Clinical Pathology. Mary Anna Thrall, DVM, MS, DACVP. Sponsored by
|
|
|
- Anastasia Janel Berry
- 5 years ago
- Views:
Transcription

1 Clinical Pathology by Mary Anna Thrall, DVM, MS, DACVP September 10, 2008 Sponsored by 1
2 CYTOLOGY: WHEN TO SEND YOUR SAMPLES TO A PATHOLOGIST, AND WHEN TO DO IT YOURSELF Mary Anna Thrall Colorado State University Fort Collins CO Ross University Basseterre, West Indies Introduction Whether a veterinarian prefers to have most cytology performed "in-house", or to send samples to a diagnostic laboratory, there are a few examples of situations in which the results are needed immediately, and should be performed in a clinic setting. The best example is bacterial peritonitis, which is almost always a surgical emergency. Other examples of cases in which the results should be obtained prior to surgery, but are not necessarily emergencies, include mast cell tumors and soft tissue sarcomas, both of which should be diagnosed prior to surgery so that the clinician will be aware of the type of lesion, and thus will widely excise to prevent recurrence. This discussion will include, examples of "STAT" cytology samples, examples of relatively simple cytologic diagnoses, and examples of relatively difficult cytologic diagnoses. Review of basics: Inflammation is characterized by the presence of numerous inflammatory cells such as neutrophils, macrophages, lymphocytes, and eosinophils. The proportions of different inflammatory cells elucidate the type of inflammation present. Qualifiers such as "mild" or "marked" can classify the severity of the reaction. Inflammation is classified as follows: Neutrophilic (purulent or suppurative) inflammation: Approximately 90% of the inflammatory cells are neutrophils. If bacteria are present, the term "septic suppurative inflammation" is used. Mixed (pyogranulomatous) inflammation: Greater than 10% but less than 50% of the cells are lymphocytes and/or macrophages. This type of inflammation is more typically seen with the inflammatory agent is a foreign body or a fungal microorganism. Mononuclear or granulomatous inflammation. The majority of cells are macrophages, giant cells, and/or epithelioid macrophages. This is most commonly seen with mycobacterial agents. Eosinophilic inflammation. This term is used when a significant proportion of the inflammatory cells are eosinophils. The percent is somewhat subjective; an eosinophilic component to inflammation is present if > than 15% of the cells are eosinophils. Bacteria. Bacteria are more easily recognized in Romanowsky stained preparations, rather than those stained with Gram stain, although the latter are useful in differentiating Gram negative from Gram-positive organisms. Most bacteria are present within the cytoplasm of neutrophils, although when large numbers are present, they may be non-phagocytized. Cocci are usually gram positive, of the genus Staphylococcus or Streptococcus, and usually occur as doublets (and are thus often mistakenly identified as Diplococci, although streptococci may occur in short chains. Small bacilli are usually gram negative, and may appear as bipolar rods, or have a "safety-pin" appearance. Gram-negative small bacilli are difficult to identify in Gram stained material, as the neutrophils and background material also stain pink. Large bacilli which are Grampositive are usually either Bacillus spp are Clostridium spp. Filamentous rods that are thin and stain pale blue with intermittent pink and dark purple areas with Romanowsky stains are usually Nocardia or Actinomyces. Both are Grampositive, and Nocardia is partially acid fast (stains pink with Acid-Fast Stain). These organisms tend to be found in large clumps or colonies on the slide, and large areas of the film may contain no organisms. These organisms may be found in both subcutaneous lesions and body cavity fluids, usually as a result of penetrating foreign bodies. Spirochetes, spiral shaped bacteria, are commonly seen in preparations from the oral cavity and cutaneous lesions contaminated with mouth organism, fecal cytology, and occasionally cat-bite abscesses. They are very fine, pale blue, and approximately 10µ in length. Neoplastic processes are diagnosed by the presence of cells where they don't belong (for example, epithelial cells in a lymph node) or by cellular criteria of malignancy. As a general rule, several criteria of malignancy should be present before a diagnosis of neoplasia is considered. Nuclear changes in malignant cells are a reflection of increased nuclear activity or replication. Some nuclear criteria are thus found in cells undergoing hyperplasia, or controlled growth (eg, fibroblasts in granulation tissue). Common nuclear criteria include variable nuclear size (anisokaryosis), variable and usually increased nucleus: cytoplasm ratio, abnormally clumped chromatin patterns, and large, multiple, and irregularly shaped nucleoli. Other nuclear changes sometimes observed include abnormal mitoses, and nuclear molding (nuclei in multinucleated cells in which 2
3 one nucleus conforms to the shape of another nucleus). While multinucleation and normal-appearing mitotic figures are commonly observed in neoplastic cells, they are also commonly observed in normal cells, such as macrophages and mesothelial cells. Cytoplasmic criteria of malignancy are less important than nuclear criteria, and include increased basophilia and vacuolation. Both of these features are more commonly seen in tumors of epithelial origin. Vacuoles in tumor cells are sometimes simply a reflection of rapid growth and degeneration. In adenocarcinoma cells, however, characteristic perinuclear vacuolation, representative of the secretory and packaging role of the cell, is commonly observed. When large secretory droplets (Lassen bodies) compress the nucleus to the side of the cell, the cell is termed a "signet ring" cell. Normal cells that imbibe fluids can also have this appearance, however. Classification of neoplasms. Discrete round cell tumors. Cells from round cell tumors are small, discrete (individualized), and round. Lymphoma, plasma cell tumors, mast cell tumors, histiocytomas, malignant histiocytosis, and transmissible venereal tumors are typically classified as discrete cell tumors. Lymphoma can be found in virtually any organ, including skin. While neoplastic lymphoid cells may be either small lymphocytes or large lymphoblasts, they are more commonly lymphoblastic. If they are small they may have abnormal features, such as retained nucleoli, or cytoplasmic projections; PCR is usually required to confirm the diagnosis. When lymphoblastic, the cytologic diagnosis is relatively simple. Lymphoblasts, the predominant cell type, are approximately twice the size of neutrophils and have scant cytoplasm that is light to medium blue and is occasionally vacuolated, most commonly in the cat. Nuclei are usually indented with fine to stippled chromatin and usually contain one to three prominent nucleoli. While plasma cell tumors are most commonly found in the bone marrow, they may also proliferate in the liver, lymph nodes, spleen, etc. in patients with disseminated disease. Solitary plasma cell tumor masses may also occur subcutaneously and in the oral cavity. These tumors consist of plasma cells, many of which are usually somewhat immature or poorly differentiated. They have small nuclei with stippled chromatin, abundant basophilic cytoplasm, often a clear perinuclear area, and if neoplastic, multinucleated. Mast cell tumors are made up of mast cells, which are round cells that are usually slightly larger than lymphoblasts. They have variable numbers of distinctive small purple staining granules within the cytoplasm. The nucleus is round to oval and usually stains somewhat pale, presumably because the granules take up the stain. The cells are somewhat fragile, and free granules are usually present. Eosinophils are often present in aspirates of mast cell tumors. The granules in some mast cell tumors sometimes do not stain with Diff-Quik. Transmissible Venereal Tumors are sexually transmitted tumors of dogs. The tumors are malignant in behavior, but respond well to chemotherapy and radiation therapy. They exfoliate many discrete cells that have a moderate amount of light blue cytoplasm containing many distinct small vacuoles. The nuclei are round with coarse chromatin and large prominent nucleoli. They are usually found on mucous membranes of the penis, vagina, nose, etc. Histiocytomas are tumors of dogs, usually young, which regress spontaneously. The cells have a moderate amount of pale blue cytoplasm, round nuclei with fine chromatin and indistinct nucleoli. As they regress, they are infiltrated with small lymphocytes, which may be more numerous than the histiocytoma cells. The background fluid in aspirates is often darker than the cytoplasm of the cells, giving them a very pale appearance. Malignant histiocytosis cells are pleomorphic, large, discrete, markedly atypical mononuclear cells; nuclei are round to oval to reniform. Features suggestive of malignant histiocytosis include atypical histiocytic cells with features of malignancy including marked anisocytosis and anisokaryosis, prominent nucleoli, bizarre mitotic figures, marked phagocytosis of erythrocytes, leukocytes, and other tumor cells, and moderate amounts of lightly basophilic, vacuolated cytoplasm. The presence of multinucleated giant cells in the absence of inflammatory cells also supports the diagnosis. Neutrophils, eosinophils, small lymphocytes and plasma cells may be present in small numbers. Tumors of Epithelial Origin (Carcinomas and Adenocarcinomas). Neoplastic epithelial cells are usually much larger and have more cytoplasm than do cells from discrete cell tumors. They usually exhibit many of the criteria of malignancy discussed above. Various types of epithelial tumors, such as thyroid carcinomas, mammary carcinomas, prostate carcinomas, transitional cell carcinomas, perianal adenomas and adenocarcinomas, basal cell tumors, squamous cell carcinomas, sebaceous cell carcinomas, etc. have characteristics which aid in identification. 3
4 Tumors of Connective Tissue (Mesenchymal) Origin (Sarcomas). Spindle-cell tumors are similar in appearance to normal connective tissue cells, but exhibit variable criteria of malignancy. More malignant, less well differentiated cells, are less spindled in appearance. They usually appear individually, rather than in clumps as do epithelial cells. They usually have indistinct cytoplasmic borders, pale blue cytoplasm which may contain a few vacuoles, and large oval nuclei with prominent, usually multiple nucleoli. The appearance varies somewhat according to the tissue type, but tumors of mesenchymal origin are usually difficult to distinguish. Osteosarcomas usually have a distinctive appearance, in that the cells look like giant plasma cells, with the nucleus appearing to protrude from one end of the cell. The cytoplasm usually contains small eosinophilic granules. Background pink-colored matrix is usually present. Chondrosarcomas and myxosarcomas usually also have background matrix. Liposarcomas have a distinctive appearance, in that the cytoplasm contains multiple small fat vacuoles. Melanomas are classified as mesenchymal tumors, but their appearance is distinctive, in that some cells appear similar to epithelial cells, some are spindled, and yet others appear to be round and discrete. If the cells contain melanin granules (usually fine gray dust-like particles), they are readily diagnosable. However, many are amelanotic. Examples of cytologic preparations that should be evaluated "in-house" when possible. Bacterial peritonitis Obtaining the cytologic findings on abdominal fluid that contains bacteria 24 hours following collection of the fluid is often dismaying, as the animal has usually already expired. Thus it is important to be able to recognize the presence of bacteria at the time of collection. A fresh, direct film of the fluid should be made by placing a drop of fluid on a glass slide, placing a spreader slide directly on top of the drop, allowing the drop to spread, and pulling the two glass slides apart. By placing two drops of fluid on a slide, two preparations can be made simultaneously. The film is allowed to air dry, then stained with a Romanowsky stain such as Wrights, Wrights-Giemsa, Diff-Quik, etc. Even if one is going to send the fluid to a diagnostic laboratory for fluid analysis, it is important to send fresh air-dried films to accompany the fluid, as cells degenerate quickly, and degree of neutrophil degeneration is helpful in deciding if bacteria are present Bacteria stain blue with Romanowsky stains, and must be distinguished from background protein and stain sediment. They are usually somewhat uniform in size, present within the cytoplasm of neutrophils, and if present in large numbers, may be both free and phagocytized. Even the presence of very small numbers of bacteria is significant. If different types of bacteria are seen, GI rupture should be suspected. Large GI ruptures can be difficult to distinguish cytologically from GI aspirates. Usually the leukogram or clinical condition of the animal is helpful. Animals with GI ruptures are usually in shock, and usually have degenerative left shifts. If only one type of bacterium is present, sources other than the GI tract should be suspected. For example, two animals recently presented with all streptococci in the abdominal fluid. One dog had a ruptured bladder, and one had a ruptured uterus. If only Clostridial organisms are seen, ruptured liver abscess should be suspected. If large numbers of non-phagocytized bacteria are present, and almost all neutrophils contain phagocytized bacteria, the prognosis is usually poor. In addition to examining the slide, it is also useful to perform total nucleated cells counts and protein concentration on fluids, and color, clarity, odor, etc., should be noted. It would be very unusual for an animal with bacteria in the abdominal cavity to have a low cell concentration in the fluid; usually the cell count is greater than 25,000cells/µl, and may be greater than 1000,000/µl. Total nucleated cell counts can be determined by the same methodology as leukocyte counts for whole blood, using either a hemocytometer (Unopette system) or an electronic cell counter Total protein by refractometry should be determined by using the plasma protein scale of the refractometer. Inflammatory fluids usually contain greater than 3 grams of protein/dl. While specific gravity may be measured on the urine specific gravity scale, it does not add to information other than as an index of protein content. Examples of disorders that should be diagnosed prior to surgery Mast Cell Tumors should be widely excised, submitted for histopathology and graded to help ascertain a prognosis. Completeness of surgical excision (margins) is evaluated via histopathology. Three centimeters of normal tissue is considered desirable. Soft tissue sarcomas include fibrosarcomas, peripheral nerve sheath tumors, and hemangiopericytomas. These tumors should also be completely excised, as they tend to recur at the tumor site. They may be difficult to distinguish from fibroplasia (granulation tissue). 4
5 Examples of relatively simple cytology samples Non-inflammatory, non-neoplastic lesions Epidermal cysts arise from either sebaceous or squamous epithelial cells. The material from these cysts is usually gray to creamy. Films of the material contain abundant amorphous blue material that appears to be cytoplasmic remnants of cells. A few identifiable sebaceous epithelial cells or superficial squamous epithelial cells may be present. Cholesterol clefts are almost always present, and appear as large square to rectangular negative images. A few inflammatory cells may be present. Salivary mucoceles. Aspirates of sialoceles contain abundant cloud-like pink to violet to pale blue mucin. Large cells with small nuclei and abundant foamy cytoplasm (these may be macrophages or salivary epithelial cells) are numerous. Gold-colored rhomboidal hematoidin crystals free and within macrophages are usually present, and result from RBC breakdown. Malassezia canis is a common, normal yeast inhabitant of the ear canal of dogs and cats. However, occasionally overgrowth of the organism occurs, and a brown thick discharge will be present. These organisms are not usually accompanied by inflammatory cells. They are found in large numbers free and on the surface of superficial epithelial cells; they are approximately 3 µ in diameter, slightly oval, and broad-based budding is commonly seen. Inflammatory lesions Most inflammatory lesions can be identified quite quickly by cytology (see discussion above). While inflammatory cells are easily recognizable, some practice is required to identify various types of microorganisms. One must also remember that neoplastic processes can be accompanied by inflammation. Neoplastic lesions Neoplastic lesions that are usually readily identifiable include most of the discrete cell tumors, with the possible exception of malignant histiocytosis, which can sometimes be difficult to differentiate from granulomatous inflammation. Sarcomas usually are also relatively simple to diagnose, but can be confused with normal fibroplasia. Criteria of malignancy are usually helpful to differentiate these. Lipomas, benign mesenchymal tumors, are very common, and quite easy to diagnose based on cytology. Fat cells (lipocytes, adipocytes) are very large (approx µ) with clear cytoplasm (representative of where large fat globules were before staining) and a distinct, sometimes folded cytoplasmic membrane. The nucleus is small and dense, usually pressed against the cytoplasmic membrane. They often are washed away in the staining process. If the slide appears greasy prior to staining, and has nothing on it after staining, it was likely an aspirate of fat tissue. Normal fat tissue and lipomas cannot be differentiated based on cytology. Examples of relatively difficult cytology samples Neoplastic abdominal effusions Mesothelial cells tend to proliferate and exfoliate when fluid accumulates in a body cavity. They may appear singly or in clusters of 2,4, 8, or 16 cells. They are large (12-30 µ), have light to dark basophilic cytoplasm, and have single or multiple, round to oval nuclei with one or more nucleoli. Cells in mitosis may be seen. The cytoplasmic border may appear to have a pink "fringe" around it. Unfortunately, mesothelial cells can be very difficult to differentiate from epithelial cells. If epithelial cells are present in an abdominal fluid, it is an indication of neoplasia (carcinoma), so this is one differential that should probably be made by a clinical pathologist. Most helpful in differentiating mesothelial cells from carcinoma cells are the sheer numbers of cells present, as well as the size of the clusters. When carcinoma cells are exfoliating, large numbers are usually observed, and clusters of up to 100 cells may be observed. Mesothelial cells are usually in small clusters, often consisting of no more than 8 cells. Small cell variant of lymphoma Although malignancy of lymphoid tissue is almost always characterized by a predominance of immature lymphoid cells (lymphoblasts), occasionally, lymphoid tumors may be composed entirely of small lymphocytes. If an aspirate of an enlarged lymph node consists of a homogeneous population of small lymphocytes with no cytologic suggestion of antigenic stimulation (ie, presence of plasma cells), PCR is indicated. Other Other types of cytologic samples that are inherently difficult include nasal cytology, mammary gland cytology, cytology of the bladder, liver cytology, and cytology of most other intra-abdominal organs. The difficulty is usually because of an inability to distinguish malignant from benign processes in many of these tissues. 5
6 Cytology of Lymph Nodes Mary Anna Thrall Colorado State University Fort Collins CO Introduction We have historically diagnosed canine lymphoma based on cytologic evaluation of lymph nodes. If the diagnosis was not definitive based on cytology, we would recommend excisional biopsy and histopathologic evaluation of the node. However, we have learned that lymphoma cannot be diagnosed more accurately by histopathology. Fortunately, we now have a recently developed tool, polymerase chain reaction (PCR) for gene rearrangement, which can accurately diagnose those cases in which the cytologic diagnosis is questionable. This discussion will review the cytologic approach to diagnosis of lymph node enlargement, then discuss the value of PCR in those cases in which cytology is not definitive. Lymph node enlargement, whether localized or generalized, is the primary indication for lymph node aspiration cytology. Lymph node aspiration cytology is also indicated to determine if neoplastic metastasis to a lymph node has occurred. If a definitive diagnosis cannot be made on the basis of the cytologic examination, excisional biopsy for histopathologic examination should be performed. Lymph nodes were probably the first structures to be studied by aspiration cytology. The aspiration of lymph nodes to search for trypanosomes in human patients with sleeping sickness was reported in Aspiration cytology of lymph nodes has been increasingly advocated in both human and veterinary medicine. Because of the inexpensiveness and small amount of time required, lymph node aspiration cytology should be performed as a routine diagnostic procedure whenever indicated. Cytology of lymph nodes Selection of the lymph nodes to be aspirated should be made on the basis of clinical findings. In animals with generalized lymphadenopathy, at least two nodes should be aspirated. Lymph nodes draining the oral cavity and gastrointestinal tract tend to be antigenically stimulated under normal conditions and should not be chosen if others are available. Superficial lymph nodes can usually be aspirated without using a local anesthetic, since the procedure is usually no more painful than venipuncture. Inflamed lymph nodes tend to be more painful than those affected with a neoplastic disorder. Material aspirated should be placed on glass slides, and "pull" films made, such as is done when making films from bone marrow aspirates. Imprints of biopsied nodes can also be made. Lymphoid cells are very fragile and only slight pressure should be placed on the spreader slide. Identification of cell types Small lymphocytes These cells are similar to the small lymphocyte found in blood. The nucleus is slightly larger than a red blood cell. The nuclear chromatin is densely packed. The cytoplasm is generally scanty and consists of a narrow rim around the nucleus. The small lymphocyte is the primary cell type present in normal and hyperplastic nodes. Medium lymphocytes Medium sized lymphocytges have a nuclear diameter approximately equal to two red blood cells and have less densely packed nuclear chromatin. Lymphoblasts The nuclear chromatin is fine and diffuse. A nucleolus is usually observed. They are approximately 2 to 4 times the size of the mature lymphocyte. They may possess a broad or narrow rim of cytoplasm, but it is most commonly scanty. Lymphoblasts are present in small numbers in normal nodes and usually do not exceed 15% of the total cell population in hyperplastic lymph nodes. Plasma cells and plasmablasts These cells are derived from antigen stimulated B lymphocytes. The nucleus of plasma cells is eccentrically placed, the cytoplasm is generally quite basophilic and a perinuclear clear area may be present. The cytoplasm may contain vacuoles. Plasma cells that commonly seen in reactive lymph nodes. Plasmablasts, B cells which have undergone blast transformation, are similar to lymphoblasts but have more cytoplasm which is basophilic and sometimes vacuolated. 6
7 Neutrophils Any node undergoing an inflammatory process will contain many neutrophils. These may appear healthy and intact whether the inflammatory process is septic or non-septic. Degenerative changes in the nucleus of the neutrophil may indicate septic inflammation. Karyolysis and karyorrhexis may be present. Bacteria may be observed within the cytoplasm of the neutrophils in thin portions of the smear where the neutrophil is spread out on the slide. Macrophages These may be observed in certain chronic inflammatory conditions. These cells are phagocytic and may contain cellular debris. When macrophages develop some of the characteristics of epithelial cells, such as abundant cytoplasm, they are often referred to as epithelioid cells. Care should be taken not to confuse epithelioid cells with metastatic carcinoma cells. Mast cells Mast cellsmay be seen in all lymph node aspirates but are usually few in number. If large numbers are present, one may diagnose mast cell neoplasia with metastatic involvement of the lymph node. Neoplastic cells Tumor cells, such as carcinoma cells, may be seen in lymph nodes to which neoplasms have metastasized. The presence of cells not belonging to the normal population of the lymph node will attract attention. Malignant cells are usually quite pleomorphic, with an increase in the nuclear size in relation to the cytoplasm. The nuclei vary in size and shape. Nucleoli are often prominent and multiple. Many mitotic figures and multinucleated cells may be observed. Cytoplasmic vacuolation may be present. The cytoplasm of malignant epithelial cells commonly stains quite basophilic. Cytoplasmic fragments Small flakes of cytoplasm approximately 1-5 mm in diameter may be observed lying between the cells. These cytoplasmic fragments have been referred to as lymphoglandular bodies and are a characteristic feature of lymphoid tissue aspirates. They should not be confused with platelets or organisms. Pigment Hemosiderin is frequently seen in lymph nodes and may be intracellular or extracellular, probably as a result of cell breakage at the time of film preparation. Hemosiderin is a pigment resulting from RBC degradation that stains blue-green to black and is usually within macrophages. Melanin is usually golden brown to black but may be confused with hemosiderin. If necessary, a Prussian blue stain can be used to stain hemosiderin blue-black and confirm its presence. Melanin may be present within macrophages in nodes draining pigmented lesions or may be seen in melanocytes with metastatic melanoma. It may be difficult to differentiate macrophages that contain melanin from melanocytes; melanin within macrophages usually consists of homogeneous clumps within phagolysosomes, while melanin in melanocytes consists of individual melanin granules. Interpretation Normal lymph node Small lymphocytes are the predominant cell type and comprise 85 to 90% of the cells observed. Small numbers of macrophages, medium lymphocytes, lymphoblasts, plasma cells, and neutrophils may be present. Benign lymphoid hyperplasia (Immunologically Reactive Node) Small lymphocytes predominate. Variable numbers of medium lymphocytes and lymphoblasts may be observed. Mature and immature plasma cells are increased in number. Macrophages, neutrophils, eosinophils and mast cells may be increased in number. Aggregates or syncytia of macrophages may be seen in aspirates of benign hyperplastic lymph nodes. These aggregates should not be confused with clusters of metastatic epithelial cells. Nodes become reactive or hyperplastic when antigenically stimulated. Reactive nodes draining inflamed skin frequently contain increased numbers of eosinophils and mast cells, particularly if the skin pathology is a result of an allergic reaction. Lymphadenitis The cytology of an inflamed lymph node is variable depending on the etiology; neutrophils, eosinophils or macrophages may predominate. If the most predominant cell is the neutrophil, the inflammation is classified as purulent. If the predominant cell is the macrophage, the inflammatory response is classified as granulomatous. Most bacterial infections result in a purulent inflammatory response. An exception is Mycobacterium tuberculosis, which results in a granulomatous inflammatory reaction with abundant epithelioid cells. Mixed inflammatory reactions are usually seen in animals with systemic fungal disease such as coccidioidomycosis, histoplasmosis, blastomycosis, and cryptococcosis. However, aspirates 7
8 of nodes infected with Cryptococcus neoformans may have very little cellular response; aspirations often yield only large numbers of the organism. Other organisms, such as Leishmania, and Ehrlichia may also be seen in lymph node aspirates. Metastatic neoplasia Malignant tumors commonly metastasize via lymphatics, resulting in proliferation of neoplastic tissue in the lymph node. These neoplasms can often be diagnosed from lymph node aspirates. Diagnostic success is due to the ease with which alien tumor cells can be distinguished from the normal constituents of the node. The cytology is variable depending on the degree of node involvement. The node is usually quite reactive with numerous plasma cells. At times aspirates may yield only tumor cells, with complete displacement of normal lymphoid elements. Metastatic tumors commonly diagnosed include carcinomas, mast cell tumors, and malignant melanomas. Sarcomas are less frequently aspirated from lymph nodes. Rarely, myeloproliferative neoplasia may be present within lymph nodes. When attempting to aspirate the mandibular lymph node in the dog, the salivary gland may be mistakenly sampled. Normal salivary gland cells should not be confused with metastatic neoplastic epithelial cells. Primary lymphoid neoplasia (Lymphoma) Malignancy of lymphoid tissue is almost always characterized by a predominance of immature lymphoid cells (lymphoblasts). The lymphoblasts may be of uniform size and morphology or they may be pleomorphic. Numerous cells in mitosis may be present. Small lymphocytes and macrophages may be present in variable numbers. Plasma cells are usually quite few in number, which aids in the differentiation between lymphoma and lymphoid hyperplasia. Occasionally, lymphoid tumors may be composed entirely of small lymphocytes. If an aspirate of an enlarged lymph node consists of a homogeneous population of small lymphocytes with no cytologic suggestion of benign lymphoid hyperplasia, PCR is indicated. Aspirates of multiple enlarged nodes may aid in the cytologic diagnosis of lymphoma. Polymerase Chain Reaction (PCR) In certain situations, lymphoma can be difficult to distinguish from a benign reactive proliferation of lymphocytes (hyperplasia). Because clonality is the hallmark of malignancy, an assay has been developed that uses the polymerase chain reaction to amplify the variable regions of immunoglobulin genes and T-cell receptor genes to detect the presence of a clonal lymphocyte population. Gene rearrangement is appropriate for the immunophenotype (immunoglobulin gene rearrangement in B-cell lymphoma and T-cell receptor gene rearrangement in T-cell lymphoma). The clonal rearrangement can be detected when very small amounts of the DNA is derived from neoplastic cells Because all lymphomas are clonal expansions of lymphocytes, each particular neoplasm contains DNA regions that are unique in both length and sequence. The CDR3 region of both immunoglobulin and T-cell receptor (TCR) genes encodes the antigen-binding region of the respective receptor and contains the majority of this unique sequence. While it is assumed that malignancy is always clonal, all clonal expansions of lymphocytes are not necessarily malignancies, and it is important to consider this possibility if samples have clonal rearrangements but no other evidence of lymphoma. However, to date, only one dog without lymphoma (a dog with ehrlichiosis) has tested positive. Sample submission: Aspirates of lymph nodes (or other organs) can be submitted in about 1 ml of physiologic saline (LRS, NormR). Two to three aspirates, with rinsing the syringe in the saline each time, should provide adequate material. Alternatively, cytology slides (stained or unstained) can be scraped and PCR performed on the scraped cells. Samples should be sent to Colorado State University Diagnostic Laboratory, Attention: Dr. Anne Avery, Fort Collins CO Selected References 1. Burnett RC, Vernau W, Modiano JF, Olver CF, Moore PF, Avery A. Diagnosis of Canine Lymphoid Neoplasia Using Clonal Rearrangements of Antigen Receptor Genes. Vet Pathol, 2003: 40: Duncan JR: The Lymph Nodes. In Diagnostic Cytology of the Dog and Cat. R Cowell and R Tyler, Editors. American Veterinary Publications, Inc.,1989, pp Duncan JR. The lymph nodes. In Diagnostic Cytology of the Dog and Cat. R Cowell, R Tyler, Meinkoth JH, Editors. American Veterinary Publications, Inc.,1999, pp Raskin R. Lymphoid system. In Atlas of Canine and Feline Cytology. R Raskin and D Meyer. WB Saunders Co, Philadelphia, 2001, pp Thrall MA. Cytology of Lymphoid Tissue. Comp. Cont. Educ.1987, 9:
9 CYTOLOGY OF BLOOD Mary Anna Thrall INTRODUCTION Overview to the diagnostic usefulness of blood film examinations Examination of blood films by technicians or veterinarians can provide a large amount of diagnostically useful information, and should remain a component of the complete blood count (CBC). Systemic examination of a blood film can provide useful information related to erythrocytes, leukocytes and platelets. Critical to blood film evaluation is adequate blood film preparation. Blood films are prepared by placing a small drop of blood on a clean glass microscope slide. The end of a second slide is placed against the surface of the first slide at a 30 degree angle and drawn back into the drop of blood. When the blood has spread along most of the width of the spreader slide, it is then pushed forward with a steady, even, rapid motion. A properly prepared blood film is thin, with even distribution of cells. After air drying, the film should be stained with Wright's or Wright's Giemsa stain. A quick stain that usually gives acceptable results is Diff-Quik (Harleco). Low-power magnification (100x) is used to note cell numbers and to scan the feathered edge for platelet clumps, large abnormal cells, and microfilariae. The observer should then select a portion of the film near the thin end, referred to as the counting area, and switch to the oil-immersion objective (1000x) to complete the evaluation. The interpretation of blood film morphology must be made in conjunction with other quantitative data from the complete blood count (CBC). The blood film can also be used for quality assurance that the total nucleated cell count and platelet count are correct. ERYTHROCYTES Normal red cell morphology varies among different species. Most mammalian erythrocytes are round, and somewhat biconcave-disk shaped. Species with smaller RBCs, such as the cat, have less concavity. Briefly, the significant differences between species are size, shape, amount of central pallor, tendency to form rouleaux, presence of basophilic stippling in regenerative response to anemia, and presence of reticulocytes in response to anemia. Erythrocyte morphology is often an important aid in the diagnosis of cause of anemia, and is sometimes helpful in the diagnosis of other disorders. This discussion will concentrate on those morphologic changes, categorized according to color, size, shape, structures in or on erythrocytes, and cell arrangement on blood film, which are most diagnostically useful. COLOR Polychromasia: Polychromatophilic cells are young erythrocytes which have been released early. They are usually large and are more blue-colored, due to the presence of organelles, than mature RBCs. The presence or absence of polychromatophilic RBCs is very important when determining the cause of anemia. If immature cells are released, the likely cause of the anemia is blood loss or blood destruction, with the marrow attempting to compensate by early release of cells (regenerative anemia). If the anemia is due to erythroid hypoplasia or aplasia within the marrow, polychromatophilic cells will not be increased (non-regenerative anemia). Horses are unique in that they do not release polychromatophilic cells in the face of anemia. While degree of polychromasia correlates well with the reticulocyte count, it is less subjective to evaluate 9
10 the regenerative response by counting reticulocytes. The reticulocyte is analogous to the polychromatophilic RBC, but is stained with a vital stain such as new methylene blue or brilliant cresyl blue, which causes the organelles to clump into visible granules. The count is performed by enumerating 1000 RBC as either reticulocytes or non-reticulocytes. The resultant percentage may be multiplied by the RBC count to determine reticulocytes/µl of blood. In general, greater than 60,000 reticulocytes/µl blood is considered a regenerative response to anemia. Cats are unique, in that they produce two forms of reticulocytes, aggregate and punctate. The aggregate form has clumped organelles and represents newly released cells. The punctate form has variable numbers of individual dots in the RBC and represents cells released 12 hours to 12 days earlier. To assess the current marrow status, only aggregates should be counted. Hypochromasia: Hypochromic red blood cells are pale with increased central pallor as a result of decreased hemoglobin concentration due to iron deficiency. One needs to distinguish hypochromic cells from bowl-shaped or "punched-out" cells, which are insignificant. SIZE Variation in RBC size is termed anisocytosis, which may be due to the presence of large cells (macrocytes) or small cells (microcytes), or both. Microcytic RBCs. Cells must be markedly decreased in size before microcytosis can be visually detected. Mean corpuscular volume (MCV) is more valuable in assessing size of erythrocytes. Using automated cell counting systems, a histogram or volume distribution curve of the erythrocyte population is generated. MCV is determined from analysis of the volume distribution curve and the hematocrit is then calculated by multiplying the MCV by the RBC concentration. The only important cause of true microcytosis is iron deficiency anemia. Dogs with portocaval shunts may have microcytic anemia without iron deficiency. Some breeds of dogs (Akitas) normally have smaller RBCs. (Spherocytes are not microcytic, in that their volume is normal). The hallmark of iron deficiency anemia is a decreased MCV. Early in iron deficiency anemia there are two populations of cells due to the remaining normal cells. Also, during recovery of iron deficiency, larger cell population appears. In some cases the MCV may be normal, although the animal has a microcytic population of cells. Anemia is initially regenerative; may become non-regenerative in the very late stages or may be non-regenerative with concurrent inflammatory disease (anemia of chronic disease). Iron deficiency anemia is always a result of chronic external blood loss in adult animals. In young animals which are nursing, particularly pigs and kittens, iron deficiency anemia is very common. After animals begin to eat solid food, they rapidly repopulate the blood with large cells. Macrocytic RBCs. The most common cause of macrocytosis is increased numbers of immature RBC, which will usually also be polychromatophilic (exception is the horse). Macrocytosis is usually associated with a relative hypochromasia and decreased MCHC. Less common causes are Poodle macrocytosis (rare), inherited stomatocytosis (Alaskan malamute, Miniature schnauzer), and some anti-epileptic drugs (rare). Vitamin B12 deficiency is a common cause of macrocytic anemia in human, but is very rarely seen in domestic animals. SHAPE Abnormally shaped erythrocytes are called poikilocytes. Some shape changes are suggestive of certain disease entities. 10
11 Spiculated cells are RBCs with one or more surface spicules. It is a general term which includes echinocytes, acanthocytes, keratocytes and schistocytes. Again, it is better to be as specific as possible when describing shape changes, as certain types of spiculated cells have been associated with certain diseases. Schistocytes, or RBC fragments, are usually due to shearing of the red cell by intravascular trauma. This may be observed with disseminated intravascular coagulopathy (DIC) as a result of RBCs being broken by fibrin strands, with vascular neoplasms such as hemangiosarcoma, and with iron deficiency. In animals with DIC, there is usually a concurrent thrombocytopenia. In dogs with hemangiosarcoma, there are usually acanthocytes present as well as fragments. In iron deficiency anemia, the fragmentation is apparently a result of oxidative injury leading to membrane lesions or increased susceptibility to intravascular trauma. Initially the RBC develops what appears to be a blister or vacuole which is thought to represent an oxidative injury where inner membrane surfaces are crosslinked across the cell. Exclusion of hemoglobin may account for the colorless area. These lesions subsequently enlarge, break open to form "apple-stem cells" and keratocytes, a spiculated red cell with two or more pointed projections. The projections from the keratocytes probably then fragment from the cell. Acanthocytes, or spur cells, are irregular, spiculated red cells with few, unevenly distributed surface projections of variable length and diameter. They are thought to result from changes in cholesterol concentration in the red cell membrane. They are seen in patients with altered lipid metabolism such as may occur with liver disease (seen most commonly in cats with hepatic lipidosis; occur occasionally in dogs with end-stage liver disease). They are seen quite consistently in dogs with hemangiosarcoma; pathogenesis of this shape change with hemangiosarcoma is not known. The presence of acanthocytes in middle age to old large-breed dogs that have a concurrent regenerative anemia are almost diagnostic of hemangiosarcoma. Echinocytes (burr cells) are spiculated cells with numerous short, evenly spaced, blunt to sharp surface projections which are quite uniform in size and shape. Echinocyte formation can be an artifactual result (crenation) of ph change from slow drying of blood films, has been associated with renal disease and lymphosarcoma (or its treatment) in dogs, following exercise in horses, and following rattlesnake envenomation in dogs. Spherocytes are small, darkly staining cells lacking central pallor. They are not easily detected in domestic species other than dogs, because other species do not have the central pallor that is so prominent in dog erythrocytes. Spherocytes have a reduced amount of membrane as a result of partial phagocytosis which occurs because antibody and/or complement is on the surface of the RBC. They are very significant in that they suggest immune-mediated hemolytic anemia, and are considered more diagnostically important than a positive Coombs test. Spherocytes may also be seen following blood transfusion with mismatched blood. STRUCTURES IN OR ON ERYTHROCYTES Heinz bodies. Oxidative denaturation of hemoglobin results in Heinz body formation; however, cats normally have small numbers of Heinz bodies. They are difficult to see on Wright's stained blood films, particularly in the dog, but may appear as small eccentric pale objects within the red cell or protruding slightly from the red cell margin and are usually 0.5 to 1.0 µm in 11
12 diameter, but may be larger. In dogs with oxidative injury to RBC, eccentrocyte formation may be more apparent, in which hemoglobin shifts to one side of the cell. When stained with vital stains such as new methylene blue, Heinz bodies appear as blue structures. Heinz bodies decrease deformability of red cells, making them more susceptible to hemolysis. Oxidative drugs and compounds known to induce Heinz body formation include onions, benzocaine, acetaminophen, methylene blue, and propylene glycol (used in semi-moist cat foods). Ill cats may develop a high concentration of Heinz bodies without being exposed to oxidant chemicals or drugs. The most common disorders associated with increased concentration of Heinz bodies are diabetes mellitus, lymphosarcoma, and hyperthyroidism. Basophilic stippling. In vivo aggregation of ribosomes into small basophilic granules is referred to as basophilic stippling (Fig 6), normally associated with immature erythrocytes (regenerative response to anemia) in ruminants and seen to a lesser extent in cats and dogs with intensely regenerative anemias. When not associated with anemia it is suggestive of lead poisoning. Nucleated erythrocytes (rubricytes, metarubricytes). Increased numbers of RBCs in which the nucleus remains are associated with regenerative anemias and early release of these cells in response to hypoxia. Increased numbers of nucleated RBC may also be seen in animals with non-functioning spleens or microvascular injury. Increased nucleated RBCs out of proportion to the degree of anemia is associated with lead poisoning. In animals with erythroid leukemia, immature nucleated red cells are often present in the absence of polychromasia. Howell-Jolly bodies. Nuclear remnants in erythrocytes are termed Howell-Jolly bodies and are small round blue inclusions; a few may be seen normally. Increased numbers are associated with regenerative anemia, splenectomy, and suppressed splenic function. Parasites. The primary parasitic disease of cat RBCs, and probably the most common cause of hemolytic anemia in the cat, is Hemobartonella felis), a rickettsial organism which is the causative agent of feline infectious anemia. It is attached to the RBC membrane and appears as either a rod-shaped organism on the periphery of the RBC or a delicate basophilic ring on the cell. They are commonly an opportunist, and often seen secondary to some other disease. A less common parasite is the protozoan Cytauxzoon felis, which appears as a ring 0.5 to 1.5 µm in diameter and contains a small basophilic nucleus. Erythrocyte parasites are rare in the dog. Hemobartonella canis usually only occurs in dogs which have been splenectomized or have non-functional spleens. Organisms appear as small dots which chain across the surface of the erythrocyte. It is common to see spherocytes and agglutination in addition to the parasite. Babesia canis and Babesia gibsoni are protozoal red cell parasites of the dog which produce severe hemolytic anemia. B. canis usually appears as tear drop shaped structures; B. gibsoni is smaller and varies considerably in size and shape. Viral inclusions. Viral inclusions are rarely seen in erythrocytes from dogs with distemper. Distemper inclusions are variable in size (approximately 1.0 to 2.0 µm), number, and color (faint blue to magenta), and are seen more frequently in polychromatophilic erythrocytes. 12
13 ARRANGEMENT ON BLOOD FILM Rouleaux formation: Rouleaux formation is the spontaneous association of erythrocytes in linear stacks, appearing similar to stacks of coins. Marked rouleaux formation is normal in the horse, and a slight amount is normal in the dog and cat. Rouleaux is enhanced when concentration of plasma proteins such as fibrinogen or immunoglobulins is increased. Increased rouleaux formation is often suggestive of a gammopathy. Agglutination: Agglutination of RBCs results in irregular spherical clumps of cells (3 to many) as a result of antibodyrelated bridging of RBCs. Agglutination is very suggestive of immune mediated hemolytic anemia, but may be seen following mismatched blood transfusion. To confirm that agglutination is taking place, mix a small quantity of blood with a drop of isotonic saline; agglutination will persist, while rouleaux will disperse. Agglutination may be so marked that it can be seen grossly on the blood film and on the side of the EDTA tube. Coombs test is not indicated if agglutination is already present, and in fact the Coombs test is often negative in these animals, presumably because the antibody washes off of erythrocytes. LEUKOCYTES While morphologic abnormalities of leukocytes are sometimes diagnostically useful, quantitative data obtained from the CBC are usually more helpful. Importantly, absolute, rather than relative, concentration of leukocytes should be interpreted. Typically, leukograms can be classified as either normal, stress (or steroid), inflammatory, or excitement. Stress leukogram from endogenous or exogenous steroids results in lymphopenia and neutrophilia (2- fold increase). Inflammatory leukograms are characterized by an increase in immature neutrophils that may be accompanied by a neutrophilia. Monocytosis may be present. Excitement leukograms occur with fear, excitement, or strenuous exercise as a result of increased epinephrine. Neutrophils are transiently shifted from the marginal neutrophil pool to the circulating pool, resulting in a neutrophilia without a left shift. In addition, lymphocytosis is also present. Epinephrine-associated changes are more common in young animals and the cat. Neutropenia is usually due to production problems (viruses, drugs and toxins, irradiation, myelopthisis,etc), consumption (as with an overwhelming bacterial infection or immune mediated destruction), or sequestration, as is thought to occur with endotoxemia. Morphologic abnormalities of leukocytes may be inherited or acquired. Examples of inherited abnormalities of neutrophils include Pelger-Huet anomaly (lack of nuclear segmentation), Birman cat neutrophil granulation anomaly, lysosomal storage diseases in which leukocytes may be granulated (such as mucopolysaccharidoses and GM2 gangliosidosis), and Chediak-Higashi syndrome, in which lysosomes are fused, appearing as large pink inclusions in neutrophils. Acquired abnormalities of neutrophils includes "toxic" changes, including cytoplasmic basophilia, Doehle bodies, and vacuoles, which are usually associated with inflammation, infection, drug toxicity, etc; these changes are thought to be due to decreased time of neutrophil maturation within the marrow. Intracytoplasmic neutrophil inclusions may be seen with Ehrlichia species or Hepatozoon canis. Lymphocytosis is usually due to excitement in cats, leukemia, or certain types of chronic antigenic stimulation, such as with ehrlichiosis. Lymphopenia is common and is usually due to stress or exogenous corticosteroids. Acquired lymphocyte abnormalities include "reactive" changes, usually appearing as increased size and cytoplasmic basophilia. Increased numbers of lymphocytes containing cytoplasmic granules may be seen with certain types of chronic antigenic 13
14 stimulation, such as ehrlichiosis. Abnormalities of lymphocytes are seen with several inherited lysosomal storage disorders. Lymphocytes are vacuolated in several of these disorders, such as GM1 gangliosidosis, alpha mannosidosis, Niemann-Pick disease types A,B, and C, and acid lipase deficiency. Lymphocytes contain granules in the mucopolysaccharidoses and GM2 gangliosidosis. PLATELETS Quantitative abnormalities of platelets include thrombocytosis, which is usually due to excitement, and may be seen with iron deficiency anemia, inflammation, and neoplasia, and thrombocytopenia, which is due to production problems (drugs, chemicals, immune mediated destruction of megakaryocytes, etc), consumption (such as is seen with disseminated intravascular coagulopathy), and destruction (immune mediated). Morphologic abnormalities are unusual; giant platelets are usually associated with early release, often indicative of increased production. References Thrall MA: Erythrocyte Morphology. In Thrall MA, Baker D, Campbell T, DeNicola D, Fettman MG, Lassen ED, Rebar AH, Weiser MG: Veterinary Hematology and Clinical Chemistry. Lippincott, Williams and Wilkins, Baltimore, 2004, pp Thrall MA: Classification of and Diagnostic approach to Anemia. In Thrall MA, Baker D, Campbell T, DeNicola D, Fettman MG, Lassen ED, Rebar AH, Weiser MG: Veterinary Hematology and Clinical Chemistry. Lippincott, Williams and Wilkins, Baltimore, 2004, pp Thrall MA: Regenerative anemia. In Thrall MA, Baker D, Campbell T, DeNicola D, Fettman MG, Lassen ED, Rebar AH, Weiser MG: Veterinary Hematology and Clinical Chemistry. Lippincott, Williams and Wilkins, Baltimore, 2004, pp Thrall MA: Non-regenerative anemia. In Thrall MA, Baker D, Campbell T, DeNicola D, Fettman MG, Lassen ED, Rebar AH, Weiser MG: Veterinary Hematology and Clinical Chemistry. Lippincott, Williams and Wilkins, Baltimore, 2004, pp Weiser MG, Thrall MA: Interpretation of Leukocyte Responses in Disease. In Thrall MA, Baker D, Campbell T, DeNicola D, Fettman MG, Lassen ED, Rebar AH, Weiser MG: Veterinary Hematology and Clinical Chemistry. Lippincott, Williams and Wilkins, Baltimore, Lippincott, Williams and Wilkins, Baltimore, 2004, pp


15 What Your Cell Counter Does Not Tell You About Leukocytes Glade Weiser, DVM, DipACVP College of Veterinary Medicine & Biomedical Sciences Colorado State University and Heska Corporation, Fort Collins / Loveland, Colorado Mary Anna Thrall, DVM, MS, DipACVP College of Veterinary Medicine & Biomedical Sciences; Colorado State University, Fort Collins, Colorado and Ross University School of Veterinary Medicine, St. Kitts, West Indies INTRODUCTION Instrumentation with varying degrees of differential capability has made its way to the individual veterinary facility over the past 15+ years. Reduction in size and cost of systems has made it possible to incorporate automated differential technology into benchtop hematology analyzers. However, the capability and use of this technology has debatably been misrepresented to veterinary users. Many users perceive that with an automated hematology analyzer blood film examination is not needed for clinical hematology. In both human and veterinary hematology, the automated differential is not intended to replace the blood film for leukocyte evaluation. It is intended to reduce labor-time by aiding the user to place samples into one of two categories: 1. Samples that may benefit from additional microscopic evaluation after meeting defined abnormal criteria. 2. Samples that have a high probability of limited additional value from microscopic evaluation. Development of criteria for microscopic follow-up evaluation in human hematology is relatively easy because most hemograms are normal and human cells behave more predictably in analytical systems. In veterinary hematology, samples are more complex because a higher proportion have abnormalities. In addition, cells of individual animals have more variable behavior in these systems; this may be related to biologic variation within a species such as the dog. The purpose of this section is to develop criteria and rationale for monitoring the automated differential in the veterinary setting and outline important diagnostic leukocyte morphology that is only evident on the blood film. Automated Leukocyte differentiation technology It is important to understand the capabilities and limitations of various technologies used in automated leukocyte differentiation in order to develop criteria for which samples should receive follow-up by microscopy. All cell counting systems make measurements on a large number of individual cells. Cell counting systems are based on either the electronic impedance principle or variations on the theme of light scatter. Impedance systems. Electronic impedance systems measure individual cell volume after differential shrinkage by lytic reagents. They differentiate leukocytes into 3 major populations as indicated in the following diagram Particle Volume (fl) Software categorizes leukocytes based on differential shrinkage and final volume of lymphocytes, mononuclear cells, and granulocytes. These systems usually have good subpopulation resolution. Limitations are as follows. Occasional canine 15




16 samples may have unexplained neutrophil collapse that clouds resolution of the subpopulations. With some experience, this can be monitored by inspection of the histogram. There is normal variation from dog to dog and cat to cat in the granulocyte volume distribution. Floating thresholds will deal with these variations in calculating granulocyte concentration, to a degree. Certain cell abnormalities are not distinguished and are included in one of the three subpopulations; these include NRBC, left shifted neutrophils, blast cells, and eosinophils. Light scatter systems. Some light scatter systems categorize cell particles after lysis based on forward light scatter, an index of size, and side scatter, an index of granularity or complexity as a primary set of measurements to resolve 3 cell populations. Additional measurements resolve other minor cell populations. The total WBC and RBC and PLT measurements are done by the electronic impedance principle. The following two plots are from dog blood analyzed on the Cell-dyn system. M G M? G? L L? Experience with this system indicates satisfactory WBC differential analysis in approximately 50% of cases. The other 50% have problems with subpopulation resolution. Another system, Bayer Advia, measures forward light scatter, an index of size, and peroxidase staining intensity. Representative cytograms are shown below. M N M? Size L E L? Peroxidase intensity 16



17 Resolution of cell populations is variable and often requires operator intervention with microscopy to correct the results. Abnormal cell types are only detected by microscopy. In addition, eosinophil behavior is inconsistent across a species as illustrated below. The case on the left had an eosinophil population that is poorly resolved between the neutrophil and eosinophil region. The case on the right had prominent eosinophilia by microscopy, but on the instrument cytogram the eosinophils were not present in the eosinophil region and had moved to the monocyte region. Use of light scatter systems for veterinary applications may be summarized as follows. These systems are very efficacious for high throughput analysis of normal, homogeneous animal populations such as those in toxicology studies. For clinical application purposes these systems have variable reliability for the differential from sample to sample that requires some method of monitoring. Monitoring the system s cytograms for proper individual sample differential resolution is complex and requires considerable skill. The best correlation is achieved for neutrophils; other cell populations are more variable. In addition, certain cell abnormalities are not distinguished and are included in one of the three subpopulations; these include NRBC, left shifted neutrophils, blast cells, and eosinophils. As a result, many laboratories default to microscopy differentials on all samples. Development of Criteria for Use of Blood Films with Leukocyte Data One approach used by many laboratories is to routinely default to a manual differential for all samples. It is paradoxical to invest in the most expensive technology and then not utilize the components that add cost, but that is the way it is. Most large laboratories have a high proportion of abnormal blood samples. This inherently is associated with mis-analysis of WBC populations. Therefore, this approach is based on the experience that the proportion of samples requiring a microscopy differential on light scatter systems is so high that it is easier to perform microscopy differentials than it is to sort the samples by other criteria. An approach that may be considered in the veterinary practice facility is an algorithm for evaluation of each sample for additional microscopy follow-up. This is particularly useful if the hematology workload deals with predominantly normal samples for health and pre-anesthetic exams. It is recommended that a blood film be made and rapid stained for each sample. The rationale is that the morphology will be available for rapid low power screening of the differential results, evaluation of any low platelet concentrations, and evaluation of erythrocytes if anemia is present. Only a subset of slides will be needed for the more labor intensive microscopy differential. The consideration should start with determining if the automated leukogram data are normal or not. Then, use of the blood films is described as follows. Normal leukogram data. When the total WBC concentration and differential are normal, it is likely that the instrument system has performed a highly reliable differential. However, it is recommended that the blood film be scanned on low power for any possible surprises in the WBC. With a little experience, it is possible to verify the reliability of the automated differential with a low power scan in less than one minute. For cases in which there is a surprise WBC abnormality, a microscopy differential should be performed on high power. Abnormal leukogram data. These may be categorized by the following patterns 1 : Leukopenia: The data are very likely reliable. The most common abnormality resulting intext bb leucopenia is neutropenia. The slide should be scanned on low power for any abnormal cells such as blasts. In addition, the neutrophils should be examined for 17
18 left shift (presence of band neutrophils) and toxic change; this is helpful to distinguish inflammatory consumption from immune mediated destruction or a production failure. (For a description of band neutrophils and toic change, see text box at bottom) Leukocytosis with granulocytic predominance: This is the most common abnormal leukocyte pattern in dogs and cats. These are usually neutrophilias combined with lymphopenia. The histogram should be examined. If the neutrophil or granulocyte region is properly positioned, the data have a high probability of being reliable. This pattern can be easily verified by a low power scan of the blood film. Neutrophils should be examined for left shift and toxic change. If any band neutrophils are found on the scan, a microscopy nucleated cell differential count should be performed. Other significant abnormalities that may be missed by the cell counter are the presence of neoplastic cells of hematopoietic origin (either myeloid or lymphoid) and eosinophilia. Leukocytosis with lymphoid predominance: This pattern is always associated with some form of lymphoproliferative process. Less commonly, extreme metarubricytosis may also mimic this pattern on the instrument. The slide should be scanned for the presence of lymphoblasts and the lymphocyte morphology should be examined. A microscopy differential should be performed because the blasts present may move from the instrument s lymphoid region to other regions of the differential. Mild to moderate lymphocytosis with normal lymphocyte morphology is associated with excitement response (usually in the young cat), Addison's disease 2 (rarely), and chronic canine ehrlichiosis 3, 4. In the latter disease, granular lymphocytes may be present. Marked lymphocytosis (>30,000 lymphocytes/µl) is almost always associated with lymphoid leukemia. If the lymphocyte morphology is normal and the lymphocytosis is marked, the likely diagnosis is chronic lymphocytic leukemia (CLL). Ehrlichiosis and CLL can be differentiated by testing for ehrlichiosis by measuring antibody titers, and performing PCR for lymphoma, which detects the presence of neoplastic lymphoid cells because of their clonal rearrangement of antigen receptor genes 5. This systematic use of blood films in conjunction with the hematology instrument will build user experience and competency to recognize normal from abnormal and to be able to characterize basic abnormal findings. Unusual abnormal findings may be referred to a pathologist for review. While monitoring leukocytes, the blood film is also readily available for review of erythrocyte and platelet abnormalities. Band neutrophils are immature neutrophils that have nuclei that are U or S shaped, with parallel sides. The nucleus is not constricted more than 2/3 the diameter in any place along its length. If they are increased in concentration, it is an indication of the presence a significant inflammatory process. Toxic neutrophils are characterized by cytoplasmic basophilia, cytoplasmic Doehle bodies, cytoplasmic vacuoles or "foaminess", and very rarely, intensely stained primary granules (toxic granulation). Doehle bodies are 0.5 to 2.0 µm angular blue grey particles, usually at the periphery of the cell. They represent aggregations of rough endoplasmic reticulum. These "toxic" changes are due to decreased time of neutrophil maturation within the marrow. Additional detail on abnormal leukocyte morphology is available 1. References: 1. Weiser MG, Thrall MA: Interpretation of Leukocyte Responses in Disease. In Thrall MA, Baker D, Campbell T, DeNicola D, Fettman MG, Lassen ED, Rebar AH, Weiser MG: Veterinary Hematology and Clinical Chemistry. Lippincott, Williams and Wilkins, Baltimore, pp Peterson ME, Kintzer P, Pretreatment clinical and laboratory findings in dogs with hypoadrenocortidcism: 225 cases. JAVMA, 1996, 208: Weiser MG, Thrall MA, Fulton R, et al: Granular lymphocytosis and hyperproteinemia in dogs with chronic ehrlichiosis. JAAHA 27: 84-88, Heeb HL, Willkerson MJ, Chun R, et al: Large granular lymphocytosis, lymphocyte subset inversion, thrombocytopenia, dysproteiinemia, and positive Ehrlichia serology in a dog. JAAHA 39: , Burnett RC, Vernau W, Modiano JF, Olver CF, Moore PF, Avery A. Diagnosis of Canine Lymphoid Neoplasia Using Clonal Rearrangements of Antigen Receptor Genes. Vet Pathol, 2003: 40:
19 Integration of Blood Film Findings and Automated Instrumentation Data Mary Anna Thrall, DVM, MS, DACVP College of Veterinary Medicine & Biomedical Sciences; Colorado State University, Fort Collins, Colorado and Ross University School of Veterinary Medicine, St. Kitts, West Indies. Case 1 Signalment and History: 11 year old male cat. Lethargy and polydypsia. One month ago PCV was 38%. CBC Reference Range Packed cell volume (%) RBC (x10 6 /µl) Hgb (g/dl) MCV (fl) MCHC(g/dl) Reticulocytes(µl) 155, ,000 Figure: Histogram Solid line = patient; Dashed line = normal Relative Number Cell Volume (fl) Nucleated cells (µl x10 3 ) Metamyelocytes (µl x10 3 ) Band neutrophils (µl x10 3 ) Seg. neutrophils (µl x10 3 ) Lymphocytes (µl x10 3 ) Monocytes (µl x10 3 ) Eosinophils (µl x10 3 ) Nucleated RBCs (µl x10 3 ) Platelets (x 10 3 / µl) Adeq Plasma protein (g/dl)
20 Case 2 Signalment: Five year old, spayed female, Cocker spaniel. History: Acutely lethargic Physical Examination: Pale, slightly icteric, mucous membranes Hematology Reference Range Packed cell volume (%) Hemoglobin (g/dl) RBC (10 6 /µl) MCV (fl) MCHC (g/dl) Reticulocytes (x 10 3 / µl) 123 <60 Histogram Solid line = patient; Dashed line = normal Relative Number RDW Cell Volume (fl) Total nucleated cell count (x10 3 /µl) Segmented neutrophils (x10 3 /µl) Band neutrophils (x10 3 /µl) Metamyelocytes (x10 3 /µl) Monocytes (x10 3 /µl) Lymphocytes (x10 3 /µl) Eosinophils (x10 3 /µl) NRBCs (µl x10 3 ) Platelets (x 10 3 / µl) Plasma protein (g/dl)
21 Case 3 Signalment and history: Eleven year old DSH spayed female cat presented for anorexia and lethargy. Hematology Reference Range Packed cell volume (%) RBC (x10 6 /µl) Hgb (g/dl) MCV (fl) MCHC (g/dl) Reticulocytes(µl) 7, ,000 Histogram Solid line = patient; Dashed line = normal Relative Number RDW Cell Volume (fl) Nucleated cells (µl x10 3 ) Metamyelocytes (µl x10 3 ) Band neutrophils (µl x10 3 ) Seg. neutrophils (µl x10 3 ) Lymphocytes (µl x10 3 ) Monocytes (µl x10 3 ) Nucleated RBCs (µl x10 3 ) Blasts (µl x10 3 ) Platelets (x 10 3 / µl) Adeq Plasma protein (g/dl)
22 Case 4 Signalment and history: Seventeen year old male cat presented for lethargy and enlarged abdomen. Liver disease suspected, but biochemical profile normal. Hematology Reference Range Packed cell volume (%) MCV (fl) MCH(g/dl) Reticulocytes(µl) ND 0-60,000 Histogram Solid line = patient; Dashed line = normal Relative Number RDW Cell Volume (fl) Nucleated cells (µl x10 3 ) Metamyelocytes (µl x10 3 ) - 0 Band neutrophils (µl x10 3 ) Seg. neutrophils (µl x10 3 ) Lymphocytes (µl x10 3 ) Monocytes (µl x10 3 ) Eosinophils (µl x10 3 ) Basophils (µl x10 3 ) 0.8 rare Platelets (x 10 3 / µl) Adeq Plasma protein (g/dl)
23 Case 5 Signalment One year old pointer History: Treated for neck or back pain with corticosteroids by referring veterinarian. Dog was thought to have GI parasites due to occult blood in feces, and was treated with antihelminthics. The dog returned one month later with a PCV of 15% and MCV of 40 fl. At that time the dog had an abdominal effusion. Physical Examination: Painful abdomen, pale mucous membranes Hematology Reference Range Packed cell volume (%) Hemoglobin (g/dl) RBC (10 6 /µl) MCV (fl) MCHC (g/dl) Reticulocytes (x 10 3 / µl) 18 <60 Histogram Solid line = patient; Dashed line = normal Relative Number RDW Cell Volume (fl) Total nucleated cell count (x10 3 /µl) Segmented neutrophils (x10 3 /µl) Band neutrophils (x10 3 /µl) Metamyelocytes (x10 3 /µl) Monocytes (x10 3 /µl) Lymphocytes (x10 3 /µl) Eosinophils (x10 3 /µl) Platelets (x 10 3 / µl) Plasma protein (g/dl) Case 6 Signalment and History: 6 year old female Labrador. Instrument WBC Data Reference Range Nucleated cells (µl x10 3 ) Neutrophils (µl x10 3 ) Lymphocytes (µl x10 3 ) Monocytes (µl x10 3 )
24 Case 7 Signalment and History: 2 year old male German Shorthaired pointer. Instrument Data Reference Range Nucleated cells (µl x10 3 ) Neutrophils (µl x10 3 ) Lymphocytes (µl x10 3 ) Monocytes (µl x10 3 ) Packed cell volume (%) Hemoglobin (g/dl) RBC (10 6 /µl) MCV (fl) RDW (%) MCHC (g/dl) PLT (µl x10 3 ) Relative Number Cell Volume (fl) 24
25 BIOCHEMICAL PROFILE INTERPRETATION- OVERVIEW Mary Anna Thrall, DVM, MS, Diplomate ACVP Colorado State University Fort Collins CO Introduction Laboratory tests are usually used to make a diagnosis, establish a prognosis, monitor response to therapy, or to establish a minimum database during health. Patient test results are compared to normal or reference values provided by the laboratory. For the reference value to be meaningful, similar test methods must have been used to establish the reference range as are used to test the patient. In addition, animals used to establish the reference range should usually be similar to the patient. For example, similarity in age may be important, as reference ranges for some parameters may markedly differ in different aged animals. To establish meaningful reference values, a laboratory must test numerous healthy animals, using the same instrumentation and reagents. If the sample size is less than 40, then it is usually best to eliminate obvious outliers and give the observed lowest and highest value for each parameter as the best estimate for the central 95% reference limits. When possible, tests should be validated by examining sick animals with and without the disease in question in order to establish test diagnostic sensitivity, diagnostic specificity, and predictive values. Diagnostic specificity and sensitivity may be high when comparing sick and healthy individuals, but are usually low when used to differentiate diseases with similar clinical signs. The veterinarian frequently faces the challenge of multiple diseases as presenting with overlapping test results. In general, more weight is placed on large increases and decreases in patient values compared to normal values. Biochemical profiles should be interpreted by developing pattern recognition, rather than evaluating each parameter and listing the causes that might increase or decrease each specific test. In other words, groups of tests should be evaluated together to determine if a diagnostic pattern is present. The results of groups of tests, taken together with other findings such as complete blood count and urinalysis results, history, and physical exam, can usually lead the clinician or laboratorian to a differential and sometimes definitive diagnosis. For example, the combination of low glucose, low BUN, low cholesterol, and low albumin suggests either end-stage liver disease, in which urea, cholesterol, glucose, and albumin are not being synthesized, or malassimilation, in which protein, glucose, and cholesterol and other lipids are not being absorbed. Glucose. Hyperglycemia is commonly seen as a result of catecholamine release (excitement, fear, exercise) or stress (endogenous or exogenous glucocorticoids) Glucose in cats may go as high as 350 mg/dl I response to excitement. Marked hyperglycemia (>200) in other species is almost always due to a lack of insulin or insulin resistance (diabetes mellitus), pancreatic islet amyloidosis (cats), recurrent pancreatic inflammation, etc. Phaeochromocytomas have rarely been reported to cause hyperglycemia. Hypoglycemia occurs when the body cannot make adequate amounts of glucose, glucose is transported into cells excessively, or if glucose if utilized too rapidly. The most common cause of low glucose is artifactual, and occurs when the serum is not removed from the clot and the RBCs continue to use glucose, which decreases approximately 10 mg/dl/hour. Common causes of non-artifactual hypoglycemia include puppy hypoglycemia in immature toy breed dogs with minimal gluconeogenic reserve, insulin-producing tumors of the pancreas in older dogs, excessive insulin therapy, starvation, end stage liver disease, large hepatomas, Addison s disease, and septicemia. Septicemia is a relatively common cause of hypoglycemia. Other less common causes of hypoglycemia are hunting dog hypoglycemia, glycogen storage diseases, and terminal pregnancy. Blood urea nitrogen (BUN). Although small quantities of urea are ingested, the majority is synthesized in the liver from ammonia. The ammonia is either formed from protein catabolism or absorbed from the large intestine. From the liver, urea enters the blood stream to be distributed to all intracellular and extracellular fluids, as it is a very small molecule ((MW=60). Almost all urea is ultimately excreted by the kidney, although negligible amounts are excreted in sweat and feces. Urea is freely filtered by the glomerulus. Consequently, diminished glomerular filtration results in increased BUN concentrations. Depending on the rate of urine flow, 25 to 75% of the filtered urea is passively reabsorbed with water in the proximal tubule. High rates of urine flow decrease tubular reabsorbtion of urea, while low rates of urine flow increase tubular reabsorption. Renal nephrons can concentrate urea up to 50-fold greater than plasma. One can readily understand how fluid therapy can thus markedly decrease BUN (by decreasing the amount of urea that is reabsorbed). The urea concentration in the blood is expressed in terms of BUN content. The molecular weight of urea is 60, including 2 N atoms with a MW of 28. Urea nitrogen can be converted to urea by multiplying by 60/28 which is For example, if BUN is 20 mg/dl, urea is
26 mg/dl (20 x 2.14). Factors influencing BUN concentration inlude the production/intake rate, body fluid balance, and the excretion rate. Production/intake rate. High protein diets and hemorrhage into the GI tract can cause mild increases in BUN (usually <45 mg/dl). The peak effect of protein or nitrogen absorption on BUN concentration occurs between 4.5 and 10 hours following hemorrhage or protein consumption. A BUN/Creatinine ratio of approximately 28 is usually observed in dogs with upper gastrointestinal hemorrhage. Rapid catabolism of body proteins and drugs that cause increased protein catabolism (corticosteroids, thyroid hormone) can also cause mild increases. Decreased production of urea due to severe liver disease or decreased protein intake (eg, starvation, malassimilation) will result in decreased BUN. Body fluid balance. Dehydration will cause BUN to be increased as a result of decreased enal perfusion and glomerular filtration, and excessive tubular reabsorption due to increased urine flow. Excretion rate. As glomerular filtration rate is reduced, BUN concentration increases proportionately. Approximately 75% of the nephrons must be nonfunctional before BUN concentration are increased out of the reference range. Azotemia, the term used to describe an increase in plasma conentration of non-protein nitrogen compounds, principally urea and creatinine, is classified as pre-renal, renal, and postrenal. Pre-renal azotemia is a result of diminished glomerular filtration rate (GFR) in the presence of otherwise normal renal function. Causes of decreased GFR include dehydration, shock, reduced blood volume, heart failure, etc. Although increased BUN in patients with massive GI hemorrhage is explained on the basis of increased absorption of amino acids following digestion of blood proteins, hypovolemia is probably the most important factor. Renal azotemia is a result of diminished glomerular filtration rate and urea retention from acute or chronic renal disease. Uremia is a clinical syndrome which occurs with protracted severe azotemia, and includes acidosis, nausea, vomiting, electrolyte imbalance, anemia, etc. The urine specific gravity is very helpful in differentiating pre-renal from renal azotemia. Concentrating ability of the kidney is impaired when approximately 66% of the nephrons are nonfunctional. Animals which are azotemic but still concentrating are azotemic as a result of pre-renal disorders. Animals which are dehydrated and azotemic and non-concentrating urine have renal azotemia. Exceptions to this rule are few, but include animals with mineralocorticoid deficiency (Addison s) in which renal medullary wash-out of sodium has occurred and concentration capacity is severely impaired, as well as other disorders which interfere with ADH function. In general, dogs which are dehydrated or azotemic and have normal kidney function should be concentrating maximally; the urine specific gravity should be at least > 1.025, and probably > Cats should concentrate into the circulation. Post-renal azotemia is a result of urinary tract obstruction or leakage so that urea is reabsorbed into the circulation. Creatinine. Decreased glomerular filtration from any cause, including decreased renal perfusion, affects creatinine similar to BUN. However, since creatinine is a larger molecule and is not reabsorbed by renal tubules, body fluid status has a lesser effect on creatinine than on BUN. Since almost all of the urine creatinine is filtered by the glomerulus and none is reabsorbed, endogenous creatinine clearance is commonly used as an index of dlomerular filtration rate. Because creatinine is independent of factors such as diet and urine flow rate, it is preferred over BUN by some clinicians. However, creatinine rises more slowly than BUN in renal disease, and decreases more slowly with diuresis or dialysis. BUN/creatinine ratios are popular in human medicine in establishing the etiology of azotemia. In dogs and cats, BUN/Cr ratios are not significantly different in pre-renal, renal, and post-renal azotemia. Perhaps because urine flow rate is normally low and urine is more concentrated in dogs and cats (compared to man), thus there is less alteration from normal in urine flow rates and urea reabsorption during pre and post-renal disorders. Calcium. Both ionized and bound calcium (total calcium) are routinely measured, although most laboratories are equipped to measure ionized calcium. Approximately ½ of the calcium is bound to albumin, while approximately ½ is the physiologically active ionized calcium. Ionized calcium increases with acidosis, and decreases with alkalosis. Hypocalcemia is usually corrected by taking into account the albumin concentration. The following formula is used: Adjusted serum calcium = Ca (mg/dl) albumin (g/dl) Hypercalcemia is associated with hypercalcemia of malignancy (pseudohyperparathyroidism), which is most caused by lymphoma and perirectal aprocrine gland adenocarcinoma in the dog, and fibrosarcoma in the cat. Other causes of hypercalcemia include certain granulomatous diseases (blastomycosis), primary hyperpharathyroidism, hypervitaminosis D (including cholecalciferol-containing rodenticide toxicosis), Addison s disease, renal failure (common in horses, rare in dogs and cats), and rarely, osteolytic bone lesions. High serum concentrations of calcium interferes with ADH receptors, so that animals with hypercalcemia lose their concentrating ability, and commonly present for polyuria/polydipsia. High calcium concentration also result in calcification of soft tissues, especially kidney and lung. A common diagnostic problem in animals that are hypercalcemic and azotemic is determining if the animal has primary renal failure with secondary hypercalcemia, or hypercalcemia which has resulted in renal failure. In small animals, the latter is much more common. 26
27 Hypocalcemia is associated with hypoparathyroidism (usually iatrogenic), renal failure (secondary renal hyperparathyroidism), ethylene glycol toxicosis, pancreatitis, secondary nutritional hyperparathyroidism (inadequate Ca intake, excess phosphorus intake, low Vitamin D intake), eclampsia, metaldehyde (snail bait) toxicosis, and hypercalcitonism (C-cell thryoid neoplasms). Prior to mathematically adjusting the calcium, hypocalcemia is most commonly associated with hypalbuminemia. If the sample is mistakenly collected in EDTA, calcium concentrations will be very low. Renal failure may result in hypocalcmia because of several mechanisms. The active form of vitamin D is metabolized by the kidney, so animals with renal failure do not absorb adequate amounts of dietary calcium. Usually calcium concentrations remain in the low normal range in animals with renal failure. Calcium also decreases in response to hyperphosphatemia. Approximately 50% of animals with ethylene glycol toxicosis are hypocalcemic because oxalic acid, a metabolite of ethylene glycol, binds calcium. Pancreatitis commonly results in mild hypocalcemia; this may be due to hyperglucagonemia or areas of fat necrosis binding calcium around the pancreas. Phosphorus. Hyperphosphatemia in adults in associated with decreased glomerular filtration (pre-renal, renal, post-renal) as phosphorus is normally eliminated through the kidney. When phosphorus and calcium are both high (as in renal failure due to hypercalcemia) the phosphorus x calcium product is calculated to predict the time of soft tissue mineralization. Serum phosphorus concentrations are normally high in young growing animals., exogenous phosphorus intake (such as phosphoruscontaining enemas), hypervitaminosis D, and hypoparathyroidism. Hypophosphatemia is seen in the early stages of primary hyperparathyroidism and hypercalcemia of malignancy and may therefore aid in differentiating these two causes of hypercalcemia from hypervitaminosis D. However, hypercalcemia in primary hyperparathyroidism and hypercalcemia of malignancy soon leads to calcification of the kidnesy and decreased glomerular filtration, which causes hyperphosphatemia. Other causes of hypophosphatemia include avitaminosis D, eclampsia, and lack of intake (starvation or malabsorption). Acid-base status effects phosphorus levels, in that with respiratory alkalosis, phosphorus moves into cells, resulting in an apparent hypophosphatemia. Mild hypophosphatemia is also seen in patiens with Cushing s disease. The most sever, to the point of being life-threatening, cause of hypophosphatemia is diabetes mellitus, in which phosphorus concentration may be < 1 mg/dl, thus affecting heart muscle function and neurologic status (causes seizures). In diabetic patients, intracellular phosphate moves into the extracellular fluid and is excreted in the urine. The osmotic diuresis associated with diabetes enhances this loss. Total Protein. Typically, total protein and albumin are measured, and the globulin is calculated to be the difference between albumin and total protein. The liver produces all of the albumin and many of the globulins, with the remaining globulins being produced by lymphocytes and plasma cells. The production of albumin is in part controlled by mechanisms regulating colloidal osmotic pressure, and is affected by alterations in globulin concentration. Abnormalities in serum proteins are usually not diagnostic of a specific disease, but rather are indicative of situations in which either protein intake, synthesis or catabolism has been altered, or protein loss is accelerated. Hypoproteinemiaa. Inadequate albumin intake may be a result of starvation, inadequate protein digestion or absorption, or severe intestinal parasitism. Inadequate albumin synthesis is a result of severe liver disease, such as cirrhosis, diffuse neoplasia, or vascular shunts (portocaval syndrome). Excessive protein loss may be due to protein-losing glomerulonephropathy (primarily albumin lost) protein losing enteropathy (albumin and globulin lost), hemorrhage, or massive exudative lesions. Young animals have lower total protein concentration than adults. Hyperproteinemia. Hyperproteinemia may be due to increased globulin concentrations. In such cases, serum should be submitted for protein electrophoresis to determine if the gammopathy is monoclonal or polyclonal. With monoclonal gammopathies, one specific type of immunoglobulin is increased due to a clonal expansion of a specific type of immunoglobulin-producing lymphocyte or plasma cell. With polyclonal gammopathies, multiple types of immunoglobulins are increased, as a result of immunoglobulin-producing cells undergoing antigenic stimulation. The only cause of hyperalbuminemia is dehydration or fluid shifts Bilirubin. Bilirubin is a metabolite of hemoglobin degradation by macrophages, which phagocytize aged and abnormal erythrocytes. Bilirubin is released from the macrophage and carried by albumin to the liver, where it is conjugated in the hepatocyte and secreted by the canalicular membrane into the bile. Hyperbilirubinemia occurs when there is accelerated destruction of erythrocytes, with hepatocellular disease, and when there is obstruction to bile flow (cholestasis). Determination of free and conjugated bilirubin is not particularly helpful in determining which of the above abnormalities is occurring. Packed cell volume, serum alkaline phosphatase activity, and other tests to evaluate the liver and the patency of bile flow are indicated. 27
28 Cholesterol. Hypercholesterolemia is seen in animals with hypothyroidism, diabetes mellitus, pancreatitis, cholestatic liver disease, Cushing s disease, glucocorticosteroid therapy, and the nephrotic syndrome with glomerulonephropathy. Diets high in cholesterol can also result in hypercholesterolemia. Hypocholesterolemia is seen in patients with severe, end-stage liver disease in which cholesterol can no longer by synthesized, and in disorders in which cholesterol intake is decreased, such as starvation, malabsorption, and maldigestion. Cholesterol is one of the precursors of bile acids. Serum bile acid concentration is a useful indicator of liver function as bile acids are made by the liver, excreted in the bile, reabsorbed by the ilium into the portal circulation, and removed effectively by the liver. Any disturbance of liver function results in bile acids escaping into the peripheral blood, increasing serum bile acid concentration. Serum bile acids are a more sensitive test of liver function than is bilirubin, as they will increase prior to the development of icterus. Bile acids are of no diagnostic usefulness in the icteric patient. SERUM ENZYME ACTIVITY. Increased activity of enzymes released into the serum is diagnostically useful if the enzyme or isoenzyme activity which is being measured is organ or tissue specific. Enzymes may be increased in the blood as a result of increased leakage from injured cells, or subsequent to increased production stimulated by cholestasis or drug administration. The most diagnostically useful and commonly included enzymes on small animal diagnostic panels are alkaline phosphatase, alanine aminotransferase (SGPT), amylase, and lipase. Alkaline phosphatase (ALP) is found in numerous tissues, but the activity seen in blood comes primarily from bonealkaline phosphatase and liver-alkaline phosphatase that increases in response to cholestasis. In the dog, two isoenzymes of ALP are liver-derived. One is induced by corticosteroids; the other by cholestasis. Increases in serum ALP activity as a result of induction of either of these isoenzymes can be marked. The steroid isoenzyme can be differentiated from the cholestasis isoenzyme by various laboratory methods, including electrophoresis, heat, and the addition of levamisole to the serum (in vitro). If Cushings s disease and steroid administration are eliminated as differential diagnoses, large increases in alkaline phosphatase are due to cholestasis. Marked increase in serum alkaline phosphatase activity in the cat is almost always due to cholestasis, frequently associated with hepatic lipidosis. Increases in serum bone-alp activity is seen in young growing animals; pathogenic increases in adults is rare and does not usually exceed a 4-fold increase. Alanine aminotransferase (ALT) is, for practical purposes, liver specific. (Skeletal muscle necrosis associated with X- linked muscular dystrophy in dogs has been reported to cause an increase in muscle-derived ALT; only very severe muscular necrosis has been associated with increased serum ALT activity. Creatine kinase (CPK or CK) activity can be measured to rule out muscle necrosis; severe muscle necrosis would cause a much greater increase in CK activity. Increased ALT activity is associated with hepatic cell injury in a multitude of disorders. ALT is also induced by various drugs, including corticosteroids and anti-convulsants. Aspartate aminotransferase (AST, formerly SGOT) is sometimes on small animal profiles. Since large animals do not have appreciable amounts of ALT, AST, while not liver specific, is diagnostically useful. It provides no additive diagnostic information over ALT in small animals. In animals with end-stage liver disease, ALT is usually normal or decreased, since inadequate viable hepatocytes remain to leak the enzyme into the blood. Amylase and Lipase. Increased serum activity (2 to 3x normal) is associated with acute pancreatitis. While many papers have been written on which is better, I have concluded that determining both is prudent, as one or the other is almost always increased at the time of clinical illness. Amylase and lipase are thought to be eliminated through the kidney; decreased glomerular filtration from any cause (pre-renal, renal, or post-renal) may result in an increase in serum activity of amylase and lipase. Other enzymes have been shown to be of more diagnostic usefulness (discussed elsewhere) but are not included on a biochemical profile. ELECTROLYTES Sodium, chloride, bicarbonate and potassium are routinely determined when performing a diagnostic biochemical profile. The major cations are sodium and potassium; the major anions are chloride and bicarbonate. Sodium (Na). Sodium is filtered by the glomerulus, and the majority is reabsorbed by the proximal and distal renal tubules. The distal tubular exchange of sodium and potassium is accelerated by aldosterone, promoting sodium retention and potassium excretion. Hyponatremia is seen in animals with renal disease, as the kidneys lose their ability to conserve sodium. Other causes of hyponatremia include Addison s disease, loss into third space such as uroperitoneum, congestive heart failure, diuretic adminstration, and GI losses (vomiting, diarrhea). Animals with diabetes mellitus may have a low serum sodium concentration, as hyperglycemia resulsts in an increase in serum osmolality with a shift of intracellular fluid to extracellular (ECF) fluid in an attempt to decrease extracellular fluid solute concentration by meq/l. Artifactual hyponatremia may be seen in lipemic blood samples if sodium is measured by a flame photometer, rather than an ion-specific 28
29 electrode. Sodium is restricted to the aqueous phase of serum, and if sodium is measured in both lipid and aqueous phases, sodium appears decreased. Hypernatremia is seen in conditions in which body water is loss in excess of salt (dehydration, inadequate water intake, and diabetes insipidus). Hypermatremia is seen in humans with Cushing s, but occurs very rarely in animals. Sodium and Acid/ase balance. The kidneys correct metabolic alkalosis by excreting the excess bicarbonate. However, bicarbonate can be excreted in urine only when accompanied by a cation (Na or K). Consequently, only when the quantity of Na in the ECF compartment is depleted can severe metabolic alkalosis develop. Paradoxical aciduria may occur in animals with metabolic alkalosis, in that in an attempt to conserve sodium, potassium and Hydrogen are secreted by renal tubules. Chloride. Hypochloremia occurs in animals with metabolic acidosis, prolonged vomiting and third space syndromes. Hyperchloremia is seen with dehydration. Potassium (K). Potassium is the major intracellular cation, with only 2% of the total body K being extracellular. Potasium is freely filtered by the glomerulus, then reabsorbed from the proximal tubules and secreted into the tubular fluid by distal tubular cells. Secretion is flow limited and aldosterone-dependent. Hyperkalemia is seen whenever decreased perfusion of the kidney results in oliguria or anuria, since K can no longer be secreted. Adrenal insufficiency (Addison s) commonly causes hyperkalemia and hyponatremia and hyponatremia. Diffuse cell necrosis or altered membrane permeability as a result of circulatory failure or crush-injury will result in potassium leakage and hyperkalemia. It can be difficult to distinguish renal failure (with hyperkalemia, azotemia, and an inability to concentrate) from Addison s disease, in which patients also have hyperkalemia, pre-renal azotemia and an inability to concentrate because of medullary wash-out of sodium. With acidosis. intracellular K is exchanged for extracellular H. If the kidneys are functioning, this will not usually result in hyperkalemia. Unlike man, horses, and some breeds of cattle, dog and cat erythrocytes do not contain more potassium than serum; thus hemolysis will not result in apparent hyperkalemia. The exception to this is the Akiita breed. Apparent hyperkalemia has also occurred in samples (which sat on the clot) from animals with leukemia or thrombocytosis, in which potassium leaked from these cells into the serum. Hypokalemia is associated with decreased intake, gastrointestinaql loss (vomiting, didarrhea), diuretics, and insulin therapy of diabetic animals, and chronic renal failure of cats. Total CO 2. Most of the total CO 2 is bicarbonate, and it is a crude estimate of the acid/base status (metabolic component). Increased bicarbonate indicates metabolic alkalosis; decreased bicarbonate indicates metabolic acidosis. Conversely, an increase in PCO 2 indicates respiratory acidosis, and a decrease indicates respiratory alkalosis. The lung responds to metabolic acidosis by blowing off CO 2. This measurement must be done with a blood-gas machine. Anion gap. The anion gap refers to the difference between the measured cations and meaasured anions. Since cations must equal anions, this difference, or gap, is not real, but rather represents those anions which are unmeasured. The normal gap is approximately 10 to 20 meq/l, which is somewhat species-dependent. For example, if the sodium = 150 meq/l and the potassium = 5 meq/l, and chloride = 120 meq/l and the bicarbonate = 16 meq/l, the anion gap is ( ) ( ) or = 19 meq/l. This is diagnostically useful information, as increased unmeasured anions occur in specific disorders, including ethylene gtlycol toxicosis (metabolites of EG are anions), diabetes mellitus (ketones), lactic acidosis, etc. Osmolality. Calculated osmolality (Cal Osm) is frequently given on the biochemical profile. The small molecular weight substances (sodium, potassium, glucose, and urea) determine the osmolality of serum. Osmolality can be calculated by the following formula: 1.86 [Na (meq/l) + K (MEq/L)] + glucose (mg/dl) + BUN (mg/dl) = Cal Osm (mosm/.kg). The difference between the calculated osmolality and the measured osmolality (by freezing point osmometer) is the osmole gap, which represents unmeasured substances contributing to osmolality. The only disorder which causes a large osmole gap in is ethylene glycol. toxicosis. The small molecular weight substance contributes greatly to the osmolality, and the serum concentration of ethylene glycol can be determined by calculating the osmole gap. 29


30 Making a Diagnosis in Patients with Serum Protein Abnormalities Mary Anna Thrall Typically, total protein and albumin are measured, and the globulin is calculated to be the difference between albumin and total protein. The liver produces albumin and many of the globulins, with the remaining globulins being produced by lymphocytes and plasma cells. The production of albumin is in part controlled by mechanisms regulating colloidal osmotic pressure, and is affected by alterations in globulin concentration. Abnormalities in serum proteins are usually not diagnostic of a specific disease, but rather are indicative of situations in which either protein intake, synthesis or catabolism has been altered, or protein loss is accelerated. Hypoproteinemia. Inadequate albumin intake may be a result of starvation, inadequate protein digestion or absorption, or severe intestinal parasitism. Inadequate albumin synthesis is a result of severe liver disease, such as cirrhosis, diffuse neoplasia, or vascular shunts (portocaval syndrome). Excessive protein loss may be due to protein-losing glomerulonephropathy (primarily albumin lost) protein losing enteropathy (albumin and globulin lost), hemorrhage, or massive exudative lesions. Young animals have lower total protein concentration than adults. Hyperproteinemia. Hyperproteinemia may be due to dehydration or increased globulin concentrations. If serum globulin is increased, serum should be submitted for protein electrophoresis to determine if the gammopathy is monoclonal or polyclonal. With monoclonal gammopathy, one specific type of immunoglobulin is increased due to a clonal expansion of a specific type of immunoglobulin-producing lymphocyte or plasma cell. With polyclonal gammopathy, multiple types of immunoglobulins are increased, as a result of immunoglobulin-producing cells undergoing antigenic stimulation. The only cause of hyperalbuminemia is dehydration or fluid shifts. Hypoalbuminemia with hypoglobulinemia: Concurrent hypoalbuminemia and hypoglobulinemia can result from overhydration (excessive fluid therapy), or from proportional loss of both protein fractions. The latter occurs with blood loss, protein-losing enteropathy, severe exudative skin disease, and body cavity effusions due to inflammation. In the latter two conditions, inflammation may cause an increase in globulin, even though they are being lost. Hypoalbuminemia with normal to increased globulin concentration: Decreased albumin concentration not accompanied by decreased globulin concentration can be caused by either decreased production, decreased intake, or increased loss of albumin. Decreased production of albumin may occur with liver failure. Globulins are commonly increased in animals with liver failure, presumably due to enteric-derived antigens in portal escaping removal by Kupffer cells in the liver. Decreased intake may occur with starvation, GI parasitism, intestinal malabsorption, and exocrine pancreatic insufficiency. Increased loss of albumin can occur with glomerular disease. Hypoglobulinemia with normal to increased albumin concentrations: These disorders are rare and are usually doue to either failure of passive tranfer of immunoglobulins, due to a neonate not ingesting colostrum, or due to an inherited or acquired immune deficiency. Polyclonal gammopathy: Polyclonal gammopathies can occur with chronic antigenic stimulation of any type, and are usually marked with canine ehrlichiosis and feline infectious peritonitis. (However, both of these disorders can also result in monoclonal gammopathies.) Monoclonal gammopathy. Hypoalbuminemia often accompanies monoclonal gammopathy. Causes of monoclonal gammopathies include multiple myeloma, extramedullary plasmacytomas (rarely), and lymphoma (approximatley 5% of cases). Non-neoplastic causes of monoclonal gammopathies are infrequent, and include canine ehrlichiosis, leishmaniasis, lymphoplasmacytic stomatitis, in cats, feline infectious peritonitis in cats, and a disorder called benign or idiopathic monoclonal gammopathy. However, cases of idiopathic monoclonal gammopathy are almost always finally diagnosed as multiple myeloma. Monoclonal gammopathy Albumin Globulin Polyclonal gammopathy 30
31 Multiple myeloma: Plasma cells are derived from B lymphocytes, and typically secrete immunoglobulins. Plasma cell myeloma is a relatively rare lymphoproliferative neoplasm in which plasma cells or their precursors proliferate abnormally. As implied by the term "multiple myeloma", plasma cells proliferate in the bone marrow at multiple sites. The incidence of multiple myeloma in cats is thought to be even lower than in dogs, and is usually not associated with FeLV or FIV infections. While these plasma cell proliferations may be detected by examination of marrow films, plasma cells are only rarely seen on blood films. When plasma cell leukemia is present, survival time is usually less. Markedly increased plasma cell concentration in the bone marrow (greater than 20 percent of all nucleated cells) is often due to plasma cell neoplasia; however, plasma cell proliferation may also occur secondary to chronic antigenic stimulation. Neoplastic plasma cells often are seen in large aggregates, and sometimes appear slightly abnormal or immature, with occasional multinucleated plasma cells present. However, they may appear very well differentiated, and are then difficult to distinguish from normal plasma cells. Plasma cells may occasionally have a ruffled eosinophilic cytoplasmic margin that appears similar to a flame. These are termed flaming plasma cells or flame cells. An important diagnostic and clinical manifestation of plasma cell myeloma is the presence of a monoclonal or biclonal gammopathy, usually IgG or IgA, but ocasionally IgM. The immunoglobulins synthesized by malignant plasma cells are also known as paraproteins. Other diagnostic features include the presence of Bence-Jones protein (light chains of immunoglobulins) in the urine and radiographic evidence of osteolysis. Two or three of these four features are traditionally considered essential to diagnose plasma cell myeloma. However, dogs with chronic ehrlichiosis may have a monoclonal gammopathy and markedly increased concentration of plasma cells in the bone marrow. Other disorders in which monoclonal gammopathies may be seen include chronic lymphocytic leukemia, lymphoma, feline infectious peritonitis, and extramedullary plasmacytoma. Clinical signs associated with multiple myeloma are usually associated with plasma cell infiltration of marrow and other organs, or with increased concentration of circulating immunoglobulins that may result in increased visocosity of the blood (hyperviscosity syndrome). Lethargy, anorexia, lameness, bleeding from the nares, paresis, polyuria, and polydipsia are relatively common. Fundoscopic changes such as retinal hemorrhages and engorged retinal blood vessels are commonly observed. Renal disease is relatively common, and is usually associated with the abnormal proteins interfering with tubular and glomerular function, but is sometimes secondary to hypercalcemia with subsequent calcification of renal tissue. Central nervous system impairment may result from serum hyperviscosity and subsequent sludging of blood in small vessels. Bleeding diatheses, seen in approximately onethird of dogs with multiple myeloma, may be due to thrombocytopenia, but can also result from the abnormal immunoglobulins interfering with platelet function. Skeletal lesions are rare in cats with multilple myeloma. Dogs with multiple myeloma that are treated with alkylating agents such as melphalan or cyclophosphamide often have survival times of one to two years. Reported survival time in treated cats is usually less. Animals with multiple myeloma that are azotemic or have severe anemia, neutropenia or thrombocytopenia usually have a poorer prognosis. Hypercalcemia, Bence-Jones proteinuria, and extensive bony lesions are also associated with a shorter survival time. In humans, treatment with thalidomide and stem cell transplantation offer improved survival rates. 31
32 Example of hypoproteinemia: Signalment: 5 years, FS, canine History: On phenobarbital to control seizures for 2 1/2 years. Vomiting daily and lethargic for one month. Physical Exam: Lethargic, icteric, pendulous abdomen; arthritic and appeared older than stated age CBC Reference Range Packed cell volume (%) Hemoglobin (g/dl) RBC (10 6 /µl) MCV (fl) MCHC (g/dl) Total nucleated cell count (x10 3 /µl) Segmented neutrophils (x10 3 /µl) Band neutrophils (x10 3 /µl) Monocytes (x10 3 /µl) Lymphocytes (x10 3 /µl) Eosinophils (x10 3 /µl) Platelets (x 10 3 / µl) Plasma protein (g/dl) Hemopathology: slt toxic neutrophils, many echinocytes PROFILE Glucose (mg/dl) Blood Urea Nitrogen (mg/dl) Creatinine (mg/dl) Calcium (mg/dl) Phosphorus (mg/dl) Total Protein (g/dl) Albumin (g/dl) Globulin (g/dl) Total Bilirubin (mg/dl) Cholesterol Alanine aminotransferase (IU/L) Aspartate aminotransferase (IU/L) Alkaline phosphatase (IU/L) Gamma glutamyl transferase (IU/L) Sodium (meq/l) Potassium (meq/l) Chloride (meq/l) Total CO 2 (meq/l) Anion Gap (meq/l) Lipase (IU/L) Urine Analysis Color orange-yellow Urine Sediment Transparency cloudy WBCs/hpf 8-10 Specific Gravity RBCs/hpf 0-2 Protein 2+ Epithelial cells/hpf Glucose neg Casts/lpf neg Bilirubin 4+ Crystals neg Blood 3+ Bacteria 4+ rods PH 6.0 Other ketones 3+ Coagulation Profile Prothrombin time (seconds) Activated partial thromboplastin time (seconds)
33 Example of hyperproteinemia Case Signalment: 10 year old, spayed female dog. History: Lethargy, weight loss, sneezing, dyspnea, and nasal discharge. Physical Examination: Pale mucous membranes, moderately enlarged lymph nodes, enlarged spleen. CBC Ref Range PCV (%) MCV (fl) WBC (x10 3 /µl) Segs (x10 3 /µl) Monos (x10 3 /µl) Lymphs (x10 3 /µl) Platelets(x10 3 / µl) Tot protein (g/dl) Hemopathology: Many well differentiated lymphocytes with abundant pale blue cytoplasm containing several azurophilic granules. PROFILE Ref range Glucose (mg/dl) BUN (mg/dl) Creatinine (mg/dl) Calcium (mg/dl) Phos (mg/dl) Tot Prot(g/dl) Albumin (g/dl) Globulin (g/dl) Tot Bili (mg/dl) Cholesterol (mg/dl) ALT (IU/L) AST (IU/L) ALP (IU/L) GGT (IU/L) Na (meq/l) K (meq/l) Cl(mEq/L) Total CO 2 (meq/l) Anion Gap(mEq/L) PROTEIN ELECTROPHORESIS Albumin α-1 Globulin α -2 Globulin β -1 Globulin β -2 Globulin γ Globulin Coagulation Profile Pro time (secs) APPT (seconds)
34 Bone marrow cytology Erythroid hypoplasia, lymphoid hyperplasia, and plasmacytosis. Alb Globulin 34
35 DIAGNOSTIC VALUE OF SERUM CALCIUM MA Thrall, DVM, MS, Dip ACVP Colorado State University Fort Collins CO Introduction Abnormal serum calcium concentration is a significant finding that usually aids in diagnosis. Approximately 50% of calcium is bound to plasma proteins (principally albumin), <10% is in mineral complexes with inorganic phosphates, and the remaining portion exists in the ionized form. Most automated chemistry analyzers determine the total concentration of calcium in the serum. Ionized calcium is typically ordered as a special test to be analyzed apart from the routine chemistry panel. Acid/base balance affects the proportion of ionized and bound calcium. During acidosis, protein-bound Ca is driven into solution, increasing ionized Ca concentration. Conversely, alkalosis decreases ionized Ca concentrations. These shifts have clinical importance, in that acidotic animals with hypocalcemia often don t show clinical signs, whereas alkalotic animals with the same serum calcium may be severely affected clinically. The most critical signs of imbalances in Ca metabolism relate predominantly to its role in synaptic neural signal transmission, skeletal muscle contraction, and cardiovascular muscle function. Another important aspect of calcium-protein interaction relates to the effects of changes in albumin concentration on total Ca concentration in the blood. Albumin concentration can markedly alter the apparent Ca concentration as reported in the standard diagnostic panel. The most common cause of apparent hypocalcemia is hypoalbuminemia. The fraction of Ca bound to albumin is decreased as the absolute amount of albumin available is decreased. In an attempt to correct total Ca concentration for albumin abnormalities, formulas have been derived for use in dogs: adjusted [Ca] (mg/dl) = total [Ca] (mg/dl) - [albumin] (g/dl) HYPOCALCEMIA Clinical signs in hypocalcemic animals depend on severity of decrease in ionized calcium. Mild decreases are associated with non-specific signs such as anorexia, nervousness, and a stiff gait. More severe decreases result in parathesias, hyperventilation, and generalized tetany or seizures (paresis in ruminants). When hypocalcemia is not due to hypoalbuminemia, and blood has not been mistakenly collected in EDTA, which markedly decreases plasma calcium concentration, several differential diagnoses should be considered. Causes of hypocalcemia may include renal disease (secondary renal hyperparathyroidism), ethylene glycol toxicosis, metaldehyde (snail bait) toxicosis, eclampsia, acute pancreatitis, hypoparathyroidism, nutritional secondary hyperparathyroidism (inadequate calcium intake, inadequate Vitamin D intake, excess phosphorus intake), intestinal malabsorption, phosphate-containing enemas, citrate toxicity (from multiple blood transfusions), hypomagnesemia, massive tissue degeneration (with release of phosphorus and precipitation of calcium), and hypercalcitonism (C-cell thyroid neoplasms). Renal Disease. While animals with chronic renal disease usually have calcium concentrations in the low-normal range, hypocalcemia may ultimately develop. Chronic renal disease may result not only in phosphorus (P) retention and reduced vitamin D hydroxylation, but also impaired tubular Ca reabsorption. Approximately 85% of glomerular filtration must be lost before persistent hyperphosphatemia develops. An increase in serum phosphorus concentration can result in a reciprocal decrease in serum calcium concentration, which leads to release of parathyroid hormone (PTH) from the parathyroid glands. Parathormone stimulates bone demineralization in order to increase blood calcium concentration. PTH also stimulates renal 1a-hydroxylation of vitamin D to produce the most active form of Vitamin D, calcitriol. Calcitriol promotes both intestinal absorption and distal renal tubular reabsorption of Ca by stimulating the synthesis of a calcium-binding protein which is important for epithelial cell uptake of Ca in the kidney and intestine. If renal disease is severe, activation of Vitamin D is impaired, resulting in diminished intestinal absorption and renal reabsorption of calcium. Ethylene glycol toxicosis. Approximately 30 to 50% of animals with late-stage ethylene glycol toxicosis are hypocalcemic. Oxalic acid, one of the metabolites of ethylene glycol, binds calcium, resulting in hypocalcemia and calcium oxalate crystal deposition in kidneys and urine. Pancreatitis. Hypocalcemia is sometimes seen with acute pancreatitis, probably as a result of lipase release into the peritoneal cavity, and saponification of hydrolyzed fats with calcium. 35
36 Hypoparathyroidism. The classic biochemical findings in animals with hypoparathyroidism are hypocalcemia (both ionized and total) and hyperphosphatemia. The primary differential diagnosis for this combination of electrolyte imbalances is renal failure; however, patients with renal failure are azotemic. Hypoparathyroidism can be confirmed by measuring PTH on serum following fasting. Nutritional secondary hyperparathyroidism. Hyperphosphatemia resulting from excessive dietary intake of phosphorus induces a secondary hypocalcemia and hypocalcitriolemia, which in turn stimulate PTH release. Ultimately, PTH induces bone demineralization to restore blood Ca levels, resulting in osteopenia and metabolic bone disease. Dietary calcium deficiency or vitamin D deficiency can induce a similar condition of secondary hyperparathyroidism, but without hyperphosphatemia. Hypomagnesemia. Hypomagnesemia results in impaired PTH release and calcitriol resistance leading to secondary hypocalcemia. Hypomagnesemia and hypocalcemia (ionized) associated with protein-losing enteropathy. While animals with protein-losing enteropathy may have hypocalcemia secondary to hypoalbuminemia, the hypocalcemia may be due to a decrease in the ionized form of calcium, with an accompanying hypomagnesemia. This may be due to intestinal loss, malabsorption, and/or abnormalities of vitamin D and parathyroid hormone metabolism. Electrolyte replacement may be required to avoid neurologic and metabolic problems. It is reported to be more common in Yorkshire terriers. (Kimmel SE, Waddel LS, Michel KE. Hypomagnesemia and hypocalcemia associated with protein-losing enteropathy in Yorkshire trriers:five cases ( ). J Am Vet Med Assoc 2000;217: Bush WW, Kimmel Se, Wosar MA et al. Secondary hypoparathyroidism attributed to hypomagnesemia in a dog with protein-losing enteropathy. J Am Vet Med Assoc 2001;219: ) In summary, hypocalcemia is often accompanied by hyperphosphatemia if there is nutritional or renal secondary hyperparathyroidism, ethylene glycol toxicosis, or primary hypoparathyroidism. Urinary FECa may be helpful in determining the cause of hypocalcemia. If the kidneys and the hormonal axis which regulates Ca reabsorption are functioning normally, calcium will be retained by the kidney in hypocalcemic patients. Increased FECa during hypocalcemia may indicate disturbances in either hormonal control or renal responsiveness to the disorder. Treatment of hypocalcemia is usually only necessary for patients with primary hypoparathyroidism, hypoparathyroidism secondary to thyroidectomy with accompanying parathyroid damage, eclampsia, or citrate toxicity. A 10% calcium salt ( gluconate or chloride) solution is administered to effect. Cardiac arrhythmias may occur; EKG monitoring is desirable. Calcium cannot be administered in bicarbonate-containing solutions, as mixing of the two can result in calcium carbonate precipitation. HYPERCALCEMIA The earliest clinical signs of hypercalcemia are polyuria and polydipsia, resulting from impaired response of distal renal tubules to antidiuretic hormone. Decreased excitability of neuromuscular tissue results in lethargy, muscle weakness, inappetence, and constipation. Severe hypercalcemia (>14 mg/dl) results in such a high calcium x phosphorus product that mineralization of renal tissue and subsequent acute renal failure occur. Mineralization of soft tissue occurs when the calcium x phosphorus product exceeds mg/dl. Hypercalcemia may be caused by a variety of disorders, including hypercalcemia of malignancy, granulomatous inflammatory disease (usually related to a systemic fungal infection such as blastomycosis), primary hyperparathyroidism, hypervitaminosis D, hypoadrenocorticism, and renal disease. Because hypercalcemia occasionally occurs secondary to renal disease, determining if the renal disease resulted in hypercalcemia, or if hypercalcemia lead to renal disease, is sometimes problematic. The latter is much more common. Hypercalcemia of malignancy (pseudohyperparathyroidism) has been reported with many tumor types, but is most often associated with lymphoma, perirectal apocrine gland adenocarcinoma, and more rarely, adenocarcinomas of various other tissues. Mechanisms vary, but are usually related to PTH-like peptide release from tumor tissue. Physical examination, in particular lymph node evaluation and rectal examination, should be performed to search for an underlying neoplastic process. Chest and abdominal radiographs, as well as a bone marrow aspirate, should be performed to detect lymphoma that is not apparent by external lymph node evaluation. Recently, two adult dogs were found to have hypercalcemia related to schistosomiasis and increased parathyroid hormone-related protein (PTHrP. North American schistosomiasis is caused by Heterobilharzia americana. Clinical findings may include dermatitis, coughing, diarrhea, and anorexia. Clinicopathological findings may include hypercalcemia, hyperglobulinemia, hypoalbuminemia, anemia, and eosinophilia. Diagnosis by fecal examination is difficult. Praziquantel or fenbendazole treatment may be curative or palliative. These are the first reported cases of hypercalcemia with elevated PTHrP in animals without diagnosed malignancy. Elevation of PTHrP has not been previously reported in hypercalcemic humans or in animals with granulomatous inflammation (J Am Anim Hosp Assoc (4): ).. 36
37 Primary hyperparathyroidism is quite rare compared to hypercalcemia of malignancy. PTH promotes increased urinary excretion of phosphorus by inhibiting its reabsorption in the renal proximal tubules. Thus, while patients are initially hyercalcemic and hypophosphatemic, once secondary renal mineralization and renal failure occur, animals become hyperphosphatemic. A tumor of the parathyroid may be detected on physical examination. Diagnosis is confirmed by serum PTH concentration. Incidence is higher in Keeshond breed. Vitamin D toxicosis has been observed in animals fed a diet inadvertently over-supplemented with vitamin D, and in animals that the owner overdosed with vitamin supplements. Also, some calcium /Vitamin D supplements, such as Viactin, are in the form of candy or candy bars that animals may eat accidentally. Consumption of certain wild plants that accumulate vitamin D-like substances has also resulted in intoxication (Cestrum dinurum: Solanum m., Trisetum spp.). Severe and acute vitamin D toxicity may result from consumption of rodenticides which contain cholecalciferol. Hyperphosphatemia occurs approximately 12 hours following ingestion of cholecalciferol-containing rodenticides; hypercalcemia occurs approximately 24 hours following ingestion. Death occurs due to mineralization of soft tissue, especially lungs and kidneys. Diagnosis is confirmed by increased serum cholecalciferol concentration. Some ointments (Calcipotriene, Devonex) used to treat psoriasis in people contain vitamin D analogs and have been reported to cause vitamin D toxicosis in the case of accidental ingestion by pets. The antidote that is most successful in treating vitamin D toxicosis in dogs is pamidronate (AJVR 2000;61:9-13) Hypoadrenocorticism. Mild to moderate hypercalcemia (<13 mg/dl) occurs in some patients with hypoadrenocorticism. While the hypercalcemia is sometimes associated with increased albumin concentrations due to dehydration, this is not always the case. The pathophysiology may be related to decreased glucocorticoids (glucocorticoids reduce GI calcium uptake), or calcium retention by the kidney, as related to sodium loss. Electrolyte abnormalities other than hypercalcemia, such as hyponatremia and hyperkalemia, are usually much more significant in these patients. Renal disease. A small number of dogs, probably less than 5%, become hypercalcemic secondary to renal disease. The mechanism is not completely understood, but may be related to sodium loss and calcium retention by the kidneys. Horses with renal disease develop hypercalcemia and hypophosphatemia in approximately 25-33% of the cases. Grape and Raisin Toxicosis Ingestion of a large quantity of grapes or raisins (0.5 to 1 oz/kg) have been reported to cause hypercalcemia ranging from mg/dl, hyperphosphatemia, azotemia, and oliguria and anuria. The pathogenesis is not yet understood, nor is it known if the acute renal faiure is secondary to the hypercalemia and mineralization of the kidneys, or if the kidney failure leads to the hypercalcemia. Clinical signs include vomiting, diarrhea, abdominal pain, and death associated with renal failure. (JAVMA 2001;219:434,436.) Idiopathic hypercalcemia in cats. The incidence of unexplained hypercalcemia (idiopathic) appears to be increasing in cats. This may be diet related (acidifying diets to decrease struvite formation). In any case these cats are normophosphatemic, hypercalcemic (total and ionized) and treatment with prednisone (12.5 mg/day) seems to reverse the hypercalcemia. Urolithiasis (calcium oxalate or struvite) is expected in 50-75% of the cats. (J Vet Intern Med 2000; 14: ) While treatment of hypercalcemia usually consists of treating the underlying problem, severe hypercalcemia in some situations should be considered a medical emergency, and diuresis to increase calcium excretion in the urine should be attempted by giving intravenous fluids (0.9% sodium chloride) and a diuretic such as furosemide. Salmon calcitonin to promote bone deposition, and glucocorticoids to reduce GI uptake, may be helpful. Once patients are oliguric or anuric, peritoneal dialysis to remove calcium may be helpful, but prognosis is poor. The antidote that is most successful in treating vitamin D toxicosis in dogs is pamidronate (AJVR 2000;61:9-13) 37
38 Case 36 Signalment: 2 year old male mixed breed dog History: Weight loss, lethargy; Physical Exam: Thin dog, pendulous abdomen Hematology Unremarkable Biochemical Profile Reference Range Glucose (mg/dl) 64 (3.5) ( mmol/l) BUN (mg/dl) 6 (2.1) 7-28 ( mmol/l) Creatinine (mg/dl) Calcium (mg/dl) 7.4 (1.85) ( mmol/l) Phosphorus (mg/dl) Total Protein (g/dl) Albumin (g/dl) Globulin (g/dl) Total Bili (mg/dl) Cholesterol (mg/dl) 65 (1.7) ( mmol/l) ALT (IU) ALP (IU) Bile Acids (µmol/l) Sodium (meq/l) Potassium (meq/l) Chloride (meq/l) Body Fluid Analysis Abdominal Fluid: Total Protein (g/dl) 1.0 Nucleated cell count (/µl) 1500 Segmented neutrophils (%) 60 Lmphocytes (%) 22 Macrophages (%) 18 Morphology: neutrophils non-degenerate 38
39 Case 25 Signalment: 3year old male cat History: acute lethargy, vomiting, and anorexia. Physical examination: Obese, almost comatose Hematology Reference Range Packed cell volume (%) Total white blood cell count(x10 3 /µl) Segmented neutrophils(x10 3 /µl) Monocytes(x10 3 /µl) Lymphocytes(x10 3 /µl) Platelets (x 103/ µl) adequate Biochemical Profile Glucose (mg/dl) Blood Urea Nitrogen (mg/dl) Creatinine (mg/dl) Calcium (mg/dl) Phosphorus (mg/dl) Total Protein (g/dl) Albumin (g/dl) Globulin (g/dl) Total Bilirubin (mg/dl) Alanine aminotransferase (IU) Alkaline phosphatase (IU) Sodium (meq/l) Potassium (meq/l) Chloride (meq/l) Total CO 2 (meq/l) Anion Gap (meq/l) Calculated osmolality (mosm/kg) Measured Osmolality (mosm/kg) Osmolal Gap (mosm/kg) 46 <10 Urinalysis (cystocentesis) Color Yellow Urine Sediment Transparency Cloudy WBCs/hpf 2-3 Specific Gravity RBCs/hpf 2-3 Protein 1+ Epithelial cells/hpf 1-3 transitional Glucose 1+ Casts/lpf 0 Bilirubin Negative Crystals Calcium oxalate (monohydrate) Blood 1+ Bacteria 0 ph
40 Case 01 Signalment: Six year old male castrated male Fox terrier. History: Intermittent vomiting and diarrhea for past seven weeks, seizured for a few minutes a few hours before presentation on 8/8. Physical Examination: Lethargic, weak, "bloated" Hematology 8/8 8/17 Reference Range Packed cell volume (%) Hgb (g/dl) RBC (10 6 /µl) MCV (fl) MCHC (g/dl) Total nucleated cell count (x10 3 /µl) Segmented neutrophils (x10 3 /µl) 14.4 (83 %) Band neutrophils (x10 3 /µl) 0.3 (2%) Monocytes (x10 3 /µl) 0.3 (2%) Lymphocytes (x10 3 /µl) 1.9 (11%) Eosinophils(x10 3 /µl) Platelets (x 10 3 / µl) Plasma protein (g/dl) Reticulocytes (x10 3 ) 80,000 (2.1%) 209,450 (7.1%) 0-60,000 Hemopathology: slight polychromasia, slt toxic neuts Biochemical Profile sl hemolyzed Glucose (mg/dl) Blood Urea Nitrogen (mg/dl) Creatinine (mg/dl) Calcium (mg/dl) Phosphorus (mg/dl) Magnesium (mg/dl) Total Protein (g/dl) Albumin (g/dl) Globulin (g/dl) Total Bilirubin (mg/dl) Cholesterol (mg/dl) Alanine aminotransferase (IU/L) Aspartate aminotransferase (IU/L) Alkaline phosphatase (IU/L) Creatine kinase (IU/L) GGT (IU/L) Sodium (meq/l) Potassium (meq/l) Chloride (meq/l) Bicarbonate (meq/l) Anion Gap (meq/l) Calc. osmolality (mosm/l) Iron TIBC Sat percent UIBC <10 13 Ioniized calcium was done on the istat in ccu three times (dates not known) The results were.96,.80, and Coagulation Protime (sec) APTT (sec) Antithrombin 45% and 59% of NHP 40
41 Case 24 Signalment: 6 month old DSH female cat History: Vomiting, weakness, acute onset. Physical exam: tachypnea for 24 hours, weakness Hematology Reference Range PCV (%) WBC (µl) Segs (µl) Bands (µl) Lymphs (µl) Monos (µl) Biochemical Profile Glucose (mg/dl) 150 (8.2) ( mmol/L) BUN (mg/dl) 45 (16.1) ( mmol/l) Creatinine (mg/dl) 2.2 ( ( µmol/l) Calcium (mg/dl) 18 (4.5) ( mmol/l) Phosphorus (mg/dl) 9.5 (3.1) ( mmol/l) Total Protein (g/dl) Albumin (g/dl) Globulin (g/dl) Total Bilirubin (mg/dl) Cholesterol ALT (IU) Alk Phos (IU) Sodium (meq/l) Potassium (meq/l) Chloride (meq/l) Total CO 2 (meq/l) Blood Gas Data (arterial) ph PCO2 (mmhg) PO2 (mmhg) HCO3 (meq/l) Urinalysis Specific gravity Gran casts/hpf 2 41
42 Case 22 Signalment: 8 years, M, canine History: polydipsia Physical: slightly dehydrated Hematology Reference Range Packed cell volume (%) Hemoglobin (g/dl) RBC (10 6 /µl) MCV (fl) Total nucleated cell count (x103/µl) Segmented neutrophils (x103/µl) Monocytes (x103/µl) Lymphocytes (x103/µl) Platelets (x 103/ µl) Plasma protein (g/dl) Hemopathology: clumped platelets Biochemical Profile Glucose (mg/dl) Blood Urea Nitrogen (mg/dl) 33 (11.8) 7-28 ( mmol/l) Creatinine (mg/dl) 2.9 (256) ( µmol/l) Calcium (mg/dl) 15.4 (3.85) ( mmol/l) Phosphorus (mg/dl) 7.1 (2.3) ( mmol/l) Total Protein (g/dl) Albumin (g/dl) Globulin (g/dl) Total Bilirubin (mg/dl) 1.0 (17) (0-6.8 µmol/l) Cholesterol Alanine aminotransferase (IU/L) Aspartate aminotransferase (IU/L) Alkaline phosphatase (IU/L) Gamma glutamyl transferase (IU/L) Sodium (meq/l) Potassium (meq/l) Chloride (meq/l) Total CO 2 (meq/l) Anion Gap (meq/l) Urinalysis Color straw Urine Sediment Transparency clear WBCs/hpf 2-3 Specific Gravity RBCs/hpf 1-2 Protein 2+ Epithelial cells/hpf neg Glucose neg Casts/lpf neg Bilirubin 2+ Crystals neg Blood neg Bacteria neg ph 6.5 Other UPC 2.6 Fractional excretion Na (%) 1.73 <1.0 Ca (%)
43 Case 23 Signalment: 9 yr old female dog History: polydipsia, polyuria Physical exam: mass in pelvic inlet Biochemical Profile Reference Range Glucose (mg/dl) Blood Urea Nitrogen (mg/dl) ( Creatinine (mg/dl) Total Protein (g/dl) Albumin (g/dl) Calcium (mg/dl) 16.4 (4.5) ( mmol/l) Phosphorus (mg/dl) Total Bilirubin (mg/dl) Alanine aminotransferase (IU) Alkaline phosphatase (IU) Sodium (meq/l) Potassium (meq/l) Chloride (meq/l) Total CO 2 (meq/l) Urinalysis Urine specific gravity
44 Case 57 Signalment: 6 years, M, canine History: lethargic, quit eating Physical: depressed, weak pulse, apparent weakness Hematology Reference Range Packed cell volume (%) Hemoglobin (g/dl) RBC (10 6 /µl) MCV (fl) MCHC (g/dl) Total nucleated cell count (x103/µl) Segmented neutrophils (x103/µl) Monocytes (x103/µl) Lymphocytes (x103/µl) Eosinophils (x103/µl) Platelets (x 103/ µl) Plasma protein (g/dl) Hemopathology: few acanthocytes, few echinocytes, few schistocytes/fragments Biochemical Profile Glucose (mg/dl) Blood Urea Nitrogen (mg/dl) 95 (33.9) 7-28 ( mmol/l) Creatinine (mg/dl) 3.8 (334) ( µmol/l) Calcium (mg/dl) 14.3 (3.57) ( mmol/l) Phosphorus (mg/dl) 9.9 (3.2) ( mmol/l) Total Protein (g/dl) Albumin (g/dl) Globulin (g/dl) Total Bilirubin (mg/dl) Cholesterol Alanine aminotransferase (IU/L) Aspartate aminotransferase (IU/L) Alkaline phosphatase (IU/L) Gamma glutamyl transferase (IU/L) Sodium (meq/l) Potassium (meq/l) Chloride (meq/l) Total CO 2 (meq/l) Anion Gap (meq/l) Amylase (IU/L) Lipase (IU/L) Blood Gas Data (arterial) ph PO2 (mmhg) PCO2 (mmhg) HCO3 (meq/l) ionized Ca++ (mg/dl) Urine Analysis Color yellow Urine Sediment Transparency cloudy WBCs/hpf 1-4 Specific Gravity RBCs/hpf 1-2 Protein neg Epithelial cells/hpf 1-2 Glucose neg Casts/lpf neg Bilirubin trace Crystals neg Blood neg Bacteria neg ph 6.0 Other UPC
45 Making a Diagnosis in Patients with Serum Glucose Abnormalities Mary Anna Thrall Glucose in blood is derived from food and is also produced by the liver through gluconeogenesis and glycogenolysis. Gluconeogenesis is glucose formation from non-carbohydrate sources, primarily amino acids (from protein) and glycerol (from fat. Glycogenolysis is the hydrolysis of hepatocyte glycogen to glucose. Blood glucose concentrations vary, depending on time since the last meal, hormonal influences, and use of glucose by peripheral tissues such as skeletal muscle. Hormones affect blood glucose concentration by regulating hepatic production and controlling peripheral utilization of glucose. Insulin is secreted by pancreatic islet B cells. Insulin lowers blood glucose concentrations by promoting glucose uptake by liver, skeletal muscle and fat, inhibiting gluconeogenesis in the liver, and promoting liver glycogen formation and storage. Glucocorticoids increase blood glucose concentrations by promoting hepatic gluconeogenesis, and by inhibiting cellular insulin receptor affinity and insulin action on glucose metabolism, thus decreasing peripheral utilization of glucose and increasing hepatic synthesis of glucose. Glucagon is secreted by pancreatic islet alpha cells. Glucagon increases blood glucose concentrations by stimulating hepatic gluconeogenesis and hepatic glycogenolysis, and inhibiting cellular insulin receptor affinity. Catecholamines (epinephrine and norepinephrine) increase blood glucose concentrations by increasing hepatic glycogenolysis, inhibiting insulin secretion, and stimulating glucagon secretion. Growth hormone increases blood glucose concentrations by inhibiting insulin-mediated uptake of glucose by hepatocytes, muscle cells and adipose cells, and increasing hepatic glucose production. Extreme physical activity may result in decreased blood glucose concentration due to increased usage of glucose by skeletal muscle. In normal animals, however, blood glucose concentrations are stable during most types of physical activity. Hypoglycemia: Hypoglycemia occurs when the body cannot make adequate amounts of glucose, glucose is transported into cells excessively, or if glucose if utilized too rapidly. The most common cause of low serum glucose is artifactual, and occurs when the serum is not removed from the clot and the erythrocytes continue to use glucose, which decreases approximately 10 mg/dl/hour. Serum or plasma to be analyzed for blood glucose concentration should be separated from erythrocytes within 30 minutes. Sodium fluoride anticoagulant inhibits glycolysis and should be used if serum or plasma cannot be separated from cells within 30 minutes. Common causes of non-artifactual hypoglycemia include puppy hypoglycemia in immature toy breed dogs with minimal gluconeogenic reserve, insulin-producing tumors of the pancreas, excessive insulin therapy, starvation, end stage liver disease, large hepatomas, Addison s disease, and septicemia. Septicemia is a relatively common cause of hypoglycemia. Other less common causes of hypoglycemia are hunting dog hypoglycemia, glycogen storage diseases, and terminal pregnancy. Increased insulin production or therapeutic insulin overdose: Neoplasms of the β cells of the pancreatic islets (β cell tumors, insulinomas) are the most common source of increased insulin production. Insulinoma has been reported in dogs, cats and ferrets. Therapeutic insulin overdose can occur when treating diabetes mellitus. Increased insulin concentration decreases gluconeogenesis and glycogenolysis and increases cellular utilization of glucose. Hypoadrenocorticism: Hypoglycemia occurs inconsistently in dogs with hypoadrenocorticism, and many dogs with this syndrome have normal blood glucose concentrations. Hypoglycemia, when present, is usually mild and probably results from decreased gluconeogenesis and increased insulin-mediated uptake of glucose by muscle tissue. Liver failure: Liver failure results in decreased hepatic gluconeogenesis and glycogenolysis. Hypoglycemia occurs only after loss of more than 70% of functional capacity. Extreme exertion. This occurs in hunting dogs and endurance horses. Possible underlying causes include depletion of glycogen stores, increased glucose utilization, and decreased epinephrine response to hypoglycemia. Sepsis. Hypoglycemia occurs inconsistently with sepsis. Hyperglycemia is more common in animals with early sepsis while hypoglycemic is more common in animals with advanced and/or later sepsis. The causes of hypoglycemia in association with sepsis are not completely understood. Possible causes include impaired gluconeogenesis and glycogenolysis and increased utilization of glucose by tissues including leukocytes. 45
46 Glycogen storage diseases. These diseases are inherited defects in glycogenolysis and result in accumulation of glycogen in cells of the liver, kidney and myocardium. Type I (von Gierke s disease) and type II (Pompe s disease) glycogen storage diseases are associated with hypoglycemia in dogs. Juvenile hypoglycemia in toy and miniature dog breeds (puppy hypoglycemia): This syndrome is usually seen in puppies < 6 months old. Clinical signs are often triggered by stresses such as diarrhea, fasting and/or parasitism. Inadequate storage pools of glycogen and protein probably play an important role in this syndrome. Inadequate hepatic enzymes for gluconeogenesis may also contribute. Neoplasia other than insulinoma. Hypoglycemia has been reported in association with numerous types of tumors. Possible causes of hypoglycemia in association with such neoplasms include excessive glucose utilization by the tumor and secretion of insulin-like substances by the tumor. Secretion of an insulin-like molecule, insulin-like growth factor, is involved in the pathogenesis of hypoglycemia associated with some types of tumors. Hyperglycemia: Hyperglycemia is commonly seen as a result of catecholamine release (excitement, fear, exercise) or stress (endogenous or exogenous glucocorticoids) Glucose in cats may go as high as 400 mg/dl in response to excitement. Marked hyperglycemia (>200) in other species is almost always due to a lack of insulin (diabetes mellitus), pancreatic islet amyloidosis (cats), recurrent pancreatic inflammation, etc. Phaeochromocytomas have rarely been reported to cause hyperglycemia. Ethylene glycol toxicosis causes mild to marked hyperglycemia in approximately 50% of affected animals and is attributed to inhibition of glucose metabolism by aldehydes, increased epinephrine and endogenous corticosteroids, and uremia. Dogs and cats should be fasted for 12 hours prior to sampling to avoid postprandial hyperglycemia. (However, potentially hypoglycemic animals should not be fasted prior to sampling since severe hypoglycemia may result.) Diabetes mellitus. Diabetes mellitus is caused by a deficiency of insulin production or interference with the action of insulin in target tissues, resulting in abnormal glucose metabolism. Altered protein and lipid metabolism also occurs in diabetes mellitus. Animals with diabetes mellitus usually have blood glucose concentrations above the renal threshold and, therefore, glucosuria. Diabetes mellitus has been classified by its underlying causes as Type 1 and Type 2 and by the dependence of the affected animal on insulin therapy as insulin dependent and non-insulin dependent. These two classification schemes overlap, resulting in confusion as to the types of diabetes mellitus occurring in animals. Type 1 diabetes mellitus results from immune-mediated destruction of pancreatic beta cells by cellular and humoral mechanisms. Animals with type 1 diabetes mellitus are insulin dependent. Type 1 diabetes is the most frequent cause of diabetes in dogs, but has not been welldocumented in cats. Pancreatitis is thought to be a major predisposing factor to diabetes mellitus in dogs. Islet injury secondary to pancreatic inflammation and resultant decreased insulin production is the most likely pathogenesis. Type 2 diabetes mellitus results from impaired beta cell function as a result of causes other than immune-mediated beta cell destruction. Animals with type 2 diabetes mellitus may be either insulin dependent or non-insulin dependent. This is the most common type of diabetes mellitus in cats but can also occur in dogs. Approximately 50% to 70% of cats with type 2 diabetes mellitus are insulin dependent. A sluggish insulin response to hyperglycemia (decreased capacity to produce insulin) and a poor tissue response to insulin (insulin resistance) are the underlying features of type 2 of diabetes mellitus. Deposition of amyloid in the pancreatic islets is found in most cats with type 2 diabetes mellitus. Obesity is considered a major risk factor for diabetes mellitus in cats. Obesity-associated glucose intolerance and insulin resistance which has not yet become clinical diabetes mellitus probably occurs in all species and, given the incidence of obesity, may be more common than clinical diabetes mellitus. Increased blood glucocorticoid concentration is the most common cause of hyperglycemia. Increased blood glucocorticoid concentrations can result from glucocorticoid treatment or from increased endogenous glucocorticoid production secondary to stress or hyperadrenocorticism. Hyperglycemia commonly occurs in cats, but only rarely in dogs, receiving long-term anti-inflammatory doses of steroids. Blood glucose concentrations are usually below the renal threshold, but higher concentrations can occur. Prolonged increases in blood glucocorticoid concentrations result in impaired insulin secretion by β cells and insulin resistance due to receptor or post-receptor defects. This can lead to β cell exhaustion atrophy and result in insulin dependent diabetes mellitus. 46
47 Increased blood catecholamine concentrations. Catecholamines are released as a result of exertion, fear or pain. Increased catecholamine production also occurs with certain tumors of the adrenal gland (pheochromocytomas). Increased growth hormone. Insulin resistant diabetes mellitus has been reported in a dog and a cat with growth hormone producing acidophilic pituitary adenomas which produce excess growth hormone. The insulin resistance resulting from excessive growth hormone in the dog might have led to alterations in β cells of the islets of Langerhans and subsequent diabetes mellitus. Glucagon-producing tumors. Glucagon-producing tumors in the pancreas have been reported in two dogs that were hyperglycemic. These dogs had blood glucose concentrations >300 mg/dl but were not ketoacidotic. Increased progesterone production. Progesterone stimulates secretion of growth hormone, which can result in hyperglycemia. Increased progesterone concentration and hyperglycemia can occur during diestrus in bitches. Increased serum progesterone concentrations during pregnancy can cause a pre-clinically diabetic bitch to become overtly diabetic. In bitches that are known to be diabetic, increased serum progesterone concentrations during pregnancy can cause difficulty with therapeutic regulation of blood glucose concentration. Drugs. A variety of drugs can cause hyperglycemia. These include glucocorticoids, adrenocorticotrophic hormone (ACTH), megestrol acetate in cats, ketamine in cats, and fluids containing glucose. Additional Laboratory tests: Urine glucose analysis: Glucosuria occurs when blood glucose concentrations exceed the renal threshold for that species. Renal thresholds of various species are 180 to 220 mg/dl in the dog and cat. Decreased renal thresholds are usually the result of proximal tubular abnormalities. These abnormalities include primary renal glycosuria of Norwegian Elkhounds, Fanconi syndrome, amyloidosis in dogs (nearly 20% have glucosuria), and exposure to nephrotoxins including aminoglycosides, ethylene glycol, and amphoterocin B. Animals with hypercalcemia and resulting proximal tubular damage may also have glucosuria resulting from a decreased renal threshhold. The intravenous glucose tolerance test is useful in detecting decreased glucose tolerance in persistently hyperglycemic animal. This test can also be used in detecting increased glucose tolerance in animals with persistently low normal glucose concentrations. Measurement of concurrent serum insulin and glucose concentrations is preferred to performing the intravenous glucose tolerance test in persistently hypoglycemic animals (see discussion of serum insulin in hypoglycemic animals below). Chemical restraining agents (e.g. ketamine, xylazine, thiopental, acetylpromazine, morphine) should be avoided when performing glucose tolerance tests since these tend to delay the disappearance of glucose (i.e. cause decreased glucose tolerance). Fast for 12 to 24 hours. Do not fast hypoglycemic animals. Blood glucose concentrations of potentially hypoglycemic dogs should be monitored during this period, and the fasting period ended if hypoglycemia is detected. Administer 0.5 g glucose (50% solution) /kg IV over a 30 second period. Collect blood samples for glucose analysis prior to administration and at 5, 15, 25, 35, 45, and 60 minutes after administration. Plot glucose concentrations on log scale vs. time on arithmetic scale. Calculate time for blood glucose to decrease by 50% (T 1/2 ). The IV glucose tolerance test can be used in combination with insulin assays to classify diabetes mellitus as insulin dependent or non-insulin dependent. Serum insulin assay: Measurement of serum insulin concentration is useful in evaluating both hyperglycemic and hypoglycemic disorders. Serum insulin concentrations are most diagnostically useful when compared to serum glucose concentrations. Serum for insulin assay should be harvested from clotted blood within 30 minutes and immediately assayed or frozen.. If the animal being tested is sporadically hypoglycemic, serum insulin measurements should be done while the animal is hypoglycemic. A protocol for performing this comparison in hypoglycemic dogs is as follows: Withhold food early on the morning of the test day (7 to 8 AM). Monitor blood glucose concentrations on an hourly basis until the concentration is <60 mg/dl. In dogs with insulinomas, life-threatening hypoglycemia can develop during the fasting period, and careful monitoring is imperative. Most dogs with insulin-secreting tumors develop hypoglycemia 8 to 10 hours after a meal, but more than 24 hours of fasting is required in some dogs. An insulin-secreting tumor is not likely if a glucose concentration <60 mg/dl is not induced by this process. When the blood glucose concentration is <60 mg/dl, obtain a serum sample for blood glucose and insulin analysis. After obtaining these samples, feed the dog several small meals before returning it to its previous feeding schedule. In normal dogs, the serum insulin concentration should decrease as the blood 47
48 glucose concentration decreases. In normal fasted dogs, blood glucose concentrations are typically 70 to 100 mg/dl, and serum insulin concentrations are typically 5 to 20 µu/ml. In fasted dogs with insulinomas, serum insulin concentrations will not decrease as glucose concentrations decrease. If the blood glucose concentration is <60 mg/dl, and the serum insulin concentration is increased, an insulin-secreting tumor is likely. If the blood glucose concentration is <60 mg/dl, and the serum insulin concentration is in the middle to upper reference interval, an insulin-secreting tumor is a possibility. This occurs in about 25% of dogs with insulinomas. If the blood glucose concentration is <60 mg/dl, and the serum insulin concentration is decreased, an insulin-secreting tumor is unlikely. Serum insulin in hyperglycemic animals: Concurrent measurement of serum insulin and blood glucose concentrations during an intravenous glucose tolerance test can be used to confirm abnormalities in insulin secretion. The test is performed by administering glucose intravenously at the dosage recommend in the previous discussion of the intravenous glucose tolerance test. Serum insulin concentrations are measured on samples obtained prior to and at 5, 15, 30, 60 and 120 minutes after administration of glucose. These measurements may aid in characterizing diabetes mellitus as insulin dependent or noninsulin dependent. Application of this test in evaluation of diabetics is limited, since almost all non-obese dogs have insulin dependent diabetes mellitus, and insulin secretion in cats with non-insulin dependent diabetes mellitus is unpredictable. In normal dogs, serum insulin concentration increases 5 to 10 fold at 5 minutes and returns to baseline by 60 minutes after intravenous glucose administration. In normal cats, serum insulin concentration increases 2 to 3 fold by 5 to 15 minutes and returns to near the baseline concentration at 120 minutes after intravenous glucose administration. Very low baseline serum insulin concentration with little or no increased in serum insulin concentration in response to intravenous glucose administration is suggestive of insulin dependent diabetes mellitus. Normal to increased baseline serum insulin concentration with a response to intravenous glucose injection that varies from none to normal to delayed (e.g. below normal increase in insulin concentration during first hour but normal to exaggerated increase in serum insulin concentration by two hours after glucose injection) is suggestive of non-insulin dependent diabetes mellitus. Fructosamine is a general term referring to any glycated protein (a protein with an attached carbohydrate). Glucose combines with the amine groups of albumin and other proteins in the blood and, through a series of chemical reactions, this results in the formation of stable compounds called fructosamines. Fructosamine is formed in normal animals, but high blood glucose concentrations result in formation of increased amounts. Serum or plasma fructosamine concentration is an indicator of blood glucose concentrations during the previous 2 to 3 weeks (based on average life-span of proteins involved in this complex). Fructosamine provides more reliable information about the long-term state of glucose metabolism than does blood glucose concentration which only reveals a momentary situation. Fructosamine, therefore, has potential in diagnosis of diabetes mellitus and in monitoring the therapy of diabetics. Increased fructosamine concentrations suggest increased blood glucose concentrations and, in diabetic animals being receiving insulin treatment, a lack of therapeutic control of blood glucose concentrations during the previous 2 to 3 weeks. Albumin is the most frequent protein incorporated into the fructosamine molecule. Hypoalbuminemia can, therefore, result in falsely decreased fructosamine concentrations. Fructosamine is also useful in distinguishing excitement-induced hyperglycemia from diabetic hyperglycemia in cats. Fructosamine concentrations are within reference ranges in cats with hyperglycemia caused by excitement since this is a short-term change, and animals must be hyperglycemic for approximately four days before increased fructosamine concentrations are detected. Fructosamine concentrations tend to be increased in diabetic cats since this hyperglycemia persists for a long time period (specificity = 86% and sensitivity = 93%). Serum or plasma (heparin or EDTA but not Na fluoride) can be assayed. Fructosamine is stable at refrigerator temperatures for up to 2 weeks and frozen for up to 2 months. Lipemia does not interfere with this assay, but more than slight hemolysis will interfere. Glycated hemoglobin (GHb) is formed in erythrocytes as a result of an irreversible reaction between carbohydrates (especially glucose) and hemoglobin. Blood GHb concentration reflects glucose status over a longer time period than does serum fructosamine concentration because erythrocytes have longer life-spans than do protein molecules. Glycated hemoglobin can be used in the same situations as fructosamine. The shorter time period gauged by fructosamine as compared to GHb might be an advantage since it allows earlier recognition of deteriorating control of hyperglycemia and of return to adequate control of hyperglycemia. 48
49 LABORATORY EVALUATION OF LIVER DISEASE OVERVIEW AND CASE DISCUSSION Mary Anna Thrall, D.V.M., MS Diplomate, ACVP College of Veterinary Medicine and Biomedical Sciences Colorado State University Fort Collins, CO Biochemical profiles can usually determine if liver disease (cholestasis or hepatocyte injury), and/or liver failure are present, although laboratory evaluation of the liver may not provide a specific diagnosis. Liver disease may be caused by a number of processes which result in hepatocyte injury and/or cholestasis, such as hypoxia, metabolic disorders, toxicosis, inflammation, neoplasia, trauma, and intra- or extrahepatic biliary stasis. Liver failure may result from various types of liver disease, and is recognized by failure to clear the blood of substances normally eliminated by the liver and failure to synthesize substances normally produced by the liver. Approximately 75% of functional liver must be lost before biochemical evidence of liver failure is seen. Tests to detect liver disease and failure include serum enzyme assays which detect hepatocyte injury, serum enzyme assays which detect cholestasis, and tests which evaluate liver function. ENZYME ASSAYS WHICH DETECT HEPATOCYTE INJURY Increased serum enzyme activities can result from either leakage from damaged cells (leakage enzymes), or increased production of an enzyme (induction enzymes). Hepatocyte injury is detected by measuring serum activities of enzymes which have leaked from hepatocytes. The leakage enzymes evaluated most commonly in dogs and cats are alanine aminotransferase (ALT), the enzyme formerly known as serum glutamic pyruvic transaminase (SGPT), and aspartate aminotransferase (AST), the enzyme formerly known as serum glutamic oxaloacetic transaminase (SGOT). Other leakage enzymes that are less commonly assayed are sorbitol dehydrogenase (SDH) and glutamate dehydrogenase (GLDH). Alanine aminotransferase is quite liver specific, although serum activities may increase in dogs and cats with severe muscle damage. Any disorder which causes hepatocyte injury or death, including hypoxia, metabolic alterations resulting in hepatocyte lipid accumulation, bacterial or chemical toxins and drugs, inflammation, or neoplasia, can result in increased ALT activity in the serum. In dogs, increased blood glucocorticoid concentration commonly results in a two to five-fold increase in serum ALT activity, either due to increased ALT production or mild hepatocyte injury. Serum ALT activity may increase by as much as 40-fold in dogs with glucocorticoid hepatopathy. Anticonvulsant drugs also cause increased ALT activity in dogs, probably by induction as well as hepatoctye injury. Serum activity of ALT is proportional to the number of hepatocytes which are injured, but the magnitude of increase is not a reliable indicator of the severity of the damage. Aspartate aminotransferase is present in muscle as well as liver, and thus is not liver specific. However, AST is more sensitive than ALT for detecting certain types of hepatocyte injury, thus both are often analyzed. Assaying for a specific muscle enzyme such as creatine kinase can identify the source of increased AST activity. Sorbitol dehydrogenase is liver specific, but has no advantage over ALT in dogs and cats; disadvantages include poor in-vitro stability. Glutamate dehydrogenase is also liver specific, but the assay for GLDH is difficult and not widely available, and in dogs and cats, it offers no advantages over ALT. ENZYME ASSAYS WHICH DETECT CHOLESTASIS Cholestasis is usually detected by measuring serum activities of induced enzymes or by measuring serum concentrations of substances normally excreted through the biliary system. Lesions involving the intra- or extrahepatic biliary system are common causes of cholestasis, but disorders resulting in hepatocyte swelling, such as lipidosis or inflammation, can also result in obstruction of small bile canaliculi. Two serum enzymes used to detect cholestasis are alkaline phosphatase (ALP) and gamma glutamyl transferase (GGT). 49
50 Alkaline phosphatase. Although all ALP activity is measured when performing a biochemical profile, specific isoenzymes produced by various tissues can be detected by other laboratory methods; differentiation of isoenzymes from bone (BALP), liver (LALP), and corticosteroid-induced (CiALP) is useful when the cause of increased ALP is not obvious from other laboratory tests. While cholestasis is the main cause of LALP induction, drugs such as anticonvulsants (phenobarbital, phenytoin, primidone) and glucocorticosteroids induce LALP production, as well. While corticosteroids can induce LALP, they also induce CiALP. The magnitude of CiALP increase does not usually correlate with the presence or absence of steroid hepatopathy. Increased serum ALP activity may also be associated with increased osteoblastic activity; growing animals have serum ALP activity which is increased over that of adults due to increased BALP. For example, kittens less than 5 months of age normally have serum ALP activity of IU/L, while reference range for adult cats is 2-20 IU/L. Mild increases in serum ALP activity is seen in patients with various bone diseases in which there is increased osteoblastic activity. The half-life of ALP is shorter in cats than in dogs and consequently, mild increases in serum ALP are considered more significant in cats. Gamma glutamyl transferase is present in various tissues, but most of the serum activity originates in the liver. Increased GGT production occurs with cholestasis, and in dogs, is secondary to induction by corticosteroids. Moreover, acute hepatic injury can result in increases in serum GGT activity. Serum GGT activity increases at about the same rate as serum ALP activity with cholestasis. In dogs receiving anticonvulsant medication, serum GGT activity increases to approximately 2-3 times the upper end of the reference range TESTS OF LIVER FUNCTION Substances which are normally removed from the blood by the liver, and are then metabolized and/or excreted via the biliary system, include bilirubin, bile acids, cholesterol, ammonia, and exogenous substances. Bilirubin is a by-product of hemoglobin breakdown and is transported to the liver, where it is extracted from a carrier protein and enters hepatocytes. There bilirubin attaches to a binding protein, ligandin, and is conjugated to a sugar group (glucuronic acid) and is then secreted into bile canaliculi and excreted in bile. Some conjugated bilirubin leaks into the blood and is either excreted by the kidney or is bound to protein (delta bilirubin). Hyperbilirubinemia can result from increased production of bilirubin due to increased erythrocyte destruction, decreased uptake and/or conjugation by hepatocytes, and disruption or blockage of bile flow (cholestasis), either intrahepatic or extrahepatic. If hyperbilirubinemia is caused by cholestasis, serum ALP and GGT activities will be increased. Delta bilirubin tends to accumulate during cholestatic disease, and has a half-life of approximately 2 weeks. Measurement of delta bilirubin can provide insight into duration of cholestatic disease. Serum bile acid concentration is a useful indicator of liver function. Bile acids are synthesized in hepatocytes from cholesterol, are conjugated to amino acids, and are secreted via the biliary system into the intestine, where they emulsify fat and aid in fat digestion and absorption. Approximately 95% of bile acids are reabsorbed into the blood from the ileum, and are cleared from the portal circulation by the liver and reutilized. Causes of increased serum bile acid concentration include deviation of the portal circulation (portosystemic shunts or cirrhosis), decrease in hepatocyte uptake of bile acids (e.g., hepatitis, necrosis, hepatic lipidosis, glucocorticoid hepatopathy, decreased functional liver), and decreased bile acid excretion by the liver and subsequent regurgitation into systemic circulation (cholestasis or bile duct or gall bladder rupture). Bile acids are usually measured following fasting (preprandial) and following a fatty meal (postprandial). Magnitude of increase is not useful for predicting type of liver disease, although markedly increased postprandial bile acid concentrations are suggestive of portosystemic shunts. In general, bile acid concentration is more sensitive for detecting liver disease than are most other tests for liver injury or function, and bile acid concentration has replaced measurement of plasma ammonia concentration and ammonia tolerance test, as well as BSP and ICG excretion tests. If bile acids are normal, liver disease can usually be eliminated as a diagnosis. Decreased serum concentrations of blood constituents normally synthesized by the liver, including albumin, urea, cholesterol, coagulation factors and glucose, may suggest liver failure. Hypoalbuminemia is not usually noted until 60 to 80% of liver function is lost. Other causes of hypoalbuminemia to consider are decreased intake (e.g., starvation or malabsorption/maldigestion) and excessive loss (e.g., protein losing enteropathy, glomerulonephropathy). Urea is synthesized from ammonia by hepatocytes. Consequently, blood urea nitrogen (BUN) concentration decreases with liver failure. Other causes of decreased BUN concentration include diuresis and inadequate protein intake. Hypocholesterolemia is seen with hepatic failure, since the liver is a major site of cholesterol synthesis; conversely, serum cholesterol concentration is increased with cholestasis, since bile is a major route of cholesterol excretion from the body. In patients with both cholestasis and failure, serum cholesterol concentrations may be normal. Other causes of hypocholesterolemia include inadequate intake, such as may be seen with starvation or malabsorption/maldigestion syndromes. 50
51 Coagulation factors 1, 2, 5, 9, and 10 are synthesized in the liver. Moreover, blockage of bile flow can result in decreased absorption of vitamin K with subsequent decreased production of vitamin K dependent coagulation factors (2, 7,9, 10). In patients with severe liver failure, reduced synthesis of these factors results in increased activated clotting time, and prolongation of one-stage prothrombin time and activated partial thromboplastin time. Hypoglycemia may be seen in patients with liver failure, since the liver plays a key role in gluconeogenesis and glycogenolysis. However, postprandial hyperglycemia may be seen due to decreased glucose uptake by the liver. PROFILE ABNORMALITIES IN VARIOUS TYPES OF LIVER DISEASE Profile abnormalities may be similar in different liver diseases, thus diagnosis of a specific type of liver disease is often not possible. While biochemical profiles can determine the presence of hepatocellular damage, cholestasis, and liver failure, other diagnostic procedures such as liver biopsy, ultrasound examination, and radiography are often necessary to definitely diagnose liver disease. Certain patterns of abnormalities are associated with certain disorders, and examples of these follow. Portosystemic shunts result in increased serum bile acid concentrations; other findings associated with liver failure may be present. Evidence of cholestasis and hepatocellular damage is usually not present unless the shunt is acquired. Microcytic anemia with decreased serum iron is common, and while sometimes associated with chronic blood loss, is usually due to abnormal iron metabolism. Hepatic necrosis results in increased activities of leakage enzymes and diffuse necrosis may lead to cholestasis. Bile acid concentrations and other liver function tests are usually normal unless necrosis is diffuse. Hypoxemia or mild toxic damage results in increased leakage enzyme activities. Evidence of cholestasis is usually not present. Hepatic lipidosis results in increases in leakage enzymes, as well as evidence of cholestasis. For example, 75 % of cats with hepatic lipidosis have increased ALT, 80% have increased ALP, but only 15% have increased GGT. Bile acid concentrations are usually increased. Steroid hepatopathy in dogs causes increased ALT, markedly increased ALP, and inconsistent increases in bilirubin and bile acid concentrations. Other hepatic function tests are usually normal. Biliary abnormalities, such as cholangitis, cholangiohepatitis, and bile duct obstruction, usually result in mild increase in leakage enzymes, but marked increase in induced enzymes. Bilirubin concentrations are moderately to markedly increased and bile acid concentrations are usually increased. Other tests of liver function are usually normal unless these diseases progress to liver failure. Chronic progressive liver disease, whatever the cause, has moderate to severe inflammation as a common feature. Necrosis, fibrosis, and cirrhosis can also occur. Serum activities of leakage and induced enzymes are mild to moderately increased. Bilirubin and bile acids concentrations are inconsistently increased. Other tests of hepatic function are normal until the disease results in liver failure. Liver failure (end-stage liver disease) occurs when 60-80% of functional mass is lost. Leakage enzymes are often normal or only mildly increased, while induced enzymes are moderately to markedly increased due to cholestasis. Bilirubin and bile acid concentrations are increased, and other findings include hypoglycemia, decreased BUN concentration, hypoalbuminemia, hypocholesterolemia, and abnormal coagulation tests. 51
! Lymphadenitis Suppurative Mixed Mononuclear (macrophagic( or granulomatous! Metastatic neoplasia!")
52 Cytology of Lymph Nodes Mary Anna Thrall Colorado State University Ross University Indications Lymph node enlargement Suspect metastasis Causes of lymphadenopathy! Hyperplasia/ Reactive (Antigenic stimulation)! Lymphadenitis Suppurative Mixed Mononuclear (macrophagic( or granulomatous! Metastatic neoplasia! Primary Neoplasia (lymphoma) Types of cells seen in lymph nodes! Small lymphocytes! Intermediate-sized lymphocytes! Lymphoblasts! Plasma cells! Macrophages! Eosinophils! Mast cells! Abnormal cells (metastatic neoplastic cells) Lymphadenopathy CELL Types Hyperplasia/ Reactive - Increased Plasma Cells Lymphadenitis - Neutrophils or Macrophages Metastatic neoplasia - clumps of neoplastic cells such as mast cells, epithelial cells, mesenchymal cells Lymphoma - > 50% lymphoblasts Or uniform population of small slightly atypical lymphs 1





53 L REACTIVE LYMPH NODES: (HYPERPLASIA) Increased plasma cells Increased lymphoblasts (but usually not > 20% 2






54 Reactive lymph nodes In most cases you do NOT find the cause for the reactive node in the cytologic specimen. The antigen stimulating the node is outside the node but in its field of drainage. LYMPHADENDITIS 3




")


55 Lymphoma Lymph nodes: If > than 50% lymphoblasts, likely lymphoma. Small cell variants are difficult {PCR (dogs) or flow cytology (cats) indicated} Other tissues: should be no lymphoblasts present 100 X oil LYMPHOMA 4



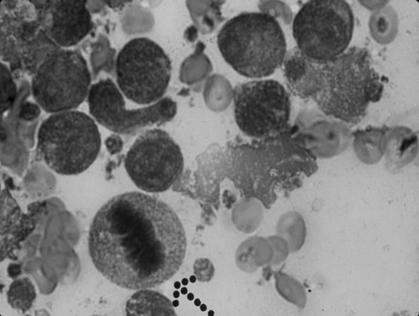


56 Bone marrow aspirate 5
!")





57 DNA Clonality assay (PARR - PCR for antigen receptor rearrangements)! Used to determine if lymphocytes are derived from a single clone! Sensitivity and specificity: Dogs: overall 80% sensitive, 94% specific. Cats: estimated sensitivity 65%. No data yet on specificity.! No formalin fixed samples! Colorado State University Diagnostic Laboratory 300 West Drake Rd. Rm E-100 Fort Collins, CO US $105 Diagnostic gels!"#$%&'" Pos Control B cell T cell Immunoglobulin primers ()!)*+)!$+,-, *"++ EVOLUTION OF a B CELL LYMPHOMA./"0"!%$%&)! &!&%&$+,*1"() *+&!&*$+, /"(&00&)! /"*2//"!*" 6





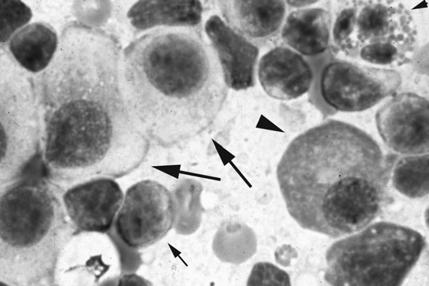
58 Metastatic Neoplasia M Fig 10. Metastatic mast cell tumor in a lymph node. Mast cells are indicated by arrows, and small lymphocytes by arrowheads. 345,667,,(89:;9:94<,=:;9,<8>>,9?=@A,;9:4B8C,D49E,F4GGHI?4J7,,.@@A>K,;9:4B4B5, =:;9,<8>>;,:A8,4BC4<:98C,LK,>:A58,:AA@D;M,N>:;=:,<8>>,LK,>:A58,:AA@DE8:CM,$BC, ;=:>>,>K=NE@<K98,LK,;=:>>,:AA@DM,:BC,8@;4B@NE4> LK,;=:>>,:AA@DE8:C7, 7




!")

59 Fig 12. Aspirate of same lymph node as shown in Fig 11, when stained With a traditional Wright s stain. Problems Perinodal fat! Missed lymph node! Perinodal Fat (esp( popliteal)! Salivary gland! Understained slides! Look for etiologies in reactive and inflamed nodes, but uncommon to find them 8





60 9
Almost any suspected tumor can be aspirated easily and safely. Some masses are more risky to aspirate including:
 DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
Diagnostic Cytology of Cancer Cases
 Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION
 EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES COPYRIGHTED MATERIAL SECOND EDITION
 VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
Blood smear analysis in the emergency veterinary patient
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Blood smear analysis in the emergency veterinary patient Author : Ashley Wemple Categories : RVNs Date : April 1, 2010 Ashley
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Blood smear analysis in the emergency veterinary patient Author : Ashley Wemple Categories : RVNs Date : April 1, 2010 Ashley
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology
 Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology CABOT RINGS Cabot rings in a patient with hemolytic anemia. Cabot ring (red arrow) and Howell-Jolly body (blue arrow). Observed in
Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology CABOT RINGS Cabot rings in a patient with hemolytic anemia. Cabot ring (red arrow) and Howell-Jolly body (blue arrow). Observed in
Proceeding of the SEVC Southern European Veterinary Conference
 www.ivis.org Proceeding of the SEVC Southern European Veterinary Conference Oct. 17-19, 2008 Barcelona, Spain http://www.sevc.info Reprinted in the IVIS website with the permission of the SEVC www.ivis.org
www.ivis.org Proceeding of the SEVC Southern European Veterinary Conference Oct. 17-19, 2008 Barcelona, Spain http://www.sevc.info Reprinted in the IVIS website with the permission of the SEVC www.ivis.org
Cytology of Inflammatory Cutaneous lesions in the Dog and Cat
 Cytology of Inflammatory Cutaneous lesions in the Dog and Cat Rick L. Cowell, DVM, MS, MRCVS, Diplomate ACVP Clinical Pathologist IDEXX Laboratories Inc A. Cytologic Patterns of Inflammation: 1. Neutrophilic
Cytology of Inflammatory Cutaneous lesions in the Dog and Cat Rick L. Cowell, DVM, MS, MRCVS, Diplomate ACVP Clinical Pathologist IDEXX Laboratories Inc A. Cytologic Patterns of Inflammation: 1. Neutrophilic
RED BLOOD CELLS IMPORTANCE OF FILM EXAMINATION: PART ONE
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk RED BLOOD CELLS IMPORTANCE OF FILM EXAMINATION: PART ONE Author : Mark Richer Categories : Vets Date : March 25, 2013 Mark
Vet Times The website for the veterinary profession https://www.vettimes.co.uk RED BLOOD CELLS IMPORTANCE OF FILM EXAMINATION: PART ONE Author : Mark Richer Categories : Vets Date : March 25, 2013 Mark
Hematology Unit Lab 1 Review Material
 Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
CYTOLOGY OF THE LIVER
 CYTOLOGY OF THE LIVER Maxey L. Wellman, DVM, PhD, DACVP (Clinical Pathology) Professor, Department of Veterinary Biosciences, College of Veterinary Medicine, The Ohio State University, Columbus, OH, USA
CYTOLOGY OF THE LIVER Maxey L. Wellman, DVM, PhD, DACVP (Clinical Pathology) Professor, Department of Veterinary Biosciences, College of Veterinary Medicine, The Ohio State University, Columbus, OH, USA
EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES
 EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Cytology of NeoPlasia
 PEEr reviewed Cytology of NeoPlasia An Essential Component of Diagnosis Anne Barger, DVM, MS, Diplomate ACVP Cytology is a quick, easy, and inexpensive diagnostic tool. It is commonly used for the diagnosis
PEEr reviewed Cytology of NeoPlasia An Essential Component of Diagnosis Anne Barger, DVM, MS, Diplomate ACVP Cytology is a quick, easy, and inexpensive diagnostic tool. It is commonly used for the diagnosis
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal 1 0.
 Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS
 EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE
 Log Out Help current login :lcytryn@montefiore.org HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE Lawrence Cytryn, M.D. - Course Director 1998 Edward Burns, M.D. Images used by permission within AECOM
Log Out Help current login :lcytryn@montefiore.org HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE Lawrence Cytryn, M.D. - Course Director 1998 Edward Burns, M.D. Images used by permission within AECOM
EDUCATIONAL COMMENTARY DIFFERENTIATING IMMATURE PERIPHERAL BLOOD CELLS
 Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Guide to the 1-3 Minute Blood Film Microscopic Review: Why and How?
 Guide to the 1-3 Minute Blood Film Microscopic Review: Why and How? Dennis B. DeNicola, DVM, PhD, DACVP Chief Veterinary Educator IDEXX Laboratories, Inc. Westbrook, ME USA Adjunct Professor of Veterinary
Guide to the 1-3 Minute Blood Film Microscopic Review: Why and How? Dennis B. DeNicola, DVM, PhD, DACVP Chief Veterinary Educator IDEXX Laboratories, Inc. Westbrook, ME USA Adjunct Professor of Veterinary
THE BLOOD FILM REVIEW
 IN-CLINIC HEMATOLOGY Peer Reviewed In-Clinic Hematology: THE BLOOD FILM REVIEW Leslie Sharkey, DVM, PhD, Diplomate ACVP (Clinical Pathology), and Daniel Heinrich, DVM University of Minnesota A complete
IN-CLINIC HEMATOLOGY Peer Reviewed In-Clinic Hematology: THE BLOOD FILM REVIEW Leslie Sharkey, DVM, PhD, Diplomate ACVP (Clinical Pathology), and Daniel Heinrich, DVM University of Minnesota A complete
Submission of samples. Cytology of Lumps and Bumps. Evaluation of samples. Use caution interpreting. Criteria of malignancy.
 Submission of samples Cytology of Lumps and Bumps Paul Avery VMD, PhD, DACVP paul.avery@colostate.edu Air dry only No wet fixation using formalin or ethanol Stain 1-2 on-site to evaluate quality Send all
Submission of samples Cytology of Lumps and Bumps Paul Avery VMD, PhD, DACVP paul.avery@colostate.edu Air dry only No wet fixation using formalin or ethanol Stain 1-2 on-site to evaluate quality Send all
HISTOPATHOLOGY. Shannon Martinson
 HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
Proudly Presents: CLINICAL PATHOLOGY
 Chicago Veterinary Medical Association Shaping the Future of Veterinary Medicine - Promoting the Human-Animal Bond Proudly Presents: CLINICAL PATHOLOGY With: ANNE BARGER DVM, MS, DACVP April 13, 2016 Chicago
Chicago Veterinary Medical Association Shaping the Future of Veterinary Medicine - Promoting the Human-Animal Bond Proudly Presents: CLINICAL PATHOLOGY With: ANNE BARGER DVM, MS, DACVP April 13, 2016 Chicago
HEMATOLOGY: BLOOD SMEAR REVIEW IN THE EMERGENCY SETTING
 HEMATOLOGY: BLOOD SMEAR REVIEW IN THE EMERGENCY SETTING Deanna Schaefer, DVM, MS, MT(ASCP), Dipl ACVP Assistant Professor, Veterinary Clinical Pathology, University of Tennessee The main objective of this
HEMATOLOGY: BLOOD SMEAR REVIEW IN THE EMERGENCY SETTING Deanna Schaefer, DVM, MS, MT(ASCP), Dipl ACVP Assistant Professor, Veterinary Clinical Pathology, University of Tennessee The main objective of this
Blood Cell Identification Graded
 BCP-21 Blood Cell Identification Graded Case History The patient is a 37-year-old female with a history of multiple sickle cell crises. She now presents with avascular necrosis of the left hip. Laboratory
BCP-21 Blood Cell Identification Graded Case History The patient is a 37-year-old female with a history of multiple sickle cell crises. She now presents with avascular necrosis of the left hip. Laboratory
Contents. Section Editor David Blomberg, MD
 Contents A Closer Look At Discussions...viii Heme CAPsules Video...ix Foreword...x Preface to First Edition...xii Preface to Second Edition...xiii Contributors...xiv Current and Past HCMRC Members...xv
Contents A Closer Look At Discussions...viii Heme CAPsules Video...ix Foreword...x Preface to First Edition...xii Preface to Second Edition...xiii Contributors...xiv Current and Past HCMRC Members...xv
Blood Cell Identification Graded
 Blood Cell Identification Graded Case History The patient was a five-day-old girl with an elevated unconjugated bilirubin and a weakly positive direct antiglobulin test (DAT). Her CBC showed: WBC = 11.0
Blood Cell Identification Graded Case History The patient was a five-day-old girl with an elevated unconjugated bilirubin and a weakly positive direct antiglobulin test (DAT). Her CBC showed: WBC = 11.0
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Incorporating Differentials Into Every Complete Blood Count. Paige Flowers, LVT Dogwood Veterinary Internal Medicine
 Incorporating Differentials Into Every Complete Blood Count Paige Flowers, LVT Dogwood Veterinary Internal Medicine Complete Blood Count Diagnostic performed to evaluate the quantity and morphology of
Incorporating Differentials Into Every Complete Blood Count Paige Flowers, LVT Dogwood Veterinary Internal Medicine Complete Blood Count Diagnostic performed to evaluate the quantity and morphology of
Cytoplasmic changes Nuclear changes
 The presence of infection in the female genital tract may procure certain cellular changes in the epithelium. Such changes are seen in nucleus and cytoplasm surrounding the nucleus. Cytoplasmic changes
The presence of infection in the female genital tract may procure certain cellular changes in the epithelium. Such changes are seen in nucleus and cytoplasm surrounding the nucleus. Cytoplasmic changes
EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES
 EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Cytology in Veterinary Practice: Sample Collection, Slide Preparation and Interpretation Guidelines
 Cytology in Veterinary Practice: Sample Collection, Slide Preparation and Interpretation Guidelines ASPIRATION OF A MASS A. Rick Alleman, DVM, PhD, DABVP, DACVP Lighthouse Veterinary Consultants, LLC Gainesville,
Cytology in Veterinary Practice: Sample Collection, Slide Preparation and Interpretation Guidelines ASPIRATION OF A MASS A. Rick Alleman, DVM, PhD, DABVP, DACVP Lighthouse Veterinary Consultants, LLC Gainesville,
Table of Contents. Preface xi. Acknowledgments xiii. Part I Overview of the Diagnostic Process 1. 1 Overview of Grading and Staging 3
 Table of Contents Preface xi Acknowledgments xiii Part I Overview of the Diagnostic Process 1 1 Overview of Grading and Staging 3 Identification of the process 3 Identification of tumor types 5 Grading
Table of Contents Preface xi Acknowledgments xiii Part I Overview of the Diagnostic Process 1 1 Overview of Grading and Staging 3 Identification of the process 3 Identification of tumor types 5 Grading
A Look at the Lymphoid System Rose Raskin, DVM, PhD, DACVP Purdue University West Lafayette, IN
 A Look at the Lymphoid System Rose Raskin, DVM, PhD, DACVP Purdue University West Lafayette, IN The lymphoid organs commonly biopsied include the peripheral and internal lymph nodes, spleen, and occasionally
A Look at the Lymphoid System Rose Raskin, DVM, PhD, DACVP Purdue University West Lafayette, IN The lymphoid organs commonly biopsied include the peripheral and internal lymph nodes, spleen, and occasionally
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
By Dr. Mohamed Saad Daoud
 By Dr. Mohamed Saad Daoud Part I Introduction Types of White Blood Cells Genesis of the White Blood Cells Life Span of the White Blood Cells Dr. Mohamed Saad Daoud 2 Leucocytes Introduction: Infectious
By Dr. Mohamed Saad Daoud Part I Introduction Types of White Blood Cells Genesis of the White Blood Cells Life Span of the White Blood Cells Dr. Mohamed Saad Daoud 2 Leucocytes Introduction: Infectious
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016
 NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016 Results from this proficiency test event are available at: http://www.wadsworth.org/regulatory/clep/pt/summaries SLIDE
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016 Results from this proficiency test event are available at: http://www.wadsworth.org/regulatory/clep/pt/summaries SLIDE
EPIDEMIOLOGICAL AND MORPHOLOGICAL CHARACTERISTICS OF CUTANEOUS ROUND CELL TUMORS DIAGNOSED USING ASPIRATIVE CYTOLOGY IN DOGS
 Scientific Works. Series C. Veterinary Medicine. Vol. LXIII (1) ISSN 2065-1295; ISSN 2343-9394 (CD-ROM); ISSN 2067-3663 (Online); ISSN-L 2065-1295 Abstract EPIDEMIOLOGICAL AND MORPHOLOGICAL CHARACTERISTICS
Scientific Works. Series C. Veterinary Medicine. Vol. LXIII (1) ISSN 2065-1295; ISSN 2343-9394 (CD-ROM); ISSN 2067-3663 (Online); ISSN-L 2065-1295 Abstract EPIDEMIOLOGICAL AND MORPHOLOGICAL CHARACTERISTICS
Proceeding of the LAVC Latin American Veterinary Conference Oct , 2009 Lima, Peru
 Close this window to return to IVIS www.ivis.org Proceeding of the LAVC Latin American Veterinary Conference Oct. 16-19, 2009 Lima, Peru Reprinted in the IVIS website with the permission of the LAVC http://www.ivis.org/
Close this window to return to IVIS www.ivis.org Proceeding of the LAVC Latin American Veterinary Conference Oct. 16-19, 2009 Lima, Peru Reprinted in the IVIS website with the permission of the LAVC http://www.ivis.org/
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal/
 Cell Identification BMD-09 Participants Identification No. % Evaluation Mitotic figure 233 96.7 Educational Erythrocyte precursor, abnormal/ 4 1.7 Educational dysplastic nuclear features Erythrocyte precursor
Cell Identification BMD-09 Participants Identification No. % Evaluation Mitotic figure 233 96.7 Educational Erythrocyte precursor, abnormal/ 4 1.7 Educational dysplastic nuclear features Erythrocyte precursor
A CASE ORIENTED APPROACH Alan H. Rebar, DVM, PhD, DACVP
 RED CELL RESPONSES IN DISEASE: A CASE ORIENTED APPROACH Alan H. Rebar, DVM, PhD, DACVP CLINICAL PATHOLOGY Introduction Anemia is one of the most common disease syndromes in domestic animals and may be
RED CELL RESPONSES IN DISEASE: A CASE ORIENTED APPROACH Alan H. Rebar, DVM, PhD, DACVP CLINICAL PATHOLOGY Introduction Anemia is one of the most common disease syndromes in domestic animals and may be
LGM International, Inc.
 Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Blood & Blood Formation
 Module IB Blood & Blood Formation Histology and Embryology Martin Špaček, MD (m.spacek@centrum.cz) http://www.lf3.cuni.cz/histologie Approximately 7% of a person's weight is blood (about 5 L) Blood consists
Module IB Blood & Blood Formation Histology and Embryology Martin Špaček, MD (m.spacek@centrum.cz) http://www.lf3.cuni.cz/histologie Approximately 7% of a person's weight is blood (about 5 L) Blood consists
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES
 namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
Prof. Mahmoud Rushdi Faculty of Veterinary Medicine Assiut University Egypt. RBCs counts. Anaemia.
 By Prof. Mahmoud Rushdi Faculty of Veterinary Medicine Assiut University Egypt ١ RBCs counts Normal Anaemia Polycythaemia Morphological Etiological Relative Absolute Size Stain Shape Inclusion Hemorrhagic
By Prof. Mahmoud Rushdi Faculty of Veterinary Medicine Assiut University Egypt ١ RBCs counts Normal Anaemia Polycythaemia Morphological Etiological Relative Absolute Size Stain Shape Inclusion Hemorrhagic
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
Reactive and Neoplastic Lymphocytosis
 Reactive and Neoplastic Lymphocytosis Koranda A. Walsh, VMD, BS Assistant Professor, Clinical Pathobiology University of Pennsylvania School of Veterinary Medicine PLEASE NOTE: These notes are meant as
Reactive and Neoplastic Lymphocytosis Koranda A. Walsh, VMD, BS Assistant Professor, Clinical Pathobiology University of Pennsylvania School of Veterinary Medicine PLEASE NOTE: These notes are meant as
Blood Cells. Dr. Sami Zaqout. Dr. Sami Zaqout Faculty of Medicine IUG
 Blood Cells Dr. Sami Zaqout Blood Blood Blood cells (45%) Erythrocytes Platelets Leukocytes Plasma (55%) Hematocrit tubes with blood Composition of Plasma Plasma Aqueous solution (90%) Substances (10%)
Blood Cells Dr. Sami Zaqout Blood Blood Blood cells (45%) Erythrocytes Platelets Leukocytes Plasma (55%) Hematocrit tubes with blood Composition of Plasma Plasma Aqueous solution (90%) Substances (10%)
Blood: Functions. Liquid connective tissue 3 general functions 1. Transportation. 2. Regulation. 3. Protection
 Blood Elements Lecture Objectives List blood components. Classify formed elements of blood. Discuss the scientific basis of the above classification. Describe the basic structure of erythrocytes and criteria
Blood Elements Lecture Objectives List blood components. Classify formed elements of blood. Discuss the scientific basis of the above classification. Describe the basic structure of erythrocytes and criteria
Interpreting the CBC. Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired
 Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Principles of Surgical Oncology. Winnie Achilles Tierklinik Hollabrunn Lastenstrasse Hollabrunn
 Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
Introduction. 23 rd Annual Seminar in Pathology. FLUIDS, Part 1. Pittsburgh, PA Gladwyn Leiman UVMMC, VT
 23 rd Annual Seminar in Pathology Pittsburgh, PA Gladwyn Leiman UVMMC, VT FLUIDS, Part 1 "Blue walls", Claudia Hansen, 2009 Introduction o Challenging to everyone o Almost any benign or malignant process
23 rd Annual Seminar in Pathology Pittsburgh, PA Gladwyn Leiman UVMMC, VT FLUIDS, Part 1 "Blue walls", Claudia Hansen, 2009 Introduction o Challenging to everyone o Almost any benign or malignant process
Requirements: Glass slides Leishman stain Microscopes Disposable needles Vials containing anticoagulants Methylated-spirit Staining rack
 Aim: To make a blood smear and to count the different types of leucocytes present in a stained blood smear and express their relative counts in percentage Principle - The blood contains various types of
Aim: To make a blood smear and to count the different types of leucocytes present in a stained blood smear and express their relative counts in percentage Principle - The blood contains various types of
Dr. Issraa Ali Hussein
 CLINICAL 09888888;rCYTOLOGY Dr. Issraa Ali Hussein objectives Define diagnostic cytology (clinical cytology). Explain the differences between histopathology and cytopathology. Recognize the methods for
CLINICAL 09888888;rCYTOLOGY Dr. Issraa Ali Hussein objectives Define diagnostic cytology (clinical cytology). Explain the differences between histopathology and cytopathology. Recognize the methods for
Drop of Blood Unravels Mysteries. Prof. Salma Afrose Department of Hematology Dhaka Medical College
 Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005
 Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Laboratory
Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Laboratory
Peripheral Blood Smear Examination. Momtazmanesh MD. Ped. Hematologist & Oncologist Loghman General Hospital
 1395 Peripheral Blood Smear Examination Momtazmanesh MD. Ped. Hematologist & Oncologist Loghman General Hospital Peripheral Blood Smear A peripheral blood smear is a snapshot of the cells that are present
1395 Peripheral Blood Smear Examination Momtazmanesh MD. Ped. Hematologist & Oncologist Loghman General Hospital Peripheral Blood Smear A peripheral blood smear is a snapshot of the cells that are present
A case of giant cell tumour of soft parts in a horse Francesco Cian 1, Sarah Whiteoak 2, Jennifer Stewart 1
 A case of giant cell tumour of soft parts in a horse Francesco Cian 1, Sarah Whiteoak 2, Jennifer Stewart 1 1 Animal Health Trust, Newmarket, UK 2 608 Equine and Farm Vets, Rowington, UK Signalment: Horse,
A case of giant cell tumour of soft parts in a horse Francesco Cian 1, Sarah Whiteoak 2, Jennifer Stewart 1 1 Animal Health Trust, Newmarket, UK 2 608 Equine and Farm Vets, Rowington, UK Signalment: Horse,
٢٨/٠١/١٤٣٧. Prof. M. Rushdi.
 ١ PARAMETERS OF LEUCOCYTES PICTURE TtlWBC Total WBCs count Differential LC Hemocytometer Blood film Blood Cell Counter Blood Cell Counter INTERPRETATION OF LEUCOCYTES PICTURE 1.Leucocytosis. 2. Leucopenia.
١ PARAMETERS OF LEUCOCYTES PICTURE TtlWBC Total WBCs count Differential LC Hemocytometer Blood film Blood Cell Counter Blood Cell Counter INTERPRETATION OF LEUCOCYTES PICTURE 1.Leucocytosis. 2. Leucopenia.
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Pathology of the Hematopoietic System GROSS/HISTO LAB
 Pathology of the Hematopoietic System GROSS/HISTO LAB Paul Hanna (thanks to Dr s Aburto, Martinson & Fenton) Fall 2014 Slide 1 Spleen from a Beaver Give a morphologic diagnosis and possible etiology &
Pathology of the Hematopoietic System GROSS/HISTO LAB Paul Hanna (thanks to Dr s Aburto, Martinson & Fenton) Fall 2014 Slide 1 Spleen from a Beaver Give a morphologic diagnosis and possible etiology &
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Indication of peripheral blood smear exmination:
 Indication of peripheral blood smear exmination: 1. For carried out differential WBC count. 2. For differential diagnosis of anemia. 3. For detection of parasites. 4. For diagnosis of leucemoid reaction.
Indication of peripheral blood smear exmination: 1. For carried out differential WBC count. 2. For differential diagnosis of anemia. 3. For detection of parasites. 4. For diagnosis of leucemoid reaction.
ADVANCED HAEMATOLOGY BATTLE OF THE BANDS. Dennis B. DeNicola, DVM, PhD, DACVP IDEXX Laboratories, Inc. Westbrook, Maine, USA BACKGROUND
 ADVANCED HAEMATOLOGY BATTLE OF THE BANDS Dennis B. DeNicola, DVM, PhD, DACVP IDEXX Laboratories, Inc. Westbrook, Maine, USA BACKGROUND The identification of immature neutrophils (bands, metamyelocytes,
ADVANCED HAEMATOLOGY BATTLE OF THE BANDS Dennis B. DeNicola, DVM, PhD, DACVP IDEXX Laboratories, Inc. Westbrook, Maine, USA BACKGROUND The identification of immature neutrophils (bands, metamyelocytes,
Canine Histiocytic Disorders DR. MEREDITH GAUTHIER, DVM DACVIM (ONCOLOGY) OCTOBER 29, 2015
 OCTOBER 29, 2015") Canine Histiocytic Disorders DR. MEREDITH GAUTHIER, DVM DACVIM (ONCOLOGY) OCTOBER 29, 2015 Canine Histiocytes! Cells derived from CD34+ stem cells and blood monocytes! Macrophages! Dendritic cells (DC)!
Canine Histiocytic Disorders DR. MEREDITH GAUTHIER, DVM DACVIM (ONCOLOGY) OCTOBER 29, 2015 Canine Histiocytes! Cells derived from CD34+ stem cells and blood monocytes! Macrophages! Dendritic cells (DC)!
Neoplasia part I. Dr. Mohsen Dashti. Clinical Medicine & Pathology nd Lecture
 Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Pathology of the Hematopoietic System. Case studies
 Pathology of the Hematopoietic System Case studies Shannon Martinson, September 2015 Signalment: 9 yr-old MC cat Case Study 1 History: Cat had been anorexic and developed bleeding in the eyes Physical
Pathology of the Hematopoietic System Case studies Shannon Martinson, September 2015 Signalment: 9 yr-old MC cat Case Study 1 History: Cat had been anorexic and developed bleeding in the eyes Physical
Individual cells Extracellular matrix
 Connective Tissue Connective Tissue Elements Individual cells Extracellular matrix»fibers» Collagen» Elastic» Reticular»Ground Substance» PG (proteoglycans)» GAG (glycosaminoglycan)» GP (glycoprotein)
Connective Tissue Connective Tissue Elements Individual cells Extracellular matrix»fibers» Collagen» Elastic» Reticular»Ground Substance» PG (proteoglycans)» GAG (glycosaminoglycan)» GP (glycoprotein)
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
Blood DLC, Retic count, PCV, Hb and ESR. Dr. Tamara Alqudah
 Blood DLC, Retic count, PCV, Hb and ESR Dr. Tamara Alqudah Differential Leukocyte Count (DLC) There are 5 main types of WBCs: 1. Neutrophils: 40-80% 2. Eosinophils: 1-6 % 3. Basophils: < 1-2% 4. Lymphocytes:
Blood DLC, Retic count, PCV, Hb and ESR Dr. Tamara Alqudah Differential Leukocyte Count (DLC) There are 5 main types of WBCs: 1. Neutrophils: 40-80% 2. Eosinophils: 1-6 % 3. Basophils: < 1-2% 4. Lymphocytes:
Whole Blood. Lab 29A. Blood. Plasma. Whole Blood. Formed Elements. Plasma: Fluid component. Formed elements: Cells and fragments
 Whole Blood Lab 29A. Blood Plasma: Fluid component Water (90%) Dissolved plasma proteins Other solutes Formed elements: Cells and fragments RBCs (carry Oxygen) WBCs (immunity) Platelets (cell fragments
Whole Blood Lab 29A. Blood Plasma: Fluid component Water (90%) Dissolved plasma proteins Other solutes Formed elements: Cells and fragments RBCs (carry Oxygen) WBCs (immunity) Platelets (cell fragments
Formation of Blood Cells
 Hematopoiesis Lecture Objectives Name organs responsible for hematopoiesis in the fetus. List the developmental stages of hematopoiesis both prenatally and postnatally. Outline the major steps of post
Hematopoiesis Lecture Objectives Name organs responsible for hematopoiesis in the fetus. List the developmental stages of hematopoiesis both prenatally and postnatally. Outline the major steps of post
AVIAN HEMATOLOGY. MVDr. Zora Knotková, Ph.D. MVDr. Anna Hrdá, Ph.D.
 AVIAN HEMATOLOGY MVDr. Zora Knotková, Ph.D. MVDr. Anna Hrdá, Ph.D. Avian and Exotic Animal Clinic University of Veterinary and Pharmaceutical Sciences, Brno, Czech Republic HEMATOLOGIC TESTS Form an excellent
AVIAN HEMATOLOGY MVDr. Zora Knotková, Ph.D. MVDr. Anna Hrdá, Ph.D. Avian and Exotic Animal Clinic University of Veterinary and Pharmaceutical Sciences, Brno, Czech Republic HEMATOLOGIC TESTS Form an excellent
COMPANY OR UNIVERSITY
 CONTRIBUTOR NAME Daniel Heinrich, DVM CONTRIBUTOR EMAIL dheinric@umn.edu COAUTHORS Jed Overmann, DVM, DACVP; Davis Seelig DVM, PhD, DACVP & Matthew Sturos, DVM COMPANY OR UNIVERSITY University of Minnesota
CONTRIBUTOR NAME Daniel Heinrich, DVM CONTRIBUTOR EMAIL dheinric@umn.edu COAUTHORS Jed Overmann, DVM, DACVP; Davis Seelig DVM, PhD, DACVP & Matthew Sturos, DVM COMPANY OR UNIVERSITY University of Minnesota
Collect and label sample according to standard protocols. Gently invert tube 8-10 times immediately after draw. DO NOT SHAKE. Do not centrifuge.
 Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
CH 11 Blood OUTLINE: Functions of Blood Composition of Blood Blood Cell Disorders Blood Types Blood Clotting Functions of Blood Transportation
 1 CH 11 Blood OUTLINE: Functions of Blood Composition of Blood Blood Cell Disorders Blood Types Functions of Blood Transportation Protection Regulation ph Temperature Composition of Blood Plasma: liquid
1 CH 11 Blood OUTLINE: Functions of Blood Composition of Blood Blood Cell Disorders Blood Types Functions of Blood Transportation Protection Regulation ph Temperature Composition of Blood Plasma: liquid
The liver is involved in nearly every biochemical process required to maintain. Cytologic Evaluation of the Liver: Aspiration Findings and Limitations
 CE 798 V Vol. 24, No. 10 October 2002 Article #4 (1.5 contact hours) Refereed Peer Review Comments? Questions? Email: compendium@medimedia.com Web: VetLearn.com Fax: 800-556-3288 KEY FACTS Exfoliative
CE 798 V Vol. 24, No. 10 October 2002 Article #4 (1.5 contact hours) Refereed Peer Review Comments? Questions? Email: compendium@medimedia.com Web: VetLearn.com Fax: 800-556-3288 KEY FACTS Exfoliative
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
HISTOLOGY VIRTUAL LABORATORY BLOOD AND LYMPHATICS SYSTEM
 HISTOLOGY VIRTUAL LABORATORY BLOOD AND LYMPHATICS SYSTEM Login: http://histopath.westernu.edu Histology Atlas AND Virtual Histology links. I. HEMATOLOGY - PERIPHERAL BLOOD Purpose: To be able to identify
HISTOLOGY VIRTUAL LABORATORY BLOOD AND LYMPHATICS SYSTEM Login: http://histopath.westernu.edu Histology Atlas AND Virtual Histology links. I. HEMATOLOGY - PERIPHERAL BLOOD Purpose: To be able to identify
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP
 Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP I. Introduction The purpose of this material is to provide information that may be useful in the identification of tumors
Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP I. Introduction The purpose of this material is to provide information that may be useful in the identification of tumors
Hemopoiesis and Blood
 Hemopoiesis and Blood Blood Cells o o o Erythrocytes Leukocytes Thrombocytes Function o Transport nutrients and wastes throughout the bloodstream, fight foreign antigens and blood coagulation. Location
Hemopoiesis and Blood Blood Cells o o o Erythrocytes Leukocytes Thrombocytes Function o Transport nutrients and wastes throughout the bloodstream, fight foreign antigens and blood coagulation. Location
Urine Sediment Photomicrographs/Photographs
 Urine Sediment Photomicrographs/Photographs Case History CMP-17 This urine sample is from a 48-year-old male with a 30-year history of diabetes mellitus and new onset renal failure. Laboratory data include:
Urine Sediment Photomicrographs/Photographs Case History CMP-17 This urine sample is from a 48-year-old male with a 30-year history of diabetes mellitus and new onset renal failure. Laboratory data include:
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Tumors of the Spleen
 Tumors of the Spleen 803-808-7387 www.gracepets.com These notes are provided to help you understand the diagnosis or possible diagnosis of cancer in your pet. For general information on cancer in pets
Tumors of the Spleen 803-808-7387 www.gracepets.com These notes are provided to help you understand the diagnosis or possible diagnosis of cancer in your pet. For general information on cancer in pets
ASSESSMENT OF AVIAN ANAEMIA
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk ASSESSMENT OF AVIAN ANAEMIA Author : KATE ENGLISH Categories : Vets Date : July 21, 2008 KATE ENGLISH discusses how anaemia
Vet Times The website for the veterinary profession https://www.vettimes.co.uk ASSESSMENT OF AVIAN ANAEMIA Author : KATE ENGLISH Categories : Vets Date : July 21, 2008 KATE ENGLISH discusses how anaemia
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Canine Cutaneous Melanoma
 Canine Cutaneous Melanoma By Elizabeth Downing Clinical Advisor: Dr. Angharad Waite, VMD Basic Science Advisor: Dr. Cheryl Balkman, DVM, DACVIM Senior Seminar Paper Cornell University College of Veterinary
Canine Cutaneous Melanoma By Elizabeth Downing Clinical Advisor: Dr. Angharad Waite, VMD Basic Science Advisor: Dr. Cheryl Balkman, DVM, DACVIM Senior Seminar Paper Cornell University College of Veterinary
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Sheet #7. Dr. Heba Kalbouneh. Dr. Heba Kalbouneh. Dr. Heba Kalbouneh
 Sheet #7 Dr. Heba Kalbouneh Dr. Heba Kalbouneh Dr. Heba Kalbouneh Connective tissue The differences between epithelial and connective tissue - Epithelial cells are tightly packed (no or minimal spaces
Sheet #7 Dr. Heba Kalbouneh Dr. Heba Kalbouneh Dr. Heba Kalbouneh Connective tissue The differences between epithelial and connective tissue - Epithelial cells are tightly packed (no or minimal spaces
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Proper Slide Preparation
 Hematology Essentials: A Foundation for WBC Review Using Case Studies Christine Hinz, MS, MLS(ASCP) CM Proper Slide Preparation smooth, homogenous film 1/2 to 3/4 the slide length straight feather edge
Hematology Essentials: A Foundation for WBC Review Using Case Studies Christine Hinz, MS, MLS(ASCP) CM Proper Slide Preparation smooth, homogenous film 1/2 to 3/4 the slide length straight feather edge
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
temperature 38 o C (100.4 o F) The temperature of blood is slightly higher than the normal body temperature of 37 o C (98.6 o F).
 The temperature of blood is slightly higher than the normal body temperature of 37 o C (98.6 o F).") 1 Chapter 1 Blood Definition -Blood is a type of connective tissue that consists of cells surrounded by a fluid extracellular matrix. -Blood, blood vessels, and the heart collectively form the cardiovascular
1 Chapter 1 Blood Definition -Blood is a type of connective tissue that consists of cells surrounded by a fluid extracellular matrix. -Blood, blood vessels, and the heart collectively form the cardiovascular
2015 Descriptive Vet Path Course. Histo Exam #3 KEY
 2015 Descriptive Vet Path Course Histo Exam #3 KEY Test 3, Slide 1 Tissue from a guinea pig. MORPHOLOGIC DIAGNOSIS: Heart: Multifocally and randomly (1 pt), within the left and right ventricular myocardium
2015 Descriptive Vet Path Course Histo Exam #3 KEY Test 3, Slide 1 Tissue from a guinea pig. MORPHOLOGIC DIAGNOSIS: Heart: Multifocally and randomly (1 pt), within the left and right ventricular myocardium
Proceeding of the LAVC Latin American Veterinary Conference Oct , 2009 Lima, Peru
 Close this window to return to IVIS www.ivis.org Proceeding of the LAVC Latin American Veterinary Conference Oct. 16-19, 2009 Lima, Peru Reprinted in the IVIS website with the permission of the LAVC http://www.ivis.org/
Close this window to return to IVIS www.ivis.org Proceeding of the LAVC Latin American Veterinary Conference Oct. 16-19, 2009 Lima, Peru Reprinted in the IVIS website with the permission of the LAVC http://www.ivis.org/
Blood Cell Identification Graded
 Blood Cell Identification Graded Case History The patient is a 20-year-old female with sickle cell disease who presents with bilateral leg pain for 3 days. She is scheduled to have bilateral hip and leg
Blood Cell Identification Graded Case History The patient is a 20-year-old female with sickle cell disease who presents with bilateral leg pain for 3 days. She is scheduled to have bilateral hip and leg