بسم هللا الرحمن الرحيم
|
|
|
- Catherine Boyd
- 5 years ago
- Views:
Transcription
1 بسم هللا الرحمن الرحيم
2 Pediatric Asthma Case Scenario Adel Reyad
3 Case Presentation Sara is a 30-month-old girl who has about 4-month history of a runny nose and coughing. The cough seems to be worse during the night and early morning.
4 Case Presentation For the last 3 nights, cough has interrupted her sleep. Several cough preparations have been tried and have failed.
5 Case Presentation She was recently seen by a pediatrician who prescribed Montelukast, but no improvement has been observed. There has been no fever.
6 Case Presentation Father is a smoker, but tries not to smoke in the house or in the car.
7 Medical History: She is a full-term girl, delivered by SVD. Breast-fed for first 2 months.
8 Medical History: She had skin problems (dryness and erythema in the face and neck) from the age of 6 months to 1 year. She was treated with skin emollients and topical hydrocortisone.
9 Family History: Father had frequent "bronchitis" until age of 12 years. Mother has morning sneezing with clear rhinorrhea. Sister, aged 5 years, is healthy.
10 Social History: Father works in an IT firm. Mother is a house-wife. Child attends daycare.
11 Review of Systems: Negative (other than respiratory).
12 Current Medications: Montelukast, 4 mg chewable tab every night Over-the-counter cough suppressants for symptom relief 3 to 4 times a week. Salbutamol syrup
13 Physical Exam: Height is in 75th percentile, weight in 50th percentile. Adequate progress observed in the growth chart since birth. Active, alert, happy child.
14 Physical Exam: Normal ears and throat exam and no rhonchi or wheezing detected on auscultation with the child at rest.
15 Physical Exam: The mother was asked to take the child to the corridor and play area and have her run until tired and return while still breathing rapidly.
16 Physical Exam: On subsequent auscultation, a few scattered expiratory wheezes were detected in both lungs. Some skin dryness but no active skin lesions were present.
17 Lab Tests: Complete blood count : normal CRP : negative. A chest film performed 3 weeks ago was read as normal.
18 Case Discussion
19 Diagnosis and Differential Diagnosis
20 HOW TO DIAGNOSE ASTHMA?


21 Asthma can be diagnosed by patient's symptoms medical history.

22 HISTORY NIGHT DAY CORTISONE LEVEL
23 Timing of cough



24 WORS T Day time Night time BETTER Dawn time Early morning
25 Family or child history of asthma or atopic diseases Good response to bronchodilators e.g. Salbutamol Coughing or wheezing on exertion (Exercise induced asthma)
26 DURATION OF COUGH
27 Following Viral Infection e.g. URTI Normally the course is about 1-2 weeks In Asthmatics : The course is usually prolonged more than 2 weeks
28 Symptoms occur or worsen in a seasonal pattern Symptoms occur or worsen with: Animals with fur Aerosol chemicals Changes in temperature Drugs (Aspirin and BBlockers) Exercise Smoke Strong emotions
29 Features suggesting asthma in children years Feature Cough UPDATED 2017 Characteristics suggesting asthma 5 Recurrent or persistent non-productive cough that may be worse at night or accompanied by some wheezing and breathing difficulties. Cough occurring with exercise, laughing, crying or exposure to tobacco smoke in the absence of an apparent respiratory infection Prolonged cough in infancy, and cough without cold symptoms, are associated with later parent-reported physician-diagnosed asthma, independent of infant wheeze Wheezing Recurrent wheezing, including during sleep or with triggers such as activity, laughing, crying or exposure to tobacco smoke or air pollution Difficult or heavy breathing or shortness of breath Occurring with exercise, laughing, or crying Not running, playing or laughing at the same intensity as other Reduced activity children; tires earlier during walks (wants to be carried) Other allergic disease (atopic dermatitis or allergic rhinitis) Past or family history Asthma in first-degree relatives Therapeutic trial Clinical improvement during 2 3 months of with low dose ICS and controller treatment and worsening when treatment is stopped as-needed SABA GINA 2017, Box 6-2
30 Feature Characteristics suggesting asthma Cough Recurrent or persistent non-productive cough that may be worse at night or accompanied by some wheezing and breathing difficulties. Cough occurring with exercise, laughing, crying or exposure to tobacco smoke in the absence of an apparent respiratory infection Prolonged cough in infancy, and cough without cold symptoms, are associated with later parent-reported physician-diagnosed asthma, independent of infant wheeze
31 Wheezing Recurrent wheezing, including: during sleep with triggers such as activity, laughing, crying exposure to tobacco smoke or air pollution Difficult or heavy breathing or shortness of breath Occurring with exercise, laughing, or crying Not running, playing or laughing at Reduced the same intensity as other activity children; tires earlier during walks (wants to be carried)
32 Past or family history Other allergic disease (atopic dermatitis or allergic rhinitis) Asthma in first-degree relatives Therapeutic trial with Clinical improvement during low dose 2 3 months of controller treatment ICS and asand worsening when treatment is stopped needed SABA
33 Common differential diagnoses of asthma in children Condition years Typical features Recurrent viral Mainly cough, runny congested nose for respiratory <10 days; wheeze usually mild; infections No symptoms between infections Gastro- Cough when feeding; recurrent chest infections; esophageal vomits easily especially after large feeds; poor response to asthma medications reflux Foreign body aspiration Episode of abrupt severe cough and/or stridor during eating or play; recurrent chest infections and cough; focal lung signs GINA 2017, Box 6-3 (1/2)
34 ALLERGIC RHINITIS

35 Allergic Rhinitis


36 Epidemiology of Allergic Rhinitis It affects approximately 10 to 25% of the population common in children. Evidence showed that up to 80 % of asthma patients had coexisting allergic rhinitis.
37 Up to 80% of all asthmatic patients have allergic rhinitis All asthmatic patients Adapted from Bousquet J et al J Allergy Clin Immunol 2001;108(suppl 5):S147 S334; Sibbald B, Rink E Thorax 1991;46: ; Leynaert B et al J Allergy Clin Immunol 1999;104: ; Brydon MJ Asthma J 1996:29 32.
38 Up to 40% of patients with Allergic Rhinitis have Asthma Allergic Rhinitis patients Adapted from Bousquet J et al J Allergy Clin Immunol 2001;108(suppl 5):S147 S334; Sibbald B, Rink E Thorax 1991;46: ; Leynaert B et al J Allergy Clin Immunol 1999;104: ; Brydon MJ Asthma J 1996:29 32.
39 Pathophysiology of Allergic Rhinitis and Asthma 1 Common triggers 2 Similar inflammatory cascade on exposure to allergens 3 Similar pattern of early- and late-phase responses 4 Infiltration by the same inflammatory cells 5 Several potential connecting pathways, including systemic transmission of inflammatory mediators 6 Cysteinyl leukotrienes are common mediators in upper and lower airway diseases Adapted from National Institutes of Health Global Initiative for Asthma: Global Strategy for Asthma Management and Prevention: A Pocket Guide for Physicians and Nurses. Publication No B. Bethesda, MD: National Institutes of Health, 1998; Casale TB, Amin BV Clin Rev Allergy Immunol 2001;21(1):27 49; Workshop Expert Panel Management of Allergic Rhinitis and its Impact on Asthma (ARIA) Pocket Guide. A Pocket Guide for Physicians and Nurses. 2001; Kay AB N Engl J Med 2001;344:30 37; Varner AE, Lemanske RF Jr. In: Asthma and Rhinitis. 2nd ed. Oxford, UK: Blackwell Science, 2000: ; Togias A J Allergy Clin Immunol 2000;105(6 pt 2):S599 S604; Togias A Allergy 1999; 54(suppl 57):
40 Diagnosis of Allergic Rhinitis
41 Typical history of allergic symptoms Diagnostic tests
.")
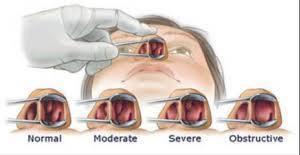
42 Typical symptoms of allergic rhinitis: Rhinorrhea, sneezing, nasal obstruction, nasal pruritus and (allergic salute). Ocular symptoms: Conjunctival injection, pruritus, excessive tearing and (allergic shiners)
43 Classification of Allergic Rhinitis Intermittent Symptoms < 4 days/week or < 4 weeks Mild Persistent Symptoms > 4 days/week & > 4 weeks Moderate severe One or more items *Normal sleep *Normal daily activities, sport, leisure *No work or school problems *Abnormal sleep *Impairment of daily activities, sport, leisure *Work or school problems
44 Allergic Rhinitis Co-morbidities Asthma Allergic Rhinitis Diminished quality of life Otitis Media
45

46

47

48

49

50

51

52

53

54

55

56

57

58

59
60 Final Diagnosis: Co-morbid Asthma and Allergic Rhinitis. The diagnosis of asthma in a child of this age is essentially a clinical diagnosis. A therapeutic response to a treatment plan should also help to solidify the diagnosis.
61 Asthma Management GINA 2014
62 TREATMENT CONTROLLERS (PREVENTION) RELEIVERS (RESCUE) NON-STOP MUST-STOP MEDICINE MEDICINE
63 TREATMENT CONTROLLERS RELEIVERS KETOTIFEN B-AGONIST (NO MORE PRESENT IN GINA GUIDELINES) SALBUTAMOL,TERBUTALIN INHALERS: AMINOPHYLLIN XXXX *INTAL: 3-4 TIMES/DAY MUCO-REGULATORS XXXX *ICS: TOPICAL 200 ug SEVERE ASTHMA SAFE ORAL / IV STEROID *LABA: (+ ICS) 5 YEARS PREDNISOLONE (LTRA) MONTELUKAST FULL DOSE, SHORT COURSE
64 Stepwise approach pharmacotherapy children years STEP 4 STEP 1 PREFERRED CONTROLLER CHOICE Daily low dose ICS Other controller options Leukotriene receptor antagonist (LTRA) Intermittent ICS STEP 3 Double 䇺low dose䇻 ICS Low dose ICS + LTRA Continue controller & refer for specialist assessment Add LTRA Inc. ICS frequency Add intermitt ICS As-needed short-acting beta2-agonist (all children) RELIEVER CONSIDER THIS STEP FOR CHILDREN WITH: STEP 2 Infrequent viral wheezing and no or few interval symptoms Not wellcontrolled on double ICS Symptom pattern consistent with asthma and asthma symptoms not well-controlled, or exacerbations per year Asthma diagnosis, and not well-controlled on low dose ICS Symptom pattern not consistent with asthma but wheezing episodes occur frequently, e.g. every 6 8 weeks. Give diagnostic trial for 3 months. First check diagnosis, inhaler skills, adherence, exposures GINA 2017, Box 6-5 (3/8)

65 Step children inhaled SABA years as-needed STEP 4 PREFERRED CONTROLLER CHOICE STEP 1 Daily low dose ICS Other controller options RELIEVER STEP 2 Leukotriene receptor antagonist (LTRA) Intermittent ICS STEP 3 Double 䇺low dose䇻 ICS Continue controller & refer for specialist assessment Add LTRA Inc. ICS Low dose ICS + LTRA frequency Add intermitt ICS As-needed short-acting beta2-agonist (all children) Infrequent CONSIDER viral THIS STEP FOR wheezing CHILDREN WITH: and no or few interval symptoms Symptom pattern consistent with asthma and asthma symptoms not well-controlled, or exacerbations per year Symptom pattern not consistent with asthma but wheezing episodes occur frequently, e.g. every 6 8 weeks. Give diagnostic trial for 3 months. Not wellasthma diagnosis, and controlled not well-controlled on on double low dose ICS ICS First check diagnosis, inhaler skills, adherence, exposures GINA 2017, Box 6-5 (5/8)
66 Step children years initial controller + as-needed SABA STEP 4 STEP 1 PREFERRED CONTROLLER CHOICE Daily low dose ICS Other controller options Leukotriene receptor antagonist (LTRA) Intermittent ICS STEP 3 Double 䇺low dose䇻 ICS Continue controller & refer for specialist assessment Add LTRA Inc. ICS Low dose ICS + LTRA frequency Add intermitt ICS As-needed short-acting beta2-agonist (all children) RELIEVER CONSIDER THIS STEP FOR CHILDREN WITH: STEP 2 Infrequent viral wheezing and no or few interval symptoms Symptom pattern consistent with asthma and asthma symptoms not well-controlled, or exacerbations per year Symptom pattern not consistent with asthma but wheezing episodes occur frequently, e.g. every 6 8 weeks. Give diagnostic trial for 3 months. Not wellasthma diagnosis, and controlled not well-controlled on on double low dose ICS ICS First check diagnosis, inhaler skills, adherence, exposures GINA 2017, Box 6-5 (5/8)
67 Step children years medium dose ICS + as-needed inhaled SABA STEP 4 STEP 1 PREFERRED CONTROLLER CHOICE Other controller options RELIEVER CONSIDER THIS STEP FOR CHILDREN WITH: STEP 2 Daily low dose ICS Leukotriene receptor antagonist (LTRA) Intermittent ICS STEP 3 Continue controller & refer for specialist assessment Double 䇺low dose䇻 ICS Low dose ICS + Add LTRA Inc. ICS frequency Add intermitt ICS LTRA As-needed short-acting beta2-agonist (all children) Infrequent viral wheezing and no or few interval symptoms Symptom pattern consistent with asthma and asthma symptoms not well-controlled, or exacerbations per year Symptom pattern not consistent with asthma but wheezing episodes occur frequently, e.g. every 6 8 weeks. Give diagnostic trial for 3 months. Asthma diagnosis, and not wellcontrolled on low dose ICS Not wellcontrolled on double ICS First check diagnosis, inhaler skills, adherence, exposures GINA 2017, Box 6-5 (5/8)
68 Step children assessment years refer for expert STEP 4 STEP 1 PREFERRED CONTROLLER CHOICE Other controller options RELIEVER CONSIDER THIS STEP FOR CHILDREN WITH: Continue controller STEP 2 & refer for Double specialist 䇺low dose䇻 assessmen Daily low dose ICS ICS AddtLTRA Inc ICS Leukotriene receptor antagonist (LTRA) Low dose ICS + LTRA freq.uency Intermittent ICS Add intermit ICS As-needed short-acting beta -agonist (all children) STEP 3 2 Infrequent viral wheezing and no or few interval symptoms Symptom pattern consistent with asthma and asthma symptoms not well-controlled, or exacerbations per year Symptom pattern not consistent with asthma but wheezing episodes occur frequently, e.g. every 6 8 weeks. Give diagnostic trial for 3 months. Asthma diagnosis, and Not wellnot well-controlled oncontrolled on low dose ICS double ICS First check diagnosis, inhaler skills, adherence, exposures GINA 2017, Box 6-5 (5/8)
69 Initial assessment of acute asthma exacerbations in children years Symptoms Mild Severe* Altered consciousness Oximetry on presentation (SaO2)** Speech Pulse rate No Agitated, confused or drowsy >95% <92% Sentences Words >200 beats/min (0 3 years) <100 beats/min >180 beats/min (4 5 years) Central cyanosis Absent Likely to be present Wheeze intensity Variable Chest may be quiet *Any of these features indicates a severe exacerbation **Oximetry before treatment with oxygen or bronchodilator Take i to a ou t the hild s or al develop e tal apa ility GINA 2017, Box 6-9
70 Indications for immediate transfer to hospital for children years Transfer immediately to hospital if ANY of the following are present: Features of severe exacerbation at initial or subsequent assessment Child is unable to speak or drink Cyanosis Subcostal retraction Oxygen saturation <92% when breathing room air Silent chest on auscultation Lack of response to initial bronchodilator treatment Lack of response to 6 puffs of inhaled SABA (2 separate puffs, repeated 3 times) over 1-2 hours Persisting tachypnea* despite 3 administrations of inhaled SABA, even if the childrespiratory shows clinical signs *Normal ratesother (breaths/minute): 0-2 months: <60;of 2-12improvement months: <50; 1-5 yrs: <40 Unable to be managed at home Social environment that impairs delivery of acute treatment Parent/carer unable to manage child at home GINA 2017, Box 6-10
71 Initial management of asthma exacerbations in children years Therapy Supplemental oxygen Inhaled SABA Dose and administration 24% delivered by face mask (usually 1L/min) to maintain oxygen saturation 94-98% 2 6 puffs of salbutamol by spacer, or 2.5mg by nebulizer, every 20 min for first hour, then reassess severity. If symptoms persist or recur, give an additional 2-3 puffs per hour. Admit to hospital if >10 puffs required in 3-4 hours. Give initial dose of oral prednisolone (1-2mg/kg up to Systemic maximum of 20mg for children <2 years; 30 mg for 2corticosteroids 5 years) GINA 2017, Box 6-11 (1/2)
72 Initial management of asthma exacerbations in children years Additional options in the first hour of treatment For moderate/severe exacerbations, give 2 Ipratropium puffs of ipratropium bromide 80mcg (or 250mcg by nebulizer) every 20 minutes for bromide one hour only Magnesium sulfate Consider nebulized isotonic MgSO4 (150mg) 3 doses in first hour for hildre 2 years with severe exacerbation GINA 2017, Box 6-11 (2/2)


 Oral corticosteroids")
 Oral or IV corticosteroids Consider IV magnesium Consider high dose ICS GINA 2016, Box 4-4")
73 Management of Asthma exacerbation in Acute care facility MILD or MODERATE SEVERE Talks in phrases Prefers sitting to lying Not agitated Respiratory rate increased Accessory muscles not used Pulse rate bpm O2 saturation (on air) 90 95% PEF >50% predicted or best Talks in words Sits hunched forwards Agitated Respiratory rate >30/min Accessory muscles being used Pulse rate >120 bpm O2 saturation (on air) < 90% PEF 50% predicted or best Short-acting beta2-agonists Consider ipratropium bromide Controlled O2 to maintain saturation 93 95% (children 94-98%) Oral corticosteroids Short-acting beta2-agonists Ipratropium bromide Controlled O2 to maintain saturation 93 95% (children 94-98%) Oral or IV corticosteroids Consider IV magnesium Consider high dose ICS GINA 2016, Box 4-4 (3/4) Global Initiative for Asthma
 Controlled O2 to maintain saturation 93 95% (children 94-98%) Oral corticosteroids Oral or IV corticosteroids Consider IV magnesium Consider high dose ICS If continuing")
 FEV1 or PEF <60% of predicted or personal best,or lack of clinical response SEVERE Continue")
74 Management of Asthma exacerbation in Acute care facility Short-acting beta2-agonists Short-acting beta2-agonists Consider ipratropium bromide Ipratropium bromide Controlled O2 to maintain saturation 93 95% (children 94-98%) Controlled O2 to maintain saturation 93 95% (children 94-98%) Oral corticosteroids Oral or IV corticosteroids Consider IV magnesium Consider high dose ICS If continuing deterioration, treat as severe and re-assess for ICU ASSESS CLINICAL PROGRESS FREQUENTLY MEASURE LUNG FUNCTION in all patients one hour after initial treatment FEV1 or PEF 60-80% of predicted or personal best and symptoms improved MODERATE Consider for discharge planning GINA 2016, Box 4-4 (4/4) FEV1 or PEF <60% of predicted or personal best,or lack of clinical response SEVERE Continue treatment as above and reassess frequently Global Initiative for Asthma

75 Initial management of asthma exacerbations in children years Therapy Dose and administration Supplemental oxygen 24% delivered by face mask (usually 1L/min) to maintain oxygen saturation 94-98% Inhaled SABA 2 6 puffs of salbutamol by spacer, or 2.5mg by nebulizer, every 20 min for first hour, then reassess severity. If symptoms persist or recur, give an additional 2-3 puffs per hour. Admit to hospital if >10 puffs required in 3-4 hours. Systemic corticosteroids Give initial dose of oral prednisolone (1-2mg/kg up to maximum of 20mg for children <2 years; 30 mg for 2-5 years) Inhaled steroids Very high-dose inhaled steroids may Additional options in the first hour of treatment Ipratropium bromide EFFECTIVE For moderate/severe exacerbations, give 2 puffs of ipratropium bromide 80mcg (or 250mcg by nebulizer) every 20 minutes for one hour only also be either Consider during the exacerbation Magnesium nebulized isotonic MgSO (150mg) 3 doses or in first sulfate hour for children 2 years with severe exacerbation preemptively after a common cold 4 GINA 2015, Box 6-11 (2/2) Global Initiative for Asthma
76 Step 1 (children 5 years) as-needed inhaled SABA Oral bronchodilator therapy is NOT recommended (slower onset of action, more side-effects) GINA 2014
77 Step 3 (children 5 years) medium dose ICS + as-needed inhaled SABA check adherence, inhaler technique and environmental exposures Review response after 3 months GINA 2014



78 Choosing an inhaler device for children 5 years Age Preferred device Alternate device 0 3 years Pressurized metered dose inhaler plus dedicated spacer with face mask Nebulizer with face mask 4 5 years Pressurized metered dose inhaler plus dedicated spacer with mouthpiece Pressurized metered dose inhaler plus dedicated spacer with face mask, or nebulizer with mouthpiece or face mask GINA 2017, Box 6-6 Global Initiative for Asthma
79 Indications of Theophylline There are four clinical circumstances for which theophylline may be considered in the treatment of asthma [25]: Additive maintenance therapy in a patient whose asthma is not adequately controlled with conventional doses of inhaled glucocorticoids, or when addition of a long acting beta agonist either provides no benefit or actually causes worsening of control [26].
80 Indications of Theophylline Primary maintenance therapy in a patient who is more likely to adhere to an oral than an inhaled regimen and montelukast is not sufficiently effective.
81 Indications of Theophylline Primary maintenance therapy when the administration of an inhaled glucocorticoid is difficult or cumbersome (eg, toddlers and preschool-age children) and montelukast is not effective.
82 Indications of Theophylline Additive acute therapy in the intensive care unit for patients failing to respond to vigorous use of inhaled beta2-selective agonists in combination with ipratropium and/or intravenous magnesium and systemically administered glucocorticoids, although evidence for benefit in this situation is lacking.
83 "Theophylline: Pediatric drug information" Dosing: Pediatric Doses should be individualized based on steady-state serum concentrations and ideal body weight. Acute symptoms: Manufacturer's labeling: Loading dose: Oral, IV: Asthma exacerbations: The treatment of asthma exacerbations with theophylline is not supported or recommended by current clinical practice guidelines (GINA 2015; NAEPP 2007).
84 "Theophylline: Pediatric drug information" If no theophylline received within the previous 24 hours: 4.6 mg/kg loading dose (~5.8 mg/kg hydrous aminophylline) IV or 5 mg/kg orally. Loading dose intended to achieve a serum level of approximately 10 mcg/ml; loading doses should be given intravenously (preferred) or with a rapidly absorbed oral product (not an extended-release product). Note: On the average, for every 1 mg/kg theophylline given, blood levels will rise 2 mcg/ml. If theophylline has been administered in the previous 24 hours: A loading dose is not recommended without obtaining a serum theophylline concentration. The loading dose should be calculated as follows: Dose = (desired serum theophylline concentration measured serum theophylline concentration) (Vd)

85 Medications used in acute asthma GINA: In acute asthma, the use of intravenous aminophylline did not result in any additional bronchodilation compared to standard care with B2-agonists & should not be used.
86 Magnesium Sulfate In acute severe asthma I.V. or Nebulized Together with B2-agonist and systemic steroids Systematic review and meta-analysis (March 2013) 25 trials, 1754 patients Improves pulmonary functions and reduces hospital admissions in children Nebulized MgSO4 is beneficial for adults and children starting 2 ys. Nebulized isotonic MgSO4 (150 mg) 3 doses in the 1st hour. I.V. Dose: mg/kg can be repeated up to 2.5g
87 Dexamethasone in Asthma Giving children with acute asthma flare-ups 1-2 doses of dexamethasone in the Emergency Department provides equivalent relief to a 5-day course of prednisone with less vomiting. (Pediatrics. Online February 10, 2014)

88 Role of Nebulised Corticosteroid in Acute Asthma Attack
 Placebo at half-hourly intervals for three doses Single dose of oral prednisolone (2 mg/kg) Budesonide group Nebulized 0.5 % salbutamol (0.")
89 Trial protocol Prednisolone group Nebulized 0.5 % salbutamol (0.15mg/kg) Placebo at half-hourly intervals for three doses Single dose of oral prednisolone (2 mg/kg) Budesonide group Nebulized 0.5 % salbutamol (0.15mg/kg) Budesonide (800 μg) at half-hourly intervals for three doses Single dose of oral prednisolone ( 2mg/kg) Single dose of placebo tablets

90 The proportion of patients who were fit for discharge at the end of 2 h after the third dose of nebulization was significantly higher in the budesonide group than in the prednisolone group Patients fit for Discharge at the end of treatment 70% 60% [VALUE] 50% P % 30% [VALUE] 20% 10% 0% Budesonide Prednisolone
91 Conclusion The data suggest that a combination of nebulized salbutamol and budesonide should be preferred in the emergency room management of children with acute moderate to severe exacerbation of asthma and who are not on prior oral or inhaled steroid therapy.



92 2014
93 Patients Number 3,099 Patient Population Children aged 2 to 12 years with moderate or severe acute
 Ipratropium 250 µg/dose.")
94 Trial Protocol Eligible children were randomized within the pharmacy to receive three doses of : Budesonide solution (500 µg/dose) Or placebo(normal saline). Patients also received : B2 -agonist (2.5 mg salbutamol if patient weight was 20 kg or 5 mg if 0 kg) Ipratropium 250 µg/dose. Each dose every 20 min by jet nebulization over 1 hour

95 Conclusion Hospital Admission Rate : The addition of budesonide nebulization decreased the admission rate of severe acute asthma by 33.5 %

96 2013
97 Conclusion Rates of complete remission : 2 h post treatment were: 84.7% in the BUD group 46.3% in the control group Need for SCS therapy : 16.9% in the BUD group 46.3% in the controls group
98 ANTIPYRETICS PARACETAMOL ALLOWED?? IBUPROFEN ALLOWED DICLOFENAC?? CONTRAINDICATED

99 GUIDELINES ITALY

100 GUIDELINES UK

101 GUIDELINES CANADA

102 GUIDELINES UK

103 GUIDELINES USA

104 GUIDELINES WHO
105 GUIDELINES USA
106 UNNECESSARY THERAPY ANTIBIOTICS MUCOLYTICS COUGH SYRUPS IONIZERS BREATHING EXERCISES PHYSIOTHERAPY IS INDICATED IN CHILDREN ONLY WHERE LOBAR COLLAPSE IS DOCUMENTED
 OR Add ICS to LTRA Step down if appropriate Step Up Therapy to Gain Control ICS Symptoms INSUFFICIENT CONTROLc Increase ICS dose (800 µg BDP equivalent) OR Add LTRA")
107 PRACTALL treatment guidelines No more one cornerstone in asthma management Step down if appropriate (200 µg BDP equivalent) OR LTRAa (Dose depends on age) Inflammation INSUFFICIENT CONTROLb Increase ICS dose (400 µg BDP equivalent) OR Add ICS to LTRA Step down if appropriate Step Up Therapy to Gain Control ICS Symptoms INSUFFICIENT CONTROLc Increase ICS dose (800 µg BDP equivalent) OR Add LTRA to ICS OR Add LABA INSUFFICIENT CONTROL c Consider other options Theophylline SR Oral corticosteroids



108 Growth Growth Rate Montelukast 5 mg (n=481) 7.0 Mean growth rate (cm/year) 6.5 Fluticasone 200 mg (n=482) 6.0 p= Months 12
109 The mean growth rate over 12 months of treatment was 6.2 cm/year in the montelukast group and 5.8 cm/year in the fluticasone group. Although statistically significant, this 4 mm difference in growth over one year may not be clinically important
110 The Childhood Asthma Management Program (CAMP) study randomised 1041 children aged 5 12 years with mild to moderate asthma to treatment with inhaled budesonide, nedocromil, or placebo for a duration of 4 to 6 years.17,18 This long-term study showed NO IMPAIRMENT IN GROWTH with budesonide compared with placebo

111 MANAGEMENT OF ALLERGIC RHINITIS
112 1- Environmental Control AVOIDANCE Cigarette SMOKING Furred Pets?!
113 2- Drug Treatment Intranasal Steroids Recommended for the treatment of allergic rhinitis in children 2 years and older. THE MOST EFFECTIVE DRUGS
114 Topical CROMONES modestly effective.
115 Montelukast Recommended in the treatment of allergic rhinitis especially seasonal.

116 CAUTION IM and long-term use of oral glucocorticosteroids are NOT RECOMMENDED due to safety concern. Intranasal decongestants may be used for a short period of time in patients with severe nasal obstruction. Oral nasal decongestants (and their associations) may be used in the treatment of allergic rhinitis in ADULTS, but side effects are common.
117 ARIA Guidelines Recommend a Combined Approach to Managing Asthma and Allergic Rhinitis Patients with allergic rhinitis should be evaluated for asthma Patients with asthma should be evaluated for allergic rhinitis A strategy should combine the treatment of upper and lower airways in terms of efficacy and tolerability ARIA: Allergic Rhinitis & its Impact on Asthma Adapted from Bousquet J et al J Allergy Clin Immunol 2001;108(suppl 5):S147 S334.
118 PRACTALL Guidelines 2008 ICS (200 µg BDP equivalent) OR A first-line treatment for persistent asthma First-line treatment for persistent asthma Should be introduced as initial maintenance treatment when asthma control inadequate Evidence supports LTRA as initial controller therapy for mild asthma in children Atopy and poor lung function predict favorable response Younger age (<10 years) and high levels of urinary leukotrienes predict favorable response If control inadequate on low dose, identify reasons. If indicated, an increased ICS dose or additional therapy with LTRAs or LABAs should be considered Therapy for patients who cannot or will not use ICS Useful also as add-on therapy to ICS: different and complementary mechanisms of action Effect in older children begins to disappear as soon as treatment is discontinued New evidence does not support a diseasemodifying role after cessation of treatment in preschool children LTRA (Dose depends on age) Suggested for viral-induced wheeze in young children Benefit shown in children as young as 6 months LTRA may be particularly useful if the patient has Adapted from Bacharier LB, et al. Allergy. 2008;63(1):5 34. concomitant rhinitis


119 Guidelines Confirm The Role of Montelukast in Asthma with AR A more prominent role in asthma management A UNIQUE ROLE in patients with asthma and AR High efficacy in AR Superior to AH on nasal blockage The RECOMMENDED DRUG in patient with asthma and AR
120 Thank You
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Medicine Dr. Kawa Lecture 4 - Treatment of asthma :
 Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Nguyen Tien Dung A/Prof. PhD. MD Head of Pediatric Department - Bach Mai Hospital
 Nguyen Tien Dung A/Prof. PhD. MD Head of Pediatric Department - Bach Mai Hospital A girl patient 11 years old admitted to Bach mai Hospital at 4h15, 12nd November because of difficult breathing She has
Nguyen Tien Dung A/Prof. PhD. MD Head of Pediatric Department - Bach Mai Hospital A girl patient 11 years old admitted to Bach mai Hospital at 4h15, 12nd November because of difficult breathing She has
Case approach in Asthma and COPD. Assoc.Prof.Sunee Lertsinudom BSc.Grad.Diplo.BCP. Department of Clinical pharmacy Khonkaen University
 Case approach in Asthma and COPD Assoc.Prof.Sunee Lertsinudom BSc.Grad.Diplo.BCP. Department of Clinical pharmacy Khonkaen University Asthma Diagnosis History and patterns of symptoms Physical examination
Case approach in Asthma and COPD Assoc.Prof.Sunee Lertsinudom BSc.Grad.Diplo.BCP. Department of Clinical pharmacy Khonkaen University Asthma Diagnosis History and patterns of symptoms Physical examination
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Management of Acute Asthma Exacerbations in Children 2012 Update. Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch
 Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Pathology of Asthma Epidemiology
 Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Supplementary Medications during asthma attack. Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus
 Supplementary Medications during asthma attack Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus Conflicts of Interest None Definition of Asthma Airway narrowing that is
Supplementary Medications during asthma attack Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus Conflicts of Interest None Definition of Asthma Airway narrowing that is
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Management of wheeze in pre-school children. Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne
 Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
In 2002, it was reported that 72 of 1000
 REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Children 5 Years and Younger) A Guide for Health Care Professionals Updated 2015 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND PREVENTION
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Children 5 Years and Younger) A Guide for Health Care Professionals Updated 2015 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND PREVENTION
Getting Asthma treatment right. Dr David Cremonesini Specialist Pediatrician American Hospital
 Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Practical Approach to Managing Paediatric Asthma
 Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
ARIA. At-A-Glance Pocket Reference 2007
 ARIA_Glance_2007_8pg:ARIA_Glance_English 9/14/07 3:10 PM Page 1 ARIA At-A-Glance Pocket Reference 2007 1 st Edition NEW ARIA UPDATE BASED ON THE ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMA WORKSHOP REPORT
ARIA_Glance_2007_8pg:ARIA_Glance_English 9/14/07 3:10 PM Page 1 ARIA At-A-Glance Pocket Reference 2007 1 st Edition NEW ARIA UPDATE BASED ON THE ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMA WORKSHOP REPORT
Respiratory Health. Asthma and COPD
 Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Asthma/wheeze management plan
 Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
AT TRIAGE. Alberta Acute Childhood Asthma Pathway: Evidence based* recommendations For Emergency / Urgent Care
 1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health.
 Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health Background: These guidelines are provided to assist physicians and
Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health Background: These guidelines are provided to assist physicians and
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
10/6/2014. Tommy s Story: An Overview of Asthma Mangement. Disclosure. Objectives for this talk.
 Tommy s Story: An Overview of Asthma Mangement Clifton C. Lee, MD, FAAP, FHM Associate Professor of Pediatrics Chief, Pediatric Hospital Medicine Children s Hospital of Richmond at VCU Disclosure Obviously,
Tommy s Story: An Overview of Asthma Mangement Clifton C. Lee, MD, FAAP, FHM Associate Professor of Pediatrics Chief, Pediatric Hospital Medicine Children s Hospital of Richmond at VCU Disclosure Obviously,
PEDIATRIC ACUTE ASTHMA SCORE (P.A.A.S.) GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze
 GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze") Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Australian Asthma Handbook. Key table and figures Version 1.2
 Australian Asthma Handbook Key table and figures Version 1.2 DIAGNOSIS OF ASTHMA Figure. Steps in the diagnosis of asthma in adults Table. Findings that increase or decrease the probability of asthma in
Australian Asthma Handbook Key table and figures Version 1.2 DIAGNOSIS OF ASTHMA Figure. Steps in the diagnosis of asthma in adults Table. Findings that increase or decrease the probability of asthma in
An Update on Allergic Rhinitis. Mike Levin Division of Asthma and Allergy Department of Paediatrics University of Cape Town Red Cross Hospital
 An Update on Allergic Rhinitis Mike Levin Division of Asthma and Allergy Department of Paediatrics University of Cape Town Red Cross Hospital Allergic Rhinitis Common condition with increasing prevalence
An Update on Allergic Rhinitis Mike Levin Division of Asthma and Allergy Department of Paediatrics University of Cape Town Red Cross Hospital Allergic Rhinitis Common condition with increasing prevalence
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Title Protocol for the Management of Asthma
 Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
 β 2004 2004 o β β β β 2004 β β β β β β β β β 2004 2004 2004 2004 2004 β 2004 2004 2004 2004 β β 2004 β β β β β β β 2004 β β β β β β 2004 β β β β STEP 5: CONTINUOUS OR FREQUENT USE OF ORAL
β 2004 2004 o β β β β 2004 β β β β β β β β β 2004 2004 2004 2004 2004 β 2004 2004 2004 2004 β β 2004 β β β β β β β 2004 β β β β β β 2004 β β β β STEP 5: CONTINUOUS OR FREQUENT USE OF ORAL
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Management of acute severe asthma in adults in general practice. Moderate asthma Acute severe asthma Life-threatening asthma INITIAL ASSESSMENT
 British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
beclometasone 100 MDI 2 puffs twice a day (recently changed to non CFC (Clenil Modulite))
)") Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies
 Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Asthma Care in the Emergency Department Clinical Practice Guideline
 Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
Your Guide to MANAGING ASTHMA
 Your Guide to MANAGING ASTHMA Asthma affects more than 24 MILLION AMERICANS. It is a chronic disease that causes your airways to become inflamed, making it hard to breathe. There is no cure for asthma.
Your Guide to MANAGING ASTHMA Asthma affects more than 24 MILLION AMERICANS. It is a chronic disease that causes your airways to become inflamed, making it hard to breathe. There is no cure for asthma.
Candidate. Within the 8 minutes you are required to do the following:
 Candidate You are a member of the paediatrics team. Lisa is a 7 year old girl who has presented to ED with wheeze on a background of known asthma. The emergency department has provided the following information:
Candidate You are a member of the paediatrics team. Lisa is a 7 year old girl who has presented to ED with wheeze on a background of known asthma. The emergency department has provided the following information:
HealthPartners Care Coordination Clinical Care Planning and Resource Guide ASTHMA
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
Asthma in the Athlete
 Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN. Dr Lại Lê Hưng Respiratory Department
 TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Asthma Assessment & Review
 ASTHMA RESOURCE PACK Section 5B Asthma Assessment & Review In this section: 1. Primary Care initial assessment and review Asthma Resource Pack Section 5B: Asthma Assessment & Review Version 3.0 Last Updated:
ASTHMA RESOURCE PACK Section 5B Asthma Assessment & Review In this section: 1. Primary Care initial assessment and review Asthma Resource Pack Section 5B: Asthma Assessment & Review Version 3.0 Last Updated:
National Asthma Educator Certification Board Detailed Content Outline
 I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma
 Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Monocast Description Indications
 Monocast Tablet Description The active ingredient of Monocast tablet is Montelukast Sodium INN. Montelukast is a selective and orally active leukotriene receptor antagonist that inhibits the cysteinyl
Monocast Tablet Description The active ingredient of Monocast tablet is Montelukast Sodium INN. Montelukast is a selective and orally active leukotriene receptor antagonist that inhibits the cysteinyl
Integrated Cardiopulmonary Pharmacology Third Edition
 Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
3 RESPIRATORY SYSTEM
 3 RESPIRATORY SYSTEM 3.01 ANTIASTHMATICS 3.01a BETA 2 AGONIST ASTHMA, CHRONIC BRONCHITIS & EMPHYSEMA Salbutamol Inhaler 100ug/dose [Albuterol] (Ventolin) Salbutamol Sulphate Respirator Solution 0.5% (5mg/ml),
3 RESPIRATORY SYSTEM 3.01 ANTIASTHMATICS 3.01a BETA 2 AGONIST ASTHMA, CHRONIC BRONCHITIS & EMPHYSEMA Salbutamol Inhaler 100ug/dose [Albuterol] (Ventolin) Salbutamol Sulphate Respirator Solution 0.5% (5mg/ml),
GUIDE LINE SUMMARY THE DIAGNOSIS AND TREATMENT OF ADULT ASTHMA BEST PRACTICE EV I DENCE-BASED KEY MESSAGES. Diagnosis.
 THE DIAGSIS AND TREATMENT OF ADULT ASTHMA The purpose of the guideline is to provide an evidence-based summary of the diagnostic management and treatment options available for asthma in the adult population
THE DIAGSIS AND TREATMENT OF ADULT ASTHMA The purpose of the guideline is to provide an evidence-based summary of the diagnostic management and treatment options available for asthma in the adult population
Some Facts About Asthma
 Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
EXACERBATIONS IN ADULTS WHEN TO REFER
 06 Bronchial Asthma Contributors: Dr Chong Phui Nah Dr Tang Wern Ee PRESENTATION AND DIAGNOSIS CLASSIFICATION OF ASTHMA BY LEVEL OF CONTROL ASSESSMENT OF ASTHMA CONTROL USING THE ASTHMA CONTROL TEST ASTHMA
06 Bronchial Asthma Contributors: Dr Chong Phui Nah Dr Tang Wern Ee PRESENTATION AND DIAGNOSIS CLASSIFICATION OF ASTHMA BY LEVEL OF CONTROL ASSESSMENT OF ASTHMA CONTROL USING THE ASTHMA CONTROL TEST ASTHMA
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma By Mayo Clinic staff
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
Medications Affecting The Respiratory System
 Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Childhood Asthma. The pathophysiology of asthma is an interplay. CME Case Study. Case Study. By Moyez B. Ladhani, MD, CCFP, FAAP, FRCPC
 CME Case Study Childhood Asthma By Moyez B. Ladhani, MD, CCFP, FAAP, FRCPC Case Study A two-year-old child presents to your office with a cough, which has been present for three weeks. It is worse at nighttime
CME Case Study Childhood Asthma By Moyez B. Ladhani, MD, CCFP, FAAP, FRCPC Case Study A two-year-old child presents to your office with a cough, which has been present for three weeks. It is worse at nighttime
Asthma. The prevalence of asthma has been increasing worldwide, but why this is happening is not known.
 Asthma What is asthma? Asthma is a chronic disorder of the airways of the lungs. The airways are reactive and may be inflamed even when symptoms are not present. The extent and severity of airway irritation
Asthma What is asthma? Asthma is a chronic disorder of the airways of the lungs. The airways are reactive and may be inflamed even when symptoms are not present. The extent and severity of airway irritation
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Assessing wheeze in pre-school children
 Assessing wheeze in pre-school children 8 Wheeze in children aged less than five years has many potential causes. Often it is regarded as the first sign of asthma, however, a substantial proportion of
Assessing wheeze in pre-school children 8 Wheeze in children aged less than five years has many potential causes. Often it is regarded as the first sign of asthma, however, a substantial proportion of
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Preschool Asthma What you need to know in 10 minutes
 Preschool Asthma What you need to know in 10 minutes Alan Kaplan MD CCFP(EM) FCFP Family Physician Airways Group of Canada Respiratory Medicine section CFPC Faculty/Presenter Disclosure Faculty: Alan Kaplan
Preschool Asthma What you need to know in 10 minutes Alan Kaplan MD CCFP(EM) FCFP Family Physician Airways Group of Canada Respiratory Medicine section CFPC Faculty/Presenter Disclosure Faculty: Alan Kaplan
INTERNAL ONLY STANDING ORDER EMERGENCY DEPARTMENTS SALBUTAMOL SULFATE Administration by Accredited Emergency Nurses for symptom relief of asthma
 POLICY STATEMENT This order may only be activated under the specific circumstances set out in the section Indications and provided there are no contraindications present. The administering nurse must be
POLICY STATEMENT This order may only be activated under the specific circumstances set out in the section Indications and provided there are no contraindications present. The administering nurse must be
Public Dissemination
 1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Current guidelines for the management of asthma in young children
 Review pissn 2092-7355 eissn 2092-7363 Current guidelines for the management of asthma in young children Paul C Potter* Allergy Diagnostic & Clinical Research Unit, University of Cape Town Lung Institute,
Review pissn 2092-7355 eissn 2092-7363 Current guidelines for the management of asthma in young children Paul C Potter* Allergy Diagnostic & Clinical Research Unit, University of Cape Town Lung Institute,
Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma
 Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma - 2005 Criteria that suggest the diagnosis of Asthma: The symptoms of dyspnea, cough and/or wheezing,
Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma - 2005 Criteria that suggest the diagnosis of Asthma: The symptoms of dyspnea, cough and/or wheezing,