Management Algorithms for Primary and Metastatic Liver Cancer
|
|
|
- Charles Tate
- 5 years ago
- Views:
Transcription

1 Management Algorithms for Primary and Metastatic Liver Cancer Chief, Division of Surgical Oncology Head Hepatobiliary & Pancreatic Surgery City of Hope Comprehensive Cancer Center
")
2 Cancer statistics, 2018, Volume: 68, Issue: 1, Pages: 7-30, First published: 04 January 2018, DOI: ( /caac.21442)



3 Less than 10% of HCC arises in normal liver More than 80% of HCC is associated with liver cirrhosis from Hepatitis B and C 90% 10% Other risk factors: Hemochromatosis, Alcoholic liver disease, Tyrosinosis, Aflatoxin (Africa), Vinyl Polymer, NASH HCC is present in 20-40% of patients with cirrhosis and HBV and HCV at autopsy

4 Ascites Umbilical Hernia Hematemesis Melena / Bleeding per rectum Muscle Wasting Hypoalbuminemia Encephalopathy


5 Most patients with HCC die from liver failure (15-20% Mortality) HCC is multicentric in >80% of patients with cirrhosis


6 Primary Tumor TX Primary tumor cannot be assessed T0 No evidence of primary tumor T1 Solitary tumor 2 cm or less in greatest dimension without vascular invasion T2 Solitary tumor 2 cm or less in greatest dimension with vascular invasion, or Multiple tumors limited to one lobe, none more than 2 cm in greatest dimension, without vascular invasion, or A solitary tumor more than 2 cm in greatest dimension without vascular invasion T3 Solitary tumor more than 2 cm in greatest dimension with vascular invasion, or Multiple tumors limited to one lobe, none more than 2 cm in greatest dimension, with vascular invasion, or Multiple tumors limited to one lobe, any more than 2 cm in greatest dimension, with or without vascular invasion T4 Multiple tumors in more than one lobe, or tumor involves a major branch of portal or hepatic veins Lymph Node Involvement NX Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Regional lymph node metastasis Distant Metastasis MX Presence of distant metastasis cannot be assessed M0 No distant metastasis M1 Distant metastasis STAGE GROUPING Stage I T1, N0, M0 Stage II T2, N0, M0 Stage III T1, N1, M0 T2, N1, M0 T3, N0, M0 T3, N0, M0 Stage IVA T4, any N, M0 Stage IVB Any T, any N, M1

7 CHILDS Classification Ascites None Easily controlled Poorly controlled Albumin > <3.0 Bilirubin < >3.0 Encephalopathy None Mild Advanced Nutritional Status Excellent Good Poor Modified CHILD-PUGH Classification Ascites None Controlled medically Poorly controlled Albumin > <2.8 Bilirubin < >3.0 Encephalopathy None Controlled medically Poorly controlled INR < >2.25 Childs A: 5-7 pnts Childs B: 8-10 points Childs C: points
8 MILAN CRITERIA 1 UCSF CRITERIA 2 Solitary lesion 5 cm or 3 lesions none > 3 cm Solitary lesion 6.5 cm or 3 lesions none > 4.5 cm and total tumor diameter 8 cm MELD Score R = (0.957 X log e (creatinine mg/dl) X log e [total bilirubin mg/dl] X log e [INR] ) X 10 (1) Mazzaferro et. al. N Engl J Med 1996; 334: (2) Yao et.al. Hepatology 2001;33:
9 Metabolic 4% Fulminant 6% PSC 11% Other 2% Hep C 24% PBC 12% Hep B 7% Cryptogenic 13% Alcohol 21%
10


11 1967


12


13






14 1981: Didier Houssin & Henri Bismuth- First Reduced Size Liver Graft 1987: Rudolf Pichlmayer- First Split Liver Transplantation Gridelli, B. (2013). Nat. Rev. Gastroenterol. Hepatol. doi: /nrgastro




15 Living Donor Liver- Dissection & Transection Truly a pleasure


16 Duct- Duct Roux-en-Y



17

18 Colon & Rectal Cancer 140, 000 New Cases 20-30% Synchronous Liver Mets 70-80% No Liver Mets 25% Liver Mets Untreated <1% Alive 5 yrs Resected 60% Alive 5 yr
19

20
21


22 Greek Mythology- Prometheus Prometheus had stolen fire from Zeus and given it to the mortals in their dark caves. He had Hepheistos shackle Prometheus to the side of a crag, high in the Caucasus mountains. Each day, Prometheus would be tormented by Zeus eagle as it tore at his immortal flesh and tried to devour his liver. Each night, as the frost bit it s way into his sleep, the torn flesh would mend so the eagle could begin anew at the first touch of Dawn.


23 Challenges of Liver Surgery Anatomical Challenges No Bloodless plane exists It s deceptive surface anatomy leads into rather than away from the its largest vessels Complex inflow and outflow tracts cross at right angles Metabolic- Post Chemo Histologic Simplicity belies its Metabolic Complexity It has been one of the last organs to yield to the rapid surgical advances made in the 19 th century

24 Claude Couinaud working with his collection of liver casts

25 RP RA 7m





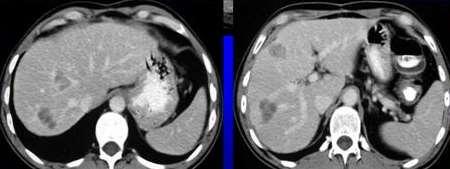
26 CT Scan is always Good- BUT Nothing like a great MRI with EOVIST PET is meaningless for Anatomic Imaging- Great for Extrahepatic Disease




27 Intra-op Ultrasonography detects 25-35% more lesions than CT, MRI and Transabdominal US Now the Standard of Care- However MRI Better
28 1. Surgery 2. Chemotherapy 3. Microwave Ablation/ Radiofrequency Ablation 4. Irreversible Electroporation (NanoKnife) 5. Hepatic Artery Infusion Pump 6. Radiation/ Radioembolization (SIRT) 7. Cryotherapy 8. Ethanol Injection 9. Transplant 10. Gene Therapy


29
 Ionic agitation causes")

 Percutaneous, Laparoscopic, or Open Approach Microwaves")

30 RF ablation- alternating electric current in the radio-frequency range ( khz) Ionic agitation causes frictional heat, thermal injury Spherical Ablation Area up to 7cm Temperatures raised above 90 C (well above the C necessary to destroy tissue.) Percutaneous, Laparoscopic, or Open Approach Microwaves to induce an ultra-high-speed (2450 MHz) alternating electric field Rotation of water molecules Thermal coagulation of tissue Excellent role for mets < 3 cm
 is a way to increase cell")


31 Reversible Electroporation Irreversible Electroporation Irreversible electroporation (IRE) is a way to increase cell membrane permeability by subjecting it to an electrical field that leads to cell death in soft tissue lesions. It does this by opening permanent, nano-sized pores in the membranes of the lesion s cells. This irreversible damage causes natural cell death.


32 Post-chemo liver is SICK Different Beast Friable Oozy Steatotic Steatohepatitis Sinusoidal Obstruction
33 Schoellhammer HF, Singh G, Leong L. J Natl Compr Canc Netw Sep;11 Suppl 4:S3-8. PMID:
34 Guye ML, Schoellhammer HF, Chiu LW, Kim J, Lai L, Singh G. In J Surg Oncol Dec; 4(4):

35

:437-41. doi: 10.1016/j.ijsu.2014.03.009.")
36 ALPPS- Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy 40%-80% within 6-9 days ALPPS- Hypertropy of FLR 8%-27% within 2-60 days PVL/PVE- Hypertropy of FLR 9 Days Later Operative morbidity 16%-64% Mortality 12%-23% Int J Surg. 2014;12(5): doi: /j.ijsu Epub2014 Apr 2.

37 Feb 21 st 2012


38 SS Feb 21 st 2012
39 NCCN Recommendations (2017 Condensed) First Line Second Line 3 rd or 4 th Line 4 th or 5 th Line FOLFOX or FOLFIRI + anti-egfr Alternate chemo +/-anti-angiogenic TAS-102 or Regorafenib RAS-WT Left Colon Treat like 1 st Line RAS-MT Chemo +antiangiogenic FOLFIRI or Irinotecan + Anti- EGFR FOLFIRI or irinotecan + anti- EGFR or ant-egfr TAS-102 or regorafenib TAS-102 or regorafenib MCRC FOLFOX or FOLFIRI or XELOX+/- BEV Alternate chemo +/- antiangiogenics TAS-102 or regorafenib RAS-MT or Right colon with RAS- WT FOLFOXIRI +/- BEV CAP+/- BEV TAS-102 or regorafenib FOLFOX or CAPOX or FOLFIR +/-antiangiogenic Right colon: consider anti- EGFR only 2 nd line and beyond Alternate Chemo TAS-102 or Regorafenib 5-FU +/- BEV FOLFOX or CAPOX or FOLFIRI +/- antiangiogenic Alternate Chemo TAS-102 or regorafenib For MSI-H patients consider pembrolizumab or nivolumab for second line and beyond or 1 st line poor PS



40 Apr 13 th 2012
 B: Wedge Resection of Seg 4B/ 5")


41 SS June 28 th 2012 C A B Surgery : discharged POD 8 Right Hemicolectomy A: Right Posterior Sectionectomy (Seg 6 & 7) B: Wedge Resection of Seg 4B/ 5 lesion..sitting right on the portal vein. So basically enucleated..no attempt at getting margins C: Wedge Resection of lesions in Seg 2 and 4A. No attempt at getting margins.as this was sitting on the bifurcation of the left hepatic vein. Bed Nanoknifed (Irreversible Electroporation). Grossly all tumor removed.


42 SS Mar 19 th 2018 Schoellhammer HF,., Gagandeep S. BMC Cancer 2015, 15:271.



43 Surgery Chemotherapy Resectable 10% Unresectable 90% 5yr Survival: >60% 5yr Survival: 1-2% 2 Worlds ignoring each other
44
45 Anti-Angiogenesis Ramucirumab Regorafenib Aflibercept Anti-EGFR Bevacizumab Panitumumab 2004 Cetuximab TAS-102 Cytotoxics Oxaliplatin Capecitabine 1996 Irinotecan 1960 s 5-Fluorouracil
46


47 Stump of Right Hepatic Vein IVC Stump of Rt. Portal Vein




48



49


50 Dec 13 th, 2006


51



52



53

54 Johns Hopkins Europe John Hopkins: Annals of Surgery. 235(6):759-66
55 Margins are an indicator and NOT a governor of prognosis N= 557 Univariate Analysis 49.6 m Scheele J et al. Surg Onc Clin N Amer; 2003; 12: Pawlik et al. Annals of Surgery: 241: , 2005
56 Japanese Experience Hepatic LN+ does NOT matter- Resect Celiac LN + Maybe/ Maybe Not > 4 LN+ the Survival adv is lost CEA levels matter SIZE does NOT matter (3 or >6cm) Wedge Res = Anatomic Resections Adjuvant Chemo is a must HAI does NOT offer any advantage John Hopkins: Annals of Surgery. 235(6):759-66, 2002 Japanese Multicenter Study: Dis Col & Rec: 46: S22-31, 2003

57 HAI Better response rate for multiple colorectal liver mets



58 HAI = Systemic Chemo ( ) Results showed no evidence of an advantage in progression-free survival or overall survival for the IHA group; Thus continued use of this regimen cannot be recommended outside of a clinical trial Volume 361, Issue 9355, 1 February 2003, Pages
59 Survival data available for 344 patients (98.6%) Liver Resection Synchronous with Hepatic Arterial Infusion Pump (HAIP) for Colorectal Cancer Liver Metastases: Results alone or with Liver Resection. I. Konstantinidis..G. Singh. Regional Cancer Therapies Meeting.2/2017.


60


61
62 Resection Plans for Laparoscopic Resections





63 Meet the Parents Mr. & Mrs. Robot da Vinci Si da Vinci Xi
64 Perfect Cases for the Robot
65 Is Robotics/ MIS the future of Surgery? YES Are we there today? NO Does that mean we stop trying? NO
66 RESECTABLE YES NO Surgery Can it be MADE resectable? Chemo Palliative Resection + MWA Chemotherapy and reassessment Portal Vein Embolization SIRT Staged Hepatectomy HAIP

67 What is Removed BUT What is Left Behind Key surgical question is no longer WHO IS RESECTABLE but rather WHO IS NOT RESECTABLE Future Liver Remnant of 20% (30%) Adequate Inflow and Outflow At least 2 Contiguous Segments Capability of Resecting all visible Dz RFA/ MWA to Compliment or as an Adjunct Nanoknife to Compliment or as an Adjunct ONLY absolute CONTRAINDICATION to surgery for CRLM is the presence of NON-TREATABLE DISEASE ELSEWHERE

68 The Future- is Still Multi-Modality Surgery X Research Radiology RTh X X CTh TEAM SPORT Gene Th X X Imm Th Surgeon Medical Oncologist Radiation Oncologist Gastroenterologist Radiologist Oncology Nurse Specialist Stoma Nurse Social Worker Nutritionist gsingh@coh.org Cell: (310)

69
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
LiverGroup.org. Case Report Form (CRF) for STAGED procedures
 for STAGED procedures") Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Surgical management of HCC. Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London
 Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers
 Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases
 Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Trattamento chirurgico delle lesioni epatiche secondarie difficili. Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica
 Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
How to integrate surgery in the treatment of patients with liver-only metastatic disease
 How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Colorectal Liver Metastases Metachronous
 Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Liver Tumors. Patient Education. Treatment options 8 4A. About the Liver. Surgical Specialties
 Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age. Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010
 Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Disclosure. Nothing to Disclose Will not be discussing off label use of any of the medications
 Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Management of Stage IV Colorectal Cancer: Expanding the Horizon
 Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER
 OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE METASTASES
 LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Management of HepatoCellular Carcinoma
 9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Risk factors for cancer recurrence or death within 6 months after liver resection in patients with colorectal cancer liver metastasis
 ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Liver metastases: treatment planning. PJ Valette
 Liver metastases: treatment planning PJ Valette Liver metastases removal December 2010 April 2011 : after chemotherapy June 2011 : after resection of left lobe mets & portal embol. Sept 2011 : 1 year after
Liver metastases: treatment planning PJ Valette Liver metastases removal December 2010 April 2011 : after chemotherapy June 2011 : after resection of left lobe mets & portal embol. Sept 2011 : 1 year after
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
COME HOME Innovative Oncology Business Solutions, Inc.
 COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD
 UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
The Surgical Management of Colorectal Metastases
 11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
The ESMO consensus conference on metastatic colorectal cancer
 ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto
 Milano 05.10.2018 Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto Salvatore Corallo U.O.C. Oncologia Medica IRCCS Istituto Nazionale dei Tumori Milano CRC in elderly patients
Milano 05.10.2018 Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto Salvatore Corallo U.O.C. Oncologia Medica IRCCS Istituto Nazionale dei Tumori Milano CRC in elderly patients
Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma
 Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness
Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness
GASTROINTESTINAL MALIGNANCIES
 Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA. Shawn Pelletier, MD
 TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HCA
 UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA DISCLOSURE I have no financial relationship(s) relevant to the
UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA DISCLOSURE I have no financial relationship(s) relevant to the
Ghosts in the Machine: Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand
 Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Cholangiocarcinoma. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Advances in percutaneous ablation for hepatocellular carcinoma
 Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Liver transplantation: Hepatocellular carcinoma
 Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
A Brief Overview of Screening and Management of Colorectal Cancer
 A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
NCCN Guidelines for Hepatobiliary Cancers V Web teleconference on 10/24/17
 Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Introduction. Case Report
 Case Report A patient who showed a pathologically complete response after undergoing treatment with XELOX plus bevacizumab for synchronous liver metastasis of grade H2 from sigmoid colon cancer Yasuhito
Case Report A patient who showed a pathologically complete response after undergoing treatment with XELOX plus bevacizumab for synchronous liver metastasis of grade H2 from sigmoid colon cancer Yasuhito
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
COLORECTAL CANCER 44
 COLORECTAL CANCER 44 Colorectal Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by Stuart M. Lichtman, MD Memorial Sloan-Kettering Cancer Center Commack,
COLORECTAL CANCER 44 Colorectal Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by Stuart M. Lichtman, MD Memorial Sloan-Kettering Cancer Center Commack,
Hepatocellular Carcinoma: Transplantation, Resection or Ablation?
 Hepatocellular Carcinoma: Transplantation, Resection or Ablation? Roberto Gedaly MD Chief, Abdominal Transplantation Transplant Service Line University of Kentucky Nothing to disclose Disclosure Objective
Hepatocellular Carcinoma: Transplantation, Resection or Ablation? Roberto Gedaly MD Chief, Abdominal Transplantation Transplant Service Line University of Kentucky Nothing to disclose Disclosure Objective
LIVER SURGERY 2. Case 1. Med 5 Refresher Course (Surgery) 2013/14. Dr Sunny Cheung
 2013/14. Dr Sunny Cheung") LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
Liver surgery, acute GI tract bleeding
 Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Current Treatment Strategies for Hilar and Intrahepatic Cholangiocarcinoma
 Current Treatment Strategies for Hilar and Intrahepatic Cholangiocarcinoma Jean-Nicolas Vauthey, MD, FACS Professor of Surgery Chief Hepato-Pancreato-Biliary Section Department of Surgical Oncology Crescent
Current Treatment Strategies for Hilar and Intrahepatic Cholangiocarcinoma Jean-Nicolas Vauthey, MD, FACS Professor of Surgery Chief Hepato-Pancreato-Biliary Section Department of Surgical Oncology Crescent
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS?
 IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy
 Original Article Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy Rebecca C. Auer, MD 1 ; Rebekah R. White, MD 2 ; Nancy E. Kemeny, MD
Original Article Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy Rebecca C. Auer, MD 1 ; Rebekah R. White, MD 2 ; Nancy E. Kemeny, MD
INTERACTIVE SESSION 2
 INTERACTIVE SESSION 2 2 patients with lung metastases, with complete response after oncologic treatment - Clinical Case Presentation: Dr. Esther Casado Dr. Sergi Call - Expert Opinion: Dr. Raúl Embún Dr.
INTERACTIVE SESSION 2 2 patients with lung metastases, with complete response after oncologic treatment - Clinical Case Presentation: Dr. Esther Casado Dr. Sergi Call - Expert Opinion: Dr. Raúl Embún Dr.
Diagnosed with Metastatic Colorectal Cancer?
 ESSENTIALS Metastatic Colorectal Cancer Diagnosed with Metastatic Colorectal Cancer? It can be frightening to learn you or a loved one has been diagnosed with metastatic colorectal cancer. It is important
ESSENTIALS Metastatic Colorectal Cancer Diagnosed with Metastatic Colorectal Cancer? It can be frightening to learn you or a loved one has been diagnosed with metastatic colorectal cancer. It is important
Embolotherapy for Cholangiocarcinoma: 2016 Update
 Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Aintree University Hospital
 Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
Hepatocellular Carcinoma (HCC)
") Title Slide Hepatocellular Carcinoma (HCC) Professor Muhammad Umar MBBS, MCPS, FCPS (PAK), FACG (USA), FRCP (L), FRCP (G), ASGE-M(USA), AGAF (USA) Chair & Professor of Medicine Rawalpindi Medical College
Title Slide Hepatocellular Carcinoma (HCC) Professor Muhammad Umar MBBS, MCPS, FCPS (PAK), FACG (USA), FRCP (L), FRCP (G), ASGE-M(USA), AGAF (USA) Chair & Professor of Medicine Rawalpindi Medical College
Liver Directed Therapy for Hepatocellular Carcinoma
 Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
New Energy Sources for Local Ablation Therapy. Jeong Kyong Lee, MD Ewha Womans University
 New Energy Sources for Local Ablation Therapy Jeong Kyong Lee, MD Ewha Womans University New Energy Sources for Local Ablation Therapy Microwave Ablation Irreversible Electroporation Cryoablation Microwave
New Energy Sources for Local Ablation Therapy Jeong Kyong Lee, MD Ewha Womans University New Energy Sources for Local Ablation Therapy Microwave Ablation Irreversible Electroporation Cryoablation Microwave
Colorectal Cancer Therapy and Associated Toxicity
 Colorectal Cancer Therapy and Associated Toxicity Mountain States Cancer Conference November 6, 2010 Colin D. Weekes, M.D., Ph.D Assistant Professor University of Colorado GI Cancers Are Common 2009 Estimated
Colorectal Cancer Therapy and Associated Toxicity Mountain States Cancer Conference November 6, 2010 Colin D. Weekes, M.D., Ph.D Assistant Professor University of Colorado GI Cancers Are Common 2009 Estimated
2/20/14& Medical Management of Colon and Rectal Cancer: An Overview. Outline / Learning Objectives. How common is colon cancer?
 Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Colorectal liver metastases: making the unresectable resectable using irreversible electroporation for microscopic positive margins acasereport
 Schoellhammer et al. BMC Cancer (2015) 15:271 DOI 10.1186/s12885-015-1279-9 CASE REPORT Open Access Colorectal liver metastases: making the unresectable resectable using irreversible electroporation for
Schoellhammer et al. BMC Cancer (2015) 15:271 DOI 10.1186/s12885-015-1279-9 CASE REPORT Open Access Colorectal liver metastases: making the unresectable resectable using irreversible electroporation for
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Colorectal Cancer at the MemorialCare Todd Cancer Institute at Long Beach Memorial
 Colorectal Cancer at the MemorialCare Todd Cancer Institute at Long Beach Memorial ANNUAL REPOR T (562) 933-0900 MemorialCare.org/TCI 2810 Long Beach Blvd. Long Beach, CA 90806 #3 Colorectal cancer is
Colorectal Cancer at the MemorialCare Todd Cancer Institute at Long Beach Memorial ANNUAL REPOR T (562) 933-0900 MemorialCare.org/TCI 2810 Long Beach Blvd. Long Beach, CA 90806 #3 Colorectal cancer is
Behandeling van colorectale levermetastasen. Rol van beeldvorming van de lever bij colorectaal carcinoom
 Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
Parenchyma saving resectionsfictions. (Colorectal liver metastasis)
") Parenchyma saving resectionsfictions or facts? (Colorectal liver metastasis) Bjørn Edwin, professor, MD, PhD Section manager, Clinical Research The Interventional Center and HPB-Department Oslo University
Parenchyma saving resectionsfictions or facts? (Colorectal liver metastasis) Bjørn Edwin, professor, MD, PhD Section manager, Clinical Research The Interventional Center and HPB-Department Oslo University
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting