Dr Ross Keenan. Neuroradiologist Christchurch Hospital
|
|
|
- Leon Walsh
- 6 years ago
- Views:
Transcription

1 Dr Ross Keenan Neuroradiologist Christchurch Hospital
2 Imaging Dr Ross Keenan Consultant Adult & Paediatric Neuroradiologist GP CPD Conference, August 2013 Workshop, Friday pm 16 August 2013 Edgar Centre Dunedin
3 Imaging 2013 Dr Ross Keenan, Neuroradiologist Disclosures: Christchurch Hospital (CDHB) Christchurch Radiology Group (CRG) NZ Brain Research Institute (NZBRI, VdV)
4 Definition: generic clinical definition: clinical event with sudden onset neurologic deficit > 24 hrs stroke is not an imaging diagnosis not all strokes are the same!!
5 Thrombolysis Evidence Base IST3 International Stroke Trial 3 (2013) Conclusion IST-3 provides evidence that thrombolysis with iv alteplase (rtpa) for acute ischemic stroke does not affect survival, but does lead to statistically significant, clinically relevant improvements in functional outcome and health related quality of life (QOL) that are sustained for at least 18 months Reference: IST-3 Lancet Neurol 2013; 12:
6 Guidelines 1 AHA/ASA Guidelines in Acute Ischemic Stroke Stroke 2013
7 Action Door to physician Door to stroke team Door to CT initiation Door to CT interpretation Door to drug ( 80% compliance) Door to stroke unit admission Time 10 minutes 15 minutes 25 minutes 45 minutes 60 minutes 3 hours time is brain AHA/ASA Guidelines in Acute Ischemic Stroke_Stroke 2013
8 National Institutes of Health Stroke Scale (NIHSS) Stroke IA Level of consciousness 0-Alert, 1-Drowsy, 2-Obtunded, 3-Coma/unresponsive 1B Orientation questions (2) 0-Answers both correctly, 1-Answers 1 correctly, 2-Answers neither correctly 1C Response to commands (2) 0-Performs both tasks correctly, 1-Performs 1 task correctly, 2-Performs neither 2 Gaze 0-Normal horizontal movements, 1-Partial gaze palsy, 2-Complete gaze palsy 3 Visual fields 4 Facial movement 5 Motor function (arm) a. Left b. Right 6 Motor function (leg) a. Left b. Right 0-No visual field defect, 1-Partial hemianopia, 2-Complete hemianopia, 3-Bilateral hemianopia 0-Normal, 1-Minor facial weakness, 2-Partial facial weakness, 3-Complete unilateral palsy 0-No drift, 1-Drift before 5 seconds, 2 -Falls before 10 seconds, 3-No effort against gravity, 4-No movement 0-No drift, 1-Drift before 5 seconds, 2-Falls before 5 seconds, 3-No effort against gravity, 4-No movement 7 Limb ataxia 0-No ataxia, 1-Ataxia in 1 limb, 2-Ataxia in 2 limbs 8 Sensory 0-No sensory loss, 1-Mild sensory loss, 2-Severe sensory loss 9 Language 0-Normal, 1-Mild aphasia, 2-Severe aphasia, 3-Mute or global aphasia 10 Articulation 0-Normal, 1-Mild dysarthria, 2-Severe dysarthria 11 Extinction or inattention 0-Absent, 1-Mild (loss 1 sensory modality lost), 2-Severe (loss 2 modalities lost) AHA/ASA Guidelines in Acute Ischemic Stroke_Stroke 2013
9 Immediate Evaluation in Suspected Acute Ischemic Stroke All patients Brain imaging - non contrast CT or MRI Blood glucose O 2 saturation Serum electrolytes/renal function tests* Full blood count, including platelet count* Markers of cardiac ischemia* AHA/ASA Guidelines in Acute Ischemic Stroke_Stroke 2013
10 Stroke mimicks
11 Imaging stroke mimicks is the stroke an acute ischemic infarct?


12 mimicks M61yr R hemiparesis, CT R > L bilateral spontaneous SDH


13 mimicks M61yr R hemiplegia, 2 week F/U isodense CT SDH, conservative Rx


14 mimicks M76yr dysphasia +/- behavioural, diagnostic CT 1



15 mimicks M76yr dysphasia +/- behavioural, F/U MRI day 44



16 mimicks M33yr acute R hemiplegia, MRI


17 mimicks M19yr acute stroke-like episode, MRI 1


18 mimicks M52yr L hemiplegia? acute episode, MRI 1


19 mimicks M52yr L hemiplegia? acute episode, MRI 1


20 mimicks M52yr L hemiplegia? acute episode, CT-PET chest lung Ca

21 mimicks F63yr Acute onset dysphasia, R hemiparesis, hemianopia

22 mimicks F63yr Acute onset dysphasia, R hemiparesis, hemianopia


23 mimicks F63yr Acute onset dysphasia, R hemiparesis, hemianopia
24 Clinical stroke mimicks Stroke clinical-only evaluation stroke mimicks up to 20% clinical + imaging evaluation (NECT) reduces to < 3% Causes seizure* complicated migraine* conversion disorders* tumour demyelination - acute plaques infection - meningoencephalitis
25 Clinical features of Stroke mimicks Stroke Psychogenic Seizures Hypoglycemia Migraine with aura (complicated migraine) Hypertensive encephalopathy Wernicke s encephalopathy CNS abscess CNS tumor Drug toxicity Lack of objective cranial nerve findings, neurological findings in a nonvascular distribution, inconsistent examination History of seizures, witnessed seizure activity, postictal period History of diabetes, low serum glucose, decreased level of consciousness History of similar events, preceding aura, headache Headache, delirium, significant hypertension, cortical blindness, cerebral edema, seizure History of alcohol abuse, ataxia, ophthalmoplegia, confusion History of drug abuse, endocarditis, medical device implant with fever Gradual progression of symptoms, other primary malignancy, seizure at onset Lithium, phenytoin, carbamazepine AHA/ASA Guidelines in Acute Ischemic Stroke_Stroke 2013
26 True stroke
27 Stroke: Ischemic Stroke (ASCO phenotypic system ) Atherosclerotic thromboembolic infarcts (40-45% all strokes) commonest, atherosclerotic plaque, carotid bifurcation > siphon thromboemboli to large arteries esp MCA Small-vessel occlusion (lacunar) (15-30% all strokes) penetrating vessels, subcortical <15mm, thromboembolic, atherosclerotic Cardioembolism (15-25% all strokes) IHD-MI, valvular disease, arrhythmia, AF Other - indeterminant Hemorrhagic Stroke Reference: ASCO phenotypic system
28 Ischemic Stroke TOAST Classification Large-artery atherosclerosis - thromboembolic Cardioembolism Small-vessel occlusion (lacune) Stroke - indeterminate aetiology a. >/= 2 causes identified b. negative evaluation no cause identified c. incomplete evaluation Reference: Trial of Org in Acute Stroke Treatment (TOAST)
29 TOAST Classification Ischemic Strokes Features Large artery atherosclerosis Cardioembolism Lacunar infarct Other Clinical Imaging Other cortical,cerebellar syn. lacunar syn. corticocerebellar, brainstem, subcortical infarct >15mm subcortical or brainstem infarct <15mm / / / /- +/- ICA stenosis cardiac - other
30 Ischemic Stroke: Imaging Infarct Aging Hyperacute infarct < 12hrs = acute stroke thrombolysis group Acute infarct > 12hrs - 7days Subacute infarct 7-30 days Chronic infarct > 30 days
31 Imaging Goals in Clinical Acute Stroke: Exclude stroke mimicks (3-20%) imaging unable to exclude seizure/conversion disorders Exclude acute hemorrhagic lesions absolute contraindication to acute thrombolysis SDH, SAH, ICH, IVH Confirm clinical acute ischaemic stroke CT >> MRI acute infarct signs significant CT normal imaging rate < 4.5hrs Characterisation acute ischaemic stroke penumbra/core determine potential thrombolysis treatment target penumbra zone penumbra = ischemic but viable at risk tissue Cardiovascular imaging cardiovascular assessment for stroke causation


32 Imaging Goals Acute Stroke: x 4 P s P parenchyma confirm acute ischemic stroke, exclude mimics/hemorrhage P perfusion CT perfusion, MTT x CBF = CBV classification CBV compensated, oligaemic CBV ischemic penumbra, infarct core P penumbra determine potential Rx target = ischaemic but viable tissue P pipes assess craniocervical vessels and intracardiac structures

33 Acute Stroke Imaging Acute Neuroimaging CT C - >> MR Mass. General Protocol CT C -, CTA, CTP Craniocervical Vascular imaging Doppler CTA MRA DSA Cardiac imaging Echo, CMRI R J Keenan CRG 2009

34 Strategy: Neuroimaging CT +/- CT perfusion MR +/- MR perfusion (Gadolinium DSC or ASL) Neurovascular Imaging Intracranial CTA or MRA +/- DSA Extracranial Doppler US, CTA or MRA +/- DSA Cardiac Imaging Echocardiography TTE or TOE Cardiac MRI Medical Workup Blood screen, Coagulation screen, ECG, Telemetry-Holter
35 Haemorrhagic stroke
 Fusiform aneurysm (mycotic, post traumatic, dissection, atheroma) Vascular malformations AVM pial or dural type (DAVF) cavernous hemangioma")
36 Hemorrhagic Stroke, ICH: Traumatic Hypertensive Infarction Angiopathy Aneurysm Arteriosclerotic Primary ICH Arterial ischemic infarct (hemorrhagic transformation) Venous infarction (DVST hemorrhage) CAA Primary ICH Berry aneurysm (saccular, congenital) Fusiform aneurysm (mycotic, post traumatic, dissection, atheroma) Vascular malformations AVM pial or dural type (DAVF) cavernous hemangioma (cavernoma) venous angioma
37 Imaging Intracranial hemorrhage (ICH) hypertensive (primary ICH) cerebral amyloid/congophilic angiopathy (CAA) aneurysmal SAH moya moya vasculopathy


38 F63yr Acute right hemispheric stroke syndrome - CT 3 hours


39 F63yr Lobar hemispheric subacute ICH CT 10days


40 F63yr Lobar hemispheric chronic ICH MRI 1year


41 F65yr Acute L hemispheric stroke syndrome


42 F65yr Acute L hemispheric stroke syndrome

43 F65yr Acute L hemispheric stroke syndrome



44 F65yr Acute L hemispheric stroke syndrome


45 F61yr sudden onset headache, confusion, visual


46 F61yr sudden onset headache, confusion, visual


47 F61yr day 4 post acute SAH deterioration CT rebleed


48 F61yr CTA/DSA basilar tip aneurysm favorable for endovascular coiling


49 F51yr recurrent headache without neurologic deficit


50 F51yr recurrent headache without neurologic deficit


51 M42yr collapse GCS 6, dilated non-responsive pupils


52 M42yr collapse GCS 6, dilated non-responsive pupils
53 Acute Ischemic Stroke
54 Imaging Large Artery Thromboembolic Infarction
55


56


57


58

59


60 CBF map


61 MTT map Stroke CBV map MTT 12sec CBV 40%

62 ASPECTS System: Stroke Aspect Score based on 10 MCA regions, 1 point assigned/region. Cumulative score = Total 10 subtracting 1 point/region involved on C - CT


63


64 3 hr CT pre thrombolysis 24hr CT post thrombolysis malignant infarct


65 24hr CT post thrombolysis malignant infarct
66 Imaging Cardioembolic infarction


67 Hx cardiac surgery, ataxic, R hemiparesis


68 Hx cardiac surgery, ataxic, R hemiparesis

69 R ICA stenosis < 30% L ICA stenosis 60-69%
")
) Hx")



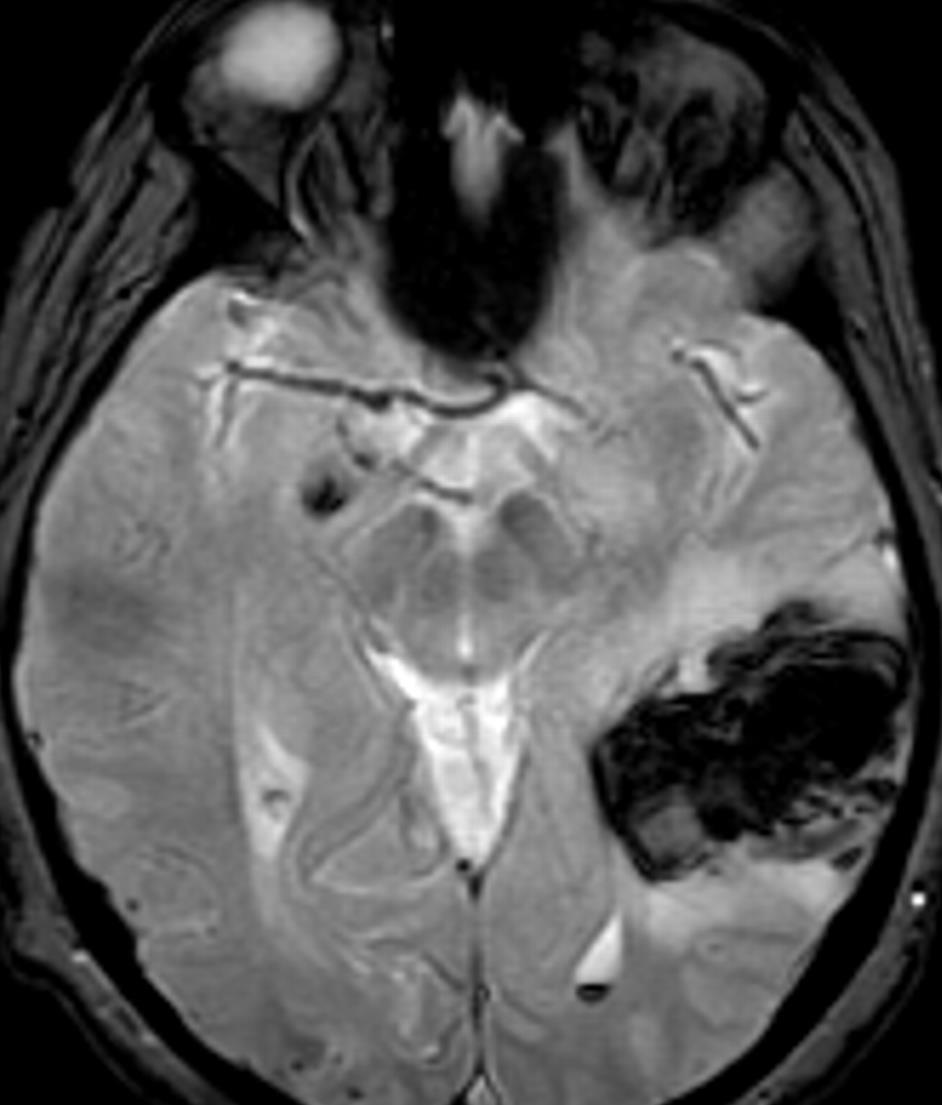
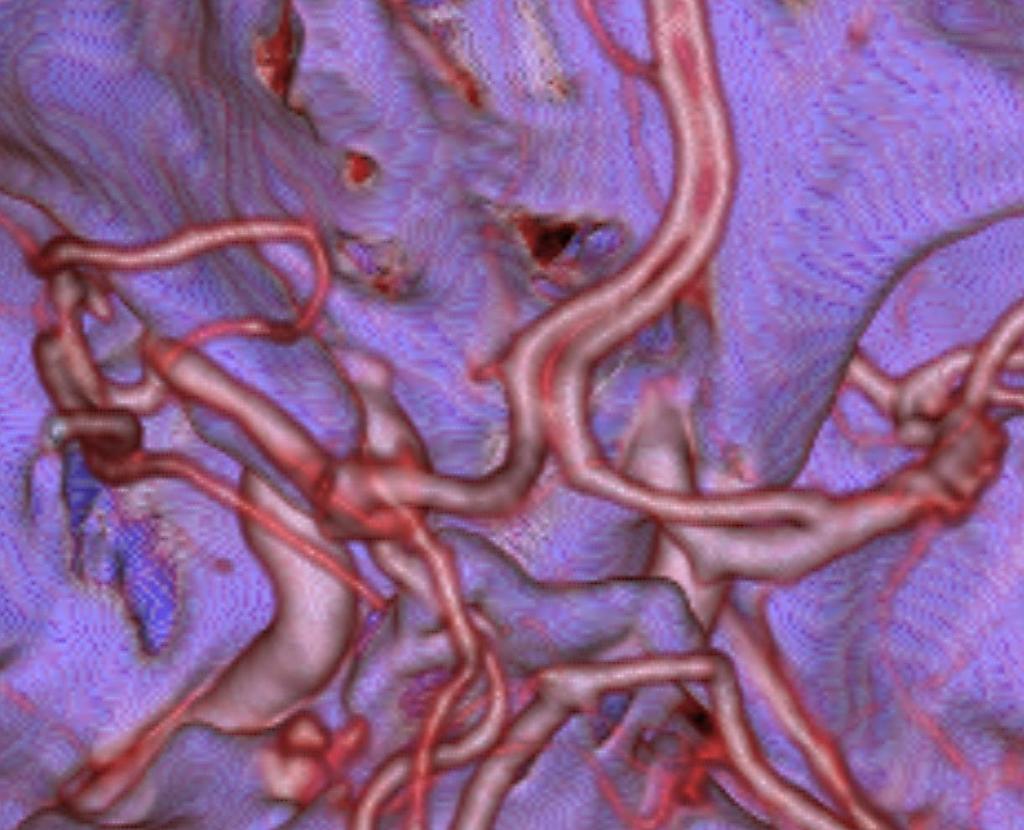
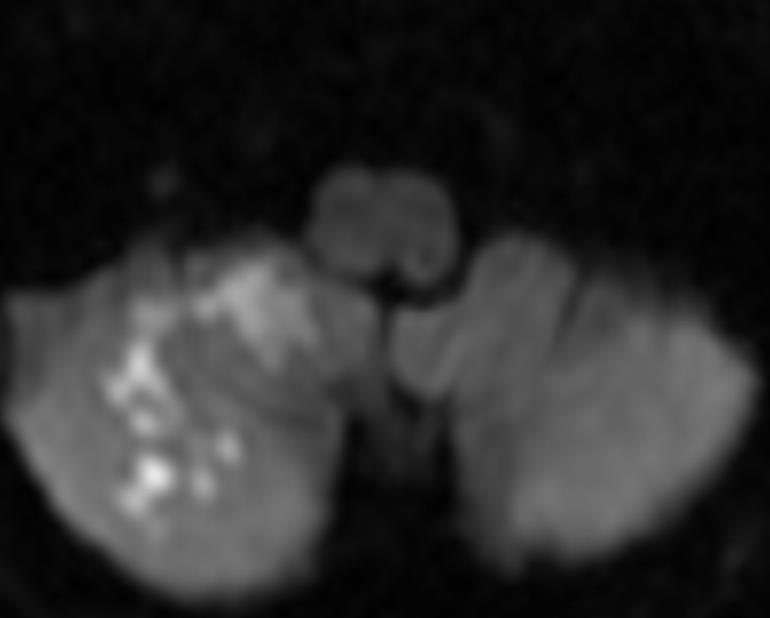
70 Figure 1 (Fiesta) Figure 2 (MDE)) Hx cardiac surgery. MR embolic infarcts. Echo apical hypokinesis Dr R J Keenan CRG 2012
")
 Hx")



71 Figure 3 (Fiesta) Figure 4 (MDE) Hx cardiac surgery. MR embolic infarcts. Echo apical hypokinesis Dr R J Keenan CRG 2012


72 F35 left neck pain and ataxia


73 F35 left neck pain and ataxia


74 F35 left neck pain and ataxia


75 F35 left neck pain and ataxia
76 Imaging Lacunar infarction


77 Imaging F77yr acute L mild facial weakness


78 Imaging F77yr acute L mild facial weakness


79 Imaging F77yr acute L mild facial weakness


80 F61yr acute rotatory nystagmus, nausea-vomiting


81 F61yr acute rotatory nystagmus, nausea-vomiting, L facial sensory


82 M66yr acute onset R leg weakness, CT normal


83 M66yr acute onset R leg weakness, CT normal
84 Imaging Craniocervical Vascular Imaging extracranial carotid stenosis carotid complicated plaque valvular lesions LV thrombus


85 TIA


86 TIA



87 TIA


88 TIA F83yr Carotid Doppler - RICA severe stenosis 80-95%


89 TIA F83yr Extracranial CTA - RICA severe stenosis


90 TIA F83yr Carotid Doppler - LICA severe stenosis 80-95%


91 TIA F83yr Extracranial CTA - LICA severe stenosis

92 Line graph shows carotid artery percent diameter reduction in asymptomatic carotid stenosis vs annual ipsilateral stroke risk. *Comparison of 50%-75% vs 76%-99% stenosis. Copyright American Heart Association


93 Copyright American Heart Association F83yr Extracranial CTA - RICA severe stenosis


94 Copyright American Heart Association M56 Acute left hemiplegia and dysphasia


95 Copyright American Heart Association M56 Acute left hemiplegia and dysphasia


96 M56 Acute left hemiplegia and dysphasia, ICA free floating thrombus Copyright American Heart Association


97 M56 Acute left hemiplegia and dysphasia, ICA free floating thrombus Copyright American Heart Association


98 Copyright American Heart Association M56 Acute left hemiplegia and dysphasia, AoV mass


99 Copyright American Heart Association M56 chronic MCA occlusive infarct, ICA thrombus, AoV mass


100 M74 Doppler LICA occlusion


101 M74 Doppler RICA occlusion


102 M54yr neck discomfit, R sided weakness


103 MRA MRA



104 RICA LICA COW


105 CTA LICA MR T2
106 Guidelines 2 AHA/ASA Guidelines in Acute Ischemic Stroke Stroke 2013
107 Recommendations for Acute Non resolved Cerebral Ischemic Syndromes (infarction) 1. Emergency brain imaging is recommended before initiating any specific therapy to treat acute ischemic stroke (Class I; Level of Evidence A). NECT is sufficient for emergency management. 2. Either NECT-MRI is recommended before iv rtpa administration to exclude ICH (absolute contraindication) and to determine whether CT hypodensity or MRI hyperintensity of ischemia is present - (Class I; Level of Evidence A). 3. Intravenous fibrinolytic therapy is recommended in the setting of early ischemic changes (other than frank hypodensity) on CT, regardless of their extent - (Class I; Level of Evidence A). 4. A noninvasive intracranial vascular study is strongly recommended during the initial imaging evaluation of the acute stroke patient if either intra-arterial fibrinolysis or mechanical thrombectomy is contemplated for management but should not delay intravenous rtpa if indicated (Class I; Level of Evidence A). 5. In intravenous fibrinolysis candidates, brain imaging study should be interpreted within 45 minutes of patient arrival in ED by a physician with expertise in reading CT and MRI studies of the brain parenchyma (Class I; Level of Evidence C). 6. CT-MRI perfusion and DWI imaging, including measures of infarct core-penumbra, may be considered for the selection of patients for acute reperfusion therapy beyond the time windows (CHC Hospital> 4.5hrs) for intravenous fibrinolysis. These techniques provide additional information that may improve diagnosis, mechanism, and severity of ischemic stroke and allow more informed clinical decision making (Class IIb; Level of Evidence B) 7. Frank hypodensity on NECT may increase the risk of hemorrhage with fibrinolysis and should be considered in treatment decisions. If frank hypodensity involves more than 1/3 MCA territory, iv rtpa treatment should be withheld (Class III; Level of Evidence A). AHA/ASA Guidelines in Acute Ischemic Stroke_Stroke 2013
108 TIA Summary Recommendations for Resolved Cerebral Ischemic Syndromes (TIA) 1. (TIA): a transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction. 2. Patients with TIAs are at high risk of early stroke, and their risk may be stratified by clinical scale, vessel imaging, and diffusion magnetic resonance imaging. 3. Diagnostic recommendations for TIA patients: - undergo neuroimaging < 24 hours post symptom onset, preferably MRI - imaging extracranial cervical vessels should be performed (Doppler CT-MRA) - noninvasive imaging of intracranial vessels is reasonable (CTA/MRA) 4. ECG should occur as soon as possible after TIA - prolonged cardiac monitoring (Holter) and echocardiography are reasonable in patients in whom a vascular etiology is not identified 5. Routine blood tests are reasonable 6. Reasonable to hospitalize patients with TIA if presenting within 72 hours and have an ABCD 2 score 3, indicating high risk of early recurrence, or the evaluation cannot be rapidly completed on an outpatient basis. AHA/ASA Statement: Definition & Evaluation of TIA_Stroke 2009
109 Thrombolysis Evidence Base - pre IST3 study 2013 Acute ischemic stroke thrombolysis selection Ideal candidates Less favorable early < 90min > 180min age < 60 age > 80 lower BP very high BP normal glucose high glucose minimal EIC on CT extensive CT scan (high ASPECTS) (low ASPECTS) no leukariosis severe leukoariosis moderate - severe deficits very mild deficits small - moderate clot burden heavy clot burden no NINDS protocol violations NINDS violation
110 Thrombolysis Evidence Base IST3 International Stroke Trial 3 (2013) Thrombolysis in acute ischaemic stroke Baseline characteristics n = 3035 multicenter randomised controlled trial, acute ischemic stroke Rx rtpa (alteplase) thrombolysis < 6hrs post onset 2003 License 0-3hrs, <80yr, NIHSS % 2008 ECASS hr, <80yr, NIHSS % > 80yrs 53% > 4.5hrs 33% Reference: IST-3 Lancet Neurol 2013; 12:
111 Thrombolysis Evidence Base IST3 (2013) Acute Ischemic Stroke - Thrombolysis selection Rx < 3rs from onset age no barrier robust evidence of benefit benefit across broad range of strokes Rx 3-4.5hrs from onset no benefit for uncertain pts use strict ECASS3 criteria yrs - no significant improvement - exclusions: Phx stroke + DM previous stroke/trauma Reference: IST-3 Lancet Neurol 2013; 12:
112 Thrombolysis Evidence Base IST3 International Stroke Trial 3 (2013) Conclusion IST-3 provides evidence that thrombolysis with iv alteplase (rtpa) for acute ischemic stroke does not affect survival, but does lead to statistically significant, clinically relevant improvements in functional outcome and health related quality of life (QOL) that are sustained for at least 18 months Reference: IST-3 Lancet Neurol 2013; 12:
113 Questions
114 END

115 Reference: IST-3 Lancet Neurol 2013; 12: Stroke Thrombolysis Evidence Base IST3 (2013) Acute Ischemic Stroke results 0-6hrs rtpa control Outcome: Alive and independent Symptomatic ICH Mortality 7 days Mortality 6 months 37% 35% 7% 1% 11% 7% 27% 27%
 TIA Symptom")


116 TIA MRI DWI lesion Frequency in Patients with TIAs_(pooled data n = 818) TIA Symptom Duration (hrs) MRI DWI Restriction (%) % % % % % % % AHA/ASA Statement: Definition & Evaluation of TIA_Stroke 2009
117 TIA Summary Recommendations for Resolved Cerebral Ischemic Syndromes (TIA) 1. TIAs are sudden brief episodes of focal neurological dysfunction resulting from focal cerebral ischemia not associated with permanent cerebral infarction. 2. TIAs are traditionally defined as sudden onset, focal neurologic deficits of presumed vascular origin lasting < 24 hours. 3. Recent studies from many groups worldwide have demonstrated that this arbitrary time threshold was too broad. 30% - 50% of classically defined TIAs show brain injury on diffusion-weighted MRI. 4. Several groups have proffered neuroimaging-based, operational definitions of TIA such as a brief episode of neurological dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting < 1 hour, without evidence of acute infarction 5. These newer definitions have not yet been formally considered or adopted by authoritative organizations. 6. Stroke and TIA are a spectrum of brain ischemia. Each are markers of reduced cerebral blood flow and an increased risk of disability and death. TIAs offer an opportunity to initiate treatment that can forestall the onset of permanently disabling injury. AHA/ASA Statement: Definition & Evaluation of TIA_Stroke 2009
118 TIA TIA Class 1 Recommendations: 1. TIA should undergo neuroimaging evaluation < 24 hours of symptom onset. MRI, including DWI, is the preferred brain diagnostic imaging modality. If MRI is not available, head CT should be performed (Class I, Level of Evidence B). 2. Noninvasive imaging of the extracranial-intracranial vessels should be performed routinely (Class I, Level of Evidence A). 3. Noninvasive testing of the intracranial vasculature reliably excludes the presence of intracranial stenosis and is reasonable to obtain when knowledge of intracranial steno-occlusive disease will alter management. Reliable diagnosis of intracranial stenosis requires DSA to confirm abnormalities detected with noninvasive testing. (Class I, Level of Evidence A) 4. Suspected TIA should be evaluated as soon as possible after an event (Class I, Level of Evidence B). AHA/ASA Statement: Definition & Evaluation of TIA_Stroke 2009
. 2.")
119 TIA TIA Class 2 Recommendations: 1. Assessment of the extracranial vasculature may involve any of the following: Carotid Doppler/TCD, MRA, or CTA, depending on local availability and expertise (Class IIa, Level of Evidence B). 2. If only noninvasive testing is performed before endarterectomy, it is reasonable to pursue 2 concordant noninvasive findings; otherwise, DSA should be considered (Class IIa, Level of Evidence B). 3. Role of plaque characteristics and detection of MESs is not yet defined (Class IIb, Level of Evidence B). 4. ECG should be performed as soon as possible after TIA (Class I, Level of Evidence B). Cardiac monitoring (telemetry or Holter) is useful in patients with an unclear origin after initial brain imaging and ECG (Class IIa, Level of Evidence B). 5. Echocardiography (at least TTE) is reasonable in the evaluation of patients with suspected TIAs, especially in patients in whom no cause has been identified by other elements of the workup (Class IIa, Level of Evidence B). TEE is useful in identifying PFO, aortic arch atherosclerosis, and valvular disease and is reasonable when identification of these conditions will alter management (Class IIa, Level of Evidence B). 6. Routine blood tests (FBC, U&Es, LFTs, PTT and partial thromboplastin time, and fasting lipid profile are reasonable (Class IIa, Level of Evidence B). 7. Hospitalisation reasonable in TIA if presenting < 72 hours any of the following criteria are present: a. ABCD score of 3 (Class IIa, Level of Evidence C). b. ABCD score of 0-2 and uncertainty that outpatient workup can be completed < 2 days (Class IIa, Level of Evidence C). c. ABCD score of 0-2 and other evidence that indicates the patient s event was caused by focal ischemia (Class IIa, Level of Evidence C). AHA/ASA Statement: Definition & Evaluation of TIA_Stroke 2009
120 Imaging Ischaemia : cerebrovascular reserve impairment stress brain perfusion imaging (acetazolamide) hypoperfusion rest brain hypoperfusion, CBF lesion infarction necrosis
 Carotid Doppler US CT Angiography Carotid COW (CTA)")
121 Imaging Techniques: Stroke CT Head C - (NECT) Neuroperfusion Imaging (CTP) MRI Head (MRI) MRA extracranial carotid - intracranial COW (MRA) Carotid Doppler US CT Angiography Carotid COW (CTA) Echocardiography
122 END
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Emergently? Michigan Institute for Neurological Disorders. Garden City Hospital, Garden City, Michigan
 Why Should TIA be Treated Emergently? Anne M. Pawlak, D.O. F.A.C.N. Michigan Institute for Neurological Disorders Director Neurology Residency Program, Garden City Hospital, Garden City, Michigan According
Why Should TIA be Treated Emergently? Anne M. Pawlak, D.O. F.A.C.N. Michigan Institute for Neurological Disorders Director Neurology Residency Program, Garden City Hospital, Garden City, Michigan According
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Background. Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
 for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Advanced Neuroimaging for Acute Stroke
 Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
The Language of Stroke
 The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
Disclosure. + Outline. What is a stroke? Role of imaging in stroke Ischemic stroke Venous infarct Current topics
 + Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
+ Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
with susceptibility-weighted imaging and computed tomography perfusion abnormalities in diagnosis of classic migraine
 Emerg Radiol (2012) 19:565 569 DOI 10.1007/s10140-012-1051-2 CASE REPORT Susceptibility-weighted imaging and computed tomography perfusion abnormalities in diagnosis of classic migraine Christopher Miller
Emerg Radiol (2012) 19:565 569 DOI 10.1007/s10140-012-1051-2 CASE REPORT Susceptibility-weighted imaging and computed tomography perfusion abnormalities in diagnosis of classic migraine Christopher Miller
CT INTERPRETATION COURSE
 CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)).
).") 12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging
 The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Place for Interventional Radiology in Acute Stroke
 Place for Interventional Radiology in Acute Stroke Dr Lakmalie Paranahewa MBBS, MD(Radiology), FRCR Consultant Interventional Radiologist Asiri Group of Hospitals Objectives Imaging in Stroke Neurovascular
Place for Interventional Radiology in Acute Stroke Dr Lakmalie Paranahewa MBBS, MD(Radiology), FRCR Consultant Interventional Radiologist Asiri Group of Hospitals Objectives Imaging in Stroke Neurovascular
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
ACUTE CENTRAL PERIFERALEMBOLISM
 EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Acute Ischemic Stroke Mechanism, Diagnosis, Treatment
 Acute Ischemic Stroke Mechanism, Diagnosis, Treatment IM Resident Lecture December 2016 Mohammad Shafie, MD PhD MEng Department of Neurology UC Irvine Objectives Better understanding of stroke mechanisms
Acute Ischemic Stroke Mechanism, Diagnosis, Treatment IM Resident Lecture December 2016 Mohammad Shafie, MD PhD MEng Department of Neurology UC Irvine Objectives Better understanding of stroke mechanisms
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Permanent foramen ovale: when to close?
 Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL The following is a list of variables and how to complete each one:
 MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
UPDATE ON STROKE IN OLDER PEOPLE: CLINICAL CASES IN EVERYDAY PRACTICE
 UPDATE ON STROKE IN OLDER PEOPLE: CLINICAL CASES IN EVERYDAY PRACTICE Joseph SK Kwan Clinical Associate Professor, HKU Honorary Consultant, Queen Mary Hospital & Grantham Hospital CASE: 82 YEAR OLD LADY
UPDATE ON STROKE IN OLDER PEOPLE: CLINICAL CASES IN EVERYDAY PRACTICE Joseph SK Kwan Clinical Associate Professor, HKU Honorary Consultant, Queen Mary Hospital & Grantham Hospital CASE: 82 YEAR OLD LADY
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew