Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
|
|
|
- Cornelia Kennedy
- 6 years ago
- Views:
Transcription
1 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD
2 New (2017) WHO
3 WHO 2017 (endocrine book; for pancreas)
4 WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended to be used also for GI NETs
5 Change # 1: Tumor vs Carcinoma further clarified (but still problematic)
6 I have a metastatic NE neoplasm in the liver, what do I call it?

7 How do we report a NET in the liver?
8 CASE: WD neuroendocrine neoplasm in the liver DIAGNOSIS: METASTATIC WELL-DIFFERENTIATED NEUROENDOCRINE TUMOR*, GRADE 1 Comment: This tumor is a WDNET. It is NOT a PD carcinoma (not a high grade neuroendocrine carcinoma). Mitotic activity is < 2/10 ; Ki67 < 2% (Grade 1 of 3).
9 Change #2: Ki67 > 20% can be tumor OR carcinoma
10 Change #3: Ki67 between 2 and 2.99 is G1 (not G2)
11 Change #3: Ki67 between 2 and 2.99 is G1 (not G2) ~ 15% of PanNETs fall to this 2-3% range (Reid, M. Modern Pathol, 2014)
12 WDNETs Diagnostic pitfalls
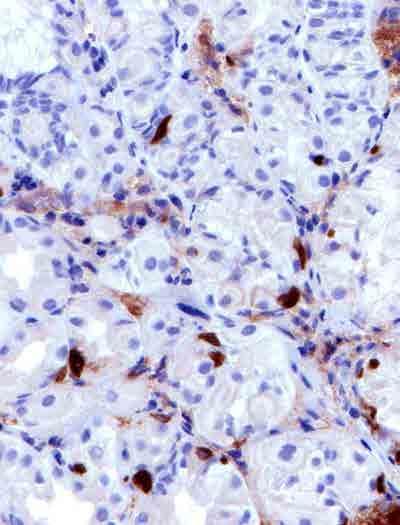
13 WDNET Diagnostic problems Crush artefacts (in biopsies) Atypical patterns Especially tubular patterns Chromogranin-A negativity (common in appendiceal and rectal ones)

14 Problem: Limited bx - Mucosal component can be small - Artifacts common

15 Degenerated gland appearance

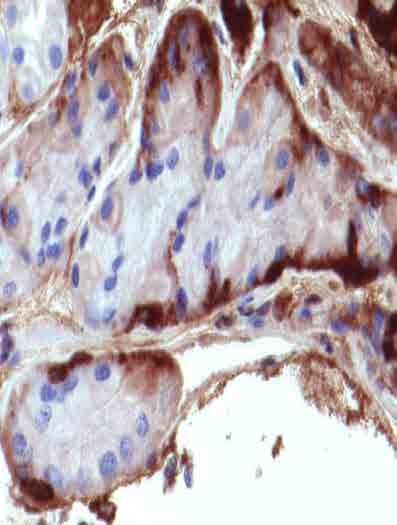
16 Ampullary tumor: Original dx, adenoca. Pitfall: Glandular patterns

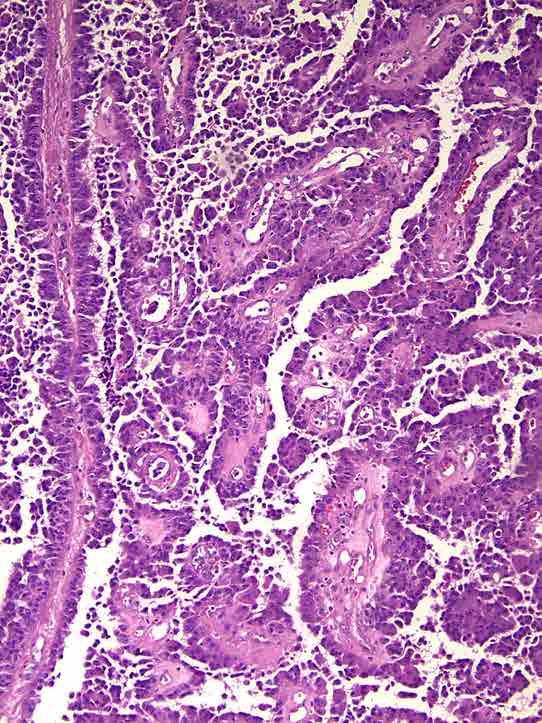
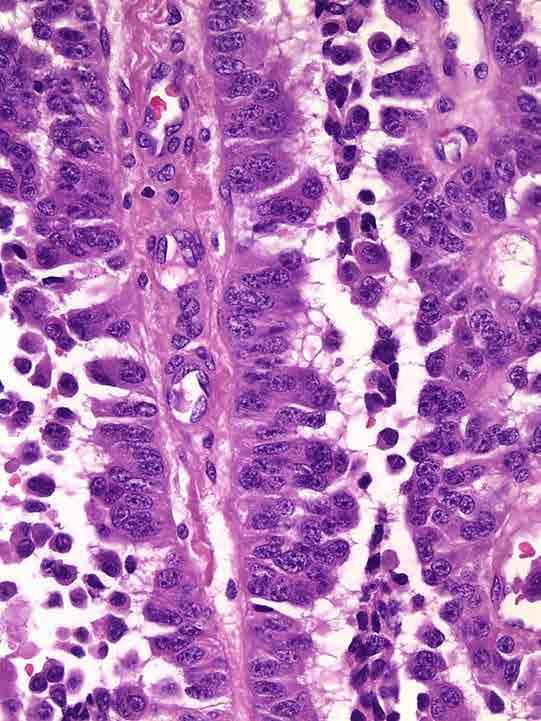
17 Ampullary somatostatinoma ( GLANDULAR psammomatous carcinoid )


18 Ampullary somatostatinoma Glandular psammomatous carcinoid Glandular pattern Psammoma bodies Neurofibromatosis LN metastasis in % (despite their small size )

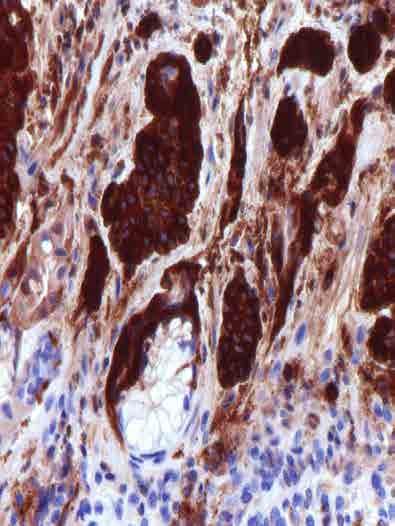
19 Intraluminal mucin may be prominent, but no convincing intracytoplasmic mucin
 of")
20 Tubular WDNET (carcinoid) of appendix


21 PanNETs: Morphologic spectrum is wider than appreciated In addition to the classical nested and trabecular patterns

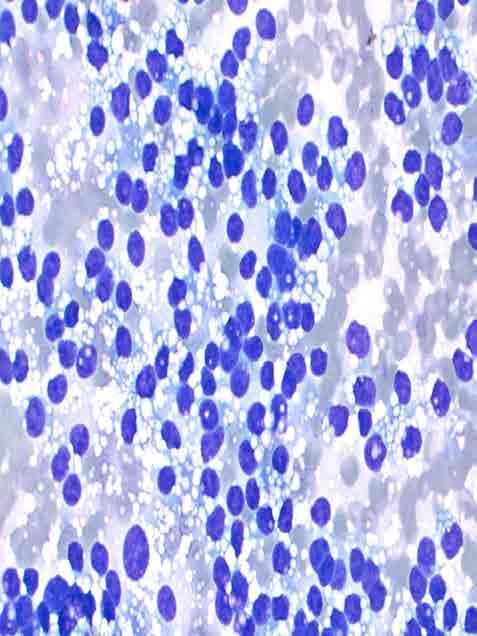
22 PanNETs: Nucleoli may be prominent on cytology
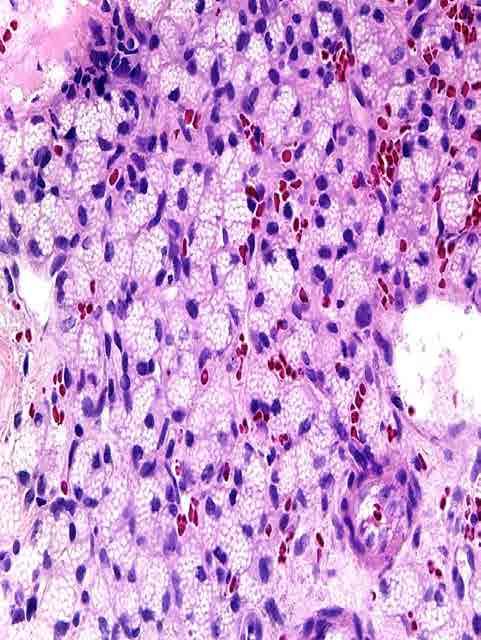
23 Lipid-rich PanNETs:


24 Oncocytic PanNETs: Probably more aggressive


25 Pleomorphic Variant of PanNET: Has no clinical significance Note single plasmacytoid cells and cells with focal degenerative endocrine atypia
26
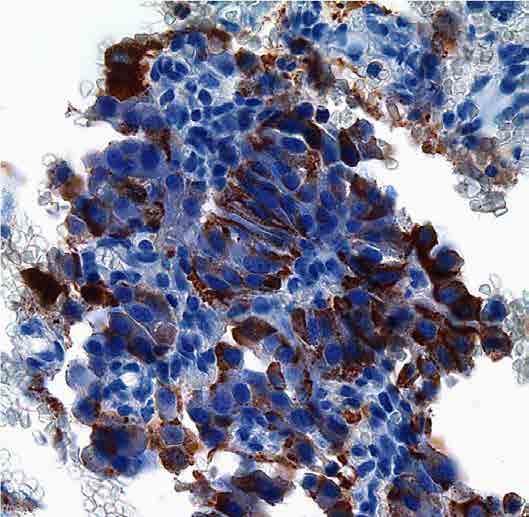
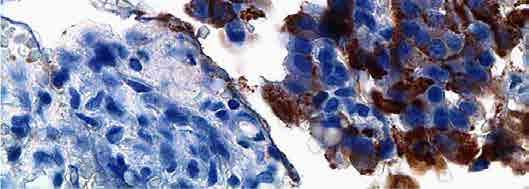
27 CHROMOGRANIN CHROMATIN
 CK19 (good ductal")
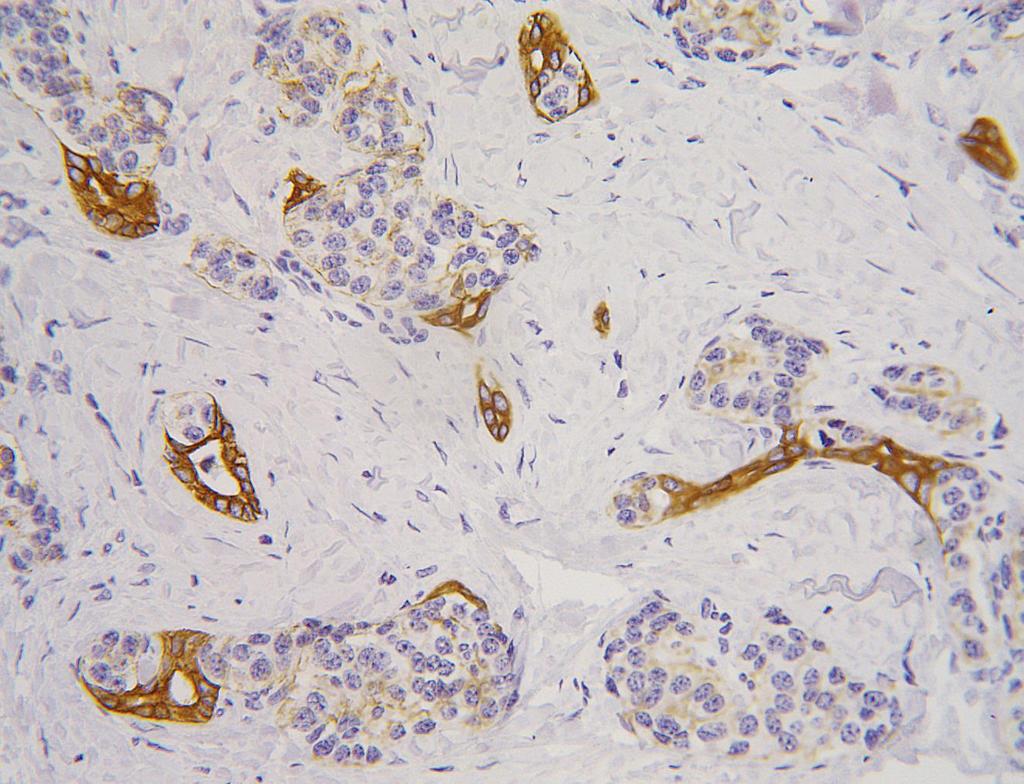
28 Benign ducts can be prominent in PanNETs (NO significance) CK19 (good ductal marker)
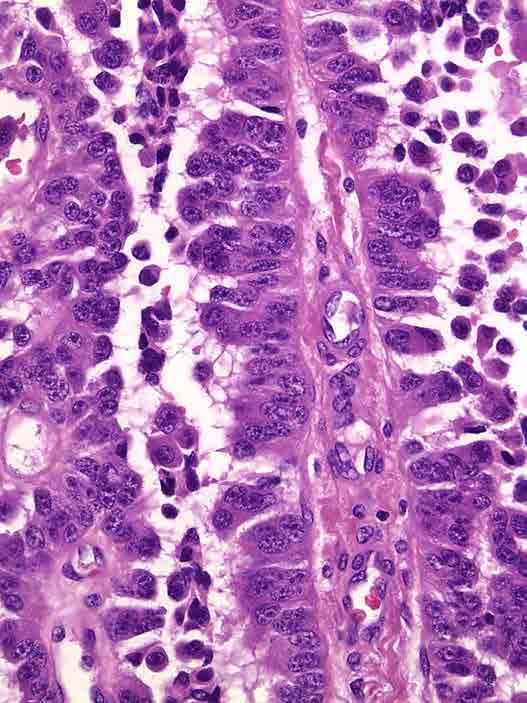
29 Ductulo-insular PanNET
30 WDNETs Determinants of outcome; Reporting
31 Determinants of biologic behavior in GI WDNETs ( carcinoids ) 1. Location 2. Cell type 3. Clinical setting, syndromic background 4. Size (stage) 5. Grade 6. Adjunct histologic/biologic parameters
32 Most appendiceal classical WDNETs (carcinoid) are asymptomatic Most are microscopic; 2% of autopsies Most rectal ones are non-metastatic Most < 1 cm Ileal or colonic: Mets are common Most are advanced at diagnosis
33 Determinants of biologic behavior in NETs 1. Location 2. Cell type / hormonal status Most insulinomas are benign but they are also small at diagnosis (> 70% are < 1 cm). Most glucagonomas are malignant but they are also higher stage (large; >3 cm) at diagnosis 3. Clinical setting, syndromic background 4. Size (stage) 5. Grade 6. Adjunct histologic/biologic parameters
34 Determinants of biologic behavior in GI NETs ( carcinoids ) 1. Location 2. Cell type 3. Clinical setting, syndromic background 4. Size (stage) 5. Grade 6. Adjunct histologic/biologic parameters
35 The importance of clinical setting Example: Gastric NETs Type I (hypergastrinemia-related / ELC cell) Typically benign course Type II (ZE or MEN syndrome) Type III (Sporadic) Typically aggressive
36 Stomach- Enterochromaffin-like cell lesions Etiology Atrophic gastritis Medication Gastrinoma Hypo or achlorhydria Sustained hypergastrinemia Genetic factors? ELC Hyperplasia ELC Dysplasia ELC NET (carcinoid)
37 Enterochromaffin- like cell lesions in the stomach Hyperplasia Rare cells Linear Micronodular
; Vanoli et al, Human")
38 Dysplasia Nodules > 150 microns Conglomerated micronodules Microinfiltration in the lamina propria New stroma ENETS /TNM proposal: Tis (In-situ tumor/dysplasia); Vanoli et al, Human Pathol, 2013
39 SP Report If it is all composed of tiny clusters Stomach, bx: ELC-cell proliferation in the background of atrophic gastritis If it also shows conglomerated, large clusters Minute WDNET of type A (see comment), arising in the background of ELC-cell proliferation and atrophic gastritis

40 Type A or type 1 carcinoid (NET)
41 The importance of clinical setting Example: Gastric NETs Type I (hypergastrinemia-related / ELC cell) Typically benign course Type II (ZE or MEN syndrome) Type III (Sporadic) Typically aggressive
42 Determinants of biologic behavior in NETs 1. Location 2. Cell type 3. Clinical setting, syndromic background 4. Stage (depth, size and mets) 5. Grade 6. Adjunct histologic/biologic parameters
43 Determinants of biologic behavior in GI NETs 1. Location 2. Cell type 3. Clinical setting, syndromic background 4. Size (stage) 5. Grade 6. Adjunct histologic/biologic parameters
44 WHO 2017 (endocrine book; for pancreas)
45 Problems with Ki67: How to count?
46 Problems with Ki67: How to count? 1. Refuse to count? 2. Eyeballing 3. Counting # of cells by live microscope 4. Have the machine count it (automated) 5. Have someone else count it 6. Counting # of cells by static field pictures from a computer
47 Problems with Ki67: How to count? 1. Refuse to count 2. Eyeballing (guess-timating)

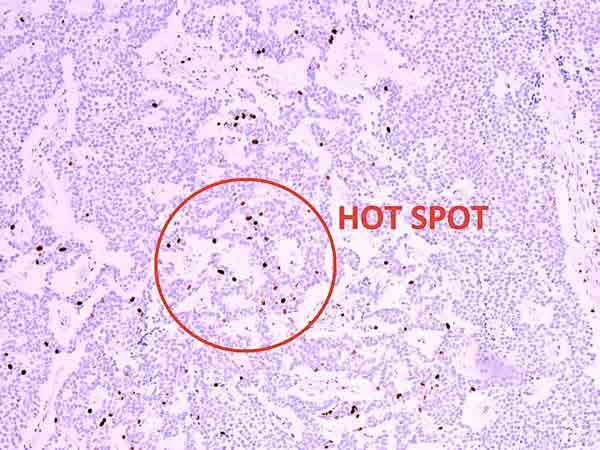
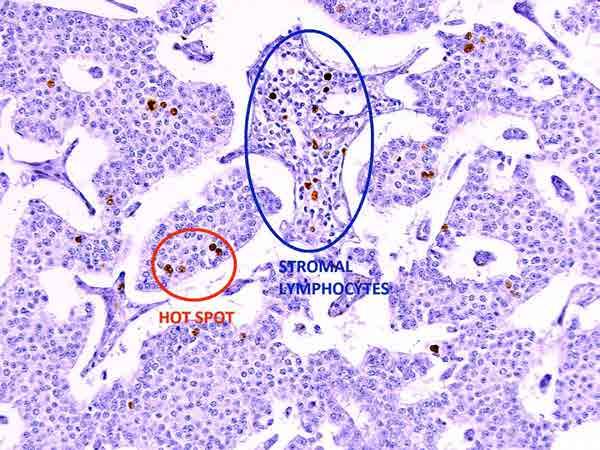
48 Results of eye-balling of Ki67 index by 18 observers in 45 cases illustrates striking inter-observer variability (as well as grade variability)
49 Problems with Ki67: How to count? 1. Refuse to count 2. Eyeballing About 60 % of the cases have an index close to the categorical cut-offs: Only ~ 5% are in the extremes (< 1% and > 30%) Reid et al. Mod Pathol. 2014
50 Problems with Ki67: How to count? 1. Refuse to count 2. Eyeballing 3. Counting # of cells by live microscope
51 Problems with Ki67: How to count? 1. Refuse to count 2. Eyeballing 3. Counting # of cells by live microscope
52 Problems with Ki67: How to count? 1. Refuse to count 2. Eyeballing 3. Counting # of cells by live microscope 4. Have the machine count it (automated)
53 Problems with Ki67: How to count? 1. Refuse to count 2. Eyeballing 3. Counting # of cells by live microscope 4. Have the machine count it (automated) Machine also counts: Hemosiderin Lymphocytes Endothelial cells Etc
54 Problems with Ki67: How to count? 1. Refuse to count 2. Eyeballing 3. Counting # of cells by live microscope 4. Have the machine count it (automated) 5. Have someone else count it
55 Problems with Ki67: How to count? 1. Refuse to count 2. Eyeballing 3. Counting # of cells by live microscope 4. Have the machine count it (automated) 5. Have someone else count it Counting # of cells by static field pictures from a computer
 in daily")
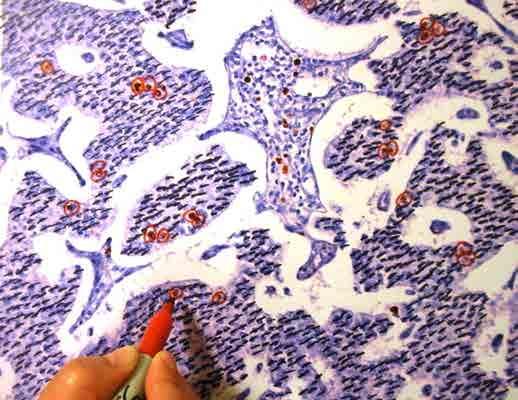
56 Manual count on camera-captured-printed image is the most applicable approach (practical and accurate) in daily life



57
58

59 37 (pos) (37 pos neg) 10%
60 Current Surg Path Report Ileum; resection: - Well differentiated neuroendocrine tumor (classical carcinoid), Grade 1 of 3 in the WHO-2010 classification (see comment). Size: 2 cm Depth of invasion: Deep in muscularis propria VI: - ; PNI: - Margins: - LNs: 0/14. AJCC-stage: T2, N0; ENETS-Stage: T2, N0 Comment: - Mitotic activity: 1/10 HPF - Ki-67: 1.8 % - Neuroendocrine markers: Not performed (classical carcinoid)

61
62 Beyond WDNET. NET-3 vs PDNEC
63 Well-differentiated PanNET (2 examples)

64 (Morphologically) Well-differentiated but Ki67 > 20%
65 (Morphologically) Well-differentiated but Ki67 > 20%: [ GRADE DISCORDANT NE TUMOR] Diagnosis: Well-differentiated PanNE TUMOR, grade 3 of 3 by Ki67 proliferation index Comment: NET-3 (per WHO 2017) NOT a PDNEC Reference: Basturk et al, Am J Surg Pathol, 2014 Basturk et al, Am J Surg Pathol, 2015

66 Poorly differentiated NE carcinoma
67 IHC for confirming NE differentiation Chromogranin Synaptophysin CD56 (cautiously) But, NOT NSE or others It is advisable to have the support of at least one of these markers in order to distinguish true NECs from incomplete examples or its mimickers


68 PD NE carcinoma (ki67 typically > 50%) Diagnosis: Poorly differentiated neuroendocrine carcinoma Reference: Basturk et al, Am J Surg Pathol, 2014 Basturk et al, Am J Surg Pathol, 2015
69 Poorly diff NEC- Problem: DDx from other PD neoplasms Focal NE differentiation in the classical carcinomas. Poor prognosis? Poorly differentiated carcinoma, NOS Medullary carcinoma Basaloid/cloacogenic-type squamous ca Melanoma Sarcomas with epithelioid features
70 Poorly diff NEC- Problem: DDx from other PD neoplasms Focal NE differentiation in the classical carcinomas. Poor prognosis? Poorly differentiated carcinoma, NOS Medullary carcinoma Basaloid/cloacogenic-type squamous ca Melanoma Sarcomas with epithelioid features Any convincing NE component should be recognized and reported duly
.")
71 Poorly diff NECs of GI/PB Often associated with conventional adenocarcinoma and adenoma component Most are not transformation of WD-NET Aggressive behavior (worse than ordinary carcinomas of respective sites). Small cell therapy protocol may work better than ordinary ca protocols (inadequate data).
72 And then there are the tougher ones
73

74 Ambiguous group : WD? PD? Ki %

75 Loss of RB; positivity of P53: PDNEC If present, loss of ATRX/DAXX: WDNET Rb loss Tang et al, Am J Surg Pathol Jun 1
76 Conclusions NENs can display unusual morphologies that ought to be kept in mind All NENs are malignant neoplasms (although incipient precursor lesions do occur but difficult to define) WDNETs ought to be graded and staged as any other malignancy WHO 2017 clearly distinguishes WDNET from PDNEC based on the morphology (not Ki67)
77 Conclusions Grade-discordant NETs (well-diff by morphology but Ki67> 20) now has a specific home as WDNET-G3 G3 NEN does NOT mean PDNEC Ambiguous cases (in between WDNET and PDNEC) do occur Associated w/ increased aggressive behavior relative to G1/2 tumors but better than G3 PDNEC New molecular/ihc markers (p53, Rb, DAXX, ATRX) can help with classification

78

79 CASE FOR DISCUSSION Appendiceal tumor: relatively intact wall; layers preserved

80 A subtle infiltrate of very well-formed glandular units

81 Composed of goblet cells; very similar to colonic crypts

82 Classical Goblet cell carcinoid Is it really a carcinoid? Chromogranin, only focal Ordinary carcinoid pattern is very very uncommon If low-grade/low-stage (confined to the appendix), behaves like a carcinoid (prognosis is good)

83 THIS CASE ALSO SHOWED Compressed, ill-defined, irregular glandular units

84 Areas with stromal mucin deposition was prominent

85 Mucin was associated with disorganized neoplastic cells
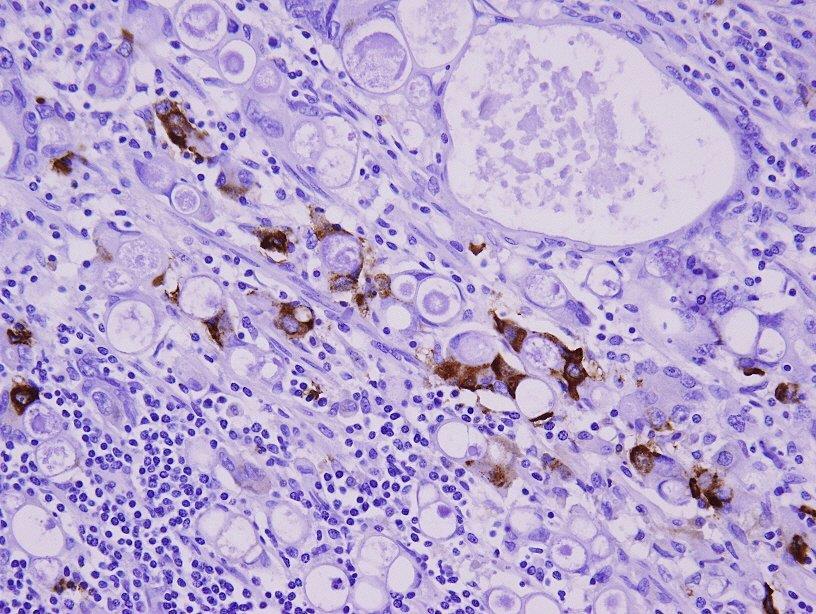
86 CHROMOGRANIN
87 CASE -Diagnosis ADENOCARCINOMA EX-GCC APPENDICEAL CRYPT CELL ADENOCARCINOMA WHO: Mixed GCC-adenocarcinoma
88
 2. Crypt like structures 3. Small clusters of goblet cells 4. Microglandular units")
89 Distinctive features of adenoca ex GCC (appendiceal crypt cell adenocarcinoma) allow it to be recognized as an appendiceal primary even in metastatic sites: 1. Goblet cells (with voluminous pale-basophilic cytoplasm) 2. Crypt like structures 3. Small clusters of goblet cells 4. Microglandular units

90 Small glandular units composed of goblet type cells

91 Signet-ring like cells with voluminous cytoplasm, in small clusters: Most likely appendiceal (less likely gastric)

92 Especially if they form small, round glandular elements

93 Small round glands resembling crypts, even if without goblet cells: Still, highly suggestive of appendiceal origin
94 NEGATIVE < 10% 10-75% DIFFUSE (> 75%) Chromo Synapto CD
 Chromo 47 31 14 4 Synapto 36")

 is")
95 NEGATIVE < 10% 10-75% DIFFUSE (> 75%) Chromo Synapto CD Appendiceal crypt cell adenocarcinoma (Adenocarcinoma ex-goblet-cell- carcinoid ) is NOT a neuroendocrine tumor

96 Morphologic ddx is upper- GI (gastric) carcinoma signet-ring like cells small tubular configuration IHC: Lower-GI profile CDX2 98% MUC2-76% CK20-90% Upper GI markers mostly negative: (MUC1 11%, MUC5AC 20%, MUC6 2%; CK7 16%).
97 Conclusions NENs can display unusual morphologies that ought to be kept in mind All NENs are malignant neoplasms (although incipient precursor lesions do occur but difficult to define) WDNETs ought to be graded and staged as any other malignancy WHO 2017 clearly distinguishes WDNET from PDNEC based on the morphology (not Ki67)
98 Conclusions Grade-discordant NETs (well-diff by morphology but Ki67> 20) now has a specific home as WDNET-G3 G3 NEN does NOT mean PDNEC Ambiguous cases (in between WDNET and PDNEC) do occur Associated w/ increased aggressive behavior relative to G1/2 tumors but better than G3 PDNEC New molecular/ihc markers (p53, Rb, DAXX, ATRX) can help with classification
99 Conclusion Adenocarcinoma ex-gcc is NOT a neuroendocrine tumor per se, but rather an appendiceal type adenocarcinoma with cyrpt cell differentiation
100
101 Determining the site of origin of a metastatic NET Is it needed? Is it possible?
102 Determining the site of origin of a NET Often not possible; lots of overlaps Often not necessary WD-NET is a perfectly adequate diagnosis Don t be cornered by your clinicians to commit Imaging studies (octreotide scan and PET) and serologic studies (serotonin etc) are very successful in identifying the primary Having said that, few site-specific patterns do exist (and good to be aware of)

103 NET in the pancreas:
104

105 CDX2 Islet is negative
")
106 Isl1 (islet-1)

107 Ileal tumor resected subsequently

108 The current impression on the sitespecificity of the markers Yang et al, AJSP, July, 2017,
NO DISCLOSURES. 1. Incipient neoplasia: Dysplasia/Tis NEUROENDOCRINE TUMORS OF THE GI AND PANCREATOBILIARY TRACT
 3002: CYTO- HISTOLOGY OF NEUROENDOCRINE NEOPLASMS OF LUNG, GASTROINTESTINAL TRACT AND PANCREAS Momin Siddiqui, MD, FIAC Professor Divisional Director and Chief of Cytopathology Emory University Hospital
3002: CYTO- HISTOLOGY OF NEUROENDOCRINE NEOPLASMS OF LUNG, GASTROINTESTINAL TRACT AND PANCREAS Momin Siddiqui, MD, FIAC Professor Divisional Director and Chief of Cytopathology Emory University Hospital
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
3/23/2017. Differentiation: Differentiation: Immunohistochemistry. Well Differentiated vs. Poorly Differentiated Neuroendocrine Neoplasms
 Disclosure Statement When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 Dr. Klimstra receives royalty payments
Disclosure Statement When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 Dr. Klimstra receives royalty payments
Syllabus. Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix. Appendiceal tumors. Summary provided Complete presentation
 2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms
: Neuroendocrine Neoplasms") When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 David S. Klimstra, MD Chairman, Department of Pathology James
When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 David S. Klimstra, MD Chairman, Department of Pathology James
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Neuroendocrine neoplasms of the lung
 Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Pancreatic Cancer: The ABCs of the AJCC and WHO
 Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Small cell neuroendocrine carcinoma icd 10
 Small cell neuroendocrine carcinoma icd 10 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM C34.90 - includes detailed rules, notes, synonyms, ICD -9- crosswalks, DRG. In most series, LCLC's
Small cell neuroendocrine carcinoma icd 10 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM C34.90 - includes detailed rules, notes, synonyms, ICD -9- crosswalks, DRG. In most series, LCLC's
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Unknown Slides Conference
 Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Case in discussion. Common diagnostic problems in gallbladder pathology 62, F
 Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Nasal Cavity and Paranasal Sinuses
 Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
FINALIZED SEER SINQ QUESTIONS
 0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012
 Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Biliary Tract Neoplasia: A Cyto-histologic Review. Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital
 Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
DIAGNOSTIC DILEMMA. Case Reports Clinical history. Materials and Methods
 DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency
 Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
5/21/2018. An Update on Pancreas Neoplasms. Arief Suriawinata, M.D. Lines of Differentiation in Pancreatic Neoplasms
 An Update on Pancreas Neoplasms Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and Laboratory Medicine Dartmouth-Hitchcock
An Update on Pancreas Neoplasms Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and Laboratory Medicine Dartmouth-Hitchcock
Rare GI Malignancies
 Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
The pathology of neuroendocrine tumours of the gut
 The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The pathology of neuroendocrine tumours (NETs)
The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The pathology of neuroendocrine tumours (NETs)
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Case 3 - GYN. History: 66 year old, routine Pap test. Dr. Stelow
 Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Ascitic Fluid and Use of Immunocytochemistry. Mercè Jordà, University of Miami
 Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
3/22/2017. Disclosure of Relevant Financial Relationships. Disclosure of Relevant Financial Relationships. Grading G1. Grading. Ki67 index V.
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
A218 : Esophagus cancer tissues. (formalin fixed)
") (formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
(formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Overview. Disclosure. PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes. N. Volkan Adsay, MD
 PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes N. Volkan Adsay, MD Professor and Vice-Chair Director of Anatomic Pathology Emory University and Emory Winship Cancer Institute Atlanta,
PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes N. Volkan Adsay, MD Professor and Vice-Chair Director of Anatomic Pathology Emory University and Emory Winship Cancer Institute Atlanta,
3/22/2017. Disclosure of Relevant Financial Relationships. Ki-67 in Pancreatic Neuroendocrine Neoplasms According to WHO 2017.
 Disclosure of Relevant Financial Relationships Ki-67 in Pancreatic Neuroendocrine Neoplasms According to WHO 2017. USCAP requires that all planners (Education Committee) in a position to influence or control
Disclosure of Relevant Financial Relationships Ki-67 in Pancreatic Neuroendocrine Neoplasms According to WHO 2017. USCAP requires that all planners (Education Committee) in a position to influence or control
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis.
 Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Liver Specialty Evening Conference. Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle
 Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD
 CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications. Andres A. Roma, MD Cleveland Clinic
 Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Case #1 FNA of nodule in left lobe of thyroid in 67 y.o. woman
 Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Disclosures 5/27/2012. Outline of Talk. Outline of Talk. When Is LCIS Clinically Significant? Classic LCIS. Classic LCIS
 When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation