Review Article Vulvar Skin Disorders throughout Lifetime: About Some Representative Dermatoses
|
|
|
- Christian Weaver
- 5 years ago
- Views:
Transcription
1 Hindawi Publishing Corporation BioMed Research International Volume 2014, Article ID , 6 pages Review Article Vulvar Skin Disorders throughout Lifetime: About Some Representative Dermatoses Jean Doyen, 1 Stéphanie Demoulin, 2 Katty Delbecque, 3 Frédéric Goffin, 1 Frédéric Kridelka, 1 and Philippe Delvenne 3 1 Department of Gynecology and Obstetrics, Regional Hospital Citadelle, 4000 Liege, Belgium 2 Laboratory of Experimental Pathology, GIGA-Cancer, University of Liege, 4000 Liege, Belgium 3 Department of Pathology, University Hospital of Liege, 4000 Liege, Belgium Correspondence should be addressed to Philippe Delvenne; p.delvenne@ulg.ac.be Received 31 October 2013; Accepted 12 December 2013; Published 8 January 2014 Academic Editor: Gérald E. Piérard Copyright 2014 Jean Doyen et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The objective of this paper is to present general considerations which should be kept in mind by clinicians in charge of women with vulvar diseases. Four representative vulvar dermatoses are described. Lichen simplex chronicus is a pathological condition related to chemical and mechanical irritant agents. Detrimental effects of these irritants, in the presence of other dermatoses, have to be considered when therapeutic responses are unsatisfactory. Lichen sclerosus is the most common vulvar dermatosis in elderly. However, it should be kept in mind that it may be diagnosed at any age. Lichen planus, in spite of sharing a similar range of etiological factors with lichen sclerosus, is a very distinct entity. Finally, Paget s disease, although rare, is also described especially because of the challenge it represents both clinically and therapeutically. 1. Introduction Vulva is, for many reasons, to be regarded as a particular anatomic area. Considering anatomy and patient s own point of view, this region is of course not easily self-observable and, asapartofgenitalia,oftenquiteunknownandmysterious,for cultural or emotional reasons. It is composed of several folds including clitoral hood, labia majora and minora, hymen, and anal margin. Microscopically, vulva is covered by different types of epithelia, depending on the area of interest, including, from its lateral to medial region, keratinized hair bearing skin, partially keratinized hairless skin, and, beyond Hart s line, mucous membrane of the vestibule. A large number and variety of adnexal structures are associated with vulvar skin in its different sections, such as pilosebaceous units, sebaceous and sweat glands, mucous secretory glands, muscle fibers, and deeper major or minor vestibular glands. Vicinity of underlying vascular structures can also modify vulvar aspects. Therefore, any component of blood and lymphatic vessels can be affected through malformations, tumors, or dystrophic changes. From a pathological point of view, vulva, as a part of genitalia, can be affected by specific disorders such as multifocal HPV lesions of any degree or vulvar expression of a vaginal infection. Vulva can also exhibit specific dermatological diseases for which signs can be observed elsewhere on the body,suchasinlichensclerosusorpsoriasis.however,vulva can also exhibit signs of a large variety of diseases, such as digestive, hematological, immunological, and endocrine disorders. This leads us to consider any vulvar disorder as a potential expression of a very large panel of diseases. Clinically, if many vulvar lesions are reasonably characteristic, numerous clinical manifestations are not specific of one disorder and some diseases can express different morphological patterns. For these reasons, the revision should follow unexpected no-response to empirical treatment resulting from a clinical diagnosis. Frequently, pathological patterns cannot be automatically related to one single cause. Biopsy is certainly an important diagnostic step in many circumstances. As biopsy is an invasive procedure, especially onthevulva,specialcareshouldbetaken.unlessforvery suspicious lesions that require prompt diagnosis, topical
2 2 BioMed Research International treatments, especially corticosteroids, should be stopped 3 to 4 weeks before performing biopsy to allow natural histological expression of the disease. Local anesthesia is mandatory and biopsy should be performed using a 4 to 5 mm punch device to avoid crushing artifacts occurring with biopsy forceps. As a consequence of these considerations, it seems quite difficult to present a classification of disorders affecting vulva which all medical specialties would agree with. Classification oftheinternalsocietyforthestudyofvulvardiseases appears credible as it is periodically revisited and as it is the result of consensus between gynecologists, dermatologists, and pathologists. At the present time, 2006 ISSVD Classification [1] is still relevant. But, as this classification is of minor help for diagnosis, ISSVD formulated in 2011 a complementary classification as an approach to clinical diagnosis [2]. Clinicians dealing with vulvar complaints should always keep in mind these preliminary considerations and, as a consequence, be convinced that treating vulvar disorders needs a complete anamnestic investigation, examination of the lower genital tract, skin, and sometimes oral mucosae, and dialog between colleagues. Furthermore, special attention should be paid to psychosexual status of patients suffering from vulvar disorders, as they are often present, either as a cause or a consequence of the disease. Effect of vulvar diseases on self-regard, affective, and sexual life is potentially important. Therefore, time should be given for exhaustive explanations about etiology, nature, and course of the disease and consequences, if any, on sexual life. Causal treatment should also be associated with protective measures avoiding contacts with mechanical and chemical irritants. A nonexhaustive list of common recommendations includes avoiding fabric softeners, pads, detergents, cosmetic products containing color additives and flavors, and synthetic underwear. This is sometimes sufficient to eradicate irritant and contact dermatitis and limits risk of poor response to true dermatoses. In addition, any coexisting disorder, such as diabetes mellitus or urine incontinence, should be under control. Too often, women suffering from vulvar complains, especially itching, are still nowadays offered symptomatic treatment without diagnostic process or even without examination, such as over-the-counter delivery of any cream. This may, in some cases, lead, even in young people, to delayed diagnosis of life-threatening diseases, such as squamous cell carcinoma (SCC). For this reason, in the presence of vulvar complains, a diagnostic pathway including systematic physical examination is always mandatory. This raises the question of vulvar screening. Even if vulva shares some diseases with cervix and vagina, especially through HPV dependent lesions, the place of screening is not comparable. Indeed, vulvar cancer is ten times less frequent than cervical one. Most vulvar lesions are symptomatic, and vulva is accessible to observation. As a consequence, vulvar cytology development has a minor place, if any. On the contrary, vulvoscopy has to be regarded as a valid tool, especially in complicated clinical presentations and in situations where there is a risk of intraepithelial neoplasia or microinvasion [3]. Of course, this paper does not pretend to overview all the aspects of vulvar diseases. Consequently, selecting some of the most representative vulvar dermatoses is subjective. The four selected vulvar diseases described below illustrate the variety of pathologies which may be encountered and for which awareness is necessary. Lichen simplex chronicus, a nonspecific disorder, may be the expression of a so common contact dermatitis but may also reveal another underlying disease. Lichen sclerosus is the most current vulvar dermatosis in elderly and often easy to treat, requiring a sustained attention. Lichen planus, in spite of having some common points with the previous one, is clearly distinct and often more difficult to evaluate. Finally, vulvar Paget s disease remains a pathological condition difficult to handle because it is clinically nonspecific, rare, and easily missed and for which new treatments are necessary. 2. Lichen Simplex Chronicus This disorder is a chronic eczematous condition characterized by intense pruritus. Rubbing and scratching produce poorly demarcatedplaquesofthickenedlichenifiedskin.scalemay be subtle and results in slightly shining. Erosions and fissures can result from scratching and become infected. In children, atopic dermatis can result in lichen simplex chronicus, most often characterized by a widespread inflammatory eruption instead of vulvar lesions. Adults are more likely to present genital eczema. Treatment requires a three-steps process. The first step consists in identifying and eliminating all irritant and allergen exposures. Secondly, treatment requires the breaking of the itch-scratch-itch cycle, especially during nighttime sedation, with oral antihistamine drug taken at bedtime and high potency topical corticosteroid, once a day at bedtime. Additionally, identifying and treating concomitant infection are needed. Clinical control after one month is recommended. In some cases, another underlying pruritic condition might be revealed. If treatment fails or lichen simplex chronicus recurs, attention should be paid to psychological status of the patient. Psychological disturbances may as well be a cause or a consequence of persisting or recurring lesions. They should be treated specifically with appropriate support. As a result, surgical resection of a lichenified prominent labia majora should be an exceptional procedure. Pathologic analysis is of course necessary. 3. Lichen Sclerosus Lichen sclerosus is one of the most common dermatoses affecting vulva in elderly. The disease is sometimes asymptomatic, but pruritus is frequent and represents by far the main complaint. However, depending on the way disease has developed, other complaints may be expressed. Pain may result from fissures and induce, for example, dyspareunia or constipation when perianal. Dyspareunia may also be due to introitus narrowing.
 Representative example of a lichen sclerosus biopsy specimen showing a thinned epidermis with slight hyperkeratosis, loss of the rete ridges, and a band of homogenized collagen below the")

3 BioMed Research International 3 (a) (b) Figure 1: (a) Irregular white to brown patch on the vulvar skin of a 74-year-old woman. (b) Representative example of a lichen sclerosus biopsy specimen showing a thinned epidermis with slight hyperkeratosis, loss of the rete ridges, and a band of homogenized collagen below the dermoepidermal junction. Pathology is characterized by epithelial thinning down, sclerosis of the upper derma, and inflammatory infiltrate underneath (Figure 1(b)). Hyperkeratotic changes may also occur in some locations. Thin epithelium was previously thought to represent an atrophic state but is probably due to accelerated maturation. For that reason, this disease is no more called lichen sclerosus atrophicus. As a consequence, androgen-containing creams are no more up to date treatments, as they are not justified and as they induce virilization, locally (clitoral hypertrophy), or, sometimes, with general signs. Clinically, vulvar lichen sclerosus induces mainly whitening of the skin, due to sclerosis (Figure 1(a)). Topography is variable from focal to large bilateral extension and from periclitoral to perianal area. Labia minora are often affected, either thickened or reduced. Clitoral hood may merge, bury clitoris, and result in pseudocyst formation, containing smegma. Sclerosis of the introitus may result in sexual impairment and dyspareunia. Inflammatory stages during which pruritus may be especially present can induce some degreeofstromalcongestionandskinredness,fissuring,and hyperkeratotic reaction. Thinning of the skin, combined with itching, results in petechia. Dystrophy and chronic irritation are probably a favorable condition for inducing nuclear atypia in the deepest layers of epithelium, resulting in high grade vulvar intraepithelial neoplasia (VIN) of a differentiated type. As a consequence, most vulvar SCC of elderly occur on dystrophic vulva and result from degenerating focal VIN. Vagina is never affected. On the other hand, extragenital manifestationscanbeobserved. Etiology of lichen sclerosus is unknown but related to an autoimmune mechanism. Other autoimmune diseases occur in 21% of patients: thyroiditis (12%), alopecia areata (9%), and vitiligo (6%) are the most frequent ones. It is more frequent inwomenthaninmen.genitallocalizationcanoccuratall time from prepubertal age to elderly and is more common at theseagesthaninmiddleages[4]. In children, lichen sclerosus may be difficult to diagnose in some instances, or diagnosis is simply not expected. This should explain why mean interval between symptoms and diagnosis is reported to be around 1.7 years. At this period of life, vulvar folds are not completely developed, and vulvar folds changes nearly do not appear. Whitening may be present. Fissures can be nearly the only manifestation, especially around anus, inducing pain and constipation. These children may be suspected to be victim of sexual abuse, and this should be carefully taken in consideration. Furthermore, lichen sclerosus and abuse may coexist, the second triggering the first one. For that reason, any unexplained observation such as poor response to treatment should raise special attention [4]. Any parasitic origin such as oxyurosis should also be considered. Inyoungwomen,clinicalpresentationisnotespecially different than in elderly, but special attention should be paid to long-term risk of atrophic changes due to their effect on sexual life. In elderly, the most important part of the treatment is the control of pruritus. But sexual complains are not rare, because long-term progression of the disease, added to natural atrophic changes of lower genital tract, alters vestibular anatomy and function. Periodic examination of the vulva under treatment remains important at this age, even in the absenceofcomplain,becauseanypersistentdystrophicarea should be suspected to bear epithelial atypia and represent a VIN focus. Occurrence of SCC is debated in its causative relation to lichen sclerosus. Although this cancer occurs in no more than 5% of lichen sclerosus. In contrast, histologic signs of lichen sclerosus are present in 33% of cases of SCC of the vulva [4]. Older age and epithelial hyperplasia are independent risk factors. The presumed pathway would imply successively lichen sclerosus, hyperplasia, and lower atypia representing differentiated type VIN, then leading to carcinoma. However, this sequence is not well understood and even controversial [5]. Considering hypertrophic forms of lichen sclerosus as a potential precancerous disease is not unanimously admitted. In a short series of patients with hyperplastic changes in lichen sclerosus, in whom followup was available for at least 5 years, no progression to cancer was noticed [6]. This
4 4 BioMed Research International might be taken into consideration to avoid unuseful surgery. However, biopsy is necessary to assess the absence of atypia and observation is recommended in foci of hyperplastic epithelium in lichen sclerosus. The presence of epithelial atypia in association with lichensclerosusisalsocontroversial.itiscommonlyadmitted that VIN associated with lichen sclerosus is a differentiated type and that overexpression of p53 is present, contrary to what happens in undifferentiated type VIN, induced by HPV, and in which overexpression of p16 is encountered [5]. Once again, common link between differentiated type VIN and lichen sclerosus is debated [6], and at least one report previously showed that VIN associated with lichen sclerosus is most often of the undifferentiated type [7]. These data illustrate how it is difficult to obtain agreement between members from one or from different communities. This, in turn, affects dialog between clinicians and pathologists and sometimes makes surgical decisions difficult to discuss. Treatment of lichen sclerosus is nearly always based on the use of potent corticosteroid cream. Application in the adequate area is to be teached, especially in elderly, because the area is not always easy to reach. Patients have to learn the way cream must be applied until complete skin absorption. Treatment effect has to be followed up on both complaints and objective vulvar appearance. This allows detecting wrong appliance of treatment or nonresponding suspect areas. Treatment must be adjusted, and applications reduced to minimal frequency and amount of cream needed. This reduces secondary effects risk of long-term use and leaves therapeutic margin if disease gets more active later. When disease is totally under control, stopping treatment for sometimes long periods should be debated. It is certainly indicated in younger patients and has to be discussed in older ones, who should always be followed up on a long-term basis, either treated or not, even if objective cancer occurrence risk is lower than 5%. The place of topical calcineurin inhibitors in the treatment of lichen sclerosus and other conditions such as lichen planus is worth thinking about. Topical calcineurin inhibitors are to be considered as a second-line treatment, when all reasonably possible adjustments of corticoid creams have been tested [8]. In some instances, corticoid creams are not or no more tolerated (delayed-type hypersensitivity reactions) or become less efficient, leading to increasing treatment doses (tachyphylaxis). They may also induce rebound erythroderma or lead to cutaneous atrophy. The main advantages of calcineurin inhibitors are to avoid tachyphylaxis and cutaneous atrophy. Nevertheless, they are associated with secondary effects. Topical calcineurin inhibitors commonly induce transient local burning or irritation. Facial flushing after alcohol ingestion and rosaceiform dermatitis may also less commonly occur [9]. Long-term safety profile of topical calcineurin inhibitors has been questioned, especially as they have been suspected to increase cancer risk. However, it seems reasonable to assess that this risk has been overestimated. It is, in fact, not higher than in the general population [10]. It has been demonstrated that potential systemic effects of topical calcineurin inhibitors are lower than that of corticosteroids, due to their weaker permeation potential. For that reason, lymphoproliferative changes observed in monkeys did not result in a higher risk in patients. Risk of immunosuppression was not documented by any increased risk of systemic or skin infections. Photocarcinogenicity was not described in patients using topical regimens [9]. Eventually, SCC occurring in the presence of topical calcineurin inhibitors was investigated by the US FDA. Twenty nine cases were reported worldwide and only 3 occurred in cases of lichen sclerosus [4]. Considering all these aspects, topical calcineurin inhibitors should be regarded as a second-line treatment. It has to be presented as an off-label option, if possible for short durations, owing to previous considerations and to their costs, clearly higher than that of corticosteroids [4]. Surgical treatment is limited to some indications: surgery of clitoral hood when clitoral phimosis is sexually detrimental or when a painful pseudocyst has developed; enlargement of introitus when superficial dyspareunia occurs; resection of dystrophic zones when biopsy demonstrates associated VIN or vulvectomy in the presence of carcinoma. 4. Lichen Planus Lichen planus (Figure 2) is a more uncommon condition that may be asymptomatic, itchy, or more frequently painful. This is mainly due to frequent erosive forms, especially those affecting vestibulae. Chronic vaginal discharge and dyspareunia are frequently associated. Pathology may show different patterns, in relation to different clinical appearances. Epidermis can be thickened or erosive. Basal cell layer shows some areas of vacuolar degeneration. A band-like mononuclear infiltrate is present in the upper dermis (Figure2(b)). Clinically, vulvar lesions can be represented by different patterns, including violaceous shiny papules, reticular white networks, or erosive forms, especially on the vestibulae and vagina (Figure 2(a)). Actually, in contrast to lichen sclerosus, it can extend to vagina and turn, in this location, to extremely invalidating and difficult to treat erosive vaginitis. Extragenital and buccal locations are frequent. Erosive vulvovaginogingival lichen planus is known as the syndrome of Hewitt and Pelisse. Consensus on the diagnostic criteria for erosive vulvar lichen planus was recently defined by members of Vulvar Diseases Societies [11]. Nine criteria were gathered of which three should be present to support the diagnostic: (i) well-demarcated erosions/erythematous areas at the vaginal introitus; (ii) presence of a hyperkeratotic border to lesions and/or Wickham striae in surrounding skin; (iii) symptoms of pain/burning; (iv) scarring/loss of normal architecture; (v) presence of vaginal inflammation; (vi) involvement of other mucosal surfaces; (vii) presence of a well-defined inflammatory band involving the dermoepidermal junction; (viii) presence of an inflammatory band consisting predominantly of lymphocytes; and (ix) signs of basal layer degeneration.


 (b) Figure 3: (a) Wide red area extending mainly on the left")
 Representative example of Paget s disease biopsy specimen")


















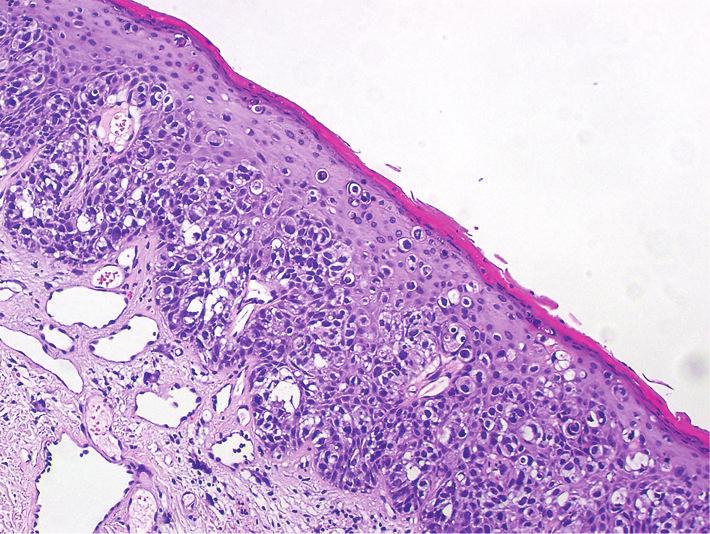
5 BioMed Research International 5 (a) (b) Figure 2: (a) Wide vestibular erythematous erosive lichen planus in a 79-year-old woman. (b) Representative example of a lichen planus biopsy specimen showing an irregular hyperkeratosis and a lymphoid dermal infiltrate appearing as a distinct band close to the epidermis. (a) (b) Figure 3: (a) Wide red area extending mainly on the left side of the vulva in a 65-year-old woman with Paget s disease. (b) Representative example of Paget s disease biopsy specimen showing many glandular neoplastic cells with clear cytoplasm present singly or in small nests within the epidermis. Etiology is, as for lichen sclerosus, suspected to be autoimmune. Moreover, in some cases, mixed forms of lichen planus and sclerosus are encountered. This disease is rare in younger and older patients. Most of affected people are middle aged around 30 to 60 years. Treatment is targeted against complains. Pruritic lesions respond to local applications of highly potent corticoid creams, but response may be more difficult to achieve than in lichen sclerosus. Far more difficult is, anyway, the control of dyspareunia, related to vestibular and vaginal erosions. These conditions always respond to some degree to the same treatment, but results are often precarious, incomplete, or, in the end, not satisfactory. Topical corticoid use in the vagina may require specific preparations, incorporating, for example, corticoid drug in adeps solidus suppositories or in carbopol gel. Topical calcineurin inhibitors may have to be tried when results are not satisfactory. Systemic oral corticoids are considered when topical treatments fail. Surgery is sometimes necessary to lyse vaginal adhesions or to restore vestibular anatomy in case of impaired sexual function. But these conditions are difficult to treat and satisfactory results are far from being the rule. 5. Vulvar Paget s Disease Paget s disease is mainly a disease of elderly. Mean age is around 65 years of age. A special attention should be paid to this rare disease, because its clinical appearance might suggest other conditions, such as eczema, lichen simplex chronicus, psoriasis, high grade VIN, and others. This consideration illustrates the fact that a high degree of suspicion must legitimately lead to prompt biopsy in the presence of nonspecific clinical presentations, especially if a first-line treatment fails to induce clinical improvement. On the contrary, the nonspecific presentation and complaints, in frequently old patients, explain the time between onset of complaints and diagnosis, estimated around two years [12]. Here again, pruritus is a common initial symptom. Pain can substitute when erosion occurs. Complaints are limited to the often quite delineated involved area. Clinically, the lesion is often described as red, welldelineated, with a scaling or sometimes erosive surface, in the area of keratinized vulvar skin, and as far as perianal region (Figure 3(a)). The lesion is chronic, and a history of local discomfort may exist years before diagnosis. Early clinical signs are probably highly nonspecific, as it can be
6 6 BioMed Research International seen in early recurrences observed during followup, where still asymptomatic patients present minor erosions or slight focal redness. Pathology is the only reliable key for diagnosis and requires scattered large clear muciparous cells with nuclear atypia, inside the epidermis (Figure 3(b)). They can be present also in skin appendages. Underlying chronic infiltrate is often described. Presence of these cells in the dermis reflects an invasive form, which is a rare occurrence of the disease. Etiology is related to the glandular nature of abnormal cells and to the fact that Paget s disease, either mammary or extramammary, appears nearly exclusively in skin areas where apocrine glands are present. However, some believe that malignant cells are pluripotent epidermal ones. In spite of the fact that invasive disease is rare, association with underlying internal malignancies is a wellknown characteristic of the disease, but its frequency is diversely appreciated and should be probably around 10 to 20%. For that reason, different authors recommend routine endoscopic genital-urinary and intestinal tract exploration to be performed [13]. Treatment is mainly surgical, especially when diagnosed for the first time. Unfortunately, the procedure is far from being always satisfactory. The lesion is not well delineated as the clinical presentation might suggest, and the disease is often present, somewhat far from the apparent margin. Recommended surgical margin goes up to 2 to 3 centimeters outside apparent limit of the disease, depending on whether it seems well delineated or not. Some surgeons perform frozen section margins control during surgery, but even this precaution may lead to final pathology reporting up to 10% positive margins [13]. Others reported failure rates of 20 to 60%, even if variant surgical procedures, such as Mohs micrographic surgery, improve results with recurrence rates lowered down to 16% [12]. Other treatments are currently offered and include interferon alpha, topical fluorouracil, imiquimod, CO 2 laser ablation, and, more recently, photodynamic therapy [14]. They should be considered as alternatives to surgery or to cure recurrences, while regarding radiotherapy as the ultimate solution, due to its long-term secondary effects, and taking into account the fact that any further treatment would possibly be difficult or impossible to use after radiotherapy. Due to the nature of the disease, and its frequent microscopic extension to apparently normal surrounding skin, posttreatment biopsies are of low interest. Clinical remission and symptoms resolution are reasonable results for treatment [12]. 6. Conclusion The examples of these four frequent vulvar dermatoses underscore the importance of considering a wide range of diagnosestoobtainanaccuratediagnosis.aclosecooperation between clinicians and pathologists is also mandatory. Finally, exhaustive explanations relative to diagnosis and treatment and psychological support for the patient have to be integrated in the management of these diseases. Conflict of Interests The authors declare that there is no conflict of interests regarding the publication of this paper. References [1] P. J. Lynch, M. Moyal-Barrocco, F. Bogliatto, L. Micheletti, and J. Scurry, 2006 ISSVD classification of vulvar dermatoses: pathologic subsets and their clinical correlates, The Journal of Reproductive Medicine,vol.52,no.1,pp.3 9,2007. [2] P. J. Lynch, M. Moyal-Barracco, J. Scurry, and C. Stockdale, 2011 ISSVD terminology and classification of vulvar dermatological disorders: an approach to clinical diagnosis, Journal of Lower Genital Tract Disease,vol.16,no.4,pp ,2012. [3] L. J. Eva, Screening and follow up of vulval skin disorders, Best Practice & Research Clinical Obstetrics & Gynaecology, vol.26, no. 2, pp , [4] S.K.FistarolandP.H.Itin, Diagnosisandtreatmentoflichen sclerosus, American Journal of Clinical Dermatology,vol.14,no. 1, pp , [5] M. del Pino, L. Rodriguez-Carunchio, and J. Ordi, Pathways of vulvar intraepithelial neoplasia and squamous cell carcinoma, Histopathology,vol.62,no.1,pp ,2013. [6] W. Weyers, Hypertrophic lichen sclerosus with dyskeratosis and parakeratosis a common presentation of vulvar lichen sclerosus not associated with significant risk of malignancy, The American Journal of Dermatopathology, vol.35,no.7,pp , [7]M.VanSeters,F.J.W.TenKate,M.VanBeurdenetal., In the absence of (early) invasive carcinoma, vulvar intraepithelial neoplasia associated with lichen sclerosus is mainly of undifferentiated type: new insights in histology and aetiology, Journal of Clinical Pathology, vol. 60, no. 5, pp , [8] A. T. Goldstein, A. Creasey, R. Pfau, D. Phillips, and L. J. Burrows, A double-blind, randomized controlled trial of clobetasol versus pimecrolimus in patients with vulvar lichen sclerosus, Journal of the American Academy of Dermatology,vol.64,no.6, pp. e99 e104, [9] B. A. Cook and E. M. Warshaw, Role of topical calcineurin inhibitors in the treatment of seborrheic dermatitis, American Journal of Clinical Dermatology,vol.10,no.2,pp ,2009. [10] E. C. Siegfried, J. C. Jaworski, and A. A. Hebert, Topical calcineurin inhibitors and lymphoma risk: evidence update with implications for daily practice, American Journal of Clinical Dermatology,vol.14,no.3,pp ,2013. [11] R. C. Simpson, K. S. Thomas, P. Leighton, and R. Murphy, Diagnostic criteria for erosive lichen planus affecting the vulva: an international electronic-delphi consensus exercise, British Journal of Dermatology,vol.169,no.2,pp ,2013. [12] P. Sanderson, A. Innamaa, J. Palmer, and J. Tidy, Imiquimod therapy for extramammary Paget s disease of the vulva: a viable non-surgical alternative, Journal of Obstetrics & Gynecology, vol. 33, pp , [13] J.Y.W.Chan,G.K.H.Li,J.H.Chung,andV.L.Y.Chow, Extramammary Paget s disease: 20 years of experience in Chinese population, International Journal of Surgical Oncology, vol. 2012,ArticleID416418,5pages,2012. [14] C. Anton, A. V. D. C. Luiz, F. M. Carvalho, E. C. Baracat, and J. P. Carvalho, Clinical treatment of vulvar Paget s disease: a case report, Clinics, vol. 66, no. 6, pp , 2011.
Disorders of the vulva
 Vulval lesions Disorders of the vulva Terminology standardised by the International Society for the Study of Vulvovaginal Disease(ISSVD) Classification 1.Nonneoplastic epithelial disorders of vulva Lichen
Vulval lesions Disorders of the vulva Terminology standardised by the International Society for the Study of Vulvovaginal Disease(ISSVD) Classification 1.Nonneoplastic epithelial disorders of vulva Lichen
Diseases of the vulva
 Diseases of the vulva 1. Bartholin Cyst - Infection of the Bartholin gland produces an acute inflammation within the gland (adenitis) and may result in an abscess. Bartholin duct cysts - Are relatively
Diseases of the vulva 1. Bartholin Cyst - Infection of the Bartholin gland produces an acute inflammation within the gland (adenitis) and may result in an abscess. Bartholin duct cysts - Are relatively
Clinically Microscopically Pathogenesis: autoimmune not lifetime
 Vulvar Diseases: Can be divided to non-neoplastic and neoplastic diseases. The neoplastic diseases are much less common. Of those, squamous cell carcinoma is the most common. most common in postmenopausal
Vulvar Diseases: Can be divided to non-neoplastic and neoplastic diseases. The neoplastic diseases are much less common. Of those, squamous cell carcinoma is the most common. most common in postmenopausal
Lichen sclerosus. Lichen planus
 Lichen sclerosus Lichen planus Dr Fiona Lewis, Consultant Dermatologist, Heatherwood and Wexham Park NHS Foundation Trust & St John s Institute of Dermatology, GSTT Outline Typical features of lichen sclerosus
Lichen sclerosus Lichen planus Dr Fiona Lewis, Consultant Dermatologist, Heatherwood and Wexham Park NHS Foundation Trust & St John s Institute of Dermatology, GSTT Outline Typical features of lichen sclerosus
The Case of Mrs. Virginia Jones* Asst. Professor Division of Gyne-Oncology University of British Columbia, Department of Gynecology Vancouver, Canada
 Case title: Case authors: Case synopsis: The Case of Mrs. Virginia Jones* Dr. Leslie A. Sadownik Asst. Professor Division of Gyne-Oncology University of British Columbia, Department of Gynecology Vancouver,
Case title: Case authors: Case synopsis: The Case of Mrs. Virginia Jones* Dr. Leslie A. Sadownik Asst. Professor Division of Gyne-Oncology University of British Columbia, Department of Gynecology Vancouver,
Vaginal involvement in genital erosive lichen planus
 Acta Obstetricia et Gynecologica. 2010; 89: 966 970 SHORT REPORT Vaginal involvement in genital erosive lichen planus ANNE LISE ORDING HELGESEN 1,2,3, PETTER GJERSVIK 3,4, PETER JEBSEN 5, ROLF KIRSCHNER
Acta Obstetricia et Gynecologica. 2010; 89: 966 970 SHORT REPORT Vaginal involvement in genital erosive lichen planus ANNE LISE ORDING HELGESEN 1,2,3, PETTER GJERSVIK 3,4, PETER JEBSEN 5, ROLF KIRSCHNER
VULVAR CARCINOMA. Page 1 of 5
 VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
OCCG SERVICE SPECIFICATION (2017/18)
") OCCG SERVICE SPECIFICATION (2017/18) Primary Care Service for Skin Cancers: Dermatology Shared Care Monitoring for Melanoma, Lichen Sclerosus and Squamos Cell Carcinoma 1. Background For patients who have
OCCG SERVICE SPECIFICATION (2017/18) Primary Care Service for Skin Cancers: Dermatology Shared Care Monitoring for Melanoma, Lichen Sclerosus and Squamos Cell Carcinoma 1. Background For patients who have
VIN/VAIN O C T O B E R 3 RD J M O R G A N
 VIN/VAIN O C T O B E R 3 RD 2 0 1 8 J M O R G A N Vaginal Intraepithelial Neoplasia VAIN I, II, III Incidence 0.1/100,000 women in US Mean age 50s (J Womens Health (Larchmt) 2009:18:1731) (J Obstet Gynaecol
VIN/VAIN O C T O B E R 3 RD 2 0 1 8 J M O R G A N Vaginal Intraepithelial Neoplasia VAIN I, II, III Incidence 0.1/100,000 women in US Mean age 50s (J Womens Health (Larchmt) 2009:18:1731) (J Obstet Gynaecol
Meet the ISSVD. President ISSVD. Jacob Bornstein, MD
 Meet the ISSVD Jacob Bornstein, MD President ISSVD Chairman, Department of Obstetrics and Gynecology Western Galilee Hospital Bar-Ilan University Faculty of Medicine Nahariya, Israel ISSVD Symposium: The
Meet the ISSVD Jacob Bornstein, MD President ISSVD Chairman, Department of Obstetrics and Gynecology Western Galilee Hospital Bar-Ilan University Faculty of Medicine Nahariya, Israel ISSVD Symposium: The
Spectrum of Vulvar Lesions in an Obstetrics and Gynecology Outpatient Clinic
 in an Obstetrics and Gynecology Outpatient Clinic Ozhan Ozdemir, Mustafa Erkan Sari, Funda Arpaci Ertugrul, Ertugrul Sen, Bunyamin Ugur Ilgin, Cemal Atalay Ankara Numune Education and Research Hospital,
in an Obstetrics and Gynecology Outpatient Clinic Ozhan Ozdemir, Mustafa Erkan Sari, Funda Arpaci Ertugrul, Ertugrul Sen, Bunyamin Ugur Ilgin, Cemal Atalay Ankara Numune Education and Research Hospital,
Management of benign vulval dermatoses in primary care
 PRESCRIBING IN PRACTICE Management of benign vulval dermatoses in primary care MITESH PATEL AND DAVID NUNNS SPL Vulval dermatoses can be difficult to manage in primary care, and GPs need to be aware of
PRESCRIBING IN PRACTICE Management of benign vulval dermatoses in primary care MITESH PATEL AND DAVID NUNNS SPL Vulval dermatoses can be difficult to manage in primary care, and GPs need to be aware of
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
4/3/2017 DIAGNOSIS AND THERAPY OF RECURRENT VULVOVAGINAL SYMPTOMS BACTERIAL VAGINOSIS EPIDEMIOLOGY OBJECTIVES
 DIAGNOSIS AND THERAPY OF RECURRENT VULVOVAGINAL SYMPTOMS KELLY HODGES, MD (NO DISCLOSURES) OBJECTIVES REVIEW THE TWO MOST COMMON CAUSES OF RECURRENT ABNORMAL DISCHARGE (CANDIDA AND BV) REVIEW THE MOST
DIAGNOSIS AND THERAPY OF RECURRENT VULVOVAGINAL SYMPTOMS KELLY HODGES, MD (NO DISCLOSURES) OBJECTIVES REVIEW THE TWO MOST COMMON CAUSES OF RECURRENT ABNORMAL DISCHARGE (CANDIDA AND BV) REVIEW THE MOST
Conflicts of interest
 Vulvar Cases 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology)
Vulvar Cases 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology)
Summary. Accepted for publication 18 May Key words genital lichen planus, oral lichen planus, vulval lichen planus
 CLINICAL AND LABORATORY INVESTIGATIONS DOI 10.1111/j.1365-2133.2006.07480.x Prevalence of vulval lichen planus in a cohort of women with oral lichen planus: an interdisciplinary study P. Belfiore, O. Di
CLINICAL AND LABORATORY INVESTIGATIONS DOI 10.1111/j.1365-2133.2006.07480.x Prevalence of vulval lichen planus in a cohort of women with oral lichen planus: an interdisciplinary study P. Belfiore, O. Di
Squamous Cell Neoplasia and Precursor Lesions
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
HOW TO DIAGNOSE VULVAR DISEASES:
 HOW TO DIAGNOSE VULVAR DISEASES: Diagnostic approach. Normal findings. Maria Sol Peremateu, MD A wide spectrum of benign, premalignant, and malignant lesions may occur on the vulva. Some of the disorders
HOW TO DIAGNOSE VULVAR DISEASES: Diagnostic approach. Normal findings. Maria Sol Peremateu, MD A wide spectrum of benign, premalignant, and malignant lesions may occur on the vulva. Some of the disorders
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Treatment of Bowenoid and Basaloid Vulvar Intraepithelial Neoplasia 2/3 with Imiquimod 5% Cream DO NOT DUPLICATE
 The Journal of Reproductive Medicine Treatment of Bowenoid and Basaloid Vulvar Intraepithelial Neoplasia 2/3 with Imiquimod 5% Cream Claudia Marchitelli, M.D., Graciela Secco, M.D., Myriam Perrotta, M.D.,
The Journal of Reproductive Medicine Treatment of Bowenoid and Basaloid Vulvar Intraepithelial Neoplasia 2/3 with Imiquimod 5% Cream Claudia Marchitelli, M.D., Graciela Secco, M.D., Myriam Perrotta, M.D.,
The use of CO2 laser for patients with Lichen sclerosus
 The use of CO2 laser for patients with Lichen sclerosus Dr. Christina Kuhler-Obbarius, Elisabeth Kunkel, Dr. Matthias Theden-Schow, Hamburg, Germany Our clinical center located in Hamburg includes eight
The use of CO2 laser for patients with Lichen sclerosus Dr. Christina Kuhler-Obbarius, Elisabeth Kunkel, Dr. Matthias Theden-Schow, Hamburg, Germany Our clinical center located in Hamburg includes eight
Clinical Scoring System to Detect Malignant and Premalignant Vulval Lesions
 The Journal of Obstetrics and Gynecology of India (January February 2014) 64(1):41 46 DOI 10.1007/s13224-013-0458-3 ORIGINAL ARTICLE Clinical Scoring System to Detect Malignant and Premalignant Vulval
The Journal of Obstetrics and Gynecology of India (January February 2014) 64(1):41 46 DOI 10.1007/s13224-013-0458-3 ORIGINAL ARTICLE Clinical Scoring System to Detect Malignant and Premalignant Vulval
Nomenclature (terminology) refers to the naming of
 refers to the naming of") 2011 ISSVD Terminology and Classification of Vulvar Dermatological Disorders: An Approach to Clinical Diagnosis Peter J. Lynch, MD, Micheline Moyal-Barracco, MD, James Scurry, MD, and Colleen Stockdale,
2011 ISSVD Terminology and Classification of Vulvar Dermatological Disorders: An Approach to Clinical Diagnosis Peter J. Lynch, MD, Micheline Moyal-Barracco, MD, James Scurry, MD, and Colleen Stockdale,
Vulval dermatoses. Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough
 Vulval dermatoses Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough Pigmentation Vulvodynia Ulcers Genetic Pruritus VULVAL
Vulval dermatoses Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough Pigmentation Vulvodynia Ulcers Genetic Pruritus VULVAL
Lichen planus. Information for patients Gynaecology
 Lichen planus Information for patients Gynaecology page 2 of 8 What is lichen planus? Lichen planus is a non-cancerous, inflammatory skin condition that causes an itchy, non-infectious rash (small purple
Lichen planus Information for patients Gynaecology page 2 of 8 What is lichen planus? Lichen planus is a non-cancerous, inflammatory skin condition that causes an itchy, non-infectious rash (small purple
Vulval Intraepithelial Neoplasia (VIN)
") Vulval Intraepithelial Neoplasia (VIN) Exceptional healthcare, personally delivered What is it? Vulval intraepithelial neoplasia (VIN) is a condition where there are pre-cancerous cells in the skin of
Vulval Intraepithelial Neoplasia (VIN) Exceptional healthcare, personally delivered What is it? Vulval intraepithelial neoplasia (VIN) is a condition where there are pre-cancerous cells in the skin of
Journal of International Academy of Forensic Science & Pathology (JIAFP)
") Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Kelly H. Tyler, MD, FACOG, FAAD S052 Gender Dermatology: Diagnosis and Treatment of Genital Skin Disorders Vulvar Dermatitis
 Vulvar Dermatitis Kelly H. Tyler, MD, FACOG, FAAD Assistant Professor The Ohio State University Department of Internal Medicine, Division of Dermatology Department of Obstetrics and Gynecology Center for
Vulvar Dermatitis Kelly H. Tyler, MD, FACOG, FAAD Assistant Professor The Ohio State University Department of Internal Medicine, Division of Dermatology Department of Obstetrics and Gynecology Center for
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
Access from the University of Nottingham repository:
 Simpson, Rosalind C. and Nunns, David (2017) Skin diseases affecting the vulva. Obstetrics, Gynaecology and Reproductive Medicine, 27 (3). pp. 77-85. ISSN 1879-3622 Access from the University of Nottingham
Simpson, Rosalind C. and Nunns, David (2017) Skin diseases affecting the vulva. Obstetrics, Gynaecology and Reproductive Medicine, 27 (3). pp. 77-85. ISSN 1879-3622 Access from the University of Nottingham
Postmenopausal Vulvar Pruritus - Colposcopic Diagnosis and Treatment
 Postmenopausal Vulvar Pruritus - Colposcopic Diagnosis and Treatment Pages with reference to book, From 315 To 317 A Bilge Sener, Neslihan C. Seckin, Oya Gokmen ( Departments of Menopause, Dr. Z.T.B. Women
Postmenopausal Vulvar Pruritus - Colposcopic Diagnosis and Treatment Pages with reference to book, From 315 To 317 A Bilge Sener, Neslihan C. Seckin, Oya Gokmen ( Departments of Menopause, Dr. Z.T.B. Women
Inflammatory Dermatoses of the Vulva for the General/Gyn Pathologist with emphasis in the lichenoid pattern
 Inflammatory Dermatoses of the Vulva for the General/Gyn Pathologist with emphasis in the lichenoid pattern By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor
Inflammatory Dermatoses of the Vulva for the General/Gyn Pathologist with emphasis in the lichenoid pattern By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor
Advanced Training Skills Module August Vulval Disease
 Introduction Vulval Disease This module is designed to provide training in all aspects of vulval disease. Successful completion of the ATSM will equip an individual to develop this aspect of care in their
Introduction Vulval Disease This module is designed to provide training in all aspects of vulval disease. Successful completion of the ATSM will equip an individual to develop this aspect of care in their
WHITE PAPER SmartXide 2 V 2 LR. MonaLisa Touch Dual Probe Therapy for the Treatment of Lichen Sclerosus and Vaginal Atrophy
 WHITE PAPER SmartXide 2 V 2 LR MonaLisa Touch Dual Probe Therapy for the Treatment of Lichen Sclerosus and Vaginal Atrophy DEKA White Paper SMARTXIDE 2 V 2 LR November 2015 MonaLisa Touch Dual Probe Therapy
WHITE PAPER SmartXide 2 V 2 LR MonaLisa Touch Dual Probe Therapy for the Treatment of Lichen Sclerosus and Vaginal Atrophy DEKA White Paper SMARTXIDE 2 V 2 LR November 2015 MonaLisa Touch Dual Probe Therapy
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Vulvar Disease Clinical Cases
 Vulvar Disease Clinical Cases Hope K. Haefner, MD Professor University of Michigan Health System February 27, 2015 Cartagena Conflicts of Interest Hope Haefner, MD is on the Advisory Board of Merck Co.,
Vulvar Disease Clinical Cases Hope K. Haefner, MD Professor University of Michigan Health System February 27, 2015 Cartagena Conflicts of Interest Hope Haefner, MD is on the Advisory Board of Merck Co.,
PACKAGE LEAFLET: INFORMATION FOR THE USER. Flutarzole 0,05% w/w cream, Fluticasone propionate
 PACKAGE LEAFLET: INFORMATION FOR THE USER Flutarzole 0,05% w/w cream, Fluticasone propionate 1. IDENTIFICATION OF THE MEDICINAL PRODUCT 1.1. Trade name Flutarzole 1.2. Composition Active substance: Fluticasone
PACKAGE LEAFLET: INFORMATION FOR THE USER Flutarzole 0,05% w/w cream, Fluticasone propionate 1. IDENTIFICATION OF THE MEDICINAL PRODUCT 1.1. Trade name Flutarzole 1.2. Composition Active substance: Fluticasone
Rameshwar Gutte and Uday Khopkar
 Extragenital unilateral lichen sclerosus et atrophicus in a child: a case report Rameshwar Gutte and Uday Khopkar Department of Dermatolgy, Seth GSMC and KEM Hospital, Parel, Mumbai-400012, India Egyptian
Extragenital unilateral lichen sclerosus et atrophicus in a child: a case report Rameshwar Gutte and Uday Khopkar Department of Dermatolgy, Seth GSMC and KEM Hospital, Parel, Mumbai-400012, India Egyptian
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Asymptomatic Undiagnosed Lichen Sclerosus
 Asymptomatic Undiagnosed Lichen Sclerosus Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology) Geisel School of Medicine at Dartmouth Lebanon, NH, USA Disclosures
Asymptomatic Undiagnosed Lichen Sclerosus Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology) Geisel School of Medicine at Dartmouth Lebanon, NH, USA Disclosures
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Human Papillomavirus Induced Squamous Intraepithelial Lesions in Vulvar Lichen Planus
 ORIGINAL RESEARCH ARTICLE Human Papillomavirus Induced Squamous Intraepithelial Lesions in Vulvar Lichen Planus Sigrid Regauer, MD, 1 Barbara Eberz, MD, 2 and Olaf Reich, MD 3 Objectives: Approximately
ORIGINAL RESEARCH ARTICLE Human Papillomavirus Induced Squamous Intraepithelial Lesions in Vulvar Lichen Planus Sigrid Regauer, MD, 1 Barbara Eberz, MD, 2 and Olaf Reich, MD 3 Objectives: Approximately
Lichenoid dermatitis of the Vulva: Diagnosis and Differential Diagnosis for the Gynecological Pathologist
 Lichenoid dermatitis of the Vulva: Diagnosis and Differential Diagnosis for the Gynecological Pathologist Maria Angelica Selim, MD Professor of Pathology and Dermatology Duke University Medical Center
Lichenoid dermatitis of the Vulva: Diagnosis and Differential Diagnosis for the Gynecological Pathologist Maria Angelica Selim, MD Professor of Pathology and Dermatology Duke University Medical Center
MALE GENITAL (PENIS) LICHEN SCLEROSUS
 LICHEN SCLEROSUS") MALE GENITAL (PENIS) LICHEN SCLEROSUS What are the aims of this leaflet? This leaflet has been written to help you understand more about male genital lichen sclerosus (also known as balanitis xerotica
MALE GENITAL (PENIS) LICHEN SCLEROSUS What are the aims of this leaflet? This leaflet has been written to help you understand more about male genital lichen sclerosus (also known as balanitis xerotica
Vulval intraepithelial neoplasia. Information for patients Gynaecology
 Vulval intraepithelial neoplasia Information for patients Gynaecology page 2 of 8 What is vulval intraepithelial neoplasia? Vulval intraepithelial neoplasia (VIN) is not cancer. VIN is a disease of the
Vulval intraepithelial neoplasia Information for patients Gynaecology page 2 of 8 What is vulval intraepithelial neoplasia? Vulval intraepithelial neoplasia (VIN) is not cancer. VIN is a disease of the
What are the symptoms of a vulval skin condition?
 Information for you Published in December 2013 Skin conditions of the vulva About this information This information is for you if you want to know about skin conditions affecting the vulva. If you are
Information for you Published in December 2013 Skin conditions of the vulva About this information This information is for you if you want to know about skin conditions affecting the vulva. If you are
Gynecological Cancers
 Gynecological Cancers Outline Ovarian Cancer Uterine (Endometrial) Cancer Cervical Cancer Vulvar Cancer Vaginal Cancer Overian Cancer Ovarian cancer is cancer that forms in the tissue of the ovary and
Gynecological Cancers Outline Ovarian Cancer Uterine (Endometrial) Cancer Cervical Cancer Vulvar Cancer Vaginal Cancer Overian Cancer Ovarian cancer is cancer that forms in the tissue of the ovary and
Diagnosis and Management of Vulvar Disorders
 Diagnosis and Management of Vulvar Disorders Kelly H. Tyler, MD, FACOG, FAAD Assistant Professor The Ohio State University Department of Internal Medicine, Division of Dermatology Department of Obstetrics
Diagnosis and Management of Vulvar Disorders Kelly H. Tyler, MD, FACOG, FAAD Assistant Professor The Ohio State University Department of Internal Medicine, Division of Dermatology Department of Obstetrics
Vulvar squamous cell carcinoma
 The Clinical Significance of Stratifying Vulval Squamous Carcinoma into HPV and Non-HPV Related Variants C. BLAKE GILKS MD FRCPC Dept of Pathology, University of British Columbia Vulvar squamous cell carcinoma
The Clinical Significance of Stratifying Vulval Squamous Carcinoma into HPV and Non-HPV Related Variants C. BLAKE GILKS MD FRCPC Dept of Pathology, University of British Columbia Vulvar squamous cell carcinoma
Dysplasia, Mimics and Other Controversies
 Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
الاكزيماتيد= Eczematid
 1 / 7 2 / 7 Pityriasis Debate confusing of hypopigmentation characterized increasing surrounded differ hypomelanotic "progressive exists alba misnomer extensive a to observed term the applied term derived
1 / 7 2 / 7 Pityriasis Debate confusing of hypopigmentation characterized increasing surrounded differ hypomelanotic "progressive exists alba misnomer extensive a to observed term the applied term derived
JMSCR Vol 05 Issue 10 Page October 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i10.125 Histomorphological Study of Lichen Planus
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i10.125 Histomorphological Study of Lichen Planus
11/1/18. Age and Vulvar Pathology ANATOMY. Prepuce Clitoris Vestibule Hart line. Labia. minora. Labia. majora. Fourchette.
 Age and Vulvar Pathology Maria Angelica Selim, MD Professor of Pathology and Dermatology Director Dermatopathology Unit Duke University Medical Center Labia minora Labia majora Bartholin s duct Prepuce
Age and Vulvar Pathology Maria Angelica Selim, MD Professor of Pathology and Dermatology Director Dermatopathology Unit Duke University Medical Center Labia minora Labia majora Bartholin s duct Prepuce
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
3/25/2019. J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse
 J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse 1 4 th most common GYN cancer 5% of malignancies of GYN type. 4850 new cases annually 1030 deaths Cigarette smoking Vulvar dystrophy (Lichen
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse 1 4 th most common GYN cancer 5% of malignancies of GYN type. 4850 new cases annually 1030 deaths Cigarette smoking Vulvar dystrophy (Lichen
Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva Malignant melanoma sho
 Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
CASE 4 21/07/2017. Ectopic Prostatic Tissue in Cervix. Female 31. LLETZ for borderline nuclear abnormalities
 Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Vulvar intraepithelial neoplasia: Current concepts
 Vulvar intraepithelial neoplasia: Current concepts L. Stewart Massad, M.D. Dept. of Obstetrics & Gynecology Washington University School of Medicine St. Louis, MO Disclosure I have no financial ties to
Vulvar intraepithelial neoplasia: Current concepts L. Stewart Massad, M.D. Dept. of Obstetrics & Gynecology Washington University School of Medicine St. Louis, MO Disclosure I have no financial ties to
Vulva Cancer Histopathology Reporting Proforma
 Vulva Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Ethnicity Unknown AboriginalTorres
Vulva Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Ethnicity Unknown AboriginalTorres
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Lichen sclerosus. Information for patients Gynaecology
 Lichen sclerosus Information for patients Gynaecology page 2 of 8 What is lichen sclerosus? Lichen sclerosus is a skin condition that most often affects the vulva (the outer folds of skin around your vagina).
Lichen sclerosus Information for patients Gynaecology page 2 of 8 What is lichen sclerosus? Lichen sclerosus is a skin condition that most often affects the vulva (the outer folds of skin around your vagina).
Conflicts of interest. Genital Lichen Planus. Objectives. Lichen Planus. Genital Lichen Planus. Author Up To Date. Vulvar Lichen Planus Patterns
 Genital Lichen Planus Lynette J. Margesson MD FRCPC AAD Washington Mucous Membrane Symposium Saturday, March 2, 2019 Conflicts of interest Author Up To Date Little evidence based treatment Too few studies
Genital Lichen Planus Lynette J. Margesson MD FRCPC AAD Washington Mucous Membrane Symposium Saturday, March 2, 2019 Conflicts of interest Author Up To Date Little evidence based treatment Too few studies
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Mousa. Lina Al-Lawama. Enas Ajarma. 0 P a g e
 3 Mousa Lina Al-Lawama Enas Ajarma 0 P a g e رب اشرح لي صدري ويسر لي أمري واحلل عقدة من لساني يفقهوا قولي -Last time we were talking about vulvar pathology (non neoplastic epithelial disorder :lichen chronicus
3 Mousa Lina Al-Lawama Enas Ajarma 0 P a g e رب اشرح لي صدري ويسر لي أمري واحلل عقدة من لساني يفقهوا قولي -Last time we were talking about vulvar pathology (non neoplastic epithelial disorder :lichen chronicus
الطلاوة = Leukoplakia LEUKOPLAKIA
 LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
BAP-oma & BEYOND MICHAEL A NOWAK, MD
 BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
Disclosures Dr. Lynette Margesson
 Management of Vulvar Pruritus 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and
Management of Vulvar Pruritus 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines
 Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Case 1. Case Studies in Vulvovaginal Disease. Disclosures. What is your diagnosis? Case 1. Lichen sclerosus 10/19/2018
 Case 1 Case Studies in Vulvovaginal Disease Leah Moynihan, RNC, MSN Women & Infants Hospital of Rhode Island Division of Urogynecology & Reconstructive Pelvic Surgery Disclosures I have no relevant financial
Case 1 Case Studies in Vulvovaginal Disease Leah Moynihan, RNC, MSN Women & Infants Hospital of Rhode Island Division of Urogynecology & Reconstructive Pelvic Surgery Disclosures I have no relevant financial
Actinic keratosis (AK): Dr Sarma s simple guide
: Dr Sarma s simple guide") Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Eczema & Dermatitis Clinical features: Histopathological features: Classification:
 Eczema & Dermatitis Eczema is an inflammatory reactive pattern of skin to many and different stimuli characterized by itching, redness, scaling and clustered papulovesicles. Eczema and dermatitis are synonymous
Eczema & Dermatitis Eczema is an inflammatory reactive pattern of skin to many and different stimuli characterized by itching, redness, scaling and clustered papulovesicles. Eczema and dermatitis are synonymous
Patient Satisfaction of Surgical Treatment of Clitoral Phimosis and Labial Adhesions Caused by Lichen Sclerosus
 ORIGINAL RESEARCH WOMEN S SEXUAL HEALTH Patient Satisfaction of Surgical Treatment of Clitoral Phimosis and Labial Adhesions Caused by Lichen Sclerosus Anne N. Flynn, MD,* Michelle King, MSc, Mollie Rieff,
ORIGINAL RESEARCH WOMEN S SEXUAL HEALTH Patient Satisfaction of Surgical Treatment of Clitoral Phimosis and Labial Adhesions Caused by Lichen Sclerosus Anne N. Flynn, MD,* Michelle King, MSc, Mollie Rieff,
Clearance in vulvar lichen sclerosus: a realistic treatment endpoint or a chimera?
 DOI: 10.1111/jdv.14516 JEADV SHORT REPORT Clearance in vulvar lichen sclerosus: a realistic treatment endpoint or a chimera? A. Borghi,* A. Virgili, S. Minghetti, G. Toni, M. Corazza Dipartimento di Scienze
DOI: 10.1111/jdv.14516 JEADV SHORT REPORT Clearance in vulvar lichen sclerosus: a realistic treatment endpoint or a chimera? A. Borghi,* A. Virgili, S. Minghetti, G. Toni, M. Corazza Dipartimento di Scienze
Preface to the Second Edition
 Preface to the Second Edition This second edition of Diagnosis of Endometrial Biopsies and Curettings: A Practical Approach follows a number of favorable comments we received about the first edition. As
Preface to the Second Edition This second edition of Diagnosis of Endometrial Biopsies and Curettings: A Practical Approach follows a number of favorable comments we received about the first edition. As
Your Diagnosis Is? Test Your Knowledge of Various Vulvovaginal Conditions
 Your Diagnosis Is? Test Your Knowledge of Various Vulvovaginal Conditions Hope K. Haefner, MD Professor University of Michigan Health System Ann Arbor, Michigan February, 2017 Industry Support and Financial
Your Diagnosis Is? Test Your Knowledge of Various Vulvovaginal Conditions Hope K. Haefner, MD Professor University of Michigan Health System Ann Arbor, Michigan February, 2017 Industry Support and Financial
Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions. Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX
 1 Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX Susan Müller, DMD, MS Professor Department of Pathology
1 Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX Susan Müller, DMD, MS Professor Department of Pathology
Chapter 6 Squamous Cell Carcinoma: Variants and Challenges
 Chapter 6 Squamous Cell Carcinoma: Variants and Challenges Michael B. Morgan EPIDEMIOLOGY: Second most common skin cancer, rare in the dark-skinned races. ETIOLOGY: Ultraviolet light, HPV infection. PATHOGENESIS:
Chapter 6 Squamous Cell Carcinoma: Variants and Challenges Michael B. Morgan EPIDEMIOLOGY: Second most common skin cancer, rare in the dark-skinned races. ETIOLOGY: Ultraviolet light, HPV infection. PATHOGENESIS:
Prescribing Information
 Prescribing Information Pr DERMOVATE Cream (clobetasol propionate cream, USP) Pr DERMOVATE Ointment (clobetasol propionate ointment, USP) Topical corticosteroid TaroPharma Preparation Date: A Division
Prescribing Information Pr DERMOVATE Cream (clobetasol propionate cream, USP) Pr DERMOVATE Ointment (clobetasol propionate ointment, USP) Topical corticosteroid TaroPharma Preparation Date: A Division
FORUM 044 VULVAR DISEASE: WHAT DO YOU KNOW? AN OVERVIEW
 FORUM 044 VULVAR DISEASE: WHAT DO YOU KNOW? AN OVERVIEW Vulvar Neoplasms: Benign and Malignant Jill Allbritton, MD March 2, 2019 NO DISCLOSURES WITH INDUSTRY Jill Allbritton, MD Forum 044 Vulvar Disease:
FORUM 044 VULVAR DISEASE: WHAT DO YOU KNOW? AN OVERVIEW Vulvar Neoplasms: Benign and Malignant Jill Allbritton, MD March 2, 2019 NO DISCLOSURES WITH INDUSTRY Jill Allbritton, MD Forum 044 Vulvar Disease:
Genital Lesions in Dermatopathology
 Genital Lesions in Dermatopathology Janis M. Taube, MD Director of Dermatopathology Associate Professor of Dermatology and Pathology Johns Hopkins University SOM Overview Vulvovaginal pathology Inflammatory
Genital Lesions in Dermatopathology Janis M. Taube, MD Director of Dermatopathology Associate Professor of Dermatology and Pathology Johns Hopkins University SOM Overview Vulvovaginal pathology Inflammatory
WELCOME. Training village
 WELCOME Training village PERFORM EASY AND PAINLESS VAGINAL DRYNESS TREATMENT WITH ELEA Dr Bertrand Durantet Aesthetic Doctor LYON France PART 1 FEATURES ON ELEA THE MAGNETIC SUPPORT THE FOOT PEDAL THE
WELCOME Training village PERFORM EASY AND PAINLESS VAGINAL DRYNESS TREATMENT WITH ELEA Dr Bertrand Durantet Aesthetic Doctor LYON France PART 1 FEATURES ON ELEA THE MAGNETIC SUPPORT THE FOOT PEDAL THE
Anal intraepithelial neoplasia. Information for patients Gynaecology
 Anal intraepithelial neoplasia Information for patients Gynaecology What is anal intraepithelial neoplasia? Anal intraepithelial neoplasia (AIN) is not cancer. AIN describes the presence of abnormal cells
Anal intraepithelial neoplasia Information for patients Gynaecology What is anal intraepithelial neoplasia? Anal intraepithelial neoplasia (AIN) is not cancer. AIN describes the presence of abnormal cells
R. F. Falkenstern-Ge, 1 S. Bode-Erdmann, 2 G. Ott, 2 M. Wohlleber, 1 and M. Kohlhäufl Introduction. 2. Histology
 Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Neoplasia part I. Dr. Mohsen Dashti. Clinical Medicine & Pathology nd Lecture
 Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Genital Lesions in Dermatopathology
 Genital Lesions in Dermatopathology Janis M. Taube, MD Director of Dermatopathology Associate Professor of Dermatology and Pathology Johns Hopkins University SOM Overview Vulvovaginal lesions Non-Neoplastic
Genital Lesions in Dermatopathology Janis M. Taube, MD Director of Dermatopathology Associate Professor of Dermatology and Pathology Johns Hopkins University SOM Overview Vulvovaginal lesions Non-Neoplastic
Policy #: 127 Latest Review Date: June 2011
 Name of Policy: Mohs Micrographic Surgery Policy #: 127 Latest Review Date: June 2011 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates. Background/Definitions:
Name of Policy: Mohs Micrographic Surgery Policy #: 127 Latest Review Date: June 2011 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates. Background/Definitions:
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: mohs_micrographic_surgery 07/2004 11/2017 11/2018 11/2017 Description of Procedure or Service Mohs Micrographic
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: mohs_micrographic_surgery 07/2004 11/2017 11/2018 11/2017 Description of Procedure or Service Mohs Micrographic
Topics in Women s Health. Ann Laros, MD University of Iowa
 Topics in Women s Health Ann Laros, MD University of Iowa Topics in Women s Health 1. Cervical cancer screening guidelines 2. ACHA Pap and STI data 3. Vulvar pearls 4. Genital HSV 2012 Cervical Cancer
Topics in Women s Health Ann Laros, MD University of Iowa Topics in Women s Health 1. Cervical cancer screening guidelines 2. ACHA Pap and STI data 3. Vulvar pearls 4. Genital HSV 2012 Cervical Cancer
Cervical Dysplasia and HPV
 Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Gynaecological Malignancies
 Gynaecological Malignancies Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Overview Genital tract tumors
Gynaecological Malignancies Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Overview Genital tract tumors
Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary
 Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary Glossary of Terms Colposcopy is the examination of the cervix, vagina and, in
Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary Glossary of Terms Colposcopy is the examination of the cervix, vagina and, in
Acantholytic Anaplastic Extramammary Paget s Disease: A Case Report and Review of the Literature
 Ann Dermatol Vol. 23, Suppl. 2, 2011 http://dx.doi.org/10.5021/ad.2011.23.s2.s226 CASE REPORT Acantholytic Anaplastic Extramammary Paget s Disease: A Case Report and Review of the Literature Yu-Jin Oh,
Ann Dermatol Vol. 23, Suppl. 2, 2011 http://dx.doi.org/10.5021/ad.2011.23.s2.s226 CASE REPORT Acantholytic Anaplastic Extramammary Paget s Disease: A Case Report and Review of the Literature Yu-Jin Oh,
ISPUB.COM. A Case of Actinic Lichen Planus. K Choi, H Kim, H Kim, Y Park INTRODUCTION CASE REPORT
 ISPUB.COM The Internet Journal of Dermatology Volume 8 Number K Choi, H Kim, H Kim, Y Park Citation K Choi, H Kim, H Kim, Y Park.. The Internet Journal of Dermatology. 2009 Volume 8 Number. Abstract The
ISPUB.COM The Internet Journal of Dermatology Volume 8 Number K Choi, H Kim, H Kim, Y Park Citation K Choi, H Kim, H Kim, Y Park.. The Internet Journal of Dermatology. 2009 Volume 8 Number. Abstract The
A QUANTITATIVE EVALUATION OF EPITHELIUM AND INFLAMMATORY INFILTRATE OF LICHEN PLANUS AND LICHENOID REACTIONS
 A QUANTITATIVE EVALUATION OF EPITHELIUM AND INFLAMMATORY INFILTRATE OF LICHEN PLANUS AND LICHENOID REACTIONS 1 2 Usha Balan Nitin Gonsalves Maji Jose 1 Departments of Oral & Maxillofacial Pathology, KMCT
A QUANTITATIVE EVALUATION OF EPITHELIUM AND INFLAMMATORY INFILTRATE OF LICHEN PLANUS AND LICHENOID REACTIONS 1 2 Usha Balan Nitin Gonsalves Maji Jose 1 Departments of Oral & Maxillofacial Pathology, KMCT