Bill Howie, DNP, CRNA, CCRN. Care of Patients with Complex Needs: The Basics. 2015
|
|
|
- Florence McKinney
- 5 years ago
- Views:
Transcription


1 Bill Howie, DNP, CRNA, CCRN. Care of Patients with Complex Needs: The Basics. 2015
2 Discuss the concept of mechanism of injury and how it helps guide management of care. Describe why it is important to have a high index of suspicion when considering the care of a trauma patient. Provide strategies to minimize or prevent primary injury. Discuss the concept of secondary injury, and how to minimize this type of injury.
3 Discuss appropriate lab values necessary to provide optimal patient care (follow trends). Formulate a dynamic plan of care for the critically ill/injured patient. List 5 components of the primary survey as they relate to assessment of the patient. Define shock. Delineate the six major causes or types of shock.
4 Define damage control surgery. Define and discuss damage control resuscitation Describe the three stages of damage control surgery. Name at least 5 basic rules of trauma. Discuss the definitive management a trauma patient s airway. Include a brief description of the necessary steps and how many people are required to safely accomplish them.
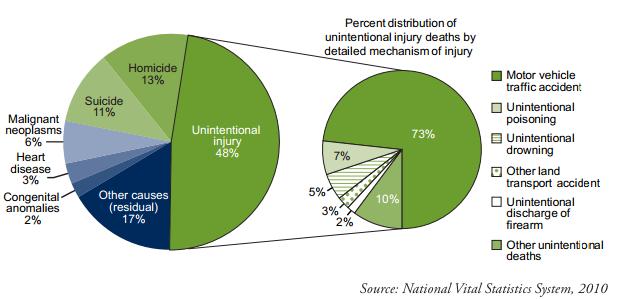
5 Trauma, whether caused by unintentional or intentional injury, is the leading cause of death in the USA from birth to 44 years of age (CDC 2006). 160,000 deaths/year, 340,000 permanently disabled, $107 billion/year in medical fees, hospitalization, and lost wages. Assaults/GSW s cost on average $40,000 per pt. (70% not insured) at the WFSTC.
6 A structural alteration or physical imbalance brought about by acute exposure to mechanical, thermal, electrical or chemical energy. At times, the trauma can be caused by and lack of heat, food, water, or O2. In cases of blunt and penetrating trauma, a transfer of energy leads to the ultimate damage produced to the victim. The precipitating cause of the traumatic injury is typically referred to as the mechanism of injury.
7 Each year the STC admits about 8000 pts. 72% are male, 28% are female. Statistics: 42% MVC (about 34% did not use a seatbelt); 5% MCC (90% did not wear a helmet); 6% Pedestrian struck; 17% Fall; 8% GSW; 8% Stabbed; 84% Blunt Trauma; 16% Penetrating Trauma

8

9

10
11
12

13

14
15 What is a mechanism of injury? Why is it important to consider how a patient is injured? What are the most common mechanisms of injury seen at the STC and in the US? Does the mechanism of injury have an impact on how the patient is triaged and sent to a given facility for further work-up?
16
17 The Internet Journal of Advanced Nursing Practice ISSN,

18
19 ABC (Disability Exposure) (Reassess) This process is dynamic, not static (the primary survey). Primary Survey/ Secondary Survey. Work-up =standard tests (History, X-ray exams, Lab work, Physical exam etc.). Index of suspicion must be high, and based on presentation and mechanism. Why?
20 All patients should receive: 100% 02 3 to 5 minutes with an effective mask fit. Suction immediately available. Cricoid pressure (for suspected full stomach). In line stabilization (for suspected C-spine injury). All appropriate airway equipment and pharmacologic agents available. End tidal C02 confirmation. How many people are required to safely manage the airway?
21
22 Airway Commitment to a definitive airway Your first try is usually your best try RSI is usually the rule If it isn t within 3 feet of you, it might as well be on the moon If we can bag, we re going to go, if we can t bag, we re going to go (push the relaxant) The surgeon is your friend



23 Definitive Airway Cpmtrol Rapid Sequence Induction, Inline w/ cricoid Preoxygenate Cricoid & inline Check etco2, cricoid pressure Rapid DL no neck extension
24 The skillful and appropriate placement of an endotracheal tube is the best way to: Ensure delivery of adequate oxygenation. Ensure optimal ventilation. Protect the lungs from aspiration. Facilitate optimal resuscitation of the patient. Direct laryngoscopy with orotracheal intubation is the principle method used in acute trauma patients because of speed and technical advantages. (Wilson, Grande, & Hoyt Trauma 2007).
25 In the hands of experienced anesthesia, rapid sequence intubation followed by direct laryngoscopy is a remarkably effective approach to emergency airway management. An algorithm designed around this approach can achieve very high levels of success. During the first hour after admission, 6088 patients required intubation, of whom 21 (0.3%) received a surgical airway. During the first 24 h, 10 more patients, for a total of 31, received a surgical airway, during approximately 32,000 attempts (0.1%). Stephens CT, Kahntroff S, Dutton RP. (2009, ).
26 Rapid sequence induction(rsi) with in line cervical spine stabilization is considered the gold standard in airway management in the acutely injured trauma patient. Assisted ventilation (modified RSI) is frequently justified because trauma patients are often hypoxic and hypercapnic. Following intubation, the ETT position must be confirmed with measurement of ETc02.
27 Inability to ventilate or intubate constitutes an emergency condition. Airway adjuncts such as the Glidescope and bougie are useful backup strategies to the standard direct laryngoscopy. Adjuncts such as the LMA and the esophageal combitube are useful backup options to temporize until a definitive airway can be obtained. A surgical airway (cricothyrotomy or tracheostomy must be considered when endotracheal intubation is deemed impossible ).
28 Treat all trauma airways as an unstable c- spine and full stomach until proven otherwise


29

30
31 Various studies have noted less movement with the GlideScope and fiberoptic airway management techniques Mean movement approx 11 with the Glidescope, and 14 with a standard Macintosh intubation. (a max of 19 vs 29 ) The light wand or trach light produces even less movement Turkstra et al. (2005) Anesth Analg: 101(4) pp Kill, et al. (2013) Videolaryngoscopy with glidescope reduces C spine movement. J Emerg Med: 44(4) pp
32

33

34
35 Traumatic Shock is a state triggered by failure to deliver adequate O2 to the cells in the body. Clinical indicators of shock include: LOC, BP, UO, lactate and CRT HR, acidosis, O2 demand coupled with decreased 02 delivery produces lactate Cyanosis, pallor, and low or absent pulse ox.
36 A failure of adequate oxygen delivery or utilization at the cellular level, perpetuated by cellular and humoral responses. Prolonged shock results in a cumulative oxygen debt and in disruption of end-organ integrity and homeostasis. (Dutton, 2006)
37 Cardiogenic: Pump failure Hemorrhagic: Decreased fluid Anemic: Decreased O2 carrying Neurogenic: Loss of vascular tone Toxic/Endotoxic/Anaphylaxis/Sepsis Traumatic Shock: Acute accident/injury. Can be a combination of factors
38 Decreased O2 uptake by the lungs Decreased O2 carrying capacity Decreased vascular volume and tone Decreased cardiac function (Causes can include: tension pneumo, tamponade, ischemia or contusion, decreased inotropic state, drugs, CNS injury and failure of cellular metabolism(sepsis).
39 Diminished blood pressure Decreased mentation Cyanosis, pallor, diaphoresis Hypothermia/Hyperthermia Decreased urine output Absent pulse oximetry signal
40 Novel Indices to Detect Shock Shock Index HR / SBP (>0.9) Better indicator than hypotension alone ABC 4 parameters: penetrating mechanism, positive FAST, SBP < 90, HR > or more: 75% sensitive 86% specific for predicting massive transfusion Cocci MN, et al. Emerg Med Clin North Am 2007; 25: Nunez TC, et al. J Trauma 2009; 66:
41 Using a Sequential Organ Failure Assessment (SOFA) score and serum lactate levels 50 ICU patients were studied. It was concluded that: An unfavorable outcome (worsening SOFA score) was 7 times more likely in a patient with abnormal peripheral perfusion (cool extremities)than in one with normal peripheral perfusion (CRT) A patient with abnormal CRT was 5 times more likely to have hyperlactatemia than a patient with normal CRT
42 Lima et al (2009) The prognostic value of the subjective assessment of peripheral perfusion in critically ill patients. Crit Care Med: 37(3) pp
 and ultimately patient")
43 Tachycardia. Vasoconstriction. Cardiac output. Narrow pulse pressure. MAP. Blood flow. Mounting metabolic debt leading to apoptosis (cellular death) and ultimately patient death.
44 I) Up to 15% of blood volume= anxiety. II) Up to 30%= increased HR, normal BP, Increased RR,decreased UO, anxiety. III) Up to 40%= Increased HR,RR, anxiety, confusion,decreased BP, oliguria. IV) Greater than 40%= Increased HR,RR, anuric, confusion leading to lethargy.
45 Compensated Traumatic Shock (not an issue if homeostasis returned) Decompensated Traumatic Shock (Lack of perfusion builds a Debt of local cell damage that yields a toxic effect when perfusion restored) Sub-Acute Irreversible Shock=MSOF Acute Irreversible Shock=PPBBBOL
46 Wilson (2007, 217)
47 MacGarty & Nott (2013) Disaster Medicine: A Case Based Approach: Springer-Verlag London. H

48

49 Sihler K C, Napolitano L M Chest 2009;136:
50
51 The stages of traumatic shock are closely related to the body s response to hemorrhage or inadequate perfusion. Macrocirculatory response is mediated by the neuroendocrine system. Microcirculatory responses will determine the overall patient outcome.
52 Prime trigger of neuroendocrine response to shock. The tendency is to maintain perfusion to the heart and brain, at the expense of other tissues. Kidneys and adrenal glands produce renin, angiotensin, aldosterone, cortisol, erythropoientin, and catecholamines.
53 Initially, well maintained in early shock. Lactate, free radicals and other factors are released from ischemic cell beds to act as negative inotropes. The lungs tend to be a filter for the inflammatory by-products. This can unfortunately lead to ARDS and MSOF.

54 The gut is one of the earliest organ systems altered by poor perfusion. Glucose, nutritional status, and coagulation function can result from liver insult. Skeletal muscles are a prime source of lactate and free radicals. Sepsis is a result of the bodies altered immune system.
55 Volume resuscitation and blood/blood product transfusion is the mainstay of treatment for hemorrhagic shock. Large bore IV access and rapid infusion systems are invaluable adjuncts in the early resuscitation stages. Hypothermia worsens acid-base disorders, coagulopathies and myocardial function. Use fluid warmers, convection forced-air blankets, increased OR room temperature, and the like to combat this preventable problem.

56
57 Sihler K C, Napolitano L M Chest 2009;136:
58 Definition of massive hemorrhage Loss of one blood volume over 24 hours. Loss of 50% blood volume over 3 hours. Loss of 150 ml per minute.
59 Total blood volume for 70 kg adult.07 x 70 kg = 4.9 liters. 50% of total blood volume for 70 kg adult.50 x 4.9 liters = 2.45 liters. 40% of total blood volume for 70 kg adult.40 x 4.9 liters = 1.96 liters. Note: An acute loss of 40% blood volume is immediately life threatening!
60 The Problem Trauma mortality 40% related to failed hemorrhage control Sauaia A, et al: J Trauma 1995; 38: Massive hemorrhage 2 nd cause of pre-hospital death Mackenzie EJ, et al: J Trauma 2000, pp
61 Potentially Preventable Injury Mortality Of the injured who will die, 50% die before they reach a hospital. Head injury is the major cause of death in the field and in the hospital. Uncontrolled hemorrhage or MOF-related shock is the cause of death in about 40% of deaths. About 20% of hemorrhagic deaths appear to have been potentially preventable.

62 Sources of Life-Threatening Hemorrhage Chest. Abdomen. Retroperitoneum. Soft Tissue Compartment. External ( The Street ).
63 Laboratory Evidence of Shock Metabolic acidosis / base deficit Elevated lactate Anemia Elevated osmolarity {Coagulopathy}
64 Mortality of Massive Transfusion Mortality versus units of blood transfusion. Average mortality 47% if more than 10 units. Mortality 28% if received 10 to 19 units. Mortality 65% if received 20 to 39 units. Mortality 83% if received 40 or more units. Wilson WK, et al. Am Surg. 1987; 53:
65 Mortality 22% 1-10 units. Mortality 30% units. Mortality 50% units. Mortality 59% greater than 40 units*. *One patient received 126 units RBC s and was discharged to home.

66 The goal of treatment is the rapid and effective return of an adequate blood volume. Adequate return implies that body hemostasis, oxygen carrying capability, and oncotic pressure are returned to pre-insult levels and are maintained through-out the hospitalization period. Metabolic demands must be met.
67 Clinical Presentation: DEFINITION of MASSIVE TRANSFUSION EVENT (MTE): Hypovolemic shock and coagulopathy can lead to widespread cellular dysfunction and organ damage. The MTE will provide a guide for efficient and effective delivery of blood products for Trauma and other patients who meet criteria for massive transfusion.
68 Criteria for activation of MTE 1. Loss of Blood volume in the first hour of activation: Adult patients requiring >4 units of RBCs Pediatric Patients requiring >20 ml/kg of RBCs 2. Loss of RBC units in the first 12 hours of resuscitation: Adults using more than 10 units of RBCs Pediatric patients using greater than 0.1 units/kg of RBCs
69 Final 2014 Declaration of a Massive Transfusion Event (MTE) 1. To assure availability of needed blood products in appropriate ratios for massive transfusion 2. To assure appropriate and timely notification of the Blood Bank to allow them to prepare 1 X SBP <90 within 10 minutes of admission OR 2 X SBP <100 within 10 minutes of admission OR Unable to obtain blood pressure AND Penetrating torso trauma OR Positive FAST OR Obvious ongoing external blood loss OR Plans to take patient directly to OR EXCLUSION: Cardiac Arrest with no ROSC More than 2 units of uncrossmatched PRBC are being given Note: The first 2 units of uncrossed PRBCs are often given to catch up with blood loss that may not be ongoing. Thawed group AB universal donor plasma is typically not needed in this situation unless there is obvious coagulopathy. Group AB plasma should be given with the next 2U of PRBC and in an equal ratio to PRBC thereafter if concern for ongoing hemorrhage Physician discretion TRU Tech/Charge RN or OR RN calls the Blood Bank at Should state: 1. We are declaring a Massive Transfusion Event 2. Patient s MRN and STC number and name, if known. 3. Patient s sex and approximate age 4. Name of Physician in Charge (Trauma or Anesthesia Attending) Cross-match sample should be immediately tubed to the Blood Bank Once the sample is received and tested, the Blood Bank will immediately prepare: 6 units of type-specific or compatible PRBC 6 units of type-specific or compatible plasma 1 bag of apheresis platelets (6 equivalent units) The TRU (OR) should send a Tech/Volunteer to the Blood Bank Type specific or compatible RBC s and plasma should be ready within minutes. DO NOT wait for all products if there is a delay in dispense The Blood Bank will continue to prepare: 6 units of type-specific or compatible PRBC 6 units of type-specific or compatible plasma 1 bag of apheresis platelets (6 equivalent units) until informed that the MTE is terminated Once the need for massive transfusion is over, the TRU or OR calls the Blood Bank at Should state: 1. We are ending the Massive Transfusion Event 2. Patient s MRN and STC number and name, if known. Uncrossed matched group O PRBC and group AB plasma should be given until type-specific or compatible products are available. The completed cards should be sent to the Blood Bank as products are used. Please also call the Blood Bank with ANY use of O Rh-neg PRBC so it can be replaced
70 Expedite control of hemorrhage. Limited crystalloid infusion. BP systolic. Blood products early and often: 1:1:1. Frequent lab studies (lactate, ionized Ca).
71 1. Minimize agent effects of Volatile Anesthetics on CV system. 2. Higher narcotic approach why? We often have no idea how volume contracted a patient is CO= HR x SV. Volatile Agents effect SV and afterload. Narcotics primarily effect HR only. If we control for HR and BP drops then we can assume volume depletion.
72 1. Supportive fluid resuscitation: Avoid acute exsanguination. Minimize risk of organ system failure. Facilitate hemostasis. 2. Preservation of homeostasis: Temperature. Pulmonary function.
73 BP > 100 systolic Cardiac output normal or high Adequate Perfusion! Lactate, base deficit. Mixed venous oximetry. New technology.
74 Damage control Failure of standard methods. Hypothermia and coagulopathy. Acidosis and metabolic abnormalities. Principles of damage control Obtain surgical hemostasis. Temporize hollow viscus injury. Pack coagulopathic bleeding. Resuscitate and correct hypothermia.

75 Pre-hospital fluids (too much of a good thing?)

76 Prehospital Fluids

77 Exposure 34 C was the critical point at which enzyme activity slowed significantly, and at which significant alteration in platelet activity was seen. Fibrinolysis was not significantly affected at any of the measured temperatures Watts, Dorraine Day, et al. "Hypothermic coagulopathy in trauma: effect of varying levels of hypothermia on enzyme speed, platelet function, and fibrinolytic activity." The Journal of Trauma and Acute Care Surgery 44.5 (1998): Keeping pt warm Warm blood products Bair hugger type devices Warm operating room
78 Monitoring Basic Advanced A line CVP? PPV- FloTrac TEE Labs- CBC, coags, lytes, ABGs POC Hemoque- Hgb istat- lytes/gases ROTEM- coagulation


79 Clotting Dynamics
80 Trauma Associated Coagulopathy Hemorrhage Massive transfusion Hypothermia Acidosis Coagulopathy

81 Lethal Triad Coagulopathy Acidosis Hypothermia
82 More than the Lethal Trial Hess JR, Brohi K, Dutton RP; et al. The coagulopathy of trauma: a review of mechanisms, J Trauma
83 Early Management: Anesthesia 1. Supportive fluid resuscitation: Avoid acute exsanguination Minimize risk of organ system failure Facilitate hemostasis 2. Preservation of homeostasis: Temperature Pulmonary function
84 Adjuncts to Hemostasis Damage control Failure of standard methods Hypothermia and coagulopathy Acidosis and metabolic abnormalities Principles of damage control Obtain surgical hemostasis Temporize hollow viscus injury Pack coagulopathic bleeding Resuscitate and correct hypothermia
85 Damage Control Surgery (DCS) To minimize the occurrence of: Bleeding begets volume resuscitation begets more bleeding begets lethal triad begets death; Damage Control has emerged Acidosis Hypothermia Coagulopathy DCS avoids extensive procedures on unstable patients, stabilizes potentially lethal problems at initial operation, and applies staged surgery after successful initial resuscitation (Cirocchi R., et al. (2010) Damage control surgery for abdominal trauma. Cochrane database of systematic reviews. Issue 1
86 Dutton, RP. Damage Control Anesthesia. Trauma Care. 2005;15:
87
88
89 Damage Control Resuscitation In severely injured casualties DCR consists of 2 parts and is initiated within minutes of facility arrival Resuscitate to keep SBP approx 90 mm Hg (to prevent rebleeding from any recently clotted vessels) Intravascular volume restoration using a 1:1 or 1:2 ratio of FFP to PRBCs (minimize dilutional coagulopathy) It is critical that major sources of blleding are addressed visa a vie Damage Control Surgery concepts Holcomb JB., et al. (2007) Damage control resuscitation: Directly addressing the early coagulopathy of trauma. J Trauma
90 Resuscitation Strategies Ratio based resuscitation RBC:FFP:PLTs (currently 1:1:1) Ongoing studies will help guide this concept Laboratory based resuscitation Lab delays Lost samples Point of Care Coagulation con centrates ROTEM
91 Component Therapy Dutton, R. P. (2012), Resuscitative strategies to maintain homeostasis during damage control surgery. Br J Surg, 99: doi: /bjs.7731
92 Dilution Is Inevitable When Giving Blood Components Whole blood 500 ml Hct 38% 50% Plts 150 K 400 K Plasma coagulation factors = 100% Components 1 U PRBC = 335 ml with Hct 55% 1 U Plts = 50 ml with 5.5 x Plts 1 U plasma = 275 ml with 80% coagulation activity Thus: 1 U PRBC + 1 U Plts + 1 U FFP = 660 ml with Hct 29%, Plts 88 K/µL, and coagulation activity 65%. FFP, fresh frozen plasma; Hct, hematocrit; PRBC, packed red blood cells.
93 Avoid the 5 H s hypoxia, hyoventilation, hypovolemia, hypotension, hypothermia. Always practice universal precautions. Intubate/protect the airway early with CHI, airway trauma(blunt/penetrating, burns). Remain suspicious(was anything missed?) Do not forget the family/significant others (keep them informed and help them get support).
94 Always use the largest and shortest bore IV catheter possible(secure it well however, under pressure and poorly secured it might work its way out).one line is rarely enough. A urinary catheter is a standard monitor for volume resuscitation (hematuria can be one of the most confirming signs of a transfusion reaction under general anesthesia).
95 Alert the Blood Bank early if a massive resuscitation is expected. An extra pair or two of hands makes the resuscitation process much easier. Consider cell salvage (if appropriate) and don t forget to request a perfusionist and a Rapid infusion system (RIS) or an FMS 2000 or a level 1 system (you must warm the blood products).
96 Track patient perfusion by sending ABG s and periodic Lactate levels. Track homeostasis by monitoring CBC s, coags (TEG) and electrolytes. Track ionized calcium levels. Urine output can aid in assessment. Note for respiratory variation in pulse ox and arterial waveforms. If arterial pressure monitoring is employed, make sure the connection is tight and the pressure bag for flush has adequate flow.
97 Don t loose track of fluids administered. Stack bags on the floor, and fill out those blood product slips (after the case is over is better than not at all). Universal precautions for all-(gloves, mask, and eye protection are mandatory). Keep track of blood loss-watch for phantom suction. Cell save as much as possible.
98 Combat hypothermia. Utilize Forced Air Warming Devices, Fluid Warmers, and warm the environment as much as possible. Cover all portions of body possible during surgery). Try not to fall too far behind with your resuscitation efforts. The surgeons can help by quickly repairing bleeders, and if all else fails pack the wound or clamp vessels and get ready to go off to Angio (damage control surgery).
99 A retrospective study looked at 3,286 trauma patient and found that: Reactive thrombocytosis is a common finding in trauma patient in the ICU It was associated with more severally injured patients and produced a higher rate of DVTs/ PEs However, patients with higher platelet counts had significantly lower mortality rates and longer ICU and hospital stays than patients who did not have thrombocytosis Salim A., et al. (2009) What is the significance of thrombocytosis in patients with trauma? J Trauma. 66(5)
100 The C-spine is never initially clear. The stomach is always full. Altered LOC is caused by a head injury. The patient is always hypovolemic. Partial airway obstruction may progress to complete obstruction. The patient may already be premedicated.
101 Ali H. Mokdad,et.al. (2004). Causes of preventable deaths in the United States. Journal of the American Medical Association, 291(10), Dutton R.P. Fluid management for trauma: Where are we now? (2006). Continuing Education in Anesthesia, Critical Care & Pain 6(4), Smith, C.E.(ed.). (2008). Trauma Anesthesia. NY: Cambridge University Press.
,866-72. Wilson, W.C., Grande, C.M., & Hoyt, D.B. (2007). Trauma emergency resuscitation perioperative anesthesia surgical management.")
102 Stephens CT, Kahntroff S, Dutton RP. (2009). The success of emergency endotracheal intubation in trauma patients: A 10-year experience at a major adult trauma referral center. Anesthesia & Analgesia, 103(3), Wilson, W.C., Grande, C.M., & Hoyt, D.B. (2007). Trauma emergency resuscitation perioperative anesthesia surgical management. New York: Informa Healthcare.
103 Shock is defined physiologically as inadequate delivery of substrates and oxygen to meet the metabolic needs of the tissues. As cells are starved of oxygen and substrate, they can no longer sustain efficient aerobic oxygen production. Aerobic metabolism generates 36 ATP molecules per glucose molecule. As oxygen delivery (DO 2 ) is impaired, the cell must switch to the much less efficient anaerobic metabolic pathway, which generates only 2 ATP molecules per molecule of glucose, with resulting production and accumulation of lactic acid. (Adam J Schwarz, MD Emedicine 2009)
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
1 Chapter 10 Shock 2 Shock Shock: Inadequate State of collapse and failure of the system Leads to inadequate circulation Without adequate blood flow,
 1 Chapter 10 Shock 2 Shock Shock: Inadequate State of collapse and failure of the system Leads to inadequate circulation Without adequate blood flow, cannot get rid of metabolic wastes Results in hypoperfusion
1 Chapter 10 Shock 2 Shock Shock: Inadequate State of collapse and failure of the system Leads to inadequate circulation Without adequate blood flow, cannot get rid of metabolic wastes Results in hypoperfusion
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Introduction (1 of 3)
") Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Shock. Perfusion. The cardiovascular system s circulation of blood and oxygen to all the cells in different tissues and organs of the body
 Shock Chapter 10 Shock State of collapse and failure of the cardiovascular system Leads to inadequate circulation Without adequate blood flow, cells cannot get rid of metabolic wastes The result- hypoperfusion
Shock Chapter 10 Shock State of collapse and failure of the cardiovascular system Leads to inadequate circulation Without adequate blood flow, cells cannot get rid of metabolic wastes The result- hypoperfusion
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Trauma, Shock, Multiple Organ Dysfunction. Class 14 Objectives
 Trauma, Shock, Multiple Organ Dysfunction University of San Francisco Dr. M. Maag 2003 Margaret Maag Class 14 Objectives Upon completion of this lesson, the student will be able to apply the previously
Trauma, Shock, Multiple Organ Dysfunction University of San Francisco Dr. M. Maag 2003 Margaret Maag Class 14 Objectives Upon completion of this lesson, the student will be able to apply the previously
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Circulatory shock. Types, Etiology, Pathophysiology. Physiology of Circulation: The Vessels. 600,000 miles of vessels containing 5-6 liters of blood
 Circulatory shock Types, Etiology, Pathophysiology Blagoi Marinov, MD, PhD Pathophysiology Dept. Physiology of Circulation: The Vessels 600,000 miles of vessels containing 5-6 liters of blood Vessel tone
Circulatory shock Types, Etiology, Pathophysiology Blagoi Marinov, MD, PhD Pathophysiology Dept. Physiology of Circulation: The Vessels 600,000 miles of vessels containing 5-6 liters of blood Vessel tone
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
Where Have we Come From, and Where are we Going
 Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
The Future of EMS as Revealed through Research. A Window into the Near Future
 The Future of EMS as Revealed through Research A Window into the Near Future Raymond L. Fowler, M.D., FACEP Co-Principal Investigator National Institutes of Health Resuscitation Outcomes Consortium --------------------
The Future of EMS as Revealed through Research A Window into the Near Future Raymond L. Fowler, M.D., FACEP Co-Principal Investigator National Institutes of Health Resuscitation Outcomes Consortium --------------------
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Damage Control Resuscitation
 Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Hypotension / Shock. Adult Medical Section Protocols. Protocol 30
 Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
SHOCK. May 12, 2011 Body and Disease
 SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 406 Manage Shock Casualties TERMINAL LEARNING OBJECTIVES 1. Given a casualty in an operational environment,
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 406 Manage Shock Casualties TERMINAL LEARNING OBJECTIVES 1. Given a casualty in an operational environment,
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
anesthesia & mass casualty events
 anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Objectives. Objectives. Shock. Objectives. Cardiac output. Review of Blood Flow and Perfusion. Review the components of perfusion
 Objectives Shock Review the components of perfusion Cardiac output Perfusion at the capillary level Perfusion and cellular metabolism Aerobic metabolism and energy production Objectives Identify the stages
Objectives Shock Review the components of perfusion Cardiac output Perfusion at the capillary level Perfusion and cellular metabolism Aerobic metabolism and energy production Objectives Identify the stages
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 6.1 Define key terms introduced in this chapter. Slides 11, 15, 17, 26, 27, 31, 33, 37, 40 42, 44, 45, 51, 58 6.2 Describe the basic roles and structures
Introduction to Emergency Medical Care 1 OBJECTIVES 6.1 Define key terms introduced in this chapter. Slides 11, 15, 17, 26, 27, 31, 33, 37, 40 42, 44, 45, 51, 58 6.2 Describe the basic roles and structures
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
APPROACH TO TRAUMA CARE
 APPROACH TO TRAUMA CARE Timothy Murray, RN, CFRN Jan 2017 OBJECTIVES Demonstrate Concepts of Primary and Secondary Patient Assessment Establish Management Priorities in Trauma Situations Initiating Interventions
APPROACH TO TRAUMA CARE Timothy Murray, RN, CFRN Jan 2017 OBJECTIVES Demonstrate Concepts of Primary and Secondary Patient Assessment Establish Management Priorities in Trauma Situations Initiating Interventions
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
Chapter Goal. Learning Objectives. Chapter 17. Hemorrhage & Shock
 Chapter 17 Hemorrhage & Shock Chapter Goal Use assessment findings to formulate field impression and implement treatment plan for patient with hemorrhage or shock Learning Objectives Describe epidemiology,
Chapter 17 Hemorrhage & Shock Chapter Goal Use assessment findings to formulate field impression and implement treatment plan for patient with hemorrhage or shock Learning Objectives Describe epidemiology,
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine
 Running on Empty Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine Nationwide id Children s Hospital Associate Professor, Department of Pediatrics The Ohio State
Running on Empty Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine Nationwide id Children s Hospital Associate Professor, Department of Pediatrics The Ohio State