Rebound Intracranial Hypertension Following Treatment of Spinal CSF Leaks
|
|
|
- Ambrose Carson
- 5 years ago
- Views:
Transcription
1 Rebound Intracranial Hypertension Following Treatment of Spinal CSF Leaks Deborah I. Friedman, MD, MPH University of Texas Southwestern Medical Center Dallas, Texas
2 Disclosures (past 2 years): Role Advisory Board Organization Alder BioPharmaceuticals, Amgen, Avanir, Biohaven Pharmaceuticals, electrocore, Eli Lilly, Supernus, Teva, Zosano Speaker Consultant Grant support Support: Clinical trial site PI Board of Directors Editorial Board Contributing author Allergan, Amgen, Avanir, electrocore, Supernus, Teva Avanir, Eli Lilly, electrocore, Autonomic Technologies, Inc. Merck Eli Lilly, Autonomic Technologies, Inc, Zosano American Headache Society, Spinal CSF Leak Foundation Headache, Neurology Reviews Medlink Neurology, Medscape
3 Other Disclosures There are no FDA approved medications indicated for the treatment of (headaches associated with) intracranial hypertension Due to limited literature on this subject, much of the content is my opinion based on experience treating patients with the pseudotumor cerebri syndrome (idiopathic intracranial hypertension) and those with rebound intracranial hypertension.
4 Learning Objectives Describe the differential diagnosis of rebound intracranial hypertension Develop a rational strategy for headache management in patients with RIH
5 Case Presentation 46-year-old woman with orthostatic headaches for 10 years Occurred after being upright for 6-7 hours, 7 out of 10 Top of head, sharp with nuchal aching Photophobia, constant tinnitus; pulsatile tinnitus in the AM Daily, constant Relieved only with sleep and at high altitude Also with occipital headaches and interscapular tension and burning neck pain
6 1 year prior she work up two days in a row with a wet ear and a halo of blood and clear liquid on the pillowcase Headaches worsened after this Evaluation for skull base CSF leak was negative Started on topiramate 100 mg daily LP 5 years prior for possible IIH showed OP 150 mm CSF CT myelogram showed multiple perineural cysts but no leak Headaches improved for 1 month after non-targeted blood patch

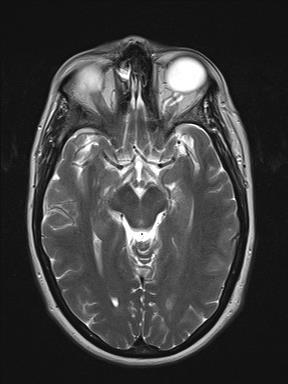
7 Imaging 2 years prior
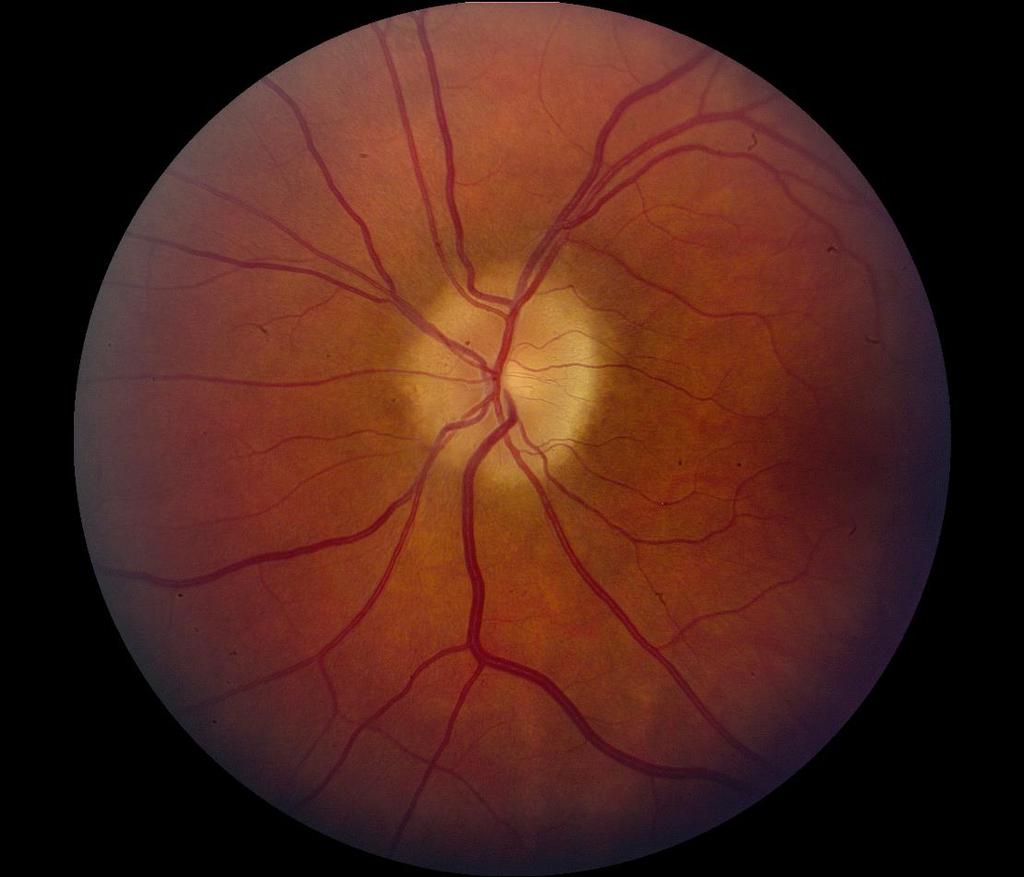
8 PMHx: Ehlers Danlos syndrome Exam: BMI 28 kg/m 2 Normal optic nerves with spontaneous venous pulsations Normal neuro exam Trendelenburg test: 7 5 out of 10 in 10 minutes

9 Targeted blood patch of perineural cyst at T10-11 gave short-lived relief Topiramate discontinued for possible exacerbation of intracranial hypotension Subsequent blood patches with relief for 5-9 weeks.
10 Developed a different headache 10 days after her last blood patch Worse when lying flat Awakened with headache that resolved minutes of being upright, then the previous orthostatic headache began 4 hours later More history. Gained 30 pounds after stopping topiramate Life long history of transient visual obscurations when standing

11
12 Characteristics of Rebound Intracranial Hypertension (RIH) Headaches Usually occur within hours to days of epidural blood patch (or surgery) Headache phenotype is completely different than SIH headache Location (often frontal or retro-orbital) Orthostatic component disappears May be worse upon awakening Patients may be unable to sleep flat Kranz PG et al. AJNR 2014;35:
13 Why Does RIH Occur? 1. Overcorrection of SIH (mechanism uncertain) Disrupted spinal CSF absorption from blood patch Upregulation of CSF production (unlikely) 2. The primary problem was unrecognized intracranial hypertension Self decompression via spinal CSF leak (Optic nerve sheath, sella, skull base leak, spinal leak)
 Locations of headache: Frontal 68% Ocular 47% (usually bilateral) Nuchal 47% Unilateral 30% Posterior 39%")

14 High Pressure Headaches in IIH: IIHTT Headache Characteristics at Baseline (n=165) HA present in 84% at baseline (70 ACZ, 69 PBO) Locations of headache: Frontal 68% Ocular 47% (usually bilateral) Nuchal 47% Unilateral 30% Posterior 39% Global 36% Characterization of pain: Pressure-like 47% Throbbing 42% Stabbing 5% Wall M et al. JAMA 2014;311: Friedman DI et al. Headache 2017;57: Yunisova G et al. Headache 2017;57: ACZ = Acetazolamide, PBO = placebo
15 IIH-related symptoms Constant visual loss (34%) Transient visual obscurations (68%) Diplopia (22%) Dizziness (53%) Headache with none of the above (14%)
16 Migraine associated symptoms were common (86%): Photophobia (70%), phonophobia (52%), nausea (47%), vomiting (17%), worsened with routine physical activity (50%) Headache phenotype (ICHD -3 beta) Migraine 52% Probable migraine 16% Tension-type 22% Probable tension-type 4% Not classifiable 7% Friedman DI et al. Headache 2017;57:

17 Why Does IIH Cause Headaches? Pain sensitive structures in the brain Meninges Veins Increased central venous pressure Venous sinus stenosis Central sensitization?
18 Was IIH the Initial Problem? Clues on History and Exam Prior diagnosis of IIH/PTCS Obesity or recent weight gain Other risk factors for IIH (cyclines, vitamin A, etc.) Undiagnosed/untreated sleep apnea History (or symptoms of) prior skull base leak CSF rhinorrhea or otorrhea Other IIH symptoms in the past Pulsatile tinnitus Friedman DI, Liu G, Digre KB. Neurology 2013;81:
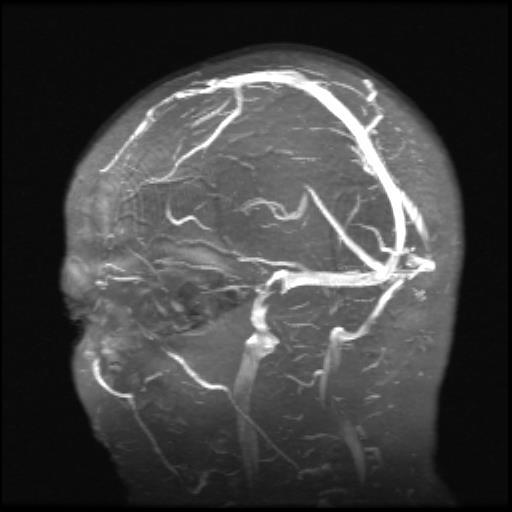
19 Previous imaging signs of increased ICP The opposite of what is seen in SIH: Empty sella Expanded perioptic subarachnoid space Tortuous optic nerve Venous sinus stenosis Tonsillar descent can occur with high or low pressure No other evidence of brain sag





20 Imaging Abnormalities* Protrusion of optic nerve papilla into the vitreous, flattening of posterior sclera, expanded and tortuous optic nerve sheath complex Expanded/empty sella Flattening of posterior sclerae where optic nerve leaves the globe *in the appropriate clinical context Bidot S et al. J Neuro-ophthalmol 2-15;35: Agid R, Farb RI. Minerva Med 2006;97:365-70


21 Neuro-Ophthalmic Symptoms and Signs Transient obscurations of vision Blurred vision Visual field defects Binocular diplopia Usually horizontal Abducens palsy Loss of previously present spontaneous venous pulsations Papilledema Mokri B. Mayo Clin Proc 2002;77:1241-6




22 Papilledema Helpful: Disc elevation, obliteration of optic cup Peripapillary halo, obscuration of vessels crossing the disc margin Normal Grade 2 Grade 3 Grade 4 Grade 5
23 Treatments Discontinue caffeine Low sodium diet Sleep reclining or sitting, elevate head of bed Sleep apnea evaluation/treatment as indicated Therapeutic lumbar puncture Medical management CSF pressure-lowering agents (oral; IV glycerol helpful in one case report of RIH) Management of IIH (e.g., weight loss) Procedural options Tsui H et al. EurJ Neurol 2006;13: Friedman DI. Continuum 2018;24:
 Third choice: Furosemide or bumetanide Fourth choice: You choose Allergic patient (no cross reaction with sulfa antibiotics): Triamterene")
24 Medical Management of CSF Pressure First choice: Acetazolamide Starting dose (adults) 500 mg BID Titrate up to 2000 mg BID as tolerated Second choice: Methazolamide Starting dose 25 mg BID Titrate up to mg BID as tolerated (not renally excreted) Third choice: Furosemide or bumetanide Fourth choice: You choose Allergic patient (no cross reaction with sulfa antibiotics): Triamterene Spironolactone (also good for PCOS) Ethacrynic acid Be careful if combining diuretics!
25 Considerations for Headache Treatment Headache Phenotype ICHD classification Location, character of pain, duration, associated features (nausea, photophobia, phonophobia, etc.) Migraine Tension-type Hemicrania continua
26 Symptomatic Treatment of Headache Naproxen Acetaminophen Other NSAIDs Indomethacin may lower ICP Triptans, dihydroergotamine (migraine phenotype or previous history of migraine) Avoid butalbital, caffeine Avoid opioids if possible although may be needed short-term Antiemetics as needed
27 Preventive Medications Headaches at least once a week Symptomatic medications >3 days weekly Start low, go slow Leverage possible side effects - many cause weight gain Silberstein SD et al. Neurology 2012;78: Holland S et al. Neurology 2012;78:
28 Medications Advantages Disadvantages Comments Topiramate Zonisamide Weight loss pcsf lowering effect Tolerability Renal stones Pregnancy TCAs (low dose) Sleep disturbance Weight gain with higher doses Indomethacin May lower pcsf Tolerability Naproxen No adverse effect on weight loss in IIHTT OnabotulinumtoxinA No systemic AEs CM phenotype SSRI/SNRI Calcium channel blockers Beta blockers Co-morbid depression Possible weight gain Peripheral edema Worsen depression Exercise intolerance
29 Medications Advantages Disadvantages Comments Gabapentin Weight gain Riboflavin Unknown: Devices (neuromodulation) GCRP targeted treatments Cannabinoids
30 Shunting for Headaches in IIH - JHMI (n=115 procedures) 1 procedure 46% 2 procedures 24% 3-5 procedures 19% >6 procedures 12% 95% had HA improvement at one month Recurrent headache in 48% at 36 months Revision more common with LP shunts McGirt MJ et al. J Neurosurg 2004;101:627-32
31 Transverse Sinus Stenting For IIH (any reason) Literature Review of 19 studies (207 individuals) Inconsistent criteria used for stenting (not all had papilledema) Headache and ICP were only universal findings Gradients varied and were not always measured 192 patients presented with headache (duration weeks to years) Headache after stenting Complete resolution in 72 (38%) Improvement in 83 (43%) No change in 35 (18%) Worse in 2 (1%) Long term durability not reported Teleb MS et al. Interven Neurol 2014;2:132-43
32 Summary: Headache and ICP Feature IIH SIH Primary HA Location Often frontal Often posterior Anywhere Postural component Usually none Often worse when upright Timing Morning or no fluctuation Latter part of day Nocturnal awakening Yes Yes Possible Worse with Valsalva, exertion, bending Migrainous associated symptoms Yes Yes Yes Yes Yes Yes Effect of caffeine None or worse Improvement Either Depends on HA type Patterns vary by HA type Effect of high altitude Worsens Improves Often worse Trendelenburg No effect Often improves No Pulsatile tinnitus Common Uncommon Uncommon
33 Summary: Other features Feature IIH SIH Primary HA Pulsatile tinnitus Common Rare (not pulsatile) May be present TVOs Common No No (or > seconds and not postural) Body habitus Usually obese Often slim or normal All Joint hypermobility Uncommon Common Uncommon Sex Usually female Male or female Male or female Neck or back pain Common Common Common Radicular pain Yes No No Papilledema Usually present No No Venous pulsations Absent Usually present Usually present Friedman DI. Continuum 2018;24:
34 Summary: Diagnostic Tests Feature IIH SIH Primary HA Sella / Pituitary Empty sella Enlarged pituitary Sometimes empty; pituitary enlarges in pregnancy Ventricular size Normal Normal Normal Tonsillar descent Possible Common Possible Flat posterior sclera Common No No Distended optic nerve sheath complex Common No Rare Flat anterior pons No Yes No LP opening pressure High Low, normal or high Anything Post LP headache? Possible Possible Possible Improvement of headache with LP? Often No Possible
35 Back to the Case Acetazolamide started was poorly tolerated at the dose needed to help headache (had to take it in the middle of the night) severe cognitive effects Changed to methazolamide, better tolerated but did not work as well Added furosemide without benefit Several therapeutic LPs helped only briefly Patient distraught
36 Considered options: VP shunt Optic nerve sheath fenestration Stenting
37
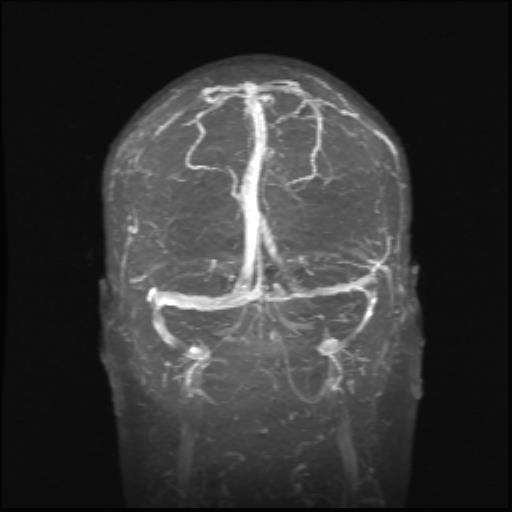
38 Vision good and not felt to be a good candidate for ONSF Agreed to avoid shunt because of EDS Evaluated for a stent and had procedure done Right transverse sinus stented (and through to be fenestrated rather than having arachnoid granulation) Pre-procedure gradient 21 mm Hg across stenosis Post-procedure gradient <5 mm Hg stenosis

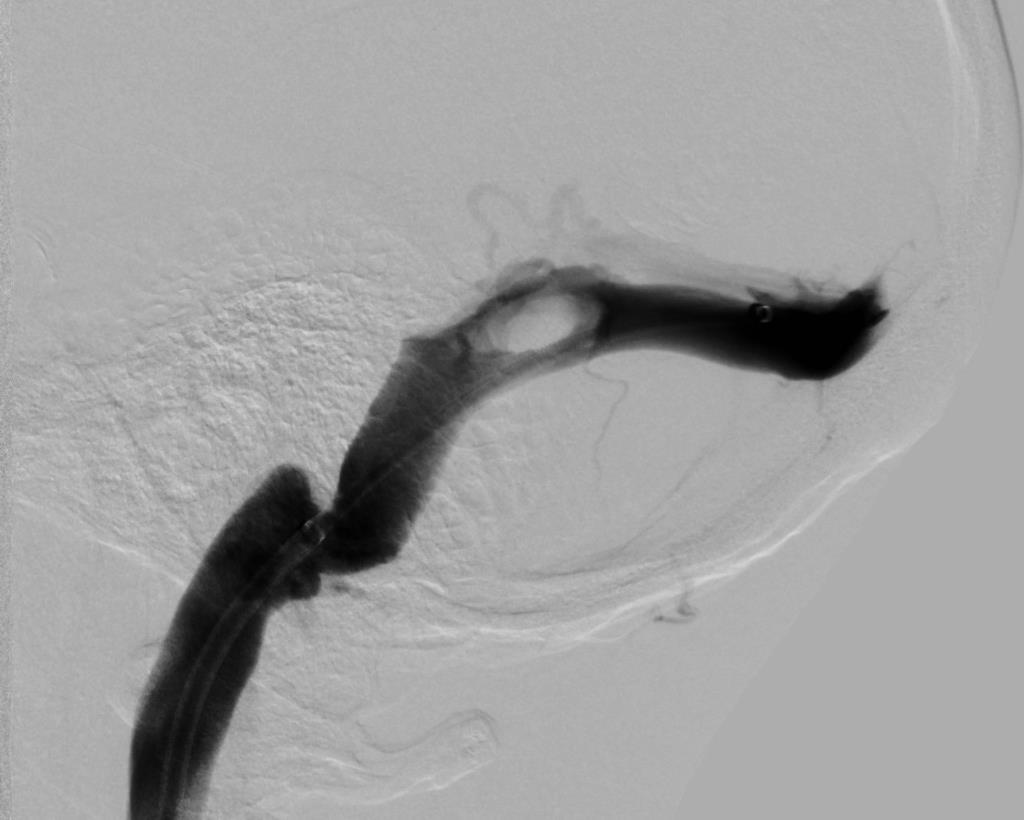

39 Before stent After stent
40 Take Home Points RIH headache is different than SIH headache and usually begins within hours to days of blood patches Therapeutic LP may be enough to relieve symptoms First line for medical treatment: acetazolamide or methazolamide It is possible for patient with primary IIH to develop cranial and spinal CSF leaks evaluate patient for evidence of preexisting IIH Headaches are usually self-limited although may take months to resolve Surgery is the last option to treat headache alone
41
Spontaneous Intracranial Hypotension Diagnosis and Treatment
 Spontaneous Intracranial Hypotension Diagnosis and Treatment John W. Engstrom MD, Philip R. Weinstein MD, and William P. Dillon M.D. University of California, San Francisco Spontaneous Intracranial Hypotension
Spontaneous Intracranial Hypotension Diagnosis and Treatment John W. Engstrom MD, Philip R. Weinstein MD, and William P. Dillon M.D. University of California, San Francisco Spontaneous Intracranial Hypotension
NANOS Patient Brochure
 NANOS Patient Brochure Pseudotumor Cerebri Copyright 2016. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for
NANOS Patient Brochure Pseudotumor Cerebri Copyright 2016. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for
Khalil Zahra, M.D Neuro-interventional radiology
 Khalil Zahra, M.D Neuro-interventional radiology 1 Disclosure None 2 Outline Etiology and pathogensis Imaging techniques and Features Literature review Treatment modalities Endovascular techniques Long
Khalil Zahra, M.D Neuro-interventional radiology 1 Disclosure None 2 Outline Etiology and pathogensis Imaging techniques and Features Literature review Treatment modalities Endovascular techniques Long
11/10/2017. Headache and Increased Pressure: A tale of 2 cases. Kathleen Digre MD University of Utah TWO CASES. 23 yo medical practice manager
 Headache and Increased Pressure: A tale of 2 cases Kathleen Digre MD University of Utah TWO CASES 23 yo medical practice manager September 2016 began developing intense frontal headaches first intermittent
Headache and Increased Pressure: A tale of 2 cases Kathleen Digre MD University of Utah TWO CASES 23 yo medical practice manager September 2016 began developing intense frontal headaches first intermittent
Coexistence of migraine and idiopathic intracranial hypertension without papilledema
 / GX'~C1~.. Coexistence of migraine and idiopathic intracranial hypertension without papilledema Ninan T. Mathew, MD; K. Ravishankar, MD; and Luis C. Sanin, MD!
/ GX'~C1~.. Coexistence of migraine and idiopathic intracranial hypertension without papilledema Ninan T. Mathew, MD; K. Ravishankar, MD; and Luis C. Sanin, MD!
Papilledema. Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D.
 Papilledema Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D. Papilledema specifically refers to optic nerve head swelling secondary to increased intracranial pressure (IICP). Optic nerve swelling from
Papilledema Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D. Papilledema specifically refers to optic nerve head swelling secondary to increased intracranial pressure (IICP). Optic nerve swelling from
Differential Diagnosis of Orthostatic Headache
 Differential Diagnosis of Orthostatic Headache MORRIS LEVIN, MD PROFESSOR OF NEUROLOGY CHIEF, DIVISION OF HEADACHE MEDICINE, UCSF Disclosures Consulting for Amgen, Lilly, Allergan, Supernus, Pernix No
Differential Diagnosis of Orthostatic Headache MORRIS LEVIN, MD PROFESSOR OF NEUROLOGY CHIEF, DIVISION OF HEADACHE MEDICINE, UCSF Disclosures Consulting for Amgen, Lilly, Allergan, Supernus, Pernix No
Sudden Headache and visual disturbances in a young woman
 Sudden Headache and visual disturbances in a young woman A. Soupart, MD, PhD Department of Internal Medicine BSIM, December 12, 2014 48 years old woman with Sudden Headache 7/2014 * Admitted for Headache
Sudden Headache and visual disturbances in a young woman A. Soupart, MD, PhD Department of Internal Medicine BSIM, December 12, 2014 48 years old woman with Sudden Headache 7/2014 * Admitted for Headache
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings. Jonathan A. Micieli, MD Valérie Biousse, MD
 Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
ISSN doi: /head VC 2017 American Headache Society Published by Wiley Periodicals, Inc.
 ISSN 0017-8748 Headache doi: 10.1111/head.13153 VC 2017 American Headache Society Published by Wiley Periodicals, Inc. Research Submissions Headache in Idiopathic Intracranial Hypertension: Findings From
ISSN 0017-8748 Headache doi: 10.1111/head.13153 VC 2017 American Headache Society Published by Wiley Periodicals, Inc. Research Submissions Headache in Idiopathic Intracranial Hypertension: Findings From
BMB Disclosures. Papilledema can be a. Neurological Emergency, Causing Preventable Blindness
 Reasonable Doubt: Can High Intracranial Pressure Occur Without Papilledema? 15 February 2013 Jonathan C. Horton hortonj@vision.ucsf.edu http://www.ucsf.edu/hortonlab BMB Disclosures Financial Disclosures
Reasonable Doubt: Can High Intracranial Pressure Occur Without Papilledema? 15 February 2013 Jonathan C. Horton hortonj@vision.ucsf.edu http://www.ucsf.edu/hortonlab BMB Disclosures Financial Disclosures
Intracranial hypertension and headache. Daniel Tibussek, MD
 Intracranial hypertension and headache. Daniel Tibussek, MD none Disclosures Overview Case Clinical presentation of pediatric PTC Nomenclature, Definition What is intracranial hypertension? Diagnostic
Intracranial hypertension and headache. Daniel Tibussek, MD none Disclosures Overview Case Clinical presentation of pediatric PTC Nomenclature, Definition What is intracranial hypertension? Diagnostic
Intracranial hypotension secondary to spinal CSF leak: diagnosis
 Intracranial hypotension secondary to spinal CSF leak: diagnosis Spinal cerebrospinal fluid (CSF) leak is an important and underdiagnosed cause of new onset headache that is treatable. Cerebrospinal fluid
Intracranial hypotension secondary to spinal CSF leak: diagnosis Spinal cerebrospinal fluid (CSF) leak is an important and underdiagnosed cause of new onset headache that is treatable. Cerebrospinal fluid
The headache profile of idiopathic intracranial hypertension
 The headache profile of idiopathic intracranial hypertension Michael Wall CEPHALALGIA Wall M. The headache profile of idiopathic intracranial hypertension. Cephalalgia 1990;10:331-5. Oslo. ISSN 0333-1024
The headache profile of idiopathic intracranial hypertension Michael Wall CEPHALALGIA Wall M. The headache profile of idiopathic intracranial hypertension. Cephalalgia 1990;10:331-5. Oslo. ISSN 0333-1024
NEURO QUIZ 45 EHLERS DANLOS SYNDROME
 NEURO QUIZ 45 EHLERS DANLOS SYNDROME Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D START 1. Regarding
NEURO QUIZ 45 EHLERS DANLOS SYNDROME Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D START 1. Regarding
Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt
 The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (5), Page 4556-4560 Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt Ali K. Ali, Maamoun M. Abo Shousha, Mohammed
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (5), Page 4556-4560 Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt Ali K. Ali, Maamoun M. Abo Shousha, Mohammed
THE SWOLLEN DISC. Valerie Biousse, MD Emory University School of Medicine Atlanta, GA
 THE SWOLLEN DISC Valerie Biousse, MD Emory University School of Medicine Atlanta, GA Updated from: Neuro-Ophthalmology Illustrated. Biousse V, Newman NJ. Thieme, New-York,NY. 2 nd Ed, 2016. Edema of the
THE SWOLLEN DISC Valerie Biousse, MD Emory University School of Medicine Atlanta, GA Updated from: Neuro-Ophthalmology Illustrated. Biousse V, Newman NJ. Thieme, New-York,NY. 2 nd Ed, 2016. Edema of the
Low PRESSURE Headaches. What they area and what can you do? Kathleen B. Digre MD University of Utah
 Low PRESSURE Headaches aka Low CSF volume headache: What they area and what can you do? Kathleen B. Digre MD University of Utah Disclosure: I have a part ownership on a patent for thin filmed technology
Low PRESSURE Headaches aka Low CSF volume headache: What they area and what can you do? Kathleen B. Digre MD University of Utah Disclosure: I have a part ownership on a patent for thin filmed technology
What is IIH? Idiopathic Intracranial Hypertension (IIH)
") What is IIH? Idiopathic Intracranial Hypertension (IIH) What is Idiopathic Intracranial Hypertension? Idiopathic intracranial hypertension (IIH), also known as benign intracranial hypertension or pseudotumour
What is IIH? Idiopathic Intracranial Hypertension (IIH) What is Idiopathic Intracranial Hypertension? Idiopathic intracranial hypertension (IIH), also known as benign intracranial hypertension or pseudotumour
Chronic Daily Headaches
 Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Idiopathic Intracranial Hypertension
 Idiopathic Intracranial Hypertension Dr. Mar'n Su+onBrown MD. FRCPC Neuro-Ophthalmology, Neurology Div of Neurology, Island Health Clinical Assistant Professor, Div of Neurology, UBC Stroke Rapid Assessment
Idiopathic Intracranial Hypertension Dr. Mar'n Su+onBrown MD. FRCPC Neuro-Ophthalmology, Neurology Div of Neurology, Island Health Clinical Assistant Professor, Div of Neurology, UBC Stroke Rapid Assessment
Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health
 Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health History 15 year old African female with CC of Headache. Onset: 2 weeks ago Location: Frontal Character: Sharp & Throbbing Radiation: None
Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health History 15 year old African female with CC of Headache. Onset: 2 weeks ago Location: Frontal Character: Sharp & Throbbing Radiation: None
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline. Scottish intercollegiate Guidelines Network SIGN
 A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
Remembering Donald J. Dalessio, MD The Headache Clinic Featuring the Baylor Scott & White Headache Clinic in Temple, Texas.
 Spinal Cerebrospinal Fluid Leak An Under-recognized Cause of Headache More common than expected, why is this type of headache so often misdiagnosed or the diagnosis is delayed? Challenging the One Size
Spinal Cerebrospinal Fluid Leak An Under-recognized Cause of Headache More common than expected, why is this type of headache so often misdiagnosed or the diagnosis is delayed? Challenging the One Size
Neuro-Ocular Grand Rounds
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
HEADACHES THE RED FLAGS
 HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
A case of a patient with chronic headache. Focus on Migraine. None related to the presentation Grants to conduct clinical trials from: Speaker bureau:
 Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Differentiating Migraine from Other Headache Types to Target Treatment Peter J. Goadsby, MD, PhD
 Differentiating Migraine from Other Headache Types to Target Treatment Peter J. Goadsby, MD, PhD University of California, San Francisco San Francisco, CA King's College London London, England Learning
Differentiating Migraine from Other Headache Types to Target Treatment Peter J. Goadsby, MD, PhD University of California, San Francisco San Francisco, CA King's College London London, England Learning
Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology
 David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology") Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology 26 year old 5 3, 300 pound female with papilledema,
Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology 26 year old 5 3, 300 pound female with papilledema,
OPTIC NERVE SWELLING IN CHILDHOOD
 OPTIC NERVE SWELLING IN CHILDHOOD Melissa W. Ko, MD, FAAN One of the main findings on a pediatric neurologic examination that can instill fear and lead to an urgent referral to neuro-ophthalmology is the
OPTIC NERVE SWELLING IN CHILDHOOD Melissa W. Ko, MD, FAAN One of the main findings on a pediatric neurologic examination that can instill fear and lead to an urgent referral to neuro-ophthalmology is the
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation.
 I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
The Ehlers Danlos syndromes (EDS) are a mixed group of. Neurological and Spinal Manifestations of the Ehlers-Danlos Syndromes FOR NON-EXPERTS
 are a mixed group of. Neurological and Spinal Manifestations of the Ehlers-Danlos Syndromes FOR NON-EXPERTS") The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
IDIOPATHIC INTRACRANIAL HYPERTENSION
 IDIOPATHIC INTRACRANIAL HYPERTENSION ASSESSMENT OF VISUAL FUNCTION AND PROGNOSIS FOR VISUAL OUTCOME Doctor of Philosophy thesis Anglia Ruskin University, Cambridge Fiona J. Rowe Department of Orthoptics,
IDIOPATHIC INTRACRANIAL HYPERTENSION ASSESSMENT OF VISUAL FUNCTION AND PROGNOSIS FOR VISUAL OUTCOME Doctor of Philosophy thesis Anglia Ruskin University, Cambridge Fiona J. Rowe Department of Orthoptics,
Headache Syndrome. Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL
 Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Mechanisms of Headache in Intracranial Hypotension
 Mechanisms of Headache in Intracranial Hypotension Stephen D Silberstein, MD Jefferson Headache Center Thomas Jefferson University Hospital Philadelphia, PA Stephen D. Silberstein, MD, FACP Director, Jefferson
Mechanisms of Headache in Intracranial Hypotension Stephen D Silberstein, MD Jefferson Headache Center Thomas Jefferson University Hospital Philadelphia, PA Stephen D. Silberstein, MD, FACP Director, Jefferson
Pearls, Pitfalls and Advances in Neuro-Ophthalmology
 Pearls, Pitfalls and Advances in Neuro-Ophthalmology Nancy J. Newman, MD Emory University Atlanta, GA Consultant for Gensight Biologics, Santhera Data Safety Monitoring Board for Quark AION Study Medical-legal
Pearls, Pitfalls and Advances in Neuro-Ophthalmology Nancy J. Newman, MD Emory University Atlanta, GA Consultant for Gensight Biologics, Santhera Data Safety Monitoring Board for Quark AION Study Medical-legal
6/2/2017. Objectives. Statement of Problem: Migraine Headaches Are Common. Chronic Headache In Pediatrics, Botox and Beyond
 Chronic Headache In Pediatrics, Botox and Beyond Ken Mack MD PhD Mayo Clinic 2015 MFMER slide-1 Objectives Understand pediatric chronic headache presentations Review evidence for the treatment of chronic
Chronic Headache In Pediatrics, Botox and Beyond Ken Mack MD PhD Mayo Clinic 2015 MFMER slide-1 Objectives Understand pediatric chronic headache presentations Review evidence for the treatment of chronic
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017
 Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Headache. Karen Thaxter
 Headache Karen Thaxter An eight year old girl is taken to her paediatrician because she has been complaining of almost daily pain at the back of her head for the past 4 months. She states that each headache
Headache Karen Thaxter An eight year old girl is taken to her paediatrician because she has been complaining of almost daily pain at the back of her head for the past 4 months. She states that each headache
Paediatric headaches. Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services. Brevity, levity, repetition
 Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Outpatient Headache Care Guideline
 1 Outpatient Care Guideline Inclusion criteria: children > 3 yrs with headaches Is urgent emergency department, neuroimaging, or Neurology consultation indicated? Referral to ED if: New severe headache
1 Outpatient Care Guideline Inclusion criteria: children > 3 yrs with headaches Is urgent emergency department, neuroimaging, or Neurology consultation indicated? Referral to ED if: New severe headache
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in
 HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
11/10/2017. THE BRIDGE Course Objectives. THE BRIDGE Course Objectives
 THE BRIDGE Course Objectives Describe clinical characteristics associated with migraine diagnosis in adult and pediatric populations. Identify barriers and risk factors impacting the clinical course of
THE BRIDGE Course Objectives Describe clinical characteristics associated with migraine diagnosis in adult and pediatric populations. Identify barriers and risk factors impacting the clinical course of
 Ian Carroll MD, MS https://med.stanford.edu/profiles/ian-carroll CarrollCSFleak@gmail.com SIH and/or POTS? Disclosures No Conflicts of Interest This work is supported by the Considine CSF Leaks Fund Thank
Ian Carroll MD, MS https://med.stanford.edu/profiles/ian-carroll CarrollCSFleak@gmail.com SIH and/or POTS? Disclosures No Conflicts of Interest This work is supported by the Considine CSF Leaks Fund Thank
Triptans: Nonresponse, Recurrence, and Serious AEs for Many Patients
 Efficacy, Safety, and Tolerability of Rimegepant 75 mg, an Oral CGRP Receptor Antagonist, for the Acute Treatment of Migraine: Results from a Phase 3, Double-Blind, Randomized, Placebo-Controlled Trial,
Efficacy, Safety, and Tolerability of Rimegepant 75 mg, an Oral CGRP Receptor Antagonist, for the Acute Treatment of Migraine: Results from a Phase 3, Double-Blind, Randomized, Placebo-Controlled Trial,
Lynda J. Krasenbaum, MSN, ANP BC. Associate Director New York Headache Center
 Diagnosing Headache in Adults and Adolescents Lynda J. Krasenbaum, MSN, ANP BC Associate Director New York Headache Center New York, New York Learning Objectives Understand the diagnostic challenges of
Diagnosing Headache in Adults and Adolescents Lynda J. Krasenbaum, MSN, ANP BC Associate Director New York Headache Center New York, New York Learning Objectives Understand the diagnostic challenges of
Glossary. Working to relieve the pressure!
 A Acetazolamide - see Diamox Amitriptyline - a drug which is used in low dosage in IIH to treat some of the symptoms of the condition. Analgesic - a drug used to relieve pain, often referred to as painkillers.
A Acetazolamide - see Diamox Amitriptyline - a drug which is used in low dosage in IIH to treat some of the symptoms of the condition. Analgesic - a drug used to relieve pain, often referred to as painkillers.
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy
 HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
Neurological Dilemmas in Primary Care
 Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
National Hospital for Neurology and Neurosurgery
 National Hospital for Neurology and Neurosurgery Venous sinus stents (for the treatment of venous sinus stenosis and idiopathic intracranial hypertension) Lysholm Department of Neuroradiology If you would
National Hospital for Neurology and Neurosurgery Venous sinus stents (for the treatment of venous sinus stenosis and idiopathic intracranial hypertension) Lysholm Department of Neuroradiology If you would
Spontaneous Cerebrospinal Fluid Rhinorrhea as the Presenting Symptom of Idiopathic Intracranial Hypertension: A Case Series
 CASE REPORT Spontaneous Cerebrospinal Fluid Rhinorrhea as the Presenting Symptom of Idiopathic Intracranial Hypertension: A Case Series Hossein Ghalaenovi 1, Maziar Azar 1, Morteza Taheri 1, Mahdi Safdarian
CASE REPORT Spontaneous Cerebrospinal Fluid Rhinorrhea as the Presenting Symptom of Idiopathic Intracranial Hypertension: A Case Series Hossein Ghalaenovi 1, Maziar Azar 1, Morteza Taheri 1, Mahdi Safdarian
MIGRAINE UPDATE. Objectives & Disclosures. Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment.
 MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
6/4/2018. Headache. Headaches. Headache. Migraine Headaches. Headache. Red Flag signs and symptoms. Imaging CT without contrast.
 Presented by M.D. Shepherd, M.D. OH MY ACHING HEAD! Estimated that one half of the adult population is affected by a headache disorder International Society Classification Primary : Tension s 40% of the
Presented by M.D. Shepherd, M.D. OH MY ACHING HEAD! Estimated that one half of the adult population is affected by a headache disorder International Society Classification Primary : Tension s 40% of the
An Organized Approach to the Patient with Papilledema and IIH
 An Organized Approach to the Patient with Papilledema and IIH Leonard V. Messner, OD, FAAO James L. Fanelli, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized
An Organized Approach to the Patient with Papilledema and IIH Leonard V. Messner, OD, FAAO James L. Fanelli, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized
CHRONIC HEADACHES IN CHILDHOOD
 CHRONIC HEADACHES IN CHILDHOOD EDWIN LIU, MD PEDIATRIC NEUROLOGISTS OF PALM BEACH PEDIATRIC SLEEP CENTERS OF FLORIDA ASSISTANT CLINICAL PROFESSOR FSU ASSISTANT CLINICAL PROFESSOR NOVA SOUTHEASTERN PEDIATRIC
CHRONIC HEADACHES IN CHILDHOOD EDWIN LIU, MD PEDIATRIC NEUROLOGISTS OF PALM BEACH PEDIATRIC SLEEP CENTERS OF FLORIDA ASSISTANT CLINICAL PROFESSOR FSU ASSISTANT CLINICAL PROFESSOR NOVA SOUTHEASTERN PEDIATRIC
continuing medical education
 In collaboration with Jeddah Primary Care CME unit This is a CME (Continuing Medical Education) article. It is presented to you in collaboration with the Middle East CME organizations. Self-test answers
In collaboration with Jeddah Primary Care CME unit This is a CME (Continuing Medical Education) article. It is presented to you in collaboration with the Middle East CME organizations. Self-test answers
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Chronic Migraine in Primary Care. December 11 th, 2017 Werner J. Becker University of Calgary
 Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
Richard B. Lipton, 1 Joel Saper, 2 Messoud Ashina, 3 David Biondi, 4 Suman Bhattacharya, 4 Joe Hirman, 5 Barbara Schaeffler, 4 Roger Cady 4
 A Phase 3, Randomized, Double-blind, Placebo-Controlled Study to Evaluate the Efficacy and Safety of for the Preventive Treatment of Chronic Migraine: Results of the PROMISE-2 (PRevention Of Migraine via
A Phase 3, Randomized, Double-blind, Placebo-Controlled Study to Evaluate the Efficacy and Safety of for the Preventive Treatment of Chronic Migraine: Results of the PROMISE-2 (PRevention Of Migraine via
12/2/16. Ways to differentiate:
 Nate Lighthizer, O.D., F.A.A.O. Assistant Dean for Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic Oklahoma College of Optometry lighthiz@nsuok.edu
Nate Lighthizer, O.D., F.A.A.O. Assistant Dean for Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic Oklahoma College of Optometry lighthiz@nsuok.edu
Headache evaluation and management after concussion. Assistant Professor
 Headache evaluation and management after concussion Juliette Preston, M.D. Assistant Professor OHSU Headache Center OVERVIEW Introduction Definition Acute post-traumatic headache Red flags Persistent post-traumatic
Headache evaluation and management after concussion Juliette Preston, M.D. Assistant Professor OHSU Headache Center OVERVIEW Introduction Definition Acute post-traumatic headache Red flags Persistent post-traumatic
UCNS Course A Review of ICHD-3b
 UCNS Course A Review of ICHD-3b Andrew D. Hershey, M.D., Ph.D., FAHS Endowed Chair and Director of Neurology Director, Cincinnati Children s Headache Center Professor of Neurology and Pediatrics University
UCNS Course A Review of ICHD-3b Andrew D. Hershey, M.D., Ph.D., FAHS Endowed Chair and Director of Neurology Director, Cincinnati Children s Headache Center Professor of Neurology and Pediatrics University
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Medical treatment and Monitoring in IIH
 Medical treatment and Monitoring in IIH Introduction When you have Idiopathic Intracranial Hypertension it is important that your vision, symptoms and medication are monitored on a regular basis. This
Medical treatment and Monitoring in IIH Introduction When you have Idiopathic Intracranial Hypertension it is important that your vision, symptoms and medication are monitored on a regular basis. This
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, II. Management of Refractory Headaches
 October 23, II. Management of Refractory Headaches") Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Meningoceles in Idiopathic Intracranial Hypertension
 Neuroradiology/Head and Neck Imaging Original Research Bialer et al. Meningoceles in IIH Neuroradiology/Head and Neck Imaging Original Research Omer Y. Bialer 1 Mario Perez Rueda 1 Beau B. Bruce 1,2 Nancy
Neuroradiology/Head and Neck Imaging Original Research Bialer et al. Meningoceles in IIH Neuroradiology/Head and Neck Imaging Original Research Omer Y. Bialer 1 Mario Perez Rueda 1 Beau B. Bruce 1,2 Nancy
A Case of Stent Placement for Intracranial Hypertension Associated with Venous Sinus Stenosis
 DOI: 10.5797/jnet.cr.2016-0080 A Case of Stent Placement for Intracranial Hypertension Associated with Venous Sinus Stenosis Rei Yamaguchi, Koji Sato, Hiroya Fujimaki, and Ken Asakura Objective: We encountered
DOI: 10.5797/jnet.cr.2016-0080 A Case of Stent Placement for Intracranial Hypertension Associated with Venous Sinus Stenosis Rei Yamaguchi, Koji Sato, Hiroya Fujimaki, and Ken Asakura Objective: We encountered
Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE
 Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE IHS Classification 1989 (updated 2004) Primary Headaches 4 categories Migraine Tension-type Cluster and other trigeminal
Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE IHS Classification 1989 (updated 2004) Primary Headaches 4 categories Migraine Tension-type Cluster and other trigeminal
PITFALLS IN PAPILLOEDEMA
 PITFALLS IN PAPILLOEDEMA SRC 2013 Why care about papilloedema? Dr Neil Shuey FRACP MBBS(Hons) MScOptom St Vincent s Hospital, Melbourne Royal Victorian Eye & Ear Hospital Disclosures: Travel grants Biogen
PITFALLS IN PAPILLOEDEMA SRC 2013 Why care about papilloedema? Dr Neil Shuey FRACP MBBS(Hons) MScOptom St Vincent s Hospital, Melbourne Royal Victorian Eye & Ear Hospital Disclosures: Travel grants Biogen
Dural venous sinus angioplasty and stenting for the treatment of idiopathic intracranial hypertension
 1 Department of Interventional Neuroradiology, Oregon Health and Science University, Portland, Oregon, USA 2 School of Medicine, Oregon Health and Science University, Portland, Oregon, USA 3 Department
1 Department of Interventional Neuroradiology, Oregon Health and Science University, Portland, Oregon, USA 2 School of Medicine, Oregon Health and Science University, Portland, Oregon, USA 3 Department
10/31/2017 PRIMARY CARE AND HEADACHE DISCLOSURES WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Primary Care 67%
 PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
Is it Papilloedema? John Ross Ainsworth Orthoptic staff Birmingham Children s Hospital Birmingham and Midland Eye Centre University of Birmingham
 Is it Papilloedema? John Ross Ainsworth Orthoptic staff Birmingham Children s Hospital Birmingham and Midland Eye Centre University of Birmingham Aims Children/young people A bit about hypoplasia / NFL
Is it Papilloedema? John Ross Ainsworth Orthoptic staff Birmingham Children s Hospital Birmingham and Midland Eye Centre University of Birmingham Aims Children/young people A bit about hypoplasia / NFL
Headaches in Pregnancy Before, During, and After
 Headaches in Pregnancy Before, During, and After Robert Kaniecki, MD Director, UPMC Headache Center Assistant Professor of Neurology University of Pittsburgh Headaches and Pregnancy Pre-pregnancy counseling
Headaches in Pregnancy Before, During, and After Robert Kaniecki, MD Director, UPMC Headache Center Assistant Professor of Neurology University of Pittsburgh Headaches and Pregnancy Pre-pregnancy counseling
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา
 ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
Headache. Headache Case. Migraine Headache. Eric Kraus, MD. Types» Without aura (common)» With aura (classic)
» With aura (classic)") Headache Eric Kraus, MD Headache Case This 23 year-old female has headaches behind the right eye that cause her to lay down in a quiet room. They have a throbbing quality and she may vomit. Migraine Headache
Headache Eric Kraus, MD Headache Case This 23 year-old female has headaches behind the right eye that cause her to lay down in a quiet room. They have a throbbing quality and she may vomit. Migraine Headache
CSF Leaks. Abnormal communication between the subarachnoid space and the tympanomastoid space or nasal cavity. Presenting symptoms:
 CSF Leaks Steven Wright, M.D. Faculty Advisor: Matthew Ryan, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2005 CSF Leaks Abnormal communication
CSF Leaks Steven Wright, M.D. Faculty Advisor: Matthew Ryan, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2005 CSF Leaks Abnormal communication
FINANCIAL DISCLOSURE. No relevant financial relationships
 Sleep and Headache Paul Mathew, MD, FAHS Director of Continuing Medical Education John R. Graham Headache Center Brigham & Women s Hospital Director of Headache Medicine Cambridge Health Alliance Harvard
Sleep and Headache Paul Mathew, MD, FAHS Director of Continuing Medical Education John R. Graham Headache Center Brigham & Women s Hospital Director of Headache Medicine Cambridge Health Alliance Harvard
Chief Complaint. History. History of Similar Episodes. A 10 Year-Old Boy With Headache
 A 10 Year-Old Boy With Headache Chief Complaint Recent Advances in Neurology 2013 10 year-old boy presented with his fifth lifetime bout of left-sided head pain followed by diplopia. Amy A. Gelfand, MD
A 10 Year-Old Boy With Headache Chief Complaint Recent Advances in Neurology 2013 10 year-old boy presented with his fifth lifetime bout of left-sided head pain followed by diplopia. Amy A. Gelfand, MD
MOHAMED LOTFY, M.D.*; MOATAZ A. EL-AWADY, M.D.**; ASHRAF E. ZAGHLOUL, M.D.** and TAREK NEHAD, M.D.***
 Med. J. Cairo Univ., Vol. 84, No. 2, December: 301-306, 2016 www.medicaljournalofcairouniversity.net Effect of Therapeutic Lumbar Puncture on the Visual Outcome and the Further Need for Surgery in Patients
Med. J. Cairo Univ., Vol. 84, No. 2, December: 301-306, 2016 www.medicaljournalofcairouniversity.net Effect of Therapeutic Lumbar Puncture on the Visual Outcome and the Further Need for Surgery in Patients
Headaches in Children and Adolescents. Paul Shillito
 Headaches in Children and Adolescents Paul Shillito Topics For Discussion What s different about childhood migraine Chronic daily headache (CDH) Tumours and other things to worry about Management of childhood
Headaches in Children and Adolescents Paul Shillito Topics For Discussion What s different about childhood migraine Chronic daily headache (CDH) Tumours and other things to worry about Management of childhood
Refractory Headache Challenges and Strategies. David W. Dodick, M.D. Department of Neurology Mayo Clinic Phoenix Arizona USA
 Refractory Headache Challenges and Strategies David W. Dodick, M.D. Department of Neurology Mayo Clinic Phoenix Arizona USA Headache Masters School, Tokyo 2013 Definition of refractory/intractability depends
Refractory Headache Challenges and Strategies David W. Dodick, M.D. Department of Neurology Mayo Clinic Phoenix Arizona USA Headache Masters School, Tokyo 2013 Definition of refractory/intractability depends
Current Migraine Treatment Therapy. Daniel Kassicieh, DO, FAAN
 Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Disclosures. Objectives 6/2/2017
 Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetazolamide, in idiopathic intracranial hypertension, 49 52, 60 Angiography, computed tomography, in cranial nerve palsy, 103 107 digital
Index Note: Page numbers of article titles are in boldface type. A Acetazolamide, in idiopathic intracranial hypertension, 49 52, 60 Angiography, computed tomography, in cranial nerve palsy, 103 107 digital
Unit #3: Dry Lab A. David A. Morton, Ph.D.
 Unit #3: Dry Lab A David A. Morton, Ph.D. Skull Intracranial Hemorrhage Pg. 26 Epidural Hematoma Pg. 26 Skull Pg. 26 Subdural Hematoma Pg. 26 Subdural Hematoma Pg. 26 Subarachnoid Hemorrhage Pg. 26 Subarachnoid
Unit #3: Dry Lab A David A. Morton, Ph.D. Skull Intracranial Hemorrhage Pg. 26 Epidural Hematoma Pg. 26 Skull Pg. 26 Subdural Hematoma Pg. 26 Subdural Hematoma Pg. 26 Subarachnoid Hemorrhage Pg. 26 Subarachnoid
Headache Master School Japan-Osaka 2016 II. Management of refractory headaches Case Presentation 2. SUNCT/SUNA: concept, management and prognosis
 Headache Master School Japan-Osaka 2016 II. Management of refractory headaches Case Presentation 2. SUNCT/SUNA: concept, management and prognosis Noboru Imai(Department of Neurology, Japanese Red Cross
Headache Master School Japan-Osaka 2016 II. Management of refractory headaches Case Presentation 2. SUNCT/SUNA: concept, management and prognosis Noboru Imai(Department of Neurology, Japanese Red Cross
Trigeminal Autonomic Cephalalgias. Disclosures. Objectives 6/20/2018. Rashmi Halker Singh, MD FAHS UCNS Review Course June 2018
 Trigeminal Autonomic Cephalalgias Rashmi Halker Singh, MD FAHS UCNS Review Course June 2018 Disclosures Honoraria from Allergan and Amgen for advisory board, Current Neurology and Neuroscience Reports
Trigeminal Autonomic Cephalalgias Rashmi Halker Singh, MD FAHS UCNS Review Course June 2018 Disclosures Honoraria from Allergan and Amgen for advisory board, Current Neurology and Neuroscience Reports
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
While some patients with SIH recover without intervention
 ORIGINAL RESEARCH P.H. Luetmer K.M. Schwartz L.J. Eckel C.H. Hunt R.E. Carter F.E. Diehn When Should I Do Dynamic CT Myelography? Predicting Fast Spinal CSF Leaks in Patients with Spontaneous Intracranial
ORIGINAL RESEARCH P.H. Luetmer K.M. Schwartz L.J. Eckel C.H. Hunt R.E. Carter F.E. Diehn When Should I Do Dynamic CT Myelography? Predicting Fast Spinal CSF Leaks in Patients with Spontaneous Intracranial
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Treatment of spontaneous intracranial hypotension: evolution of the therapeutic and diagnostic modalities
 DOI 10.1007/s10072-013-1364-2 BRIEF COMMUNICATION Treatment of spontaneous intracranial hypotension: evolution of the therapeutic and diagnostic modalities Angelo Franzini G. Messina L. Chiapparini G.
DOI 10.1007/s10072-013-1364-2 BRIEF COMMUNICATION Treatment of spontaneous intracranial hypotension: evolution of the therapeutic and diagnostic modalities Angelo Franzini G. Messina L. Chiapparini G.
Faculty Disclosure. Karen L. Bremer, MD. Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Carotid Cavernous Fistula
 Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
How could I be having migraine when I don't have a headache?
 Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Headache and Facial Pain. Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology
 Headache and Facial Pain Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology Introduction It is the most common neurologic complain The diagnosis usually
Headache and Facial Pain Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology Introduction It is the most common neurologic complain The diagnosis usually
Brain Meninges, Ventricles and CSF
 Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid