DR WAFULA Z NALWA, MBCHB
|
|
|
- Lucy Greene
- 5 years ago
- Views:
Transcription
1 GLYCEMIC CONTROL, CARDIOVASCULAR RISK FACTOR PROFILE AND THE THERAPEUTIC INTEREVENTIONS IN TYPE 2 DIABETES MELLITUS PATIENTS AT THE NEW NYANZA PROVINCIAL GENERAL HOSPITAL KISUMU DR WAFULA Z NALWA, MBCHB
2 Supervisors 1. DR MARK JOSHI 2. DR KIRTIDA ACHARYA 3. DR ANGELA AMAYO 4. DR G P O OGUTU
3 Introduction Epidemiology Classification Diagnosis Treatment Complications CAD risk factors Local data Results Discussion
4 Introduction The number of people with type 2 diabetes around the world is estimated to rise from 151 million in 2000 to 350 million by This is expected to affect healthcare and social support systems 2-3. Intensive therapy and cardiovascular risk reduction are beneficial in diabetes mellitus 4-6. A comprehensive therapeutic strategy to mitigate against their effects is required.
5 Introduction Type 2 Diabetes mellitus is due to defects in insulin secretion, insulin action, or both. Cardiovascular risk factors in these patients occur in clusters of obesity, dyslipidemia, hypertension and or microalbuminuria. It is associated with long-term damage, dysfunction, and failure of various organs through varied mechanisms 6-7
6 THE CLASSIFICATION OF DIABETES MELLITUS The etiopathogenic classification of diabetes includes 8 a) Type 1 diabetes results from β-cell destruction b) Type 2 diabetes results from a progressive insulin secretory defect on the background of insulin resistance. c) Other specific types of diabetes: d) Gestational diabetes mellitus (GDM) diagnosed during pregnancy.
7 DIAGNOSIS OF DIABETES MELLITUS Diabetes Care 2003; 26:3160. A1C > 6.5% OR FPG of >7.0mmol/l. Fasting- no caloric intake for at least 8 h. OR Symptoms of hyperglycemia and random blood glucose of 11.1Mmol/l. OR 2-hr plasma glucose of 11.1mmol/l during an OGTT.
8 THE COMPLICATIONS OF DIABETES MELLITUS These are divided into acute and chronic complications. The chronic complications are in turn divided into: a) Vascular complications: a) The microvascular complications are retinopathy, neuropathy and nephropathy. b) The macrovascular complications include coronary heart disease, cerebrovascular disease and peripheral vascular disease. b) Nonvascular complications a) GI tract, genitourinary tract, cataracts, glaucoma and skin.
9 PATHOGENESIS OF MICROVASCULAR COMPLICATIONS: a) Formation of advanced glycosylation end products 10 b) Increased glucose metabolism, via the sorbitol pathway 11 c) Increased formation of diacylglycerol leading to activation of protein kinase C (PKC): d) Increased the glucose flux through the hexosamine pathway. e) Growth factors : VEGF, TGF-β, PDGF, EGF, IGF-I, GH, BFGF, and even insulin.
10 CAD risk factors Diabetes patients have a greater burden of atherogenic risk factors than non diabetics. They often occur in clusters and may be divided into: a) Non-modifiable- Age, sex, family history. b) Modifiable- hypertension, hyper-glycemia, hyperinsulinemia, obesity, dyslipidemia, cigarette smoking, microalbuminuria, obesity, lack of exercise, alcohol intake, haematological, dietary.
11 THERAPEUTIC STRATEGIES IN TYPE 2 DIABETE MELLITUS Therapeutic strategies must be multi-pronged. a) Diabetes education b) Evaluation for microvascular, macrovascular and neurologic complications. c) Normalization of glycemia d) Minimization or elimination of cardiovascular risk factors. Eg blood pressure, dyslipidemia, obesity, cigarette smoking, excess alcohol use etc a) Avoidance of drugs that can aggravate abnormalities of insulin or lipid metabolism.
12 Drugs Summary of glucose lowering interventions Greatest effect Metformin Sulfonylurea Decrease in A1C Insulin Moderate effectiveness Thiazolidinediones GLP 1 Agonist Alpha glucosidase inhibitors Glinides Pramlintide Dipeptidyl peptyidase 4P4 inhibitor
13 Therapeutic strategies Tier 1 Good Evidence/experience Lifestyle At diagnosis Metformin Lifestyle + Metformin Inadequate response Add Basal Insulin/Sulfonylurea Lifestyle + Metformin Inadequate control Add Intensive Insulin Therapy
14 Therapeutic strategies Tier 2 Limited experience and evidence At diagnosis Lifestyle + Metformin Lifestyle, metformin, Pioglitazone Lifestyle, metformin, Glucagon-like Peptide-1 Agonist Inadequate control Add Sulfonylurea Add insulin Inadequate control Lifestyle + Metformin + Intensive Insulin
15 TREATMENT GOALS FOR ADULT PATIENTS DIABETES MELLITUS Parameter Level HB A1C < 7.0% * Pre-prandial capillary plasma glucose Peak postprandial capillary plasma glucose Blood pressure LDL cholesterol HDL cholesterol Triglycerides ( mmol/l) (<10.0 mmol/l) <130/80mmHg <2.6mmol/l >1.1mmo/l <1.7mmol/l Key concepts in setting glycemic goals: A1C is the primary target for glycemic control. Postprandial glucose may be targeted if A1C goals are not met despite reaching pre-prandial glucose goals
16 Cardiovascular risk profile and the interventions in 2001 and 2007 studies: Variable Vaghela, 2001 Mwendwa, 2001 Nguchu, 2007 Wafula, 2009 Obesity by WHR 49.1% % Obesity by WC 65.7% % Obesity by BMI 66.9% 66.1% Hypertension 64.8% 50% 60% Elevated LDL 88% 35% 73.7% Smoking 31.5% 73% 8.4% Family h/o DM 77.8% 48% Family h/o HTN 66.7% 24% Drugs OHA only 48.1% 74% 43.2% Insulin only 5.6% 13% 42.1% OHA, insulin, 46.3% 11% 1.1% Diet only 2% 5.3% Statin < 1% - 8.4% Aspirin 9.3% % ARB/ACE I - - -
17 Justification of the study Chronic illnesses may soon surpass infectious diseases as the leading cause of morbidity and mortality in the developing world. The outlying hospitals will bear most of this burden. Provincial (level 5) hospitals. The New Nyanza Provincial General Hospital is on such hospital. There is no data from the western region of this country. This study was therefore designed to characterize the patients and evaluate the care accorded to these patients in this setting. Passionate desire to stimulate interest in research beyond the confines and comfort of the Kenyatta National Hospital
18 RESEARCH QUESTION How well is diabetes being controlled at a provincial (level 5) hospital, what are the prevalent coronary artery disease risk factors and what pharmaco-therapeutic interventions are being utilised?
19 BROAD OBJECTIVE To determine the patient characteristics, level of glycemic control and pharmaco-therapeutic strategies utilised for both glycemic control and cardiovascular risk reduction in type 2 diabetes mellitus patients at the NNPGH.
20 SPECIFIC OBJECTIVES 1. To describe demographics of type 2 diabetes mellitus: Age, gender, educational attainment, employment status, and residence. 2. To determine the level of glycemic control. (Using; HBA1C, FPG, 1hr PPG ) and the predictors of glycemic control. 3. To determine the pharmacologic regimens used in glycemic control. 4. To describe the cardiovascular risk factors: Family history of diabetes mellitus or hypertension, obesity, hypertension, alcohol use &smoking. Lipid profile, Estimated GFR, Urine albumin to creatinine ratio. 5. To determine the utilization of pharmacotherapeutic interventions for risk reduction: Statins, anti-platelets & anti-hypertensive
21 METHODS AND MATERIALS. Study design Study site Study population Inclusion criteria Exclusion criteria Sample size estimation=118
22 RESULTS MMED thesis,2009
23 800 patients were screened 100- newly diagnosed 90- type eligible for the study did not return 57- did not consent 153 enrolled 29-did not complete study 5- had incomplete data 119 analysed History, Physical findings: weight, height, BP, WC, HC. Lab results: HBA1C, FPG,PPG, serum lipid profile, serum creatinine, UACR
24 Socio-demographics of the study population Characteristic Frequency (%) Sex Marital status Male Female Married Widowed Divorced Residence Employment status Urban Rural Employed Never employed Retired Unemployed Level of education None Primary Secondary Tertiary
 Female (%) n-70 (58.8) Male (%) n-49(41.")
25 Distribution by Sex Total (%). n-119(100) Female (%) n-70 (58.8) Male (%) n-49(41.2) Male :female ratio 1:1.7
26 Distribution by Age Variable Study Range Male Female P Value mean Age 58.4 (8.9) Age Sex P value Female Male (2.9%) 10 (14.3%) 24 (34.3%) 30 (42.9%) 4 (5.7%) 0 (0.0%) 1 (2.0%) 4 (8.2%) 22 (44.9%) 17 (34.7%) 4 (8.2%) 1 (2.0%) 0.549

27 Distribution by Residence
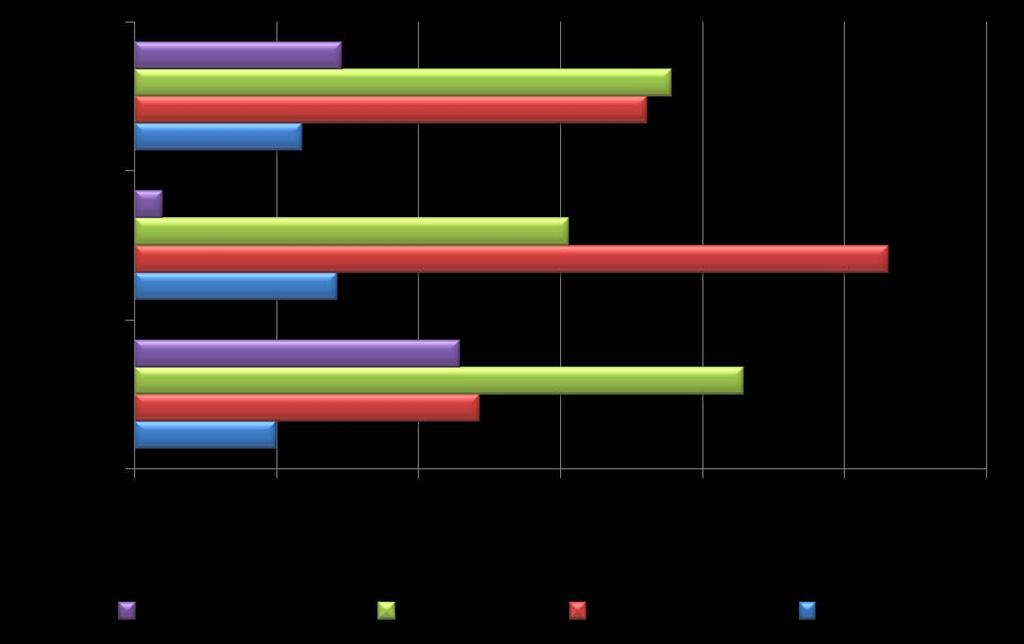
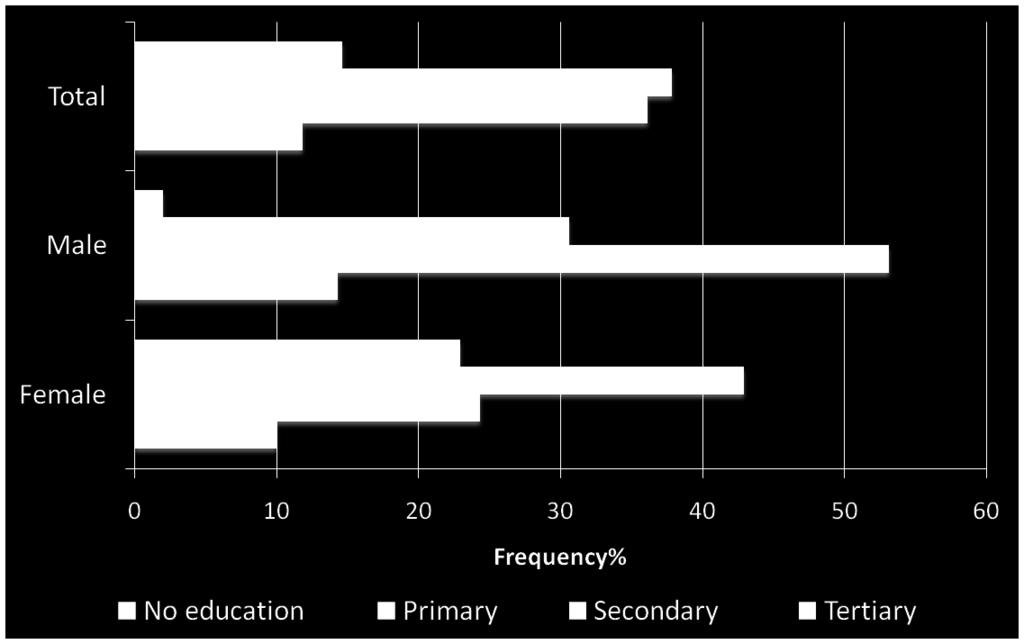
28 Educational Attainment
29 Glycemic control
30 Glycemic control Variable Mean Range HBA1C F PG 8.8 (4.0) HR PPG 15.5 (4.9) Variable Control Category Frequency % HBA1C Good (<7%) Poor (>=7%) FPG (8.8(4.0)mmol/L < > HR PPG 15.5(0.95)mmol/L <10mmol/l >=10mmol/l




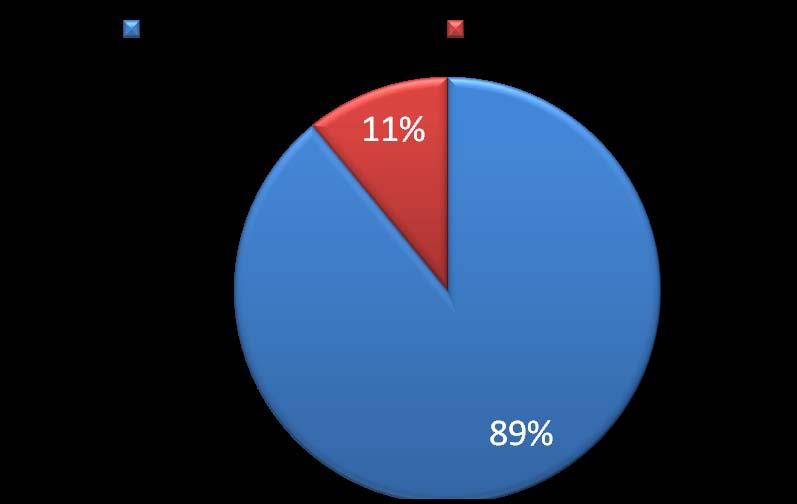
31 Categorization of glycemic control using HBA1C % 13% HBA1C <7 HBA1C >7 87%

32 Prevalent Drugs used for glycemic control
33 CV risk factors
34 CV risk factors Family history Variable Characteristic Number Frequency% Relative with diabetes (n=119) Relative specified (diabetes) (n=56) Relative with hypertension (n=119) Relative specified (hypertension) (n=43) Yes st degree Yes st degree Smoking Smoking status EVER smoked (male-14) Alcohol use Drink alcohol Yes (male-5) Quantity of alcohol (n=8) 2units/day 3units/day
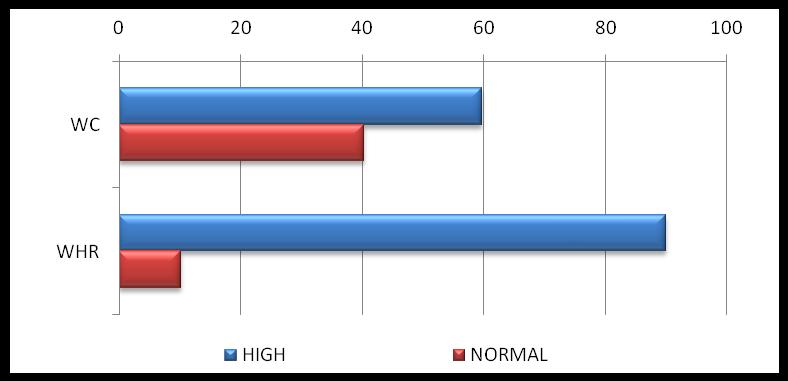
35 CVD risk factors Variable BMI Categorization N=119 Underweight Normal weight Overweight Class I Obesity Class II Obesity Class III Obesity Frequency % (68.9%) WC High M>102; F=88 Waist hip ratio High
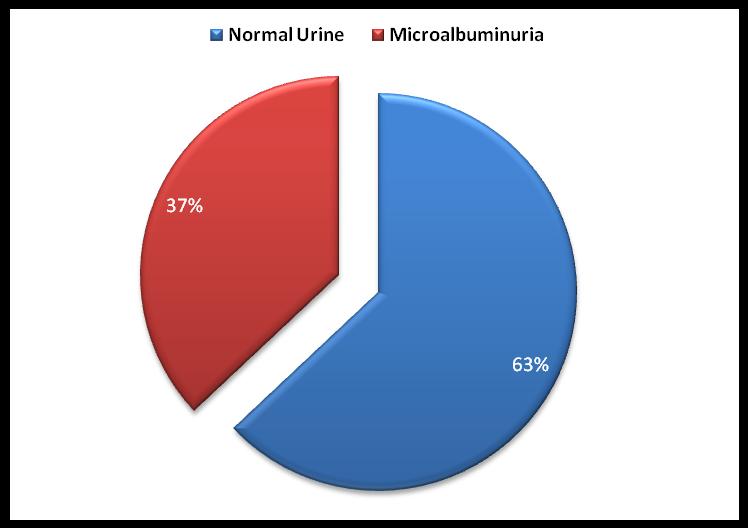
36 CVD risk factors-biochemical Variable Category No. of patients Frequency % Total cholesterol Desirable LDL <2.6mmol/l HDL >= TG <1.7mmol/l Microalbuminuria Microalbuminuria Estimated GFR Stage 0 Stage 1 Stage 2 Stage 3 Stage 4 Stage
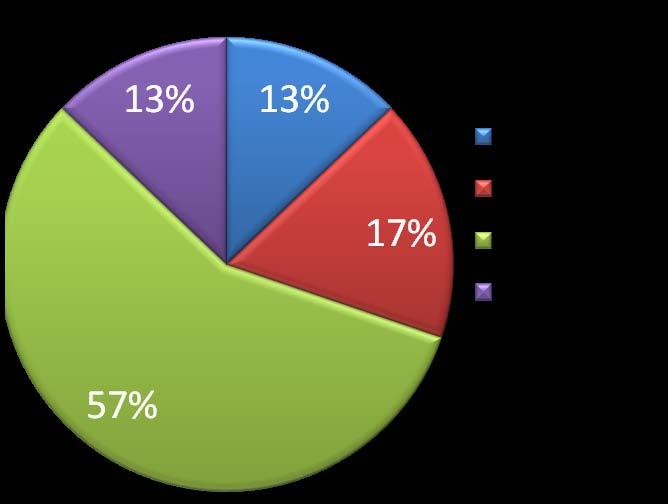
37 Categorization of obesity
38 Categorization of BP Variable Categorization Total (n=119) On treatment (n=95) BP <130/80 >130/ % 44.5% % 52.6%
39 Categorization by FPG and 1HR PPG PPG FPG

40 Lipids at target 120 At Target Not at target LDL HDL TG
41 Clustering of lipid abnormalities Variable Frequency Number Frequency Lipids % 41.2% 26.9% 6.7% One lipid High LDL Low HDL High TG % 18.4% 10.2% Two lipids LDL+TG LDL+HDL HDL+TG % 46.9% 9.4%
42 Microalbuminuria

43 Categorization by estimated GFR
44 CVD Risk factor interventions
45 CV risk factor clustering RF combination Frequency Percent % 14.3% 23.5% 31.1% 21.8% 4.2% 2.5%
46 Prevalent agents for CVD risk reduction 79.8 Yes No Antihypertensives Antiplatelet Statins Characteristic Number Frequency (%) BP drugs Yes No a. RAS I b. Others


47 Prevalent anti-hypertensives, BP and HBA1C at target in patients with microalbuminuria Other ACE/ARB+other ACE/ARB 10 0 Microalbuminuria Normal-urine P=0.011
48 At target: Therapeutic interventions Variable Target level On treatment Number Proportion HBA1C (n=119) <7 % % BP (n=95) <130/80mmHg % LDL (n=9) <2.6mmol/l %
49 There was no correlation between sociodemographic characteristics and glycemic control(chi-square)
50 Comparisons between the well and the poorly controlled diabetes (student-test) Mean s of variables HBA1C category P value <7% (n=104) >=7% (n=15) Age Waist circumference (cm) * Waist-to-hip ratio Systolic BP(mmHg) * Diastolic BP (mmhg)) * BMI (Kg/m 2) * Fasting glucose (mmol/l) * Postprandial glucose (mmol/l) * Total cholesterol HDL TG LDL (mmol/l) Albumin/creatinine ratio * GFR Age
51 There was no definite predictor of glycemic control on Logistic regression analysis
52 Discussion The mean age for the study was 58.4yrs, 93(78.15%)were between 50 to 69 yrs of age- Elderly population according to our life expectancy in Kenya This is 10 or so years lower than the west. There were more females than males (58.8% vs 41.2%) This is in tandem with the different health seeking behaviour between the sexes. It is replicated at KNH The study population was rural in keeping with the catchment area of the Hospital and city KNH mainly urban-78% Mwendwa. Most patients 88(73.9%) had basic education and were 53 (44.5%) retired Primary and secondary education-in keeping with literacy levels in most rural settings in Kenya.
53 Risk factors-family history There was a modest risk in terms of family history of: Diabetes- 47.1% Hypertension -36.1% Vaghela at KNH found 77.8% and 66.7% for diabetes and hypertension respectively. What factors contribute to increased risk in rural areas other than family history? Prevalence of affected First degree relative: 76.8%-diabetes 81.5 %-hypertension. This is in keeping with the polygenic nature of inheritance of this two conditions. An affected patient likely has an affected 1 st degree relative
54 Risk factors-duration of disease The median duration of disease was 6.0 years; This may be reflected in better glycemic control due to residual pancreatic reserve. Longer duration is associated with poor glycemic control, poor response to OHAs and higher change over to insulin This finding may be an under estimate of the duration of disease. to the long latent period of asymptomatic diabetes, This was shorter than that seen at KNH Vaghela 2001: found a mean duration of disease of 7.6 ( )yrs Nturibi 2007: Mean duration of diabetes /- 4.23yrs
55 Risk factors-bmi, WC, WHR Using BMI, our pick-up rate for obesity was (20.2%). This was lower than that at KNH-Mwendwa-66% and Vaghela 66.7%. Obesity was picked better using WC-59.7% and WHR-89.9%. Thus WHR was a much more sensitive measure than BMI and WC in this population. The caveat to this observation is the limited utility of WC,WHR in patients with BMIs above 35.
56 Risk factors-hypertension The prevalence of hypertension was 78.9% with no significant gender difference. 47.4% (45) of the patients were well controlled on antihypertensive treatment. This is in keeping with the 50% observation in the management of hypertension. The mean BP was lower at 129/77mmHg compared to 143/87.1mmHg found at KNH by Vaghela This should translate to lower CAD, CV, CCF and even PAD through a lower atherosclerosis rate and microvascular disease rate? Role of hospital setting
57 Risk factors-dyslipidemia LDL was elevated in 72(60.5%); HDL low in 35(29.4%) and TG elevated in 30 (25.2%) of patients. 37(31%) of patients had 2 or more lipid abnormalities. There were various combinations of raised LDL, low HDL or raised TG. This means at least a third of the patients are at high risk for CV and require statin therapy, yet only 9% were on statins. Often TG are elevated with decreased HDL -? Dietary factors, low alcohol use, genetic factors; in our study, a minority had these combination
58 Risk factors-alcohol, cigarette smoking There was a low prevalence of cigarette smoking and alcohol utilization. The quantities involved were not sufficient to constitute significant risk.? Effect of socio-economics-little money as retirees to spend. This low rate augers well with reduced CVD risk. Smoking hampers glycemic control, promotes dyslipidemia and accelerates atherosclerosis in addition to an increased event and mortality rate
59 Risk factors-microalbuminuria and CKD 44(37%) of patients had microalbuminuria Only 18.5% of patients had a normal GFR. Most of the rest were in stage 2 and 3 of CKD. It may suggest disease duration of more than 10 years. 1. It is not surprising given the low uptake of Reno-protective medications 2. Without intervention, the risk of progression to ESRD and subsequent mortality is high. 3. There is need to increase the uptake of interventions to prevent or slow down the progression to ERSD.
60 Cardiovascular risk interventions in 2001, 2007, 2009 studies Variable Vaghela, 2001 Mwendwa, 2001 Nguchu, 2007 Wafula, 2009 Drugs OHA only 48.1% 74% 43.2% 83 (69.7%) Insulin only 5.6% 13% 42.1% 26 (21.8%) OHA, insulin, 46.3% 11% 1.1% 8 (6.7%) Diet only 2% 5.3% - Statin < 1% - 8.4% 9 (7.6%) Aspirin 9.3% % 11 (9.2%) ARB/ACE I (57.1%) These patients were generally >40yrs with more than 2 CV risk factors. They required a comprehensive approach to manage the CV risk factors beyond Blood pressure and glycemic control
61 Glycemic control, therapies and the predictors There was good glycemic control with 104 (87.4%) of patients having HBA1c < 7.0% Vaghela and Nyamu had 30% and 18% good control respectively. Most patients were on OHAs +/-Insulin-91 (76.4%);Insulin 34 (28.5%). What are the determinants of glycemic control in this population? Diet, lifestyle and genetics What is the magnitude of the effect of closer clinic visits? 2-3 monthly at Nyanza vs KNH 6/12 to 1year There was concordance between FPG and HBA 1C. This provides internal validity to the results It suggests that FPG can and should be used in resource limited settings as we await cheaper HBA1C kits to monitor control.
62 PHARMACOTHERAPEUTIC INTERVENTIONS FOR CAD RISK REDUCTION 1. ACE-I/ARBs were used in 68 (57.1%) of patients on antihypertensives. Microalbuminuria was found in 44 (37.0%) of patients. There was no difference between those with or without; 52.3% vs 61.3% (p=0.334). Microalbuminuria was not the driver of RAAS Inhibitor prescription 2. LDL was elevated in 72 (60.5%) of patients yet only 9 (7.6%) were on statins. Serum lipid levels were not the driver of prescription 3. Platelet agents were used in only 11 (9.2%) of the patients. This should have been higher with the risk factor clustering seen earlier
63 PHARMACOTHERAPEUTIC INTERVENTIONS FOR CAD RISK REDUCTION Overall the following proportions of patients were on various forms of treatment: a) 99% - glycemic control agents b) 79.8%-on anti hypertensive treatment c) 9.2% -on antiplatelet agents d) 7.6% -on statins
64 Predictors/associations of glycemic control There was NO independent predictor of glycemic control. There was good correlation between A1C and FPG There may be a role for reverse causation in that the abnormalities seen in the patients with poor control were in themselves a result of the poor control rather than the causes of poor control
65 Study Limitations Selection bias may have influenced the results by selecting, willing, highly motivated and financially able patients. Single HBA1c values may not accurately reflect overall glycemic control over many years. Single spot urine may have been affected by the day to day variability. The non-probability sampling technique did not control for confounders. Hospital based study may not reflect disease in general population No immunological studies to rule out LADA. Hemoglobinopathies not tested for, for exclusion purposes. The definition of type 2 diabetes was by phenotype.
66 Conclusion 1 1. This study was the first of its kind in the Western Kenya. 2. Glycemic control can be achieved in technologically challenged environments. 3. Hypertension was a common problem 4. There was a significant familial component in these patients 5. Obesity was common in this rural population
67 Conclusion 2 6. Dyslipidemia, particularly raised LDL cholesterol was common. 7. Renal dysfunction was very common. 8. In general, the uptake of evidence based Interventions for cardiovascular risk factor reduction was low. 9. There is need for better designed studies to verify the various determinants of glycemic control
68 Recommendations Encourage use of FPG in resource limited settings. WHR can be used to effectively monitor central obesity. Provide facilities to measure biochemical RF for CAD to facilitate the necessary interventions. Study on prevalence of complications in this population in view of the results found in this study. Study the predictors of glycemic control Encourage evidence based practice with adequate senior supervision and instruction
69 Asante!
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES
 Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES Objectives u At conclusion of the lecture the participant will be able to: 1. Differentiate between the classifications of diabetes
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES Objectives u At conclusion of the lecture the participant will be able to: 1. Differentiate between the classifications of diabetes
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Section 1: 1: Trends. Section 2: 2: Comparisons to to Overall Portland Area Area Results for for
 Section 1: 1: Trends 1 Patients in the Diabetes Register 2 Gender of Patients with Diabetes 2 Age of Patients with Diabetes 3 Diabetes Type 3 Duration of Diabetes 4 Weight Control 5 Hemoglobin A1c 6 Blood
Section 1: 1: Trends 1 Patients in the Diabetes Register 2 Gender of Patients with Diabetes 2 Age of Patients with Diabetes 3 Diabetes Type 3 Duration of Diabetes 4 Weight Control 5 Hemoglobin A1c 6 Blood
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes
 Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes Authored by Clifford Bailey and James LaSalle on behalf of the Global Partnership for Effective Diabetes Management. The
Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes Authored by Clifford Bailey and James LaSalle on behalf of the Global Partnership for Effective Diabetes Management. The
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES
 RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Clinical Practice Guideline Key Points
 Clinical Practice Guideline Key Points Clinical Practice Guideline 2008 Key Points Diabetes Mellitus Provided by: Highmark Endocrinology Clinical Quality Improvement Committee In accordance with Highmark
Clinical Practice Guideline Key Points Clinical Practice Guideline 2008 Key Points Diabetes Mellitus Provided by: Highmark Endocrinology Clinical Quality Improvement Committee In accordance with Highmark
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
SCIENTIFIC STUDY REPORT
 PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Objectives. Objectives. Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015
 Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015 Presentation downloaded from http://ce.unthsc.edu Objectives Understand that the obesity epidemic is also affecting children and adolescents
Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015 Presentation downloaded from http://ce.unthsc.edu Objectives Understand that the obesity epidemic is also affecting children and adolescents
Table S1. Characteristics associated with frequency of nut consumption (full entire sample; Nn=4,416).
.") Table S1. Characteristics associated with frequency of nut (full entire sample; Nn=4,416). Daily nut Nn= 212 Weekly nut Nn= 487 Monthly nut Nn= 1,276 Infrequent or never nut Nn= 2,441 Sex; n (%) men 52
Table S1. Characteristics associated with frequency of nut (full entire sample; Nn=4,416). Daily nut Nn= 212 Weekly nut Nn= 487 Monthly nut Nn= 1,276 Infrequent or never nut Nn= 2,441 Sex; n (%) men 52
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Sect S io ecn ti 1 o : n Trend 1: Tres nds
 Section 1: 1: Trends 1 Patients in the Diabetes Register 2 Gender of Patients with Diabetes 2 Age of Patients with Diabetes 3 Diabetes Type 3 Duration of Diabetes 4 Weight Control 5 Hemoglobin A1c 6 Blood
Section 1: 1: Trends 1 Patients in the Diabetes Register 2 Gender of Patients with Diabetes 2 Age of Patients with Diabetes 3 Diabetes Type 3 Duration of Diabetes 4 Weight Control 5 Hemoglobin A1c 6 Blood
CARDIOVASCULAR RISK FACTORS IN PATIENTS WITH RHEUMATOID ARTHRITIS AT KENYATTA NATIONAL HOSPITAL
 CARDIOVASCULAR RISK FACTORS IN PATIENTS WITH RHEUMATOID ARTHRITIS AT KENYATTA NATIONAL HOSPITAL Kirui K Fredrick MBCHB,MMED KEMRI/WRP HIV PROGRAM KERICHO EPIDEMIOLOGY Rheumatoid arthritis (RA) is a disease
CARDIOVASCULAR RISK FACTORS IN PATIENTS WITH RHEUMATOID ARTHRITIS AT KENYATTA NATIONAL HOSPITAL Kirui K Fredrick MBCHB,MMED KEMRI/WRP HIV PROGRAM KERICHO EPIDEMIOLOGY Rheumatoid arthritis (RA) is a disease
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus. Eiman Ali Basheir. Mob: /1/2019
 Diabetes Mellitus Eiman Ali Basheir Mob: 091520385 27/1/2019 Learning Outcomes Discuss the WHO criteria for Diabetes Mellitus diagnosis Describe the steps taken to confirm diagnosis Interpret GTT. Discuss
Diabetes Mellitus Eiman Ali Basheir Mob: 091520385 27/1/2019 Learning Outcomes Discuss the WHO criteria for Diabetes Mellitus diagnosis Describe the steps taken to confirm diagnosis Interpret GTT. Discuss
CHAPTER 3 DIABETES MELLITUS, OBESITY, HYPERTENSION AND DYSLIPIDEMIA IN ADULT CENTRAL KERALA POPULATION
 CHAPTER 3 DIABETES MELLITUS, OBESITY, HYPERTENSION AND DYSLIPIDEMIA IN ADULT CENTRAL KERALA POPULATION 3.1 BACKGROUND Diabetes mellitus (DM) and impaired glucose tolerance (IGT) have reached epidemic proportions
CHAPTER 3 DIABETES MELLITUS, OBESITY, HYPERTENSION AND DYSLIPIDEMIA IN ADULT CENTRAL KERALA POPULATION 3.1 BACKGROUND Diabetes mellitus (DM) and impaired glucose tolerance (IGT) have reached epidemic proportions
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
ASSeSSing the risk of fatal cardiovascular disease
 ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Modified version focused on CCNC Quality Measures and Feedback Processes
 Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Audit Results, Portland Area, Site-Specific Trends
 Site-Specific Trends The following report contains information from your program's annual diabetes audit submission to the Indian Health Service over the past few years. The report was prepared for your
Site-Specific Trends The following report contains information from your program's annual diabetes audit submission to the Indian Health Service over the past few years. The report was prepared for your
Standards of Medical Care In Diabetes
 Standards of Medical Care In Diabetes - 2017 Robert E. Ratner, MD, FACP, FACE Professor of Medicine Georgetown University School of Medicine Disclosed no conflict of interest Standards of Care Professional.diabetes.org/SOC
Standards of Medical Care In Diabetes - 2017 Robert E. Ratner, MD, FACP, FACE Professor of Medicine Georgetown University School of Medicine Disclosed no conflict of interest Standards of Care Professional.diabetes.org/SOC
Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead
 Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead Today s Presentation HbA1c & diagnosing Diabetes What is Impaired Glucose & IGR? Implications
Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead Today s Presentation HbA1c & diagnosing Diabetes What is Impaired Glucose & IGR? Implications
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY
 MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
Chapter 37: Exercise Prescription in Patients with Diabetes
 Chapter 37: Exercise Prescription in Patients with Diabetes American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
Chapter 37: Exercise Prescription in Patients with Diabetes American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
TUE Physician Guidelines Medical Information to Support the Decisions of TUE Committees Diabetes Mellitus DIABETES MELLITUS
 DIABETES MELLITUS 1. Introduction Diabetes is a global epidemic with 415 million people affected worldwide equivalent to the total population of the USA, Canada and Mexico. In recognition of this, the
DIABETES MELLITUS 1. Introduction Diabetes is a global epidemic with 415 million people affected worldwide equivalent to the total population of the USA, Canada and Mexico. In recognition of this, the
STANDARDS OF MEDICAL CARE IN DIABETES 2014
 STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Depok-Indonesia STEPS Survey 2003
 The STEPS survey of chronic disease risk factors in Indonesia/Depok was carried out from February 2003 to March 2003. Indonesia/Depok carried out Step 1, Step 2 and Step 3. Socio demographic and behavioural
The STEPS survey of chronic disease risk factors in Indonesia/Depok was carried out from February 2003 to March 2003. Indonesia/Depok carried out Step 1, Step 2 and Step 3. Socio demographic and behavioural
Cardiovascular Complications in Diabetes
 What is all the fuss about? Cardiovascular Complications in Diabetes Dina Shrestha MD Consultant Endocrinologist Norvic International Hospital and Medical College Hospital for Advanced Medicine and Surgery
What is all the fuss about? Cardiovascular Complications in Diabetes Dina Shrestha MD Consultant Endocrinologist Norvic International Hospital and Medical College Hospital for Advanced Medicine and Surgery
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: Evaluation and Care Management
 Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
DIABETES MEASURES GROUP OVERVIEW
 2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Addressing Addressing Challenges in Type 2 Challenges in Type 2 Diabetes Diabetes Speaker:
 Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Total risk management of Cardiovascular diseases Nobuhiro Yamada
 Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
RCHC Clinical Guidelines Type 2 Diabetes; Adults
 RCHC Clinical Guidelines Type 2 Diabetes; Adults Screening for diabetes in asymptomatic adults 1 Population: Aged > 45 years; Aged < 45 years who are overweight (BMI> 25kg/m 2 ) and have an additional
RCHC Clinical Guidelines Type 2 Diabetes; Adults Screening for diabetes in asymptomatic adults 1 Population: Aged > 45 years; Aged < 45 years who are overweight (BMI> 25kg/m 2 ) and have an additional
Supplementary Online Content
 Supplementary Online Content Larsen JR, Vedtofte L, Jakobsen MSL, et al. Effect of liraglutide treatment on prediabetes and overweight or obesity in clozapine- or olanzapine-treated patients with schizophrenia
Supplementary Online Content Larsen JR, Vedtofte L, Jakobsen MSL, et al. Effect of liraglutide treatment on prediabetes and overweight or obesity in clozapine- or olanzapine-treated patients with schizophrenia
Impact of Physical Activity on Metabolic Change in Type 2 Diabetes Mellitus Patients
 2012 International Conference on Life Science and Engineering IPCBEE vol.45 (2012) (2012) IACSIT Press, Singapore DOI: 10.7763/IPCBEE. 2012. V45. 14 Impact of Physical Activity on Metabolic Change in Type
2012 International Conference on Life Science and Engineering IPCBEE vol.45 (2012) (2012) IACSIT Press, Singapore DOI: 10.7763/IPCBEE. 2012. V45. 14 Impact of Physical Activity on Metabolic Change in Type
Inernal Medicine by Prof. El Sayed Abdel Fatah Eid. Diabetes Mellitus. Prof. El Sayed Abdel Fattah Eid. Lecturer of Internal Medicine Delta University
 Diabetes Mellitus By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University (Diabetes Mellitus) Definition: Diabetes mellitus comprises a heterogeneous group of metabolic diseases
Diabetes Mellitus By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University (Diabetes Mellitus) Definition: Diabetes mellitus comprises a heterogeneous group of metabolic diseases
28-Aug-15. RACGP guidelines 2014/15. ADS guidelines Part 1 T2D Guidelines. Part 2 What comes after metformin?
 Part 1 T2D Guidelines Oral therapies in T2 diabetes Dr Gary Kilov T2D Guidelines - What s New? What comes after metformin? 1 RACGP guidelines 2014/15 ADA-EASD: Anti-Hyperglycaemic therapy 2015 3 4 Inzucchi
Part 1 T2D Guidelines Oral therapies in T2 diabetes Dr Gary Kilov T2D Guidelines - What s New? What comes after metformin? 1 RACGP guidelines 2014/15 ADA-EASD: Anti-Hyperglycaemic therapy 2015 3 4 Inzucchi
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
The State of Play of Diabetes Indicators
 The State of Play of Diabetes Indicators South Australian and National Information Catherine Chittleborough Janet Grant Anne Taylor April 2003 Diabetes Clearing House Population Research and Outcome Studies
The State of Play of Diabetes Indicators South Australian and National Information Catherine Chittleborough Janet Grant Anne Taylor April 2003 Diabetes Clearing House Population Research and Outcome Studies
Diabetes Mellitus (DM) - Dr Hiren Patt
 - Dr Hiren Patt") Diabetes Mellitus (DM) - Dr Hiren Patt What is DM? FPG 2-Hour PG on OGTT Diabetes Mellitus Diabetes Mellitus 126 mg/dl 100 mg/dl Impaired Fasting Glucose 200 mg/dl 140 mg/dl Impaired Glucose Tolerance
Diabetes Mellitus (DM) - Dr Hiren Patt What is DM? FPG 2-Hour PG on OGTT Diabetes Mellitus Diabetes Mellitus 126 mg/dl 100 mg/dl Impaired Fasting Glucose 200 mg/dl 140 mg/dl Impaired Glucose Tolerance
Philippine Practice Guidelines for the Diagnosis & Management of Type 2 Diabetes Mellitus
 Philippine Practice Guidelines for the Diagnosis & Management of Type 2 Diabetes Mellitus Iris Thiele Isip Tan MD, MSc, FPCP, FPSEM Chief, Medical Informatics Unit Associate Professor IV, UP College of
Philippine Practice Guidelines for the Diagnosis & Management of Type 2 Diabetes Mellitus Iris Thiele Isip Tan MD, MSc, FPCP, FPSEM Chief, Medical Informatics Unit Associate Professor IV, UP College of
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
Diabetes: Staying Two Steps Ahead. The prevalence of diabetes is increasing. What causes Type 2 diabetes?
 Focus on CME at the University of University Manitoba of Manitoba : Staying Two Steps Ahead By Shagufta Khan, MD; and Liam J. Murphy, MD The prevalence of diabetes is increasing worldwide and will double
Focus on CME at the University of University Manitoba of Manitoba : Staying Two Steps Ahead By Shagufta Khan, MD; and Liam J. Murphy, MD The prevalence of diabetes is increasing worldwide and will double
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Section 1: 1: Trends. Section 2: 2: Comparisons to to Overall Portland Area Area Results for for
 Section 1: 1: Trends 2 Patients in the Diabetes Register 3 Diabetes Type 3 Gender of Patients with Diabetes 4 Age of Patients with Diabetes 4 Duration of Diabetes 5 Weight Control 6 Hemoglobin A1c 7 Blood
Section 1: 1: Trends 2 Patients in the Diabetes Register 3 Diabetes Type 3 Gender of Patients with Diabetes 4 Age of Patients with Diabetes 4 Duration of Diabetes 5 Weight Control 6 Hemoglobin A1c 7 Blood
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ
 ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Solomon SD, Uno H, Lewis EF, et al. Erythropoietic response
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Solomon SD, Uno H, Lewis EF, et al. Erythropoietic response
Executive Summary: Standards of Medical Care in Diabetes 2010
 E X E C U T I V E S U M M A R Y Executive Summary: Standards of Medical Care in Diabetes 2010 Current criteria for the diagnosis of diabetes A1C 6.5%: The test should be performed in a laboratory using
E X E C U T I V E S U M M A R Y Executive Summary: Standards of Medical Care in Diabetes 2010 Current criteria for the diagnosis of diabetes A1C 6.5%: The test should be performed in a laboratory using
Diabetes is a chronic illness that requires
 P O S I T I O N S T A T E M E N T Standards of Medical Care for Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Diabetes is a chronic illness that requires continuing medical care and patient
P O S I T I O N S T A T E M E N T Standards of Medical Care for Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Diabetes is a chronic illness that requires continuing medical care and patient
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Optimizing Postpartum Maternal Health to Prevent Chronic Diseases
 Optimizing Postpartum Maternal Health to Prevent Chronic Diseases Amy Loden, MD, FACP, NCMP Disclosures Research: None Financial: none applicable to this presentation PRIUM QEssentials Market Research
Optimizing Postpartum Maternal Health to Prevent Chronic Diseases Amy Loden, MD, FACP, NCMP Disclosures Research: None Financial: none applicable to this presentation PRIUM QEssentials Market Research
Management of DM in Older Adults: It s not all about sugar! Who needs treatment for DM? Peggy Odegard, Pharm.D., BCPS, CDE
 Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Chronic Benefit Application Form Cardiovascular Disease and Diabetes
 Chronic Benefit Application Form Cardiovascular Disease and Diabetes 19 West Street, Houghton, South Africa, 2198 Postnet Suite 411, Private Bag X1, Melrose Arch, 2076 Tel: +27 (11) 715 3000 Fax: +27 (11)
Chronic Benefit Application Form Cardiovascular Disease and Diabetes 19 West Street, Houghton, South Africa, 2198 Postnet Suite 411, Private Bag X1, Melrose Arch, 2076 Tel: +27 (11) 715 3000 Fax: +27 (11)
CE on SUNDAY Newark, NJ October 18, 2009
 CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 2:45 PM 3:45 PM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Addressing Challenges in Type 2 Diabetes ACPE #
CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 2:45 PM 3:45 PM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Addressing Challenges in Type 2 Diabetes ACPE #
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
A Study to Show Postprandial Hypertriglyceridemia as a Risk Factor for Macrovascular Complications in Type 2 Diabetis Mellitus
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/21 A Study to Show Postprandial Hypertriglyceridemia as a Risk Factor for Macrovascular Complications in Bingi Srinivas
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/21 A Study to Show Postprandial Hypertriglyceridemia as a Risk Factor for Macrovascular Complications in Bingi Srinivas
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
11/4/2014. Outline. Pharmacists Objectives. Diabetes Update: What s New in Pharmacy Technician Objectives. Overview: Type 2 Diabetes Mellitus
 Diabetes Update: What s New in 2014 Dr. Amy P. Witte, Pharm.D. Associate Professor, Pharmacy Practice UIW Feik School of Pharmacy CTSHP Fall Seminar La Cantera Hill Country Resort October 25, 2014 Pharmacists
Diabetes Update: What s New in 2014 Dr. Amy P. Witte, Pharm.D. Associate Professor, Pharmacy Practice UIW Feik School of Pharmacy CTSHP Fall Seminar La Cantera Hill Country Resort October 25, 2014 Pharmacists
Diabetes mellitus. Treatment
 Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists