Zubair W. Baloch, MD, PhD: Consultant for Veracyyte, INC Tarik M. Elsheikh, MD: Nothing to disclose
|
|
|
- Martin Roy Armstrong
- 6 years ago
- Views:
Transcription



1 Cytology Works shop #8 Zubair W. Baloch, MD, PhD: Consultantt for Veracyte, INC Tarik M. Elsheik kh, MD: Nothing to disclose
2 Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair W. Baloch, MD, PhD Tarik M. Elsheikh, MD Disclosures Zubair W. Baloch, MD, PhD Veracyte, INC Consultant Tarik M. Elsheikh, MD None Cystic Lesions of Head and Neck: Zubair W. Baloch, MD, PhD 1

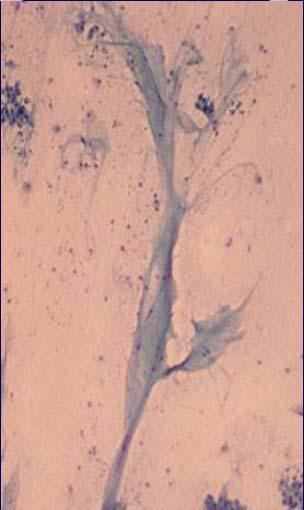
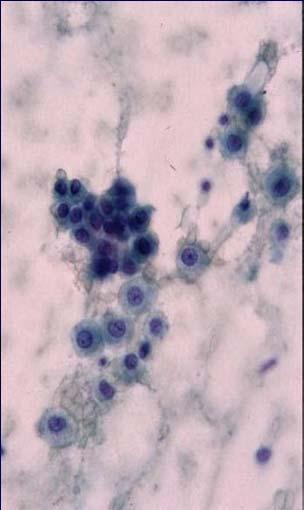
3 Objectives Generate a cytologic differential diagnosis for various cystic and solid head and neck lesions. Recognize the pitfalls in the cytologic and histologic diagnosis of primary and metastatic head and neck lesions. Discuss the value of special techniques in the diagnosis of head and neck and salivary gland tumors. Case 1 60 year old man with right neck mass? Tail of parotid mass vs. lymph node US cystic mass Favor metastasis to cervical node Thyroid US no suspicious nodules Panendoscopy No mucosal abnormalities? Mass of right tonsil FNA of right neck mass 2


4 FNA of right neck mass FNA of right neck mass Cytology Dx: Squamous cell carcinoma Tonsil Biopsy Squamous cell carcinoma 3
5 Incidence of unsuspected carcinoma in cervical cystic lesions Study Incidence (%) No. of Patients Krogdahl (1979) 4 7/161 Cinberg et. al (1982) 22 4/18 Granstrom & Edstrom (1989) 21 9/42 Flannagan et. al (1994) 16 4/25 Gourin & Johnson (2000) 10 12/121 Sheahan et. al (2002) 24 8/33 Sensitivity of FNA in the diagnosis of malignancy in cystic neck lesions Study Sensitivity (%) Cinberg et al. (1982) 33 Granstrom & Edstrom (1989) 33 Flannagan et al. (1994) 50 Gourin & Johnson (2000) 37.5 Sheahan et al. (2002) 73 Moatamed et al. (2009) 76 Baykul et al. (2010) 90 Cystic Lesions of the Neck Congenital Acquired Majority of neck cysts in newborns and infants are developmental Children and adults Inflammatory or neoplastic 4
6 Congenital / Developmental Cystic Lesions of the Neck Traumatic Inflammatory Neoplastic Benign Neoplastic Malignant Branchial Cleft Cyst Areriovenous fistula Abscess Cystic Schwannoma Cystic Nodal Mets from SCC Thyroglossal duct cyst Laryngocele Tuberculosis Parathyroid cyst Cystic Nodal Mets from PTC Lymphatic malformations Ludwigs Angina* Goitrous nodule or Cystic PTC Cystic Mets from other organs Epidermoid or Dermoid HIV related Lymphoepithelial cyst Thymic cyst Salivary gland Bronchogenic & Esophageal duplication cysts Ranula Salivary Gland Congenital Cysts First Branchial Cleft Cyst Residual embryonic tract Extends from external auditory canal (EAC) through the parotid gland to the submandibular region Type 1 Periauricular Type 2 Periparotid (extending from the EAC to the angle of mandible) II, III, IV branchial cleft cysts Branchial Cleft Cyst FNA Turbid white yellow fluid Variable number of squamous cells and aellualr squames Cellular debris Inflammatory cells Squamous cell with atypia? Branchial cleft cyst in older patients? 5


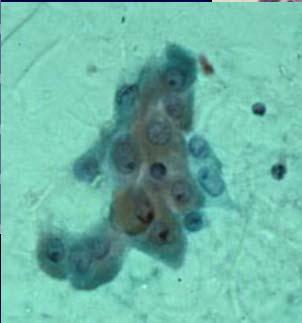
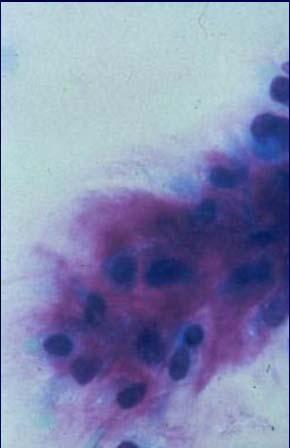
7 Benign Squamous Cystic Lesion vs. Cystic Mets of Squamous Carcinoma Not so easy 45 year old man with left neck cystic mass 45 year old man with left neck cystic mass Atypical squamous cells in the background of marked acute inflammation 6


8 45 year old man with left neck cystic mass 45 year old man with left neck cystic mass Inflamed branchial cleft cyst Benign Squamous Cystic Lesion vs. Cystic Mets of Squamous Carcinoma Cytologic Features Benign Mean/Std.Err Malignant Mean/Std.Err P-value Cell-Groups 1.0 / / 0.28 <.0001 Single Cells 3.3 / / 0.34 NS Anucleate Cells 2.9 / / 0.33 NS Nuclear Atypia 0.58 / / 0.15 <.0001 Backgr-Necrosis 1.0 / / 0.27 <.0004 Backgr-Infl 1.0 / / 0.35 NS P53 staining 1.1 / /.14 NS 7



9 Benign Squamous Cystic Lesion vs. Cystic Mets of Squamous Carcinoma Inflamed Branchial Cleft Cyst Cystic Mets of Squamous Carcinoma Benign Squamous Cystic Lesion vs. Cystic Mets of Squamous Carcinoma Clues Clinical history could be occult primary Inflammation common in benign Acute inflammation with keratinizing squamous lesions N/C ratio Maintained in benign lesions Nuclear atypia Excisional biopsy P53, p16 HPV in Squamous Cell Carcinoma 8
10 Head & Neck Squamous Cell Carcinomas (HNSCCs) HNSCCs 6.5% of annual cancer cases worldwide Estimated 38/100,000 new cases/yr (U.S.) Median age = 60 yrs 2/3 Males: 1/3 Females Incidence in Western Europe and U.S increasing over last few decades Oncogenesis of HPV Multistep/Multifactor process Oncogenes Modification of cellular genes Possible genetic susceptibility of host Impaired cell mediated immunity Genome of dsdna incorporation Early Region encodes for Early Proteins E1 E7 (important in pathogenesis and transformation) E6, E7 classified as oncogenes E6 binds to p53 and degrades it E7 binds to prb and causes dysfunction Results in inhibition of the cell cycle control and facilitation of tumor development HPV in Oropharyngeal Cancer Significantly higher HPV prevalence found in oropharyngeal SCCs that oral or laryngeal SCCs (Kreimer et al., 2005) Proposed that HPV positive oropharyngeal SCC is a distinct entity, less dependant on smoking and alcohol use (Klussmann et al, 2003) 9
11 HPV in Other Head & Neck Tumors Prevalence varies in the literature Possibly due to methods of analysis 14 35% by PCR 25% by Southern Blot 18% by FISH Most common HPV locations (other than oropharynx) [Dahlstrand & Dalianis, 2005] Tongue Cancer (19 100%) Laryngeal Cancer (10 50%) Termine et al Subgroup Number of Studies Mean prevalence (%) HNSCC n.s OSCC ISH based PCR based HNSCC n.s.s. ISH based 2 n.c. HNSCC n.s.s. PCR based OSCC PCR based OSCC ISH based Overall HPV Status and Prognosis 10

 HPV +ve tumors favorable independent of tumor stage, gender, age or differentiation HPV and Prognosis in Oropharyngeal Cancer Gillison et al.")
12 HPV and Prognosis in Oropharyngeal Cancer HPV may be a favorable prognostic factor (Gillison et al, 2000;Mellin et al., 2000) Mellin et al., pts with tonsillar cancer 52% of pts with HPV +ve tumors were disease free after 3 years 21% of pts with HPV ve tumors were disease free after 3 years Pts with HPV +ve tumors had significantly increased 5 year survival rates compared to HPV ve tumors (53% vs. 31%, p=0.047) HPV +ve tumors favorable independent of tumor stage, gender, age or differentiation HPV and Prognosis in Oropharyngeal Cancer Gillison et al., head and neck cancer patients 60 oropharyngeal cancers (mostly tonsil) Results: Disease specific survival significantly higher for HPV +ve tumors No change in disease specific survival for other head and neck cancers Multiples studies have shown no change in survival for HPV +ve tumors (except oropharynx)[reviewed by Dahlstrand & Dalia, 2005] How Adequate are Head and Neck Fine needle Aspiration Specimens for HPV Molecular Analysis? Vs. 11
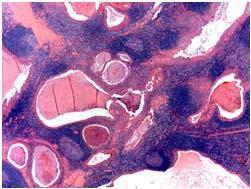
13 How Adequate are Head and Neck Fine needle Aspiration Specimens for HPV Molecular Analysis? 42 specimens in 40 patients 37 LN s & 5 others ites On site evaluation in 41 (98%) Final diagnosis SCC in all 9 cases >80% tumor necrosis Adequate DNA for molecular analysis 28 (67%) 7 (25%) necrotic specimens had adequate for HPV analysis Thyroglossal Duct Cyst Most common congenital neck mass Located in mid line or paramedian (left side) Closely related to hyoid bone 20% Suprahyoid, 65% infrahyoid & 15% at the level of hyoid bone (Grossman & Yousem 1994) Characteristic appearance on US, CT and MRI Hypoechoic thin walled cyst Debris Hemorrhage or infection Solid mass Carcinoma (95% PTC & 5% SCC) Thyroglossal Duct Cyst Differential diagnosis Dermoid cyst Necrotic lymphadenopathy Cystic goitrous nodule arising from thyroid isthmus Thymic cyst Branchial cleft cyst paramedian location Cystic hygroma paramedian location 12




14 Thyroglossal Duct Cyst FNA Thyroglossal Duct Cyst Lined by respiratory or squamous epithelium, or both Mucus glands seen in 60% of cases Infection Granulation tissue or scar Thyroid tissue Routine section 5%; serial sections 40% Thyroglossal Duct Cyst Carcinoma 95% PTC & 5% SCC Criteria Demonstration of thyroglossal remnant Normal thyroid gland (US exam?) to differentiate from PTC metastasis from thyroid 13




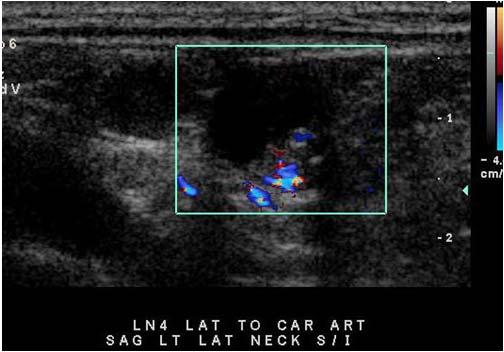
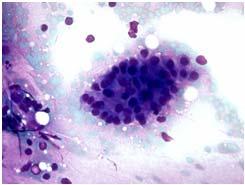
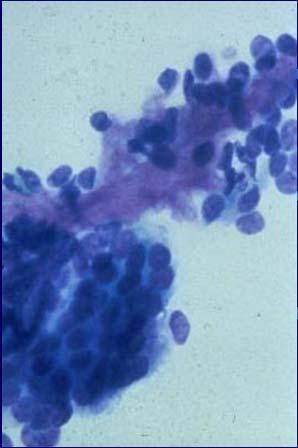
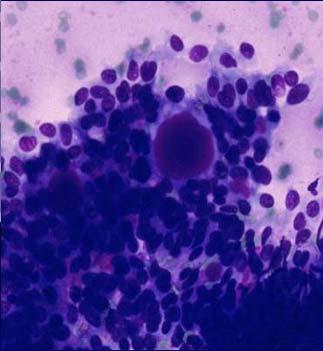
15 Thyroglossal Duct Cyst Carcinoma Thyroglossal Duct Cyst Carcinoma 35 year old woman with left lateral neck cystic mass 14





16 35 year old woman with left lateral neck cystic mass 35 year old woman with left lateral neck cystic mass Cytology Diagnosis: Lymphocytes and few macrophages in a background of colloid type material. Rule out metastatic papillary thyroid carcinoma 35 year old woman with left lateral neck cystic mass Histology Diagnosis: Metastatic papillary thyroid carcinoma; TTF 1 and Thyroglobulin positive 15


17 35 year old woman with left lateral neck cystic mass Total Thyroidectomy Histology Diagnosis: Papillary microcarcinoma 0.9 cm Cystic neck mass with no history Lymphocytes Colloid like background material Macrophages No epithelial cells Suspicious for thyroid cancer metastasis What next? Cystic neck mass suspicious for thyroid carcinoma metastasis On site evaluation suspicious Ultrasound examination of thyroid Aspiration of suspicious thyroid nodule Thyroglobulin level assessment of the aspirate No on site evaluation Recommend ultrasound evaluation of thyroid Repeat FNA with thyroglobulin level assessment of the aspirate 16
 25 0 3 10* 1** 0 NTS (n=35) 5 0 0 0 0 30 NDX(n=23) 3 0 1 0 0 19 ATYP (n=15) 9 0 0 4* 0")


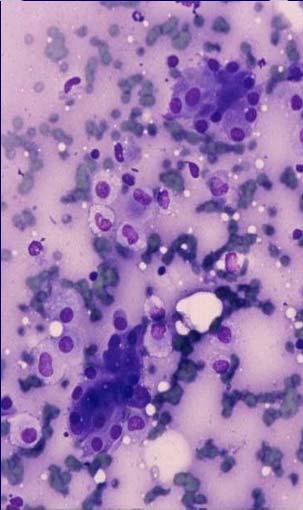
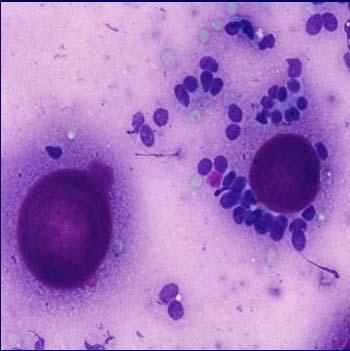
18 Thyroglobulin measurement in the lymph node aspirates of patients with PTC TG Levels 10 ng/ml TG Levels 10 ng/ml Cytologic-DX PTC Other CA No F/U PTC Other CA No F/U PTC (n=39) * 1** 0 NTS (n=35) NDX(n=23) ATYP (n=15) * 0 1 OTHER (n=3) 0 1*** 0 0 1**** 0 DX = Diagnosis, TG = Thyroglobulin, F/U = surgical pathology follow- up, PTC = Papillary thyroid carcinoma, CA = Carcinoma, NTS = No tumor seen, NDX = Non-diagnostic, ATYP = Atypical/Suspicious, * = includes cases of tall cell variant of papillary carcinoma, ** = metastatic well-differentiated follicular derived carcinoma *** = poorly differentiated carcinoma, **** = carcinoma not otherwise specified. 32 year old man with bilateral parotid gland masses 32 year old man with bilateral parotid gland masses 17


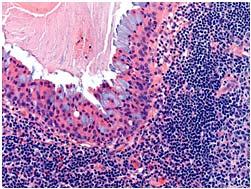
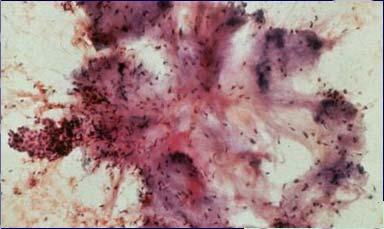
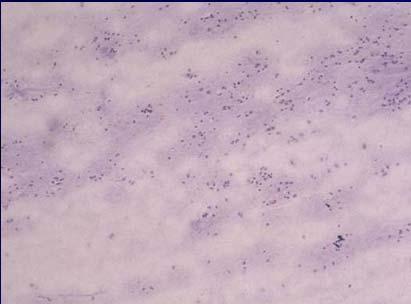
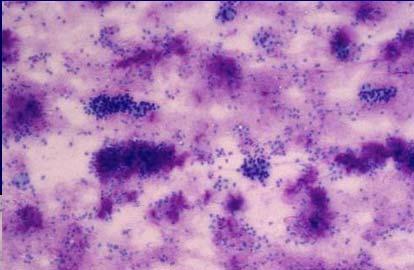
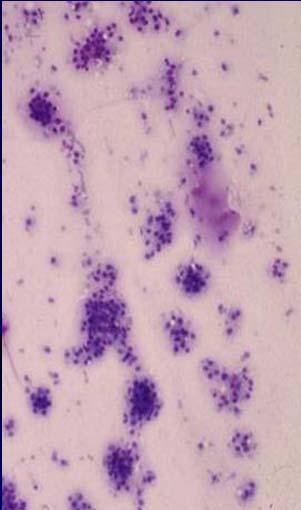
19 32 year old man with bilateral parotid gland masses HIV + Lymphoepithelial Cyst Warthin s Tumor Primarily occurs within parotid gland Second most common salivary gland neoplasm 5 10% Believed to originate from salivary duct remnants entrapped within glandular lymphoid tissue Clinical features: year old Common in men Bilateral Cytology Warthin s Tumor Mixed population of lymphocytes Sheets of oncocytes Background debris ( grossly mobile oil consistency) 18




20 Warthin s Tumor Cytology Oncocytic Mucoepidermoid Carcinoma 19
21 Overlapping Cytologic Features Lymphocytes Chai et al (Diag Cytopathol 1997) 61 cases with prominent lymphoid component Warthins 33 cases Warthins 31, Benign cyst 1, SCCA 1 Other epithelial malignancies 6 cases Oncocytoma; Pleomorphic adenoma, ACC Lymphomas 12 cases Benign 10 Overlapping Cytologic Features Lymphocytes Intraparotid LN Lymphoepithelial cyst Chronic Sialadenitis Warthin s Acinic cell carcinoma Mucoepidermoid Carcinoma Lymphoma Approach to cystic neck lesion Background Mucoid Histiocytes & lymphocytes Mucus retention cyst Salivary gland Chronic sialadenitis Sialolithiasis Mucoepidermoid carcinoma Myxoid and chondroid fragments Pleomorphic adenoma rare Atypical cells Malignancy Mets vs. primary 20
22 Approach to cystic neck lesion Background watery proteinaceous fluid Lymphocytic infiltrate & few epithelial cells Lymphoepithelial cyst Thyroglossal duct cyst midline location Salivary gland Lymphocytes and oncocytes Warthin s tumor Atypical keratinized cells Squamous cell carcinoma Metaplasia in benign tumor history of previous FNA Keratinized cells Atypical Squamous cell carcinoma Branchial cleft cyst Approach to cystic neck lesion Benign vs. malignant squamous cystic lesion Background inflammation? Necrotic debris Cellularity increased in SCC? Abnormal keratinization / Dyskeratosis Nuclear atypia Approach to cystic neck lesion Cystic mass suspicious for thyroid cancer Recommend ultrasound of thyroid and aspiration of suspicious nodules TTF 1 and thyroglobulin (should do both) if enough cells Thyroglobulin assessment of FNA specimen 21

23 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Case #1: Parotid mass, 56 yo male What is your Diagnosis? A. Pleomorphic adenoma B. Basal cell adenoma C. Adenoid cystic carcinoma D. LG mucoepidermoid carcinoma 22
24 Diagnosis? A. PA B. Basal cell adenoma C. Adenoid cystic CA D. LG mucoepidermoid CA Case #2: Submandibular mass, 37 yo man Diagnostic Challenges and Problems Cystic lesions Low grade malignancies Cellular benign neoplasms Atypical inflammatory changes Atypical lymphoid infiltrates Unusual cytologic presentation of common lesions Rare unusual lesions Primary Salivary Gland Neoplasms Benign Malignant Pleomorphic adenoma Basal cell adenoma Warthin tumor LG Mucoepidermoid CA Acinic cell carcinoma Adenoid cystic carcinoma HG and Undifferentiated CA 23



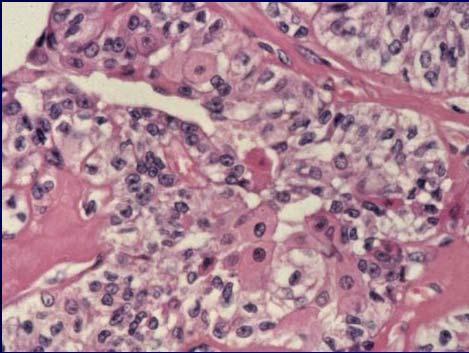
25 Key Cytologic Features Low power architectural appearance Size of cells and amount of cytoplasm Nucleoli Character of single cells in background Character of background substance Basal Cell Adenoma 2% of SG tumors Small cells Tightly cohesive clusters Background naked nuclei Can not distinguish from malignant basaloid tumors Minimal cytoplasm Round to oval nuclei Finely-coarsely granular chromatin Occasional small nucleoli 24



 Solid")

26 Amorphous extracellular hyaline material may be seen at periphery of cell clusters. Not specific for membranous BCA Cytology Adenoid Cystic Carcinoma Cribriform (Well Differentiated) Clusters and branching multilayered groups of basaloid cells surrounding globules of homogenous acellular material (reduplicated basal lamina PAS+) Solid (Poorly Differentiated) Loosely cohesive groups of cells with increased nuclear atypia and prominent nucleoli Acellular material (globules) lacking 25





27 Case study Salivary Gland Neoplasms with Basaloid Cell Features Architectural features are most important Never make a definitive Dx of BCA Cribriform ACC can be accurately diagnosed, but must exclude membranous BCA Solid BCA and solid ACC are indistinguishable Basal cell adenocarcinoma: indistinguishable cytologically from BCA and ACC 26



28 Sample Cytologic Diagnosis DX: Cellular neoplasm with basaloid cell features, see comment Comment: Differential diagnosis includes basal cell adenoma and adenoid cystic carcinoma (Ki 67). Basal cell adenoma is favored (suggested). Histologic confirmation is needed for a definitive diagnosis. Pleomorphic Adenoma 75% of major salivary gland tumors Female, years Aspirates of thick gelatinous consistency Mixture of epithelial and mesenchymal elements Epithelial/myoepithelial rich variant (CPA) 27


29 Chondroid stroma in PA Myxoid stroma in PA 28
 suspect basaloid cell tumor Atypical cytologic features Case #3: Cellular Pleomorphic Adenoma 40 year old female presented with a")
30 Pleomorphic Adenoma Biphasic Cellular/Epithelial Mesenchymal Problems in Cytologic Diagnosis of Pleomorphic Adenoma Predominance of one component if myxoid stroma predominates, may mistake for cyst fluid or LG mucoepidermoid CA if epithelial cells predominate (CPA) suspect basaloid cell tumor Atypical cytologic features Case #3: Cellular Pleomorphic Adenoma 40 year old female presented with a submandibular mass 29



31 LG Mucoepidermoid Carcinoma Cytology Intermediate cells Mucus producing cells - resemble macrophages Squamous cells - cohesive clusters of cells resembling metaplastic squames. Occasional paranuclear vacuoles No fully keratinized epidermoid cells Mucin and debris in background 30
32 31


33 PA BCA PA BCA or ACC PA ACC 32

34 Case #1: Parotid mass, 56 yo male What is your Diagnosis? A. Pleomorphic adenoma B. Basal cell adenoma C. Adenoid cystic carcinoma D. LG mucoepidermoid carcinoma Case 1 33




35 Diagnosis? A. PA B. Basal cell adenoma C. Adenoid cystic CA D. LG mucoepidermoid CA Case #2: Submandibular mass, 37 yo man Mucin vs. Stroma 34
36 The Many Cytologic Faces of Pleomorphic Adenoma Basal Cell Adenoma Adenoid Cystic Carcinoma Low grade malignancies such as LG mucoepidermoid CA and acinic cell CA FNA of Salivary Glands Summary Must exclude PA before making a diagnosis of another neoplasm Must exclude ACC and low grade malignancies before making a Dx of PA FNA can distinguish in most instances between basaloid neoplasms (ACC, BCA) and PA FNA of Salivary Glands Summary 2 Cellular neoplasm NOS (LG CA vs. B9) Familiarity with variable FNA appearances of SG tumors and awareness of potential pitfalls can prevent many false positive and negative diagnoses FNA should be interpreted in context of clinical and radiologic findings 35
Workshop 2. Controversies and Diagnostic Challenges in Head and Neck Cytopathology. Zubair Baloch, MD,PhD. Veracyte, Inc: Consultant
 Workshop 2 Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair Baloch, MD,PhD Veracyte, Inc: Consultant Tarik Elsheikh, MD There are no disclosures necessary. Controversies and
Workshop 2 Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair Baloch, MD,PhD Veracyte, Inc: Consultant Tarik Elsheikh, MD There are no disclosures necessary. Controversies and
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY. F ZAHRA ALY, MD, PhD
 ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology
 Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology Review some of the more common cytodiagnoses of the Head and Neck Establish an approach to some of the diagnostic
Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology Review some of the more common cytodiagnoses of the Head and Neck Establish an approach to some of the diagnostic
Salivary gland cytology. Salivary gland cytology. Triage helps the clinician. Salivary gland tumors. Diagnostic difficulties
 Salivary gland cytology Salivary Gland Cytology Pınar Fırat, MD Professor of Pathology İ.U. İstanbul Faculty of Medicine Çapa, İstanbul It is a reliable diagnostic test However, definitive subclassification
Salivary gland cytology Salivary Gland Cytology Pınar Fırat, MD Professor of Pathology İ.U. İstanbul Faculty of Medicine Çapa, İstanbul It is a reliable diagnostic test However, definitive subclassification
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
Disclosure of Relevant Financial Relationships
 Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Research Article Transmucosal Fine Needle Aspiration of Oral and Pharyngeal Lesions
 International Scholarly Research Network ISRN Pathology Volume 2011, Article ID 267145, 7 pages doi:10.5402/2011/267145 Research Article Transmucosal Fine Needle Aspiration of Oral and Pharyngeal Lesions
International Scholarly Research Network ISRN Pathology Volume 2011, Article ID 267145, 7 pages doi:10.5402/2011/267145 Research Article Transmucosal Fine Needle Aspiration of Oral and Pharyngeal Lesions
Dr Nick McIvor. Dr John Chaplin. Head & Neck Surgeon Auckland City Hospital Auckland. Auckland Head & Neck Surgeon Gillies Hospital Auckland
 Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Salivary gland Workshop Trondheim 31th may 2012
 Salivary gland Workshop Trondheim 31th may 2012 Peter Jebsen cytopathologist Oslo University Hospital Rikshospitalet Anna Bofin ass. Professor St. Olavs Hospital, Trondheim Drying artifacts Lymfocytes
Salivary gland Workshop Trondheim 31th may 2012 Peter Jebsen cytopathologist Oslo University Hospital Rikshospitalet Anna Bofin ass. Professor St. Olavs Hospital, Trondheim Drying artifacts Lymfocytes
Case #1 FNA of nodule in left lobe of thyroid in 67 y.o. woman
 Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu
 Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Educational Cases EQA November T.J. Palmer Raigmore Hospital Inverness
 Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
Salivary Gland FNA ATYPICAL : Criteria and Controversies
 Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Pathology of Selected Head and Neck Lesions. Adel Assaad MD Department of Pathology
 Pathology of Selected Head and Neck Lesions Adel Assaad MD Department of Pathology 1 NOSE Infections 2 Zygomycosis (Mucormycosis) Opportunistic infection caused by "bread mold fungi," including Rhizopus,
Pathology of Selected Head and Neck Lesions Adel Assaad MD Department of Pathology 1 NOSE Infections 2 Zygomycosis (Mucormycosis) Opportunistic infection caused by "bread mold fungi," including Rhizopus,
Head and Neck Case Studies
 Head and Neck Case Studies John Chaplin & Nick McIvor www.headneck.co.nz Head and Neck lumps every lump must have a diagnosis Working diagnosis» +/- investigations Review» +/- investigations auckland head
Head and Neck Case Studies John Chaplin & Nick McIvor www.headneck.co.nz Head and Neck lumps every lump must have a diagnosis Working diagnosis» +/- investigations Review» +/- investigations auckland head
Salivary ultrasound. Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK
 Salivary ultrasound Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK Two main groups of patients with presenting symptoms of: Obstructive or chronic inflammatory symptoms (salivary
Salivary ultrasound Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK Two main groups of patients with presenting symptoms of: Obstructive or chronic inflammatory symptoms (salivary
3/22/2017. Disclosure of Relevant Financial Relationships. Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Disclosure
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Disclosure
Cystic Head and Neck Lesions
 Cystic Head and Neck Lesions Disclosures None Brad Wright, MD 19 March 2018 Key points Huge variety of cystic lesions in H&N May be cystic, necrotic, or solid but cystic-appearing Patient age, clinical
Cystic Head and Neck Lesions Disclosures None Brad Wright, MD 19 March 2018 Key points Huge variety of cystic lesions in H&N May be cystic, necrotic, or solid but cystic-appearing Patient age, clinical
CN 925/15 History. Microscopic Findings
 CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Notice of Faculty Disclosures
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF SQUAMOUS CYSTS OF THE HEAD AND
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF SQUAMOUS CYSTS OF THE HEAD AND
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland
 Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Enterprise Interest None
 Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
Ultrasound Interpretation of Non-Thyroid Neck Pathology
 Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Introduction 10/27/2011. Follicular Lesion/Atypia of Undetermined Significance
 Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
ORIGINAL ARTICLE. Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population
 ORIGINAL ARTICLE Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population Erik G. Cohen, MD; Snehal G. Patel, MD; Oscar Lin, MD; Jay O. Boyle, MD; Dennis H. Kraus, MD; Bhuvanesh
ORIGINAL ARTICLE Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population Erik G. Cohen, MD; Snehal G. Patel, MD; Oscar Lin, MD; Jay O. Boyle, MD; Dennis H. Kraus, MD; Bhuvanesh
(CYLINDROMA) ATLAS OF HEAD AND NECK PATHOLOGY ADENOID CYSTIC CARCINOMA
 ATLAS OF HEAD AND NECK PATHOLOGY ADENOID CYSTIC CARCINOMA") (CYLINDROMA) This malignant tumor is poorly encapsulated and while seemingly well defined within the affected gland, there is usually infiltration of surrounding tissue on closer examination. The cut surface
(CYLINDROMA) This malignant tumor is poorly encapsulated and while seemingly well defined within the affected gland, there is usually infiltration of surrounding tissue on closer examination. The cut surface
PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD
 PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses CASE 1 Case 1 A 2
PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses CASE 1 Case 1 A 2
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
doi: /j.anl
 doi: 10.1016/j.anl.2006.07.001 Synchronous unilateral parotid gland neoplasms of three different histological types Shuho Tanaka 1, Keiji Tabuchi 1, Keiko Oikawa 1, Rika Kohanawa 1, Hideki Okubo 1, Dai
doi: 10.1016/j.anl.2006.07.001 Synchronous unilateral parotid gland neoplasms of three different histological types Shuho Tanaka 1, Keiji Tabuchi 1, Keiko Oikawa 1, Rika Kohanawa 1, Hideki Okubo 1, Dai
3/28/2017. Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center
 Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland
 The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
ISPUB.COM. Salivary duct carcinoma of parotid gland. V Kinnera, R Nandyala, M Yootla, K Mandyam INTRODUCTION CASE REPORT
 ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 V Kinnera, R Nandyala, M Yootla, K Mandyam Citation V Kinnera, R Nandyala, M Yootla, K Mandyam.. The Internet Journal of Pathology. 2008 Volume
ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 V Kinnera, R Nandyala, M Yootla, K Mandyam Citation V Kinnera, R Nandyala, M Yootla, K Mandyam.. The Internet Journal of Pathology. 2008 Volume
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
Imaging Work-Up of a Neck Mass - Adults & Children
 Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
FNA Biopsy of Salivary Gland
 FNA Biopsy of Salivary Gland Richard M. DeMay, MD Professor of Pathology Director of Cytopathology The University of Chicago Objective: To describe the use of FNA Bx to diagnose salivary gland lesions
FNA Biopsy of Salivary Gland Richard M. DeMay, MD Professor of Pathology Director of Cytopathology The University of Chicago Objective: To describe the use of FNA Bx to diagnose salivary gland lesions
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Basaloid neoplasms of the head and neck. Basaloid SCC. Clinico-pathologic features 5/5/11. Basaloid Tumors Head and Neck
 Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors
 An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Boston, MA An Integrated
An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Boston, MA An Integrated
Oncocytic carcinoma: A rare malignancy of the parotid gland
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
PAAF vs Core Biopsy en Lesiones Mamarias Case #1
 5/19/2014 PAAF vs Core Biopsy en Lesiones Mamarias Case #1 Fine Needle Aspiration Cytology of Breast: Correlation with Needle Core Biopsy 64-year-old woman Mass in breast Syed Hoda, MD CD31 Post-Radiation
5/19/2014 PAAF vs Core Biopsy en Lesiones Mamarias Case #1 Fine Needle Aspiration Cytology of Breast: Correlation with Needle Core Biopsy 64-year-old woman Mass in breast Syed Hoda, MD CD31 Post-Radiation
encapsulated thyroid nodule with a follicular architecture and some form of atypia. The problem is when to diagnose
 Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions
 Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Head and Neck SCC. HPV in Tumors of the Head and Neck. Overview. Role of HPV in Pathogenesis of Head & Neck Tumors
 HPV in Tumors of the Head and Neck Christina Kong, M.D. Associate Professor, Stanford Dept of Pathology Director, Cytopathology Laboratory & Cytopathology Fellowship ckong@stanford.edu Head and Neck SCC
HPV in Tumors of the Head and Neck Christina Kong, M.D. Associate Professor, Stanford Dept of Pathology Director, Cytopathology Laboratory & Cytopathology Fellowship ckong@stanford.edu Head and Neck SCC
Cytomorphological study of major salivary gland lesions: a 5-year experience at a tertiary care center
 Original article Cytomorphological study of major salivary gland lesions: a 5year experience at a tertiary care center Aruna S, Prathiksha Pai, Shreekant K. Kittur Department of Pathology, Belagavi Institute
Original article Cytomorphological study of major salivary gland lesions: a 5year experience at a tertiary care center Aruna S, Prathiksha Pai, Shreekant K. Kittur Department of Pathology, Belagavi Institute
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Imaging Technique. Ultrasound Imaging of the Salivary Glands. Parotid Gland. The Major Salivary Glands. Parotid Gland: Stenson s Duct.
 Ultrasound Imaging of the Salivary Glands Edward G. Grant MD Professor & Chairman, Dept of Radiology USC Keck School of Medicine edgrant@usc.edu edgrant@usc.edu Imaging Technique Linear array transducer
Ultrasound Imaging of the Salivary Glands Edward G. Grant MD Professor & Chairman, Dept of Radiology USC Keck School of Medicine edgrant@usc.edu edgrant@usc.edu Imaging Technique Linear array transducer
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Cytologic Evaluation of the Enlarged Neck Node: FNAC Utility in Metastatic Neck Disease
 ISPUB.COM The Internet Journal of Pathology Volume 6 Number 2 Cytologic Evaluation of the Enlarged Neck Node: FNAC Utility in Metastatic Neck Disease I Bagwan, S Kane, R Chinoy Citation I Bagwan, S Kane,
ISPUB.COM The Internet Journal of Pathology Volume 6 Number 2 Cytologic Evaluation of the Enlarged Neck Node: FNAC Utility in Metastatic Neck Disease I Bagwan, S Kane, R Chinoy Citation I Bagwan, S Kane,
Diagnostic Cytology of Cancer Cases
 Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases
 Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Thyroid pathology Practical part
 Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Human Papillomavirus and Head and Neck Cancer. Ed Stelow, MD
 Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017
 Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017 Dr Mary Toner Consultant Pathologist St James Hospital Trinity College
Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017 Dr Mary Toner Consultant Pathologist St James Hospital Trinity College
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
Congenital Neck Masses C. Stefan Kénel-Pierre, MD
 Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
Cytomorphological spectrum of pleomorphic adenoma with emphasis on differential diagnosis and diagnostic pitfalls
 Original Research Article DOI: 10.18231/2394-6792.2017.0102 Cytomorphological spectrum of pleomorphic adenoma with emphasis on differential diagnosis and diagnostic pitfalls Vaneet Kaur Sandhu 1,*, Navtej
Original Research Article DOI: 10.18231/2394-6792.2017.0102 Cytomorphological spectrum of pleomorphic adenoma with emphasis on differential diagnosis and diagnostic pitfalls Vaneet Kaur Sandhu 1,*, Navtej
PLEOMORPHIC ADENOMA ( BENIGN MIXED TUMOR )
") ( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery