Management of severe burns
|
|
|
- Ethel Campbell
- 5 years ago
- Views:
Transcription

1 Management of severe burns
2 Who gets admitted to the ICU? Large % surface area burns >25% adults >15% children/elderly Inhalational or airway burns Multi-trauma Co-morbidities


3 Burns centres Regional referral National Burns Centre >30% Prolonged ventilation >15% child/elderly Chemical Electrical

4 BURN=TRAUMA ultimate distracting injury RX as trauma EMST approach EMSB Burn specific care
5 Fundamentals of burn care Accurate burn assessment Early aggressive resuscitation Aggressive wound management and escharotomy Support of the patient until the wound is covered
6 LD50 is increasing Burn Size (%TBSA) Year
7 Basic First Aid STOP THE BURNING PROCESS COOL-running tap water, 20 minutes not of value >3 hours post burn minimise hypothermia COVER
8 What are the key determinants of burn severity? Depth Size Other very important factors Age Co-morbidities First aid Inhalation injury Other injuries

9 Burn depth

10

11 How do you assess burn area? Rule of 1 s Rule of 9 s Charts Only count dermal and full thickness burns
12 Wallace Rule of nine s
13 Lund & Browder chart

14 Paediatric burns assessment
15 Resuscitation Goals Minimise burn shock Maintain perfusion without fluid overload Fluids Adults >20% Paeds >10% Delay in fluid resus Inc mortality
16 Burn Shock The burn wound is a 3-dimensional mass of damaged tissue Loss of fluid/electrolytes and proteins into interstitium WCC release of vasoactive substrances Microthrombi

17 Burn Shock
18 How do we see this clinically?? Hypovolaemia Reduced UO,BP High Hct Oedema Low CO Lactate Other end organ injury Major burns non burnt tissue becomes oedematous

19 Fluid resuscitation- the formulae Modified Parkland formula 4 ml/kg/%tbsa burned/first 24 hours 50% over first 8 hours from injury 50% over next 16 hours MANY others e.g Brooke uses 2ml/kg/%SA Galveston & Shriners calc SA Military I:O ratio Required in adult >20% kid>10%
20 Fluid Therapy in burns- Monitoring response Invasive BP, pulse rate and pressure, cap refill Urine output Adults UO 0.5ml/kg/hr Kids <30kg 1ml/kg/hr Lactate Haematocrit Na- useful >24hr

21 Must not set and forget The minute by minute, hour by hour titration of volume to effect Resuscitation endpoints: BP, urine, capillary refill, lactate, Hb, sodium ScvO2, PiCCO, echocardiography Avoid boluses if possible
22 Enteral Which fluid? First 24 hours Buffered isotonic crystalloid Plasmalyte (WARMED!) Colloid- NOT synthetic! 4% albumin Cochrane review 2011 no reduction mortality?after 24hr?12hr Transfuse RBC as needed Significant blood loss when debriding

23 FLUID CREEP Oedema Local Ischaemia Conversion of zone of stasis Generalised Airway Pulmonary Gut Limbs Jackson burn wound model Zone coagulation Zone stasis Zone hyperaemia
24 Complications of fluid resuscitation Limb ischaemia/ compartment syndrome Abdominal compartment syndrome Gut oedema Abdominal wall burns Very poor outcome especially if laparostomy is required May occur within 24 hours
25 Abdominal compartment syndrome

26 Airway Major burns Swelling 1-3hr post injury and continues normal tissue swell Intubate early Avoid suxamethonium >24hr post injury Beware cuff leak Secure- screw or wire
27 Guide only Assessment VERY hard size and weight of patient 100kg 55% burn = 22L in 24hr 85kg 43% =14.6L Doesn t take into account depth of burn Delayed resuscitation Tends to underestimate fluid requirements Pre-existing dehydration, other injuries, electrical etc.

28 Maxillary screw Not in children Wire cutters to remove

29 Inhalational injury Doubles the mortality rate Mortality trends don t follow recent improvements in cutaneous burns Injury Above larynx-heat Below larynx- chemical Systemic toxicity
30 Inhalational injury Supplemental O 2 (humidified) 100% if CO inhalation suspected Decreases half life from 2.5 hours to 40 mins Early intubation prior to swelling Bronchoscopy Lung protective ventilation Advanced ventilation- ECMO, oscillator
31 Exam question Outline the pathophysiology and clinical features of a smoke inhalation injury in a patient with major burns

32 Escharotomy Escharotomy NOT fasciotomy Fasciotomy for compartment syndrome- incise fascia


33 Escharotomy

34 EMSB Primary survey Resuscitation Secondary survey Investigations NG Tetanus Analgesia Documentation & Disp

35 Complications AVOID HYPOTHERMIA Cover Clean dressing SSD-discuss Heated rooms and fluids
36 Most important issue in burn care DEBRIDEMENT AND EARLY COVERAGE

37 OR Scrub down Debridement Grafting Dressing changes
38 The Function of a burn dressing Comfort Metabolic Protective IDEAL DRESSING Facilitate wound healing Acceptable appearance Promote comfort & function Cheap & easy to handle
39 Basic Principals There is NO perfect dressing different dressings achieve different things The ultimate dressing is the patient s own skin via spontaneous healing or via grafting

40 Aggressive wound care Cut off the eschar as early as possible and close the wound Improved mortality and length of stay Issues surround coverage of wounds Ideally with autograft Not usually possible with large burns. Skin substitutes Buy time until grafting or healing occurs
41 Wound care Topical agents Compresses gauze, silver containing (Acticoat) Biosynthetics Dermal replacement/biologics Barrier Waterproof and breathable

42 SSD Silver sulphadiazine Delivers silver to the wound Antiimicrobial and inflammatory Messy Forms pseudoeschar CI- pregnancy, <2/12 old
43 Nomenclature of dermal replacements Allograft = cadaver = homograft Autograft = patients own skin Increases burn area = donor site Xenograft = pig Synthetic skin substitutes Cultured epithelial autograft
44 2 layer membrane Biobrane Inner- allows nylon allows fibrovascular ingrowth Outer silastic- barrier to fluid and bacteria Uses Typically used Donor site Dressing over autograft / allograft Toxic epidermal necrolysis

45 Allograft= Cadaver Temporary skin cover Needs vascular bed Rejected 14-21/7
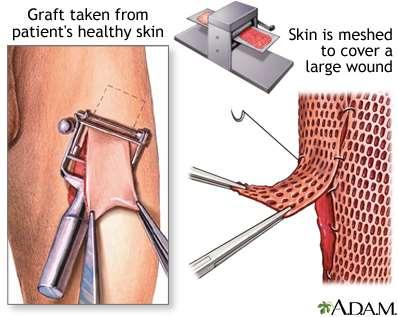
46 Autograft
47 Integra Bilaminar dermal replacement Silicone, collagen & glycosaminoglycans Creates a neodermis Infiltration by host fibroblasts & neovascularisation Thin split skin graft over Intolerant of wound infection Expensive
48 Skin Culture Autograft Epidermal cells are replicated But.. No dermis Fragile graft Approx 50% take Cost
49 Support until wound coverage Organ support Analgesia Background Cover procedures Temperature Nutrition
50 Prevent infection Nurse in isolation Aggressive infection surveillance Early wound care Prophylactic antibiotics No evidence unless contaminated Rectal tube Antibiotic impregnated lines
51 Infection GNB wound infection can kill in hours Vigilant Early signs Gut distension/ng asps Loss of glucose control UO tails off Inotropes whiff Low temp-consider what s normal
52 Infection Theatre for review- don t delay Antibiotics Previous micro Gram negative cover Consider other source once wounds excluded
53 Hypermetabolic response to burns BSA >25% Begins within 5/7 lasts upto 12months Ebb phase <48hr Low CO, metabolic rate, glucose intolerance Flow phase Within 5/7 Hyperdynamic and hypermetabolic Oxandrolone, Bblockers, rhgh
54 Analgesic agents Opioids Morphine, methadone, fentanyl Anaesthetic agents Ketamine, benzodiazepines Non opioids Paracetamol, Gabapentin, NSAIDs
55 Nutrition NJ tube Supplements- zinc, folate, multivits REE
56 With respect to the clinical assessment of a patient presenting with a severe burn injury sustained in a house fire: a) Outline how burns are classified. b) List three methods for estimating the total body surface area affected by a burn injury. c)other than the burn type and extent,list the other important features of the physical examination that should be noted as part of the initial clinical assessment of the patient described above.
57 55yo 60% burn some debridement and grafting Returns from OR following further debridement BP 85/50 Outline causes and Mx of his hypotension
58 Other considerations DVT prophylaxis Control of bowels Ulcer prophylaxis Eye care Family
59 Burns hot case Exam limited! If early <48hr Resus Other traumatic injuries Toxins CO ARDS ventilation Escharotomies Later Infection Oedema Nutrition
60 Anabolic agents Human Growth Hormone Accelerate donor healing Restore nitrogen balance Oxandrolone Beta- blocking agents Anti catabolic agent
61 Key points Burns=trauma Look for other injuries First aid vital Assess size and depth Fluid formulas a guide only Circumferential burns Prevent hypothermia
62 Summary The severely burned patient is a trauma patient Challenging Time and resource consuming Early aggressive resuscitation, and definitive wound care defines outcome Requires a multi-disciplinary team approach
BURNS MODULE. In the paediatric population consider non-accidental injury as a mechanism for burn injuries.
 BURNS MODULE INTRODUCTION Burns are a common cause of trauma. Most burn injuries are a result of flame burns, with scalds also occurring commonly. Electrical and chemical burns are less common. 1 Concurrent
BURNS MODULE INTRODUCTION Burns are a common cause of trauma. Most burn injuries are a result of flame burns, with scalds also occurring commonly. Electrical and chemical burns are less common. 1 Concurrent
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 46 Caring for Clients with Burns Types of Burns Thermal Dry heat flame Moist heat steam or hot liquid
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 46 Caring for Clients with Burns Types of Burns Thermal Dry heat flame Moist heat steam or hot liquid
Burn Management. Praz Patcha, MD 13 March 2014
 Burn Management Praz Patcha, MD 13 March 2014 Epidemiology 500,000 / yr 40,000 to 60,000 requiring admission < 1% total injuries in US but $10.4 billion Risk Factors Age Location Demographics Socioeconomics
Burn Management Praz Patcha, MD 13 March 2014 Epidemiology 500,000 / yr 40,000 to 60,000 requiring admission < 1% total injuries in US but $10.4 billion Risk Factors Age Location Demographics Socioeconomics
Appendix. Sedatives and Pain Medications. Gabapentin ( mg po q8h) or Pregabalin ( mg po q8h)
 or Pregabalin ( mg po q8h)") Appendix Sedatives and Pain Medications Non-intubated patients Non-opioid analgesics Acetaminophen (500 1,000 mg po q6h) NSAID (Ibuprofen, Naprosyn, Celebrex) Gabapentin (100 300 mg po q8h) or Pregabalin
Appendix Sedatives and Pain Medications Non-intubated patients Non-opioid analgesics Acetaminophen (500 1,000 mg po q6h) NSAID (Ibuprofen, Naprosyn, Celebrex) Gabapentin (100 300 mg po q8h) or Pregabalin
EmergencyKT: Management of Thermal Injury in Adult Patients
 EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator
 Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department
 Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department Functions Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or
Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department Functions Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test
 Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
Responsibility This guideline applies to teams of health professions caring for burn patients.
 Page 1 of 9 Guideline: Initial Assessment & Management of Burn Injuries Purpose This document provides a guideline for the initial assessment and management of burn patients. It is not intended as a full
Page 1 of 9 Guideline: Initial Assessment & Management of Burn Injuries Purpose This document provides a guideline for the initial assessment and management of burn patients. It is not intended as a full
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Burn Injuries & Its Management M JARI.MD
 Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Printed copies of this document may not be up to date, obtain the most recent version from Author Position
 Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle Author Position PICU/BURNS Consultant CATS Consultant Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle Author Position PICU/BURNS Consultant CATS Consultant Document Owner E. Polke
Burn & Soft Tissue Service Orientation Slides
 Burn & Soft Tissue Service Orientation Slides Damien Wilson Carter, MD Director, Burn/Soft Tissue Service Sue Reeder, BSN, CWOCN Burn Resource Nurse Specialist Scope ALL Burn injuries (> Age 12) Cold injury/
Burn & Soft Tissue Service Orientation Slides Damien Wilson Carter, MD Director, Burn/Soft Tissue Service Sue Reeder, BSN, CWOCN Burn Resource Nurse Specialist Scope ALL Burn injuries (> Age 12) Cold injury/
Printed copies of this document may not be up to date, obtain the most recent version from Author Position
 Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle, L Chigaru Author Position PICU/BURNS Consultant CATS Consultants Document
Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle, L Chigaru Author Position PICU/BURNS Consultant CATS Consultants Document
Burn Priorities of Care: Triage/Treatment/Transfer. Via Christi Regional Burn Center Sarah Fischer, MSN, RN
 Burn Priorities of Care: Triage/Treatment/Transfer Via Christi Regional Burn Center Sarah Fischer, MSN, RN Disclosure I have nothing to disclose Objectives Identify American Burn Association referral criteria
Burn Priorities of Care: Triage/Treatment/Transfer Via Christi Regional Burn Center Sarah Fischer, MSN, RN Disclosure I have nothing to disclose Objectives Identify American Burn Association referral criteria
Applicable to. Team Members Performing MD House Staff APRN/PA RN LPN
 Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 Burn Care and Management WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A., RN.ORG,
Burn Care and Management WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A., RN.ORG,
Wisecracks 1. What are the indications for an escharotomy 2. What are the primary considerations in mechanical ventilation of burn patients
 Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Approved By: Airway and Breathing A. Initially give humidified high flow oxygen at 15 L (100%) using a nonrebreather
 using a nonrebreather") Subject: BURN CARE CLINICAL GUIDELINE Originator: Approval Date: 2015 Approved By: Policy: All burn patients presenting to XXXXXX Hospital will have appropriate assessment, stabilization and evaluation
Subject: BURN CARE CLINICAL GUIDELINE Originator: Approval Date: 2015 Approved By: Policy: All burn patients presenting to XXXXXX Hospital will have appropriate assessment, stabilization and evaluation
Objectives. Initial Burn Care and Fluid Resuscitation 6/5/2015 INITIAL MANAGEMENT
 Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline
 TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
Advanced Paediatric Nursing. Burn Trauma. 26 April Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH
, Burns Centre, Surgery, PWH") Advanced Paediatric Nursing Burn Trauma 26 April 2016 Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH Objective: Understand burn trauma in children Understand Important nursing interventions in burn
Advanced Paediatric Nursing Burn Trauma 26 April 2016 Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH Objective: Understand burn trauma in children Understand Important nursing interventions in burn
Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns.
 Major Burns HELI.CLI.08 Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns. Procedure Management of Severe Burns For Review Aug 2015 1. Introduction
Major Burns HELI.CLI.08 Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns. Procedure Management of Severe Burns For Review Aug 2015 1. Introduction
Chapter 23 Caring for Clients with Burns
 Chapter 23 Caring for Clients with Burns Burn Injuries 4500 people die from burns each year High risk group ~ children and the elderly The most common cause of burns Smoking material Scalding Lighting
Chapter 23 Caring for Clients with Burns Burn Injuries 4500 people die from burns each year High risk group ~ children and the elderly The most common cause of burns Smoking material Scalding Lighting
IMMEDIATE EMERGENCY BURN CARE » THERMAL BURNS » ELECTRICAL BURNS » CHEMICAL BURNS FIRST AID FOR THE THREE MAJOR CATEGORIES
 IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Burns. A Comprehensive Review Assessment & Management
 Burns A Comprehensive Review Assessment & Management 1 Objectives Understand types of Burns Understand the pathophysiology of the Burns Understand Rule of Nine Understand Classification of Burns Identify
Burns A Comprehensive Review Assessment & Management 1 Objectives Understand types of Burns Understand the pathophysiology of the Burns Understand Rule of Nine Understand Classification of Burns Identify
Burn injury. A : patent airway with smoking inhalation, stridor. D: E4V5M6,pupil 2mm RTLBE
 Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
Burns Management in the Emergency Department
 Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Sidney Miller, MD, FACS Professor of Surgery Director of Research and Development Ohio State University Burn Center
 Management of the Burn Patient Sidney Miller, MD, FACS Professor of Surgery Director of Research and Development Ohio State University Burn Center American Burn Association Transfer Criteria Burn > 10%
Management of the Burn Patient Sidney Miller, MD, FACS Professor of Surgery Director of Research and Development Ohio State University Burn Center American Burn Association Transfer Criteria Burn > 10%
Dr. Muhammad Shamim. FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg)
, FACS (USA), FICS (USA), MHPE (Nl & Eg)") Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Salman bin Abdulaziz University Email: surgeon.shamim@gmail.com Web: surgeonshamim.com
Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Salman bin Abdulaziz University Email: surgeon.shamim@gmail.com Web: surgeonshamim.com
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Wound Care in the Community. Lisa Sutherland MSc Tissue Viability Senior Lead Ipswich Hospital & Community NHS Trusts
 Wound Care in the Community Lisa Sutherland MSc Tissue Viability Senior Lead Ipswich Hospital & Community NHS Trusts What are the key elements? What is the patient s goal or aim for the wound? What are
Wound Care in the Community Lisa Sutherland MSc Tissue Viability Senior Lead Ipswich Hospital & Community NHS Trusts What are the key elements? What is the patient s goal or aim for the wound? What are
Advances in Paediatric Burn Management. Bernard Carney Burns Unit Women s and Children s Hospital
 Advances in Paediatric Burn Management Bernard Carney Burns Unit Women s and Children s Hospital WCH Paediatric burns service Women s and Children s Hospital 0 to 18 years of age 200-220 inpatients 350-400
Advances in Paediatric Burn Management Bernard Carney Burns Unit Women s and Children s Hospital WCH Paediatric burns service Women s and Children s Hospital 0 to 18 years of age 200-220 inpatients 350-400
Pediatrics Grand Rounds 1 June University of Texas Health Science Center at San Antonio. Management of Burn Wounds. Management of Burn Wounds
 Management of Burn Wounds Management of Burn Wounds History of Burn Care Pathophysiology of Burn Lillian F. Liao, MD, MPH Division of Trauma and Emergency Surgery Department of Surgery UTHSCSA Acute burn
Management of Burn Wounds Management of Burn Wounds History of Burn Care Pathophysiology of Burn Lillian F. Liao, MD, MPH Division of Trauma and Emergency Surgery Department of Surgery UTHSCSA Acute burn
Burn Resuscitation Formulas. John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX
 Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
EMERGENCYROOM BURN MANAGEMENT
 EMERGENCYROOM INITIAL ASSESSMENT PRIMARY SURVEY A = Airway and C-spine immobilization B = Breathing and Ventilation C = Circulation D = Disability, Neurologic Deficit E = Expose (remove all clothing and
EMERGENCYROOM INITIAL ASSESSMENT PRIMARY SURVEY A = Airway and C-spine immobilization B = Breathing and Ventilation C = Circulation D = Disability, Neurologic Deficit E = Expose (remove all clothing and
Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie
 Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie History 3 yo boy, presents to pediatric ED with mother Child can be heard crying inside waiting/patient room, has both hands bandaged
Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie History 3 yo boy, presents to pediatric ED with mother Child can be heard crying inside waiting/patient room, has both hands bandaged
Management of Acute Burn Injuries: The First 24 Hours
 Speaker Disclosure I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. I will not discuss off label uses of any pharmaceutical products or medical devices. Management of Acute
Speaker Disclosure I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. I will not discuss off label uses of any pharmaceutical products or medical devices. Management of Acute
Modern management of paediatric burns
 Modern management of paediatric burns Burn injuries pose a major threat to children in South Africa and remain a devastating injury, because of the resulting severe emotional and physical scarring and
Modern management of paediatric burns Burn injuries pose a major threat to children in South Africa and remain a devastating injury, because of the resulting severe emotional and physical scarring and
Cellular and Tissue Effects. Pathophysiology of the Burn Wound. Special Topics: Thermal Burns & Smoke Inhalation
 Special Topics: Thermal Burns & Smoke Inhalation MEDICAL RESPONDER AND RECEIVER SEMINAR; EXPLOSION AND BLAST INJURIES Pathophysiology of the Burn Wound The burn wound is the source of virtually all ill
Special Topics: Thermal Burns & Smoke Inhalation MEDICAL RESPONDER AND RECEIVER SEMINAR; EXPLOSION AND BLAST INJURIES Pathophysiology of the Burn Wound The burn wound is the source of virtually all ill
Management of Burns under Prolonged Field Care
 This Role 1, prolonged field care (PFC) guideline is intended to be used after TCCC Guidelines when evacuation to higher level of care is not immediately possible. A provider of PFC must first and foremost
This Role 1, prolonged field care (PFC) guideline is intended to be used after TCCC Guidelines when evacuation to higher level of care is not immediately possible. A provider of PFC must first and foremost
At the conclusion of this course the learner will be able to
 Objectives At the conclusion of this course the learner will be able to 1. Discuss basic anatomy and pathophysiology of burns 2. Describe burn injuries in terms of size, depth, coloration and characteristics
Objectives At the conclusion of this course the learner will be able to 1. Discuss basic anatomy and pathophysiology of burns 2. Describe burn injuries in terms of size, depth, coloration and characteristics
Acute And perioperative care of the burn-injured patient. Anesthesiology, V 122, No 2
 Acute And perioperative care of the burn-injured patient Anesthesiology, V 122, No 2 Reporter:R4 沈士鈞 Supervisor: 蔡欣怡醫師 Pathophysiology Initial evaluation and management Anesthetic managemen nt Pathophysiology
Acute And perioperative care of the burn-injured patient Anesthesiology, V 122, No 2 Reporter:R4 沈士鈞 Supervisor: 蔡欣怡醫師 Pathophysiology Initial evaluation and management Anesthetic managemen nt Pathophysiology
TITLE OF CASE: Burn Injuries and Management
 TITLE OF CASE: Burn Injuries and Management AUTHOR OF CASE: Magdalena Malinowska SUMMARY: Patient is a 23 year old female who was brought in by EMS to the Emergency Room post a motor vehicle accident in
TITLE OF CASE: Burn Injuries and Management AUTHOR OF CASE: Magdalena Malinowska SUMMARY: Patient is a 23 year old female who was brought in by EMS to the Emergency Room post a motor vehicle accident in
Thermal Injuries. Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03
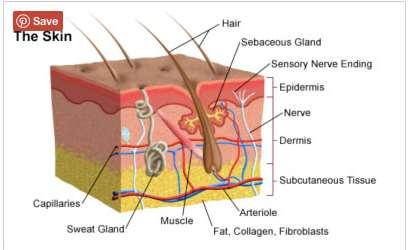
 Thermal Injuries Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03 INTRODUCTION Anatomy of the skin The skin has three anatomical layers Epidermis Dermis Subcutaneous
Thermal Injuries Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03 INTRODUCTION Anatomy of the skin The skin has three anatomical layers Epidermis Dermis Subcutaneous
Research Article The Introduction of a Protocol for the Use of Biobrane for Facial Burns in Children
 Hindawi Publishing Corporation Plastic Surgery International Volume 2011, Article ID 858093, 5 pages doi:10.1155/2011/858093 Research Article The Introduction of a Protocol for the Use of Biobrane for
Hindawi Publishing Corporation Plastic Surgery International Volume 2011, Article ID 858093, 5 pages doi:10.1155/2011/858093 Research Article The Introduction of a Protocol for the Use of Biobrane for
Management of Complex Wounds with Vacuum Assisted Closure
 Management of Complex Wounds with Vacuum Assisted Closure Wendy McInnes Vascular / Wound Nurse Practitioner The Queen Elizabeth Hospital, Adelaide, South Australia Treasurer ANZSVN wendy.mcinnes@health.sa.gov.au
Management of Complex Wounds with Vacuum Assisted Closure Wendy McInnes Vascular / Wound Nurse Practitioner The Queen Elizabeth Hospital, Adelaide, South Australia Treasurer ANZSVN wendy.mcinnes@health.sa.gov.au
LRI Emergency Department. Burn injuries management in adults
 LRI Emergency Department Clinical guideline for: Burn injuries management in adults Authors: Approved by: Martin Wiese Reena Agarwal Claire Porter EF guidelines committee Approval date: 21 Sep 16 Approval
LRI Emergency Department Clinical guideline for: Burn injuries management in adults Authors: Approved by: Martin Wiese Reena Agarwal Claire Porter EF guidelines committee Approval date: 21 Sep 16 Approval
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Appropriate Dressing Selection For Treating Wounds
 Appropriate Dressing Selection For Treating Wounds Criteria to Consider for an IDEAL DRESSING Exudate Management Be able to provide for moist wound healing by absorbing exudate or adding moisture Secure
Appropriate Dressing Selection For Treating Wounds Criteria to Consider for an IDEAL DRESSING Exudate Management Be able to provide for moist wound healing by absorbing exudate or adding moisture Secure
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
BASICS OF BURN MANAGEMENT
 BASICS OF BURN MANAGEMENT Dr S M Keswani Cosmetic Surgeon National Burns Centre, Airoli,Navi-Mumbai Breach Candy Hospital Wockhardt Hospital National Burns Centre, Airoli, Navi-Mumbai. CLASSIFICATION 1.
BASICS OF BURN MANAGEMENT Dr S M Keswani Cosmetic Surgeon National Burns Centre, Airoli,Navi-Mumbai Breach Candy Hospital Wockhardt Hospital National Burns Centre, Airoli, Navi-Mumbai. CLASSIFICATION 1.
Initial assessment. ATLS/ABLS protocol and assess for other injuries/fractures based on mechanism. Inhalational injury. Vascular compromise:
 Complex Hand Burns Brent Egeland, MD Assistant Professor Dell Medical School Department of Surgery and Perioperative Care Institute of Reconstructive Plastic Surgery Plastic, Hand, and Reconstructive Microsurgery
Complex Hand Burns Brent Egeland, MD Assistant Professor Dell Medical School Department of Surgery and Perioperative Care Institute of Reconstructive Plastic Surgery Plastic, Hand, and Reconstructive Microsurgery
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose.
 Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. Debbie Harrell RN, MSN, Shriners Hospitals for Children Cincinnati Cincinnati, Ohio
Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. Debbie Harrell RN, MSN, Shriners Hospitals for Children Cincinnati Cincinnati, Ohio
Burn wounds - Determining the size and type degree
 1 Burn wounds - Determining the size and type degree Determining surface area of burn (Open hand only for small burns) 1 2 Burn depth Most burns are a combination of superficial and deeper burns and the
1 Burn wounds - Determining the size and type degree Determining surface area of burn (Open hand only for small burns) 1 2 Burn depth Most burns are a combination of superficial and deeper burns and the
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
BLS, ILS, ALS OTEP BURNS BURN INTRODUCTION TYPES OF BURNS
 BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
Burn Wound Assessment and Infections
 Burn Wound Assessment and Infections Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Family Health:
Burn Wound Assessment and Infections Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Family Health:
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
MY STRATEGY FOR TREATING BURN INJURIES. Warren Garner MD FACS Keck School of Medicine at USC Los Angeles, CA
 MY STRATEGY FOR TREATING BURN INJURIES Warren Garner MD FACS Keck School of Medicine at USC Los Angeles, CA ASSUMPTIONS: Burns which heal to normal have best outcome. Medical risk, functional recovery,
MY STRATEGY FOR TREATING BURN INJURIES Warren Garner MD FACS Keck School of Medicine at USC Los Angeles, CA ASSUMPTIONS: Burns which heal to normal have best outcome. Medical risk, functional recovery,
Small Animal Benchmark May 2013
 Small Animal Benchmark May 2013 A 5-year-old MC yellow Laborador Retriever (35 kg) is referred for management of the burn injury depicted below. This injury was suspected to have been sustained from prolonged
Small Animal Benchmark May 2013 A 5-year-old MC yellow Laborador Retriever (35 kg) is referred for management of the burn injury depicted below. This injury was suspected to have been sustained from prolonged
Advazorb. Hydrophilic foam dressing range
 Advazorb Hydrophilic foam dressing range Advazorb A comprehensive range of patient friendly, absorbent foam dressings Non-adhesive and atraumatic silicone adhesive options Designed to manage exudate whilst
Advazorb Hydrophilic foam dressing range Advazorb A comprehensive range of patient friendly, absorbent foam dressings Non-adhesive and atraumatic silicone adhesive options Designed to manage exudate whilst
CARE OF PATIENTS WITH BURNS. NUR 240 Donna Ricketts, MSN, RN, OCN
 CARE OF PATIENTS WITH BURNS NUR 240 Donna Ricketts, MSN, RN, OCN INCIDENCE/PREVALENCE OF BURN INJURY 5 th most common unintentional injury deaths 3 rd leading cause of fatal home injuries 4,000 burn deaths
CARE OF PATIENTS WITH BURNS NUR 240 Donna Ricketts, MSN, RN, OCN INCIDENCE/PREVALENCE OF BURN INJURY 5 th most common unintentional injury deaths 3 rd leading cause of fatal home injuries 4,000 burn deaths
Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6
 Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES
 INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
Thermal Burns PFN: SOMEML07. Terminal Learning Objective. References. Hours: 3.0 Instructor: Action: Communicate knowledge of thermal burns
 Thermal Burns PFN: SOMEML07 Hours: 3.0 Instructor: Slide 1 Terminal Learning Objective Action: Communicate knowledge of thermal burns Condition: Given a lecture in a classroom environment Standard: Received
Thermal Burns PFN: SOMEML07 Hours: 3.0 Instructor: Slide 1 Terminal Learning Objective Action: Communicate knowledge of thermal burns Condition: Given a lecture in a classroom environment Standard: Received
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Guidelines for the management of paediatric burns
 Guidelines for the management of paediatric burns Are there signs of airway injury? If yes contact anaesthetist! Is burn TBSA >10% If appropriate COOL THE BURN! Heat room. Insert IVC. Obtain FBC, U&,E
Guidelines for the management of paediatric burns Are there signs of airway injury? If yes contact anaesthetist! Is burn TBSA >10% If appropriate COOL THE BURN! Heat room. Insert IVC. Obtain FBC, U&,E
Modern management of paediatric burns
 Modern management of paediatric burns Burn injuries pose a major threat to children in South Africa and remain a devastating injury, because of the resulting severe emotional and physical scarring and
Modern management of paediatric burns Burn injuries pose a major threat to children in South Africa and remain a devastating injury, because of the resulting severe emotional and physical scarring and
The Parkland Formula Under Fire: Is the Criticism Justified?
 The Parkland Formula Under Fire: Is the Criticism Justified? Jennifer Blumetti, MD, John L. Hunt, MD, Brett D. Arnoldo, MD, Jennifer K. Parks, MPH, Gary F. Purdue, MD Controversy has continued regarding
The Parkland Formula Under Fire: Is the Criticism Justified? Jennifer Blumetti, MD, John L. Hunt, MD, Brett D. Arnoldo, MD, Jennifer K. Parks, MPH, Gary F. Purdue, MD Controversy has continued regarding
Intro Who should read this document 2 Key practice points 2 What is new in this version 3 Background 3 Guideline Subsection headings
 Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Appropriate use of silver dressings
 Appropriate use of silver dressings David Keast, Center Director, Aging Rehabilitation and Geriatric Care Research Centre, St Joseph s Parkwood Hospital, London, Ontario, Canada Role of antimicrobial dressings
Appropriate use of silver dressings David Keast, Center Director, Aging Rehabilitation and Geriatric Care Research Centre, St Joseph s Parkwood Hospital, London, Ontario, Canada Role of antimicrobial dressings
Update on Burn Care and Resuscitation
 Niknam Eshraghi, M.D., F.A.C.S General and Burn Surgery; The Oregon Clinic Director; Oregon Burn Center, Legacy Emanuel Medical Center Affiliate Professor of Surgery, Oregon Health Sciences University
Niknam Eshraghi, M.D., F.A.C.S General and Burn Surgery; The Oregon Clinic Director; Oregon Burn Center, Legacy Emanuel Medical Center Affiliate Professor of Surgery, Oregon Health Sciences University
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Post Resuscitation Care
 Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Northern Burn Care Operational Delivery Network Referral Information Pack
 Northern Burn Care Operational Delivery Network Referral Information Pack Northern Burn Care ODN Burns Referral Pack Pack includes: 1. NBCODN Burns services Contact information 2. Burns Referral Flow chart.
Northern Burn Care Operational Delivery Network Referral Information Pack Northern Burn Care ODN Burns Referral Pack Pack includes: 1. NBCODN Burns services Contact information 2. Burns Referral Flow chart.
Epidemiology. Burn Rehabilitation. Epidemiology. Epidemiology. United States. United States Cause of injury. Incidence has declined
 Burn Rehabilitation Peter Esselman, MD Professor and Chair Department of Rehabilitation Medicine University of Washington Epidemiology United States 450,000 burn injuries/year in USA that receive medical
Burn Rehabilitation Peter Esselman, MD Professor and Chair Department of Rehabilitation Medicine University of Washington Epidemiology United States 450,000 burn injuries/year in USA that receive medical
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
DOCUMENT CONTROL PAGE
 DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
Proceedings of the 36th World Small Animal Veterinary Congress WSAVA
 www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Patient Details Hospital number NHS number. Surname First name DOB. Permanent address. Post code. Mobile No. Temporary. Mother DOB. Father.
 Burns Unit Page 12 Paediatric Burn Injuries - Assessment & Admission Burns Unit Page 1 Discharge Patient Details Hospital number NHS number Admission date Injury date Hospital Use time time Time: Discharge
Burns Unit Page 12 Paediatric Burn Injuries - Assessment & Admission Burns Unit Page 1 Discharge Patient Details Hospital number NHS number Admission date Injury date Hospital Use time time Time: Discharge
Essex and Herts Air Ambulance Trust (EHAAT) Essex and Herts Air Ambulance: a focused case series for pre-hospital practice
 Essex and Herts Air Ambulance: a focused case series for pre-hospital practice") Essex and Herts Air Ambulance: a focused case series for pre-hospital practice Case 1: management of a paediatric burn Erica Ley, critical care paramedic, Essex and Herts Air Ambulance; Adam Chesters,
Essex and Herts Air Ambulance: a focused case series for pre-hospital practice Case 1: management of a paediatric burn Erica Ley, critical care paramedic, Essex and Herts Air Ambulance; Adam Chesters,
January Adult Burn Injured patients
 Guideline Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version goes out of date): Explicit definition
Guideline Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version goes out of date): Explicit definition
We look forward to serving you.
 ADVANCED CARE GEMCORE360 offers healthcare professionals a simple, clear and cost-effective wound care range while ensuring excellent clinical outcomes for their patients. 1 At GEMCO Medical, we strive
ADVANCED CARE GEMCORE360 offers healthcare professionals a simple, clear and cost-effective wound care range while ensuring excellent clinical outcomes for their patients. 1 At GEMCO Medical, we strive
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital. Mr Adam Bialostocki Plastic Surgeon, Tauranga
 Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital Mr Adam Bialostocki Plastic Surgeon, Tauranga Mr. Adam Bialostocki Plastic Surgeon Minor Burns First Aid Remove the burning agent / wet clothes
Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital Mr Adam Bialostocki Plastic Surgeon, Tauranga Mr. Adam Bialostocki Plastic Surgeon Minor Burns First Aid Remove the burning agent / wet clothes
Lower Extremity Wound Evaluation and Treatment
 Lower Extremity Wound Evaluation and Treatment Boni-Jo Silbernagel, DPM Describe effective lower extremity wound evaluation and treatment. Discuss changes in theories of treatment in wound care and implications
Lower Extremity Wound Evaluation and Treatment Boni-Jo Silbernagel, DPM Describe effective lower extremity wound evaluation and treatment. Discuss changes in theories of treatment in wound care and implications
Partnering the burn community
 * At smith&nephew we seek imaginative solutions that improve wound outcomes for patients and at the same time conserve resources for healthcare systems. Partnering the burn community Dedicated to the management
* At smith&nephew we seek imaginative solutions that improve wound outcomes for patients and at the same time conserve resources for healthcare systems. Partnering the burn community Dedicated to the management
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation