TIAs and posterior circulation problems
|
|
|
- Madeline Kennedy
- 5 years ago
- Views:
Transcription


1 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health

2
3 How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in Australia annually TIA/minor stroke ~40% ischaemic brain episodes 30-40% patients with ischaemic stroke have an earlier TIA/minor stroke Difficult to accurately count Non-presentation Mimics hard to differentiate retrospectively
 or minor stroke A J Coull et al.")
4 Cumulative risk of stroke after a transient ischaemic attack (TIA) or minor stroke A J Coull et al. BMJ 2004
5 TIA: a rubbish diagnostic label Terribly inaccurate acronym Thanks in advance Totally inexplicable attack TIA = TNA This is Art Acute Cerebrovascular Syndrome?
6 TIA: a brief history The classic definition (mid 1960s): sudden, focal neurological deficit of presumed vascular origin lasting <24 hours Time threshold completely arbitrary Assumed no symptoms = no brain injury RIND abandoned in 1970s Recognition that prolonged symptoms associated with cerebral infarction Recent recognition that symptoms <24 hours associated with cerebral infarction
7 TIA: the inconsistencies Based on concept of no brain injury entrenched ennui TIA thought benign (at least it wasn t a stroke!) 1/3 traditional TIAs have infarction Duration of symptoms doesn t discriminate 1/3 of those with symptoms <1 hour have +ve DWI indicating ischaemic injury
8 TIA: the inconsistencies Stroke and TIA on a spectrum of brain ischaemia TIA an opportunity to prevent disabling injury, including cognitive impairment TIA a marker of high risk for vascular death NOT BENIGN!
9 TIA: the new tissue-based definition a transient episode of neurological dysfunction caused by focal brain, spinal cord or retinal ischaemia, without acute infarction ASA recommendation (2009): TIA patients should undergo neuroimaging within 24 hours of symptom onset, preferably with magnetic resonance imaging, including diffusion sequences
10 Stroke versus TIA Stroke and TIA are the same condition: If patient has symptoms, it is a stroke TIA lasts minutes if arrive to ED with symptoms, it is stroke In NINDS study, if signs at 1hr; 97% signs at 24 Distinction only retrospective Stroke symptoms are urgent New definition of stroke is imaging based

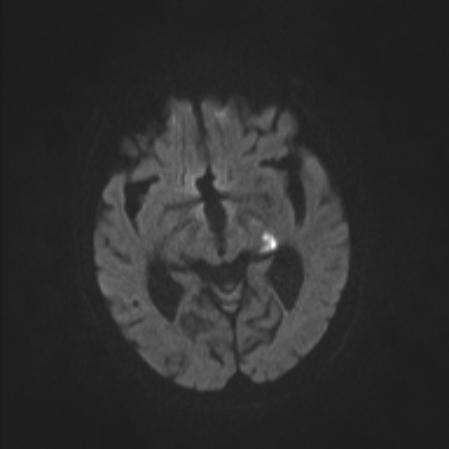
11 MRI confirmed TIA 77 year old woman; sudden onset sensory disturbance in Left foot; clumsy foot; signs resolved at assessment
12 What should you do? Symptoms and signs fully resolved? If not, this is stroke! Acute therapy will be the initial focus Yes? assessment & investigation is the same
13 Stroke or mimic? Stroke likely: Sudden onset exact time of onset Patient well at onset Focal neurology history and signs Referable to Left or Right brain Sub-typing possible (Oxfordshire types) Greater neurological deficit Abnormal vascular signs BP, PVD, AF, valvular disease
14 Oxfordshire stroke subtypes TACI - large anterior circulation stroke hemiparesis, HH, cortical signs PACI smaller anterior circulation stroke e.g. monoparesis; dysphasia alone LACI lacunar syndromes pure motor hemiparesis most common implications for underlying cause POCI posterior circulation territory Isolated HH, brainstem or cerebellar signs.
15 Stroke or mimic? Stroke unlikely: Known history of cognitive impairment Confusion (beware isolated dysphasia) Unwell during last week No neurological signs Signs in other symptoms e.g. chest crackles Seizure at onset Loss of consciousness without focal signs Isolated vertigo
16
17 ROSIER scale Recognition of stroke in the ER Check BSL If <3.5 mmol treat and reassess once BSL normal Loss of consciousness/syncope = -1 Seizure activity = -1 New acute: Asymmetric facial weakness = +1 Asymmetric arm weakness = +1 Asymmetric leg weakness = +1 Speech disturbance = +1 Visual field defect = +1 Stroke unlikely if total score 0
18 Basilar Occlusion Often preceding transient symptoms: Diplopia Bilateral visual disturbance Vertigo PLUS hearing loss/other sympts Transient LOC with quadriparesis Dysarthria with quadriparesis/sensory loss
19 Basilar occlusion High index of suspicion with unconscious collapse and GCS at presentation Quadriparesis, upgoing plantars Check the eyes Likely loss of normal VOR Pupillary changes Consider adding CT angiogram if NCCT excludes brainstem/large hemispheric ICH
20 The science of strokeology Time since event determines short term risk Pre-existing vascular risk (BP, IHD, AF, smoking) Co-existing brain disease e.g. dementia Sudden onset, mins to hours (not secs), recurrence Predictive symptoms: weakness, dysphasia Negative predictors: sensory symptoms, especially if multiply repeated vertigo alone Careful systematic neuro exam Investigations: brain and vascular imaging, ECG The tunnel of truth
21 The world of mimics Syncope Peripheral vestibulopathy Migraine Anxiety and hysteria Delerium Hypoglycaemia Peripheral neuropathy e.g. radial Partial seizures Transient global amnesia
22 Vertigo is it stroke Key is to take an excellent history Detailed history of symptoms and time course Have there been other episodes? Ask specifically about other brainstem symptoms Check with witness
23 Vertigo is it stroke? The physical exam: Full neurological exam - careful attention to the eyes Is there a skew deviation (are the eyes level) Do they move smoothly and together in all directions? Is there vertical nystagmus? Are the pupils equal and react normally? Is there a ptosis? Head impulse test
24 Caution needed here! Beware vomiting and can t walk Beware sudden deafness with vertigo Beware the patient with large cerebellar infarct who looks a million dollars Collapse and unconsciousness Think basilar occlusion Take a history for preceding events Look at the eye movements

25
26 EXPRESS and SOS-TIA Marked benefits from: early clinical assessment rapid investigations CT brain, ECG for AF, Carotid imaging Other urgent initiation secondary prevention Triple therapy: antiplatelet, antihypertensive, statin Targetted treatment e.g. CEA, warfarin for AF Inpatient care better than outpatient?
27 Essential Investigations (1) History and examination Exclude mimics Check blood sugar!!! Large artery or lacunar; anterior or posterior OCSP classification TACI, PACI, LACI, POCI Brain imaging CT mandatory and urgent! Exclude mimics; ICH or ischaemic CT stroke in up to 20% Old strokes topography and number Early ischaemic changes More established change (non-dominant)
28 Essential investigations (2) Mechanism? BSL mimic, diabetes Systemic disease UEC, FBE, ESR Fasting lipids and sugar ECG - AF, ACS or other high risk cardiac source Carotid duplex - high grade symptomatic stenosis Rare specific causes e.g. dissection; venous sinus thrombosis; GCA; endocarditis Assess risk factors BP, smoking, lipids, diabetes
29 Key investigations All patients with stroke symptoms need CT brain as soon as possible BSL, UEC, FBE, ESR, CXR ECG Most will need carotid duplex ultrasound

30
31 Targeted role for stroke MRI Confirm stroke or non-stroke diagnosis Brainstem events Minor/transient event functional vs real deficit; stroke versus tumour Accurately define the topography of stroke Small artery versus large artery Influences further investigations Added value Shows old/other changes in brain including microhaemorrhages Non-invasive view of brain arteries
32 ABCD2 a prognostic score Age 60 years = 1 BP (systolic >140 and/or diastolic 90) = 1 Clinical features unilat weakness =2; speech =1; other =0 Duration >60 mins =2; =1; <10 =0 Diabetes 2 day ABCD 2 risk: 1% if = % if = % if = 6-7
33 ABCD2 the positives A new focus on TIA recognition, risk factors, stroke risk in ED and GP? a diagnostic tool for the non-expert Predicts risk moderately in some populations AUC 0.72 in systematic review AUC only 0.62 in Australian setting
34 ABCD2 the negatives Misclassifies 1/2 of those with high risk mechanisms Ignores carotid stenosis and AF Cook book approach to TIA Doesn t differentiate mimic from TIA Ignores importance of expert detailed history and clinical examination Used to justify non-urgent expert assessment Most recurrent stroke events < 2 days

35
36 Stroke prevention strategies Carotid endarterectomy for >70% stenosis Warfarin for AF and high risk cardiac sources Anti-platelet agent Risk factor management BP lowering Lipid lowering Education of patient and family
37 Basilar thrombosis IV alteplase if <4.5 hours and eligible If presenting late or severe syndrome and/or not responding to thrombolysis, consider urgent transfer for clot retrieval Outcomes influenced by age, severity of symptoms, time from onset BASICS registry no benefit from treatment beyond 9 hours in severe

38 Clot retrieval



39
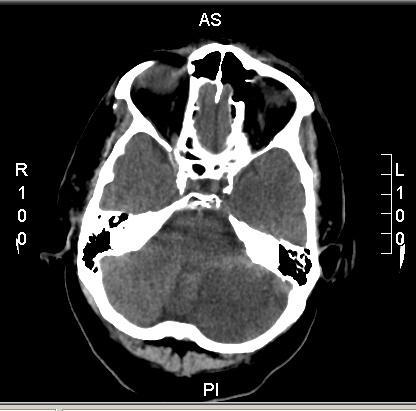
40 Cerebellar stroke
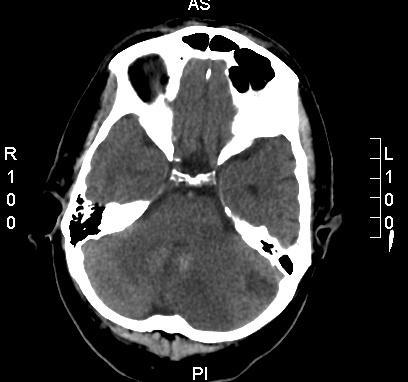
41 Cerebellar stroke
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
PAPER F National Collaborating Centre for Chronic Conditions at the Royal College of Physicians
 6.3 Early carotid imaging in acute stroke or TIA Evidence Tables IMAG4: Which patients with suspected stroke/tia should be referred for urgent carotid imaging? Reference Ahmed AS, Foley E, Brannigan AE
6.3 Early carotid imaging in acute stroke or TIA Evidence Tables IMAG4: Which patients with suspected stroke/tia should be referred for urgent carotid imaging? Reference Ahmed AS, Foley E, Brannigan AE
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Stroke and transient ischaemic attack -
 Stroke and transient ischaemic attack Stroke and transient ischaemic attack - cerebrovascular accident unspecified G66) I60-I64, G45 (Clinical term: Stroke and Presenting complaints Usually sudden on-set
Stroke and transient ischaemic attack Stroke and transient ischaemic attack - cerebrovascular accident unspecified G66) I60-I64, G45 (Clinical term: Stroke and Presenting complaints Usually sudden on-set
The Psychiatrist s Guide to TIA and Stroke
 The Psychiatrist s Guide to TIA and Stroke Dr Sam Limaye Consultant Stroke Physician, LTHT Key Learning Outcomes understand recent advances and current practice in the diagnosis, investigation, and management
The Psychiatrist s Guide to TIA and Stroke Dr Sam Limaye Consultant Stroke Physician, LTHT Key Learning Outcomes understand recent advances and current practice in the diagnosis, investigation, and management
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide
 User Guide") New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
How well does the Oxfordshire Community Stroke Project classification predict the site and size of the infarct on brain imaging?
 558 Neurosciences Trials Unit, Department of Clinical Neurosciences, Western General Hospital, Edinburgh EH4 2XU, UK G E Mead S C Lewis J M Wardlaw M S Dennis C P Warlow Correspondence to: Dr S C Lewis,
558 Neurosciences Trials Unit, Department of Clinical Neurosciences, Western General Hospital, Edinburgh EH4 2XU, UK G E Mead S C Lewis J M Wardlaw M S Dennis C P Warlow Correspondence to: Dr S C Lewis,
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
GOVERNANCE BOARD. 14th January Clinical Audit of Stroke Services. At Shrewsbury and Telford Hospitals NHS Trust
 GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
Stroke/Carotid Artery Disease Outcome Detail (Form 121/132)
") In Ext2 these outcomes are only adjudicated for Medical Record Cohort (MRC) ppts. ID WHI Participant Common ID Col#1 ASCSOURCE Ascertainment Source Col#2 1 Local Form 121 1,112 14.4 2 Central Form 121
In Ext2 these outcomes are only adjudicated for Medical Record Cohort (MRC) ppts. ID WHI Participant Common ID Col#1 ASCSOURCE Ascertainment Source Col#2 1 Local Form 121 1,112 14.4 2 Central Form 121
Standard NICE (CG ) RCP (2016)
 RCP (2016)") Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
TRANSIENT ISCHEMIC ATTACK (TIA)
") TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
Emergently? Michigan Institute for Neurological Disorders. Garden City Hospital, Garden City, Michigan
 Why Should TIA be Treated Emergently? Anne M. Pawlak, D.O. F.A.C.N. Michigan Institute for Neurological Disorders Director Neurology Residency Program, Garden City Hospital, Garden City, Michigan According
Why Should TIA be Treated Emergently? Anne M. Pawlak, D.O. F.A.C.N. Michigan Institute for Neurological Disorders Director Neurology Residency Program, Garden City Hospital, Garden City, Michigan According
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Emergency Department Stroke Registry Indicator Specifications 2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates)
") 2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates) Summary of Changes I62.9 added to hemorrhagic stroke ICD-10-CM diagnosis code list (table 3) Measure Description Methodology Rationale Measurement
2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates) Summary of Changes I62.9 added to hemorrhagic stroke ICD-10-CM diagnosis code list (table 3) Measure Description Methodology Rationale Measurement
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
PFO closure group total no. PFO closure group no. of males
 Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Stroke/Carotid Artery Disease Outcome Detail (Form 121/132, CaD ppts)
") This file contains outcomes collected through the end of Ext1. ID WHI Participant Common ID Col#1 N Missing 0 ASCSOURCE Ascertainment Source Col#2 1 Local Form 121 241 14.9 2 Central Form 121 112 6.9 3
This file contains outcomes collected through the end of Ext1. ID WHI Participant Common ID Col#1 N Missing 0 ASCSOURCE Ascertainment Source Col#2 1 Local Form 121 241 14.9 2 Central Form 121 112 6.9 3
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Therapy for Acute Stroke. Systems of Care for TIA
 Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
P1: OTA/XYZ P2: ABC c01 BLBK231-Ginsberg December 23, :43 Printer Name: Yet to Come. Part 1. The Neurological Approach COPYRIGHTED MATERIAL
 Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Referral Guideline for Patients with TIA
 DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
Understanding transient ischaemic attack
 chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
Strategies for Stroke
 Ischemic stroke is a complex disease, the management of which involves features of cardiology, internal medicine and rehabilitative medicine. Is there a thorough, yet simplified, approach to acute ischemic
Ischemic stroke is a complex disease, the management of which involves features of cardiology, internal medicine and rehabilitative medicine. Is there a thorough, yet simplified, approach to acute ischemic
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS
 STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
Dizziness: Neurological Aspect
 Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to
 It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
Suspected neurological conditions: clinical questions
 Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
How do we assess risk in TIA?
 How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
Development of an RANP role, Acute Medicine. Emily Bury RANP, Acute Medicine
 Development of an RANP role, Acute Medicine Emily Bury RANP, Acute Medicine Background 2010 National Acute Medicine Programme NAMP recommends established the in development of ANP Ireland. posts with emphasis
Development of an RANP role, Acute Medicine Emily Bury RANP, Acute Medicine Background 2010 National Acute Medicine Programme NAMP recommends established the in development of ANP Ireland. posts with emphasis
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL The following is a list of variables and how to complete each one:
 MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA)
") NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA) Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers
NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA) Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
The Silent and Apparent Neurological Injury in Transcatheter Aortic Valve Implantation Study (SANITY)
") The Silent and Apparent Neurological Injury in Transcatheter Aortic Valve Implantation Study (SANITY) Jonathon Fanning, Allan Wesley, Darren Walters, Eamonn Eeles, David Platts, John Fraser The University
The Silent and Apparent Neurological Injury in Transcatheter Aortic Valve Implantation Study (SANITY) Jonathon Fanning, Allan Wesley, Darren Walters, Eamonn Eeles, David Platts, John Fraser The University
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK
 Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Management of Acute Confusional State in Older People
 Management of Acute Confusional State in Older People BACKGROUND Acute confusional state or delirium occurs in 15-20% of all admissions to hospital. It is more likely to occur on a background of pre existing
Management of Acute Confusional State in Older People BACKGROUND Acute confusional state or delirium occurs in 15-20% of all admissions to hospital. It is more likely to occur on a background of pre existing
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
The Big 3 of Vertigo
 They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
TIA triage in Not all that glitters is gold
 TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
What could be reffered to as dizziness by the patient?
 What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Vertebrobasilar Insufficiency
 Equilibrium Res Vol. (3) Vertebrobasilar Insufficiency Toshiaki Yamanaka Department of Otolaryngology-Head and Neck Surgery, Nara Medical University School of Medicine Vertebrobasilar insufficiency (VBI)
Equilibrium Res Vol. (3) Vertebrobasilar Insufficiency Toshiaki Yamanaka Department of Otolaryngology-Head and Neck Surgery, Nara Medical University School of Medicine Vertebrobasilar insufficiency (VBI)
Acute Vestibular Syndrome (AVS) 12/5/2017
 12/5/2017") Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary