Stroke in the Emergency Room: What do we need to know?
|
|
|
- Maryann Blair
- 5 years ago
- Views:
Transcription

1 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1
2 Outline Definition Introduction ti Clinical Presentation Differential diagnosis Urgent assessment in the ER Intravenous thrombolysis Post thrombolysis care 3 Definition A STROKE is an acute, non convulsive neurologic dfiit deficit 3 types: ischemic, Intracerebral hemorrhage, subarachnoid hemorrhage Diagnosis is clinical Imaging and laboratory data help differentiate the type of stroke, and confirm the diagnosis 4 2


3 5 Introduction Stroke is an emergency The non emergent approach to treating stroke is replaced by a rapid and systematic approach (time limited treatment) Early assessment + intervention start in the pre hospital setting Therefore, initial minutes hour in ED are crucial 6 3
4 Clinical Presentation History is very important (>> examination) SUDDEN weakness SUDDEN numbness/sensory deficits SUDDEN loss of ability to understand, produce speech SUDDEN dysarthria SUDDEN vision loss (monocular or binocular) SUDDEN imbalance, vertigo, dizziness 7 Clinical Presentation Pain is not a common symptom of stroke Headache more common with ICH, SAH Other pain (Chest, retro orbital, cervical) might signal underlying cause of stroke Aortic dissection, AMI, carotid/vertebral artery dissection Memory loss is not a symptom of stroke Transient Global Amnesia (TGA) 8 4
 involved")

5 Clinical Presentation Localization Loss of consciousness occur in stroke when: Brainstem (ARAS) involved Extensive bihemispheric involvement Bi thalamic involvement Large ICH with tissue shifts/midline structures IVH SAH
")

;")

6 Clinical Presentation Localization Language disturbances (aphasia) Dominant hemisphere cortical/immediate subcortical area Agnosia (neglect, inability to perceive sensory stimulation); Apraxia Non dominant hemisphere cortical/immediate subcortical area Anosognosia, asomatognosia
7 Clinical Presentation Localization Forced gaze deviation Away from the weak side: ipsilateral frontal, ipsilateral thalamic To the weak side: contralateral pons, contralateral thalamic Bilateral ptosis/apraxia of eyelid opening (gives the false impression of sleepiness) Non dominant hemisphere (large) 13 Clinical Presentation Localization Visual fields cut (HH, HQ) Contralateral occipital, posterior parietal, medial temporal lesion Visual loss Monocular: retina Binocular: bilateral occipital 14 7
8 Clinical Presentation Localization Diplopia (double vision) Monocular: retinal, vitreal, corneal, conversion/malingering Binocular: thalamus, midbrain, pons, cerebellar INO (MLF lesion medial midbrain, pons) Skew deviation Thalamus, cerebellum, pons Vertigo, dizziness Brainstem, cerebellum, inner ear apparatus
9 Clinical Presentation Localization Dilated, unreactive pupils Midbrain (CN III nuclei, fibers) Pinpoint pupils Pons, thalamus Midposition pupils midbrain i 17 Differential Diagnosis Stroke mimics Seizures Non convulsive Complex partial (confusion, aphasia) Post ictal state, post ictal weakness/paralysis Migraine (complicated or hemiplegic) Hypoglycemia, hyperglycemia Peripheral nerve injuries/palsies (not acute) Syncope/cardiac arrhythmias Conversion, malingering 18 9
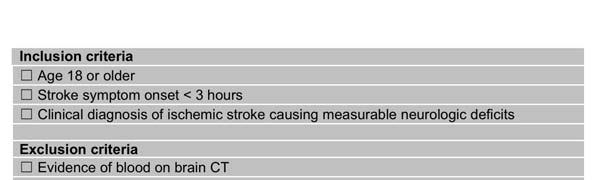
10 Urgent assessment in the ER ABC, O 2 if needed, IV access, CBC, coags, BMP History. Particular attention to establishing last known well time Code stroke: a stroke team member at bedside in 15 min CTbrain (non contrasted): differentiate ICH, SAH and others, from IS MRI should not delay thrombolysis if indicated 19 Urgent assessment in the ER Review inclusion & exclusion criteria for thrombolysis Discuss with patient and family members EKG, CXRay, CE (should not delay thrombolysis) Aggressively treat hyper and hypoglycemia, hyperthermia 20 10

 Loss of")
 Unilateral")

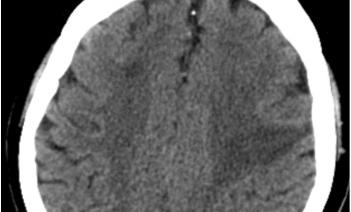
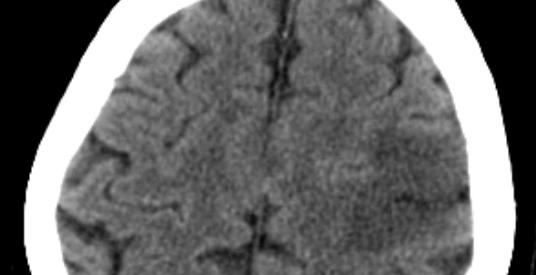
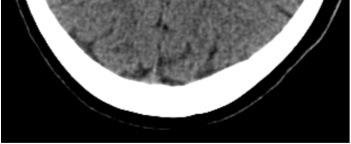
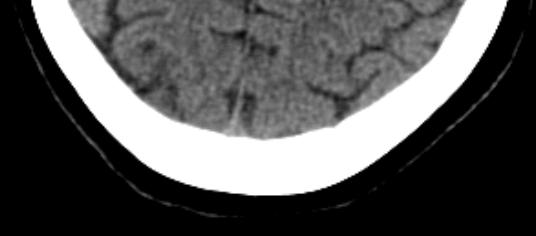
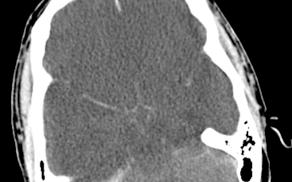
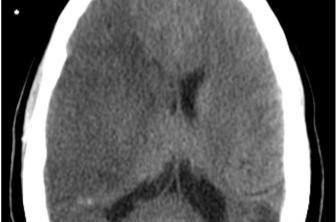
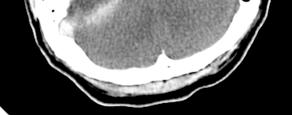
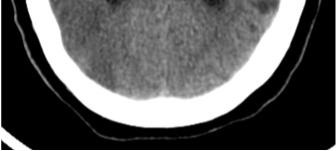
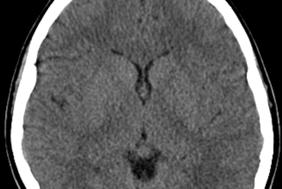
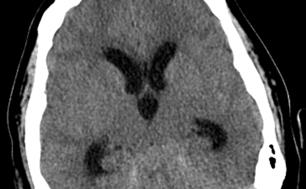
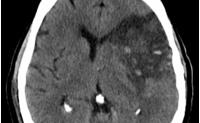
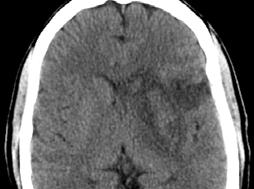
11 Urgent assessment in the ER Signs of early ischemia on CT: Loss of Gray white differentiation Loss of differentiation of cortical ribbon (insular cortex) Loss of differentiation of caudate head and surrounding white matter (IC) Unilateral dense MCA sign CT also helpful to look for complications Cerebral edema HCP Hemorrhagic conversion
12

13



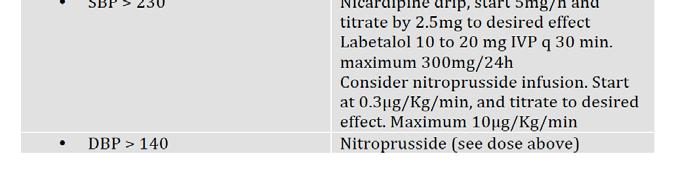
14 Urgent assessment in the ER blood pressure treatment in IS 27 Urgent assessment in the ER blood pressure treatment in IS 28 14


15 IV thrombolysis Remains the only approved acute therapy for ischemic i stroke 29 Tissue plasminogen activator Tissue plasminogen activator plasminogen plasmin plasmin plasmin Fibrin Fibrinogen 30 15
16 31 IV thrombolysis 32 16
: Age > 80y Severe stroke (NIHSS score>25 or >1/3 of MCA territory on CT")
17 33 IV thrombolysis up to 4.5h Exclusion (different than 0 to 3 hours): Age > 80y Severe stroke (NIHSS score>25 or >1/3 of MCA territory on CT or MRI) Patients on oral anticoagulants regardless of INR Previous stroke AND Diabetes 34 17
 Widely adopted in most stroke centers Benefit < than that seen between 0 3h Consent; adherence to")
 10% of dose given as bolus over 1 min 90% infusion over one hour Pharmacokinetics Half life 10 to 15 min")
18 Implications of ECASS III AHA guidelines: IV t PA should be considered for eligible ibl patients t Not FDA approved yet (approved in Europe) Widely adopted in most stroke centers Benefit < than that seen between 0 3h Consent; adherence to inclusion/exclusion criteria Time is brain 35 IV thrombolysis IV t PA dose 0.9mg/Kg (max 90mg) 10% of dose given as bolus over 1 min 90% infusion over one hour Pharmacokinetics Half life 10 to 15 min Adverse events: Bleeding Angioedema (1 to 2% of patients on ACE ) 36 18
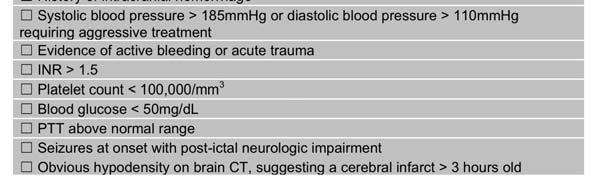
19 Who is eligible to receive IV t PA Clinically Clinical diagnosis of ischemic stroke causing measurable deficit Onset of symptoms < 4.5 hours prior to starting IV t PA No symptoms suggestive of subarachnoid hemorrhage (thunderclap headache, LOC) Symptoms not rapidly improving no head trauma, prior stroke in previous 3 months no history of intracerebral hemorrhage 37 Who is eligible to receive IV t PA Clinically No major surgery in previous 14 days No GI or UT hemorrhage in previous 21 days No arterial puncture at non compressible site in previous 7 days No evidence of active bleeding of major trauma on exam No seizure with post ictal neurologic deficits BPs < 185 mmhg and BPd < 110 mmhg (not requiring more than 3 doses of IV anti hypertensive to lower) 38 19


 Platelets >")

20 Who is eligible to receive IV t PA Laboratory and Imaging Head CT showing no blood (ICH, SDH, SAH, EDH) Platelets > 100,000 INR < 1.5 PTT within normal range Glucose > 50 mg/dl
21 Who is eligible to receive IV t PA Warnings High NIHSS score ( > 22) Older patients ( > 77 years) Patients with early ischemic changes on head CT however, to increase # of patients treated with t PA, and given lack of evidence for most exclusion criteria, many are relaxing criteria to t PA administration (with no increase in rate of complications) 41 IV t PA in the era of new anticoagulants Direct thrombin inhibitors (Dabigatran) Factor Xa inhibitors (Apixaban, Rivaroxaban) 42 21
22 IV t PA in the era of new anticoagulants Direct thrombin inhibitors (Dabigatran) Check thrombin time (TT). 10 min If normal (laboratory/coagulation analyzer specific; sec) proceed with IV t PA regardless of time of last dose Factor Xa inhibitors (Apixaban, Rivaroxaban) Check a prothrombin time If < upper limit of normal (laboratory/coagulation analyzer specific; 15.7 sec) proceed with IV t PA regardless of time of last dose Written consent 43 Beyond IV thrombolysis if onset > 4.5h OR patient ineligible for IV t PA OR fails to improve following IV t PA OR on new oral AC, consider other interventions IA t PA Mechanical embolectomy and thrombectomy 44 22
23 Post thrombolysis care Following t PA administration: BP check and control (ok in arm with IV) Frequent neurologic evaluation (beware new HA or one with changing characteristics) NIHSS at 24 hours No invasive procedure unless necessary No ASA, Plavix, or Aggrenox. No Lovenox or Heparin x 24 hours NPO until swallowing evaluated ±CT head at 24 hours

, type and screen If bleeding:")
24 Complications following t PA Beware angioedema Treat with steroids, H1 and H2 blockers for 24h (or longer if needed) Bruising common. If severe in one place, consider Fx Mucosal bleeding is usually self limited and does not require any specific therapy Deterioration and/or new HA warrants brain CT, stopping infusion (if ongoing), type and screen If bleeding: PLTS, cryoprecipitate, FFP 47 Stroke mimics and IV t PA Risk of complications is low to non existent 48 24



25 Stroke mimics and IV t PA
26 Thank You 26
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology
 Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Page 1 of 7. Intraparenchymal hemorrhage or subarachnoid hemorrhage. Consult neurosurgery
 Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Acute Ischemic Stroke Mechanism, Diagnosis, Treatment
 Acute Ischemic Stroke Mechanism, Diagnosis, Treatment IM Resident Lecture December 2016 Mohammad Shafie, MD PhD MEng Department of Neurology UC Irvine Objectives Better understanding of stroke mechanisms
Acute Ischemic Stroke Mechanism, Diagnosis, Treatment IM Resident Lecture December 2016 Mohammad Shafie, MD PhD MEng Department of Neurology UC Irvine Objectives Better understanding of stroke mechanisms
HYPERACUTE STROKE CASE STUDIES. By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH
 HYPERACUTE STROKE CASE STUDIES By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH MC Case study 82 years old, lady 9:30 well, in touch with her son 11:30 hairdresser came to her house and found her
HYPERACUTE STROKE CASE STUDIES By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH MC Case study 82 years old, lady 9:30 well, in touch with her son 11:30 hairdresser came to her house and found her
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Updated tpa Guidelines: Expanding the opportunity for good outcomes. Benjamin Morrow, MSN RN UPMC Stroke Institute
 Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Standard NICE (CG ) RCP (2016)
 RCP (2016)") Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
ED Stroke Panel Page 1 of 2
 ED Stroke Panel Page 1 of 2 Reference EMMC *************************Usec: Call Operator to page a Stroke Alert ********************** Laboratory Bedside Glucose Monitoring ONCE Notify provider if glucose
ED Stroke Panel Page 1 of 2 Reference EMMC *************************Usec: Call Operator to page a Stroke Alert ********************** Laboratory Bedside Glucose Monitoring ONCE Notify provider if glucose
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Brain Attacks and Acute Stroke Management
 Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
When Not To Give TPA Steve Phillips Division of Neurology
 When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Inclusion criteria Cautionary inclusion Exclusion criteria 1. Diagnosis of ischemic stroke causing measurable neurological deficit.
 Guidelines for the use of IV recombinant tissue plasminogen activator (rt-pa), Endovascular Thrombectomy (EVT), or rt-pa+evt in the treatment of acute ischemic stroke at Kingston General Hospital Rationale
Guidelines for the use of IV recombinant tissue plasminogen activator (rt-pa), Endovascular Thrombectomy (EVT), or rt-pa+evt in the treatment of acute ischemic stroke at Kingston General Hospital Rationale
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
The Language of Stroke
 The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
 Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,