Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ
|
|
|
- Marilynn Bond
- 5 years ago
- Views:
Transcription
1 Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ
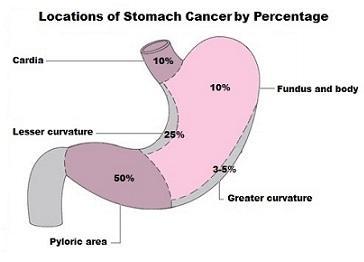
2 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology f. Staging g. Treatment of early/localised disease h. Treatment of metastatic disease 4. Oesophageal cancer
3 Division according to localisation of the primary tumor: Gastric Cancer Pancreatic Cancer Oesophageal Cancer Biliary Cancer* HCC*

4
5
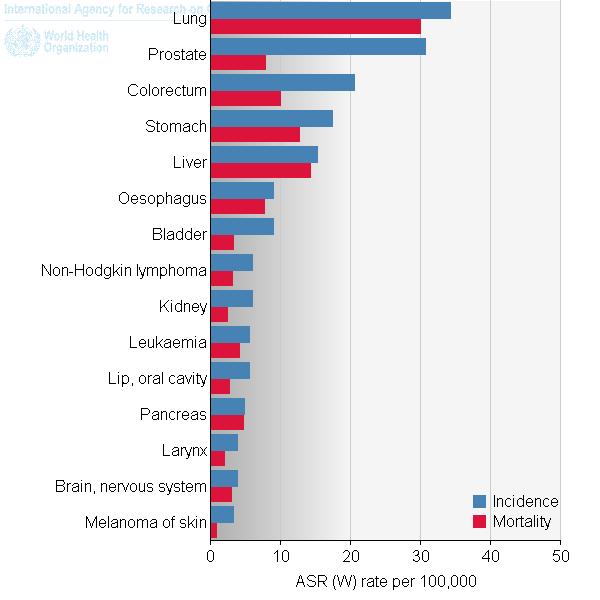
6 GASTRIC CANCER Decline in incidence (Western Europe, North America) 5-year survival rate 15% The most common upper GI cancer Inherited genetic predisposition 1-3% PANCREATIC CANCER Incidence is rising Mean age at onset - ca. 70 years 5-year SR when surgically resected 20% 5-year SR 5% in metastatic setting One of most fatal cancers for both sexes Only <10% due to inherited germline mutations

7 GASTRIC CANCER Helicobacter pylori infection Tobacco use Alcohol use High salt diet Processed meat Nitrozoamines Male gender Low fruit and vegetable intake PANCREATIC CANCER Cigarette smoking Obesity Chronic pancreatitis Alcohol consumption Red meat, saturated fat Processed food Helicobacter pylori, HBV High fruit&folate intake reduces the risk
8 GASTRIC CANCER PANCREATIC CANCER Syndromes predisposing: HDGC (hereditary diffuse gastric cancer) HNPCC FAP Peutz Jegher s syndrome Syndromes predisposing: Li-Fraumeni syndrome HNPCC BRCA2 mutation! Peutz-Jegher s syndrome
9
10

11
12

13
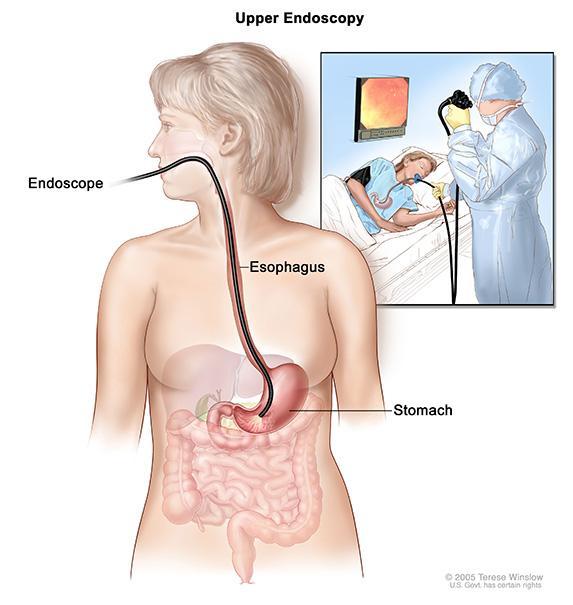
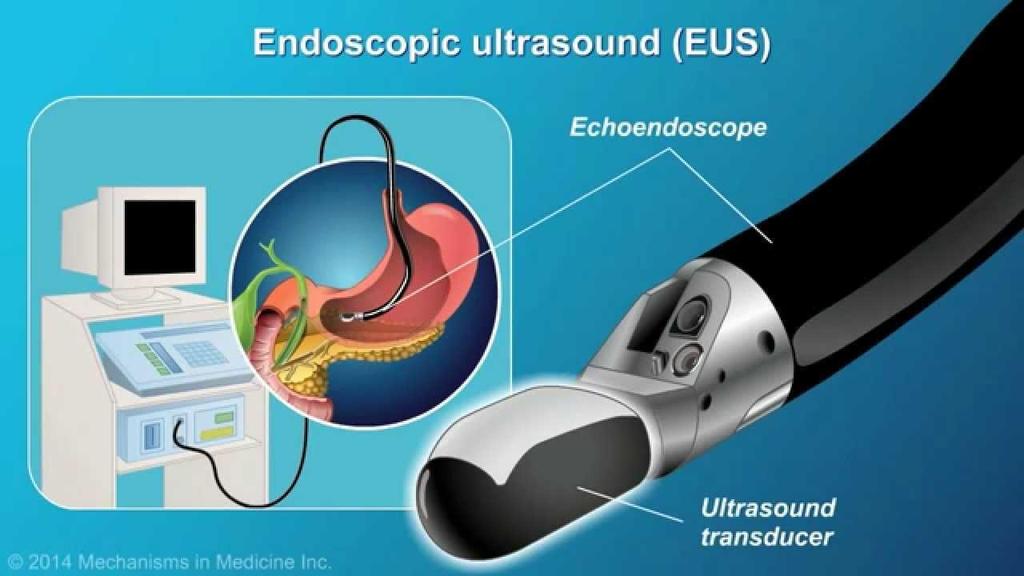
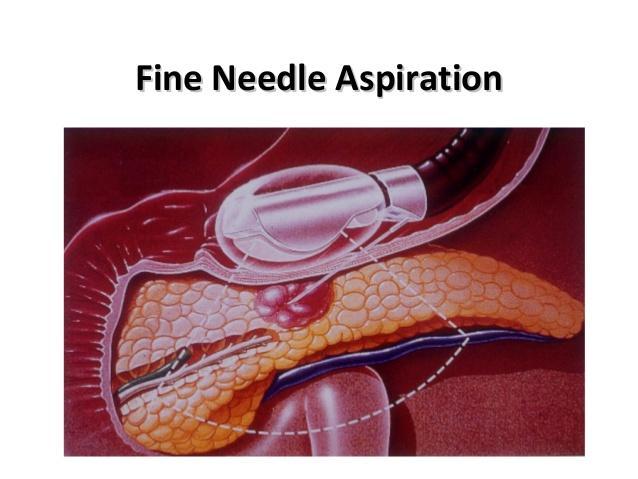
14 Histopathological examination by means of biopsy (primary tumor or metastases?) Stomach gastroscopy Pancreas depending on the staging (no biopsy -> resection/eus-guided biopsy/biopsy of metastases) Both types of cancer CT scan for staging EUS additional method (different indication in gastric & pancreatic cancer)* *remember both cancers are commonly diagnosed at already advanced stage (!)
15
16 Do we need EUS in advanced gastric or pancreatic cancer? Why/why not? If you have had a primary tumor located in pancreas and metastases in the liver, which one would you decide to take biopsy from? Or maybe both? Do we routinely use PET for staging of pancreatic or gasric cancer?
?")
17 Is MRI a better diagnostic method in gastric cancer? Is MRI a better diagnostic method in pancreatic cancer? Why do we perform EUS in gastric cancer (metastases excluded)? Why do we perform EUS in pancreatic cancer (metastases excluded)?
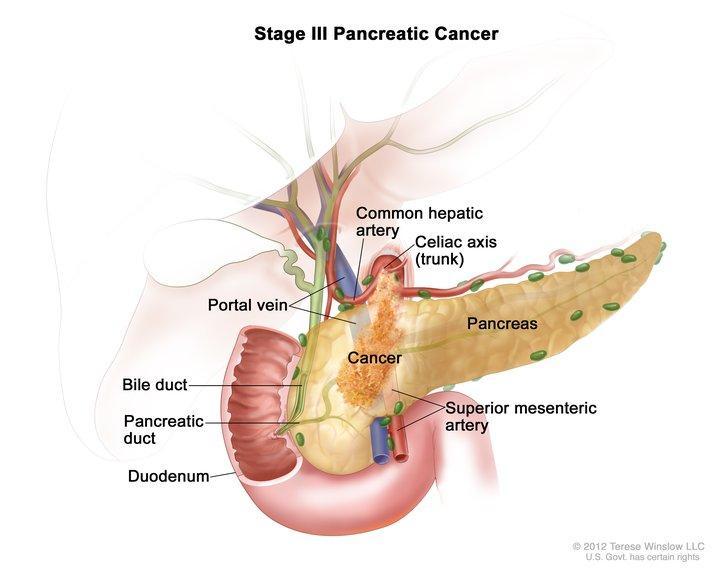
 or submucosal dissection (ESD) IN PANCREATIC CANCER Assessment of vascular invasion Prediction of resectability But limited value in detection of metastatic lymph")
18 IN GASTRIC CANCER Assessment of the T and N stage Determine proximal and distal extent of the tumor Decision regrding endoscopic resection (endoscopic mucosal resection (EMR) or submucosal dissection (ESD) IN PANCREATIC CANCER Assessment of vascular invasion Prediction of resectability But limited value in detection of metastatic lymph nodes
19
20
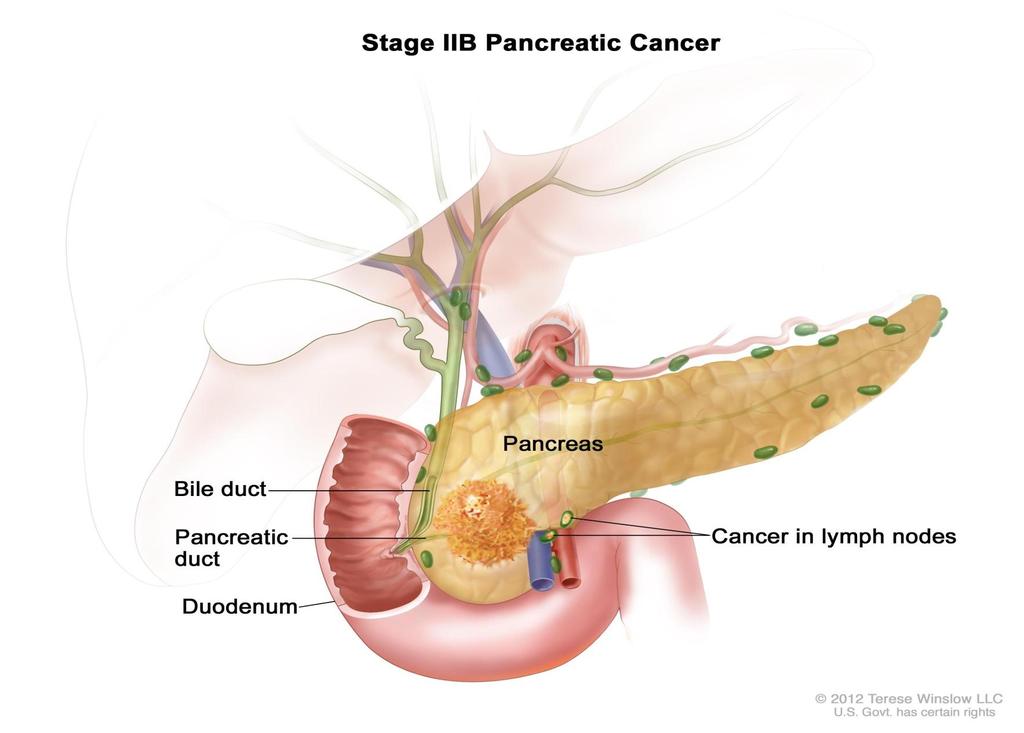
21 GASTRIC CANCER PANCREATIC CANCER 90% adenocarcinoma Other: GIST, NET, lymphomas, MANEC 95% adenocarcinoma (80-85% PDAC pancreatic ductal adenocarcinoma) Other acinar cell pc (better prognosis), undifferentiated/adenosqu amous carcinomas (worse) NET

22 Staging & Treatment
23
24
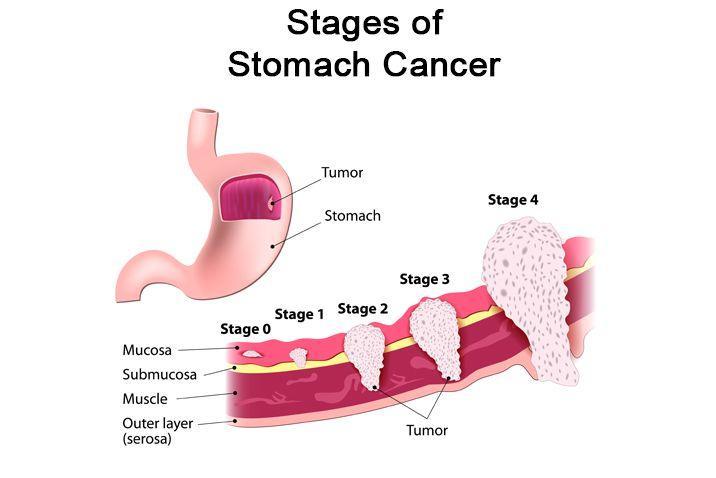
25 IA -> T1aN0 (confined to the mucosa, non-ulcerated, <2cm, well-diferentiated): ESD IA -> T1N0 (not for local treatment): sugery (gastrectomy + perigastric lymph nodes, D1+) IB-III (>=T2N0): perioperative chemotherapy + surgery (gastrectomy+ D2 lymphadenectomy) or surgery + adjuvant chemoradiotherapy IV: metastases -> pallaitive treatment: BSC or systemic chemotherapy (cth) Inoperable cases with no metastases cth or BSC
26 T stage! decision about neodajuvant treatment (-> back to EUS) M stage decision systemic chth, no surgery (-> back to CT : commonly liver, lymph nodes (not reginal lymph nodes!), adjacent structures CT -> low sensivity to detect peritoneal spread (very common in gastric cancer) -> consider laparoscopy in T3/4 stage
27 Systemic treatment -> chemotherapy Doublet or triplet chemoterapy > better than monoterapy Mainly fluoropirymidines/platinum agents/anthracyclines Palliation of symptoms -> radiotherapy (primary tumor, bone metastases)! Remember to assess HER2 overexpression! When HER2 positive gastric cancer -> add trastuzumab to chemotherapy (TRA+CX)
28 Do we resect the primary tumor when metastases are already present? Does it influcence overall survival?

29 Staging & Treatment
30
31
32
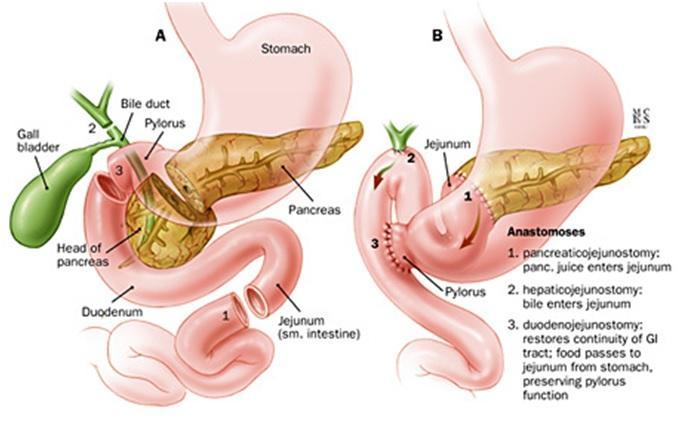
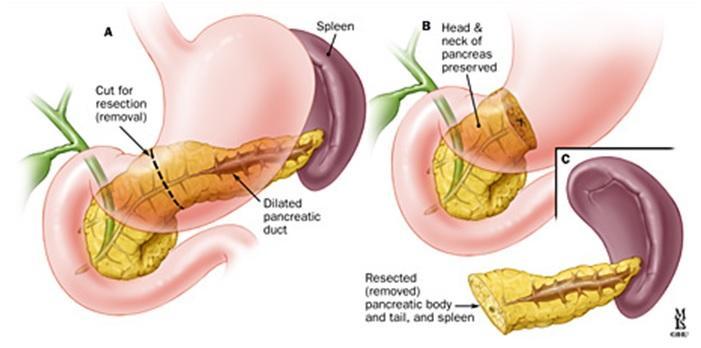
33 What s the standard of care for pancreatic cancer? a. Open surgery b. Laparoscopy c. Both
34 What determines the type of surgery in pancreatic cancer?
35 Pancreatic cancer surgery involves lymphadenectomy Standard lymphadenectomy include removal of 15 or more lymphnodes but AJCC recommended 10 LN, 8th edition of TNM says 12 lymph nodes
36 CONKO-001 gemcytabine better than observation Improves DFS ( 6 mth) and OS ( 2,5 mth) ESPAC-3 trial -> GEM vs fluorouracil No difference in OS FU more toxic, mainly mucositis ESPAC-4 trial -> GEM+cabecitabine> GEM 5 yr OS 29% vs 16% LANCET 2017 mos 2,5 mth
37
38 CT scan for localisation of metastases Patient genarall condition Performance status, nutritional status & comorbidities Biopsy to confirm diagnosis (histopathology!) Systemic chemotherapy FOLFIRINOX or GEM/Nab-PTX PS 0-1 Gemcytabine alone PS2, bilirubin 1.5xUNL
39 What will be the best choice for patient with metastatic pancreatic cnacer with performance status 3?
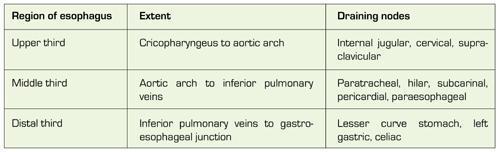
40 SCC Risk factors: smoking & alcohol consumption Incidence increases with age, peak 70 yo Men Women Incidence in stable Mortality declined Localistion: more often proximal or middle ADENOCARCINOMA Risk factors: obesity&gastrooesophageal reflux Age (increases with age) Men (4x)>Women Incidence is rising Mortality rates are rising Localisation: more often distal
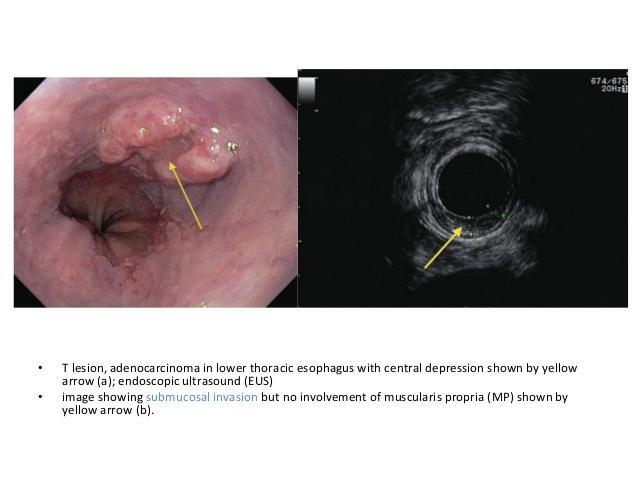
41 Dysphagia, Odynophagia! Especially associated with WEIGHT LOSS Emesis GI bleeding Recurrent Aspiration
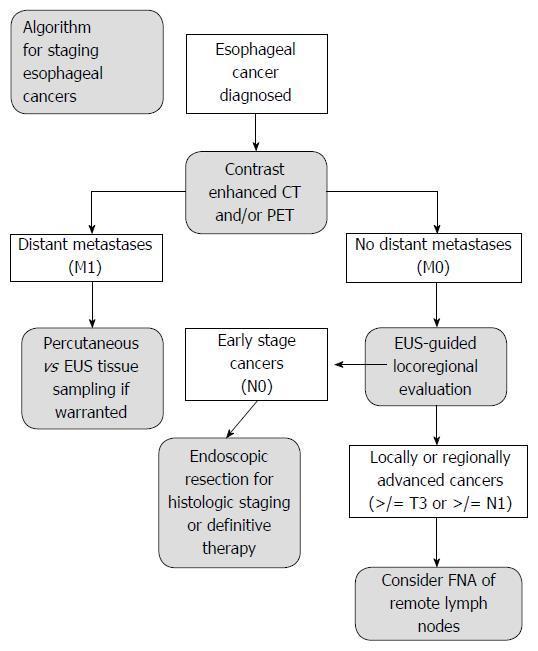
42 Endoscopy of upper GI Biopsy -> DIAGNOSIS Clinical examination CT neck, chest, abdomen -> STAGING EUS -> endoscopic ultrasound (very high sensitivity and specificity for T feature) -> T&N evaluation = determination of resectability PET/CT: candidates for oesophagectomy, to find undetected metastases
43
44
45 Tracheobronchoscopy To rule out invasion of respiratory tract Tumors at or above tracheal bifurcation Laparoscopy To exclude peritoneal involvement OGJ, T3/T4 Exploration for synchronous cancer SCC -> due to the shared risk factors with other cancers Mainly: HNC (ENT specialist), lung cancer (bronchoscopy)

46 Remember about nutritional status assessment and nutritional support from the very beginning and for the whole period of treatment
47
48
49 Endoscopic methods for T1a adenocarcinoma a) Endoscopic mucosal resection (EMR) b) Endoscopic submucosal dissection (ESR) For limited disease (T1-T2N0) -> SURGERY: a) Transthoracic oesophagectomy (Ivor-Lewis procedure) b) Or hybrid minimally invasive oesophagectomy (IL proc.+laproscopic gastric mobilisation&open right thoracotomy) -> lower complication rate
50 SCC ADENOCARCINOMA Preoperative treatment for both -> higher rate of R0 resection, better local control&survival Either A. Preoperative CRT + surgery Or B. Definitive CRT (slavage surgery an option) CRT without surgery is recommended fo cervically localised tumors Either A. Preoperative CRT+ surgery Or B. Perioperative chemotherapy (platinum/fluoropyrimidine) +surgery Always surgery!
51 Cisplatin/5-FU + RTH Gy (1.8-2 Gy/fr) Carboplatin AUC2 + paclitaxel 50 mg/m2, weekly, for 5 weeks + RTH 41.4 Gy/23fractions -> CROSS trial (T1N1, T2-T3N0-1 included)
52

53 Why do we go for PET after crth in radical treatment of oesophageal cancer? Why this diagnostic procedure? What if we observe CR after neoadjuvant treatment in radiological examinations? Is PET relevant for identification of CR?
54 Symptoms palliation: Ex. Brachytherapy for relief of dysphagia Metal stent placement Additional: HER2 testing in metastatic AC of oesophagus (esp. lower/ogj) Systemic treatment: AC: treatment according to gastric cancer guidelines (no strong evidence) SCC: cth value uncertain, cisplatin/5fu, cisplatin doubltes RR, no OS benefit; results worse than for AC

55
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
NICE guideline Published: 24 January 2018 nice.org.uk/guidance/ng83
 Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
B Breast cancer, managing risk of lobular, in hereditary diffuse gastric cancer, 51
 Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Protocol for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER
 Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER Patient information given at each stage following agreed information pathway
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER Patient information given at each stage following agreed information pathway
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Pancreatic Adenocarcinoma
 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
GASTROINTESTINAL MALIGNANCIES
 Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
CASE DISCUSSION ON GASTRIC CANCER BASED ON ESMO GUIDELINES
 ESMO Preceptorship GI Tumours Singapore 20-22 nd October CASE DISCUSSION ON GASTRIC CANCER BASED ON ESMO GUIDELINES Professor. J-Y. Douillard MD PhD ESMO Chief Medical Officer CLINICAL PRACTICE GUIDELINES
ESMO Preceptorship GI Tumours Singapore 20-22 nd October CASE DISCUSSION ON GASTRIC CANCER BASED ON ESMO GUIDELINES Professor. J-Y. Douillard MD PhD ESMO Chief Medical Officer CLINICAL PRACTICE GUIDELINES
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Overview. What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013
 What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
The incidence of pancreatic cancer is rising in India and is higher in the urban male population in the western and northern parts of India.
 Published on: 9 Jun 2015 Pancreatic Cancer What Is Cancer? The body is made up of cells, which grow and die in a controlled way. Sometimes, cells keep on growing without control, causing an abnormal growth
Published on: 9 Jun 2015 Pancreatic Cancer What Is Cancer? The body is made up of cells, which grow and die in a controlled way. Sometimes, cells keep on growing without control, causing an abnormal growth
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
Approaches to Surgical Treatment of Gastric Cancer. Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service
 Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Oesophagogastric Cancer The Patient s Pathway
 National helpline: 0121 704 9860 V1 Oesophagogastric Cancer The Patient s Pathway {Based on The St Thomas Hospital Pathway} Registered Charity No. 1062461 Contents Introduction 3-5 Curative pathway 5-7
National helpline: 0121 704 9860 V1 Oesophagogastric Cancer The Patient s Pathway {Based on The St Thomas Hospital Pathway} Registered Charity No. 1062461 Contents Introduction 3-5 Curative pathway 5-7
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
GUIDELINE NUMBER: 87. Management of oesophageal and gastric cancer. DATE ISSUED: June 2006 CLINICAL SERVICES INVOLVED: Upper GI
 GUIELINE NUMER: 87 GUIELINE TITLE: Management of oesophageal and gastric cancer ATE ISSUE: June 2006 LINIAL SERVIES INVOLVE: Upper GI Levels of Evidence 1++ High quality meta-analyses, systematic reviews
GUIELINE NUMER: 87 GUIELINE TITLE: Management of oesophageal and gastric cancer ATE ISSUE: June 2006 LINIAL SERVIES INVOLVE: Upper GI Levels of Evidence 1++ High quality meta-analyses, systematic reviews
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
GASTRIC CANCER. Joyce Au SUNY Downstate Grand Rounds July 11, 2013
 GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
GI Tumor Board 3/8/2018. Case #1 IDEA. Case #1 Question #1 What is the next step in management?
 GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
Endometrial Cancer. Incidence. Types 3/25/2019
 Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Ines Buccimazza 16 TH UP CONTROVERSIES AND PROBLEMS IN SURGERY SYMPOSIUM
 BILATERAL MASTECTOMY IS NOT ROUTINELY JUSTIFIED IN PATIENTS WITH BILATERAL AXILLARY LYMPHADENOPATHY AND ONLY ONE DETECTABLE PRIMARY BREAST CANCER LESION SURGERY SYMPOSIUM Ines Buccimazza Breast Unit Department
BILATERAL MASTECTOMY IS NOT ROUTINELY JUSTIFIED IN PATIENTS WITH BILATERAL AXILLARY LYMPHADENOPATHY AND ONLY ONE DETECTABLE PRIMARY BREAST CANCER LESION SURGERY SYMPOSIUM Ines Buccimazza Breast Unit Department
LUNG CANCER. Agnieszka Słowik, MD. Department of Oncology, University Hospital in Cracow Jagiellonian University
 LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
Esophageal and GEJ Cancers. Case Presentations
 Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
Gastric (Stomach) Cancer
 Cancer") Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
Gastric Cancer: Surgery and Regional Therapy. Epidemiology. Risk factors
 Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Pancreatic Cancer: Medical Therapeutic Approaches
 Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
Lung cancer Surgery. 17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY March, 2017 Berlin, Germany
 17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY 24-29 March, 2017 Berlin, Germany Lung cancer Surgery Sven Hillinger MD, Thoracic Surgery, University Hospital Zurich Case 1 59 y, female, 40 py, incidental
17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY 24-29 March, 2017 Berlin, Germany Lung cancer Surgery Sven Hillinger MD, Thoracic Surgery, University Hospital Zurich Case 1 59 y, female, 40 py, incidental
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Gastric Cancer. Introduction
 Gastric Cancer Introduction Despite advances in surgery and the use of multimodality therapy, survival outcomes remain poor for gastric cancer patients. There is an urgent need for more effective therapies
Gastric Cancer Introduction Despite advances in surgery and the use of multimodality therapy, survival outcomes remain poor for gastric cancer patients. There is an urgent need for more effective therapies
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Surveillance of Individuals At High Risk For Developing Pancreatic Cancer
 Surveillance of Individuals At High Risk For Developing Pancreatic Cancer Marco Bruno Erasmus Medical Center, Rotterdam Pancreatic Cancer Facts & figures One of the most fatal malignancies Overall 5-year
Surveillance of Individuals At High Risk For Developing Pancreatic Cancer Marco Bruno Erasmus Medical Center, Rotterdam Pancreatic Cancer Facts & figures One of the most fatal malignancies Overall 5-year
Gastric adenocarcinoma Bern
 Gastric adenocarcinoma 18.10.2017 Bern Epidemiology Worldwide 5th cancer with 950 000 new cases per year, 161 000 in Europe, 683 in Switzerland 3 rd cause of mortality worldwide, 485 cases/year in Switzerland
Gastric adenocarcinoma 18.10.2017 Bern Epidemiology Worldwide 5th cancer with 950 000 new cases per year, 161 000 in Europe, 683 in Switzerland 3 rd cause of mortality worldwide, 485 cases/year in Switzerland
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
RECENT ADVANCES IN PACREATIC NEOPLASMS. DrTK Marumo GIT/HPB Surgeon Charlotte Maxeke JohannesburgAcademic Hospital
 RECENT ADVANCES IN PACREATIC NEOPLASMS DrTK Marumo GIT/HPB Surgeon Charlotte Maxeke JohannesburgAcademic Hospital CONTENT: GENETICS EARLY DIAGNOSIS CHEMOTHERAPY NEOADJUVANT ADJUVANT PRIMARY PALLIATIVE
RECENT ADVANCES IN PACREATIC NEOPLASMS DrTK Marumo GIT/HPB Surgeon Charlotte Maxeke JohannesburgAcademic Hospital CONTENT: GENETICS EARLY DIAGNOSIS CHEMOTHERAPY NEOADJUVANT ADJUVANT PRIMARY PALLIATIVE
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
This page explains some of the medical words that you may hear when you are finding out about pancreatic cancer and how it is treated.
 A-Z of medical words This page explains some of the medical words that you may hear when you are finding out about pancreatic cancer and how it is treated. Absorption: once your food has been broken down,
A-Z of medical words This page explains some of the medical words that you may hear when you are finding out about pancreatic cancer and how it is treated. Absorption: once your food has been broken down,
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
When to Refer for OGD and the Work Up of Upper GI Malignancies
 When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Determining Resectability and Appropriate Surgery for Esophageal Cancer
 Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Guidelines for the management of oesophageal and gastric cancer
 1 Department of Surgery, Royal Marsden NHS Foundation Trust, London, UK 2 School of Social and Community Medicine, University of Bristol, Bristol, UK 3 Northern Oesophago-Gastric Unit, Royal Victoria Infirmary,
1 Department of Surgery, Royal Marsden NHS Foundation Trust, London, UK 2 School of Social and Community Medicine, University of Bristol, Bristol, UK 3 Northern Oesophago-Gastric Unit, Royal Victoria Infirmary,
GCIG Rare Tumour Brainstorming Day
 GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Breast Cancer Breast Managed Clinical Network
 Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
Oesophago gastric cancer the disease and the challenges. Muntzer Mughal
 Oesophago gastric cancer the disease and the challenges Muntzer Mughal Oesophago gastric cancer How common is it? What causes it? What are the symptoms? How is it treated? Recent advances in: Detection
Oesophago gastric cancer the disease and the challenges Muntzer Mughal Oesophago gastric cancer How common is it? What causes it? What are the symptoms? How is it treated? Recent advances in: Detection