CNS VASO-OCCLUSIVE DISEASE IN CHILDREN
|
|
|
- Amy Sherman
- 5 years ago
- Views:
Transcription
1 CNS VASO-OCCLUSIVE DISEASE IN CHILDREN Osama Atawneh MD, Tareq Hindi MD, Mustafa Hejazi MD and Anwar Dudin MD Pediatric Department, Augusta Victoria Hospital-Jerusalem INTRODUCTION Stroke is rare in children, with an incidence of 2.6 to 3.1/ Cerebral infarction occurs among children of all ages. The causes of stroke may be thrombotic, embolic, or hemorrhagic. Most commonly, pediatric stroke is caused by structural abnormalities of cerebral vasculature, inflammatory conditions that involve cerebral vessels, or congenital heart disease. Diagnosis still relies heavily on clinical recognition of the cardinal signs of focal cerebral injury. Topographic determination of the injured cerebral area has been enhanced by the advent of neuroradiologic methods such as MRI. Nonetheless, several disorders may mimic presentation of focal cerebral infarction; differentiating them from stroke depends heavily on an accurate history and physical examination. CASE REPORT: MOYAMOYA DISEASE IN A BEDOUIN CHILD. A female child born to first-degree consanguineous Bedouin parents, living in Ezzaria town near Jerusalem came to medical attention for the first time at 20 months of age. This full term infant was a product of uneventful pregnancy, home delivery without complications. Birth weight was 2.5 kg. She developed normally without any significant medical illness till the age of 20 months, when after awaking from a sleep she developed abnormal movement. She had sudden blinking of right eye and tonic-clonic movements of the right hand, with crying, for about 30min which resolved spontaneously. There was no history of fever, vomiting or diarrhea, but she had dry cough for the last week.no history of drug ingestion or head trauma. Upon arrival to the hospital she was fully conscious, temperature was 36.7º C, respiratory rate: 28/min, blood pressure: 88/43mmHg, pulse: 150 beats/min, weight: kg (10%), height: 77cm (< 5%), HC: 45.5 cm,o 2 sat: 95%. On examination, she had mild congested throat, good air entry bilaterally, harsh breathing, no heart murmur, soft abdomen, 30
2 spleen and liver not enlarged. Meningeal signs were negative, she had abnormal gait with mild right sided limping. Laboratory investigations showed: - CBC: Hg: 11.8 g/dl, MCV: 77, WBC: /mm³, Platelets /mm³. - ABG: PH:7.42, p CO2 :34, p O2 :72, HCO 3 :21,BE:-2, O 2 Sat:94% - Calcium:9.4 mg/dl, Creatinin: 0.4 mg/dl, Random blood sugar:108 mg/dl. Chest X-ray revealed left upper lobe hazy infiltration. Brain CT scan was normal. EEG noted a focal activity in temporo-parietal area. The patient was treated with Erythromycin for chest infection and discharged home in good general condition with no focal neurological deficit. One week later, she presented with one day history of focal left sided convulsion with loss of consciousness for about 5 minutes, followed by weakness of left side.temperature was 36.7º C, blood pressure 88/57mmHg, respiratory rate 28/min, heart rate 159 beats/min. She looked ill, distressed, dehydrated. She had evident left sided hemiplegia with facial involvement on the same side. Investigations on admission were not significant: - CBC: Hb: 10.9 g/dl, WBC: 7 600/mm³, Platelets /mm 3. - ESR: 15 mm/1 st hour. - Na: 139 meq/l, K: 4.0 meq/l. Cholesterol: 87 mg/dl, Triglycerides: 108 mg/dl, SGOT: 55 IU/L, SGPT: 11 IU/L, Alkakine phosphatase: 303 IU/L, Total Protein: 5.9 g/dl, albumin: 3.9 g/dl. - Blood Gases: ph: 7.48, P CO2 :24, P O2 :76, O 2 Sat: 96%, HCO 3 : 18, BE: Urine Analysis: Free. - Blood Culture: Negative. - CSF analysis: T. cell's: 0.0, Protein: 5mg/dl, Glucose: 74 mg/dl. CSF Culture: Negative. CSF Lactic acid: 1.1 mmol/l (N= ). - Serum Lactic acid: 0.9 mmol/l. - Protein C, S, Anti thrombin III, Leiden factor V were within normal range. 31
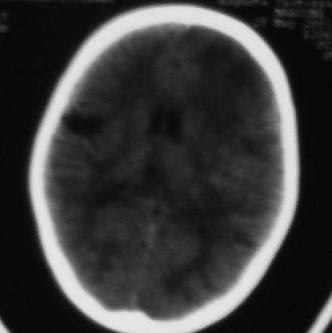
3 - ANA: Negative. - Plasma amino acids: Concentration of homocystein and methionin were normal. - Urine organic Acids: showed no specific or diagnostic feature. - Repeated Brain CT: showed large low attenuation area in right parietal region (figure 1). - Cardiac echography was normal. The patient was treated with supportive measures: correction of fluids and electrolytes, vitamins, physiotherapy, and was started on carbamazepine. Her general condition improved especially weakness of her left leg significantly decreased. The facial palsy resolved. No convulsions were stated during the two weeks of hospitalization. Follow-up evaluation showed nearly resolution of her left sided weakness, return to normal gait and use of her left hand. At the age of 27 months, she presented with 2 days history of fever, runny nose and cough. One day later, she was noticed to have right sided weakness (limping on the right leg, less use of her right hand). On examination, she was conscious, afebrile, respiratory rate 32/min, blood pressure 111/71mmHg, heart rate 150 beats/min, O 2 sat: 98%. She was hypoactive but meningeal signs were negative. Cranial nerves showed no deficit. She had right sided weakness (power 3/5 on both hands and legs) with facial involvement on the same side, deep tendon reflexes were exaggerated on both knees, babinski sign was positive on the right side. Repeated brain CT showed a large low attenuation area on right parietal region and a large new one on the left fronto-parietal region (figure 2). MRA demonstrated severe stenosis of both supraclenoid internal carotid arteries and multiple stenosis on both middle and anterior cerebral arteries (figure 3 and 4). The management was supportive with Biotin, Q 10 enzymes, B complex, and low dose of aspirin (100 mg once daily). The patient progress was satisfactory, the weakness significantly improved and she started to use her right hand better, with mild limping on the right side. 32
4 DISCUSSION Recurrent attacks of alternating hemiplegia (ischemic stroke), with no underlying metabolic, coagulation or cardiac cause raised the suspicion of arterial occlusion in this infant. Brain MRA showed changes typical for Moyamoya disease. Reviewing the literature, this is one of the youngest reported cases of Moyamoya disease. The youngest reported case was a 4 months old infant (1). A second case has been described in a 20- month-old girl with Down syndrome who presented with seizure and hemiparesis (2). Moyamoya disease (MMD) is a progressive occlusive disease of the cerebral vasculature with particular involvement of the circle of Willis and the arteries that feed it. Moyamoya ("puff of smoke") characterizes the appearance on angiography of abnormal vascular collateral networks that develop adjacent to the stenotic vessels. Pathologically, MMD is characterized by intimal thickening in the walls of the terminal portions of the internal carotid vessels bilaterally. Approximately, 10% of cases of Moyamoya syndrome are due to a genetic cause (autosomal recessive trait) and are termed primary Moyamoya syndrome.two genetic locations have been identified as significant in primary Moyamoya syndrome: 3p26-p24.2 and 17q25 (3). Secondary Moyamoya syndrome refers to cases in which the syndrome is a consequence or result of another underlying disorder (Neurofibromatosis type I, sickle cell disease (4), tuberous sclerosis, meningitis, retinitis pigmentosa, fibromuscular dysplasia, atherosclerosis, Down syndrome, and Fanconi s anemia and following radiation therapy to the skull base of children(5) ). MMD occurs primarily in Asians, but it also can occur (with varying degrees of severity) in Caucasians, African Americans, Haitians, and Hispanics. About 10 years ago, Goto and Yonekawa reported the worldwide distribution of Moyamoya disease at that time (6). The female-to-male ratio was 1.8:1. Moyamoya syndrome may occur at any age, it most often occurs between the ages of five and ten years and during the third and fourth decades of life. Symptoms vary with age of onset. Cerebral ischemic events are more common in children. Children with Moyamoya syndrome may have convulsions, involuntary muscle movements, hemiplegia or paralysis of one limb. Some children may show signs of mental retardation. Patients tend to develop one or more of the following visual disturbances: blindness in one 33
5 half of the visual field of one or both eyes (hemianopia), diplopia, bilaterally (right and left) decreased visual acuity, and the inability to recognize objects. Later onset is characterized by bleeding. Adults are more prone to intracranial bleeding below the middle covering of the brain (subarachnoid). This may be followed by accumulation of excessive amounts of watery fluid in the optic disks (papilledema) and fainting. Neurosis (mainly anxiety) usually occurs in adult Moyamoya patients. Patients usually have sudden interruptions of the blood supply to the brain (cerebral infarctions), which can lead to brain death. DIAGNOSIS In the presence of atypical features such as young age and absence of obvious risk factors for stroke the diagnosis is suspected. Cerebral angiography is the admitted standard for diagnosis. The following findings support the diagnosis: stenosis or occlusion at the terminal portion of the internal carotid artery or the proximal portion of the anterior or middle cerebral arteries, abnormal vascular networks in the vicinity of the occlusive or stenotic areas and bilateralism of the described findings. Magnetic resonance angiography (MRA) can be performed. Any of these findings on MRA may reduce the need for conventional angiography. In Moyamoya disease, color-coded ultrasound is diagnostic for the lesion of the internal carotid artery. TREATMENT Medical treatment is advised for patients experiencing ministrokes. Aspirin, vasodilators (calcium- channel blockers) and/or anticoagulants may be prescribed. Surgical treatment has been reasonably successful, especially among children, and various surgical approaches have been developed. Response of patients to these complex and very complicated surgeries varies. Genetic counseling may be of benefit for patients and their families if they have the hereditary form of Moyamoya syndrome. 34

6 FIGURE 1 FIGURE 2 35

7 FIGURE 3 36


8 FIGURE 4 37
9 REFERENCES 1-Sribnick EA, Goldblatt MR, Campbell JW, add et al. Moyamoya disease in a four-month-old: a case study. Clin Pediatr (Phila) 2003;42(3): Fung CW, Kwong KL, Tsui EY. Moyamoya syndrome in a child with Down syndrome. Hong Kong Med J2003;9(1): McKusick VA, Ed. Online Mendelian Inheritance in Man (OMIM). The Johns Hopkins University. Moyamoya Disease 2. Entry Number; : Last Edit Date; 8/15/ Dobson SR, Holden KR, Nietert PJ, et al. Moyamoya syndrome in childhood sickle cell disease: a predictive factor for recurrent cerebrovascular events. Blood 2002;99(31): Kondoh T, Morishita A, Kamei M, add et al. Moyamoya syndrome after prophylactic cranial irradiation for acute lymphocytic leukemia. Pediatr Neurosurg 2003 ;39(5): Goto Y, Yonekawa Y: Worldwide distribution of moyamoya disease. Neurol Med Chir (Tokyo) 1992;32:
A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur.
 A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur. 6 year old school going child. Apparently normal till 3 yrs when she developed
A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur. 6 year old school going child. Apparently normal till 3 yrs when she developed
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
Arterial Ischemic Stroke with Protein S Deficiency in Pakistan
 Case Reports Arterial Ischemic Stroke with Protein S Deficiency in Pakistan Faika Usman, Ali Hassan, Arsalan Ahmad From Section of Neurology, Department of Medicine, Shifa International Hospitals and College
Case Reports Arterial Ischemic Stroke with Protein S Deficiency in Pakistan Faika Usman, Ali Hassan, Arsalan Ahmad From Section of Neurology, Department of Medicine, Shifa International Hospitals and College
Moyamoya Disease A Vasculopathy and an Uncommon Cause of Recurrent Cerebrovascular Accidents
 Moyamoya Disease A Vasculopathy and an Uncommon Cause of Recurrent Cerebrovascular Accidents Yasmin S. Hamirani, Md 1 *, Mohammad Valikhani, Md 2, Allison Sweney, Ms Iii 2, Hafsa Khan, Md 2, Mohammad Pathan,
Moyamoya Disease A Vasculopathy and an Uncommon Cause of Recurrent Cerebrovascular Accidents Yasmin S. Hamirani, Md 1 *, Mohammad Valikhani, Md 2, Allison Sweney, Ms Iii 2, Hafsa Khan, Md 2, Mohammad Pathan,
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
SWISS SOCIETY OF NEONATOLOGY. Neonatal cerebral infarction
 SWISS SOCIETY OF NEONATOLOGY Neonatal cerebral infarction May 2002 2 Mann C, Neonatal and Pediatric Intensive Care Unit, Landeskrankenhaus und Akademisches Lehrkrankenhaus Feldkirch, Austria Swiss Society
SWISS SOCIETY OF NEONATOLOGY Neonatal cerebral infarction May 2002 2 Mann C, Neonatal and Pediatric Intensive Care Unit, Landeskrankenhaus und Akademisches Lehrkrankenhaus Feldkirch, Austria Swiss Society
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Moyamoya disease in the midwestern United States
 Neurosurg Focus 5 (5):Article 1, 1998 Moyamoya disease in the midwestern United States Nicholas M. Wetjen, B.S., P. Charles Garell, M.D., Nicholas V. Stence, and Christopher M. Loftus, M.D. Division of
Neurosurg Focus 5 (5):Article 1, 1998 Moyamoya disease in the midwestern United States Nicholas M. Wetjen, B.S., P. Charles Garell, M.D., Nicholas V. Stence, and Christopher M. Loftus, M.D. Division of
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Guidelines for management of stroke in childhood
 Guidelines for management of stroke in childhood A clinical syndrome typified by rapidly developing signs of focal or global disturbance of cerebral functions, lasting more than 24 hrs or leading to death,
Guidelines for management of stroke in childhood A clinical syndrome typified by rapidly developing signs of focal or global disturbance of cerebral functions, lasting more than 24 hrs or leading to death,
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Internal Carotid Artery Dissection
 May 2011 Internal Carotid Artery Dissection Carolyn April, HMS IV Agenda Presentation of a clinical case Discussion of the clinical features of ICA dissection Discussion of the imaging modalities used
May 2011 Internal Carotid Artery Dissection Carolyn April, HMS IV Agenda Presentation of a clinical case Discussion of the clinical features of ICA dissection Discussion of the imaging modalities used
There are several types of epilepsy. Each of them have different causes, symptoms and treatment.
 1 EPILEPSY Epilepsy is a group of neurological diseases where the nerve cell activity in the brain is disrupted, causing seizures of unusual sensations, behavior and sometimes loss of consciousness. Epileptic
1 EPILEPSY Epilepsy is a group of neurological diseases where the nerve cell activity in the brain is disrupted, causing seizures of unusual sensations, behavior and sometimes loss of consciousness. Epileptic
MOYA Moya disease is a rare idiopathic
 Research Papers Moya Moya Cases Treated with Encephaloduroarteriosynangiosis Parimal Tripathi, Varsha Tripathi, Ronak J. Naik and Jaimin M. Patel From Gujarat Cancer & Research Institute, Ahmedabad; Sterling
Research Papers Moya Moya Cases Treated with Encephaloduroarteriosynangiosis Parimal Tripathi, Varsha Tripathi, Ronak J. Naik and Jaimin M. Patel From Gujarat Cancer & Research Institute, Ahmedabad; Sterling
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MP (PAEDIATRICS) EXAMINATION - JULY/AUGUST 2012' PAPER I STRUCTURED ESSAY QUESTIONS
 EXAMINATION - JULY/AUGUST 2012' PAPER I STRUCTURED ESSAY QUESTIONS") CO POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MP (PAEDIATRICS) EXAMINATION - JULY/AUGUST 2012' Date 16 th July 2012 Time :- 9.00 a.m. - 12.00 noon PAPER I STRUCTURED ESSAY QUESTIONS Answer
CO POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MP (PAEDIATRICS) EXAMINATION - JULY/AUGUST 2012' Date 16 th July 2012 Time :- 9.00 a.m. - 12.00 noon PAPER I STRUCTURED ESSAY QUESTIONS Answer
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
NEONATAL SEIZURES-PGPYREXIA REVIEW
 NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
Recent Advances in Neurology Difficult Cases
 Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
10/19/12. Uncommon Causes of Stroke. José Biller, MD, FACP, FAAN, FAHA Disclosures. Dr. Biller has no disclosures to report
 10/19/12 Uncommon Causes of Stroke José Biller, MD, FACP, FAAN, FAHA Loyola University Chicago Stritch School of Medicine Chicago, IL José Biller, MD, FACP, FAAN, FAHA Disclosures Dr. Biller has no disclosures
10/19/12 Uncommon Causes of Stroke José Biller, MD, FACP, FAAN, FAHA Loyola University Chicago Stritch School of Medicine Chicago, IL José Biller, MD, FACP, FAAN, FAHA Disclosures Dr. Biller has no disclosures
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech
 Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech Beatrice E. Gee, MD Medical Director, Sickle Cell and Hematology Program Children s
Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech Beatrice E. Gee, MD Medical Director, Sickle Cell and Hematology Program Children s
Imaging of Moya Moya Disease
 Abstract Imaging of Moya Moya Disease Pages with reference to book, From 181 To 185 Rashid Ahmed, Hurnera Ahsan ( Liaquat National Hospital, Karachi. ) Moya Moya disease is a rare disease causing occlusion
Abstract Imaging of Moya Moya Disease Pages with reference to book, From 181 To 185 Rashid Ahmed, Hurnera Ahsan ( Liaquat National Hospital, Karachi. ) Moya Moya disease is a rare disease causing occlusion
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
Talking About The Facts: Stroke In Children
 Talking About The Facts: Stroke In Children AWARENESS LEADS TO A QUICKER RESPONSE AND LIFESAVING OUTCOMES FOR CHILDREN. Pediatric Stroke Warriors continues to strengthen communities by providing support
Talking About The Facts: Stroke In Children AWARENESS LEADS TO A QUICKER RESPONSE AND LIFESAVING OUTCOMES FOR CHILDREN. Pediatric Stroke Warriors continues to strengthen communities by providing support
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report
 Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography
 Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography Case report ELISHA S. GURDJIAN, M.D., BLAISE AUDET, M.D., RENATO W. SIBAYAN, M.D., AND LLYWELLYN
Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography Case report ELISHA S. GURDJIAN, M.D., BLAISE AUDET, M.D., RENATO W. SIBAYAN, M.D., AND LLYWELLYN
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
بسم هللا الرحمن الرحيم كليه طب الموصل
 بسم هللا الرحمن الرحيم المقابسة الجراحية الثانية كليه طب الموصل فرع الجراحه A rare complication of linear skull fracture Presented by Hassan Qusay Ismaeel History was taken from the mother of the patient
بسم هللا الرحمن الرحيم المقابسة الجراحية الثانية كليه طب الموصل فرع الجراحه A rare complication of linear skull fracture Presented by Hassan Qusay Ismaeel History was taken from the mother of the patient
Cardiovascular Disease
 Cardiovascular Disease Chapter 15 Introduction Cardiovascular disease (CVD) is the leading cause of death in the U.S. One American dies from CVD every 33 seconds Nearly half of all Americans will die from
Cardiovascular Disease Chapter 15 Introduction Cardiovascular disease (CVD) is the leading cause of death in the U.S. One American dies from CVD every 33 seconds Nearly half of all Americans will die from
DISCUSSION BY: Dr M. R. Shakeebi, MD, Rheumatologist
 Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
CMS Limitations Guide MRA Radiology Services
 CMS Limitations Guide MRA Radiology Services Starting July 1, 2008, CMS has placed numerous medical necessity limits on tests and procedures. This reference guide provides you with all of the latest changes.
CMS Limitations Guide MRA Radiology Services Starting July 1, 2008, CMS has placed numerous medical necessity limits on tests and procedures. This reference guide provides you with all of the latest changes.
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Longitudinal anterior-to-posterior shift of collateral channels in patients with moyamoya disease: an implication for its hemorrhagic onset
 CLINICAL ARTICLE Longitudinal anterior-to-posterior shift of collateral channels in patients with moyamoya disease: an implication for its hemorrhagic onset Shusuke Yamamoto, MD, Satoshi Hori, MD, PhD,
CLINICAL ARTICLE Longitudinal anterior-to-posterior shift of collateral channels in patients with moyamoya disease: an implication for its hemorrhagic onset Shusuke Yamamoto, MD, Satoshi Hori, MD, PhD,
Treatment of Unruptured Vertebral Artery Dissecting Aneurysms
 33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
CLINICAL CASE PRESENTATION
 European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
What is the appropriate evaluation of cryptogenic stroke, and when is a hypercoagulability work-up needed? David E. Thaler, MD, PhD, FAHA
 What is the appropriate evaluation of cryptogenic stroke, and when is a hypercoagulability work-up needed? David E. Thaler, MD, PhD, FAHA Neurologist in Chief, Tufts Medical Center Professor and Chair
What is the appropriate evaluation of cryptogenic stroke, and when is a hypercoagulability work-up needed? David E. Thaler, MD, PhD, FAHA Neurologist in Chief, Tufts Medical Center Professor and Chair
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
David Dredge, MD MGH Child Neurology CME Course September 9, 2017
 David Dredge, MD MGH Child Neurology CME Course September 9, 2017 } 25-40,000 children experience their first nonfebrile seizure each year } AAN/CNS guidelines developed in early 2000s and subsequently
David Dredge, MD MGH Child Neurology CME Course September 9, 2017 } 25-40,000 children experience their first nonfebrile seizure each year } AAN/CNS guidelines developed in early 2000s and subsequently
Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography
 Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography Kazumi Kimura, Yoichiro Hashimoto, Teruyuki Hirano, Makoto Uchino, and Masayuki Ando PURPOSE: To determine
Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography Kazumi Kimura, Yoichiro Hashimoto, Teruyuki Hirano, Makoto Uchino, and Masayuki Ando PURPOSE: To determine
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Uroradiology For Medical Students
 Uroradiology For Medical Students Lesson 8 Computerized Tomography 2 American Urological Association Objectives In this lesson you will: Gain more experience reading CT images Learn how computer generated
Uroradiology For Medical Students Lesson 8 Computerized Tomography 2 American Urological Association Objectives In this lesson you will: Gain more experience reading CT images Learn how computer generated
PORT WINE STAINS AND STURGE-WEBER SYNDROME
 PORT WINE STAINS AND STURGE-WEBER SYNDROME Ong Hian Tat It is important for general practitioners to recognize cutaneous port-wine stains as these could signify important association with Sturge Weber
PORT WINE STAINS AND STURGE-WEBER SYNDROME Ong Hian Tat It is important for general practitioners to recognize cutaneous port-wine stains as these could signify important association with Sturge Weber
Childhood Stroke: Risk Factors, Symptoms and Prognosis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-childrens-health/childhood-stroke-risk-factors-symptoms-andprognosis/3657/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-childrens-health/childhood-stroke-risk-factors-symptoms-andprognosis/3657/
Admission Medical Information Form
 Return Form to: Admission Medical Information Form Part I: To Be Completed by Family or Staff of Birth: Sex: M F Race: Marital Status: Home Address: Phone Number: Number/Street City State Zip Last Time
Return Form to: Admission Medical Information Form Part I: To Be Completed by Family or Staff of Birth: Sex: M F Race: Marital Status: Home Address: Phone Number: Number/Street City State Zip Last Time
1.3 What is the mechanism of action of adrenaline in anaphylactic shock? (20 marks)
") DCH Examination -Short Answer Questions Time - Two and half hours Model paper 1.1 A 10 month old child presented with urticaria within one hour following ingestion of an egg. Mother claims that a week
DCH Examination -Short Answer Questions Time - Two and half hours Model paper 1.1 A 10 month old child presented with urticaria within one hour following ingestion of an egg. Mother claims that a week
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Hong Kong College of Emergency Medicine. Joint Clinical Meeting OSCE Answer Key
 Hong Kong College of Emergency Medicine Joint Clinical Meeting OSCE Answer Key Question 1 A full term new born was delivered in the A&E. What are the five components of Apgar score? (1.5 marks) Skin color
Hong Kong College of Emergency Medicine Joint Clinical Meeting OSCE Answer Key Question 1 A full term new born was delivered in the A&E. What are the five components of Apgar score? (1.5 marks) Skin color
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
A RARE NEUROLOGICAL PRESENTATION OF SLE. Dr Yoganand M N Dr Prithvi P Nayak
 A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
Sickle Cell Disease. Edward Malters, MD
 Sickle Cell Disease Edward Malters, MD Introduction Vaso-occlusive phenomena and hemolysis are the clinical hallmarks of Sickle Cell Disease (SCD) Inherited disorder due to homozygosity for the abnormal
Sickle Cell Disease Edward Malters, MD Introduction Vaso-occlusive phenomena and hemolysis are the clinical hallmarks of Sickle Cell Disease (SCD) Inherited disorder due to homozygosity for the abnormal
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Neurological examination of the neurosurgical patient. Dániel Bereczki SU Department of Neurology
 Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Moyamoya syndrome associated with cocaine abuse Case report
 Neurosurg Focus 5 (5):Article 7, 1998 Moyamoya syndrome associated with cocaine abuse Case report Marc S. Schwartz, M.D., and R. Michael Scott, M.D. Division of Neurosurgery, Albany Medical College, Albany,
Neurosurg Focus 5 (5):Article 7, 1998 Moyamoya syndrome associated with cocaine abuse Case report Marc S. Schwartz, M.D., and R. Michael Scott, M.D. Division of Neurosurgery, Albany Medical College, Albany,
CT and MR Imaging in Young Stroke Patients
 CT and MR Imaging in Young Stroke Patients Ashfaq A. Razzaq,Behram A. Khan,Shahid Baig ( Department of Neurology, Aga Khan University Hospital, Karachi. ) Abstract Pages with reference to book, From 66
CT and MR Imaging in Young Stroke Patients Ashfaq A. Razzaq,Behram A. Khan,Shahid Baig ( Department of Neurology, Aga Khan University Hospital, Karachi. ) Abstract Pages with reference to book, From 66
Diagnosing Epilepsy in Children and Adolescents
 2019 Annual Epilepsy Pediatric Patient Care Conference Diagnosing Epilepsy in Children and Adolescents Korwyn Williams, MD, PhD Staff Epileptologist, BNI at PCH Clinical Assistant Professor, Department
2019 Annual Epilepsy Pediatric Patient Care Conference Diagnosing Epilepsy in Children and Adolescents Korwyn Williams, MD, PhD Staff Epileptologist, BNI at PCH Clinical Assistant Professor, Department
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Case presentation. By Dr ARSHIYA SIDDIQUA P.G General Medicine
 Case presentation By Dr ARSHIYA SIDDIQUA P.G General Medicine Chief complaints. A 22 yr old male patient came to the hospital with complaints of weakness of both upper limbs and lower limbs since 1 week
Case presentation By Dr ARSHIYA SIDDIQUA P.G General Medicine Chief complaints. A 22 yr old male patient came to the hospital with complaints of weakness of both upper limbs and lower limbs since 1 week
New Patient Questionnaire
 New Patient Questionnaire Name: Primary Care Physician: Date of Birth: / / Home Phone: ( ) Cell Phone: ( ) Why are you seeing a cardiologist? (please answer in detail) Have you ever seen a cardiologist
New Patient Questionnaire Name: Primary Care Physician: Date of Birth: / / Home Phone: ( ) Cell Phone: ( ) Why are you seeing a cardiologist? (please answer in detail) Have you ever seen a cardiologist
Pregnancy and Neurological Disorders
 Pregnancy and Neurological Disorders Myles Connor NHS Borders and University of Edinburgh, United Kingdom Outline Why is it important? Specific conditions Eclampsia Cerebrovascular disease Epilepsy Idiopathic
Pregnancy and Neurological Disorders Myles Connor NHS Borders and University of Edinburgh, United Kingdom Outline Why is it important? Specific conditions Eclampsia Cerebrovascular disease Epilepsy Idiopathic
Permanent neonatal diabetes mellitus. Case Report
 Rawal Medical Journal An official publication of Pakistan Medical Association Rawalpindi Islamabad branch Established 1975 Volume 36 Number 4 October - December 2011 Case Report Permanent neonatal diabetes
Rawal Medical Journal An official publication of Pakistan Medical Association Rawalpindi Islamabad branch Established 1975 Volume 36 Number 4 October - December 2011 Case Report Permanent neonatal diabetes
Guidelines for the Immediate Management of Paediatric Patients with Sickle Cell Disease (SCD) and Acute Neurological Symptoms
 and Acute Neurological Symptoms") Guidelines for the Immediate Management of Paediatric Patients with Sickle Cell Disease (SCD) and Acute Neurological Symptoms Document Information Version: 2 Date: Sept 2014 Authors (incl. job title):
Guidelines for the Immediate Management of Paediatric Patients with Sickle Cell Disease (SCD) and Acute Neurological Symptoms Document Information Version: 2 Date: Sept 2014 Authors (incl. job title):
Laser Vein Center Thomas Wright MD Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
Spontaneous cervicocephalic arterial dissection with headache and neck pain as the only symptom
 J Headache Pain (2012) 13:247 253 DOI 10.1007/s10194-012-0420-2 BRIEF REPORT Spontaneous cervicocephalic arterial dissection with headache and neck pain as the only symptom Hajime Maruyama Harumitsu Nagoya
J Headache Pain (2012) 13:247 253 DOI 10.1007/s10194-012-0420-2 BRIEF REPORT Spontaneous cervicocephalic arterial dissection with headache and neck pain as the only symptom Hajime Maruyama Harumitsu Nagoya
Neuro-Ocular Grand Rounds
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Overview Blood supply of the brain What is moyamoya disease? > 1
 Moyamoya Disease Overview Moyamoya disease is caused by blocked arteries at the base of the brain. The name "moyamoya" means "puff of smoke" in Japanese and describes the appearance of tiny vessels that
Moyamoya Disease Overview Moyamoya disease is caused by blocked arteries at the base of the brain. The name "moyamoya" means "puff of smoke" in Japanese and describes the appearance of tiny vessels that
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Patient Encounters in the Primary Care Setting
 Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1 Clinical Cases Learning
Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1 Clinical Cases Learning
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease
 Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease Summary Outline of the presentation of stroke in paediatric patients with sickle cell disease, urgent investigations,
Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease Summary Outline of the presentation of stroke in paediatric patients with sickle cell disease, urgent investigations,
Convulsive Disorder and Cardiac Disease. Running Rachael, Active Ashlee, Sassy Savannah
 Convulsive Disorder and Cardiac Disease Running Rachael, Active Ashlee, Sassy Savannah Convulsive Disorder Seizure is over. Pay attention to how long the seizure lasts. Stay calm. Make the person as comfortable
Convulsive Disorder and Cardiac Disease Running Rachael, Active Ashlee, Sassy Savannah Convulsive Disorder Seizure is over. Pay attention to how long the seizure lasts. Stay calm. Make the person as comfortable
Child-Youth Epilepsy Overview, epidemiology, terminology. Glen Fenton, MD Professor, Child Neurology and Epilepsy University of New Mexico
 Child-Youth Epilepsy Overview, epidemiology, terminology Glen Fenton, MD Professor, Child Neurology and Epilepsy University of New Mexico New onset seizure case An 8-year-old girl has a witnessed seizure
Child-Youth Epilepsy Overview, epidemiology, terminology Glen Fenton, MD Professor, Child Neurology and Epilepsy University of New Mexico New onset seizure case An 8-year-old girl has a witnessed seizure
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on Needed to be resuscitated at birth
 No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
X-Plain Seizures And Epilepsy Reference Summary
 X-Plain Seizures And Epilepsy Reference Summary Introduction More than 2 million people in the United States have been diagnosed with epilepsy or have experienced a seizure. During a seizure, a person
X-Plain Seizures And Epilepsy Reference Summary Introduction More than 2 million people in the United States have been diagnosed with epilepsy or have experienced a seizure. During a seizure, a person
PEDIATRIC MEDICAL HISTORY QUESTIONNAIRE
 Division of Otolaryngology Main Phone: 847 504-3300 Main Fax: 847 504-3305 Mihir Bhayani, MD Judy L. Chen, MD Mark E. Gerber, MD, FACS, FAAP Joseph Raviv, MD Ilana Seligman, MD, FACS, FAAP Michael J. Shinners,
Division of Otolaryngology Main Phone: 847 504-3300 Main Fax: 847 504-3305 Mihir Bhayani, MD Judy L. Chen, MD Mark E. Gerber, MD, FACS, FAAP Joseph Raviv, MD Ilana Seligman, MD, FACS, FAAP Michael J. Shinners,