ECG (EKG) Interpretation
|
|
|
- Beatrix Harvey
- 5 years ago
- Views:
Transcription
1 ECG (EKG) Interpretation As with all investigations the most important things are your findings on history, examination and basic observations. Having a good system will avoid making errors. To start with we will cover the basics of the ECG, how it is recorded and the basic physiology. The 12-lead ECG misleadingly only has 10 electrodes (sometimes also called leads but to avoid confusion we will refer to them as electrodes). The leads can be thought of as taking a picture of the heart s electrical activity from 12 different positions using information picked up by the 10 electrodes. These comprise 4 limb electrodes and 6 chest electrodes.
2 Electrode positions on an ECG (EKG).
3 When electrical activity (or depolarisation) travels towards a lead, the deflection is net positive. When the activity travels away from the lead the deflection is net negative. If it is at 90 degrees then the complex is isoelectric i.e. the R and S wave are the same size. This can often be seen in V.

4 The electrical activity on an ECG (EKG).

5 The electrical activity on an ECG (EKG).
6 The areas represented on the ECG are summarized below: V1, V2 = RV V3, V4 = septum V5, V6 = L side of the heart Lead I = L side of the heart Lead II = inferior territory Lead III = inferior territory avf = inferior territory (remember F for feet ) avl = L side of the heart avr = R side of the heart
7 The ECG can be broken down into the individual components. For the purpose of this we will look at lead II. All boxes are based on the assumption that the paper speed is running at 25mm/sec, therefore 1 large square is equivalent to 0.2 secs and a small square to 0.04 secs.

8 The segments of the ECG.
9 What do the segments of the ECG represent? P-wave: Atrial contraction PR interval: Represents the time taken for excitation to spread from the sino-atrial (SA) node across the atrium and down to the ventricular muscle via the bundle of His. QRS: Ventricular contraction ST segment: Ventricular relaxation T-wave: Ventricular repolarisation Normal duration of ECG segments: PR interval: secs (3-5 small squares) QRS: <0.12 secs (3 small squares) QTc: secs
10 How to read an ECG There are many different systems to interpret the ECG. This system ensures you will never miss anything: 1. Patient details 2. Situation details 3. Rate 4. Rhthm 5. Axis 6. P-wave and P-R interval 7. Q-wave and QRS complex 8. ST segment 9. QT interval 10.T-wave These components will now be explained in more detail.
11 1. Patient details Patient s name, date of birth and hospital number Location This becomes important as in the ED or acute medical setting doctors are often shown multiple ECGs. You need to know where your patient is in order to ensure that they can be moved to a higher dependency area if appropriate.
12 2. Situation details When was the ECG done? The time The number of the ECG if it is one of a series If you are concerned that there are dynamic changes in an ECG it is helpful to ask for serial ECGs (usually three ECGs recorded 10 minutes apart) so they can be compared. These should always be labelled 1, 2 and 3. Did the patient have chest pain at the time? Or other relevant clinical details. For example, if you are wanted an ECG to look for changes of hyperkalaemia, note the patient s potassium level on the ECG.
13 3. Measuring the rate on an ECG Rate can be calculated in a number of ways: Count the number of QRSs on one line of the ECG (usually lead II running along the bottom) and multiply by six. Count the number of large squares between R waves and divide 300 by this number (if the patient is in atrial fibrillation it is more accurate to report a rate range rather than a single value).
14 4. Assessing the rhythm on an ECG Is the rhythm regular or irregular? If it is irregular is it regularly or irregularly irregular? Rhythm can be difficult to assess especially in bradycardia or tachycardia. It may be helpful to use the paper test. To do this place a piece of scrap paper over the ECG and mark a dot next to the top of a QRS complex, draw another dot next to the top of the next QRS then slide the paper along the ECG. If the rhythm is regular you should see that your two dots match to the tops of the QRS complexes throughout the ECG.
15 5. Assessing the axis on an ECG Axis is the sum of all the electrical activity in the heart. The contraction travels from the atria to the right and left ventricles. As the left ventricle is larger and more muscular normal axis lies to the left (at -30 degrees to 90 degrees see Figure ). As a general rule if the net deflections in leads I and avf are positive then the axis is normal. If lead I has a net negative deflection whilst avf is positive then there is right axis deviation. If lead I has a positive deflection and avf has a negative deflection then there is left axis deviation
16 If you want to work it out more precisely you can use the method below: Count the number of small squares of positive or negative deflection in avf and make a dot on the avf axis (see Figure 5) moving a mm for each small square counted (e.g. x mm up for negative and x mm down for positive deflections). Count the number of small squares of positive or negative deflection in lead 1 and make a dot on the lead 1 axis moving a mm from the centre of the chart for each small square counted (e.g. x mm right for negative and x mm left for positive deflections). Draw a horizontal line through your lead 1 dot and a vertical line through your avf dot then draw a line from this intersection back through 0 and this will give you the accurate axis.

17 The axis of the heart a useful diagram for assessing the cardiac axis using the method above.
18 Causes of axis deviation Left axis deviation Right axis deviation o Can be normal if the diaphragms o Normal in children or young thin are raised e.g. Ascites, pregnancy adults. o Left ventricular hypertrophy (LVH) o Right ventricular hypertrophy (RVH) o Left anterior hemiblock (see notes o Often due to respiratory disease on heart block) o Pulmonary embolism (PE) o Inferior myocardial infaction o Anterolateral myocardial infarction o Hyperkalaemia o Left posterior hemiblock (rare) o Vertricular tachycardia (VT) o Septal defect o Paced rhythm
19 6. P-wave and PR interval Can you see a p-wave? If the rhythm is atrial fibrillation, atrial flutter or a junctional tachycardia you may not be able to. At this point you can also assess whether each p wave is associated with a QRS complex. P-waves not in association with QRS complexes indicate complete heart block. Assess p-wave morphology In some cases there can be a notched (or bifid) p-wave known as p mitrale, indicative of left atrial hypertrophy which may be caused by mitral stenosis. There may be tall peaked p-waves. This is called p-pulmonale and is indicative of right atrial hypertrophy often secondary to tricuspid stenosis or pulmonary hypertension.
20 A similar picture can be seen in hypokalaemia (known as pseudo p-pulmonale ). The PR interval may be prolonged in first degree heart block (described in more detail later). The PR interval may be shortened when there is rapid conduction via an accessory pathway, for example in Wolff Parkinson White syndrome. PR depression may be seen in pericarditis.
21 7. Assessing Q-wave and QRS complex Q-wave A q-wave is an initial downward deflection in the QRS complex. These are normal in left-sided chest leads (V5, 6, lead I, avl) as they represent septal depolarization from left to right. This is as long as they are <0.04secs long (1 small square) and <2mm deep. If q-waves are larger than this or present in other leads they are pathological.
22 QRS complex Width The QRS complex normally lasts for < 0.12 secs (3 small squares). Causes of a wide QRS: Bundle branch blocks (LBBB or RBBB) Hyperkalaemia Paced rhythm Ventricular pre-excitation (e.g. Wolf Parkinson White) Ventricular rhythm Tricyclic antidepressant (TCA) poisoning
23 Shape and height The QRS may be small (or low voltage) in pericardial effusion, high BMI, emphysema, cardiomyopathy and cardiac amyloid. The QRS is tall in left ventricular hypertrophy (LVH) The criteria suggestive of LVH on the ECG is if the height of the R wave in V6 + the depth of the S wave in V1. If this value is >35mm this is suggestive of LVH. The QRS can also be tall in young, fit people (especially if thin).
24 8. ST segment The ST segment can be normal, elevated or depressed. To be significant the S-T segment must be depressed or elevated by 1 or more millimeters in 2 consecutive limb leads or 2 or more millimeters in 2 consecutive chest leads. Look out for reciprocal changes. ST elevation indicates infarction. ST depression is normally due to ischaemia. ST segment depression may also be seen in digoxin toxicity. Here the ST depression will be downsloping (sometimes known as the reverse tick sign).
25 NB: High-takeoff A mimic of ST elevation is high-takeoff. High-takeoff is also known as benign early repolarization. High-takeoff is where there is widespread concave ST elevation, often with a slurring of the j-point (start of the ST segment). It is most prominent in leads V2-5, is usually in young health people and is benign. The best ways to differentiate it from myocardial infarction are: The ST segments are concave; they are most prominent in V2-5; they have a slurred start (j-point); the ST elevation is usually minimal compared to the amplitude of the t-wave; there are no reciprocal changes; the ST segments do not change over time.
26 9. QT interval The QT interval is the time between the start of the q-wave and the end of the t-wave. The QT interval is corrected for heart rate giving the QTc. As a quick check, if the t-waves occur over half way between the QRS complexes the QTc may be lengthened Not an accurate method but very quick! A long QTc interval (known as long QT ) is especially important to identify in patients with a history of collapse or transient loss of consciousness.
27 Causes of long QT: Drugs Metabolic Familial Other o Tricyclic antidepressan ts (TCAs) o Hypothermia o o o o Terfenadine Erythromycin Amiodarone Phenothiazin es o o o Hypokalaemia Hypocalcaemi a Hypothyroidis m o o o Long QT syndrome Brugada syndrome Arrhythmogenic RV dysplasia o o IHD Myocardi tis o Quinidine
28 10. T-wave The t-wave can be flattened or inverted for a number of reasons: Normal variant Commonly inverted in avr and V1 and often in V2 and V3 in people of afro-caribbean descent. Ischaemia Ventricular hypertrophy (strain pattern) usually in lateral leads LBBB (t-wave inversion in the anterolateral leads) Digoxin Hypokalaemia (can cause flattened t-waves)
29 N.B. Hyperkalaemia causes peaked T waves. The classic changes in hyperkalaemia are: Small p-wave Tall, tented (peaked) t-wave Wide QRS Widening of the QRS indicates severe cardiac toxicity
30 Summary Following steps 1-10 above give the ideal system for interpreting an ECG. If you work through these steps you will be unlikely to miss anything significant.

31 Heart blocks and bundle branch blocks on ECGs (EKGs) In order to understand heart blocks it is important to have an understanding of the conduction system of the heart:
32 Passage of current through the heart The initial signal originates at the sinoatrial node (SAN) It is conducted through the myocardium of the atria and then passes via the atrio ventricular node (AVN) to the bundle of His. This bundle then splits into two bundle branches (left and right) The left bundle further splits into anterior and posterior fascicles (more on that later) Conduction continues through the Purkinjie fibres and finally into the ventricular muscle which contracts in systole which corresponds to the QRS complex Below we discuss what happens when the conduction system is interrupted. The figure below gives an overview but we will look at each block in more detail.
33

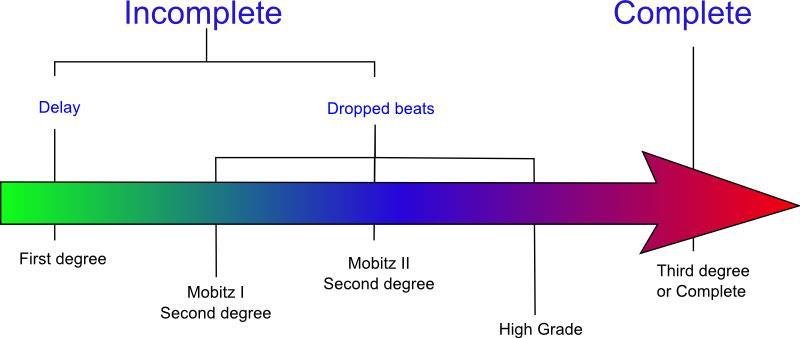
34 1 st degree heart block 1st degree block indicates slowed transmission of electrical activity through the AV node therefore giving a prolonged PR interval. It can be a normal variant.

35 2 nd degree heart block There are two varieties of 2nd degree heart block to be aware of: Mobitz type 1 (Wenckebach) In Wenckebach block The PR interval prolongs from beat to beat and then one beat is not transmitted. This is a normal variant and requires no further investigation or treatment.

36 Mobitz Type 2 In Mobitz type 2 the PR interval is constant. However, there is an occasional non transmitted beat which may also be seen as 2:1 or 3:1 block here there are alternate conducted and non-conducted beats. The above ECG shows 2:1 block with 2 P-waves for every one QRS
37 Significance of type 2 heart blocks Wencheback is a normal variant 2:1 and Mobitz type 2 blocks are pathological; they may precede 3 rd degree or complete heart block
.")
38 3 rd degree heart block (complete heart block) In 3rd degree heart blocks the connections between the atria and the ventricles are completely lost. The atrial rate continues as normal (as seen by regular p-waves). However, the actual heart rate is slow reflecting a ventricular escape rhythm which is generated from a focus within the ventricular muscle its self. Each p-wave is not associated with a QRS complex and the QRS complex is wide reflecting its ventricular origins.
39 Bundle branch blocks (BBBs) Refer back to the figure below as you read about the different blocks:

40 Right bundle branch block (RBBB) RBBB may be a normal variant especially if the pattern is present but with a normal QRS duration. ootherwise it may indicate problems with the right side of the heart. In RBBB you will see wide complexes with a RSR pattern in V1 and deep S wave in V6.
41 How RBBB works From first principles RBBB occurs as left ventricular contraction happens just prior to right ventricular contraction (as the R bundle is not working) where they would normally contract together. Remember that the positive deflection is caused by depolarization travelling towards that lead. Therefore: Initially there is septal depolarization (left to right) causing a small R wave in V1 and Q wave in V6 Then LV contraction causes an S wave in V1 and R wave in V6 Then RV contraction causes an R wave in V1 and a deep S wave in V6

42 Left bundle branch block (LBBB) This is always pathological and relates to left heart disease. If acute it may indicate acute myocardial infarction and is one of the indications for thrombolysis or transfer for PCI. This is one of the situations that illustrates the importance of having access to old ECGs.
43 How LBBB works In LBBB you will see wide complexes with a negative (sometimes W shaped) complex in V1 and an M pattern in V4 -V6 and T wave inversion in the anterolateral leads. The T wave inversion is due to abnormal repolarization (after abnormal depolarization) rather than ischaemia. From first principles: The septum depolarizes from R to L causing a Q wave in V 1 and a R wave in V6 The R ventricular contraction occurs first causing an R wave in V1 and a S wave in V6 Then LV contraction causes an S wave in V1 and a further R wave in V6
44 Causes of bundle branch blocks (BBBs) Right bundle branch block (RBBB) Left bundle branch block (LBBB) o Ischaemic Heart Disease (MI) o Normal in young, tall thin people o Hypertension o Idiopathic o LVH o Right ventricular strain (PE or chronic respiratory disease) o o Aortic valve disease Post aortic valve replacement o Ischaemic Heart Disease o RV pacemaker o Myocarditis o Myocarditis o Cardiomyopathy
45 Fascicular blocks The left bundle can also be split into anterior and posterior fascicles (as shown in the figure above) and block can affect either of these. Anterior fascicular block If the anterior fascicle is blocked the cardiac axis swings round to the left causing left axis deviation. This is known as left anterior hemiblock It is often caused by LVH Posterior fascicular block Uncommonly the left posterior fascicle is exclusively blocked in which case there is right axis deviation. Bifascicular block If the left anterior fascicle (or left posterior fascicle but this is much less common) and the right bundle are blocked you will see both right bundle branch block and left axis deviation, this is known as bifascicular block. This is clinically important as the patient may intermittently go into complete heart block as they are solely relying on the posterior fascicle for ventricular contraction.

46 This ECG shows bifasicular block
47 Trifascicular block If there is bifasicular block with a prolonged pr interval (i.e. first degree block) this is known as trifasicular block as there is block in 2 fasicles and a delay in the 3 rd As with bifasicular block it should be treated urgently as it may deteriorate into complete heart block
48 ECG (EKG) examples and quiz For each of the questions below a short clinical scenario is given followed by the 12-lead ECG. Review the ECG (EKG), present it according to the structure in ECG interpretation and attempt a diagnosis before clicking on the plus symbol to see the answer.

49 Question 1 A 35 year old man presents with palpitations. He has been drinking heavily with friends over the weekend. This is his ECG. Present your findings and give a diagnosis.
50 Answer Presentation: Rate Rhythm Axis PR/P-wave QRS ST/T-wave QTc/other Irregularly irregular Normal No p-wave seen. Fibrillating base line Narrow Normal Normal Diagnosis: This ECG shows atrial fibrillation (AF) with a fast ventricular response. With this history the underlying diagnosis would fit with a holiday heart syndrome.

51 Question 2 A 45 year old business man presents with a feeling that his heart is racing. He also has some shortness of breath. This is his ECG. Present your findings and give a diagnosis.
52 Answer Presentation: Rate 150 Rhythm Axis PR/P-wave QRS Regular Normal No p-waves. Seesaw baseline Narrow QTc/other Normal Diagnosis: This is atrial flutter. The atria contract at 300 beats per minute causing a seesaw baseline. Beats are transmitted with a 2:1, 3:1 or 4:1 block, leading to ventricular rates of 150, 100 and 75 BPM respectively.

53 Question 3 A 75 year old man with a history of COPD presents with fever and increased sputum production. An ECG is taken in the emergency department. What does it show?
54 Answer Presentation: Rate Rhythm Axis PR/P wave QRS ST/T wave QTc/other Irregularly irregular Normal Polymorphic p-waves (see arrows) Narrow Normal Normal Diagnosis: This is polymorphic atrial tachycardia. It occurs in respiratory disease and reflects an aberrant foci of atrial excitation. The morphology of the p-waves is therefore variable but all p-waves are transmitted via the bundle of His and therefore the QRS complexes are all the same.

55 Question 4 A 65 year old man is found unresponsive. He has no central pulse and is making no respiratory effort. Surprisingly someone has done an ECG. What would you do?
56 Answer We will not go through the ECG as the most important information is in the clinical history. This is pulseless electrical activity (PEA). It is the most extreme example of why you should look at the patient in conjunction with the ECG! There are no specific ECG changes in PEA the most important thing is to recognize that this patient is in cardiac arrest and to start chest compressions and Advanced Life Support (ALS) immediately. However, the ECG may help you ascertain the underlying pathology. In this case there are low voltage QRS complexes which may simply due to large body habitus or could indicate pathology interrupting the signal between the heart and the electrode. This can include pericardial fluid or pneumothorax. This is worth thinking about as tamponade and tension pneumothorax are both reversible causes of PEA.

57 Question 5 A fit and well 31 year old man presents for a routine insurance medical. This is his ECG. Present your findings and give the diagnosis.
58 Answer Presentation: Rate 85 Rhythm Axis PR/P-wave QRS ST/T-wave QTc/other Regular Normal Normal Narrow Normal Normal Diagnosis: This is a normal ECG. There are many variants of normal and it is worth looking at as many ECGs as possible to get exposed to the common variants. It is crucial to remember that a very sick patient can have a normal ECG so always use all the information available to you and don t rely on the ECG alone.

59 Question 6 A 65 year old man with a history of ischaemic heart disease is found unresponsive. He has no central pulse and is making no respiratory effort. This is his ECG. What is the diagnosis and what will you do?
60 Answer Presentation: Rate 150 Rhythm Axis PR/P wave QRS ST/T wave Regular Left axis deviation Not visible Wide Unable to assess QTc/other Unable to assess Diagnosis: This is ventricular tachycardia (VT) and in this case the patient is in cardiac arrest as they have no central pulse. He should be treated as per ALS guidelines with chest compressions beginning immediately. This is a shockable rhythm and should be treated using the ALS algorithm with DC cardioversion and adrenaline. If the patient was conscious the ALS algorithm would not be necessary and management depends on symptoms. If acutely symptomatic urgent DC cardioversion is indicated. If there were no symptoms of decompensation (e.g. shortness of breath, chest pain, shock, confusion, syncope) he could be managed pharmaceutically in the first instance.

61 Question 7 A 40 year old lady comes to the emergency department from her husband s funeral with a sensation of fluttering in her chest. She is feeling very anxious. An ECG is performed. What is the diagnosis?
62 Answer Presentation: Rate 160 Rhythm Axis PR/P wave QRS ST/T wave Regular Normal Not visible Narrow Slight lateral ST depression QTc/other Normal Diagnosis: The history makes a sinus tachycardia secondary to anxiety seem likely. However, sinus rhythm rarely goes above 120 BPM and in this case there are no p-waves visible. This is therefore a junctional supraventricular tachycardia (SVT): a narrow-complex tachycardia originating from the AV node. Treatment includes vagal manoeuvres followed by adenosine. Atrial flutter would be a reasonable differential as the rate is regular and close to 150. However, there is no variation in the baseline and not a hint of sawtooth appearance so this is less likely than SVT.

63 Question 8 A 58 year old man who attends the emergency department with chest pain loses consciousness whilst he is having his initial ECG. He has no central pulse and is taking occasional deep breaths. What is going on?
64 Answer Presentation: Rate Initially 100, then 300 Rhythm PR/P wave QRS ST/T wave QTc/other Initially regular, then irregular Initially present, then unable to visualise Initially narrow, then wide Initially massive ST elevation in II III and avf with reciprocal depression in I and avl. Then unable to visualise Unable to assess Diagnosis: This is ECG initially shows an inferior STEMI, which then deteriorates into ventricular fibrillation (VF). The breaths described are agonal breaths this does not represent normal respiratory effort and resuscitation for cardiac arrest with CPR should be started immediately. Remember: in collapse with abnormal breathing and no central pulse always start CPR.

65 Question 9 A 72 year old lady presents with collapse. This is her ECG. Present your findings. How would you proceed?
66 Answer Presentation: Rate Rhythm Axis PR/P wave QRS ST/T wave 50 bpm Regular Normal Normal Narrow Normal QTc/other Normal Diagnosis: This is sinus bradycardia. In a young fit person this rate may be normal. However, in the context of a more elderly person and presenting with collapse it should be further investigated. A medication review, blood tests including thyroid function, repeat ECGs, chest x-ray, echocardiogram and 24-hour tape would be reasonable first-line investigations.

67 Question 10 A 60 year old man presents with tight central chest pain radiating to his left shoulder. This is his initial ECG. Present your findings and give a diagnosis.
68 Answer Presentation: Rate 90 Rhythm Axis PR/P wave QRS ST/T wave Regular Normal Normal Narrow Grossly elevated in V2, V3, V4, V5 and V6. Reciprocal depression in II, III and avf. QTc/other Normal Diagnosis: This patient has ST elevation in the anterior and lateral leads. This is therefore an anterolateral ST elevation MI (STEMI). This dramatic ST elevation is also referred to as tombstone ST elevation, both for its resemblance to a tombstone and as a reflection on the poor prognosis without rapid intervention. What would you do? This patient should be assessed and treated urgently for a STEMI, ideally with primary angioplasty (primary coronary intervention: PCI). Immediate management also includes aspirin, clopidogrel, heparin, nitrites, morphine and controlled oxygen.

69 Question 11 A 55 year old renal dialysis patient presents to the emergency department having missed his last session of dialysis due to feeling dizzy and unwell. This is his ECG. Present your findings and give a diagnosis.
70 Answer Presentation: Rate Rhythm Axis PR/P wave QRS ST/T wave Irregular Unable to establish Not visible Widened Merged with QRS QTc/other Unable to assess Diagnosis: This is the classic sine wave ECG pattern of severe hyperkalaemia. It can quickly deteriorate into ventricular fibrillation (VF). There are three main ECG changes in hyperkalaemia: 1. In the early stages of you may only see tenting or peaking of the t-waves. 2. Later changes involve a decrease in height of the p-wave and increase in length of the PR interval as conduction is slowed through the atrial myocardium. 3. This is later accompanied by widening of the QRS and merging of the QRS complex and the t-wave. This pattern eventually deteriorates to the sine wave pattern seen above.
71 What would you do? This is a medical emergency. Treatment is with 10ml 10% calcium gluconate for cardioprotection, followed by 10 units of fast acting insulin (with 50ml 50% dextrose) to drive potassium into the intracellular space. Inhaled salbutamol has a similar effect if there is no IV access. Bicarbonate 50ml IV can also be given. Ultimately total body potassium needs to be decreased in this case urgent dialysis or haemofiltration is indicated.

72 Question 12 A 65 year old woman presents with chest pain radiating to her jaw and down her left arm. It feels like her normal angina but on this occasion it has not eased with GTN spray. This is her ECG. Present your findings and give the diagnosis.
73 Answer Presentation: Rate 60 Rhythm Axis PR/P wave QRS ST/T wave Normal Normal Normal Normal T wave inverted in II III and avf, V4 V5. ST elevation in avr>1mm QTc/other Normal Diagnosis: On initial inspection this looks like an inferolateral NSTEMI. There is (we assume new) t-wave inversion in consecutive leads which fit with an anatomical territory (inferolateral) and most importantly there is ongoing ischaemic sounding chest pain not eased by GTN. However, note the ST elevation in avr. As such, this is more suggestive of critical left main stem occlusion. This ECG should therefore be discussed with cardiology with a view to urgent PCI.

74 Question 13 A 25 year old man presents with a collapse which occurred as he was playing in a football match. He has suffered episodes of fainting in the past. This is his ECG. What is the diagnosis?
75 Answer Presentation: Rate 60 Rhythm Axis PR/P wave QRS ST/T wave Regular Normal Shortened PR interval Slurred upstroke on QRS Normal QTc/other Normal Diagnosis: This picture of shortened PR interval and slurred QRS upstroke also know as a delta wave are typical of Wolff-Parkinson White (WPW) syndrome. These changes represent transmission through an accessory pathway. The history of collapse in this case is concerning as these episodes could be due to re-entrant tachycardias which can be fatal. Other features not seen here which may be present in WPW include a dominant R wave in V1 and T wave inversion in the anterior chest leads.

76 A further example to illustrate the delta wave is shown below:

77 Question 14 An 18 year old man signs up to join the army. He is fit and well. This is his ECG taken at his medical examination. Is it normal?
78 Answer Presentation: Rate 60 Rhythm Axis PR/P wave QRS ST/T wave Regular Normal Prolonged PR interval Wide in the inferior lateral leads Abnormal in V1, V2 and V3 with unusuallyshaped coved ST elevation QTc/other Normal Diagnosis: No it is certainly not normal. This ECG is characteristic of Brugada Syndrome (Type 1). In leads V1 V3 there is >2mm ST elevation, the T waves are inverted and the ST segment has a characteristic coved shape. This condition has a high risk of sudden death from ventricular fibrillation (VF). Treatment is with an implantable cardioverterdefibillator (ICD).

79 Question 15 A 58 year old smoker presents with tight epigastric pain. He looks sweaty and unwell. One of the nurses shows you his routine ECG. What is the diagnosis?
80 Answer Presentation: Rate 45 Rhythm Axis QRS ST/T wave Regular Normal Narrow Dramatic ST depression in V1 V3 Diagnosis: This is acute posterior MI. What we see in the anterior leads is the equivalent of upside down ST elevation. Imagine flipping the ECG paper over and looking at it from behind or looking at the ECG in a mirror held along the inferior border. You would see ST elevation (the deep ST depression reversed), t-wave inversion (upright t-waves seen upside down) and this represents what is going on in the posterior region of the heart. Another clue is the bradycardia seen in this case: the vessels supplying the posterior of the heart also supply the pacemaker region of the SA node.

81 Question 16 A 29 year old presents with central chest pain. She has a history of recent flu-like illness but no significant past medical history. This is her ECG. What is the diagnosis?
82 Answer Presentation: Rate 60 Rhythm Axis PR/P wave QRS ST/T wave QTc/other Regular Normal PR segment depression Narrow Widespread ST elevation (saddle shaped) Normal Diagnosis: The diagnosis is pericarditis. Pericarditis often presents in young people after a history of viral illness. He you can see the characteristic widespread saddle-shaped ST elevation and PR depression.

83 Question 17 A 70 year old woman presents with sudden onset of chest pain. The pain is crushing in nature and radiates up to her jaw. This is her ECG. Present your findings and give the diagnosis.
84 Answer Presentation: Rate 100 Rhythm Axis PR/P wave QRS ST/T wave QTc/other Regular Normal Every p-wave followed by a QRS Narrow ST elevation in II III and avf Normal Diagnosis: This ECG shows ST elevation in the inferior region of the heart. This patient should be assessed and treated urgently for a STEMI, ideally with primary angioplasty. Immediate management also includes aspirin, clopidogrel, heparin, nitrites, morphine and controlled oxygen.

85 Question 18 A 45 woman has just stepped off a flight from Japan when she develops severe pleuritic chest pain and shortness of breath. On examination her chest is clear. Present your findings. What is the most likely diagnosis?
86 Answer Presentation: Rate 100 Rhythm Axis PR/P wave QRS ST/T wave Regular Right axis deviation Normal Wide right bundle branch block (RBBB) T wave inversion in lead III QTc/other Normal Diagnosis: Given the history, examination and ECG findings, pulmonary embolism (PE) is the most likely diagnosis. In PE the constellation of ECG findings of S1Q3T3 is classically described. It refers to a deep S wave in lead I, pathological Q wave in lead III and inverted T in V3 (and other anterior leads). However, though it may be classical it is extremely rare in clinical practice! The most commonly observed ECG abnormality in PE is a sinus tachycardia. There may also be RBBB or a RV strain pattern with T wave inversion in V1 to V4.

87 Question 19 It is early January and a middle-aged man is found lying in a park. He is surrounded by bottles of Buckfast and has a GCS of 9. An ECG is performed in the ambulance. What is going on?
88 Answer Presentation: Rate 50 Rhythm Axis PR/P wave QRS ST/T wave Regular Normal Normal Narrow Normal QTc/other J wave visible after the QRS Diagnosis: This patient is hypothermic. The positive deflection after the QRS but before the t-wave is an Osbourne J-wave; these can also be seen in subarachnoid haemorrhage (SAH) and hypercalcaemia. Classically a hypothermic patient is bradycardic and their ECG will show J-waves. Treatment in this case would be with gentle rewarming provided there was no immediate risk to life from an arrhythmia.

89 Question 20 A 61 year old woman presents to the emergency department with diarrhoea and vomiting. She has recently been started on furosemide by her GP for hypertension. What has happened?
90 Answer Presentation: Rate 85 Rhythm Axis PR/P wave QRS ST/T wave QTc/other Regular Left axis (may be normal) Normal Narrow Normal Prolonged QTc Diagnosis: This ECG shows changes consistent with hypokalaemia. This has likely be precipitated by the new loop diuretic. Note also that furosemide is not a first-line treatment for hypertension. Classically hypokalaemia causes t-wave flattening with ST depression. In severe cases you may see a U-wave. This is a positive deflection following the t-wave but preceding the p- wave. These are found in hypokalaemia but also in hypercalcaemia and thyrotoxicosis.

91 Question 21 An 18 year old lady is found collapsed at home. When you see her she has a GCS of 10 and you notice that her pupils are dilated. This is her ECG. Present your findings and give the diagnosis.
92 Answer Presentation: Rate 85 Rhythm PR/P wave QRS ST/T wave QTc/other Regular Unable to assess Wide Wide Prolonged Diagnosis: The diagnosis is tricyclic antidepressant overdose. This causes widening of the QRS complex and lengthening of the QT interval due to blockade of sodium channels
93 [/toggle_item] [toggle_item title= What would you do? active= false ] A,B,C,D,E (ventilation may be required) Bloods including paracetamol level; ABG (likely metabolic acidosis) Activated charcoal if within 8hrs of ingestion Sodium bicarbonate (50ml of 8.4%) Give if any arrhythmia or QRS>110 Further options: If ventricular tachycardia: lignocaine (avoid beta blockers, amiodarone and calcium blockers) If seizures: benzodiazepines

94 Question 22 A 45 year old man is found collapsed at home. There is no history available. This is his ECG. What is the diagnosis?
95 Answer Presentation: Rate Rhythm Axis PR/P wave QRS ST/T wave QTc/other Highly variable up to 300 bpm Irregular Unable to assess Absent during episodes of extreme tachycardia Wide Unable to assess Unable to assess Diagnosis: This is a difficult case and shows runs of polymorphic VT or Torsades de pointes (literally translated as twisting of the points). It has a number of causes including medications (especially psychotropics) and electrolyte imbalance. Essentially any cause of long QT can precipitate polymorphic VT. Management in the first instance is magnesium 2g IV, independent of serum magnesium concentration before treating any other cause of long QT.

96 Question 23 A 50 year old man presents with collapse. He has been unwell recently with a chest infection for which he has been prescribed clarithromycin from his GP. He also takes medication for his hayfever at this time of year. What is most concerning here?
97 Answer Presentation: Rate 60 Rhythm Axis PR/P wave QRS ST/T wave Regular Normal Normal Narrow Normal QTc/other Prolonged QT interval Diagnosis: This patient has a prolonged QT interval and a cause for this should be sought. Medications are the likely culprits in this case: both clarithromycin and the antihistamine diphenhydramine can cause prolonged QT interval. The normal length of the QT varies with heart rate and there is a formula that is applied to correct for this. ECG machines automatically provide you with this corrected QT (QTc). Normal QTc is generally under 480ms. As a rule of thumb, if the end of the QT interval is over over half way to the next QRS then consider long QT.
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
a lecture series by SWESEMJR
 Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
Ben Taylor, PhD, PA-C
 Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants
 Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
PATIENT S NAME, DATE/TIME,
 ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG
ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1
 usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1") If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Electrocardiogram ECG. Hilal Al Saffar FRCP FACC College of medicine,baghdad University
 Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
3/4/2018. March Martina Frost, PA C Desert Cardiology. Electricity moving towards/away from electrode create downward/upward directions of waves
 March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
This presentation will deal with the basics of ECG description as well as the physiological basics of
 Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG Interpretation. Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction
 * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction") ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
A few new tools for better detection and understanding of STEMIs in the field.
 A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
, David Stultz, MD.
 http://www.dilbert.com EKG Rounds Handouts available at http://www.drstultz.com January 5, 2004 David Stultz, MD Cardiology Fellow, PGY 4 Overview of Topics How to read an EKG Normal EKG Determination
http://www.dilbert.com EKG Rounds Handouts available at http://www.drstultz.com January 5, 2004 David Stultz, MD Cardiology Fellow, PGY 4 Overview of Topics How to read an EKG Normal EKG Determination
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
also aid the clinician in recognizing both the obvious and subtle abnormalities that may help guide therapy.
 Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
ECG (MCQs) In the fundamental rules of the ECG all the following are right EXCEP:
 In the fundamental rules of the ECG all the following are right EXCEP:") ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
The ECG in healthy people
 The ECG in healthy people The normal cardiac rhythm 3 The heart rate 3 Extrasystoles 7 The P wave 7 The PR interval The QRS complex 3 The ST segment 29 The T wave 33 The QT interval 42 The ECG in athletes
The ECG in healthy people The normal cardiac rhythm 3 The heart rate 3 Extrasystoles 7 The P wave 7 The PR interval The QRS complex 3 The ST segment 29 The T wave 33 The QT interval 42 The ECG in athletes
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
2/7/ LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
 12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Case 1. Case 2. Case 3
 Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C. For more presentations
 ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
12 Lead EKG. The Basics
 12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
Lab Activity 24 EKG. Portland Community College BI 232
 Lab Activity 24 EKG Reference: Dubin, Dale. Rapid Interpretation of EKG s. 6 th edition. Tampa: Cover Publishing Company, 2000. Portland Community College BI 232 Graph Paper 1 second equals 25 little boxes
Lab Activity 24 EKG Reference: Dubin, Dale. Rapid Interpretation of EKG s. 6 th edition. Tampa: Cover Publishing Company, 2000. Portland Community College BI 232 Graph Paper 1 second equals 25 little boxes
Update on Palpitations and AF February 28 th 2018
 Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Pathologic ECG. Adelina Vlad, MD PhD
 Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
ECG Practice Strips Discussion part 1:
 ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
6/19/2018. Background Athlete s heart. Ultimate question. Applying the International Criteria for ECG
 Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON