Surgery for Gastric and Oesophageal Cancer
|
|
|
- Charles Aron Campbell
- 5 years ago
- Views:
Transcription
1 Surgery for Gastric and Oesophageal Cancer

2 Trends in cancer mortality, England and Wales SMR base 1980
3 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death 13,500 people in year survival - oesophageal 10% 5 year survival - gastric 15%
4 Oesophago-Gastric Cancer The Local Problem North Trent Cancer Network Population 1.8m 30 October June cases of oesophagogastric cancer 155 resections (21%) 1 year survival Resected 77% Palliative oncology 34% Best supportive care 18%
5 Symptoms Physical signs Dysphagia Vomiting GI bleed Symptoms of anaemia Weight loss Dyspepsia Reflux
6 Epidemiology Marked increase in the incidence of lower 1/3 oesophageal and G-O junction adenocarcinoma in last 20 years Corresponding decrease in the incidence in distal gastric cancer and squamous cell cancer of the oesophagus.
7 Oesophageal Cancer Aetiology Smoking Alcohol G-O reflux Barrett s oesophagus
8 Why?
9 Medically fit No metastases Resectable Medically unfit Metastases Unresectable Operate Palliate
10

11 11
12 Restore Swallowing

13
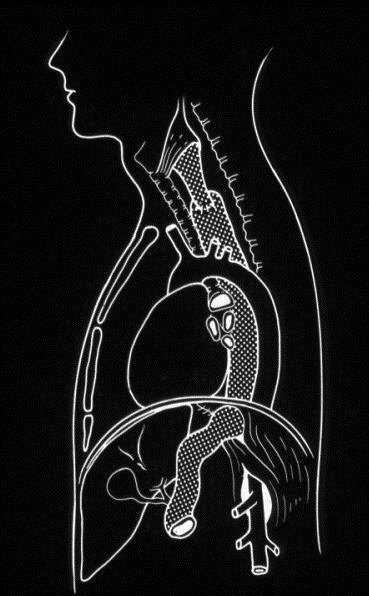
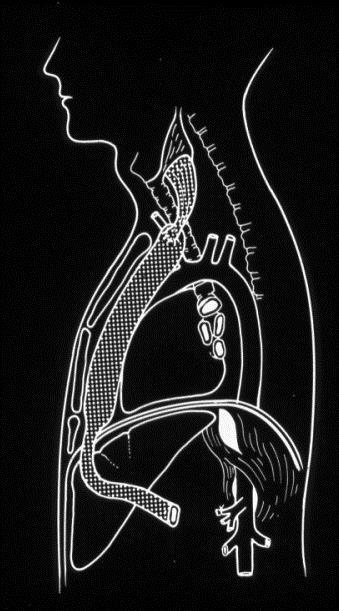
14 Surgical Approaches Thoraco abdominal Left thoracic Right thoracic (Ivor-Lewis) McKeown (3-Stage) Transhiatal 14
15
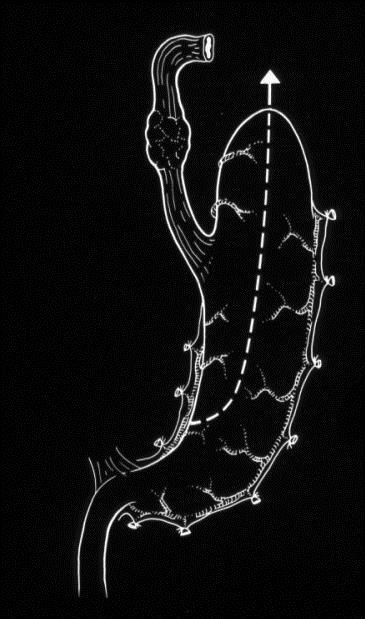
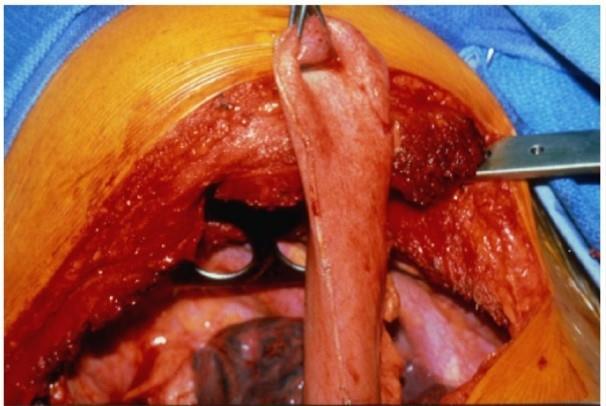
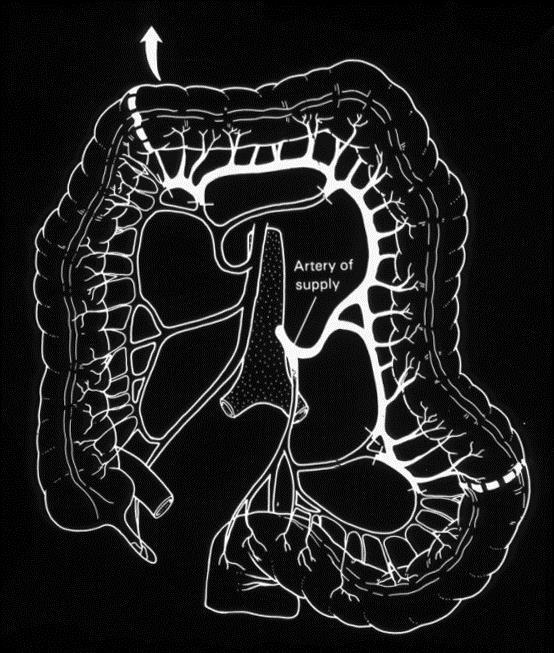
16 Oesophageal Replacement Stomach (+/- pyloroplasty) Jejunum Colon (which segment?) Which route? 16
17

18 24

19 25

20 20
21 26
22
23
24



25 MRC trial OEO2 Resectable Oesophageal Carcinoma SCC / ACA Randomised Chemotherapy + Surgery (CS) Surgery alone (S) n=400 n=402
26 Kaplan-Meier curve showing survival from date of randomisation CS S p=0.004 OE 02 Trial
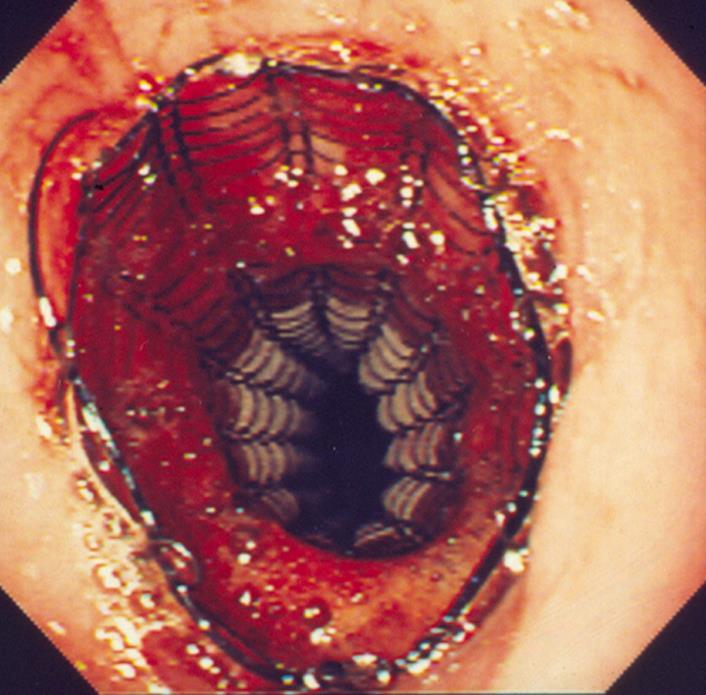
27 Oesophageal Carcinoma Conclusions Incidence is increasing Selection of patients for surgery has improved Peri operative mortality rate has fallen Expandable metal stents have improved palliative treatment for unresectable carcinomas Use of neoadjuvant treatments may improve survival rates Long term outcome for patients with oesophageal carcinoma remains dismal
28

29 29
30 CDH1 Family Tree Familial Diffuse Gastric Cancer

31 Aetiology of Gastric Cancer Napoleon Bonaparte Diet: Full of salt preserved foods, very little fruit & vegetables common foods for long military campaigns Genetic: father died of stomach cancer H.Pylori: Chronic H.Pylori infection Pre cancerous changes: CAG
32 Gastric Cancer : Problems Late diagnosis Few curative resections Low 5 year survival High operative mortality Little specialisation
33 LAPAROSCOPY Peritoneal metastases Direct invasion of other organs Avoids open / close laparotomy Better surgical planning Anaesthetic assessment
34 DISTAL TUMOURS Stenosis Bleeding» Surgery
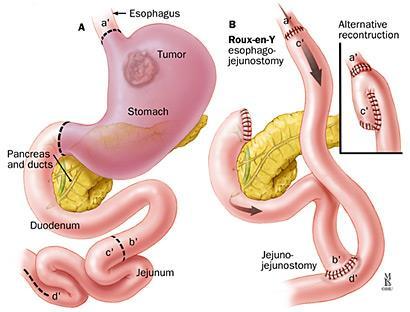
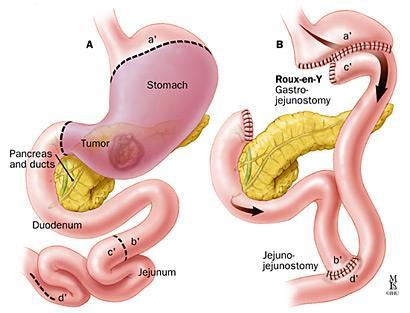
35 Gastric Resections Roux-en-Y 52
36 36

37 Lymphadenectomy 53
38 MAGIC Trial UK MRC Adjuvant Gastric Infusional Chemotherapy E epirubicin 3 cycles pre op C cisplatin 3 cycles post op F 5-FU

39 MAGIC Trial patients Chemo & surgery 250 Surgery 253


40 MAGIC Trial Disease free survival Chemo-Surgery- Chemo Surgery 2 years 48% 40% 5 years 36% 23%
41 Gastric Cancer - Conclusions Incidence decreasing Pre-operative chemotherapy improves survival Better surgical results in specialist units Early diagnosis essential
42 Complications! 42
43 Pulmonary Complications Pain and atelectasis Impaired movement of diaphragm Extensive lymphadenectomy resulting in a form of acute pulmonary oedema Post chemotherapy/ irradiation bronchiolitis 43
44 Management Thoracic epidural combined with morphine PCA Early extubation or overnight ventilation? CPAP or not? Fluid restrict? 44
45 Anastomotic leak Early < 72 hours - technical. Re-exploration and repair Late > 1 week reflects local ischaemia +/or tension in anastomotic site. Manage conservatively. 45
46 Prevention of complications Pain control respiratory care and physio and nebulisers fluid balance inotropes versus vasoconstrictors nutrition with feeding jejunostomy? Manage on HDU or ITU 46
47 Oesophageal Carcinoma

48 Oesophageal Carcinoma
49 Oesophageal Carcinoma

50 Oesophageal Carcinoma
51 51
52 52
53 53
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
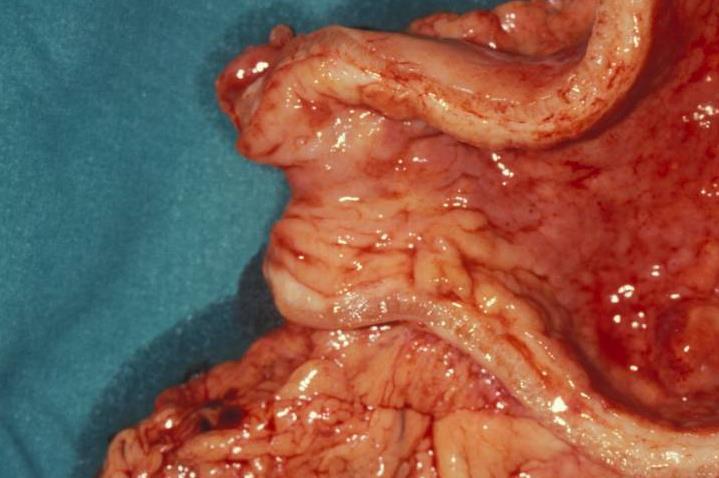
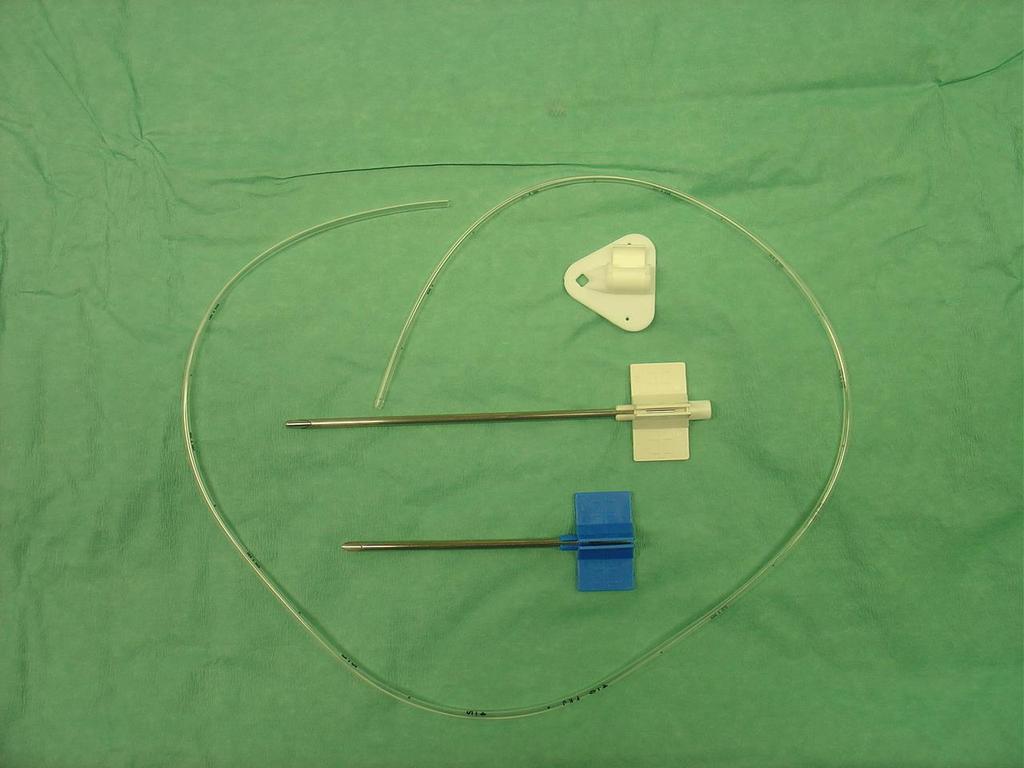
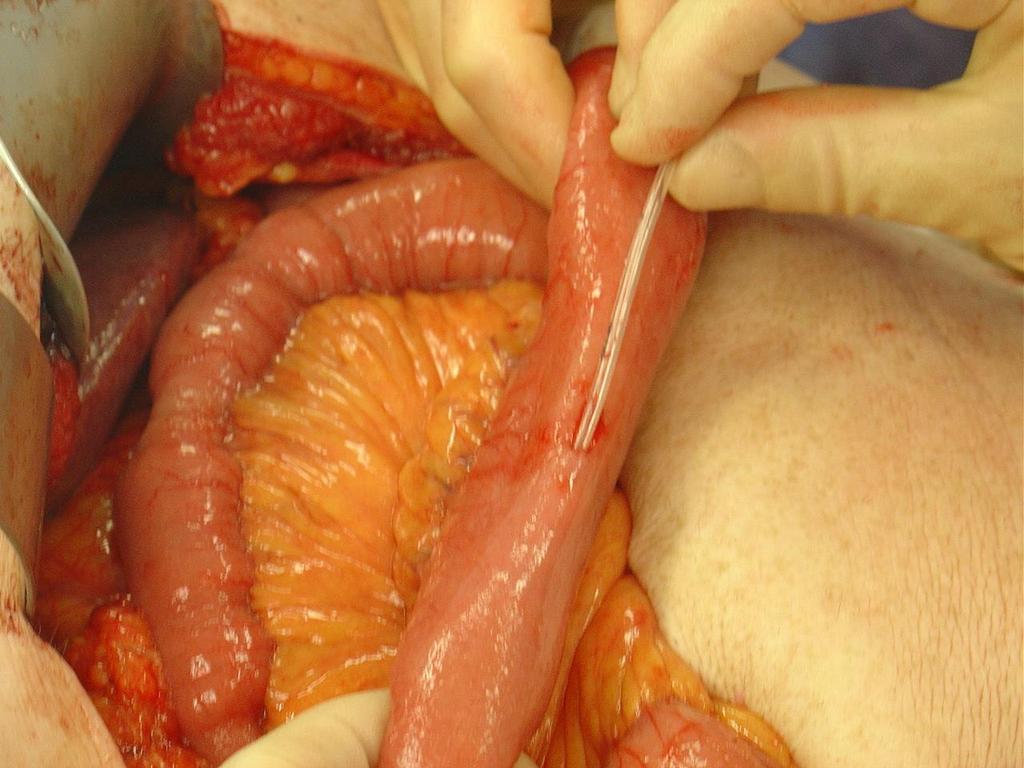
Jejunostomy after oesophagectomy, how and why I do it
 Jejunostomy after oesophagectomy, how and why I do it Graeme Couper. Consultant Oesophago-gastric Surgeon, The Royal Infirmary of Edinburgh BAPEN Conference 2010 2nd & 3rd November Harrogate International
Jejunostomy after oesophagectomy, how and why I do it Graeme Couper. Consultant Oesophago-gastric Surgeon, The Royal Infirmary of Edinburgh BAPEN Conference 2010 2nd & 3rd November Harrogate International
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
NICE guideline Published: 24 January 2018 nice.org.uk/guidance/ng83
 Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Oesophagogastric Cancer The Patient s Pathway
 National helpline: 0121 704 9860 V1 Oesophagogastric Cancer The Patient s Pathway {Based on The St Thomas Hospital Pathway} Registered Charity No. 1062461 Contents Introduction 3-5 Curative pathway 5-7
National helpline: 0121 704 9860 V1 Oesophagogastric Cancer The Patient s Pathway {Based on The St Thomas Hospital Pathway} Registered Charity No. 1062461 Contents Introduction 3-5 Curative pathway 5-7
ESOPHAGEAL CANCER. Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds
 ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
FTS Oesophagectomy: minimal research to date 3,4
 Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
A 16 yr old boy with aggressive ca esophagus. DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health
 A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
GUIDELINE NUMBER: 87. Management of oesophageal and gastric cancer. DATE ISSUED: June 2006 CLINICAL SERVICES INVOLVED: Upper GI
 GUIELINE NUMER: 87 GUIELINE TITLE: Management of oesophageal and gastric cancer ATE ISSUE: June 2006 LINIAL SERVIES INVOLVE: Upper GI Levels of Evidence 1++ High quality meta-analyses, systematic reviews
GUIELINE NUMER: 87 GUIELINE TITLE: Management of oesophageal and gastric cancer ATE ISSUE: June 2006 LINIAL SERVIES INVOLVE: Upper GI Levels of Evidence 1++ High quality meta-analyses, systematic reviews
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
APPLYING ENHANCED RECOVERY PRINCIPLES: EARLY TESTING IN UPPER GI CANCER
 APPLYING ENHANCED RECOVERY PRINCIPLES: EARLY TESTING IN UPPER GI CANCER William Allum Consultant Surgeon, Royal Marsden NHS Foundation Trust ? POSSIBLE Major procedure Painful Anastomotic complications
APPLYING ENHANCED RECOVERY PRINCIPLES: EARLY TESTING IN UPPER GI CANCER William Allum Consultant Surgeon, Royal Marsden NHS Foundation Trust ? POSSIBLE Major procedure Painful Anastomotic complications
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
DATA REPORT. August 2014
 AUDIT DATA REPORT August 2014 Prepared for the Australian and New Zealand Gastric and Oesophageal Surgical Association by the Royal Australasian College of Surgeons 199 Ward St, North Adelaide, SA 5006
AUDIT DATA REPORT August 2014 Prepared for the Australian and New Zealand Gastric and Oesophageal Surgical Association by the Royal Australasian College of Surgeons 199 Ward St, North Adelaide, SA 5006
Oesophago gastric cancer the disease and the challenges. Muntzer Mughal
 Oesophago gastric cancer the disease and the challenges Muntzer Mughal Oesophago gastric cancer How common is it? What causes it? What are the symptoms? How is it treated? Recent advances in: Detection
Oesophago gastric cancer the disease and the challenges Muntzer Mughal Oesophago gastric cancer How common is it? What causes it? What are the symptoms? How is it treated? Recent advances in: Detection
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand?
 MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
The 1 st Oesophago gastric Cancer Centers Meeting for The Anglia Cancer Network
 The 1 st Oesophago gastric Cancer Centers Meeting for The Anglia Cancer Network Date: Sept 28 th 2012 Venue: The Bedford Lodge Hotel Attendees: NORFOLK & NORWICH Mr Ed Cheong (UGI Cancer Lead) Dr Ben Simpson
The 1 st Oesophago gastric Cancer Centers Meeting for The Anglia Cancer Network Date: Sept 28 th 2012 Venue: The Bedford Lodge Hotel Attendees: NORFOLK & NORWICH Mr Ed Cheong (UGI Cancer Lead) Dr Ben Simpson
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Determining Resectability and Appropriate Surgery for Esophageal Cancer
 Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
A review of the management of 100 cases of
 Thorax (1972), 27, 599. A review of the management of 100 cases of benign stricture of the oesophagus S. RAPTIS' and D. MEARNS MILNE Thoracic Unit, Frenchay Hospital One hundred cases of benign stricture
Thorax (1972), 27, 599. A review of the management of 100 cases of benign stricture of the oesophagus S. RAPTIS' and D. MEARNS MILNE Thoracic Unit, Frenchay Hospital One hundred cases of benign stricture
Minimally Invasive Esophagectomy
 Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
Stenting for Esophageal Cancer Technical Issues and Outcomes
 Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Surgical strategies in esophageal cancer
 Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Management of oesophageal carcinoma
 THEME GI malignancies Management of oesophageal carcinoma Sean Mackay MD, FRACS, is an upper GIT and hepatobiliary surgeon, Peter MacCallum Cancer Institute, St Vincent s and Box Hill Hospitals, Victoria,
THEME GI malignancies Management of oesophageal carcinoma Sean Mackay MD, FRACS, is an upper GIT and hepatobiliary surgeon, Peter MacCallum Cancer Institute, St Vincent s and Box Hill Hospitals, Victoria,
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Oesophageal Cancer: The Image after Surgery
 Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT
 BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
Oesophageal Cancer: The Image after Surgery
 Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness
 Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
Palliative side-to-side oesophagogastrostomy for
 Thorax, 1981, 36, 441445 Palliative side-to-side oesophagogastrostomy for unresectable carcinoma of the oesophagus and cardia KOING-BO KWUN AND PAUL A KIRSCHNER From the Department ofsurgery and Division
Thorax, 1981, 36, 441445 Palliative side-to-side oesophagogastrostomy for unresectable carcinoma of the oesophagus and cardia KOING-BO KWUN AND PAUL A KIRSCHNER From the Department ofsurgery and Division
OESOPHAGO-GASTRIC CANCER 2016
 SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT OESOPHAGO-GASTRIC CANCER 2016 COMPARATIVE AUDIT REPORT Mr Peter Lamb SCAN Lead Upper GI Cancer Clinician Dr Jonathan Fletcher, Consultant Physician,
SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT OESOPHAGO-GASTRIC CANCER 2016 COMPARATIVE AUDIT REPORT Mr Peter Lamb SCAN Lead Upper GI Cancer Clinician Dr Jonathan Fletcher, Consultant Physician,
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ
 Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
17. Oesophagus. Upper gastrointestinal cancer
 110 17. Upper gastrointestinal cancer Oesophagus Radical treatment For patients with localised disease, the standard curative approach to treatment is either surgery + perioperative chemotherapy, surgery
110 17. Upper gastrointestinal cancer Oesophagus Radical treatment For patients with localised disease, the standard curative approach to treatment is either surgery + perioperative chemotherapy, surgery
Protocol for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER
 Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER Patient information given at each stage following agreed information pathway
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER Patient information given at each stage following agreed information pathway
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
 Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
National Oesophago-Gastric Cancer Audit Progress Report 2014
 National Oesophago-Gastric Cancer Audit Progress Report 2014 An Audit of the care received by people with Oesophago-Gastric Cancer in England and Wales 1 This report was prepared by Clinical Effectiveness
National Oesophago-Gastric Cancer Audit Progress Report 2014 An Audit of the care received by people with Oesophago-Gastric Cancer in England and Wales 1 This report was prepared by Clinical Effectiveness
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Douglas G. Adler MD. ACG Regional Postgraduate Course - Nashville, TN Copyright 2013 American College of Gastroenterology
 Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY GASTRIC CARCINOMA E PANIERI G CHINNERY B ROBERTSON INTRODUCTION Gastric neoplasms are common, and because they often present late, they arefrequently incurable.
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY GASTRIC CARCINOMA E PANIERI G CHINNERY B ROBERTSON INTRODUCTION Gastric neoplasms are common, and because they often present late, they arefrequently incurable.
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Is a Metallic Stent Useful for Non Resectable Esophageal Cancer?
 Original Article Is a Metallic Stent Useful for Non Resectable Esophageal Cancer? Shinsuke Wada, MD, 1 Tsuyoshi Noguchi, MD, 1 Shinsuke Takeno, MD, 1 Hatsuo Moriyama, MD, 1 Tsuyoshi Hashimoto, MD, 1 Yuzo
Original Article Is a Metallic Stent Useful for Non Resectable Esophageal Cancer? Shinsuke Wada, MD, 1 Tsuyoshi Noguchi, MD, 1 Shinsuke Takeno, MD, 1 Hatsuo Moriyama, MD, 1 Tsuyoshi Hashimoto, MD, 1 Yuzo
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Gastro-oesophageal junction cancers (ICD10 C15.2, C15.5, C16.0) 1
 1") Gastro-oesophageal junction cancers (ICD10 C15., C15.5, C16.0) 1 In England cancers of the gastro-oesophageal junction account for 0% of all cancers arising in the upper gastro-intestinal tract and are
Gastro-oesophageal junction cancers (ICD10 C15., C15.5, C16.0) 1 In England cancers of the gastro-oesophageal junction account for 0% of all cancers arising in the upper gastro-intestinal tract and are
Second Database Report. The Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland
 The Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland Second Database Report 24 Prepared by Mr Richard Hardwick MD FRCS Ms Sharon Davies on behalf of the Association of Upper
The Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland Second Database Report 24 Prepared by Mr Richard Hardwick MD FRCS Ms Sharon Davies on behalf of the Association of Upper
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran
 Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
DEPARTMENT OF ONCOLOGY ELECTIVE
 DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition
 22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
Upper GI. Oesophageal & Gastric Cancer. Tumour Group: Regimen name / acronym Cisplatin/5-FU with concomitant RT. Place in therapy
 Tumour Group: Upper GI Tumour Type: Oesophageal & Gastric Cancer Primary Cisplatin/5-FU with concomitant RT Alternative Regimen: Oxaliplatin/ 5FU with concomitant RT (FOLFOX6-RT) Cisplatin Carboplatin
Tumour Group: Upper GI Tumour Type: Oesophageal & Gastric Cancer Primary Cisplatin/5-FU with concomitant RT Alternative Regimen: Oxaliplatin/ 5FU with concomitant RT (FOLFOX6-RT) Cisplatin Carboplatin
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Minimally Invasive Esophagectomy
 American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
When to Refer for OGD and the Work Up of Upper GI Malignancies
 When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
Guidelines for the management of oesophageal and gastric cancer
 1 Department of Surgery, Royal Marsden NHS Foundation Trust, London, UK 2 School of Social and Community Medicine, University of Bristol, Bristol, UK 3 Northern Oesophago-Gastric Unit, Royal Victoria Infirmary,
1 Department of Surgery, Royal Marsden NHS Foundation Trust, London, UK 2 School of Social and Community Medicine, University of Bristol, Bristol, UK 3 Northern Oesophago-Gastric Unit, Royal Victoria Infirmary,
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
POSTOPERATIVE COMPLICATIONS OF TRANSTHORACIC ESOPHAGECTOMY FOR ESOPHAGEAL CARCINOMA
 International International Multidisciplinary Multidisciplinary e Journal/ e-journal Dr. A. Razaque Shaikh, Dr. Khenpal Das, Dr Shahida Khatoon ISSN 2277. (133-140) - 4262 POSTOPERATIVE COMPLICATIONS OF
International International Multidisciplinary Multidisciplinary e Journal/ e-journal Dr. A. Razaque Shaikh, Dr. Khenpal Das, Dr Shahida Khatoon ISSN 2277. (133-140) - 4262 POSTOPERATIVE COMPLICATIONS OF
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
MOLECULAR AND CLINICAL ONCOLOGY 3: , 2015
 MOLECULAR AND CLINICAL ONCOLOGY 3: 133-138, 2015 Assessment of health related quality of life of patients with esophageal squamous cell carcinoma following esophagectomy using EORTC quality of life questionnaires
MOLECULAR AND CLINICAL ONCOLOGY 3: 133-138, 2015 Assessment of health related quality of life of patients with esophageal squamous cell carcinoma following esophagectomy using EORTC quality of life questionnaires
National Oesophago-Gastric Cancer Audit
 National Oesophago-Gastric Cancer Audit An audit of the care received by people with Oesophago-Gastric Cancer in England and Wales First Annual Report 2008 Prepared in partnership with: National Oesophago-Gastric
National Oesophago-Gastric Cancer Audit An audit of the care received by people with Oesophago-Gastric Cancer in England and Wales First Annual Report 2008 Prepared in partnership with: National Oesophago-Gastric
Implementing PAthways for Early Diagnosis (I-PACED)
") Implementing PAthways for Early Diagnosis (I-PACED) Cancer Jeanne Potts 13 11 20 Clinical Nurse Specialist Cancer Council Victoria Cancer Council 27 th June 2018 cancercouncil.com.au Background OCPs describe
Implementing PAthways for Early Diagnosis (I-PACED) Cancer Jeanne Potts 13 11 20 Clinical Nurse Specialist Cancer Council Victoria Cancer Council 27 th June 2018 cancercouncil.com.au Background OCPs describe
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
Paraoesophageal Hernia
 Paraoesophageal Hernia Grand Round Adam Cichowitz Surgical Registrar Paraoesophageal Hernia Type of hiatal hernia Transdiaphragmatic migration of abdominal content gastric fundus gastric body pylorus colon
Paraoesophageal Hernia Grand Round Adam Cichowitz Surgical Registrar Paraoesophageal Hernia Type of hiatal hernia Transdiaphragmatic migration of abdominal content gastric fundus gastric body pylorus colon
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
When Stomach is Not Available
 When Stomach is Not Available Shanda Blackmon, M.D., M.P.H., FACS Associate Professor, Thoracic Surgery, Mayo Clinic 2014 MFMER slide-1 Objectives To review options for long-segment esophageal replacement
When Stomach is Not Available Shanda Blackmon, M.D., M.P.H., FACS Associate Professor, Thoracic Surgery, Mayo Clinic 2014 MFMER slide-1 Objectives To review options for long-segment esophageal replacement
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
RTC Dec Felicitas Koller and Eric Grogan
 RTC Dec 11 2009 Felicitas Koller and Eric Grogan Cancer Statistics, United States Number of patients 200000 150000 100000 50000 0 Lung Breast New Cases Deaths Esophageal Colorectal Prostate http://www.cancer.org/statistics
RTC Dec 11 2009 Felicitas Koller and Eric Grogan Cancer Statistics, United States Number of patients 200000 150000 100000 50000 0 Lung Breast New Cases Deaths Esophageal Colorectal Prostate http://www.cancer.org/statistics
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Pancreatic Cancer Where are we?
 Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: What is the treatment
: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: What is the treatment
AATS Focus on Thoracic Surgery: Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017?
 AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.