3/23/2017. Differentiation: Differentiation: Immunohistochemistry. Well Differentiated vs. Poorly Differentiated Neuroendocrine Neoplasms
|
|
|
- Eugene Booker
- 6 years ago
- Views:
Transcription
: Neuroendocrine Neoplasms Arthur Purdy")




")




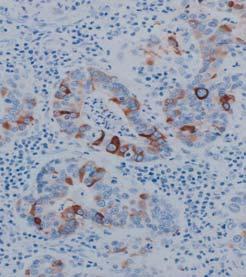
1 Disclosure Statement When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 Dr. Klimstra receives royalty payments from Up To Date and the American Registry of Pathology PET CT David S. Klimstra, MD Chairman, Department of Pathology James Ewing Alumni Chair of Pathology Attending Pathologist Memorial Sloan Kettering Cancer Center Professor of Pathology and Laboratory Medicine Weill Cornell Medical College Neuroendocrine Neoplasms Diverse but related groups of tumors Lung, thymus, pancreas, GI tract, other sites Characteristic pathologic features Immunohistochemical evidence of neuroendocrine differentiation (chromogranin / synaptophysin / CD56) Differentiation: Extent of resemblance of the cells of a neoplasm to their normal cellular counterparts Usually closely linked to grade (for NETs) Range of biological aggressiveness Can be either well differentiated tumors or poorly differentiated carcinomas Differentiation: Immunohistochemistry A Synaptophysin Well Differentiated vs. Poorly Differentiated Neuroendocrine Neoplasms Two different families Both share neuroendocrine differentiation Can be difficult to distinguish Fundamentally different Cell of origin Relationship to non-ne neoplasia Genetic background Clinical aggressiveness Treatment CarcinoidTumor Small Cell Carcinoma 1


 Carcinoid tumor / atypical carcinoid tumor (lung, thymus) Poorly Differentiated NECs Small cell carcinoma Large cell neuroendocrine carcinoma Mixed")
 Use of Immunohistochemistry in Neuroendocrine Neoplasms Recognition of Neuroendocrine Differentiation Diagnosis (recognition of neuroendocrine")
2 Well Differentiated Classification of Pulmonary Neuroendocrine Neoplasms Low Grade Carcinoid Tumor Intermediate Grade Atypical Carcinoid Tumor WHO 2010 Grading of GEP-NETs Grade Mitoses Ki-67 Index G1 < 2 / 10 H.P.F. < 3% G / 10 H.P.F. 3-20% Poorly Differentiated High Grade Small Cell Carcinoma Large Cell Neuroendocrine Carcinoma G3 > 20 / 10 H.P.F. > 20% Poorly Differentiated (High Grade ) Neuroendocrine Carcinoma Pancreatic NETs: Overall Survival by Grade Rindi et al., J Natl Cancer Inst 2012; 104: 764 Terminology for Neuroendocrine Neoplasms: WHO 2010/2015 Well Differentiated NETs Well differentiated NET (pancreas, GI tract, etc.) Carcinoid tumor / atypical carcinoid tumor (lung, thymus) Poorly Differentiated NECs Small cell carcinoma Large cell neuroendocrine carcinoma Mixed neuroendocrine carcinoma (with component of adenocarcinoma, squamous cell carcinoma, etc.) Use of Immunohistochemistry in Neuroendocrine Neoplasms Recognition of Neuroendocrine Differentiation Diagnosis (recognition of neuroendocrine differentiation) Delineation of primary site PET-CT PET-CT Well Differentiated Neuroendocrine (Carcinoid) Tumor Determination of grade, classification, prognosis 2
 Neuron specific enolase (NSE) CD57 / Leu7 PET-CT PGP9.")
 Pulmonary carcinoid tumor 3% (368) Duodenal NET 7% (61) Ileal NET 4% (51) Pancreatic NET 17% (108) Thymic carcinoid tumor 19% (95) Pheochromocytoma 1%")
 Ileal NET 2% (58) Pancreatic NET 1% (75) Thymic carcinoid tumor 21% (101) Pheochromocytoma 2% (188) Pulmonary small cell carcinoma 25% (97) Pulmonary large cell NE carcinoma 17% (268) Source:")
3 Recognition of Neuroendocrine Differentiation PET-CT Poorly Differentiated Neuroendocrine Carcinoma Recognition of Neuroendocrine Differentiation: Immunohistochemical Markers Conventional markers A Synaptophysin CD56 (neural cell adhesion molecular / NCAM) Neuron specific enolase (NSE) CD57 / Leu7 PET-CT PGP9.5 Novel markers Synaptic vesicle protein 2 (SV2) Achaete-scute complex homolog (MASH1) Insulinoma-associated protein 1 (INSM1) Neuroendocrine secretory protein 55 (NESP55) Sensitivity of A Sensitivity of Synaptophysin % Negative (n) Pulmonary carcinoid tumor 3% (368) Duodenal NET 7% (61) Ileal NET 4% (51) Pancreatic NET 17% (108) Thymic carcinoid tumor 19% (95) Pheochromocytoma 1% (182) Pulmonary small cell carcinoma 57% (596) Pulmonary large cell NE carcinoma 37% (252) % Negative (n) Pulmonary carcinoid tumor 2% (333) Pulmonary atypical carcinoid tumor 10% (115) Rectal NET 4% (28) Ileal NET 2% (58) Pancreatic NET 1% (75) Thymic carcinoid tumor 21% (101) Pheochromocytoma 2% (188) Pulmonary small cell carcinoma 25% (97) Pulmonary large cell NE carcinoma 17% (268) Source: Immunoquery Source: Immunoquery Small Bowel Tumor with Mesenteric Deposits Tumor positive with somatostatin receptor scintigraphy Synaptophysin CD56 3
 4% (584) GIST 1% (88) Adrenal cortical carcinoma 2% (81) 63% (269) Renal cell carcinoma 2% (379) Clear cell sarcoma 25% (59) Melanoma 11% (114) Source:")
 Adrenal cortical carcinoma 88% (49) Melanoma 7% (130) Adult granulosa cell tumor 100% (40) Synovial sarcoma 51% (68) Rhabdomyosarcoma 76% (34) Granular cell tumor")
 Tumors Sensitivity For most primary sites, chromogranin and synaptophysin are highly sensitive When used in combination, ~95% positive Specificity Certain specific non-ne")
 Are immunohistochemical stains for general neuroendocrine markers mandated as necessary in all cases? Agree strongly 23.53% 4 Agree with minor reservation 11.")
4 Specificity of and Synaptophysin % % Synaptophysin Positive (n) Positive (n) Breast ductal carcinoma 2% (287) Breast colloid carcinoma 18% (112) 41% (105) Pulmonary adenocarcinoma 2% (689) 11% (689) Pulmonary squamous cell carcinoma 2% (586) 4% (584) GIST 1% (88) Adrenal cortical carcinoma 2% (81) 63% (269) Renal cell carcinoma 2% (379) Clear cell sarcoma 25% (59) Melanoma 11% (114) Source: Immunoquery Specificity of CD56 for Neuroendocrine Neoplasms % Positive (n) Lung adenocarcinoma 3% (639) Lung squamous cell carcinoma 9% (520) Renal cell carcinoma 17% (455) Pancreatic solid pseudopapillary neoplasm 98% (152) Adrenal cortical carcinoma 88% (49) Melanoma 7% (130) Adult granulosa cell tumor 100% (40) Synovial sarcoma 51% (68) Rhabdomyosarcoma 76% (34) Granular cell tumor 95% (58) Glioma 36% (148) Dendritic cell tumor 94% (164) Nk T-cell lymphoma 74% (267) Chloroma 27% (62) Source: Immunoquery Immunohistochemical Staining for the Diagnosis of Well Differentiated Neuroendocrine (Carcinoid) Tumors Sensitivity For most primary sites, chromogranin and synaptophysin are highly sensitive When used in combination, ~95% positive Specificity Certain specific non-ne neoplasms stain predictably PET-CT 2-5% idiosyncratic staining of other neoplasms Is it necessary? Specific differential diagnoses Metastatic disease What about histologically typical primary tumors? (Am J Surg Pathol 2010;34: ) Are immunohistochemical stains for general neuroendocrine markers mandated as necessary in all cases? Agree strongly 23.53% 4 Agree with minor reservation 11.76% 2 Agree with major reservation 0% 0 Disagree with minor reservation (disagree mildly) 11.76% 2 Disagree with major reservation (disagree moderately) 23.53% 4 Disagree strongly 29.41% 5 Totals 100% 17 NO AGREEMENT Immunohistochemical Staining for the Diagnosis of Poorly Differentiated Neuroendocrine Carcinomas Small cell carcinoma NOT mandated when classic morphologic findings are present Consider ruling out alternatives (e.g., basaloid squamous cell carcinoma, spindle cell carcinoid tumor, primitive neuroectodermal tumor, etc.) or synaptophysin positive in ~75% of cases Large cell neuroendocrine carcinoma NE marker expression required for diagnosis Must be positive in 100% of cases (by definition) Which makers? Thoracic vs. gastroenteropancreatic How strongly / diffusely positive? WHO 2015: The diagnosis of LCNEC requires immunohistochemistry for confirmation of neuroendocrine differentiation. In decreasing order of frequency, NCAM/CD56 stains % of LCNEC cases, followed by chromogranin A in 80 85%, and synaptophysin in 50 60%. NCAM/CD56 needs a note of caution because of its lower specificity for neuroendocrine differentiation in lung cancer, but it is the mostsensitivemarkerin the appropriate morphological context of a neuroendocrine neoplasm. Aand synaptophysin are the most reliable stains for diagnostic accuracy in distinguishing LCNEC from non-neuroendocrine tumours, and one positive marker is enough if the staining is clear-cut. Large Cell Neuroendocrine Carcinoma Chr Syn CD56 4









5 Large Cell Neuroendocrine Carcinoma Chr Syn CD56 Large Cell Lung Carcinoma Large Cell Carcinoma with Neuroendocrine Morphology Large Cell Undifferentiated Carcinoma Large Cell Neuroendocrine Carcinoma Large Cell Carcinoma with Neuroendocrine Morphology Large Cell Carcinoma with Neuroendocrine Differentiation Chr, Synapto, CD56 Large Cell Carcinoma with Neuroendocrine Differentiation Genomic subgroups in LCNEC Gene alterations typical of: SCLC Adeno SCLC SCLC/SqCC TP53 78% Number of altered genes per case RB1 40% KRAS 22% STK11 40% MYCL 7% MYCN 2% IRS2 4% SOX2 11% FGFR1 4% PTEN 4% MEN1 SCLC like NSCLC like (predominantly adeno like) Carcinoidlike Loss total loss total Gain amp Mutation total mut Loss Gain Missense mutation Truncating mutation Loss by IHC/WT gene Rekhtman et al., Clin Cancer Res2016; 22:


")




 Mixed Adenocarcinoma Neuroendocrine")



6 3/23/2017 Mixed Adenocarcinoma Neuroendocrine Carcinoma Combined Neuroendocrine Carcinomas At least 30% of both neuroendocrine and non-neuroendocrine components Adenocarcinoma most common ( MANEC ) Also squamous, pancreatic acinar, other exocrine types Neuroendocrine component usually poorly differentiated; small cell carcinoma or LCNEC Lung, colon, pancreas, gallbladder, etc. Various combinations Biphasic Waxing and waning Amphicrine Aggressive biology; evolving genomic data; treatment as small cell carcinoma (?) Mixed Adenocarcinoma Neuroendocrine Carcinoma Synaptophysin Pancreas Mixed Acinar Neuroendocrine Carcinoma Chymotrypsin Adenocarcinoma with Neuroendocrine Differentiation Morphologically adenocarcinoma Neuroendocrine component <30% Neuroendocrine differentiation detected incidentally Focal NE differentiation: no prognostic impact Role of IHC for NE markers??? 6










")


7 Synaptophysin Synaptophysin Neuroendocrine Differentiation in Carcinomas: Treatment Implications Small cell carcinoma (lung or extrapulmonary) Platinum + etoposide Large cell neuroendocrine carcinoma Commonly treated like small cell carcinoma Few compelling studies; no randomized trials Carcinoma with neuroendocrine morphology / differentiation / features / minor elements / etc. Who knows???? Neuroendocrine Neoplasms: Determination of Grade, Classification, and Prognosis WHO 2010 Grading of GEP-NETs Grade Mitoses Ki-67 Index G1 < 2 / 10 H.P.F. < 3% ENETS/WHO Grading of GEP-NETs: Provisions Count mitoses in 50 high power fields Assess Ki67 based on counting 2000 (500) cells Assess Ki67 in hot spots If mitotic rate and Ki67 are discordant, assign higher grade G / 10 H.P.F. 3-20% G3 > 20 / 10 H.P.F. > 20% Poorly Differentiated (High Grade ) Neuroendocrine Carcinoma Ki67 7

 Eyeballed estimate Digital image analysis Ki67% = 1.")

 Eyeballed Estimate Interobserver (n=20) Intraclass")

8 Ki67 Labeling Index of NETs Digital Image Analysis for Ki67 Quantification Strong predictor of prognosis Correlates well with mitotic index Sharp separation of well and poorly differentiated neuroendocrine neoplasms Methods of Assessment Manual counting (2000 cells per ENETS) Eyeballed estimate Digital image analysis Ki67% = 1.7 Consistency of Ki67 Determination by Digital Image Analysis, Manual Cell Counting, and Eyeballed Estimate Determining the Ki67 Labeling Index of NETs: How We Do It Image Analysis vs. Manual Counting Image Analysis vs. Eyeballed Estimate (Mean of 20 observers) Eyeballed Estimate Interobserver (n=20) Intraclass Correlation (ICC) 95% Confidence Interval Tang et al. Am J Surg Pathol 2012; 36: Courtesy of Dr. Laura H. Tang Ki67: variation in labeling intensity My count of Ki67 positive cells in this highlighted area is? A. <3 B. 4-6 C D. >10 8













 165 Ki 67 G1")

9 Ki67 Ki67 Heterogeneity in PanNETs Inst. 1 Inst. 2 Inst. 3 Heterogeneity of Ki67 Labeling in NETs: Impact on Prognostic Significance of Grading Heterogeneity of Ki67 Labeling in NETs: Impact on Prognostic Significance of Grading 45 resected hepatic metastases of WD NETs Virtual biopsy TMA Yang et al., Am J Surg Pathol 2011; 35: Ki67 on virtual biopsies and on whole sections 47% of cases with G1 vs. G2 heterogeneity Define grade based on highest Ki67 on whole sections: G2 identified in 48% of core biopsies (3 cores) G2 identified in 35% of core biopsies (1 core) Predictive value of G1 on core biopsy: 65% (3 cores); 59% (1 core) Ki67 and Mitotic Rate Discordance in PanNETs Ki67 and Mitotic Rate Discordance in PanNETs 297 WD PanNETs with Ki 67 data ( ) 36% discordance 264 Mitotic G1 33 Mitotic G2 Mitotic rate: <1 per 10 hpf (G1) Ki-67: 15% positive (G2) 165 Ki 67 G1 99 Ki 67 G2 McCall et al., Am J Surg Pathol 2013; 37: Ki 67 G1 25 Ki 67 G2 9



 36%")







 Mitotic rate")



10 Ki67 and Mitotic Rate Discordance in PanNETs 264 Mitotic G1 165 Ki 67 G1 99 Ki 67 G2 McCall et al., Am J Surg Pathol 2013; 37: WD PanNETs with Ki 67 data ( ) 36% discordance 33 Mitotic G2 8 Ki 67 G1 25 Ki 67 G2 Ki-67 G2/mitotic G1 PanNETs have decreased overall survival Percentage Surviving K1M1 K2M Survival in Years p < 0.01 Well Differentiated PanNET What about G2 / G3 discordance?? (well differentiated tumor vs. poorly differentiated carcinoma) Mitotic rate = 8 / 10 HPF Mitotic rate = 12 / 10 HPF Ki67 = 45% Ki67 = 55% Poorly Differentiated Neuroendocrine Carcinoma Progression of Low Grade to High Grade Neuroendocrine Tumor Ki67 Mitoses <1/10 HPF Mitoses 13/10 HPF 10


 Median survival = 11 mos. Response rate = 31% Stable disease rate = 33% Ki67 < 55% predicted a lower response rate (15% vs 42%, p < 0.")

11 Mixed Ductal Neuroendocrine Carcinoma of Pancreas Ki67 = 2% G1 Ki67 = 45% G3 Tang et al., Clin Cancer Res 2016; 22: 1011 Genetics of Neuroendocrine Neoplasms of the Pancreas Gene Small Cell Large Cell NEC W.D. PanNET Ductal ACa Small Cell Lung CA KRAS 25% 33% 0% >90% 0 10% CDKN2A 11% 50% 0% 80 95% 0 10% TP53 100% 90% 4% 75% 80% SMAD4 0% 10% 0% 55% 0% RB1 89% 50% 0% 13% 90% DAXX/ATRX 0% 0% 43% 0% MEN1 0% 0% 44% 0% 0% mtor genes 15% 1% Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3) Reviewed clinical data on advanced stage G3 NECs, Ki67 > 20% 252 patients received chemotherapy (platinum-based) Median survival = 11 mos. Response rate = 31% Stable disease rate = 33% Ki67 < 55% predicted a lower response rate (15% vs 42%, p < 0.001) Ki67 < 55% predicted a better survival (14 vs 10 months, P < 0.001) Yachida et al., Am J Surg Pathol 2012; 36: 173 Jiao et al., Science 2011; 331: 1199 Sorbye et al., Ann Oncol 2013; 24: Conclusion: Survival of High Grade Neuroendocrine Neoplasms of the Pancreas Some G3 NETs with Ki % may be well differentiated biologically!! ( Well Differentiated NET with an Elevated Proliferative Rate or Well Differentiated NET, G3 ) Basturk et al., Am J SurgPathol 2015; 39:
 NE Neoplasms Well differentiated NE tumor* Grade Mitoses Ki-67 Index G1 <2 / 10 HPF </= 2% G2 2-20 / 10 HPF")

 from G3 NET?")
12 WD NE Tumor PD NE Carcinoma Grading of Pancreatic Neuroendocrine Neoplasms (WHO 2017) Stable Disease Grade Progression NE Tumor Lower Grade High Grade Carcinoma NE Carcinoma High Grade Rapid Disease Disease Progression Progression, Death Two Pathways to the Development of High Grade (G3) NE Neoplasms Well differentiated NE tumor* Grade Mitoses Ki-67 Index G1 <2 / 10 HPF </= 2% G / 10 HPF 3-20% G3** >20 / 10 HPF >20% *Organoid architecture, well differentiated cytology, absence of non-neuroendocrine carcinoma components, may have components of G1 or G2, usually strong immunoexpression of general NE markers **mitoses usually <20/HPF; Ki 67 >20% but usually <50% Poorly differentiated NE carcinoma* Grade Mitoses Ki-67 Index G3** >20 / 10 HPF >20% *Small cell carcinoma and large cell NE carcinoma; less organoid architecture, classic cytology of small cell and large cell NE CA, absence of G1 or G2 NE components, may have non-neuroendocrine carcinoma components, less diffuse immunoexpression of general NE markers **mitoses >20/10 HPF; Ki67 >20% and usually >50% G1 G2 G3 G3 How to distinguish G3 NEC (esp. large cell NE carcinoma) from G3 NET? WDNET PDNEC Ki67% Large Cell NEC Pancreatic G3 NE Neoplasms G3 NET How to distinguish G3 NEC (esp. large cell NE carcinoma) from G3 NET? Clinical clues History of well differentiated NET? Octreotide scan positive? FDG-PET positive? Morphologic clues Lower grade component? Non-neuroendocrine component? Mitotic rate? Molecular clues Status of TP53, RB1, DAXX, ATRX, MEN1 12
 PD-NEC PD-NEC WD-NET TP53")





 pancreatic NE neoplasms were morphologically ambiguous Ambiguous")


 morphologically")




13 Well Differentiated PanNETs (G1-3) Exhibit a Different Molecular Phenotype from Poorly Differentiated NECs (G3) PD-NEC PD-NEC WD-NET TP53 RB1 DAXX / ATRX MEN1 p53 Rb WD PanNET 4% 0 43% 44% PD PanNEC 56% 72% 0 0 p53 Rb DAXX Jiao et al. Science 2011; 331: 1199 Yachida et al., Am J Surg Pathol 2012; 36: 173 Tang et al., Am J Surg Pathol 2016; 40: 1192 Classification of 33 High Grade Pancreatic Neuroendocrine Neoplasms by Secondary Evidence Immunohistochemical Initial Consensus Abnormalities Other Histologic Components Confirmed Classification G1/G2 WD-NET WD-NET WD-NET WD-NET DAXX G1/G2 WD-NET WD-NET WD-NET ATRX G1/G2 WD-NET WD-NET WD-NET G1/G2 WD-NET WD-NET Disease Specific Survival of High Grade (G3) Pancreatic Neuroendocrine Neoplasms WD-NET DAXX G1/G2 WD-NET WD-NET WD-NET G1/G2 WD-NET WD-NET Ambiguous G1/G2 WD-NET WD-NET /33 (58%) of high grade (G3) pancreatic NE neoplasms were morphologically ambiguous Ambiguous G1/G2 WD-NET WD-NET Ambiguous DAXX G1/G2 WD-NET WD-NET Ambiguous ATRX G1/G2 WD-NET WD-NET Ambiguous DAXX G1/G2 WD-NET WD-NET Ambiguous G1/G2 WD-NET WD-NET Ambiguous ATRX WD-NET Ambiguous DAXX G1/G2 WD-NET WD-NET Ambiguous DAXX G1/G2 WD-NET WD-NET Ambiguous G1/G2 WD-NET WD-NET Ambiguous G1/G2 WD-NET WD-NET Ambiguous G1/G2 WD-NET WD-NET Ambiguous G1/G2 WD-NET WD-NET Ambiguous p53/rb PD-NEC Ambiguous p53/smad4 Ductal adenocarcinoma PD-NEC Ambiguous p53/rb PD-NEC 18/19 (95%) morphologically ambiguous high grade pancreatic NEneoplasms successfully classified Percent survival WD-NET PD-NEC p< (N=20) (N=12) Ambiguous p53/rb PD-NEC Ambiguous p53 PD-NEC Ambiguous Undetermined PD-NEC-LCC DAXX G1/G2 WD-NET WD-NET PD-NEC-LCC Rb PD-NEC PD-NEC-LCC Ductal adenocarcinoma PD-NEC PD-NEC-SCC p53 Ductal adenocarcinoma PD-NEC PD-NEC-SCC Rb PD-NEC Months PD-NEC-SCC p53/rb Ductal adenocarcinoma PD-NEC PD-NEC Rb PD-NEC Tang et al., Am J Surg Pathol 2016; 40: 1192 PD-NEC p53 PD-NEC Tang et al., Am J Surg Pathol 2016; 40: 1192 Sequencing of Pancreatic Neuroendocrine Neoplasms at MSKCC p53 p53 13
14 Distinction of G3 NEC from G3 NET: Practical Issues Primary site Pancreas Most common DAXX/ATRX, MEN1 Other GI / pulmonary NETs WD G3 NETs uncommon Formal WHO classification pending p53, Rb, associated exocrine elements for PD Morphology for WD Role of Ki67 >50% = usually PD NEC <50% = either WD NET or PD NEC Role of mitotic rate <20 per 10 HPF = WD NET >20 per 10 HPF = PD NEC Use of Immunohistochemistry in Neuroendocrine Neoplasms: Conclusions IHC is needed for neuroendocrine neoplasm diagnosis, classification, and grading Limitations exist in interpretation and significance Exercise pragmatism, not nihilism IHC is just one tool in the diagnostic arsenal use morphology, clinical findings, molecular data, and common sense! 14
When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms
: Neuroendocrine Neoplasms") When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 David S. Klimstra, MD Chairman, Department of Pathology James
When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 David S. Klimstra, MD Chairman, Department of Pathology James
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Neuroendocrine neoplasms of the lung
 Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
3/22/2017. Disclosure of Relevant Financial Relationships. Ki-67 in Pancreatic Neuroendocrine Neoplasms According to WHO 2017.
 Disclosure of Relevant Financial Relationships Ki-67 in Pancreatic Neuroendocrine Neoplasms According to WHO 2017. USCAP requires that all planners (Education Committee) in a position to influence or control
Disclosure of Relevant Financial Relationships Ki-67 in Pancreatic Neuroendocrine Neoplasms According to WHO 2017. USCAP requires that all planners (Education Committee) in a position to influence or control
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Pancreatic Cancer: The ABCs of the AJCC and WHO
 Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens
 is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens") Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Small cell neuroendocrine carcinoma icd 10
 Small cell neuroendocrine carcinoma icd 10 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM C34.90 - includes detailed rules, notes, synonyms, ICD -9- crosswalks, DRG. In most series, LCLC's
Small cell neuroendocrine carcinoma icd 10 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM C34.90 - includes detailed rules, notes, synonyms, ICD -9- crosswalks, DRG. In most series, LCLC's
Prognostic factors and treatment of gastroenteropancreatic G3 neuroendocrine carcinomas.
 Prognostic factors and treatment of gastroenteropancreatic G3 neuroendocrine carcinomas. Halfdan Sorbye Medical Oncologist Professor, MD Dept of Oncology Haukeland Univ Hospital Bergen, Norway Gastroenteropancreatic
Prognostic factors and treatment of gastroenteropancreatic G3 neuroendocrine carcinomas. Halfdan Sorbye Medical Oncologist Professor, MD Dept of Oncology Haukeland Univ Hospital Bergen, Norway Gastroenteropancreatic
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Hot of the press. Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ
 Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
The clinically challenging entity of liver metastasis from tumors of unknown primary
 The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
Lung neuroendocrine tumors: pathological characteristics
 Review Article Lung neuroendocrine tumors: pathological characteristics Luisella Righi 1, Gaia Gatti 1, Marco Volante 1, Mauro Papotti 2 1 Department of Oncology, San Luigi Hospital, Orbassano, Italy;
Review Article Lung neuroendocrine tumors: pathological characteristics Luisella Righi 1, Gaia Gatti 1, Marco Volante 1, Mauro Papotti 2 1 Department of Oncology, San Luigi Hospital, Orbassano, Italy;
WHO e TNM: Importanza della classificazione nell approccio terapeutico
 WHO e TNM: Importanza della classificazione nell approccio terapeutico Marco Volante Mauro Papotti Dipartimento di Scienze Cliniche e Biologiche Ospedale San Luigi Orbassano, Torino Rare tumors Heterogeneous
WHO e TNM: Importanza della classificazione nell approccio terapeutico Marco Volante Mauro Papotti Dipartimento di Scienze Cliniche e Biologiche Ospedale San Luigi Orbassano, Torino Rare tumors Heterogeneous
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
EUS FNA NEUROENDOCRINE TUMORS. A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain)
") EUS FNA NEUROENDOCRINE TUMORS A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain) GI NEUROENDOCRINE TUMORS GENERAL CONCEPTS Rare neoplasms arising from the neuroendocrine cells of the GI tract Include:
EUS FNA NEUROENDOCRINE TUMORS A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain) GI NEUROENDOCRINE TUMORS GENERAL CONCEPTS Rare neoplasms arising from the neuroendocrine cells of the GI tract Include:
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Enterprise Interest. Pfizer, Roche, BMS, MSD, Novartis
 Enterprise Interest Pfizer, Roche, BMS, MSD, Novartis Beyond the WHO 2015 classification of lung neuroendocrine tumours Genomics of lung NETs & identification of biomarkers for prognosis and therapy Prof.
Enterprise Interest Pfizer, Roche, BMS, MSD, Novartis Beyond the WHO 2015 classification of lung neuroendocrine tumours Genomics of lung NETs & identification of biomarkers for prognosis and therapy Prof.
NO DISCLOSURES. 1. Incipient neoplasia: Dysplasia/Tis NEUROENDOCRINE TUMORS OF THE GI AND PANCREATOBILIARY TRACT
 3002: CYTO- HISTOLOGY OF NEUROENDOCRINE NEOPLASMS OF LUNG, GASTROINTESTINAL TRACT AND PANCREAS Momin Siddiqui, MD, FIAC Professor Divisional Director and Chief of Cytopathology Emory University Hospital
3002: CYTO- HISTOLOGY OF NEUROENDOCRINE NEOPLASMS OF LUNG, GASTROINTESTINAL TRACT AND PANCREAS Momin Siddiqui, MD, FIAC Professor Divisional Director and Chief of Cytopathology Emory University Hospital
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Histology: Its Influence on Therapeutic Decision Making
 Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Immunohistochemical Profile of Lung Tumors in Image Guided Biopsies
 Original Article DOI: 10.21276/APALM.1342 Immunohistochemical Profile of Lung Tumors in Image Guided Biopsies T. Pavithra 1 *, A. Dhanalakshmi 1, C. Lalitha 1, K.B. Lavanya 1 and S. Shifa 2 Department
Original Article DOI: 10.21276/APALM.1342 Immunohistochemical Profile of Lung Tumors in Image Guided Biopsies T. Pavithra 1 *, A. Dhanalakshmi 1, C. Lalitha 1, K.B. Lavanya 1 and S. Shifa 2 Department
EBUS-TBNA Diagnosis and Staging of Lung Cancer
 EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
ORIGINAL ARTICLE. Am J Surg Pathol Volume 00, Number 00,
 ORIGINAL ARTICLE The High-grade (WHO G3) Pancreatic Neuroendocrine Tumor Category Is Morphologically and Biologically Heterogenous and Includes Both Well Differentiated and Poorly Differentiated Neoplasms
ORIGINAL ARTICLE The High-grade (WHO G3) Pancreatic Neuroendocrine Tumor Category Is Morphologically and Biologically Heterogenous and Includes Both Well Differentiated and Poorly Differentiated Neoplasms
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
NEUROENDOCRINE DIFFERENTIATION IN EPITHELIAL TUMORS Marco Volante
 NEUROENDOCRINE DIFFERENTIATION IN EPITHELIAL TUMORS Marco Volante University of Turin, San Luigi Hospital, Orbassano, Turin, Italy marco.volante@unito.it pure NE tum..a grey zone pure non-ne ca. 0% NE
NEUROENDOCRINE DIFFERENTIATION IN EPITHELIAL TUMORS Marco Volante University of Turin, San Luigi Hospital, Orbassano, Turin, Italy marco.volante@unito.it pure NE tum..a grey zone pure non-ne ca. 0% NE
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Small cell lung cancer and large cell neuroendocrine tumours interobserver variability. Michael den Bakker Erasmus MC
 Small cell lung cancer and large cell neuroendocrine tumours interobserver variability Michael den Bakker Erasmus MC PPC London 2007 WEB presentation Pulmonary pathology Club presentation, London, November
Small cell lung cancer and large cell neuroendocrine tumours interobserver variability Michael den Bakker Erasmus MC PPC London 2007 WEB presentation Pulmonary pathology Club presentation, London, November
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες
 NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY
 HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
CRITICAL ANALYSIS OF NEN GUIDELINES. G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines
 CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach
 The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
Genetics of Pancreatic Neuroendocrine Tumors Saturday March 2, 2013
 Genetics of Pancreatic Neuroendocrine Tumors Saturday March 2, 2013 Ralph H. Hruban, M.D. Professor of Pathology and Oncology The Sol Goldman Pancreatic Cancer Research Center The Johns Hopkins Medical
Genetics of Pancreatic Neuroendocrine Tumors Saturday March 2, 2013 Ralph H. Hruban, M.D. Professor of Pathology and Oncology The Sol Goldman Pancreatic Cancer Research Center The Johns Hopkins Medical
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
I. Diagnosis of the cancer type in CUP
 Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
OUTLINE OUTLINE 25/04/2018. Massimo Milione MD, PhD. General Features and Classifications. Ki67 role?
 25/04/2018 Massimo Milione MD, PhD Department of Pathology and Laboratory Medicine Fondazione IRCCS Istituto Nazionale Tumori Milano- Italy massimo.milione@istitutotumori.mi.it OUTLINE General Features
25/04/2018 Massimo Milione MD, PhD Department of Pathology and Laboratory Medicine Fondazione IRCCS Istituto Nazionale Tumori Milano- Italy massimo.milione@istitutotumori.mi.it OUTLINE General Features
Chibueze Onyemkpa 1, Alan Davis 1, Michael McLeod 1, Tolutope Oyasiji 1,2. Original Article
 Original Article Typical carcinoids, goblet cell carcinoids, mixed adenoneuroendocrine carcinomas, neuroendocrine carcinomas and adenocarcinomas of the appendix: a comparative analysis of survival profile
Original Article Typical carcinoids, goblet cell carcinoids, mixed adenoneuroendocrine carcinomas, neuroendocrine carcinomas and adenocarcinomas of the appendix: a comparative analysis of survival profile
Neoplasms Of The Lung: Based On The Proceedings Of The 57th Annual Anatomic Pathology Slide Seminar Of The American Society Of Clinical Pathologists
 Neoplasms Of The Lung: Based On The Proceedings Of The 57th Annual Anatomic Pathology Slide Seminar Of The American Society Of Clinical Pathologists By David H. Dail;Samuel P. Hammar;Darryl Carter If you
Neoplasms Of The Lung: Based On The Proceedings Of The 57th Annual Anatomic Pathology Slide Seminar Of The American Society Of Clinical Pathologists By David H. Dail;Samuel P. Hammar;Darryl Carter If you
Disclosure of Relevant Financial Relationships NON-SMALL CELL LUNG CANCER: 70% PRESENT IN ADVANCED STAGE
 MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Next generation image analysis for immunohistochemistry quantitation
 Next generation image analysis for immunohistochemistry quantitation Ben Vainer Department of Pathology, Rigshospitalet University of Copenhagen Medical Center Men are only so good as their technical developments
Next generation image analysis for immunohistochemistry quantitation Ben Vainer Department of Pathology, Rigshospitalet University of Copenhagen Medical Center Men are only so good as their technical developments
Fast, automated, precise
 Thermo Scientific B R A H M S / NSE Immunodiagnostic Assays Fast, automated, precise Neuroendocrine tumor markers on KRYPTOR Systems First and only fully automated CgA assay worldwide Shortest time to
Thermo Scientific B R A H M S / NSE Immunodiagnostic Assays Fast, automated, precise Neuroendocrine tumor markers on KRYPTOR Systems First and only fully automated CgA assay worldwide Shortest time to
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas
 Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
5/21/2018. An Update on Pancreas Neoplasms. Arief Suriawinata, M.D. Lines of Differentiation in Pancreatic Neoplasms
 An Update on Pancreas Neoplasms Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and Laboratory Medicine Dartmouth-Hitchcock
An Update on Pancreas Neoplasms Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and Laboratory Medicine Dartmouth-Hitchcock
Histopathological diagnosis of CUP
 Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
CODING TUMOUR MORPHOLOGY. Otto Visser
 CODING TUMOUR MORPHOLOGY Otto Visser INTRODUCTION The morphology describes the tissue of the tumour closest to normal tissue Well differentiated tumours are closest to normal Undifferentiated tumours show
CODING TUMOUR MORPHOLOGY Otto Visser INTRODUCTION The morphology describes the tissue of the tumour closest to normal tissue Well differentiated tumours are closest to normal Undifferentiated tumours show
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC
 Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources
 Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Basaloid Carcinoma of the Lung: A Really Dismal Histologic Variant?
 Carcinoma of the Lung: A Really Dismal Histologic Variant? Dae Joon Kim, MD, Kil Dong Kim, MD, Dong Hwan Shin, MD, Jae Y Ro, MD, and Kyung Young Chung, MD Departments of Thoracic and Cardiovascular Surgery,
Carcinoma of the Lung: A Really Dismal Histologic Variant? Dae Joon Kim, MD, Kil Dong Kim, MD, Dong Hwan Shin, MD, Jae Y Ro, MD, and Kyung Young Chung, MD Departments of Thoracic and Cardiovascular Surgery,
Neuroendocrine Tumor of Unknown Primary Accompanied with Stomach Adenocarcinoma
 J Gastric Cancer 2011;11(4):234-238 http://dx.doi.org/10.5230/jgc.2011.11.4.234 Case Report Neuroendocrine Tumor of Unknown Primary Accompanied with Stomach Adenocarcinoma Ho-Yeun Kim, Sung-Il Choi 1,
J Gastric Cancer 2011;11(4):234-238 http://dx.doi.org/10.5230/jgc.2011.11.4.234 Case Report Neuroendocrine Tumor of Unknown Primary Accompanied with Stomach Adenocarcinoma Ho-Yeun Kim, Sung-Il Choi 1,
Large-Cell Neuroendocrine Carcinoma of the Lung
 Accurate classification of this malignancy will help to guide management decisions regarding resection and adjuvant therapy. Manus Island Tree Snail_2281. Photograph courtesy of Henry Domke, MD. www.henrydomke.com.
Accurate classification of this malignancy will help to guide management decisions regarding resection and adjuvant therapy. Manus Island Tree Snail_2281. Photograph courtesy of Henry Domke, MD. www.henrydomke.com.
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case
 Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
5/1/2009. Squamous Dysplasia/CIS AAH DIPNECH. Adenocarcinoma
 Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
Immunohistochemical classification of the unknown primary tumour (UPT) Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark") Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Financial disclosures
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung
 Case Reports Jpn J Clin Oncol 2011;41(6)797 802 doi:10.1093/jjco/hyr034 Advance Access Publication 16 March 2011 Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung Taichiro
Case Reports Jpn J Clin Oncol 2011;41(6)797 802 doi:10.1093/jjco/hyr034 Advance Access Publication 16 March 2011 Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung Taichiro
The Impact of Adjuvant Chemotherapy in Pulmonary Large Cell Neuroendocrine Carcinoma (LCNC)
") The Impact of Adjuvant Chemotherapy in Pulmonary Large Cell Neuroendocrine Carcinoma (LCNC) Disclosure None Background Torino, Italy LCNC Rare tumor (2% to 3% all resected primary lung cancers) Preoperative
The Impact of Adjuvant Chemotherapy in Pulmonary Large Cell Neuroendocrine Carcinoma (LCNC) Disclosure None Background Torino, Italy LCNC Rare tumor (2% to 3% all resected primary lung cancers) Preoperative
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
What the oncologist needs to know from the pathologist?
 Grade 3 GEP Neuroendocrine Neoplasms: from pathology to the clinic and back What the oncologist needs to know from the pathologist? Marianne Pavel Friedrich Alexander Universität Erlangen-Nürnberg 30th
Grade 3 GEP Neuroendocrine Neoplasms: from pathology to the clinic and back What the oncologist needs to know from the pathologist? Marianne Pavel Friedrich Alexander Universität Erlangen-Nürnberg 30th
What s New in Adrenal Gland Pathology. Marina Scarpelli
 What s New in Adrenal Gland Pathology Marina Scarpelli Background Histological criteria for adrenocortical proliferative lesions Immunohistochemical markers Molecular markers Histological Criteria for
What s New in Adrenal Gland Pathology Marina Scarpelli Background Histological criteria for adrenocortical proliferative lesions Immunohistochemical markers Molecular markers Histological Criteria for
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Solid pseudopapillary tumour of the pancreas: Report of five cases
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
3/22/2017. Disclosure of Relevant Financial Relationships. Disclosure of Relevant Financial Relationships. Grading G1. Grading. Ki67 index V.
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship