GASTRIC CANCER. Joyce Au SUNY Downstate Grand Rounds July 11, 2013
|
|
|
- Juniper Flynn
- 6 years ago
- Views:
Transcription
1 GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013
2 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory laparotomy and omental patch repair for perforated gastric ulcer in 2012 Soc hx: 30 pack years; assisted living facility
3 Thin NAD AAO RRR Clear BS b/l Abd soft, ND, NT, well healed midline scar Ext no edema No CVA tenderness
4 CBC: 10.3 / 14.3 / 44.7 / 280 BMP: 137 / 4.4 / 100 / 26 / 11 / 0.71 / 95 Coags: 10.1 / 0.9 / 25.2 EKG normal sinus rhythm Chest CT normal, no metastasis Abd CT irregular mass at antrum causing partial gastric outlet obstruction, no metastasis
5 OR EGD - ulcerated mass in the antrum Findings: antral mass, no liver or peritoneal lesions Procedure: subtotal gastrectomy with D2 lymphadenectomy and Billroth II reconstruction EBL: 50ml JP by duodenal stump
6 Patient pulled out NG on POD#4 Started on clear liquid diet on POD#5 which was tolerated and advanced JP was removed Discharged back to assisted living on POD#7
7 Pathology 3 cm moderately differentiated adenocarcinoma Intestinal type Invasion into muscularis propria Negative margins 0/23 LN
8 GASTRIC CANCER Introduction Workup Surgery Chemoradiation
9 INTRODUCTION World s 4 th leading cause of cancer-related death >10,000 deaths from gastric cancer annually in the U.S.
10 Risk factors Ethnicity Japanese, Koreans, Native Americans, Hawaiians > Chinese, African Americans, Latinos > Caucasians, Filipinos Male > female Obesity (proximal CA) Prior radiation, EBV (proximal, diffuse type) History of gastric resection
11 Diet salt, smoked, cured, nitrates, nitrites, nitrosamines carcinogenic N- nitroso compounds Tobacco Pernicious anemia (synchronous lesions) Villous adenomas in gastric polyps H. pylori
12 Genetic Hereditary diffuse gastric cancer Autosomal dominant CDH1 mutation for E-cadherin Prophylactic gastrectomy Li-Fraumeni syndrome - p53 mutation BRCA2 HNPCC FAP Peutz-Jeghers syndrome
13 Pathology Arise from mucous-producing cells in 95% Lauren classification INTESTINAL TYPE Well to moderately differentiated Intestinal metaplasia, chronic gastritis Older, male, lower socioeconomic Proximal tumors DIFFUSE TYPE Poorly differentiated Signet cells, mucin Younger, obese Distal tumor WHO classification tubular, mucinous, papillary, signet cell
 cancer Most lesions are in the antrum Recently, have decreasing distal lesions and")
14 Distal vs. proximal (cardia) cancer Most lesions are in the antrum Recently, have decreasing distal lesions and increasing cardia lesions 9% involve entire stomach linitus plastica Lesser curvature > greater curvature
15 Presentation Most common sx: weight loss, epigastric pain, vomiting, anorexia 10% with signs of metastatic disease Virchow node, Sister Mary Joseph node Blummer shelf Ascites, jaundice, liver mass Asymptomatic from EGD screening in Japan and Korea
16 WORKUP H&P EGD 4-6 bx for dx; surgical planning; palliative interventions (ablation, stents, etc.) EUS - 75% accuracy in staging; FNA Chest/abd/pelvis CT 66-77% accuracy in staging Laparoscopy <5 mm lesions seen in about 30% patients Peritoneal cytology 3-9 month median survival; M1 MD Anderson Surgical Oncology Handbook, 5 th ed.
17 7 th edition AJCC Staging, 2010 Tumors in the GEJ, or arising <5 cm from GEJ and crosses the GEJ are staged as esophageal carcinomas Tumors in the lamina propria are now T1a Fewer nodes for higher nodal status (ex. N1=1-2 LN) + peritoneal cytology is M1 Washington et al. Ann Surg Oncol 2010;17:
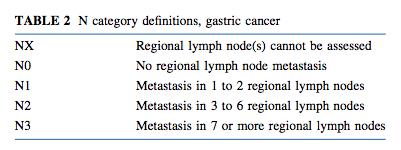
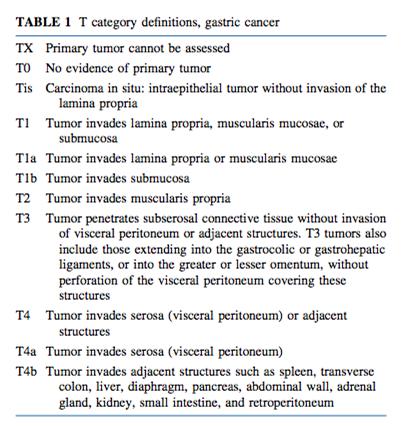
18 (tnm)

19 1 Washington et al. Ann Surg Oncol 2010;17:
20 SURGERY
21 History 400 B.C. Aesculapius cut out a stomach ulcer Pean in 1879 and Rydigier in 1880 resected the pylorus, but their patients died Billroth in 1881 performed the 1 st successful gastrectomy with gastroduodenostomy Wolfler in 1882 performed a palliative loop gastrojejunostomy Billroth in 1885 reconstructed with gastrojejunostomy
22 A.) Gastrectomy B.) Splenectomy C.) Lymphadenectomy D.) Reconstruction
23 A.) What kind of gastrectomy? Unresectable if encasing major vascular structures, N3 or N4, or peritoneal or distant metastasis Endoscopic mucosal resection in Japan Limited to mucosa (Tis or T1a), <1 cm with depressed types, <2 cm with elevated types, well-differentiated No randomized controlled trials on it
24 Participants patients, 31 centers Intervention subtotal gastrectomy; vs. total gastrectomy; both with D2 Similar 5-year survival Bozzetti et al. Ann Surg 1999;230:
25 Subtotal gastrectomy 25-30% remnant supplied by short gastrics 5-6 cm proximal margin Frozen section to confirm negative margin With negative margin as a requirement, subtotal gastrectomy is preferred for better nutritional status and quality of life
26 B.) What about splenectomy? Splenectomy did not improve survival, even with metastatic LN by splenic hilum or artery Yu et al. Br J Surg 2006;93:
27 Splenectomy with greater septic complications Up to two-fold risk of postoperative morbidity and mortality with splenectomy and distal pancreatectomy Unless there is malignant invasion into the spleen, splenectomy should be avoided Fang et al. Hepatogastroenterology 2012;59: Csendes et al. Surgery 2002;131: Bozzetti et al. Ann Surg 1997;226:
28 C.) Lymphadenectomy D1 or D2? Goal to examine at least 16 LN D1 = perigastric LN; within 3 cm D2 = perigastric LN + LN of the celiac and its main branches
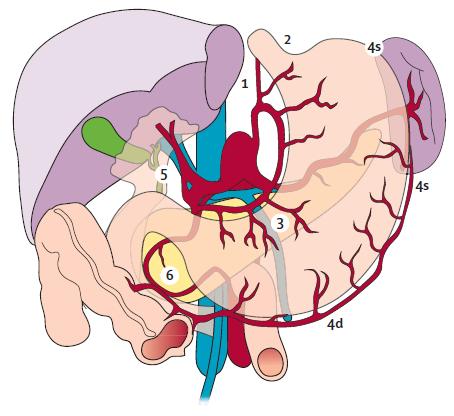
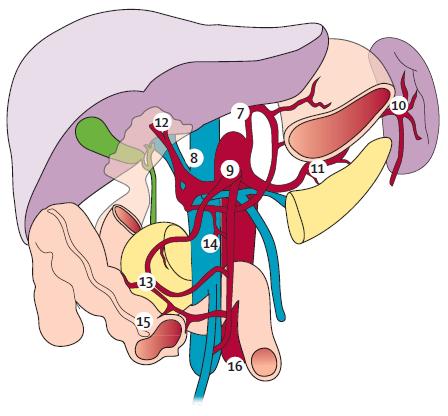
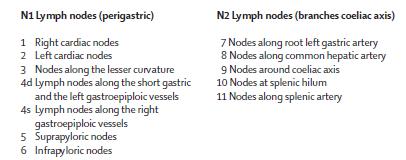
29 D1 D2


30 D2 is a standard in Asia Studies in the West question D1 vs. D2

31 MRC ST01 Participants: 400 patients Intervention: D2, with pancreatectomy & splenectomy; vs. D1 Similar 5-year survival (33% vs. 35%) Similar gastric-cancer related survival and recurrencefree survival Cuschieri et al. Br J Cancer 1999;79:
32 Participants: 711 patients, 80 hospitals Intervention: D2, with pancreatectomy & splenectomy; vs. D1 Outcomes: Higher postoperative mortality (10% vs. 4%) Higher postoperative morbidity (43% vs. 25%) Higher reoperation (18% vs. 8%) Similar 5-year relapse rate (37% vs. 43%) Similar 5-year survival (47% vs. 45%) Bonenkamp et al. NEJM 1999;340:
 Among patients with N2 disease, trend for greater survival with D2 dissection (21% vs. 0%, p=0.")
33 Outcome at 11 years Similar survival at 11 years (35% vs. 30%) Among patients with N2 disease, trend for greater survival with D2 dissection (21% vs. 0%, p=0.078) Greater morbidity and mortality with D2, pancreatectomy, splenectomy, age >70 years Hartgrink et al. J Clin Onc 2004;22:
 Less regional recurrence (13% vs. 19%) Less metastasis (11% vs. 17%) Songun et al.")
34 Outcome at 15 years D2 with less gastric-cancer related deaths (37% vs. 48%) Less local recurrence (12% vs. 22%) Less regional recurrence (13% vs. 19%) Less metastasis (11% vs. 17%) Songun et al. Lancet Oncol 2010;11:
35 Addition of para-aortic LN dissection did not improve survival but did increase blood loss and operative time compared to D2 dissection Modified D2 lymphadenectomy without pancreatectomy or splenectomy by experienced surgeons can be recommended; otherwise, D1 lymphadenectomy is recommended Sasako et al. NEJM 2008;359:
36 D.) Reconstruction Many options Subtotal gastrectomy - Billroth II Total gastrectomy - Roux-en-y
 Sakuramoto et al postop S-1 (prodrug fluorouracil) Boige et al preop 5FU,")
37 CHEMORADIATION Macdonald et al postop 5FU, leucovorin + radiation Cunningham et al MAGIC trial: pre and postop epirubicin, cisplatin, 5FU ( ECF ) Sakuramoto et al postop S-1 (prodrug fluorouracil) Boige et al preop 5FU, cisplatin
38 If tumor is T2 or higher, +LN perioperative chemotherapy preoperative chemoradiation If patient did not receive preoperative treatment, and is T3 or higher, or T1-2,+LN, or T2N0 with high risk features postoperative chemoradiation If patient had D2 resection and is T3 or higher, or T1-2,+LN postoperative chemotherapy
39 TAKE-HOME POINTS LN status has become more powerful in staging as a prognostic indicator for gastric cancer Unless mandated by extent of invasion, total gastrectomy and splenectomy are not necessary and to be avoided Modified D2 lymphadenectomy in experienced centers may offer long-term survival benefit Chemotherapy and radiation improve survival
40 QUESTIONS 1.) Which of the following on gastric cancer is NOT true? a. Highest incidence is in Japan b. Predominance among males or females varies geographically c. Incidence and death rates in the U.S. have decreased d. Higher incidence in patients who have undergone gastric resection for duodenal ulcer
41 2.) 65M has a biopsy proven gastric carcinoma on the lesser curvature, 5 cm distal to the esophagogastric junction. CT showed enlarged LN, which are confirmed by laparoscopy. The most appropriate surgical therapy would be: a. esophagogastrectomy with colonic interposition b. subtotal gastrectomy with a Billroth II anastomosis c. total gastrectomy d. total gastrectomy and splenectomy e. esophagogastrectomy with jejunal interposition
42 3.) A 65M has a total gastrectomy for a T2N1M0 gastric adenocarcinoma. The margins of resection are negative. This patient should also receive: a. external beam radiation b. fluorouracil-based chemotherapy c. a and b d. cisplatinum and external beam radiation e. no additional therapy
43 Thank you
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
SURGICAL MANAGEMENT OF GASTRIC CANCER
 SURGICAL MANAGEMENT OF GASTRIC CANCER Irina Kovatch, PGY 4 Kings County Medical Center Morbidity and Mortality January 13, 2011 Case Presentation 60 yo M admitted to medicine on 10/24/2010 with c/o persistent
SURGICAL MANAGEMENT OF GASTRIC CANCER Irina Kovatch, PGY 4 Kings County Medical Center Morbidity and Mortality January 13, 2011 Case Presentation 60 yo M admitted to medicine on 10/24/2010 with c/o persistent
Gastric Cancer: Surgery and Regional Therapy. Epidemiology. Risk factors
 Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Approaches to Surgical Treatment of Gastric Cancer. Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service
 Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
B Breast cancer, managing risk of lobular, in hereditary diffuse gastric cancer, 51
 Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
TUMORS OF THE STOMACH AND SMALL BOWEL
 gastrointestinal tract and abdomen TUMORS OF THE STOMACH AND SMALL BOWEL L. Mark Knab, MD, David J. Bentrem, MD, FACS, and Jeffrey D. Wayne, MD, FACS * Gastric Adenocarcinoma The incidence of gastric carcinoma
gastrointestinal tract and abdomen TUMORS OF THE STOMACH AND SMALL BOWEL L. Mark Knab, MD, David J. Bentrem, MD, FACS, and Jeffrey D. Wayne, MD, FACS * Gastric Adenocarcinoma The incidence of gastric carcinoma
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
GASTRIC CANCER DR AMIR ASHRAFI
 GASTRIC CANCER DR AMIR ASHRAFI Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common
GASTRIC CANCER DR AMIR ASHRAFI Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common
Gastric Tumors Dr. Taha
 Gastric Tumors Dr. Taha BENIGN TUMORS: Leiomyomas: smooth muscle tumors, equal in men /women, typically located in the middle &distal stomach. Can grow into the lumen with secondary ulceration & bleeding.
Gastric Tumors Dr. Taha BENIGN TUMORS: Leiomyomas: smooth muscle tumors, equal in men /women, typically located in the middle &distal stomach. Can grow into the lumen with secondary ulceration & bleeding.
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
Conventional Gastrectomy for Gastric Cancer. Franklin Wright UCHSC Department of Surgery Grand Rounds January 14, 2008
 Conventional Gastrectomy for Gastric Cancer Franklin Wright UCHSC Department of Surgery Grand Rounds January 14, 2008 Overview Gastric Adenocarcinoma Conventional vs Radical Lymphadenectomy Non-randomized
Conventional Gastrectomy for Gastric Cancer Franklin Wright UCHSC Department of Surgery Grand Rounds January 14, 2008 Overview Gastric Adenocarcinoma Conventional vs Radical Lymphadenectomy Non-randomized
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Printed by Hadi Ranjkeshzadeh on 11/12/2010 4:40:23 PM. For personal use only. Not approved for distribution. Copyright 2010 National Comprehensive
 Discussion Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform consensus. Category 2A: The recommendation
Discussion Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform consensus. Category 2A: The recommendation
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ.
 Professor of Surgery, Taibah Univ.") By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
Gastric Cancer: Etiologic Factors. H. Pylori diet (salt, nitrates) lifestyle (smoking, obesity) familial (~10% in West) diet hereditary
 lifestyle (smoking, obesity) familial (~10% in West) diet hereditary") Issue #1: Premalignant Lesions Gastric Cancer: Etiologic Factors H. Pylori diet (salt, nitrates) lifestyle (smoking, obesity) familial (~10% in West) diet hereditary HNPCC DGC Lauren Classification of
Issue #1: Premalignant Lesions Gastric Cancer: Etiologic Factors H. Pylori diet (salt, nitrates) lifestyle (smoking, obesity) familial (~10% in West) diet hereditary HNPCC DGC Lauren Classification of
Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy and Extended Lymphadenectomy
 International Surgical Oncology Volume 2012, Article ID 307670, 7 pages doi:10.1155/2012/307670 Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy
International Surgical Oncology Volume 2012, Article ID 307670, 7 pages doi:10.1155/2012/307670 Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy
intent treatment be in the elderly?
 Gastric cancer: How strong can curative intent treatment be in the elderly? Caio Max S. Rocha Lima, M.D. Professor of Medicine University of Miami & Sylvester Cancer Center Gastric cancer: epidemiology
Gastric cancer: How strong can curative intent treatment be in the elderly? Caio Max S. Rocha Lima, M.D. Professor of Medicine University of Miami & Sylvester Cancer Center Gastric cancer: epidemiology
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
International Journal of Medical Science and Health Research
 A Retrospective Study of Clinicopathological Profiles of Proximal Gastrectomy Vs Distal Gastrectomy in Carcinoma Stomach and Its Incidence in our Population Dr Magesh kumar J 1, Dr V Naveen Kumar 2, Dr
A Retrospective Study of Clinicopathological Profiles of Proximal Gastrectomy Vs Distal Gastrectomy in Carcinoma Stomach and Its Incidence in our Population Dr Magesh kumar J 1, Dr V Naveen Kumar 2, Dr
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Stomach. R.B. Kolachalam, MD
 Stomach R.B. Kolachalam, MD Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum Gastric Anatomy body of the stomach: site of mechanical
Stomach R.B. Kolachalam, MD Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum Gastric Anatomy body of the stomach: site of mechanical
위 ESD 후내시경소견 성균관대학교의과대학내과이준행
 위 ESD 후내시경소견 성균관대학교의과대학내과이준행 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다. ESD 후정상내시경소견 성균관대학교의과대학내과이준행 처음의뢰되었을때의사진 ESD M/D, 18mm, LP, RM (-), L/V (-) 추적내시경소견 2
위 ESD 후내시경소견 성균관대학교의과대학내과이준행 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다. ESD 후정상내시경소견 성균관대학교의과대학내과이준행 처음의뢰되었을때의사진 ESD M/D, 18mm, LP, RM (-), L/V (-) 추적내시경소견 2
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Laparoscopy-assisted D2 radical distal subtotal gastrectomy
 Masters of Gastrointestinal Surgery Laparoscopy-assisted D2 radical distal subtotal gastrectomy Xiaogeng Chen, Weihua Li, Jinsi Wang, Changshun Yang Department of Tumor Surgery, Fujian Provincial Hospital,
Masters of Gastrointestinal Surgery Laparoscopy-assisted D2 radical distal subtotal gastrectomy Xiaogeng Chen, Weihua Li, Jinsi Wang, Changshun Yang Department of Tumor Surgery, Fujian Provincial Hospital,
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
I. Technical Issues. Surgical Resection of Gastric Cancer. Surgical Resection of Gastric Cancer Evidence & Issues. French and Italian RCT Antral Ca
 Surgical Resection of Gastric Cancer Evidence & Issues Carol J. Swallow Department of Surgical Oncology Princess Margaret and Mount Sinai Hospitals University of Toronto Surgical Problems in Proximal GI
Surgical Resection of Gastric Cancer Evidence & Issues Carol J. Swallow Department of Surgical Oncology Princess Margaret and Mount Sinai Hospitals University of Toronto Surgical Problems in Proximal GI
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
Case Presentation. PMH: HTN, BPH, strabismus PSH: appendectomy Medications: norvasc, tamsulosin NKDA SH/FH: negative
 Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
General Data. Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission :
 General Data Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission : 92-07-09 1 Chief complaint Upper abdominal fullness 30 minutes after having foods with sometimes epigastralgia
General Data Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission : 92-07-09 1 Chief complaint Upper abdominal fullness 30 minutes after having foods with sometimes epigastralgia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN
 Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
Hereditary Gastric Cancer
 Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
 Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Case Report Late Onset Remnant Gastric Cancer with Afferent Loop Syndrome 47 Years after Billroth II Surgery
 Case Reports in Surgery Volume 2015, Article ID 730897, 4 pages http://dx.doi.org/10.1155/2015/730897 Case Report Late Onset Remnant Gastric Cancer with Afferent Loop Syndrome 47 Years after Billroth II
Case Reports in Surgery Volume 2015, Article ID 730897, 4 pages http://dx.doi.org/10.1155/2015/730897 Case Report Late Onset Remnant Gastric Cancer with Afferent Loop Syndrome 47 Years after Billroth II
Comparison of lymph node number and prognosis in gastric cancer patients with perigastric lymph nodes retrieved by surgeons and pathologists
 Original Article Comparison of lymph node number and prognosis in gastric cancer patients with perigastric lymph nodes retrieved by surgeons and pathologists Lixin Jiang, Zengwu Yao, Yifei Zhang, Jinchen
Original Article Comparison of lymph node number and prognosis in gastric cancer patients with perigastric lymph nodes retrieved by surgeons and pathologists Lixin Jiang, Zengwu Yao, Yifei Zhang, Jinchen
A Retrospective Study of Survival and Patterns of Failure in Gastric Cancer after Adjuvant Chemoradiation
 Med. J. Cairo Univ., Vol. 82, No. 2, December: 131-138, 2014 www.medicaljournalofcairouniversity.net A Retrospective Study of Survival and Patterns of Failure in Gastric Cancer after Adjuvant Chemoradiation
Med. J. Cairo Univ., Vol. 82, No. 2, December: 131-138, 2014 www.medicaljournalofcairouniversity.net A Retrospective Study of Survival and Patterns of Failure in Gastric Cancer after Adjuvant Chemoradiation
Gallbladder Cancer. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Gallbladder Cancer GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: September 2006 This guideline is a statement of
Gallbladder Cancer GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: September 2006 This guideline is a statement of
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ
 Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Akiko Serizawa *, Kiyoaki Taniguchi, Takuji Yamada, Kunihiko Amano, Sho Kotake, Shunichi Ito and Masakazu Yamamoto
 Serizawa et al. Surgical Case Reports (2018) 4:88 https://doi.org/10.1186/s40792-018-0494-4 CASE REPORT Successful conversion surgery for unresectable gastric cancer with giant paraaortic lymph node metastasis
Serizawa et al. Surgical Case Reports (2018) 4:88 https://doi.org/10.1186/s40792-018-0494-4 CASE REPORT Successful conversion surgery for unresectable gastric cancer with giant paraaortic lymph node metastasis
Gastric (Stomach) Cancer
 Cancer") Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
Prognosis of Patients With Gastric Cancer Who Underwent Proximal Gastrectomy
 Int Surg 2012;97:275 279 Prognosis of Patients With Gastric Cancer Who Underwent Proximal Gastrectomy Masahide Ikeguchi, Abdul Kader, Seigo Takaya, Youji Fukumoto, Tomohiro Osaki, Hiroaki Saito, Shigeru
Int Surg 2012;97:275 279 Prognosis of Patients With Gastric Cancer Who Underwent Proximal Gastrectomy Masahide Ikeguchi, Abdul Kader, Seigo Takaya, Youji Fukumoto, Tomohiro Osaki, Hiroaki Saito, Shigeru
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy
 Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
A218 : Esophagus cancer tissues. (formalin fixed)
") (formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
(formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
Subtotal gastrectomy for gastric cancer
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v20.i38.13667 World J Gastroenterol 2014 October 14; 20(38): 13667-13680 ISSN 1007-9327
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v20.i38.13667 World J Gastroenterol 2014 October 14; 20(38): 13667-13680 ISSN 1007-9327
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Surgical Treatment of Localized Gastric Cancer
 13 Surgical Treatment of Localized Gastric Cancer JOHN I. LEW, MD MITCHELL C. POSNER, MD Theodor Billroth performed the first successful gastric resection (a distal subtotal gastrectomy for stomach cancer)
13 Surgical Treatment of Localized Gastric Cancer JOHN I. LEW, MD MITCHELL C. POSNER, MD Theodor Billroth performed the first successful gastric resection (a distal subtotal gastrectomy for stomach cancer)
gastric cancer; lymph node dissection;
 Yonago Acta Medica 18;61:175 181 Original Article Therapeutic Value of Lymph Node Dissection Along the Superior Mesenteric Vein and the Posterior Surface of the Pancreatic Head in Gastric Cancer Located
Yonago Acta Medica 18;61:175 181 Original Article Therapeutic Value of Lymph Node Dissection Along the Superior Mesenteric Vein and the Posterior Surface of the Pancreatic Head in Gastric Cancer Located
New developments in pathogenesis, gastric cancer. Matthias Ebert. II. Medizinische Klinik Klinikum rechts der Isar TU München
 New developments in pathogenesis, diagnosis, therapy and prevention of gastric cancer Matthias Ebert II. Medizinische Klinik Klinikum rechts der Isar TU München Gastric Cancer Pathogenesis Diagnosis Treatment
New developments in pathogenesis, diagnosis, therapy and prevention of gastric cancer Matthias Ebert II. Medizinische Klinik Klinikum rechts der Isar TU München Gastric Cancer Pathogenesis Diagnosis Treatment
Patient. Male 76 year old C.C: abdominal pain
 Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
 Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY GASTRIC CARCINOMA E PANIERI G CHINNERY B ROBERTSON INTRODUCTION Gastric neoplasms are common, and because they often present late, they arefrequently incurable.
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY GASTRIC CARCINOMA E PANIERI G CHINNERY B ROBERTSON INTRODUCTION Gastric neoplasms are common, and because they often present late, they arefrequently incurable.
Subtotal versus total gastrectomy for T3 adenocarcinoma of the antrum
 Gastric Cancer (2003) 6: 237 242 DOI 10.1007/s10120-003-0261-4 Original article 2003 by International and Japanese Gastric Cancer Associations Subtotal versus total gastrectomy for T3 adenocarcinoma of
Gastric Cancer (2003) 6: 237 242 DOI 10.1007/s10120-003-0261-4 Original article 2003 by International and Japanese Gastric Cancer Associations Subtotal versus total gastrectomy for T3 adenocarcinoma of
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
GASTROINTESTINAL MALIGNANCIES
 Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Update on Hereditary Gastric Cancer. Dr. Savtaj Brar MD MSc Surgical Oncologist Assistant Professor of Surgery
 Update on Hereditary Gastric Cancer Dr. Savtaj Brar MD MSc Surgical Oncologist Assistant Professor of Surgery Disclosures None Outline 1. Discuss new consensus guidelines on hereditary diffuse gastric
Update on Hereditary Gastric Cancer Dr. Savtaj Brar MD MSc Surgical Oncologist Assistant Professor of Surgery Disclosures None Outline 1. Discuss new consensus guidelines on hereditary diffuse gastric
Gastric Adenocarcinoma Surgery and Adjuvant Therapy
 Gastric Adenocarcinoma and Adjuvant Therapy Sameer H. Patel, MD, David A. Kooby, MD* KEYWORDS Gastric cancer Gastric resection Adjuvant therapy Gastric adenocarcinoma Although the incidence of gastric
Gastric Adenocarcinoma and Adjuvant Therapy Sameer H. Patel, MD, David A. Kooby, MD* KEYWORDS Gastric cancer Gastric resection Adjuvant therapy Gastric adenocarcinoma Although the incidence of gastric
Gastric adenocarcinoma Bern
 Gastric adenocarcinoma 18.10.2017 Bern Epidemiology Worldwide 5th cancer with 950 000 new cases per year, 161 000 in Europe, 683 in Switzerland 3 rd cause of mortality worldwide, 485 cases/year in Switzerland
Gastric adenocarcinoma 18.10.2017 Bern Epidemiology Worldwide 5th cancer with 950 000 new cases per year, 161 000 in Europe, 683 in Switzerland 3 rd cause of mortality worldwide, 485 cases/year in Switzerland
Perioperative versus adjuvant management of gastric cancer, update 2013
 Perioperative versus adjuvant management of gastric cancer, update 2013 Cornelis J.H. van de Velde, MD, PhD,FRCPS and FACS,Hon. Professor of Surgery President ECCO - the European Cancer Organization Past-President
Perioperative versus adjuvant management of gastric cancer, update 2013 Cornelis J.H. van de Velde, MD, PhD,FRCPS and FACS,Hon. Professor of Surgery President ECCO - the European Cancer Organization Past-President
Treatment Strategy for Non-curative Resection of Early Gastric Cancer. Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea
 Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Surgical Treatment of Gastric Cancer
 SMGr up Surgical Treatment of Gastric Cancer Igor Correia de Farias 1 *, Maria Luiza Leite de Medeiros 2, Wilson Luiz da Costa Júnior 1, Heber Salvador de Castro Ribeiro 1, Alessandro Landskron Diniz 1,
SMGr up Surgical Treatment of Gastric Cancer Igor Correia de Farias 1 *, Maria Luiza Leite de Medeiros 2, Wilson Luiz da Costa Júnior 1, Heber Salvador de Castro Ribeiro 1, Alessandro Landskron Diniz 1,
WHICH LYMPH NODES SHOULD BE
 Y.K.: 82 Y.O. WOMAN WITH ANEMIA No GI symptoms. Chronic AF taking coumadin: INR=2.1. HCT=24. Anemia persists despite Rx. Colonoscopy: tumor in ascending colon. Bx: adenocarcinoma. Rx: Laparoscopic right
Y.K.: 82 Y.O. WOMAN WITH ANEMIA No GI symptoms. Chronic AF taking coumadin: INR=2.1. HCT=24. Anemia persists despite Rx. Colonoscopy: tumor in ascending colon. Bx: adenocarcinoma. Rx: Laparoscopic right
Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer
 Masters of Gastrointestinal Surgery Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer Xin Ye, Jian-Chun Yu, Wei-Ming
Masters of Gastrointestinal Surgery Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer Xin Ye, Jian-Chun Yu, Wei-Ming
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
GASTROESOPHAGEAL CANCER EPIDEMIOLOGY AND CLINICAL PRESENTATION. Prof Eric Van Cutsem, MD, PhD University Hospitals Leuven Belgium
 GASTROESOPHAGEAL CANCER EPIDEMIOLOGY AND CLINICAL PRESENTATION Prof Eric Van Cutsem, MD, PhD University Hospitals Leuven Belgium Leuven city hall and University Leuven: capital of beer AnheuserBusch-InBev
GASTROESOPHAGEAL CANCER EPIDEMIOLOGY AND CLINICAL PRESENTATION Prof Eric Van Cutsem, MD, PhD University Hospitals Leuven Belgium Leuven city hall and University Leuven: capital of beer AnheuserBusch-InBev
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy
 Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Esophagus & Stomach 2014-2015 NAACCR Webinar Series April 2, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Esophagus & Stomach 2014-2015 NAACCR Webinar Series April 2, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Gastric and GE Junction Cancer: Epidemiology and Clinical Presentation
 Gastric and GE Junction Cancer: Epidemiology and Clinical Presentation ESMO Preceptorship Programme Gastrointestinal Tumours Singapore 20-22 November, 2018 Dr. Cheng Ean CHEE Consultant Medical Oncologist
Gastric and GE Junction Cancer: Epidemiology and Clinical Presentation ESMO Preceptorship Programme Gastrointestinal Tumours Singapore 20-22 November, 2018 Dr. Cheng Ean CHEE Consultant Medical Oncologist
Radiotherapy for Gastric Cancer. Nitin Ohri, M.D. Montefiore Medical Center Albert Einstein College of Medicine 12/15/2012
 Radiotherapy for Gastric Cancer Nitin Ohri, M.D. Montefiore Medical Center Albert Einstein College of Medicine 12/15/2012 Disclosures I have no conflicts of interest to disclose. Outline Background Treatment
Radiotherapy for Gastric Cancer Nitin Ohri, M.D. Montefiore Medical Center Albert Einstein College of Medicine 12/15/2012 Disclosures I have no conflicts of interest to disclose. Outline Background Treatment
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death