Liver, Pancreas and Biliary System. Wirana Angthong, M.D.
|
|
|
- Egbert Kelley
- 6 years ago
- Views:
Transcription




1 Liver, Pancreas and Biliary System Wirana Angthong, M.D.
2 Objectives
3 Outline Anatomy Imaging Techniques Common Diseases
4 Outline Anatomy Imaging Techniques Common Diseases

5 Liver anatomy Morphological anatomy: 3 lobes Right lobe Median fissure Middle hepatic vein Left lobe Caudate lobe Ligamentum venosum



6 Liver anatomy RL LL




7 Liver anatomy LL RL



8 Caudate lobe C C


9 Hepatic vasculature Portal V Splenic V IMV SMV

10 Pancreas anatomy H N B T





11 Pancreas anatomy

12 Pancreas anatomy


13 Pancreas anatomy



14 Biliary system anatomy
15 Outline Anatomy Imaging Techniques Common Diseases Plain film radiograph Ultrasonography Computed tomography Magnetic resonance imaging ERCP Endoscopic retrograde cholangiography
16 Outline Anatomy Imaging Techniques Common Diseases Plain film radiograph Ultrasonography Computed tomography Magnetic resonance imaging ERCP Endoscopic retrograde cholangiography



17 Plain film radiograph Air Fat Soft tissue Calcification Metallic Organomegaly Abnormal air Abnormal calcification Foreign bodies
18 Plain film radiograph Low sensitivity, low specificity Radiation Pregnancy
19 Outline Anatomy Imaging Techniques Common Diseases Plain film radiograph Ultrasonography Computed tomography Magnetic resonance imaging ERCP Endoscopic retrograde cholangiography



20 Ultrasonography Convex probe: 2-6 MHz Abdomen Pelvis Linear probe: 7-12 MHz Breast Thyroid Testis
21 Ultrasonography Preparation Upper abdomen Lower abdomen Fasting 4-6 hr Whole abdomen = upper + lower
22 Ultrasonography Preparation Upper abdomen Lower abdomen No fasting But full bladder Whole abdomen = upper + lower
23 Ultrasonography Preparation Upper abdomen Lower abdomen Whole abdomen = upper + lower



24 Ultrasonography



25 Ultrasonography



26 Ultrasonography



27 Ultrasonography
28 Ultrasonography Indication RUQ mass Abnormal liver function test Abdominal pain Jaundice Abnormal vascular structures Abdominal trauma
29 Ultrasonography Indication Search for liver metastasis Search for occult primary neoplasm Guidance for biopsy/ drainage procedure Treatment follow-up
30 Ultrasonography No radiation No intravenous contrast media administration Portable obesity Gas Operator dependent Distal common bile duct: difficult to evaluate





31 Ultrasonography
 High resolution")


32 Endoscopic Ultrasound (EUS) High resolution because of proximity of pancreas to the probe Utility: Diagnosis small tumors, and for which a biopsy is needed.
33 Outline Anatomy Imaging Techniques Common Diseases Plain film radiograph Ultrasonography Computed tomography Magnetic resonance imaging ERCP Endoscopic retrograde cholangiography

34 Computed tomography











35 Computed tomography
36 Computed tomography Contrast agent: iodine based contrast media Preparation Fasting 4-6 hr History allergy, asthma, renal insufficiency Indication Mass Infiltrative disease Abdominal pain Abnormal calcification
37 Computed tomography Indication Biliary tract obstruction Abnormal vascular structure Abdominal trauma Tumor staging, treatment planning Treatment follow-up
38 Computed tomography Fast Multiplanar imaging High sensitive to detection of calcification and gas Radiation Risk of contrast allergy Risk in patient with renal insufficiency Pregnancy

39 Multiphase or Dynamic contrast enhanced CT scan Intravenous contrast: marker for where blood travels in tissue Intravascular space Extracellular interstitial space
40 Multiphase or Dynamic contrast enhanced CT scan Intravenous contrast: marker for where blood travels in tissue Disease alter blood flow to affected tissues Contrast enhancement: character of disease character of underlying organ

41 Multiphase or Dynamic contrast enhanced CT scan Alter in blood flow characteristic can be imaged by different times following contrast media Multiphase or dynamic contrast enhanced CT scan Liver: dual blood supply
42 Phase of hepatic contrast enhancement Contrast enhancement (HU) Aorta PV Liver 15-30s Arterial P 60-70s Portovenous P Time (s)
43 Liver protocol Noncontrast study Arterial phase study Porto-venous phase study




44 Liver protocol Noncontrast study Calcification, hemorrhage, iron deposit Determination of precontrast attenuation Arterial phase study Porto-venous phase study




45 Liver protocol Noncontrast study Arterial phase study s Hypervascular masses: HCC, hemangioma, hypervascular metastasis Porto-venous phase study




46 Liver protocol Noncontrast study Arterial phase study Porto-venous phase study s Hypovascular masses Intrahepatic duct dilation





47 CT: liver mass Hypervascular mass in cirrhosis: HCC Multiple hypovascular masses: metastases
48 Outline Anatomy Imaging Techniques Common Diseases Plain film radiograph Ultrasonography Computed tomography Magnetic resonance imaging






49 MRI upper abdomen with MRCP MRI upper abdomen: pre and postcontrast MRCP Magnetic Resonance Cholangiopancreatography
50 MRI Contrast agent: Gadolinium based contrast agent Preparation Fasting 4-6 hr Remove all metallic objects History: contraindication for Gadolinium Severe renal insufficiency, acute renal failure, Pregnancy




51 GBCA in Severe Renal Insufficiency and AKI Stratta P et al. Rheumatology 2010;49:
 but predominantly skin Relatively spares the face and neck unlike systemic sclerosis Strongly correlated with exposure to GBCAs Usually manifests within")

52 Nephrogenic systemic fibrosis (NSF) Systemic disorder characterized by widespread tissue fibrosis, affects many organs (lungs, heart, MSK etc.) but predominantly skin Relatively spares the face and neck unlike systemic sclerosis Strongly correlated with exposure to GBCAs Usually manifests within 2-10 wks of exposure Diagnosis: Clinical presentation in the setting of severe renal insufficiency ( GFR < 30) + Confirmatory cutaneous histopathological findings. Shellock FG et al. AJR 2008;191: Cowper SE et al. Lancet 2000; 356: Daram SR et al. Am J Kidney Dis 2005; 46: Kuo PH et al. Radiology 2007; 242:
53 Causes and Associations GBCAs administrations: Stability: Linear < Macrocyclic Non-ionic < Ionic High-dose and multiple exposure Most unconfounded cases: Gadodiamide (Omniscan) Gadopentetate (Magnevist) Gadoversetamide (Optimark) Chronic kidney disease Stage 4 Severe CKD GFR Stage 5 End-stage CKD GFR < 15 (or dialysis) Acute kidney injury of any severity Hepatic sufficiency/ Hepatorenal syndrome Vascular injury, venous thrombosis* * Fuluru K Radiographics 2009 ACR 2013 Manual Version 9 Kaewalia AJR 2012;199:17-23
54 Recommendation Who should we screen to identify at risk patients? Serum Cr NOT necessary in all patients egfr is recommended for following patients Within 6 weeks of the MRI study Patient > 60 History of renal disease including Dialysis Kidney transplant, kidney surgery Single kidney History of know cancer involving kidneys History of HT requiring medical therapy History of DM ACR 2013 Manual Version 9 Kaewalia AJR 2012;199:17-23
55 MRI Indication Biliary tract stone: MRCP Tumor staging, treatment planning Treatment follow-up CT contrast media ERCP ERCP
56 MRI No radiation Multiplanar imaging Superior soft tissue contrast: better detection, characterization Safer contrast agent than CT: much lessor associated with nephrotoxicity and allergic reaction Expensive Not widely available Longer acquisition time




57 MR superior soft tissue contrast
58 MRI Cardiac pacemaker Foreign body Metallic clip: ferromagnetic aneurysm clip Cochlear implant Avoiding in first trimester pregnancy (teratogenic effect)
59 Outline Anatomy Imaging Techniques Common Diseases Plain film radiograph Ultrasonography Computed tomography Magnetic resonance imaging ERCP Endoscopic retrograde cholangiography
 Luminal")
 + Pancreatogram")
60 ERCP (Endoscopic retrograde cholangiopancreatography) Luminal endoscopy and fluoroscopic imaging Cholangiogram (CBD) + Pancreatogram (pancreatic duct)
61 ERCP (Endoscopic retrograde cholangiopancreatography) Diagnose and treat conditions associated with pancreatobiliary system Indication Inconclusive ultrasound, CT or MRI/ MRCP findings Therapeutic procedure: stone removal, treatment bile duct stricture and biopsy Acute pancreatitis
62 Outline Anatomy Imaging Techniques Common Diseases
63 Common disease Hepatomegaly Liver cirrhosis and portal hypertension Liver abscess Gallstone and bile duct stone Biliary tract obstruction Acute cholecystitis Acute and chronic pancreatitis




64 Hepatomegaly > 15.5 cm

65 Liver cirrhosis


66 Liver cirrhosis Irreversible remodeling of hepatic architecture with fibrosis and hepatic nodules Most are regenerative nodule (RN): localized proliferation of hepatocytes and supporting stroma in response to liver injury (stimuli, alter circulation)
67 Liver cirrhosis Role of imaging Evaluate liver size Evaluate portal hypertension Screening hepatocellular carcinoma (HCC)





68 Liver cirrhosis

69 Portal hypertension Increased portal flow Increase resistant to portal flow Prehepatic portal hypertension Portal vein thrombosis Splenic vein, SMV, IMV thrombosis Intrahepatic portal hypertension Liver cirrhosis Hepatic vein thrombosis Posthepatic portal hypertension IVC thrombosis Cardiac disease: constrictive pericarditis


70 Portal hypertension


71 Portal hypertension
72 Portal hypertension Collateral circulation or portosystemic circulation Coronary vein or gastric vein esophageal vein azygos/ hemiazygos vein gastroesophageal varices Recanalization of paraumbilical vein caput medusae Inferior mesenteric vein internal iliac vein hemorrhoidal venous plexus internal hemorrhoid






73 Portal hypertension
74 Portal hypertension Plain film Ascites Splenomegaly


75 Portal hypertension Plain film Ascites Loss of definition of edge of liver/ spleen Medial displacement of solid organ and bowel loops away from properitoneal fat stripe Separation of bowel loops Centrally located bowel loops Bulging of the flank Increased density of abdomen Fluid accumulation in pelvis Splenomegaly

76 Portal hypertension Plain film Ascites Splenomegaly Tip of spleen extends below rib 12 th Displacement of splenic flexure of colon or displacement of stomach medially




77 Portal hypertension US Enlargement portal vein > 13 mm Hepatofugal blood flow Ascites Splenomegaly Portosystemic circulation: varices Normal: Hepatopedal Hepatofugal



78 Portal hypertension CT Liver cirrhosis Ascites Enlarged portal vein > 13 vein Portosystemic circulation

79 Liver abscess Hepatic pyogenic abscess Bacterial infection: E coli, K pneumoniae Hepatic amebic abscess Entamoeba histolytica Hepatic fungal abscess Candida albicans
80 Pyogenic abscess 5 Routes: Biliary route: Ascending cholangitis Portal route: Intra-abdominal infection (diverticulitis, appendicitis) Hepatic artery route: Septicemia from bacterial endocarditis Direct extension from adjacent organ Trauma: Blunt, penetrating injury

81 Pyogenic abscess Plain film Elevation of right hemidiaphragm Right pleural effusion Hepatomegaly Gas, air-fluid level




82 Pyogenic abscess US Nonspecific Cannot distinguish from other hepatic mass (HCC, metastasis)




83 Pyogenic abscess CT and MR Hypodensity mass Smooth rim enhancement Cluster Gas or air-fluid level

84 Hepatic amebic abscess Route: portal system Usually solitary


85 Fungal abscess Immunocompromised host Hematologic malignancy Candida, Aspergillus, Cryptococcus
86 Gallstone Cholesterol stones: Most common Obesity, female > male Pigment or calcium bilirubinate stone Excessive hemolysis, thalassemia Mixed stone Calcium carbonate stones Calcium
87 Gallstone Plain film Depend on calcium composition 80-85% miss gallstone Pigment, mixed, calcium carbonate stones: radio-opaque Cholesterol stone: not visible


88 Gallstone
89 Gallstone US The best way to detect gallstone All stones appear similar on US, independent on stone composition. Mobile Echogenic intraluminal structure Posterior acoustic shadow



90 Gallstone
91 Gallstone CT Density vary from heavily calcified to hypodense Depend on calcium composition Dense calcification: Sensitivity in detect calcification >>> plain film radiograph Pigment Mixed Calcium carbonate Hypodensity pure cholesterol stone can be missed



92 Gallstone






93 Gallstone MRCP Similar ERCP All stones appear similar on US, independent on stone composition.



94 Porcelain gallbladder Calcification in GB wall Associated with chronic inflammation Increased risk of malignancy

95 Common bile duct stone Most located at distal CBD, near ampulla of Vater Plain film Not useful, very low sensitivity

96 Common bile duct stone US Similar gallstone Hyperechoic structure with posterior acoustic shadow Proximal ductal dilation > 25% may not be visualized distal CBD


97 Normal CBD in US < 7 mm



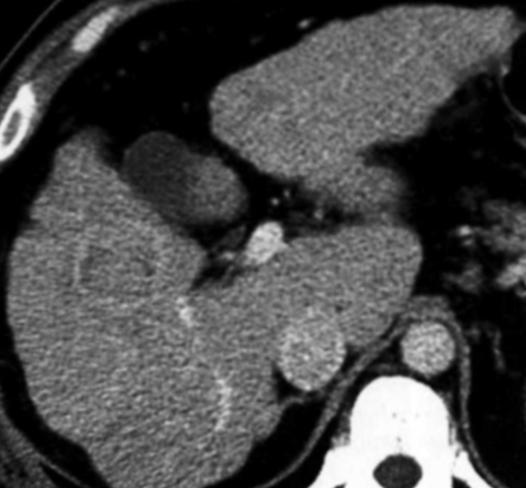
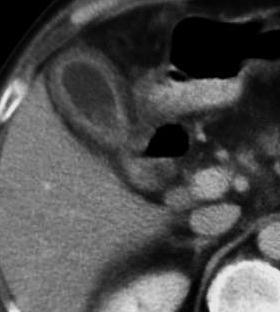
98 CBD stones
99 CBD stones CT and MRI Similar gallstone Proximal ductal dilation




100 CBD stones



101 CBD stones
102 Biliary tract obstruction CBD stone Malignancy CholangioCA Ampullary neoplasm Pancreatic malignancy Duodenal carcinoma Disorder of sphincter of Oddi Ampullary stenosis Inflammatory strictures Prior Sx Prior choledocholithiasis Prior liary infection (ascending cholangitis)


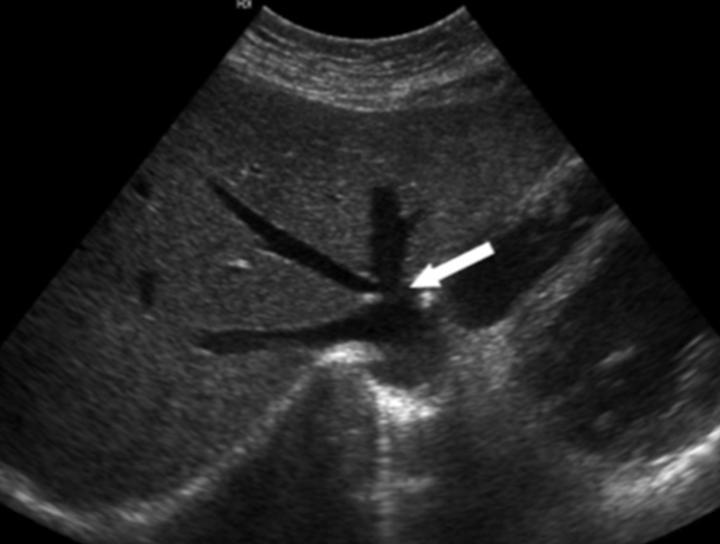
103 Biliary tract obstruction Role of imaging Confirm the presence of obstruction Location of obstruction Cause of obstruction Stone Stricture Tumor US is a screening modality IHD dilation EHD dilation




104 IHD dilation > 2 mm in diameter, parallel channel sign Lack of Doppler signal Irregular, tortuous wall Stellate configuration centrally


105 Normal IHD and CBD







106 IHD dilation Normal CT Normal MRI




107 IHD dilation


108 EHD dilation > 7 mm Longitudinal normal CBD




109 EHD dilation Transverse normal CBD



110 EHD dilation




111 EHD dilation


112 EHD dilation

113 EHD dilation
114 Biliary tract obstruction Investigation US CT or MRI with MRCP ERCP

115 Acute cholecystitis Obstruction of GB by stone at neck or cystic duct Plain film Not useful may detect radio-opaque stone
116 Acute cholecystitis US Gallstone Gallbladder wall thickening Distend gallbladder Pericholecystic fluid Tender at gallbladder; US Murphy s sign positive



117 Normal gallbladder vs wall thickening Wall thickening > 3 mm Normal GB wall < 3 mm



118 Acute cholecystitis




119 Acute cholecystitis
120 Emphysematous cholecystitis Less common Vascular insufficiency of cystic artery Facilitating infection of gas-forming organisms (eg, Clostridium or Escherichia coli) Considered as surgical emergency



121 Emphysematous cholecystitis

122 Acute pancreatitis Activation of pancreatic enzymes within the pancreas leads to organ injury Autodigestion Parenchymal edema and peripancreatic fat necrosis Pancreatic necrosis, hemorrhage
123 Acute pancreatitis Most common: Alcohol abuse Gallstone Less common: Trauma Sepsis Medication Post ERCP
124 Acute pancreatitis Plain film Colon cutoff sign Abrupt termination of gas at splenic flexure Inflammation extends to phrenicocolic ligament Function spasm/ luminal narrowing




125 Acute pancreatitis


126 Acute pancreatitis US Not be used for exclude the diagnosis Enlarge, decreased echogenicity (compare with liver) Peripancreatic fluid collection Detect gallstone US normal pancreas





127 Acute pancreatitis CT normal pancreas
128 Chronic pancreatitis Permanent impairment of pancreatic function Permanent morphologic change as a result of persistent inflammation Findings: Pancreatic calcification Ductal dilation Parenchymal atrophy




129 Chronic pancreatitis
130 Summary Acute abdominal pain Palpable mass Jaundice Abnormal liver function test
131 Summary Acute abdominal pain Plain film US CT or MRI with MRCP Palpable mass Jaundice Abnormal liver function test
132 Summary Acute abdominal pain Palpable mass US CT or MRI Jaundice Abnormal liver function test
133 Summary Acute abdominal pain Palpable mass Jaundice US CT or MRI with MRCP Abnormal liver function test
134 Summary Acute abdominal pain Palpable mass Jaundice Abnormal liver function test US CT or MRI
135 THANK YOU FOR YOUR ATTENTION
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of common diseases of hepatobiliary and GI system
 Imaging of common diseases of hepatobiliary and GI system Natthaporn Tanpowpong, M.D. Diagnostic radiology Faculty of Medicine, Chulalongkorn University Normal plain radiograph A = Common bile duct
Imaging of common diseases of hepatobiliary and GI system Natthaporn Tanpowpong, M.D. Diagnostic radiology Faculty of Medicine, Chulalongkorn University Normal plain radiograph A = Common bile duct
Radiology of hepatobiliary diseases
 GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
Abdominal ultrasound:
 Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Normal Sonographic Anatomy
 hapter 2:The Liver DUNSTAN ABRAHAM Normal Sonographic Anatomy Homogeneous, echogenic texture (Figure 2-1) Measures approximately 15 cm in length and 10 12.5 cm anterior to posterior; measurement taken
hapter 2:The Liver DUNSTAN ABRAHAM Normal Sonographic Anatomy Homogeneous, echogenic texture (Figure 2-1) Measures approximately 15 cm in length and 10 12.5 cm anterior to posterior; measurement taken
Alice Fung, MD Oregon Health and Science University
 Alice Fung, MD Oregon Health and Science University Disclosure Comments The speaker Alice Fung, MD Has relevant financial relationships to disclose. Received honorarium from (Guerbet). This individual
Alice Fung, MD Oregon Health and Science University Disclosure Comments The speaker Alice Fung, MD Has relevant financial relationships to disclose. Received honorarium from (Guerbet). This individual
Hepatic Imaging: What Every Practitioner Should Know
 Hepatic Imaging: What Every Practitioner Should Know Shuchi K. Rodgers, MD Section Chief, Abdominal Imaging Director of Ultrasound Department of Radiology Einstein Medical Center rodgerss@einstein.edu
Hepatic Imaging: What Every Practitioner Should Know Shuchi K. Rodgers, MD Section Chief, Abdominal Imaging Director of Ultrasound Department of Radiology Einstein Medical Center rodgerss@einstein.edu
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning
 Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Gastrointestinal System: Accessory Organ Disorders
 Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
IMAGING OF LIVER, BILIARY TREE, PANCREAS
 IMAGING OF LIVER, BILIARY TREE, PANCREAS Department of Radiology West China Hospital, Sichuan University Yao Jin Learning Points The methodology for imaging the LBP (liver, biliary tree, and pancreas )
IMAGING OF LIVER, BILIARY TREE, PANCREAS Department of Radiology West China Hospital, Sichuan University Yao Jin Learning Points The methodology for imaging the LBP (liver, biliary tree, and pancreas )
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
IT 의료융합 1 차임상세미나 복부질환초음파 이재영
 IT 의료융합 1 차임상세미나 2013-4-3 복부질환초음파 이재영 나는오늘누구를위하여 종을울리나? 전통적의료 의사 공학설계자 의사 최첨단진단장비들 USG, CT, MRI 환자 환자 현대의료 사용자중심의사고 US in the Abdomen Detection DDx Look Behavior Response by external stimuli Guiding Tool
IT 의료융합 1 차임상세미나 2013-4-3 복부질환초음파 이재영 나는오늘누구를위하여 종을울리나? 전통적의료 의사 공학설계자 의사 최첨단진단장비들 USG, CT, MRI 환자 환자 현대의료 사용자중심의사고 US in the Abdomen Detection DDx Look Behavior Response by external stimuli Guiding Tool
My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract
 My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract Objectives PoCUS for Biliary Disease PoCUS for Renal Colic PoCUS for Urinary Retention Biliary Disease A patient presents
My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract Objectives PoCUS for Biliary Disease PoCUS for Renal Colic PoCUS for Urinary Retention Biliary Disease A patient presents
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno. Objectives. Why?
 Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Appendix 9: Endoscopic Ultrasound in Gastroenterology
 Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography (EUS) in gastroenterology. It includes standards for theoretical
Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography (EUS) in gastroenterology. It includes standards for theoretical
Abdomen and Retroperitoneum Ultrasound Protocols
 Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento
 Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento https://www.google.com/search?sa=g&hl=en&q=public+disclosure&tbm=isch&tbs=simg:caqsigeahwelekju2aqaaawlelcmpwgaygpgcamskpib_1qnza7ai
Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento https://www.google.com/search?sa=g&hl=en&q=public+disclosure&tbm=isch&tbs=simg:caqsigeahwelekju2aqaaawlelcmpwgaygpgcamskpib_1qnza7ai
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
HEPATO-BILIARY IMAGING
 HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Vascular Imaging in the Pediatric Abdomen. Jonathan Swanson, MD
 Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
Portal Venous Thrombosis: Tumor VS Bland Thrombus
 June 2015 Portal Venous Thrombosis: Tumor VS Bland Thrombus SERGIO ALFARO, HARVARD MEDICAL SCHOOL YEAR III GILLIAN LIEBERMAN, MD Overview 2 Index Patient History Portal Venous Thrombosis (PVT) Imaging
June 2015 Portal Venous Thrombosis: Tumor VS Bland Thrombus SERGIO ALFARO, HARVARD MEDICAL SCHOOL YEAR III GILLIAN LIEBERMAN, MD Overview 2 Index Patient History Portal Venous Thrombosis (PVT) Imaging
Policies, Standards, and Guidelines. Guidelines for Abdominal Ultrasound Examination
 Policies, Standards, and Guidelines Guidelines for Abdominal Ultrasound Examination Approved by Council Feb 2018 Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to
Policies, Standards, and Guidelines Guidelines for Abdominal Ultrasound Examination Approved by Council Feb 2018 Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Gallbladder & Pancreas Ultrasonography
 복부초음파 : 담낭과췌장 Gallbladder & Pancreas Ultrasonography 김정훈 Department of Radiology 1 Interaction of sound with matter (1) 반사 (Reflection) (2) 굴절 (Refraction) (3) 흡수 (Absorption) (4) 산란 (Scattering) 음향저항
복부초음파 : 담낭과췌장 Gallbladder & Pancreas Ultrasonography 김정훈 Department of Radiology 1 Interaction of sound with matter (1) 반사 (Reflection) (2) 굴절 (Refraction) (3) 흡수 (Absorption) (4) 산란 (Scattering) 음향저항
Abdominal Ultrasound. Diane Hallinen, MD. Bloodroot
 Abdominal Ultrasound Diane Hallinen, MD Bloodroot Abdominal Ultrasound Vasculature Hepatobiliary Spleen Kidney Bladder Bowel Where to put the probe? Vasculature We are going to talk about Celiac Trunk
Abdominal Ultrasound Diane Hallinen, MD Bloodroot Abdominal Ultrasound Vasculature Hepatobiliary Spleen Kidney Bladder Bowel Where to put the probe? Vasculature We are going to talk about Celiac Trunk
Body MRI from the Liver to the Bladder
 Body MRI from the Liver to the Bladder I Want You! Audience Participation Methodist Hospital Continuing Education Seminar Jordan Swensson, MD November 7, 2015 Objectives Observe the uses of MRI for organs
Body MRI from the Liver to the Bladder I Want You! Audience Participation Methodist Hospital Continuing Education Seminar Jordan Swensson, MD November 7, 2015 Objectives Observe the uses of MRI for organs
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Abdomen Sonography Examination Content Outline
 Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Anatomy Jessica Ferguson Ashley Dobos May 31, 2006 LIVER
 Anatomy Jessica Ferguson Ashley Dobos May 31, 2006 LIVER 1) Other Names: Reidel s Lobe normal anatomic variant; projection of the right lobe that can extend as far as the iliac crest (Tempkin, p.54, Anatomy).
Anatomy Jessica Ferguson Ashley Dobos May 31, 2006 LIVER 1) Other Names: Reidel s Lobe normal anatomic variant; projection of the right lobe that can extend as far as the iliac crest (Tempkin, p.54, Anatomy).
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
In any operation. Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications.
 In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
EFSUMB EUROPEAN FEDERATION OF SOCIETIES FOR ULTRASOUND IN MEDICINE AND BIOLOGY Building a European Ultrasound Community
 MINIMUM TRAINING REQUIREMENTS FOR THE PRACTICE OF MEDICAL ULTRASOUND IN EUROPE Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography
MINIMUM TRAINING REQUIREMENTS FOR THE PRACTICE OF MEDICAL ULTRASOUND IN EUROPE Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Pediatric Hepatobiliary, Pancreatic & Splenic US
 Pediatric Hepatobiliary, Pancreatic & Splenic US Susan J. Back, MD Department of Radiology, The Children s Hospital of Philadelphia No Disclosures Objectives Normal Abnormal: cases and US advances Objectives
Pediatric Hepatobiliary, Pancreatic & Splenic US Susan J. Back, MD Department of Radiology, The Children s Hospital of Philadelphia No Disclosures Objectives Normal Abnormal: cases and US advances Objectives
US in non-traumatic acute abdomen. Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university
 US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Imaging Guided Biopsy. Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer
 Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Q129. Which of the following is NOT true about lymph node?
 Q129. Which of the following is NOT true about lymph node? (1). Normal lymph node is not seen in the ultrasound image (2). It is general that high frequency probe is used due to normal lymph node is located
Q129. Which of the following is NOT true about lymph node? (1). Normal lymph node is not seen in the ultrasound image (2). It is general that high frequency probe is used due to normal lymph node is located
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
MRI Abdomen Protocol Pancreas/MRCP with Contrast
 MRI Abdomen Protocol Pancreas/MRCP with Contrast Reviewed By: Brett Mollard, MD; Anna Ellermeier, MD Last Reviewed: July 2018 Contact: (866) 761-4200 Standard uses: 1. Characterization of cystic and solid
MRI Abdomen Protocol Pancreas/MRCP with Contrast Reviewed By: Brett Mollard, MD; Anna Ellermeier, MD Last Reviewed: July 2018 Contact: (866) 761-4200 Standard uses: 1. Characterization of cystic and solid
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Surface Anatomy. Location Shape Weight Role of Five Surfaces Borders Fissures Lobes Peritoneal Lig
 The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
Anatomical and Functional MRI of the Pancreas
 Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
The Focal Hepatic Lesion: Radiologic Assessment
 The Focal Hepatic Lesion: Radiologic Assessment Kevin Kuo, Harvard Medical School Year III Our Patient: PS 67 y/o female w/ long history of alcohol use Drinking since age 18, up to one bottle of wine/day
The Focal Hepatic Lesion: Radiologic Assessment Kevin Kuo, Harvard Medical School Year III Our Patient: PS 67 y/o female w/ long history of alcohol use Drinking since age 18, up to one bottle of wine/day
Biliary cancers: imaging diagnosis. Study of 30 cases
 Biliary cancers: imaging diagnosis. Study of 30 cases N Hammoune, S Semlali, M Eddarai, T. Amil, M Zentar, S. El Kandri,, M Benameur,, S Chaouir. Radiology Department. Mohamed V Military Hospital. Rabat-
Biliary cancers: imaging diagnosis. Study of 30 cases N Hammoune, S Semlali, M Eddarai, T. Amil, M Zentar, S. El Kandri,, M Benameur,, S Chaouir. Radiology Department. Mohamed V Military Hospital. Rabat-
Abdominal Imaging - 9 Topics in 90 min
 Abdominal Imaging 9 topics in 90 min Antonio C. Westphalen, MD PhD Departments of Radiology and Biomedical Imaging, and Urology Liver Biliary tree Gallbladder Pancreas Kidneys Small bowel Colon Abscess?
Abdominal Imaging 9 topics in 90 min Antonio C. Westphalen, MD PhD Departments of Radiology and Biomedical Imaging, and Urology Liver Biliary tree Gallbladder Pancreas Kidneys Small bowel Colon Abscess?
Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011
 Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011 Reported: Analysis Summary for: Abdomen Examination Survey Dates 06/13/2011-06/26/2011 Invited Respondents 6,000 Surveys with Demographics
Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011 Reported: Analysis Summary for: Abdomen Examination Survey Dates 06/13/2011-06/26/2011 Invited Respondents 6,000 Surveys with Demographics
Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review
 Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
1 Right & left Hepatic ducts Gastric Impression of spleen
 Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Outline. Introduction to imaging modalities of the urinary system. Case base learning of common diseases in urinary tract
 Outline Introduction to imaging modalities of the urinary system Case base learning of common diseases in urinary tract Outline Introduction to imaging modalities of the urinary system Case base learning
Outline Introduction to imaging modalities of the urinary system Case base learning of common diseases in urinary tract Outline Introduction to imaging modalities of the urinary system Case base learning
Outline. Introduction to imaging modalities of the urinary system. Case base learning of common diseases in urinary tract
 Outline Introduction to imaging modalities of the urinary system Case base learning of common diseases in urinary tract Diagnostic Investigations in Urinary System PLAIN KUB EXCRETORY UROGRAPHY RETROGRADE
Outline Introduction to imaging modalities of the urinary system Case base learning of common diseases in urinary tract Diagnostic Investigations in Urinary System PLAIN KUB EXCRETORY UROGRAPHY RETROGRADE
Elastography in the. technically difficult patient. EPIQ ultrasound system. Ultrasound
 Ultrasound Elastography in the technically difficult patient EPIQ ultrasound system Chairman Department of Diagnostic Radiology Allegheny General Hospital Pittsburgh, PA, USA You can offer more information
Ultrasound Elastography in the technically difficult patient EPIQ ultrasound system Chairman Department of Diagnostic Radiology Allegheny General Hospital Pittsburgh, PA, USA You can offer more information
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O
 ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
US LI-RADS v2017 CORE
 US LI-RADS v2017 CORE Screening or surveillance US in patient at high risk for HCC US category US-1 US-2 US-3 Negative Subthreshold Positive Category Concept Definition US-1 Negative US-2 Subthreshold
US LI-RADS v2017 CORE Screening or surveillance US in patient at high risk for HCC US category US-1 US-2 US-3 Negative Subthreshold Positive Category Concept Definition US-1 Negative US-2 Subthreshold
Small Plicae Circularis. Short Closely packed together. Sparse, completely absent at distal part Lymphoid Nodule
 Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Imaging of Biliary Tract Emergencies in Jorge A. Soto, MD Professor of Radiology Boston University Medical Center.
 Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Extraosseous myeloma: imaging features
 Extraosseous myeloma: imaging features C. Santos Montón, R. Corrales, J. M. Bastida Bermejo, M. Villanueva Delgado, R. E. Correa Soto, J. M. Alonso Sánchez; Salamanca/ES Learning objectives -To review
Extraosseous myeloma: imaging features C. Santos Montón, R. Corrales, J. M. Bastida Bermejo, M. Villanueva Delgado, R. E. Correa Soto, J. M. Alonso Sánchez; Salamanca/ES Learning objectives -To review
Basic Abdominal Sonography
 24S Basic Abdominal Sonography Procedural Overview JOHN FATCHETT II, RDMS is provided. Patient preparation (i.e., fasting) scanning techniques, spleen, transducer. evaluation of abdominal anatomy in the
24S Basic Abdominal Sonography Procedural Overview JOHN FATCHETT II, RDMS is provided. Patient preparation (i.e., fasting) scanning techniques, spleen, transducer. evaluation of abdominal anatomy in the
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
PORTAL HYPERTENSION. Tianjin Medical University LIU JIAN
 PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Case Study: #3: Gallbladder Carcinoma?
 Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
Radiology of the abdomen Lecture -1-
 Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein
: Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein") Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Abdominal radiology 腹部放射線學
 Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Multi modality Imaging in Acute Pancreatitis. Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009
 Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Appropriate Imaging Tests Lead to Meaningful Results. Dr. Richard Wasley May 2011
 Appropriate Imaging Tests Lead to Meaningful Results Dr. Richard Wasley May 2011 Summarize the advantages and limitations of specific imaging tests and why clinical information is so important to radiologists
Appropriate Imaging Tests Lead to Meaningful Results Dr. Richard Wasley May 2011 Summarize the advantages and limitations of specific imaging tests and why clinical information is so important to radiologists
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
Clinics in Diagnostic Imaging (79)
") Singapore Med J 2002 Vol 43(11) : 591-596 M e d i c a l E d u c a t i o n Clinics in Diagnostic Imaging (79) P Lerttumnongtum, M Muttarak, K Wasanavijit 1a Fig. 1a Subcostal US scan taken at the porta
Singapore Med J 2002 Vol 43(11) : 591-596 M e d i c a l E d u c a t i o n Clinics in Diagnostic Imaging (79) P Lerttumnongtum, M Muttarak, K Wasanavijit 1a Fig. 1a Subcostal US scan taken at the porta
Spontaneous portosystemic venous shunts in liver cirrhosis: Anatomy, pathophysiology, hemodynamic changes and imaging findings
 Spontaneous portosystemic venous shunts in liver cirrhosis: Anatomy, pathophysiology, hemodynamic changes and imaging findings Poster No.: C-3193 Congress: ECR 2010 Type: Educational Exhibit Topic: Vascular
Spontaneous portosystemic venous shunts in liver cirrhosis: Anatomy, pathophysiology, hemodynamic changes and imaging findings Poster No.: C-3193 Congress: ECR 2010 Type: Educational Exhibit Topic: Vascular
PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY. THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel
 PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel. 0925111552 Professional skills-2 THE URINARY SYSTEM The urinary system (review anatomy and physiology)
PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel. 0925111552 Professional skills-2 THE URINARY SYSTEM The urinary system (review anatomy and physiology)
ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE
 ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE Dr. Sohan kumar sah *, Dr. Liu Sibin, Dr. sumendra raj pandey, Dr. Prakashmaan shah, Dr. Gaurishankar pandit, Dr. Suraj kurmi and Dr. Sanjay kumar jaiswal
ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE Dr. Sohan kumar sah *, Dr. Liu Sibin, Dr. sumendra raj pandey, Dr. Prakashmaan shah, Dr. Gaurishankar pandit, Dr. Suraj kurmi and Dr. Sanjay kumar jaiswal
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Objectives. Hepatobiliary Ultrasound: Anatomy, Technique, Pathology. RUQ: Normal Anatomy. Emergency Ultrasound: Gallbladder Location
 Hepatobiliary Ultrasound: Anatomy, Technique, Pathology Laleh Gharahbaghian, MD FAAEM Associate Director, EM Ultrasound Co-Director, EM Ultrasound Fellowship Stanford University Medical Center Seric Cusick,
Hepatobiliary Ultrasound: Anatomy, Technique, Pathology Laleh Gharahbaghian, MD FAAEM Associate Director, EM Ultrasound Co-Director, EM Ultrasound Fellowship Stanford University Medical Center Seric Cusick,
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
LIVER PHYSIOLOGY AND DISEASE
 GASTROENTEROLOGY C opy ri~ht 1972 by The Williams & Wilkins Co. Vol. 62. No.3 Printed in U.S.A. LIVER PHYSIOLOGY AND DISEASE SPLENOMEGALY IN UNCOMPLICATED BILIARY TRACT AND PANCREATIC DISEASE PETER B.
GASTROENTEROLOGY C opy ri~ht 1972 by The Williams & Wilkins Co. Vol. 62. No.3 Printed in U.S.A. LIVER PHYSIOLOGY AND DISEASE SPLENOMEGALY IN UNCOMPLICATED BILIARY TRACT AND PANCREATIC DISEASE PETER B.
Question 1 History. Likely Diagnosis Differential. Further Investigation or Management. Requires Paediatric Surgical referral for laparotomy
 Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,