LOWER LIMB DOPPLER ULTRASOUND FOR THE STUDY OF VENOUS INSUFFICIENCY
|
|
|
- Prosper Stafford
- 6 years ago
- Views:
Transcription
1 Revista Chilena de Radiología. 2009; 15(4): -. 1 LOWER LIMB DOPPLER ULTRASOUND FOR THE STUDY OF VENOUS INSUFFICIENCY Dr. Paola Paolinelli G. Diagnostic Imaging Service, Clinica Las Condes, Santiago, Chile. Abstract Venous insufficiency is defined as an impaired venous return, which affects the superficial or the deep system, or both.this condition may be caused either by an alteration in the muscle pump, a venous obstruction, a valvular incompetente, or right-sided heart failure. It translates into a dynamic venous hypertension manifested through the development of varicose veins or trophic skin changes. The surface failure is due to the presence of veno-venous shunts, which provoke a flow loss from the deep system through a vanishing point and then returns through another entry point. The study is performed with the patient in standing position, by stimulation of muscle pump through various exercises or increasing central pressure with Valsalva maneuver. The mapping is a graphic expression of the study and must show the type of shunt, location, and pattern of varicose veins. Keywords: Venous Doppler exam, Venous insufficiency, Venous mapping, Venovenous shunts, Ultrasound. Paolinelli P et al. Ultrasonido Doppler de extremidades inferiores para el estudio de la insuficiencia venosa. Rev Chil Radiol (4): Corresponding author: Dr. Paola Paolinelli G. ppaolinelli@clinicalascondes.cl Received 27 October 2009, accepted 20 November 2009.
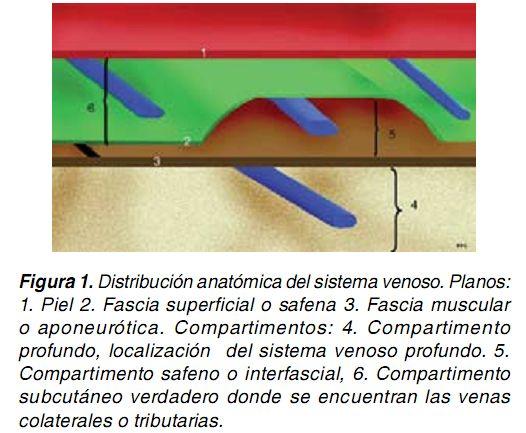
2 Revista Chilena de Radiología. 2009; 15(4): -. 2 Introduction Venous insufficiency is a highly prevalent condition clinically manifested by the presence of varicose veins, telangiectasias, skin trophic changes, and ulcers. Color Doppler exam has proven to be a useful tool for the study of venous insufficiency and its consequences, by determining the source of reflux, the relationship between different venous systems, and the detection of anatomical variants. A properly conducted study is very useful for surgeons in treatment planning. Therefore, knowing in detail the anatomy and its variants, the physiopathology and presentation patterns of disease, is of vital importance. I. Normal anatomy and variants The venous system is divided into three sections: deep, superficial, and communicating systems (1). (a) Deep system Also called primary network (2), is located in the deep compartment under the muscular fascia or deep fascia and follows a path parallel to the arteries. (b) Surface System (1) It comprises interconnected venous structures that drain into two major veins: the internal saphenous vein or great saphenous, and the small saphenous or external saphenous vein. The subcutaneous space, where superficial veins are to be found, is separated by a membrane termed superficial or venous fascia, in a deeper subcutaneous site located between superficial fascia and muscle fascia (called interfascial or saphenous compartment), and a truly subcutaneous compartment between the fascia and the skin (Figure 1). Figure 1. Anatomic distribution of venous system. Planes: (1) Skin. (2) Superficial or saphenous fascia. (3) Aponeurotic or muscle fascia. Compartments: (4) Deep compartment, location of deep venous system. (5) Saphenous or interfascial compartment. (6) Truly subcutaneous compartment, where collateral or tributaries veins are to be found.
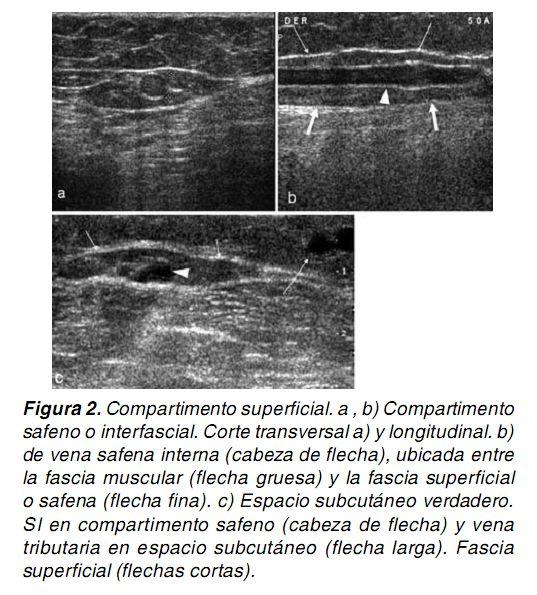
3 Revista Chilena de Radiología. 2009; 15(4): -. 3 Saphenous compartment contains the secondary network (2), which comprises the internal and external saphenous veins, the anterior accessory saphenous vein, the thigh extension of the external saphenous vein (also known as vein of Giacomini, femoropopliteal vein or anastomotic magna), the medial and lateral marginal veins of the foot, and the dorsal venous arch of the foot. Through ultrasound (US) exam it is easily recognized by its biconvex appearance limited by the fascias, the so-called "saphenous eye sign" (Figure 2a) given that its configuration resembles this organ. Figure 2. Superficial compartment. (a, b) Saphenous or interfascial compartment. Transverse cross-section ( a) and longitudinal section (b) of internal saphenous vein ( arrowhead), located between the muscle fascia (thick arrow) and superficial or saphenous fascia (thin arrow). (c) Truly subcutaneous space. Internal saphenous vein in saphenous compartment ( arrowhead) and tributary vein in subcutaneous space (long arrow). Superficial fascia (short arrows). Tertiary network is located in the truly subcutaneous space (2), which comprises tributaries or collateral veins (Figure 2c). Any venous structure located in this compartment should be considered as collateral or tributary veins. Location has a physiological importance since as a result of being in an open compartment they are more likely to suffer strain, unlike the saphenous veins. (c) Communicating or perforating system Formed by veins running through the muscle fascia, draining venous flow from the surface into the deep system (Figure 3). Anatomy of the superficial and perforating systems, as well as superficial tributaries, will be thoroughly reviewed. Figure 3. Communicating or perforating vein that perforates the muscle fascia (arrows), with normal flow from the superficial to the deep system.
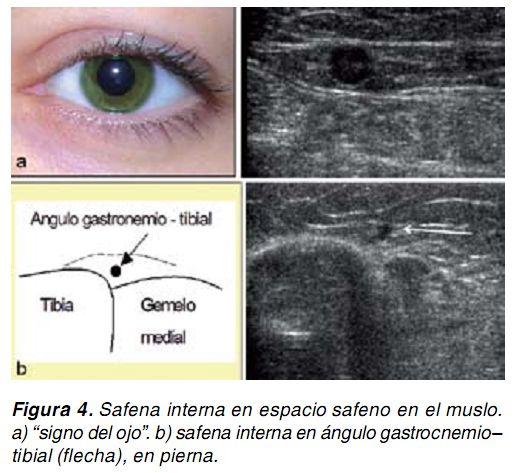
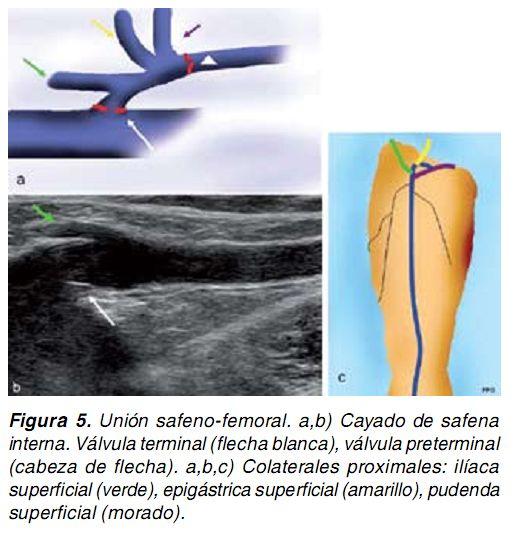
4 Revista Chilena de Radiología. 2009; 15(4): -. 4 SUPERFICIAL VEINS 1. Internal saphenous system (GSV) It extends from the anterior aspect of the medial malleollus as a continuation of the medial marginal vein of foot, ascends through the medial aspect of the leg and thigh to reach the saphenous-femoral junction (SFJ) at groin. It is located in the saphenous or interfascial compartment, with its typical appearance in the thigh (sign of the eye) (Figure 4a), and in the leg it lies in the gastrocnemiustibial angle (Figure 4b), co vered by the superficial fascia. This fascia may be difficult to identify in exceedingly thin patients or in knee and ankle. Deep system drainage It occurs at the saphenofemoral junction or arch of the internal saphenous vein, which is located in the inguinal region. Adjacent to the ostium, it presents a terminal valve, that is usually easily visualized, and a preterminal valve, a further 2 cm distal which marks the distal area of the SFJ. Tributaries or collateral veins open between these two valves (1) (Figure 5). Figure 4. (a) Internal saphenous vein in saphenous space in the thigh. "Eye sign". (b) Internal saphenous vein in gastrocnemius-tibial angle (arrow) in leg. Figure 5. Saphenous-femoral junction. (a, b) Arch of internal saphenous vein. Terminal valve (white arrow), preterminal valve (arrowhead). (a, b, c) Proximal collateral veins: superficial iliac vein (green), superficial epigastric vein (yellow), superficial pudendal vein (purple). Tributary or collateral veins Internal saphenous vein is often accompanied by parallel veins of different sizes which might be confused with the very same saphenous vein or regarded as a double saphenous vein, but they are easily distinguishable due to their location above the superficial fascia. There are relatively constant tributary veins: (a) Tributaries draining directly into the arch of the internal saphenous vein: Tributaries are classified into proximal and distal veins (1). Proximal veins drain the abdominal wall and pudendal areas, being divided into the superficial iliac,
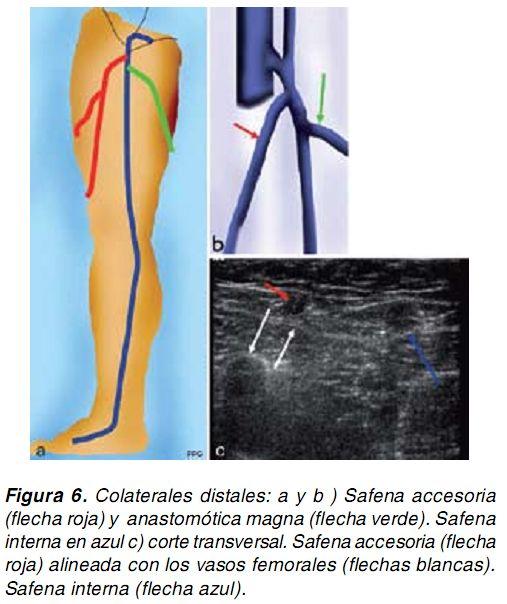
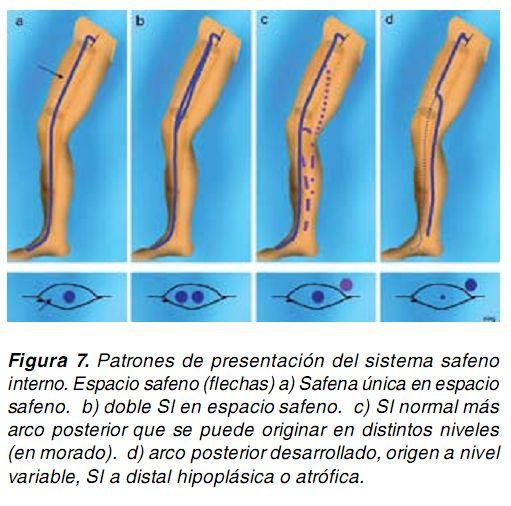
5 Revista Chilena de Radiología. 2009; 15(4): -. 5 the superficial epigastric, and superficial pudendal veins. (Figure 5). They are formed either by a single vein or by several venous channels. These veins are clinically relevant because they can cause reflux towards the internal saphenous vein, compromising the arc valve. Distal collateral veins are typically two: one lateral and one medial (Figure 6). The lateral is termed accessory saphenous vein and it is present in 40% of patients. It travels along the anterior aspect of the thigh and drains into the internal saphenous vein, adjacent to the sapheno-femoral junction, where a fairly constant lymph node can be found. It is easily recognizable and distinguishable from internal saphenous vein because it is aligned with the femoral vessels, in contrast to the internal saphenous vein, that lies medial to them (Figure 6c). It is very important to recognize and describe it, especially in varices with normal internal saphenous vein or in postoperative relapses. Figure 6. Distal collaterals: (a and b) Accessory saphenous vein (red arrow) and anastomotic magna (green arrow). Internal s aphenous vein in blue. (c) Cross-section. Accessory saphenous vein (red arrow) aligned with the femoral vessels (white arrows). Internal saphenous vein (blue arrow). The medial collateral vein, which usually binds distal to the preterminal valve, continues in the external saphenous vein along the posterior aspect of the thigh; it is called anastomotic magna or vein of Giacomini (Figure 8). There is another tributary vein, the central vein of the lymph node, which lies adjacent to the accessory saphenous vein. Occasionally, it may be incompetent and generate reflux towards the internal saphenous vein. (b) Tributaries draining into the internal saphenous vein One of the most consistent collateral veins corresponds to the so-called posterior arch, with wide variability in its drainage into the internal saphenous vein; it is often responsible for developing varicose veins in venous insufficiency. Patterns of presentation of the internal saphenous system Various different patterns of presentation of the internal saphenous system and its tributaries are recognized; they are grouped as follows (Figure 7):
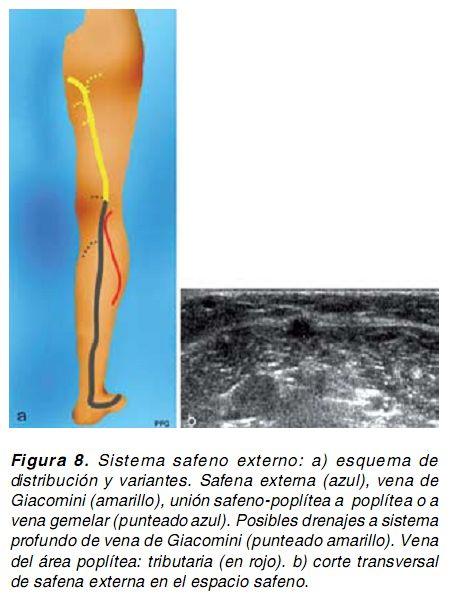
6 Revista Chilena de Radiología. 2009; 15(4): -. 6 (a) Unique saphenous vein running transversally in the interfascial compartment at thigh and leg level, with no tributaries identified (Figure 7a). (b) Presence of double internal saphenous vein in interfascial compartment, with variable extension into thigh and leg, with no collateral veins (Figure 7b). (c) Presence of normal internal saphenous vein in interfascial compartment, both in thigh and leg. The origin of the posterior tributary arc is variable at thigh, knee or leg level (Figure 7c). (d) Presentation similar to above, with hypoplasia or atrophy of the internal saphenous vein distal to tributary vein. Origin of the tributary may also be at thigh, knee or leg level (Figure 7d). The presence of accessory saphenous vein can be associated with any of these patterns. Figure 7. Patterns of presentation of the internal saphenous system. Saphenous space (arrows). (a) Unique saphenous vein in saphenous space. (b) Double internal saphenous vein in saphenous space. (c) Normal internal saphenous vein plus posterior arch that can arise at different levels (in purple). (d) Developed posterior arch with origin at variable level, internal saphenous vein distal to hypoplastic or atrophic vein. 2. External saphenous system (SSV) The external saphenous or small saphenous vein originates behind the lateral malleolus as a continuation of the lateral marginal vein of the foot (Figure 8) and ascends through the posterior aspect of the calf, between the two fascias, in the interfascial compartment (Figure 8b). It may appear doubled or triple d. Deep system drainage Drainage into the deep system is variable; it may present the following patterns: drainage into the popliteal vein through saphenous-popliteal junction in popliteal fossa or distal thigh (being the most common); drainage into the deep veins of the leg (gemelar veins) or continuation to the thigh through anastomotic magna, which opens into the proximal internal saphenous vein (most often), in veins of the gluteal area, in posterior perforating veins, posterolateral thigh perforating veins, or in several subcutaneous branches (Figure 8). In 2/3 of people who have the anastomotic magna, a saphenous-popliteal junction is not found (4).
7 Revista Chilena de Radiología. 2009; 15(4): -. 7 Figure 8. External saphenous system. (a) Distribution scheme and variants. External saphenous vein (in blue), vein of Giacomini ( in yellow), saphenous popliteal junction to popliteal vein or gemelar vein (blue dotted line). Possible drains of Giacomini vein into deep system ( yellow dotted line). Popliteal area vein: tributary ( in red). (b) Cross-section of external saphenous vein in saphenous space. Variants and Collaterals The vein of the popliteal area is an important superficial collateral that runs subcutaneously through the posterior aspect of the popliteal area, calf and leg, sometimes parallel to the external saphenous vein and drains into the popliteal vein, lateral to the saphenous popliteal junction. Veins can also be seen accompanying the sciatic nerve in the posterior aspect of the leg and thigh, which may be confused with the external saphenous vein (Figure 14d). 3. Veins of the foot The superficial system is also divided in two components: the dorsal venous arch and the medial and lateral marginal veins that give origin to the saphenous vein; they are located under the surperficial fascia, whereas collateral veins of the dorsum of the foot are located subcutaneously and continue onto the collateral veins of the leg. 4. Communicating or perforating veins The largest veins correspond to the archs of the internal saphenous and the external saphenous veins. Most of them drain the blood flow into the deep system ( entrance communicating veins). It is important to identify insufficient communicating veins with reverse flow. II. PHYSIOLOGY AND PHYSIOPATHOLOGY 1. Physiology The venous system acts as an important blood reservoir and conductor. It receives blood from the capillaries and takes it to the heart, against both gravity and a fluctuating thoracic-abdominal pressure; it lacks a pump of its own.to have an adequate drainage to the heart, a permeable venous system,
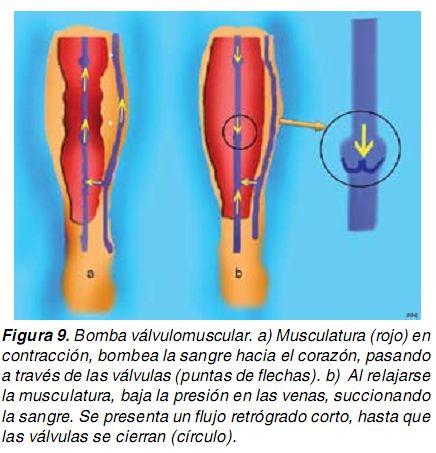
8 Revista Chilena de Radiología. 2009; 15(4): -. 8 undamaged valvular and muscular system (valve-muscle pump), and a preserved cardiac function are required (Figure 9). In standing position, the hydrostatic pressure of the dorsal veins of the foot would be that of the continuous column of blood running down from the right atrium to the foot if there were no valves interrupting and fractionating this migrating flow. When the muscles of lower extremities contract (muscular systole), pressure increases, thus pumping blood to the heart (Figure 9 a). By relaxing the muscles (muscular diastole), pressure falls producing reflux, which is hindered by the valves (Fi gure 9b); this is the phenomenon searched for when the study is performed in standing position. In this article the terms systole and diastole will not be used, as they might lead to confusion. The superficial system drains into the deep system through the archs and perforating and/or communicating veins to subsequently ascend through the deep system. Figure 9. Valvular muscular pump. (a) Contraction of muscles (in red) pumps blood to the heart, passing through the valves (arrowheads). (b) By relaxing the muscles, pressure in the veins is diminished, thus creating a sucking effect. A short retrograde flow occurs, process that continues until the valves close (circle). 2. Physiopathology Venous dysfunction is defined as an impaired venous return, which compromises the superficial system, the deep system, or both, whose cause may be alteration in the muscle pump, venous occlusion, valvular incompetence, or right heart failure. When the seal of a venous valve fails, hydrostatic pressure is transmitted in its entirety from the right atrium to the foot and blood reflux occurs, which determines the clinical manifestations of venous insufficiency, such as vascular dilation and dystrophic phenomena of the skin. Conceptually, the anterograde flow is defined as the one having physiological direction (towards the heart), whereas retrograde flow runs in opposite direction. The vanishing point is the site where blood flows from deep to superficial compartment and the entry point is the place where blood flows from the superficial to the deep compartment (1).
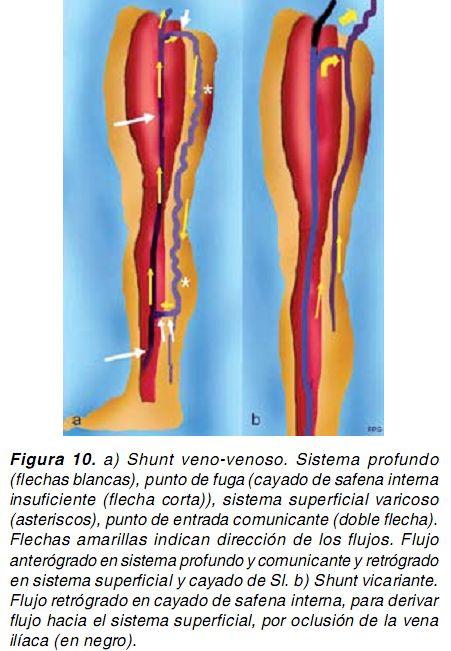
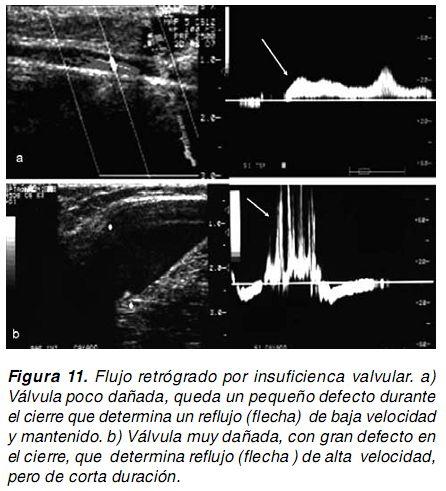
9 Revista Chilena de Radiología. 2009; 15(4): -. 9 The phenomenon of superficial insufficiency can be described as a venovenous shunt or retrograde loop, which comprises the vanishing point (e.g., the saphenous-femoral junction, or an insufficient perforating vein), an usually retrograde pathway, being varicose veins its visible part, and finally, a re-entry point to the deep venous system (via perforating veins) (2) (Figure 10a). This shunt may be activated during the contraction and/or muscle relaxation and has to be differentiated from other pathologies that may manifest similarly. A clear example of this is the vicarious flow that occurs in response to a venous occlusion, where the superficial system acts as a bridge or collateral pathway for allowing the blood flow to ascend (Figure 10b). Figure 10. (a) Veno-venous shunt. Deep system (white arrows), vanishing point (arch of the insufficient internal saphenous vein (short arrow)), varicose superficial system (asterisks), point of entry (double arrow). Yellow arrows indicate direction of flows. Antegrade flow in deep system and communicating veins; retrograde flow in superficial system and in the arch of internal saphenous vein. (b) Vicarious shunt. Retrograde flow in the arch of internal saphenous vein, to propel flow to the superficial system, by iliac vein occlusion (in black). Traditionally, reflux has been defined as the presence of retrograde flow with a duration > 0.5 sec (Van Bemmelen et al.) In fact, considering a fixed period of time can lead to error because characteristics of the reflux will depend on the state of the damaged valve. If damage is not so important and the closure defect is small, a long-duration and low-velocity reflux will occur (Figure 11a). On the contrary, if the damage is very severe, a short-duration and high-velocity reflux will take place (Figure 11b). Therefore, criteria for reflux include retrograde flow during muscle relaxation longer than 0.5 sec, or shorter if the velocity is greater than the anterograde velocity during muscle contraction (Figure 12). Figure 11. Retrograde flow due to valve insufficiency. (a) Slightly damaged valve, with a small defect at closure point which determines a sustained and low-velocity reflux (arrow). (b) Valve badly damaged, with large defect at closure point, which determines a high-velocity and short-duration reflux (arrow)
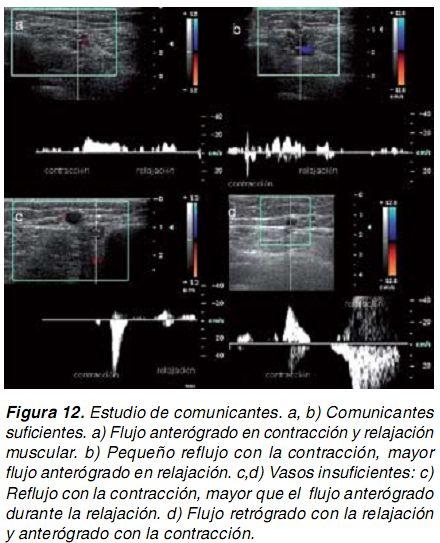
10 Revista Chilena de Radiología. 2009; 15(4): As explained above, perforating veins (or communicating veins) transmit the surface blood flow to the deep system ( antegrade flow). These veins may be insufficient, thus acting as vanishing points, and/or act as entry communicating veins, which are responsible for taking back to the deep system the flow that has escaped from it. When studied with Doppler US (3), they may have a continuous antegrade flow (Figure 12 a) or a slight retrograde flow during muscle contraction, whereas during relaxation it shows an antegrade flow greater than retrograde flow (Figure 12 b). When retrograde flow occurs during muscle relaxation (Figure 12d) or when retrograde flow during muscle contraction is greater than the antegrade flow during muscle relaxation (3) (Figure 12c), insufficient communicating vein is diagnosed. Figure 12. Study of communicating veins. (a, b) Sufficient communicating veins. (a) Antegrade flow in muscle contraction and relaxation. (b) Small reflux with contraction, greater antegrade flow during relaxation. (c, d) Insufficient vessels: (c) Reflux with contraction, greater than antegrade flow during relaxation. (d) Retrograde flow with relaxation and antegrade flow with contraction. III. PATTERNS OF SUPERFICIAL VENOUS INSUFFICIENCY To ensure a successful surgical treatment it is highly important to determine the anatomy and hemodynamic behavior of the venous system in order to identify which are the vanishing points that determine varices, re-entry points, and so forth. Generally, the disease presents repeated patterns among patients, alone or in combination, which can be grouped as follows (2,3): 1. Internal saphenous vein insufficiency (a) With insufficient arch (Figure 13a and b) - to the foot: rare to find - to the knee: most frequent; generally, the insufficiency continues through the posterior tributary vein to the lower leg (b) With sufficient arch: Reflux can be fed by (Figure 13c): - Collateral veins of the arch
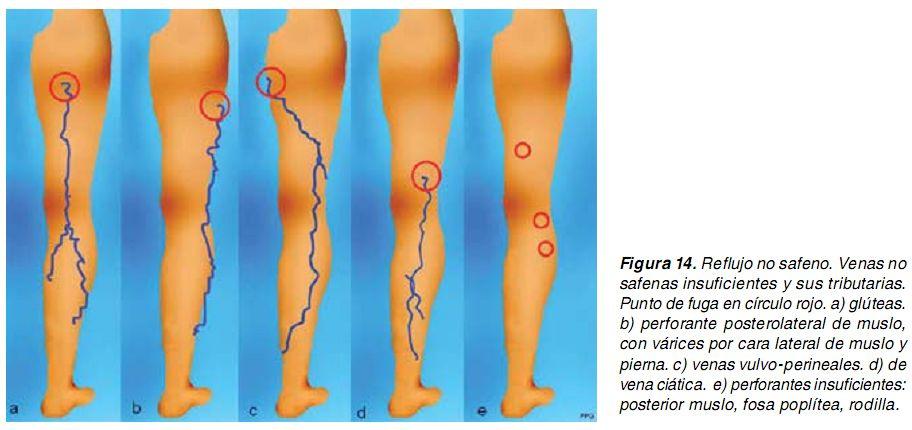
11 Revista Chilena de Radiología. 2009; 15(4): Thigh perforating veins - Anastomotic magna - Tributary vein coming from the external saphenous system. Extension towards the leg is variable and insufficiency of the accessory saphenous vein, with or without involvement of the internal saphenous vein, must be included. 2. Insufficiency of the external saphenous vein (Figure 13d) (a) From the insufficient arch (saphenous-popliteal junction), usually limited to the upper half of leg (b) With sufficient or absent arch; insufficiency coming from the anastomotic magna Figure 13. Patterns of internal saphenous system insufficiency. Internal Saphenous vein in blue, tributary veins in yellow. Red circles, vanishing points. Insufficient vessels, dotted lines. Entry communicating veins in green. (a) Insufficient internal saphenous vein from arch to the foot. (b) Insufficiency from the arch to tributary vein, which continues insufficient. Distally, the internal saphenous vein is normal. This is the commonest pattern. (c) Sufficient arch. Vanishing point from tributary veins: arch collateral veins (1), Giacomini vein (2), vulvoperineal veins (3), of external saphenous (4). Variable to distal. (d) External saphenous vein. Insufficiency due to arch or vein of Giacomini (less frequently seen). 3. Non-saphenous reflux (Figure 14) Is the one that primarily does not compromise the saphenous system, but may be connected to it. It is rare in men, predominantly found in women due to their own etiologic mechanisms (5) such as pregnancy and hormone load. They are varicose veins that originate from vulvo-perineal, gluteal, and intrapelviana regions, ( due to insufficient ovarian veins), and also because of perforating and sciatic veins. They are located in lateral and posterior thigh, popliteal fossa, and lateral knee. IV. ULTRASONOGRAPHY The objective of vascular Doppler study is to confirm venous permeability, identify the type of venous insufficiency (deep, superficia l, and/or of
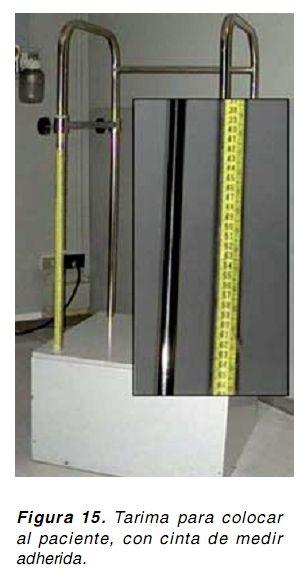
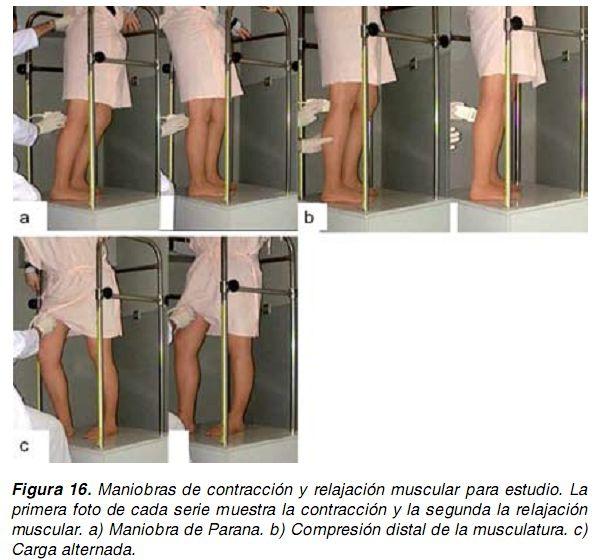
12 Revista Chilena de Radiología. 2009; 15(4): communicating veins), determine the points of reflux/entry, and perform the vein mapping (graphic expression of the study) as follows: 1. Discard thrombosis The study begins with patient in semisitting or standing position, with graduated compression of venous structures, recording variability of the curve in common femoral vein to discard iliac axis occlusion. Through this procedure we discard that a retrograde flow pattern actually may correspond to a vicarious flow (Figure 10b). 2. Detection of insufficiency (for deep, superficial, and communicating systems) It is performed in a standing position; the patient is placed on a protected platform with a system for measuring the height of insufficient communicating veins (Figure 15). Figure 14. Non-saphenous reflux. Insufficient non-saphenous veins and their tributaries. Vanishing point in red circle. (a) Glutes. (b) Posterolateral thigh perforating veins, with varices on the lateral aspect of the thigh and leg. (c) Vulvoperineal veins. (d) Sciatic vein. (e) Insufficient perforating veins: posterior thigh, popliteal fossa, knee. To force a retrograde flow in order to check indemnity of valves, thoracoabdominal pressure can be increased or contraction and relaxation of lower limb muscles can be induced: - Increase of thoracoabdominal pressure: Valsalva maneuver is employed. It is useful in veins above the knee. - Contraction (systole) followed by muscle relaxation (diastole): muscles act as a sponge, forcing blood to fall in diastole to test the valves (Figure 16). It can be obtained through different techniques: - Parana Maneuver, technique where a standing patient is slightly pushed offbalance ( forward or backward) to cause muscle contraction for maintaining balance, followed by muscle relaxation. - Alternating weight-bearing in extremities: patient bears his/her weight on the extremity under study, and then on the other limb.
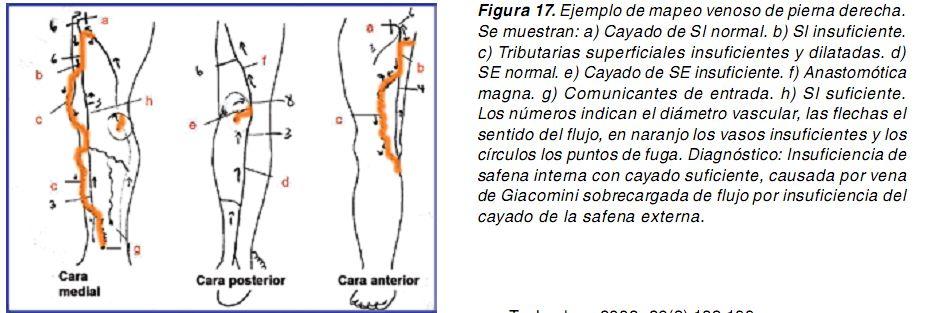
13 Revista Chilena de Radiología. 2009; 15(4): Voluntary muscle contraction - Dorsiflexion of the toes: the most comfortable technique for both patient and operator. - Distal compression applied with the hand To obtain more reliable information, one maneuver or a combination of them may be carried out. At Doppler examination, the first stage of contraction or muscle compression manifests as an upward flow jet, and in the second phase ( relaxation) reflux becomes evident (Figure 12). Assessment of incompetent communicating veins is performed similarly, recording their location in centimeters in relation to the ground (more objective than related to the malleolus) by using a measuring tape attached to the board, or by marking directly on the skin. Figure 15. Board to place the patient, with tape measure attached to it. 3. Vein mapping A diagram showing vanishing points, venous flow direction, varicose packages, communicating at entry, and insufficient veins, has to be drawn. It is recommended to register vein diameters and to mark which vessels are insufficient ( registering height), besides drawing arrows to show blood flow direction (Figure 17). Figure 16. Muscle contraction and relaxation maneuvers. The first photo of each series shows muscle contraction and the second one shows muscle relaxation. (a) Parana Maneuver. (b) Distal compression of muscles. (c) alternating weight-bearing. Figure 17. Example of right leg vein mapping. Shown: (a) Arch of normal internal sphenous vein. (b) Insufficient internal sphenous vein. (c) Insufficient and dilated superficial tributaries. (d) Normal external sphenous vein. (e) Insufficient external saphenous vein arch. (f) Anastomotic magna. (h) Sufficient internal saphenous vein. Numbers indicate the vascular diameter; arrows indicate blood flow direction; in orange, insufficient vessels; circles show vanishing points. Diagnosis: Internal saphenous vein insufficiency with sufficient arc caused by Giacomini vein that is overloaded due to insufficiency of the external saphenous vein arch.
14 Revista Chilena de Radiología. 2009; 15(4): PATIENTS WITH RELAPSED VARICES Common clinical patterns of venous insufficiency change when the patient has undergone surgery; nevertheless, these patterns have to be taken into account whenever new sites of vanishing points and tributary veins need to be detected. Concerning the internal saphenous system, awareness of accessory saphenous veins and tributaries coming from the gluteal or pudendal-perineal regions (from the pelvis) as well as development of neovascularization in the arch area, whether linked or not to a long remnant, is of vital importance. In the external saphenous system, the presence of perforating veins must be searched for. Conclusions In the cases of venous insufficiency it is crucial to carry out a complete study of the venous system both anatomically and hemodynamically, thus enabling surgeons to properly implement the surgery. Knowledge of normal venous anatomy, its variations, and patterns of saphenous and non-saphenous reflux is of great help for conducting imagedirected studies. References 1. Stefano Ricci, Mihael Georgiev,.Ultrasound Anatomy of the Superficial Veins of the Lower Limb. The Journal of Vascular Technology 2002; 26(3): J. Juan Samsó, J. FontcubertaGarcía, et al. Guía básica para el diagnóstico no invasivo de la insuficiencia venosa. Angiologia 2002; 54 (1): Miguel García-Gimeno, Santiago Rodríguez-Camarero, et al. Duplex mapping of 2036 primary varicose veins. J Vasc Surg 2009; 49: Constantinos T. Delis, et al. Prevalence, anatomic patterns, valvular competence, and clinical signifi cance of the Giacomini vein. J Vasc Surg 2004; 40: Nicos Labropoulos, Jay Tiongson, et al. Nonsaphe- nous superficial vein reflux. J Vasc Surg 2001; 34:
15 Revista Chilena de Radiología. 2009; 15(4): -. 15
16
17

18
19
20
21
22
23
24
25
26
27
28
29
30
Venous Reflux Duplex Exam
 Venous Reflux Duplex Exam GWENDOLYN CARMEL, RVT PHYSIOLOGIST, DEPARTMENT OF VASCULAR SURGERY NEW JERSEY VETERANS HEALTHCARE CENTER EAST ORANGE, NJ PURPOSE: To identify patterns of incompetence and which
Venous Reflux Duplex Exam GWENDOLYN CARMEL, RVT PHYSIOLOGIST, DEPARTMENT OF VASCULAR SURGERY NEW JERSEY VETERANS HEALTHCARE CENTER EAST ORANGE, NJ PURPOSE: To identify patterns of incompetence and which
Venous drainage of the lower limb
 Venous drainage of the lower limb INTRODUCTION It is of immense clinical and surgical importance. The venous blood against gravity. FACTORS HELPING THE VENOUS DRAINAGE OF THE LOWER LIMB The contraction
Venous drainage of the lower limb INTRODUCTION It is of immense clinical and surgical importance. The venous blood against gravity. FACTORS HELPING THE VENOUS DRAINAGE OF THE LOWER LIMB The contraction
Doppler Sonography in the ambulatory hemodynamics surgery of the venous insufficiency
 Doppler Sonography in the ambulatory hemodynamics surgery of the venous insufficiency Poster No.: C-0164 Congress: ECR 2013 Type: Educational Exhibit Authors: M. García Carriazo, C. Gómez de la Heras,
Doppler Sonography in the ambulatory hemodynamics surgery of the venous insufficiency Poster No.: C-0164 Congress: ECR 2013 Type: Educational Exhibit Authors: M. García Carriazo, C. Gómez de la Heras,
Segmental GSV reflux
 Segmental GSV reflux History of presentation A 43 year old female presented with right lower extremity varicose veins and swelling. She had symptoms of aching, heaviness and tiredness in the right leg.
Segmental GSV reflux History of presentation A 43 year old female presented with right lower extremity varicose veins and swelling. She had symptoms of aching, heaviness and tiredness in the right leg.
Anatomy. Patterns of reflux. Technique. Testing Reflux time Patient position. Difficult! Learning. NOT system optimisation. Clinical Assesment
 Anatomy Patterns of reflux Awareness Technique Testing Reflux time Patient position Difficult! Learning NOT system optimisation Enlarged Clinical Assesment Twisted Where are the symptoms? Why they are
Anatomy Patterns of reflux Awareness Technique Testing Reflux time Patient position Difficult! Learning NOT system optimisation Enlarged Clinical Assesment Twisted Where are the symptoms? Why they are
NCVH. Ultrasongraphy: State of the Art Vein Forum 2015 A Multidisciplinary Approach to Otptimizing Venous Circulation From Wounds to WOW
 Ultrasongraphy: State of the Art 2015 NCVH New Cardiovascular Horizons Vein Forum 2015 A Multidisciplinary Approach to Otptimizing Venous Circulation From Wounds to WOW Anil K. Chagarlamudi, M.D. Cardiovascular
Ultrasongraphy: State of the Art 2015 NCVH New Cardiovascular Horizons Vein Forum 2015 A Multidisciplinary Approach to Otptimizing Venous Circulation From Wounds to WOW Anil K. Chagarlamudi, M.D. Cardiovascular
High Level Overview: Venous Anatomy of Lower Extremities. Anatomy of a Vein 5/11/2015. Barbara Deusterman, RN
 High Level Overview: Venous Anatomy of Lower Extremities Barbara Deusterman, RN What does this anatomy lecture have to do with visually guided sclerotherapy (VGS)? May 11, 2015 2 Anatomy of a Vein Almeida,
High Level Overview: Venous Anatomy of Lower Extremities Barbara Deusterman, RN What does this anatomy lecture have to do with visually guided sclerotherapy (VGS)? May 11, 2015 2 Anatomy of a Vein Almeida,
Clinical/Duplex Evaluation of Varicose Veins: Who to Treat?
 Clinical/Duplex Evaluation of Varicose Veins: Who to Treat? Sanjoy Kundu MD, FASA, FCIRSE, FSIR The Vein Institute of Toronto Scarborough Vascular Group Scarborough Vascular Ultrasound Scarborough Vascular
Clinical/Duplex Evaluation of Varicose Veins: Who to Treat? Sanjoy Kundu MD, FASA, FCIRSE, FSIR The Vein Institute of Toronto Scarborough Vascular Group Scarborough Vascular Ultrasound Scarborough Vascular
: A guide to Doppler US evaluation of chronic lower limb venous insufficiency
 : A guide to Doppler US evaluation of chronic lower limb venous insufficiency Poster No.: C-1781 Congress: ECR 2011 Type: Educational Exhibit Authors: T. M. O. Couto, H. Patricio, Â. Moreira, A. Estevao
: A guide to Doppler US evaluation of chronic lower limb venous insufficiency Poster No.: C-1781 Congress: ECR 2011 Type: Educational Exhibit Authors: T. M. O. Couto, H. Patricio, Â. Moreira, A. Estevao
Step by step ultrasound examination of varicose veins. Dr. Özgün Sensebat Vascular Surgeon Private Vascular Clinic Dorsten & Borken, Germany
 Step by step ultrasound examination of varicose Dr. Özgün Sensebat Vascular Surgeon Private Vascular Clinic Dorsten & Borken, Germany Required technical setup: B-mode vessel imaging combined with color
Step by step ultrasound examination of varicose Dr. Özgün Sensebat Vascular Surgeon Private Vascular Clinic Dorsten & Borken, Germany Required technical setup: B-mode vessel imaging combined with color
VENOUS DRAINAGE OF THE LOWER LIMB
 Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Femoral Artery. Its entrance to the thigh Position Midway between ASIS and pubic symphysis
 Lower Limb Vessels Lecture Objectives Describe the major arteries of the lower limb. Describe the deep and superficial veins of the lower limb. Describe the topographical relationships of the arteries
Lower Limb Vessels Lecture Objectives Describe the major arteries of the lower limb. Describe the deep and superficial veins of the lower limb. Describe the topographical relationships of the arteries
Interactive Learning Session
 Chronic Venous Disease - Part I Interactive Learning Session 2011 Ali Sabbour Prof of Vascular Surgery http://mic.shams.edu.eg/moodle6 Login as a guest Surgery 2 Ali Sabbour - Chronic Venous Disease Intended
Chronic Venous Disease - Part I Interactive Learning Session 2011 Ali Sabbour Prof of Vascular Surgery http://mic.shams.edu.eg/moodle6 Login as a guest Surgery 2 Ali Sabbour - Chronic Venous Disease Intended
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS
 HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
INTERNATIONAL AYURVEDIC MEDICAL JOURNAL. Arya ashok 1, Swapna kumary 2
 INTERNATIONAL AYURVEDIC MEDICAL JOURNAL International Ayurvedic Medical Journal, (ISSN: 0 09) (November, 07) () UNILATERAL VARIATION OF GREAT SAPHENOUS VEIN- A CADAVERIC STUDY Arya ashok, Swapna kumary
INTERNATIONAL AYURVEDIC MEDICAL JOURNAL International Ayurvedic Medical Journal, (ISSN: 0 09) (November, 07) () UNILATERAL VARIATION OF GREAT SAPHENOUS VEIN- A CADAVERIC STUDY Arya ashok, Swapna kumary
Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing?
 Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing? Susan Whitelaw RVT, RDMS PURPOSE Duplex imaging of the lower extremity veins is performed to assess the deep
Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing? Susan Whitelaw RVT, RDMS PURPOSE Duplex imaging of the lower extremity veins is performed to assess the deep
Patient assessment and strategy making for endovenous treatment
 Patient assessment and strategy making for endovenous treatment Raghu Kolluri, MD Director Vascular Medicine OhioHealth Riverside Methodist Hospital Columbus, OH Disclosures Current Medtronic Consultant/
Patient assessment and strategy making for endovenous treatment Raghu Kolluri, MD Director Vascular Medicine OhioHealth Riverside Methodist Hospital Columbus, OH Disclosures Current Medtronic Consultant/
Lower Extremity Venous Insufficiency Evaluation
 VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Lower Extremity Venous Insufficiency Evaluation This Protocol was prepared by members of the Society for Vascular Ultrasound (SVU) as a template
VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Lower Extremity Venous Insufficiency Evaluation This Protocol was prepared by members of the Society for Vascular Ultrasound (SVU) as a template
Clinical case. Symptomatic anterior accessory great saphenous vein (AAGSV) reflux
 reflux") Clinical case Symptomatic anterior accessory great saphenous vein (AAGSV) reflux A 70 year-old female presents with symptomatic varicose veins on left leg for more than 10 years. She complains of heaviness,
Clinical case Symptomatic anterior accessory great saphenous vein (AAGSV) reflux A 70 year-old female presents with symptomatic varicose veins on left leg for more than 10 years. She complains of heaviness,
Let s Take a Look Venous Insufficiency Ultrasound Techniques
 Let s Take a Look Venous Insufficiency Ultrasound Techniques Brent Wilkinson RVT, RDMS Steve Schomaker RVT, RDCS, RDMS Let s take a look Differentiate between normal venous flow and venous insufficiency
Let s Take a Look Venous Insufficiency Ultrasound Techniques Brent Wilkinson RVT, RDMS Steve Schomaker RVT, RDCS, RDMS Let s take a look Differentiate between normal venous flow and venous insufficiency
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY
 RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
Anatomy MCQs Week 13
 Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
Chronic Venous Insufficiency
 Chronic Venous Insufficiency None Disclosures Lesley Enfinger, MSN,NP-C Chronic Venous Insufficiency Over 24 Million Americans affected by Chronic Venous Insufficiency (CVI) 10 x More Americans suffer
Chronic Venous Insufficiency None Disclosures Lesley Enfinger, MSN,NP-C Chronic Venous Insufficiency Over 24 Million Americans affected by Chronic Venous Insufficiency (CVI) 10 x More Americans suffer
Leg. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Recurrent Varicose Veins We All See Them
 We All See Them November 4, 2017 Austin, TX Arlington Heights, IL No conflicts Terminology REVAS REcurrent Varices After Surgery PREVAIT PREsence of Varices After Interventional Treatment Recurrent varices
We All See Them November 4, 2017 Austin, TX Arlington Heights, IL No conflicts Terminology REVAS REcurrent Varices After Surgery PREVAIT PREsence of Varices After Interventional Treatment Recurrent varices
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
Determine the patients relative risk of thrombosis. Be confident that you have had a meaningful discussion with the patient.
 Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
Rare Vascular Anomalies in the Femoral Triangle During Varicose Vein Surgery
 Korean J Thorac Cardiovasc Surg 2017;50:99-104 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2017.50.2.99 Rare Vascular Anomalies in the Femoral Triangle
Korean J Thorac Cardiovasc Surg 2017;50:99-104 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2017.50.2.99 Rare Vascular Anomalies in the Femoral Triangle
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
ABDOMINAL WALL & RECTUS SHEATH
 ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
DISSECTION SCHEDULE. Session I - Hip (Front) & Thigh (Superficial)
 & Thigh (Superficial)") DISSECTION SCHEDULE Session I - Hip (Front) & Thigh (Superficial) Surface anatomy Inguinal region Gluteal region Thigh Leg Foot bones Hip bone Femur Superficial fascia Great saphenous vein Superficial
DISSECTION SCHEDULE Session I - Hip (Front) & Thigh (Superficial) Surface anatomy Inguinal region Gluteal region Thigh Leg Foot bones Hip bone Femur Superficial fascia Great saphenous vein Superficial
Clinico-Anatomical and Radiological Correlation of Varicose Veins of Lower Limb A Cross-sectional Study
 ORIGINAL RESEARCH www.ijcmr.com Clinico-Anatomical and Radiological Correlation of Varicose Veins of Lower Limb A Cross-sectional Study Lalatendu Swain 1, Mamata Singh 2, Prabhat Nalini Rautray 3 ABSTRACT
ORIGINAL RESEARCH www.ijcmr.com Clinico-Anatomical and Radiological Correlation of Varicose Veins of Lower Limb A Cross-sectional Study Lalatendu Swain 1, Mamata Singh 2, Prabhat Nalini Rautray 3 ABSTRACT
Linda Antonucci, RPhS, RVT, RDCS
 Linda Antonucci, RPhS, RVT, RDCS DISCLOSURE Linda Antonucci, RPhS, RVT, RDCS I have no financial relationships to disclose relevant to this talk. SIMILARITIESBETWEEN ARTERIES AND VEINS Composed of three
Linda Antonucci, RPhS, RVT, RDCS DISCLOSURE Linda Antonucci, RPhS, RVT, RDCS I have no financial relationships to disclose relevant to this talk. SIMILARITIESBETWEEN ARTERIES AND VEINS Composed of three
Chronic Venous Insufficiency Compression and Beyond
 Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
LOWER EXTREMITY VENOUS COMPRESSION ULTRASOUND. CPT Stacey Good, DO Emergency Medicine Ultrasound Fellow Madigan Army Medical Center
 LOWER EXTREMITY VENOUS COMPRESSION ULTRASOUND CPT Stacey Good, DO Emergency Medicine Ultrasound Fellow Madigan Army Medical Center Learning Objectives Setup and patient positioning for optimizing success
LOWER EXTREMITY VENOUS COMPRESSION ULTRASOUND CPT Stacey Good, DO Emergency Medicine Ultrasound Fellow Madigan Army Medical Center Learning Objectives Setup and patient positioning for optimizing success
Prof. Nabil CHAKFE et coll.
 Prof. Nabil CHAKFE et coll. For the Department of Vascular Surgery and Kidney Transplantation University Hospital of Strasbourg, FRANCE Popliteal artery entrapment: misdiagnosed Epidemiology Prevalence:
Prof. Nabil CHAKFE et coll. For the Department of Vascular Surgery and Kidney Transplantation University Hospital of Strasbourg, FRANCE Popliteal artery entrapment: misdiagnosed Epidemiology Prevalence:
1-Muscles: 2-Blood supply: Branches of the profunda femoris artery. 3-Nerve supply: Sciatic nerve
 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t r i n g p a r t o r i s c h i a l p a r t ) 2-Blood supply:
1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t r i n g p a r t o r i s c h i a l p a r t ) 2-Blood supply:
Lumbar Plexus. Ventral rami L1 L4 Supplies: Major nerves.. Abdominal wall External genitalia Anteromedial thigh
 Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Guidelines, Policies and Statements D20 Statement on Peripheral Venous Ultrasound
 Guidelines, Policies and Statements D20 Statement on Peripheral Venous Ultrasound Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Guidelines, Policies and Statements D20 Statement on Peripheral Venous Ultrasound Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
VESSELS: GROSS ANATOMY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
Femoral Triangle and Adductor Canal. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Femoral Triangle and Adductor Canal Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Femoral Triangle and Adductor Canal Femoral triangle Is a triangular depressed area located in the upper
Femoral Triangle and Adductor Canal Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Femoral Triangle and Adductor Canal Femoral triangle Is a triangular depressed area located in the upper
Lower Limb Nerves. Clinical Anatomy
 Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
The Evaluation & Treatment of Pelvic Venous Disorders
 The Evaluation & Treatment of Pelvic Venous Disorders Mark H. Meissner, MD Professor of Surgery University of Washington School of Medicine Seattle, Washington Pelvic Venous Disorders Pelvic Congestion
The Evaluation & Treatment of Pelvic Venous Disorders Mark H. Meissner, MD Professor of Surgery University of Washington School of Medicine Seattle, Washington Pelvic Venous Disorders Pelvic Congestion
The role of ultrasound duplex in endovenous procedures
 The role of ultrasound duplex in endovenous procedures Neophytos A. Zambas MD, PhD Vascular Surgeon Polyclinic Ygia, Limassol, Cyprus ΚΕΑΕΧ ΚΥΠΡΙΑΚΗ ΕΤΑΙΡΕΙΑ ΑΓΓΕΙΑΚΗΣ ΚΑΙ ΕΝΔΑΓΓΕΙΑΚΗΣ ΧΕΙΡΟΥΡΓΙΚΗΣ Pre
The role of ultrasound duplex in endovenous procedures Neophytos A. Zambas MD, PhD Vascular Surgeon Polyclinic Ygia, Limassol, Cyprus ΚΕΑΕΧ ΚΥΠΡΙΑΚΗ ΕΤΑΙΡΕΙΑ ΑΓΓΕΙΑΚΗΣ ΚΑΙ ΕΝΔΑΓΓΕΙΑΚΗΣ ΧΕΙΡΟΥΡΓΙΚΗΣ Pre
Controversies & updates in Vascular Surgery. Paris - february
 Controversies & updates in Vascular Surgery Paris - february 09 2019 Venous session Recurrence at the popliteal fossea Pathogenesis and duplex investigation Philippe LEMASLE Le Chesnay - France I have
Controversies & updates in Vascular Surgery Paris - february 09 2019 Venous session Recurrence at the popliteal fossea Pathogenesis and duplex investigation Philippe LEMASLE Le Chesnay - France I have
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh:
 5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
Introduction. Background Evidence System of examination Diagnoses & Variants Final actions Limitation of the examination
 Rule in DVT Introduction Background Evidence System of examination Diagnoses & Variants Final actions Limitation of the examination BACKGROUND Common presentation Influence initial management NICE Guidelines
Rule in DVT Introduction Background Evidence System of examination Diagnoses & Variants Final actions Limitation of the examination BACKGROUND Common presentation Influence initial management NICE Guidelines
Mohammad Ashraf. Abdulrahman Al-Hanbali. Ahmad Salman. 1 P a g e
 - 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
- 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
YOU MUST BRING GLOVES FOR THIS ACTIVITY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 5e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 5e. All text references are for this textbook. 2) Observe and sketch histology slide
Ali Yaghi. Omar Eyad. Ahmad Salman. 1 P a g e
 5 Ali Yaghi Omar Eyad Ahmad Salman 1 P a g e **There are two types of groin hernia; the femoral hernia and the inguinal hernia. But how can we differentiate between the inguinal hernia and the femoral
5 Ali Yaghi Omar Eyad Ahmad Salman 1 P a g e **There are two types of groin hernia; the femoral hernia and the inguinal hernia. But how can we differentiate between the inguinal hernia and the femoral
Lecture 09. Popliteal Fossa. BY Dr Farooq Khan Aurakzai
 Lecture 09 Popliteal Fossa BY Dr Farooq Khan Aurakzai Dated: 14.02.2018 What is popliteus? Introduction Anything relating to, or near the part of the leg behind the knee. From New Latin popliteus the muscle
Lecture 09 Popliteal Fossa BY Dr Farooq Khan Aurakzai Dated: 14.02.2018 What is popliteus? Introduction Anything relating to, or near the part of the leg behind the knee. From New Latin popliteus the muscle
Varicose Vein Information Sheet
 Neil Goldstein, MD Joseph Hewett, MD Board- Certified Physicians in Interventional, Diagnostic, and Vascular Radiology, Surgery, Vascular Surgery and Phlebology Varicose Vein Information Sheet PREVALENCE
Neil Goldstein, MD Joseph Hewett, MD Board- Certified Physicians in Interventional, Diagnostic, and Vascular Radiology, Surgery, Vascular Surgery and Phlebology Varicose Vein Information Sheet PREVALENCE
rotation of the hip Flexion of the knee Iliac fossa of iliac Lesser trochanter Femoral nerve Flexion of the thigh at the hip shaft of tibia
 Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Doppler examination of lower limb venous insufficiency: consensus among specialists
 Update in Radiology Doppler examination of lower limb venous insufficiency: consensus among specialists H. Berardi and A. Ciccioli* Imaging Diagnosis Department, Hospital Interzonal General de Agudos Dr.
Update in Radiology Doppler examination of lower limb venous insufficiency: consensus among specialists H. Berardi and A. Ciccioli* Imaging Diagnosis Department, Hospital Interzonal General de Agudos Dr.
Doppler ultrasound in the evaluation of chronic venous insufficiency: A step-by-step morphological and hemodynamic review
 Doppler ultrasound in the evaluation of chronic venous insufficiency: A step-by-step morphological and hemodynamic review Poster No.: C-3206 Congress: ECR 2010 Type: Educational Exhibit Topic: Vascular
Doppler ultrasound in the evaluation of chronic venous insufficiency: A step-by-step morphological and hemodynamic review Poster No.: C-3206 Congress: ECR 2010 Type: Educational Exhibit Topic: Vascular
musculoskeletal system <lower limb vessle> <1> done by:renad abu ruman &rama alawamleh
 musculoskeletal system done by:renad abu ruman &rama alawamleh The entrance to the anterior compartment of the leg is through lingual lig. & superior ramus, & to the posterior compartment
musculoskeletal system done by:renad abu ruman &rama alawamleh The entrance to the anterior compartment of the leg is through lingual lig. & superior ramus, & to the posterior compartment
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT. Dr Farooq Khan Aurakzai. Dated:
 Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
BEDSIDE ULTRASOUND BEDSIDE ULTRASOUND. Deep Vein Thrombosis. Probe used
 BEDSIDE ULTRASOUND Part 2 Diagnosis of deep vein thrombosis Kishore Kumar Pichamuthu, Professor, Department of Critical Care, CMC, Vellore Summary: Deep vein thrombosis (DVT) is a problem encountered in
BEDSIDE ULTRASOUND Part 2 Diagnosis of deep vein thrombosis Kishore Kumar Pichamuthu, Professor, Department of Critical Care, CMC, Vellore Summary: Deep vein thrombosis (DVT) is a problem encountered in
Latmedical, LLC is the exclusive Caribbean distributor
 No-Varix Graduated Compression Hosiery is manufactured by TEXPON S.A., the only Latin- American company certified with the norm ISO 9001:00 with scope of manufacture of graduate compression hosiery for
No-Varix Graduated Compression Hosiery is manufactured by TEXPON S.A., the only Latin- American company certified with the norm ISO 9001:00 with scope of manufacture of graduate compression hosiery for
Ultrasound Guided Lower Extremity Blocks
 Ultrasound Guided Lower Extremity Blocks CONTENTS: 1. Femoral Nerve Block 2. Popliteal Nerve Block Updated December 2017 1 1. Femoral Nerve Block Indications Surgery involving the knee, anterior thigh,
Ultrasound Guided Lower Extremity Blocks CONTENTS: 1. Femoral Nerve Block 2. Popliteal Nerve Block Updated December 2017 1 1. Femoral Nerve Block Indications Surgery involving the knee, anterior thigh,
As with any intervention, selection of an appropriate
 DVT: ccess Decisions for Interventions ssessing the advantages and disadvantages of venous access options is crucial for safe and successful DVT intervention. Y JOHN. KUFMN, MD, MS, FSIR, FH, FCIRSE, EIR
DVT: ccess Decisions for Interventions ssessing the advantages and disadvantages of venous access options is crucial for safe and successful DVT intervention. Y JOHN. KUFMN, MD, MS, FSIR, FH, FCIRSE, EIR
Vein Disease Treatment
 MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
Fig MHz cm/s. Table 1 Fig. 2. Fig. 3, 4. Fig. 5
 GE Fig. 1 3. 5 MHz 7 10 MHz 3. 5 5. 0 MHz B 10 20 cm/s Table 1 Fig. 2 Fig. 1 1 2 3 3 3 : 1 2 3 Fig. 3, 4 Fig. 5 Table 1 a b c Fig. 2 a B b B c Fig. 6 Table 1 Fig. 7 a b c Fig. 3 a AV b A VV c 1 cm 2 1
GE Fig. 1 3. 5 MHz 7 10 MHz 3. 5 5. 0 MHz B 10 20 cm/s Table 1 Fig. 2 Fig. 1 1 2 3 3 3 : 1 2 3 Fig. 3, 4 Fig. 5 Table 1 a b c Fig. 2 a B b B c Fig. 6 Table 1 Fig. 7 a b c Fig. 3 a AV b A VV c 1 cm 2 1
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
Contents of the Posterior Fascial Compartment of the Thigh
 Contents of the Posterior Fascial Compartment of the Thigh 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t
Contents of the Posterior Fascial Compartment of the Thigh 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t
The Lower Limb VI: The Leg. Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa
 The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
Healthy Legs For Life! Prevention is better then cure
 Healthy Legs For Life! Prevention is better then cure Ellie Lindsay Independent Specialist Practitioner Associate Lecturer, CRICP, London Visiting Fellow, Queensland University of Technology Occurrence
Healthy Legs For Life! Prevention is better then cure Ellie Lindsay Independent Specialist Practitioner Associate Lecturer, CRICP, London Visiting Fellow, Queensland University of Technology Occurrence
Lower Limb Venous Ultrasound. Colin P. Griffin MSc, BSc (Hons)
") Lower Limb Venous Ultrasound Colin P. Griffin MSc, BSc (Hons) Peripheral Vessels Lower Limb Peripheral Vessels Lower Limb Venous Deep System Common Iliac External/Internal Iliac Common Femoral Femoral
Lower Limb Venous Ultrasound Colin P. Griffin MSc, BSc (Hons) Peripheral Vessels Lower Limb Peripheral Vessels Lower Limb Venous Deep System Common Iliac External/Internal Iliac Common Femoral Femoral
The thigh. Prof. Oluwadiya KS
 The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
O R I G I N A L A R T I C L E
 O R I G I N A L A R T I C L E Folia Morphol. Vol. 64, No. 4, pp. 287 291 Copyright 2005 Via Medica ISSN 0015 5659 www.fm.viamedica.pl The topography of the superficial veins of the hind leg in the baboon
O R I G I N A L A R T I C L E Folia Morphol. Vol. 64, No. 4, pp. 287 291 Copyright 2005 Via Medica ISSN 0015 5659 www.fm.viamedica.pl The topography of the superficial veins of the hind leg in the baboon
The Thoracic wall including the diaphragm. Prof Oluwadiya KS
 The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
To describe he knee joint, ligaments, structure & To list the main features of other lower limb joints
 To describe he knee joint, ligaments, structure & neurovascular supply To demonstrate the ankle joint anatomy To list the main features of other lower limb joints To list main groups of lymph nodes in
To describe he knee joint, ligaments, structure & neurovascular supply To demonstrate the ankle joint anatomy To list the main features of other lower limb joints To list main groups of lymph nodes in
CORONARY ARTERY BYPASS GRAFTING (CABG) (Part 1) Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST
 (Part 1) Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST") CORONARY ARTERY BYPASS GRAFTING (CABG) (Part 1) Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST I have constructed this lecture based on publications by leading cardiothoracic American surgeons: Timothy
CORONARY ARTERY BYPASS GRAFTING (CABG) (Part 1) Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST I have constructed this lecture based on publications by leading cardiothoracic American surgeons: Timothy
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Materials and Methods
 Veins and Lymphatics 2015; volume 4:4703 Associations between flow in paratibial perforating veins and great saphenous vein patterns of reflux Carlos Alberto Engelhorn, 1,2 Ana Luiza Dias Valiente Engelhorn,
Veins and Lymphatics 2015; volume 4:4703 Associations between flow in paratibial perforating veins and great saphenous vein patterns of reflux Carlos Alberto Engelhorn, 1,2 Ana Luiza Dias Valiente Engelhorn,
BOGOMOLETS NATIONAL MEDICAL UNIVERSITY. Department of Human Anatomy GUIDELINES. The theme of the lesson The vessels of the lower limb.
 BOGOMOLETS NATIONAL MEDICAL UNIVERSITY Department of Human Anatomy GUIDELINES Academic discipline HUMAN ANATOMY Module 2 The theme of the lesson The vessels of the lower limb. Course Faculties І Medical
BOGOMOLETS NATIONAL MEDICAL UNIVERSITY Department of Human Anatomy GUIDELINES Academic discipline HUMAN ANATOMY Module 2 The theme of the lesson The vessels of the lower limb. Course Faculties І Medical
How varicose veins occur
 Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
Misc Anatomy. Upper Limb! 2. Lower Limb! 5. Venous Drainage! Head & neck! 8
 Misc Anatomy Upper Limb! 2 Arteries!... 2 Veins!... 2 Spaces!... 4 Lower Limb! 5 Arteries!... 5 Venous Drainage!... 6 Spaces!... 7 Head & neck! 8 Artery!... 8 Ultrasound View for IJ CVL!... 8 Arteries
Misc Anatomy Upper Limb! 2 Arteries!... 2 Veins!... 2 Spaces!... 4 Lower Limb! 5 Arteries!... 5 Venous Drainage!... 6 Spaces!... 7 Head & neck! 8 Artery!... 8 Ultrasound View for IJ CVL!... 8 Arteries
DISORDERS OF VENOUS SYSTEM
 DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
Non-invasive examination
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Duplex Ultrasound Evaluation of Patients With Chronic Venous Disease of the Lower Extremities
 Vascular and Interventional Radiology Review Khilnani Chronic Venous Disease of the Lower Extremities Vascular and Interventional Radiology Review Neil M. Khilnani 1 Khilnani NM Keywords: chronic venous
Vascular and Interventional Radiology Review Khilnani Chronic Venous Disease of the Lower Extremities Vascular and Interventional Radiology Review Neil M. Khilnani 1 Khilnani NM Keywords: chronic venous
The femoral artery and its branches in the baboon Papio anubis
 O R I G I N A L A R T I C L E Folia Morphol. Vol. 66, No. 4, pp. 291 295 Copyright 2007 Via Medica ISSN 0015 5659 www.fm.viamedica.pl The femoral artery and its branches in the baboon Papio anubis Dyl
O R I G I N A L A R T I C L E Folia Morphol. Vol. 66, No. 4, pp. 291 295 Copyright 2007 Via Medica ISSN 0015 5659 www.fm.viamedica.pl The femoral artery and its branches in the baboon Papio anubis Dyl
Doppler ultrasound evaluation of pattern of venous incompetance and relation with skin changes in varicose vein patients
 Doppler ultrasound evaluation of pattern of venous incompetance and relation with skin changes in varicose vein patients Pant HP 1, Sharma S 2, Bhattarai S 1, Pandit SP 3, Maharjan D 2 1 Radiology resident,
Doppler ultrasound evaluation of pattern of venous incompetance and relation with skin changes in varicose vein patients Pant HP 1, Sharma S 2, Bhattarai S 1, Pandit SP 3, Maharjan D 2 1 Radiology resident,
Endothermal Ablation for Venous Insufficiency. Dr. S. Kundu Medical Director The Vein Institute of Toronto
 Endothermal Ablation for Venous Insufficiency Dr. S. Kundu Medical Director The Vein Institute of Toronto Objective: remove the GSV from the circulation 1. Surgical - HL & stripping 2. Chemical sclerotherapy
Endothermal Ablation for Venous Insufficiency Dr. S. Kundu Medical Director The Vein Institute of Toronto Objective: remove the GSV from the circulation 1. Surgical - HL & stripping 2. Chemical sclerotherapy
Selection and work up for the right patients suspected of deep venous disease
 Selection and work up for the right patients suspected of deep venous disease R A G H U K O L L U R I, M S, M D, R V T S Y S T E M M E D I C A L D I R E C T O R V A S C U L A R M E D I C I N E / V A S
Selection and work up for the right patients suspected of deep venous disease R A G H U K O L L U R I, M S, M D, R V T S Y S T E M M E D I C A L D I R E C T O R V A S C U L A R M E D I C I N E / V A S
Anterior and Medial compartments of the thigh. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
History is Flawed. A New Paradigm for Abdominal & Pelvic Venous Disorders
 History is Flawed A New Paradigm for Abdominal & Pelvic Venous Disorders Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Medicine University of Washington School of Medicine Disclosures
History is Flawed A New Paradigm for Abdominal & Pelvic Venous Disorders Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Medicine University of Washington School of Medicine Disclosures
chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis, Klippel- Trenaunay syndrome DVT CVD
 Online publication August 27, 2009 chronic venous disorders: CVD CEAP 4 CEAP CVD J Jpn Coll Angiol, 2009, 49: 201 205 chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis,
Online publication August 27, 2009 chronic venous disorders: CVD CEAP 4 CEAP CVD J Jpn Coll Angiol, 2009, 49: 201 205 chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis,
Gluteal region DR. GITANJALI KHORWAL
 Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Recurrent varicose veins. Information for patients Sheffield Vascular Institute
 Recurrent varicose veins Information for patients Sheffield Vascular Institute You have been diagnosed as having varicose veins that have recurred (come back). This leaflet explains more about recurrent
Recurrent varicose veins Information for patients Sheffield Vascular Institute You have been diagnosed as having varicose veins that have recurred (come back). This leaflet explains more about recurrent
Major Veins of the Body
 Major Veins of the Body Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Major Veins of the Body Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Priorities Forum Statement
 Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Edinburgh Vein Study Follow Up
 This thesis has been submitted in fulfilment of the requirements for a postgraduate degree (e.g. PhD, MPhil, DClinPsychol) at the University of Edinburgh. Please note the following terms and conditions
This thesis has been submitted in fulfilment of the requirements for a postgraduate degree (e.g. PhD, MPhil, DClinPsychol) at the University of Edinburgh. Please note the following terms and conditions
Controversies & updates in Vascular Surgery
 Controversies & updates in Vascular Surgery Paris - january 24 2018 Venous session VENOUS ODDITIES DUPLEX IMAGE Philippe LEMASLE Le Chesnay - France I have no financial relationship to disclose Case n
Controversies & updates in Vascular Surgery Paris - january 24 2018 Venous session VENOUS ODDITIES DUPLEX IMAGE Philippe LEMASLE Le Chesnay - France I have no financial relationship to disclose Case n