Albumin In SubArachnoid Hemorrhage: The ALISAH Study
|
|
|
- Allen Todd
- 6 years ago
- Views:
Transcription
1 Albumin In SubArachnoid Hemorrhage: The ALISAH Study Jose I Suarez, M.D. Professor of Neurology Neurointensivist and Vascular Neurologist Head Section of Neurocritical Care and Vascular Neurology Department of Neurology Baylor College of Medicine, Houston, TX Baylor St Luke s Medical Center
2 SAH: epidemiology Leading cause of non-traumatic SAH is aneurysmal rupture: 37,000/y in US Mean age of presentation is 55 and women are more likely than men to experience it (1.6:1.0) The average case fatality for SAH is 51%, with approximately one third of survivors remaining dependent
3 SAH: complications Virtually everybody experiences a medical complication SAH patients are critically ill In about 40% of cases complications are lifethreatening Anticipating and preventing complications is very important
4 SAH: complications Delayed Cerebral Ischemia (46% of patients) Vasospasm Emboli Microthrombi formation Hydrocephalus (20%) Rebleeding (7%) Seizures (24%) Hyponatremia (30%)
5 Schematic review of the complex interplay of secondary insults leading to secondary brain damage after SAH Springborg, J. B. et al. Br. J. Anaesth : with permission

6 Human Albumin He & Carter, Nature 1992;358:
7 25% Human Albumin Wilkes & Navickis: small-trial bias favoring control group: no evidence that albumin affected mortality: RR for death 1.1 (CI ) (Ann Int Med 2001;135:149-64) Cochrane Library report: neither improved outcome nor increased survival (Cochrane Database Syst Rev 2002;2:CD000567) SAFE: randomized double-blind controlled trial of fluid resuscitation in the intensive care: similar outcomes at 28 days; treated group (4% human albumin) achieved better intravascular treatment (N Engl J Med 2004;350: )
8 Features SAH and ALB (Suarez et al., J Neurosurg 2004;100:585-90) Group 1 with HA (n=37) Group 2 without HA (n=47) Age in years 53.0± ± Hospital days 15.8± ±6 0.2 In-hospital death (%) Hypomagnesemi a after admission (%) p-value <0.001 CHF (%) Hydrocephalus (%) Sympt VSP (%) Hospital cost 62±39 81± (thousands US$) GOS 2 (%) <0.05 Logistic regression (adjusting for age, sex, race, GCS, head CT on admission) the use of HA was Independently associated with good outcome (OR 3.2, 95%CI )

9
10 Albumin in Subarachnoid Hemorrhage (ALISAH) Study Supported by the NINDS 1RO1NS Study intervention provided by: GRIFOLS International IND sponsored by FDA: BB-IND # ClinicalTrials.gov Identifier: NCT
11 ALISAH ALISAH was a three-year multicenter open-label nonrandomized dose-finding clinical trial funded by NINDS ALISAH was to include a maximum of 80 patients with SAH Six centers recruited patients: BCM (St Luke s and Ben Taub Hosp), Johns Hopkins (JHH and Bayview Hosp), U of Toronto, Penn State, U of Calgary, Case Western Reserve University Data Coordinating Center: Medical University of South Carolina
12 ALISAH Aims Determine the maximum tolerated dose of ALB therapy based on the rate of treatment related serious adverse events during treatment: severe-to-life-threatening heart failure and anaphylactic reaction. Obtain preliminary estimates of the ALB treatment effect using (1) the incidence of symptomatic vasospasm within 15 days after symptom onset, (2) Glasgow Outcome Scale, (3) Barthel Index, (4) modified Rankin Scale, (5) NIH Stroke Scale, and (6) Stroke Impact Scale at 3 months.
13 ALISAH: ALB Dosage Regimen: 70 kg person Dosage level number Dosage (g/kg body weight/da yx 7days) Volume to infuse (ml) per day Infusion rate (ml/hour) Dosage delivery time (hours)

14
15
16 Results (Suarez JI et al., Acta Neurochirurgica 2015) Outcome Tier 1 (0.625 Tier 2 (1.25 Tier 3 (1.875 All groups g/kg) g/kg) g/kg) TCD vasospasm 15/20 (75%) 11/20 (55%) 2/7 (28.6%) 28/47 (59.6%) DCI 4/20 (20%) 3/20 (15%) 1/7 (14.3%) 8/47 (17%) Cerebral infarction: 5/11 (45%) 3/18 (16%) 1/4 (25%) 9/33 (27%) - New 3/11 (27%) 3/18 (16%) 0 6/33 (18%) - Old 2/11 (18%) 0 1/4 (25%) 3/33 (9%) - Vascular All MCA 1 MCA, 2 ACA MCA 7 MCA, 2 ACA territory
17 ALISAH II We wanted to undertake a Phase II study: Futility analysis design Discussions with NINDS: Concerns about wasting time and money Concerns about trial fatigue Decision to move to a Phase III clinical trial
18 ALISAH III A multicenter blinded, randomized, controlled Phase III design Study period: 4-5 years Study population:18-80 year old patients presenting within 72 hours of SAH Study sites: 85 sites from North America, South America, Australia and New Zealand, Hong Kong, and Europe
19 ALISAH II Phase III randomized, placebo-controlled clinical trial NSDK review: Why Phase III at this stage? Resubmit as Phase II Wait for ALIAS to be completed It has not worked for other conditions Is human albumin still used for SAH? More animal data
20 Human Albumin Usage Survey
21 Albumin usage questionnaire We constructed a 27-question survey to gauge intensivists views on their current use of human albumin in SAH patients. We obtained IRB approval at the Baylor College of Medicine Survey was ed to members of the Neurocritical Care Society (NCS), and selected practitioners caring for SAH patients from Canada (members of CCCTG), Australia and New Zealand (ANZICS-CTG) and Hong Kong (Chinese University of Hong Kong) Time line: 11/15/12 12/15/12
22 Results We received 361 responses Response rate: NCS: 50% Canada: 100% Australia: 100% Hong Kong: 100% Most responders were physicians (80%) who work in academic institutions (73%)


23 Does your hospital have a set protocol for SAH management? Does your protocol include human albumin administration? Do you administer human albumin outside your management protocol?


24 Human albumin concentration commonly used Indications for human albumin administration

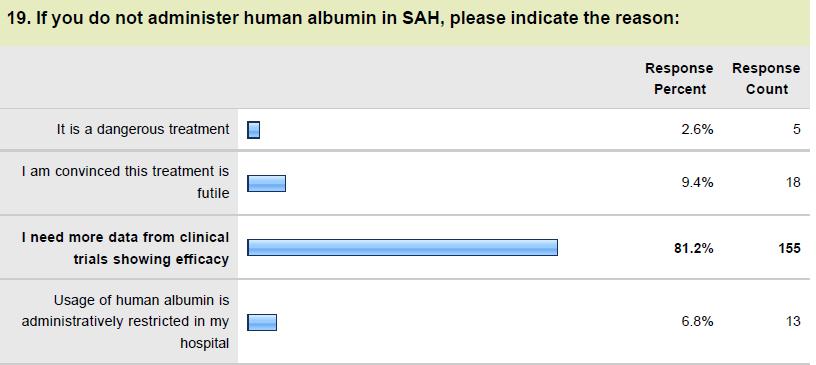
25


26


27
28 Albumin Use in US Academic Centers: UHC database Suarez JI et al, Crit Care Med 2016 In Press
29 METHODS We used the University HealthSystem Consortium (UHC) database to identify all hospitalized adult patients ( 18 years of age) who received albumin between 2009 and 2013 including SAH patients UHC is an alliance of more than 90% of academic medical centers in the US (120 academic medical centers and their 299 affiliated hospitals
30 UHC database: 12,366,264 records Trends in Patients' Receiving Albumin as a Percent of All Inpatients Discharged Between 2009 and 2013 by Year and Type of Hospitalization Patients Receiving Albumin as % of All Discharges 16% 14% 12% 10% 8% 6% 4% 2% 0% 15.1% 14.1% 13.4% 11.7% 12.4% 7.5% 6.2% 6.5% 6.8% 7.1% 2.5% 2.7% 2.7% 2.9% 3.0% Year of Discharge of Patients All cases Surgical Medical
31 UHC database: 12,366,264 records 12% Trend in Mortality by Albumin Administration Status 10% 10.6% 10.1% 9.6% 9.4% 9.1% 8% Mortality, % 6% 4% 2% 2.34% 2.31% 2.32% 2.31% 2.35% 1.80% 1.78% 1.79% 1.77% 1.79% 0% Year of Discharge from Hospital No albumin Received albumin All discharges
32
33 Albumin use is SAH: UHC database We studied 38,066 adult SAH patients: 8,413 (22%) received HA and 29,653 (78%) did not. Most patients were White (61%) and female (67%). HA use has remained low and unchanged in medical patients but has decreased in surgical cases, especially in higher-volume centers. Patients with low SOI had a higher mortality rate (4.0% in albumin group and 0.9% in non-albumin group, p < 0.001), whereas those with high SOI had a significantly lower mortality rate (28.8% in albumin group and 45.5% in no albumin group, p < 0.001). Surgical cases that received albumin had lower mortality compared to medical cases (30.0% vs 4.0%). Mortality rates were lower in surgical cases that received albumin compared to those who did not (25.5% vs 34.6%).

34


35
36 UHC database: SAH (n=30,461) Trend in Albumin Use Among Surgical SAH Patients by Center Average Annual SAH Volume Trend in Albumin Use Among Medical SAH Patients by Center Average Annual SAH Volume 50% 50% 45% 45% 40% 40% 35% 35% 30% 25% 20% 15% < > 60 30% 25% 20% 15% < > 60 10% 10% 5% 5% 0% %
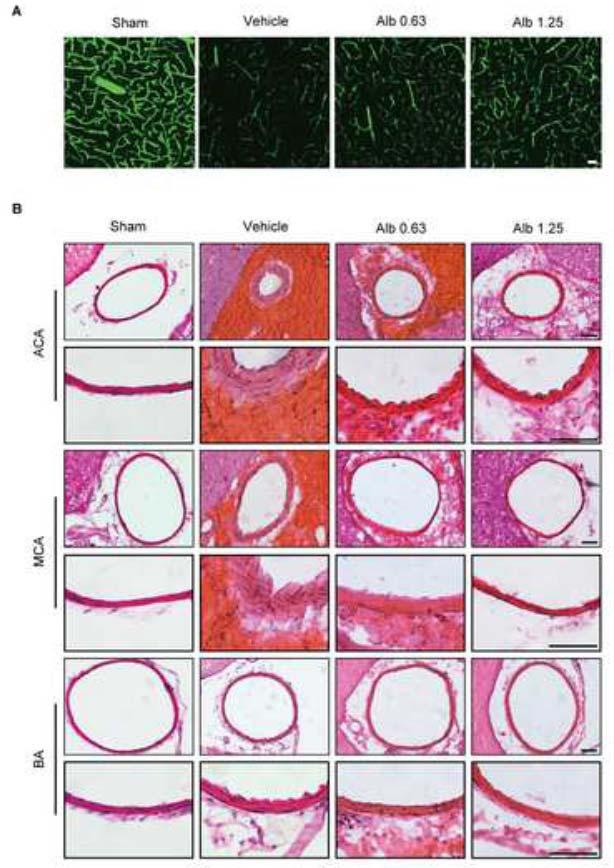
37 Recent Animal Data
38 Critical Care Medicine, 2015

39

40

41
42 What s next?
43 ALISAH II
44 ALISAH II The proposed ALISAH II study will be a five-year multicenter, adaptive randomized, placebo-controlled, double-masked Phase II clinical trial investigating the futility of the administration of 25% HA compared to placebo in SAH patients
45 Primary Aim AIM 1 is to determine the potential of 25% HA for further development and application in patients with SAH. The primary null hypothesis is that the intervention (25% HA) reduces the proportion of patients with poor outcome compared to the hypothesized poor outcome rate: duration Primary efficacy outcome measure is the GOS, dichotomized to define poor functional outcome as GOS 3 at 90 days.
46 AIM 2 To assess further safety of 25%HA: Incidence of neurological deterioration within 15 days after symptom onset; Incidence of rebleeding, hydrocephalus, seizures, and delayed cerebral ischemia within 15 days; Incidence of delayed cerebral ischemia (with and without vasospasm) within 15 days; Plasma osmolality and serum albumin within 15 days; Serum magnesium, blood pressure, and heart rate within 15 days; BI, mrs, NIHSS, MOCA and Stroke Impact Scale at 3 and 6 months.
47 AIM 3 To determine feasibility of effectively blinding therapeutic interventions. We will mask both saline placebo and 25% HA. A questionnaire will be prepared for distribution to each site after every patient is enrolled.
48 AIM 4 To evaluate feasibility of application of study protocol in a larger number of sites ALISAH II will have between clinical sites in the US and Canada (NIH StrokeNet and Neurocritical Care Research Network NCRN).
49 Proposed design Eligible subjects will be randomized to either HA (4 arms) or normal saline placebo (1 arm) and the primary outcome will be assessed at the 90-day clinic visit. The 4 HA treatment arms will be as follows: 1.25 g/kg/d x 7 days; 1.25 g/kg/d x 5 days; 1.25 g/kg/d x 3 days; and 1.25 g/kg/d x 1 day.
50 Proposed design ALISAH II will follow a novel adaptive design and will proceed in six stages. As the trial progresses no interim hypothesis tests will be conducted. Rather, the interim goal will be to allocate a majority of the albumin treated patients to the arm with the maximum effect through a response adaptive allocation (RAR) algorithm. Upon completion of the trial, a hypothesis test comparing the maximum effect arm and the control will be conducted.
51 Albumin in Subarachnoid Hemorrhage Trial (ALISAH II) Stage I Stage II Stage III Stage IV Stage V Stage VI Control (N = 100) N = 35 N = 13 N = 13 N = 13 N = 13 N = 13 Albumin (N = 225) N = 80 1:1:1:1 N = 29 RAR N = 29 RAR N = 29 RAR N = 29 RAR N = 29 RAR
52 Purpose of adaptive design This adaptive design seeks to answer two questions: (1) Which duration yields the maximum treatment effect, and (2) Is the selected duration non-futile when compared to a saline control.
53 Inclusion Criteria Patients (male or female) must be at least 18 but younger than 80. Onset of new neurological signs of SAH within 72 hours of initiation of treatment with 25% HA. Clinical signs consistent with the diagnosis of SAH including severe thunderclap headache, cranial nerve abnormalities, decreased level of consciousness, meningismus and focal neurological deficits. Head CT demonstrates SAH (modified Fisher rating scale 2-4). DSA or CTA reveals the presence of saccular aneurysm(s) in a location that explains the SAH. Treatment of cerebral aneurysm carried out prior to treatment initiation and within 72 hours of symptom onset. (Accepted treatments of aneurysms include surgical clipping or endovascular embolization.) Signed and dated informed written consent by the subject or his/her legallyauthorized representative (LAR). 25%HA infusion must be initiated within 72 hours of SAH symptom onset
54 Exclusion Criteria Time of symptom onset cannot be reliably assessed. No demonstrable aneurysm by DSA or CTA. Evidence of traumatic, mycotic, or fusiform aneurysm by DSA. World Federation of Neurological Surgeons (WFNS) scale of V Head CT rating scale of 0 1 History within the past 6 months, and/or physical findings on admission of decompensated heart failure (NYHA Class III and IV or heart failure requiring hospitalization) Patient has received HA prior to treatment assignment during the present admission. Hospitalization for or diagnosis of acute coronary syndrome (AMI) within the preceding 3 months Symptoms or electrocardiographic signs indicative of AMI on admission
55 Exclusion Criteria ECG evidence and/or physical findings compatible with second- or third-degree heart block, or ofcardiac arrhythmia associated with hemodynamic instability Echocardiogram performed before treatment revealing a left ventricular ejection fraction < 40% Serum creatinine > 2.0 mg/dl or creatinine clearance < 50 ml/min Pregnancy, lactation or parturition within previous 30 days Known allergy to albumin
56 Exclusion Criteria Severe prior physical disability that precludes evaluation of clinical outcome measures (mrs > 2) History of severe chronic obstructive lung disease (FEV1 < 50% predicted, increased shortness of breath, repeated exacerbations which have an impact on patients quality of life, and a fixed ratio postbronchodilator FEV1/FVC <0.7) History of confirmed or suspected liver failure (increased prothrombin time, elevated liver enzymes, hypoalbuminemia, and hyperbilirrubinemia with or without peripheral edema and encephalopathy) Current participation in another drug treatment protocol Severe terminal disease with life expectancy less than 6 months Inability to follow the protocol or return for the 90-day visit



57


58 Thank you! Baylor St Luke s Medical Center
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F.
 THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
(aneurysmal subarachnoid hemorrhage, 17%~60% :SAH. ,asah , 22%~49% : Willis. :1927 Moniz ;(3) 2. ischemic neurological deficit,dind) SAH) SAH ;(6)
 2. ischemic neurological deficit,dind) SAH) SAH ;(6)") ,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Clinical Review of 20 Cases of Terson s Syndrome
 34 Clinical Review of 20 Cases of Terson s Syndrome Takashi SUGAWARA, M.D., Yoshio TAKASATO, M.D., Hiroyuki MASAOKA, M.D., Yoshihisa OHTA, M.D., Takanori HAYAKAWA, M.D., Hiroshi YATSUSHIGE, M.D., Shogo
34 Clinical Review of 20 Cases of Terson s Syndrome Takashi SUGAWARA, M.D., Yoshio TAKASATO, M.D., Hiroyuki MASAOKA, M.D., Yoshihisa OHTA, M.D., Takanori HAYAKAWA, M.D., Hiroshi YATSUSHIGE, M.D., Shogo
a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)).
).") 12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
2016 Top Papers in Critical Care
 2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience
2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience
はじめに 対象と方法 39: , 2017 SAH 183 WFNS
 39:107 原 著 39: 107 112, 2017 1 2 1 1 1 1 要旨 SAH 2010 1 2013 12 SAH 253 183 64 70 WFNS I III 72.7 Fisher CT 3 86.3 19.9 16.6 GR MD 73.2 73.1 80 WFNS Key words: subarachnoid hemorrhage, prognosis, rate of
39:107 原 著 39: 107 112, 2017 1 2 1 1 1 1 要旨 SAH 2010 1 2013 12 SAH 253 183 64 70 WFNS I III 72.7 Fisher CT 3 86.3 19.9 16.6 GR MD 73.2 73.1 80 WFNS Key words: subarachnoid hemorrhage, prognosis, rate of
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
N E W T O N. Hänggi D, Etminan N, Macdonald RL, Steiger HJ, Mayer SA, Aldrich F, Diringer MN, Hoh BJ, Mocco J, Strange P, Faleck HJ, Miller M
 N E W T O N Nimodipine microparticles to Enhance recovery While reducing TOxicity after subarachnoid hemorrhage Phase 1/2a Multicenter, Controlled, Randomized, Open Label, Dose Escalation, Safety, Tolerability,
N E W T O N Nimodipine microparticles to Enhance recovery While reducing TOxicity after subarachnoid hemorrhage Phase 1/2a Multicenter, Controlled, Randomized, Open Label, Dose Escalation, Safety, Tolerability,
The Albumin in Subarachnoid Hemorrhage (ALISAH) Multicenter Pilot Clinical Trial Safety and Neurologic Outcomes
 Multicenter Pilot Clinical Trial Safety and Neurologic Outcomes") The Albumin in Subarachnoid Hemorrhage (ALISAH) Multicenter Pilot Clinical Trial Safety and Neurologic Outcomes Jose I. Suarez, MD; Renee H. Martin, PhD; Eusebia Calvillo, RN; Catherine Dillon, RN; Eric
The Albumin in Subarachnoid Hemorrhage (ALISAH) Multicenter Pilot Clinical Trial Safety and Neurologic Outcomes Jose I. Suarez, MD; Renee H. Martin, PhD; Eusebia Calvillo, RN; Catherine Dillon, RN; Eric
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD
 Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD") FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
The Albumin in Subarachnoid Hemorrhage (ALISAH) Multicenter Pilot Clinical Trial Safety and Neurologic Outcomes
 Multicenter Pilot Clinical Trial Safety and Neurologic Outcomes") The Albumin in Subarachnoid Hemorrhage (ALISAH) Multicenter Pilot Clinical Trial Safety and Neurologic Outcomes Jose I. Suarez, MD; Renee H. Martin, PhD; Eusebia Calvillo, RN; Catherine Dillon, RN; Eric
The Albumin in Subarachnoid Hemorrhage (ALISAH) Multicenter Pilot Clinical Trial Safety and Neurologic Outcomes Jose I. Suarez, MD; Renee H. Martin, PhD; Eusebia Calvillo, RN; Catherine Dillon, RN; Eric
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Canadian Best Practice Recommendations for Stroke Care 3.6 Acute Subarachnoid Hemorrhage
 Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Raw and Quantitative EEG for Identification of Ischemia
 Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group
 Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital
 ISPUB.COM The Internet Journal of Neurosurgery Volume 9 Number 2 Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital A Granger, R Laherty Citation A Granger, R Laherty.
ISPUB.COM The Internet Journal of Neurosurgery Volume 9 Number 2 Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital A Granger, R Laherty Citation A Granger, R Laherty.
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
GSK Medicine: Study Number: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Predictors of Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage: A Cardiac Focus
 Neurocrit Care (2010) 13:366 372 DOI 10.1007/s12028-010-9408-4 ORIGINAL ARTICLE Predictors of Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage: A Cardiac Focus Khalil Yousef Elizabeth
Neurocrit Care (2010) 13:366 372 DOI 10.1007/s12028-010-9408-4 ORIGINAL ARTICLE Predictors of Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage: A Cardiac Focus Khalil Yousef Elizabeth
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
Canadian Stroke Best Practices Table 3.3A Screening and Assessment Tools for Acute Stroke
 Canadian Stroke Best Practices Table 3.3A Screening and s for Acute Stroke Neurological Status/Stroke Severity assess mentation (level of consciousness, orientation and speech) and motor function (face,
Canadian Stroke Best Practices Table 3.3A Screening and s for Acute Stroke Neurological Status/Stroke Severity assess mentation (level of consciousness, orientation and speech) and motor function (face,
Table 3.1: Canadian Stroke Best Practice Recommendations Screening and Assessment Tools for Acute Stroke Severity
 Table 3.1: Assessment Tool Number and description of Items Neurological Status/Stroke Severity Canadian Neurological Scale (CNS)(1) Items assess mentation (level of consciousness, orientation and speech)
Table 3.1: Assessment Tool Number and description of Items Neurological Status/Stroke Severity Canadian Neurological Scale (CNS)(1) Items assess mentation (level of consciousness, orientation and speech)
Cerebral Aneurysms. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health
 Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Clinical manifestations, diagnosis and medical management of
 Clinical manifestations, diagnosis and medical management of aneurysmal SAH David Bervini, MD MAdvSurg Department of Neurosurgery Inselspital University of Bern Switzerland 1 2 3 Aneurysmal SAH Incidence:
Clinical manifestations, diagnosis and medical management of aneurysmal SAH David Bervini, MD MAdvSurg Department of Neurosurgery Inselspital University of Bern Switzerland 1 2 3 Aneurysmal SAH Incidence:
Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs)
") Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs) Eric L. Zager, MD University of Pennsylvania Department of Neurosurgery No Disclosures Brain AVMs Incidence ~1 in 100,000
Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs) Eric L. Zager, MD University of Pennsylvania Department of Neurosurgery No Disclosures Brain AVMs Incidence ~1 in 100,000
Product: Omecamtiv Mecarbil Clinical Study Report: Date: 02 April 2014 Page 1
 Date: 02 April 2014 Page 1. 2. SYNOPSIS Name of Sponsor: Amgen Inc. Name of Finished Product: Omecamtiv mecarbil injection Name of Active Ingredient: Omecamtiv mecarbil (AMG 423) Title of Study: A double-blind,
Date: 02 April 2014 Page 1. 2. SYNOPSIS Name of Sponsor: Amgen Inc. Name of Finished Product: Omecamtiv mecarbil injection Name of Active Ingredient: Omecamtiv mecarbil (AMG 423) Title of Study: A double-blind,
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
The tpa Cage Match. Disclosures. Cage Match. Cage Match 1/27/2014. January 8, Advisory Boards
 The tpa Cage Match January 8, 2014 Andy Jagoda, MD, FACEP Professor and Chair of Emergency Medicine Mount Sinai School of Medicine New York, New York Advisory Boards Disclosures Astra Zeneca, Pfizer, CSL
The tpa Cage Match January 8, 2014 Andy Jagoda, MD, FACEP Professor and Chair of Emergency Medicine Mount Sinai School of Medicine New York, New York Advisory Boards Disclosures Astra Zeneca, Pfizer, CSL
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Appendix e-1. University HealthSystem Consortium (UHC) database description
 database description") Appendix e-1. University HealthSystem Consortium (UHC) database description UHC is an alliance of academic medical centers and their affiliated hospitals. Member institutions have the goal of sharing clinical,
Appendix e-1. University HealthSystem Consortium (UHC) database description UHC is an alliance of academic medical centers and their affiliated hospitals. Member institutions have the goal of sharing clinical,
FOCUS: Fluoxetine Or Control Under Supervision Results. Martin Dennis on behalf of the FOCUS collaborators
 FOCUS: Fluoxetine Or Control Under Supervision Results Martin Dennis on behalf of the FOCUS collaborators Background Pre clinical and imaging studies had suggested benefits from fluoxetine (and other SSRIs)
FOCUS: Fluoxetine Or Control Under Supervision Results Martin Dennis on behalf of the FOCUS collaborators Background Pre clinical and imaging studies had suggested benefits from fluoxetine (and other SSRIs)
SPECIALIZED UNITS: DO THEY SAVE LIVES? NEUROCRITICAL CARE
 SPECIALIZED UNITS: DO THEY SAVE LIVES? NEUROCRITICAL CARE David Zygun MD MSc FRCPC Zone Clinical Department Head Critical Care Medicine, Edmonton Zone Professor and Director Division of Critical Care Medicine
SPECIALIZED UNITS: DO THEY SAVE LIVES? NEUROCRITICAL CARE David Zygun MD MSc FRCPC Zone Clinical Department Head Critical Care Medicine, Edmonton Zone Professor and Director Division of Critical Care Medicine
National Collaborating Centre for Chronic Conditions at the Royal College of Physicians
 13. Surgery for acute stroke 13.2 Surgical referral for decompressive hemicraniectomy Reference Gupta R, Connolly ES, Mayer S et al. Hemicraniectomy for massive middle cerebral artery territory infarction:
13. Surgery for acute stroke 13.2 Surgical referral for decompressive hemicraniectomy Reference Gupta R, Connolly ES, Mayer S et al. Hemicraniectomy for massive middle cerebral artery territory infarction:
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Method Hannah Shotton
 #asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
#asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
Disclosures. Objectives. Critical Care Management of Subarachnoid Hemorrhage. Nothing to disclose
 Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Progress Review. Mervyn D.I. Vergouwen, MD, PhD; Rob J. de Haan, PhD; Marinus Vermeulen, MD, PhD; Yvo B.W.E.M. Roos, MD, PhD
 Progress Review Effect of Statin Treatment on Vasospasm, Delayed Cerebral Ischemia, and Functional Outcome in Patients With Aneurysmal Subarachnoid Hemorrhage A Systematic Review and Meta-Analysis Update
Progress Review Effect of Statin Treatment on Vasospasm, Delayed Cerebral Ischemia, and Functional Outcome in Patients With Aneurysmal Subarachnoid Hemorrhage A Systematic Review and Meta-Analysis Update
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial
 Trial") The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
Thrombectomy with the preset stent-retriever. Insights from the ARTESp* trial
 Thrombectomy with the preset stent-retriever Insights from the ARTESp* trial Wiebke Kurre, MD Klinikum Stuttgart - Germany * Acute Recanalization of Thrombo-Embolic Ischemic Stroke with preset (ARTESp)
Thrombectomy with the preset stent-retriever Insights from the ARTESp* trial Wiebke Kurre, MD Klinikum Stuttgart - Germany * Acute Recanalization of Thrombo-Embolic Ischemic Stroke with preset (ARTESp)
Long-term impact & outcomes of neurological critical illness
 Long-term impact & outcomes of neurological critical illness M. Elizabeth Wilcox, MD MPH Assistant Professor of Critical Care Medicine, University of Toronto Staff Physician, University Health Network
Long-term impact & outcomes of neurological critical illness M. Elizabeth Wilcox, MD MPH Assistant Professor of Critical Care Medicine, University of Toronto Staff Physician, University Health Network
Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity
 Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity Hannah Jordan A. Study Purpose and Rationale Pulseless electrical activity during cardiac arrest carries a
Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity Hannah Jordan A. Study Purpose and Rationale Pulseless electrical activity during cardiac arrest carries a
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Clinical trial registration no.: NCT (clinicaltrials.gov) https://thejns.org/doi/abs/ / jns161301
 https://thejns.org/doi/abs/ / jns161301") CLINICAL ARTICLE J Neurosurg 128:120 125, 2018 Analysis of saccular aneurysms in the Barrow Ruptured Aneurysm Trial Robert F. Spetzler, MD, 1 Joseph M. Zabramski, MD, 1 Cameron G. McDougall, MD, 1 Felipe
CLINICAL ARTICLE J Neurosurg 128:120 125, 2018 Analysis of saccular aneurysms in the Barrow Ruptured Aneurysm Trial Robert F. Spetzler, MD, 1 Joseph M. Zabramski, MD, 1 Cameron G. McDougall, MD, 1 Felipe
Is there even a time window?
 Is there even a time window? A brief summary of key 2018 trials: DAWN and DEFUSE-3 For Neurosciences Update Conference, February 22, 2018 Maxim D. Hammer, M.D. Executive Summary Based on DAWN and DEFUSE-3,
Is there even a time window? A brief summary of key 2018 trials: DAWN and DEFUSE-3 For Neurosciences Update Conference, February 22, 2018 Maxim D. Hammer, M.D. Executive Summary Based on DAWN and DEFUSE-3,
Quantitative Analysis of Hemorrhage Volume for Predicting Delayed Cerebral Ischemia After Subarachnoid Hemorrhage
 Quantitative Analysis of Hemorrhage Volume for Predicting Delayed Cerebral Ischemia After Subarachnoid Hemorrhage Sang-Bae Ko, MD, PhD; H. Alex Choi, MD; Amanda Mary Carpenter, BA; Raimund Helbok, MD;
Quantitative Analysis of Hemorrhage Volume for Predicting Delayed Cerebral Ischemia After Subarachnoid Hemorrhage Sang-Bae Ko, MD, PhD; H. Alex Choi, MD; Amanda Mary Carpenter, BA; Raimund Helbok, MD;
THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS. 1. Cardiovascular Disease
 THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS 1. Cardiovascular Disease Cardiovascular disease is considered to have developed if there was a definite manifestation
THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS 1. Cardiovascular Disease Cardiovascular disease is considered to have developed if there was a definite manifestation
Coronary Angiography after Cardiac Arrest without ST-Segment Elevation: the COACT trial
 Coronary Angiography after Cardiac Arrest without ST-Segment Elevation: the On behalf of the COACT investigators Jorrit Lemkes, MD, Interventional cardiologist Amsterdam UMC, Vrije Universiteit Amsterdam,
Coronary Angiography after Cardiac Arrest without ST-Segment Elevation: the On behalf of the COACT investigators Jorrit Lemkes, MD, Interventional cardiologist Amsterdam UMC, Vrije Universiteit Amsterdam,
Small UIAs, <7 mm in diameter, uncommonly cause aneurysmal symptoms and are the most frequently detected incidentally.
 Research grant from Stryker Neurovascular Research grant from Covidien/ Medtronic Consultant and proctor for Stryker Neurovascular Consultant and proctor for Covidien/ Medtronic Consultant for Codman Neurovascular
Research grant from Stryker Neurovascular Research grant from Covidien/ Medtronic Consultant and proctor for Stryker Neurovascular Consultant and proctor for Covidien/ Medtronic Consultant for Codman Neurovascular
Stroke Net Grand Round Webinar
 Stroke Net Grand Round Webinar Preconditioning the Brain for Stroke Prevention April 4, 2019 Sebastian Koch University of Miami Department of Neurology None Unique challenges in brain conditioning Review
Stroke Net Grand Round Webinar Preconditioning the Brain for Stroke Prevention April 4, 2019 Sebastian Koch University of Miami Department of Neurology None Unique challenges in brain conditioning Review
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Supplementary Online Content
 Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
Patrick Altmann October 2012
 Cerebrolysin in Patients With Acute Ischemic Stroke in Asia The CASTA trial Wolf-Dieter Heiss, Michael Brainin, Natan M. Bornstein, Jaakko Tuomilehto, Zhen Hong Stroke. 2012 Mar;43(3):630-6. Epub 2012
Cerebrolysin in Patients With Acute Ischemic Stroke in Asia The CASTA trial Wolf-Dieter Heiss, Michael Brainin, Natan M. Bornstein, Jaakko Tuomilehto, Zhen Hong Stroke. 2012 Mar;43(3):630-6. Epub 2012
Introduction. Introduction. Introduction. Results. Method
 Standard cardiopulmonary resuscitation versus active compression-decompression cardiopulmonary resuscitation with augmentation of negative intrathoracic pressure for out-of-hospital cardiac arrest: a randomized
Standard cardiopulmonary resuscitation versus active compression-decompression cardiopulmonary resuscitation with augmentation of negative intrathoracic pressure for out-of-hospital cardiac arrest: a randomized
Challenges in the Design and Analysis of Non-Inferiority Trials: A Case Study. Key Points from FDA Guidance
 Challenges in the Design and Analysis of Non-Inferiority Trials: A Case Study Valerie Durkalski NETT Statistical and Data Management Center (NINDS U01 NS059041) Division of Biostatistics & Epidemiology
Challenges in the Design and Analysis of Non-Inferiority Trials: A Case Study Valerie Durkalski NETT Statistical and Data Management Center (NINDS U01 NS059041) Division of Biostatistics & Epidemiology
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Navigation-guided Burr Hole Aspiration Surgery for Acute Cerebellar Infarction
 FPⅣ-1 Navigation-guided Burr Hole Aspiration Surgery for Acute Cerebellar Infarction Eun-Sung Park, Dae-Won Kim, Sung-Don Kang Department of Neurosurgery, School of Medicine, Wonkwang University, Iksan,
FPⅣ-1 Navigation-guided Burr Hole Aspiration Surgery for Acute Cerebellar Infarction Eun-Sung Park, Dae-Won Kim, Sung-Don Kang Department of Neurosurgery, School of Medicine, Wonkwang University, Iksan,
Small and medium size intracranial aneurysms - a 5 years retrospective analysis trial and multimodal treatment
 Romanian Neurosurgery (2015) XXIX 4: 417-426 417 DOI: 10.1515/romneu-2015-0057 Small and medium size intracranial aneurysms - a 5 years retrospective analysis trial and multimodal treatment Valentin Munteanu
Romanian Neurosurgery (2015) XXIX 4: 417-426 417 DOI: 10.1515/romneu-2015-0057 Small and medium size intracranial aneurysms - a 5 years retrospective analysis trial and multimodal treatment Valentin Munteanu
Received: 15 September 2014 /Accepted: 20 November 2014 /Published online: 6 December 2014 # Springer-Verlag Berlin Heidelberg 2014
 Neuroradiology (2015) 57:269 274 DOI 10.1007/s00234-014-1472-6 DIAGNOSTIC NEURORADIOLOGY Quantification of structural cerebral abnormalities on MRI 18 months after aneurysmal subarachnoid hemorrhage in
Neuroradiology (2015) 57:269 274 DOI 10.1007/s00234-014-1472-6 DIAGNOSTIC NEURORADIOLOGY Quantification of structural cerebral abnormalities on MRI 18 months after aneurysmal subarachnoid hemorrhage in
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography
 Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Vote Using Your Phone!
 Update on Stroke Certification Jean Range, MS, RN The Joint Commission February 28, 2014 Vote Using Your Phone! Answer multiple choice questions by texting a code to 22333. Your phone carrier s texting
Update on Stroke Certification Jean Range, MS, RN The Joint Commission February 28, 2014 Vote Using Your Phone! Answer multiple choice questions by texting a code to 22333. Your phone carrier s texting
Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage
 Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage Sushant P. Kale, MD, MPH,* Randall C. Edgell, MD,* Amer Alshekhlee, MD,* Afshin Borhani Haghighi, MD,* Justin Sweeny, MD, Jason Felton, MD,
Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage Sushant P. Kale, MD, MPH,* Randall C. Edgell, MD,* Amer Alshekhlee, MD,* Afshin Borhani Haghighi, MD,* Justin Sweeny, MD, Jason Felton, MD,
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Monitoring of Regional Cerebral Blood Flow Using an Implanted Cerebral Thermal Perfusion Probe Archived Medical Policy
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided