This page intentionally left blank
|
|
|
- Kenneth Manning
- 5 years ago
- Views:
Transcription

1
2 This page intentionally left blank
3 Interpretation of Emergency Head CT A Practical Handbook
4
 Edin, FCEM Consultant in Paediatric and Adult Emergency Medicine Wexham Park Hospital, Slough Rakesh R.")
5 Interpretation of Emergency Head CT A Practical Handbook Erskine J. Holmes, MRCS Consultant in Emergency Medicine Wexham Park Hospital, Slough Anna C. Forest-Hay, MA, FRCS (A&E) Edin, FCEM Consultant in Paediatric and Adult Emergency Medicine Wexham Park Hospital, Slough Rakesh R. Misra, BSc (Hons), FRCS (Eng), FRCR Consultant Radiologist, Wycombe Hospital Buckinghamshire Hospitals NHS Trust Editor R. R. Misra
6 CAMBRIDGE UNIVERSITY PRESS Cambridge, New York, Melbourne, Madrid, Cape Town, Singapore, São Paulo Cambridge University Press The Edinburgh Building, Cambridge CB2 8RU, UK Published in the United States of America by Cambridge University Press, New York Information on this title: E. J. Holmes, A. C. Forrest-Hay, R. R. Misra 2008 This publication is in copyright. Subject to statutory exception and to the provision of relevant collective licensing agreements, no reproduction of any part may take place without the written permission of Cambridge University Press. First published in print format 2008 ISBN ISBN ebook (EBL) paperback Cambridge University Press has no responsibility for the persistence or accuracy of urls for external or third-party internet websites referred to in this publication, and does not guarantee that any content on such websites is, or will remain, accurate or appropriate. Every effort has been made in preparing this publication to provide accurate and up-todate information which is in accord with accepted standards and practice at the time of publication. Although case histories are drawn from actual cases, every effort has been made to disguise the identities of the individuals involved. Nevertheless, the authors, editors and publishers can make no warranties that the information contained herein is totally free from error, not least because clinical standards are constantly changing through research and regulation. The authors, editors and publishers therefore disclaim all liability for direct or consequential damages resulting from the use of material contained in this publication. Readers are strongly advised to pay careful attention to information provided by the manufacturer of any drugs or equipment that they plan to use.
7 Dedicated to my wife Jill for her support, help and love over the years. E. J. H. I would like to dedicate this book to my father, Iain, for being my inspiration and mentor. A. F-H. Dedicated to my beautiful wife, Rachel, and children, Rohan, Ela and Krishan, for allowing me the time to write this book. R. R. M.
8
9 CONTENTS Acknowledgements Preface Abbreviations Introduction page ix xi xii xiii Section 1 1 Fundamentals of CT imaging 3 History 3 Technical details 4 Windowing and grey scale 6 Tissue characteristics 6 Image artefacts 8 Important anatomical considerations 10 Review of normal anatomy 10 Review of vascular territories 22 Review of vascular anatomy 33 Section 2 35 Reviewing a CT scan 36 Acute stroke 38 Ischaemic stroke 38 Haemorrhagic stroke 45 Subdural haematoma (SDH) 50 Extradural haematoma 54 Subarachnoid haemorrhage 58 Cerebral venous sinus thrombosis 62 Contusions 64 Skull fractures 68 Meningitis 71 Raised intracranial pressure 74 vii
10 Contents Hydrocephalus 77 Abscesses 80 Arteriovenous malformation 83 Solitary lesions 86 Multiple lesions 89 Self-assessment section 92 Self Assessment Answers 95 Appendices 101 Differential diagnosis of intracerebral lesions 103 CT guidelines for head trauma 105 Proposed algorithm for the emergency management of acute stroke 106 Information required prior to neurosurgical referral 108 viii
11 ACKNOWLEDGEMENTS The authors would sincerely like to thank Dr Jagrit Shah, Consultant Radiologist, Queen s Medical Centre, Nottingham, for generously donating several key images. We would also like to thank Dr Matthew Burn, Consultant Stroke Physician, Wycombe Hospital, Buckinghamshire Hospitals NHS Trust. Matthew read and edited the final manuscript, and provided invaluable advice from a Stroke Physician s perspective. His contribution is greatly appreciated. Sincere thanks to Luc Bouwman CT Product Manager, Toshiba Medical Systems, Europe, for meticulously drawing all the superb images in Section 1. ix
12
13 PREFACE Welcome to the first handbook of CT brain interpretation. Focus has been placed on including a greater number of images than would normally be found in a book of this size. The resolution has been heightened and the accompanying text limited to precise details, in order to achieve our goal: that is to equip a wide variety of medical professionals with a general understanding of head CT. A schema is provided by which to analyse the images, in order to develop greater confidence to diagnose the most common and critical problems. It is hoped that this book will be invaluable to individuals who find themselves, more and more, in the acute decision-making setting. This includes Emergency Physicians, Surgeons, Neurosurgeons, Trauma or Orthopaedic Surgeons, Radiographers and Elderly Care physicians. It is also intended to be instructive to radiology trainees and medical students alike. All choice topics are included, thus lending itself as an excellent revision aid for anyone preparing for a postgraduate exam. Small enough to carry around, we hope we have provided a reliable reference for what you need to remember, regardless of the time of day or night. xi
14 ABBREVIATIONS ACom APTT AVM BP CCF CSF CT CTV CVA ECA ECG EDH ETA ETT GCS HR HU i.m. INR i.v. ICA LP M:F MCA NICE PCom RIND RR SAH SDH SLE SSS TIA WCC Anterior communicating Activated partial thromboplastin time Arteriovenous malformation Blood pressure Congestive cardiac failure Cerebrospinal fluid Computer tomography CT venogram Cerebrovascular accident External carotid artery Electrocardiogram Extradural haemorrhage Estimated time of arrival Endotracheal tube Glasgow Coma Scale Heart rate Hounsfield Unit intramuscular International normalised ratio Intravenous Internal carotid artery Lumbar puncture Male:female Middle cerebral artery National Institute of Clinical Excellence Posterior communicating Reversible ischaemic neurological deficit Respiratory rate Subarachnoid haemorrhage Subdural haematoma Systemic lupus erythematosus Superior sagittal sinus Transient ischaemic attack White cell count xii
15 INTRODUCTION Computer tomography (CT) is now widely available and is being used more and more, unlike magnetic resonance imaging, 24 hours a day, 7 days a week. CT is often the initial imaging modality of choice; not only for diagnosis but also to guide treatment. The most common request for CT out of hours is brain imaging. CT is a vital tool in the assessment of patients with serious head injury. It remains the investigation of choice for the assessment of acute haemorrhage and bony injury. Consequently, patient management has been transformed since its inception, as rapid imaging and diagnosis of intracranial pathology can facilitate emergency intervention. Equally, a delay in diagnosis, and treatment, may adversely affect outcome and prognosis. Patient s expectations of modern medical technology are high. There are ever-increasing time pressures to form rapid diagnoses, and improve efficiency, in the face of a more litigious society. The European Working Time Directive is likely to make doctors feel more vulnerable, with shift patterns reducing personal experience and training opportunities. Furthermore, the multidisciplinary team on duty in the Hospital at Night Scheme may not possess the appropriate expertise between them to interpret emergency imaging. Yet, the NICE guidelines are in place to further increase the number of CT scans performed out of hours. To add to this, the nationwide shortage of radiologists results in a limited CT service available out of hours. Hence we have the dilemma of how to provide an adequate emergency imaging service coupled with who will interpret the images. The College of Emergency Medicine has stipulated that Specialist Registrars in Emergency Medicine are expected to be able to diagnose brain pathology from CT scans of the head. Currently, in many hospitals around the country it is routine for CT head scans, performed out of hours, to be interpreted by the requesting doctor. This is likely to be a progressive future trend, with a variety of speciality groups needing to acquire these skills. Analogous to this is ECG interpretation; originally the domain of the Cardiologist, this is now a routine general investigation interpreted by most clinicians. It is not inconceivable that medical students, and junior medical staff alike, may need to acquire the basic skills to analyse CT abnormalities in the future, if we are to keep pace with the everincreasing demand. The purpose of this book is to provide a systematic approach by which to interpret and provisionally report head CT scans, based on learning to recognise common pathologies from an archive of representative images. xiii
16
17 SECTION 1
18
19 Fundamentals of CT imaging I History In the early 1970s Sir Godfrey Hounsfield s research produced the first clinically useful CT scans. Original scanners took approximately 6 minutes to perform a rotation (one slice) and 20 minutes to reconstruct. Despite many technological advances since then, the principles remain the same. On early scanners the tube rotated around a stationary patient with the table then moved to enable a further acquisition. The machine rotated clockwise and counter-clockwise as power was supplied via acable. Modern-day helical or spiral scanners obtain power via slip ring technology, thus allowing continuous tube rotation as the patient moves through the scanner automatically. This allows a volume of data to be acquired in a single rotation, with the benefits of faster scanning, faster patient throughput and less re-imaging as patient movement artefact is reduced. New multi-slice scanners use existing helical scanning technology but have multiple rows of detectors to acquire multiple slices per tube rotation. In turn, advanced computer processing power allows reconstructive techniques, such as three-dimensional and multiplanar reformats, to be more easily accessible. Consequently, scans are now performed routinely at a reporting workstation where the image can be viewed dynamically. Fundamentals of CT imaging Patient/table movement Single slice helical CT. The X-ray tube continuously rotates as the patient moves through at a constant rate. Single slice system. 3


20 IInterpretation of Emergency Head CT 4 Multidetector helical CT: four detectors shown here. Technical details Patient/table movement The X-ray tube produces a narrow fan-shaped beam of collimated X-rays, which pass through the patient to reach a bank of detectors opposite the source. X-rays are attenuated differentially by the patient, depending on the tissues through which they pass. Low density tissues such as fat/aerated lung absorb fewer X-rays, allowing more to reach the detector. The opposite is true of dense tissues such as bone. The amount of transmitted radiation received provides information on the density of the tissue. A CT slice is divided up into a matrix of squares, e.g , and The slice thickness determines the volume of these squares; these are called voxels. Using mathematical calculations, the degree to which a tissue absorbs radiation within each voxel, the linear attenuation coefficient, m, is calculated and assigned a value related to the average attenuation of the tissues within it the CT number or Hounsfield Unit. Each value of m is assigned a grey scale value on the display monitor and is presented as a square picture element (pixel) on the image. Spiral scanners acquire a volume of information from which an axial slice is reconstructed, as above, using computer technology. Slices are created from data during the reconstruction phase. Pitch is defined as the distance moved by the table in millimetres, during one complete rotation of the X-ray tube, divided by the slice thickness in millimetres. In general, increasing pitch (increase table speed with a fixed slice thickness) reduces radiation dose; as a result image resolution can be affected and thus a compromise usually exists. Distance moved by the table during one complete rotation Pitch ¼ Slice thickness

21 Ring of fixed detectors Fan angle Rotating X-ray tube and a fan beam of X-rays I Fundamentals of CT imaging Patient Helical system. Ring of detectors surrounding a patient. Patient/table movement Patient/table movement The pitch is low with the table moving less for each tube revolution, resulting in a sharper image. The pitch is high, effectively stretching out the helix. The table moves more for each revolution, resulting in some loss of image quality. 5
22 IInterpretation of Emergency Head CT Windowing and grey scale Modern CT scanners are able to differentiate in excess of 2000 CT numbers; however, the human eye can differentiate only around 30 shades of grey. To maximise the perception of medically important features, images can be digitally processed to meet a variety of clinical requirements. The grey scale values assigned to processed CT numbers on a display monitor, can be adjusted to suit special application requirements. Contrast can be enhanced by assigning just a narrow interval of CT numbers to the entire grey scale on the display monitor. This is called window technique; the range of CT numbers displayed on the whole grey scale being called the window width and the average value the window level. Changes in window width alter contrast, and changes in window level select the structures in the image to be displayed on the grey scale, i.e. from black to white. Narrowing the window compresses the grey scale to enable better differentiation of tissues within the chosen window. For example, in assessment of CT of the head, a narrow window of approximately 80 HU is used, thus allowing the eye to discriminate tissues only 2 3 HU apart. In practical terms, if we centre the window at 30 HU, then CT numbers above 70 will appear white and those below 10 will appear black. This allows subtle differences in tissue densities to be identified. Conversely, if the window is widened to 1500 HU, then each detectable shade of grey would cover 50 HU and soft tissue differentiation would be lost; however bone/soft tissue interfaces would be apparent. In practical terms the window width and level are preset on the workstation and can be adjusted by choosing the appropriate setting, i.e. a window setting for brain, posterior fossa, bone, etc. Tissue characteristics 6 Unlike conventional radiography, CT has relatively good contrast resolution and can therefore differentiate between tissues which vary only slightly in density. This is extremely valuable when assessing the brain, as grey and white matter vary only slightly in density. Artefacts aside, the densest structure in the head is bone, appearing white on CT. This is followed by acute haematoma, which is denser than flowing blood, due to clot retraction and loss of water. Blood is thought to be hyperdense due to the relative density of the haemoglobin molecule. With time, blood appears isodense and then hypodense, compared to brain parenchyma, due to clot resorption. Rebleeding and layering of blood (haematocrit effect due to gravity) can often cause confusion.
23 Brain can be differentiated into grey and white matter due to the difference in fatty myelin content between the two. Typically white matter (higher fatty myelin content HU 30) is darker than the adjacent grey matter (HU 40). Fat and air have low attenuation values and can be readily identified. CSF has a similar attenuation value to water, appearing black. Pathological processes may become apparent due to oedema within, or adjacent to, an abnormality. Oedema is less dense than normal brain. Occasionally the use of a contrast medium will reveal an abnormality either due to the inherent vascular nature of a lesion or due to alteration in the normal blood brain barrier. Tumours may be very variable in their appearance, but may be hyperdense due to a high nuclear/cytoplasmic ratio or tumour calcification. I Fundamentals of CT imaging Air Water Lung Fat Soft tissue Bone Bone Soft tissue Water 0 Fat Lung Air 1000 Hounsfield Scale of CT numbers. 7
24 Image artefacts IInterpretation of Emergency Head CT An artefact is a visual impression in the image of a feature that does not actually exist in the tissue being imaged. They are important to recognise so as not to be confused with pathology. Artefacts may occur due to scanner malfunction, patient movement and the presence of extrinsic objects within the slice being scanned, e.g. a metal foreign body. Fortunately, many artefacts have now been reduced or eliminated by advances in CT speed and technology. Motion artefacts Occur with voluntary and involuntary patient motion. Tend to result in streak patterns. Can be reduced by patient co-operation, quicker scan times and software compensation. Partial volume artefacts The CT number reflects the average attenuation within the voxel and thus, if a highly attenuating structure is present within the voxel, it will raise the average attenuation value partial volume artefact. Contamination can occur especially with thicker slices and near bony prominences. Always review the slices above and below to assess for structures likely to cause partial volume artefacts. Reduced by using thinner slices (e.g. posterior fossa) and software compensation. Metallic artefacts The attenuation coefficient of metal is much greater than any structure within the body. As a result, radiation is completely attenuated by the object and information about adjacent structures is lost. Produces characteristic star-shaped streak artefacts Can be reduced by widening the window; at a cost to intracranial detail. Again, software manipulation may help. Beam hardening artefacts Results from an increase in the average energy of the x-ray beam as it passes through a tissue. Think of CT as using a spectrum of radiation energy; low energy radiation is filtered out by high density structures such as bone, leaving higher energy radiation which is less absorbed by soft tissues, thus reducing tissue differentiation. Characterised by linear bands of low attenuation connecting two areas of high density, such as bone, e.g. the posterior fossa. Can be reduced by using a filter to adjust the spectrum of radiation and by post-processing software. 8
.")


25 I Fundamentals of CT imaging Beam hardening artefact: band of low attenuation across the pons (arrowheads). This reduces tissue differentiation and is characteristic of beam-hardening artefact. Motion artefact: characteristic movement blurring. Metallic artefact. Gross star-shaped metallic streaks due to gunshot pellets. 9

26 IInterpretation of Emergency Head CT Important anatomical considerations Review of normal anatomy Key for cerebral anatomy 1 ¼ Sphenoid sinus 2 ¼ Medulla oblongata 3 ¼ cerebellum Temporal Lobe 10

27 4 ¼ Fourth ventricle 5 ¼ Middle cerebellar peduncle 6 ¼ Sigmoid sinus 7 ¼ Petrous temporal bone and mastoid air cells 8 ¼ Cerebellopontine angle 9 ¼ Pons 10 ¼ Pituitary fossa 10 I Important anatomical considerations Frontal Lobe Temporal Lobe 11

28 IInterpretation of Emergency Head CT 11 ¼ Cerebellar vermis 12 ¼ Basilar artery 13 ¼ Prepontine cistern 14 ¼ Dorsum sellae 15 ¼ Temporal horn of lateral ventricle Frontal Lobe Temporal Lobe 12

29 16 ¼ Ambient cistern 17 ¼ Interpeduncular cistern 18 ¼ Cerebral peduncle 19 ¼ Sylvian fissure I Important anatomical considerations Frontal Lobe Temporal Lobe 13

30 IInterpretation of Emergency Head CT 20 ¼ Supra vermian cistern 21 ¼ Frontal horn of lateral ventricle 21a ¼ Third ventricle a Frontal Lobe Occipital Lobe Temporal Lobe 14

31 22 ¼ Head of caudate nucleus 23 ¼ Insular cortex 24 ¼ External capsule 25 ¼ Lentiform nucleus 26 ¼ Thalamus I Important anatomical considerations Frontal Lobe Occipital Lobe Temporal Lobe 15

32 IInterpretation of Emergency Head CT 27 ¼ Interhemispheric fissure 28 ¼ Anterior limb of internal capsule 29 ¼ Genu of internal capsule 30 ¼ Posterior limb of internal capsule 31 ¼ Trigone of lateral ventricle and calcified choroid plexus 32 ¼ Occipital horn of lateral ventricle Frontal Lobe Occipital Lobe Temporal Lobe Parietal Lobe 16

33 33 ¼ Body of lateral ventricle 34 ¼ Corona radiata I 33 Important anatomical considerations 34 Frontal Lobe Temporal Lobe Parietal Lobe 17

34 IInterpretation of Emergency Head CT 35 ¼ Centrum semiovale FB ¼ Frontal bone PB ¼ Parietal bone OB ¼ Occipital bone FB PB 35 OB Frontal Lobe Temporal Lobe Parietal Lobe 18

35 36 ¼ Pre-central gyrus 37 ¼ Central sulcus 38 ¼ Post-central gyrus I 27 Important anatomical considerations Frontal Lobe Parietal Lobe 19

36 39 ¼ Superior sagittal sinus. IInterpretation of Emergency Head CT Frontal Lobe Parietal Lobe 20

37 I Important anatomical considerations Frontal Lobe Parietal Lobe 21

38 Review of vascular territories IInterpretation of Emergency Head CT Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Terminal branches of the posterior cerebral artery 22

39 I Important anatomical considerations Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Anterior choroidal artery Terminal branches of the posterior cerebral artery 23

40 IInterpretation of Emergency Head CT Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Anterior choroidal artery Terminal branches of the posterior cerebral artery Penetrating branches of the anterior cerebral artery 24 Penetrating branches of the posterior cerebral artery and posterior communicating artery

41 I Important anatomical considerations Penetrating branches of the middle cerebral artery Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Anterior choroidal artery Terminal branches of the posterior cerebral artery Penetrating branches of the anterior cerebral artery Penetrating branches of the posterior cerebral artery and posterior communicating artery 25

42 IInterpretation of Emergency Head CT Penetrating branches of the middle cerebral artery Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Terminal branches of the posterior cerebral artery Penetrating branches of the posterior cerebral artery and posterior communicating artery 26 Anterior choroidal artery

43 I Important anatomical considerations Penetrating branches of the middle cerebral artery Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Terminal branches of the posterior cerebral artery Penetrating branches of the posterior cerebral artery and posterior communicating artery 27

44 IInterpretation of Emergency Head CT Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Terminal branches of the posterior cerebral artery 28

45 I Important anatomical considerations Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Terminal branches of the posterior cerebral artery 29

46 IInterpretation of Emergency Head CT Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery Terminal branches of the posterior cerebral artery 30

47 I Important anatomical considerations Terminal branches of the anterior cerebral artery Terminal branches of the middle cerebral artery 31

48 IInterpretation of Emergency Head CT Terminal branches of the anterior cerebral artery 32

49 Review of vascular anatomy Key for vascular anatomy 1 Anterior cerebral artery 2 Middle cerebral artery 3 Internal carotid artery 4 Right vertebral artery 5 Cortical branches of the middle cerebral artery 6 Posterior cerebral artery 7 Basilar artery 8 Left vertebral artery I Important anatomical considerations A R L 33
50
51 SECTION 2
52 II Reviewing a CT scan Interpretation of Emergency Head CT Suggested systematic approach to interpretation Check patient information and review scan protocol (e.g. non-contrast/ contrast enhanced). Check the scout image. May reveal a fracture or gross abnormality not obvious on the axial images. Review alignment of upper cervical vertebrae. A quick first pass is recommend, noting gross pathology, followed by a more detailed analysis of the images. Use the mnemonic ABBCS to remember important structures. Finally, extend search pattern to include orbits, sinuses, oropharynx, ears, craniocervical junction, face, vault and scalp. ABBCS 36 A Asymmetry Assess all slices comparing one side with another, remembering to allow for head tilt and to account for various forms of artefact. B Blood Acute haemorrhage appears hyperdense in relation to brain, due to clot retraction and water loss. Haemorrhage typically has a CT number in the range of HU. Assess for both blood overlying the cerebral hemispheres, and within the brain parenchyma. Assess the ventricles and CSF spaces for the presence or layering of blood. Review the sulci and fissures for subtle evidence of a SAH. Remember slow-flowing blood within a vessel can mimic clot. Conversely clot within a vessel is an important diagnosis: Venous sinus thrombosis Dense MCA sign in acute CVA B Brain Abnormal density Hyperdensity acute blood (free and within vessels), tumour, bone, contrast and artefact/foreign body. Hypodensity oedema/infarct, air and tumour. Displacement Look for midline shift. Examine midline structures such as the falx cerebri, pituitary and pineal glands. Look for asymmetry of CSF spaces such as effacement of an anterior horn of the lateral ventricles or loss of sulcal pattern suggesting oedema.
53 Assess for effacement of the basal cisterns and tonsillar herniation at the foramen magnum, as an indicator of raised intracranial pressure. Grey/white matter differentiation Normal grey/white matter differentiation should be readily apparent; white matter is of slightly reduced attenuation in comparison to grey matter due to increased fatty myelin content. In an early infarct, oedema leads to loss of the normal grey/white matter differentiation. This can be subtle and again only apparent when comparing both sides; identify normal structures such as internal capsule, thalamus, lentiform and caudate nuclei. C CSF spaces Cisterns, sulci and ventricles Assess the sizes of the ventricles and sulci, in proportion to each other and the brain parenchyma. Identify normal cisterns (quadrigeminal plate, suprasellar and the mid brain region) and fissures (interhemispheric and Sylvian). The ventricles often hold the key to analysing the image: Pathology may be primary, within a ventricle, or may result from secondary compression from adjacent brain pathology. If a ventricle is enlarged, consider whether it is due to an obstructive/non-communicating or non-obstructive cause. The former depends on site and the latter usually involves pathology in the subarachnoid space. Dilatation ex vacuo is caused by loss/atrophy of brain tissue, often resulting in abnormal secondary enlargement of the adjacent ventricle. Small ventricles can be normal in children (increases in size with age). Diffuse brain swelling can result in ventricular compression and reduced conspicuity of the normal sulcal/gyral pattern. Causes include metabolic/anoxic injury, infection, trauma and superior sagittal sinus thrombosis. S Skull and scalp Assess the scalp for soft tissue injury. Can be useful in patients where a full history is absent. Can help to localise coup and contracoup injuries. Carefully assess the bony vault underlying a soft tissue injury for evidence of a fracture. Assess the bony vault for shape, symmetry and mineralisation (focal sclerotic or lytic lesions). Remember to adjust windowing to optimise bony detail. II Reviewing a CT scan 37
54 II Interpretation of Emergency Head CT Acute stroke Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease (50%) Small vessel disease of penetrating arteries (25%) ¼ lacunar infarct Cardiogenic emboli (20%) Non-atheromatous causes (5%) Ischaemic infarction of the brain may be secondary to thrombosis or embolic disease. Transient ischaemic attacks (TIAs) precede a quarter of ischaemic strokes, and over 40% of these are in the 7 days before the stroke. The risk is highest in those patients with carotid stenosis or artial fibrillation. The incidence of stroke increases with age, although one in four people who experience a stroke are under 65 yrs. Risk factors include hypertension, smoking, diabetes, hyperlipidaemia, atherosclerosis, atrial fibrillation, the oral contraceptive pill and obesity. Temporal classification TIA ¼ transient ischaemic attack. The clinical syndrome lasts less than 24 hours, although in a proportion there may be infarction on cerebral imaging. Progressing stroke ¼ stepwise or gradually progressing accumulative neurological deficit evolving over hours or days Completed stroke ¼ persistent stable neurological deficit cerebral infarction as end stage of prolonged ischemia. Thrombolysis therapy has the potential to revolutionise the rapid assessment and treatment of ischaemic strokes (see Appendix 2) 38 Clinical features Spectrum of presentation from mild symptoms and signs, in a well patient, to a moribund comatosed patient. Commonly presents with unilateral weakness and/or sensory loss, visual field defect, dysphasia, and inattention/neglect.
55 Lacunar infarcts typically present with a purely motor and/or sensory deficit. Features of cortical involvement (visual field defect, dysphasia or inattention/neglect) are absent. Posterior circulation infarcts commonly present with vertigo, ataxia, diplopia, dysarthria, dysphasia or bilateral limb signs. The neurological deficit can be sudden, often occurring during sleep. This makes the time of onset difficult to ascertain. Radiological features CT features Hyperacute infarct (< 12 hours): Non-contrast CT may appear normal in up to 60%. However, contrary to general opinion, the CT may be abnormal in up to 75% of patients with MCA infarction, imaged within the first 3 hours. Hyperdense MCA sign represents acute intraluminal thrombus, and is seen in 25 50% of acute MCA occlusions. It is recognised as focal or linear white density within the MCA in the Sylvian fissure. Although not sensitive, it is a relatively specific sign. The normally well-defined lentiform nucleus becomes obscured in 50 80% of acute MCA occlusions. Acute infarction * hours Low-density basal ganglia Loss of normal grey/white differentiation secondary to oedema Look for the insular ribbon sign ¼ hypodense extreme capsule no longer distinguishable from insular cortex. Loss of the normal sulcal pattern is suspicious of underlying oedema. * 1 7 days Area of hypodensity in a vascular distribution (in 70%) due to cytotoxic oedema Mass effect local or generalised compression of the ventricles, basal cisterns and midline shift. Haemorrhagic transformation may occur after 2 4 days in up to 70%. Subacute/chronic infarction (> 7 days months) Decrease of mass effect and ex vacuo dilatation of ventricles. Loss of parenchymal mass, with associated sulcal/ventricular widening, due to encephalomalacia. II Acute stroke 39




56 II Interpretation of Emergency Head CT Left MCA territory infarcts: two examples of a hyperdense left MCA due to acute intraluminal thrombus (arrowheads). Two examples of early left MCA territory infarction. Note the subtle effacement of grey/white matter differentiation, due to oedema, and the insular ribbon sign. 40

 middle")

57 II Acute stroke Large areas of hypodensity within the left (top images) and right (bottom images) middle cerebral artery vascular territories, due to cytotoxic oedema. 41




58 II Interpretation of Emergency Head CT Lacunar infarct left lentiform nucleus (arrowhead). Infarct right superior frontal lobe (arrowhead). Small cerebellar infarct (arrowhead). Right posterior watershed infarct. This is an infarct at the watershed between middle and posterior cerebral artery territories (arrowheads). 42
.")



59 II Acute stroke Posterior cerebral artery territory infarct (arrowhead). Generalised low attenuation within the deep white matter of both cerebral hemispheres due to small vessel disease (arrowheads). Large infarct involving both the left middle and posterior cerebral artery territories. Another example of a right superior frontal lobe infarct. 43




60 II Interpretation of Emergency Head CT Chronic right MCA territory infarction. The infarcted area is of CSF density due to loss of brain substance, secondary to encephalomalacia, i.e. CSF eventually fills the dead space left following infarction. As a result, there is widening of local sulcal spaces and ex vacuo dilatation of adjacent ventricles, in this case the Sylvian fissure and right occipital horn, respectively. 44 Chronic right posterior watershed infarct. Chronic left posterior cerebral artery territory infarct with ex vacuo dilatation of the left occipital horn.
61 Haemorrhagic stroke Characteristics Haemorrhagic strokes account for only 10 15% of CVAs. Haemorrhagic stroke is associated with a high mortality rate, with only about 40% of patients surviving the first year. Small intracerebral arteries, often damaged by chronic hypertension, rupture and blood leaks directly into the parenchyma. Haematoma, with resulting oedema, leads to mass effect and further compromise to blood supply. In patients who present early, about a third will have haematoma expansion over the first few hours. Risk factors: Hypertension, underlying brain pathology, bleeding diatheses, anticoagulation treatment, thrombolysis therapy and cocaine abuse. II Acute stroke Clinical features Haemorrhagic and ischaemic strokes are difficult to distinguish clinically. Patients with haemorrhagic strokes are generally sicker, with abrupt onset and rapid deterioration. Common symptoms are headache, decreased conscious level, seizures, nausea and vomiting. Hypertension is characteristic. ECG changes may include myocardial ischaemia or dysrhythmias. Radiological features Non-contrast head CT is the investigation of choice. Acute haemorrhage is hyperdense. Surrounding oedema will result in loss of the grey/white matter differentiation. Mass effect will result in compression of overlying sulci, ventricular compression, midline shift and reduction in the size of the basal cisterns. Site and size of the haemorrhage are important, and will influence future treatment options. 45




62 II Interpretation of Emergency Head CT Large acute left parieto-occipital parenchymal haemorrhage. Right frontal haemorrhage with rupture in to the adjacent ventricles and further subarachnoid haemorrhage. Large acute haemorrhage within the left middle cerebral artery territory, with rupture in to the ventricular system and mass effect. Acute parenchymal haemorrhage within the right cerebellar hemisphere. 46




63 II Acute stroke Acute left superior parietal haemorrhage. Large acute left parieto-occipital haemorrhage with rupture into the ventricular system. Large acute left occipital haemorrhage with significant associated mass effect. Acute haemorrhage centred on the left thalamus and lentiform nucleus with intraventricular rupture. 47


64 II Interpretation of Emergency Head CT Acute haemorrhage layering in the left temporal horn. Acute haemorrhage centred on the right thalamus and lentiform nucleus with intraventricular rupture. 48


65 II Acute stroke Small acute right thalamic haemorrhage. Acute intraventricular haemorrhage. Additional acute focal haemorrhage within the central pons. 49
66 II Subdural haematoma (SDH) Interpretation of Emergency Head CT Characteristics Subdural haemorrhage arises between the inner layer of dura and arachnoid membrane of the brain. Bleeding results from torn bridging veins that cross the potential space between the cerebral cortex and dural venous sinuses. May be acute, subacute or chronic. 10% are bilateral. Acute SDH carries a high mortality and morbidity. Direct pressure results in ischaemia on the adjacent brain. Rebleeding secondary to osmotic expansion, or further trauma, leads to acute on chronic haemorrhage. The aetiology of chronic SDH is often unclear. Most likely from minor trauma in the preceding few weeks. In 50% of cases no such history is obtainable. Subdural haematomas are more common in elderly and alcoholic patients, where the subdural spaces are larger due to age related involution and/or atrophy. Subdural haemorrhage in the newborn is usually due to obstetric trauma. In neonates, non-accidental injury needs to be considered. Clinical features Acute SDH Patients often present following severe head trauma. Associated with underlying brain injury (50%) with a worse long-term prognosis than extradural haematoma. Patients generally have a decreased level of consciousness with focal neurological defects or seizures. There may be signs of raised intracranial pressure. Patients with a primary or secondary coagulopathy (e.g. alcoholics) may develop an acute SDH after only minor head trauma. A small acute SDH may be asymptomatic. 50 Chronic SDH Chronic SDH is the result of: Resolving phase of medically managed acute subdural haematoma. Repeated episodes of subclinical haemorrhage until becoming symptomatic. Chronic SDH often presents in the elderly with vague symptoms of gradual depression, personality changes, fluctuations of consciousness, unexplained headaches or evolving hemiplegia.
67 Predisposing factors: alcoholism, increased age, epilepsy, coagulopathy and prior placement of ventricular shunt. Over 75% occur in patients >50 years of age! Radiological features Location Blood is seen over the cerebral convexity, often extending into the interhemispheric fissure, along the tentorial margins, and beneath the temporal and occipital lobes. Do not cross the midline. Bilateral in 15 25% of adults (common in elderly) and in 80 85% in infants. II Subdural haematoma (SDH) CT features Acute SDH Peripheral high density crescentic fluid collection between the skull and cerebral hemisphere usually with: A concave inner margin. A small haematoma may only minimally press into brain substance. Convex outer margin following normal contour of cranial vault. Occasionally with a blood fluid level. Signs of mass effect with compression of overlying sulci, ventricular compression, midline shift and reduction in the size of the basal cisterns. Subacute SDH After approximately 1 to 2 weeks the subdural collection becomes isodense to grey matter; therefore detection may be challenging and only be recognised due to persistent mass effect: Effacement of cortical sulci. Deviation of lateral ventricle. Midline shift, white matter buckling. Displacement of grey white matter interfaces. Contrast enhancement will often define cortical subdural interface. Chronic SDH After approximately 2 weeks, chronic SDH s are often hypodense crescentic collections, with or without mass effect. Acute-on-chronic SDHs can further complicate the images, with hyperdense fresh haemorrhage intermixed, or layering posteriorly, within the chronic collection. Complex septated collections, and in rare cases calcification, may develop. 51
.")

.")

68 II Interpretation of Emergency Head CT Shallow acute left subdural haematoma (arrows). Large acute right subdural haematoma (arrowheads). 52 Acute subdural haemorrhage along the tentorium and over the left temporal lobe (white arrowheads). Additional subarachnoid haemorrhage (black arrowhead). Acute subdural haematoma over the left cerebral convexity, with an additional acute on chronic interhemispheric subdural collection (arrowheads).
 with")



69 II Subdural haematoma (SDH) Mixed density left subdural collection (arrowheads) with significant mass effect and midline shift to the right. Left isodense/hypodense subdural collection (arrowheads) with midline shift to the right. Large left isodense/ hypodense subdural haematoma (arrowheads) with associated mass effect. Large left chronic subdural haematoma (arrowheads). 53
70 II Extradural haematoma Interpretation of Emergency Head CT Characteristics An extradural haemorrhage arises within the potential space between the skull and dura. The young are more frequently affected as the dura is more easily stripped away from the skull. The dura becomes more adherent with age. 2% of all serious head injuries. Less than 1% of all children with cranial trauma. Rarely, extradural haematomas can occur spontaneously. Associated with a skull fracture in 75 95% of cases. Most commonly bleeding is from a lacerated (middle) meningeal artery/vein, adjacent to the inner table, from a fracture of the adjacent calvarium. Early diagnosis is imperative, as prognosis is good with early intervention. Conversely, a delay may result in cerebral herniation and brainstem compression. Types Acute extradural haematoma (60%) from arterial bleeding. Subacute haematoma (30%). Chronic haematoma (10%) from venous bleeding. Clinical features Patients often present with a history of head trauma. Associated with a variable level of consciousness. 20% to 50% have a brief loss of consciousness at the time of impact. As the haematoma continues to expand, they suffer a rapid deterioration. This lucid interval is referred to as the talk and die presentation. Neurological examination may reveal lateralising signs with a unilateral up-going plantar response. A sensitive sign in the conscious patient is pronator drift of the upper limb, when asked to hold both arms outstretched with the palms upwards. Close neurological observation is necessary to detect rising intracranial pressure; clinically, an escalating blood pressure with associated bradycardia. 54 Radiological features Location 66% temporoparietal (most often from laceration of middle meningeal artery).
71 29% frontal pole, parieto-occipital region, between occipital lobes and posterior fossa (most often from laceration of the dural sinuses from a fracture). Disruption of the sagittal sinus may create a vertex epidural haematoma. CT features Biconvex hyperdense elliptical collection with a sharply defined edge. Mixed density suggests active bleeding. Haematoma does not cross suture lines unless a diastatic suture fracture is present. May separate the venous sinuses and falx from the skull; this is the only type of intracranial haemorrhage to do this. Mass effect depends on the size of the haemorrhage and associated oedema. Venous bleeding is more variable in shape. Associated fracture line may be seen. II Extradural haematoma 55


72 II Interpretation of Emergency Head CT Subtle acute extradural haemorrhage (arrow). Acute right extradural haemorrhage (arrowheads). 56
 is hyperdense and isodense indicating both acute and subacute")
, subarachnoid haemorrhage (curved arrow) and")
73 II Extradural haematoma Right extradural haemorrhage. The collection (arrow) is hyperdense and isodense indicating both acute and subacute haemorrhage. In addition, there is evidence of subarachnoid haemorrhage (arrowheads). Acute extradural haemorrhage (arrowhead), subarachnoid haemorrhage (curved arrow) and multifocal contusions (arrows). 57
74 II Subarachnoid haemorrhage Interpretation of Emergency Head CT Characteristics Subarachnoid haemorrhage accounts for 10% of CVAs. Causes Spontaneous ruptured aneurysm (72%), AVM (10%) and hypertensive haemorrhage. Trauma. Blood enters the subarachnoid space onto the surface of the brain, between the pia and arachnoid, and may lead to raised intracranial pressure by obstructing the ventricular outflow of CSF. Incidence increases with age and peaks at age 50 years. Approximately 80% of cases of SAH occur in people aged years, with 15% occurring in people aged years % of patients with aneurysmal SAH have symptoms from a sentinel bleed, days prior to rupture. Morbidity can be severe and is increased by rebleeding, which often occurs in the first few days, and cerebral vasospasm 7 to 14 days after the initial event. 45% mortality within 8 weeks. Berry aneurysms are associated with hypertension, polycystic kidney disease, SLE, connective tissue disorders, AVMs and long term analgesic use. In 20% of non-traumatic SAH s, no lesion is found at post-mortem. 58 Clinical features SAH classically presents with a sudden onset of a severe thunderclap occipital headache, often described as the worst headache in their life. Associated with physical or emotional stress, coitus or head trauma % occur at rest. A leading cause of maternal mortality, accounting for 6 25% of maternal deaths during pregnancy. Meningeal irritation generates symptoms of neck stiffness, photophobia and low back pain, with a positive Kernig s sign. Focal neurological signs include third nerve palsy from compression by an expanding berry aneurysm of the posterior communicating artery of the Circle of Willis. Consider SAH in the comatosed or fitting patient. Fundoscopy may reveal papilloedema and subhyaloid retinal haemorrhages. Lumbar puncture (LP) is performed 12 hours after the onset of symptoms to evaluate xanthochromia. 15% of LPs are falsely negative.
75 Radiological features Location of aneurysm rupture Approximately 85% of saccular aneurysms occur in the anterior circulation. The most common sites of rupture are as follows: The internal carotid artery, including the posterior communicating (PCom) junction (41%). The anterior communicating (ACom) artery/anterior cerebral artery (34%). The middle cerebral artery (MCA) (20%). The vertebrobasilar and other arteries (5%). CT features CT scan without contrast. CT scan findings are positive in approximately 92% of patients who have SAH. Sensitivity decreases with time from onset of ictus. 98% within the first 12 hours and 93% within 24 hours. Decreases to 80% at 72 hours and 50% at 1 week. May be falsely negative in patients with small hemorrhages and in those with severe anaemia. The location of blood within the subarachnoid space correlates directly with the location of the aneurysm rupture in 70% of cases. Blood localised to the basal cisterns, the Sylvian or intrahemispheric fissures suggests rupture of a saccular aneurysm. Blood found lying over the cerebral convexities or within the superficial brain parenchyma suggests rupture of an AVM or mycotic aneurysm. ACom artery aneurysms are often associated with interhemispheric and intraventricular haemorrhages. MCA and PCom artery aneurysms are associated with intraparenchymal haemorrhages. Serial CT allows for surveillance of developing mass effect and hydrocephalus; up to 20% of patients develop some degree of obstructive hydrocephalus in the first 2 weeks post-ictus. A contrast-enhanced CT scan may reveal an underlying AVM; however, a non-contrast study should always be performed before considering a contrast study, so as not to interfere with the visualisation of subarachnoid blood. II Subarachnoid haemorrhage 59

.")


76 II Interpretation of Emergency Head CT Two examples of subtle subarachnoid haemorrhage. Faint hyperdense subarachnoid blood is seen outlining cerebral sulci (arrowheads). Subarachnoid blood seen predominantly within the right cerebral hemisphere with overlying soft tissue contusion. Hyperdense subarachnoid blood outlining several sulci within the left cerebral hemisphere. 60

.")

.")
77 II Subarachnoid haemorrhage Unenhanced scan and a CT angiogram. Extensive subarachnoid haemorrhage secondary to a ruptured MCA aneurysm (arrowheads). Extensive hyperdense subarachnoid haemorrhage outlining the basal cisterns. Subarachnoid blood within the suprasellar cistern (black arrowhead). Additional acute subdural haemorrhage along the tentorium and over the left temporal lobe (white arrowheads). 61
78 II Cerebral venous sinus thrombosis Interpretation of Emergency Head CT Characteristics Rare cause of stroke, affecting both sexes equally. Risk factors Septic causes (esp. in childhood): mastoiditis, facial cellulitis, meningitis, encephalitis, brain abscess, intracranial empyema. Aseptic causes: Hypercoagulable states: polycythemia rubra vera, idiopathic thrombocytosis, thrombocytopaenia, pregnancy, oral contraceptive pill. Low-flow state: CCF, shock. In one-third of patients no aetiology is found. Clinical features Classically presents with sudden, severe headache, worsened by coughing and associated with vomiting. Focal neurological deficit may be seen if venous infarction occurs. Cranial nerve palsies are characteristic. Seizures may occur. Sigmoid sinus thrombosis causes cerebellar signs and lower cranial nerve palsies. Periorbital oedema and chemosis are seen with cavernous sinus thrombosis. Fundoscopy may show papilloedema or retinal vein thrombosis. 62 Radiological features CT features CT may be normal. Non-contrast CT Hyperdense material within a vessel representing thrombosed blood. Not reliable as also seen with slow flowing blood. Cerebral infarction not characteristic of an arterial territory. Contrast CT Look for the delta / empty triangle sign (seen in 70%). This is a filling defect within the straight/superior sagittal sinus, and represents flow around a central non-enhanced clot. Gyral enhancement peripheral to an infarct, in 30 40%. Co-existing signs of infection or inflammation (e.g. sinusitis/mastoiditis) should raise suspicion.




79 II Cerebral venous sinus thrombosis Sagittal sinus thrombosis. Scans pre- and post-contrast. On the pre-contrast study, hyperdense material is seen within the sagittal sinus. This is an unreliable sign for acute thrombus. However, following contrast,the delta signisclearlyvisible. Venous haemorrhage in the left frontoparietal cortex due to sagittal sinus thrombosis. Image from a CTV demonstrating a filling defect in the SSS anteriorly and posteriorly, representing thrombus. The foci of haemorrhage in the right frontal parenchyma are typical of those seen with sinus thrombosis. 63
80 II Contusions Interpretation of Emergency Head CT Characteristics Traumatic injury to cortical surface of brain. Commonest form of traumatic cerebral injury: 20% of head injuries. Children:adults ¼ 2:1. Usually the result of linear acceleration/deceleration forces or penetrating injuries. Often described as coup / contra-coup injuries: Coup injury site of the direct impact on the stationary brain. Contra-coup site of impact of the moving brain upon the stationary. inner table, opposite to the site of the coup injury. Cerebral contusions are also produced secondary to depressed skull fractures and are associated with other intracranial injuries. Clinical features Patients often present with a history of head trauma or external signs of injury. Usually associated with a brief loss of consciousness. Confusion and altered GCS may be prolonged. Headache with vomiting in the conscious patient. Focal neurological deficit may occur if contusions arise near the sensorimotor cortex. Most patients make an uneventful recovery, but a few develop raised intracranial pressure, post-traumatic seizures and persisting focal neurological deficits. Beware the elderly, alcoholics and those taking anticoagulants that are at increased risk of haemorrhage. 64 Radiological features CT features Location Often multiple bilateral lesions at the interface between grey and white matter. Commonly along anterior, lateral and inferior surfaces of frontal and temporal lobes. Less frequently seen in parietal and occipital lobes and the posterior fossa. CT sensitive for haemorrhage in the acute post-traumatic period. The site of scalp swelling often indicates the site of the coup injury.
81 Focal/multiple areas of low attenuation, representing oedema, are intermixed with tiny areas of increased density, representing petechial haemorrhage. In children, a common appearance is of diffuse cerebral swelling without haemorrhage in the acute post-traumatic period. True extent becomes apparent over time with progression of cell necrosis, oedema and mass effect. II Contusions 65

.")
82 II Interpretation of Emergency Head CT Multi-focal contusions within both frontal lobes, with additional acute subarachnoid haemorrhage on the tentorium (arrowheads). Marked left fronto-parietal soft tissue swelling (astrerisk). Subtle left parieto-occipital contusions. 66

.")
83 II Contusions Large contusions in the right frontal and temporal lobes. Right temporal contusions, with subtle high density subarachnoid blood outlining sulci posteriorly (arrow). Note the adjacent subcutaneous soft tissue and left frontal swelling. 67
84 II Skull fractures Interpretation of Emergency Head CT Characteristics Result from trauma to the head. Classified as linear, depressed or base of skull fractures. Linear fractures are often uncomplicated and do not require treatment. However temporal bone fractures may result in an extradural haematoma. Depressed skull fractures may require surgery to elevate the bone fragments to prevent brain injury. Increased significance if the fracture is open, or communicates with an adjacent sinus, due to increased risk of infection. In basal skull fractures prophylactic antibiotics were once routinely prescribed to reduce the risk of meningitis, but their effectiveness is not validated and use is now restricted. Clinical features Open fractures underlie scalp lacerations and are often diagnosed during evaluation of the wound for closure. Depressed skull fractures are often palpable or visible during examination but may be masked by swelling around the area. Clinical signs of base of skull fracture: CSF rhinorrhoea. Haemotympanum. Bleeding from the external auditory meatus. Racoon eyes. Subconjunctival haemorrhage (with no posterior limit). Battle s sign (bruising over the mastoid area). Cranial nerve deficits. Blotting paper may be helpful in diagnosing CSF rhinorrhoea. 68


85 II Skull fractures Left parietal bone fracture (arrowheads) with marked overlying soft tissue contusion. Depressed skull fracture (arrow). Radiological features CT features Look closely at the initial scout image as this may demonstrate a fracture. Soft tissue swelling, or an underlying brain abnormality, may be associated with a fracture. Fractures may be missed if appropriate window parameters are not chosen. Always assess for fractures on bony windows. Fractures appear as sharply defined lines and should not be mistaken for a suture or vascular groove; a vascular groove often branches and both have typical sites. The presence of intracranial air may be secondary to an open fracture or connection with an air-containing sinus. 69



86 II Interpretation of Emergency Head CT Base of skull fracture (arrows). Complex vault fracture (arrows). Bilateral comminuted temporal bone fractures (arrows). 70
87 Meningitis II Characteristics Defined as inflammation of the meninges. Anatomically divided into: Inflammation of the dura, sometimes referred to as pachymeningitis less common. Inflammation of the arachnoid membrane and subarachnoid space, referred to as leptomeningitis more common. Meningoencephalitis also involves the parenchyma. Since the introduction of the haemophilus influenza vaccine, the average age of presentation has risen from 15 months to 25 years. Overcrowded closed communities (e.g. schools, day centres) predispose patients to meningitis, especially if immunocompromised. Concurrent illnesses such as pneumonia or other sites of sepsis (e.g. sinusitis, mastoiditis, otitis media) may contribute. Despite medical advances morbidity rates remain high. Meningitis Clinical features Fever, neck stiffness, photophobia, unremitting headache, mental status changes, with CSF findings, are essentials for diagnosis. Kernig s sign pain and resistance on passive knee extension with hips fully flexed. Brudzinski s sign hips flex on bending head forward. Seizures and cranial nerve palsies are common. Patients may present with signs of raised intracranial pressure. Detection at the extremes of age is difficult: Children may present with poor feeding, irritability, lethargy and vomiting. The elderly may only have a low grade fever and delirium. CSF sampling reveals raised WCC, predominantly neutrophils, with low glucose and high protein, in cases of bacterial meningitis. 71
88 II Interpretation of Emergency Head CT Radiological features CT features Non-contrast CT is often normal. Contrast enhanced CT Enhancement of the meningeal surfaces is a non-specific and often an inconsistent finding in patients with meningitis. When present, enhancement is usually seen over the cerebral convexities and in the interhemispheric and Sylvian fissures. Intense contrast enhancement, with associated meningeal thickening, is suggestive of granulomatous meningitis (such as TB and sarcoidosis). Associated obliteration of the basal cisterns, Sylvian fissures and suprasellar cistern. The cerebral sulci may be effaced, with associated flattening of the ventricles, due to cerebral oedema. Cerebral infarction is not uncommon. 72
, in a")

89 II Meningitis Leptomeningitis: dense haemorrhagic leptomeningeal collection over the right cerebral hemisphere (arrowheads), in a young patient with sinusitis. Meningeal enhancement in a patient with pneumococcal meningitis, outlining a subdural empyema (arrowheads). 73
90 II Raised intracranial pressure Interpretation of Emergency Head CT Characteristics The skull defines a fixed volume. Increasing the volume of contents, or brain swelling from any cause, rapidly increases intracranial pressure. Causes of raised intracranial pressure include: Haemorrhage (subdural, extradural, subarachnoid, intracerebral, intraventricular). Brain abscess. Meningoencephalitis. Primary or metastatic tumours. Hydrocephalus. Cerebral oedema (vasogenic, cytotoxic or interstitial). Clinical features Patients often present with a vague history of listlessness, irritability, drowsiness, early morning headaches, nausea and vomiting. The presentation may be acute with sudden neurological deterioration. Classic progression of symptoms: Bradycardia. Rising blood pressure. Respiratory depression (Cushings response). Pupillary constriction and then dilation. Third nerve palsy dilated ipsilateral pupil and ophthalmoplegia develop as intracranial pressure increases. Papilloedema is an unreliable sign. Look for absence of venous pulsation. 74
91 Radiological features CT features CSF spaces are reduced in size with effacement of sulci and the basal cisterns. Herniation of brain parenchyma (representing shift of the normal brain, through or across regions, to another site due to mass effect) occurs late. Types of cerebral herniation: Subfalcine herniation most common form of herniation and occurs as the brain extends under the falx in the supratentorial cerebrum. Transtentorial herniation occurs when the brain traverses across the tentorium at the level of the tentorial incisura. Can be divided into ascending and descending transtentorial herniation. Descending transtentorial herniation is caused by mass effect in the cerebrum which pushes the supratentorial brain through the incisura into the posterior fossa. Ascending transtentorial herniation is caused by mass effect in the posterior fossa which pushes the infratentorial brain through the incisura in an upward direction. Cerebellar tonsillar herniation cerebellar tonsils are forced through the foramen magnum. II Raised intracranial pressure 75
.")
 into the posterior fossa.")
92 II Interpretation of Emergency Head CT Subfalcine herniation: large left parenchymal haemorrhage with significant associated mass effect. There is midline shift to the right with sub-falcine herniation (arrowheads). 76 Transtentorial herniation: supratentorial mass effect (cause not shown) pushes the supratentorial brain through the incisura (arrow) into the posterior fossa. Tonsillar herniation: the cerebellar tonsils descend with increasing intracranial pressure, resulting in crowding of the foramen magnum (arrowheads).
93 Hydrocephalus II Characteristics Hydrocephalus results from an excess of CSF, due to an imbalance between CSF production and absorption, resulting in increased intraventricular pressure. Classified as communicating and non-communicating hydrocephalus: Communicating hydrocephalus ¼ elevated intraventricular pressure secondary to obstruction of CSF flow beyond the outlet of 4th ventricle. This may be due to impeded CSF flow over the cerebral convexities and/or impeded reabsorption of CSF by the arachnoid villi. Causes Subarachnoid haemorrhage, meningeal metastases and granulomatous meningitis. A less common cause of communicating hydrocephalus results from rapid CSF production, e.g. choroid plexus papilloma. Non-communicating hydrocephalus ¼ blockage of CSF flow within the ventricular system, with dilatation proximal to the obstruction. Often referred to as obstructive hydrocephalus. Location of obstruction / causes: Lateral ventricles, e.g. ependymoma, meningioma. Foramen of Monro, e.g. third ventricular colloid cyst. Third ventricle, e.g. large pituitary adenoma, craniopharyngioma. Aqueduct of Sylvius, e.g. congenital aqueduct stenosis, post intraventricular haemorrhage. Fourth ventricle/foraminae of Luschka and Magendie, e.g. congenital obstruction, intraventricular tumour, extrinsic compression. Hydrocephalus Clinical features Neonates/infancy. Enlarged cranium, bulging fontanelles, widely separated cranial sutures, vomiting, sleepiness and irritability. Older children and adults: headaches, nausea, vomiting, papilloedema, diplopia, problems with balance and coordination, gait disturbance, urinary incontinence, and changes in cognition including memory loss. Radiological features Non-communicating hydrocephalus Ventricular dilatation proximal to the level of an obstructing lesion. Dilatation of the occipital horns precedes dilatation of the frontal horns. Commensurate dilatation of the temporal horns with lateral ventricles. 77
94 II Interpretation of Emergency Head CT Progressive enlargement of the ventricular system, disproportionate to narrowed and effaced cortical sulci. Periventricular low attenuation is seen with acute onset of hydrocephalus; this represents interstitial oedema from transependymal flow of CSF. The obstructing lesion may be evident. Communicating hydrocephalus Symmetrical enlargement of the lateral, third, and fourth ventricles. Normal/effaced cerebral sulci. Dilatation of subarachnoid cisterns. Periventricular low attenuation, secondary to transependymal CSF flow, may be seen with acute onset hydrocephalus. 78



95 II Hydrocephalus Acute hydrocephalus: periventricular low attenuation is seen (arrows) representing interstitial oedema from transependymal flow of CSF. Obstructive hydrocephalus secondary to a hyperdense colloid cyst, at the level of the foramen of Munro. There is resultant dilatation of both frontal horns and trigones, and generalised effacement of cerebral sulci, due to brain swelling. Acute parenchymal, subarachnoid and intraventricular haemorrhage, with resultant dilatation of the temporal horns (arrows) due to developing communicating hydrocephalus. 79
96 II Abscesses Interpretation of Emergency Head CT Characteristics Localised purulent bacterial infection often developing in an area of cerebritis. Causes Extension from adjacent sinonasal infection, mastoiditis, otitis media. Generalised septicaemia: Respiratory causes: bronchiectasis, lung abscesses, empyema and pneumonia. Cardiac causes: right to left shunt, AVM and endocarditis. Osteomyelitis. Penetrating trauma or surgery. Predisposing factors Diabetes mellitus. Steroids/immunosuppressive therapy. Immune deficiency. Causative organisms Anaerobic streptococcus (most common). Staphylococcus. Bacteroides. Multiple organisms in 20%. Mycobacterium/salmonella more commonly in developing countries. Toxoplasmosis in AIDS patients. Clinical features Patients may present with headaches, vomiting, seizures, and altered mental state, in association with spiking pyrexia. Cranial nerve palsies or localised peripheral neurological deficits may be present. Signs of raised intracranial pressure. Source of sepsis may be clearly identifiable, or the patient may present with pyrexia of unknown origin. Diagnosis and treatment is difficult in those who are immunosuppressed. Significant long-term morbidity. Complications include cavernous sinus thrombosis, venous infarction and coning. 80 Radiological features CT features Location Supratentorial: infratentorial ¼ 2:1
97 Typically at the corticomedullary junction in the frontal and temporal lobes. Non-contrast CT Low density lesion with associated mass effect. Gas within lesion due to gas-forming organisms. Contrast-enhanced CT Ring enhancement, with central necrosis, and surrounding oedema. Homogeneous enhancement in lesions < 5 mm. Lesions may be multi-loculated and adjacent daughter abscesses may develop. II Abscesses 81


98 II Interpretation of Emergency Head CT Cerebral abscess. Scan pre- and post-contrast. Right superior parietal ring enhancing lesion (arrows), with surrounding vasogenic oedema. 82
99 Arteriovenous malformation II Characteristics Congenital abnormality consisting of abnormally dilated tortuous arteries and veins, with closely packed abnormal pathological vessels which shunt blood between the two. Most common intracerebral vascular lesion. 80% occur by the age of 40; 20% present under 20 years of age. May be part of a congenital syndrome, e.g. Sturge Weber. Venous malformations are less common, e.g. medullary venous malformation, cavernous malformation. Arterio-venous fistulae are usually post-traumatic. Arteriovenous malformation Clinical features Often asymptomatic. 10% are diagnosed incidentally. May present with headaches, seizures (non focal in 40%), acute intracranial haemorrhage (50%) or progressive neurological deficit (50%). Radiological features Location Supratentorial (90%): parietal > frontal > temporal > occipital lobe. Infratentorial (10%). Vascular supply Pial branches of ICA in 75% of supratentorial lesions, in 50% of posterior fossa lesions. Dural branches of ECA in 25% with infratentorial lesions. CT features Non-contrast CT Irregular lesion with large feeding arteries and draining veins. Mixed density lesion (60%), composed of large dense vessels, haemorrhage and calcification. Isodense lesion (15%), which may only be recognisable by associated mass effect. Low-density lesion (15%) due to atrophy secondary to associated local cerebral ischaemia. 10% are not visualised on unenhanced CT. 83
100 II Interpretation of Emergency Head CT Contrast-enhanced CT Dense serpiginous enhancement in 80%, representing tortuous dilated vessels. Lack of mass effect and oedema unless thrombosed or secondary haemorrhage. No enhancement in thrombosed AVM. Adjacent brain atrophy due to local cerebral ischaemia. 84
.")

101 II Arteriovenous malformation Arteriovenous malformation: mixed density lesion composed of coarse calcification, and faintly hyperdense vessels (arrowhead). Marked enhancement post-contrast. Arteriovenous malformation: large, faintly hyperdense, cortical vessels seen at the right vertex (arrowheads), with marked enhancement post-contrast. 85
102 II Solitary lesions 86 Interpretation of Emergency Head CT Characteristics Solitary space-occupying lesions are usually tumours. 30% are secondary tumours from breast, lung or melanoma primary lesions. Metastases tend to be most commonly found in the supratentorial compartment with the exception of those from renal cell carcinoma that tend to be in the posterior fossa. Primary tumours (e.g. astrocytoma, glioblastoma multiforme, oligodendrogliomas, ependymomas) have a < 50% 5-year survival. Frontal lobe masses often present late. Other solitary lesions include cerebral abscess, aneurysm, tuberculoma, granuloma or cyst. Clinical features May present with signs of raised intracranial pressure. Seizures, with or without a localising aura, are a common first presentation in adults. Focal neurology may evolve. There may be false localising signs. Solitary mass lesions can cause local effects, e.g. proptosis or epistaxis. Patients may present with odd behaviour, headache or vomiting. The presence of papilloedema is unreliable. Clinical presentation may help localise the site of the lesion: Temporal lobe complex partial seizures, hallucinations, déjà vu, taste, smell, dysphasia, field defects, fugue, functional psychosis and hypersexuality. Frontal lobe hemiparesis, seizures, personality change, grasp reflex (unilateral is significant), expressive dysphasia (Broca s area) and anosmia. Parietal lobe hemisensory loss, decreased stereognosis, sensory inattention, dysphasia and Gerstmann s syndrome (finger agnosia, left/right disorientation, dysgraphia, acalculia). Occipital lobe contralateral visual field defects. Cerebellum past pointing, intention tremor, nystagmus, dysdiadochokinesis and truncal ataxia (worse if eyes open). Cerebello-pontine angle nystagmus, reduced corneal reflex, fifth and seventh cranial nerve palsies, ipsilateral cerebellar signs and ipsilateral deafness. Mid-brain unequal pupils, confabulation, somnolence and an inability to direct the eyes up or down.
103 Radiological features Cerebral masses encompass a spectrum of appearances. Lesions may be hypodense, isodense or hyperdense (see Appendix 1). May be seen due to asymmetry or the presence of oedema and mass effect. Calcification may be present. Appearance post-contrast is often helpful. II Solitary lesions 87

. Right frontal glioma.")


104 II Interpretation of Emergency Head CT Left parafalcine meningioma: Scans pre- and post-i.v. contrast. The lesion is faintly hyperdense prior to contrast and avidly enhances post-contrast (arrowheads). Right frontal glioma. Scans pre- and post-contrast. Subtle heterogeneous, ill-defined mass within the right supra-orbital frontal lobe (arrowheads). Significant enhancement is seen post-contrast, with central non-enhancement, due to necrosis. The peripheral low density relates to vasogenic oedema. 88
105 Multiple lesions II Characteristics Neoplastic causes: Brain metastases are the most common neoplastic intracerebral lesion. They are found in up to 24% of all patients that die from cancer, and represent 20 30% of all brain tumours in adults. Infective causes: For example, cerebral abscesses, granulomata. Vascular causes: Multiple lesions of varying age are seen in multi-infarct dementia. Inflammatory causes: Demyelinating plaques can be seen as multiple low density lesions on CT, predominantly in the periventricular deep white matter. Traumatic causes: Contusions are frequently multiple after head trauma. Multiple lesions Clinical features Depends on the underlying pathology. See solitary lesions. Radiological features Contrast is taken up in tumours, inflammatory granulation tissue or areas of damage to the blood brain barrier. Melanoma and adenocarcinoma metastases may appear hyperdense prior to contrast. Calcification in malignant tumours is uncommon but, if present, suggests an adenocarcinoma. Calcification following granulomatous infection in not uncommon. Haemorrhage into metastases occurs infrequently, and when present suggests hypervascular tumours such as melanoma or hypernephroma. A follow-up CT performed two weeks after a traumatic event makes multiple contusions more conspicuous. 89

.")
106 II Interpretation of Emergency Head CT Multiple cerebral metastases. On this unenhanced scan their position is inferred by the associated oedema (arrows). 90 Multiple necrotic ring-enhancing metastases.


107 II Multiple lesions Multiple solid-enhancing metastases with prominent surrounding vasogenic oedema. Multiple ring-enhancing tuberculomas. 91



108 II Self-assessment section Interpretation of Emergency Head CT Below are 12 random cases that vary in complexity from easy to difficult. This test is somewhat artificial as no clinical information is given and hence assessment is blind. Formulate a provisional report and compare to the annotated answers at the end. Case 1. Case Case 3. Case 4.




109 II Self-assessment section Case 5. Case 6. Case 7. Case 8. 93



110 II Interpretation of Emergency Head CT Case 9. Case 10. Case 11. Case
, suggesting that it is somewhat chronic, and exerts mass effect on the adjacent cerebral hemisphere (white arrowheads).")
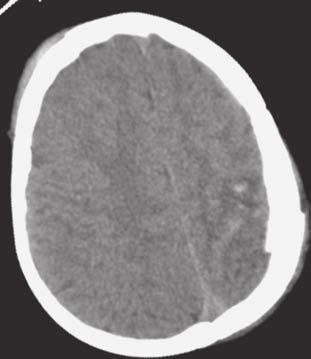
111 Self Assessment Answers II Self Assessment Answers Case 1. A large collection is seen over the left cerebral convexity. This is slightly hypodense to grey matter (asterisk), suggesting that it is somewhat chronic, and exerts mass effect on the adjacent cerebral hemisphere (white arrowheads). Additionally, linear hyperdensity is also seen within the collection (black arrowheads), indicating more acute haemorrhage. Diagnosis: Acute on chronic subdural haemorrhage. Case 2. A shallow hyperdense collection is seen over the right frontal lobe (arrowheads). Diagnosis: Acute subdural haemorrhage. 95
112 II Interpretation of Emergency Head CT Case 3. Large area of low density, involving both grey and white matter, within the left middle cerebral artery territory (arrowheads). This does not demonstrate haemorrhagic transformation. Diagnosis: Acute left middle cerebral artery territory infarct. 96 Case 4. Focal area of hyperdensity centred upon the right thalamus and lentiform nucleus (arrowhead). Diagnosis: Acute parenchymal haemorrhage. This type of haemorrhage has a strong association with uncontrolled hypertension.
. Diagnosis: Acute subarachnoid haemorrhage.")
113 II Self Assessment Answers Case 5. A shallow hyperdense collection is seen over the left cerebral convexity (arrowheads). Diagnosis: Acute subdural haemorrhage. Case 6. Subtle linear hyperdensity is seen outlining several sulci within the left cerebral hemisphere (arrowheads). Diagnosis: Acute subarachnoid haemorrhage. 97
.")
. 2.")
114 II Interpretation of Emergency Head CT Case 7. Axial scan viewed on bone windows, demonstrating sharply marginated defects within the left occipital bone (arrowheads). Diagnosis: Left occipital fracture. 98 Case Hyperdense biconvex collection over the right temporal lobe (straight white arrowheads). 2. Linear hyperdensity outlining the basal cisterns (curved arrowheads). 3. Focal parenchymal hyperdensity (black arrowheads). Diagnosis: Acute extradural haemorrhage with additional subarachnoid haemorrhage and parenchymal contusions.
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Imaging of Acute Cerebral Trauma
 July, 2005 Imaging of Acute Cerebral Trauma Louis Rivera, Harvard Medical School, Year III 46 y/o Female s/p Trauma - Unrestrained? MVC requiring Med Flight - Facial bruising/swelling - DEEP COMA - SEIZURES
July, 2005 Imaging of Acute Cerebral Trauma Louis Rivera, Harvard Medical School, Year III 46 y/o Female s/p Trauma - Unrestrained? MVC requiring Med Flight - Facial bruising/swelling - DEEP COMA - SEIZURES
Slide 1. Slide 2. Slide 3. Tomography vs Topography. Computed Tomography (CT): A simplified Topographical review of the Brain. Learning Objective
: A simplified Topographical review of the Brain. Learning Objective") Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
How to Read a Head CT. Andrew D. Perron, MD, FACEP. Head CT. Head CT. Head CT. Head CT. EM Residency Program Director
 Blood Can Be Very Bad How to Read a Head CT EM Residency Program Director (or How I learned to stop worrying and love computed tomography ) Department of Emergency Medicine Maine Medical Center Portland,
Blood Can Be Very Bad How to Read a Head CT EM Residency Program Director (or How I learned to stop worrying and love computed tomography ) Department of Emergency Medicine Maine Medical Center Portland,
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
NEURO IMAGING OF ACUTE STROKE
 1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
Brain Meninges, Ventricles and CSF
 Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CNS Imaging. Dr Amir Monir, MD. Lecturer of radiodiagnosis.
 CNS Imaging Dr Amir Monir, MD Lecturer of radiodiagnosis www.dramir.net Types of radiological examinations you know Plain X ray X ray with contrast GIT : barium (swallow, meal, follow through, enema) ERCP
CNS Imaging Dr Amir Monir, MD Lecturer of radiodiagnosis www.dramir.net Types of radiological examinations you know Plain X ray X ray with contrast GIT : barium (swallow, meal, follow through, enema) ERCP
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Acute Ischaemic Stroke
 Acute Ischaemic Stroke CT or MR SCA READIG FORM SCA ID: DATE OF READIG: SCA QUALIT: Good Moderate Poor Comment: READER ID: TPE OF SCA: CT: Without contrast: With contrast: MR: Diffusion: Perfusion ote
Acute Ischaemic Stroke CT or MR SCA READIG FORM SCA ID: DATE OF READIG: SCA QUALIT: Good Moderate Poor Comment: READER ID: TPE OF SCA: CT: Without contrast: With contrast: MR: Diffusion: Perfusion ote
Brain ميهاربا لض اف دمح ا د The Meninges 1- Dura Mater of the Brain endosteal layer does not extend meningeal layer falx cerebri tentorium cerebelli
 .احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
.احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
CT INTERPRETATION COURSE
 CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
CT - Brain Examination
 CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
Applicable Neuroradiology
 For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
Medical Neuroscience Tutorial Notes
 Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Sectional Anatomy Head Practice Problems
 1. Which of the following is illustrated by #3? (Fig. 5-42) A) maxillary sinus B) vomer C) septal cartilage D) perpendicular plate of ethmoid bone 2. What number illustrates the cornea? (Fig. 5-42) A)
1. Which of the following is illustrated by #3? (Fig. 5-42) A) maxillary sinus B) vomer C) septal cartilage D) perpendicular plate of ethmoid bone 2. What number illustrates the cornea? (Fig. 5-42) A)
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT
 Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
41 year old female with headache. Elena G. Violari MD and Leo Wolansky MD
 41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
Benign brain lesions
 Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cambridge Pocket Clinicians
 Headache Cambridge Pocket Clinicians Cambridge Pocket Clinicians provide practical, portable, note-based guidance for medical trainees, junior doctors, residents, and those from outside the field seeking
Headache Cambridge Pocket Clinicians Cambridge Pocket Clinicians provide practical, portable, note-based guidance for medical trainees, junior doctors, residents, and those from outside the field seeking
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
TRANSVERSE SECTION PLANE Scalp 2. Cranium. 13. Superior sagittal sinus
 TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
Cranial Cavity REFERENCES: OBJECTIVES OSTEOLOGY. Stephen A. Gudas, PT, PhD
 Stephen A. Gudas, PT, PhD Cranial Cavity REFERENCES: Moore and Agur, Essential Clinical Anatomy (ECA), 3rd ed., pp. 496 498; 500 507; 512 514 Grant s Atlas 12 th ed., Figs 7.6; 7.19 7.30. Grant s Dissector
Stephen A. Gudas, PT, PhD Cranial Cavity REFERENCES: Moore and Agur, Essential Clinical Anatomy (ECA), 3rd ed., pp. 496 498; 500 507; 512 514 Grant s Atlas 12 th ed., Figs 7.6; 7.19 7.30. Grant s Dissector
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM
 Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
THE ROLE OF IMAGING IN DIAGNOSIS OF SUBDURAL HEMATOMA: REVIEW ARTICLE
 THE ROLE OF IMAGING IN DIAGNOSIS OF SUBDURAL HEMATOMA: REVIEW ARTICLE * Dr. Sumendra Raj Pandey, Prof. Dr. Liu Pei WU, Dr. Sohan Kumar Sah, Dr. Lalu Yadav, Md. Sadam Husen Haque and Rajan KR. Chaurasiya
THE ROLE OF IMAGING IN DIAGNOSIS OF SUBDURAL HEMATOMA: REVIEW ARTICLE * Dr. Sumendra Raj Pandey, Prof. Dr. Liu Pei WU, Dr. Sohan Kumar Sah, Dr. Lalu Yadav, Md. Sadam Husen Haque and Rajan KR. Chaurasiya
HYPERACUTE STROKE CASE STUDIES. By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH
 HYPERACUTE STROKE CASE STUDIES By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH MC Case study 82 years old, lady 9:30 well, in touch with her son 11:30 hairdresser came to her house and found her
HYPERACUTE STROKE CASE STUDIES By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH MC Case study 82 years old, lady 9:30 well, in touch with her son 11:30 hairdresser came to her house and found her
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
OBJECTIVES. At the end of the lecture, students should be able to: List the cerebral arteries.
 DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
Cerebral hemisphere. Parietal Frontal Occipital Temporal
 Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
Neuropathology Of Head Trauma. Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center
 Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
STROKE - IMAGING. Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli.
 STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE
 Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE") Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
Imaging of Cerebrovascular Disease
 Imaging of Cerebrovascular Disease A Practical Guide Val M. Runge, MD Editor-in-Chief of Investigative Radiology Institute for Diagnostic, Interventional, and Pediatric Radiology Inselspital, University
Imaging of Cerebrovascular Disease A Practical Guide Val M. Runge, MD Editor-in-Chief of Investigative Radiology Institute for Diagnostic, Interventional, and Pediatric Radiology Inselspital, University
ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES
 ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES LABORATORY OBJECTIVES: 1. Histology: Identify structures indicated on three different slides or images of nervous system tissue. These images
ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES LABORATORY OBJECTIVES: 1. Histology: Identify structures indicated on three different slides or images of nervous system tissue. These images
What Is an Arteriovenous malformation (AVM)?
?") American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
The "filling defect" sign helps localise the site of intracranial aneurysm rupture on an unenhanced CT
 The "filling defect" sign helps localise the site of intracranial aneurysm rupture on an unenhanced CT Poster No.: C-3380 Congress: ECR 2010 Type: Topic: Authors: Keywords: DOI: Educational Exhibit Neuro
The "filling defect" sign helps localise the site of intracranial aneurysm rupture on an unenhanced CT Poster No.: C-3380 Congress: ECR 2010 Type: Topic: Authors: Keywords: DOI: Educational Exhibit Neuro
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018
 Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Blood Supply of Brain and Spinal Cord Arterial Supply of Brain The brain receives blood
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Blood Supply of Brain and Spinal Cord Arterial Supply of Brain The brain receives blood
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 14 The Brain and Cranial Nerves Introduction The purpose of the chapter is to: 1. Understand how the brain is organized, protected, and supplied
Principles of Anatomy and Physiology 14 th Edition CHAPTER 14 The Brain and Cranial Nerves Introduction The purpose of the chapter is to: 1. Understand how the brain is organized, protected, and supplied
Unit 18: Cranial Cavity and Contents
 Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Regional and Lobe Parcellation Rhesus Monkey Brain Atlas. Manual Tracing for Parcellation Template
 Regional and Lobe Parcellation Rhesus Monkey Brain Atlas Manual Tracing for Parcellation Template Overview of Tracing Guidelines A) Traces are performed in a systematic order they, allowing the more easily
Regional and Lobe Parcellation Rhesus Monkey Brain Atlas Manual Tracing for Parcellation Template Overview of Tracing Guidelines A) Traces are performed in a systematic order they, allowing the more easily
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
CT angiography and its role in the investigation of intracranial haemorrhage
 CT angiography and its role in the investigation of intracranial haemorrhage RD Magazine, 39, 458, 29-30 Dr M Igra Radiology SPR Leeds General Infirmary Dr I Djoukhadar Research fellow Wolfson Molecular
CT angiography and its role in the investigation of intracranial haemorrhage RD Magazine, 39, 458, 29-30 Dr M Igra Radiology SPR Leeds General Infirmary Dr I Djoukhadar Research fellow Wolfson Molecular
Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY
 Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY Objectives At the end of the lecture, the students should be able to: List the parts of the nervous system. List the function
Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY Objectives At the end of the lecture, the students should be able to: List the parts of the nervous system. List the function
Dating Neurological Injury
 Dating Neurological Injury wwwwwwwww Jeff L. Creasy Dating Neurological Injury A Forensic Guide for Radiologists, Other Expert Medical Witnesses, and Attorneys Jeff L. Creasy Associate Professor of Neuroradiology
Dating Neurological Injury wwwwwwwww Jeff L. Creasy Dating Neurological Injury A Forensic Guide for Radiologists, Other Expert Medical Witnesses, and Attorneys Jeff L. Creasy Associate Professor of Neuroradiology
Case Conference: Neuroradiology. Case 1: Tumor Case 1: 22yo F w/ HA and prior Seizures
 Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Neurosonography: State of the art
 Neurosonography: State of the art Lisa H Lowe, MD, FAAP Professor and Academic Chair, University MO-Kansas City Pediatric Radiologist, Children s Mercy Hospitals and Clinics Learning objectives After this
Neurosonography: State of the art Lisa H Lowe, MD, FAAP Professor and Academic Chair, University MO-Kansas City Pediatric Radiologist, Children s Mercy Hospitals and Clinics Learning objectives After this
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16
 The Brain Chapter 14 and select portions of Chapter 16") Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Nervous System The Brain and Spinal Cord Unit 7b
 Nervous System The Brain and Spinal Cord Unit 7b Chetek High School Mrs. Michaelsen 9.12 Meninges A. Meninges 1. The organs of the CNS are covered by membranes a. The meninges are divided into 3 layers:
Nervous System The Brain and Spinal Cord Unit 7b Chetek High School Mrs. Michaelsen 9.12 Meninges A. Meninges 1. The organs of the CNS are covered by membranes a. The meninges are divided into 3 layers:
b. The groove between the two crests is called 2. The neural folds move toward each other & the fuse to create a
 Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
Cranial cavity. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Cranial cavity Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology The Meninges The brain in the skull is surrounded by three membranes or meninges: 1-DURA MATER 2-ARACHNOID MATER 3-PIA MATER
Cranial cavity Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology The Meninges The brain in the skull is surrounded by three membranes or meninges: 1-DURA MATER 2-ARACHNOID MATER 3-PIA MATER
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University