Ann Janssens, MD, PhD. Department of Hematology, UZ Leuven BHS course 8 november 2014
|
|
|
- Tyrone Casey
- 5 years ago
- Views:
Transcription


1 Ann Janssens, MD, PhD Department of Hematology, UZ Leuven BHS course 8 november 2014







2 The history of platelets, megakaryocytes and thrombopoietin



 Megakaryocyte")


3 Platelet homeostasis etpo Production Platelet Pool Normal platelet lifespan 9-10d Normal Splenic Destruction Platelet production: /d Platelet count: /µl Platelet Production Platelets/megakaryocyte Endogenous thrombopoietin (etpo) Megakaryocyte precursor Megakaryocyte Platelet 1 Kuter et al PNAS 91:11104, 1994; 2 Stoffel et al Blood 87:567, 1996; 3 Gurney et al Science 265:1445, 1994; 4 de Sauvage et al JEM 183:651, 1996


 JAK2 JAK2 Nuclear")

 Platelets Bone")
4 Thrombopoietin signaling and megakaryocyte maturation Thrombopoietin Pluripotent Progenitor Megakaryocyte Progenitor Mitotic Expansion TPO-R (Mpl) JAK2 JAK2 Nuclear Maturation (End mitosis) Cell membrane S T A T 5 P P P Cytoplasmic Maturation (Platelet Specific Granules) Platelets Bone Marrow Proplatelet Formations Peripheral Blood



5 Thrombopoietin production: constitutive or regulated?

6 Izak et al. F1000Prime reports, 2014


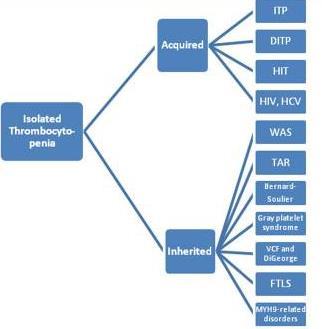
7 Peripheral destruction Autoimmune Primary ITP Secondary ITP Drug induced: HIT, Alloimmune: posttransfusion, neonatal Pregnancy induced TTP-HUS DIC Hemangiomas Insufficient production AA MDS Myelofibrosis Bone marrow invasion Bone marrow toxicity Megaloblastic anemia Hereditary disorders others Platelet sequestration due to hypersplenism Portal hypertension (cardiac, cirrhosis, V. Porta or V. Cava thrombosis Gaucher Myelofibrosis Viral infections Dilution due to massive transfusion
8 In vitro agglutination of platelets when blood is collected in EDTA tubes ( 2% of all thrombocytopenias detected on EDTA blood) Measure platelets on blood collected in citrate or heparine tubes Look for agregates on the peripheral blood smear


9
10 Personal and familial history Recent infections Vaccinations ( >MMR, < H. Influenzae, pneumococci, Hep B,..) Malignancies Pregnancy Recent travels Recent transfusions Alcohol abuse Dietary habits, beverages, herbal preparations Risk factors for HIV and viral hepatitis Medication: especially those started 1 to 2 weeks before the onset of thrombocytopenia, recent exposure to heparine
11 Clinical examination with special attention to: Bleeding symptoms: pecheciae, purpura, ecchymoses Lymphadenopathy Spleno-, hepatomegaly Skeletal abnormalities Dysmorphy Skin abnormalities
12 Complete blood count Isolated vs pancytopenia With neutrophilia or lymphocytosis Blood smear True vs pseudo Platelet morphology: giant platelets, vs microthrombocytes Toxic granulation in the neutrophils Pelger Huet, blasts Atypical lymphocytes Fragmentocytes Tear drops, nucleated red blood cells Additional investigations LDH Coombs, hapto, bilirubin Renal function Coagulation Liver function Virus serology, Bone marrow examination

13 Lacey et al, Semin Thromb Hemost, 1977

14 fatal haemorrhage if platelets < 30000/ l persistently age < 40y: 0,4%/y age 40-60y: 1,2%/y age > 60y: 13% /y Cohen et al, Arch Intern Med, 2000



15 Petechiae Purpura Bruises




16 Mucous membrane bleeding Epistaxis Gingival UG-GI tract Intracerebral bleeding



17


18
19 Dentistry: 10 à 20 x 10 9 /L Extractions: 30 x 10 9 /L Regional dental block: 30 x 10 9 /L Lumbar puncture: 50 x 10 9 /L GI endoscopy with biopsy: 20 x 10 9 /L Bronchoscopy: 20 x 10 9 /L ( 50 if also biopsy) Organ biopsy: 50 x 10 9 /L (lower for bone biopsy) Minor surgery: 50 x 10 9 /L Major surgery: 80 x 10 9 /L Epidural: 80 x 10 9 /L British Committee for Standards in Haematology General Haematology Task Force. Br J Haematol. 2003;120: Webert KE, et al. Blood. 2003;102:
20



21 A. Janssens, C. Lambert, G. Bries, A. Bosly, D. Selleslag, Y. Beguin Belgian Journal of Hematology. 2013;4(1) (March 2013)


22 Isolated thrombocytopenia Threshold platelets for ITP-diagnosis /µl instead of /µl Normal complete blood count and peripheral smear Avoid Purpura: bleeding symptoms frequently absent or minimal at the onset of disease Rodeghiero et al, Blood 2009;113:

23 Basic evaluation Potential utility Unproven benefit Personal and family history Clinical examination Full blood count with reticulocytes and Coombs Peripheral blood film!!! Immunoglobulins Blood group? HIV, hep C, H pylori? Bone marrow in selected patients Antiplatelet antibodies Antiphospholipid antibodies Thyroid function and antithyroid antibodies pregnancy test Antinuclear antibodies PCR for CMV and parvovirus Hep B Chest radiograph Abdominal ultrasound Biological fitness Thrombopoitin Reticulated platelets Bleeding time Platelet survival time Serum complement MANDATORY!!!
24 Primary: no obvious initiating and/or underlying cause Avoid idiopathic SLE 5% APS 2% CVID 1% Primary 80% Cines DB, et al. Blood. 2009;113: CLL 2% Evan s 2% ALPS, post-tx 1% HIV 1% Hep C 2% H. pylori 1% Postvaccine 1% Misc systemic infection 2%
25 25% develop thrombocytopenia 15-25% of ITP pat are pos for ANF Bleeding risk? Activity of SLE? Vasculitis? Severe thr-penia with active SLE: treat SLE Severe thr-cytopenia without active SLE: treat as primary ITP; rituximab; splenectomy if refractory thrombopenia with thrombotic events and poor outcome of pregnancy Lupus anticoagulans and anticardiolipin AB pos +/- 40 (10-70)% of pat with ITP has APLAs treat as primary ITP, also good outcome with rituximab Aspirin? (hypothyroidism,thyrotoxicosis) 25-50% ITP patients has antithyroid AB Control of the underlying thyroid disease 10% develop ITP with or without AIHA Treat as primary ITP Avoid immunosuppressive agents rituximab
26 thrombocytopenia 1 to 4 weeks after an acute infection with mumps, rubella, EBV, CMV, appears sudden and can be severe remits mostly in 2 to 4w HIV, hep C, H. Pylori insidious onset, no tendency to remit spontaneously Stasi, Sem Hematol, 2009
27 US: prevalence of anti-hcv AB: 2% Platelets <150000/μl: 41% chronic Hep C (19% in chronic hep B) Platelets <50000/μl: +/- 9% chronic hep C Associated with cryoglobulins and anticardiolipin AB Bleeding symptoms at higher platelet counts Treatment Interferon-α with antiviral treatment Corticosteroids ( try to avoid) Cavé: increase in viral load, elevation in transaminases IGIV Splenectomy TPO-R agonists Nagamine et al. J Hepatol 1996 Rajan et al. Br J Haematol 2005 Stasi, Sem Hematol, 2009
28 Before HAART: 5 to 30% of HIV + patients develop thrombocytopenia (<150000/μl) Incidence of thrombocytopenia higher with an increase in immunosuppression If diagnosed before the stage of AIDS: thrombocytopenia mostly mild (can have additional bleeding problems: hemophilia, hep C, liver disease in drug addicts, ) Treatment Antiretroviral therapy ( can take weeks) Corticosteroids, IGIV Splenectomy TPO-R agonists Stasi, Sem Hematol, 2009
29 Prevelance depends on socio-economic conditions Prevalence in adult ITP: 20-80% (Japan 70%, Italy 50%, US 22%) Diagnostic methods: urea breath test and stool Ag test: highest sensitivity and specificity Association with dyspepsia???? Older than ITP without H. Pylori Eradication therapy: ORR 50 (14-100) % ( higher ORR in Japan), persistent response 70% Higher ORR in ITP with a short duration and a higher platelet count >30000 Platelet responses after 3d to 24 w (2 weeks in Italian trial) No responses to eradication therapy in pat H. Pylori neg Stasi, Sem Hematol, 2009
30 AITP can occur in all lymphoproliferative disorders However more frequent with (1-5%) (can occur at any time in the course of CLL), remission) 20%(mild)) (0,2-1%) (can occur at any time in the course of Ho, also in 1(severe)- Liebman, Sem Hematol,2009
31 Corticosteroids, IGIV, splenectomy Rituximab monotherapy or in combination with cyclophosphamide-dexamethasone Alemtuzumab Cyclosporine, Cellcept TPO-R agonists Ho treatment if active disease Corticosteroids, IGIV, splenectomy azathioprine Cytotoxic treatment against the LGL-clone Cyclosporine Alemtuzumab Corticosteroids, IGIV Rituximab,cellcept, SCT Liebman, Sem Hematol,2009
32 Eliminate the trombocytopenia inducing drug Heparin Quinine, tonic water Valproic acid Non steroidal inflammatory agents
33 HAT: 10-30%: binding of heparin to platelets with platelet aggregation (non-immune) ( first days of treatment, > 80000/ l, no bleeding or thrombosis, resolves even with continuing heparin) HIT: 5% if IV, <1% with LMWH, thrombocytopenia moderate to severe, 30-75% has a thrombotic event, venous predominance (2.5/1), late onset till 20d after stop heparin

34
35 Discontinue all heparin products Alternative non heparin anticoagulants Direct thrombin inhibitors Argatroban Lepirudin Bivalirudin Factor X inhibitors (Arixtra) Vit K antagonists: NO Novel anticoagulants (Pradaxa, Xarelto, Eliquis) Heparinoids Danaparoid ( antix and anti-ii activity) (Orgaran)
36 Non immune: directly toxic to megakaryocytes Linezolid ( >10D 32%) Immune: after 1 to 2 weeks, severe bleeding 5 different mechanisms

proteïne :drug(metaboliet) :PF-4 :neo-epitope Aster et al.")
37 Drug-induced ITP Mechanisms: 1 auto-antibodies 2 neo-epitope 3 hapteen gold 1 2 penicillins abciximab 4 drug specific 5 quinine type 6 Immune complex 6 Kinine, NSAIM, AB, anticonvulsiva heparin FAB FC :immuunglobuline :(glyco)proteïne :drug(metaboliet) :PF-4 :neo-epitope Aster et al., NEJM 2007
38 Autologeous Allogeneic Post liver transplantation


39 Active bleeding OR platelets <10000/ l treatment is obligatory No or mild bleeding AND platelets / l treatment is a potential option ( evaluation of pat characteristics) No bleeding AND platelets >30000/ l no need for treatment unless special circumstances Stasi, Eur J Haematol, 2009
 Uremia")

40 Platelet count Previous major bleeding Age Life style: sedendary (office workers) vs active ( physical jobs), contact sports Additional risk factors for bleeding Platelet dysfunction or hemostatic defect (clopidogrel, ASA, po anticoagulantia) Uremia Untreated or poorly controled hypertension, Aneurysms Fever or Infections Chronic liver disease or alcoholism History of peptic ulcer Tolerance of expected adverse events of treatment Medical interventions that may cause bleeding Accessibily of care Patient s preferences ( anxiety, )



41 Minimize bleeding symptoms or risk of bleeding Decrease activity restrictions and improve QOL Minimize exposure to potentially toxic therapy
 Persistent ITP (3 à12m) ( time in")
 Rodeghiero et al, Blood")
42 Newly diagnosed ITP (<3m) (retrospective diagnosis) Persistent ITP (3 à12m) ( time in which spontaneous remission can occur) Chronic ITP (>12m) Rodeghiero et al, Blood 2009:113;




43


44 Table 2: Corticosteroids



45 : vomiting 3x/d since 1week; blood exam solitary thrombocytopenia: 12000/µl; not pregnant Some petechiae legs, 1 bruise, last period more explicit; no mucosal bleeding Corticosteroids IV because of the vomiting with a rapid rise of platelets, exacerbation of migraine ( gastroscopy neg, CT brain neg)


46 : petechiae arms, legs and face and also epistaxis; solitary thrombocytopenia 2000/µl Nasal cautery, corticosteroids IV and platelet transfusion Hospital discharge at d 4 with platelets of 3000/µl, nobleeding symptoms anymore and with Medrol 64mg/d d18

 No sustained response but safe")
47 Iron deficiency anemia, depression : diagnosis of ITP, Medrol 64mg/d with rapid platelet increase Tapering corticosteroids very slowly ( stop ) No sustained response but safe platelet count


48 Table 3: Immunoglobulins (IGIV)
 02-2007: IGIV monthly (4x) with tapering of")
49 : diagnosis of ITP : platelets 16000/µl : Medrol 64 mg/d (corticorefractory) : IGIV monthly (4x) with tapering of corticosteroids

50 Relapse after a long treatment-free interval can be managed by restarting first line treatment. Long term steroid use (> 5mg prednisone or equivalent) must be avoided.


51 Azathioprine Cyclosporine Cyclophosphamide Danazol dapsone Mycophenolate mofetil Rituximab Splenectomy TPO-mimetica Vinca alkaloiden
52 Splenectomy (IB) TPO-R agonists after splenectomy TPO-R agonists if a contraindication for splenectomy (IB) TPO-R agonists after failure to corticosteroids or IgIV (2C) Rituximab after failure to corticosteroids,igiv or splenectomy (2C)
, the BHS guideline panel on adult ITP : BHS recommendations Splenectomy as it is the only treatment with a curative potential and has an acceptable safety profile.")
53 For adult ITP patients who are intolerant or unresponsive to or relapse after initial corticosteroid treatment and have a risk of bleeding (platelets < /µl OR bleeding symptoms), the BHS guideline panel on adult ITP : BHS recommendations Splenectomy as it is the only treatment with a curative potential and has an acceptable safety profile. If possible, splenectomy should be delayed to at least twelve months after diagnosis as spontaneous remission can occur TPO-R agonists for patients who are refractory to or relapse after splenectomy or who have a contra-indication to splenectomy irrespective of the duration of ITP BHS suggestion in TPO-R agonist refractory patients Rituximab, azathioprine, cyclophosphamide, cyclosporine A, danazol, dapsone, mycophenolate mofetil and vincristine/vinblastine are potential treatment options




54 Vaccination strategy 11/2013: *Prevenar 13 with/or without Pneumo 23/8w; boost with Pneumo 23/5y (rationale?) *Nimenrix

55 *
56 For adult ITP patients who are intolerant or unresponsive to or relapse after initial corticosteroid treatment and have a risk of bleeding (platelets < /µl OR bleeding symptoms), the BHS guideline panel on adult ITP : BHS recommendations Splenectomy as it is the only treatment with a curative potential and has an acceptable safety profile. If possible, splenectomy should be delayed to at least twelve months after diagnosis as spontaneous remission can occur TPO-R agonists for patients who are refractory to or relapse after splenectomy or who have a contra-indication to splenectomy irrespective of the duration of ITP BHS suggestion in TPO-R agonist refractory patients Rituximab, azathioprine, cyclophosphamide, cyclosporine A, danazol, dapsone, mycophenolate mofetil and vincristine/vinblastine are potential treatment options
57 Characteristics of treatment with TPO-R agonists : general

58 TPO-R agonists are very well tolerated: 5% of patients discontinue therapy because of side effects Experience in the clinic does not exceed seven years, suspicion for possible risks of long-term use is warranted
59 Characteristics of treatment with TPO-R agonists : dosing Response as long as therapy is maintained. Cavé compliance and adherence!!! +/- 15% can stop TPO-R agonists with long-term remission
, the BHS guideline panel on adult ITP : BHS recommendations Splenectomy as it is the only treatment with a curative potential and has an acceptable safety profile.")
60 For adult ITP patients who are intolerant or unresponsive to or relapse after initial corticosteroid treatment and have a risk of bleeding (platelets < /µl OR bleeding symptoms), the BHS guideline panel on adult ITP : BHS recommendations Splenectomy as it is the only treatment with a curative potential and has an acceptable safety profile. If possible, splenectomy should be delayed to at least twelve months after diagnosis as spontaneous remission can occur TPO-R agonists for patients who are refractory to or relapse after splenectomy or who have a contra-indication to splenectomy irrespective of the duration of ITP BHS suggestion in TPO-R agonist refractory patients Rituximab, azathioprine, cyclophosphamide, cyclosporine A, danazol, dapsone, mycophenolate mofetil and vincristine/vinblastine are potential treatment options
 ORR 57%, CR 41%")
 Time to response 1 to 6,34 w Cavé: Late onset neutropenia")


61 Most patients: concomitant therapy Dose: most frequently used 375 mg/m²/w x4 ORR 62,5%, CR 46,3% (all) ORR 57%, CR 41% (non-splenectomized: n=368)) ORR 68%, CR 39% (children: n= 323 pat) Time to response 1 to 6,34 w Cavé: Late onset neutropenia Hypogammaglobulinemia Hep B reactivation PML Duration of response : PR <6m, CR 12m Long-term response: 5y ( 21% of adults, 26% of children) Arnold et al, Ann Intern Med, 2007;146:25-33 Auger et al, B J Hematol 2012 epub Liang et al, PLoS ONE 2012;5: Patel et al, Blood, 2012;119:

62 Azathioprine, cyclophosphamide, cyclosporine A, danazol, dapsone, mycophenolate mofetil and vincristine have been used after treatment failure for decades. Variable individual responses Long-term side effects such as immune suppression
63 Antifibrinolytic agents (tranexamic acid : 3 g/day per os) Oral iron supplements if iron deficient Local application of adrenalin soaked nose pads Nasal cautery Hormone substitutes to prevent menorrhagia Control of blood pressure Stop ASA, antiplatelet agents, anticoagulation if appropriate : except case of recent stent, ischemic heart disease, several peripheral arterial occlusive disease Avoid nonsteroidal anti-inflammatory drugs or ASA
64 1. ITP patients with platelet counts higher than 30000/µl and absence of bleeding signs do not need treatment. 2. Corticosteroids with or without intravenous IVIg are the preferred treatment options for patients with ITP newly diagnosed or relapsing after a long-term treatment-free period. 3. Splenectomy is recommended as second-line treatment as it is the treatment with the highest curative potential and an acceptable safety profile. If possible, splenectomy should be delayed to at least twelve months after diagnosis as spontaneous remission can occur. 4. TPO-R agonists are recommended for patients who are refractory to or relapse after splenectomy or who are unfit for splenectomy, irrespective of the duration of ITP. 5. Rituximab, azathioprine, cyclophosphamide, cyclosporine A, danazol, dapsone, mycophenolate mofetil and vincristine/vinblastine are potential treatment options, especially for patients refractory to TPO-R agonists.



65 Megakaryocyte differentiation Congenital amegakaryocytic T T with absent radii T with radio-ulnar synostosis Megakaryocyte maturation Familial platelet disorder /AML Paris-Trousseau & Jacobsen syndrome GATA-1 related T GFI 1B- related T ANKRD26- related T Gray platelet syndrome Pecci et al, Br J Hematol 2014 Proplatelet formation and platelet release MYH9-related disease ACTN1-related T FLNA-related T Wiskott-Aldrich syndrome & X-linked T Bernard Soulier S

66
Dr Kannan S Consultant Hematologist Sahyadri Speciality Hospital, Pune K E M Hospital, Pune
 IMMUNE THROMBOCYTOPENIA Dr Kannan S Consultant Hematologist Sahyadri Speciality Hospital, Pune K E M Hospital, Pune ITP Megakaryocytes Definition of ITP Primary immune thrombocytopenia Platelet count
IMMUNE THROMBOCYTOPENIA Dr Kannan S Consultant Hematologist Sahyadri Speciality Hospital, Pune K E M Hospital, Pune ITP Megakaryocytes Definition of ITP Primary immune thrombocytopenia Platelet count
Acute Immune Thrombocytopenic Purpura (ITP) in Childhood
 in Childhood") Acute Immune Thrombocytopenic Purpura (ITP) in Childhood Guideline developed by Robert Saylors, MD, in collaboration with the ANGELS team. Last reviewed by Robert Saylors, MD September 22, 2016. Key Points
Acute Immune Thrombocytopenic Purpura (ITP) in Childhood Guideline developed by Robert Saylors, MD, in collaboration with the ANGELS team. Last reviewed by Robert Saylors, MD September 22, 2016. Key Points
Hemostatic System - general information
 PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
Diagnosis and Management of Immune Thrombocytopenias. Thomas L. Ortel, M.D., Ph.D. Duke University Medical Center 2 November 2016
 Diagnosis and Management of Immune Thrombocytopenias Thomas L. Ortel, M.D., Ph.D. Duke University Medical Center 2 November 2016 Disclosures Research support: NIH, CDC, Eisai, Pfizer, Daiichi Sankyo, GlaxoSmithKline,
Diagnosis and Management of Immune Thrombocytopenias Thomas L. Ortel, M.D., Ph.D. Duke University Medical Center 2 November 2016 Disclosures Research support: NIH, CDC, Eisai, Pfizer, Daiichi Sankyo, GlaxoSmithKline,
Evolution of clinical guidelines for ITP: Role of Romiplostim
 Slovenian Haematological Society 16 April 2010, Podčetrtek Evolution of clinical guidelines for ITP: Role of Romiplostim Dr. Roberto Stasi Department of Haematology St George's Hospital London Is there
Slovenian Haematological Society 16 April 2010, Podčetrtek Evolution of clinical guidelines for ITP: Role of Romiplostim Dr. Roberto Stasi Department of Haematology St George's Hospital London Is there
Thrombocytopenia: a practial approach
 Thrombocytopenia: a practial approach Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Outline Introduction and
Thrombocytopenia: a practial approach Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Outline Introduction and
QUICK REFERENCE Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP)
") QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY
 V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY Kharkov Regional Centre of Cardiovascular surgery V.N. Karazin Kharkov National University Department of Internal Medicine Immune thrombocytopenic purpura Abduyeva
V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY Kharkov Regional Centre of Cardiovascular surgery V.N. Karazin Kharkov National University Department of Internal Medicine Immune thrombocytopenic purpura Abduyeva
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Update on the Management of Immune Thrombocytopenic Purpura (ITP) Dr Raymond Wong Department of Medicine & Therapeutics Prince of Wales Hospital
 Dr Raymond Wong Department of Medicine & Therapeutics Prince of Wales Hospital") Update on the Management of Immune Thrombocytopenic Purpura (ITP) Dr Raymond Wong Department of Medicine & Therapeutics Prince of Wales Hospital Immune Thrombocytopenia (ITP) Immune-mediated acquired disease
Update on the Management of Immune Thrombocytopenic Purpura (ITP) Dr Raymond Wong Department of Medicine & Therapeutics Prince of Wales Hospital Immune Thrombocytopenia (ITP) Immune-mediated acquired disease
Contemporary perspectives and initial management of pediatric ITP. William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA
 Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Thrombocytopenia. Dr Lynda Vandertuin May 6, 2014
 Dr Lynda Vandertuin May 6, 2014 1 Presentation 1. Definition 2. Platelet Physiology, Thromboiesis, & Platelet Function 3. Bleeding Risk 4. Clinical Diagnosis 5. Differential Diagnosis 6. Classification
Dr Lynda Vandertuin May 6, 2014 1 Presentation 1. Definition 2. Platelet Physiology, Thromboiesis, & Platelet Function 3. Bleeding Risk 4. Clinical Diagnosis 5. Differential Diagnosis 6. Classification
The function of the bone marrow. Living with Aplastic Anemia. A Case Study - I. Hypocellular bone marrow failure 5/14/2018
 The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
Case Presentation. A Case from the Clinic. Additional Data. Examination and Data 10/27/2013
 Northwestern University Feinberg School of Medicine Treatment of Severe Thrombocytopenia in Systemic Lupus Erythematosus: The Role of New Agents Disclosures: Advisory Board: Incyte Corporation Speaker
Northwestern University Feinberg School of Medicine Treatment of Severe Thrombocytopenia in Systemic Lupus Erythematosus: The Role of New Agents Disclosures: Advisory Board: Incyte Corporation Speaker
Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014
 Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014 The notification letter which contains details of the decision to widen the restriction criteria for rituximab and eltrombopag
Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014 The notification letter which contains details of the decision to widen the restriction criteria for rituximab and eltrombopag
REVIEW ARTICLE. Immune Thrombocytopenic Purpura ADARSH A K, LAKSHMI KRISHNA INTRODUCTION CLASSIFICATION
 ADARSH A K, LAKSHMI KRISHNA REVIEW ARTICLE INTRODUCTION ITP or immune thrombocytopenic purpura is an autoimmune disorder characterized by increased platelet destruction & platelet count < 1 lakh. It is
ADARSH A K, LAKSHMI KRISHNA REVIEW ARTICLE INTRODUCTION ITP or immune thrombocytopenic purpura is an autoimmune disorder characterized by increased platelet destruction & platelet count < 1 lakh. It is
EDUCATIONAL COMMENTARY PLATELET DISORDERS
 EDUCATIONAL COMMENTARY PLATELET DISORDERS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Earn
EDUCATIONAL COMMENTARY PLATELET DISORDERS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Earn
thrombopoietin receptor agonists and University of Washington January 13, 2012
 Tickle me eltrombopag: thrombopoietin receptor agonists and the regulation of platelet production Manoj Menon University of Washington January 13, 2012 Outline Clinical case Pathophysiology of ITP Therapeutic
Tickle me eltrombopag: thrombopoietin receptor agonists and the regulation of platelet production Manoj Menon University of Washington January 13, 2012 Outline Clinical case Pathophysiology of ITP Therapeutic
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust
 Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Approach to thrombocytopenia and management of ITP. Dr.Aby Abraham Dept of Clinical Haematology
 Approach to thrombocytopenia and management of ITP Dr.Aby Abraham Dept of Clinical Haematology 04-08-2014 Causes of thrombocytopenia Thrombocytopenia Pseudo True Decreased production Increased destruction
Approach to thrombocytopenia and management of ITP Dr.Aby Abraham Dept of Clinical Haematology 04-08-2014 Causes of thrombocytopenia Thrombocytopenia Pseudo True Decreased production Increased destruction
Hematology, Transfusion and Cell Therapy
 hematol transfus cell ther. 2018;40(1):50 74 Hematology, Transfusion and Cell Therapy www.rbhh.org Special article Guideline on immune thrombocytopenia in adults: Associação Brasileira de Hematologia,
hematol transfus cell ther. 2018;40(1):50 74 Hematology, Transfusion and Cell Therapy www.rbhh.org Special article Guideline on immune thrombocytopenia in adults: Associação Brasileira de Hematologia,
The Evolving Role of Reticulated Platelets
 The Evolving Role of Kyle Riding, PhD, MLS(ASCP) CM University of Central Florida Session Objectives Platelets Recall the process involved in megakaryopoiesis and thrombocytopoiesis Explain the various
The Evolving Role of Kyle Riding, PhD, MLS(ASCP) CM University of Central Florida Session Objectives Platelets Recall the process involved in megakaryopoiesis and thrombocytopoiesis Explain the various
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Scottish Medicines Consortium
 Scottish Medicines Consortium romiplostim, 250 microgram vial of powder for solution for subcutaneous injection (Nplate ) No. (553/09) Amgen 08 May 2009 (Issued 4 September 2009) The Scottish Medicines
Scottish Medicines Consortium romiplostim, 250 microgram vial of powder for solution for subcutaneous injection (Nplate ) No. (553/09) Amgen 08 May 2009 (Issued 4 September 2009) The Scottish Medicines
UKITP INITAL INFORMATION SHEET (2.4)
") UKITP INITAL INFORMATION SHEET (2.4) Barts Health NHS Trust The Royal London Hospital Pathology and Pharmacy Building 80 Newark Street, London E1 2ES Centre for Haematology Institute of and Molecular Science
UKITP INITAL INFORMATION SHEET (2.4) Barts Health NHS Trust The Royal London Hospital Pathology and Pharmacy Building 80 Newark Street, London E1 2ES Centre for Haematology Institute of and Molecular Science
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
GOOD MORNING! Thursday, July Heidi Murphy, MD Leslie Carter-King, MD
 GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
Autoimmune haematological disorders
 Autoimmune haematological disorders Dr. Demeter Judit demjud@bel1.sote.hu Semmelweis University, Ist Department of Medicine Thrombocytopenia Examination of the thrombocytopenic patient 1. Exclusion of
Autoimmune haematological disorders Dr. Demeter Judit demjud@bel1.sote.hu Semmelweis University, Ist Department of Medicine Thrombocytopenia Examination of the thrombocytopenic patient 1. Exclusion of
What is the next step after failure of steroids in ITP? Splenectomy & Rituximab
 What is the next step after failure of steroids in ITP? Splenectomy & Rituximab Dr. Roberto Stasi Department of Haematology St George's Hospital and Medical School London Factors that contribute to ITP
What is the next step after failure of steroids in ITP? Splenectomy & Rituximab Dr. Roberto Stasi Department of Haematology St George's Hospital and Medical School London Factors that contribute to ITP
Treatment pathway for adult patients with immune (idiopathic) thrombocytopenic purpura (ITP)
 thrombocytopenic purpura (ITP)") Prescribing Clinical Network Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) Crawley and Horsham & Mid-Sussex CCG Treatment pathway for adult
Prescribing Clinical Network Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) Crawley and Horsham & Mid-Sussex CCG Treatment pathway for adult
Bleeding Disorders.2 MS Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD
 Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Expert Review: Updates in Immune Thrombocytopenia. Reference Slides
 Expert Review: Updates in Immune Thrombocytopenia Reference Slides Immune Thrombocytopenia (ITP): Overview ITP causality 1,2 Suboptimal platelet production Dysregulated adaptive immune system Increased
Expert Review: Updates in Immune Thrombocytopenia Reference Slides Immune Thrombocytopenia (ITP): Overview ITP causality 1,2 Suboptimal platelet production Dysregulated adaptive immune system Increased
Outline. What is aplastic anemia? 9/19/2012. Aplastic Anemia Current Thinking on the Disease, Diagnosis, and Non-Transplant Treatment Options
 Aplastic Anemia Current Thinking on the Disease, Diagnosis, and Non-Transplant Treatment Options Carlos M. de Castro, MD Duke University Medical Center Outline What is Aplastic Anemia? What other diseases
Aplastic Anemia Current Thinking on the Disease, Diagnosis, and Non-Transplant Treatment Options Carlos M. de Castro, MD Duke University Medical Center Outline What is Aplastic Anemia? What other diseases
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Cynthia Fata, MD, MSPH 6/23/15
 Cynthia Fata, MD, MSPH 6/23/15 Clinical case presentation Introduction to thrombopoietin Development of thrombopoietic agents Clinical Indications Eltrombopag use in aplastic anemia Future uses 33 yo F
Cynthia Fata, MD, MSPH 6/23/15 Clinical case presentation Introduction to thrombopoietin Development of thrombopoietic agents Clinical Indications Eltrombopag use in aplastic anemia Future uses 33 yo F
BLEEDING (PLATELET) DISORDER. IAP UG Teaching slides
 DISORDER. IAP UG Teaching slides") BLEEDING (PLATELET) DISORDER 1 APPROACH The initial set of questions should establish the following: (1) the most common site and type of bleeding (e.g., mucocutaneous versus articular or deep muscle),
BLEEDING (PLATELET) DISORDER 1 APPROACH The initial set of questions should establish the following: (1) the most common site and type of bleeding (e.g., mucocutaneous versus articular or deep muscle),
Committee Approval Date: May 9, 2014 Next Review Date: May 2015
 Medication Policy Manual Policy No: dru180 Topic: Promacta, eltrombopag Date of Origin: May 8, 2009 Committee Approval Date: May 9, 2014 Next Review Date: May 2015 Effective Date: June 1, 2014 IMPTANT
Medication Policy Manual Policy No: dru180 Topic: Promacta, eltrombopag Date of Origin: May 8, 2009 Committee Approval Date: May 9, 2014 Next Review Date: May 2015 Effective Date: June 1, 2014 IMPTANT
Domenico Bianco, DVM, PhD, DACVIM August, 26 th 2013
 Domenico Bianco, DVM, PhD, DACVIM August, 26 th 2013 Most common hemolytic disorder in dogs Primary (idiopathic) or secondary 60-75% of cases are idiopathic Mortality as high as 70% Pathophysiology Presentation
Domenico Bianco, DVM, PhD, DACVIM August, 26 th 2013 Most common hemolytic disorder in dogs Primary (idiopathic) or secondary 60-75% of cases are idiopathic Mortality as high as 70% Pathophysiology Presentation
IVIG (intravenous immunoglobulin) Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen
 Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN
 Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 08/19/14 SECTION: DRUGS LAST REVIEW DATE: LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 RITUXAN (rituximab) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
RITUXAN (rituximab) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
PROMACTA (eltrombopag olamine) oral tablet and oral suspension
 oral tablet and oral suspension") PROMACTA (eltrombopag olamine) oral tablet and oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
PROMACTA (eltrombopag olamine) oral tablet and oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Immune Thrombocytopenia (ITP)
") Immune Thrombocytopenia (ITP) ITP - What is it? ITP is a blood disorder affecting platelets in the blood. Platelets are small cells in your blood that help your blood to clot. In ITP the body s immune
Immune Thrombocytopenia (ITP) ITP - What is it? ITP is a blood disorder affecting platelets in the blood. Platelets are small cells in your blood that help your blood to clot. In ITP the body s immune
Clinical decision making in ITP: When to treat and how to treat
 Clinical decision making in ITP: When to treat and how to treat Beng Hock Chong MBBS,PhD,FRACP, FRCPA,FRCP Professor of Medicine, University of New South Wales, Sydney and Director of Hematology, St George
Clinical decision making in ITP: When to treat and how to treat Beng Hock Chong MBBS,PhD,FRACP, FRCPA,FRCP Professor of Medicine, University of New South Wales, Sydney and Director of Hematology, St George
When the Plate is not Full
 NO DISCLOSURES DISCLOSURES When the Plate is not Full James W. Haynes, M.D. Dept of Family Medicine Univ of TN College of Medicine (Chattanooga) Thrombocytopenia Mild 70 149K / Severe < 20K > 50 often
NO DISCLOSURES DISCLOSURES When the Plate is not Full James W. Haynes, M.D. Dept of Family Medicine Univ of TN College of Medicine (Chattanooga) Thrombocytopenia Mild 70 149K / Severe < 20K > 50 often
Volume 4, Issue 1, March 2013 REPRINT. Primary immune thrombocytopenia in adults
 BELGIAN SOCIETY Belgian Journal of Hematology The Belgian Journal of Hematology is the official journal of the Belgian Hematological Society (BHS), the Belgian Society on Thrombosis and Haemostasis (BSTH),
BELGIAN SOCIETY Belgian Journal of Hematology The Belgian Journal of Hematology is the official journal of the Belgian Hematological Society (BHS), the Belgian Society on Thrombosis and Haemostasis (BSTH),
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
 DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
Idiophatic Thrombocytopenic Purpura: Current Concepts In Pathophysiology And Management
 Slovenian Society of Hematology Kranjska Gora, 3-4 October 2008 Idiophatic Thrombocytopenic Purpura: Current Concepts In Pathophysiology And Management Dr. Roberto Stasi S.C. di Oncologia ed Ematologia
Slovenian Society of Hematology Kranjska Gora, 3-4 October 2008 Idiophatic Thrombocytopenic Purpura: Current Concepts In Pathophysiology And Management Dr. Roberto Stasi S.C. di Oncologia ed Ematologia
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
The Bleeding Patient. Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand
 The Bleeding Patient Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand The Bleeding Patient If you prick us, do we not bleed? Disorders of secondary homeostasis: dysfunction
The Bleeding Patient Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand The Bleeding Patient If you prick us, do we not bleed? Disorders of secondary homeostasis: dysfunction
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
eltrombopag (Promacta )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Immune Thrombocytopenia. A Practical Guide for Nurses and Other Allied Healthcare Professionals
 Immune Thrombocytopenia A Practical Guide for Nurses and Other Allied Healthcare Professionals Contents Chapter 1: Overview of immune thrombocytopenia 3 Chapter 2: Identifying immune thrombocytopenia 7
Immune Thrombocytopenia A Practical Guide for Nurses and Other Allied Healthcare Professionals Contents Chapter 1: Overview of immune thrombocytopenia 3 Chapter 2: Identifying immune thrombocytopenia 7
THE OLD AND THE NEW OF ITP. Alison Street Malaysia April 2010
 THE OLD AND THE NEW OF ITP Alison Street Malaysia April 2010 The Harrington-Hollingsworth Experiment Harrington et al. Demonstration of a thrombocytopenic factor in the blood of patients with thrombocytopenic
THE OLD AND THE NEW OF ITP Alison Street Malaysia April 2010 The Harrington-Hollingsworth Experiment Harrington et al. Demonstration of a thrombocytopenic factor in the blood of patients with thrombocytopenic
Second line therapy for ITP should be TPO agonists. Nichola Cooper Imperial Health Care NHS Trust
 Second line therapy for ITP should be TPO agonists Nichola Cooper Imperial Health Care NHS Trust COHEM 2012 Antiplatelet antibodies Platelet count after infusion with patient plasma Hours Days T cells
Second line therapy for ITP should be TPO agonists Nichola Cooper Imperial Health Care NHS Trust COHEM 2012 Antiplatelet antibodies Platelet count after infusion with patient plasma Hours Days T cells
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Immune thrombocytopenic purpura presenting in a patient after renal transplant for diabetic nephropathy
 Rashid et al. BMC Nephrology (2018) 19:69 https://doi.org/10.1186/s12882-018-0868-7 CASE REPORT Open Access Immune thrombocytopenic purpura presenting in a patient after renal transplant for diabetic nephropathy
Rashid et al. BMC Nephrology (2018) 19:69 https://doi.org/10.1186/s12882-018-0868-7 CASE REPORT Open Access Immune thrombocytopenic purpura presenting in a patient after renal transplant for diabetic nephropathy
Immune Globulin. Prior Authorization
 MB9423 Covered Service: Yes when meets criteria below Prior Authorization Required: Additional Information: Yes as shown below Requires prior authorization through Navitus and is considered medically appropriate
MB9423 Covered Service: Yes when meets criteria below Prior Authorization Required: Additional Information: Yes as shown below Requires prior authorization through Navitus and is considered medically appropriate
Corso di Ematologia di Laboratorio Istituto Tumori, Milano novembre 2010
 Corso di Ematologia di Laboratorio Istituto Tumori, Milano 11-12 novembre 2010 Piastrinopenie Immuni: dalla patogenesi alla standardizzazione del percorso diagnostico e terapeutico Marco Ruggeri UO Ematologia,
Corso di Ematologia di Laboratorio Istituto Tumori, Milano 11-12 novembre 2010 Piastrinopenie Immuni: dalla patogenesi alla standardizzazione del percorso diagnostico e terapeutico Marco Ruggeri UO Ematologia,
Dr. Apoorva Jayarangaiah MARSHFIELD CLINIC- Saint Joseph s Hospital
 Dr. Apoorva Jayarangaiah MARSHFIELD CLINIC- Saint Joseph s Hospital A 30 year old G1P0 female of Korean descent was referred by her OBGYN during her 2 nd trimester to the Hematology Clinic for evaluation
Dr. Apoorva Jayarangaiah MARSHFIELD CLINIC- Saint Joseph s Hospital A 30 year old G1P0 female of Korean descent was referred by her OBGYN during her 2 nd trimester to the Hematology Clinic for evaluation
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Bleeding disorders. Hemostatic failure: Inappropriate and excessive bleeding either spontaneous or in response to injury.
 1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
Platelets, numbers and alternative functions Nichola Cooper Hammersmith Hospital Imperial College
 Platelets, numbers and alternative functions 2018 Nichola Cooper Hammersmith Hospital Imperial College Discussion points today What do platelets do beyond clot formation? How are platelets made? How is
Platelets, numbers and alternative functions 2018 Nichola Cooper Hammersmith Hospital Imperial College Discussion points today What do platelets do beyond clot formation? How are platelets made? How is
Hematologic Disorders. Assistant professor of anesthesia
 Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Rituximab for the treatment of Immune (Idiopathic) Thrombocytopenic Purpura (ITP)
 Thrombocytopenic Purpura (ITP)") Rituximab for the treatment of Immune (Idiopathic) Thrombocytopenic Purpura (ITP) Lead author: Stephen Erhorn Regional Drug & Therapeutics Centre (Newcastle) February 2015 2015 Summary Rituximab (MabThera,
Rituximab for the treatment of Immune (Idiopathic) Thrombocytopenic Purpura (ITP) Lead author: Stephen Erhorn Regional Drug & Therapeutics Centre (Newcastle) February 2015 2015 Summary Rituximab (MabThera,
12 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
 Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Promacta. Promacta (eltrombopag) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.15 Subject: Promacta Page: 1 of 6 Last Review Date: September 15, 2017 Promacta Description Promacta
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.15 Subject: Promacta Page: 1 of 6 Last Review Date: September 15, 2017 Promacta Description Promacta
Neutropenia Following Intravenous Immunoglobulin Therapy in Pediatric Patients with Idiopathic Thrombocytopenic Purpura
 ORIGINAL ARTICLE IJBC 2014;6(2): 81-85 Neutropenia Following Intravenous Immunoglobulin Therapy in Pediatric Patients with Idiopathic Thrombocytopenic Purpura Ansari S * 1, Shirali A 1, Khalili N 1, Daneshfar
ORIGINAL ARTICLE IJBC 2014;6(2): 81-85 Neutropenia Following Intravenous Immunoglobulin Therapy in Pediatric Patients with Idiopathic Thrombocytopenic Purpura Ansari S * 1, Shirali A 1, Khalili N 1, Daneshfar
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Il Rituximab nella ITP
 Il Rituximab nella ITP Monica Carpenedo U.O.C Ematologia e TMO, Ospedale San Gerardo, Monza Burning questions about Rituximab and ITP What is the mechanism of action? What is long term effect of treatment?
Il Rituximab nella ITP Monica Carpenedo U.O.C Ematologia e TMO, Ospedale San Gerardo, Monza Burning questions about Rituximab and ITP What is the mechanism of action? What is long term effect of treatment?
IMMATURE PLATELETS CLINICAL USE
 HAEMATOLOGY FEBRUARY 2017 WHITE PAPER IMMATURE PLATELETS CLINICAL USE Differential diagnosis of thrombocytopenia Thrombocytopenia and automated platelet measurement Thrombocytopenia is a condition characterised
HAEMATOLOGY FEBRUARY 2017 WHITE PAPER IMMATURE PLATELETS CLINICAL USE Differential diagnosis of thrombocytopenia Thrombocytopenia and automated platelet measurement Thrombocytopenia is a condition characterised
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL)
") Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
Case Report Myelofibrosis Associated with Romiplostim Treatment in a Patient with Immune Thrombocytopenia
 Volume 2012, Article ID 318597, 4 pages doi:10.1155/2012/318597 Case Report Myelofibrosis Associated with Romiplostim Treatment in a Patient with Immune Thrombocytopenia Maria Fernanda Gonzalez and Jonathan
Volume 2012, Article ID 318597, 4 pages doi:10.1155/2012/318597 Case Report Myelofibrosis Associated with Romiplostim Treatment in a Patient with Immune Thrombocytopenia Maria Fernanda Gonzalez and Jonathan
Drug Class Prior Authorization Criteria Immune Globulins
 Drug Class Prior Authorization Criteria Immune Globulins Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy has been developed through review of
Drug Class Prior Authorization Criteria Immune Globulins Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy has been developed through review of
Scottish Medicines Consortium
 Scottish Medicines Consortium eltrombopag, 25mg and 50mg film-coated tablets (Revolade ) No. (625/10) GlaxoSmithKline UK 09 July 2010 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium eltrombopag, 25mg and 50mg film-coated tablets (Revolade ) No. (625/10) GlaxoSmithKline UK 09 July 2010 The Scottish Medicines Consortium (SMC) has completed its assessment
Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist
 Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist Wisconsin Institute of Discovery Karen Rossi/Bristol-Myers Squibb Morey A. Blinder, MD Washington University, St. Louis, MO March
Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist Wisconsin Institute of Discovery Karen Rossi/Bristol-Myers Squibb Morey A. Blinder, MD Washington University, St. Louis, MO March
Overview of Aplastic Anemia. Overview of Aplastic Anemia. Epidemiology of aplastic anemia. Normal hematopoiesis 10/6/2017
 Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Rituximab for the treatment of adults with idiopathic (immune) thrombocytopenic purpura (ITP)
 thrombocytopenic purpura (ITP)") Bedfordshire and Luton Joint Prescribing Committee Date: September 2015 Review date: September 2018 Bullletin 221: Rituximab (MabThera ) for the treatment of adults with idiopathic (immune) thrombocytopenic
Bedfordshire and Luton Joint Prescribing Committee Date: September 2015 Review date: September 2018 Bullletin 221: Rituximab (MabThera ) for the treatment of adults with idiopathic (immune) thrombocytopenic
Tavalisse (fostamatinib disodium hexahydrate)
") Tavalisse (fostamatinib disodium hexahydrate) Policy Number: 5.01.661 Last Review: 07/2018 Origination: 07/2018 Next Review: 07/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Tavalisse (fostamatinib disodium hexahydrate) Policy Number: 5.01.661 Last Review: 07/2018 Origination: 07/2018 Next Review: 07/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Western Health Specialist Clinics Access & Referral Guidelines
 Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Pediatric Immune Thrombocytopenia (ITP) Cindy E. Neunert MD, MSCS Associate Professor, Pediatrics Columbia University Medical Center New York, NY
 Cindy E. Neunert MD, MSCS Associate Professor, Pediatrics Columbia University Medical Center New York, NY") Pediatric Immune Thrombocytopenia (ITP) Cindy E. Neunert MD, MSCS Associate Professor, Pediatrics Columbia University Medical Center New York, NY Objectives Review the 2011 American Society of Hematology
Pediatric Immune Thrombocytopenia (ITP) Cindy E. Neunert MD, MSCS Associate Professor, Pediatrics Columbia University Medical Center New York, NY Objectives Review the 2011 American Society of Hematology
Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature Review and Case Report
 Hindawi Case Reports in Hematology Volume 2017, Article ID 3725089, 4 pages https://doi.org/10.1155/2017/3725089 Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature
Hindawi Case Reports in Hematology Volume 2017, Article ID 3725089, 4 pages https://doi.org/10.1155/2017/3725089 Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature
Use of TPO mimetics for Indications Other Than ITP
 Use of TPO mimetics for Indications Other Than ITP Mazyar Shadman, MD, MPH Discussant: Siobán Keel, MD Hematology Fellows Conference June 28, 2013 Thrombopoietin (TPO) and other c mpl ligands TPO mimetics
Use of TPO mimetics for Indications Other Than ITP Mazyar Shadman, MD, MPH Discussant: Siobán Keel, MD Hematology Fellows Conference June 28, 2013 Thrombopoietin (TPO) and other c mpl ligands TPO mimetics
APPENDIX 2 Eight New Cases of LAHS and Review of Literature: Treatment and Follow-Up
 Supplementary Digital Content 2 Mazodier Lupus Anticoagulant- Hypoprothrombinemia Syndrome: Report of 8 Cases and Review of the Literature Medicine (Baltimore). 2012;91(5). APPEIX 2 Eight New Cases of
Supplementary Digital Content 2 Mazodier Lupus Anticoagulant- Hypoprothrombinemia Syndrome: Report of 8 Cases and Review of the Literature Medicine (Baltimore). 2012;91(5). APPEIX 2 Eight New Cases of
Immune Thrombocytopenic Purpura (ITP)
") Patient information Immune Thrombocytopenic Purpura Immune Thrombocytopenic Purpura (ITP) This leaflet is for adult patients diagnosed with Immune Thrombocytopenic Purpura also known as Immune Thrombocytopenia
Patient information Immune Thrombocytopenic Purpura Immune Thrombocytopenic Purpura (ITP) This leaflet is for adult patients diagnosed with Immune Thrombocytopenic Purpura also known as Immune Thrombocytopenia
Idiopathic Thrombocytopenic Purpura
 Idiopathic Thrombocytopenic Purpura Title of Guideline Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of idiopathic thrombocytopenic purpura Dr S Stokley, Consultant
Idiopathic Thrombocytopenic Purpura Title of Guideline Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of idiopathic thrombocytopenic purpura Dr S Stokley, Consultant
INTRODUCTION TO SET FORTH APROACH TO MANAGING ADULTS TO SET FORTH APROACH PRIMARY ( PRIMARY AUTOIMMUNE) AUTOIMMUNE ITP FROM ASH & THE BRITISH
 AUTOIMMUNE ITP FROM ASH & THE BRITISH") HOW I TREAT IDIOPATHIC THROMBOCYTOPENIC PURPURA Dauglas B. Cines, James B Bussel. Blood Oktober 2005:106(7):2244-22512251 INTRODUCTION TO SET FORTH APROACH TO MANAGING ADULTS PRIMARY (AUTOIMMUNE) ITP FROM
HOW I TREAT IDIOPATHIC THROMBOCYTOPENIC PURPURA Dauglas B. Cines, James B Bussel. Blood Oktober 2005:106(7):2244-22512251 INTRODUCTION TO SET FORTH APROACH TO MANAGING ADULTS PRIMARY (AUTOIMMUNE) ITP FROM
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Remissions after long term use of romiplostim for immune thrombocytopenia
 Published Ahead of Print on September 1, 2016, as doi:10.3324/haematol.2016.151886. Copyright 2016 Ferrata Storti Foundation. Remissions after long term use of romiplostim for immune thrombocytopenia by
Published Ahead of Print on September 1, 2016, as doi:10.3324/haematol.2016.151886. Copyright 2016 Ferrata Storti Foundation. Remissions after long term use of romiplostim for immune thrombocytopenia by
Index. Note: Page numbers of article numbers are in boldface type.
 Index Note: Page numbers of article numbers are in boldface type. A Abdomen, acute, as cancer emergency, 381 399 in cancer patients, etiologies unique to, 390 392 in perforation, 388 surgery of, portal
Index Note: Page numbers of article numbers are in boldface type. A Abdomen, acute, as cancer emergency, 381 399 in cancer patients, etiologies unique to, 390 392 in perforation, 388 surgery of, portal
Promacta. Promacta (eltrombopag) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.15 Subject: Promacta Page: 1 of 6 Last Review Date: September 20, 2018 Promacta Description Promacta
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.15 Subject: Promacta Page: 1 of 6 Last Review Date: September 20, 2018 Promacta Description Promacta
Co-existence of Common Variable Immunodeficiency (CVID) with Idiopathic Thrombocytopenic purpura (ITP)
 with Idiopathic Thrombocytopenic purpura (ITP)") ISSN 1735-1383 Iran. J. Immunol. March 2008, 5 (1), 64-67 Mohamed Osama Hegazi, Ramesh Kumar, Mubarak Alajmi, Eman Ibrahim Co-existence of Common Variable Immunodeficiency (CVID) with Idiopathic Thrombocytopenic
ISSN 1735-1383 Iran. J. Immunol. March 2008, 5 (1), 64-67 Mohamed Osama Hegazi, Ramesh Kumar, Mubarak Alajmi, Eman Ibrahim Co-existence of Common Variable Immunodeficiency (CVID) with Idiopathic Thrombocytopenic
Acquired Inhibitors of Coagulation
 Acquired Inhibitors of Coagulation Christine L Kempton, MD, MSc Emory University Disclosures for In compliance with COI policy, ISTH requires the following disclosures to the session audience: Research
Acquired Inhibitors of Coagulation Christine L Kempton, MD, MSc Emory University Disclosures for In compliance with COI policy, ISTH requires the following disclosures to the session audience: Research
How I treat acquired aplastic anemia
 How I treat acquired aplastic anemia Phillip Scheinberg and Neal S. Young Blood Volume 120(6):1185-1196 August 9, 2012 2012 by American Society of Hematology Symptoms, Signs, and Lab Findings Bruising,
How I treat acquired aplastic anemia Phillip Scheinberg and Neal S. Young Blood Volume 120(6):1185-1196 August 9, 2012 2012 by American Society of Hematology Symptoms, Signs, and Lab Findings Bruising,