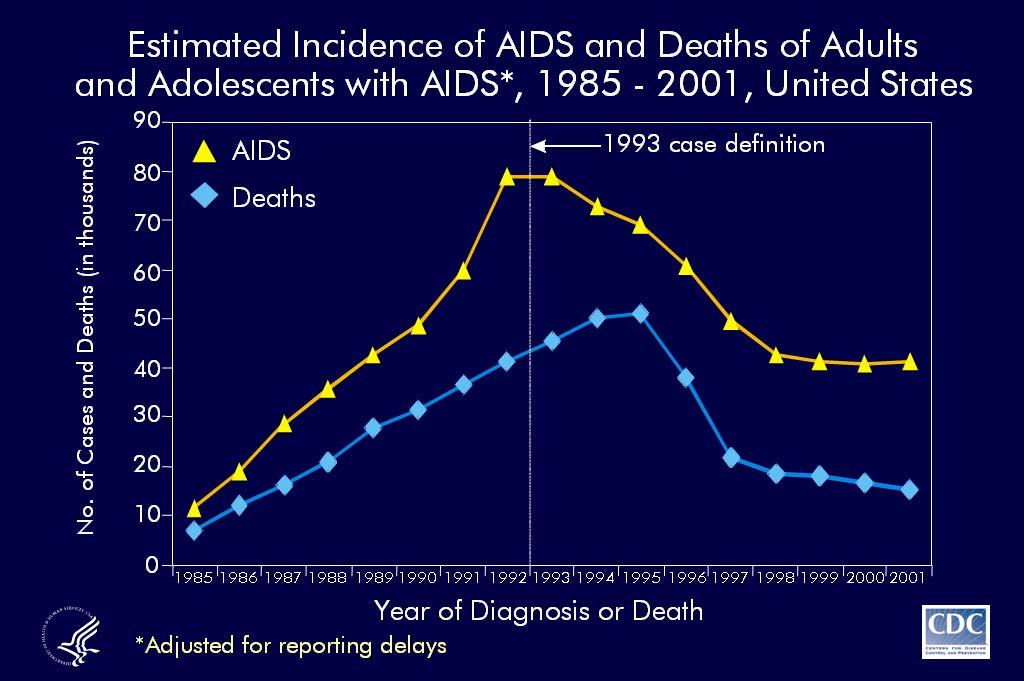
30 Population Population based based data data correlates correlates HAART HAART -PI -PI use use with with decreased decreased HIV HIV mortality mortality Palella et al EJM 1998;338:853
31 When To Start Treatment? Summary of Current Guidelines Guidelines DHHS: 7/14/03 update <www. nih.gov gov> IAS-USA: JAMA 2002 symptoms or CD4 <200 treat treat CD offer treatment consider treatment CD4 >350 defer if VL <55K; treat or defer if VL >55K consider if VL >50-100K
32 Early vs Late Treatment EARLY RX: HIV disease is progressive Rx decreases HIV RA (and resistance) and increases CD 4 (and immune function) 6+ years of virologic suppression demonstrated DELAYED RX: Risk of clinical progression low in early disease Practical factors (adherence, toxicity, quality of life outweigh benefits in early-disease) Long term effects unknown? Decrease transmission Preserve rx options Based on DHHS Guidelines 11/10/03 <www. DHHS Guidelines 11/10/03 <
33 Goal of Antiretroviral Therapy To suppress HIV RA (viral load level) as low as possible, for as long as possible To preserve or enhance immune function To delay clinical progression of HIV disease
34 DHHS Treatment Guidelines: Recommended Initial ART RTI-based regimens Preferred: ZDV (or TDF or d4t) + 3TC + EFV (except for pregnant women) Alternatives: ddi + 3TC + EFV (except for pregnant women) ZDV or d4t or ddi + 3TC + VP PI-based regimens Preferred: ZDV (or d4t) + 3TC + LPV/r Alternatives: ZDV (or d4t) + 3TC +APV/r, IDV, IDV/r, FV, or SQV/r DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
35 DHHS Treatment Guidelines: Triple RTI Regimen A 3 RTI regimen Abacavir+ Zidovudine+ + (or Stavudine) ) + Lamivudine Should only be used when an RTI-based or PI-based regimen cannot or should not be used as initial Rx eg.- drug-drug interactions; regimen complexity Randomized clinical trial comparing triple RTI vs PI-based regimens: Substantially higher rate of early virologic non-response was seen in the 3-RTI 3 arm. Tenofovir/abacavir abacavir/lamivudine or tenofovir/didanosine didanosine/lamivudine should not be used as a sole antiretroviral agent for naïve or treatment experienced patients early virologic non-response DHHS DHHS Guidelines Guidelines 11/10/03 11/10/03 < < nih.gov
36 DHHS Treatment Guidelines: ot Recommended Single-drug therapy (monotherapy( monotherapy): not potent, rapid resistance Two-drug therapy: rapid development of resistance Certain nucleoside pairs and antiretroviral components: d4t + ZDV: antagonistic d4t + ddc: : additive peripheral neuropathy d4t + ddi: : additive peripheral neuropathy Emtricitabine+lamivudine lamivudine: : similar resistance profile; no potential benefit Protease inhibitors Atazanavir+indinavir indinavir: : potential additive hyperbilirubinemia Saquinavir hard gel capsule; poor bioavailability (4%) 3 RTI regimens containing abacavir+tenofovir tenofovir+lamivudine or didanosine+tenofovor tenofovor+lamivudine Hydroxyurea: : promotes toxicity of didanosine,, increased peripheral neuropathy and pancreatitis In pregnancy: d4t + ddi (lactic acidosis) ; EFV (teratogenic( teratogenic); APV solution DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
37 What about Once Daily Dosing? ucleoside/ucleotide Analogues onnucleoside Reverse Transcriptase Inhibitors Protease Inhibitors Didanosine (enteric-coated) Efavirenz Amprenavir/ritonavir Emtricitabine evirapine Atazanavir Lamivudine Saquinavir/ritonavir Stavudine (extended-release) Tenofovir M ost of these medications have been studied in combination with twice-daily drugs, but have not been studied as components of an entirely once-daily regimen. One triple nucleoside regimen, abacavir + lamivudine + tenofovir has recently been found to have a high rate of virologic failure and should be avoided.
38 What about Once Daily Dosing? few efficacy studies of once-daily antiretroviral combinations have been conducted most are small and nonrandomized and must therefore be interpreted with caution regimens most thoroughly studied contain didanosine, efavirenz,, and lamivudine or emtricitabine didanosine + emtricitabine** + efavirenz ddi 400 mg (wt >= 60 kg), FTC 200 mg, EFV 600 mg QD RCT (compared with ddi/efv + d4t [immediaterelease, BID]); blinded to FTC and d4t 571 (286 on this regimen) Treatment naive Viral load 4.9 log10 copies/ml; CD4 = 288 cells/mm 3 60 weeks At 24 weeks, viral load <50 in 81%, compared to 70% in d4t arm. At 60 weeks, virologic failure in 7% versus 15% of d4t arm (by KM probability). 163 Better virologic and CD4 response and fewer adverse events in FTCcontaining regimen Largest RCT of a oncedaily regimen [12, 14] Once Once Daily Daily Dosing Dosing has has not not been been extensively extensively studied studiedand and these these are are not not regimens regimens of of choice choice by by DHHS DHHS guidelines. guidelines.
39 Once Daily Dosing Caveats: Paucity of long-term clinical trials with comparison to potent twice daily regimens Caveat-consequences of a missed dose: May result in inadequate drug exposure over a defined time period Consequent higher probability for development of drug resistance
40 DHHS Monitoring Guidelines Monitoring CD 4 cell counts When to measure baseline (at time of diagnosis, 2 specimens) ongoing evaluations every months Treatment decisions based on trend over time (at least 2 values) Significant change is >30% of absolute CD 4 value (or >3% of CD 4 percentage) DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
41 DHHS Monitoring Guidelines Monitoring viral load When to measure at baseline (2 specimens, weeks apart) prior to initiation of antiretroviral rx 2-88 weeks after initiation of rx ongoing evaluations every months Do not measure within weeks of acute illness or immunization Minimum sign. change is 3-fold 3 or 0.5 log DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
42 Clinical Cohort Studies: Virologic Failure Rates Cohort Amsterdam Wit, JID 99 Cleveland Valdez, Arch IM 99 Hopkins Lucas, Ann IM 99 Swiss Ledergerber,, Lancet 99 UCSF Deeks,, AIDS (% above LD, time) 40%, 48 wks 53%, 1 yr 63%, 1 yr 38%, 2 yrs 50%, 48 wks Incidence Incidence of of virologic virologic failure failure is is not not trivial! trivial!
43 Clinical Cohort Studies: Virologic Failure Rates 2002 ART Cohort collaboration 13 HIV clinical cohort studies 10 Europe, 2 Canada, 1 US individuals starting >3 3 drug ART 73% had HIV RA <400 cpm at 6 months Chene, et al., TuOrB1140, XIV AIDS Conf. 2002
44 Treatment Regimen Failure Virologic failure ot achieving HIV RA <400 cpm by wk 24 or <50 cpm by wk 48 After virologic response, repeated detection of viremia Immunologic failure Failure to increase CD4 count by cells over the first year of therapy or decrease to below baseline Clinical failure Occurrence or recurrence of HIV-related events DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
45 Why Does Treatment Fail Patients? Adherence Complicated regimens, heavy pill burden, toxicity Baseline resistance or cross-resistance resistance Use of less potent antiretroviral regimens Sequential monotherapy Drug levels and drug interactions Tissue reservoir penetration Patient not ready to take antiretrovirals
46 HIV Drug Resistance Pre-exists exists HIV genome contains 10,000 nucleotides Mutation rate of HIV is ~3 X billion virions produced daily Therefore all single (and many double) mutations are produced daily Leads to extensive viral diversity
47 HIV Drug Resistance Clinical resistance Follow HIV RA on antiretroviral therapy Genotypic resistance Perform in vitro assay to assess substitutions in viral genetic sequence; correlate with drug resistance Phenotypic resistance Perform in vitro assay to assess growth of viral strain in the presence of antiretroviral drugs
48 Prospective Resistance Studies Study Duration Design Change in VL (log cps/ml) VIRADAPT Durant Lancet wks geno vs SOC 1.2 vs 0.7* GART Baxter AIDS wks geno vs SOC 1.2 vs 0.6* ARVAL Meynard AIDS 2002 VIRA3001 Cohen, AIDS wks 16 wks geno vs pheno vs SOC pheno vs SOC 1.0 vs 1.0 vs vs 0.9* HAVAA 274 Tural,, AIDS 2002 SOC = standard of care 12 wks geno vs SOC 1.5 vs 1.2* * = p <0.05
49 Reduced Susceptibility (>10 Fold) Percent Primary HIV infection / 10 U.S. cities RTI RTI PI The The proportion proportion of of non-susceptible non-susceptible HIV HIV isolates isolates is is increasing. increasing. Year = Little, et al. EJM 2002;347:385.
50 DHHS Monitoring Guidelines Use of drug resistance assays Recommended virologic failure on rx suboptimal HIV RA suppression after starting rx acute HIV infection Consider chronic HIV infection prior to starting rx ot usually recommended after discontinuation of drugs HIV RA <1000 copies/ml DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
51 Current Approach to Salvage Rx Review antiretroviral history; assess adherence, tolerability, and PK issues Distinguish first/second from multiple failures Perform resistance testing while on drugs Identify susceptible drugs/drug classes Consider novel strategies (PK enhancement with RTV; multidrug regimens) Consider newer agents through expanded access or clinical trials Design a regimen with >3 3 active drugs (if possible) DHHS Guidelines 11/10/03 < aidsinfo.nih.gov>
52 Antiretroviral Rx: Conclusions Antiretroviral rx suppresses HIV RA, improves immune fx,, decreases disease progression and prolongs survival. The optimal time to begin therapy is not clear. The optimal initial rx is not clear, but there are effective combination regimens available. First-line rx fails in 10-60% of patients. Resistance testing demonstrates benefits in selecting antiretroviral therapy. There are a number of new drugs in development. Further research is needed.
53
54 Question 1 Emtricitabine (FTC) is similar in both structure and efficacy to which antiretroviral? A. Stavudine B. elfinavir C. Tenofovor D. Lamivudine
55 Question 2 Which would be a DEFIITE indication for initiating antitretroviral therapy as per DHHS guidelines? A. Asymptomatic, CD4>250 but <350, VL > 55,000 B. Asymptomatic, CD4<200, VL=30,000 C. Asymptomatic, CD4>350, VL>55,000 D. Asymptomatic, CD4>350, VL<55,000
56 Question 3 The most common side effect of the fusion inhibitor T-20 T (enfuvirtide( enfuvirtide) ) is: A. Diarrhea B. CS side effects- vivid dreams C. Skin irritation at injection site D. Hepatic steatosis and lactic acidosis
57 Question 4 As per the DHHS guidelines, when is HIV resistance testing not recommended? A. virologic failure while on treatment B. suboptimal HIV RA suppression after starting rx C. acute HIV infection D. HIV RA <1000 copies/ml
58 Question 5 Which most accurately describes the class level TOXICITY of protease inhibitors? A. Bone marrow suppression, anemia B. Increased hepatic transaminases, hyperglycemia, lipodystrophy and lipidemia, increased bleeding in hemophiliacs. C. Lactic acidosis and hepatic steatosis D. Rash and CS side effects (vivid dreams)
59 Answers Question 1: D Question 2: B Question 3: C Question 4: D Question 5: B
Medscape's Antiretroviral Pocket Guide for the Treatment of HIV Infection
 Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
0.14 ( 0.053%) UNAIDS 10% (94) ( ) (73-94/6 ) 8,920
 UNAIDS 10% (94) ( ) (73-94/6 ) 8,920") 0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
Treatment strategies for the developing world
 David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
Quick Reference Guide to Antiretrovirals. Guide to Antiretroviral Agents
 Author: Malte Schütz, MD June 1, 2002 Quick Reference Guide to Antiretrovirals Regular updates to this publication are posted on the Medscape Web site at http://hiv.medscape.com/updates/quickguide. Please
Author: Malte Schütz, MD June 1, 2002 Quick Reference Guide to Antiretrovirals Regular updates to this publication are posted on the Medscape Web site at http://hiv.medscape.com/updates/quickguide. Please
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care
 Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Structured Treatment Interruption in HIV Positive Patients. Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007
 Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 03/07/18 SECTION: DRUGS LAST REVIEW DATE: 02/19/19 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
Criteria for Oral PrEP
 Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
Update on Antiretroviral Treatment for HIV Infection 2008
 Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
2 nd Line Treatment and Resistance. Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012
 2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Somnuek Sungkanuparph, M.D.
 HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV - Life cycle. HIV Life Cyle
 Human Immunodeficiency Virus Retrovirus - integrated into host genome ne single-strand RA 7,000 bases HIV1 > HIV2 > HIV0 Pathology Destruction of CD4+ T lymphocytes Loss of immune function pportunistic
Human Immunodeficiency Virus Retrovirus - integrated into host genome ne single-strand RA 7,000 bases HIV1 > HIV2 > HIV0 Pathology Destruction of CD4+ T lymphocytes Loss of immune function pportunistic
HIV and AIDS. Shan Nanji
 HIV and AIDS Shan Nanji HIV 2 Description: Enveloped Positive Sense HIV 3 Structural Genes: Cleavage of gp160 leads to formation of ENV: Gp120: attachment to host CD4 T Cell Gp41: GAG (p24) Capsid protein
HIV and AIDS Shan Nanji HIV 2 Description: Enveloped Positive Sense HIV 3 Structural Genes: Cleavage of gp160 leads to formation of ENV: Gp120: attachment to host CD4 T Cell Gp41: GAG (p24) Capsid protein
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
HIV medications HIV medication and schedule plan
 Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Antiretroviral Therapy
 Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
Treatment experience in South Africa. Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand
 Treatment experience in South Africa Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand Overview South African Prevalence Adherence Combination ddi + d4t Nevirapine Hepatotoxicity
Treatment experience in South Africa Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand Overview South African Prevalence Adherence Combination ddi + d4t Nevirapine Hepatotoxicity
HIV MEDICATIONS AT A GLANCE. Atripla 600/200/300 mg tablet tablet daily. Complera 200/25/300 mg tablet tablet daily
 HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
C h a p t e r 5 5 HIV Therapy Where are We Now?
 C h a p t e r 5 5 HIV Therapy Where are We Now? AK Tripathi Professor of Medicine, Physician & Haemato-Oncologist, King George s Medical College, Lucknow Introduction Human Immunodeficiency Virus type
C h a p t e r 5 5 HIV Therapy Where are We Now? AK Tripathi Professor of Medicine, Physician & Haemato-Oncologist, King George s Medical College, Lucknow Introduction Human Immunodeficiency Virus type
Terapia antirretroviral inicial y de rescate: Utilidad actual y futura de nuevos medicamentos
 Terapia antirretroviral inicial y de rescate: Utilidad actual y futura de nuevos medicamentos (Antiretroviral Therapy Present and Future Prospects of Antiretroviral Drugs in Initial and Salvage Therapy)
Terapia antirretroviral inicial y de rescate: Utilidad actual y futura de nuevos medicamentos (Antiretroviral Therapy Present and Future Prospects of Antiretroviral Drugs in Initial and Salvage Therapy)
HIV epidemiology since HIV in the United States. HIV Transmission
 HIV epidemiology since 1999 8% increase in HIV diagnoses Men who have sex with men (MSM) increased 14% Heterosexual increased 10% IVDU decrease about 30% Young Black MSM 15% incidence HIV in the United
HIV epidemiology since 1999 8% increase in HIV diagnoses Men who have sex with men (MSM) increased 14% Heterosexual increased 10% IVDU decrease about 30% Young Black MSM 15% incidence HIV in the United
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV
 POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications
 and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications") Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Management of NRTI Resistance
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Management of NRTI Resistance David Spach, MD Principal Investigator, NW AETC Professor of Medicine, Division of Infectious Diseases University of Washington
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Management of NRTI Resistance David Spach, MD Principal Investigator, NW AETC Professor of Medicine, Division of Infectious Diseases University of Washington
When to Start ART. Reduction in HIV transmission. ? Reduction in HIV-associated inflammation and associated complications» i.e. CV disease, neuro, etc
 When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
Nobel /03/28. HIV virus and infected CD4+ T cells
 Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
MDR HIV and Total Therapeutic Failure. Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007
 MDR HIV and Total Therapeutic Failure Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007 Objectives Case study Definitions Fitness Pathogenesis of resistant virus
MDR HIV and Total Therapeutic Failure Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007 Objectives Case study Definitions Fitness Pathogenesis of resistant virus
National AIDS Treatment Advocacy Project
 National AIDS Treatment Advocacy Project T-20 (first fusion inhibitor) Nelfinavir 12 month data Latent HIV reservoir (integrated proviral DNA), CSF and protease inhibitors: preliminary data (ritonavir/saquinavir
National AIDS Treatment Advocacy Project T-20 (first fusion inhibitor) Nelfinavir 12 month data Latent HIV reservoir (integrated proviral DNA), CSF and protease inhibitors: preliminary data (ritonavir/saquinavir
ANTIRETROVIRAL TREATMENTS (Part 1of
 CCR5 CO-RECEPTOR ANTAGONISTS maraviroc (MVC) Selzentry 25mg, 75mg, FUSION INHIBITORS 20mg/mL ANTIRETROVIRAL TREATMENTS (Part 1of 5) oral soln enfuvirtide (ENF, T-20) Fuzeon 90mg/mL pwd for SC inj after
CCR5 CO-RECEPTOR ANTAGONISTS maraviroc (MVC) Selzentry 25mg, 75mg, FUSION INHIBITORS 20mg/mL ANTIRETROVIRAL TREATMENTS (Part 1of 5) oral soln enfuvirtide (ENF, T-20) Fuzeon 90mg/mL pwd for SC inj after
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Pharmacology Update Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005
 Pharmacology Update 2005 Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005 I m having a Maalox moment!!! Gastric Hypoacidity in HIV 20% incidence in HIV (unrelated to CD 4 ) Antacids, ddi tablets, H2-blockers
Pharmacology Update 2005 Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005 I m having a Maalox moment!!! Gastric Hypoacidity in HIV 20% incidence in HIV (unrelated to CD 4 ) Antacids, ddi tablets, H2-blockers
THE HIV LIFE CYCLE. Understanding How Antiretroviral Medications Work
 THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
Anumber of clinical trials have demonstrated
 IMPROVING THE UTILITY OF PHENOTYPE RESISTANCE ASSAYS: NEW CUT-POINTS AND INTERPRETATION * Richard Haubrich, MD ABSTRACT The interpretation of a phenotype assay is determined by the cut-point, which defines
IMPROVING THE UTILITY OF PHENOTYPE RESISTANCE ASSAYS: NEW CUT-POINTS AND INTERPRETATION * Richard Haubrich, MD ABSTRACT The interpretation of a phenotype assay is determined by the cut-point, which defines
This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts
 1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
When to start, when to switch ART and monitoring of ARV side effects
 When to start, when to switch ART and monitoring of ARV side effects Thanomsak Anekthananon, MD Faculty of Medicine Siriraj Hospital September 4, 2009 Recommended Websites Free e-book: HIV Medicine 2007
When to start, when to switch ART and monitoring of ARV side effects Thanomsak Anekthananon, MD Faculty of Medicine Siriraj Hospital September 4, 2009 Recommended Websites Free e-book: HIV Medicine 2007
Selecting an Initial Antiretroviral Therapy (ART) Regimen
 Regimen") Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
HIV Drugs and the HIV Lifecycle
 HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
Antiretroviral Dosing in Renal Impairment
 Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
104 MMWR December 17, 2004
 104 MMWR December 17, 2004 TABLE 8. Substantial pharmacokinetic drug-drug interactions for drugs used in the treatment of opportunistic Drugs Interacting with Mechanism/effects Recommendations Acyclovir
104 MMWR December 17, 2004 TABLE 8. Substantial pharmacokinetic drug-drug interactions for drugs used in the treatment of opportunistic Drugs Interacting with Mechanism/effects Recommendations Acyclovir
ANTIRETROVIRAL TOXICITY Strategies for prevention and treatment
 ANTIRETROVIRAL TOXICITY Strategies for prevention and treatment Francisco Antunes Professor da Faculdade de Medicina da Universidade de Lisboa e Director do Serviço de Doenças Infecciosas do Hospital de
ANTIRETROVIRAL TOXICITY Strategies for prevention and treatment Francisco Antunes Professor da Faculdade de Medicina da Universidade de Lisboa e Director do Serviço de Doenças Infecciosas do Hospital de
Viral Resistance with Topical RT-Microbicides. Ian McGowan MD PhD FRCP David Geffen School of Medicine Los Angeles
 Viral Resistance with Topical RT-Microbicides Ian McGowan MD PhD FRCP David Geffen School of Medicine Los Angeles verview What antiretrovirals (ARV) are being considered as candidate microbicides? How
Viral Resistance with Topical RT-Microbicides Ian McGowan MD PhD FRCP David Geffen School of Medicine Los Angeles verview What antiretrovirals (ARV) are being considered as candidate microbicides? How
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop
 HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
Distribution and Effectiveness of Antiretrovirals in the Central Nervous System
 Distribution and Effectiveness of Antiretrovirals in the Central Nervous System Scott Letendre, MD Associate Professor of Medicine HIV Neurobehavioral Research Center and Antiviral Research Center University
Distribution and Effectiveness of Antiretrovirals in the Central Nervous System Scott Letendre, MD Associate Professor of Medicine HIV Neurobehavioral Research Center and Antiviral Research Center University
A Genetic Test to Screen for Abacavir Hypersensitivity Reactions
 The Future of Pharmacogenetics in HIV Clinical Care A Genetic Test to Screen for Abacavir Hypersensitivity Reactions Evan Collins & Misty Bath CANAC/ACIIS 15 th Annual Conference Vancouver, BC April 2007
The Future of Pharmacogenetics in HIV Clinical Care A Genetic Test to Screen for Abacavir Hypersensitivity Reactions Evan Collins & Misty Bath CANAC/ACIIS 15 th Annual Conference Vancouver, BC April 2007
Approach for the Newly Diagnosed HIV Positive Patient
 Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV infection and Primary Care. HIV Care in /30/2013. It s not the AIDS of 85. Stephen Raffanti MD MPH Vanderbilt University School of Medicine
 HIV infection and Primary Care Stephen Raffanti MD MPH Vanderbilt University School of Medicine HIV Care in 2013 Chronic lifelong treatment with all the associated issues: medication tolerability medication
HIV infection and Primary Care Stephen Raffanti MD MPH Vanderbilt University School of Medicine HIV Care in 2013 Chronic lifelong treatment with all the associated issues: medication tolerability medication
WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION
 WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION A1. PARTICIPANT ID: ENTER NUMBER HERE - - - ONLY IF ID LABEL IS NOT AVAILABLE A2. VISIT #: A3. VERSION DATE: 1 0 /
WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION A1. PARTICIPANT ID: ENTER NUMBER HERE - - - ONLY IF ID LABEL IS NOT AVAILABLE A2. VISIT #: A3. VERSION DATE: 1 0 /
The advent of protease inhibitors (PIs) as PROCEEDINGS CLINICAL EXPECTATIONS OF EFFICACY: PROTEASE INHIBITOR POTENCY * Benjamin Young, MD, PhD
 as PROCEEDINGS CLINICAL EXPECTATIONS OF EFFICACY: PROTEASE INHIBITOR POTENCY * Benjamin Young, MD, PhD") CLINICAL EXPECTATIONS OF EFFICACY: PROTEASE INHIBITOR POTENCY * Benjamin Young, MD, PhD ABSTRACT Tremendous strides were made in reducing the morbidity and mortality associated with HIV infection with
CLINICAL EXPECTATIONS OF EFFICACY: PROTEASE INHIBITOR POTENCY * Benjamin Young, MD, PhD ABSTRACT Tremendous strides were made in reducing the morbidity and mortality associated with HIV infection with
THE STAGING AND MEDICATION OF HIV INFECTION
 Supplement A: WHO CLINICAL STAGING THE STAGING AND MEDICATION OF HIV INFECTION Clinical Stage 1 Clinical Stage 2 Clinical Stage 3 Clinical Stage 4 Asymptomatic Persistent generalized lymphadenopathy Moderate
Supplement A: WHO CLINICAL STAGING THE STAGING AND MEDICATION OF HIV INFECTION Clinical Stage 1 Clinical Stage 2 Clinical Stage 3 Clinical Stage 4 Asymptomatic Persistent generalized lymphadenopathy Moderate
/AIDS HIV/ HIV Overview. Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program
 /AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
/AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
HIV/AIDS Update 2007
 HIV/AIDS Update 2007 Joanne J. Orrick, Pharm.D., BCPS Clinical Assistant Professor University of Florida Faculty, Florida/Caribbean AIDS Education and Training Center orricjj@ufl.edu www.faetc.org orricjj@ufl.edu
HIV/AIDS Update 2007 Joanne J. Orrick, Pharm.D., BCPS Clinical Assistant Professor University of Florida Faculty, Florida/Caribbean AIDS Education and Training Center orricjj@ufl.edu www.faetc.org orricjj@ufl.edu
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Concomitant antiretroviral therapy : Avifanz must be given in combination with other antiretroviral medications.
 Avifanz Tablet Description Avifanz is the brand name for Efavirenz. Efavirenz, a synthetic antiretroviral agent, is a non-nucleoside reverse transcriptase inhibitor. While Efavirenz is pharmacologically
Avifanz Tablet Description Avifanz is the brand name for Efavirenz. Efavirenz, a synthetic antiretroviral agent, is a non-nucleoside reverse transcriptase inhibitor. While Efavirenz is pharmacologically
Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and
 Recommendations for Use of Antiretroviral s in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV-1 Transmission in the United States, June 23, 2004, CDC and updated
Recommendations for Use of Antiretroviral s in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV-1 Transmission in the United States, June 23, 2004, CDC and updated
European Guidelines. for the Clinical Management and Treatment of HIV Infected Adults
 European Guidelines for the Clinical Management and Treatment of HIV Infected Adults 2005 These Euroguidelines result from the comparison of guidelines from several European countries and from a discussion
European Guidelines for the Clinical Management and Treatment of HIV Infected Adults 2005 These Euroguidelines result from the comparison of guidelines from several European countries and from a discussion
Objectives. HIV Treatment in Recently In 1996 the introduction of protease inhibitors decreasing the death rate of those infected by 50%.
 Objectives Identify modes HIV transmission and methods of prevention. HIV Treatment in 2010 Lisa D. Inge, Pharm.D., BCPS, AAHIVE Assistant Director, Jacksonville Campus Clinical Assistant Professor University
Objectives Identify modes HIV transmission and methods of prevention. HIV Treatment in 2010 Lisa D. Inge, Pharm.D., BCPS, AAHIVE Assistant Director, Jacksonville Campus Clinical Assistant Professor University
TB/HIV Co-Infection. Tuberculosis and HIV
 TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
STRIBILD (aka. The Quad Pill)
") NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
Third Agent Advantages Disadvantages. Component Tenofovir/emtricitabine (TDF/FTC) 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily
 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily") Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
Recommendations of GESIDA/Spanish AIDS Plan on antiretroviral therapy in adults infected by the human immunodeficiency virus (Updated January 2007)
") Recommendations of GESIDA/Spanish AIDS Plan on antiretroviral therapy in adults infected by the human immunodeficiency virus (Updated January 2007) Expert Committee of GESIDA and the National AIDS Plan
Recommendations of GESIDA/Spanish AIDS Plan on antiretroviral therapy in adults infected by the human immunodeficiency virus (Updated January 2007) Expert Committee of GESIDA and the National AIDS Plan
Integrase Strand Transfer Inhibitors on the Horizon
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
June 2004 HIV/AIDS Update Part H02
 W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 June 2004 HIV/AIDS Update Part 2 707-000-04-006-H02 THIS LESSON, COMBINED WITH THE MAY 2004 LESSON, FULFILLS
W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 June 2004 HIV/AIDS Update Part 2 707-000-04-006-H02 THIS LESSON, COMBINED WITH THE MAY 2004 LESSON, FULFILLS
Occupational and Non- Occupational HIV Post-exposure Prophylaxis
 Occupational and Non- Occupational HIV Post-exposure Prophylaxis Amy V. Kindrick, MD, MPH National Clinicians Post-Exposure Prophylaxis Hotline (PEPline) University of California, San Francisco San Francisco
Occupational and Non- Occupational HIV Post-exposure Prophylaxis Amy V. Kindrick, MD, MPH National Clinicians Post-Exposure Prophylaxis Hotline (PEPline) University of California, San Francisco San Francisco
Efavirenz, stavudine and lamivudine
 efavirenz, stavudine, lamivudine: 1 efavirenz, stavudine and lamivudine First line ART treatment for HIV infection Efavirenz, stavudine and lamivudine efavirenz, stavudine, lamivudine: 2 Slide 1 Information
efavirenz, stavudine, lamivudine: 1 efavirenz, stavudine and lamivudine First line ART treatment for HIV infection Efavirenz, stavudine and lamivudine efavirenz, stavudine, lamivudine: 2 Slide 1 Information
Supplementary Figure 1. Gating strategy and quantification of integrated HIV DNA in sorted CD4 + T-cell subsets.
 Supplementary information HIV reservoir size and persistence are driven by T-cell survival and homeostatic proliferation. Chomont, N., M. El Far, P. Ancuta, L. Trautmann, F. A. Procopio, B. Yassine-Diab,
Supplementary information HIV reservoir size and persistence are driven by T-cell survival and homeostatic proliferation. Chomont, N., M. El Far, P. Ancuta, L. Trautmann, F. A. Procopio, B. Yassine-Diab,
July 2006 HIV/AIDS Update Part 2 Volume 28 Number 7. W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL
 W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 Jully 2006 HIV/AIDS Update Part 2 707-000-06-007-H02 IN THIS LESSON WE DISCUSS ANTIRETROVIRAL THERAPY, COMBINATION
W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 Jully 2006 HIV/AIDS Update Part 2 707-000-06-007-H02 IN THIS LESSON WE DISCUSS ANTIRETROVIRAL THERAPY, COMBINATION
NATAPNATIONAL. HIV 102: Care & Treatment AIDS TREATMENT ADVOCACY PROJECT. Origins of HIV. Table of Contents. National AIDS Treatment Advocacy Project
 National AIDS Treatment Advocacy Project HIV 102: Care & Treatment Written by: Jose Castro, MD University of Miami, Miller School of Medicine, Miami, FL Editorial Contributions by: Jules Levin 580 BROADWAY,
National AIDS Treatment Advocacy Project HIV 102: Care & Treatment Written by: Jose Castro, MD University of Miami, Miller School of Medicine, Miami, FL Editorial Contributions by: Jules Levin 580 BROADWAY,
PHARMACOKINETICS OF ANTIRETROVIRAL AND ANTI-HCV AGENTS
 8. PHARMACOKINETICS OF ANTIRETROVIRAL AND ANTI-HCV AGENTS David Burger José Moltó Table 8.1a: INFLUENCE OF FOOD ON ABSORPTION (AREA UNDER THE CURVE) OF ANTIRETROVIRAL AGENTS NUCLEOSIDE ANALOGUES NtRTI
8. PHARMACOKINETICS OF ANTIRETROVIRAL AND ANTI-HCV AGENTS David Burger José Moltó Table 8.1a: INFLUENCE OF FOOD ON ABSORPTION (AREA UNDER THE CURVE) OF ANTIRETROVIRAL AGENTS NUCLEOSIDE ANALOGUES NtRTI
TB Intensive Tyler, Texas December 2-4, Tuberculosis and HIV Co-Infection. Lisa Y. Armitige, MD, PhD. December 4, 2008.
 TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
HIV/AIDS HIV/AIDS: Outline. Morbidity and Mortality Weekly Report (MMWR)
") HIV/AIDS: Outline HIV/AIDS 2013 Roy M. Gulick, MD, MPH Professor of Medicine Chief, Division of Infectious Diseases Weill Medical College of Cornell University New York City January 31, 2013 Epidemiology
HIV/AIDS: Outline HIV/AIDS 2013 Roy M. Gulick, MD, MPH Professor of Medicine Chief, Division of Infectious Diseases Weill Medical College of Cornell University New York City January 31, 2013 Epidemiology
 Page 1 of 5 ENLGLISH / ESPAÑOL / PORTUGUÉS / FRANÇAIS Share 3 Drug Chart for HIV Treatment CURRENT EDITION ABOUT SENSE BACK ISSUES MSMGF HOME CONTACT US There are a number of antiretroviral (ARV) medications
Page 1 of 5 ENLGLISH / ESPAÑOL / PORTUGUÉS / FRANÇAIS Share 3 Drug Chart for HIV Treatment CURRENT EDITION ABOUT SENSE BACK ISSUES MSMGF HOME CONTACT US There are a number of antiretroviral (ARV) medications
Didactic Series. Update: 2012 HIV Treatment Guidelines. Daniel Lee, MD August 30, 2012
 Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Supplementary information
 Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
12th European AIDS Conference / EACS ARV Therapies and Therapeutic Strategies A CME Newsletter
 EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Sasisopin Kiertiburanakul, MD, MHS
 What s Newin Antiretroviral Therapy? Sasisopin Kiertiburanakul, MD, MHS Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Rotating RCPT,
What s Newin Antiretroviral Therapy? Sasisopin Kiertiburanakul, MD, MHS Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Rotating RCPT,
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
Treatment of respiratory virus infection Influenza A & B Respiratory Syncytial Virus (RSV)
") Treatment of respiratory virus infection Influenza A & B Respiratory Syncytial Virus (RSV) Amantadine and Rimantadine Use is limited to Influenza A infection. Very effective in preventing infection if
Treatment of respiratory virus infection Influenza A & B Respiratory Syncytial Virus (RSV) Amantadine and Rimantadine Use is limited to Influenza A infection. Very effective in preventing infection if
HIV Management Update 2015
 9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
YOU CAN NOW DOWNLOAD MISPLACED LESSONS FROM OUR WEBSITE (WWW.WFPROFESSIONAL.COM).
.") W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 June 2002 HIV/AIDS Update Part 2 707-000-02-006-H02 YOU CAN NOW DOWNLOAD MISPLACED LESSONS FROM OUR WEBSITE
W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 June 2002 HIV/AIDS Update Part 2 707-000-02-006-H02 YOU CAN NOW DOWNLOAD MISPLACED LESSONS FROM OUR WEBSITE
The New Agents: Management of Experienced Patients and Resistance. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 The New Agents: Management of Experienced Patients and Resistance Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine T.D. 45 year old man with HIV infection diagnosed in 2000 On multiple
The New Agents: Management of Experienced Patients and Resistance Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine T.D. 45 year old man with HIV infection diagnosed in 2000 On multiple
Pediatric Antiretroviral Resistance Challenges
 Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
HIV associated CNS disease in the era of HAART
 HIV associated CNS disease in the era of HAART CSF/CNS penetration and efficacy Acknowledgements Peter Portegies Department of Neurology, AMC Mark van der Valk Department of Internal Medicine/Infectious
HIV associated CNS disease in the era of HAART CSF/CNS penetration and efficacy Acknowledgements Peter Portegies Department of Neurology, AMC Mark van der Valk Department of Internal Medicine/Infectious