DISORDERS OF COAGULATION AND THROMBOSIS. Yunfeng Cheng Zhongshan Hospital,Fudan University
|
|
|
- Theodora Barker
- 5 years ago
- Views:
Transcription
1 DISORDERS OF COAGULATION AND THROMBOSIS Yunfeng Cheng Zhongshan Hospital,Fudan University
2 Major Components in Coagulation 1 Vessel Wall 2 Platelet 3 Coagulation factor cascade 4 Clot inhibition/lysis
3 The coagulation cascade coagulation cascade

4 The coagulation cascade
5 The coagulation cascade The coagulation cascade of secondary hemostasis has two pathways which lead to fibrin formation. contact activation pathway (the intrinsic pathway) tissue factor pathway (the extrinsic pathway) It was previously thought that the coagulation cascade consisted of two pathways of equal importance joined to a common pathway. It is now known that the primary pathway for the initiation of blood coagulation is the tissue factor pathway.
6 Hemostasis BV Injury CBC-Plt BT,(CT) PT PTT Neural Contact Damage/contact. Blood Vessel Constriction Reduced Blood flow Platelet Aggregation Primary hemostatic plug Platelet Activation Stable Hemostatic Plug Coagulation Cascade Fibrin formation Platelet study Antibody tests Factor Assay
7 Primary Hemostasis Blood vessel contraction Platelet Plug Formation HEMOSTASIS Secondary Hemostasis Activation of Clotting Cascade Deposition & Stabilization of Fibrin Tertiary Hemostasis Dissolution of Fibrin Clot Dependent on Plasminogen Activation
8 Clinical Approach to Bleeding Disorders Clinical Evaluation(who, when, where, what) 2 Laboratory Studies Approach to The Patient
9 Tests of Hemostasis: Screening tests: Bleeding.T - 10m. Platelet & BV function Prothrombin.T Extrinsic, APTT Intrinsic Thrombin.T common path. (DIC) Specific tests: Factor assays hemophilia. Tests of thrombosis TT, FDP, Platelet function studies: Adhesion, Aggregation, Release tests. Bone Marrow study
10 Bleeding: Clinical Features Local - Vs - General, spontaneous.. Hematoma / Joint Bleeds- Coag Skin / Mucosal Bleeds PLT wound / surgical bleeding Immediate - PLT Delayed - Coagulation


11 Platelet Coagulation Petechiae, Purpura Hematoma, Joint bl.

12 Blood Coagulation & Tests
13 Coagulation Cascade: Intrinsic Pathway (Contact) (XII,XI,IX,VIII) (APTT) (Factor X) Common Path (V,II) (Thrombin) Extrinsic Path Tissue - (VII) (TT) (PT) Fibrinogen Fibrin (F & FDP)
14 Coagulation factor disorders Inherited bleeding disorders Hemophilia A and B vonwillebrands disease Other factor deficiencies Acquired bleeding disorders Liver disease Vitamin K deficiency/warfarin overdose DIC
15 DISORDERS OF COAGULATION AND THROMBOSIS a. Factor VIII Deficiency-Hemophilia A b. Factor IX Deficiency-Hemophilia B c. Vitamin K Deficiency d. Disseminated Intravascular Coagulation e. Coagulation Disorders In Liver Disease f. Circulating Anticoagulants g. Inherited Prothrombotic Disorders h. Antithrombin Deficiency i. Deficiencies Of Proteins C And S j. Resistance To Activated Protein C And The Factor V Leiden Mutation k. Prothrombin Gene Mutation
16 Immune Thrombocytopenia Autoimmune Disorder Thrombocytopenia Heterogeneous
17 Should know: What is Causes Signs & Symptoms Diagnosis Treatments Living with Key points Links


18 FACTOR VIII DEFICIENCY HEMOPHILIA A Hemophilia A - Factor VIII deficiency Hemophilia B - Factor IX deficiency Hemophilia A is an inherited deficiency in clotting factor VIII, which causes increased bleeding. Hemophilia B is an inherited deficiency of Factor IX. Both X-linked recessive trait, and thus occurs in males and in homozygous females Both prolong the APTT (Activated Partial Thromboplastin Time )
19 HEMOPHILIA

20 HEMOPHILIA Queen Victoria May 1819 January 1901 Haemophilia in European royalty

21
22 Hemophilia A and B Hemophilia A Hemophilia B Coagulation factor deficiency Factor VIII Factor IX Inheritance X-linked X-linked recessive recessive Incidence 1/10,000 males 1/100,000 males Severity Complications Related to factor level <1% - Severe - spontaneous bleeding 1-5% - Moderate - bleeding with mild injury 5-25% - Mild - bleeding with surgery or trauma Soft tissue bleeding



 level")







23 FACTOR VIII DEFICIENCY HEMOPHILIA A Severity Factor VIII Clinical Features (or IX ) level Severe <1% Spontaneous bleeding Moderate 1-5% Severe bleeding after trauma or surgery Mild 5-10% Moderate bleeding after trauma or surgery Subclinical 10-25% May not have symptoms
24 Bleeds in Hemophilia Minor Bleeds Oral mucosa Intra-articular Intramuscular Major Bleeds Retroperitoneal Retropharyngeal Intracranial
25 Acutely, bleeding in hemophilics can Compromise circulation. Close off airway Lead to compartment syndrome Cause neuropathy Cause pain Set up inflammatory synovitis, which can trigger more bleeding
26 Chronically, bleeding in hemophilics can Compromise joint function and lead to accelerated DJD (hemophilic arthropathy) Lead to pseudotumor formation Weaken muscles Lead to permanent neurologic compromise.
27 Other complications of hemophilia Inhibitor formation Viral (and other) Infections Job bias
28 Inhibitors in Hemophilia Are alloantibodies formed against Factor VIII (and less commonly FIX) in patients with congenital hemophilia Inactivate exogenously administered clotting factor Must be treated with bypassing agents which less efficacious in hemostasis Increase morbidity and mortality
29 Complications - Orthopedic Hemophilic arthropathy Surgeries synovectomy - arthroscopic or isotopic joint fusion - arthrodesis joint replacement - arthroplasty
30 Complications - Viral infection HIV and hepatitis B and C Blood donation steps to improve viral safety of plasma-derived products 1. blood donors screened 2. donated blood tested for antibodies to hepatitis and HIV 3. all factor concentrate products are virally inactivated and purified
31 Hemophilia Clinical manifestations (hemophilia A & B indistinguishable) Hemarthrosis (most common) Fixed joints Soft tissue hematomas (e.g., muscle) Muscle atrophy Shortened tendons Other sites of bleeding Urinary tract CNS, neck (may be life-threatening) Prolonged bleeding after surgery or dental extractions
32 Treatment of hemophilia A Intermediate purity plasma products Virucidally treated May contain von Willebrand factor High purity (monoclonal) plasma products Virucidally treated No functional von Willebrand factor Recombinant factor VIII Virus free/no apparent risk No functional von Willebrand factor
33 Factor VIII Infusion
34 Principles of Factor Dosing What s the desired clotting factor level? What s the half life of the factor? FVIII - 12 hours FIX - 24 hours Clotting factor is dosed in Units 1 Unit is the amount of factor present in 1 ml of normal plasma What s the volume of distribution and recovery? 1 unit of FVIII raises plasma level by 2% 1 unit of FIX raises plasma level by 1%
35 Dosing guidelines for hemophilia A One unit of F VIII increases the plasma F VIII level by 2% Mild bleeding Target: 30%-50% dosing q8-12h; 1-3 days (15U/kg) Small Hemarthrosis, mild mucosal bleed, epistaxis Major bleeding Target: >50% dosing q8-12h; 7 days Major Hemarthrosis, Large muscle bleed Major bleeding Target: % q8-12h; 7-14 days (50U/kg) CNS trauma, hemorrhage, lumbar puncture Surgery Retroperitoneal hemorrhage GI bleeding Adjunctive therapy amino caproic acid (Amicar),or Tranexamic acid or DDAVP (for mild disease only)
36 Adjunctive Treatment for Hemophilia EACA (Amicar) Epsilon amino caproic acid Inhibits fibrinolysis and increases clot stability Useful in mucosal bleeding Contra-indicated in upper pole urinary bleeding DDAVP Causes release of pre-formed stores of FVIII/VWF from Weibel-Palade bodies in endothelial cells May help in mild hemophilia A Can be given as a nasal spray Efficacy must be tested before-hand
37 Hemophilia Management - In the ER History What kind of hemophilia?, how severe? Inhibitor in the past? What was last titer? Is it gone for good? What kind of factor does the patient normally take? Does the patient treat himself at home? Physical Where s the bleed? Any organ, airway, neurovascular compromise? Labs Baseline factor level (unless pt has inhibitor) Bethesda titer
38 Hemophilia Management - In the ER Give clotting factor and pain meds Decide if admission is necessary
39 Complications of therapy Formation of inhibitors (antibodies) 10-15% of severe hemophilia A patients 1-2% of severe hemophilia B patients Viral infections Hepatitis B Human parvovirus Hepatitis C Hepatitis A HIV Other
40 Agent Treatment of hemophilia B High purity factor IX Recombinant human factor IX Dose Initial dose: 100U/kg Subsequent: 50 U/kg every 24 hours fresh-frozen plasma or a plasma fraction enriched in the prothrombin complex proteins
41 Future of Hemophilia Primary prophylaxis Gene therapy Inhibitor prediction/treatment Prevention of hemophilic arthropathy viral contamination of factor products
42 Zhongshan Hospital,Fudan University
43 DISORDERS OF COAGULATION AND THROMBOSIS- part II Yunfeng Cheng Zhongshan Hospital,Fudan University
44 DISORDERS OF COAGULATION AND THROMBOSIS a. Factor VIII Deficiency-Hemophilia A b. Factor IX Deficiency-Hemophilia B c. Vitamin K Deficiency d. Disseminated Intravascular Coagulation e. Coagulation Disorders In Liver Disease f. Circulating Anticoagulants g. Inherited Prothrombotic Disorders h. Antithrombin Deficiency i. Deficiencies Of Proteins C And S j. Resistance To Activated Protein C And The Factor V Leiden Mutation k. Prothrombin Gene Mutation
45 THE CLOTTING MECHANISM INTRINSIC Collagen XII XI IX VIII EXTRINSIC Tissue Thromboplastin VII X V PROTHROMBIN (II) THROMBIN (III) FIBRINOGEN (I) FIBRIN
46 What is DIC DIC is a clinic pathologic syndrome of activated coagulation that manifests with bleeding or thrombosis. Patients with DIC have a loss of balance between the clot-promoting and lysing systems in vivo.
47 What is DIC This syndrome can have a clinical spectrum ranging from bleeding to a prothrombotic state. DIC is not a specific diagnosis, and its presence always indicates another underlying disease. Bleeding associated with DIC usually results from excess fibrinolysis; thrombosis associated with DIC results from excess thrombin formation.
48 Cause 1. Basic disease Condition associated with DIC
49 Infectious disease---the most common clinical condition associated with DIC; Severe trauma---acute DIC is often seen with serious injuries and burns caused by the release of thromboplastic material; Neoplasia---both solid tumor and cancer; Vascular disorder---large aortic aneurysms may result in local activation of coagulation; Obstetric accidents---includes amniotic fluidembolism and placental abruption, the fetus, the placenta, and the amniotic fluid are rich in thromboplastic substances.
50 DIC(DISSEMIATED INTRAVASCULAR COAGULATION) DIC can be either an explosive and life-threatening bleeding disorder or a relatively mild or subclinical disorder. Although a long list of diseases can be complicated by DIC, it is most frequently associated with obstetric catastrophes, metastatic malignancy, massive trauma, and bacterial sepsis

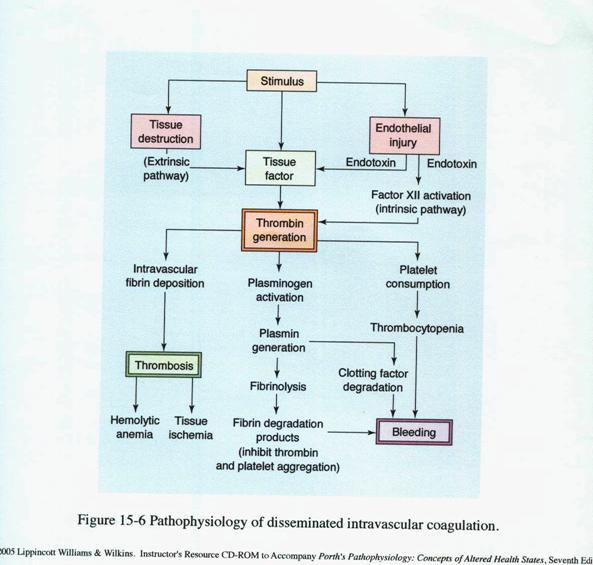
51 The pathophysiology of DIC
52 Hemostatic Balance Procoagulant Anticoagulant Activation of Blood Coagulation Suppression of Physiologic Anticoagulant Pathways Impaired Fibrinolysis
53 The pathophysiology of DIC 1) Activation of Blood Coagulation Tissue factor/factor VIIa mediated thrombin generation complex activates factor IX and X 2) Suppression of Anticoagulant reduced antithrombin III levels reduced activity of the protein C/protein S Insufficient regulation of tissue factor activity by tissue factor pathway inhibitor (TFPI)
54 The pathophysiology of DIC 3) Impaired Fibrinolysis relatively suppressed at time of maximal activation of coagulation due to increased plasminogen activator inhibitor type 1 4) Cytokines IL-6, and IL-1 mediate coagulation activation in DIC TNF- mediates dysregulation of anticoagulant and fibrinolysis IL-10 may modulate the activation of coagulation
55 Pathophysiology In DIC, a systemic activation of the coagulation system simultaneously leads to thrombus formation (compromising blood supply to various organs) and exhaustion of platelets and coagulation factors (results in hemorrhage). This is a disruption of body homeostasis. (Porth, 2001)
56 Pathophysiology hypercoagulability 1) Coagulation cascade is initiated, causing widespread fibrin formation 2) Microthrombi are deposited throughout he microcirculatory 3) Fibrin deposits result in tissue ischemia, hypoxia, necrosis 4) Leads to multi organ dysfunction hypocoagulability (the hemorrhagic phase) 1) Activates the complement system 2) Byproducts of fibrinolysis (fibrin/fibrin degradation products(fdp)) further enhance bleeding by interfering with platelet aggregation, fibrin polymerization, & thrombin activity 3) Leads to Hemorrhage
57 Pathophysiology






58 Bleeding mechanisms Consumption of clotting factors and platelets Activation of secondary fibrinolytic system Production of fibrin degradation products
59 Disturbance of circulation---shock Microthromobus blood returning to heart DIC bleeding blood volume Bradykinin,histamine vasodilation blood pressure FDP can increased to dilates vessels that cause hypotension Heart function cardiac output blood pressure
60 Ischemic tissue damagedysfunction of multiple organs Renal insufficiency Acute adrenal failure Adult respiratory distress syndrome Infarcted skin syndrome of purpura
61 The laboratory manifestations CBC PT APTT Fibrinogen D dimer FDPs Platelets falling or low. Hb dropping. Film may show RBC fragments Prolonged Prolonged Falling or decreased Increased Increased
62 Diagnosis of DIC Presence of disease associated with DIC Appropriate clinical setting Clinical evidence of thrombosis, hemorrhage or both. Laboratory studies no single test is accurate serial test are more helpful than single test


63 Clinical Manifestations of DIC


64 Microscopic findings in DIC Fragments Schistocytes Paucity of platelets
65 Disseminated intravascular coagulation Laboratory results: Prolonged PT, APTT and TT Reduced fibrinogen level Increased D-Dimers Thrombocytopenia: <100,000 or rapidly declining Microangiopathic changes in blood film Low levels of coagulation inhibitors: AT III, protein C Bachelor of Chinese Medicine
66 Clinical setting Laboratory tests Criteria Diagnosis of DIC Underlying disease Platelet count < 100 X 10 9 /L, or rapid decline PT and APTT Prolonged Presence of fibrin degradation products Low levels of coagulation inhibitors Low fibrinogen level in severe cases Bachelor of Chinese Medicine
67 Differential Diagnosis Severe liver failure Vitamin K deficiency Liver disease Thrombotic thrombocytopenic purpura Congenital abnormalities of fibrinogen
68 Stages of DIC Hypercoagulable stage Hypocoagulable stage Secondary fibrinolytic stage
69 Acute DIC Almost always secondary Consumptive coagulopathy Decreases in both coagulants & anticoagulants Severity may relate to levels of anticoagulants
70 Subacute DIC Symptoms appear within days to weeks, clotting substances are consumed but not reduced Bleeding is rarely seen but the evidence of DIC can be detected by laboratory examinations Thrombotic manifestation is commonly seen in malignant patient
71 Chronic DIC DIC develops slowly and the illness goes through within months The clinical and laboratory features of chronic DIC present over periods of month and the patient is usually not critically ill Usually symptoms are concealed
72 Treatment of DIC Treatment of underlying disorder: Stop the triggering process Supportive therapy Other treatments Plasma and platelet substitution therapy Anticoagulants Physiologic coagulation inhibitors Bachelor of Chinese Medicine
73 Treatment of DIC Platelets and Plasma to treat bleeding tendency to cover an invasive procedure for patients with a high risk of bleeding Clotting factor concentrates overcomes large volumes of plasma but not advocated because: 1) contains small amount of activated factors, and 2) DIC results in deficiency of multiple factors Bachelor of Chinese Medicine
74 Plasma therapy Indications Active bleeding Patient requiring invasive procedures Patient at high risk for bleeding complications Fresh frozen plasma(ffp): provides clotting factors, fibrinogen, inhibitors, and platelets in balanced amounts. Usual dose is ml/kg
75 Treatment of DIC Anticoagulants low dose heparin low molecular weight heparin new thrombin inhibitors (ATIII independent) useful for clinically overt thromboembolism or extensive deposition of fibrin Bachelor of Chinese Medicine
76 Concentrates of coagulation inhibitors Antithrombin concentrate reduces sepsis related mortality improvement of DIC and organ function Supportive therapeutic option in severe DIC Bachelor of Chinese Medicine
77 Coagulation Inhibitor Therapy Antithrombin Protein C concentrate Tissue Factor Pathway Inhibitor (TFPI) Heparin
78 Case Female, 29 years old Emergency admission due to placental abruption. (eight months of pregnancy), coma, petechiae, gastrointestinal bleeding,hematuria; Laboratory tests: Hb70g/L (110 to 150) platelet 85*10 9 /L (100 to 300*10 9 / L) fibrinogen 1.78g / L (2~4g/L) prothrombin time20.9 s (12-14) FDPs level is increased and the D-dimer is increased Platelet 75*10 9 /L, and fibrinogen1.6g/l, 4h after the review Diagnosis: placental abruption Disseminated intravascular coagulation
79 Case Based on the lab values, DIC is confirmed for the patient. The Platelet count is decreased, the fibrinogen level is decreased, PT and PTT levels increased and prolonged, FDPs level is increased and the D-dimer is increased (usually together, levels are 100% specificity and sensitive). If a factor assay was done one would expect the levels to show a decrease in factors VI, VIII, and IX
80 Answer for Case Study Lab abnormalities along with clinical presentation is used to confirm a diagnosis of DIC If abnormal results are obtained for PT, PTT, platelets, and fibrinogen, then the D-dimer and FDPs levels are used to confirm DIC...FDPs abnormal in 75% and D-dimer in 95%.
81 Objectives Understand the pathophysiology of Disseminated Intravascular Coagulation (DIC) Identify risk factors and etiology of DIC Describe the signs and symptoms of DIC Identify treatment modalities for DIC Define, identify and understand Acute vs Chronic DIC Develop understanding of diagnosing DIC (lab interpretations)
82 Glossary Activated PTT- aptt tests the intrinsic and common pathways D-dimer- an antigen formed as a result of plasmin lysis of cross-linked fibrin clots, documents the presence of thrombin Fibrin degradation product(fdp)- degradation products increase as plasmin biodegrades fibrinogen and fibrin,levels are elevated in % of patients with DIC Prothrombin Time(PT)- tests the extrinsic and common pathways (Porth, 2004) & (Otto, 2001)
83 Zhongshan Hospital,Fudan University
84 DISORDERS OF COAGULATION AND THROMBOSIS- part III Yunfeng Cheng Zhongshan Hospital,Fudan University
85 VITAMIN K DEFICIECY Vitamin K is a fat-soluble vitamin that plays a critical role in hemostasis. Vitamin K is converted to an active epoxide in liver microsomes and serves as a cofactor in the enzymatic carboxylation of glutamic acid residues on prothrombin complex proteins.
86 Vitamin K deficiency Source of vitamin K Green vegetables Synthesized by intestinal flora Required for synthesis Factors II, VII, IX,X Protein C and S Causes of deficiency Malnutrition Biliary obstruction Malabsorption Antibiotic therapy Treatment Vitamin K Fresh frozen plasma

87 VITAMIN K DEFICIECY
88 VITAMIN K DEFICIECY The three major causes of vitamin K deficiency: inadequate dietary intake intestinal malabsorption loss of storage sites due to hepatocellular disease.
89 VITAMIN K DEFICIECY With vitamin K deficiency: Plasma levels of all the prothrombin complex proteins (factors II, VII, IX, X; proteins C and S) decrease. Those with the shortest half-lives, factor VII and protein C, decrease first. Because of the rapid fall in factor VII, patients with mild vitamin K deficiency may have a prolonged PT and a normal APTT. Later, as the levels of the other factors fall, the APTT will also become prolonged.
90 VITAMIN K DEFICIECY Parenteral administration of 10 mg vitamin K permits normal production of prothrombin complex proteins within 8 to 10 h. Severe hemorrhage can be treated with freshfrozen plasma. Purified prothrombin complex concentrates should be avoided because they contain trace quantities of activated forms of the prothrombin complex proteins and can cause thrombosis in patients with liver disease.
91 Vitamin K antagonism Oral anticoagulants (warfarin) Both PT and APTT Prolonged PT system chosen for monitoring due to shortest half life of factor VII INR system to standardize monitoring of oral anticoagulant therapy Important: INR should not be used in other clinical context Bachelor of Chinese Medicine

92 COAGULATION DISORDERS IN LIVER DISEASE
93 COAGULATION DISORDERS IN LIVER DISEASE Causes Reduced synthesis of clotting factors Vitamin K mal-absorption Acquired functional defect of fibrinogen Failure to clear activated products of coagulation and fibrinolysis Thrombocytopenia hypersplenism Coagulation tests PT and APTT Prolonged
94 COAGULATION DISORDERS IN LIVER DISEASE Treatment of Liver disease Vitamin K Fresh frozen plasma Anticoagulation with heparin has been advocated to control DIC
95 Liver Disease Decreased synthesis of II, VII, IX, X, XI, and fibrinogen Prolongation of PT, aptt and Thrombin Time Often complicated by Gastritis, esophageal varices, DIC Treatment Fresh-frozen plasma infusion Vitamin K (usually ineffective)
96 von Willebrand Disease Clinical features von Willebrand factor Inheritance Carrier of factor VIII Anchors platelets to subendothelium Autosomal dominant Incidence 1/10,000 Clinical features Mucocutaneous bleeding
97 Laboratory evaluation of von Willebrand disease Classification Type 1 Partial quantitative deficiency Type 2 Qualitative deficiency Type 3 Total quantitative deficiency Diagnostic tests: vwf antigen, vwf activity
98 Treatment of von Willebrand disease Varies by Classification Cryoprecipitate Source of fibrinogen, factor VIII and VWF Only plasma fraction that consistently contains VWF multimers Correction of bleeding time is variable DDAVP (Deamino-8-arginine vasopressin) Increases plasma VWF levels by stimulating secretion from endothelium Duration of response is variable Used for type 1 disease Dosage 0.3 µg/kg q 12 hr IV Factor VIII concentrate Virally inactivated product Used for type 2 and 3
99 CIRCULATING ANTICOAGULANTS Circulating anticoagulants, or inhibitors, are usually IgG antibodies that interfere with coagulation reactions. They arise in 15 to 20% of patients with factor VIII or factor IX deficiency who have received plasma infusions. Nonspecific (lupus-like) inhibitors prolong coagulation tests by binding to phospholipids. lupus anticoagulant (LA), anticardiolipin antibody (ACLA)
100 CIRCULATING ANTICOAGULANTS PT,APTT, massive plasma or concentrate infusion activated prothrombin complex concentrates plasmapheresis or exchange transfusion to lower antibody titer Women who have had more than one midtrimester abortion, especially those with SLE, should have a trial of anticoagulant therapy. Patients with a single thrombotic episode (stroke or pulmonary embolus) and no other risk factor except LA or ACLA activity should be treated.
101 INHERITED PROTHROMBOTIC DISORDERS Inherited defects in the natural coagulation inhibitors (antithrombin, proteins C and S), abnormalities in the fibrinolytic system, and certain dysfibrinogenemias predispose patients to thrombosis. Factor V Leiden Increased risk of thrombosis.
102 Immune Thrombocytopenia
103 Immune Thrombocytopenia(ITP) Autoimmune Disorder Thrombocytopenia(Isolated thrombocytopenia) (< /L) Heterogeneous acquired Absence of any obvious initiation or underlying cause Introduction





104 ITP Clinical manifestations
:6511")
105 Secondary ITP Blood. 2009; 113(26):
106 Mean annual incidence (per 100,000 person-years) Epidemiology The incidence of newly diagnosed ITP in adults ranges from per persons per year Female male < Total age (year) Hematol Oncol Clin North Am. 2009;23:
107 Diagnostic approach Careful history Physical examination Complete blood count:isolated thrombocytopenia Should be excluded: Other autoimmune disease, Pseudothrombocytopenia due to EDTA, Thrombotic thrombocytopenic purpura or hemolytic uremic syndrome, Evan syndrome, aplastic anemia, Congenital thrombocytopenic disorders, Myelodysplastic syndrome, Chronic lymphocytic leukemia et al. Blood. 2010;115:
108 Three phases Newly diagnosed ITP: ( 3 months) Persistent ITP: (3 months~1 year) Chronic ITP: (>1 year) Blood. 2009; 113(11):
109 Blood. 2010;115:


110 Blood smear ITP Pseudothrombocytopenia
111 Clinical presnetation and natural history Chronic Course ~ 15% of patients remit within 1 year Bleeding manifestations: mucocutaneous bleeding is the most common, (internal bleeding or fatal intracranial hemorrhage ) PLT< 30*10 9 3% 0.4%/year----<40 years 71% 13%/year---->60 years Arch Intern Med. 2000;160:
112 Events per patient-year Estimated annual rate of bleeding according to age group 0.35 Fatal 1.75 Non-fatal % % % 1.2% % 7.3% 0.00 < > 60 Age (years) 0.00 < > 60 Age (years) Cohen YC, et al. Arch Intern Med 2000; 160:

113 Cines DB,Blanchette VS. N Engl J Med. 2002;346:

114
115 Clinial presentation and natural history of ITP in children Peak age of presentation: 5~6years; 50%~60% of children will have a febrile illness that preceded the discovery of thrombocytopenia; PLT< 20* %: None or mild bleeding; 20%: Moderate bleeding; 3%: Severe bleeding; 0.1%~0.5%: Life-threatening bleeding; 5%~10%: develop chronic ITP (>12 months)
116 Clinical situation First line (initial treatment for newly diagnosed ITP) Therapy option Anti-D Corticosteroids: dexamethasone, methylprednisolone, prednis(ol)one IVIg Second line Azathioprine Cyclosporin A Cyclophosphamide Danazol Dapsone Mycophenolate mofetil Rituximab Splenectomy Thrombopoietin (TPO) receptor agonists Vinca alkaloids Treatment for patients failing firstand second-line therapies Category A: treatment options with sufficient data TPO receptor agonists Category B: treatment options with minimal data and considered to have potential for considerable toxicity Campath-1H Combination of first- and second-line therapies Combination chemotherapy Hemopoietic stem cell transplantation (HSCT)
117 Management of primary ITP in adults Corticosteroid therapy IVIg and anti-rh-d Splenectomy Anti-CD20 therapy(rituximab) TPO receptor agnosists
118 Adjunctive therapy for bleeding disorders
119 Adjunctive drug therapy for bleeding Fresh frozen plasma Cryoprecipitate Epsilon-amino-caproic acid (Amicar) DDAVP Recombinant human factor VIIa (Novoseven)
120 Fresh frozen plasma Content - plasma (decreased factor V and VIII) Indications Multiple coagulation deficiencies (liver disease, trauma) DIC Warfarin reversal Coagulation deficiency (factor XI or VII) Dose (225 ml/unit) ml/kg Note Viral screened product ABO compatible
121 Cryoprecipitate Prepared from FFP Content Factor VIII, von Willebrand factor, fibrinogen Indications Fibrinogen deficiency Uremia von Willebrand disease Dose (1 unit = 1 bag) 1-2 units/10 kg body weight
122 Aminocaproic acid (Amicar) Mechanism Prevent activation plaminogen -> plasmin Dose 100mg/kg po or IV q 6 hr Uses Primary menorrhagia Oral bleeding Bleeding in patients with thrombocytopenia Blood loss during cardiac surgery Side effects GI toxicity Thrombi formation
123 Desmopressin (DDAVP) Mechanism Increased release of VWF from endothelium Dose 0.3µg/kg IV q12 hrs 150mg intranasal q12hrs Uses Most patients with von Willebrand disease Mild hemophilia A Side effects Facial flushing and headache Water retention and hyponatremia
124 Recombinant human factor VIIa Mechanism Activates coagulation system through extrinsic pathway Approved Use Factor VIII inhibitors in hemophiliacs Dose: (1.2 mg/vial) 90 µg/kg q 2 hr Adjust as clinically indicated
125 Summary Hemostatic Disorders BT Plt PT APTT Vascular Dis PLT Disorder Factor VIII/IX *Congenital Vit K / Liver *Acquired Combined (DIC) -
126 Thrombophilia
127 Thrombophilia Now considered a multicausal disease, with an interplay of acquired and genetic thrombotic risk factors Approximately half of venous thromboembolic episodes in patients with inherited thrombophilias occur in relation to events that are generally recognized as a predisposing states, such surgery, pregnancy, and immobilization
128 Inherited thrombophilic states Antithrombin deficiency Abnormalities in protein C and protein S system - protein C deficiency - protein S deficiency - abnormal thrombomodulin Resistance to activated protein C (FV Leiden, FV Cambridge)
129 Inherited thrombophilic states Hyperprothrombinemia (prothrombin variant G20210A) Dysfibrynogeneimia Abnormalities in fibrinolytic system - hypo- or dysplasminogenemia - elevated plasminogen activator inhibitor - decreased tissue plasminogen activator Hyperhomocysteinemia Heparin cofactor II defciency Elevated histidine-rich glycoprotein Factor XII deficiency
130 Clinical features of patients with inherited deficiencies of AT, PC, PS, and APC-resistance Venous thrombosis -- Deep vein thrombosis of the lower limbs --Pulmonary embolism --Superficial thrombophlebitis --Mesenteric vein thrombosis --Cerebral vein thrombosis Frequent family history of thrombosis First thrombosis usually at young age (<40y) Frequent recurrences Neonatal purpura fulminans (homozygous PC or PS deficiency)
131 Laboratory diagnosis of inherited thrombophilia AT: First step Heparin cofactor synthetic substrate-based assays PC: Synthetic substrate-based assays (venoms as a PC activators) AT: Second step Immunoassays, crossed immunoelectrophoresis DNA analysis PC: Immunoassays, crossed immunoelectrophoresis DNA analysis
132 Laboratory diagnosis of inherited thrombophilia PS: First step Immunoassay of total PS Immunoassay of free PS APC-resistance: APTT-based functional assays (using FV-deficient plasma) PS: Second step crossed immunoelectrophoresis DNA analysis APC-resistance: DNA analysis (mutant factor V)
133 Characteristics of AT deficiency Autosomal dominant inheritance Quantitative and qualitative defects Thrombotic phenomena in adolescence or even earlier Frequently pulmonary embolism as first clinical manifestation
134 Characteristics of PC deficiency Autosomal dominant inheritance Quantitative and qualitative defects Homozygotes die because of thrombosis in infancy Thrombotic phenomena in adolescence Skin necrosis when warfarin therapy introduced
135 Characteristics of PS deficiency Autosomal dominant inheritance Quantitative and qualitative defects Homozygotes die because of thrombosis in utero or in the early infancy Thrombotic phenomena in adolescence Skin necrosis when warfarin therapy introduced
136 DEFICIENCIES OF PROTEINS C AND S

137 PROTHROMBIN GENE MUTATION

138 Zhongshan Hospital,Fudan University
139 1. What is Hemophilia A Key points 2. The treatment of Hemophilia A 3. What is Disseminated Intravascular Coagulation; The pathophysiology of DIC 4. What is immune thrombocytopenia 5. Coagulation Disorders In Liver Disease
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Disseminated Intravascular Coagulation. M.Bahmanpour MD Assistant professor IUMS
 به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
Bleeding Disorders. Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph
 Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
ACQUIRED COAGULATION ABNORMALITIES
 ACQUIRED COAGULATION ABNORMALITIES ACQUIRED COAGULATION ABNORMALITIES - causes 1. Liver disease 2. Vitamin K deficiency 3. Increased consumption of the clotting factors (disseminated intravascular coagulation
ACQUIRED COAGULATION ABNORMALITIES ACQUIRED COAGULATION ABNORMALITIES - causes 1. Liver disease 2. Vitamin K deficiency 3. Increased consumption of the clotting factors (disseminated intravascular coagulation
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN
 Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Disseminated Intravascular Coagulation (DIC) Seminar. Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.
 Seminar. Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.") Disseminated Intravascular Coagulation (DIC) Seminar Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.2012 1 Our plan: Understand the pathophysiology Identify risk factors
Disseminated Intravascular Coagulation (DIC) Seminar Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.2012 1 Our plan: Understand the pathophysiology Identify risk factors
COAGULATIONS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin)
, FRCP(Edin)") COAGULATIONS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin) Haemostasis-blood must be maintained in a fluid state in order to function as a transport system, but must be able to solidify to form a clot following
COAGULATIONS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin) Haemostasis-blood must be maintained in a fluid state in order to function as a transport system, but must be able to solidify to form a clot following
BLEEDING DISORDERS Simple complement:
 BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
INHERITED COAGULOPATHY
 Disorder Etiology Pathophysiology and Presentation Lab Findings and Diagnosis Treatment INHERITED COAGULOPATHY HEMOPHILIA A and B Hemophilia A: deficiency in XIII (85%) Hemophilia B: deficiency in IX (15%)
Disorder Etiology Pathophysiology and Presentation Lab Findings and Diagnosis Treatment INHERITED COAGULOPATHY HEMOPHILIA A and B Hemophilia A: deficiency in XIII (85%) Hemophilia B: deficiency in IX (15%)
Pathology note 8 BLEEDING DISORDER
 Pathology note 8 BLEEDING DISORDER Slide75 ( Types of clotting factors deficiency): Today we will talk about public public factor deficiency it could be acquired or inherited, acquired diseases are more
Pathology note 8 BLEEDING DISORDER Slide75 ( Types of clotting factors deficiency): Today we will talk about public public factor deficiency it could be acquired or inherited, acquired diseases are more
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Bleeding disorders. Hemostatic failure: Inappropriate and excessive bleeding either spontaneous or in response to injury.
 1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
UNIT VI. Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav. Copyright 2011 by Saunders, an imprint of Elsevier Inc.
 UNIT VI Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav Hemostasis: Prevention of Blood Loss Vascular constriction Formation of a platelet plug Formation of a blood
UNIT VI Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav Hemostasis: Prevention of Blood Loss Vascular constriction Formation of a platelet plug Formation of a blood
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Thursday, February 26, :00 am. Regulation of Coagulation/Disseminated Intravascular Coagulation HEMOSTASIS/THROMBOSIS III
 REGULATION OF COAGULATION Introduction HEMOSTASIS/THROMBOSIS III Regulation of Coagulation/Disseminated Coagulation necessary for maintenance of vascular integrity Enough fibrinogen to clot all vessels
REGULATION OF COAGULATION Introduction HEMOSTASIS/THROMBOSIS III Regulation of Coagulation/Disseminated Coagulation necessary for maintenance of vascular integrity Enough fibrinogen to clot all vessels
PCCN Review Hematology
 PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche
 L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche Armando Tripodi Angelo Bianchi Bonomi Hemophilia and Thrombosis Center Dept. of Clinical Sciences and Community Health University
L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche Armando Tripodi Angelo Bianchi Bonomi Hemophilia and Thrombosis Center Dept. of Clinical Sciences and Community Health University
Bleeding Disorders.1 MS4.24.Feb.19. Abdallah Awidi Abbadi.MD. FRCP.FRCPath Professor
 Bleeding Disorders.1 MS4.24.Feb.19 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Professor Email: abdalla.awidi@gmail.com Hemostasis BV Injury Neural Contact Damage/contact. Blood Vessel Constriction Reduced
Bleeding Disorders.1 MS4.24.Feb.19 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Professor Email: abdalla.awidi@gmail.com Hemostasis BV Injury Neural Contact Damage/contact. Blood Vessel Constriction Reduced
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Bleeding Disorders: (Hemorrhagic Diatheses) Tests used to evaluate different aspects of hemostasis are the following:
 Tests used to evaluate different aspects of hemostasis are the following:") Bleeding Disorders: (Hemorrhagic Diatheses) Excessive bleeding can result from: 1. Increased fragility of vessels. 2. Platelet deficiency or dysfunction. 3. Derangement of coagulation. 4. Combinations
Bleeding Disorders: (Hemorrhagic Diatheses) Excessive bleeding can result from: 1. Increased fragility of vessels. 2. Platelet deficiency or dysfunction. 3. Derangement of coagulation. 4. Combinations
Hematologic Disorders. Assistant professor of anesthesia
 Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
LAMA SHATAT TTP, ITP, DIC
 TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
DIC. Bert Vandewiele Fellow Critical Care 23 May 2011
 DIC Bert Vandewiele Fellow Critical Care 23 May 2011 Dissiminated Intravascular Coagulopathie 11/3/2011 Dr. Bert Vandewiele 2 Dissiminated Intravascular Coagulopathie = Consumption coagulopathie = Defibrination
DIC Bert Vandewiele Fellow Critical Care 23 May 2011 Dissiminated Intravascular Coagulopathie 11/3/2011 Dr. Bert Vandewiele 2 Dissiminated Intravascular Coagulopathie = Consumption coagulopathie = Defibrination
Blood coagulation and fibrinolysis. Blood clotting (HAP unit 5 th )
") Blood coagulation and fibrinolysis Blood clotting (HAP unit 5 th ) Vessel injury Antithrombogenic (Favors fluid blood) Thrombogenic (Favors clotting) 3 Major systems involved Vessel wall Endothelium ECM
Blood coagulation and fibrinolysis Blood clotting (HAP unit 5 th ) Vessel injury Antithrombogenic (Favors fluid blood) Thrombogenic (Favors clotting) 3 Major systems involved Vessel wall Endothelium ECM
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Thrombosis. By Dr. Sara Mohamed Abuelgasim
 Thrombosis By Dr. Sara Mohamed Abuelgasim 1 Thrombosis Unchecked, blood coagulation would lead to dangerous occlusion of blood vessels if the protective mechanisms of coagulation factor inhibitors, blood
Thrombosis By Dr. Sara Mohamed Abuelgasim 1 Thrombosis Unchecked, blood coagulation would lead to dangerous occlusion of blood vessels if the protective mechanisms of coagulation factor inhibitors, blood
Document Title: Hemostasis: Platelet and Coagulation Disorders. Author(s): Joseph H. Hartmann (University of Michigan), DO 2012
: Joseph H. Hartmann (University of Michigan), DO 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Hemostasis: Platelet and Coagulation Disorders Author(s): Joseph H. Hartmann (University of Michigan), DO 2012 License: Unless otherwise
Project: Ghana Emergency Medicine Collaborative Document Title: Hemostasis: Platelet and Coagulation Disorders Author(s): Joseph H. Hartmann (University of Michigan), DO 2012 License: Unless otherwise
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department
 Dr. Klara Vezendi Szeged University Transfusiology Department") Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Congenital bleeding disorders
 Congenital bleeding disorders Overview Factor VIII von Willebrand Factor Complex factor VIII von Willebrand factor (vwf) complex circulate as a complex + factor IX intrinsic pathway Platelets bind via
Congenital bleeding disorders Overview Factor VIII von Willebrand Factor Complex factor VIII von Willebrand factor (vwf) complex circulate as a complex + factor IX intrinsic pathway Platelets bind via
MANAGEMENT OF COMMON BLEEDING DISORDERS. Auro Viswabandya Department of Haematology, CMC, Vellore
 MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
Haemorrhagic Disorders. Dr. Bashar Department of Pathology Mosul Medical College
 Haemorrhagic Disorders Dr. Bashar Department of Pathology Mosul Medical College Hemorrhagic Disorders These include Disorders of platelets. Disorders of blood vessels. Disorders of coagulation & fibrinolysis.
Haemorrhagic Disorders Dr. Bashar Department of Pathology Mosul Medical College Hemorrhagic Disorders These include Disorders of platelets. Disorders of blood vessels. Disorders of coagulation & fibrinolysis.
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Approach To A Bleeding Patient
 ABDUL MAJEED, RAHUL RAJEEV REVIEW ARTICLE INTRODUCTION Hemostasis is the process of forming clots in the walls of damaged blood vessels and preventing blood loss while maintaining blood in a fluid state
ABDUL MAJEED, RAHUL RAJEEV REVIEW ARTICLE INTRODUCTION Hemostasis is the process of forming clots in the walls of damaged blood vessels and preventing blood loss while maintaining blood in a fluid state
Hemostatic System - general information
 PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
Hemodynamic Disorders, Thrombosis, and Shock. Richard A. McPherson, M.D.
 Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
Bleeding Disorders HOPE Maram Al-anbar
 Bleeding Disorders HOPE Maram Al-anbar 9-9 - 2014 ^^ Attention Please ^^ We ( correction team of pediatric package^hope/2010^ ) had decided to make one lecture of bleeding disorders in place of the two
Bleeding Disorders HOPE Maram Al-anbar 9-9 - 2014 ^^ Attention Please ^^ We ( correction team of pediatric package^hope/2010^ ) had decided to make one lecture of bleeding disorders in place of the two
Part IV Antithrombotics, Anticoagulants and Fibrinolytics
 Part IV Antithrombotics, Anticoagulants and Fibrinolytics "The meaning of good and bad, of better and worse, is simply helping or hurting" Emerson Chapter 16: Blood Coagulation and Fibrinolytic System
Part IV Antithrombotics, Anticoagulants and Fibrinolytics "The meaning of good and bad, of better and worse, is simply helping or hurting" Emerson Chapter 16: Blood Coagulation and Fibrinolytic System
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion
 This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
Hemostasis. PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures
 Hemostasis PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures Disorders of Hemostasis - Hemophilia - von Willebrand Disease HEMOPHILIA A defect in the thrombin propagation phase
Hemostasis PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures Disorders of Hemostasis - Hemophilia - von Willebrand Disease HEMOPHILIA A defect in the thrombin propagation phase
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Primary Exam Physiology lecture 5. Haemostasis
 Primary Exam Physiology lecture 5 Haemostasis Haemostasis Body s response for the prevention and cessation of bleeding. Broadly consists of: Primary Haemostasis - vascular spasm and platlet plug formation
Primary Exam Physiology lecture 5 Haemostasis Haemostasis Body s response for the prevention and cessation of bleeding. Broadly consists of: Primary Haemostasis - vascular spasm and platlet plug formation
TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE
 TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE Dr Susan Russell Director HTC Sydney Children s Hospital, Randwick HFA Meeting 2015 What is von Willebrand Factor? VWF is a large multimeric protein Two
TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE Dr Susan Russell Director HTC Sydney Children s Hospital, Randwick HFA Meeting 2015 What is von Willebrand Factor? VWF is a large multimeric protein Two
Thrombophilia. Diagnosis and Management. Kevin P. Hubbard, DO, FACOI
 Thrombophilia Diagnosis and Management Kevin P. Hubbard, DO, FACOI Clinical Professor of Medicine Kansas City University of Medicine and Biosciences-College of Osteopathic Medicine Kansas City, Missouri
Thrombophilia Diagnosis and Management Kevin P. Hubbard, DO, FACOI Clinical Professor of Medicine Kansas City University of Medicine and Biosciences-College of Osteopathic Medicine Kansas City, Missouri
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Ch. 45 Blood Plasma proteins, Coagulation and Fibrinolysis Student Learning Outcomes: Describe basic components of plasma
 Chapt. 45 Ch. 45 Blood Plasma proteins, Coagulation and Fibrinolysis Student Learning Outcomes: Describe basic components of plasma Inheritance of X-linked gene for Factor VIII hemophilia A Explain the
Chapt. 45 Ch. 45 Blood Plasma proteins, Coagulation and Fibrinolysis Student Learning Outcomes: Describe basic components of plasma Inheritance of X-linked gene for Factor VIII hemophilia A Explain the
Chapter 19. Hemostasis
 Chapter 19 Hemostasis Hemostasis Hemostasis is the cessation of bleeding stopping potentially fatal leaks important in small blood vessels not effective in hemorrhage excessive bleeding from large blood
Chapter 19 Hemostasis Hemostasis Hemostasis is the cessation of bleeding stopping potentially fatal leaks important in small blood vessels not effective in hemorrhage excessive bleeding from large blood
Bleeding and Haemostasis. Saman W.Boskani HDD, FIBMS Maxillofacial Surgeon
 Bleeding and Haemostasis Saman W.Boskani HDD, FIBMS Maxillofacial Surgeon 1 Beeding Its escaping or extravasation of blood contents from blood vessels Types: - Arterial - Venous - Capillary Differences
Bleeding and Haemostasis Saman W.Boskani HDD, FIBMS Maxillofacial Surgeon 1 Beeding Its escaping or extravasation of blood contents from blood vessels Types: - Arterial - Venous - Capillary Differences
Coagulopathy Case - 3. Andy Nguyen, M.D. 2009
 Coagulopathy Case - 3 Andy Nguyen, M.D. 2009 CLINICAL HISTORY A 21 year-old male seen in the emergency room with a swollen, tender right knee. Patient is an electrician who had fallen to the ground an
Coagulopathy Case - 3 Andy Nguyen, M.D. 2009 CLINICAL HISTORY A 21 year-old male seen in the emergency room with a swollen, tender right knee. Patient is an electrician who had fallen to the ground an
EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION
 EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Topics of today lectures: Hemostasis
 Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms of hemostasis - Vascular contraction - Platelets plug - Blood coagulation (clotting) - Structure and functions of platelets - Blood
Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms of hemostasis - Vascular contraction - Platelets plug - Blood coagulation (clotting) - Structure and functions of platelets - Blood
Hematology Review. CCRN exam. The Coagulation Cascade. The Coagulation Cascade. Components include: Intrinsic pathway Extrinsic pathway Common pathway
 CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes ~ 100 units Heparin neutralization in ~ 5 min
 Nanik (Nayri) Hatsakorzian Pharm.D/MPH candidate 2014 Touro University College of Pharmacy CA Bleeding Reversal Agents Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes
Nanik (Nayri) Hatsakorzian Pharm.D/MPH candidate 2014 Touro University College of Pharmacy CA Bleeding Reversal Agents Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes
Chapter 3. Haemostatic abnormalities in patients with liver disease
 Chapter 3 Haemostatic abnormalities in patients with liver disease Ton Lisman, Frank W.G. Leebeek 1, and Philip G. de Groot Thrombosis and Haemostasis Laboratory, Department of Haematology, University
Chapter 3 Haemostatic abnormalities in patients with liver disease Ton Lisman, Frank W.G. Leebeek 1, and Philip G. de Groot Thrombosis and Haemostasis Laboratory, Department of Haematology, University
Easy Bleeding General Presentation
 Easy Bleeding General Presentation It is not uncommon for children to bleed and bruise after experiencing trauma. However, a child may also have an underlying coagulopathy, which results in easy and possibly
Easy Bleeding General Presentation It is not uncommon for children to bleed and bruise after experiencing trauma. However, a child may also have an underlying coagulopathy, which results in easy and possibly
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Easy bruising vs Coagulopathy
 Easy bruising vs Coagulopathy Sept. 19, 2015 Lakehead Summer School Chris Hillis, MD MSc FRCPC hillis@hhsc.ca @HemeHillis Aim & Objectives Aim: To increase comfort in detecting non-pathologic bleeding
Easy bruising vs Coagulopathy Sept. 19, 2015 Lakehead Summer School Chris Hillis, MD MSc FRCPC hillis@hhsc.ca @HemeHillis Aim & Objectives Aim: To increase comfort in detecting non-pathologic bleeding
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS
 QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Coagulation, Haemostasis and interpretation of Coagulation tests
 Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
Hemostasis. Learning objectives Dr. Mária Dux. Components: blood vessel wall thrombocytes (platelets) plasma proteins
 plasma proteins") Hemostasis Learning objectives 14-16 Dr. Mária Dux Components: blood vessel wall thrombocytes (platelets) plasma proteins Hemostatic balance! procoagulating activity anticoagulating activity 1 Thrombocytes
Hemostasis Learning objectives 14-16 Dr. Mária Dux Components: blood vessel wall thrombocytes (platelets) plasma proteins Hemostatic balance! procoagulating activity anticoagulating activity 1 Thrombocytes
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute lung injury (ALI) transfusion-related, 363 372. See also Transfusion-related acute lung injury (TRALI) ALI. See Acute lung injury
Index Note: Page numbers of article titles are in boldface type. A Acute lung injury (ALI) transfusion-related, 363 372. See also Transfusion-related acute lung injury (TRALI) ALI. See Acute lung injury
Oral Anticoagulant Drugs
 Oral Anticoagulant Drugs Spoiled sweet clover caused hemorrhage in cattle(1930s). Substance identified as bishydroxycoumarin. Initially used as rodenticides, still very effective, more than strychnine.
Oral Anticoagulant Drugs Spoiled sweet clover caused hemorrhage in cattle(1930s). Substance identified as bishydroxycoumarin. Initially used as rodenticides, still very effective, more than strychnine.
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
THROMBOSIS AND BLEEDING
 THROMBOSIS AND BLEEDING Klara Gadó MD. PhD. Senior Professor of Internal Medicine Semmelweis University, Budapest What is thrombosis? formation of a blood clot in a blood vessel Blood can not flow Organ
THROMBOSIS AND BLEEDING Klara Gadó MD. PhD. Senior Professor of Internal Medicine Semmelweis University, Budapest What is thrombosis? formation of a blood clot in a blood vessel Blood can not flow Organ
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital
 Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital") DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital Disseminated intravascular coagulation (DIC) Disseminated
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital Disseminated intravascular coagulation (DIC) Disseminated
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
The LaboratoryMatters
 Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. HEMOSTASIS AND THE LABORATORY This issue highlights: Primary Hemostasis Screening Tests Case
Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. HEMOSTASIS AND THE LABORATORY This issue highlights: Primary Hemostasis Screening Tests Case
Guidelines for Shared Care Centres and Community Staff
 Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombosis and emboli. Peter Nagy
 Thrombosis and emboli Peter Nagy A thrombus is any solid object developing from the blood in vivo within the vascular system or heart. Thrombosis is hemostasis in the wrong place. Major components, forms:
Thrombosis and emboli Peter Nagy A thrombus is any solid object developing from the blood in vivo within the vascular system or heart. Thrombosis is hemostasis in the wrong place. Major components, forms:
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
BLEEDING DISORDERS. JC Opperman 2012
 BLEEDING DISORDERS JC Opperman 2012 Primary and Secondary Clotting Laboratory Tests Routine screening tests Prothrombin time (PT) (INR) increased in neonates (12-18 sec) Partial thromboplastin time (PTT)
BLEEDING DISORDERS JC Opperman 2012 Primary and Secondary Clotting Laboratory Tests Routine screening tests Prothrombin time (PT) (INR) increased in neonates (12-18 sec) Partial thromboplastin time (PTT)
Are there still any valid indications for thrombophilia screening in DVT?
 Carotid artery stenosis and risk of stroke Are there still any valid indications for thrombophilia screening in DVT? Armando Mansilha MD, PhD, FEBVS Faculty of Medicine of University of Porto Munich, 2016
Carotid artery stenosis and risk of stroke Are there still any valid indications for thrombophilia screening in DVT? Armando Mansilha MD, PhD, FEBVS Faculty of Medicine of University of Porto Munich, 2016
Hemostasis Haemostasis means prevention of blood loss from blood vessels.
 ١ Hemostasis Haemostasis means prevention of blood loss from blood vessels. Bleeding is stopped by several mechanisms, which are: 1. Local vasoconstriction 2. Formation of platelet plug 3. Blood coagulation
١ Hemostasis Haemostasis means prevention of blood loss from blood vessels. Bleeding is stopped by several mechanisms, which are: 1. Local vasoconstriction 2. Formation of platelet plug 3. Blood coagulation
Blood products and plasma substitutes
 Blood products and plasma substitutes Plasma substitutes Dextran 70 and polygeline are macromolecular substances which are metabolized slowly; they may be used to expand and maintain blood volume in shock
Blood products and plasma substitutes Plasma substitutes Dextran 70 and polygeline are macromolecular substances which are metabolized slowly; they may be used to expand and maintain blood volume in shock
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
What are blood clots?
 What are blood clots? Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service GP Partner Westcliffe Medical Group Created 5/31/18 Dr. Matthew
What are blood clots? Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service GP Partner Westcliffe Medical Group Created 5/31/18 Dr. Matthew
Moath Darweesh. Omar Sami. Saleem Khreisha. 1 P a g e
 7 Moath Darweesh Omar Sami Saleem Khreisha 1 P a g e -First of all, I want to give a quick revision to simplify the whole hemostasis mechanism, it will be much easier here with me. Enjoy (you can skip
7 Moath Darweesh Omar Sami Saleem Khreisha 1 P a g e -First of all, I want to give a quick revision to simplify the whole hemostasis mechanism, it will be much easier here with me. Enjoy (you can skip
12 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
 Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Introduction to coagulation and laboratory tests
 Introduction to coagulation and laboratory tests Marc Jacquemin Special Haemostasis Laboratory Center for Molecular and Vascular Biology University of Leuven Coagulation in a blood vessel: fibrin stabilises
Introduction to coagulation and laboratory tests Marc Jacquemin Special Haemostasis Laboratory Center for Molecular and Vascular Biology University of Leuven Coagulation in a blood vessel: fibrin stabilises
HEMOSTASIS/THROMBOSIS II
 HEMOSTASIS/THROMBOSIS II Congenital/Acquired Hemorrhagic Disorders & Their Treatment COAGULATION TESTING!Bleeding time primary screening test for platelet function!if bleeding time abnormal!platelet Aggregation
HEMOSTASIS/THROMBOSIS II Congenital/Acquired Hemorrhagic Disorders & Their Treatment COAGULATION TESTING!Bleeding time primary screening test for platelet function!if bleeding time abnormal!platelet Aggregation
Pathophysiology. Tutorial 3 Hemodynamic Disorders
 Pathophysiology Tutorial 3 Hemodynamic Disorders ILOs Recall different causes of thrombosis. Explain different types of embolism and their predisposing factors. Differentiate between hemorrhage types.
Pathophysiology Tutorial 3 Hemodynamic Disorders ILOs Recall different causes of thrombosis. Explain different types of embolism and their predisposing factors. Differentiate between hemorrhage types.
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Hemostasis and. Blood Coagulation
 Hemostasis and Blood Coagulation Events in Hemostasis The term hemostasis means prevention of blood loss. Whenever a vessel is severed or ruptured, hemostasis is achieved by several mechanisms: (1) vascular
Hemostasis and Blood Coagulation Events in Hemostasis The term hemostasis means prevention of blood loss. Whenever a vessel is severed or ruptured, hemostasis is achieved by several mechanisms: (1) vascular
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Branch of medicine that deals with blood, its formation and disorders is called. Three main functions of cardiovascular system are,, and.
 Chapter 19 The Blood Human body must maintain a balance called. Body fluid inside the cells is called fluid; that outside is called or fluid. Two major fluid networks that help in connecting cells are
Chapter 19 The Blood Human body must maintain a balance called. Body fluid inside the cells is called fluid; that outside is called or fluid. Two major fluid networks that help in connecting cells are
Blood clotting. Subsequent covalent cross-linking of fibrin by a transglutaminase (factor XIII) further stabilizes the thrombus.
 further stabilizes the thrombus.") Blood clotting It is the conversion, catalyzed by thrombin, of the soluble plasma protein fibrinogen (factor I) into polymeric fibrin, which is deposited as a fibrous network in the primary thrombus. Thrombin
Blood clotting It is the conversion, catalyzed by thrombin, of the soluble plasma protein fibrinogen (factor I) into polymeric fibrin, which is deposited as a fibrous network in the primary thrombus. Thrombin
Thrombosis. Jeffrey Jhang, M.D.
 Thrombosis Jeffrey Jhang, M.D. Introduction The human hemostatic system has evolved to maintain blood flow under normal physiologic conditions while remaining primed to rapidly respond to vascular injury
Thrombosis Jeffrey Jhang, M.D. Introduction The human hemostatic system has evolved to maintain blood flow under normal physiologic conditions while remaining primed to rapidly respond to vascular injury
Online Supplementary Data. Country Number of centers Number of patients randomized
 A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility