New Medications and Prescribing Methods for Diabetic Patients
|
|
|
- Myron McGee
- 5 years ago
- Views:
Transcription

1 New Medications and Prescribing Methods for Diabetic Patients Jeffrey Stroup, PharmD, BCPS, FCCP Professor of Medicine Oklahoma State University Center for Health Sciences Department of Internal Medicine
2 Disclosure I have no relevant financial relationships or affiliations with commercial interests to disclose
3 Objectives Identify the sites of action of each of the diabetes treatments Identify contraindications and side effects of each diabetes treatment Differentiate the HbA1C reduction among each of the diabetes treatments Identify and differentiate between diabetes treatments that can cause weight gain or weight loss Identify preferred antihypertensive agents utilized in patients with diabetes Identify preferred lipid agents utilized in patients with diabetes
4 Guidelines-Goals Variable ADA Recommendations Hb A1C * <7.0% (AACE < 6.5%) Preprandial Postprandial LDL* Triglycerides HDL Non-HDL Blood Pressure* mg/dL (AACE <110mg/dL) <180mg/dL (AACE < 140mg/dL) <100mg/dL (<70mg/dL with CVD hx) <150mg/dL >40mg/dL (women > 50mg/dL) <130mg/dL (If TG > 200mg/dL) <140/90 mmhg (<130/80 in some) Al/Cr <30 Other Aspirin, Pneumococcal and Influenza vaccines Diabetes Care. 2018; 41.

5 Approach to the Management of Hyperglycemia Patient/Disease Features Risk of hypoglycemia/drug adverse effects Disease Duration Life expectancy Important comorbidities Established vascular complications more stringent low newly diagnosed long absent absent A1C 7% Few/mild Few/mild less stringent high long-standing short severe severe Patient attitude & expected treatment efforts Resources & support system highly motivated, adherent, excellent self-care capabilities readily available less motivated, nonadherent, poor self-care capabilities limited Glycemic Targets: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S55-S64
6
7 Diabetes Education - Intensive Course for 2-4 weeks with certified diabetic educator - Follow-up every 3 months, more frequent as needed Survival Skills Insulin-preparation and injection Glucometer use and calibration, keeping logs Urine/serum ketone testing Glucagon emergency kit Nutrition Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50


8 Lifestyle Intervention (From the Diabetes Prevention Program) An intensive program with the following specific goals: > 7% loss of body weight and maintenance of weight loss Dietary fat goal: < 25% of calories from fat Calorie intake goal: kcal/day > 150 minutes per week of physical activity The DPP Research Group, NEJM 346: , 2002
9
10 Sulfonylureas Sulfonylureas increase endogenous insulin secretion Sulfonylureas stimulate insulin release by binding to a specific site on the β cell K ATP channel complex (SUR) and inhibiting its activity. K ATP channel inhibition causes cell membrane depolarization and the cascade of events leading to insulin secretion Efficacy Decrease fasting plasma glucose mg/dl Reduce A1C by % Other Effects Hypoglycemia Weight gain* No specific effect on plasma lipids or blood pressure Generally the least expensive class of medication Medications in this Class: First generation sulfonylureas: chlorpropamide (Diabinese) tolazamide acetohexamide (Dymelor) tolbutamide Second generation sulfonylureas: glyburide (Micronase, Glynase, and DiaBeta) glimepiride (Amaryl) glipizide (Glucotrol, Glucotrol XL) Chan JL, Abrahamson MJ. Mayo Clin Proc 2003; 78:
11 Biguanides Biguanides decrease hepatic glucose production and increase insulinmediated peripheral glucose uptake. Metformin has specific actions on mitochondrial respiration that reduce intracellular ATP and increase AMP. Efficacy Decrease fasting plasma glucose mg/dl Reduce A1C % Other Effects Diarrhea and abdominal discomfort Lactic acidosis if improperly prescribed Cause small decrease in LDL cholesterol level and triglycerides No specific effect on blood pressure No weight gain, with possible modest weight loss B12 deficiency reported Contraindicated in patients with an egfr below 30 ml/minute/1.73 m 2.* Starting metformin in patients with an egfr between ml/minute/1.73 m 2 is not recommended. Medications in this Class: metformin (Glucophage) metformin hydrochloride extended release (Glucophage XR) Chan JL, Abrahamson MJ. Mayo Clin Proc 2003; 78:
12 Thiazolidinediones Thiazolidinediones decrease insulin resistance by making muscle and adipose cells more sensitive to insulin. They also suppress hepatic glucose production. Thiazolidinediones are ligands for the PPARγ receptor, a nuclear hormone receptor that has two isoforms and is involved in the regulation of genes related to glucose and lipid metabolism. Efficacy Decrease fasting plasma glucose ~50-80 mg/dl Reduce A1C ~ % 6 weeks for maximum effect Other Effects Weight gain, edema Contraindicated in patients with abnormal liver function or CHF (Class 3-4) Improves HDL cholesterol and plasma triglycerides; usually LDL neutral Medications in this Class: pioglitazone (Actos) bladder cancer warning rosiglitazone (Avandia) cardiovascular disease warning troglitazone (Rezulin) - taken off market due to liver toxicity Chan JL, Abrahamson MJ. Mayo Clin Proc 2003; 78:
13 Meglitinides Meglitinides stimulate insulin secretion (rapidly and for a short duration) in the presence of glucose. Like sulfonylureas, stimulate insulin release by closing K ATP channels in pancreatic β cells Efficacy Decreases peak postprandial glucose Decreases plasma glucose mg/dl ( mmol/l) Reduce A1C % Other Effects Hypoglycemia (although may be less than with sulfonylureas if patient has a variable eating schedule) Weight gain No significant effect on plasma lipid levels Safe at higher levels of serum Cr than sulfonylureas Medications in this Class: repaglinide (Prandin) nateglinide (Starlix) Chan JL, Abrahamson MJ. Mayo Clin Proc 2003; 78:
14 Alpha-glucosidase Inhibitors Alpha-glucosidase inhibitors block the enzymes that digest starches in the small intestine α-glucosidase inhibitors reduce intestinal absorption of starch, dextrin, and disaccharides by inhibiting the action of α-glucosidase in the intestinal brush border Efficacy Decrease peak postprandial glucose mg/dl Decrease fasting plasma glucose (no sig effect) Decrease A1C % Other Effects Flatulence or abdominal discomfort No specific effect on lipids or blood pressure No weight gain Contraindicated in patients with inflammatory bowel disease or cirrhosis Medications in this Class: acarbose (Precose) miglitol (Glyset) Chan JL, Abrahamson MJ. Mayo Clin Proc 2003; 78:

15 Effects of Glucagon-like peptide-1 Idris I and Donnelly R. Diabetes Obes Metab. 2007;9:
16 Incretin Mimetics Efficacy Hemoglobin A1c lowering of 0.8% 1.9% Primarily a postprandial glucose reduction with exenatide BID Less postprandial and greater fasting glucose reduction with liraglutide and weekly products Dose Exenatide (Byetta): 5 mcg subcutaneously 2 times/day (thigh, abdomen, or upper arm) 1 60 minutes before morning and evening meals, increase to 10 mcg 2 times/ day after 4 weeks if tolerated Liraglutide (Victoza): 0.6 mg subcutaneously every day (independent of meals; inject into thigh, abdomen, or upper arm); increase by weekly intervals to 1.2 mg subcutaneously every day; then 1.8 mg subcutaneously every day if needed
17 Dose Incretin Mimetics Exenatide LAR (Bydureon): 2 mg subcutaneously weekly (thigh, abdomen, or upper arm); two weeks before see effect (6-8 weeks full effect) Albiglutide (Tanzeum): 30 mg subcutaneously weekly (independent of meals; inject into thigh, abdomen, or upper arm); can increase to 50 mg after 4 weeks if needed. Dulaglutide (Trulicity): 0.75 mg subcutaneously weekly (independent of meals; inject into thigh, abdomen, or upper arm); can increase to 1.5 mg after 4 weeks if needed.
18 Incretin Mimetics Adverse Effects GI: Nausea, Vomiting, Diarrhea Headache Rare: Pancreatitis/Renal dysfunction Contraindications Gastroparesis Creatinine clearance < 30 ml/minute: Exenatide and Exenatide LAR Medullary thyroid carcinoma (MTC), personal or family history, or in patients with multiple endocrine neoplasia syndrome type 2 (MEN2): Liraglutide and Weekly products Pancreatitis
19 Incretin Mimetics Advantages Use is associated with weight loss (2-3 kg) Convenient dosing B-cell sparing effect? Disadvantages Parenteral administration Gastrointestinal adverse effects May reduce the rate and extent of absorption of drugs that require rapid absorption (pain relievers, antibiotics, and oral contraceptives); separate administration by at least 1 hour Cost
20 GLP-1 Comparison Chart Drug Byetta Bydureon Tanzeum Trulicity Victoza Generic exenatide exenatide albiglutide dulaglutide liraglutide Dosing Frequency Dosing Mixing Required Waiting Time post mixing Twice daily 5 mcg 10 mcg Weekly Weekly Weekly Daily 2 mg 30 mg 50 mg 0.75 mg 1.5 mg No Yes Yes No No None None 15 or 30 minutes None 0.6 mg 1.2 mg 1.8 mg None Needle Size 32 g; 4mm 23 g; 8 mm 29 g; 5 mm 29 g;built-in 32 g; 4 mm Auto-injector No No No Yes No Use with basal insulin Yes No Yes No Yes





21 GLP-1=glucagon-like peptide-1; GIP=glucose-dependent insulinotropic polypeptide. Mechanism of Action of DPP-IV Inhibitors GI tract Ingestion of food Release of active incretins GLP-1 and GIP DPP-4 inhibitor Inactive GLP-1 X DPP-4 enzyme Inactive GIP Pancreas Beta cells Alpha cells Glucosedependent Glucose dependent Insulin (GLP-1and GIP) Glucagon (GLP-1) Glucose uptake by peripheral tissue Hepatic glucose production Blood glucose in fasting and postprandial states Incretin hormones GLP-1 and GIP are released by the intestine throughout the day, and their levels in response to a meal.
22 Pharmacology JANUVIA (SITAGLIPTIN) ONGLYZA (SAXAGLIPTIN) TRADJENTA (LINAGLIPTIN) NESINA (ALOGLIPTIN) Dosing Frequency Dosage 25, 50, 100 mg 2.5 & 5 mg 5 mg 6.25, 12.5, 25 mg Half-life (hours) (active metabolite= 3.1) Metabolism Not extensively metabolized CYP3A4/5 > (active metabolite) Not extensively metabolized CYP2D6/3A4 Majority of Elimination Dose Adjustment in CKD/ESRD Renal Renal Bile Renal -- Combination Products




23 DPP-IV Inhibitors Good vs. Bad Low risk of hypoglycemia Weight neutral Once daily ORAL Well tolerated URI Nasal pharyngitis Headache Hypersensitivity Pancreatitis

24 Incretin Comparison GLP-1 Activation DPP-IV Inhibition Insulin Glucagon Gastric emptying Hypoglycemia +/- -- Nausea/Vomiting Weight Loss No Change Route of admin Injection Oral
25 Other Available Agents Pramlintide (Symlin ) Used in type 1 and type 2 diabetes Amylin analog (hormone co-secreted with insulin) Injectable three times daily Weight loss Colesevelam (Welchol ) Lipid agent Used in type 2 diabetes A1c reduction ~0.5% Bromocriptine (Cycloset ) Dopamine receptor agonist Used in type 2 diabetes A1c reduction ~0.5%
26 Sodium- Glucose Cotransporters Site SGLT1 Mostly intestine with some kidney SGLT2 Sugar Specificity Glucose or galactose Glucose Affinity for glucose Capacity for glucose transport Role High Km= 0.4 Mm Low Dietary glucose absorption Renal glucose reabsorption Almost exclusively kidney Low Km = 2 Mm High Renal glucose reabsorption Lee YJ, at al. Kidney Int Suppl. 2007;72:S27-S35.

27 Targeting the Kidney Chao EC, et al. Nat Rev Drug Discovery. 2010;9:
28 Effects of SGLT2 Inhibitors Inhibition of renal tubular Na + - glucose cotransporter reversal of hyperglycemia reversal of glucotoxicity Insulin sensitivity in muscle GLUT4 translocation Insulin signaling Insulin sensitivity in liver Glucose-6-phosphatase Gluconeogenesis Decreased Cori Cycle PEP carboxykinase Improved beta cell function DeFronzo RA, et al. Diabetes Obes Metab. 2012;14(1):5-14.
29 Sodium-Glucose co-transporter 2 Inhibitors. Mechanism of Action Blocks SGLT-2 receptors in the proximal tubule thus inhibiting renal reabsorption of glucose. This results in glycosuria, as well as salt and water loss. Efficacy Hemoglobin A1c lowering of 0.7% 1.1%. Lowers fasting and postprandial glucose levels Weight loss BP reduction Dose Canagliflozin (Invokana): 100 mg once daily; may increase to 300 mg Dapagliflozin (Farxiga): 5 mg once daily; may increase to 10 mg Empagliflozin (Jardiance): 10 mg daily once daily; may increase to 25 mg
30 Dose Adjustments for Renal Insufficiency egfr (ml/min/1.73m 2) Canagliflozin (Invokana) Dapagliflozin (Farxiga) Empagliflozin (Jardiance) > 60 No dosage adjustment No dosage adjustment No dosage adjustment mg daily Not recommended for egfr <60 No dosage adjustment < 45 Not recommended Not recommended Not recommended INVOKANA [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; FARXIGA [prescribing information]. Bristol-Myers Squibb & AstraZeneca Pharmaceuticals, Inc.; JARDIANCE [prescribing information]. Boehringer Ingelheim Pharmaceuticals, Inc. & Eli Lilly and Company; 2014.
31
32 SGLT-2 Inhibitors Adverse Effects Genital mycotic infections Women: % (SGLT2) vs % (placebo) Men (more common if uncircumcised): % (SGLT2) vs % (placebo) Urinary tract infections % (SGLT2) vs % (placebo) Polyuria Risk of hypotension and hypovolemia due to osmotic diuresis Euglycemic ketoacidosis (EKA, eudka) Invokana PI; Farxiga PI; Jardiance PI
33 SGLT-2 Inhibitor Summary Advantages Once daily oral administration Effect independent of insulin secretion or insulin resistance Low risk of hypoglycemia Decreases both FBG and PPG Weight Loss (2-3kg) Blood pressure lowering (~5 mmhg SBP) Concerns Polyuria (additional ml/day) Dehydration Hypotension Genital mycotic infection Urinary tract infection
34 The History of Insulins 1889: Pancreas & DM 1951: Lente insulins 1921: Extraction of insulin 1970 s: Single source insulins 1980 s: Premixed insulin. 1922: 1st successful use Human insulin of insulin 1990 s: Insulin Analogs s: Joslin advocates (Quick-acting insulin). tight glycemic control DCCT/UKPDS 1936: PZI insulin 2000: Basal Insulin. DCCT/EDIC 1946: NPH insulin 2006: Inhaled Insulin


35 Insulin Therapy in Type 2 Diabetes Arguments for Earlier Use
 or substituting Asp for Pro 28B (aspart) gives analogues with reduced tendencies for molecular self-association that are faster acting.")
36 Insulin analogues. Modifications of native insulin can alter its pharmacokinetic profile. Reversing amino acids 28 and 29 in the B chain (lispro) or substituting Asp for Pro 28B (aspart) gives analogues with reduced tendencies for molecular self-association that are faster acting. Altering Asp 3B to Lys and Lys 29B to Glu produces an insulin (glulisine) with a more rapid onset and a shorter duration of action. Substituting Gly for Asn 21A and lengthening the B chain by adding Arg 31 and Arg 32 produces a derivative (glargine) with reduced solubility at ph 7.4 that is, consequently, absorbed more slowly and acts over a longer period of time. Deleting Thr 30B and adding a myristoyl group to the ε-amino group of Lys 29B (detemir) enhances reversible binding to albumin, thereby slowing transport across vascular endothelium to tissues and providing prolonged action. Insulin degludec is LysB29(Nεhexadecandioyl-γ-Glu) des(b30) human insulin. When degludec is injected subcutaneously, it forms multihexameric complexes that slow absorption; degludec also binds well to albumin; these two characteristics contribute to the prolonged effect of degludec (>24 h at steady state).
37 Comparison of Human Insulins Insulin Onset Peak Duration Lispro, Aspart, Glulisine 5-15 mins 1-2 hrs 3-5 hrs Inhaled Insulin Minutes min 2-3 hrs Human Regular mins 2-4 hrs 6-8 hrs Human NPH 1-2 hrs 6-12 hrs hrs Insulin Detemir 3-4 hrs Peakless hrs Insulin Glargine 4-6 hrs Peakless ~24 hrs Glargine U300 6 hrs Peakless ~30-36 hrs Insulin Degludec 6 hrs Peakless ~42 hrs
38 Profiles Human Insulin and Analogs Aspart, Lispro, Glulisine Regular Plasma insulin levels NPH Detemir Glargine Rosenstock J. Clin Cornerstone. 2001;4:50. Hours
39 Mimicking Nature Breakfast Lunch Dinner Insulin Action 4:00 8:00 12:00 16:00 20:00 24:00 4:00 8:00 Time Adapted with permission from Leahy J. In: Leahy J, Cefalu W, eds. Insulin Therapy. New York: Marcel Dekker; 2002:87; Nathan DM. N Engl J Med. 2002;347:1342
40 Evening Basal Insulin Bedtime NPH µu/ml B L D Normal pattern NPH Time of day B=breakfast; L=lunch; D=dinner
41 Split-Mixed Regimen Human Insulins µu/ml NPH Regular B L D NPH Regular Normal pattern Time of day B=breakfast; L=lunch; D=dinner
42 Multiple Daily Injections Human Insulins µu/ml NPH Regular Regular Regular NPH B L D Normal pattern B=breakfast; L=lunch; D=dinner Time of day
43 Basal-Bolus Insulin Treatment With Insulin Analogues µu/ml Lispro, glulisine, or aspart B L D Glargine qd or Detemir qd or bid Normal pattern Time of day B=breakfast; L=lunch; D=dinner
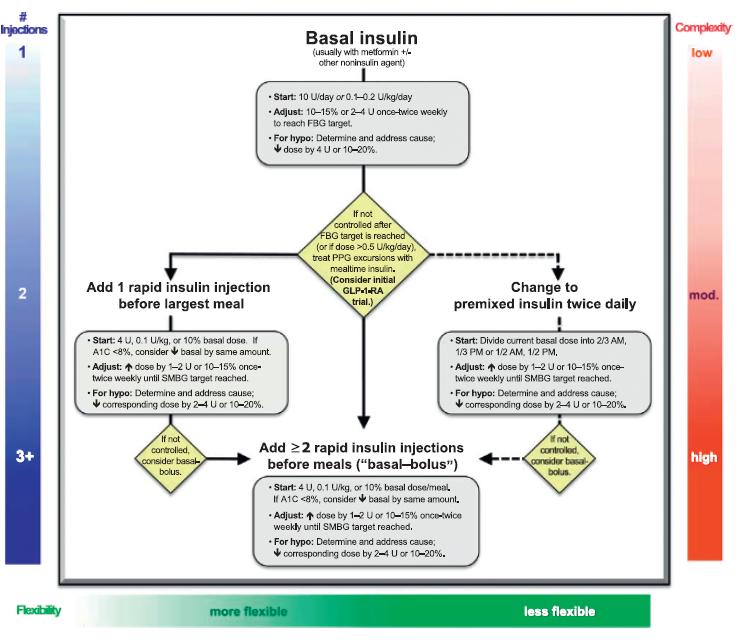
44 How To Initiate Insulin Therapy? Type 1 Patients Utilize a Basal/Bolus Approach Target Fasting & Postprandial Blood Sugars Type 2 Patients Failing Oral Therapy 1 st Target Fasting Blood Sugar Forced Titration Schedule
45 Initiating Insulin Therapy Empiric Dosing (daily dose) Insulin Analogues Type 1: 0.5 units/kg/d Type 2: units/kg/d (obesity, activities) Give 50% as Basal Insulin Give 50% as Bolus Insulin Split into three doses Adjust accordingly: Carbohydrate Counting
46 Initiating Basal Insulin Therapy Suppresses glucose production between meals and overnight Continue oral agent(s) at same dosage (may eventually reduce) Add single bedtime insulin dose (10 20 Units) [weight based at 0.2U/kg] Glargine Detemir NPH Adjust dose according to Fasting Blood Sugars Adjust the insulin dose every 3-4 days as needed Increase 2 U if FBG mg/dl Increase 4 U if FBG mg/dl Increase 6 U if FBG mg/dl Increase 8 U if FBG >180 mg/dl Treat to target (usually FPG mg/dl)
47 Riddle MC et al. Diabetes Care. 2003;26: Rosenstock J et al. Diabetologia. 2008;51: Treat to Target
48 Prandial Insulin Dose Adjustments Prandial insulin limits hyperglycemia after meals Set dose with meals Example dosing: 2-5 units with each meal to start Carbohydrate counting Typical start: 1 unit for every 10-15g of carbohydrate Correction scales
49 Initiating Pre-Meal Dosing Discontinue SFU or Meglitinide Initiate with the largest meal Once at goal, move to the next largest meal Diabetes Obes Metab. 2008; 10:
50 Humulin 70/30 70% NPH, 30% Regular Humulin 50/50 50% NPH, 50% Regular Humalog Mix 75/25 Mixed Insulins 75% lispro protamine, 25% lispro Humalog Mix 50/50 50% lispro protamine, 50% lispro Novolin 70/30 70% NPH, 30% Regular Novolog Mix 70/30 70% aspart protamine, 30% aspart

51 Respiratory Tract Surface Area - Total surface area of lungs = 140m 2 - Alveoli = regulation tennis court - Bronchi= blue towel

52 Insulin Human Inhalation Powder Inhaled, ultra-rapid-acting mealtime insulin Indicated for adults with T1DM or T2DM Administer at beginning of each meal 4 (blue), 8 (green), and 12 (yellow) unit packets Foil package; 2 blister cards, 15 cartridges each; strips of three; 2 inhalers. Dosing Insulin-naive patients: 4 units before each meal Prandial SC insulin users: convert 1:1 (round up to nearest 4 units) Afrezza Prescribing Information. October 2014.
53
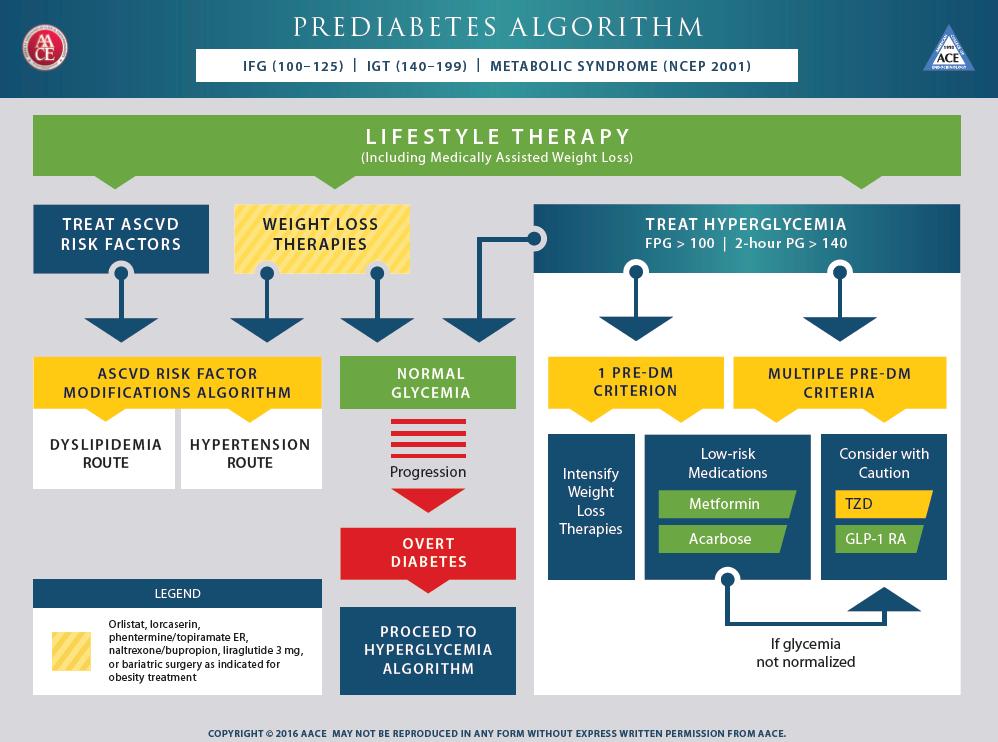
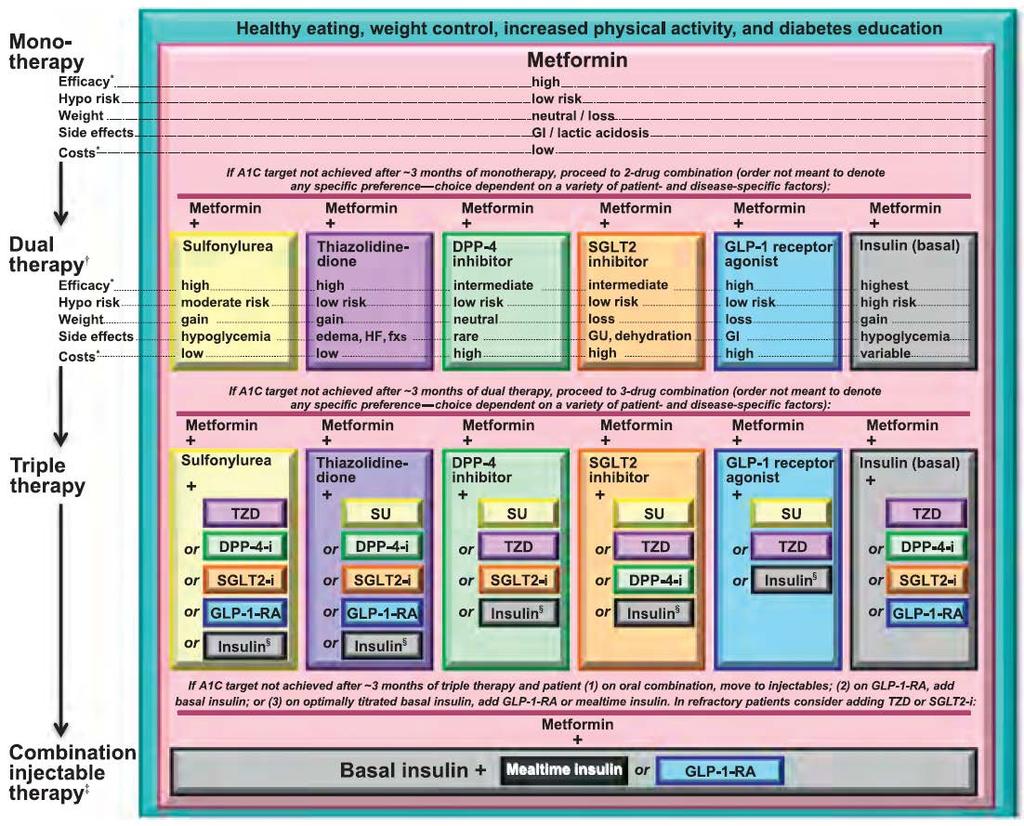
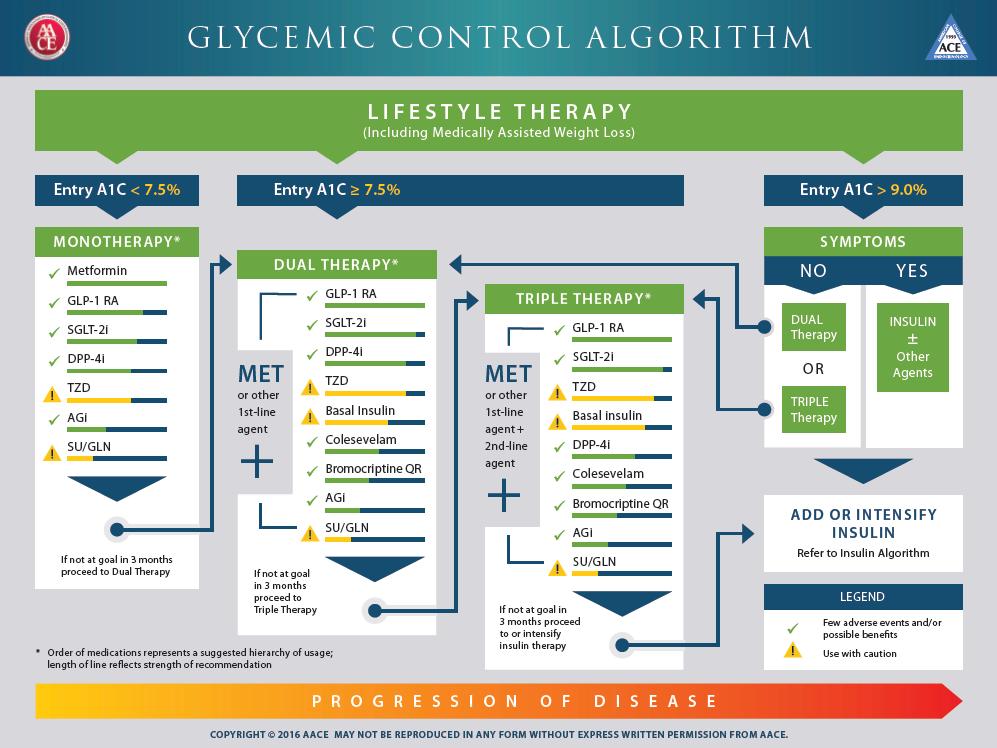
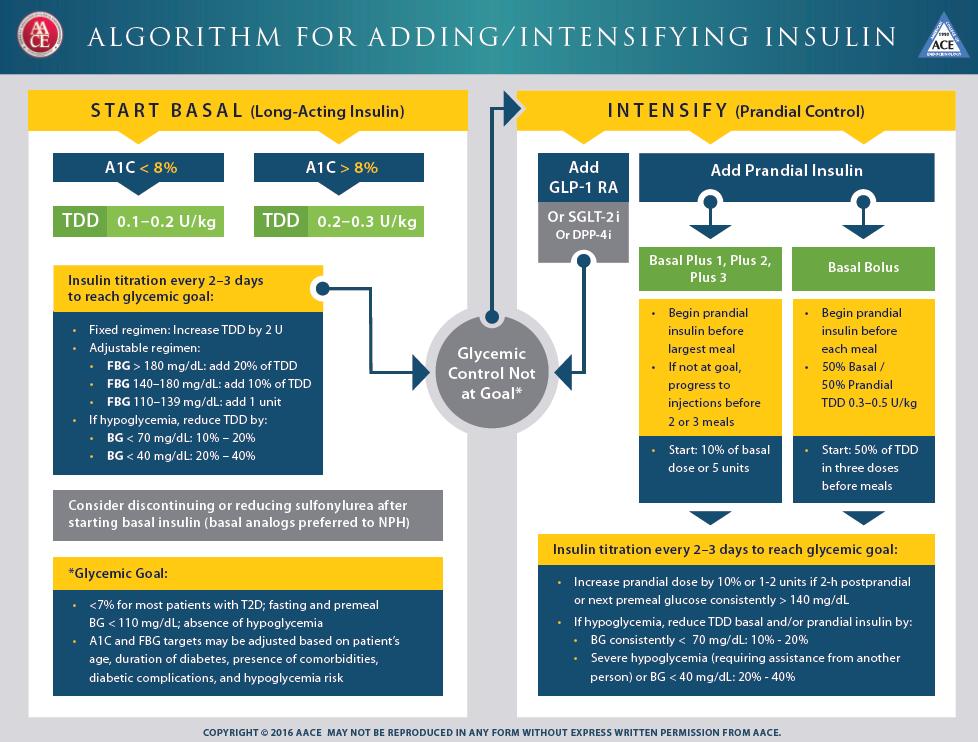
54 Treatment Guideline Algorithms American Diabetes Association American Association of Clinical Endocrinologists*

55
56
57
58
59
60 Which of the following drugs used in treatment of Type 2 DM is consistently associated with weight loss? 1. Sulfonylureas 2. Thiazolidinediones 3. Glucagon-like peptide 1 analogs 4. Insulin
61 Which of the following treatments for Type 2 DM is associated with the most profound reduction in HbA1c? 1. Metformin 2. Insulin 3. Sulfonylureas 4. Thiazolidinediones
62 Which of the following agents is contraindicated with Class 3 or 4 Heart Failure? 1. Thiazolidinediones 2. Insulin 3. Sulfonylureas 4. Bromocriptine
63 Which of the following classes of diabetes medications works primarily at the level of the kidney? 1. DPP-IV inhibitors 2. Sulfonylureas 3. Insulin 4. SGLT-2 inhibitors
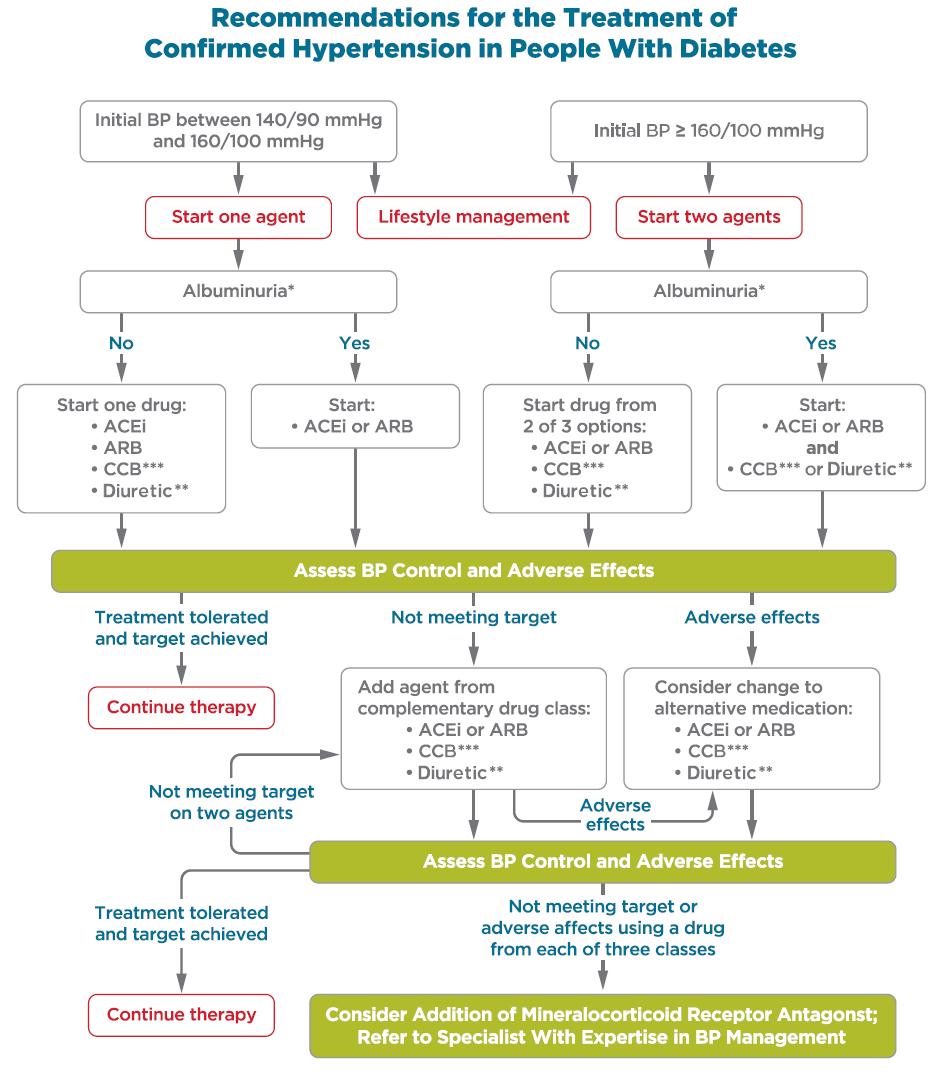
64 ADA Recommendations-HTN
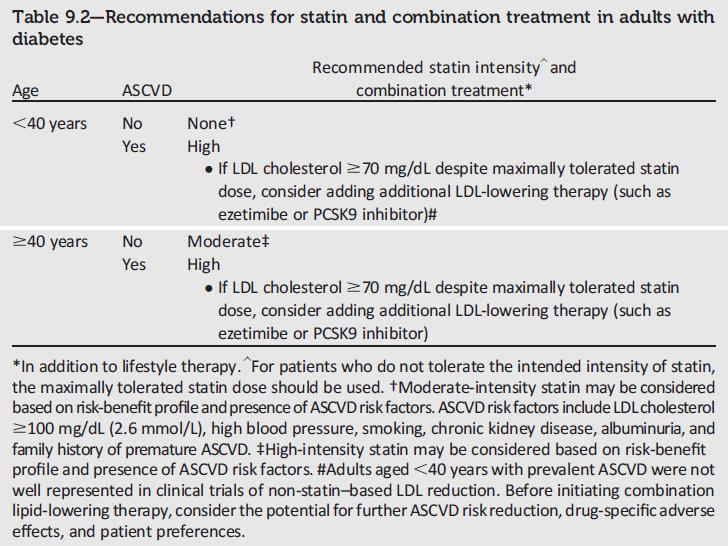
65 ADA Recommendations-Statins

66 High- and Moderate-Intensity Statin Therapy Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
67
68 Which of the following agents is preferred as an antihypertensive in patients with diabetes? 1. Beta blockers 2. ACE Inhibitors 3. Loop Diuretics 4. Hydralazine

69 QUESTIONS
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Oral Medication for the Management of Diabetes Mechanism of. Duration of Daily Dosing Action
 Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
Non-Insulin Diabetes Medications Summary
 Non-Insulin Diabetes Medications Summary Medications marked with an asterisk (*) can cause hypoglycemia INSULIN SECRETAGOGUES Sulfonylureas* GLYBURIDE* (Diabeta) (Micronase) production. Side effects: Potential
Non-Insulin Diabetes Medications Summary Medications marked with an asterisk (*) can cause hypoglycemia INSULIN SECRETAGOGUES Sulfonylureas* GLYBURIDE* (Diabeta) (Micronase) production. Side effects: Potential
Diabetes Medications: Oral Anti-Hyperglycemic Medications
 Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018
 Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
4/9/2018 HOW TO REGULATE DIABETES MEDICATIONS. By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE. Diagnosis
 HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions. Insulins. Rapid Short Intermediate Long Mix
 Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Type II Diabetes Improving Blood Sugar Control. Geneva Clark Briggs, Pharm.D., BCPS
 Type II Diabetes Improving Blood Sugar Control Geneva Clark Briggs, Pharm.D., BCPS Overview Importance of glucose control State of control Review available therapies Helping patients achieve control The
Type II Diabetes Improving Blood Sugar Control Geneva Clark Briggs, Pharm.D., BCPS Overview Importance of glucose control State of control Review available therapies Helping patients achieve control The
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
New Therapies for Diabetes
 Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Diabetes Treatment Guidelines
 Diabetes Treatment Guidelines For more comprehensive information about current approaches to the diagnosis and treatment of diabetes, visit the American Diabetes Association Standards of Medical Care 2018
Diabetes Treatment Guidelines For more comprehensive information about current approaches to the diagnosis and treatment of diabetes, visit the American Diabetes Association Standards of Medical Care 2018
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD. Disclosures. Objectives 9/1/2015
 Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
DIABETES. Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes. November 2013
 DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Physician Drug Reference Chart for Diabetes Antidiabetic Medications
 Drug Class Compound Brand Name Mechanism of Action Advantages Disadvantages Alpha-glucosidase inhibitors Medium Cost by Bayer Healthcare, Pfizer, Takeda Research Acarbose Miglitol Voglibose Precose Glyset
Drug Class Compound Brand Name Mechanism of Action Advantages Disadvantages Alpha-glucosidase inhibitors Medium Cost by Bayer Healthcare, Pfizer, Takeda Research Acarbose Miglitol Voglibose Precose Glyset
第十五章. Diabetes Mellitus
 Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes
 Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes Timothy S. Reid, M.D. Mercy Diabetes Center Janesville, WI Duality Statement Dr. Reid is a Speaker and Consultant
Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes Timothy S. Reid, M.D. Mercy Diabetes Center Janesville, WI Duality Statement Dr. Reid is a Speaker and Consultant
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Pharmacologic Agents for Treatment of Type 2 Diabetes
 Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
2/9/2016. The Evolving Armamentarium for Type 2 Diabetes: Incorporating New Classes in the Treatment of Our Patients. Objectives: Pharmacists
 WAYNE STATE UNIVERSITY COLLEGE OF PHARMACY & HEALTH SCIENCES FEBRUARY 28, 2016 The Evolving Armamentarium for Type 2 Diabetes: Clinical Assistant Professor, Department of Pharmacy Practice Ambulatory Care
WAYNE STATE UNIVERSITY COLLEGE OF PHARMACY & HEALTH SCIENCES FEBRUARY 28, 2016 The Evolving Armamentarium for Type 2 Diabetes: Clinical Assistant Professor, Department of Pharmacy Practice Ambulatory Care
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Diabetes Management: A diagnostic perspective
 Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Pancreatic b-cell Dysfunction in Type 2 Diabetes ZIAD KAHWASH, M.D. Insulin resistance: Defects in Insulin Signaling
 Plasma insulin (mu/ml) ZIAD KAHWASH, M.D. resistance: Defects in Signaling Increased glucose production Glucose Insufficient glucose disposal X Liver glucagon insulin Pancreas Peripheral tissues (skeletal
Plasma insulin (mu/ml) ZIAD KAHWASH, M.D. resistance: Defects in Signaling Increased glucose production Glucose Insufficient glucose disposal X Liver glucagon insulin Pancreas Peripheral tissues (skeletal
Advanced Practice Education Associates. Endocrine
 Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control
 Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
1/15/2018. Disclosures. Current Diabetes Medications. Objectives NON-INSULIN AGENTS. Diabetes Med Classes. Mealtime
 Disclosures Current Diabetes Medications None Claire Baker, M.D. Diabetes & Endocrine Associates January 24, 2018 Objectives Identify categories of diabetes medications Understand the pharmacology of diabetes
Disclosures Current Diabetes Medications None Claire Baker, M.D. Diabetes & Endocrine Associates January 24, 2018 Objectives Identify categories of diabetes medications Understand the pharmacology of diabetes
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Antidiabetic Agents CHAPTER BIGUANIDES
 ajt/shutterstock, Inc. CHAPTER 2 Antidiabetic Agents Charles Ruchalski, PharmD, BCPS BIGUANIDES For newly diagnosed patients with type 2 diabetes, the biguanide metformin is the drug of choice for initial
ajt/shutterstock, Inc. CHAPTER 2 Antidiabetic Agents Charles Ruchalski, PharmD, BCPS BIGUANIDES For newly diagnosed patients with type 2 diabetes, the biguanide metformin is the drug of choice for initial
How to Fight Diabetes and Win. Diabetes. Medications
 How to Fight Diabetes and Win Diabetes Medications MEDICATIONS FOR DIABETES According to the American Diabetes Association, 85% of adults diagnosed with diabetes take insulin and/or oral medication to
How to Fight Diabetes and Win Diabetes Medications MEDICATIONS FOR DIABETES According to the American Diabetes Association, 85% of adults diagnosed with diabetes take insulin and/or oral medication to
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Pharmacology. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea
Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18
 Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18 No conflicts of interest Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM ADA
Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18 No conflicts of interest Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM ADA
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Update on Diabetes Mellitus
 Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Oral and Injectable Medication Options for Diabetes Treatment
 Oral and Injectable Medication Options for Diabetes Treatment Presented by: Dr. Daphne E. Smith, Pharm.D., CDE Clinical Assistant Professor/Clinical Pharmacist-University of Illinois at Chicago College
Oral and Injectable Medication Options for Diabetes Treatment Presented by: Dr. Daphne E. Smith, Pharm.D., CDE Clinical Assistant Professor/Clinical Pharmacist-University of Illinois at Chicago College
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes. Overview. Prevalence of Overweight in the U.S.
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Diabetes Family Medicine Board Review
 Diabetes Family Medicine Board Review Sarah Kim, MD Associate Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March 21, 2018 No disclosures Diabetes Test Topics Majority Type
Diabetes Family Medicine Board Review Sarah Kim, MD Associate Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March 21, 2018 No disclosures Diabetes Test Topics Majority Type
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Diabetes Family Medicine Board Review
 Diabetes Family Medicine Board Review Sarah Kim, MD Assistant Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March 10, 2016 No disclosures Diabetes Test Topics Majority Type
Diabetes Family Medicine Board Review Sarah Kim, MD Assistant Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March 10, 2016 No disclosures Diabetes Test Topics Majority Type
Diabetes Mellitus. Intended Learning Objectives:
 Intended Learning Objectives: Diabetes Mellitus 1. Compare and contrast the differences between the drug therapy recommendations of several of the latest and leading diabetes guidelines. 2. Assess the
Intended Learning Objectives: Diabetes Mellitus 1. Compare and contrast the differences between the drug therapy recommendations of several of the latest and leading diabetes guidelines. 2. Assess the
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
2018 Diabetes Summit Managing Diabetes: An Art and a Science
 2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
No disclosures. Diabetes Test Topics. Case #1. Diabetes Family Medicine Board Review: Improving Clinical Care Across the Lifespan
 Diabetes Family Medicine Board Review: Improving Clinical Care Across the Lifespan No disclosures Sarah Kim, MD Assistant Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March
Diabetes Family Medicine Board Review: Improving Clinical Care Across the Lifespan No disclosures Sarah Kim, MD Assistant Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
3/22/2017. Type 2 Diabetes Pathophysiology and Pharmacology Review. Accreditation Statement
 Type 2 Diabetes Pathophysiology and Pharmacology Review Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA This
Type 2 Diabetes Pathophysiology and Pharmacology Review Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA This
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Endo 2 SLO Practice (online) Page 1 of 7
 Page 1 of 7") Endo 2 SLO Practice (online) Page 1 of 7 1. A long- acting insulin, like Lantus is for? A. When the next meal is within 30-60 minutes of the injection B. Over night use or for ½ of the day often combined
Endo 2 SLO Practice (online) Page 1 of 7 1. A long- acting insulin, like Lantus is for? A. When the next meal is within 30-60 minutes of the injection B. Over night use or for ½ of the day often combined
A New Therapeutic Strategey for Type II Diabetes: Update 2008
 Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes