IBD advanced course 2nd meeting IGA Meeting Hilton TLV
|
|
|
- Ginger Sullivan
- 5 years ago
- Views:
Transcription
1 IBD advanced course 2nd meeting IGA Meeting Hilton TLV
2
3 Age Sanjeet is 24 years of age at diagnosis 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
4 Age- as a Prognostic Factor: Although it is common to diagnose ulcerative colitis in young adults, an established diagnosis at a younger age (<30 years) has been shown to increase the risk of disease relapse (p<0.01), and is associated with a higher risk of colectomy (HR=0.28, 95% CI= ; p=0.003), compared with diagnosis at an older age ( 50 years). [1] [1] Solberg IC, Lygren I, Jahnsen J, Aadland E, Høie O, Cvancarova M, et al. Clinical course during the first 10 years of ulcerative colitis: results from a population based inception cohort (IBSEN Study). Scand J Gastroenterol. 2009;44:431 40
5 Gender The patient is a male 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
6 Gender-as a Prognostic Factor: Colectomy rates in UC have been shown to be significantly higher in men compared with women, both for early ( 90 days from diagnosis) colectomy (men vs women: 2.6% vs 1.1%; HR=2.37, 95% CI= ; p=0.0009), and for late (>90 days from diagnosis) colectomy (HR=1.28, 95% CI= ; p=0.036). [2] [2] Targownik LE, Singh H, Nugent Z, Bernstein CN. The epidemiology of colectomy in ulcerative colitis: results from a populationbased cohort. Am J Gastroenterol. 2012;107:
7 Lifestyle The patient is an ex-smoker 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
8 Smoking- as a Prognostic Factor: Active smoking in UC was shown to be associated with a lower risk of: Flares (HR=0.8, 95% CI= ) [3] Hospitalisation (p=0.01) [4] Colectomy (OR=0.57, 95% CI= ) [5] [3] Höie O, Wolters F, Riis L, Aamodt G, Solberg C, Bernklev T, et al. Ulcerative colitis: patient characteristics may predict 10-year disease recurrence in a European-wide population-based cohort. Am J Gastroenterol. 2007;102: link [4] Odes HS, Fich A, Reif S, Halak A, Lavy A, Keter D, et al. Effects of current cigarette smoking on clinical course of Crohn's disease and ulcerative colitis. Dig Dis Sci. 2001;46: link [5] Cosnes J. Tobacco and IBD: relevance in the understanding of disease mechanisms and clinical practice. Best Pract Res Clin Gastroenterol. 2004;18: link
9 Laboratory Tests Serum albumin 38 g/l (normal range: g/l) CRP = 3.2 mg/l (normal value: <5 mg/l) 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
10 Lab-as a Prognostic Factor: A high serum albumin level has indirectly been shown to be associated with an improved response to medical therapy (OR: 1.10, 95% CI= ; P=0.001). [7] At diagnosis, an elevated CRP level is associated with an increased risk of colectomy (OR=4.8, 95% CI= ; p=0.02). [8] An increased CRP level is also associated with a higher risk of medical treatment failure, particularly in acute-severe colitis (p<0.01). [9] [7] Ho GT, Mowat C, Goddard CJ, Fennell JM, Shah NB, Prescott RJ, Satsangi J. Predicting the outcome of severe ulcerative colitis: development of a novel risk score to aid early selection of patients for second-line medical therapy or surgery. Aliment Pharmacol Ther. 2004;19: link [8] Henriksen M, Jahnsen J, Lygren I, Stray N, Sauar J, Vatn MH, Moum B; IBSEN Study Group. C-reactive protein: a predictive factor and marker of inflammation in inflammatory bowel disease. Results from a prospective population-based study. Gut. 2008;57: link [9] Travis SP, Farrant JM, Ricketts C, Nolan DJ, Mortensen NM, Kettlewell MG, Jewell DP. Predicting outcome in severe ulcerative colitis. Gut. 1996;38: link
11
12 Treatment The patient required steroids to induce remission at the first presentation, and was then maintained with 5-ASA treatment. 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
13 Treatment- as a Prognostic Factor: The need for steroids at first presentation is a surrogate marker of more aggressive disease and has been associated with higher colectomy rates in patients with UC (HR=1.8; 95% CI= ). [17] [17] Samuel S, Ingle SB, Dhillon S, Yadav S, Harmsen WS, Zinsmeister AR, et al. Cumulative incidence and risk factors for hospitalization

14
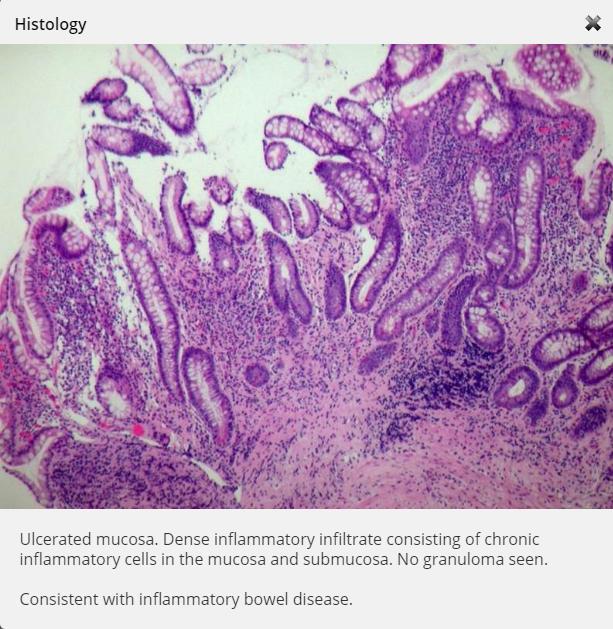
15 Histology Although endoscopy showed inactive disease, the histologic examination showed active disease with the presence of neutrophils in the crypts, crypt distortion and a dense infiltrate of plasma cells at the base of the crypts (basal plasmacytosis). 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
16 Histology- as a Prognostic Factor: Active histology has been associated with an increased risk of colorectal cancer in patients with UC (OR=5.1, 95% CI= ; p<0.001). [16] Also, the presence of basal plasmacytosis has been shown to be an independent predictor of disease relapse in UC (HR=4.5, 95% CI= ; p=0.003). [19] [16] Rutter M, Saunders B, Wilkinson K, Rumbles S, Schofield G, Kamm M, et al. Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis. Gastroenterology. 2004;126:451 9 [19] Bitton A, Peppercorn MA, Antonioli DA, Niles JL, Shah S, Bousvaros A, et al. Clinical, biological, and histologic parameters as predictors of relapse in ulcerative colitis. Gastroenterology. 2001;120:13 20
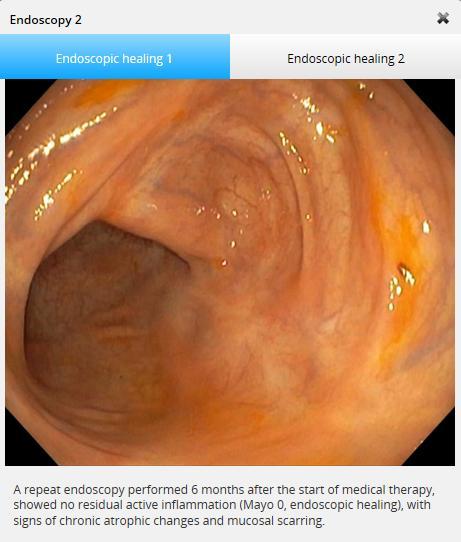
17 Rapid step-up care approach The following factors for treatment were considered at the outset: The patient s response to steroids should be assessed after 4 8 weeks. The target is to obtain full symptom control (normal stools 1 2 times/day, no blood, no tenesmus) with mucosal healing (endoscopic Mayo sub-score=0/1, but ideally Mayo 0, as sustained remission is more frequent if Mayo 0 is reached versus Mayo 1). If this target is not achieved, a purine analogue and/or biologic treatment should be discussed with the patient. A purine alone may be insufficient if the patient does not respond properly to steroid induction. Purine may be adapted in case of full disease control but with steroid-dependency. A biologic treatment would be adapted to both steroid-refractoriness or steroid-dependency.
18
19 Lifestyle, age & clinical symptoms He currently smokes cigarettes/day He is 29 years old at diagnosis He has lower abdominal pain that he scored as 7/10 subjectively. 7 bowel movements per day; 6 quite loose; occasional rectal bleeding and pain on defecation.
20 Lifestyle & age- as a Prognostic Factor: Smoking may predict increased need for therapy escalation [EL3], progression to complicated disease behavior [EL3], need for surgery [EL3] (relative risk=1.31, 95% CI= ) (2) and post-operative recurrence in CD [EL3] (p<0.001, OR=2.15; 95% CI= ) (3) Younger age, and perianal disease, at diagnosis are associated with a disabling CD course [EL4] (6-8) Younger age at diagnosis (adults <40 years) increases risk of surgery [EL2] (p=0.02, OR=0.84 per 5 years, 95% CI= ) (9) [2] Cosnes J, Carbonnel F, Beaugerie L, Le Quintrec Y, Gendre JP. Effects of cigarette smoking on the long-term course of Crohn's disease. Gastroenterology. 1996;110(2): [3] Reese GE, Nanidis T, Borysiewicz C, Yamamoto T, Orchard T, Tekkis PP. The effect of smoking after surgery for Crohn's disease: a meta-analysis of observational studies. Int J Colorectal Dis. 2008;23(12): [6] Beaugerie L, Seksik P, Nion-Larmurier I, Gendre JP, Cosnes J. Predictors of Crohn's disease. Gastroenterology. 2006;130(3):650 6 link [7] Loly C, Belaiche J, Louis E. Predictors of severe Crohn s disease. Scand J Gastroenterol. 2008;43: [8] Kruis W, Katalinic A, Klugmann T, Franke GR, Weismuller J, Leifeld L, et al. Predictive factors for an uncomplicated long-term course of Crohn s disease: a retrospective analysis. J Crohns Colitis. 2013;7:e [9] Tremaine WJ, Timmons LJ, Loftus EV, Jr., Pardi DS, Sandborn WJ, Harmsen WS, et al. Age at onset of inflammatory bowel disease and the risk of surgery for non-neoplastic bowel disease. Aliment Pharmacol Ther. 2007;25(12): l

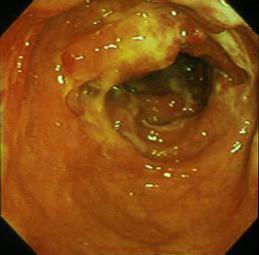
21 Endoscopy
22 Endoscopy- Endoscopic severity of CD can predict development of penetrating complications [EL4] (11) Extensive and deep ulcers at colonoscopy in patients with colonic CD may predict the need for surgery (RR=5.43) [EL3] (11) However, the endoscopy results do not show severe (deep or extensive) ulceration in the colon. [11] Allez M, Lemann M, Bonnet J, Cattan P, Jian R, Modigliani R. Long-term outcome of patients with active Crohn s disease exhibiting extensive and deep ulcerations at colonoscopy. Am J Gastroenterol. 2002;97:947 53

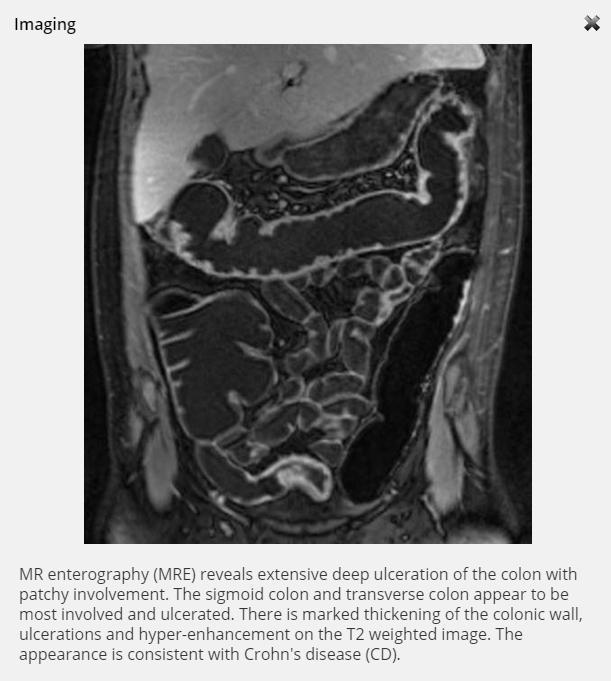
23 Imaging A 30-cm-long segment of ileum adjacent to the cecum is narrowed with marked thickening of the ileal wall, ulcerations and hyper-enhancement on the T2 weighted image. The lumen is narrowed. Some of the ulcers penetrate into adjoining tissue. The ileum proximal to it is mildly dilated. The colon appears to be normal. The appearance is consistent with Crohn's disease 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
24 Imaging- as a Prognostic Factor: Disease located in the small bowel carries a higher risk for surgery than isolated colonic disease [EL2] (OR=2.39; 95% CI= ) (4) Penetrating and stricturing phenotypes at diagnosis are independent risk factors for surgery [EL2] (HR=8.6; 95% CI= ) (5) [4] Lazarev M, Huang C, Bitton A, Cho JH, Duerr RH, McGovern DP, et al. Relationship between proximal Crohn's disease location and disease behavior and surgery: a cross-sectional study of the IBD Genetics Consortium. Am J Gastroenterol. 2013;108(1): [5] Biroulet LP, et al. S1184 Cumulative Incidence of and Risk Factors for Major Abdominal Surgery in a Population-Based Cohort of Crohn's Disease. Gastroenterology. 2010;138(5, Supplement 1):S 199
25 Histology
26 Histology- as a Prognostic Factor: There is little data to support use of biopsy images for prognosis in CD; however, morphometric analysis of early biopsies may have the potential to predict clinical phenotypes and outcomes such as surgery in Crohn's colitis [EL4] (10) [10] Klein A, Eliakim R, Karban A, Mazor Y, Ben-Izhak O, Chowers Y, Sabo E. Early histological findings quantified by histomorphometry allow prediction of clinical phenotypes in Crohn's colitis patients. Anal Quant Cytopathol Histpathol. 2013;35:95 104

27 Extra intestinal Manifestations: EIM 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
28 EIM- as a Prognostic Factor: Extra-intestinal manifestations [EL3] seem to predict disease progression to complicated behavior in CD (8)
29 HBI Score
 [1] Panaccione R, et al.")
30 Treatment The HBI score shows the patient has moderate disease; he receives systemic steroids (prednisone) for induction of remission on first flare based on a treatment paradigm for remission induction in moderate luminal Crohn's disease. (1) [1] Panaccione R, et al. Review article: treatment algorithms to maximize remission and minimize corticosteroid dependence in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2008;28:674 88
31 Treatment- as a Prognostic Factor: Initial requirement for steroids on first flare may be an independent risk factor (OR=3.1, 95% CI= ) for disabling disease during the 5 years following diagnosis (6, 7) [6] Beaugerie L, Seksik P, Nion-Larmurier I, Gendre JP, Cosnes J. Predictors of Crohn's disease. Gastroenterology. 2006;130(3):650 6 [7] Loly C, Belaiche J, Louis E. Predictors of severe Crohn s disease. Scand J Gastroenterol. 2008;43:948 54
32 EXPERT INSIGHT ON MANAGING GREG Based upon the diagnosis and prognosis for Greg: Expedited Step up? Top down? [1] Panaccione R, et al. Review article: treatment algorithms to maximize remission and minimize corticosteroid dependence in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2008;28:674 88
33


34 Endoscopy 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
35 Endoscopy- as a Prognostic Factor: Extensive or deep ulcers at colonoscopy in patients with colonic CD may predict the need for surgery in adult patients (RR=5.43, 95% CI= ). [EL3] (11) Endoscopic severity of CD can predict development of penetrating complications. [EL4] (11) [11] Allez M, Lemann M, Bonnet J, Cattan P, Jian R, Modigliani R. Long term outcome of patients with active Crohn s disease exhibiting extensive and deep ulcerations at colonoscopy. Am J Gastroenterol. 2002;97:947 53
36 Imaging
37 Imaging- as a Prognostic Factor: The MRE image supports the colonoscopy image showing deep and extensive ulceration of the colon which may predict the need for surgery in adults with colonic CD (RR=5.43, 95% CI= ). [EL3] (11) [11] Allez M, Lemann M, Bonnet J, Cattan P, Jian R, Modigliani R. Long term outcome of patients with active Crohn s disease exhibiting extensive and deep ulcerations at colonoscopy. Am J Gastroenterol. 2002;97:947 53

38 Histology Deep ulcerations present in the mucosa and submucosa. Dense inflammatory infiltrate consisting of chronic inflammatory cells in the mucosa and submucosa. No granuloma seen. Rectal mucosa has mild inflammatory cell infiltration only with no ulceration. Appearance is consistent with inflammatory bowel disease and favors Crohn's disease. 1:Non- Predictors 2:Favorable prognosis 3:Poor prognosis
39 Histology- as a Prognostic Factor: There are few data to support use of biopsy images for prognosis in CD but morphometric analysis of early biopsies may have the potential to predict clinical phenotypes and outcomes such as surgery in Crohn's colitis. [EL4] (12) However, in this case, the histology confirms that ulceration observed on colonoscopy is deep which, when taken together, may be associated with prediction of surgical need (RR=5.43, 95% CI= ). [EL3] (11) [11] Allez M, Lemann M, Bonnet J, Cattan P, Jian R, Modigliani R. Long term outcome of patients with active Crohn s disease exhibiting extensive and deep ulcerations at colonoscopy. Am J Gastroenterol. 2002;97: link [12] Klein A, et al. Early histological findings quantified by histomorphometry allow prediction of clinical phenotypes in Crohn s colitis patients. Anal Quant Cytopathol Histpathol. 2013;35:95 104
40 MANAGING LEAH Based on the diagnosis and prognosis for the patient [15] Panaccione R, Rutgeerts P, Sandborn WJ, Feagan B, Schreiber S, Ghosh S. Review article: treatment algorithms to maximize remission and minimize corticosteroid dependence in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2008;28:674 88
41


42 Colonoscopy shows active inflammation up to 45 cm above the anal margin. There is complete loss of the vascular pattern, moderate friability with bleeding upon contact, small erosions, but no large or deep ulcers. A series of inflammatory pseudopolyps is also present in the sigmoid. The mucosa is normal beyond 45 cm up to the caecum. Ulcerative colitis endoscopic index of severity (UCEIS) = 6 Endoscopic Mayo score = 2 Endoscopy Left colon 50 cm above anus Sigmoid colon 35 cm above anus


43 Colonoscopy shows active inflammation up to 45 cm above the anal margin. There is complete loss of the vascular pattern, moderate friability with bleeding upon contact, small erosions, but no large or deep ulcers. A series of inflammatory pseudopolyps is also present in the sigmoid. The mucosa is normal beyond 45 cm up to the caecum. Ulcerative colitis endoscopic index of severity (UCEIS) = 6 Endoscopic Mayo score = 2 Endoscopy Sigmoid colon 20 cm above anus Rectum
44 Endoscopy- as a Prognostic Factor: There is no sign of severe colitis (deep ulcers, mucosal abrasion, well-like ulcers, etc.) or extensive disease. [EL3] (18) However, presence of multiple pseudopolyps may be associated with an increased risk of colorectal cancer development (OR=2.5; 95% CI= ). [EL3] (19) [18] Beaugerie L, Sokol H. Clinical, serological and genetic predictors of inflammatory bowel disease course. World J Gastroenterol. 2012;18: link [19] Velayos FS, Loftus EV Jr, Jess T, Harmsen WS, Bida J, Zinsmeister AR, Tremaine WJ, Sandborn WJ. Predictive and protective factors associated with colorectal cancer in ulcerative colitis: a case-control study. Gastroenterology. 2006;130:1941 9
45 EXPERT INSIGHT ON MANAGING FRANCIS: Based on the diagnosis and prognosis for the patient, including the background risk of colorectal neoplasia The following factors for treatment were considered at the outset: Steroids with low systemic bioavailability (budesonide or beclomethasone) are recommended to avoid systemic toxicity. (23 ) As colonic release of the drug is important suppositories or foam are preferred and are better tolerated by patients than enemas, where available. (24) Response to steroids should be assessed after 4 8 weeks (22 ).The target is to obtain full symptom control (normal stools 1 2 times/day, no blood, no tenesmus) with mucosal healing (endoscopic Mayo sub-score=0/1, but ideally Mayo 0, as sustained remission is more frequent if Mayo 0 is reached versus Mayo 1). [EL3] (24, 25) If this target is not achieved, a purine analogue and/or biologic treatment should be discussed. Purine alone may be insufficient if the patient does not respond properly to steroid induction. Purine may be adapted in case of full disease control but with steroid-dependency. A biologic treatment would be adapted to both steroidrefractoriness or steroid-dependency. (26) [22] Panaccione R, Rutgeerts P, Sandborn WJ, Feagan B, Schreiber S, Ghosh S. Review article: treatment algorithms to maximize remission and minimize corticosteroid dependence in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2008;28: [23] Fasci Spurio F, Aratari A, Margagnoni G, Clemente V, Moretti A, Papi C. Low bioavailability and traditional systemic steroids in IBD: can the former take over the latter? J Gastrointestin Liver Dis. 2013;22:65 71 [24] Ruddell WS, Dickinson RJ, Dixon MF, Axon AT. Treatment of distal ulcerative colitis(proctosigmoiditis) in relapse: comparison of hydrocortisone enemas and rectal hydrocortisone foam. Gut. 1980;21: [25] Boal Carvalho P, Dias de Castro F, Rosa B, Moreira MJ, Cotter J. Mucosal healing in ulcerative colitis -when zero is better. J Crohns Colitis. 2016;10:20 25 [26] Dignass A, Lindsay JO, Sturm A, Windsor A, Colombel JF, Allez M, et al. Second European evidence - based consensus on the diagnosis and management of ulcerative colitis part 2: current management. J Crohns Colitis. 2012;6:
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND. Fabrizio Parente
 NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
Op#mizing)Management)in)IBD:) Mucosal)Healing)
Management)in)IBD:) Mucosal)Healing)") Op#mizing)Management)in)IBD:) Mucosal)Healing) Vipul&Jairath&MD&PhD& Associate&Professor&of&Medicine,&Epidemiology&and& Biosta=s=cs& Western&University&&& Division&of&Gastroenterology,&& London&Health&Sciences&Network&
Op#mizing)Management)in)IBD:) Mucosal)Healing) Vipul&Jairath&MD&PhD& Associate&Professor&of&Medicine,&Epidemiology&and& Biosta=s=cs& Western&University&&& Division&of&Gastroenterology,&& London&Health&Sciences&Network&
Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis
 Alimentary Pharmacology and Therapeutics Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis G. R. Lichtenstein*,
Alimentary Pharmacology and Therapeutics Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis G. R. Lichtenstein*,
Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA
 Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA Endpoints Overview Hospitalization Surgery Colorectal cancer
Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA Endpoints Overview Hospitalization Surgery Colorectal cancer
Crohn disease is a chronic inflammatory bowel disease
 GASTROENTEROLOGY 2010;139:1147 1155 Risk Factors Associated With Progression to Intestinal Complications of Crohn s Disease in a Population-Based Cohort KELVIN T. THIA,*, WILLIAM J. SANDBORN,* WILLIAM
GASTROENTEROLOGY 2010;139:1147 1155 Risk Factors Associated With Progression to Intestinal Complications of Crohn s Disease in a Population-Based Cohort KELVIN T. THIA,*, WILLIAM J. SANDBORN,* WILLIAM
Disease behavior in adult patients- are there predictors for stricture or fistula formation?
 Disease behavior in adult patients- are there predictors for stricture or fistula formation? Falk Symposium 168, Madrid, Spain Iris Dotan, M.D., Head, IBD Center, Department of Gastroenterology and Liver
Disease behavior in adult patients- are there predictors for stricture or fistula formation? Falk Symposium 168, Madrid, Spain Iris Dotan, M.D., Head, IBD Center, Department of Gastroenterology and Liver
Crohn s disease is a chronic recurrent inflammation of the
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:1430 1438 Clinical Course in Crohn s Disease: Results of a Norwegian Population-Based Ten-Year Follow-Up Study INGER CAMILLA SOLBERG,* MORTEN H. VATN, OLE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:1430 1438 Clinical Course in Crohn s Disease: Results of a Norwegian Population-Based Ten-Year Follow-Up Study INGER CAMILLA SOLBERG,* MORTEN H. VATN, OLE
Mucosal Healing in Ulcerative Colitis When Zero is Better
 Journal of Crohn's and Colitis, 2016, 20 25 doi:10.1093/ecco-jcc/jjv180 Advance Access publication October 5, 2015 Original Article Original Article Mucosal Healing in Ulcerative Colitis When Zero is Better
Journal of Crohn's and Colitis, 2016, 20 25 doi:10.1093/ecco-jcc/jjv180 Advance Access publication October 5, 2015 Original Article Original Article Mucosal Healing in Ulcerative Colitis When Zero is Better
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals
 Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker
Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Personalized Medicine in IBD: Where Are We in 2013
 Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation
 ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis
 Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University JKM 2014 Svartz N. Acta Med Scand
Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University JKM 2014 Svartz N. Acta Med Scand
As clinicians we would all agree that the goal for our
 CURRENT CONTROVERSIES: PRO, CON, AND BALANCE Controversies in Mucosal Healing in Ulcerative Colitis Sunanda Kane, MD,* Frances Lu, MD, Asher Kornbluth, MD, Dahlia Awais, MD, and Peter D.R. Higgins, MD,
CURRENT CONTROVERSIES: PRO, CON, AND BALANCE Controversies in Mucosal Healing in Ulcerative Colitis Sunanda Kane, MD,* Frances Lu, MD, Asher Kornbluth, MD, Dahlia Awais, MD, and Peter D.R. Higgins, MD,
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Clinical Predictors of Colectomy in Patients with Ulcerative Colitis: Systematic Review and Meta-analysis of Cohort Studies
 Journal of Crohn's and Colitis, 2015, 156 163 doi:10.1093/ecco-jcc/jju016 Advance Access publication December 10, 2014 Original Article Original Article Clinical Predictors of Colectomy in Patients with
Journal of Crohn's and Colitis, 2015, 156 163 doi:10.1093/ecco-jcc/jju016 Advance Access publication December 10, 2014 Original Article Original Article Clinical Predictors of Colectomy in Patients with
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
FERRING PHARMACEUTICALS. Enjoy The simple COR/939/2014/CH3
 Enjoy The simple pleasures of life COR/939/2014/CH3 Ulcerative colitis disrupts the simple pleasures in life Patients with ulcerative colitis may live with a considerable symptom burden despite medical
Enjoy The simple pleasures of life COR/939/2014/CH3 Ulcerative colitis disrupts the simple pleasures in life Patients with ulcerative colitis may live with a considerable symptom burden despite medical
Guided by Dr. Michal Amitai Head of Abdominal Imaging Department of Diagnostic Imaging Sheba Medical Center Sackler School of Medicine, Tel Aviv
 Guided by Dr. Michal Amitai Head of Abdominal Imaging Department of Diagnostic Imaging Sheba Medical Center Sackler School of Medicine, Tel Aviv University 1 SHARE study My year Collaboration between gastroenterology
Guided by Dr. Michal Amitai Head of Abdominal Imaging Department of Diagnostic Imaging Sheba Medical Center Sackler School of Medicine, Tel Aviv University 1 SHARE study My year Collaboration between gastroenterology
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Title: Accuracy of calprotectin in evaluating sub- clinical inflammation in Ulcerative
 PROTOCOL ACERTIVE STUDY Title: Accuracy of calprotectin in evaluating sub- clinical inflammation in Ulcerative colitis (ACERTIVE) Sponsor: Portuguese IBD Study Group (Grupo de Estudos da Doença Inflamatória
PROTOCOL ACERTIVE STUDY Title: Accuracy of calprotectin in evaluating sub- clinical inflammation in Ulcerative colitis (ACERTIVE) Sponsor: Portuguese IBD Study Group (Grupo de Estudos da Doença Inflamatória
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases?
 How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
Clinical Study Clinical Study of the Relation between Mucosal Healing and Long-Term Outcomes in Ulcerative Colitis
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2013, Article ID 192794, 6 pages http://dx.doi.org/10.1155/2013/192794 Clinical Study Clinical Study of the Relation between
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2013, Article ID 192794, 6 pages http://dx.doi.org/10.1155/2013/192794 Clinical Study Clinical Study of the Relation between
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Response to First Intravenous Steroid Therapy Determines the Subsequent Risk of Colectomy in Ulcerative Colitis Patients
 Response to First Intravenous Steroid Therapy Determines the Subsequent Risk of Colectomy in Ulcerative Colitis Patients Tamás Molnár 1, Klaudia Farkas 1, Tibor Nyári 2, Zoltán Szepes 1, Ferenc Nagy 1,
Response to First Intravenous Steroid Therapy Determines the Subsequent Risk of Colectomy in Ulcerative Colitis Patients Tamás Molnár 1, Klaudia Farkas 1, Tibor Nyári 2, Zoltán Szepes 1, Ferenc Nagy 1,
Ulcerative colitis (UC) is a. The Patient with Newly Diagnosed Ulcerative Colitis: Anticipating the Questions and Individualizing the Answers
 is a. The Patient with Newly Diagnosed Ulcerative Colitis: Anticipating the Questions and Individualizing the Answers") The Patient with Newly Diagnosed Ulcerative Colitis: Anticipating the Questions and Individualizing the Answers James Gregor, MD, Division of Gastroenterology, The University of Western Ontario, London,
The Patient with Newly Diagnosed Ulcerative Colitis: Anticipating the Questions and Individualizing the Answers James Gregor, MD, Division of Gastroenterology, The University of Western Ontario, London,
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Endoscopy in IBD. F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M.
 Frankfurt/M.") F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts
 Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Cancer Risk with IBD Therapies How to Discuss with your Patients?
 Cancer Risk with IBD Therapies How to Discuss with your Patients? Douglas L Nguyen, MD Assistant Clinical Professor of Medicine University of California, Irvine Medical Center H.H. Chao Comprehensive Digestive
Cancer Risk with IBD Therapies How to Discuss with your Patients? Douglas L Nguyen, MD Assistant Clinical Professor of Medicine University of California, Irvine Medical Center H.H. Chao Comprehensive Digestive
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Narrow band imaging efficiency in evaluation of mucosal healing/ relapse of ulcerative colitis
 Original article Narrow band imaging efficiency in evaluation of mucosal healing/ relapse of ulcerative colitis Authors Seiko Sasanuma 1, Kazuo Ohtsuka 1, 2, Shin-ei Kudo 1, Noriyuki Ogata 1, Yasuharu
Original article Narrow band imaging efficiency in evaluation of mucosal healing/ relapse of ulcerative colitis Authors Seiko Sasanuma 1, Kazuo Ohtsuka 1, 2, Shin-ei Kudo 1, Noriyuki Ogata 1, Yasuharu
Inflammatory Bowel Disease: Clinical updates. Dr Jeff Chao Princess Alexandra Hospital
 Inflammatory Bowel Disease: Clinical updates Dr Jeff Chao Princess Alexandra Hospital Inflammatory bowel disease 2017 Clinical updates and future directions Pathogenesis Treatment targets Therapeutic agents
Inflammatory Bowel Disease: Clinical updates Dr Jeff Chao Princess Alexandra Hospital Inflammatory bowel disease 2017 Clinical updates and future directions Pathogenesis Treatment targets Therapeutic agents
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Endoscopy in Inflammatory Bowel Disease DR. REENA KHANNA
 Endoscopy in Inflammatory Bowel Disease DR. REENA KHANNA ASSISTANT PROFESSOR, UNIVERSITY OF WESTERN ONTARIO Background Clinical trials in ulcerative colitis and Crohn s disease require validated instruments
Endoscopy in Inflammatory Bowel Disease DR. REENA KHANNA ASSISTANT PROFESSOR, UNIVERSITY OF WESTERN ONTARIO Background Clinical trials in ulcerative colitis and Crohn s disease require validated instruments
Advances in Inflammatory Bowel Diseases. Regional Institute of Gastroenterology and Hepatology Octavian Fodor Cluj-Napoca, Romania
 Chapter 01 Inflammatory Bowel Diseases: Epidemiology and Natural History Roxana Zaharie 1,2 and Florin Zaharie 1,2 * 1 University of Medicine and Pharmacy Iuliu Hatieganu Cluj-Napoca, Romania 2 Regional
Chapter 01 Inflammatory Bowel Diseases: Epidemiology and Natural History Roxana Zaharie 1,2 and Florin Zaharie 1,2 * 1 University of Medicine and Pharmacy Iuliu Hatieganu Cluj-Napoca, Romania 2 Regional
Lewis Score Prognostic Value in Patients with Isolated Small Bowel Crohn s Disease
 Journal of Crohn's and Colitis Advance Access published October 9, 2015 Journal of Crohn's and Colitis, 2015, 1 6 doi:10.1093/ecco-jcc/jjv166 Original Article Original Article Lewis Score Prognostic Value
Journal of Crohn's and Colitis Advance Access published October 9, 2015 Journal of Crohn's and Colitis, 2015, 1 6 doi:10.1093/ecco-jcc/jjv166 Original Article Original Article Lewis Score Prognostic Value
What do we need for diagnosis of IBD
 What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease
 5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center University it of Chicago Medical
5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center University it of Chicago Medical
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Fibrotic complications of inflammatory bowel disease
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fibrotic complications of inflammatory bowel disease Gerhard Rogler, Department of Gastroenterology
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fibrotic complications of inflammatory bowel disease Gerhard Rogler, Department of Gastroenterology
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital
 IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
Evaluation of the severity of ulcerative colitis using endoscopic dual red imaging targeting deep vessels
 Evaluation of the severity of ulcerative colitis using endoscopic dual red imaging targeting deep vessels Authors Makoto Naganuma 1, 2, Naohisa Yahagi 3,RiekoBessho 1, Keiko Ohno 1, Mari Arai 1, Makoto
Evaluation of the severity of ulcerative colitis using endoscopic dual red imaging targeting deep vessels Authors Makoto Naganuma 1, 2, Naohisa Yahagi 3,RiekoBessho 1, Keiko Ohno 1, Mari Arai 1, Makoto
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Long-term outcome after infliximab for refractory ulcerative colitis
 Journal of Crohn's and Colitis (2008) 2, 219 225 available at www.sciencedirect.com Long-term outcome after infliximab for refractory ulcerative colitis Marc Ferrante a, Séverine Vermeire a, Herma Fidder
Journal of Crohn's and Colitis (2008) 2, 219 225 available at www.sciencedirect.com Long-term outcome after infliximab for refractory ulcerative colitis Marc Ferrante a, Séverine Vermeire a, Herma Fidder
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
Scheduled Maintenance Therapy with Infliximab Improves the Prognosis of Crohn s Disease: A Single Center Prospective Cohort Study in Japan
 Tohoku J. Exp. Med., 2010, 220, 207-215 Infliximab Improves the Prognosis of Crohn s Disease 207 Scheduled Maintenance Therapy with Infliximab Improves the Prognosis of Crohn s Disease: A Single Center
Tohoku J. Exp. Med., 2010, 220, 207-215 Infliximab Improves the Prognosis of Crohn s Disease 207 Scheduled Maintenance Therapy with Infliximab Improves the Prognosis of Crohn s Disease: A Single Center
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Agenda. Predictive markers in IBD. Management of ulcerative colitis. Management of Crohn s disease
 Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
TREATMENT OF INPATIENTS WITH ACUTE SEVERE ULCERATIVE COLITIS
 TREATMENT OF INPATIENTS WITH ACUTE SEVERE ULCERATIVE COLITIS Target Audience: Physicians, Physician Assistants, Nurse Practitioners and Nurses impacted by the protocol. Scope/Patient Population: All adult
TREATMENT OF INPATIENTS WITH ACUTE SEVERE ULCERATIVE COLITIS Target Audience: Physicians, Physician Assistants, Nurse Practitioners and Nurses impacted by the protocol. Scope/Patient Population: All adult
CRC and Dysplasia in IBD: Objectives of Talk. Colorectal Cancer and Dysplasia in IBD: A Case-Based Approach. Page 1
 Colorectal Cancer and in IBD: A Case-Based Approach Fernando Velayos MD MPH Associate Director of Translational Research University of California, San Francisco Center for Crohn s s and Colitis CRC and
Colorectal Cancer and in IBD: A Case-Based Approach Fernando Velayos MD MPH Associate Director of Translational Research University of California, San Francisco Center for Crohn s s and Colitis CRC and
High Percentage of IBD Patients with Indefinite Fecal Calprotectin Levels: Additional Value of a Combination Score
 Dig Dis Sci (2017) 62:465 472 DOI 10.1007/s10620-016-4397-6 ORIGINAL ARTICLE High Percentage of IBD Patients with Indefinite Fecal Calprotectin Levels: Additional Value of a Combination Score Alexander
Dig Dis Sci (2017) 62:465 472 DOI 10.1007/s10620-016-4397-6 ORIGINAL ARTICLE High Percentage of IBD Patients with Indefinite Fecal Calprotectin Levels: Additional Value of a Combination Score Alexander
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
Endpoints for Stopping Treatment in UC
 Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Title: Author: Journal:
 IMPORTANT COPYRIGHT NOTICE: This electronic article is provided to you by courtesy of Ferring Pharmaceuticals. The document is provided for personal usage only. Further reproduction and/or distribution
IMPORTANT COPYRIGHT NOTICE: This electronic article is provided to you by courtesy of Ferring Pharmaceuticals. The document is provided for personal usage only. Further reproduction and/or distribution
Early Mucosal Healing With Infliximab Is Associated With Improved Longterm Clinical Outcomes in Ulcerative Colitis
 GASTROENTEROLOGY 2011;141:1194 1201 Early Mucosal Healing With Infliximab Is Associated With Improved Longterm Clinical Outcomes in Ulcerative Colitis JEAN FRÉDÉRIC COLOMBEL,* PAUL RUTGEERTS, WALTER REINISCH,
GASTROENTEROLOGY 2011;141:1194 1201 Early Mucosal Healing With Infliximab Is Associated With Improved Longterm Clinical Outcomes in Ulcerative Colitis JEAN FRÉDÉRIC COLOMBEL,* PAUL RUTGEERTS, WALTER REINISCH,
Research Article Correlation between Histological Activity and Endoscopic, Clinical, and Serologic Activities in Patients with Ulcerative Colitis
 Gastroenterology Research and Practice Volume 16, Article ID 58351, 7 pages http://dx.doi.org/1.1155/16/58351 Research Article Correlation between Histological Activity and Endoscopic, Clinical, and Serologic
Gastroenterology Research and Practice Volume 16, Article ID 58351, 7 pages http://dx.doi.org/1.1155/16/58351 Research Article Correlation between Histological Activity and Endoscopic, Clinical, and Serologic
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Low Bioavailability and Traditional Systemic Steroids in IBD: Can the Former Take Over the Latter?
 REVIEWS Low Bioavailability and Traditional Systemic Steroids in IBD: Can the Former Take Over the Latter? Federica Fascì Spurio, Annalisa Aratari, Giovanna Margagnoni, Valeria Clemente, Alessandra Moretti,
REVIEWS Low Bioavailability and Traditional Systemic Steroids in IBD: Can the Former Take Over the Latter? Federica Fascì Spurio, Annalisa Aratari, Giovanna Margagnoni, Valeria Clemente, Alessandra Moretti,
ORIGINAL ARTICLE. Abstract. Introduction
 ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 1-5 Effectiveness of adalimumab for ambulatory ulcerative colitis patients after failure of infliximab treatment: a first real-life experience in
ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 1-5 Effectiveness of adalimumab for ambulatory ulcerative colitis patients after failure of infliximab treatment: a first real-life experience in
Diagnostic techniques for surveillance of dysplasia
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Diagnostic techniques for surveillance of dysplasia Gerhard Rogler, Department of Gastroenterology
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Diagnostic techniques for surveillance of dysplasia Gerhard Rogler, Department of Gastroenterology
Changing treatment paradigms for the management of inflammatory bowel disease
 REVIEW Korean J Intern Med 2018;33:28-35 Changing treatment paradigms for the management of inflammatory bowel disease Jong Pil Im 1, Byong Duk Ye 2, You Sun Kim 3, and Joo Sung Kim 1 1 Department of Internal
REVIEW Korean J Intern Med 2018;33:28-35 Changing treatment paradigms for the management of inflammatory bowel disease Jong Pil Im 1, Byong Duk Ye 2, You Sun Kim 3, and Joo Sung Kim 1 1 Department of Internal
Clinical Efficacy of Beclomethasone Dipropionate in Korean Patients with Ulcerative Colitis
 Original Article Yonsei Med J 2017 Jan;58(1):144-149 pissn: 0513-5796 eissn: 1976-2437 Clinical Efficacy of Beclomethasone Dipropionate in Korean Patients with Ulcerative Colitis Yoon Jee Lee, Jae Hee
Original Article Yonsei Med J 2017 Jan;58(1):144-149 pissn: 0513-5796 eissn: 1976-2437 Clinical Efficacy of Beclomethasone Dipropionate in Korean Patients with Ulcerative Colitis Yoon Jee Lee, Jae Hee
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Trends in Biologic Therapy for Crohn s Disease: Where Are We and Where Are We Going? CME
 Trends in Biologic Therapy for Crohn s Disease: Where Are We and Where Are We Going? CME Uma Mahadevan-Velayos, MD Supported by independent educational grants from View this activity online at: medscape.org/column/crohns
Trends in Biologic Therapy for Crohn s Disease: Where Are We and Where Are We Going? CME Uma Mahadevan-Velayos, MD Supported by independent educational grants from View this activity online at: medscape.org/column/crohns
TREATMENT OF INPATIENTS WITH ACUTE SEVERE ULCERATIVE COLITIS
 TREATMENT OF INPATIENTS WITH ACUTE SEVERE ULCERATIVE COLITIS Target Audience: Physicians, Physician Assistants, Nurse Practitioners and Nurses impacted by the protocol. Scope/Patient Population: All adult
TREATMENT OF INPATIENTS WITH ACUTE SEVERE ULCERATIVE COLITIS Target Audience: Physicians, Physician Assistants, Nurse Practitioners and Nurses impacted by the protocol. Scope/Patient Population: All adult
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
children Crohn s disease in MR enterography for GI Complications Microscopy Characterization Primary sclerosing cholangitis Anorectal fistulae
 MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease
 Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease Mark Lazarev, MD Summary Inflammatory bowel disease (IBD) is a complex disease that is costly both in terms of medical costs
Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease Mark Lazarev, MD Summary Inflammatory bowel disease (IBD) is a complex disease that is costly both in terms of medical costs
The role of endoscopy in inflammatory bowel disease
 European Review for Medical and Pharmacological Sciences The role of endoscopy in inflammatory bowel disease M. DAPERNO, R. SOSTEGNI, A. LAVAGNA, L. CROCELLÀ, E. ERCOLE, C. RIGAZIO, R. ROCCA, A. PERA Center
European Review for Medical and Pharmacological Sciences The role of endoscopy in inflammatory bowel disease M. DAPERNO, R. SOSTEGNI, A. LAVAGNA, L. CROCELLÀ, E. ERCOLE, C. RIGAZIO, R. ROCCA, A. PERA Center
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Outcomes of immunosuppressors and biologic drugs in inflammatory bowel diseases: a real life experience
 Outcomes of immunosuppressors and biologic drugs in inflammatory bowel Treatments and therapeutic approaches in IBD are constantly evolving. The newly emerged biologic treatments are one such evolving
Outcomes of immunosuppressors and biologic drugs in inflammatory bowel Treatments and therapeutic approaches in IBD are constantly evolving. The newly emerged biologic treatments are one such evolving
PLEASE SCROLL DOWN FOR ARTICLE
 This article was downloaded by: [UIO University Of Oslo] On: 29 August 2009 Access details: Access Details: [subscription number 906401845] Publisher Informa Healthcare Informa Ltd Registered in England
This article was downloaded by: [UIO University Of Oslo] On: 29 August 2009 Access details: Access Details: [subscription number 906401845] Publisher Informa Healthcare Informa Ltd Registered in England
IBD Case Studies. David Rowbotham. Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital
 IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives