World Journal of Gastroenterology
|
|
|
- Annice Parrish
- 5 years ago
- Views:
Transcription
: 3701-3884 Published by Baishideng Publishing Group")
1 ISSN (print) ISSN (online) World Journal of Gastroenterology World J Gastroenterol 2016 April 14; 22(14): Published by Baishideng Publishing Group Inc
, Argentina (7), Australia (31), Austria (9), Belgium (11), Brazil (20), Brunei Darussalam (1), Bulgaria (2), Cambodia (1), Canada (26), Chile (4),")
, Iran (10), Ireland (9), Israel (18), Italy (194), Japan (149), Jordan (1), Kuwait (1), Lebanon (7), Lithuania (1), Malaysia (1), Mexico (11), Morocco (1), Netherlands (5), New Zealand")
, Spain (51), Sri Lanka (1), Sudan (1), Sweden (12), Switzerland (5), Thailand (7), Trinidad and Tobago (1), Tunisia (2), Turkey (55), United Kingdom (49), United States (180), Venezuela")
2 Editorial Board The World Journal of Gastroenterology Editorial Board consists of 1376 members, representing a team of worldwide experts in gastroenterology and hepatology. They are from 68 countries, including Algeria (2), Argentina (7), Australia (31), Austria (9), Belgium (11), Brazil (20), Brunei Darussalam (1), Bulgaria (2), Cambodia (1), Canada (26), Chile (4), China (164), Croatia (2), Cuba (1), Czech (6), Denmark (2), Egypt (9), Estonia (2), Finland (6), France (20), Germany (58), Greece (31), Guatemala (1), Hungary (15), Iceland (1), India (33), Indonesia (2), Iran (10), Ireland (9), Israel (18), Italy (194), Japan (149), Jordan (1), Kuwait (1), Lebanon (7), Lithuania (1), Malaysia (1), Mexico (11), Morocco (1), Netherlands (5), New Zealand (4), Nigeria (3), Norway (6), Pakistan (6), Poland (12), Portugal (8), Puerto Rico (1), Qatar (1), Romania (10), Russia (3), Saudi Arabia (2), Singapore (7), Slovenia (2), South Africa (1), South Korea (69), Spain (51), Sri Lanka (1), Sudan (1), Sweden (12), Switzerland (5), Thailand (7), Trinidad and Tobago (1), Tunisia (2), Turkey (55), United Kingdom (49), United States (180), Venezuela (1), and Vietnam (1). EDITORS-IN-CHIEF Stephen C Strom, Stockholm Andrzej S Tarnawski, Long Beach Damian Garcia-Olmo, Madrid ASSOCIATE EDITORS Yung-Jue Bang, Seoul Vincent Di Martino, Besancon Daniel T Farkas, Bronx Roberto J Firpi, Gainesville Maria Gazouli, Athens Chung-Feng Huang, Kaohsiung Namir Katkhouda, Los Angeles Anna Kramvis, Johannesburg Wolfgang Kruis, Cologne Peter L Lakatos, Budapest Han Chu Lee, Seoul Christine McDonald, Cleveland Nahum Mendez-Sanchez, Mexico City George K Michalopoulos, Pittsburgh Suk Woo Nam, Seoul Shu-You Peng, Hangzhou Daniel von Renteln, Montreal Angelo Sangiovanni, Milan Hildegard M Schuller, Knoxville Dong-Wan Seo, Seoul Adrian John Stanley, Glasgow Jurgen Stein, Frankfurt Bei-Cheng Sun, Nanjing Yoshio Yamaoka, Yufu GUEST EDITORIAL BOARD MEMBERS Jia-Ming Chang, Taipei Jane CJ Chao, Taipei Kuen-Feng Chen, Taipei Tai-An Chiang, Tainan Yi-You Chiou, Taipei Seng-Kee Chuah, Kaohsiung Wan-Long Chuang, Kaohsiung How-Ran Guo, Tainan Ming-Chih Hou, Taipei Po-Shiuan Hsieh, Taipei Ching-Chuan Hsieh, Chiayi county Jun-Te Hsu, Taoyuan Chung-Ping Hsu, Taichung Chien-Ching Hung, Taipei Chao-Hung Hung, Kaohsiung Chen-Guo Ker, Kaohsiung Yung-Chih Lai, Taipei Teng-Yu Lee, Taichung City Wei-Jei Lee, Taoyuan Jin-Ching Lee, Kaohsiung Jen-Kou Lin, Taipei Ya-Wen Lin, Taipei Hui-kang Liu, Taipei Min-Hsiung Pan, Taipei Bor-Shyang Sheu, Tainan Hon-Yi Shi, Kaohsiung Fung-Chang Sung, Taichung Dar-In Tai, Taipei Jung-Fa Tsai, Kaohsiung Yao-Chou Tsai, New Taipei City Chih-Chi Wang, Kaohsiung Liang-Shun Wang, New Taipei City Hsiu-Po Wang, Taipei Jaw-Yuan Wang, Kaohsiung Yuan-Huang Wang, Taipei Yuan-Chuen Wang, Taichung Deng-Chyang Wu, Kaohsiung Shun-Fa Yang, Taichung Hsu-Heng Yen, Changhua MEMBERS OF THE EDITORIAL BOARD Algeria Saadi Berkane, Algiers Samir Rouabhia, Batna Argentina N Tolosa de Talamoni, Córdoba Eduardo de Santibanes, Buenos Aires Bernardo Frider, Capital Federal Guillermo Mazzolini, Pilar Carlos Jose Pirola, Buenos Aires Bernabé Matías Quesada, Buenos Aires María Fernanda Troncoso, Buenos Aires Australia Golo Ahlenstiel, Westmead Minoti V Apte, Sydney Jacqueline S Barrett, Melbourne Michael Beard, Adelaide Filip Braet, Sydney Guy D Eslick, Sydney Christine Feinle-Bisset, Adelaide Mark D Gorrell, Sydney Michael Horowitz, Adelaide I January 1, 2016






3 Gordon Stanley Howarth, Roseworthy Seungha Kang, Brisbane Alfred King Lam, Gold Coast Ian C Lawrance, PerthFremantle Barbara Anne Leggett, Brisbane Daniel A Lemberg, Sydney Rupert W Leong, Sydney Finlay A Macrae, Victoria Vance Matthews, Melbourne David L Morris, Sydney Reme Mountifield, Bedford Park Hans J Netter, Melbourne Nam Q Nguyen, Adelaide Liang Qiao, Westmead Rajvinder Singh, Adelaide Ross Cyril Smith, StLeonards Kevin J Spring, Sydney Debbie Trinder, Fremantle Daniel R van Langenberg, Box Hill David Ian Watson, Adelaide Desmond Yip, Garran Li Zhang, Sydney Austria Felix Aigner, Innsbruck Gabriela A Berlakovich, Vienna Herwig R Cerwenka, Graz Peter Ferenci, Wien Alfred Gangl, Vienna Kurt Lenz, Linz Markus Peck-Radosavljevic, Vienna Markus Raderer, Vienna Stefan Riss, Vienna Belgium Michael George Adler, Brussels Benedicte Y De Winter, Antwerp Mark De Ridder, Jette Olivier Detry, Liege Denis Dufrane Dufrane, Brussels Sven M Francque, Edegem Nikos Kotzampassakis, Liège Geert KMM Robaeys, Genk Xavier Sagaert, Leuven Peter Starkel, Brussels Eddie Wisse, Keerbergen Brazil SMP Balzan, Santa Cruz do Sul JLF Caboclo, Sao jose do rio preto Fábio Guilherme Campos, Sao Paulo Claudia RL Cardoso, Rio de Janeiro Roberto J Carvalho-Filho, Sao Paulo Carla Daltro, Salvador José Sebastiao dos Santos, Ribeirao Preto Eduardo LR Mello, Rio de Janeiro Sthela Maria Murad-Regadas, Fortaleza Claudia PMS Oliveira, Sao Paulo Júlio C Pereira-Lima, Porto Alegre Marcos V Perini, Sao Paulo Vietla Satyanarayana Rao, Fortaleza Raquel Rocha, Salvador AC Simoes e Silva, Belo Horizonte Mauricio F Silva, Porto Alefre Aytan Miranda Sipahi, Sao Paulo Rosa Leonôra Salerno Soares, Niterói Cristiane Valle Tovo, Porto Alegre Eduardo Garcia Vilela, Belo Horizonte Brunei Darussalam Vui Heng Chong, Bandar Seri Begawan Bulgaria Tanya Kirilova Kadiyska, Sofia Mihaela Petrova, Sofia Cambodia Francois Rouet, Phnom Penh Canada Brian Bressler, Vancouver Frank J Burczynski, Winnipeg Wangxue Chen, Ottawa Francesco Crea, Vancouver Mirko Diksic, Montreal Jane A Foster, Hamilton Hugh J Freeman, Vancouver Shahrokh M Ghobadloo, Ottawa Yuewen Gong, Winnipeg Philip H Gordon, Quebec Rakesh Kumar, Edmonton Wolfgang A Kunze, Hamilton Patrick Labonte, Laval Zhikang Peng, Winnipeg Jayadev Raju, Ottawa Maitreyi Raman, Calgary Giada Sebastiani, Montreal Maida J Sewitch, Montreal Eldon A Shaffer, Alberta Christopher W Teshima, Edmonton Jean Sévigny, Québec Pingchang Yang, Hamilton Pingchang Yang, Hamilton Eric M Yoshida, Vancouver Bin Zheng, Edmonton Chile Marcelo A Beltran, La Serena Flavio Nervi, Santiago Adolfo Parra-Blanco, Santiago Alejandro Soza, Santiago China Zhao-Xiang Bian, Hong Kong San-Jun Cai, Shanghai Guang-Wen Cao, Shanghai Long Chen, Nanjing Ru-Fu Chen, Guangzhou George G Chen, Hong Kong Li-Bo Chen, Wuhan Jia-Xu Chen, Beijing Hong-Song Chen, Beijing Lin Chen, Beijing Yang-Chao Chen, Hong Kong Zhen Chen, Shanghai Ying-Sheng Cheng, Shanghai Kent-Man Chu, Hong Kong Zhi-Jun Dai, Xi an Jing-Yu Deng, Tianjin Yi-Qi Du, Shanghai Zhi Du, Tianjin Hani El-Nezami, Hong Kong Bao-Ying Fei, Hangzhou Chang-Ming Gao, Nanjing Jian-Ping Gong, Chongqing Zuo-Jiong Gong, Wuhan Jing-Shan Gong, Shenzhen Guo-Li Gu, Beijing Yong-Song Guan, Chengdu Mao-Lin Guo, Luoyang Jun-Ming Guo, Ningbo Yan-Mei Guo, Shanghai Xiao-Zhong Guo, Shenyang Guo-Hong Han, Xi an Ming-Liang He, Hong Kong Peng Hou, Xi an Zhao-Hui Huang, Wuxi Feng Ji, Hangzhou Simon Law, Hong Kong Yu-Yuan Li, Guangzhou Meng-Sen Li, Haikou Shu-De Li, Shanghai Zong-Fang Li, Xi an Qing-Quan Li, Shanghai Kang Li, Lasa Han Liang, Tianjin Xing e Liu, Hangzhou Zheng-Wen Liu, Xi an Xiao-Fang Liu, Yantai Bin Liu, Tianjin Quan-Da Liu, Beijing Hai-Feng Liu, Beijing Fei Liu, Shanghai Ai-Guo Lu, Shanghai He-Sheng Luo, Wuhan Xiao-Peng Ma, Shanghai Yong Meng, Shantou Ke-Jun Nan, Xi an Siew Chien Ng, Hong Kong Simon SM Ng, Hong Kong Zhao-Shan Niu, Qingdao Di Qu, Shanghai Ju-Wei Mu, Beijing Rui-Hua Shi, Nanjing Bao-Min Shi, Shanghai Xiao-Dong Sun, Hangzhou Si-Yu Sun, Shenyang Guang-Hong Tan, Haikou Wen-Fu Tang, Chengdu Anthony YB Teoh, Hong Kong Wei-Dong Tong, Chongqing Eric Tse, Hong Kong Hong Tu, Shanghai II January 1, 2016






4 Rong Tu, Haikou Jian-She Wang, Shanghai Kai Wang, Jinan Xiao-Ping Wang, Xianyang Xiu-Yan Wang, Shanghai Dao-Rong Wang, Yangzhou De-Sheng Wang, Xi an Chun-You Wang, Wuhan Ge Wang, Chongqing Xi-Shan Wang, Harbin Wei-hong Wang, Beijing Zhen-Ning Wang, Shenyang Wai Man Raymond Wong, Hong Kong Chun-Ming Wong, Hong Kong Jian Wu, Shanghai Sheng-Li Wu, Xi an Wu-Jun Wu, Xi an Qing Xia, Chengdu Yan Xin, Shenyang Dong-Ping Xu, Beijing Jian-Min Xu, Shanghai Wei Xu, Changchun Ming Yan, Jinan Xin-Min Yan, Kunming Yi-Qun Yan, Shanghai Feng Yang, Shanghai Yong-Ping Yang, Beijing He-Rui Yao, Guangzhou Thomas Yau, Hong Kong Winnie Yeo, Hong Kong Jing You, Kunming Jian-Qing Yu, Wuhan Ying-Yan Yu, Shanghai Wei-Zheng Zeng, Chengdu Zong-Ming Zhang, Beijing Dian-Liang Zhang, Qingdao Ya-Ping Zhang, Shijiazhuang You-Cheng Zhang, Lanzhou Jian-Zhong Zhang, Beijing Ji-Yuan Zhang, Beijing Hai-Tao Zhao, Beijing Jian Zhao, Shanghai Jian-Hong Zhong, Nanning Ying-Qiang Zhong, Guangzhou Ping-Hong Zhou, Shanghai Yan-Ming Zhou, Xiamen Tong Zhou, Nanchong Li-Ming Zhou, Chengdu Guo-Xiong Zhou, Nantong Feng-Shang Zhu, Shanghai Jiang-Fan Zhu, Shanghai Zhao-Hui Zhu, Beijing Croatia Tajana Filipec Kanizaj, Zagreb Mario Tadic, Zagreb Cuba Damian Casadesus, Havana Czech Jan Bures, Hradec Kralove Marcela Kopacova, Hradec Kralove Otto Kucera, Hradec Kralove Marek Minarik, Prague Pavel Soucek, Prague Miroslav Zavoral, Prague Denmark Vibeke Andersen, Odense E Michael Danielsen, Copenhagen Egypt Mohamed MM Abdel-Latif, Assiut Hussein Atta, Cairo Ashraf Elbahrawy, Cairo Mortada Hassan El-Shabrawi, Cairo Mona El Said El-Raziky, Cairo Elrashdy M Redwan, New Borg Alrab Zeinab Nabil Ahmed Said, Cairo Ragaa HM Salama, Assiut Maha Maher Shehata, Mansoura Estonia Margus Lember, Tartu Tamara Vorobjova, Tartu Finland Marko Kalliomäki, Turku Thomas Kietzmann, Oulu Kaija-Leena Kolho, Helsinki Eija Korkeila, Turku Heikki Makisalo, Helsinki Tanja Pessi, Tampere France Armando Abergel Clermont, Ferrand Elie K Chouillard, Polssy Pierre Cordelier, Toulouse Pascal P Crenn, Garches Catherine Daniel, Lille Fanny Daniel, Paris Cedric Dray, Toulouse Benoit Foligne, Lille Jean-Noel Freund, Strasbourg Hervé Guillou, Toulouse Nathalie Janel, Paris Majid Khatib, Bordeaux Jacques Marescaux, Strasbourg Jean-Claude Marie, Paris Driffa Moussata, Pierre Benite Hang Nguyen, Clermont-Ferrand Hugo Perazzo, Paris Alain L Servin, Chatenay-Malabry Chang Xian Zhang, Lyon Germany Stavros A Antoniou, Monchengladbach Erwin Biecker, Siegburg Hubert E Blum, Freiburg Thomas Bock, Berlin Katja Breitkopf-Heinlein, Mannheim Elke Cario, Essen Güralp Onur Ceyhan, Munich Angel Cid-Arregui, Heidelberg Michael Clemens Roggendorf, München Christoph F Dietrich, Bad Mergentheim Valentin Fuhrmann, Hamburg Nikolaus Gassler, Aachen Andreas Geier, Wuerzburg Markus Gerhard, Munich Anton Gillessen, Muenster Thorsten Oliver Goetze, Offenbach Daniel Nils Gotthardt, Heidelberg Robert Grützmann, Dresden Thilo Hackert, Heidelberg Claus Hellerbrand, Regensburg Harald Peter Hoensch, Darmstadt Jens Hoeppner, Freiburg Richard Hummel, Muenster Jakob Robert Izbicki, Hamburg Gernot Maximilian Kaiser, Essen Matthias Kapischke, Hamburg Michael Keese, Frankfurt Andrej Khandoga, Munich Jorg Kleeff, Munich Alfred Koenigsrainer, Tuebingen Peter Christopher Konturek, Saalfeld Michael Linnebacher, Rostock Stefan Maier, Kaufbeuren Oliver Mann, Hamburg Marc E Martignoni, Munic Thomas Minor, Bonn Oliver Moeschler, Osnabrueck Jonas Mudter, Eutin Sebastian Mueller, Heidelberg Matthias Ocker, Berlin Andreas Ommer, Essen Albrecht Piiper, Frankfurt Esther Raskopf, Bonn Christoph Reichel, Bad Brückenau Elke Roeb, Giessen Udo Rolle, Frankfurt Karl-Herbert Schafer, Zweibrücken Peter Schemmer, Heidelberg Andreas G Schreyer, Regensburg Manuel A Silva, Penzberg Georgios C Sotiropoulos, Essen Ulrike S Stein, Berlin Dirk Uhlmann, Leipzig Michael Weiss, Halle Hong-Lei Weng, Mannheim Karsten Wursthorn, Hamburg Greece Alexandra Alexopoulou, Athens Nikolaos Antonakopoulos, Athens Stelios F Assimakopoulos, Patras Grigoris Chatzimavroudis, Thessaloniki Evangelos Cholongitas, Thessaloniki Gregory Christodoulidis, Larisa George N Dalekos, Larissa Urania Georgopoulou, Athens Eleni Gigi, Thessaloniki III January 1, 2016






5 Stavros Gourgiotis, Athens Leontios J Hadjileontiadis, Thessaloniki Thomas Hyphantis, Ioannina Ioannis Kanellos, Thessaloniki Stylianos Karatapanis, Rhodes Michael Koutsilieris, Athens Spiros D Ladas, Athens Theodoros K Liakakos, Athens Emanuel K Manesis, Athens Spilios Manolakopoulos, Athens Gerassimos John Mantzaris, Athens Athanasios D Marinis, Piraeus Nikolaos Ioannis Nikiteas, Athens Konstantinos X Papamichael, Athens George Sgourakis, Athens Konstantinos C Thomopoulos, Patras Konstantinos Triantafyllou, Athens Christos Triantos, Patras Georgios Zacharakis, Athens Petros Zezos, Alexandroupolis Demosthenes E Ziogas, Ioannina Guatemala Carlos Maria Parellada, Guatemala Hungary Mihaly Boros, Szeged Tamás Decsi, Pécs Gyula Farkas, Szeged Andrea Furka, Debrecen Y vette Mandi, Szeged Peter L Lakatos, Budapest Pal Miheller, Budapest Tamás Molnar, Szeged Attila Olah, Gyor Maria Papp, Debrecen Zoltan Rakonczay, Szeged Ferenc Sipos, Budapest Miklós Tanyi, Debrecen Tibor Wittmann, Szeged Iceland Tryggvi Bjorn Stefánsson, Reykjavík Indiad Brij B Agarwal, New Delhi Deepak N Amarapurkar, Mumbai Shams ul Bari, Srinagar Sriparna Basu, Varanasi Runu Chakravarty, Kolkata Devendra C Desai, Mumbai Nutan D Desai, Mumbai Suneela Sunil Dhaneshwar, Pune Radha K Dhiman, Chandigarh Pankaj Garg, Mohali Uday C Ghoshal, Lucknow Kalpesh Jani, Vadodara Premashis Kar, New Delhi Jyotdeep Kaur, Chandigarh Rakesh Kochhar, Chandigarh Pradyumna K Mishra, Mumbai Asish K Mukhopadhyay, Kolkata Imtiyaz Murtaza, Srinagar P Nagarajan, New Delhi Samiran Nundy, Delhi Gopal Pande, Hyderabad Benjamin Perakath, Vellore Arun Prasad, New Delhi D Nageshwar Reddy, Hyderabad Lekha Saha, Chandigarh Sundeep Singh Saluja, New Delhi Mahesh Prakash Sharma, New Delhi Sadiq Saleem Sikora, Bangalore Sarman Singh, New Delhi Rajeev Sinha, Jhansi Rupjyoti Talukdar, Hyderabad Rakesh Kumar Tandon, New Delhi Narayanan Thirumoorthy, Coimbatore Indonesia David Handojo Muljono, Jakarta Andi Utama, Jakarta Iran Arezoo Aghakhani, Tehran Seyed Mohsen Dehghani, Shiraz Ahad Eshraghian, Shiraz Hossein Khedmat, Tehran Sadegh Massarrat, Tehran Marjan Mohammadi, Tehran Roja Rahimi, Tehran Farzaneh Sabahi, Tehran Majid Sadeghizadeh, Tehran Farideh Siavoshi, Tehran Ireland Gary Alan Bass, Dublin David J Brayden, Dublin Ronan A Cahill, Dublin Glen A Doherty, Dublin Liam J Fanning, Cork Barry Philip McMahon, Dublin RossMcManus, Dublin Dervla O Malley, Cork Sinead M Smith, Dublin Israel Dan Carter, Ramat Gan Jorge-Shmuel Delgado, Metar Eli Magen, Ashdod Nitsan Maharshak, Tel Aviv Shaul Mordechai, Beer Sheva Menachem Moshkowitz, Tel Aviv William Bahij Nseir, Nazareth Shimon Reif, Jerusalem Ram Reifen, Rehovot Ariella Bar-Gil Shitrit, Jerusalem Noam Shussman, Jerusalem Igor Sukhotnik, Haifa Nir Wasserberg, Petach Tiqwa Jacob Yahav, Rehovot Doron Levi Zamir, Gedera Shira Zelber-Sagi, Haifa Romy Zemel, Petach-Tikva Italy Ludovico Abenavoli, Catanzaro Luigi Elio Adinolfi, Naples Carlo Virginio Agostoni, Milan Anna Alisi, Rome Piero Luigi Almasio, Palermo Donato Francesco Altomare, Bari Amedeo Amedei, Florence Pietro Andreone, Bologna Imerio Angriman, Padova Vito Annese, Florence Paolo Aurello, Rome Salavtore Auricchio, Naples Gian Luca Baiocchi, Brescia Gianpaolo Balzano, Milan Antonio Basoli, Rome Gabrio Bassotti, San Sisto Mauro Bernardi, Bologna Alberto Biondi, Rome Ennio Biscaldi, Genova Massimo Bolognesi, Padua Luigi Bonavina, Milano Aldo Bove, Chieti Raffaele Bruno, Pavia Luigi Brusciano, Napoli Giuseppe Cabibbo, Palermo Carlo Calabrese, Bologna Daniele Calistri, Meldola Vincenza Calvaruso, Palermo Lorenzo Camellini, Reggio Emilia Marco Candela, Bologna Raffaele Capasso, Naples Lucia Carulli, Modena Renato David Caviglia, Rome Luigina Cellini, Chieti Giuseppe Chiarioni, Verona Claudio Chiesa, Rome Michele Cicala, Roma Rachele Ciccocioppo, Pavia Sandro Contini, Parma Gaetano Corso, Foggia Renato Costi, Parma Alessandro Cucchetti, Bologna Rosario Cuomo, Napoli Giuseppe Currò, Messina Paola De Nardi, Milano Giovanni D De Palma, Naples Raffaele De Palma, Napoli Giuseppina De Petro, Brescia Valli De Re, Aviano Paolo De Simone, Pisa Giuliana Decorti, Trieste Emanuele Miraglia del Giudice, Napoli Isidoro Di Carlo, Catania Matteo Nicola Dario Di Minno, Naples Massimo Donadelli, Verona Mirko D Onofrio, Verona Maria Pina Dore, Sassari Luca Elli, Milano Massimiliano Fabozzi, Aosta IV January 1, 2016

6 Massimo Falconi, Ancona Ezio Falletto, Turin Silvia Fargion, Milan Matteo Fassan, Verona Gianfranco Delle Fave, Roma Alessandro Federico, Naples Francesco Feo, Sassari Davide Festi, Bologna Natale Figura, Siena Vincenzo Formica, Rome Mirella Fraquelli, Milan Marzio Frazzoni, Modena Walter Fries, Messina Gennaro Galizia, Naples Andrea Galli, Florence Matteo Garcovich, Rome Eugenio Gaudio, Rome Paola Ghiorzo, Genoa Edoardo G Giannini, Genova Luca Gianotti, Monza Maria Cecilia Giron, Padova Alberto Grassi, Rimini Gabriele Grassi, Trieste Francesco Greco, Bergamo Luigi Greco, Naples Antonio Grieco, Rome Fabio Grizzi, Rozzano Laurino Grossi, Pescara Simone Guglielmetti, Milan Tiberiu Hershcovici, Jerusalem Calogero Iacono, Verona Enzo Ierardi, Bari Amedeo Indriolo, Bergamo Raffaele Iorio, Naples Paola Iovino, Salerno Angelo A Izzo, Naples Loreta Kondili, Rome Filippo La Torre, Rome Giuseppe La Torre, Rome Giovanni Latella, L Aquila Salvatore Leonardi, Catania Massimo Libra, Catania Anna Licata, Palermo C armela Loguercio, Naples Amedeo Lonardo, Modena Carmelo Luigiano, Catania Francesco Luzza, Catanzaro Giovanni Maconi, Milano Antonio Macrì, Messina Mariano Malaguarnera, Catania Francesco Manguso, Napoli Tommaso Maria Manzia, Rome Daniele Marrelli, Siena Gabriele Masselli, Rome Sara Massironi, Milan Giuseppe Mazzarella, Avellino Michele Milella, Rome Giovanni Milito, Rome Antonella d Arminio Monforte, Milan Fabrizio Montecucco, Genoa Giovanni Monteleone, Rome Mario Morino, Torino Vincenzo La Mura, Milan Gerardo Nardone, Naples Riccardo Nascimbeni, Brescia Gabriella Nesi, Florence Giuseppe Nigri, Rome Erica Novo, Turin Veronica Ojetti, Rome Michele Orditura, Naples Fabio Pace, Seriate Lucia Pacifico, Rome Omero Alessandro Paoluzi, Rome Valerio Pazienza, San Giovanni Rotondo Rinaldo Pellicano, Turin Adriano M Pellicelli, Rome Nadia Peparini, Ciampino Mario Pescatori, Rome Antonio Picardi, Rome Alberto Pilotto, Padova Alberto Piperno, Monza Anna Chiara Piscaglia, Rome Maurizio Pompili, Rome Francesca Romana Ponziani, Rome Cosimo Prantera, Rome Girolamo Ranieri, Bari Carlo Ratto, Tome Barbara Renga, Perugia Alessandro Repici, Rozzano Maria Elena Riccioni, Rome Lucia Ricci-Vitiani, Rome Luciana Rigoli, Messina Mario Rizzetto, Torino Ballarin Roberto, Modena Roberto G Romanelli, Florence Claudio Romano, Messina Luca Roncucci, Modena Cesare Ruffolo, Treviso L ucia Sacchetti, Napoli Rodolfo Sacco, Pisa Lapo Sali, Florence Romina Salpini, Rome Giulio Aniello, Santoro Treviso Armando Santoro, Rozzano Edoardo Savarino, Padua Marco Senzolo, Padua Annalucia Serafino, Rome Giuseppe S Sica, Rome Pierpaolo Sileri, Rome Cosimo Sperti, Padua Vincenzo Stanghellini, Bologna Cristina Stasi, Florence Gabriele Stocco, Trieste Roberto Tarquini, Florence Mario Testini, Bari Guido Torzilli, Milan Guido Alberto Massimo, Tiberio Brescia Giuseppe Toffoli, Aviano Alberto Tommasini, Trieste Francesco Tonelli, Florence Cesare Tosetti Porretta, Terme Lucio Trevisani, Cona Guglielmo M Trovato, Catania Mariapia Vairetti, Pavia Luca Vittorio Valenti, Milano Mariateresa T Ventura, Bari Giuseppe Verlato, Verona Marco Vivarelli, Ancona Giovanni Li Volti, Catania Giuseppe Zanotti, Padua Vincenzo Zara, Lecce Gianguglielmo Zehender, Milan Anna Linda Zignego, Florence Rocco Antonio Zoccali, Messina Angelo Zullo, Rome Japan Yasushi Adachi, Sapporo Takafumi Ando, Nagoya Masahiro Arai, Tokyo Makoto Arai, Chiba Takaaki Arigami, Kagoshima Itaru Endo,Yokohama Munechika Enjoji, Fukuoka Shunji Fujimori, Tokyo Yasuhiro Fujino, Akashi Toshiyoshi Fujiwara, Okayama Yosuke Fukunaga, Tokyo Toshio Fukusato, Tokyo Takahisa Furuta, Hamamatsu Osamu Handa, Kyoto Naoki Hashimoto, Osaka Yoichi Hiasa, Toon Masatsugu Hiraki, Saga Satoshi Hirano, Sapporo Keiji Hirata, Fukuoka Toru Hiyama, Higashihiroshima Akira Hokama, Nishihara Shu Hoteya, Tokyo Masao Ichinose, Wakayama Tatsuya Ide, Kurume Masahiro Iizuka, Akita Toshiro Iizuka, Tokyo Kenichi Ikejima, Tokyo Tetsuya Ikemoto, Tokushima Hiroyuki Imaeda, Saitama Atsushi Imagawa, Kan-onji Hiroo Imazu, Tokyo Shuji Isaji, Tsu Toru Ishikawa, Niigata Toshiyuki Ishiwata, Tokyo Soichi Itaba, Kitakyushu Yoshiaki Iwasaki, Okayama Tatehiro Kagawa, Isehara Satoru Kakizaki, Maebashi Naomi Kakushima, Shizuoka Terumi Kamisawa, Tokyo Akihide Kamiya, Isehara Osamu Kanauchi, Tokyo Tatsuo Kanda, Chiba Shin Kariya, Okayama Shigeyuki Kawa, Matsumoto Takumi Kawaguchi, Kurume Takashi Kawai, Tokyo Soo Ryang Kim, Kobe Shinsuke Kiriyama, Gunma Tsuneo Kitamura, Urayasu Masayuki Kitano, Osakasayama Hirotoshi Kobayashi, Tokyo Hironori Koga, Kurume Takashi Kojima, Sapporo Satoshi Kokura, Kyoto Shuhei Komatsu, Kyoto Tadashi Kondo, Tokyo Yasuteru Kondo, Sendai Yasuhiro Kuramitsu, Yamaguchi Yukinori Kurokawa, Osaka Shin Maeda, Yokohama Koutarou Maeda, Toyoake V January 1, 2016











7 Hitoshi Maruyama, Chiba Atsushi Masamune, Sendai Hiroyuki Matsubayashi, Suntogun Akihisa Matsuda, Inzai Hirofumi Matsui, Tsukuba Akira Matsumori, Kyoto Yoichi Matsuo, Nagoya Y Matsuzaki, Ami Toshihiro Mitaka, Sapporo Kouichi Miura, Akita Shinichi Miyagawa, Matumoto Eiji Miyoshi, Suita Toru Mizuguchi, Sapporo Nobumasa Mizuno, Nagoya Zenichi Morise, Nagoya Tomohiko Moriyama, Fukuoka Kunihiko Murase, Tusima Michihiro Mutoh, Tsukiji Akihito Nagahara, Tokyo Hikaru Nagahara, Tokyo Hidenari Nagai, Tokyo Koichi Nagata, Shimotsuke-shi Masaki Nagaya, Kawasaki Hisato Nakajima, Nishi-Shinbashi Toshifusa Nakajima, Tokyo Hiroshi Nakano, Kawasaki Hiroshi Nakase, Kyoto Toshiyuki Nakayama, Nagasaki Takahiro Nakazawa, Nagoya Shoji Natsugoe, Kagoshima City Tsutomu Nishida, Suita Shuji Nomoto, Naogya Sachiyo Nomura, Tokyo Takeshi Ogura, Takatsukishi Nobuhiro Ohkohchi, Tsukuba Toshifumi Ohkusa, Kashiwa Hirohide Ohnishi, Akita Teruo Okano, Tokyo Satoshi Osawa, Hamamatsu Motoyuki Otsuka, Tokyo Michitaka Ozaki, Sapporo Satoru Saito, Yokohama Naoaki Sakata, Sendai Ken Sato, Maebashi Toshiro Sato, Tokyo Tomoyuki Shibata, Toyoake Tomohiko Shimatani, Kure Yukihiro Shimizu, Nanto Tadashi Shimoyama, Hirosaki Masayuki Sho, Nara Ikuo Shoji, Kobe Atsushi Sofuni, Tokyo Takeshi Suda, Niigata M Sugimoto, Hamamatsu Ken Sugimoto, Hamamatsu Haruhiko Sugimura, Hamamatsu Shoichiro Sumi, Kyoto Hidekazu Suzuki, Tokyo Masahiro Tajika, Nagoya Hitoshi Takagi, Takasaki Toru Takahashi, Niigata Yoshihisa Takahashi, Tokyo Shinsuke Takeno, Fukuoka Akihiro Tamori, Osaka Kyosuke Tanaka, Tsu Shinji Tanaka, Hiroshima Atsushi Tanaka, Tokyo Yasuhito Tanaka, Nagoya Shinji Tanaka, Tokyo Minoru Tomizawa, Yotsukaido City Kyoko Tsukiyama-Kohara, Kagoshima Takuya Watanabe, Niigata Kazuhiro Watanabe, Sendai Satoshi Yamagiwa, Niigata Takayuki Yamamoto, Yokkaichi Hiroshi Yamamoto, Otsu Kosho Yamanouchi, Nagasaki Ichiro Yasuda, Gifu Yutaka Yata, Maebashi-city Shin-ichi Yokota, Sapporo Norimasa Yoshida, Kyoto Hiroshi Yoshida, Tama-City Hitoshi Yoshiji, Kashihara Kazuhiko Yoshimatsu, Tokyo Kentaro Yoshioka, Toyoake Nobuhiro Zaima, Nara Jordan Khaled Ali Jadallah, Irbid Kuwait Islam Khan, Kuwait Lebanon Bassam N Abboud, Beirut Kassem A Barada, Beirut Marwan Ghosn, Beirut Iyad A Issa, Beirut Fadi H Mourad, Beirut AIa Sharara, Beirut Rita Slim, Beirut Lithuania Antanas Mickevicius, Kaunas Malaysia Huck Joo Tan, Petaling Jaya Mexico Richard A Awad, Mexico City Carlos R Camara-Lemarroy, Monterrey Norberto C Chavez-Tapia, Mexico City Wolfgang Gaertner, Mexico City Diego Garcia-Compean, Monterrey Arturo Panduro, Guadalajara OT Teramoto-Matsubara, Mexico City Felix Tellez-Avila, Mexico City Omar Vergara-Fernandez, Mexico City Saúl Villa-Trevino, Cuidad de México Morocco Samir Ahboucha, Khouribga Netherlands Robert J de Knegt, Rotterdam Tom Johannes Gerardus Gevers, Nijmegen Menno Hoekstra, Leiden BW Marcel Spanier, Arnhem Karel van Erpecum, Utrecht New Zealand Leo K Cheng, Auckland Andrew Stewart Day, Christchurch Jonathan Barnes Koea, Auckland Max Petrov, Auckland Nigeria Olufunmilayo Adenike Lesi, Lagos Jesse Abiodun Otegbayo, Ibadan Stella Ifeanyi Smith, Lagos Norway Trond Berg, Oslo Trond Arnulf Buanes, Krokkleiva Thomas de Lange, Rud Magdy El-Salhy, Stord Rasmus Goll, Tromso Dag Arne Lihaug Hoff, Aalesund Pakistan Zaigham Abbas, Karachi Usman A Ashfaq, Faisalabad Muhammad Adnan Bawany, Hyderabad Muhammad Idrees, Lahore Saeed Sadiq Hamid, Karachi Yasir Waheed, Islamabad Poland Thomas Brzozowski, Cracow Magdalena Chmiela, Lodz Krzysztof Jonderko, Sosnowiec Anna Kasicka-Jonderko, Sosnowiec Michal Kukla, Katowice Tomasz Hubert Mach, Krakow Agata Mulak, Wroclaw Danuta Owczarek, Kraków Piotr Socha, Warsaw Piotr Stalke, Gdansk Julian Teodor Swierczynski, Gdansk Anna M Zawilak-Pawlik, Wroclaw Portugal Marie Isabelle Cremers, Setubal Ceu Figueiredo, Porto Ana Isabel Lopes, LIsbon M Paula Macedo, Lisboa Ricardo Marcos, Porto Rui T Marinho, Lisboa Guida Portela-Gomes, Estoril VI January 1, 2016








8 Filipa F Vale, Lisbon Puerto Rico Caroline B Appleyard, Ponce Qatar Abdulbari Bener, Doha Romania Mihai Ciocirlan, Bucharest Dan LucianDumitrascu, Cluj-Napoca Carmen Fierbinteanu-Braticevici, Bucharest Romeo G Mihaila, Sibiu Lucian Negreanu, Bucharest Adrian Saftoiu, Craiova Andrada Seicean, Cluj-Napoca Ioan Sporea, Timisoara Letiţia Adela Maria Streba, Craiova Anca Trifan, Iasi Russia Victor Pasechnikov, Stavropol Vasiliy Ivanovich Reshetnyak, Moscow Vitaly Skoropad, Obninsk Saudi Arabia Abdul-Wahed N Meshikhes, Dammam M Ezzedien Rabie, Khamis Mushait Singapore Brian KP Goh, Singapore Richie Soong, Singapore Ker-Kan Tan, Singapore Kok-Yang Tan, Singapore Yee-Joo Tan, Singapore Mark Wong, Singapore Hong Ping Xia, Singapore Slovenia Matjaz Homan, Ljubljana Martina Perse, Ljubljana South Korea Sang Hoon Ahn, Seoul Seung Hyuk Baik, Seoul Soon Koo Baik, Wonju Soo-Cheon Chae, Iksan Byung-Ho Choe, Daegu Suck Chei Choi, Iksan Hoon Jai Chun, Seoul Yeun-Jun Chung, Seoul Young-Hwa Chung, Seoul Ki-Baik Hahm, Seongnam Sang Young Han, Busan Seok Joo Han, Seoul Seung-Heon Hong, Iksan Jin-Hyeok Hwang, Seoungnam Jeong Won Jang, Seoul Jin-Young Jang, Seoul Dae-Won Jun, Seoul Young Do Jung, Kwangju Gyeong Hoon Kang, Seoul Sung-Bum Kang, Seoul Koo Jeong Kang, Daegu Ki Mun Kang, Jinju Chang Moo Kang, Seodaemun-gu Gwang Ha Kim, Busan Sang Soo Kim, Goyang-si Jin Cheon Kim, Seoul Tae Il Kim, Seoul Jin Hong Kim, Suwon Kyung Mo Kim, Seoul Kyongmin Kim, Suwon Hyung-Ho Kim, Seongnam Seoung Hoon Kim, Goyang Sang Il Kim, Seoul Hyun-Soo Kim, Wonju Jung Mogg Kim, Seoul Dong Yi Kim, Gwangju Kyun-Hwan Kim, Seoul Jong-Han Kim, Ansan Sang Wun Kim, Seoul Ja-Lok Ku, Seoul Kyu Taek Lee, Seoul Hae-Wan Lee, Chuncheon Inchul Lee, Seoul Jung Eun Lee, Seoul Sang Chul Lee, Daejeon Song Woo Lee, Ansan-si Hyuk-Joon Lee, Seoul Seong-Wook Lee, Yongin Kil Yeon Lee, Seoul Jong-Inn Lee, Seoul Kyung A Lee, Seoul Jong-Baeck Lim, Seoul Eun-Yi Moon, Seoul SH Noh, Seoul Seung Woon Paik, Seoul Won Sang Park, Seoul Sung-Joo Park, Iksan Kyung Sik Park, Daegu Se Hoon Park, Seoul Yoonkyung Park, Gwangju Seung-Wan Ryu, Daegu Il Han Song, Cheonan Myeong Jun Song, Daejeon Yun Kyoung Yim, Daejeon Dae-Yeul Yu Daejeon Spain Mariam Aguas, Valencia Raul J Andrade, Málaga Antonio Arroyo, Elche Josep M Bordas, Barcelona Lisardo Boscá, Madrid Ricardo Robles Campos, Murcia Jordi Camps, Reus Carlos Cervera Barcelona Alfonso Clemente, Granada Pilar Codoner-Franch, Valencia Fernando J Corrales, Pamplona Fermin Sánchez de Medina, Granada Alberto Herreros de Tejada, Majadahonda Enrique de-madaria, Alicante JE Dominguez-Munoz, Santiago de Compostela Vicente Felipo, Valencia CM Fernandez-Rodriguez, Madrid Carmen Frontela-Saseta, Murcia Julio Galvez, Granada Maria Teresa García, Vigo MI Garcia-Fernandez, Málaga Emilio Gonzalez-Reimers, La Laguna Marcel Jimenez, Bellaterra Angel Lanas, Zaragoza Juan Ramón Larrubia, Guadalajara Antonio Lopez-Sanroman, Madrid Vicente Lorenzo-Zuniga, Badalona Alfredo J Lucendo, Tomelloso Vicenta Soledad Martinez-Zorzano, Vigo José Manuel Martin-Villa, Madrid Julio Mayol, Madrid Manuel Morales-Ruiz, Barcelona Alfredo Moreno-Egea, Murcia Albert Pares, Barcelona Maria Pellise, Barcelona José Perea, Madrid Miguel Angel Plaza, Zaragoza María J Pozo, Cáceres Enrique Quintero, La Laguna Jose M Ramia, Madrid Francisco Rodriguez-Frias, Barcelona Silvia Ruiz-Gaspa, Barcelona Xavier Serra-Aracil, Barcelona Vincent Soriano, Madrid Javier Suarez, Pamplona Carlos Taxonera, Madrid M Isabel Torres, Jaén Manuel Vazquez-Carrera, Barcelona Benito Velayos, Valladolid Silvia Vidal, Barcelona Sri Lanka Arjuna Priyadarsin De Silva, Colombo Sudan Ishag Adam, Khartoum Sweden Roland G Andersson, Lund Bergthor Björnsson, Linkoping Johan Christopher Bohr, Örebro Mauro D Amato, Stockholm Thomas Franzen, Norrkoping Evangelos Kalaitzakis, Lund Riadh Sadik, Gothenburg Per Anders Sandstrom, Linkoping Ervin Toth, Malmö Konstantinos Tsimogiannis, Vasteras Apostolos V Tsolakis, Uppsala VII January 1, 2016





9 Switzerland Gieri Cathomas, Liestal Jean Louis Frossard, Geneve Christian Toso, Geneva Stephan Robert Vavricka, Zurich Dominique Velin, Lausanne Thailand Thawatchai Akaraviputh, Bangkok P Yoysungnoen Chintana, Pathumthani Veerapol Kukongviriyapan, Muang Vijittra Leardkamolkarn, Bangkok Varut Lohsiriwat, Bangkok Somchai Pinlaor, Khaon Kaen D Wattanasirichaigoon, Bangkok Trinidad and Tobago B Shivananda Nayak, Mount Hope Tunisia Ibtissem Ghedira, Sousse Lilia Zouiten-Mekki, Tunis Turkey Inci Alican, Istanbul Mustafa Altindis, Sakarya Mutay Aslan, Antalya Oktar Asoglu, Istanbul Yasemin Hatice Balaban, Istanbul Metin Basaranoglu, Ankara Yusuf Bayraktar, Ankara Süleyman Bayram, Adiyaman Ahmet Bilici, Istanbul Ahmet Sedat Boyacioglu, Ankara Züleyha Akkan Cetinkaya, Kocaeli Cavit Col, Bolu Yasar Colak, Istanbul Cagatay Erden Daphan, Kirikkale Mehmet Demir, Hatay Ahmet Merih Dobrucali, Istanbul Gülsüm Ozlem Elpek, Antalya Ayse Basak Engin, Ankara Eren Ersoy, Ankara Osman Ersoy, Ankara Yusuf Ziya Erzin, Istanbul Mukaddes Esrefoglu, Istanbul Levent Filik, Ankara Ozgur Harmanci, Ankara Koray Hekimoglu, Ankara Abdurrahman Kadayifci, Gaziantep Cem Kalayci, Istanbul Selin Kapan, Istanbul Huseyin Kayadibi, Adana Sabahattin Kaymakoglu, Istanbul Metin Kement, Istanbul Mevlut Kurt, Bolu Resat Ozaras, Istanbul Elvan Ozbek, Adapazari Cengiz Ozcan, Mersin Hasan Ozen, Ankara Halil Ozguc, Bursa Mehmet Ozturk, Izmir Orhan V Ozkan, Sakarya Semra Paydas, Adana Ozlem Durmaz Suoglu, Istanbul Ilker Tasci, Ankara Müge Tecder-ünal, Ankara Mesut Tez, Ankara Serdar Topaloglu, Trabzon Murat Toruner, Ankara Gokhan Tumgor, Adana Oguz Uskudar, Adana Mehmet Yalniz, Elazig Mehmet Yaman, Elazig Veli Yazisiz, Antalya Yusuf Yilmaz, Istanbul Ozlem Yilmaz, Izmir Oya Yucel, Istanbul Ilhami Yuksel, Ankara United Kingdom Nadeem Ahmad Afzal, Southampton Navneet K Ahluwalia, Stockport Yeng S Ang, Lancashire Ramesh P Arasaradnam, Coventry Ian Leonard Phillip Beales, Norwich John Beynon, Swansea Barbara Braden, Oxford Simon Bramhall, Birmingham Geoffrey Burnstock, London Ian Chau, Sutton Thean Soon Chew, London Helen G Coleman, Belfast Anil Dhawan, London Sunil Dolwani, Cardiff Piers Gatenby, London Anil T George, London Pasquale Giordano, London Paul Henderson, Edinburgh Georgina Louise Hold, Aberdeen Stefan Hubscher, Birmingham Robin D Hughes, London Nusrat Husain, Manchester Matt W Johnson, Luton Konrad Koss, Macclesfield Anastasios Koulaouzidis, Edinburgh Simon Lal, Salford John S Leeds, Aberdeen JK K Limdi, Manchester Hongxiang Liu, Cambridge Michael Joseph McGarvey, London Michael Anthony Mendall, London Alexander H Mirnezami, Southampton J Bernadette Moore, Guildford Claudio Nicoletti, Norwich Savvas Papagrigoriadis, London Sylvia LF Pender, Southampton David Mark Pritchard, Liverpool James A Ross, Edinburgh Kamran Rostami, Worcester Xiong Z Ruan, London Frank I Tovey, London Dhiraj Tripathi, Birmingham Vamsi R Velchuru, Great Yarmouth Nicholas T Ventham, Edinburgh Diego Vergani, London Jack Westwood Winter, Glasgow Terence Wong, London Ling Yang, Oxford United States Daniel E Abbott, Cincinnati Ghassan K Abou-Alfa, New York Julian Abrams, New York David William Adelson, Los Angeles Jonathan Steven Alexander, Shreveport Tauseef Ali, Oklahoma City Mohamed R Ali, Sacramento Rajagopal N Aravalli, Minneapolis Hassan Ashktorab, Washington Shashi Bala, Worcester Charles F Barish, Raleigh P Patrick Basu, New York Robert L Bell, Berkeley Heights David Bentrem, Chicago Henry J Binder, New Haven Joshua Bleier, Philadelphia Wojciech Blonski, Johnson City Kenneth Boorom, Corvallis Brian Boulay, Chicago Carla W Brady, Durham Kyle E Brown, Iowa City Adeel A Butt, Pittsburgh Weibiao Cao, Providence Andrea Castillo, Cheney Fernando J Castro, Weston Adam S Cheifetz, Boston Xiaoxin Luke Chen, Durham Ramsey Cheung, Palo Alto Parimal Chowdhury, Little Rock Edward John Ciaccio, New York Dahn L Clemens, Omaha Yingzi Cong, Galveston Laura Iris Cosen-Binker, Boston Joseph John Cullen, Lowa Mark J Czaja, Bronx Mariana D Dabeva, Bronx Christopher James Damman, Seattle Isabelle G De Plaen, Chicago Punita Dhawan, Nashville Hui Dong, La Jolla Wael El-Rifai, Nashville Sukru H Emre, New Haven Paul Feuerstadt, Hamden Josef E Fischer, Boston Laurie N Fishman, Boston Joseph Che Forbi, Atlanta Temitope Foster, Atlanta Amy E Foxx-Orenstein, Scottsdale Daniel E Freedberg, New York Shai Friedland, Palo Alto Virgilio George, Indianapolis Ajay Goel, Dallas Oliver Grundmann, Gainesville Stefano Guandalini, Chicago Chakshu Gupta, St. Joseph Grigoriy E Gurvits, New York VIII January 1, 2016


10 Xiaonan Han, Cincinnati Mohamed Hassan, Jackson Martin Hauer-Jensen, Little Rock Koichi Hayano, Boston Yingli Hee, Atlanta Samuel B Ho, San Diego Jason Ken Hou, Houston Lifang Hou, Chicago K-Qin Hu, Orange Jamal A Ibdah, Columbia Robert Thomas Jensen, Bethesda Huanguang Charlie Jia, Gainesville Rome Jutabha, Los Angeles Andreas M Kaiser, Los Angeles Avinash Kambadakone, Boston David Edward Kaplan, Philadelphia Randeep Kashyap, Rochester Rashmi Kaul, Tulsa Ali Keshavarzian, Chicago Amir Maqbul Khan, Marshall Nabeel Hasan Khan, New Orleans Sahil Khanna, Rochester Kusum K Kharbanda, Omaha Hyun Sik Kim, Pittsburgh Joseph Kim, Duarte Jae S Kim, Gainesville Miran Kim, Providence Timothy R Koch, Washington Burton I Korelitz, New York Betsy Kren, Minneapolis Shiu-Ming Kuo, Buffalo Michelle Lai, Boston Andreas Larentzakis, Boston Edward Wolfgang Lee, Los Angeles Daniel A Leffler, Boston Michael Leitman, New York Suthat Liangpunsakul, Indianapolis Joseph K Lim, New Haven Elaine Y Lin, Bronx Henry C Lin, Albuquerque Rohit Loomba, La Jolla James David Luketich, Pittsburgh Li Ma, Stanford Mohammad F Madhoun, Oklahoma City Thomas C Mahl, Buffalo Ashish Malhotra, Bettendorf Pranoti Mandrekar, Worcester John Marks, Wynnewood Wendy M Mars, Pittsburgh Julien Vahe Matricon, San Antonio Craig J McClain, Louisville Tamir Miloh, Phoenix Ayse Leyla Mindikoglu, Baltimore Huanbiao Mo, Denton Klaus Monkemuller, Birmingham John Morton, Stanford Adnan Muhammad, Tampa Michael J Nowicki, Jackson Patrick I Okolo, Baltimore Giusepp Orlando, Winston Salem Natalia A Osna, Omaha Virendra N Pandey, Newark Mansour A Parsi, Cleveland Michael F Picco, Jacksonville Daniel S Pratt, Boston Xiaofa Qin, Newark Janardan K Reddy, Chicago Victor E Reyes, Galveston Jon Marc Rhoads, Houston Giulia Roda, New York Jean-Francois Armand Rossignol, Tampa Paul A Rufo, Boston Madhusudana Girija Sanal, New York Miguel Saps, Chicago Sushil Sarna, Galveston Ann O Scheimann, Baltimore Bernd Schnabl, La Jolla Matthew J Schuchert, Pittsburgh Ekihiro Seki, La Jolla Chanjuan Shi, Nashville David Quan Shih, Los Angeles Shadab A Siddiqi, Orlando William B Silverman, Iowa City Shashideep Singhal, New York Bronislaw L Slomiany, Newark Steven F Solga, Bethlehem Byoung-Joon Song, Bethesda Dario Sorrentino, Roanoke Scott R Steele, Fort Lewis Branko Stefanovic, Tallahassee Arun Swaminath, New York Kazuaki Takabe, Richmond Naoki Tanaka, Bethesda Hans Ludger Tillmann, Durham George Triadafilopoulos, Stanford John Richardson Thompson, Nashville Andrew Ukleja, Weston Miranda AL van Tilburg, Chapel Hill Gilberto Vaughan, Atlanta Vijayakumar Velu, Atlanta Gebhard Wagener, New York Kasper Saonun Wang, Los Angeles Xiangbing Wang, New Brunswick Daoyan Wei, Houston Theodore H Welling, Ann Arbor C Mel Wilcox, Birmingham Jacqueline Lee Wolf, Boston Laura Ann Woollett, Cincinnati Harry Hua-Xiang Xia, East Hanover Wen Xie, Pittsburgh Guang Yu Yang, Chicago Michele T Yip-Schneider, Indianapolis Sam Zakhari, Bethesda Kezhong Zhang, Detroit Huiping Zhou, Richmond Xiao-Jian Zhou, Cambridge Richard Zubarik, Burlington Venezuela Miguel Angel Chiurillo, Barquisimeto Vietnam Van Bang Nguyen, Hanoi IX January 1, 2016
11 S Contents Weekly Volume 22 Number 14 April 14, 2016 TOPIC HIGHLIGHT 3701 From prolonging life to prolonging working life: Tackling unemployment among liver-transplant recipients Åberg F 3712 Elastography for the pancreas: Current status and future perspective Kawada N, Tanaka S REVIEW 3725 Biomarkers for detection of alcohol consumption in liver transplantation Staufer K, Yegles M ORIGINAL ARTICLE Basic Study 3735 Phosphatase and tensin homolog is a differential diagnostic marker between nonalcoholic and alcoholic fatty liver disease Sanchez-Pareja A, Clément S, Peyrou M, Spahr L, Negro F, Rubbia-Brandt L, Foti M 3746 S-adenosyl-L-methionine modifies antioxidant-enzymes, glutathione-biosynthesis and methionine adenosyltransferases-1/2 in hepatitis C virus-expressing cells Lozano-Sepulveda SA, Bautista-Osorio E, Merino-Mascorro JA, Varela-Rey M, Muñoz-Espinosa LE, Cordero-Perez P, Martinez-Chantar ML, Rivas-Estilla AM 3758 Evaluation of therapeutic effectiveness of 131 I-antiEGFR-BSA-PCL in a mouse model of colorectal cancer Li W, Ji YH, Li CX, Liu ZY, Li N, Fang L, Chang J, Tan J 3769 Hypothalamic paraventricular nucleus stimulation reduces intestinal injury in rats with ulcerative colitis Deng QJ, Deng DJ, Che J, Zhao HR, Yu JJ, Lu YY Case Control Study 3777 Multi-locus genetic risk score predicts risk for Crohn's disease in Slovenian population Zupančič K, Skok K, Repnik K, Weersma RK, Potočnik U, Skok P Retrospective Cohort Study 3785 Characteristics and outcomes of chronic liver disease patients with acute deteriorated liver function by severity of underlying liver disease Hong YS, Sinn DH, Gwak GY, Cho J, Kang D, Paik YH, Choi MS, Lee JH, Koh KC, Paik SW April 14, 2016 Volume 22 Issue 14
12 Contents World Journal of Gastroenterology Volume 22 Number 14 April 14, 2016 Retrospective Study 3793 Multicenter study of endoscopic preoperative biliary drainage for malignant distal biliary obstruction Sasahira N, Hamada T, Togawa O, Yamamoto R, Iwai T, Tamada K, Kawaguchi Y, Shimura K, Koike T, Yoshida Y, Sugimori K, Ryozawa S, Kakimoto T, Nishikawa K, Kitamura K, Imamura T, Mizuide M, Toda N, Maetani I, Sakai Y, Itoi T, Nagahama M, Nakai Y, Isayama H 3803 High-dose hepatitis B immunoglobulin therapy in hepatocellular carcinoma with hepatitis B virus-dna/ hepatitis B e antigen-positive patients after living donor liver transplantation Lee EC, Kim SH, Lee SD, Park H, Lee SA, Park SJ 3813 Vascularizing lymph node dissection for advanced gastric cancer: A single-institution experience Han FH, Zhou SN, Li HM, He YL, Zhan WH 3821 Early enteral nutrition vs parenteral nutrition following pancreaticoduodenectomy: Experience from a single center Lu JW, Liu C, Du ZQ, Liu XM, Lv Y, Zhang XF 3829 Oncogenic Wnt3a expression as an estimable prognostic marker for hepatocellular carcinoma Pan LH, Yao M, Cai Y, Gu JJ, Yang XL, Wang L, Yao DF Clinical Trials Study 3837 Endoscopic management of unresectable malignant gastroduodenal obstruction with a nitinol uncovered metal stent: A prospective Japanese multicenter study Sasaki R, Sakai Y, Tsuyuguchi T, Nishikawa T, Fujimoto T, Mikami S, Sugiyama H, Yokosuka O Observational Study 3845 Autofluorescence imaging endoscopy can distinguish non-erosive reflux disease from functional heartburn: A pilot study Luo X, Guo XX, Wang WF, Peng LH, Yang YS, Uedo N 3852 Integrin αvβ6 and matrix metalloproteinase 9 correlate with survival in gastric cancer Lian PL, Liu Z, Yang GY, Zhao R, Zhang ZY, Chen YG, Zhuang ZN, Xu KS Prospective Study 3860 Cost-effectiveness of Crohn's disease post-operative care Wright EK, Kamm MA, Dr Cruz P, Hamilton AL, Ritchie KJ, Bell SJ, Brown SJ, Connell WR, Desmond PV, Liew D CASE REPORT 3869 Ileo-right hemi-colonic cervical pull-up on a non-supercharged ileocolic arterial pedicle: A technical and case report Weiss ARR, Hackl C, Soeder Y, Schlitt HJ, Dahlke MH II April 14, 2016 Volume 22 Issue 14
13 Contents World Journal of Gastroenterology Volume 22 Number 14 April 14, Rare cause of odynophagia: Giant esophageal ulcer Veroux M, Aprile G, Amore FF, Corona D, Giaquinta A, Veroux P 3879 Case of metachronous bilateral isolated adrenal metastasis from colorectal adenocarcinoma and review of the literature Liu YY, Chen ZH, Zhai ET, Yang J, Xu JB, Cai SR, Song W III April 14, 2016 Volume 22 Issue 14
14 Contents World Journal of Gastroenterology Volume 22 Number 14 April 14, 2016 ABOUT COVER Editorial board member of World Journal of Gastroenterology, Mohamed Hassan, PhD, Lecturer, Department of Pathology and Full member, Cancer Institute, University of Mississippi Medical Center, Jackson, MS 39216, United States AIMS AND SCOPE World Journal of Gastroenterology (World J Gastroenterol, WJG, print ISSN , online ISSN , DOI: ) is a peer-reviewed open access journal. WJG was established on October 1, It is published weekly on the 7 th, 14 th, 21 st, and 28 th each month. The WJG Editorial Board consists of 1376 experts in gastroenterology and hepatology from 68 countries. The primary task of WJG is to rapidly publish high-quality original articles, reviews, and commentaries in the fields of gastroenterology, hepatology, gastrointestinal endoscopy, gastrointestinal surgery, hepatobiliary surgery, gastrointestinal oncology, gastrointestinal radiation oncology, gastrointestinal imaging, gastrointestinal interventional therapy, gastrointestinal infectious diseases, gastrointestinal pharmacology, gastrointestinal pathophysiology, gastrointestinal pathology, evidence-based medicine in gastroenterology, pancreatology, gastrointestinal laboratory medicine, gastrointestinal molecular biology, gastrointestinal immunology, gastrointestinal microbiology, gastrointestinal genetics, gastrointestinal translational medicine, gastrointestinal diagnostics, and gastrointestinal therapeutics. WJG is dedicated to become an influential and prestigious journal in gastroenterology and hepatology, to promote the development of above disciplines, and to improve the diagnostic and therapeutic skill and expertise of clinicians. INDEXING/ABSTRACTING World Journal of Gastroenterology is now indexed in Current Contents /Clinical Medicine, Science Citation Index Expanded (also known as SciSearch ), Journal Citation Reports, Index Medicus, MEDLINE, PubMed, PubMed Central, Digital Object Identifier, and Directory of Open Access Journals. According to the 2014 Journal Citation Reports released by Thomson Reuters (ISI), the 2014 impact factor for WJG is 2.369, ranking 41 among 76 journals in gastroenterology and hepatology, quartile in category Q2. FLYLEAF I-IX Editorial Board EDITORS FOR THIS ISSUE Responsible Assistant Editor: Xiang Li Responsible Electronic Editor: Shuai Ma Proofing Editor-in-Chief: Lian-Sheng Ma Responsible Science Editor: Yuan Qi Proofing Editorial Office Director: Jin-Lei Wang NAME OF JOURNAL World Journal of Gastroenterology ISSN ISSN (print) ISSN (online) LAUNCH DATE October 1, 1995 FREQUENCY Weekly EDITORS-IN-CHIEF Damian Garcia-Olmo, MD, PhD, Doctor, Professor, Surgeon, Department of Surgery, Universidad Autonoma de Madrid; Department of General Surgery, Fundacion Jimenez Diaz University Hospital, Madrid 28040, Spain Stephen C Strom, PhD, Professor, Department of Laboratory Medicine, Division of Pathology, Karolinska Institutet, Stockholm , Sweden Andrzej S Tarnawski, MD, PhD, DSc (Med), Professor of Medicine, Chief Gastroenterology, VA Long Beach Health Care System, University of California, Irvine, CA, 5901 E. Seventh Str., Long Beach, CA 90822, United States EDITORIAL OFFICE Jin-Lei Wang, Director Xiu-Xia Song, Vice Director World Journal of Gastroenterology Room 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing , China Telephone: Fax: editorialoffice@wjgnet.com Help Desk: PUBLISHER Baishideng Publishing Group Inc 8226 Regency Drive, Pleasanton, CA 94588, USA Telephone: Fax: bpgoffice@wjgnet.com Help Desk: PUBLICATION DATE April 14, 2016 COPYRIGHT 2016 Baishideng Publishing Group Inc. Articles published by this Open-Access journal are distributed under the terms of the Creative Commons Attribution Noncommercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. SPECIAL STATEMENT All articles published in journals owned by the Baishideng Publishing Group (BPG) represent the views and opinions of their authors, and not the views, opinions or policies of the BPG, except where otherwise explicitly indicated. INSTRUCTIONS TO AUTHORS Full instructions are available online at wjgnet.com/bpg/g_info_ htm ONLINE SUBMISSION IV April 14, 2016 Volume 22 Issue 14
15 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved Liver Transplantation: Global view TOPIC HIGHLIGHT From prolonging life to prolonging working life: Tackling unemployment among liver-transplant recipients Fredrik Åberg Fredrik Åberg, Transplantation and Liver Surgery Clinic, HUCH Meilahti Hospital, Helsinki University, HUS, Finland Author contributions: Åberg F solely contributed to this work. Conflict-of-interest statement: The author declares no conflict of interests for this article. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Fredrik Åberg, MD, Transplantation and Liver Surgery Clinic, HUCH Meilahti Hospital, PB 372, HUS, Finland. fredrik.aberg@helsinki.fi Telephone: Received: January 27, 2016 Peer-review started: January 30, 2016 First decision: February 18, 2016 Revised: February 19, 2016 Accepted: March 1, 2016 Article in press: March 2, 2016 Published online: April 14, 2016 Abstract Return to active and productive life is a key goal of modern liver transplantation (LT). Despite marked improvements in quality of life and functional status, a substantial proportion of LT recipients are unable to resume gainful employment. Unemployment forms a threat to physical and psychosocial health, and impairs LT cost-utility through lost productivity. In studies published after year 2000, the average post- LT employment rate is 37%, ranging from 22% to 55% by study. Significant heterogeneity exists among studies. Nonetheless, these employment rates are lower than in the general population and kidneytransplant population. Most consistent employment predictors include pre-lt employment status, male gender, functional/health status, and subjective work ability. Work ability is impaired by physical fatigue and depression, but affected also by working conditions and society. Promotion of post-lt employment is hampered by a lack of interventional studies. Prevention of pre-lt disability by effective treatment of (minimal) hepatic encephalopathy, maintaining mobility, and planning work adjustments early in the course of chronic liver disease, as well as timely post-lt physical rehabilitation, continuous encouragement, self-efficacy improvements, and depression management are key elements of successful employment-promoting strategies. Prolonging LT recipients working life would further strengthen the success of transplantation, and this is likely best achieved through multidisciplinary efforts ideally starting even before LT candidacy. Key words: Employment; Workforce; Transplantation; Quality of life; Work ability The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Outcomes after liver transplantation are steadily improving and transplant recipients are increasingly able to resume normal life. However, a considerable number of recipients are unable to resume work, and this represents an increasing challenge in the field of liver transplantation. This paper discusses possible barriers to post-transplant employment, and means to increase return-to-work among liver transplant recipients April 14, 2016 Volume 22 Issue 14
16 Åberg F. Employment after liver transplantation Åberg F. From prolonging life to prolonging working life: Tackling unemployment among liver-transplant recipients. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Liver transplantation (LT) has been established therapy for various end-stage liver diseases for more than 3 decades. With around 90% of LT recipients currently surviving the first postoperative year [1,2] and with the subsequent life expectancy now exceeding 20 years [3,4], functional outcomes and quality-of-life issues are attracting increased attention. The goal of modern LT can no longer be considered merely to prolong survival, but to achieve complete functional recovery and psychosocial re-integration with a return to active and productive life. Questionnaire-based studies demonstrate comparable quality of life of LT recipients and in the general population with some deficits mainly in physical dimensions [5,6]. In spite of this, a substantial proportion of LT recipients are unable to resume gainful employment, which can be regarded as an objective and rough indicator of quality of life and functional outcome. In this context, the relevance of employment depends on the point of view. From the patient s perspective, being employed is associated with better quality of life [6,7], increased sense of confidence, structure, purpose and meaning [8], improved psychosocial adaptation, financial stability, and a more balanced equilibrium in the family system [9]. From the transplant professional s perspective, employment serves as a surrogate marker of patients functional status, and as such becomes a relevant outcome parameter. From the societal/payer perspective, employment improves LT cost-utility by reducing costs from lost productivity, and thus high post-lt employment rates can support the rationale for transplantation funding. The most comprehensive review of employment after LT by Bravata et al [10] published in 2001 included 82 studies from the 1980s and 1990s. They reported that, respectively, 33% of patients with underlying alcoholic liver disease (ALD) and 80% with non-ald had resumed work at 3 years post-lt. Since then, the landscape of LT has evolved, with changing patient characteristics, and quality-of-life and employment issues have assumed increased focus in clinical practice. This review, with a focus on studies published after year 2000, summarizes current employment rates after LT, factors associated with (un)employment, and potential strategies to support and promote ability to resume work after LT. OCCUPATIONAL RESTRICTIONS AFTER LT Return to work is usually allowed once incisions have healed and the patient is able to perform daily activities [11]. Potential occupational restrictions include medical and surgical complications, such as risk for hypoglycemia with post-transplant diabetes, and infection susceptibility secondary to immunosuppression. However, hard data are lacking. The American Society of Transplantation Infectious Diseases Community of Practice group [12] identified risk occupations being working with animals (especially during maximal immunosuppression), health care work, construction work, and outdoors work. Nonetheless, there are few guidelines to guide decisions regarding occupational restrictions, and the group [12] recommends individualized occupation counseling with the notion that the vast majority of jobs can be made safer by simple measures including vaccination, wearing masks, and reassignment to other duties during periods of intensified immunosuppression. EMPLOYMENT RATES AFTER LT Studies from 8 countries (United States, Europe and Taiwan), published after year 2000, have reported employment rates after LT (Table 1). The non-weighted average employment rate in these studies is 37%, ranging from 22% to 55% by study (Table 1). The average employment rate is similar in US and non- US studies: 38% (range 24%-55%) and 37% (range 22%-53%), respectively. A corresponding average rate weighted by study-sample size virtually equals that reported by Huda et al [13] from the United States as this study comprised patients, more than 11-times the size of the remaining studies combined. Relevant differences among these studies include the variable time-point of employment assessment relative to LT, patient age distribution, exclusion or inclusion of retirees, mixture of liver-disease etiologies, definition of employment, structure of the welfare system and generosity of disability benefits across countries, and post-transplant rehabilitation measures. Definition of employment lacks standardization and differs in, for instance, the inclusion of full-time vs part-time employment and inclusion of students and homemakers. Moreover, there is paucity of recent data on qualitative aspects of employment: ability to return to the same type of work and income level, and the effects of physical demands of the work. No recent qualitative studies were identified that analyzed pre- to post-transplant changes in ability to perform 3702 April 14, 2016 Volume 22 Issue 14
17 Åberg F. Employment after liver transplantation Table 1 Employment rates after liver transplantation in studies published after year 2000 Year Author Country Patient number Employment rate Mean age (yr) Follow-up (mo) Ref Weng Taiwan % [16] 2012 Huda United States % - < 24 [13] 2011 Gorevski United States 91 38% 56 - [29] 2010 Duffy United States 77 35% - > 240 [53] 2010 De Baere Belgium 63 38% 58 - [14] 2009 Åberg Finland % [6] 2007 Saab United States % [17] 2006 Sargent United Kingdom 60 37% [54] 2006 Sahota United States % [18] 2006 Kirchner Germany 23 26% [55] 2005 Rongey United States % [15] 2004 Blanch Spain % [56] 2004 Cowling United States % [20] 2003 Karam France % [57] 2001 Moyzes Germany % [58] Table 2 Employment rates after kidney transplantation in studies published after year 2000 Year Author Country Patient number Employment rate Mean age (yr) Follow-up (mo) 2014 Tzvetanov United States % > Nour Canada 60 38% Helanterä Finland % Eng United States % 48 > Chisholm-Burns United States 75 39% Van der Mei Netherlands 34 67% De Baere Belgium 79 59% Bohlke Brazil % Raiz United States % Van der Mei Netherlands % Griva United Kingdom % Baines Scotland 49 18% Gross United States 87 30% Ostrowski Poland 80 74% homemaker or student duties. EMPLOYMENT COMPARED TO OTHER POPULATIONS In kidney transplant populations, reported employment rates have varied among studies from 18% to 74%, with the non-weighted average of 46% (Table 2) being somewhat higher than the 37% in LT population studies. A Belgian study comparing employment rates among different transplant types reported the highest rate among recipients of a kidney (59%), followed by heart (44%), liver (38%), and lung (28%) [14]. All rates fell below the rates in the Belgian general population (62%), but, except for kidney recipients, the rates also fell below those in the general population among persons with functional limitations (handicap or chronic physical or mental illness; 50%) [14]. It can be argued that this shortfall in employment among transplant recipients may in part be because illness may change a person s values and life priorities, and transplant recipients might therefore decide to participate in other roles that provide them with meaning. Such an effect, however, was not supported by the findings of De Baere et al [14] who reported similar or lower rates of participation in voluntary work in the transplant population (17.4%) than in the general population (21.5%). Of note, comparisons of employment with the general population have not been adjusted for social class, education level, or occupation. These limitations notwithstanding, there is a clear discrepancy in that the majority of LTs are performed on working-aged adults during their most productive years, and 87% of recipients reported improved working/functional capacity after LT in one study [6] ; yet, consistently more than 60% of LT recipients do not resume work. PREDICTORS OF EMPLOYMENT Various factors with variable definitions have been evaluated for associations with post-lt employment. The most consistent univariate predictors of employment, confirmed in at least 3 independent studies, include young age, male gender, etiology of liver disease, pre-transplant employment, and good functional/health status (Figure 1). Pre-transplant income level, subjective work ability, depression and 3703 April 14, 2016 Volume 22 Issue 14
18 Åberg F. Employment after liver transplantation Univariate factors Significant Young age Male Etiology of liver disease Pre-transplant employment Pre-transplant income level Education level Functional/health status Subjective work ability Depression Disability status Type of insurance Lack of diabetes Multivariate factors Young age Male Etiology of liver disease Pre-transplant employment Pre-transplant income level Education level Functional/health status Subjective work ability Depression Disability status Type of insurance Lack of diabetes Number of studies Figure 1 Predictors of employment after liver transplantation. Piles show the number of studies in which the variable was studied, and the dark proportion indicates the number of studies in which the variable was statistically significantly associated with employment. Univariate data are from references [6,13-18,20,29] and multivariate data from references [13-17] April 14, 2016 Volume 22 Issue 14
19 Åberg F. Employment after liver transplantation disability status were significant predictors in 2 studies each. The influence of education level, type of insurance (in US studies), and presence of diabetes remains controversial (Figure 1). Few studies performed multivariate analyses, the majority of which are from the United States (Figure 1) [13-17]. The most robust multivariate data were generated from a US study based on United Network for Organ Sharing data studying employment within 24 mo after LT between 2002 and 2008 [13] ; young age, male gender, higher education level, pre-transplant employment, absent alcoholic liver disease, and good functional status emerged as independent positive predictors of post-transplant employment. Age and gender In a 2009 Finnish study, more than 80% of recipients aged at the time of LT were able to resume work after LT, compared with less than 30% among recipients aged over 50 [6]. Moreover, younger patients were more often able to resume work within 6 mo from the transplant operation [6]. Being close to retirement age might both decrease willingness to try to resume work and, in some countries, permit disability pension on more lenient grounds. In addition, age-related work discrimination might exist among employers. Higher employment rates among male recipients may, in part, be explained by the fact that many studies have categorized homemakers as unemployed. Pre-transplant employment In multivariate analyses, pre-lt employment emerges as the strongest and most consistent predictor of post- LT employment (Figure 1) with patients employed pre-lt fold more likely to resume work after LT than those unemployed [13-15]. Moreover, the longer the pre-lt disability period, the lower the likelihood of resuming work [18]. Sahota et al [18] further reported that patients with low-skill jobs were less likely to return to work than were executives, administrators, managers, or technicians. Liver-disease etiology and severity Employment rates seem to vary by liver-disease etiology with the highest rates commonly seen among patients transplanted for cholestatic disease (primary biliary cirrhosis and primary sclerosing cholangitis) [13,19]. Patients transplanted for ALD generally exhibit somewhat lower employment rates than other patients, but this difference is diminishing in recent series [13] compared to the difference of 33% vs 80% reported by Bravata et al [10] in their 2001 review. Furthermore, such a difference has not been observed in all studies [15,20], and one series found 2.5-fold higher rates among patients transplanted for ALD compared to primary biliary cirrhosis after adjusting for age [19]. Few series have analyzed employment among patients transplanted for acute liver failure. In one series [19] with the acute liver failure group (n = 76) comprising a relatively high proportion of young patients (mean age 46 years) and very few intoxications, 61% of recipients were unemployed after LT, and early retirement secondary to disability was the most common reason. This is surprising as patients with acute liver failure are usually healthy and in the workforce before the onset of liver failure rapidly leading to LT. Therefore, patients with ALF emerge as relevant targets for enhanced post-lt rehabilitation efforts. Severity of liver disease as assessed by the Model for End-stage Liver Disease (MELD) score seems to have no impact on post-lt employment according to US studies [13,15,17]. In a Finnish series [21], we observed a drop in post-lt employment rates from 57% at MELD scores < 15 to 36%-39% at higher LT-day MELD scores. WORK ABILITY AND DISABILITY Additional employment predictors including functional/ health status, subjective work ability, and disability status broadly depict the same concept, namely work ability and disability. From an occupational health perspective, work ability is influenced by individual resources, working conditions, and society (Figure 2) [22]. Individual resources In US and Finnish studies, 60%-76% of unemployed LT recipients reported disability or early retirement due to poor health as the cause for unemployment [6,15,18], but the aspects of health and functional status that impair LT recipients work ability are incompletely understood. LT patients in the workforce have better health-related quality of life than those unemployed [6], chiefly attributed to differences in physical health dimensions [17,23] and fatigue [23,24]. Fatigue, which affects up to 60% of LT recipients and in its severe form almost half [24], is more physical fatigue and reduced activity than mental fatigue or reduced motivation [25]. Fatigue may trigger a vicious circle, leading to inactivity and thus reduction in physical fitness, thereby further increasing fatigue. Fatigue seldom resolves by itself [26], and no clear association has been found with post-lt medical complications or immunosuppression [24]. In the general population, depression is a key cause worldwide of long-term disability [27]. Up to 40% of LT recipients exhibit features of depression, and depressive symptoms are likely underrecognized among LT candidates as well [28]. Depression has been associated with unemployment and reduced survival after LT [16,29-32] April 14, 2016 Volume 22 Issue 14
20 Åberg F. Employment after liver transplantation Individual resources Health Functional capacity Generic and specific education Skills Motivation Society Employment protection laws Welfare system Universal health care access Fiscal structure Working conditions Environment Physical and mental demands Psychosocial factors Employer characteristics (flexibility, support) Figure 2 Work ability is a dynamic concept influenced by factors related to individual resources, working conditions and society. Figure constructed based on concepts presented by Ilmarinen et al [22]. Working conditions In chronic illness and disability, suitable workplace modifications, employer support, and flexible sickleave practices contribute to participation in paid work in general [33,34], but specific data for LT populations are scarce. One recent study reported that 58% of LT recipients were fit for the job performed pre-lt, and 74% would have been fit for the job with some work adjustments such as fixed shift or reduced working hours [35]. Society and socioeconomic aspects In many countries, disability benefits and early retirement serve to secure financial stability and healthcare access. This is pronounced in the United States, where health insurance is separated in private (usually obtained from the workplace or spouse) and public (e.g., Medicaid). As long-term access to public health insurance is conditional to eligibility for disability benefits or full-age retirement, LT recipients with poor earning prospects and inability to obtain private health insurance may restrain from seeking work and rely on disability income to secure health-care access. In concordance, 12%-20% of unemployed LT recipients in US studies reported they were not working due to fear of losing insurance coverage [15,18]. Clearly, the concept of post-lt disability extends beyond medical health status, but there are wide differences in pension policies across countries: in the access to benefits, generosity of benefits, and whether benefits are fixed-term or permanent [36]. In most countries, however, the annual outflow from disability pension is very low, < 1% [36]. An exception is United Kingdom with annual outflow around 7%, which is attributed to routine reassessments over time of the entitlement to benefits [36]. In addition, among disability beneficiaries who exited the benefit (excluding ageretirement), employment rates 3 year later vary from 10% in Germany to 61% in the United Kingdom [36]. When viewed against these general-population rates, the shortfall in employment among LT patients appears much less pronounced. STRATEGIES TO PROMOTE POST-LT EMPLOYMENT Promotion of post-lt employment is hampered by absent interventional studies. Given the variable and individual needs and barriers to resuming work, no single intervention will expectedly benefit all patients. Of the established employment predictors discussed above, pre-lt work ability, post-lt functional status and work ability, fatigue and depression are potentially modifiable and therefore represent targets for employment-promoting interventions. Pre-transplant work ability In advanced liver disease, patient work performance may be compromised by liver-related symptoms 3706 April 14, 2016 Volume 22 Issue 14
21 Åberg F. Employment after liver transplantation Period Goal Intervention Pre-transplant Maintain work ability and employment as long as possible Maintaining mobility by effective treatment of ascites and edema, and physiotherapy to prevent sarcopenia and improve muscle strength Management of (minimal) hepatic encephalopathy Occupational health specialist engagement Planning of work adjustments pre- and post-lt Encouragement to continue working and maintaining the goal to resume work post-lt Evaluation of partial disability benefits Immediate post-lt period (weeks-few months) Physical and mental recovery Individualized rehabilitation aiming especially for improving physical function Home training programme vs rehabilitation facility Optimization of timing > 2-3 mo post-lt Shift in focus from recovery to re-engagement with life (LT "patient" LT "recipient") Encouragement, support Stress/depression management Addressing of fears and perceived barriers to rehabilitation Referral to community employment-support services Routine re-evaluation of disability benefits Figure 3 Supporting employment and work ability in the liver transplantation setting - key goals and potential interventions at different time periods. such as fatigue, covert (minimal) or overt hepatic encephalopathy (HE), and impaired mobility secondary to decreased muscle strength, ascites and edema. Ascites and minimal HE are key drivers of impaired health-related quality of life among nonhospitalized cirrhotics [37] and features of HE, as assessed by cognitive tests, are independently associated with unemployment [38]. A Dutch study reported that regular employment was absent in nearly half of cirrhotic patients with minimal HE compared to 15% of patients without minimal HE [39]. Minimal HE causes impairment in social interaction, alertness, memory, information processing, judgment, sleep, work, home management, and coordination and psychomotor skills such as driving a car [40]. Recent guidelines [41] state that neuropsychological testing for minimal/covert HE could be applied to patients with impaired quality of life or implication on employment, and that treatment for minimal HE should be considered on a case-by-case basis. Interventional studies using lactulose or rifaximin have shown high rates of reversal of minimal HE and improvement in both quality of life [42,43] and driving simulator performance [44]. Effective control of ascites and edema is important in maintaining mobility, and exercise programs may be beneficial also in advanced liver disease [45]. Collaboration with occupational-health specialists early in the course of liver disease to plan possible job modifications both before and after LT and to educate employers about liver disease and LT can help maintain work when the patient later becomes decompensated and a candidate for LT. At this point, partial disability benefits, instead of full disability benefits, may offer the opportunity to retain a job to return to after LT. Rehabilitation Early post-lt assessment of needs for physiotherapy is imperative to reverse muscle wasting and deconditioning from the pre-lt period. Patients with strong adaptive capacity might be able to make adjustments independently, whereas those with less adaptive capacity may need assistance, for instance, via dedicated rehabilitation clinics [46]. Cirrhosisrelated hyperdynamic circulation and functional and structural cardiac alterations usually resolve within 6-12 mo post-lt [47] and risk for incisional hernias secondary to abdominal muscle strains decreases after 6 mo [11] ; these are important considerations for timing of different rehabilitation measures. The most appropriate type of exercise training in transplant recipients has not been well studied [48]. Preliminary study showed that a 12-wk fatigue-reducing physical rehabilitation program with supervised exercise training and repeated physical-activity counseling sessions was effective in improving severe fatigue and several other aspects of health including questionnairebased measures of work ability [49,50]. However, whether rehabilitation efforts truly translate into better work 3707 April 14, 2016 Volume 22 Issue 14
22 Åberg F. Employment after liver transplantation ability and higher post-lt employment rates remains unproven. Re-engagement with life Nour et al [8] interviewed kidney-transplant recipients for their recommendations on how to improve employment. Of respondents, 39% recommended further encouragement from the transplant team, and 57% called for rehabilitation programs with a focus on returning to work [8]. Screening for and management of depression is also important [28], as are efforts to increase self-efficacy [51]. The need for employmentsupport services available in the community should be assessed in collaboration with social workers. Countries that target resources towards matching workers with jobs, retraining opportunities and occupational rehabilitation exhibit higher employment rates among chronically ill persons in general [52]. Health-political discussion is warranted to strive to remove the barriers that require transplant recipients to choose between healthcare coverage and work. Financial encouragements for resuming work while maintaining easy access back to sickness benefits if medical problems ensue have been proposed [14]. Figure 3 provides a framework of elements at different time periods that, based on current evidence, deserve be incorporated in effective back-to-work programs. Patients transplanted for acute liver failure, those unemployed before LT, and young LT recipients who remain unemployed for 6 mo post-lt emerge as distinct targets for intensified vocational rehabilitation measures. It needs be acknowledged, however, that this framework is not evidence-based, owing to absent interventional studies. As patient needs and barriers to resuming work are highly individual and multifaceted, the contents of back-to-work programs will be difficult to scientifically quantify, and reproducing effective programs at another locale is likely a very challenging task. CONCLUSION As an indicator of functional recovery and social reintegration, ability to resume work is becoming a relevant outcome parameter for any transplant center or country to monitor. However, the definition of employment and work needs to be standardized in studies, and the mechanisms behind post-transplant disability are still poorly understood. Although the development and implementation of effective, targeted, and tailored post-transplant rehabilitation and re-integration programs are important unmet research needs, it seems that successful promotion of post-lt employment needs to commence pretransplant, early in the course of liver disease. Once a potential LT candidate becomes unemployed, the likelihood of being able to return to the workforce after transplantation decreases dramatically. The concerning fact, found in some healthcare settings, that LT recipients may choose to stay on disability income for fear of losing financial security and healthcare access, calls for a change in policy, to remove the barriers that require LT recipients to choose between healthcare coverage and work. Transplant professionals, social workers and patient organizations can have a key role in initiating such change in policy. REFERENCES 1 Adam R, Karam V, Delvart V, O Grady J, Mirza D, Klempnauer J, Castaing D, Neuhaus P, Jamieson N, Salizzoni M, Pollard S, Lerut J, Paul A, Garcia-Valdecasas JC, Rodríguez FS, Burroughs A. Evolution of indications and results of liver transplantation in Europe. A report from the European Liver Transplant Registry (ELTR). J Hepatol 2012; 57: [PMID: DOI: /j.jhep ] 2 Kim WR, Lake JR, Smith JM, Skeans MA, Schladt DP, Edwards EB, Harper AM, Wainright JL, Snyder JJ, Israni AK, Kasiske BL. OPTN/SRTR 2013 Annual Data Report: liver. Am J Transplant 2015; 15 Suppl 2: 1-28 [PMID: DOI: /ajt.13197] 3 Barber K, Blackwell J, Collett D, Neuberger J. Life expectancy of adult liver allograft recipients in the UK. Gut 2007; 56: [PMID: DOI: /gut ] 4 Åberg F, Gissler M, Karlsen TH, Ericzon BG, Foss A, Rasmussen A, Bennet W, Olausson M, Line PD, Nordin A, Bergquist A, Boberg KM, Castedal M, Pedersen CR, Isoniemi H. Differences in long-term survival among liver transplant recipients and the general population: a population-based Nordic study. Hepatology 2015; 61: [PMID: DOI: /hep.27538] 5 Tome S, Wells JT, Said A, Lucey MR. Quality of life after liver transplantation. A systematic review. J Hepatol 2008; 48: [PMID: DOI: /j.jhep ] 6 Aberg F, Rissanen AM, Sintonen H, Roine RP, Höckerstedt K, Isoniemi H. Health-related quality of life and employment status of liver transplant patients. Liver Transpl 2009; 15: [PMID: DOI: /lt.21651] 7 Ortiz F, Aronen P, Koskinen PK, Malmström RK, Finne P, Honkanen EO, Sintonen H, Roine RP. Health-related quality of life after kidney transplantation: who benefits the most? Transpl Int 2014; 27: [PMID: DOI: /tri.12394] 8 Nour N, Heck CS, Ross H. Factors related to participation in paid work after organ transplantation: perceptions of kidney transplant recipients. J Occup Rehabil 2015; 25: [PMID: DOI: /s ] 9 Callahan MB. Dollars and sense of successful rehabilitation. Prog Transplant 2005; 15: [PMID: ] 10 Bravata DM, Olkin I, Barnato AE, Keeffe EB, Owens DK. Employment and alcohol use after liver transplantation for alcoholic and nonalcoholic liver disease: a systematic review. Liver Transpl 2001; 7: [PMID: DOI: / jlts ] 11 McGuire BM, Rosenthal P, Brown CC, Busch AM, Calcatera SM, Claria RS, Hunt NK, Korenblat KM, Mazariegos GV, Moonka D, Orloff SL, Perry DK, Rosen CB, Scott DL, Sudan DL. Longterm management of the liver transplant patient: recommendations for the primary care doctor. Am J Transplant 2009; 9: [PMID: DOI: /j x] 12 Avery RK, Michaels MG. Strategies for safe living after solid organ transplantation. Am J Transplant 2013; 13 Suppl 4: [PMID: DOI: /ajt.12121] 13 Huda A, Newcomer R, Harrington C, Blegen MG, Keeffe EB. High rate of unemployment after liver transplantation: analysis of the United Network for Organ Sharing database. Liver Transpl 3708 April 14, 2016 Volume 22 Issue 14
23 Åberg F. Employment after liver transplantation 2012; 18: [PMID: DOI: /lt.22408] 14 De Baere C, Delva D, Kloeck A, Remans K, Vanrenterghem Y, Verleden G, Vanhaecke J, Nevens F, Dobbels F. Return to work and social participation: does type of organ transplantation matter? Transplantation 2010; 89: [PMID: DOI: /TP.0b013e3181ce77e5] 15 Rongey C, Bambha K, Vanness D, Pedersen RA, Malinchoc M, Therneau TM, Dickson ER, Kim WR. Employment and health insurance in long-term liver transplant recipients. Am J Transplant 2005; 5: [PMID: DOI: / j x] 16 Weng LC, Huang HL, Wang YW, Lee WC, Chen KH, Yang TY. The effect of self-efficacy, depression and symptom distress on employment status and leisure activities of liver transplant recipients. J Adv Nurs 2014; 70: [PMID: DOI: /jan.12315] 17 Saab S, Wiese C, Ibrahim AB, Peralta L, Durazo F, Han S, Yersiz H, Farmer DG, Ghobrial RM, Goldstein LI, Tong MJ, Busuttil RW. Employment and quality of life in liver transplant recipients. Liver Transpl 2007; 13: [PMID: DOI: / lt.21247] 18 Sahota A, Zaghla H, Adkins R, Ramji A, Lewis S, Moser J, Sher LS, Fong TL. Predictors of employment after liver transplantation. Clin Transplant 2006; 20: [PMID: DOI: /j x] 19 Aberg F, Höckerstedt K, Roine RP, Sintonen H, Isoniemi H. Influence of liver-disease etiology on long-term quality of life and employment after liver transplantation. Clin Transplant 2012; 26: [PMID: DOI: /j x] 20 Cowling T, Jennings LW, Goldstein RM, Sanchez EQ, Chinnakotla S, Klintmalm GB, Levy MF. Societal reintegration after liver transplantation: findings in alcohol-related and non-alcohol-related transplant recipients. Ann Surg 2004; 239: [PMID: DOI: /01.sla ] 21 Åberg F, Höckerstedt K, Roine RP, Isoniemi H. A High Meld Score Relates to Lower Employment Rates After Liver Transplantation. Trans Int 2011; 24: Ilmarinen J, Tuomi K. Past, present and future of work ability. In: Ilmarinen J, Lehtinen S. Past, Present and Future of Work Ability, People and Work, Research Reports. Helsinki: Finnish Institute of Occupational, 2004: Aadahl M, Hansen BA, Kirkegaard P, Groenvold M. Fatigue and physical function after orthotopic liver transplantation. Liver Transpl 2002; 8: [PMID: DOI: / jlts ] 24 Elliott C, Frith J, Pairman J, Jones DE, Newton JL. Reduction in functional ability is significant postliver transplantation compared with matched liver disease and community dwelling controls. Transpl Int 2011; 24: [PMID: DOI: / j x] 25 van den Berg-Emons R, van Ginneken B, Wijffels M, Tilanus H, Metselaar H, Stam H, Kazemier G. Fatigue is a major problem after liver transplantation. Liver Transpl 2006; 12: [PMID: DOI: /lt.20684] 26 van Ginneken BT, van den Berg-Emons RJ, van der Windt A, Tilanus HW, Metselaar HJ, Stam HJ, Kazemier G. Persistent fatigue in liver transplant recipients: a two-year follow-up study. Clin Transplant 2010; 24: E10-E16 [PMID: DOI: / j x] 27 Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basanez MG, Baxter A, Bell ML, Benjamin EJ, Bennett D, Bernabe E, Bhalla K, Bhandari B, Bikbov B, Bin Abdulhak A, Birbeck G, Black JA, Blencowe H, Blore JD, Blyth F, Bolliger I, Bonaventure A, Boufous S, Bourne R, Boussinesq M, Braithwaite T, Brayne C, Bridgett L, Brooker S, Brooks P, Brugha TS, Bryan- Hancock C, Bucello C, Buchbinder R, Buckle G, Budke CM, Burch M, Burney P, Burstein R, Calabria B, Campbell B, Canter CE, Carabin H, Carapetis J, Carmona L, Cella C, Charlson F, Chen H, Cheng AT, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahiya M, Dahodwala N, Damsere-Derry J, Danaei G, Davis A, De Leo D, Degenhardt L, Dellavalle R, Delossantos A, Denenberg J, Derrett S, Des Jarlais DC, Dharmaratne SD, Dherani M, Diaz-Torne C, Dolk H, Dorsey ER, Driscoll T, Duber H, Ebel B, Edmond K, Elbaz A, Ali SE, Erskine H, Erwin PJ, Espindola P, Ewoigbokhan SE, Farzadfar F, Feigin V, Felson DT, Ferrari A, Ferri CP, Fevre EM, Finucane MM, Flaxman S, Flood L, Foreman K, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabbe BJ, Gabriel SE, Gakidou E, Ganatra HA, Garcia B, Gaspari F, Gillum RF, Gmel G, Gosselin R, Grainger R, Groeger J, Guillemin F, Gunnell D, Gupta R, Haagsma J, Hagan H, Halasa YA, Hall W, Haring D, Haro JM, Harrison JE, Havmoeller R, Hay RJ, Higashi H, Hill C, Hoen B, Hoffman H, Hotez PJ, Hoy D, Huang JJ, Ibeanusi SE, Jacobsen KH, James SL, Jarvis D, Jasrasaria R, Jayaraman S, Johns N, Jonas JB, Karthikeyan G, Kassebaum N, Kawakami N, Keren A, Khoo JP, King CH, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lalloo R, Laslett LL, Lathlean T, Leasher JL, Lee YY, Leigh J, Lim SS, Limb E, Lin JK, Lipnick M, Lipshultz SE, Liu W, Loane M, Ohno SL, Lyons R, Ma J, Mabweijano J, MacIntyre MF, Malekzadeh R, Mallinger L, Manivannan S, Marcenes W, March L, Margolis DJ, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGill N, McGrath J, Medina-Mora ME, Meltzer M, Mensah GA, Merriman TR, Meyer AC, Miglioli V, Miller M, Miller TR, Mitchell PB, Mocumbi AO, Moffitt TE, Mokdad AA, Monasta L, Montico M, Moradi-Lakeh M, Moran A, Morawska L, Mori R, Murdoch ME, Mwaniki MK, Naidoo K, Nair MN, Naldi L, Narayan KM, Nelson PK, Nelson RG, Nevitt MC, Newton CR, Nolte S, Norman P, Norman R, O Donnell M, O Hanlon S, Olives C, Omer SB, Ortblad K, Osborne R, Ozgediz D, Page A, Pahari B, Pandian JD, Rivero AP, Patten SB, Pearce N, Padilla RP, Perez-Ruiz F, Perico N, Pesudovs K, Phillips D, Phillips MR, Pierce K, Pion S, Polanczyk GV, Polinder S, Pope CA,3rd, Popova S, Porrini E, Pourmalek F, Prince M, Pullan RL, Ramaiah KD, Ranganathan D, Razavi H, Regan M, Rehm JT, Rein DB, Remuzzi G, Richardson K, Rivara FP, Roberts T, Robinson C, De Leon FR, Ronfani L, Room R, Rosenfeld LC, Rushton L, Sacco RL, Saha S, Sampson U, Sanchez-Riera L, Sanman E, Schwebel DC, Scott JG, Segui-Gomez M, Shahraz S, Shepard DS, Shin H, Shivakoti R, Singh D, Singh GM, Singh JA, Singleton J, Sleet DA, Sliwa K, Smith E, Smith JL, Stapelberg NJ, Steer A, Steiner T, Stolk WA, Stovner LJ, Sudfeld C, Syed S, Tamburlini G, Tavakkoli M, Taylor HR, Taylor JA, Taylor WJ, Thomas B, Thomson WM, Thurston GD, Tleyjeh IM, Tonelli M, Towbin JA, Truelsen T, Tsilimbaris MK, Ubeda C, Undurraga EA, van der Werf MJ, van Os J, Vavilala MS, Venketasubramanian N, Wang M, Wang W, Watt K, Weatherall DJ, Weinstock MA, Weintraub R, Weisskopf MG, Weissman MM, White RA, Whiteford H, Wiersma ST, Wilkinson JD, Williams HC, Williams SR, Witt E, Wolfe F, Woolf AD, Wulf S, Yeh PH, Zaidi AK, Zheng ZJ, Zonies D, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries : a systematic analysis for the Global Burden of Disease Study Lancet 2012; 380: [PMID: DOI: /S (12) ] 28 Mullish BH, Kabir MS, Thursz MR, Dhar A. Review article: depression and the use of antidepressants in patients with chronic liver disease or liver transplantation. Aliment Pharmacol Ther 2014; 40: [PMID: DOI: /apt.12925] 3709 April 14, 2016 Volume 22 Issue 14
24 Åberg F. Employment after liver transplantation 29 Gorevski E, Succop P, Sachdeva J, Scott R, Benjey J, Varughese G, Martin-Boone J. Factors influencing posttransplantation employment: does depression have an impact? Transplant Proc 2011; 43: [PMID: DOI: /j.transproce ed ] 30 Newton SE. Relationship between depression and work outcomes following liver transplantation: the nursing perspective. Gastroenterol Nurs 2003; 26: [PMID: ] 31 Zahn A, Seubert L, Jünger J, Schellberg D, Weiss KH, Schemmer P, Stremmel W, Sauer P, Gotthardt DN. Factors influencing long-term quality of life and depression in German liver transplant recipients: a single-centre cross-sectional study. Ann Transplant 2013; 18: [PMID: DOI: / AOT ] 32 DiMartini A, Dew MA, Chaiffetz D, Fitzgerald MG, Devera ME, Fontes P. Early trajectories of depressive symptoms after liver transplantation for alcoholic liver disease predicts long-term survival. Am J Transplant 2011; 11: [PMID: DOI: /j x] 33 Boot CR, Koppes LL, van den Bossche SN, Anema JR, van der Beek AJ. Relation between perceived health and sick leave in employees with a chronic illness. J Occup Rehabil 2011; 21: [PMID: DOI: /s ] 34 Kaye HS, Jans LH, Jones EC. Why don t employers hire and retain workers with disabilities? J Occup Rehabil 2011; 21: [PMID: DOI: /s ] 35 Ferrario A, Verga FC, Piolatto PG, Pira E. Return to work after organ transplantation: a cross-sectional study on working ability evaluation and employment status. Transplant Proc 2014; 46: [PMID: DOI: /j.transproceed ] 36 OECD. Chapter 4: Pathways onto (and off) Disability benefits: assessing the role of policy and individual circumstances. In: OECD employment outlook Tackling the jobs crisis, Available from: URL: www. oecd. org/ employment/ emp/ pdf 37 Orr JG, Homer T, Ternent L, Newton J, McNeil CJ, Hudson M, Jones DE. Health related quality of life in people with advanced chronic liver disease. J Hepatol 2014; 61: [PMID: DOI: /j.jhep ] 38 Bajaj JS, Riggio O, Allampati S, Prakash R, Gioia S, Onori E, Piazza N, Noble NA, White MB, Mullen KD. Cognitive dysfunction is associated with poor socioeconomic status in patients with cirrhosis: an international multicenter study. Clin Gastroenterol Hepatol 2013; 11: [PMID: DOI: /j.cgh ] 39 Groeneweg M, Moerland W, Quero JC, Hop WC, Krabbe PF, Schalm SW. Screening of subclinical hepatic encephalopathy. J Hepatol 2000; 32: [PMID: ] 40 Agrawal S, Umapathy S, Dhiman RK. Minimal hepatic encephalopathy impairs quality of life. J Clin Exp Hepatol 2015; 5: S42-S48 [PMID: DOI: /j.jceh ] 41 Vilstrup H, Amodio P, Bajaj J, Cordoba J, Ferenci P, Mullen KD, Weissenborn K, Wong P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014; 60: [PMID: DOI: /hep.27210] 42 Prasad S, Dhiman RK, Duseja A, Chawla YK, Sharma A, Agarwal R. Lactulose improves cognitive functions and health-related quality of life in patients with cirrhosis who have minimal hepatic encephalopathy. Hepatology 2007; 45: [PMID: DOI: /hep.21533] 43 Sidhu SS, Goyal O, Mishra BP, Sood A, Chhina RS, Soni RK. Rifaximin improves psychometric performance and health-related quality of life in patients with minimal hepatic encephalopathy (the RIME Trial). Am J Gastroenterol 2011; 106: [PMID: DOI: /ajg ] 44 Bajaj JS, Heuman DM, Wade JB, Gibson DP, Saeian K, Wegelin JA, Hafeezullah M, Bell DE, Sterling RK, Stravitz RT, Fuchs M, Luketic V, Sanyal AJ. Rifaximin improves driving simulator performance in a randomized trial of patients with minimal hepatic encephalopathy. Gastroenterology 2011; 140: e1 [PMID: DOI: /j.gastro ] 45 Limongi V, dos Santos DC, da Silva AM, Ataide EC, Mei MF, Udo EY, Boin IF, Stucchi RS. Effects of a respiratory physiotherapeutic program in liver transplantation candidates. Transplant Proc 2014; 46: [PMID: DOI: /j.transproceed ] 46 Scott PJ. Occupational therapy services to enable liver patients to thrive following transplantation. Occup Ther Health Care 2011; 25: [PMID: DOI: / ] 47 Torregrosa M, Aguadé S, Dos L, Segura R, Gónzalez A, Evangelista A, Castell J, Margarit C, Esteban R, Guardia J, Genescà J. Cardiac alterations in cirrhosis: reversibility after liver transplantation. J Hepatol 2005; 42: [PMID: ] 48 Mathur S, Janaudis-Ferreira T, Wickerson L, Singer LG, Patcai J, Rozenberg D, Blydt-Hansen T, Hartmann EL, Haykowsky M, Helm D, High K, Howes N, Kamath BM, Lands L, Marzolini S, Sonnenday C. Meeting report: consensus recommendations for a research agenda in exercise in solid organ transplantation. Am J Transplant 2014; 14: [PMID: DOI: / ajt.12874] 49 van den Berg-Emons RJ, van Ginneken BT, Nooijen CF, Metselaar HJ, Tilanus HW, Kazemier G, Stam HJ. Fatigue after liver transplantation: effects of a rehabilitation program including exercise training and physical activity counseling. Phys Ther 2014; 94: [PMID: DOI: /ptj ] 50 van Ginneken BT, van den Berg-Emons HJ, Metselaar HJ, Tilanus HW, Kazemier G, Stam HJ. Effects of a rehabilitation programme on daily functioning, participation, health-related quality of life, anxiety and depression in liver transplant recipients. Disabil Rehabil 2010; 32: [PMID: DOI: / ] 51 Haugli L, Maeland S, Magnussen LH. What facilitates return to work? Patients experiences 3 years after occupational rehabilitation. J Occup Rehabil 2011; 21: [PMID: DOI: /s ] 52 Holland P, Nylén L, Thielen K, van der Wel KA, Chen WH, Barr B, Burström B, Diderichsen F, Andersen PK, Dahl E, Uppal S, Clayton S, Whitehead M. How do macro-level contexts and policies affect the employment chances of chronically ill and disabled people? Part II: The impact of active and passive labor market policies. Int J Health Serv 2011; 41: [PMID: ] 53 Duffy JP, Kao K, Ko CY, Farmer DG, McDiarmid SV, Hong JC, Venick RS, Feist S, Goldstein L, Saab S, Hiatt JR, Busuttil RW. Long-term patient outcome and quality of life after liver transplantation: analysis of 20-year survivors. Ann Surg 2010; 252: [PMID: DOI: / SLA.0b013e3181f5f23a] 54 Sargent S, Wainwright SP. Quality of life following emergency liver transplantation for acute liver failure. Nurs Crit Care 2006; 11: [PMID: ] 55 Kirchner GI, Rifai K, Cantz T, Nashan B, Terkamp C, Becker T, Strassburg C, Barg-Hock H, Wagner S, Lück R, Klempnauer J, Manns MP. Outcome and quality of life in patients with polycystic liver disease after liver or combined liver-kidney transplantation. Liver Transpl 2006; 12: [PMID: DOI: /lt.20780] 56 Blanch J, Sureda B, Flaviá M, Marcos V, de Pablo J, De Lazzari E, Rimola A, Vargas V, Navarro V, Margarit C, Visa J. Psychosocial adjustment to orthotopic liver transplantation in 266 recipients. Liver Transpl 2004; 10: [PMID: DOI: / lt.20076] 57 Karam VH, Gasquet I, Delvart V, Hiesse C, Dorent R, Danet C, Samuel D, Charpentier B, Gandjbakhch I, Bismuth H, Castaing D April 14, 2016 Volume 22 Issue 14
25 Åberg F. Employment after liver transplantation Quality of life in adult survivors beyond 10 years after liver, kidney, and heart transplantation. Transplantation 2003; 76: [PMID: DOI: /01.TP E] 58 Moyzes D, Walter M, Rose M, Neuhaus P, Klapp BF. Return to work 5 years after liver transplantation. Transplant Proc 2001; 33: [PMID: ] P- Reviewer: Boin IFSH, Elsiesy H, Kuramitsu K S- Editor: Yu J L- Editor: A E- Editor: Liu XM 3711 April 14, 2016 Volume 22 Issue 14
26 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved Pancreatic Cancer: Global view TOPIC HIGHLIGHT Elastography for the pancreas: Current status and future perspective Natsuko Kawada, Sachiko Tanaka Natsuko Kawada, Department of Gastroenterology, Nissay Hospital, Osaka , Japan Sachiko Tanaka, Osaka Center for Cancer and Cardiovascular Diseases Prevention, Osaka , Japan Author contributions: Kawada N analyzed literature and wrote the manuscript; Tanaka S checked and approved the manuscript. Conflict-of-interest statement: The authors have no conflicts of interest to report. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Natsuko Kawada, MD, Department of Gastroenterology, Nissay Hospital, Itachibori Nishi, Osaka , Japan. natz.kawada@gmail.com Telephone: Fax: Received: December 25, 2015 Peer-review started: December 29, 2015 First decision: January 28, 2016 Revised: February 19, 2016 Accepted: March 13, 2016 Article in press: March 14, 2016 Published online: April 14, 2016 Abstract Elastography for the pancreas can be performed by either ultrasound or endoscopic ultrasound (EUS). There are two types of pancreatic elastographies based on different principles, which are strain elastography and shear wave elastography. The stiffness of tissue is estimated by measuring the grade of strain generated by external pressure in the former, whereas it is estimated by measuring propagation speed of shear wave, the transverse wave, generated by acoustic radiation impulse (ARFI) in the latter. Strain elastography is difficult to perform when the probe, the pancreas and the aorta are not located in line. Accordingly, a fine elastogram can be easily obtained in the pancreatic body but not in the pancreatic head and tail. In contrast, shear wave elastography can be easily performed in the entire pancreas because ARFI can be emitted to wherever desired. However, shear wave elastography cannot be performed by EUS to date. Recently, clinical guidelines for elastography specialized in the pancreas were published from Japanese Society of Medical Ultrasonics. The guidelines show us technical knacks of performing elastography for the pancreas. Key words: Elastography; Pancreas; Strain; Shear wave The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Elastography for the pancreas had been considered to be difficult to perform with adequate accuracy and reproducibility because the pancreas is a small organ located deep in center of the human body. This review introduces the recent innovation of elastography for the pancreas, and makes recommendations on how to use various elastographic modalities for the pancreas. The review also shows us what we can know by performing elastography for the pancreas. Elastography may be a promising imaging modality for differential diagnosis between malignant and benign pancreatic tumors, for early diagnosis of chronic pancreatitis, and for identifying high-risk patients for pancreatic cancer. Kawada N, Tanaka S. Elastography for the pancreas: Current 3712 April 14, 2016 Volume 22 Issue 14
27 Kawada N et al. Elastography for the pancreas status and future perspective. World J Gastroenterol 2016; 22(14): Available from: URL: com/ /full/v22/i14/3712.htm DOI: org/ /wjg.v22.i INTRODUCTION Elastography is an imaging modality which evaluates the stiffness of organs. There are a considerable number of studies assessing the usefulness of elastography for superficial organs including the breast [1] and the thyroid [2] and for the liver in the field of digestive systems [3-6]. Recently, the clinical guidelines for elastography mainly focused on the liver and the breast were published from Japanese Society of Ultrasound in Medicine [7,8], European Federation of Societies for Ultrasound in Medicine and Biology [9], and World Federation for Ultrasound in Medicine and Biology [10,11]. In contrast, there are far fewer studies evaluating its usefulness for the pancreas. Because pancreas is a small organ locates deep in center of the human body, it is not easy to perform elastography for the pancreas with adequate accuracy and reproducibility. In addition to that, it is not easy to confirm if an elastogram of the pancreas truly reflects the histological structure because obtaining biopsy specimens from the pancreas is difficult. In 2015, clinical practice guidelines for elastography specialized in the pancreas were published from Japanese Society of Medical Ultrasonics [12]. The guidelines show us not only the recent studies but also technical knacks of performing elastography for the pancreas, and hence these guidelines are very useful for clinical practice. Historically, clinical application of elastography had begun with strain elastography [13,14]. Strain elastography estimates the stiffness of target tissue by measuring the grade of strain generated by external pressure [15,16]. There is negative correlation between the grade of strain and the stiffness of target tissue: the greater the strain, the softer the stiffness of target tissue is. Because manual compression is ineffective for the pancreas, the strain must be generated by aortic pulsation. Ideally, the target tissue should be located in line between the probe and the aorta in order to obtain adequate strain for elastography: A fine elastogram can be easily obtained in the pancreatic body, except for the patients with severe arteriosclerosis. In contrast, a fine elastogram cannot be obtained often in the pancreatic head and tail. Shear wave elastography is another elastography based on a different principle. Shear wave elastography emits the focused ultrasound, so called acoustic radiation force impulse (ARFI), from the probe to the target tissue. Consequently, the transverse wave, so-called shear wave, is generated by ARFI, and the stiffness of the target tissue is estimated by measuring the propagation speed of shear wave (Figure 1). There is positive correlation between the propagation speed of shear wave (shear wave velocity) and the stiffness of target tissue: the faster the shear wave velocity, the harder the target tissue is. Theoretically, ARFI can be emitted to the entire pancreas wherever desired. However, passive strain of the pancreas caused by aortic pulsation can interfere with ARFI, especially in the pancreatic body. The strength of ARFI is limited to ensure safety [17], therefore, adequate shear wave may not be generated for a hard pancreatic tumor. In addition to that, no one knows if ARFI is used with contrast enhanced material in safety [18-20]. Shear wave elastography cannot be performed by endoscopic ultrasound (EUS) to date. In the past, biopsy specimens had been difficult to obtain from the pancreas. Recently, a novel technique, EUS guided-fine needle aspiration (EUS-FNA) was established, and now it is frequently performed for the pancreas in clinical practice [21-26]. However, the specimens obtained by EUS-FNA from the pancreas are much smaller compared to those obtained by fine needle biopsy from the liver. Also, EUS-FNA can cause serious adverse events such as severe pancreatitis [26-28] and needle track seeding [29]. Thus, it is still crucial to develop a non-invasive imaging modality as elastography for the pancreas. For the widespread clinical application, elastography for the pancreas must meet conditions such as adequate reproducibility, operator independency, and accuracy as high as it can reflect histological structure. However, there are little studies investigating these issues. Although there are still a considerable number of issues remained to be solved, elastography for the pancreas is a promising imaging modality because of its non-invasive nature. For the better understanding of elastography for the pancreas for readers who are not experts of the pancreas, this report introduces only the elastographies which have already been reported in the literature. Thus, we should add that other promising elastographic modalities are also available, which are not introduced in this report. ELASTOGRAPHY FOR THE PANCREAS US-elastography - Strain elastography US-elastography is a non-invasive imaging examination which can be performed by not only physicians but also medical technicians. Therefore, US-elastography seems to be an appropriate imaging modality for screening numerous asymptomatic. Because periodical screening of high-risk group, even though they are asymptomatic, is known to be necessary for early detection of pancreatic cancer [30], US-elastography can be a candidate for this periodical screening strategy. Historically, clinical application of US-elastography had begun with Real-time Tissue Elastography TM (RTE) produced by Hitachi Aloka [13,14]. In the conventional RTE, only qualitative diagnosis using color map was possible 3713 April 14, 2016 Volume 22 Issue 14

.")
28 Kawada N et al. Elastography for the pancreas Acoustic radiation force impulse Shear wave Figure 1 Measurement principle of shear wave elastography. Acoustic radiation force impulse is emitted from the probe to the target tissue. Accordingly, the transverse wave, so-called shear wave, is generated. The propagation speed of shear wave is measured by the detection pulse transmitted from the probe. Figure 2 Qualitative diagnosis in US-Real-time Tissue Elastography TM. A hypoechoic tumor was seen at the pancreatic tail in B-mode (right). In Real-time Tissue Elastography TM, blue color is seen on the tumor, green color is seen on non-tumorous area of the pancreas, and red color is seen at ventral side of the pancreas (left). (Figure 2). In the color map of RTE, the hardest tissue is displayed as blue, and the softest tissue is displayed as red. In RTE, it is known that elastogram cannot be obtained, or some artifacts will be seen for fluid component as cyst, therefore, pancreatic cystic lesions cannot be evaluated by RTE. Uchida et al [31] published the first report evaluating the usefulness of US-elastography for the pancreas in They reviewed elastograms performed for 10 normal pancreas, 5 pancreatic ductal adenocarcinomas, 2 endocrine tumors, and 5 chronic pancreatitis, and reported the typical color map observed in US-RTE as follows: homogeneous color was observed in normal pancreas, markedly hard area with soft spots was observed in pancreatic ductal adenocarcinoma, uniform and soft comparable to parenchyma was observed in neuroendocrine tumor, and mixture of various colors was observed in chronic pancreatitis. Moreover, they performed US-RTE for 53 pancreatic tumors prospectively, and reported that diagnostic accuracy of B-mode alone was about 70%-80%, while that of combination with US-RTE was more than 90%. Because qualitative diagnosis using color map was subjective and highly operator dependent, quantitative diagnosis using strain ratio was established since the second-generation RTE (Figure 3). Strain ratio is defined as the ratio of the strain of reference tissue (B) divided by the strain of target tissue (A), so that the strain 3714 April 14, 2016 Volume 22 Issue 14
 [A] is set on the tumor, and ROI [B] is set on read area around the pancreas (left).")
29 Kawada N et al. Elastography for the pancreas Figure 3 Quantitative diagnosis in US-Real-time Tissue Elastography TM. A hypoechoic tumor is seen at the pancreatic tail in B-mode (right). Region of interest (ROI) [A] is set on the tumor, and ROI [B] is set on read area around the pancreas (left). By setting ROI [A] and [B], strain [A], strain [B], and strain ration [B/A] were calculated automatically and displayed at the bottom of the screen (left). of target tissue can be digitalized. Strain ratio is the conversion of the theory called fat lesion ratio reported in the breast, which means the ratio of the strain of fat around the mammary gland divided by the strain of target tissue. This theory is based on the idea that stiffness of fat is almost equal in different individuals [32]. However, there is no consensus where to set reference area for the pancreas instead of fat around the mammary gland for the breast. Some investigators set reference area on non-tumorous area inside pancreatic parenchyma [33,34], and the other investigators set reference area on red area around the pancreas which was estimated as fat [35,36] (Figure 4). However, there is no evidence if red area around pancreas is really fat. It is known that strain ratios calculated for the same target tissue quite differ according to wherever the reference area is set. Kawada et al [33] performed the second-generation US-RTE for consecutive 36 solid pancreatic tumors. They reported that strain ration was higher in ductal adenocarcinomas compared to that in benign tumors, and different color patterns were observed between ductal adenocarcinomas of < 25 mm and those of 25 mm. The cutoff levels of strain ratio optimal for differential diagnosis between malignancy and benignancy are quite different in each report [34-36], indicating RTE is highly operator dependent and lacks adequate reproducibility. Because the pancreas locates deep in center of the body, patients body shape and body position during examination may affect measuring the strain ratio. In order to minimize such effects associated with patients body shape and body position, Kawada et al [37] compared the strain ratios obtained from the same pancreatic cancer patients with the same body position during examination before and after chemo-radiation therapy. They concluded that treatment effect evaluated histologically after chemo-radiation was greater in the group with much reduced strain ratio than that in the group with less reduced strain ratio. EUS was used in most reports evaluating RTE for the pancreas, as described later. A fine B-mode image is required for a fine elastogram, and generally a fine B-mode image is obtained within 6 cm in depth from the body surface in US. Therefore, elastogram cannot be obtained if the pancreas locates deep from the body surface, for example, in the obese. These problems will occur less frequently in EUS because the distance between the probe and the pancreas is shorter in EUS compared to that in US. In addition to that, B-mode image is easily affected by gastrointestinal gas in US, while it occurs infrequently in EUS. However, US-RTE is still considered to be a promising imaging examination for the selective patients due to its non-invasive nature. There are also other promising US-elastographies, which are Elastography TM (GE) (Figure 5), and Elastography TM (Toshiba) (Figure 6). However, there are no studies evaluating the usefulness of these instruments to date. Further information of these instruments is available in the guidelines [12]. These instruments are not available in EUS. US-elastography - Shear wave elastograhy Because manual compression is not effective for the pancreas which locates deep in center of the body, the strain must be generated by aortic pulsation. Therefore, a fine elastogram cannot be always obtained depending 3715 April 14, 2016 Volume 22 Issue 14
.")
30 Kawada N et al. Elastography for the pancreas Figure 4 Setting the different reference area in a case of pancreatic tail tumor. Strain ratio quite differs according to the reference area: When the reference area is set on non-tumorous area of the pancreas, strain ration is calculated as (upper). When the reference area was set on read area around the pancreas, strain ration is calculated as on the location of the pancreas in strain elastography. In contrast, emission of ARFI is possible for entire pancreas wherever desired in shear wave elastography. Therefore, shear wave elastography is considered as a break-through in the history of elastography for the pancreas. Virtual Touch TM Quantification (VTQ) produced by Siemens is a representative instrument of shear wave elastography. VTQ shows the stiffness of target tissue digitally by measuring shear wave velocity (SWV). SWV is displayed on the right side of the screen in m/s (Figure 7). In case of measurement failure, X,XX m/s is displayed on the screen instead of digits (Figure 8). The first report evaluating the usefulness of VTQ for the pancreas was published in 2009 [38]. In this case report, D Onofrio et al [38] reported that a pancreatic tumor which was diagnosed as solid pancreatic tumor by US and CT in advance was finally diagnosed as serous cystic neoplasm by VTQ. In this case, X,XX m/s was always displayed on the screen during VTQ which indicated the tumor was not solid but cystic. Yashima et al [39] subjected 46 patients with chronic pancreatitis and 52 normal pancreas, and measured SWV at the head, the body and the tail of the pancreas for 10 times in each case. The success rates of > 60% for measuring SWV at the head, the body and the tail of the pancreas were 69%, 75%, and 42%, respectively. They also determined the cutoff of SWV optimal for diagnosing chronic pancreatitis as 1.40 m/s by ROC analysis, and reported that 3716 April 14, 2016 Volume 22 Issue 14

![Two years later, the improved success rates of 100% for measuring SWV at the head, the body, and the tail of the pancreas were reported to be 80%, 83%, and 68%, respectively by Kawada et al [40].](/docs-images/92/109922872/images/31-1.jpg "They also determined the factors associated with the stiffness of the pancreas (> 1.40 m/s) as severe alcohol intake (OR = 3.87, P = 0.005) and deeper depth of the pancreas from the body surface 4.")
31 Kawada N et al. Elastography for the pancreas A B Figure 5 Elastography TM. A: Elastography (GE) is performed for a normal pancreas; B: Strain ration can be calculated by setting the reference area. sensitivity, specificity, PPV, and NPV for diagnosing chronic pancreatitis were 75%, 72%, 69%, and 78%, respectively. Two years later, the improved success rates of 100% for measuring SWV at the head, the body, and the tail of the pancreas were reported to be 80%, 83%, and 68%, respectively by Kawada et al [40]. They also determined the factors associated with the stiffness of the pancreas (> 1.40 m/s) as severe alcohol intake (OR = 3.87, P = 0.005) and deeper depth of the pancreas from the body surface 4.2 cm, OR = 0.10, P = 0.002) by multivariate analysis. Also, they reported that the stiffness of non-tumorous pancreas tended to be higher in patients with pancreatic ductal adenocarcinoma compared to that in patients without pancreatic ductal adenocarcinoma. The clinical implication of VTQ would be enormous if VTQ could identify the high-risk group for pancreatic cancer by measuring SWV of the pancreas because VTQ can be performed even for asymptomatic due to its non-invasive nature. Recently, series of studies evaluating the usefulness of VTQ for the pancreas were published [41-46]. A study reported the usefulness of VTQ for differential diagnosis between malignant and benign pancreatic tumors [41], and another reported the usefulness of VTQ for diagnosis of acute pancreatitis [42]. There is also a study reporting the possibility of discriminating serous cyst fluid from mucinous one [43]. As already mentioned in this text, RTE cannot evaluate cystic lesions, therefore, it is interesting if VTQ can really evaluate cystic lesions, too. In addition to these, there are studies reporting that the stiffness of the pancreas measured preoperatively could predict the incidence of post-operative pancreatic juice fistula. Harada et al [44] measured the stiffness of nontumorous pancreas preoperatively for 62 patients 3717 April 14, 2016 Volume 22 Issue 14
 is performed for a normal pancreas; B: Strain ration can be calculated by setting the reference area. who subsequently underwent pancreatectomy.")
32 Kawada N et al. Elastography for the pancreas A B Figure 6 Elastography TM (Toshiba). A: Elastography (Toshiba) is performed for a normal pancreas; B: Strain ration can be calculated by setting the reference area. who subsequently underwent pancreatectomy. They reported that there were positive correlation between SWV and histological grade of fibrosis [Spearman s rank correlation coefficient (ρ) = 0.660, P < ]. Also, they reported that post-operative pancreatic juice fistula was observed more frequently in patients with lower stiffness of the pancreas (SWV < 1.54 m/s) than in patients with higher stiffness of the pancreas (63% vs 17%, P < 0.001). Shear wave elastography had begun with the measurement of SWV, subsequently Virtual Touch TM Imaging and Quantification (VTIQ, Siemens) was developed. In VTIQ, the stiffness of organ can be displayed on the screen in color map (Figure 9). VTIQ is available in Japan since March 2012, and only linear probe can be used in VTIQ to date. There are several reports evaluating the usefulness of VTIQ for the other organs [47-50], however, there are none for the pancreas. ElastPQ produced by Philip is another instrument for shear wave elastography. In ElastPQ, SWV is shown in kpa. There are a report evaluating the correlation between VTQ and ElastPQ for the liver [51], however, there are none for the pancreas. Shear wave elastography seems to be appropriate for the pancreas for which it is not always easy to obtain adequate strain from aortic pulsation. There are more and more studies reporting the usefulness of shear wave elastography for the pancreas in recent years [40-46]. Further development of shear wave elastography, such as availability in EUS, is required April 14, 2016 Volume 22 Issue 14
 is displayed in the right side of the screen in a few seconds.")

33 Kawada N et al. Elastography for the pancreas Figure 7 Virtual Touch Quantification TM (Siemens) performed for the pancreatic head. Region of interest is set on the pancreatic head. Subsequently, acoustic radiation force impulse is emitted by pressing the button, and shear wave velocity (m/s) is displayed in the right side of the screen in a few seconds. Figure 8 Virtual Touch TM Quantification (Siemens) performed for a large tumor at the pancreatic body. Shear wave velocity cannot be measured because the tumor is too hard. X,XX m/s is displayed in the right side of the screen instead of digits. EUS-elastography - Strain elastography Hirooka et al [13] had first reported the clinical usefulness of EUS-elastography for the pancreas in 2005, there are a considerable number of reports related to EUSelastography for the pancreas [52-65]. There are also several meta-analyses related to EUS-elastography for the pancreas [52-55]. Because RTE is a single instrument in which EUS-elastography can be performed, RTE is evaluated in all reports regarding EUS-elastography for the pancreas. Recently, another EUS-elastographic instrument, ELST TM, was produced by Olympus. ELST is considered to be almost the same as RTE because the technology used in ELST was provided by Hitachi- Aloka. Most reports regarding EUS-elastography for the pancreas are associated with the differential diagnosis between benign and malignant solid pancreatic tumors. Several meta-analyses related to the differential diagnosis of pancreatic tumors have been reported since 2012 [52-55]. In summary, sensitivity of EUSelastography for the differential diagnosis of pancreatic tumors is reported to be excellent ranging from 95% to 99%, while its specificity is reported to be inadequate ranging from 67% to 76%. It is assumed that most benign pancreatic tumors are tumor forming pancreatitis, and benign pancreatitis with severe fibrosis can be as hard as malignant ductal adenocarcinoma. EUS-elastography cannot be a surrogate examination for EUS-FNA, however, EUS-elastography may be a crucial examination for the selective cases in which EUS-FNA cannot be performed [66]. The criteria for differential diagnosis between malignant and benign pancreatic tumors differ from report to report. Despite the qualitative diagnostic criteria for distinguishing malignancy from benignancy differ from report to report, most of them consist of the following two factors: (1) the dominant color within color map; and (2) the homogeneity of color map, as shown in Figure 10. In RTE, the softest tissue within ROI is displays as red while the hardest tissue within ROI is displayed as blue, and the remaining tissue is displayed as a coordinated color between red and blue according to the stiffness of the tissue. Thus, we should keep in mind that the color map observed in RTE is not an absolute one but will be changed depending on the size of ROI. Iglesias-Garcia et al [56] subjected 77 ductal adenocarcinomas, 42 tumor forming pancreatitis, and 10 endocrine tumors, and classified them according to the combination of the dominant color within color map (blue or green) and the homogeneity of color map (homogeneous or heterogeneous). When the combination of green and heterogeneous were determined as benign tumor forming pancreatitis, blue and homogeneous were determined as endocrine tumor, and blue and heterogeneous were determined as ductal adenocarcinoma, sensitivity, specificity, PPV, and NPV were 100%, 85.5%, 90.7%, and 100%, respectively. These excellent diagnostic accuracies were also shown with good concordance rate between two blinded investigators. Giovannini et al [57] conducted a multicenter study subjecting 121 patients with pancreatic tumors (92 malignant and 29 benign). In their study, pancreatic tumors were classified according to the following scoring system: Score 1, homogeneous green corresponding to normal tissue; Score 2, heterogeneous soft tissue (green, yellow, and red) corresponding to inflammatory tissue; Score 3, mixed color or honeycombed corresponding to indeterminate; Score 4, small green central area surrounded by mainly blue; Score 5, mainly blue with heterogeneous green and red corresponding advanced malignant lesion [57]. When score 1 and 2 were determined as benign and score 4 and 5 as malignant, sensitivity and specificity were 92.3% and 80%, respectively, and kappa coefficient was shown to be One of the quantitative diagnostic methods 3719 April 14, 2016 Volume 22 Issue 14
 cannot be performed for the case in which the pancreas locates deep from the body surface.")

. Dominant color and homogeneity of color are evaluated in most reports.")



34 Kawada N et al. Elastography for the pancreas A B Figure 9 Virtual Touch TM IQ (Siemens) performed for a pancreatic body tumor. Because only linear probe can be used, Virtual Touch TM IQ (VTIQ) cannot be performed for the case in which the pancreas locates deep from the body surface. Shear wave velocity can be measured post hoc at the point wherever desired (upper). In quality mode, the degree of confidence in measurement is seen for each point (lower). Green color shows the point where shear wave velocity is measured with high confidence. Homogeneity Dominant color Homogeneous Normal pancreas Heterogeneous Chronic pancreatitis Green Blue Neuroendocrine tumor Pancreatic ductal adenocarcinoma Figure 10 A representative qualitative diagnostic criteria in Real-time Tissue Elastography TM (Hitachi-Aloka). Dominant color and homogeneity of color are evaluated in most reports. The representative histology estimated by each combination of color and homogeneity are shown. frequently used for EUS-elastography is a strain ratio analysis. Itokawa et al [34] subjected 72 ductal adenocarcinomas and 7 tumor forming pancreatitis, and reported that strain ratio was significantly higher in ductal adenocarcinomas compared to that in tumor forming pancreatitis (39.08 ± vs ± 12.65, P < 0.05). Iglesias-Garcia et al [35] subjected 86 pancreatic tumors including 49 ductal adenocarcinomas, 27 tumor forming pancreatitis, 6 endocrine carcinomas, and 2 metastatic carcinomas. They reported when cutoff of strain ratio optimal for distinguishing malignancy from benignancy was determined as 6.04, sensitivity and specificity were 100% and 92.9%, respectively. Dawwas et al [36] subjected 74 ductal adenocarcinomas, 11 endocrine carcinomas, 2 metastatic carcinomas, and 17 tumor forming pancreatitis, and reported when cutoff was determined as 4.65, sensitivity and specificity were 100% and 16.7%, respectively. As shown above, optimal cutoff values of strain ratio quite differ from report to report. It is assumed that cutoff value was affected by where to set the reference area: non-tumorous pancreas was determined as reference area in the former report, whereas red area around the pancreas was determined as reference area in the latter two reports. Another quantitative diagnostic method is a strain 3720 April 14, 2016 Volume 22 Issue 14
35 Kawada N et al. Elastography for the pancreas histogram analysis. In the strain histogram analysis, the stiffness of tissue is converted into 256-grade gray scale or digits, and gray scale map or gray scale histogram is shown on the screen. Săftoiu et al [58] conducted multicenter study subjecting 258 pancreatic tumors, and performed strain histogram analysis. When cutoff of strain histogram was determined as 175 calculated by ROC analysis (AUC = 0.854, P < ), sensitivity, specificity, PPV and NPV for distinguishing malignancy from benignancy were 93.4%, 66.0%, 92.5%, 68.9%, respectively. Opačić et al [59] performed strain histogram analysis subjecting 105 pancreatic tumors, and reported when cutoff was determined as 86, sensitivity and specificity were 100% and 45%, respectively. Cutoff values also quite differ from report to report in strain histogram analysis. The other quantitative diagnostic method is a neural network analysis [57,58]. The neural network analysis is a method developed by Săftoiu et al [58] and is performed by computer which can avoid arbitrary analysis. However, the neural network analysis is not prevalent among other investigators. Next, we are moving on diffuse pancreatic diseases. Itoh et al [62] performed EUS-elastography preoperatively for the proximal side of the pancreatic tumor in order to exclude possible effects of obstructive pancreatitis, and compared the elastograms with microscopic findings of the resected specimens. They reported when using 4 parameters of mean, standard deviation, skewness, kurtosis, there were significant correlation between 4 parameters and grade of fibrosis evaluated pathologically (r = -0.75, -0.54, 0.69, and 0.67, respectively). Iglesias-Garcia et al [63] subjected 191 chronic pancreatitis, and compared strain ratio with Rosemont classification, a well-known diagnostic criteria for chronic pancreatitis evaluated by EUS. They reported that there was positive correlation between strain ratio and Rosemont classification (r = 0.813, P < ). They reported when cutoff for diagnosing chronic pancreatitis was determined as 2.25 by ROC analysis (AUC = 0.949), sensitivity was shown to be 91.1%. Janssen et al [64] found that stiffness of the normal pancreas was increasing with aging. They reported that the value of strain histogram measured in normal pancreas was significantly lower in individuals of 60 years compared to that in individuals of < 60 years, although it was significantly higher in individuals of 60 years compared to that in patients with chronic pancreatitis (110.2 vs 80.0 vs 32.4, respectively, P < 0.001). A recent study reported that EUS-elastography could predict pancreatic exocrine dysfunction in patients with chronic pancreatitis [65]. Iglesias-Garcia et al [56] hypothesized that pancreatic exocrine function was depend on the grade of pancreatic fibrosis, and measured strain ratio in 115 patients with chronic pancreatitis. They reported that there was significant correlation between strain ratio and pancreatic exocrine dysfunction evaluated by 13 C-mixed triglyceride breath test. Thus, investigations of EUS-RTE were proceeded mainly through establishing the diagnostic criteria for differential diagnosis between malignant and benign pancreatic tumors [52-61]. Because EUS is a detailed examination, investigators might often encounter a situation in which a known pancreatic tumor must be evaluated if it was malignant or not. It is important to take advantage of each modality: US-elastography for screening and EUS-elastography for detailed examination. FUTURE PERSPECTIVES The goal of elastography for the pancreas is to assure accurate elastogram enough to reflect histological structure. Also, elastography for the pancreas must be operator-independent and satisfy the adequate reproducibility. The following facts that (1) the pancreas is a small organ locates deep in center of the body; (2) obtaining the biopsy specimens from the pancreas is not easy; and (3) the pancreas is strongly affected by aortic pulsation, make difficult to achieve the goal. There may be another breakthrough by developing an instrument based on a novel principle beyond shear wave elastography in the future. Although there are several issues remained to be solved, elastography may be a promising imaging modality for early detection of chronic pancreatitis. It is known that patients with chronic pancreatitis are at risk for pancreatic cancer, therefore, chronic pancreatitis should be diagnosed within reversible stage so that it can be cured by therapeutic intervention. At the current moment, EUS is considered to be the best imaging modality which can detect early chronic pancreatitis [67,68]. However, the diagnostic criteria used in EUS, such as hyperechoic foci and stranding, are associated with calcification which are irreversible change. In contrast, elastography may detect earlier signs of chronic pancreatitis, such as parenchymal edema, only if they can be recognized as change of tissue stiffness. Also, elastography may contribute to early detection of pancreatic cancer. Early detection of pancreatic cancer is important because better prognosis cannot be achieved without its early detection. As described in the text, US-elastography can pick up the highrisk patients for pancreatic cancer from numerous asymptomatic because US-elastography can be performed as physical check-up. If diffuse or focal stiffness is detected by US-elastography, this person can undergo further detailed examination for the pancreas, which may detect early pancreatic cancer. REFERENCES 1 Itoh A, Ueno E, Tohno E, Kamma H, Takahashi H, Shiina T, Yamakawa M, Matsumura T. Breast disease: clinical application of US elastography for diagnosis. Radiology 2006; 239: [PMID: ] 3721 April 14, 2016 Volume 22 Issue 14
36 Kawada N et al. Elastography for the pancreas 2 Lyshchik A, Higashi T, Asato R, Tanaka S, Ito J, Mai JJ, Pellot- Barakat C, Insana MF, Brill AB, Saga T, Hiraoka M, Togashi K. Thyroid gland tumor diagnosis at US elastography. Radiology 2005; 237: [PMID: ] 3 Sporea I, Bota S, Peck-Radosavljevic M, Sirli R, Tanaka H, Iijima H, Badea R, Lupsor M, Fierbinteanu-Braticevici C, Petrisor A, Saito H, Ebinuma H, Friedrich-Rust M, Sarrazin C, Takahashi H, Ono N, Piscaglia F, Borghi A, D Onofrio M, Gallotti A, Ferlitsch A, Popescu A, Danila M. Acoustic Radiation Force Impulse elastography for fibrosis evaluation in patients with chronic hepatitis C: an international multicenter study. Eur J Radiol 2012; 81: [PMID: DOI: / j.ejrad ] 4 Bota S, Sporea I, Peck-Radosavljevic M, Sirli R, Tanaka H, Iijima H, Saito H, Ebinuma H, Lupsor M, Badea R, Fierbinteanu- Braticevici C, Petrisor A, Friedrich-Rust M, Sarrazin C, Takahashi H, Ono N, Piscaglia F, Marinelli S, D Onofrio M, Gallotti A, Salzl P, Popescu A, Danila M. The influence of aminotransferase levels on liver stiffness assessed by Acoustic Radiation Force Impulse Elastography: a retrospective multicentre study. Dig Liver Dis 2013; 45: [PMID: DOI: / j.dld ] 5 Hong H, Li J, Jin Y, Li Q, Li W, Wu J, Huang Z. Performance of real-time elastography for the staging of hepatic fibrosis: a metaanalysis. PLoS One 2014; 9: e [PMID: DOI: /journal.pone ] 6 Kobayashi K, Nakao H, Nishiyama T, Lin Y, Kikuchi S, Kobayashi Y, Yamamoto T, Ishii N, Ohashi T, Satoh K, Nakade Y, Ito K, Yoneda M. Diagnostic accuracy of real-time tissue elastography for the staging of liver fibrosis: a meta-analysis. Eur Radiol 2015; 25: [PMID: DOI: / s x] 7 Nakashima K, Shiina T, Sakurai M, Enokido K, Endo T, Tsunoda H, Takada E, Umemoto T, Ueno E. JSUM ultrasound elastography practice guidelines: breast. J Med Ultrasonics 2013; 40: [DOI: /s ] 8 Kudo M, Shiina T, Moriyasu F, Iijima H, Tateishi R, Yada N, Fujimoto K, Morikawa H, Hirooka M, Sumino Y, Kumada T. JSUM ultrasound elastography practice guidelines: liver. J Med Ultrasonics 2013; 40: [DOI: /s ] 9 Cosgrove D, Piscaglia F, Bamber J, Bojunga J, Correas JM, Gilja OH, Klauser AS, Sporea I, Calliada F, Cantisani V, D Onofrio M, Drakonaki EE, Fink M, Friedrich-Rust M, Fromageau J, Havre RF, Jenssen C, Ohlinger R, Săftoiu A, Schaefer F, Dietrich CF. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: Clinical applications. Ultraschall Med 2013; 34: [PMID: DOI: / s ] 10 Barr RG, Nakashima K, Amy D, Cosgrove D, Farrokh A, Schafer F, Bamber JC, Castera L, Choi BI, Chou YH, Dietrich CF, Ding H, Ferraioli G, Filice C, Friedrich-Rust M, Hall TJ, Nightingale KR, Palmeri ML, Shiina T, Suzuki S, Sporea I, Wilson S, Kudo M. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 2: breast. Ultrasound Med Biol 2015; 41: [PMID: DOI: /j.ultrasmedbio ] 11 Ferraioli G, Filice C, Castera L, Choi BI, Sporea I, Wilson SR, Cosgrove D, Dietrich CF, Amy D, Bamber JC, Barr R, Chou YH, Ding H, Farrokh A, Friedrich-Rust M, Hall TJ, Nakashima K, Nightingale KR, Palmeri ML, Schafer F, Shiina T, Suzuki S, Kudo M. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 3: liver. Ultrasound Med Biol 2015; 41: [PMID: DOI: /j.ultrasmedbio ] 12 Hirooka Y, Kuwahara T, Irisawa A, Itokawa F, Uchida H, Sasahira N, Kawada N, Itoh Y, Shiina T. JSUM ultrasound elastography practice guidelines: pancreas. J Med Ultrason (2001) 2015; 42: [PMID: DOI: /s ] 13 Hirooka Y, Itoh A, Hashimoto S. Utility of EIS: Elastography in the diagnosis of pancreatic diseases. Gastrointest Endosc 2005; 61: AB282 [DOI: /S (05) ] 14 Uchida H, Hirooka Y, Ito A, Hashimoto S, Kawashima H, Hara K, Kanamori A, Goto J, Ishikawa S, Ohmiya N, Niwa Y, Goto H. Utility of elastography in the diagnosis of pancreaic diseases using transabdominal ultrasonography. Gastroenterology 2005; 128: A Shiina T, Doyley MM, Bamber JC. Strain imaging using combined RF and envelope autocorrelation processing. Procceding of the 1996 IEEE Int Ultrasonics Symposium. San Antonio: IEEE, 1996 [DOI: /ULTSYM ] 16 Shiina T, Yamakawa M, Nitta N. Recent prognosis of ultrasound elasticity imaging technology. International Congress Series 2004; 1274: [DOI: /j.ics ] 17 Herman BA, Harris GR. Models and regulatory considerations for transient temperature rise during diagnostic ultrasound pulses. Ultrasound Med Biol 2002; 28: [PMID: ] 18 Dalecki D, Raeman CH, Child SZ, Penney DP, Mayer R, Carstensen EL. The influence of contrast agents on hemorrhage produced by lithotripter fields. Ultrasound Med Biol 1997; 23: [PMID: ] 19 Barnett SB, Duck F, Ziskin M. Recommendations on the safe use of ultrasound contrast agents. Ultrasound Med Biol 2007; 33: [PMID: ] 20 Dalecki D, Raeman CH, Child SZ, Penney DP, Carstensen EL. Remnants of Albunex nucleate acoustic cavitation. Ultrasound Med Biol 1997; 23: [PMID: ] 21 Chen G, Liu S, Zhao Y, Dai M, Zhang T. Diagnostic accuracy of endoscopic ultrasound-guided fine-needle aspiration for pancreatic cancer: a meta-analysis. Pancreatology 2013; 13: [PMID: DOI: /j.pan ] 22 Puli SR, Bechtold ML, Buxbaum JL, Eloubeidi MA. How good is endoscopic ultrasound-guided fine-needle aspiration in diagnosing the correct etiology for a solid pancreatic mass?: A meta-analysis and systematic review. Pancreas 2013; 42: [PMID: DOI: /MPA.0b013e e79] 23 Hewitt MJ, McPhail MJ, Possamai L, Dhar A, Vlavianos P, Monahan KJ. EUS-guided FNA for diagnosis of solid pancreatic neoplasms: a meta-analysis. Gastrointest Endosc 2012; 75: [PMID: DOI: /j.gie ] 24 Chen J, Yang R, Lu Y, Xia Y, Zhou H. Diagnostic accuracy of endoscopic ultrasound-guided fine-needle aspiration for solid pancreatic lesion: a systematic review. J Cancer Res Clin Oncol 2012; 138: [PMID: DOI: / s ] 25 Thosani N, Thosani S, Qiao W, Fleming JB, Bhutani MS, Guha S. Role of EUS-FNA-based cytology in the diagnosis of mucinous pancreatic cystic lesions: a systematic review and meta-analysis. Dig Dis Sci 2010; 55: [PMID: DOI: / s ] 26 Carrara S, Arcidiacono PG, Mezzi G, Petrone MC, Boemo C, Testoni PA. Pancreatic endoscopic ultrasound-guided fine needle aspiration: complication rate and clinical course in a single centre. Dig Liver Dis 2010; 42: [PMID: DOI: / j.dld ] 27 Lee LS, Saltzman JR, Bounds BC, Poneros JM, Brugge WR, Thompson CC. EUS-guided fine needle aspiration of pancreatic cysts: a retrospective analysis of complications and their predictors. Clin Gastroenterol Hepatol 2005; 3: [PMID: ] 28 Jonkman EF, van Tuyl BA, Sanders FB, Haas LE. Severe acute pancreatitis after EUS-FNA of a pancreatic cyst: a rare, but serious complication. BMJ Case Rep 2015; 2015: pii bcr [PMID: DOI: /bcr ] 29 Ngamruengphong S, Xu C, Woodward TA, Raimondo M, Stauffer JA, Asbun HJ, Wallace MB. Risk of gastric or peritoneal recurrence, and long-term outcomes, following pancreatic cancer resection with preoperative endosonographically guided fine needle aspiration. Endoscopy 2013; 45: [PMID: DOI: /s ] 30 Tanaka S, Nakaizumi A, Ioka T, Takakura R, Uehara H, Nakao M, Suzuki R, Fukuda J, Ishikawa O, Ohigashi H. Periodic ultra April 14, 2016 Volume 22 Issue 14
37 Kawada N et al. Elastography for the pancreas sonography checkup for the early detection of pancreatic cancer: preliminary report. Pancreas 2004; 28: [PMID: ] 31 Uchida H, Hirooka Y, Itoh A, Kawashima H, Hara K, Nonogaki K, Kasugai T, Ohno E, Ohmiya N, Niwa Y, Katano Y, Ishigami M, Goto H. Feasibility of tissue elastography using transcutaneous ultrasonography for the diagnosis of pancreatic diseases. Pancreas 2009; 38: [PMID: DOI: /MPA.0b013e318184db78] 32 Umemoto T, Ueno E, Matsumura T, Yamakawa M, Bando H, Mitake T, Shiina T. Ex vivo and in vivo assessment of the nonlinearity of elasticity properties of breast tissues for quantitative strain elastography. Ultrasound Med Biol 2014; 40: [PMID: DOI: /j.ultrasmedbio ] 33 Kawada N, Tanaka S, Uehara H, Takakura R, Katayama K, Fukuda J, Matsuno N, Takenaka A, Ishikawa O. Feasibility of second-generation transabdominal ultrasound-elastography to evaluate solid pancreatic tumors: preliminary report of 36 cases. Pancreas 2012; 41: [PMID: DOI: / MPA.0b013e b84] 34 Itokawa F, Itoi T, Sofuni A, Kurihara T, Tsuchiya T, Ishii K, Tsuji S, Ikeuchi N, Umeda J, Tanaka R, Yokoyama N, Moriyasu F, Kasuya K, Nagao T, Kamisawa T, Tsuchida A. EUS elastography combined with the strain ratio of tissue elasticity for diagnosis of solid pancreatic masses. J Gastroenterol 2011; 46: [PMID: DOI: /s ] 35 Iglesias-Garcia J, Larino-Noia J, Abdulkader I, Forteza J, Dominguez-Munoz JE. Quantitative endoscopic ultrasound elastography: an accurate method for the differentiation of solid pancreatic masses. Gastroenterology 2010; 139: [PMID: DOI: /j.gastro ] 36 Dawwas MF, Taha H, Leeds JS, Nayar MK, Oppong KW. Diagnostic accuracy of quantitative EUS elastography for discriminating malignant from benign solid pancreatic masses: a prospective, single-center study. Gastrointest Endosc 2012; 76: [PMID: DOI: /j.gie ] 37 Kawada N, Tanaka S, Uehara H, Katayama K, Hosoki T, Takami M, Tomita Y. Alteration of strain ratio evaluated by transabdominal ultrasound elastography may predict the efficacy of preoperative chemoradiation performed for pancreatic ductal carcinoma: preliminary results. Hepatogastroenterology 2014; 61: [PMID: ] 38 D'Onofrio M, Gallotti A, Martone E, Pozzi Mucelli R. Solid appearance of pancreatic serous cystadenoma diagnosed as cystic at ultrasound acoustic radiation force impulse imaging. JOP 2009; 10: [PMID: ] 39 Yashima Y, Sasahira N, Isayama H, Kogure H, Ikeda H, Hirano K, Mizuno S, Yagioka H, Kawakubo K, Sasaki T, Nakai Y, Tada M, Yoshida H, Omata M, Koike K. Acoustic radiation force impulse elastography for noninvasive assessment of chronic pancreatitis. J Gastroenterol 2012; 47: [PMID: DOI: / s x] 40 Kawada N, Tanaka S, Uehara H, Ohkawa K, Yamai T, Takada R, Shiroeda H, Arisawa T, Tomita Y. Potential use of point shear wave elastography for the pancreas: a single center prospective study. Eur J Radiol 2014; 83: [PMID: DOI: / j.ejrad ] 41 Park MK, Jo J, Kwon H, Cho JH, Oh JY, Noh MH, Nam KJ. Usefulness of acoustic radiation force impulse elastography in the differential diagnosis of benign and malignant solid pancreatic lesions. Ultrasonography 2014; 33: [PMID: DOI: /usg.13017] 42 Göya C, Hamidi C, Okur MH, Içer M, Oğuz A, Hattapoğlu S, Cetinçakmak MG, Teke M. The utility of acoustic radiation force impulse imaging in diagnosing acute appendicitis and staging its severity. Diagn Interv Radiol 2014; 20: [PMID: DOI: /dir ] 43 D'Onofrio M, Crosara S, Canestrini S, Demozzi E, De Robertis R, Salvia R, Bassi C, Mucelli RP. Virtual analysis of pancreatic cystic lesion fluid content by ultrasound acoustic radiation force impulse quantification. J Ultrasound Med 2013; 32: [PMID: ] 44 Harada N, Ishizawa T, Inoue Y, Aoki T, Sakamoto Y, Hasegawa K, Sugawara Y, Tanaka M, Fukayama M, Kokudo N. Acoustic radiation force impulse imaging of the pancreas for estimation of pathologic fibrosis and risk of postoperative pancreatic fistula. J Am Coll Surg 2014; 219: e5 [PMID: DOI: /j.jamcollsurg ] 45 Hatano M, Watanabe J, Kushihata F, Tohyama T, Kuroda T, Koizumi M, Kumagi T, Hisano Y, Sugita A, Takada Y. Quantification of pancreatic stiffness on intraoperative ultrasound elastography and evaluation of its relationship with postoperative pancreatic fistula. Int Surg 2015; 100: [PMID: DOI: /INTSURG-D ] 46 Lee TK, Kang CM, Park MS, Choi SH, Chung YE, Choi JY, Kim MJ. Prediction of postoperative pancreatic fistulas after pancreatectomy: assessment with acoustic radiation force impulse elastography. J Ultrasound Med 2014; 33: [PMID: DOI: /ultra ] 47 Golatta M, Schweitzer-Martin M, Harcos A, Schott S, Junkermann H, Rauch G, Sohn C, Heil J. Normal breast tissue stiffness measured by a new ultrasound technique: virtual touch tissue imaging quantification (VTIQ). Eur J Radiol 2013; 82: e676-e679 [PMID: DOI: /j.ejrad ] 48 Ianculescu V, Ciolovan LM, Dunant A, Vielh P, Mazouni C, Delaloge S, Dromain C, Blidaru A, Balleyguier C. Added value of Virtual Touch IQ shear wave elastography in the ultrasound assessment of breast lesions. Eur J Radiol 2014; 83: [PMID: DOI: /j.ejrad ] 49 Golatta M, Schweitzer-Martin M, Harcos A, Schott S, Gomez C, Stieber A, Rauch G, Domschke C, Rom J, Schütz F, Sohn C, Heil J. Evaluation of virtual touch tissue imaging quantification, a new shear wave velocity imaging method, for breast lesion assessment by ultrasound. Biomed Res Int 2014; 2014: [PMID: DOI: /2014/960262] 50 Matsuzuka T, Suzuki M, Saijo S, Ikeda M, Matsui T, Nomoto Y, Nomoto M, Imaizumi M, Tada Y, Omori K. Stiffness of salivary gland and tumor measured by new ultrasonic techniques: Virtual touch quantification and IQ. Auris Nasus Larynx 2015; 42: [PMID: DOI: /j.anl ] 51 Sporea I, Bota S, Grădinaru-Taşcău O, Şirli R, Popescu A. Comparative study between two point Shear Wave Elastographic techniques: Acoustic Radiation Force Impulse (ARFI) elastography and ElastPQ. Med Ultrason 2014; 16: [PMID: ] 52 Mei M, Ni J, Liu D, Jin P, Sun L. EUS elastography for diagnosis of solid pancreatic masses: a meta-analysis. Gastrointest Endosc 2013; 77: [PMID: DOI: / j.gie ] 53 Ying L, Lin X, Xie ZL, Tang FY, Hu YP, Shi KQ. Clinical utility of acoustic radiation force impulse imaging for identification of malignant liver lesions: a meta-analysis. Eur Radiol 2012; 22: [PMID: DOI: /s ] 54 Li X, Xu W, Shi J, Lin Y, Zeng X. Endoscopic ultrasound elastography for differentiating between pancreatic adenocarcinoma and inflammatory masses: a meta-analysis. World J Gastroenterol 2013; 19: [PMID: DOI: /wjg.v19. i ] 55 Pei Q, Zou X, Zhang X, Chen M, Guo Y, Luo H. Diagnostic value of EUS elastography in differentiation of benign and malignant solid pancreatic masses: a meta-analysis. Pancreatology 2012; 12: [PMID: DOI: /j.pan ] 56 Iglesias-Garcia J, Larino-Noia J, Abdulkader I, Forteza J, Dominguez-Munoz JE. EUS elastography for the characterization of solid pancreatic masses. Gastrointest Endosc 2009; 70: [PMID: DOI: /j.gie ] 57 Giovannini M, Thomas B, Erwan B, Christian P, Fabrice C, Benjamin E, Geneviève M, Paolo A, Pierre D, Robert Y, Walter S, Hanz S, Carl S, Christoph D, Pierre E, Jean-Luc VL, Jacques D, Peter V, Andrian S. Endoscopic ultrasound elastography for evaluation of lymph nodes and pancreatic masses: a multicenter study. World J Gastroenterol 2009; 15: [PMID: DOI: /wjg ] 3723 April 14, 2016 Volume 22 Issue 14
38 Kawada N et al. Elastography for the pancreas 58 Săftoiu A, Vilmann P. Differential diagnosis of focal pancreatic masses by semiquantitative EUS elastography: between strain ratios and strain histograms. Gastrointest Endosc 2013; 78: [PMID: DOI: /j.gie ] 59 Opačić D, Rustemović N, Kalauz M, Markoš P, Ostojić Z, Majerović M, Ledinsky I, Višnjić A, Krznarić J, Opačić M. Endoscopic ultrasound elastography strain histograms in the evaluation of patients with pancreatic masses. World J Gastroenterol 2015; 21: [PMID: DOI: /wjg.v21.i ] 60 Săftoiu A, Vilmann P, Gorunescu F, Janssen J, Hocke M, Larsen M, Iglesias-Garcia J, Arcidiacono P, Will U, Giovannini M, Dietrich CF, Havre R, Gheorghe C, McKay C, Gheonea DI, Ciurea T. Efficacy of an artificial neural network-based approach to endoscopic ultrasound elastography in diagnosis of focal pancreatic masses. Clin Gastroenterol Hepatol 2012; 10: e1 [PMID: DOI: /j.cgh ] 61 Săftoiu A, Vilmann P, Gorunescu F, Gheonea DI, Gorunescu M, Ciurea T, Popescu GL, Iordache A, Hassan H, Iordache S. Neural network analysis of dynamic sequences of EUS elastography used for the differential diagnosis of chronic pancreatitis and pancreatic cancer. Gastrointest Endosc 2008; 68: [PMID: DOI: /j.gie ] 62 Itoh Y, Itoh A, Kawashima H, Ohno E, Nakamura Y, Hiramatsu T, Sugimoto H, Sumi H, Hayashi D, Kuwahara T, Morishima T, Funasaka K, Nakamura M, Miyahara R, Ohmiya N, Katano Y, Ishigami M, Goto H, Hirooka Y. Quantitative analysis of diagnosing pancreatic fibrosis using EUS-elastography (comparison with surgical specimens). J Gastroenterol 2014; 49: [PMID: DOI: /s ] 63 Iglesias-Garcia J, Domínguez-Muñoz JE, Castiñeira-Alvariño M, Luaces-Regueira M, Lariño-Noia J. Quantitative elastography associated with endoscopic ultrasound for the diagnosis of chronic pancreatitis. Endoscopy 2013; 45: [PMID: DOI: /s ] 64 Janssen J, Papavassiliou I. Effect of aging and diffuse chronic pancreatitis on pancreas elasticity evaluated using semiquantitative EUS elastography. Ultraschall Med 2014; 35: [PMID: DOI: /s ] 65 Domínguez-Muñoz JE, Alvarez-Castro A, Lariño-Noia J, Nieto L, Iglesias-García J. Endoscopic ultrasonography of the pancreas as an indirect method to predict pancreatic exocrine insufficiency in patients with chronic pancreatitis. Pancreas 2012; 41: [PMID: DOI: /MPA.0b013e31823b5978] 66 Popescu A, Săftoiu A. Can elastography replace fine needle aspiration? Endosc Ultrasound 2014; 3: [PMID: DOI: / ] 67 Ito T, Ishiguro H, Ohara H, Kamisawa T, Sakagami J, Sata N, Takeyama Y, Hirota M, Miyakawa H, Igarashi H, Lee L, Fujiyama T, Hijioka M, Ueda K, Tachibana Y, Sogame Y, Yasuda H, Kato R, Kataoka K, Shiratori K, Sugiyama M, Okazaki K, Kawa S, Tando Y, Kinoshita Y, Watanabe M, Shimosegawa T. Evidence-based clinical practice guidelines for chronic pancreatitis J Gastroenterol 2016; 51: [PMID: DOI: /s x] 68 Shimosegawa T, Kataoka K, Kamisawa T, Miyakawa H, Ohara H, Ito T, Naruse S, Sata N, Suda K, Hirota M, Takeyama Y, Shiratori K, Hatori T, Otsuki M, Atomi Y, Sugano K, Tanaka M. The revised Japanese clinical diagnostic criteria for chronic pancreatitis. J Gastroenterol 2010; 45: [PMID: DOI: / s ] P- Reviewer: Kilickesmez O, Thierfelder KM S- Editor: Yu J L- Editor: A E- Editor: Ma S 3724 April 14, 2016 Volume 22 Issue 14
39 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Biomarkers for detection of alcohol consumption in liver transplantation REVIEW Katharina Staufer, Michel Yegles Katharina Staufer, Division of Transplantation, Department of Surgery, Medical University of Vienna, 1090 Vienna, Austria Michel Yegles, Laboratoire National de Santé, Service de Toxicologie médico-légale 1, rue Louis Rech, L-3555 Dudelange, Luxembourg Author contributions: Staufer K contributed to conception and writing of article; Yegles M contributed to scientific advise. Conflict-of-interest statement: No potential conflicts of interest. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Katharina Staufer, MD, assistant Professor, Division of Transplantation, Department of Surgery, Medical University of Vienna, A-1090, Waehringer Guertel 18-20, 1090 Vienna, Austria. katharina.staufer@meduniwien.ac.at Telephone: Fax: Received: December 21, 2015 Peer-review started: December 24, 2015 First decision: January 13, 2016 Revised: January 26, 2016 Accepted: February 20, 2016 Article in press: February 21, 2016 Published online: April 14, 2016 abstinence period of up to 6 mo prior to transplantation is mandatory, alcohol relapse after transplantation is a common event. In case of recurrence of heavy drinking, graft survival is significantly impaired. Guidelines on detection and surveillance of alcohol consumption in this patient cohort are lacking. This review summarizes the challenge of patient selection as well as the current knowledge on established and novel alcohol biomarkers with special focus on liver transplant candidates and recipients. Key words: Ethyl glucuronide; Liver cirrhosis; Shortterm alcohol markers; Long-term alcohol markers; Psychological support The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Currently, consensus statements on alcohol screening prior to and after liver transplantation are lacking. Routinely applied alcohol markers have certain limitations in the setting of liver disease and end-stage cirrhosis. Novel alcohol biomarkers, such as ethyl glucuronide in urine and hair as well as phosphatidylethanol, however, show promise to significantly improve the selection and surveillance of patients within the liver transplant setting. Staufer K, Yegles M. Biomarkers for detection of alcohol consumption in liver transplantation. World J Gastroenterol 2016; 22(14): Available from: URL: wjgnet.com/ /full/v22/i14/3725.htm DOI: org/ /wjg.v22.i Abstract Alcoholic liver disease is an established, yet controversial, indication for liver transplantation. Although an INTRODUCTION Detection of alcohol consumption and surveillance of alcohol abstention in patients with alcoholic liver 3725 April 14, 2016 Volume 22 Issue 14
40 Staufer K et al. Alcohol markers in liver transplantation disease (ALD) are at the center of attention of transplant physicians. Liver transplantation (LT) is an established treatment of end-stage ALD, which presents the second most common indication for LT in Western countries [1,2]. Due to the prevalent perception within the population and among treating physicians that ALD is a self-induced disease, and possibly perpetuated by the evident lack of donor organs, this indication is controversial [3]. Therefore, ALD as an indication for LT all the more requires transparent, comprehensible selection criteria. Since alcoholism is a life-long disease and is not cured by LT, optimal selection of patients with a low risk of alcohol relapse as well as continuous monitoring and support after LT are essential. In order to facilitate optimal patient selection for the life-saving opportunity of LT, patients currently have to undergo a thorough psychological evaluation by an experienced addiction specialist. In addition, an abstinence period of at least 3 up to 6 mo is required in most transplant centers. Nevertheless, alcohol relapse on the waiting list is detected in up to 25% [4-6] and occurs in up to 50% of liver transplant recipients [7,8]. Of these, up to 36% of patients resume heavy drinking [9-11]. Long-term outcome after LT is significantly reduced in the patient cohort with return to excessive alcohol consumption but is similar to other indications despite return to low to moderate alcohol consumption [12,13]. Therefore, our eligibility criteria to list patients need to be refined, and we need more reliable tools to predict the individual risk of relapse to heavy drinking. In addition, surveillance and concomitant psychological support after LT should take a central role. This requires continuous surveillance programs for LT recipients to avoid alcohol relapse as well as tools to maximize rates of early detection of alcohol relapse to prevent graft damage. Objective direct alcohol parameters could support evaluation by addiction specialists and improve patient selection prior to LT and optimize surveillance and early detection of alcohol consumption in liver transplant recipients. This review summarizes the challenges of detection and correct assessment of alcohol consumption. It focuses on the current knowledge on alcohol biomarkers in liver disease and their particular value within the liver transplant setting and gives insight into possible future developments. Diagnosis of ALD - A dilemma? Correct diagnosis of ALD is critical for individual treatment approaches, but it is sometimes difficult, since specific features are lacking. After ruling out different liver diseases, diagnosis has to be based on patients statement on alcohol consumption. Yet, reliable objective alcohol parameters for confirmation have not yet found their way into routine clinical use (see below). According to the current guidelines of the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD), ALD may diagnosed upon documentation of consumption of > 30 g/d of ethanol as well as the presence of clinical and/or biological signs of liver injury [14,15]. According to EASL guidelines, diagnosis should be based on clinical [such as gammaglutamyl transferase (GGT), carbohydrate deficient transferrin (CDT), aspartate aminotransferase (AST), alanine aminotransferase (ALT), mean corpuscular volume (MCV)], biological (serum fibrosis markers), and ultrasound parameters (detection of steatosis, grading of parenchymal alterations). Furthermore, liver biopsy might be required for confirmation of diagnosis. However, all mentioned parameters may be non-diagnostic in the case of mild ALD or early cirrhosis [15,16], and patients are normally asymptomatic until an advanced state of liver disease has been reached. The documentation of regular alcohol intake, however, and especially the assessment of the alcohol amount is difficult. Commonly, patients do not admit alcohol consumption or underreport or do not indicate correct amounts of alcohol intake [17-19]. Furthermore, the amount of alcohol intake and development of liver alterations or severity of liver disease are not strictly linear [20]. Clear diagnosis of alcohol consumption and ALD is complicated by the lack of definite cut-off values of ethanol identified as harmful in certain populations. In 60% of patients with regular alcohol intake > 60 g/d, hepatic steatosis was found [21,22]. In 29% of a large patient series, liver cirrhosis was detected by liver biopsy in 29% of a large series of patients with alcoholism [23]. Differential diagnosis to non-alcoholic fatty liver disease (NAFLD) (ethanol cut-off: 20 g/d for women, 30 g/d for men) and the assessment of alcohol as an additional hit to the liver are difficult. Even liver biopsy cannot safely discriminate ALD from NAFLD [24,25]. Moreover, in a meta-analysis, daily consumption of > 25 g of ethanol has been associated with an increased risk of liver cirrhosis and its complications [26]. Increased risk of mortality due to liver cirrhosis was recently found even below 25 g/d of ethanol (12-24 g/d) [27]. Thus, patients might be at risk at ethanol levels even below the current public recommendations for alcohol consumption. Requirements for suitable alcohol markers in liver disease and liver transplantation Alcohol markers for detection of alcohol consumption and prediction of alcohol relapse need to fulfill certain features in the setting of ALD and LT. Only patients with a low risk of relapse are eligible for transplant. Patients in whom alcohol relapse is detected within the waiting period may be excluded from the life April 14, 2016 Volume 22 Issue 14
41 Staufer K et al. Alcohol markers in liver transplantation saving opportunity of LT. Since alcoholism is a life-long disease that is not cured by LT, LT recipients should receive close surveillance to provide the possibility of an early detection in the case of relapse. LT recipients with alcohol relapse are at risk for the development of alcoholic hepatitis and re-cirrhosis in the liver graft. Nevertheless, in case of alcohol relapse, patients may be denied liver re-transplantation. Optimal alcohol biomarkers in the setting of LT should not be influenced by liver alterations, commonly present kidney dysfunction, changes in body composition (low fat and muscle mass in case of end-stage cirrhosis, increased body water in case of ascites), immunosuppressive medication, or multiple drug therapy and should be cheap and easily accessible. In LT candidates who get evaluated for LT or are on the waiting list, the markers need to be highly specific in order not to deny mistakenly a life-saving LT due to false positive alcohol tests. In LT recipients in whom early detection of relapse is the focus to preserve graft function, high sensitivity is of special interest. GOLD STANDARD FOR DETECTION OF ALCOHOL CONSUMPTION To date, national and international guidelines for alcohol biomarker screening of patients within the transplant setting are still lacking. Many transplant centers in Europe and the United States routinely use ethanol (EtOH) and CDT as direct markers of alcohol consumption as well as GGT and MCV as indirect markers. The recommendations of the National Institutes of Health/National Institute on Alcohol Abuse and Alcoholism [28] for ALD patients state: For screening purposes in primary care settings, interviews and questionnaires have greater sensitivity and specificity than blood tests for biochemical markers, which identify only about 10% to 30% of heavy drinkers. Nevertheless, biochemical markers may be useful when heavy drinking is suspected but the patient denies it. GGT, MCV, and CDT are recommended, nevertheless, to show certain limitations within the transplant setting (see paragraphs on indirect and direct alcohol biomarkers). Ethanol metabolism After ingestion, ethanol is absorbed via the oral, gastric, and small intestinal mucosa. About 2%-10% of ethanol are excreted via urine, sweat, and exhalation air without modification. EtOH detoxification starts within the stomach and is facilitated by alcohol dehydrogenase (ADH) (sigma-adh, about 5% of ethanol metabolism). The major part of EtOH is metabolized to acetaldehyde within the liver by ADH, catalase, and the so-called microsomal ethanol oxidizing system (MEOS; via cytochrome P450 CYP2E1; especially in case of > 50 g/d alcohol intake or chronic alcohol intake). Acetaldehyde is further metabolized to acetic acid via acetaldehyde dehydrogenase. Acetic acid is metabolized via the citrate cycle and the mitochondrial respiratory chain and exhaled as CO2. A very small amount (< 0.1%) of ethanol undergoes conjugation reactions with glucuronic acid in the presence of membrane-bound mitochondrial uridine diphosphate glucuronyl transferase to produce ethyl glucuronide (EtG) and with sulfate to produce ethyl sulfate (EtS), which are excreted in the urine [29-31]. Indirect biomarkers of alcohol consumption State markers such as MCV [32] and the liver function tests GGT, ALT, and AST are widely used for routine screening of chronic alcohol consumption. These indirect markers of alcohol consumption may yet be elevated not only in case of ALD but all other forms of acute or chronic liver disease or vitamin B12 and/or folic acid deficiency. In a recent study on 210 non-excessive drinkers, 272 excessive drinkers, and 76 patients with alcoholic cirrhosis investigating the kinetics of alcohol markers during abstinence, the diagnostic accuracy of GGT to detect excessive drinkers was moderate [area under the curve (AUC) 0.68] and was associated with the amount of alcohol consumed within the past 30 d, which is in contrast to the AST/ALT ratio [33]. In this patient cohort consisting of ALD patients only, GGT reached a sensitivity and specificity of 49.6%, and 83.9%, respectively, for the detection of excessive alcohol consumption [33]. In contrast, in a setting of 141 liver transplant candidates and recipients, different markers were analyzed for their value in screening the consumption of any amount of alcohol, and the specificities of GGT, MCV, and AST were rather low [17]. Besides low specificity for chronic alcohol intake and detection of alcohol relapse [17], these markers have also low sensitivity for recent intake of excessive alcohol amounts [34]. When using these markers, we have to be aware of certain limitations, especially within a patient collective with already significant liver disease or on multiple drug therapy [35,36]. Carbohydrate deficient transferrin Transferrin is a glycoprotein produced and secreted by the liver. The International Federation of Clinical Chemistry and Laboratory Medicine recommend that CDT should be expressed as CDT divided by the amount of total transferrin to account for individual variations in transferrin levels. In addition, the disialotransferrin glycoform of CDT (one of three isoforms) should be measured since it correlates best with the amount of ingested alcohol, as measured by high performance liquid chromatography (HPLC) [37]. CDT levels reflect continuous heavy drinking of 3727 April 14, 2016 Volume 22 Issue 14
42 Staufer K et al. Alcohol markers in liver transplantation Table 1 Biomarkers for alcohol consumption used in the liver transplant setting Biomarker Biological compartment Window of detection Confounding factors Cut off Sensitivity Specificity Number of patients Ref. Indirect markers GGT Serum - Liver disease [33] < 55 U/l [17] MCV Serum - Hematological diseases, vitamin < 94 fl [17] deficiencies AST Serum - Liver disease, muscle alterations < 35 U/L [17] ALT Serum - Liver disease < 50 U/L [17] %CDT Serum 1-2 wk Hyperbilirubinemia, liver cirrhosis/ disease, smoking, sepsis, anorexia nervosa, airway diseases, rare genetic variants, transferrin levels 2.5% [33] > 2.6% [17] > 2.6% [18] Direct markers Breath alcohol Exhalation air h Alcohol containing mouth wash 0.01 g/l [6] EtOH Serum h Unknown 0.1 g/kg [17] [55] MeOH Serum up to 48 h Unknown 5 mg/l [17] 1.5 mg/l [55] EtG Urine up to 80 h Heavily impaired kidney function, high amounts of baker's yeast/ sauerkraut, alcohol containing mouthwash, storage above 4 before measurement EtG Hair up to 6 mo EtG containing hair treatment, heavily impaired kidney function 0.5 mg/l [6] [17] 7 pg/mg [18] 1 No sensitivity/specificity calculated, since only 1 of 141 patients had elevated EtOH. In the case of CDT, only studies using the HPLC method for determination of %CDT are reported. - not reported in the cited manuscript. GGT: Gamma-glutamyl transferase; MCV: Mean corpuscular volume; AST: Aspartate amino transferase; ALT: Alanine amino transferase; CDT: Carbohydrate deficient transferrin; EtOH: Ethanol; HPLC: High-performance liquid chromatography; MeOH: Methanol; EtG: Ethyl glucuronide. 50 to 80 g of EtOH per day over a period of 7 to 15 d [38,39]. After alcohol cessation, CDT normalizes within 2 to 3 wk (t1/2: 10 d) [39]. Depending on the assay used, determination of CDT sensitivity and specificity varies. In patients with end-stage liver disease, specificity is as low as 70%, and sensitivity ranges between 46% and 73% [40-43]. A higher sensitivity and specificity of approximately 88% and 95%, respectively, has previously been achieved by combining CDT with MCV and GGT [36,40,43]. CDT is not yet suitable to detect short-term alcohol consumption, even at high doses of 80 g/d [44]. Confounding factors for the measurement of CDT besides liver cirrhosis, primary biliary cirrhosis, and hepatitis C infection are smoking, sepsis, anorexia nervosa, and airway diseases [45]. All of these conditions can lead to false positive test results. False negative results can be caused by obesity, female sex, and pregnancy [46,47]. Furthermore, genetic variants occurring in 1%-2% of patients can lead to impaired test results [48]. Direct biomarkers of alcohol consumption Currently, a range of direct alcohol biomarkers are used that detect EtOH or EtOH metabolites in different body components. We can distinguish between shortand long-term alcohol markers (table 1). Short-term alcohol markers Breath alcohol test: In general, median breath alcohol concentration (BAC) correlates well with blood alcohol concentration, bearing a sensitivity and specificity of 97% and 93%, respectively, in healthy volunteers, although the correlation is weak for individual cases [49]. The sensitivity and specificity of breath analyzers of different manufacturers often vary considerably. BAC may be influenced by consuming food within 4 h prior to testing, a longer time spent drinking, and the number of drinks consumed per hour [50]. Therefore, this test is mainly utilized in the context of drivers accused of driving under the influence and needs to be confirmed by a blood ethanol test if positive. Although breath alcohol testing has the advantage of low costs and ease of use, this method has certain limitations within the setting of LT. Mainly due to low sensitivity resulting from rapid elimination of EtOH from the body (about 0.1 g/kg per hour), patients might not be detected [51]. In a study by Erim et al [6] alcohol breath tests were used as a screening method for alcohol consumption along with self-reports in LT candidates participating in an alcohol dependence group therapy. Nobody admitted alcohol consumption, and breath testing was positive in only one out of 18 patients. Comparing these results to urinary EtG (uetg) revealed that 50% of patients had positive results. Wetterling et al [52] found similar results 3728 April 14, 2016 Volume 22 Issue 14
43 Staufer K et al. Alcohol markers in liver transplantation by comparing the detection rate of alcohol relapse in patients during a long-term alcohol dependence program: by breath alcohol tests, personal interviews, and uetg 4.4%, 5.7%, and 37.7% of alcohol relapses were discovered. In 15.6% (265 cases) of patients, alcohol consumption was detected only by uetg. In three cases, on the other hand, alcohol consumption was only detected by breath alcohol test [52]. These results illustrate that breath alcohol testing in the setting of LT might not be an ideal tool for monitoring abstinence or early detection of relapse. Blood ethanol levels: EtOH blood concentration is a measure for recent alcohol consumption and remains positive for only a few hours after alcohol intake [51]. This elimination kinetic has to be considered when performing abstinence monitoring. Carbonneau et al [4] described the utility of random measurement of blood alcohol levels in 134 liver transplant candidates on the waiting list. Of these, eight patients had detectable serum alcohol levels, three patients admitted alcohol consumption in the presence of negative EtOH levels, and 12 patients refused blood withdrawal. A higher number of random blood alcohol tests was independently associated with a lower risk of alcohol use on the waiting list [4]. Nevertheless, within an LT outpatient setting with scheduled visits, detection of alcohol relapse by elevated EtOH levels may have been limited due to an adaptation of drinking habits to scheduled visits [17,18]. Overall, blood alcohol level is a useful marker in cases of suspected alcoholization. Blood methanol levels: Methanol (MeOH), a direct metabolite of EtOH, is detectable for up to 2 d but may accumulate in body fluids in the case of continuous heavy drinking [51,53,54]. Very little data are available on patients with liver dysfunction. The sensitivity and specificity of MeOH for detection of alcohol relapse using a cut off of 5 mg/l (HS-GC/FID, Perkin-Elmer) in 141 liver transplant candidates and recipients were reported to be 22% and 99%, respectively [17]. In another study on 41 liver transplant candidates, a cut off of 1.5 mg/l was indicative of probable recent alcohol intake (ruling out other confounding factors) or 3 mg/l (regarded highly positive ) was used [55]. By measuring MeOH, more relapsers were identified than with blood EtOH levels and self-reports by Alcohol Use Disorders Identification Test (AUDIT; 32 vs 3 patients; sensitivity and specificity not given by the authors) [55]. MeOH, however, can also be endogenously produced and, therefore, might show false positive results that mistakenly deny transplantation due to suspected alcohol relapse on the waiting list [56]. More data are necessary to reliably rate the value of MeOH within the LT setting. EtG and ethyl sulfate in urine: EtG is an ethanol conjugate that can be detected up to 36 h in the blood and up to 80 h in the urine, even after complete elimination of EtOH from the body [57,58]. uetg is detectable after consuming very small amounts of alcohol ( 5 g) [58,59]. The higher the amount of alcohol intake, the longer the detection window [30,60,61]. It can easily be measured by an immunoassay (lower detection limit 0.1 mg/l) or liquid chromatographytandem mass spectrometry (LC-MS/MS). uetg and uets show good correlation [62,63]. Since uetg levels are, to a great extent, independent of liver and kidney function, uetg is a useful marker within the setting of liver disease and LT. A sensitivity and specificity of 84% and 68%, respectively, were reported with a cut off of mg/l in a large cohort of drinkers and non-drinkers with and without liver cirrhosis [59]. Sensitivity and specificity increased to 91% and 77%, respectively, when a cut off of mg/l was used in low to moderate drinkers compared to heavy drinkers [59]. In a cohort of LT candidates and recipients using a cut off of 5 mg/l of the DRI-EtGenzyme immunoassay [(EIA; Thermo Fisher Scientific Inc.; Passau, Germany] a sensitivity and specificity of 89% and 99%, respectively, could be reached [17]. In this study, uetg significantly outperformed all other tested markers, such as GGT, AST, ALT, MCV, CDT, and MeOH in predicting alcohol consumption [17]. The vast majority of patients admitted alcohol consumption only after confrontation with positive test results. A study in 109 LT candidates with ALD showed positive uetg or uets in 20% (cut offs 0.2 mg/l, and 0.1 mg/l), although only 3% of patients indicated alcohol consumption [64]. Another study comparing uetg, AUDIT-C, EtOH in blood and urine, CDT, and AST, ALT, GGT, and MCV in 121 LT candidates and recipients confirmed the high sensitivity and specificity of uetg of 89.2% and 98.8%, respectively. Combining uetg with AUDIT-C further improved detection of alcohol consumption (AUC = 0.94 vs 0.98), and additional assessment of CDT had no further benefit (AUC = 0.98) [65]. Although highly sensitive and specific, influencing factors that might lead to false positive or negative uetg results have to be taken into account. False negative results might occur in the presence of bacterial degradation in case of urinary tract infections (uets not altered) [66] but also might occur because of post collection synthesis of bacteria in the urine [67]. However, this in vitro reaction can be prevented by refrigerating, freezing, or collecting urine samples in NaF containers [59] or using dried urine on filter paper [68]. Cannabinol, ingestion of high amounts of baker s yeast, sauerkraut, non-alcoholic beer, or alcohol containing mouth washes as well as severe kidney disease can cause false positive results [59,69-71]. Recently, Høiseth et al [72] showed that chronic kidney disease increased the detection window of uetg and uets. In 14 patients with an estimated glomerular filtration rate < 60 ml/min per 1.73 m 2 and moderate use of alcohol (up to seven standard drinks per week), uetg could be detected up to as twice as long as in 3729 April 14, 2016 Volume 22 Issue 14
44 Staufer K et al. Alcohol markers in liver transplantation healthy volunteers ingesting comparable doses of alcohol. Long-term alcohol markers EtG and fatty acid ethyl ester in hair: EtG and fatty acid ethyl ester (FAEE) detection in hair allows for assessment of alcohol consumption for up to 6 mo (about 1 cm length of scalp hair strand per month). According to the recommendations of the Society of Hair Testing, patients with EtG concentrations of < 7 pg/mg are regarded as teetotallers or very rare drinkers, 7 pg/mg to 29 pg/mg strongly suggest repeated alcohol consumption, and concentrations of 30 pg/mg strongly suggest chronic excessive alcohol intake [73]. These cut-offs are valid for 0-3 cm up to 0-6 cm of proximal scalp hair segments. The analysis of FAEEs alone is not recommended to prove alcohol abstinence but may be used in cases of suspected false negative EtG results (FAEEs cut offs: 0.2 ng/mg for a 0-3 cm, 0.4 ng/mg for a 0-6 cm proximal scalp hair segment). The correlation between hetg and the amount of alcohol consumed are linear [74]. In addition to a time period of up to 6 mo, which is covered by hetg, it has the advantage of doubled sensitivity over CDT despite equal specificity [75]. Sterneck et al [18] presented promising results for the application of hetg within the transplant setting. Investigating 63 LT candidates with alcoholic liver cirrhosis and 25 patients with cirrhosis due to other reasons, hetg was compared to uetg, blood EtOH, MeOH, CDT, and psychological interviews. Although only 30% of patients admitted alcohol consumption, 62% of patients tested positive for any alcohol marker. Alcohol abstention was disproved in 83% of cases by hetg only. Sensitivity and specificity were 85% and 97%, respectively, using a cut off of 30 pg/mg in 6 cm hair strands. hetg results were independent of liver and kidney function. Recent work by the same study group analyzed the value of hetg in 104 LT recipients (31 ALD, 73 non-ald patients) in comparison to uetg, EtOH, MeOH, CDT, patients self-reports, and physicians assessments [76]. By applying hetg, the detection rate of 7% by any alcohol markers could be increased to 17%. hetg test results can be confounded by heavily impaired kidney function leading to higher hetg results [72]. Further, hair tonics, which might include EtG, can result in false positive results [77,78]. False positive FAAE results were found after use of EtOH containing lotions [79], whereas these lotions had no impact on hetg [80]. False negative or decreased hetg results can be found after bleaching, dying, and thermal hair straightening (only tested in vitro) [81-83]. Future directions Phosphatidylethanol (PEth) is a phospholipid formed only in the presence of EtOH via a transphosphatidylation catalyzed by phospholipase D in the cell membrane of peripheral blood cells [84-86]. It is a longterm alcohol parameter that becomes positive after repeated consumption of 50 g/d EtOH over a period of 2 to 3 wk measured by HPLC in whole blood and can be detected up to > 2 wk (probably up to 6 wk in some cases [87] ) after cessation of alcohol consumption [88,89]. Using LC-MS/MS, elevated PEth levels can be found after a single day of excessive alcohol intake [90]. A recent study also reported PEth to be a valuable tool for the detection of moderate alcohol consumption [91]. Novel assays even allow qualitative and quantitative measurement of PEth in dried blood spots [92,93]. PEth was described to bear higher sensitivity than CDT, GGT, or MCV (sensitivity of 99% vs 40% to 77%) [94]. Another study found an excellent diagnostic accuracy (AUC = 0.974, sensitivity 94.5%, specificity 100%) superior to that of CDT, GGT, or MCV in patients with excessive alcohol consumption taking part in a detoxification program [95]. Helander et al [96] showed the superiority of PEth over CDT for monitoring alcohol consumption in an outpatient alcohol detoxification program. In 43% of these patients alcohol consumption was detected only by PEth, in 38% by PEth plus CDT, and in 21% by EtG/EtS only. False positive or high test results can occur if samples are stored at room temperature [92]. PEtH levels are not affected by sex or age [97], and in contrast to CDT, PEth is not influenced by the presence or severity of liver disease [87,98]. Although already first described in the 1980s to be synthesized in peripheral blood [84,85], PEth still has not found its way into routine diagnostics. Data on LT candidates and recipients are currently lacking. Platelet monoaminoxidase-b (MAO-B) protein levels showed promising accuracy in detection of heavy drinking measured by immunoblotting or enzymelinked immunosorbent assay (AUC = 0.72) [99]. If combined with CDT, its performance can be improved (AUC = 0.84). Formerly investigated as a genetic trait marker of alcohol dependence, MAO-B presents an interesting target. Protein levels, in contrast to MAO-B enzymatic activity, are not impaired by smoking [100]. This marker, although promising, needs to be further validated. A recent study investigating a study cohort of 53 excessive drinkers, a control group of 49 individuals, and a validation cohort of 40 excessive drinkers and 40 controls discovered four novel proteins for the detection of excessive alcohol intake by serum proteomic analysis [101]. These proteins were AT-rich interactive domain-containing protein 4B, phosphatidylcholine-sterol acyltransferase, hepatocyte growth-factor like protein, and ADP-ribosylation factor 6. They are indirect markers of alcohol consumption and are superior to routinely used markers such as AST, ALT, GGT, MCV, and CDT (AUC = 0.70 to 0.86 vs 0.21 to 0.67). They might be involved in inflammation processes, cellular organization, protein 3730 April 14, 2016 Volume 22 Issue 14
45 Staufer K et al. Alcohol markers in liver transplantation transportation, and cell proliferation mechanistically linked to alcohol consumption and metabolism. However, to date it remains unclear whether the secretion and excretion of these proteins are influenced by liver function. CONCLUSION Alcohol biomarkers significantly improve detection of alcohol consumption. To account for various drinking patterns, we always examine several markers in combination to cover different time periods. In the setting of LT, sensitivity and specificity are of special concern, since a false positive alcohol test may deny a patient the opportunity of a life-saving LT. During the evaluation process for LT, hetg seems to be an attractive marker, since a time frame of up to 6 mo is covered and false positive results are unlikely. However, data demonstrating improved relapse rates after LT are missing, and optimal cut offs in this setting are unclear. For surveillance of patients on the waitlist for LT, a combination of uetg, PEtH, and GGT seem to be the most appropriate tools. In LT recipients, a combination of uetg, GGT, and CDT or PEtH might be valuable. Long-term follow-up after LT seems to be well covered by additional hetg concentrations. Currently, MeOH does not seem to have advantages over the mentioned parameters. Importantly, routinely assessed alcohol biomarkers prior to and after LT may help guide treatment decisions for LT and allow early referral for psychological support and alcohol detoxification programs. REFERENCES 1 Lucey MR, Schaubel DE, Guidinger MK, Tome S, Merion RM. Effect of alcoholic liver disease and hepatitis C infection on waiting list and posttransplant mortality and transplant survival benefit. Hepatology 2009; 50: [PMID: DOI: /hep.23007] 2 Burra P, Senzolo M, Adam R, Delvart V, Karam V, Germani G, Neuberger J. Liver transplantation for alcoholic liver disease in Europe: a study from the ELTR (European Liver Transplant Registry). Am J Transplant 2010; 10: [PMID: DOI: /j x] 3 O Grady JG. Liver transplantation alcohol related liver disease: (deliberately) stirring a hornet s nest! Gut 2006; 55: [PMID: DOI: /gut ] 4 Carbonneau M, Jensen LA, Bain VG, Kelly K, Meeberg G, Tandon P. Alcohol use while on the liver transplant waiting list: a single-center experience. Liver Transpl 2010; 16: [PMID: DOI: /lt.21957] 5 Iasi MS, Vieira A, Añez CI, Trindade R, Codovani NT, Favero SS, Soler WV, David AI, D Capua A, Szutan LA, Rolim EG, Iasi M. Recurrence of alcohol ingestion in liver transplantation candidates. Transplant Proc 2003; 35: [PMID: ] 6 Erim Y, Böttcher M, Dahmen U, Beck O, Broelsch CE, Helander A. Urinary ethyl glucuronide testing detects alcohol consumption in alcoholic liver disease patients awaiting liver transplantation. Liver Transpl 2007; 13: [PMID: DOI: / lt.21163] 7 Dew MA, DiMartini AF, Steel J, De Vito Dabbs A, Myaskovsky L, Unruh M, Greenhouse J. Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs. Liver Transpl 2008; 14: [PMID: DOI: /lt.21278] 8 DiMartini A, Crone C, Dew MA. Alcohol and substance use in liver transplant patients. Clin Liver Dis 2011; 15: [PMID: DOI: /j.cld ] 9 Burra P, Mioni D, Cillo U, Fagiuoli S, Senzolo M, Naccarato R, Martines D. Long-term medical and psycho-social evaluation of patients undergoing orthotopic liver transplantation for alcoholic liver disease. Transpl Int 2000; 13 Suppl 1: S174-S178 [PMID: ] 10 Mackie J, Groves K, Hoyle A, Garcia C, Garcia R, Gunson B, Neuberger J. Orthotopic liver transplantation for alcoholic liver disease: a retrospective analysis of survival, recidivism, and risk factors predisposing to recidivism. Liver Transpl 2001; 7: [PMID: DOI: /jlts ] 11 Tome S, Lucey MR. Timing of liver transplantation in alcoholic cirrhosis. J Hepatol 2003; 39: [PMID: ] 12 Cuadrado A, Fábrega E, Casafont F, Pons-Romero F. Alcohol recidivism impairs long-term patient survival after orthotopic liver transplantation for alcoholic liver disease. Liver Transpl 2005; 11: [PMID: DOI: /lt.20386] 13 Egawa H, Nishimura K, Teramukai S, Yamamoto M, Umeshita K, Furukawa H, Uemoto S. Risk factors for alcohol relapse after liver transplantation for alcoholic cirrhosis in Japan. Liver Transpl 2014; 20: [PMID: DOI: /lt.23797] 14 European Association for the Study of Liver. EASL clinical practical guidelines: management of alcoholic liver disease. J Hepatol 2012; 57: [PMID: DOI: / j.jhep ] 15 O Shea RS, Dasarathy S, McCullough AJ. Alcoholic liver disease. Am J Gastroenterol 2010; 105: 14-32; quiz 33 [PMID: DOI: /ajg ] 16 Sharp AH, Black JL, Dubel SJ, Sundarraj S, Shen JP, Yunker AM, Copeland TD, McEnery MW. Biochemical and anatomical evidence for specialized voltage-dependent calcium channel gamma isoform expression in the epileptic and ataxic mouse, stargazer. Neuroscience 2001; 105: [PMID: ] 17 Staufer K, Andresen H, Vettorazzi E, Tobias N, Nashan B, Sterneck M. Urinary ethyl glucuronide as a novel screening tool in patients pre- and post-liver transplantation improves detection of alcohol consumption. Hepatology 2011; 54: [PMID: DOI: /hep.24596] 18 Sterneck M, Yegles M, Rothkirch von G, Staufer K, Vettorazzi E, Schulz KH, Tobias N, Graeser C, Fischer L, Nashan B, Andresen- Streichert H. Determination of ethyl glucuronide in hair improves evaluation of long-term alcohol abstention in liver transplant candidates. Liver Int 2014; 34: [PMID: DOI: /liv.12243] 19 Helander A, von Wachenfeldt J, Hiltunen A, Beck O, Liljeberg P, Borg S. Comparison of urinary 5-hydroxytryptophol, breath ethanol, and self-report for detection of recent alcohol use during outpatient treatment: a study on methadone patients. Drug Alcohol Depend 1999; 56: [PMID: ] 20 Kamper-Jørgensen M, Grønbaek M, Tolstrup J, Becker U. Alcohol and cirrhosis: dose--response or threshold effect? J Hepatol 2004; 41: [PMID: DOI: /j.jhep ] 21 Becker U, Deis A, Sørensen TI, Grønbaek M, Borch-Johnsen K, Müller CF, Schnohr P, Jensen G. Prediction of risk of liver disease by alcohol intake, sex, and age: a prospective population study. Hepatology 1996; 23: [PMID: DOI: / hep ] 22 Bellentani S, Saccoccio G, Costa G, Tiribelli C, Manenti F, Sodde M, Saveria Crocè L, Sasso F, Pozzato G, Cristianini G, Brandi G. Drinking habits as cofactors of risk for alcohol induced liver damage. The Dionysos Study Group. Gut 1997; 41: [PMID: ] 23 Naveau S, Giraud V, Borotto E, Aubert A, Capron F, Chaput JC. Excess weight risk factor for alcoholic liver disease. Hepatology 1997; 25: [PMID: DOI: /hep ] 3731 April 14, 2016 Volume 22 Issue 14
46 Staufer K et al. Alcohol markers in liver transplantation 24 Pinto HC, Baptista A, Camilo ME, Valente A, Saragoça A, de Moura MC. Nonalcoholic steatohepatitis. Clinicopathological comparison with alcoholic hepatitis in ambulatory and hospitalized patients. Dig Dis Sci 1996; 41: [PMID: ] 25 Toshikuni N, Tsutsumi M, Arisawa T. Clinical differences between alcoholic liver disease and nonalcoholic fatty liver disease. World J Gastroenterol 2014; 20: [PMID: DOI: /wjg.v20.i ] 26 Corrao G, Bagnardi V, Zambon A, Torchio P. Meta-analysis of alcohol intake in relation to risk of liver cirrhosis. Alcohol Alcohol 1998; 33: [PMID: ] 27 Rehm J, Taylor B, Mohapatra S, Irving H, Baliunas D, Patra J, Roerecke M. Alcohol as a risk factor for liver cirrhosis: a systematic review and meta-analysis. Drug Alcohol Rev 2010; 29: [PMID: DOI: /j x] 28 Helping patients who drink too much. A clinician s guide. Updated 2005, edition. Available from: URL: publications/practitioner/cliniciansguide2005/clinicians_guide.htm 29 Schmitt G, Aderjan R, Keller T, Wu M. Ethyl glucuronide: an unusual ethanol metabolite in humans. Synthesis, analytical data, and determination in serum and urine. J Anal Toxicol 1995; 19: [PMID: ] 30 Dahl H, Stephanson N, Beck O, Helander A. Comparison of urinary excretion characteristics of ethanol and ethyl glucuronide. J Anal Toxicol 2002; 26: [PMID: ] 31 Helander A, Beck O. Mass spectrometric identification of ethyl sulfate as an ethanol metabolite in humans. Clin Chem 2004; 50: [PMID: DOI: /clinchem ] 32 Tønnesen H, Hejberg L, Frobenius S, Andersen JR. Erythrocyte mean cell volume--correlation to drinking pattern in heavy alcoholics. Acta Med Scand 1986; 219: [PMID: ] 33 Gough G, Heathers L, Puckett D, Westerhold C, Ren X, Yu Z, Crabb DW, Liangpunsakul S. The Utility of Commonly Used Laboratory Tests to Screen for Excessive Alcohol Use in Clinical Practice. Alcohol Clin Exp Res 2015; 39: [PMID: DOI: /acer.12780] 34 Helander A. Biological markers in alcoholism. J Neural Transm Suppl 2003; (66): [PMID: ] 35 Mundle G, Ackermann K, Munkes J, Steinle D, Mann K. Influence of age, alcohol consumption and abstinence on the sensitivity of carbohydrate-deficient transferrin, gamma-glutamyltransferase and mean corpuscular volume. Alcohol Alcohol 1999; 34: [PMID: ] 36 Hock B, Schwarz M, Domke I, Grunert VP, Wuertemberger M, Schiemann U, Horster S, Limmer C, Stecker G, Soyka M. Validity of carbohydrate-deficient transferrin (%CDT), gammaglutamyltransferase (gamma-gt) and mean corpuscular erythrocyte volume (MCV) as biomarkers for chronic alcohol abuse: a study in patients with alcohol dependence and liver disorders of nonalcoholic and alcoholic origin. Addiction 2005; 100: [PMID: DOI: /j x] 37 Jeppsson JO, Arndt T, Schellenberg F, Wielders JP, Anton RF, Whitfield JB, Helander A. Toward standardization of carbohydratedeficient transferrin (CDT) measurements: I. Analyte definition and proposal of a candidate reference method. Clin Chem Lab Med 2007; 45: [PMID: DOI: / CCLM ] 38 Helander A, Carlsson AV, Borg S. Longitudinal comparison of carbohydrate-deficient transferrin and gamma-glutamyl transferase: complementary markers of excessive alcohol consumption. Alcohol Alcohol 1996; 31: [PMID: ] 39 Stibler H. Carbohydrate-deficient transferrin in serum: a new marker of potentially harmful alcohol consumption reviewed. Clin Chem 1991; 37: [PMID: ] 40 Anttila P, Järvi K, Latvala J, Blake JE, Niemelä O. Diagnostic characteristics of different carbohydrate-deficient transferrin methods in the detection of problem drinking: effects of liver disease and alcohol consumption. Alcohol Alcohol 2003; 38: [PMID: ] 41 Heinemann A, Sterneck M, Kuhlencordt R, Rogiers X, Schulz KH, Queen B, Wischhusen F, Püschel K. Carbohydrate-deficient transferrin: diagnostic efficiency among patients with end-stage liver disease before and after liver transplantation. Alcohol Clin Exp Res 1998; 22: [PMID: ] 42 DiMartini A, Day N, Lane T, Beisler AT, Dew MA, Anton R. Carbohydrate deficient transferrin in abstaining patients with endstage liver disease. Alcohol Clin Exp Res 2001; 25: [PMID: ] 43 Salaspuro M. Carbohydrate-deficient transferrin as compared to other markers of alcoholism: a systematic review. Alcohol 1999; 19: [PMID: ] 44 Lesch OM, Walter H, Antal J, Heggli DE, Kovacz A, Leitner A, Neumeister A, Stumpf I, Sundrehagen E, Kasper S. Carbohydratedeficient transferrin as a marker of alcohol intake: a study with healthy subjects. Alcohol Alcohol 1996; 31: [PMID: ] 45 Anton RF, Lieber C, Tabakoff B. Carbohydrate-deficient transferrin and gamma-glutamyltransferase for the detection and monitoring of alcohol use: results from a multisite study. Alcohol Clin Exp Res 2002; 26: [PMID: DOI: /01.ALC F5] 46 Kenan N, Larsson A, Axelsson O, Helander A. Changes in transferrin glycosylation during pregnancy may lead to falsepositive carbohydrate-deficient transferrin (CDT) results in testing for riskful alcohol consumption. Clin Chim Acta 2011; 412: [PMID: DOI: /j.cca ] 47 Fagan KJ, Irvine KM, McWhinney BC, Fletcher LM, Horsfall LU, Johnson L, O Rourke P, Martin J, Scott I, Pretorius CJ, Ungerer JP, Powell EE. Diagnostic sensitivity of carbohydrate deficient transferrin in heavy drinkers. BMC Gastroenterol 2014; 14: 97 [PMID: DOI: / X-14-97] 48 Wuyts B, Delanghe JR, Kasvosve I, Gordeuk VR, Gangaidzo IT, Gomo ZA. Carbohydrate-deficient transferrin and chronic alcohol ingestion in subjects with transferrin CD-variants. Clin Chem Lab Med 2001; 39: [PMID: DOI: / CCLM ] 49 Jaffe DH, Siman-Tov M, Gopher A, Peleg K. Variability in the blood/breath alcohol ratio and implications for evidentiary purposes. J Forensic Sci 2013; 58: [PMID: DOI: / ] 50 Quigg Z, Hughes K, Bellis MA. Student drinking patterns and blood alcohol concentration on commercially organised pub crawls in the UK. Addict Behav 2013; 38: [PMID: DOI: /j.addbeh ] 51 Helander A, Eriksson CJ. Laboratory tests for acute alcohol consumption: results of the WHO/ISBRA Study on State and Trait Markers of Alcohol Use and Dependence. Alcohol Clin Exp Res 2002; 26: [PMID: ] 52 Wetterling T, Dibbelt L, Wetterling G, Göder R, Wurst F, Margraf M, Junghanns K. Ethyl glucuronide (EtG): better than breathalyser or self-reports to detect covert short-term relapses into drinking. Alcohol Alcohol 2014; 49: [PMID: DOI: / alcalc/agt155] 53 Haffner HT, Banger M, Graw M, Besserer K, Brink T. The kinetics of methanol elimination in alcoholics and the influence of ethanol. Forensic Sci Int 1997; 89: [PMID: ] 54 Roine RP, Eriksson CJ, Ylikahri R, Penttilä A, Salaspuro M. Methanol as a marker of alcohol abuse. Alcohol Clin Exp Res 1989; 13: [PMID: ] 55 Hempel JM, Greif-Higer G, Kaufmann T, Beutel ME. Detection of alcohol consumption in patients with alcoholic liver cirrhosis during the evaluation process for liver transplantation. Liver Transpl 2012; 18: [PMID: DOI: /lt.23468] 56 Jones AW, Skagerberg S, Yonekura T, Sato A. Metabolic interaction between endogenous methanol and exogenous ethanol studied in human volunteers by analysis of breath. Pharmacol Toxicol 1990; 66: [PMID: ] 57 Maenhout TM, De Buyzere ML, Delanghe JR. Non-oxidative ethanol metabolites as a measure of alcohol intake. Clin Chim Acta 2013; 415: [PMID: DOI: /j.cca ] 3732 April 14, 2016 Volume 22 Issue 14
47 Staufer K et al. Alcohol markers in liver transplantation 58 Wurst FM, Kempter C, Seidl S, Alt A. Ethyl glucuronide--a marker of alcohol consumption and a relapse marker with clinical and forensic implications. Alcohol Alcohol 1999; 34: [PMID: ] 59 Wurst FM, Wiesbeck GA, Metzger JW, Weinmann W. On sensitivity, specificity, and the influence of various parameters on ethyl glucuronide levels in urine--results from the WHO/ ISBRA study. Alcohol Clin Exp Res 2004; 28: [PMID: ] 60 Stephanson N, Dahl H, Helander A, Beck O. Direct quantification of ethyl glucuronide in clinical urine samples by liquid chromatography-mass spectrometry. Ther Drug Monit 2002; 24: [PMID: ] 61 Borucki K, Schreiner R, Dierkes J, Jachau K, Krause D, Westphal S, Wurst FM, Luley C, Schmidt-Gayk H. Detection of recent ethanol intake with new markers: comparison of fatty acid ethyl esters in serum and of ethyl glucuronide and the ratio of 5-hydroxytryptophol to 5-hydroxyindole acetic acid in urine. Alcohol Clin Exp Res 2005; 29: [PMID: ] 62 Jatlow PI, Agro A, Wu R, Nadim H, Toll BA, Ralevski E, Nogueira C, Shi J, Dziura JD, Petrakis IL, O Malley SS. Ethyl glucuronide and ethyl sulfate assays in clinical trials, interpretation, and limitations: results of a dose ranging alcohol challenge study and 2 clinical trials. Alcohol Clin Exp Res 2014; 38: [PMID: DOI: /acer.12407] 63 Turfus SC, Vo T, Niehaus N, Gerostamoulos D, Beyer J. An evaluation of the DRI-ETG EIA method for the determination of ethyl glucuronide concentrations in clinical and post-mortem urine. Drug Test Anal 2013; 5: [PMID: DOI: / dta.414] 64 Webzell I, Ball D, Bell J, Sherwood RA, Marsh A, O Grady JG, Heaton ND. Substance use by liver transplant candidates: an anonymous urinalysis study. Liver Transpl 2011; 17: [PMID: DOI: /lt.22370] 65 Piano S, Marchioro L, Gola E, Rosi S, Morando F, Cavallin M, Sticca A, Fasolato S, Forza G, Chiara Frigo A, Plebani M, Zanus G, Cillo U, Gatta A, Angeli P. Assessment of alcohol consumption in liver transplant candidates and recipients: the best combination of the tools available. Liver Transpl 2014; 20: [PMID: DOI: /lt.23881] 66 Helander A, Dahl H. Urinary tract infection: a risk factor for false-negative urinary ethyl glucuronide but not ethyl sulfate in the detection of recent alcohol consumption. Clin Chem 2005; 51: [PMID: DOI: /clinchem ] 67 Helander A, Olsson I, Dahl H. Postcollection synthesis of ethyl glucuronide by bacteria in urine may cause false identification of alcohol consumption. Clin Chem 2007; 53: [PMID: DOI: /clinchem ] 68 Redondo AH, Körber C, König S, Längin A, Al-Ahmad A, Weinmann W. Inhibition of bacterial degradation of EtG by collection as dried urine spots (DUS). Anal Bioanal Chem 2012; 402: [PMID: DOI: /s ] 69 Al Saabi A, Allorge D, Sauvage FL, Tournel G, Gaulier JM, Marquet P, Picard N. Involvement of UDP-glucuronosyltransferases UGT1A9 and UGT2B7 in ethanol glucuronidation, and interactions with common drugs of abuse. Drug Metab Dispos 2013; 41: [PMID: DOI: /dmd ] 70 Thierauf A, Wohlfarth A, Auwärter V, Perdekamp MG, Wurst FM, Weinmann W. Urine tested positive for ethyl glucuronide and ethyl sulfate after the consumption of yeast and sugar. Forensic Sci Int 2010; 202: e45-e47 [PMID: DOI: / j.forsciint ] 71 Thierauf A, Gnann H, Wohlfarth A, Auwärter V, Perdekamp MG, Buttler KJ, Wurst FM, Weinmann W. Urine tested positive for ethyl glucuronide and ethyl sulphate after the consumption of non-alcoholic beer. Forensic Sci Int 2010; 202: [PMID: DOI: /j.forsciint ] 72 Høiseth G, Morini L, Ganss R, Nordal K, Mørland J. Higher levels of hair ethyl glucuronide in patients with decreased kidney function. Alcohol Clin Exp Res 2013; 37 Suppl 1: E14-E16 [PMID: DOI: /j x] 73 Kintz P consensus for the use of alcohol markers in hair for assessment of both abstinence and chronic excessive alcohol consumption. Forensic Sci Int 2015; 249: A1-A2 [PMID: DOI: /j.forsciint ] 74 Crunelle CL, Yegles M, van Nuijs AL, Covaci A, De Doncker M, Maudens KE, Sabbe B, Dom G, Lambert WE, Michielsen P, Neels H. Hair ethyl glucuronide levels as a marker for alcohol use and abuse: a review of the current state of the art. Drug Alcohol Depend 2014; 134: 1-11 [PMID: DOI: /j.drugalc dep ] 75 Morini L, Politi L, Acito S, Groppi A, Polettini A. Comparison of ethyl glucuronide in hair with carbohydrate-deficient transferrin in serum as markers of chronic high levels of alcohol consumption. Forensic Sci Int 2009; 188: [PMID: DOI: /j.forsciint ] 76 Andresen-Streichert H, von Rothkirch G, Vettorazzi E, Mueller A, Lohse AW, Frederking D, Seegers B, Nashan B, Sterneck M. Determination of Ethyl Glucuronide in Hair for Detection of Alcohol Consumption in Patients After Liver Transplantation. Ther Drug Monit 2015; 37: [PMID: DOI: / FTD ] 77 Pirro V, Di Corcia D, Seganti F, Salomone A, Vincenti M. Determination of ethyl glucuronide levels in hair for the assessment of alcohol abstinence. Forensic Sci Int 2013; 232: [PMID: DOI: /j.forsciint ] 78 Arndt T, Schröfel S, Stemmerich K. Ethyl glucuronide identified in commercial hair tonics. Forensic Sci Int 2013; 231: [PMID: DOI: /j.forsciint ] 79 Hartwig S, Auwärter V, Pragst F. Effect of hair care and hair cosmetics on the concentrations of fatty acid ethyl esters in hair as markers of chronically elevated alcohol consumption. Forensic Sci Int 2003; 131: [PMID: ] 80 Martins Ferreira L, Binz T, Yegles M. The influence of ethanol containing cosmetics on ethyl glucuronide concentration in hair. Forensic Sci Int 2012; 218: [PMID: DOI: /j.forsciint ] 81 Suesse S, Pragst F, Mieczkowski T, Selavka CM, Elian A, Sachs H, Hastedt M, Rothe M, Campbell J. Practical experiences in application of hair fatty acid ethyl esters and ethyl glucuronide for detection of chronic alcohol abuse in forensic cases. Forensic Sci Int 2012; 218: [PMID: DOI: /j.forsciint ] 82 Crunelle CL, Yegles M, De Doncker M, Dom G, Cappelle D, Maudens KE, van Nuijs AL, Covaci A, Neels H. Influence of repeated permanent coloring and bleaching on ethyl glucuronide concentrations in hair from alcohol-dependent patients. Forensic Sci Int 2015; 247: [PMID: DOI: / j.forsciint ] 83 Ettlinger J, Kirchen L, Yegles M. Influence of thermal hair straightening on ethyl glucuronide content in hair. Drug Test Anal 2014; 6 Suppl 1: [PMID: DOI: /dta.1648] 84 Kinsky SC, Loader JE, Benedict SH. Phorbol ester activation of phospholipase D in human monocytes but not peripheral blood lymphocytes. Biochem Biophys Res Commun 1989; 162: [PMID: ] 85 Mueller GC, Fleming MF, LeMahieu MA, Lybrand GS, Barry KJ. Synthesis of phosphatidylethanol--a potential marker for adult males at risk for alcoholism. Proc Natl Acad Sci USA 1988; 85: [PMID: ] 86 Gustavsson L, Alling C. Formation of phosphatidylethanol in rat brain by phospholipase D. Biochem Biophys Res Commun 1987; 142: [PMID: ] 87 Stewart SH, Koch DG, Willner IR, Anton RF, Reuben A. Validation of blood phosphatidylethanol as an alcohol consumption biomarker in patients with chronic liver disease. Alcohol Clin Exp Res 2014; 38: [PMID: DOI: / acer.12442] 88 Varga A, Hansson P, Lundqvist C, Alling C. Phosphatidylethanol in blood as a marker of ethanol consumption in healthy volunteers: comparison with other markers. Alcohol Clin Exp Res 1998; 22: 3733 April 14, 2016 Volume 22 Issue 14
48 Staufer K et al. Alcohol markers in liver transplantation [PMID: ] 89 Hansson P, Caron M, Johnson G, Gustavsson L, Alling C. Blood phosphatidylethanol as a marker of alcohol abuse: levels in alcoholic males during withdrawal. Alcohol Clin Exp Res 1997; 21: [PMID: ] 90 Gnann H, Weinmann W, Thierauf A. Formation of phosphatidylethanol and its subsequent elimination during an extensive drinking experiment over 5 days. Alcohol Clin Exp Res 2012; 36: [PMID: DOI: /j x] 91 Kechagias S, Dernroth DN, Blomgren A, Hansson T, Isaksson A, Walther L, Kronstrand R, Kågedal B, Nystrom FH. Phosphatidylethanol Compared with Other Blood Tests as a Biomarker of Moderate Alcohol Consumption in Healthy Volunteers: A Prospective Randomized Study. Alcohol Alcohol 2015; 50: [PMID: DOI: /alcalc/agv038] 92 Faller A, Richter B, Kluge M, Koenig P, Seitz HK, Thierauf A, Gnann H, Winkler M, Mattern R, Skopp G. LC-MS/MS analysis of phosphatidylethanol in dried blood spots versus conventional blood specimens. Anal Bioanal Chem 2011; 401: [PMID: DOI: /s y] 93 Kummer N, Ingels AS, Wille SM, Hanak C, Verbanck P, Lambert WE, Samyn N, Stove CP. Quantification of phosphatidylethanol 16: 0/18: 1, 18: 1/18: 1, and 16: 0/16: 0 in venous blood and venous and capillary dried blood spots from patients in alcohol withdrawal and control volunteers. Anal Bioanal Chem 2016; 408: [PMID: DOI: /s ] 94 Aradottir S, Asanovska G, Gjerss S, Hansson P, Alling C. PHosphatidylethanol (PEth) concentrations in blood are correlated to reported alcohol intake in alcohol-dependent patients. Alcohol Alcohol 2006; 41: [PMID: DOI: / alcalc/agl027] 95 Hartmann S, Aradottir S, Graf M, Wiesbeck G, Lesch O, Ramskogler K, Wolfersdorf M, Alling C, Wurst FM. Phosphatidylethanol as a sensitive and specific biomarker: comparison with gamma-glutamyl transpeptidase, mean corpuscular volume and carbohydrate-deficient transferrin. Addict Biol 2007; 12: [PMID: DOI: /j x] 96 Helander A, Péter O, Zheng Y. Monitoring of the alcohol biomarkers PEth, CDT and EtG/EtS in an outpatient treatment setting. Alcohol Alcohol 2012; 47: [PMID: DOI: /alcalc/ags065] 97 Wurst FM, Thon N, Aradottir S, Hartmann S, Wiesbeck GA, Lesch O, Skala K, Wolfersdorf M, Weinmann W, Alling C. Phosphatidylethanol: normalization during detoxification, gender aspects and correlation with other biomarkers and self-reports. Addict Biol 2010; 15: [PMID: DOI: / j x] 98 Stewart SH, Reuben A, Brzezinski WA, Koch DG, Basile J, Randall PK, Miller PM. Preliminary evaluation of phosphatidylethanol and alcohol consumption in patients with liver disease and hypertension. Alcohol Alcohol 2009; 44: [PMID: DOI: /alcalc/agp039] 99 Snell LD, Ramchandani VA, Saba L, Herion D, Heilig M, George DT, Pridzun L, Helander A, Schwandt ML, Phillips MJ, Hoffman PL, Tabakoff B. The biometric measurement of alcohol consumption. Alcohol Clin Exp Res 2012; 36: [PMID: DOI: /j x] 100 Snell LD, Glanz J, Tabakoff B. Relationships between effects of smoking, gender, and alcohol dependence on platelet monoamine oxidase-b: activity, affinity labeling, and protein measurements. Alcohol Clin Exp Res 2002; 26: [PMID: ] 101 Liangpunsakul S, Lai X, Ross RA, Yu Z, Modlik E, Westerhold C, Heathers L, Paul R, O Connor S, Crabb DW, Witzmann F. Novel serum biomarkers for detection of excessive alcohol use. Alcohol Clin Exp Res 2015; 39: [PMID: DOI: / acer.12654] P- Reviewer: Ruiz-Margain A S- Editor: Ma YJ L- Editor: Filipodia E- Editor: Ma S 3734 April 14, 2016 Volume 22 Issue 14
49 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Basic Study ORIGINAL ARTICLE phosphatase and tensin homolog is a differential diagnostic marker between nonalcoholic and alcoholic fatty liver disease Andrea Sanchez-Pareja, Sophie Clément, Marion Peyrou, Laurent Spahr, Francesco Negro, Laura Rubbia-Brandt, Michelangelo Foti Andrea Sanchez-Pareja, Sophie Clément, Francesco Negro, Laura Rubbia-Brandt, Division of Clinical Pathology, University Hospital of Geneva, 1211 Geneva, Switzerland Marion Peyrou, Michelangelo Foti, Department of Cellular Physiology and Metabolism, Faculty of Medicine, University of Geneva, 1211 Geneva, Switzerland Marion Peyrou, Michelangelo Foti, Diabetes Center, Faculty of Medicine, University of Geneva, 1211 Geneva, Switzerland Laurent Spahr, Francesco Negro, Division of Gastroenterology and Hepatology, University Hospital of Geneva, 1211 Geneva, Switzerland Author contributions: Rubbia-Brandt L and Foti M contributed equally to this work; Sanchez-Pareja A and Clément S acquired the data; Sanchez-Pareja A, Clément S, Peyrou M, Negro F, Rubbia-Brandt L and Foti M analyzed and interpreted the data; Spahr L and Rubbia-Brandt L provided material; Sanchez-Pareja A, Clément S and Foti M wrote the manuscript; Peyrou M, Spahr L, Negro F, Rubbia-Brandt L and Foti M critically revised the manuscript for important intellectual content; Rubbia-Brandt L and Foti M designed the study; Negro F and Foti M obtained funding. Supported by the Swiss National Science Foundation, No (to Negro F); and the Swiss National Science Foundation, No and No. CRSII (to Foti M). Institutional review board statement: This work was approved by the Ethics Committee of the Geneva University Hospital, Geneva, Switzerland. Institutional animal care and use committee statement:no animal experimentation was performed in this work. Conflict-of-interest statement: None related to the content of this article. Data sharing statement: No additional unpublished data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Michelangelo Foti, Professor, Department of Cellular Physiology and Metabolism, Faculty of Medicine, University of Geneva, Centre Médical Universitaire, 1 rue Michel-Servet, 1211 Geneva, Switzerland. michelangelo.foti@unige.ch Telephone: Fax: Received: December 21, 2015 Peer-review started: December 22, 2015 First decision: January 13, 2016 Revised: January 28, 2016 Accepted: March 1, 2016 Article in press: March 2, 2016 Published online: April 14, 2016 Abstract AIM: To investigate the protein expression of phosphatase and tensin homolog (PTEN) in human liver biopsies of patients with alcoholic and non-alcoholic liver disease. METHODS: PTEN protein expression was assessed 3735 April 14, 2016 Volume 22 Issue 14
50 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease by immunohistochemistry in formalin-fixed, paraffinembedded liver sections of patients with non-alcoholic fatty liver disease (NAFLD) (n = 44) or alcoholic liver disease (ALD) (n = 25). Liver resections obtained from 3 healthy subjects candidate for partial liver donation served as controls. Histological evaluations were performed by two experienced pathologists, and diagnoses established based on international criteria. The intensity of the PTEN staining in nuclei was compared between steatotic and non-steatotic areas of each liver fragment analyzed. For each liver specimen, the antibody-stained sections were examined and scored blindly by three independent observers, who were unaware of the patients clinical history. RESULTS: In healthy individuals, PTEN immunostaining was intense in both the cytoplasm and nuclei of all hepatocytes. However, PTEN was strongly downregulated in both the nucleus and the cytoplasm of hepatocytes from steatotic areas in patients with NAFLD, independently of the disease stage. In contrast, no changes in PTEN protein expression were observed in patients with ALD, regardless of the presence of steatosis or the stage of the disease. The degree of PTEN downregulation in hepatocytes of patients with NAFLD correlated with the percentage of steatosis (r = , p = ) and the BMI (r = , p = ). Hovewer, in patients with ALD, PTEN expression was not correlated with the percentage of steatosis with or without obesity as a confounding factor (p = ). Finally, PTEN expression level in steatotic areas of ALD patients was significantly different from that seen in steatotic areas of NAFLD patients (p < ). CONCLUSION: PTEN protein expression is downregulated early in NAFLD, but not in ALD. PTEN immunohistochemical detection could help in the differential diagnosis of NAFLD and ALD. Key words: Fibrosis; Phosphatase and tensin homolog; Steatosis; Non-alcoholic fatty liver disease; Nonalcoholic steatohepatitis; Alcoholic liver disease; Cirrhosis; Hepatocellular carcinoma The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Non-alcoholic fatty liver disease (NAFLD) and alcoholic liver disease (ALD) display similar histopathological features making difficult to discriminate between them apart from patient history. In this report, we assessed the phosphatase and tensin homolog (PTEN) expression level by immunohistochemistry and observed that while PTEN was downregulated in steatotic hepatocytes from patients with NAFLD, its expression remained unchanged in patients with ALD. We therefore propose that the evaluation of PTEN expression could be a useful tool for the differential diagnosis of NAFLD and ALD. Sanchez-Pareja A, Clément S, Peyrou M, Spahr L, Negro F, Rubbia-Brandt L, Foti M. Phosphatase and tensin homolog is a differential diagnostic marker between nonalcoholic and alcoholic fatty liver disease. World J Gastroenterol 2016; 22(14): Available from: URL: com/ /full/v22/i14/3735.htm DOI: org/ /wjg.v22.i INTRODUCTION Non-alcoholic fatty liver disease (NAFLD) and alcoholic liver disease (ALD) are two major causes of chronic liver disease worldwide [1]. Both conditions display very similar histopathological features ranging from excessive accumulation of fat in the liver (steatosis) to steatohepatitis, fibrosis and cirrhosis [2]. Development of hepatocellular carcinoma (HCC) is a severe complication of both liver diseases. Liver biopsy is the gold standard method to confirm the diagnosis and to evaluate the degree of necroinflammatory activity and the stage of fibrosis. For the NAFLD, a scoring system (NAFLD activity score or NAS) may be useful to identify patients who are at risk to develop cirrhosis [3]. However, the differential diagnosis between ALD and NAFLD cannot be made on the basis of histological criteria alone, as it relies on patient s reported alcohol consumption, which is subject to the well-known selfreporting biases. The phosphatase and tensin homolog deleted on chromosome 10 (PTEN) is a major tumor suppressor frequently mutated/deleted or downregulated in human cancers including HCC [4,5]. The tumor suppressive activity of PTEN appears to rely on multiple functions of this protein, including antagonism of PI3K signaling in response to growth factors [6], modulation of the activity of critical factors regulating cell adhesion, migration and invasion [7-9], and maintenance of chromosome stability and DNA repair [10]. In addition, the expression or activity of a whole network of other tumour suppressors frequently altered in human cancers can be modulated by dysregulated PTEN expression or activity [11]. Importantly, recent evidence indicated that in contrast to the classical two hits Knudson s hypothesis for tumour suppressors, PTEN haploinsufficiency, or even a partial loss of its activity/expression through posttranscriptional alterations, is sufficient to promote carcinogenesis in specific organs [12]. Conditional knockout of PTEN specifically in hepatocytes was shown to induce the sequential development of steatosis, fibrosis and HCC with ageing in mice [13]. Conversely, we previously demonstrated that PTEN expression/activity was downregulated in the liver of obese human and rodent models developing hepatic steatosis [14]. Further analyses revealed that PTEN expression was downregulated in cultured hepatocytes exposed to free fatty acids [15]. Together, these data indicated that alterations of PTEN expression/activity 3736 April 14, 2016 Volume 22 Issue 14
51 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease represent an early event in NAFLD likely contributing to steatosis development. Surprisingly, studies in rodents, or using in vitro cell cultures, indicated that hepatic PTEN expression might be not decreased, but rather increased, with abusive alcohol consumption although histopathological alterations of the liver are very similar to those occurring in NAFLD [16-19]. However, whether these findings are relevant for human diseases is still unclear and the PTEN expression and activity status in the liver of patients with ALD is unknown. Based on the above observations, we hypothesized that PTEN expression level in the liver may allow discriminating between NAFLD and ALD. Thus, we investigated the expression of PTEN by immunohistochemistry in liver biopsy samples from patients displaying all histopathological stages of NAFLD and ALD. Our results demonstrate that assessing PTEN protein expression in human livers may represent an important tool for the differential diagnosis of NAFLD and ALD. MATERIALS AND METHODS Human samples Liver biopsy samples were collected between 2006 and 2015 from patients consecutively admitted at the Division of Gastroenterology and Hepatology of Geneva University Hospitals for investigation of abnormal liver function tests and fulfilling the diagnostic criteria of NAFLD or ALD [20]. Overall, a total of 69 patients were studied, including 44 obese patients with NAFLD, 17 non-obese patients with ALD and 8 obese patients with ALD. All patients had a negative serology for hepatitis B and C, tested negative for autoantibodies, have normal α-antitrypsin and ceruloplasmin serum levels and normal transferrin saturation. No patients were under medications that may induce steatohepatitislike lesions. Patients with NAFLD were obese (Median BMI 41) and consume less than 10 gr of alcohol per day. Patients with ALD had a median BMI of 26 and declared daily alcohol intake above or equal to 40 gr for women and 60 gr for men at the time of liver biopsy. Liver resections obtained from 3 healthy subjects candidate for partial liver donation served as controls. Demographic data, including age, sex, body mass index (BMI) and alcohol consumption, were collected at the time of liver biopsy. Histology and immunohistochemistry Liver biopsies were formalin-fixed, paraffin-embedded and processed for histological staining. Histological evaluations were performed by two experienced pathologists, and diagnoses established based on international criteria [20]. NAFLD activity and fibrosis were graded using the NAS score [21]. Steatosis severity was scored as follows: 0 (none) 2%, 1 (mild) = 2%-30%, 2 (moderate) = 30%-60% and 3 (severe) 60% of hepatocytes affected. All biopsy samples were processed together for the HE staining and PTEN immunohistological staining. Immunohistochemical analysis of PTEN expression was performed as previously described [14]. The intensity of the PTEN staining in nuclei was compared between steatotic (S) and non-steatotic (NS) areas of each liver fragment analyzed. Both S and NS areas from all slides were scored on a staining intensity scale from 0 to 4 with score = 0 for lack of staining, score = 1 for weak staining, score = 2 for moderate staining, score = 3 for strong staining and score = 4 representing the highest intensity. Then, the difference between NS and S areas (NS-S) was calculated. For each liver specimen, the antibodystained sections were examined and scored blindly by three independent observers, who were unaware of the patients clinical history. Statistical analyses Statistical analyses were performed using oneway analysis of variance followed by Turkey test for continuous variables and nonparametric Spearman correlation for categorical variables. RESULTS PTEN expression is downregulated in steatotic hepatocytes from patients with NAFLD PTEN expression was investigated in 44 patients with NAFLD at different stages of disease (steatosis n = 10, steatohepatitis without fibrosis n = 14, steatohepatitis with fibrosis n = 12 and cirrhosis n = 8) and compared to liver biopsy specimens from 3 healthy donors. In healthy individuals (Figure 1a and b), PTEN immunostaining was intense in both the cytoplasm and nuclei of all hepatocytes (Figure 1a and b). In the liver biopsies of patients with NAFLD, a significant decrease of PTEN expression was observed in steatotic hepatocytes, or in those in their close vicinity. Importantly, non-steatotic areas within the same specimen displayed similar immunostaining intensity than those of healthy controls, suggesting that PTEN expression was altered only in steatotic areas of NAFLD patients. Decrease of PTEN expression occurred in both the nucleus and the cytoplasm of hepatocytes. Nevertheless, only the nuclear staining was used to establish the PTEN score in order to prevent misevaluation of cytoplasmic PTEN staining potentially corrupted by the presence of large and unstained cytoplasmic lipid droplets in steatotic areas. When patients were divided according to the NAFLD stage, the expression of PTEN in steatotic areas was decreased in 9/10 patients with steatosis only (Figure 1c and d, Table 1), in 12/14 patients with steatosis and inflammatory infiltrate (Figure 1e and f, Table 1), in 11/12 patients with fibrosis (Figure 1g and h, Table 1) and 6/8 patients with cirrhosis (Figure 1i and j, Table 1). The degree of PTEN downregulation 3737 April 14, 2016 Volume 22 Issue 14
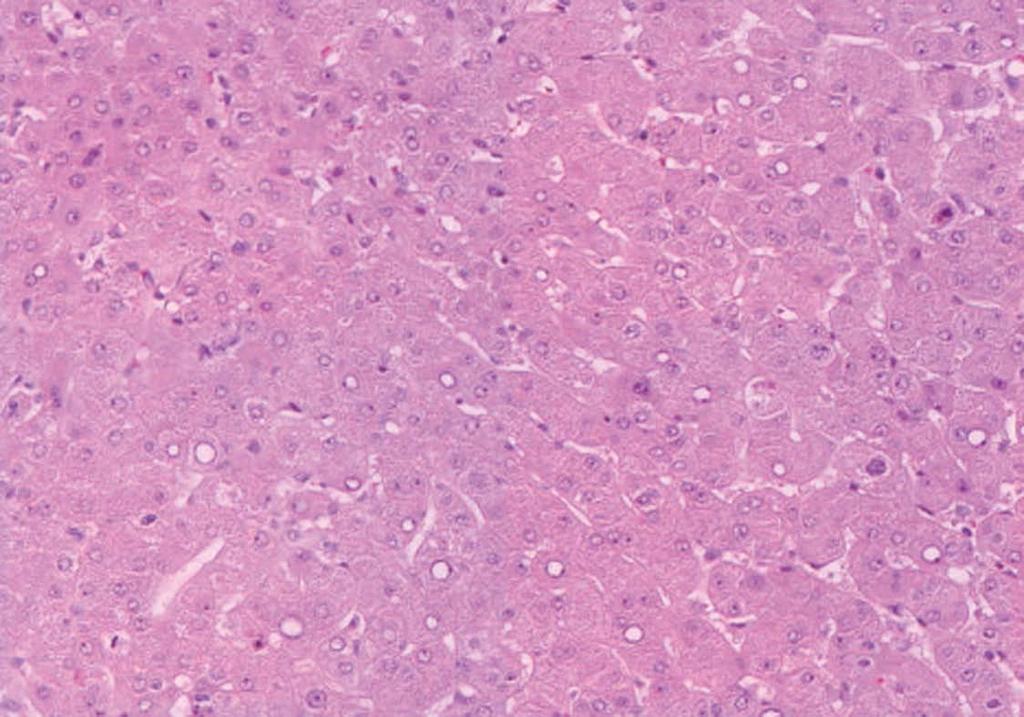
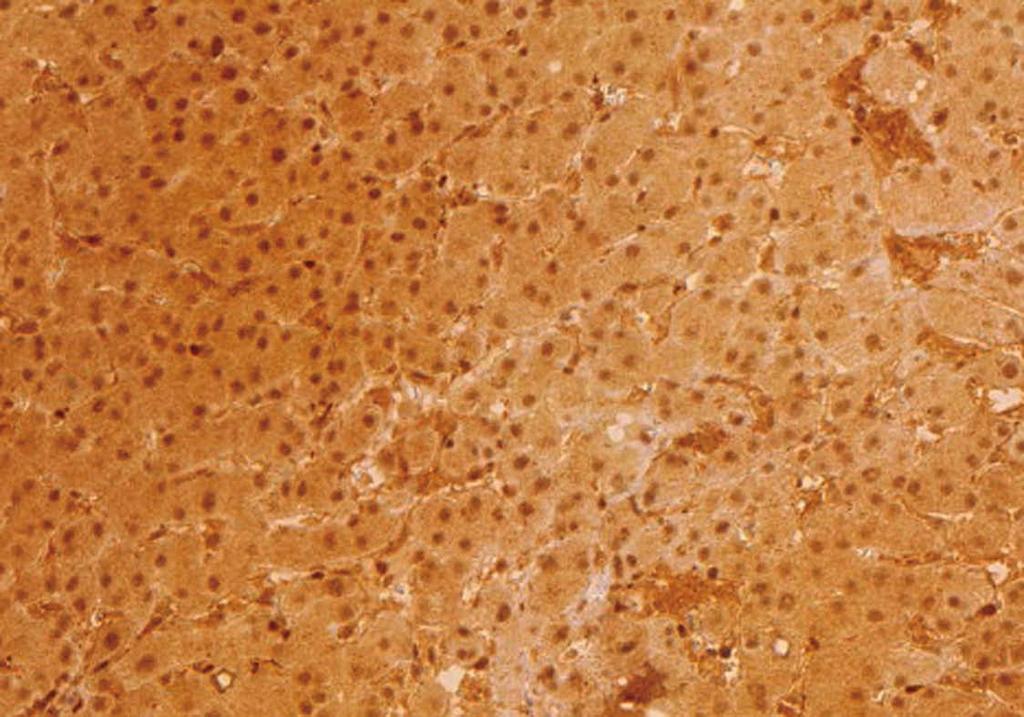
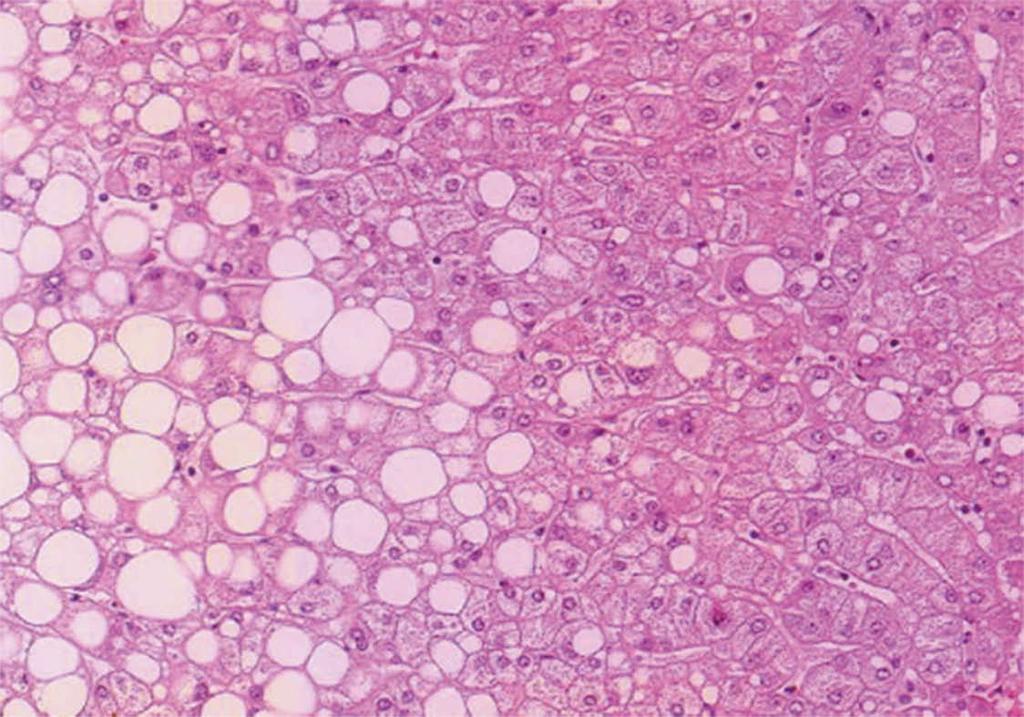
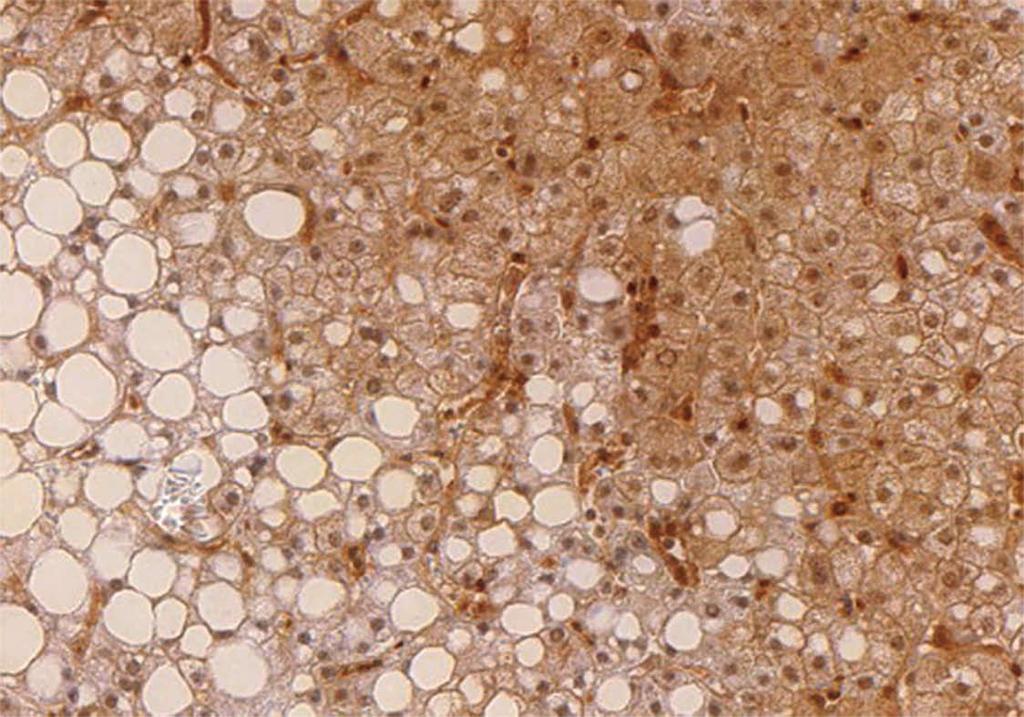
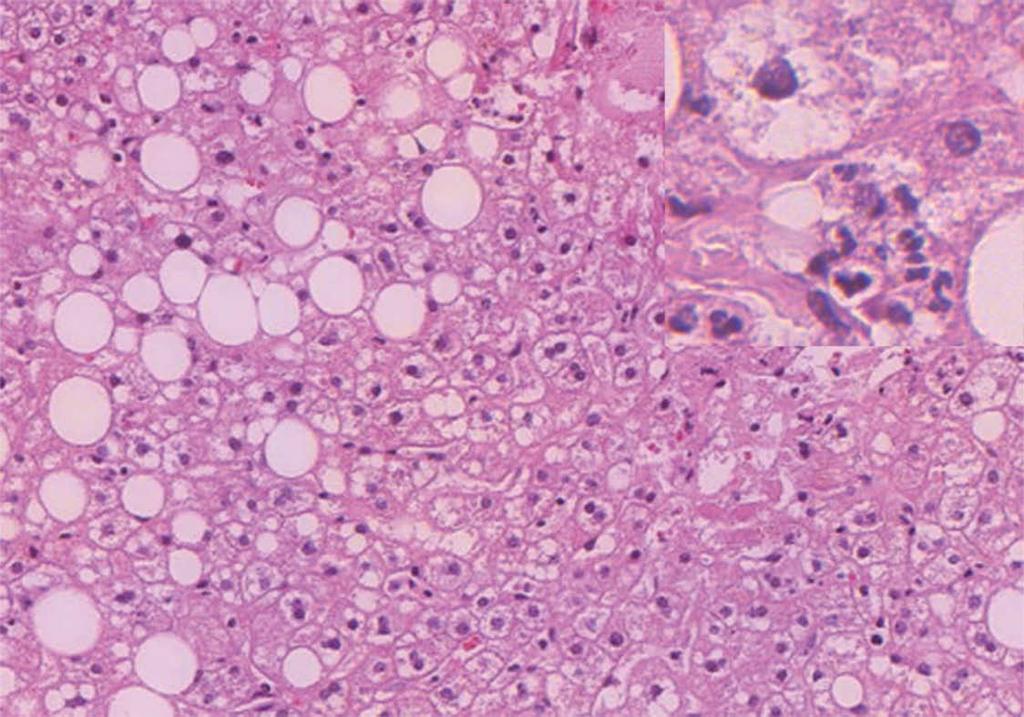
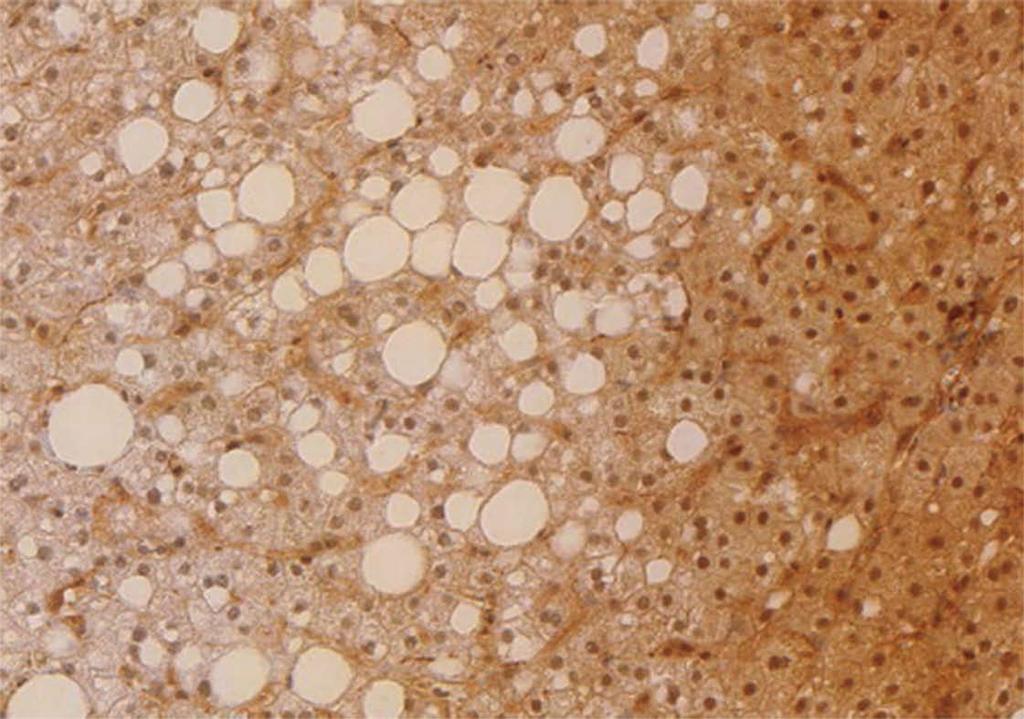
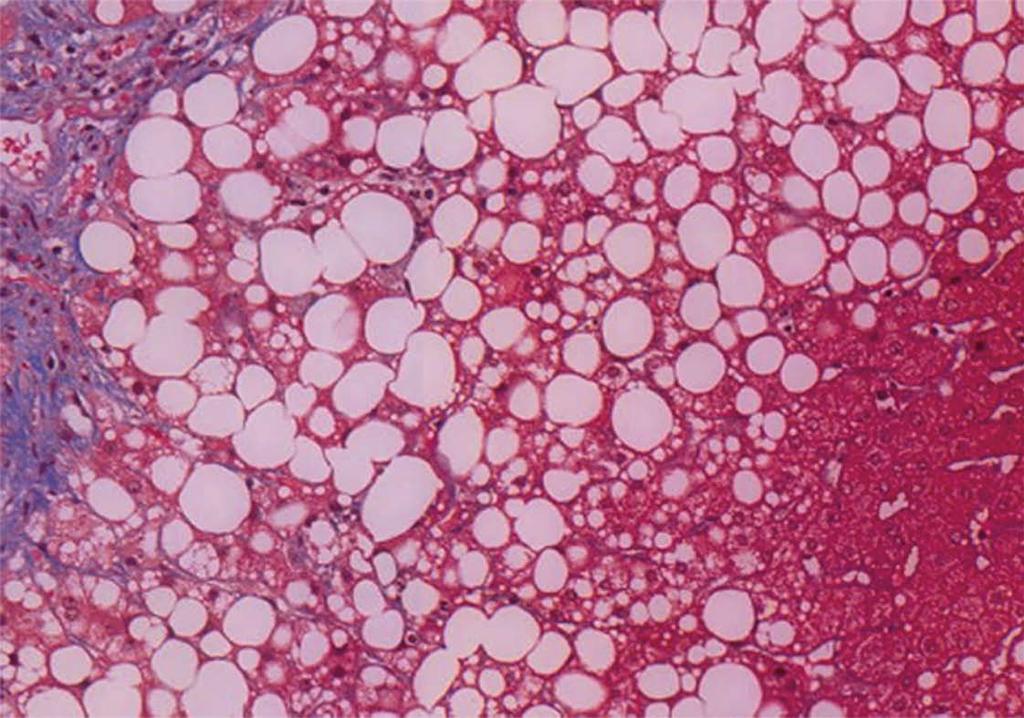
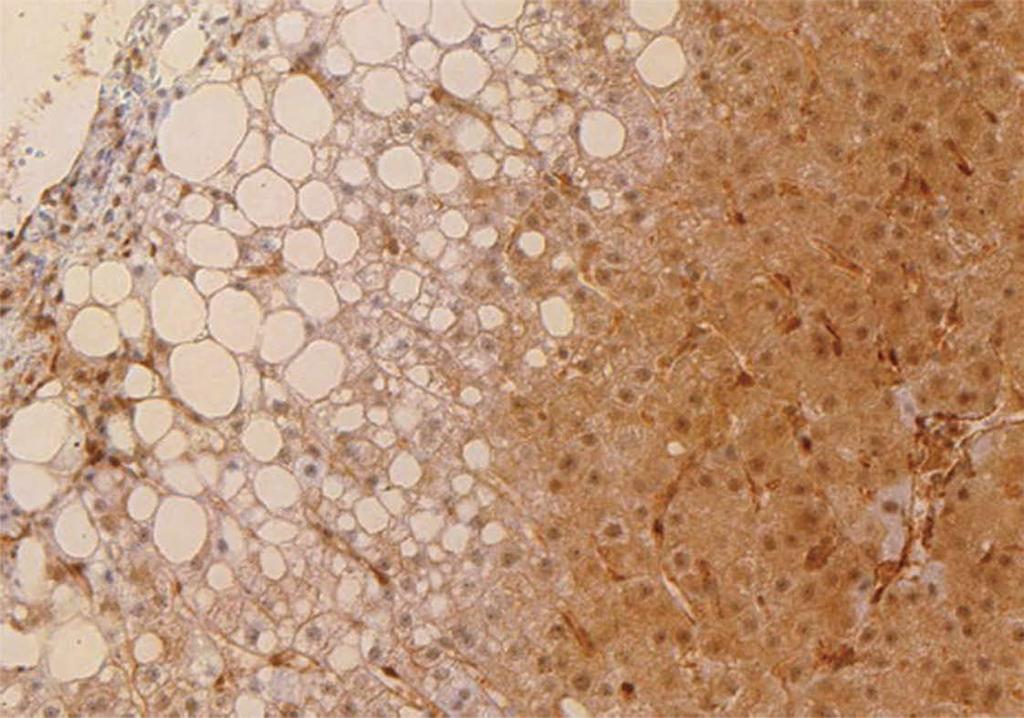
52 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease A B C D E * F G H 3738 April 14, 2016 Volume 22 Issue 14

 or of obese patients with steatosis (n = 10, C and D), nonalcoholic steatohepatitis (n = 14, E and F), fibrosis (n = 12, G and H) and cirrhosis (n = 8, I")
53 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease I J Figure 1 General histology and immunohistochemical detection of phosphatase and tensin homolog protein expression in the liver of healthy donor (hepatic resections) or patients with different stages of non-alcoholic fatty liver disease (liver biopsies). Liver sections of healthy donors (A and B) or of obese patients with steatosis (n = 10, C and D), nonalcoholic steatohepatitis (n = 14, E and F), fibrosis (n = 12, G and H) and cirrhosis (n = 8, I and J) were either stained with hematoxylin eosin (A, C, E), Masson s trichrome (G and I) or immunostained with anti-pten antibody (B, D, F, H and J). The inset in image (E) shows hepatic intralobular inflammation characterized by neutrophils (arrow) and ballooning hepatocyte (star). Scale bar = 100 µm. PTEN: Phosphatase and tensin homolog. Table 1 Demographic data, histological diagnosis of liver biopsies and phosphatase and tensin homolog expression in patients with non-alcoholic fatty liver disease Case Age/sex BMI (kg/m 2 ) Lobular inflammation Hepatocyte ballooning Steatosis score Steatosis Fibrosis NAS score Scores for PTEN expression NS S NS-S Controls 1 86/M ND % / / 2 32/F ND % / / 3 36/M ND % / / Pure steatosis 4 26/M % /M % /F % /F % /F % /M % /M % /F % /M % /M % Steatohepatitis without fibrosis 14 49/F % /F % /M % /F % /M % /F % /F % /M % /F % /F % /F % /F % /M % /F % Steatohepatitis with fibrosis 28 62/M % 1a /F % 1a /M % 1a /F % 1a /M % 1a /M % 1b /M % 1b /F % 1c /M % /F % /M % /M % April 14, 2016 Volume 22 Issue 14
54 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease Cirrhosis 40 61/M ND % /F % /M % /F % /M % /F % /F % /F % The intensity of the PTEN nuclear staining was scored in steatotic (S) and non-steatotic (NS) areas of biopsies. All slides from healthy (Controls) and obese patients were scored on a staining intensity scale from 0 to 4 with score = 4 representing the highest intensity. Difference between NS and S area (NS-S) was calculated. ND: Not determined; PTEN: Phosphatase and tensin homolog. in hepatocytes of patients with NAFLD only weakly correlated with the percentage of steatosis (r = , p = ) and the BMI (r = , p = ), but not with the NAS score (p = ), sex (p = ), age (p = ), fibrosis stage (p = ), degree of lobular inflammation (p = ) or hepatocyte ballooning (p = ). Steatosis in patients with ALD does not alter PTEN expression in hepatocytes PTEN expression was then performed on paraffinembedded liver specimens from 25 patients with ALD at different stages of disease (all had steatosis, 15 had inflammation, 13 had different degrees of fibrosis and 21 had cirrhosis) (Table 2). In contrast to NAFLD patients, the presence of steatosis in liver samples of patients with ALD was not associated with a significant decrease of PTEN expression. Indeed, the intensity of PTEN immunostaining was similar in steatotic and nonsteatotic areas of each liver biopsy, unaffected by the stage of the disease or obesity, and always comparable to the PTEN staining of healthy liver controls (Figure 2). PTEN expression was therefore not correlated with the percentage of steatosis in patients with ALD with or without obesity as a confounding factor (p = ). Finally, the PTEN expression level in steatotic areas of ALD patients was significantly different from that seen in steatotic areas of NAFLD patients (p < ). DISCUSSION NAFLD and ALD are two frequent liver diseases that require each a specific clinical management [22]. Non-alcoholic steatohepatitis is primarily managed by lifestyle interventions, i.e., body weight loss combined to increased physical activity [22-24] associated with selected insulin sensitizers [22,25] and vitamin E administration [22,26]. Patients with ALD require complete alcohol abstinence, and, in severe forms of steatohepatitis, a short course of steroids, which has been proven effective in reducing mortality [27]. Unfortunately, the differential diagnosis between NAFLD and ALD may be difficult, owing to the bias intrinsic to the self-reported nature of alcohol consumption. In addition, both NAFLD - in its steatohepatitis form - and ALD share similar histological features. However, macrovesicular steatosis is reportedly more frequent and severe in NAFLD than in ALD, whereas microvesicular steatosis, lobular inflammation, Mallory- Denk bodies, satellitosis, acute cholestasis, sclerosing hyaline necrosis and veno-occlusive disease occur more frequently in ALD than in non-alcoholic steatohepatitis [28]. Nevertheless, all these histological features remain non-specific. Although one study suggested a disease-specific pattern of fibrosis silver impregnation i.e., lattice-like in non-alcoholic steatohepatitis and solid in ALD [29], a molecular marker easy to use and able to discriminate between NAFLD and ALD has not been identified yet. Here, we show the potential role of PTEN immunostaining as a differential diagnostic marker to discriminate between ALD and NAFLD. The PTEN expression was found to be decreased in steatotic areas of the liver of patients with NAFLD, while being preserved in patients with ALD, irrespectively of the presence of obesity, steatosis and/or the liver disease stage. However, it has to be acknowledged that our group of patients with ALD is small and somewhat heterogeneous with regards to fibrosis and inflammation. Nevertheless, if our results are confirmed at a largest scale, PTEN immunostaining could be a valuable routine diagnostic tool for differentiating ALD and NAFLD therefore helping the decision making process in the clinical management of these patients. The mechanisms of lipid accumulation in NAFLD and ALD are only partially known: some appear to be shared, while others seem to follow disease-specific pathways. The unfolded protein response is activated in both NAFLD and ALD by oxidative stress, and leads to the increase of transcriptional factors, such as the sterol regulatory element binding proteins, involved in de novo fatty acid synthesis [30,31]. Adiponectin, an adipokine produced by adipocytes that stimulates fatty acid oxidation, is downregulated in both NAFLD [32] and ALD [33]. On the other hand, some mechanisms contributing to the development of steatosis might be disease-specific. For example, an augmented lipolysis in the adipose tissue leading to increased circulating free fatty acids has been reported to occur mainly in NALFD but not in ALD [30,34-36], although this difference has been recently challenged in rodent models [37]. Dysregulated immune mechanisms may also play an important role in the early events and progression of 3740 April 14, 2016 Volume 22 Issue 14

 or")
 or of patients with alcoholic")
 were stained with hematoxylin eosin (A, C and E),")
. Scale bar = 100 µm.")
. Scale bar = 100 µm.")
![PTEN: Phosphatase and tensin homolog. [38] alcohol-related liver injuries.](/docs-images/92/109922872/images/55-6.jpg "Increasing evidence currently supports a key role for PTEN in the development")

55 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease A B C D E * G F H Figure 2 General histology and immunohistochemical detection of phosphatase and tensin homolog protein expression in the liver of healthy donor (hepatic resections) or patients with different stages of alcoholic liver disease (liver biopsies). Liver sections of healthy donors (A and B) or of patients with alcoholic steatosis (C and D), alcoholic steatohepatitis (E and F) and cirrhotic alcoholic disease (G and H) were stained with hematoxylin eosin (A, C and E), Massson s trichrome (G) or immunostained with anti-pten antibody (B, D, F and H). Scale bar = 100 µm. The inset in image (E) shows hepatic intralobular inflammation characterized by neutrophils (star). Scale bar = 100 µm. PTEN: Phosphatase and tensin homolog. [38] alcohol-related liver injuries. Increasing evidence currently supports a key role for PTEN in the development of steatosis and fibrosis with distinct etiologies. First, mice bearing a hepatocyte- specific deletion of PTEN develop sequentially an extended hepatic steatosis, inflammation, fibrosis and [13,39] HCC with ageing. In vitro studies also showed that PTEN downregulation triggers lipid accumulation in 3741 April 14, 2016 Volume 22 Issue 14
56 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease Table 2 Demographic data, histological diagnosis of liver biopsies and phosphatase and tensin homolog expression in patients with alcoholic liver disease Case Age/sex BMI (kg/m 2 ) Inflammation Fibrosis Cirrhosis Steatosis Score for PTEN expression NS S NS-S Non-obese patients 1 56/F 26 - p - 100% /F 25 - psn - 40% /M % /F % /M % /F % /M 25 + psn + 70% /M 23 + psn + 80% /M % /M 24 + psn + 40% /M % /F % /F % /M 25 - p + 90% /M 20 + psn + 70% /M 20 - psn + 80% /M 23 - psn + 70% Obese patients 18 60/M 30 - psn - 70% /F 41 - p - 70% /M % /M % /M % /M 31 - psn + 5% /M 34 + psn + 90% /M % The intensity of the PTEN staining was scored in steatotic (S) and non-steatotic (NS) areas of liver sections. All liver sections from ALD patients were scored on a staining intensity scale from 0 to 4 with score = 4 representing the highest intensity. Difference between NS and S area (NS-S) was calculated. ND: Not determined; Ctrl: Controls; psn: Perisinusoidal; p: Portal; PTEN: Phosphatase and tensin homolog; ALD: Alcoholic liver disease. hepatoma cell lines [14,40]. Consistent with these studies, PTEN expression is decreased in steatotic livers of genetic and diet-induced obese rat models and in obese human subjects [14]. Hepatic PTEN downregulation was further reported in three different rodent models of liver inflammation/fibrosis induced either by a methionine/ choline deficient diet [41], or bile-duct ligation [42] or CCL4 administration [43]. In hepatitis C virus (HCV) infection, PTEN expression and/or activity were also reported to be altered in hepatocytes and to promote the development of steatosis [44]. PTEN downregulation was even reported to represent an independent prognostic factor for the survival of HCV-infected patients developing a cirrhotic HCC [45]. It thus appears that steatosis and its progression towards more severe hepatic disorders are associated with PTEN protein downregulation in the case of the metabolic syndrome and HCV infection. The observation linking PTEN downregulation with liver disease progression in NAFLD and hepatitis C may have implications for treatment. Regular statin use has been shown to upregulate PTEN in heart tissue [46,47], skeletal muscles [48] and cancer cells [49-51] through various mechanisms including decreased expression of PTEN-targeting micrornas [52], NF-κB inactivation [49] and PPARγ activation [50,51]. Regarding the relationship between statins and liver disease progression, the few data in NAFLD suggests some beneficial effect, at least on steatosis [53]. More convincing evidence has been reported in patients with chronic hepatitis C, where statin use was associated with a significantly lower liver fibrosis progression, independently of inflammation and viral load changes over time [54-56]. Thus, one cannot exclude that the beneficial effects of statins may be mediated by PTEN upregulation in the liver with NAFLD or HCV infection, however direct evidence are currently lacking. Obviously, the longterm use of statins in these conditions should also be weighed against the risk of toxicity, in particular concerning the increased risk of insulin resistance and type 2 diabetes development, which can results from PTEN upregulation in skeletal muscles [48,57,58]. Surprisingly, PTEN protein expression was reported increased in hepatoma cells exposed to ethanol [18] and in the liver of rats chronically fed with ethanol [16]. However, although PTEN expression is upregulated in the liver of ethanol-fed mice, the enzyme was shown to be highly carbonylated, a post-translational modification that decreases its phosphatase activity [59]. From these data, it results that steatosis in ALD is also associated in final with an impaired PTEN activity, although this defect is mediated by inhibition 3742 April 14, 2016 Volume 22 Issue 14
57 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease of its enzymatic activity and not by repression of its expression as it is the case with obesity and HCV infection. The mechanisms leading to PTEN protein upregulation in hepatocytes exposed to alcohol are currently unknown. One attractive hypothesis is that PTEN transcription is stimulated by the transcription factor Egr1 in response to alcohol [60,61]. However, assessing whether PTEN expression is modulated at the mrna level in human livers is technically challenging. Indeed, isolation of good quality mrna from human liver biopsies processed for histological analysis is still poorly effective and cannot be used in routine diagnostic procedures. In addition, the high expression of a PTEN pseudogene (PTENP1) in human tissues can lead to misinterpretation of analyses aiming at assessing PTEN mrna expression in pathological situations [62]. This is the reason why immunohistochemical detection of PTEN protein expression in clinical samples remains likely the gold standard method to assess PTEN expression in liver biopsies. Our data and previous reports discussed here strongly support the concept that downregulation of either the expression, or the activity, of PTEN represents an important pathological mechanism contributing to the development of fatty liver diseases with distinct etiologies. However the mechanism affecting PTEN functions are different depending on the etiologies of the diseases. In this study, we show that we can take advantage of the different molecular mechanisms affecting PTEN activity or expression in liver metabolic disorders to identify their etiology. Thus, the immunohistochemical detection of PTEN protein expression should be added to the diagnostic armamentarium of pathologists and clinicians in the differential diagnosis of NAFLD and ALD in humans. COMMENTS Background Similar histopathological alterations occur in patients suffering from nonalcoholic fatty liver disease (NAFLD) and alcoholic liver disease (ALD). Therefore, the differential diagnosis between ALD and NAFLD cannot be made on the basis of histological criteria alone, and it must rely on patient s reported alcohol consumption, which is subject to the well-known self-reporting biases. Studies in rodents, or in vitro, indicated that hepatic phosphatase and tensin homolog (PTEN) expression is decreased with obesity-associated steatosis, whereas it is increased with abusive alcohol consumption, although histopathological alterations of the liver are very similar. However, whether these findings are relevant for human diseases is still unclear and the PTEN expression and activity status in the liver of patients with ALD is unknown. Research frontiers Biomarker research in liver diseases is of growing importance not only to provide reliable differential diagnostic markers for therapeutic choices, but also as prognostic factors for progression of early stages of these diseases toward more severe pathologies such as cirrhosis and cancer. Innovations and breakthroughs Studies in rodents, or in vitro, indicate that alteration of PTEN function is a common event occurring at early stage of NAFLD, hepatitis C virus (HCV) infection and ALD. However, the molecular mechanisms underlining the loss of PTEN function are different, since they consist of the PTEN protein downregulation in NAFLD and HCV infection, whereas in ALD only PTEN activity is impaired but not its expression. In this study, the authors reported the differential expression of the PTEN protein in the liver of patients with NAFLD or ALD at various stages of these diseases, a finding of diagnostic significance. Applications Herein, the authors show that the different molecular mechanisms affecting PTEN expression in liver metabolic disorders can be an advantage to identify their etiology. Thus, the immunohistochemical detection of PTEN protein expression should be added to the diagnostic armamentarium of pathologists and clinicians in the differential diagnosis of NAFLD and ALD in humans. Terminology The two hits Knudson s hypothesis for tumour suppressors suggests that each allele of a tumour suppressor needs to be mutated, or deleted, to contribute to carcinogenesis, since one copy of a tumour suppressor is sufficient to ensure its function. Mallory-Denk bodies are damaged eosinophilic filamentous material forming inclusions in the cytoplasm of hepatocytes, in both ALD and NAFLD. Peer-review The article is very interesting and useful for clinicians. The small number of patients included in the study is a limit recognized by the authors, but most studies requiring liver biopsy in these types of pathology are difficult to achieve in a single center. A multicenter future study would be useful in this regard. Authors must underline the clinical implications of their research and add to discussion a comment on the beneficial role of statins, with regard to PTEN expression, in nonalcoholic fatty liver disease and in chronic hepatitis C. REFERENCES 1 Hellerbrand C. Pathophysiological similarities and synergisms in alcoholic and non-alcoholic steatohepatitis. Dig Dis 2010; 28: [PMID: DOI: / ] 2 Tannapfel A, Denk H, Dienes HP, Langner C, Schirmacher P, Trauner M, Flott-Rahmel B. [Histopathological diagnosis of nonalcoholic and alcoholic fatty liver disease. Grade 2 consensusbased guidelines]. Pathologe 2010; 31: [PMID: DOI: /s x] 3 Brunt EM, Kleiner DE, Wilson LA, Belt P, Neuschwander-Tetri BA. Nonalcoholic fatty liver disease (NAFLD) activity score and the histopathologic diagnosis in NAFLD: distinct clinicopathologic meanings. Hepatology 2011; 53: [PMID: DOI: /hep.24127] 4 Peyrou M, Bourgoin L, Foti M. PTEN in liver diseases and cancer. World J Gastroenterol 2010; 16: [PMID: DOI: /wjg.v16.i ] 5 Peyrou M, Bourgoin L, Foti M. PTEN in non-alcoholic fatty liver disease/non-alcoholic steatohepatitis and cancer. Dig Dis 2010; 28: [PMID: DOI: / ] 6 Maehama T, Dixon JE. The tumor suppressor, PTEN/MMAC1, dephosphorylates the lipid second messenger, phosphatidylinositol 3,4,5-trisphosphate. J Biol Chem 1998; 273: [PMID: DOI: /jbc ] 7 Zhang XC, Piccini A, Myers MP, Van Aelst L, Tonks NK. Functional analysis of the protein phosphatase activity of PTEN. Biochem J 2012; 444: [PMID: DOI: / BJ ] 8 Davidson L, Maccario H, Perera NM, Yang X, Spinelli L, Tibarewal P, Glancy B, Gray A, Weijer CJ, Downes CP, Leslie NR. Suppression of cellular proliferation and invasion by the concerted lipid and protein phosphatase activities of PTEN. Oncogene 2010; 29: [PMID: DOI: /onc ] 9 Tamura M, Gu J, Matsumoto K, Aota S, Parsons R, Yamada KM. Inhibition of cell migration, spreading, and focal adhesions by tumor suppressor PTEN. Science 1998; 280: [PMID: 3743 April 14, 2016 Volume 22 Issue 14
58 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease DOI: /science ] 10 Planchon SM, Waite KA, Eng C. The nuclear affairs of PTEN. J Cell Sci 2008; 121: [PMID: DOI: / jcs ] 11 Leslie NR, Foti M. Non-genomic loss of PTEN function in cancer: not in my genes. Trends Pharmacol Sci 2011; 32: [PMID: DOI: /j.tips ] 12 Berger AH, Knudson AG, Pandolfi PP. A continuum model for tumour suppression. Nature 2011; 476: [PMID: DOI: /nature10275] 13 Horie Y, Suzuki A, Kataoka E, Sasaki T, Hamada K, Sasaki J, Mizuno K, Hasegawa G, Kishimoto H, Iizuka M, Naito M, Enomoto K, Watanabe S, Mak TW, Nakano T. Hepatocytespecific Pten deficiency results in steatohepatitis and hepatocellular carcinomas. J Clin Invest 2004; 113: [PMID: DOI: /JCI20513] 14 Vinciguerra M, Veyrat-Durebex C, Moukil MA, Rubbia- Brandt L, Rohner-Jeanrenaud F, Foti M. PTEN down-regulation by unsaturated fatty acids triggers hepatic steatosis via an NFkappaBp65/mTOR-dependent mechanism. Gastroenterology 2008; 134: [PMID: DOI: /j.gastro ] 15 Vinciguerra M, Sgroi A, Veyrat-Durebex C, Rubbia-Brandt L, Buhler LH, Foti M. Unsaturated fatty acids inhibit the expression of tumor suppressor phosphatase and tensin homolog (PTEN) via microrna-21 up-regulation in hepatocytes. Hepatology 2009; 49: [PMID: DOI: /hep.22737] 16 Yeon JE, Califano S, Xu J, Wands JR, De La Monte SM. Potential role of PTEN phosphatase in ethanol-impaired survival signaling in the liver. Hepatology 2003; 38: [PMID: DOI: /jhep ] 17 Yao XH, Grégoire Nyomba BL. Abnormal glucose homeostasis in adult female rat offspring after intrauterine ethanol exposure. Am J Physiol Regul Integr Comp Physiol 2007; 292: R1926-R1933 [PMID: DOI: /ajpregu ] 18 Shulga N, Hoek JB, Pastorino JG. Elevated PTEN levels account for the increased sensitivity of ethanol-exposed cells to tumor necrosis factor-induced cytotoxicity. J Biol Chem 2005; 280: [PMID: DOI: /jbc.M ] 19 He J, de la Monte S, Wands JR. Acute ethanol exposure inhibits insulin signaling in the liver. Hepatology 2007; 46: [PMID: DOI: /hep.21904] 20 Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, Charlton M, Sanyal AJ. The diagnosis and management of nonalcoholic fatty liver disease: practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012; 55: [PMID: DOI: /hep.25762] 21 Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, Ferrell LD, Liu YC, Torbenson MS, Unalp-Arida A, Yeh M, McCullough AJ, Sanyal AJ. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005; 41: [PMID: DOI: / hep.20701] 22 Spahr L, Hadengue A. [Alcoholic and nonalcoholic steatohepatitis: the same disease! II. Management]. Rev Med Suisse 2005; 1: [PMID: ] 23 Huang MA, Greenson JK, Chao C, Anderson L, Peterman D, Jacobson J, Emick D, Lok AS, Conjeevaram HS. One-year intense nutritional counseling results in histological improvement in patients with non-alcoholic steatohepatitis: a pilot study. Am J Gastroenterol 2005; 100: [PMID: DOI: /j x] 24 Hickman IJ, Jonsson JR, Prins JB, Ash S, Purdie DM, Clouston AD, Powell EE. Modest weight loss and physical activity in overweight patients with chronic liver disease results in sustained improvements in alanine aminotransferase, fasting insulin, and quality of life. Gut 2004; 53: [PMID: DOI: /gut ] 25 Marchesini G, Brizi M, Bianchi G, Tomassetti S, Zoli M, Melchionda N. Metformin in non-alcoholic steatohepatitis. Lancet 2001; 358: [PMID: DOI: / S (01) ] 26 Harrison SA, Torgerson S, Hayashi P, Ward J, Schenker S. Vitamin E and vitamin C treatment improves fibrosis in patients with nonalcoholic steatohepatitis. Am J Gastroenterol 2003; 98: [PMID: DOI: /j x] 27 Mathurin P, Mendenhall CL, Carithers RL, Ramond MJ, Maddrey WC, Garstide P, Rueff B, Naveau S, Chaput JC, Poynard T. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis (AH): individual data analysis of the last three randomized placebo controlled double blind trials of corticosteroids in severe AH. J Hepatol 2002; 36: [PMID: DOI: /S (01) ] 28 Tannapfel A, Denk H, Dienes HP, Langner C, Schirmacher P, Trauner M, Flott-Rahmel B. Histopathological diagnosis of nonalcoholic and alcoholic fatty liver disease. Virchows Arch 2011; 458: [PMID: DOI: /s ] 29 Nakano M, Fukusato T. Histological study on comparison between NASH and ALD. Hepatol Res 2005; 33: [PMID: DOI: /j.hepres ] 30 Sozio MS, Liangpunsakul S, Crabb D. The role of lipid metabolism in the pathogenesis of alcoholic and nonalcoholic hepatic steatosis. Semin Liver Dis 2010; 30: [PMID: DOI: /s ] 31 Foufelle F, Ferré P. New perspectives in the regulation of hepatic glycolytic and lipogenic genes by insulin and glucose: a role for the transcription factor sterol regulatory element binding protein-1c. Biochem J 2002; 366: [PMID: DOI: / bj ] 32 Tsochatzis EA, Papatheodoridis GV, Archimandritis AJ. Adipokines in nonalcoholic steatohepatitis: from pathogenesis to implications in diagnosis and therapy. Mediators Inflamm 2009; 2009: [PMID: ] 33 Tang H, Sebastian BM, Axhemi A, Chen X, Hillian AD, Jacobsen DW, Nagy LE. Ethanol-induced oxidative stress via the CYP2E1 pathway disrupts adiponectin secretion from adipocytes. Alcohol Clin Exp Res 2012; 36: [PMID: DOI: / j x] 34 Tamura S, Shimomura I. Contribution of adipose tissue and de novo lipogenesis to nonalcoholic fatty liver disease. J Clin Invest 2005; 115: [PMID: DOI: /JCI24930] 35 Sozio M, Crabb DW. Alcohol and lipid metabolism. Am J Physiol Endocrinol Metab 2008; 295: E10-E16 [PMID: DOI: /ajpendo ] 36 Westerbacka J, Lammi K, Häkkinen AM, Rissanen A, Salminen I, Aro A, Yki-Järvinen H. Dietary fat content modifies liver fat in overweight nondiabetic subjects. J Clin Endocrinol Metab 2005; 90: [PMID: DOI: /jc ] 37 Zhong W, Zhao Y, Tang Y, Wei X, Shi X, Sun W, Sun X, Yin X, Sun X, Kim S, McClain CJ, Zhang X, Zhou Z. Chronic alcohol exposure stimulates adipose tissue lipolysis in mice: role of reverse triglyceride transport in the pathogenesis of alcoholic steatosis. Am J Pathol 2012; 180: [PMID: DOI: / j.ajpath ] 38 Bode C, Bode JC. Activation of the innate immune system and alcoholic liver disease: effects of ethanol per se or enhanced intestinal translocation of bacterial toxins induced by ethanol? Alcohol Clin Exp Res 2005; 29: 166S-171S [PMID: DOI: /01.alc ] 39 Stiles B, Wang Y, Stahl A, Bassilian S, Lee WP, Kim YJ, Sherwin R, Devaskar S, Lesche R, Magnuson MA, Wu H. Liver-specific deletion of negative regulator Pten results in fatty liver and insulin hypersensitivity [corrected]. Proc Natl Acad Sci USA 2004; 101: [PMID: DOI: /pnas ] 40 Peyrou M, Clément S, Maier C, Bourgoin L, Branche E, Conzelmann S, Kaddai V, Foti M, Negro F. PTEN protein phosphatase activity regulates hepatitis C virus secretion through modulation of cholesterol metabolism. J Hepatol 2013; 59: [PMID: DOI: /j.jhep ] 3744 April 14, 2016 Volume 22 Issue 14
59 Sanchez-Pareja A et al. PTEN and alcoholic fatty liver disease 41 Wang B, Majumder S, Nuovo G, Kutay H, Volinia S, Patel T, Schmittgen TD, Croce C, Ghoshal K, Jacob ST. Role of microrna-155 at early stages of hepatocarcinogenesis induced by choline-deficient and amino acid-defined diet in C57BL/6 mice. Hepatology 2009; 50: [PMID: DOI: / hep.23100] 42 Hao LS, Zhang XL, An JY, Karlin J, Tian XP, Dun ZN, Xie SR, Chen S. PTEN expression is down-regulated in liver tissues of rats with hepatic fibrosis induced by biliary stenosis. APMIS 2009; 117: [PMID: DOI: /j x] 43 Zheng L, Chen X, Guo J, Sun H, Liu L, Shih DQ, Zhang X. Differential expression of PTEN in hepatic tissue and hepatic stellate cells during rat liver fibrosis and its reversal. Int J Mol Med 2012; 30: [PMID: DOI: / ijmm ] 44 Clément S, Peyrou M, Sanchez-Pareja A, Bourgoin L, Ramadori P, Suter D, Vinciguerra M, Guilloux K, Pascarella S, Rubbia- Brandt L, Negro F, Foti M. Down-regulation of phosphatase and tensin homolog by hepatitis C virus core 3a in hepatocytes triggers the formation of large lipid droplets. Hepatology 2011; 54: [PMID: DOI: /hep.24340] 45 Rahman MA, Kyriazanos ID, Ono T, Yamanoi A, Kohno H, Tsuchiya M, Nagasue N. Impact of PTEN expression on the outcome of hepatitis C virus-positive cirrhotic hepatocellular carcinoma patients: possible relationship with COX II and inducible nitric oxide synthase. Int J Cancer 2002; 100: [PMID: DOI: /ijc.10458] 46 Mensah K, Mocanu MM, Yellon DM. Failure to protect the myocardium against ischemia/reperfusion injury after chronic atorvastatin treatment is recaptured by acute atorvastatin treatment: a potential role for phosphatase and tensin homolog deleted on chromosome ten? J Am Coll Cardiol 2005; 45: [PMID: DOI: /j.jacc ] 47 Ye Y, Lin Y, Atar S, Huang MH, Perez-Polo JR, Uretsky BF, Birnbaum Y. Myocardial protection by pioglitazone, atorvastatin, and their combination: mechanisms and possible interactions. Am J Physiol Heart Circ Physiol 2006; 291: H1158-H1169 [PMID: DOI: /ajpheart ] 48 Birnbaum Y, Nanhwan MK, Ling S, Perez-Polo JR, Ye Y, Bajaj M. PTEN upregulation may explain the development of insulin resistance and type 2 diabetes with high dose statins. Cardiovasc Drugs Ther 2014; 28: [PMID: DOI: / s ] 49 Ghosh-Choudhury N, Mandal CC, Ghosh-Choudhury N, Ghosh Choudhury G. Simvastatin induces derepression of PTEN expression via NFkappaB to inhibit breast cancer cell growth. Cell Signal 2010; 22: [PMID: DOI: / j.cellsig ] 50 Teresi RE, Shaiu CW, Chen CS, Chatterjee VK, Waite KA, Eng C. Increased PTEN expression due to transcriptional activation of PPARgamma by Lovastatin and Rosiglitazone. Int J Cancer 2006; 118: [PMID: DOI: /ijc.21799] 51 Teresi RE, Planchon SM, Waite KA, Eng C. Regulation of the PTEN promoter by statins and SREBP. Hum Mol Genet 2008; 17: [PMID: DOI: /hmg/ddm364] 52 Tu Y, Wan L, Bu L, Zhao D, Dong D, Huang T, Cheng Z, Shen B. MicroRNA-22 downregulation by atorvastatin in a mouse model of cardiac hypertrophy: a new mechanism for antihypertrophic intervention. Cell Physiol Biochem 2013; 31: [PMID: DOI: / ] 53 Musso G, Cassader M, Rosina F, Gambino R. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis of randomised trials. Diabetologia 2012; 55: [PMID: DOI: /s ] 54 Simon TG, King LY, Zheng H, Chung RT. Statin use is associated with a reduced risk of fibrosis progression in chronic hepatitis C. J Hepatol 2015; 62: [PMID: DOI: / j.jhep ] 55 Yang YH, Chen WC, Tsan YT, Chen MJ, Shih WT, Tsai YH, Chen PC. Statin use and the risk of cirrhosis development in patients with hepatitis C virus infection. J Hepatol 2015; 63: [PMID: DOI: /j.jhep ] 56 Butt AA, Yan P, Bonilla H, Abou-Samra AB, Shaikh OS, Simon TG, Chung RT, Rogal SS. Effect of addition of statins to antiviral therapy in hepatitis C virus-infected persons: Results from ERCHIVES. Hepatology 2015; 62: [PMID: DOI: /hep.27835] 57 Sattar N, Preiss D, Murray HM, Welsh P, Buckley BM, de Craen AJ, Seshasai SR, McMurray JJ, Freeman DJ, Jukema JW, Macfarlane PW, Packard CJ, Stott DJ, Westendorp RG, Shepherd J, Davis BR, Pressel SL, Marchioli R, Marfisi RM, Maggioni AP, Tavazzi L, Tognoni G, Kjekshus J, Pedersen TR, Cook TJ, Gotto AM, Clearfield MB, Downs JR, Nakamura H, Ohashi Y, Mizuno K, Ray KK, Ford I. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010; 375: [PMID: DOI: / S (09) ] 58 Wijesekara N, Konrad D, Eweida M, Jefferies C, Liadis N, Giacca A, Crackower M, Suzuki A, Mak TW, Kahn CR, Klip A, Woo M. Muscle-specific Pten deletion protects against insulin resistance and diabetes. Mol Cell Biol 2005; 25: [PMID: DOI: /MCB ] 59 Shearn CT, Smathers RL, Backos DS, Reigan P, Orlicky DJ, Petersen DR. Increased carbonylation of the lipid phosphatase PTEN contributes to Akt2 activation in a murine model of early alcohol-induced steatosis. Free Radic Biol Med 2013; 65: [PMID: DOI: /j.freeradbiomed ] 60 Donohue TM, Osna NA, Trambly CS, Whitaker NP, Thomes PG, Todero SL, Davis JS. Early growth response-1 contributes to steatosis development after acute ethanol administration. Alcohol Clin Exp Res 2012; 36: [PMID: DOI: / j x] 61 Baron V, Adamson ED, Calogero A, Ragona G, Mercola D. The transcription factor Egr1 is a direct regulator of multiple tumor suppressors including TGFbeta1, PTEN, p53, and fibronectin. Cancer Gene Ther 2006; 13: [PMID: DOI: /sj.cgt ] 62 Dahia PL, FitzGerald MG, Zhang X, Marsh DJ, Zheng Z, Pietsch T, von Deimling A, Haluska FG, Haber DA, Eng C. A highly conserved processed PTEN pseudogene is located on chromosome band 9p21. Oncogene 1998; 16: [PMID: DOI: /sj.onc ] P- Reviewer: Fierbinteanu-Braticevici C, Mihaila RG, Wisse E S- Editor: Ma YJ L- Editor: A E- Editor: Ma S 3745 April 14, 2016 Volume 22 Issue 14
60 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Basic Study ORIGINAL ARTICLE S-adenosyl-L-methionine modifies antioxidant-enzymes, glutathione-biosynthesis and methionine adenosyltransferases-1/2 in hepatitis C virus-expressing cells Sonia Amelia Lozano-Sepulveda, Eduardo Bautista-Osorio, Jose Angel Merino-Mascorro, Marta Varela-Rey, Linda Elsa Muñoz-Espinosa, Paula Cordero-Perez, María Luz Martinez-Chantar, Ana Maria Rivas-Estilla Sonia Amelia Lozano-Sepulveda, Eduardo Bautista-Osorio, Jose Angel Merino-Mascorro, Ana Maria Rivas-Estilla, Department of Biochemistry and Molecular Medicine, School of Medicine, Autonomous University of Nuevo Leon, Monterrey, Nuevo Leon 64460, Mexico Marta Varela-Rey, María Luz Martinez-Chantar, Metabolomic Unit, CIC biogune, CIBERehd, Parque Tecnológico de Bizkaia, Derio, Spain Linda Elsa Muñoz-Espinosa, Paula Cordero-Perez, Liver Unit, School of Medicine and Hospital Universitario, Autonomous University of Nuevo Leon, Monterrey, Nuevo Leon 64460, Mexico Author contributions: Lozano-Sepulveda SA performed the majority of experiments, analyzed the data and partially wrote the paper; Bautista-Osorio E, Varela-Rey M, Martinez-Chantar ML and Merino-Mascorro JA performed additional molecular investigations and analyzed data; Muñoz-Espinosa L and Cordero-Perez P partially designed and coordinated the research; Rivas-Estilla AM designed, coordinated the research and wrote the paper. Supported by CONACYT-Mexico, grant register CB to Rivas-Estilla AM. Institutional review board statement: In this study, we performed all experiments in vitro using cell lines and did not include humans or animals; therefore this requirement does not apply. Conflict-of-interest statement: All listed authors in this manuscript do not have financial relationships to disclose. Data sharing statement: We did not include data sharing from other researchers. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Dr. Ana Maria Rivas-Estilla, Department of Biochemistry and Molecular Medicine, School of Medicine, Autonomous University of Nuevo Leon, Francisco I. Madero y Ave. Gonzalitos s/n Col. Mitras Centro, Monterrey, Nuevo Leon 64460, Mexico. amrivas1@yahoo.ca Telephone: Received: December 26, 2015 Peer-review started: December 28, 2015 First decision: January 28, 2016 Revised: February 14, 2016 Accepted: March 1, 2016 Article in press: March 2, 2016 Published online: April 14, 2016 Abstract AIM: To elucidate the mechanism(s) by which S-adenosyl-L-methionine (SAM) decreases hepatitis C virus (HCV) expression. METHODS: We examined the effects of SAM on viral expression using an HCV subgenomic replicon cell culture system. Huh7 HCV-replicon cells were treated with 1 mmol/l SAM for different times (24-72 h), then total RNA and proteins were isolated. cdna was synthesized and real time-pcr was achieved to quantify HCV-RNA, superoxide dismutase 1 and April 14, 2016 Volume 22 Issue 14
61 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression (SOD-1, SOD-2) catalase, thioredoxin 1, methionine adenosyltransferase 1A and 2A (MAT1A, MAT2A) expression, and GAPDH and RPS18 as endogenous genes. Expression of cellular and viral protein was evaluated by western-blot analysis using antibodies vs HCV-NS5A, SOD-1, SOD-2, catalase, thioredoxin-1, MAT1A, MAT2A, GAPDH and actin. Total glutathione levels were measured at different times by Ellman s recycling method (0-24 h). Reactive oxidative species (ROS) levels were quantified by the dichlorofluorescein assay (0-48 h); Pyrrolidin dithiocarbamate (PDTC) was tested as an antioxidant control and H2O2 as a positive oxidant agent. RESULTS: SAM exposition decreased HCV-RNA levels 50%-70% compared to non-treated controls (24-72 h). SAM induced a synergic antiviral effect with standard IFN treatment but it was independent of IFN signaling. In addition, 1 mmol/l SAM exposition did not modify viral RNA stability, but it needs cellular translation machinery in order to decrease HCV expression. Total glutathione levels increased upon SAM treatment in HCV-replicon cells. Transcriptional antioxidant enzyme expression (SOD-1, SOD-2 and thioredoxin-1) was increased at different times but interestingly, there was no significant change in ROS levels upon SAM treatment, contrary to what was detected with PDTC treatment, where an average 40% reduction was observed in exposed cells. There was a turnover from MAT1A/MAT2A, since MAT1A expression was increased (2.5 fold-times at 48 h) and MAT2A was diminished (from 24 h) upon SAM treatment at both the transcriptional and translational level. CONCLUSION: A likely mechanism(s) by which SAM diminish HCV expression could involve modulating antioxidant enzymes, restoring biosynthesis of glutathione and switching MAT1/MAT2 turnover in HCV expressing cells. Key words: Hepatitis C virus; S-adenosyl-L-methionine; Superoxide dismutase 1; Superoxide dismutase 2; replication; Hepatitis C virus-rna; NS5A; Oxidative stress; Antioxidants; viral proteins; reactive oxygen species; Pyrrolidine dithiocarbamate The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: S-adenosyl-L-methionine (SAM) downregulates hepatitis C virus (HCV) expression by unknown mechanisms. We evaluated the effects of SAM on viral expression using an HCV subgenomic replicon cell culture system. We observed that SAM induces a synergic antiviral effect with standard interferon (IFN) treatment independently of IFN signaling pathways; it does not modify viral RNA stability, but it needs cellular translation machinery in order to decrease HCV expression. In addition, results demonstrated that a likely mechanism(s) by which SAM decreases HCV expression could involve modulating antioxidant enzyme systems, restoring biosynthesis of glutathione and switching methionine adenosyltransferase 1 (MAT1)/MAT2 turnover in HCV expressing cells. Lozano-Sepulveda SA, Bautista-Osorio E, Merino-Mascorro JA, Varela-Rey M, Muñoz-Espinosa LE, Cordero-Perez P, Martinez- Chantar ML, Rivas-Estilla AM. S-adenosyl-L-methionine modifies antioxidant-enzymes, glutathione-biosynthesis and methionine adenosyltransferases-1/2 in hepatitis C virusexpressing cells. World J Gastroenterol 2016; 22(14): Available from: URL: v22/i14/3746.htm DOI: i INTRODUCTION Chronic hepatitis C (CHC) is a global burden [1] ; around 3% ( million people) of the total population is infected with hepatitis C virus (HCV) [2] and CHC eventually may lead to cirrhosis and hepatocellular carcinoma (HCC) [3]. In over 70% of cases, the immune response is unable to clear the virus, resulting in viral persistence. Current standard of care is based on the mixed scheme of pegylated interferon 2α (PEG-IFN), ribavirin (RBV) [4] and a protease or a polymerase inhibitor [5]. The mechanisms by which HCV causes cell damage are poorly elucidated and different metabolic pathways have been proposed in its pathogenesis, including the active participation of oxidative stress in chronic HCV infection. A major increases in several markers of oxidative stress are reported in HCV infection, such as inflammation, iron overload and mitochondrial injury, induced by viral proteins [6]. Oxidative stress has been described to be present in CHC patients. To date, reactive oxygen species (ROS) induction has been a subject of study for understanding HCV pathogenesis [7]. Direct measures in liver tissue show that patients with CHC have an increase in ROS [8]. Cells get protection against oxidative damage by natural antioxidant molecules, notably glutathione, and several antioxidant enzymes, such as superoxide dismutases (SOD1 and SOD2), catalase (CAT), glutathione peroxidase (GPx) and thioredoxin 1 (TRX1) [9]. Studies in subjects with chronic HCV infection have found decreased levels of glutathione [10,11] and other antioxidants and enzymatic activity [12-14]. Levent et al [15], published a clinical study in which different oxidative stress markers were measured in CHC patients, showing that plasmatic SOD1 levels had a significant reduction compared with healthy subjects. A reduction in SOD1 and GPx reflects a decrease in liver synthesis and antioxidant power in patients with HCV, and this might be considered an early marker of oxidative stress. At the same time, when markers of oxidative stress were compared in patients infected with HCV, before and after treatment, the levels showed a recovery [15]. However, more data 3747 April 14, 2016 Volume 22 Issue 14
62 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression are needed in order to understand the role of HCV expression in the disturbance of oxidative stress levels in infected cells. Recently, it has been reported that S-adenosyl- L-methionine (SAM), decreases HCV RNA levels; however, the mechanism(s) involved are unknown. SAM is the main precursor of glutathione synthesis. Methionine adenosyltransferase 1A (MAT1A) enzyme is responsible of its biosynthesis in normal liver, but it is replaced by MAT2A in liver regeneration and hepatic carcinoma [16-18]. Based on this, we evaluated the effects of SAM exposition on HCV viral replication and protein expression and analyzed possible mechanisms involved using a hepatoma cell line expressing HCV proteins. Furthermore, the regulation of MAT1A and MAT2A enzymes involved in endogenous SAM synthesis was analyzed. Our findings suggest that SAM is able to diminish HCV expression at least in part through modulation of antioxidant enzymes, biosynthesis of glutathione and switching MAT1A/MAT2A turnover in HCV expressing cells. These findings suggest the possibility that SAM modulation could help to counteract HCV-induced damage. MATERIALS AND METHODS Cell culture and treatments We used a genotype 1b HCV subgenomic Huh7-replicon cell culture system (harboring the subgenomic HCV replicon I389/NS3-3), described previously [19,20]. Huh7- replicon cells were cultured in advanced Dulbecco s modified Eagle s medium (GIBCO-BRL; Grand Island, NY, United States) supplemented with 2% fetal bovine serum, 1% nonessential amino acids, 200 IU of penicillin G and 200 mg of streptomycin/ml at 37. For each experimental condition, cells were plated and 24 h later, were treated either with SAM (1-5 mmol/l), a combined treatment with PEG-IFNα + RBV (double therapy), or 5 µmol/l PDTC (time zero) and then incubated until 72 h. Cell viability was calculated by comparing the different conditions with untreated cells (100% viability). Upon each experimental condition, total RNA and proteins were extracted from the cell cultures and subjected to real-time reverse transcriptase polymerase chain reaction (RT-qPCR) and western blot analysis, respectively. S-(5 -Adenosyl)- L-methionine p-toluenesulfonate SAM) salt was purchased from Sigma (St. Louis MO, United States). RNA extraction Upon each experimental condition, total RNA was isolated from cells using Trizol reagent (Life Technologies, Carlsbad, CA, United States) as described by the manufacturer s specification [21]. Isolated RNA was washed with 75% ethanol and diluted in 30 µl of RNase-free water. Quantitative real-time RT-qPCR for HCV-RNA and mrna of antioxidant enzymes Total RNA was then subjected to RT using a highcapacity complementary DNA (cdna) archive kit (Applied Biosystems, Foster City, CA, United States) as described by the manufacturer s specifications. Two hundred ng of cdna were used to perform realtime PCR for HCV-RNA, antioxidant genes, MAT1A, MAT2A, RPS18 and GAPDH mrna quantification. HCV amplifications were done in triplicate with the following oligonucleotides: HCV-Forward ( nt), 5 -GCGTCTAGCCATGGCGTTA-3 ; HCV-Reverse ( nt), 5 -GGTTCCGCAGACCACTATGG-3 ; and the TaqMan probe ( nt), 5-FAM- CTGCACGACACTCATAC-NFQ-3. For each PCR reaction, 10 µl of TaqMan PCR Master Mix, 1 µl of 20 Assay Mix, and 9 µl of cdna diluted in RNase free-water were used. For cellular genes analyzed, Sybr green chemistry was used for detection, and the following oligonucleotides were used: for SOD-1 gene forward 5 -AGGGCATCATCAATTTCGAG-3, reverse 5 -TGCCTCTCTTCATCCTTTGG-3 ; SOD-2, forward 5 -GGAACGGGGACACTTACAAA-3, reverse 5 -CACCCTCGTGCGAATGATGG-3 ; Thioredoxin-1 f o r w a r d 5 - C TG C TTTTC A G G A A G C C TTG - 3, reverse 5 -TGTTGGCATGCATTTGACTT-3 ; MAT1A f o r ward 5 -A C ATC G G A G TC TG TG G G A G A- 3, reverse 5 -CGGTCTTGCACACTGTCTCA-3 ; MAT2A f o r ward 5 - G G TA G C C TTG G A G C A A C A G T- 3, reverse 5 -CTGGTCTCCAGCACCAATGT-3 ; CAT forward 5 -TAAGACTGACCAGGGCATC-3, reverse 5 -CAAACCTTGGTGAGATCGAA-3 ; Ribosomal-18S (RPS18) forward 5 -TGTGGTGTTGAGGAAAGCAG-3, reverse 5 -AAGTGACGCAGCCCTCTATG-3. For each PCR reaction, 10 µl of SYBR-Green PCR Master Mix, 1 µl of each oligonucleotide 10 µmol/l, and 8 µl of cdna diluted in RNase-free water were added. Conditions for temperature cycling were: setup at 50 for 2 min, then 95 for 10 min, 40 cycles of 95 for 15 s and 60 for 60 s. Data were recorded and plots were generated. GAPDH and RPS18 expression was monitored and used to normalize assays. For GAPDH- RNA expression, we used a GAPDH (20 ) assay (Applied Biosystems, Foster City, CA, United States) as described by the manufacturer s specifications. Protein extraction and immunoblot assay After each treatment, cells were lysed and proteins were extracted and quantified as we described before [22]. Fifty micrograms of protein were resolved by 12% SDS-PAGE and transferred onto PVDF membranes (Amersham Biosciences, Freiburg, Germany). Membranes were incubated with one of the following antibodies: anti-ns5a antibody (Abcam, Cambridge, MA, United States), anti-mat1, anti-mat2, anti-pkr, anti-stat1 (Abcam, Cambridge, MA, United States) 3748 April 14, 2016 Volume 22 Issue 14
.")
63 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression A %cell viability B Time (h) SAM NS5A (56 kda) GAPDH (37 kda) Control SAM 2.5 mmol/l t /h SAM 1 mmol/l SAM 5 mmol/l or anti-actin MAb (MP Biomedicals, Aurora, OH, United States). Upon washing with TBS/Tween, the membranes were exposed to horseradish-peroxidase conjugated anti-mouse IgG, anti-rabbit IgG or anti-goat IgG (Promega, Madison, WI, United States). Detection was made using Western-Blotting Chemiluminescence Luminol Reagent (Santa Cruz Biotech). We performed each experiment in triplicate, and densitometric analysis was done to quantify relative expression of each protein detected by immunoblotting. The ratios of NS5A and actin were quantified with ImageJ 1.46r 2011 software. ANOVA was used to determine statistical differences. The differences were considered significant if p < Total GSH and GSSG To determine oxidative stress levels in Huh7-replicon cells upon SAM treatment, two major indicators were evaluated at different time points and concentrations: glutathione levels and ROS production. The detection of GSH and GSSG was performed using a specific kit (GSH Assay Kit; Ann Arbor, MI, United States). Huh Lane Figure 1 Effect of S-adenosyl-L-methionine in hepatitis C virus expression and cell viability. A: Cell viability in HCV-replicon cells exposed to SAM. Huh7 HCV replicon cells were treated with SAM at indicated concentrations for 24, 48 and 72 h. Cell viability was then determined by MTT assay and the % viability was calculated by comparing the different conditions with untreated cells (100% viability); B: HCV NS5A protein levels in Huh7 HCV replicon cells treated with SAM. Huh7 HCV replicon cells ( cells) were incubated with SAM 1 mmol/l. Cell lysates were prepared, and equal amounts of protein extracts (30 µg) were subjected to immunoblot analysis to detect NS5A. GAPDH was used as a control. SAM: S-adenosyl-L-methionine; HCV: hepatitis C virus. HCV-replicon and parental cells were exposed with 1 mmol/l SAM for 1, 2, 6, 12 and 24 h. Cells were disrupted with freeze and unfreeze cycles. Supernatant was collected for the analysis and stored at -80 until the assay was done. The supernatants were low in protein (< 1 mg/ml) and were devoid of particulates so they were assayed directly without deproteinization, according to the manufacturer indications. GSSG was quantified by derivatizing GSH with 2-vinyl pyridine. The xmark Microplate Absorbance Spectrophotometer (Bio-Rad, Hercules, CA, United States) was used for the absorbance measure using a 415 nm filter. ROS level quantification. Huh7 HCV replicon cells ( cells) were incubated with 1 mmol/l SAM at different time points (0.5, 1, 3, 12, 24 and 48 h). ROS levels were assessed by DCFH-DA assay. Fluorescence was detected at 503 nm and 530 nm, excitation and emission wavelengths respectively, by GloMax -Multi Microplate Multimode Reader (Promega, Fitchburg, WI, United States). Hydrogen peroxide (H2O2, 1 µmol/l) was used as a positive damage control and pyrrolidine dithiocarbamate (PDTC, 5 µmol/l) as antioxidant control. Statistical analysis All variables were evaluated in triplicate and experimental conditions were performed at least three times. All values were scored as means ± SD. Oneway analysis of variance was done to evaluate for differences in means and the t-test was performed for comparisons. In all experiments, if p < 0.05, the differences were considered significant. RESULTS SAM treatment downregulates HCV expression First, cell viability experiments demonstrated that there were no cytotoxic effects of SAM at the concentrations of 2.5 mmol/l or less on HCV-replicon cells as demonstrated by MTT assay (Figure 1A). Also, as we previously reported, there were no cytotoxic effects of PDTC at the concentrations used. Based on this, we evaluated the effect of SAM on HCV-expression in HCV-replicon cells. We incubated cells with 1 mmol/l SAM at three different time points (24, 48 and 72 h), then cells were lysed and total proteins were extracted and subjected to western blot analysis. We observed that SAM dramatically inhibited HCV-NS5A protein levels compared with untreated cells (around 90% inhibition). In addition, this effect was time dependent because we observed a higher viral protein decrease in SAM-treated cells at 72 h post-treatment (Figure 1B). To determine if the effect of SAM on viral replication was due to the cytotoxic effect on treated cells, we evaluated cell viability and total cell count on SAM-treated cells. Figure 1A demonstrates that 3749 April 14, 2016 Volume 22 Issue 14
 - + + - - + + - - + + - PEG-IFN + RBV - - + + - - + + - - + + Time (h) 24 48 72 NS5A protein level (Fold change) 1.0 0.8 b d b d 0.6 0.4 0.2 b d 0.")
64 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression A 1.2 B 1.2 HCV-RNA level (ΔΔCt) b b b d d d 0.0 SAM (1 mmol/l) PEG-IFN + RBV Time (h) NS5A protein level (Fold change) b d b d b d 0.0 SAM (1 mmol/l) PEG-IFN + RBV Time (h) C Time (h) SAM (1 mmol/l) PEG-IFN + RBV STAT1 (87 kda) PKR (62 kda) Actin (42 kda) Lane Figure 2 Synergic antiviral effect of S-adenosyl-L-methionine plus standard interferon treatment. A: Effect of SAM and PEG-IFN + RBV on HCV-RNA levels. Huh7 HCV replicon cells ( cells) were incubated with 1 mmol/l SAM alone or SAM plus PEG-IFN (1000 UI/ml) and RBV (50 µmol/l). Cells were harvested at 24, 48 and 72 h and HCV-RNA levels were quantified by real-time RT-PCR and normalized with GAPDH and RPS18 using delta delta Ct method. Mean results from three independent experiments are shown. b p 0.01 comparison of SAM vs untreated cells; d p 0.01 comparison of SAM + PEG-IFN + RBV vs untreated cells; B: HCV NS5A protein levels in Huh7 HCV replicon cells treated with SAM PEG-IFN + RBV. Huh7 HCV replicon cells ( ) cells were incubated with 1 mmol/l SAM alone or SAM plus PEG-IFN (1000 UI/ml) and RBV (50 µmol/l). Cell lysates were prepared, and equal amounts of protein extracts (40 µg) were subjected to immunoblot analysis to detect NS5A and actin levels. The ratios of NS5A and actin were quantified with ImageJ 1.46r 2011 software, means of three blots are represented in the graphic. b p 0.01 comparison of SAM vs untreated cells; d p 0.01 comparison of SAM + PEG-IFN + RBV vs untreated cells; C: Huh7 HCV replicon cells ( cells) were incubated with 1 mmol/l SAM alone, or SAM plus PEG-IFN (1000 UI/ml) and RBV (50 µmol/l). Cells were harvested at 24, 48 and 72 h and total proteins were obtained. Cell lysates were prepared, and equal amounts of protein extracts (40 µg) were subjected to immunoblot analysis to detect STAT1, PKR and actin levels. SAM: S-adenosyl-L-methionine; HCV: hepatitis C virus; IFN: interferon; RBV: ribavirin. no significant difference in cell number and viability was present among unexposed (100% viability) and exposed cells with 1 to 5 mmol/l SAM concentration (98% and 85%, respectively) and this effect was timedependent. Based on this data, we used 1 mmol/l SAM for subsequent experiments. SAM induces a synergic antiviral effect with standard IFN treatment but it is independent of IFN signaling We further investigated whether the effect of SAM on HCV expression is similar to IFN-standard treatment (PEG-IFN + RBV). We incubated Huh7-replicon cells either with 1 mmol/l SAM, PEG-IFN + RBV or combined treatment, and then cells were harvested at three different time points. Real-time RT-PCR assay showed that viral RNA was downregulated in a time dependent fashion reaching the highest inhibition value at 72 h post-sam treatment in HCV replicon cells (60% of inhibition at 48 h and 75% of inhibition at 72 h, d P < 0.01) (Figure 2A). As we expected PEG-IFN + RBV treatment declined HCV-RNA levels at 24, 48 and 72 h upon treatment (around 80%). Interestingly, combined treatment of SAM + PEG-IFN + RBV showed a maximal inhibition of HCV-RNA at the three times of exposition (around 92% of inhibition at 24, 48 and 72 h, d P < 0.01) (Figure 2A). Taken together, these results demonstrated that SAM possesses a synergic antiviral effect in this replicon cell culture system. Next, we evaluated the effect of these treatments on HCV protein expression. Cell lysates were prepared and subjected to western blot analysis to detect NS5A protein. Results from three immunoblots were 3750 April 14, 2016 Volume 22 Issue 14
65 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression analyzed by densitometry and graphics showed similar results (Figure 2B). Basically, we found that NS5A protein levels were also decreased in a time depended manner. We also observed a synergistic effect of SAM + PEG-IFN + RBV treatment to decrease viral proteins at 24, 48 and 72 h (40%, 60% and 55% respectively) ( d P < 0.01). To investigate if this synergic antiviral effect is mediated by a higher stimulation of IFN signaling by SAM, we examined the STAT1 and PKR protein levels by western blot analysis. We found that 1 mmol/l SAM-treatment does not induce STAT1 and PKR protein expression (Figure 2C, lanes 2, 6 and 10) in Huh7-replicon cells at 24, 48 and 72 h. Contrary to this, it seems that SAM decreases STAT1 protein expression at the three times of exposure (Figure 2C, lanes 2, 6 and 10). On the other hand, immunoblot analysis of protein extracts from IFN + RBV or SAMcombined treated cells clearly showed an increase in PKR and STAT1 proteins (Figure 2C lanes 3, 4, 7, 8, 11 and 12). Together these data suggest that interferon signaling seems not stimulated by SAM exposition and therefore, inhibition of viral replication and protein synthesis by SAM may be independent of IFN-induced status. SAM exposition does not modify viral RNA stability, but it needs cellular translation machinery in order to decrease HCV expression The aforementioned results suggest the possibility that SAM-treatment may either diminish the transcription rate of viral RNA or decrease viral RNA or protein stability in addition of the negative effect on HCV- RNA levels observed before (Figure 2). To investigate this point we next explored whether SAM modifies HCV-RNA levels upon actinomycin D (Act D) and cycloheximide (CHX) treatment. Huh7 HCV-replicon cells were treated either with Act D (to block cellular mrna transcription by RNA polymerase Ⅱ) or CHX (to block the cellular translation rate of proteins) and 2 h later 1 mmol/l SAM was added. Cells were incubated for sixteen hours and then harvested in order to perform HCV-RNA quantification. We found that in Act D-treated cells, the viral RNA level was stabilized and accumulated (it was not degraded), which explains that after 16 h of treatment there was an increase in the basal levels of HCV-RNA (steadystate levels). When cells were treated simultaneously with SAM and Act D, SAM treatment was not able to decrease increased basal levels of viral RNA stabilized by Act D. On the basis of this finding, we can conclude at this point that the reduction on viral RNA mediated by SAM is an independent mechanism that does not involve alterations in its half-life and reduction of HCV- RNA stability (Figure 3A). Moreover, in the cells treated with CHX for the indicated times, we observed that HCV-RNA levels were not affected by blocking translational machinery but upon SAM addition, a slight increase of viral RNA was observed (Figure 3A). Interestingly, when we analyzed the NS5A protein levels upon CHX alone or combined with SAM treatment, we observed that protein levels were slightly decreased at 16, 24 and 36 h upon CHX stimulation compared with control cells (non-treated cells) (Figure 3B). However, when cells were exposed to CHX + SAM, the NS5A protein levels were greater than those observed in cells incubated only with SAM at the same times (Figure 3B). We found that CHX partially reversed the negative effect of SAM on HCV expression (Figure 3B; lane 4, 8 and 12). After a cell is infected by virus, numerous cellular mechanisms are triggered to prevent the virus from completing its viral cycle. Many of these mechanisms depend on the activation and increased synthesis of proteins with specific antiviral activity (as PKR, Mx1, OAS), so when cellular translation is inhibited, the synthesis of these proteins also decreases, then the levels of viral RNA could increase during this period due to the absence of inhibiting replication proteins. Together, these results suggest that cellular translation machinery and protein stability could play a role in the modulation of HCV protein synthesis by SAM in cultured cells. Effect of SAM exposition on oxidative stress markers Cells are protected against oxidative damage by natural antioxidant molecules, notably glutathione, and several antioxidant enzymes. It is reported that one of the biological activities of SAM is as antioxidative agent [23]. However, there is not enough data on whether its antioxidant properties could be implicated in the downregulation of HCV expression. We studied the modulation of oxidative stress markers in the negative regulation of HCV-RNA induced by SAM. First, we were interested in determining whether SAM could influence cellular enzymatic antioxidant systems expression, such as SOD 1 and 2 enzymes, CAT, and TRX1 in order to decrease viral expression. To evaluate this effect, mrnas levels of these enzymes were examined by quantitative real-time RT-PCR in cells expressing HCV-proteins exposed to 1 mmol/l SAM for 0 to 72 h, and then compared to non-treated cells. We observed that transcriptional expression of SOD-1, SOD-2 and TRX1 was upregulated (0.5-fold, 2.5-fold and 2 fold, respectively compared to control) at different times of exposition (24-72 h) in the same cell system (Figure 4A). SAM is the main precursor of glutathione synthesis. Next, we measured the total glutathione levels in HCVreplicon cells treated with 1 mmol/l SAM from 0 to 24 h by using Ellman s recycling method. As we expected, we found that total glutathione levels were increased in treated cells upon 6 h post-treatment (about 80%-60%) compared to control cells without SAM, and then levels began to decrease (Figure 4B). Finally, we measured if these antioxidant mecha April 14, 2016 Volume 22 Issue 14
 - + - + - + Actinomycin D - - + + - - CHX - - - - + + B Time (h) 16 24 36 SAM (1 mmol/l) CHX - + - + - + - + - + - + - - + + - - + + - - + + NS5A (56 kda) GAPDH (37 kda) Lane 1 2 3 4")
66 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression A HCV-RNA (fold change) SAM (1 mmol/l) Actinomycin D CHX B Time (h) SAM (1 mmol/l) CHX NS5A (56 kda) GAPDH (37 kda) Lane Figure 3 Role of actinomycin D and cycloheximide on the antiviral effect of S-adenosyl-L-methionine. A: SAM decreases replicon RNA levels without affecting its stability. Huh7 HCV replicon cells ( cells) were incubated with SAM 1 mmol/l, some cells were treated with actinomycin D (4 µg/ml) or CHX (50 µg/ml) for 2 h, then SAM was added. Cells were harvested 16 h later and HCV-RNA levels were quantified by real-time RT-PCR and normalized with GAPDH using ΔΔCt method. Mean results from three experiments are shown; B: CHX partially reverts the downregulated NS5A protein expression induced by SAM. Huh7 HCV replicon cells ( cells) were incubated with SAM 1 mmol/l, some cells were treated CHX (50 µg/ml) after 4 h of SAM treatment. Cells were harvested at different time points (0-36 h), then total protein was extracted and western blot for NS5A and GAPDH was performed. CHX: cycloheximide; SAM: S-adenosyl-L-methionine; HCV: hepatitis C virus. nisms up-regulated by SAM are enough to counteract the oxidative stress induced in the cells by HCV proteins and then decrease viral expression. Huh7 replicon-cells were incubated with 1 mmol/l SAM at different time points (0 to 48 h) and then ROS levels were assessed by DCFH-DA assay. A potent antioxidant, pyrrolidine dithiocarbamate (PDTC), was used as a control to decrease ROS [24] and H2O2 was used as a positive damage control. Interestingly, we observed that there was no significant variation in ROS levels in both cell types after SAM exposition at all times evaluated, in contrast to the observed with PDTC exposition where an average of 40% reduction was observed ( h) (Figure 4C). Our results suggest that the antiviral activity of SAM could be mediated at least partially by the induction of enzymatic antioxidant systems and total GSH turnover, triggering unknown signaling pathways but with minimal effect on ROS levels. Turnover of MAT1A/MAT2A is induced by SAM treatment in Huh7 replicon-cells In normal liver MAT1A is responsible for SAM biosynthesis, but upon several liver insults it is replaced by MAT2A in liver regeneration and HCC. Huh7 cells are derived from a hepatocarcinoma cell line, then in our experimental setting it was expected that MAT1A levels were downexpressed and MAT2A were major expressed. To further address the mechanisms involved in the SAM-induced downregulation of HCV expression, we evaluated the role of MAT1A and MAT2A enzymes in our cell system expressing HCV proteins. HCV replicon-cells were treated with SAM as mentioned before and then qpcr and western blot assays were performed to evaluate enzyme expression. From our results we observed two complementary phenomena (Figure 5). First, a transcriptional downregulation was observed in both enzymes at 24 h because cells were plenty of SAM, thus they do not need to synthesize it more; but later on we observed a major upregulation of MAT1A-mRNA at 48 h upon treatment (2.8 fold-times), while MAT2AmRNA synthesis was less induced (1.4 fold) (Figure 5A). This turnover from MAT1A /MAT2A at 48 h upon SAM exposition is better represented in figure 5B. Second, there was a translational upregulation of 3752 April 14, 2016 Volume 22 Issue 14
67 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression A c Control SOD1 SOD2 mrna level (ΔΔCt) a e CAT TRX B t /h a Total GSH (fold change) a 0.0 SAM (1 mmol/l) C Time (h) Normalized ROS level h 1 h 3 h 12 h 24 h 48 h SAM (1 mmol/l) PDTC (1 mmol/l) H2O2 (1 mmol/l) Figure 4 Effect of S-adenosyl-L-methionine exposition on oxidative stress markers. A: Effect of SAM on antioxidant enzyme expression. Huh7 HCV replicon cells ( cells) were incubated with 1 mmol/l SAM and then cells were harvested at 24, 48 and 72 h. SOD1, SOD2, catalase and thioredoxin 1 mrna levels were quantified by real-time RT-PCR and normalized with GAPDH and RPS18 using the delta delta Ct method. Mean results from three independent experiments are shown. a p 0.05 comparison of SOD1 expression in cells treated with SAM vs untreated cells; c p 0.05, SOD2 expression of SAM treated cells vs untreated; and e p 0.05, TRX1 expression of SAM treated cells vs untreated; B: Total glutathione amount in HCV-replicon cells treated with SAM. Huh7 HCV-replicon cells ( cells) were treated with 1 mmol/l SAM. Total glutathione level was evaluated at different times by Ellman s recycling method (0-24 h). Mean results from three independent experiments are shown; C: Effect of SAM in ROS levels. HCV replicon-containing cells ( cells) were incubated with 1 mmol/l SAM at different time points (0.5, 1, 3, 12, 24 and 48 h). ROS levels were assessed by DCFH-DA assay. Fluorescence was measured at 503 nm and 530 nm, excitation and emission wavelengths, respectively. Hydrogen peroxide (1 µmol/l H2O2) was used as a positive damage control and pyrrolidine dithiocarbamate (5 µmol/l PDTC) as antioxidant control. SAM: S-adenosyl-L-methionine; HCV: hepatitis C virus; SOD: superoxide dismutase; ROS: Reactive oxidative species; PDTC: Pyrrolidin dithiocarbamate April 14, 2016 Volume 22 Issue 14
 MATI (44 kda) MATII (44 kda) Actin (42 kda) Control MAT1A MAT2A 24 a - + MAT1A MAT1A protein since 24 to 72 h upon SAM exposition.")
68 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression A mrna level (ΔΔCt) SAM (1 mmol/l) Time (h) B 2.5 C MAT1A/MAT2A ratio Time (h) SAM (1 mmol/l) MATI (44 kda) MATII (44 kda) Actin (42 kda) Control MAT1A MAT2A 24 a - + MAT1A MAT1A protein since 24 to 72 h upon SAM exposition. Contrary to these, MAT2A protein levels were decreased upon SAM exposition since 24 to 72 h compared with untreated cells (Figure 5C). a MAT2A t /h Lane Figure 5 Effect of S-adenosyl-L-methionine on methionine adenosyltransferase 1/2 turnover. A: Assesment of MAT-mRNA: Huh7 HCV replicon cells ( cells) were incubated with 1 mmol/l SAM and then cells were harvested at 24, 48 and 72 h and MAT1 and MAT2 mrna levels were quantified by real-time RT-PCR and normalized with GAPDH and RPS18 using delta delta Ct method. Mean results from three independent experiments are shown. a p 0.05 comparison of SAM vs untreated cells; B: MAT1A/MAT2A Turnover: Measured MAT1A/MAT2A expression represented as a total; C: MAT1 and MAT2 protein expression: Huh7 HCV replicon cells ( cells) were incubated with SAM 1 mmol/l. Cells were harvested at 24, 48 and 72 h and total proteins were obtained. Cell lysates were prepared, and equal amounts of protein extracts (40 µg) were subjected to immunoblot analysis to detect MAT1, MAT2 and actin levels. SAM: S-adenosyl-L-methionine; HCV: hepatitis C virus; MAT: methionine adenosyltransferase. DISCUSSION Recently it has been reported that SAM treatment improves early virological response in CHC patients with previous nonresponse treated with PEG-IFN + RBV [25]. In this study we demonstrated that SAM alone has the capacity to downregulate transcriptional and translational HCV expression in a hepatoma cell line expressing HCV viral proteins. In addition, there are in vivo and in vitro experiments reporting that SAM could enhance the antiviral effect of IFN, based on that SAM might be related to an early viral response. Our findings reinforce partially the data presented by Feld et al [26] showing that SAM possesses antiviral action against HCV. In Feld s report the effect in vitro of the addition of SAM on viral clearance was not apparent until 72 h after interferon treatment, while in our experiments we found a clear decline of HCV expression since 24 h upon SAM alone or combined (SAM + IFN + RBV) exposition (Figures 1B and 2) and that could be due to the higher dose used in our experiments (1 mmol/l SAM). Contrary to results found by Feld et al [26], our results reveal that SAM possesses an early synergic antiviral effect when it is added to IFN + RBV treatment in HCV replicon cell culture system. On the other hand, in our study the addition of SAM to PEG-IFNα and RBV does not improve the expression of ISGs genes. We observed that PKR and STAT1 protein levels were stimulated in the presence of IFNα + RBV but not upon SAM exposition, suggesting that HCV downregulation mediated by SAM is independent of IFNα stimulated pathways. These findings could have clinical application in terms of understanding the pathophysiology of the disease. SAM is a pleiotropic molecule involved in multiple cellular reactions, participating directly in the following three types of reactions: transmethylation, transsulfuration and aminopropylation [27]. SAM is also involved in many other biochemical reactions in the human body, serving as a key metabolite that regulates hepatocyte growth, death and differentiation [28,29]. Based on this, we explored if alteration of RNA stability or basal levels are triggered by SAM or its metabolites. Based on our finding, we can suggest that the decrease in viral RNA mediated by SAM is due to an independent mechanism that does not involve alterations in its halflife and reduction of HCV-RNA stability (Figure 3A). However, SAM needs a cellular protein translation process to subsequently decrease the expression of viral proteins (Figure 3B). It has been well established that SAM is the main methyl donor in methyltransferase reactions and that SAM supplementation restores hepatic glutathione deposits, which is a well-known anti-oxidant important for prevention of liver injury. To investigate the possible mechanism(s) responsible for the SAM anti-hcv observed effect we examined antioxidant enzyme RNA levels and GSH/GSSG ratio. Previously we have 3754 April 14, 2016 Volume 22 Issue 14
69 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression reported that SOD-1, CAT and GPX enzymes expression were already induced in Huh7 replicon cells while it was almost undetectable in parental cells [30]. In this study we found that SAM up-regulated SOD1, SOD2, and thioredoxin-1 expression; induced total glutathione levels, and decreased HCV-RNA levels (Figure 4A and B) but without modification of ROS levels in Huh7 HCV replicon cells. These findings are difficult to explain because we expected ROS levels could decrease upon antioxidants enzyme and GSH/GSSG were upregulated. There are some explanations for the divergent results. One explanation could be that the site of major expression of these enzymes and turnover ratio is the cytoplasm; and as we previously reported, ROS induced by HCV proteins are mainly produced in the mitochondria [30]. Another plausible explanation is that antioxidant enzymes are triggering different signaling pathways not affecting ROS amount but decreasing viral proteins. It is possible that additional immediate-early genes are also directly affected by SOD1, SOD2 or TRX and then also affects downstream events. Furthermore, oxidants/antioxidants may have different effects on other steps of the HCV life cycle. The possibility of considering SAM as a modulator of oxidative stress levels is not new. Recent evidence from Brown et al [23] have demonstrated that an overdose of acetaminophen induces oxidative stress in the whole liver and mitochondrial subcellular fractions which in turn increases cellular levels of ROS and reactive nitrogen species and induces GSH depletion as a critical early events in acetaminophen hepatotoxicity. In cells treated with SAM, they found that acetaminophen hepatotoxicity was blocked by SAM treatment [23]. These data suggest that the antioxidant status was compromised with several important components of the antioxidant defense mechanism being significantly decreased or increased in HCV-infected cells. These findings provide new clues to further explain the mechanism(s) that indirectly suppressed HCV replication; however, the mechanism(s) still are poorly defined and additional approaches should be designed. The molecular mechanism of HCV pathogenesis remains unclear but it is well known that both viral and host factors contribute to disease outcome. MAT is an essential cellular enzyme that catalyzes the formation of SAM. In mammals, two genes (MAT1A and MAT2A) encode homologous MAT catalytic subunits which are differentially expressed among different tissue [16]. MAT1A encodes for α1 that forms dimer (MATIII) and tetramer (MATI) that are predominantly present in liver parenchymal cells; while MAT2A encoding the α2 catalytic subunit of the MATII isoenzyme that is expressed in all other tissues. In patients with chronic liver disease there is a decrease of SAM biosynthesis exacerbating liver injury, and then exogenous supplementation might represent a useful therapy [17,31,32]. However, the effectiveness of SAM treatment in chronic liver disease has not been adequately studied. Results found in this study suggest that a possible mechanism by which SAM decreases HCV expression could involve an additive effect between modulation of antioxidant enzyme systems, glutathione restore levels (GSH/GSSG) and switching MAT2A/MAT1A turnover in treated cells, because all these molecules participate in cell surviving pathways. In addition, Feld et al [26] found that STAT1, a transcription factor responsible for antiviral/ifn signaling activation, was methylated in cells treated with SAM, so, in that way, SAM could be available to translocate to the nucleus and do its function. Together these results provide new clues to explain the mechanism(s) involved in the antiviral effect of SAM against HCV. In addition, a fine balance of the MAT1A/MAT2A ratio induced by SAM should play a role in HCV replication and in the modulation of antioxidant enzymes. Therefore, if SAM can modify oxidative stress systems, gluthatione restoring and MAT1A/2A cell signaling pathways, these activities can provide hepatocytes with the capacity to counteract the damage induced by HCV infection. ACKNOWLEDGMENTS We thank Sergio Lozano-Rodriguez, MD (UANL) for his careful language assistance in the manuscript. COMMENTS Background S-adenosyl-L-methionine (SAM) is a pleiotropic molecule that is involved in multiple cellular reactions, participating directly in the following three types of reactions: transmethylation, trans-sulfuration and aminopropylation. SAM is also involved in many other biochemical reactions in the human body, serving as a key metabolite that regulates hepatocyte growth, death and differentiation. Research frontiers It has been reported that SAM treatment improves early virological response in chronic hepatitis C subjects with previous nonresponse treated with PEG- IFN + RBV, while in vitro decreases the levels of hepatitis C virus (HCV) RNA, however the implicated mechanisms are unknown. Innovations and breakthroughs Results from this study suggest that SAM is able to diminish HCV expression at least in part through modulation of antioxidant enzymes, biosynthesis of glutathione and switching methionine adenosyltransferase 1A (MAT1A)/MAT2A turnover in HCV expressing cells. Applications These findings suggest the possibility that SAM modulation could help to counteract the HCV-induced damage. Terminology HCV infection is a major global health issue, with an estimated 3% of the world s populations being chronically infected. HCV is a noncytophatic hepatotropic member of the Flaviviridae that causes acute and chronic hepatitis, and hepatocellular carcinoma. It has been shown that HCV modifies antioxidant defense mechanisms yielding a cellular oxidative imbalance and further cell death. Peer-review The authors investigated the antiviral effect of SAM with a HCV subgenomic replicon cell culture system. It s a well written paper with clear hypothesis, the 3755 April 14, 2016 Volume 22 Issue 14
70 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression data is solid and well presented. REFERENCES 1 Lavanchy D. The global burden of hepatitis C. Liver Int 2009; 29 Suppl 1: [PMID: DOI: /j x] 2 Hepatitis C--global prevalence (update). Wkly Epidemiol Rec 1999; 74: [PMID: ] 3 Burra P. Hepatitis C. Semin Liver Dis 2009; 29: [PMID: DOI: /s ] 4 Fried MW, Shiffman ML, Reddy KR, Smith C, Marinos G, Gonçales FL, Häussinger D, Diago M, Carosi G, Dhumeaux D, Craxi A, Lin A, Hoffman J, Yu J. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med 2002; 347: [PMID: DOI: /NEJMoa020047] 5 Barnard RJ, Howe JA, Ogert RA, Zeuzem S, Poordad F, Gordon SC, Ralston R, Tong X, Sniukiene V, Strizki J, Ryan D, Long J, Qiu P, Brass CA, Albrecht J, Burroughs M, Vuocolo S, Hazuda DJ. Analysis of boceprevir resistance associated amino acid variants (RAVs) in two phase 3 boceprevir clinical studies. Virology 2013; 444: [PMID: DOI: /j.virol ] 6 Ivanov AV, Bartosch B, Smirnova OA, Isaguliants MG, Kochetkov SN. HCV and oxidative stress in the liver. Viruses 2013; 5: [PMID: DOI: /v ] 7 Manns MP, McHutchison JG, Gordon SC, Rustgi VK, Shiffman M, Reindollar R, Goodman ZD, Koury K, Ling M, Albrecht JK. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised trial. Lancet 2001; 358: [PMID: DOI: /S (01) ] 8 Ryter SW, Kim HP, Hoetzel A, Park JW, Nakahira K, Wang X, Choi AM. Mechanisms of cell death in oxidative stress. Antioxid Redox Signal 2007; 9: [PMID: DOI: / ars ] 9 Vendemiale G, Grattagliano I, Portincasa P, Serviddio G, Palasciamo G, Altomare E. Oxidative stress in symptom-free HCV carriers: relation with ALT flare-up. Eur J Clin Invest 2001; 31: [PMID: DOI: /j x] 10 Yuan L, Kaplowitz N. Glutathione in liver diseases and hepatotoxicity. Mol Aspects Med 2009; 30: [PMID: DOI: /j.mam ] 11 Swietek K, Juszczyk J. Reduced glutathione concentration in erythrocytes of patients with acute and chronic viral hepatitis. J Viral Hepat 1997; 4: [PMID: DOI: / j tb00217.x] 12 Look MP, Gerard A, Rao GS, Sudhop T, Fischer HP, Sauerbruch T, Spengler U. Interferon/antioxidant combination therapy for chronic hepatitis C--a controlled pilot trial. Antiviral Res 1999; 43: [PMID: DOI: /S (99) ] 13 Venturini D, Simão AN, Barbosa DS, Lavado EL, Narciso VE, Dichi I, Dichi JB. Increased oxidative stress, decreased total antioxidant capacity, and iron overload in untreated patients with chronic hepatitis C. Dig Dis Sci 2010; 55: [PMID: DOI: /s ] 14 Shimoda-Matsubayashi S, Matsumine H, Kobayashi T, Nakagawa-Hattori Y, Shimizu Y, Mizuno Y. Structural dimorphism in the mitochondrial targeting sequence in the human manganese superoxide dismutase gene. A predictive evidence for conformational change to influence mitochondrial transport and a study of allelic association in Parkinson s disease. Biochem Biophys Res Commun 1996; 226: [PMID: DOI: / bbrc ] 15 Levent G, Ali A, Ahmet A, Polat EC, Aytaç C, Ayşe E, Ahmet S. Oxidative stress and antioxidant defense in patients with chronic hepatitis C patients before and after pegylated interferon alfa-2b plus ribavirin therapy. J Transl Med 2006; 4: 25 [PMID: DOI: / ] 16 Kotb M, Mudd SH, Mato JM, Geller AM, Kredich NM, Chou JY, Cantoni GL. Consensus nomenclature for the mammalian methionine adenosyltransferase genes and gene products. Trends Genet 1997; 13: [PMID: DOI: /S (97) ] 17 Horikawa S, Tsukada K. Molecular cloning and developmental expression of a human kidney S-adenosylmethionine synthetase. FEBS Lett 1992; 312: [PMID: DOI: / (92)81405-B] 18 Alvarez L, Corrales F, Martín-Duce A, Mato JM. Characterization of a full-length cdna encoding human liver S-adenosylmethionine synthetase: tissue-specific gene expression and mrna levels in hepatopathies. Biochem J 1993; 293 (Pt 2): [PMID: DOI: /bj ] 19 Lohmann V, Körner F, Koch J, Herian U, Theilmann L, Bartenschlager R. Replication of subgenomic hepatitis C virus RNAs in a hepatoma cell line. Science 1999; 285: [PMID: DOI: /science ] 20 Trujillo-Murillo K, Rincón-Sánchez AR, Martínez-Rodríguez H, Bosques-Padilla F, Ramos-Jiménez J, Barrera-Saldaña HA, Rojkind M, Rivas-Estilla AM. Acetylsalicylic acid inhibits hepatitis C virus RNA and protein expression through cyclooxygenase 2 signaling pathways. Hepatology 2008; 47: [PMID: DOI: /hep.22215] 21 Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal Biochem 1987; 162: [PMID: DOI: / abio ] 22 Rivas-Estilla AM, Svitkin Y, Lopez Lastra M, Hatzoglou M, Sherker A, Koromilas AE. PKR-dependent mechanisms of gene expression from a subgenomic hepatitis C virus clone. J Virol 2002; 76: [PMID: DOI: /JVI ] 23 Brown JM, Kuhlman C, Terneus MV, Labenski MT, Lamyaithong AB, Ball JG, Lau SS, Valentovic MA. S-adenosyl-l-methionine protection of acetaminophen mediated oxidative stress and identification of hepatic 4-hydroxynonenal protein adducts by mass spectrometry. Toxicol Appl Pharmacol 2014; 281: [PMID: DOI: /j.taap ] 24 Wild AC, Mulcahy RT. Pyrrolidine dithiocarbamate up-regulates the expression of the genes encoding the catalytic and regulatory subunits of gamma-glutamylcysteine synthetase and increases intracellular glutathione levels. Biochem J 1999; 338 (Pt 3): [PMID: ] 25 Filipowicz M, Bernsmeier C, Terracciano L, Duong FH, Heim MH. S-adenosyl-methionine and betaine improve early virological response in chronic hepatitis C patients with previous nonresponse. PLoS One 2010; 5: e15492 [PMID: DOI: /journal. pone ] 26 Feld JJ, Modi AA, El-Diwany R, Rotman Y, Thomas E, Ahlenstiel G, Titerence R, Koh C, Cherepanov V, Heller T, Ghany MG, Park Y, Hoofnagle JH, Liang TJ. S-adenosyl methionine improves early viral responses and interferon-stimulated gene induction in hepatitis C nonresponders. Gastroenterology 2011; 140: [PMID: DOI: /j.gastro ] 27 Lu SC. S-Adenosylmethionine. Int J Biochem Cell Biol 2000; 32: [PMID: DOI: /S (99) ] 28 Anstee QM, Day CP. S-adenosylmethionine (SAMe) therapy in liver disease: a review of current evidence and clinical utility. J Hepatol 2012; 57: [PMID: DOI: /j.jhep ] 29 Mato JM, Lu SC. Role of S-adenosyl-L-methionine in liver health and injury. Hepatology 2007; 45: [PMID: DOI: /hep.21650] 30 Rivas-Estilla AM, Bryan-Marrugo OL, Trujillo-Murillo K, Pérez-Ibave D, Charles-Niño C, Pedroza-Roldan C, Ríos-Ibarra C, Ramírez-Valles E, Ortiz-López R, Islas-Carbajal MC, Nieto N, Rincón-Sánchez AR. Cu/Zn superoxide dismutase (SOD1) induction is implicated in the antioxidative and antiviral activity of acetylsalicylic acid in HCV-expressing cells. Am J Physiol Gastrointest Liver Physiol 2012; 302: G1264-G1273 [PMID: DOI: /ajpgi ] 31 Horikawa S, Ozasa H, Ito K, Katsuyama I, Tsukada K, Sugiyama T. Expression of S-adenosylmethionine synthetase isozyme genes in regenerating rat liver after partial hepatectomy. Biochem Mol Biol 3756 April 14, 2016 Volume 22 Issue 14
71 Lozano-Sepulveda SA et al. SAM decreases HCV-RNA expression Int 1996; 40: [PMID: DOI: / ] 32 Avila MA, Berasain C, Torres L, Martín-Duce A, Corrales FJ, Yang H, Prieto J, Lu SC, Caballería J, Rodés J, Mato JM. Reduced mrna abundance of the main enzymes involved in methionine metabolism in human liver cirrhosis and hepatocellular carcinoma. J Hepatol 2000; 33: [PMID: DOI: / S (00) ] P- Reviewer: Cao GW, Le MD S- Editor: Gong ZM L- Editor: A E- Editor: Ma S 3757 April 14, 2016 Volume 22 Issue 14
72 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Basic Study ORIGINAL ARTICLE Evaluation of therapeutic effectiveness of 131 I-antiEGFR-BSA-PCL in a mouse model of colorectal cancer Wei Li, Yan-hui Ji, Cheng-xia Li, Zhong-yun Liu, Ning Li, Lei Fang, Jin Chang, Jian Tan Wei Li, Yan-hui Ji, Cheng-xia Li, Ning Li, Jian Tan, Department of Nuclear Medicine, Tianjin Medical University General Hospital, Tianjin , China Zhong-yun Liu, Yantai Institute of Coastal Zone Research, Chinese Academy of Sciences, Yantai , Shandong Province, China Lei Fang, Jin Chang, Institute of Nanobiotechnology, School of Materials Science and Engineering, Tianjin Key Laboratory of Composites and Functional Materials, Tianjin University, Tianjin , China Author contributions: Li W and Ji Yh have contributed equally to this work, and they substantially contributed to the conception and design of the study and the acquisition of the data; Li Cx, Liu Zy, Li N, Fang L, Chang J and Tan J analyzed and interpreted the data; Li W and Ji Yh drafted the article, made critical revisions related to the intellectual content of the manuscript, and approved the final version of the article to be published. Supported by the National Natural Science Foundation of China, No (to Li W); and the National Key Clinical Specialty Project. Institutional animal care and use committee statement: This study was performed in accordance with the guidelines of the National Institutes of Health Guide for the Care and Use of Laboratory Animals and was approved by the Animal Care and Use Committee of Tianjin Medical University. Conflict-of-interest statement: To the best of our knowledge, no conflict of interest exists. Data sharing statement: The technical appendix, statistical code, and dataset are available from the corresponding author at (tanpost@163.com). Participants gave informed consent for data sharing. The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are mentioned in the paper. No additional data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Jian Tan, MD, Professor of Medicine, Chief, Department of Nuclear Medicine, Tianjin Medical University General Hospital, Anshan Road 154, Heping District, Tianjin , China. tanpost@163.com Telephone: Received: August 28, 2015 Peer-review started: September 1, 2015 First decision: September 29, 2015 Revised: November 2, 2015 Accepted: January 17, 2016 Article in press: January 19, 2016 Published online: April 14, 2016 Abstract AIM: to investigate the biological effects of internal irradiation, and the therapeutic effectiveness was assessed of 131 I-labeled anti-epidermal growth factor receptor (EGFR) liposomes, derived from cetuximab, when used as a tumor-targeting carrier in a colorectal cancer mouse model. METHODS: We described the liposomes and characterized their EGFR-targeted binding and cellular uptake in EGFR-overexpressing LS180 colorectal cancer cells. After intra-tumor injections of 74 MBq (740 MBq/ml) 131 I-antiEGFR-BSA-PCL, we investigated the biological effects of internal irradiation and the therapeutic efficacy of 131 I-antiEGFR-BSA-PCL on colorectal cancer in a male BALB/c mouse model. Tumor size, body weight, histopathology, and SPECT imaging were monitored for 33 d post-therapy April 14, 2016 Volume 22 Issue 14
73 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer RESULTS: The rapid radioiodine uptake of 131 I-anti- EGFR-BSA-PCL and 131 I-BSA-PCL reached maximum levels at 4 h after incubation, and the 131 I uptake of 131 I-antiEGFR-BSA-PCL was higher than that of 131 I-BSA- PCL in vitro. The 131 I tissue distribution assay revealed that 131 I-antiEGFR-BSA-PCL was markedly taken up by the tumor. Furthermore, a tissue distribution assay revealed that 131 I-antiEGFR-BSA-PCL was markedly taken up by the tumor and reached its maximal uptake value of 21.0 ± 1.01 %ID/g (%ID/g is the percentage injected dose per gram of tissue) at 72 h following therapy; the drug concentration in the tumor was higher than that in the liver, heart, colon, or spleen. Tumor size measurements showed that tumor development was significantly inhibited by treatments with 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL. The volume of tumor increased, and treatment rate with 131 I-antiEGFR-BSA-PCL was 124% ± 7%, lower than that with 131 I-BSA-PCL (127% ± 9%), 131 I (143% ± 7%), and normal saline (146% ± 10%). The percentage losses in original body weights were 39% ± 3%, 41% ± 4%, 49% ± 5%, and 55% ± 13%, respectively. The best survival and cure rates were obtained in the group treated with 131 I-antiEGFR-BSA-PCL. The animals injected with 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL showed more uniform focused liposome distribution within the tumor area. CONCLUSION: This study demonstrated the potential beneficial application of 131 I-antiEGFR-BSA-PCL for treating colorectal cancer. 131 I-antiEGFR-BSA-PCL suppressed the development of xenografted colorectal cancer in nude mice, thereby providing a novel candidate for receptor-mediated targeted radiotherapy. Key words: radioiodine therapy; colorectal cancer; liposome; epidermal growth factor receptor; mouse The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: This paper describes liposomes that were assessed for EGFR-targeted binding and cellular uptake in EGFR-overexpressing LS180 colorectal cancer cells and a mouse model of colorectal cancer. Anti-EGFR and non-targeted liposomes were labeled with 131 I using the chloramine-t method. The time-dependent cellular uptake of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL demonstrated the slow-release effects of nanoparticles. The results of confocal microscopic analysis revealed the significant uptake of antiegfr-bsa-pcl in LS180 cells. This study also investigated the biological effects of internal irradiation and the therapeutic efficacy of 131 I-antiEGFR-BSA-PCL on colorectal cancer in a BALB/c mouse model. To address this issue, tumor size, body weight, histopathology, and SPECT imaging were monitored for 33 d post-therapy. The 131 I-antiEGFR- BSA-PCL was demonstrated to be superior in regard to cellular binding and uptake compared with control BSA- PCL in the mouse model. Li W, Ji Yh, Li Cx, Liu Zy, Li N, Fang L, Chang J, Tan J. Evaluation of therapeutic effectiveness of 131 I-antiEGFR- BSA-PCL in a mouse model of colorectal cancer. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Cancer is a major threat to public health in the 21 st century and one of the leading causes of death worldwide. However, the mechanisms of carcinogenesis, cancer invasion, and metastasis remain unclear [1]. Colorectal cancer is the third most common cancer worldwide. Approximately 25% of patients with colorectal cancer present with overt metastatic disease; metastatic disease develops in 40% to 50% of newly diagnosed patients [2]. The clinical need for image-based detection and monitoring for effective therapeutic management to reduce the mortality caused by this disease has not been met to date. Therefore, novel strategies and treatment concepts are needed, particularly because conventional cancer therapies, such as external radiation and chemotherapy, have problems such as poor specificity. These conventional therapies often cause dose-limiting side effects and inhibit the possibility of curative treatments. Nanomedicine has exploited the possibility of designing tumor-targeted nanocarriers that can deliver radionuclide payloads in a site- or molecule-selective manner based on their magnetic properties, thereby improving the effectiveness and safety of cancer molecular imaging and therapies. Many studies have proven the feasibility of the use of targeted nanoparticle probes. Nanotechnology can lead to fundamental changes and improve the current understanding of biological processes in health and disease as well as enable novel diagnostics and therapeutics for treating cancer; consequently, advances made on the basis of nanotechnology could lead to progress in healthcare [3]. Targeted drug delivery systems, such as passive and active targeting nanoparticles or nanocarriers, have been developed to improve the biodistribution, pharmacological, therapeutic, and toxic properties of chemical agents used in cancer diagnostics and therapeutics [4]. The abundant expression and signal amplification properties of these targets are mandatory for successful receptor-targeted tumor imaging and for their subsequent clinical translation [5]. The epidermal growth factor receptor (EGFR) is a transmembrane receptor belonging to the ErbB family of receptors; the EGFR family includes four transmembrane receptors, namely, EGFR, HER2, HER3, and HER4 [6]. EGFR is a cell surface receptor that plays a key role in signaling pathways, and such pathways regulate cell proliferation, angiogenesis, and tumor metastasis [7,8]. Previous studies reported that EGFR is widely overexpressed 3759 April 14, 2016 Volume 22 Issue 14
74 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer in several tumor types, including breast cancer, melanoma, brain glioblastoma, non-small cell lung cancer [9], and colorectal cancer [10] ; thus, EGFR is an attractive candidate for anti-cancer therapy. Several radionuclides have been surface-bioconjugated or after-loaded in nanoparticles to improve their effectiveness and reduce the toxicity of cancer imaging and therapies in preclinical and clinical studies. In the broad spectrum of available radionuclides, beta emitters such as 90 Y, 131 I, and 177 Lu are the most commonly used for targeted therapies [11]. 131 I provides imaging feasibility and beta-emitting therapeutic effects [12]. The application of nanotechnology for the diagnosis and treatment of colorectal cancer has the potential to improve conventional methods as well as help with the development of novel approaches for detection and therapy [13]. In the present study, 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL were successfully synthesized. These liposomes were characterized for cellular uptake, time-dependent uptake of 131 I by LS180 cells in vitro, therapeutic efficacy, histopathology, tissue distribution, and SPECT imaging in an LS180 xenografted nude mouse model. MATERIALS AND METHODS Materials The following reagents and materials used in this study were obtained: Minimum Essential Medium Eagles with Earle s Balanced Salts (MEM-EBSS; Gibco), fetal bovine serum (FBS; Gibco), rabbit polyclonal anti-human epidermal growth factor receptor antibody (Abcam, ab2430), 5 mg/ml monoclonal antibody (MERCK Inc., C225; cetuximab), and PV-6000 Polymer Detection System (ZSGB-BIO Co.). Cell line The colorectal cancer cell line LS180 was purchased from the Cell Resource Center, Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences/Peking Union Medical College (Beijing, China). The cells were maintained in MEM-EBSS medium supplemented with 10% FBS and 1% penicillin/streptomycin. The LS180 cells were grown at 37 in a humidified incubator with a mixture of 95% air and 5% CO2. Preparation of nanoparticles The cetuximab-decorated, BSA-PCL-conjugated antiegfr-bsa-pcl and BSA-PCL liposomes were synthesized by the researchers from the Department of Polymer Materials Science and Engineering of Tianjin University [14]. The antiegfr-bsa-pcl and BSA- PCL liposomes were labeled with 131 I (Beijing Atomic Hi-tech Co., Ltd.) via the chloramine T method. A detailed description and biological characterization of the compounds are presented by Ickenstein et al [15]. The labeling rate and the radiochemical purity of 131 I-labeled nanoparticles were determined by thin layer chromatography. Liposomal targeting in EGFR-overexpressing LS180 cells The cellular binding and uptake of the antiegfr- BSA-PCL and BSA-PCL liposomes were evaluated by confocal microscopy in LS180 cells. The antiegfr- BSA-PCL and BSA-PCL liposomes were first labeled by fluorescein isothiocyanate (FITC), then were added at a concentration of 1 mg/10 6 cells. The cell cultures were then incubated for 4 h at 37. After incubation, cells were washed thrice with PBS, fixed with 4% paraformaldehyde, and analyzed by confocal microscopy (laser scanning confocal microscope, Olympus FV1000; Japan). Time-dependent cellular uptake of 131 I-antiEGFR-BSA- PCL and 131 I-BSA-PCL To evaluate the time-dependent cellular uptake of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL, approximately cells per well were seeded in 96-well plates and cultured with 0.37 MBq/mL to 3.7 MBq/mL 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL for 4 h. The medium was completely removed before the cells were washed and lysed twice with ice-cold PBS. Subsequently, 200 μl of DMEM containing 10% FBS was added into each well. The cells were counted every 2 h until 24 h of incubation. Radioactivity was measured with a γ counter (LKB gamma 1261; LKB Instruments, Waverley, Australia) to calculate the counts per minute (CPM) after 24 h. All of these experiments were performed in triplicate. Animal model Experimental subjects were four-week old BALB/c female nude mice weighing 9 g to 11 g. These mice were purchased from the Beijing Experimental Animal Center of Peking Union Medical, China. Mice were kept under specific pathogen-free conditions, with a constant temperature of 25 to 27 and a constant humidity of 45% to 50% in the Laboratory Animal Center of the Tianjin Medical University, China. Animal experimentation guidelines were followed according to the regulations of Swiss veterinary law. The LS180 tumor cells, with approximately cells per 50 μl, were subcutaneously injected into the right flank of the mice. According to the principle of the human thyroid perchlorate discharge test, 0.05 mg/ml sodium perchlorate was added to the drinking water of all mice for 1 d before the experiment (approximately 21 d after tumor inoculation) to reduce the exposure of their thyroids to unwanted radiation and imaging. The growth curve experiment was terminated at 54 d after tumor inoculation, and all the mice were sacrificed. When tumor volume reached an average size of 1.0 cm 3, mice were randomly divided into four experimental groups, which were subjected to 3760 April 14, 2016 Volume 22 Issue 14
75 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer an intra-tumor injection of 74 MBq (740 MBq/ml) 131 I-antiEGFR-BSA-PCL, 131 I-BSA-PCL, 131 I, or an equivalent volume of normal saline (except in the SPECT imaging experiment). Tissue distribution of 131 I, 131 I-antiEGFR-BSA-PCL, and 131 I-BSA-PCL The mice bearing human colorectal cancer were used for the biodistribution study at day 21 after tumor inoculation. The mice in each group were sacrificed at 4, 24, and 72 h post-injection of drugs, respectively. The heart, spleen, liver, colon, and tumor samples were collected for weighing and for radioactivity measurements with a γ counter (LKB gamma 1261; LKB Instruments). %ID/g represents the percentage injected dose per gram of tissue. %ID/g was determined by the percentage of radioactivity contained within each gram of tissue compared to the total radioactivity injected into the body [16,17]. Meanwhile, the remaining spleen, liver, and tumor tissues were collected to study the histopathology of each group. Therapeutic efficacy studies Toxicity was monitored by measuring the body weight and tumor volume. During the course of treatment, the animal body weight and in vivo tumor growth were measured at day 21 after tumor cell inoculation. Mice were checked for survival every day; their body weight and tumor volume were measured every 3 d until the end of the study. The growth curve experiment was terminated at 54 d after tumor inoculation, and all mice were then sacrificed. After treatment, the length, width, and height of the tumors were measured with calipers once every 3 d. Tumor volume was calculated as follows: volume = 1/6 π length (cm) width (cm) height (cm) [18]. Histopathology studies The xenografted colorectal cancer cell line LS180 was characterized for EGFR overexpression by immunohistochemistry. For the immunohistochemical staining of EGFR, the rabbit polyclonal anti-human EGFR antibody (1:500) was used as the primary antibody, followed by PV 6000 via the two-step immunohistochemical detection of cell-associated EGFR. Mice from each group were sacrificed at 4, 24, and 72 h after the injection of different liposomes. The remaining spleen, liver, and tumor tissues were collected to study their histopathology. The organs from the four groups were dissected, fixed in 10% formalin for 48 h, embedded in paraffin, and sectioned. The sections (5-6 μm) were then stained with hematoxylin and eosin. The histopathological changes of the tissue were ultimately examined using light microscopy (Olympus 40). SPECT whole-body imaging For the SPECT imaging (Discovery VH 670; GE, United States), mice from the three treatment groups (except for the normal saline group) received an intra-tumor injection of 74 MBq (740 MBq/ml) of 131 I-antiEGFR- BSA-PCL, 131 I-BSA-PCL, and 131 I, respectively [19]. SPECT imaging was performed at 4, 24, and 72 h after injection. Animal care and use statement We ensured that mouse use was conducted in accordance with the highest scientific, humane, and ethical principles and was in compliance with regulations. We also ensured that housing conditions and care were species appropriate and that the environment was safe and secure for both animals and staff. Statistical analysis All in vitro experiments were performed in triplicate unless otherwise indicated. Statistical analyses were conducted with the SPSS software (version 17.0). The results are presented as the mean ± SD. Statistical significance was tested using Student s t-test or ANOVA, and P-values < 0.05 were considered statistically significant. RESULTS Basic properties of 131 I-BSA-PCL and 131 I-antiEGFR-BSA- PCL The dynamic light scattering measurement showed that the average diameter of 131 I-BSA-PCL and 131 I-antiEGFR-BSA-PCL was approximately 180 nm, and the polydispersity index was 0.164, in agreement with the TEM result. The mean ζ potential of the obtained protein-based vesicle was also measured and was found to be mv. The negative surface charge that resulted from the BSA shell could reduce undesired protein adsorption and provide good protection for the vesicle during the circulation in the body. The specific radioactivity was approximately MBq/mg for 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL. The labeling rate of 131 I was approximately 50%-85%, and the radiochemical purity was 95%-98%. Internalization of EGFR-BSA-PCL and BSA-PCL The effective diameter of BSA-PCL and antiegfr- BSA-PCL was approximately 180 nm [14]. To assess the binding of antiegfr-bsa-pcl and BSA-PCL to LS180 cells with EGFR overexpression, confocal microscopy was used. The confocal images and the immunofluorescence results of the LS180 cells incubated with antiegfr-bsa-pcl and BSA-PCL were compared (Figure 1). antiegfr-bsa-pcl was significantly internalized in the LS180 cells, which was shown by the appearance of strong green fluorescence. Compared with antiegfr- BSA-PCL, BSA-PCL could similarly bind to cells, but the tumor retention was minimal, and the binding green fluorescence was weaker. This result suggests that the targeting ability of antiegfr-bsa-pcl to tumor cells was enhanced by EGFR modification April 14, 2016 Volume 22 Issue 14

76 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer A DIC Fluorescence Merged mm mm mm B mm mm mm Figure 1 Confocal microscopy of LS180 cancer cells incubated with FITC-BSA-PCL and FITC-antiEGFR-BSA-PCL for 4 h. A I-antiEGFR-BSA-PCL 131 I-BSA-PCL 131 I B I-antiEGFR-BSA-PCL 131 I-BSA-PCL 131 I 1200 CPM/ CMP/ t /h Dose (MBq) Figure I uptake in LS180 cells. Time-dependent cellular uptake of 131 I-antiEGFR-BSA- PCL and 131 I-BSA-PCL To determine the iodide uptake of 131 I-antiEGFR-BSA- PCL and 131 I-BSA-PCL, time activity measurements were obtained for the LS180 cell line. The radioiodide uptake in this cell line reached its maximum level after 4 h of incubation with 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL. Furthermore, the 131 I uptake of 131 I-anti EGFR-BSA-PCL was higher than that of 131 I-BSA- PCL. Cell-associated 131 I activity was still very high after 24 h and reached 79% to 84% in LS 180 cells because the liposomes had slow-release effects (Figure 2A). The CPM in the LS180 cells increased with an increasing dose of 131 I-labeled nanoparticles. However, radioactivity was maintained at a low level in the 131 I group (Figure 2B). Growth curves for nude mice The trend of body weight growth for all study groups is shown in Figure 3. The minimum reduction in body weight was found in the 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL groups. Compared with the original body weight, mice treated with 131 I-antiEGFR-BSA-PCL, 131 I-BSA-PCL, 131 I, and normal saline demonstrated body weight losses of 39% ± 3%, 41% ± 4%, 49% ± 5%, and 55% ± 13%, respectively, on day 54 after 3762 April 14, 2016 Volume 22 Issue 14
77 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer Normal saline 131 I 131 I-BSA-PCL 131 I-antiEGFR-BSA-PCL Normal saline 131 I 131 I-BSA-PCL 131 I-antiEGFR-BSA-PCL Weight (g) Volume (cm 3 ) Time (d) after injection Time (d) after injection Figure 3 Changes in the animal body weight. Figure 4 Changes in tumor volume. tumor inoculation (P < 0.05). Tumor volume of nude mice Rapid tumor growth was observed in the xenografted colorectal cancer nude mice treated with saline or 131 I. The tumor volume change is presented in Figure 4. By contrast, tumors grew slowly in mice treated with 131 I-antiEGFR-BSA-PCL or 131 I-BSA-PCL, and the growth curves of these test groups were similar. No significant differences were observed between the other two groups: those treated with 131 I or normal saline. The data showed that treatment with 131 I-antiEGFR-BSA- PCL and 131 I-BSA-PCL significantly inhibited tumor growth. At the end of the study, the volume of tumor increase in the 131 I-antiEGFR-BSA-PCL group was 124% ± 7%, which was lower than that of the 131 I-BSA-PCL (127% ± 9%), 131 I (143% ± 7%), and normal saline (146% ± 10%) groups. The results from the groups treated with 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL were significantly different from those groups treated with 131 I and normal saline, suggesting that 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL acted similarly to suppress tumor growth. Tissue distribution of 131 I-antiEGFR-BSA-PCL, 131 I-BSA- PCL, and 131 I The tissue distribution of 131 I-antiEGFR-BSA-PCL in nude mice with human colorectal cancer xenografts was measured by γ photon counts in Figure I-anti EGFR-BSA-PCL was markedly taken up by tumor tissues. The tissue distribution assay revealed that 131 I-antiEGFR-BSA-PCL was markedly taken up by the tumor and reached its maximal uptake value of 21.0 ± 1.01 %ID/g at 72 h after the therapy. The drug concentration in the tumor was higher than those in the liver, heart, colon, or spleen at 72 h after therapy. Among the non-tumor tissues, 131 I-antiEGFR-BSA-PCL mostly accumulated in the liver and spleen. The levels of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL in tumor tissues were significantly higher than those observed in the 131 I group at 4, 24, and 72 h after treatment. Histopathology EGFR was overexpressed in the LS180 cell line (Figure 6), and the positive cell membranes were stained brown. The normal saline and 131 I-treated groups were characterized by well-developed proliferation of LS180 cells with a compact arrangement and diffusely distributed invading cancer nests; the nuclei were of various sizes and the staining color was variable. Moreover, no apparent necrosis was found in the cancer tissue (Figure 7). After the intratumoral injection of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL, xenografted colorectal cancer tissues were histopathologically examined (Figure 7). Upon comparison, a large field of the tumor tissue appeared necrotic. Evidence of dying tumor cells undergoing vacuolar degeneration of the cytoplasm was observed. Clusters of tumor cells decreased, whereas the intercellular space increased. Cellular arrangements were seen as discrete and not compact, and the cytoplasm was deeply stained. The cancerous nodes were characterized by patchy necrosis, and their tissue structure was smeared. SPECT imaging The SPECT images of LS180 tumor-bearing mice (21 d after tumor inoculation) were acquired at different time points after the intra-tumor injection of 131 I-antiEGFR- BSA-PCL, 131 I-BSA-PCL, and 131 I. The 131 I-antiEGFR- BSA-PCL and 131 I-BSA-PCL groups both exhibited slow blood clearance and maintained a relatively higher activity (primarily in the tumors, based on biodistribution data). Mice in the 131 I group had rapid blood clearance; their activity did not increase after 24 and 72 h compared with the 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL groups. SPECT images showed high uptake and targeting of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL in the tumor. The results were correlated 3763 April 14, 2016 Volume 22 Issue 14

78 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer I-antiEGFR-BSA-PCL 4 h 24 h 72 h %ID/g 10 0 Heart Liver Spleen Tumor Colon Tissus I-BSA-PCL 4 h 24 h 72 h %ID/g 10 0 Heart Liver Spleen Tumor Colon Tissus I 4 h 24 h 72 h %ID/g 10 0 Heart Liver Spleen Tumor Colon Tissus Figure 5 Tissue distribution of 131 I-antiEGFR-BSA-PCL, 131 I-BSA-PCL and 131 I. and validated with images of the biodistribution data. Figure 6 Immunohistochemical staining of LS180 colorectal cancer. DISCUSSION Colorectal cancer is the third most common cancer worldwide [2]. The C26 murine colon carcinoma model has previously been reported to have a high level of metastasis that spreads after the intraperitoneal inoculation of tumor cells in BALB/c mice [20]. EGFR is a transmembrane receptor belonging to the ErbB family of receptors; the EGFR gene is activated or up-regulated in 60% to 80% of colorectal cancer cases [6,10]. Most of the normal tissues express very low levels of EGFR. However, the liver and kidney tissues 3764 April 14, 2016 Volume 22 Issue 14

79 Li W et al. Radioiodine therapy of I-labled-liposome in mouse colorectal cancer Liver Spleen Saline group 131 I group 131 I-BSA-PCL group 131 I-antiEGFR-BSA-PCL group Tumor 131 Figure 7 Histopathology of the liver, spleen, and tumor tissue at 3 d after the end of the treatment ( 100). express moderately high levels of the receptor, which can exceed that of tumors. Conventional anticancer drugs exhibit a lack of specificity, poor solubility and distribution, unfavorable pharmacokinetics, and high-tissue damage or toxi [21] city. Radiation therapy is typically delivered through high-energy external beam radiation to irradiate the cancerous tissue. Liposomes are spherical vesicles formed by lipid bilayers. These structures have been widely investigated as carriers of tumor-targeting therapy. Radioisotopes can be trapped within the inner space of the liposome, intercalated into the double membrane of the liposome, and connected [22,23] with the surface of the liposome. However, given the close proximity of critical organs to the tumor, the delivery of a therapeutic dose of irradiation without causing serious complications is often impossible, even with technological advancements in radiation dose distribution, such as intensity-modulated radiation [24,25] therapy. Tumor-targeting therapy has overcome the lack of specificity of traditional therapeutic agents. Recent work comparing non-targeted and targeted [26] [27] nanoparticles (lipid-based or polymer-based ) has shown that the primary role of the targeting ligands is to enhance the cellular uptake of drugs by cancer cells rather than to increase their accumulation in the tumor. [12] Kao et al demonstrated the enhanced endocytosis 131 and cytotoxicity of I-C225-AuNP-PEG against EGFRoverexpressing human A549 lung carcinoma cells as well as its active targeting in an A549 tumor xenograft 3765 April 14, 2016 Volume 22 Issue 14
80 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer mouse model [12]. Chen et al [28] and Chang et al [19] reported the biodistribution, pharmacokinetics, and micro-spect/ct imaging of the 188 Re-liposome in C26 colon carcinoma ascites and solid tumor animal models. Their results demonstrated the potential benefit and advantages of the 188 Re-liposome in the C26 animal model. Bao et al [29] reported that the intratumoral injection of liposomal radionuclides had a slower clearance rate. 131 I is a radionuclide with a gamma emission of 364 kev (81.7%) and a beta emission of MeV (89.9%). This molecule has the advantages of imaging feasibility and beta-emitting therapeutic effects. In the present study, the initial treatment of colorectal cancer with 131 I-antiEGFR-BSA-PCL reduced the risk of disease progression compared with 131 I-BSA-PCL and 131 I. The decreased risk was evidenced by changes in the tumor volume, mouse survival time, and mouse weight. As shown by the data, the rates of increase of the final tumor volumes in the groups treated with 131 I-antiEGFR- BSA-PCL and 131 I-BSA-PCL were lower than those of tumor-bearing groups treated with 131 I and normal saline. However, the tumor volumes of the group treated with normal saline and the group treated with 131 I were not significantly different in terms of overall survival. The trend of the body weight growth also had the same characteristics. The 131 I-antiEGFR-BSA- PCL group also achieved the maximum suppression of tumor growth, which reflected an enhancement of cancer therapy with the use of 131 I-antiEGFR-BSA-PCL. We found that the use of 131 I-antiEGFR-BSA-PCL for the in vivo therapy of colorectal cancer was both feasible and reliable, with favorable in vivo characteristics. Results with mouse models demonstrated the steady extravasation of nanoliposomes into ascites with the gradual release of the drug, followed by drug diffusion into the tumor cellular compartment [30,31]. Wang et al [32] reported that direct intratumoral drug administration in advanced neck and head tumors was clearly appealing and immediately achieved high drug concentrations at the target sites without the associated side effects of external beam radiation or systemic chemotherapy. Their group also proved that direct injection could deliver drugs into areas of the tumor that had high interstitial pressure and large areas of avascular necrosis. This study was relevant to the present study on the pharmacokinetics and effectiveness of 131 I-antiEGFR-BSA-PCL administration in the heart, liver, spleen, colon, and tumor cells. The observed iodine uptake demonstrated the potential benefits and advantages of 131 I-antiEGFR-BSA-PCL in the LS180 animal model. The accumulation of radioactivity in the tumor was maintained at steady levels for at least 24 h. SPECT imaging is a non-invasive imaging modality that can monitor the behavior of radiotherapeutics in the same animal at different time points. After the injection of different drugs, the SPECT imaging and iodine uptake showed that the tumor uptake of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL was obvious higher than that of 131 I. In addition, the in vitro stability of the passive 131 I-antiEGFR-BSA-PCL was found to be higher after 24 h of inoculation. Some mice presented skin ulcerations at around day 13 but were healed by day 19. From the SPECT fusion images, we noticed that the 131 I-antiEGFR-BSA-PCL had the tendency to spread into the tumor, liver, spleen, and urinary bladder area. We also observed that the non-tumor tissues of the liver and spleen, which are reticuloendothelial system-rich organs, exhibited significant uptake of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL. The remarkable accumulation of these compounds in the bladder implied that renal clearance is the predominant route of excretion of radioactive metabolites. A glutathione-coated luminescent gold nanoparticle (3 nm diameter) [33] and a gadoliniumloaded dendrimer-entrapped gold nanoparticle (90 nm mean diameter) [34] were previously reported to be excreted via the urinary system. Li et al [16] showed that 131 I-labeled rhegf was markedly absorbed by tumor tissue in xenografted nude mice and reached a maximum uptake rate (16.73 %ID/g) at 120 h after intravenous injection. Their group suggested that 131 I-labeled rhegf could be absorbed by breast cancer tissues and might be a useful clinical candidate. Data from the present study also showed a low immediate clearance for both 131 I-antiEGFR-BSA-PCL and 131 I-BSA- PCL. The long phase was observed at 72 h after 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL were injected, thereby translating to a high locoregional retention rate when the immediate clearance period had passed. These data supported the notion that the injection of liposomal radionuclides could lead to higher retention rates. The anti-tumor effect of 131 I-antiEGFR-BSA-PCL could also be seen in the histopathological studies. Immunohistochemistry showed that the LS180 cell line overexpressed EGFR. The normal saline and 131 I-treated groups were characterized by welldeveloped proliferation of LS180 cells and diffusely distributed invading cancer nests. No apparent necrosis was observed in the cancer tissue. In the xenografted colorectal cancer tissues of the groups treated with 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL, a large field of the tumor tissue appeared necrotic. Evidence of dying tumor cells undergoing vacuolar degeneration of the cytoplasm was observed. The cancerous nodes were characterized by patchy necrosis, and the tissue structures were smeared. These results demonstrated that treatment with 131 I-antiEGFR-BSA- PCL and 131 I-BSA-PCL led to histopathological changes in colorectal cancer tissue that were associated with the death of the tumor cells. The above-mentioned reasons made the intraoperative injection of liposomal therapeutic radionuclides a particularly effective treatment option for advanced colorectal cancer. Although the colorectal cancer xenografted animal model used in this study was not orthotopic, the 3766 April 14, 2016 Volume 22 Issue 14
81 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer results are still valuable for interpreting the drug efficiency of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL. Therefore, the protocols used in this study revealed that the designed formulation and treatment trials were novel for a preclinical study. In conclusion, the results of this study demonstrated that 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL had superior cellular binding and higher cellular uptake compared with 131 I in vitro and in vivo. 131 I-antiEGFR- BSA-PCL suppressed the development of tumors and exhibited pronounced anti-proliferation ability against the xenografted LS180 cells in a mouse model, as demonstrated by changes in the tumor size, body weight, histopathology, and SPECT imaging. This study revealed that 131 I-antiEGFR-BSA-PCL was effective in the killing of tumors, but we did not observe a radiation induced breakdown of the kidney and liver. Therefore, 131 I-antiEGFR-BSA-PCL may be a safe drug for radiotherapy in colorectal cancer. COMMENTS Background Epidermal growth factor receptor (EGFR) is a cell-surface receptor that plays a key role in signaling pathways. Such pathways regulate cell proliferation, angiogenesis, and tumor metastases. EGFR is widely overexpressed in several tumor types, including breast cancer, melanoma, brain glioblastoma, non-small cell lung cancer, and colorectal cancer. EGFR is an attractive candidate for anticancer therapy. Research frontiers Previous experiments have already proven that EGFR is widely overexpressed in colorectal cancer. Innovations and breakthroughs This is the first study evaluating the cellular binding and cellular uptake of 131 I-antiEGFR-BSA-PCL and 131 I-BSA-PCL in vitro and in vivo. 131 I-antiEGFR- BSA-PCL suppressed the development of tumors and exhibited pronounced anti-proliferation ability against the xenografted LS180 cells in a mouse model. Applications As a novel theranostic agent, 131 I-antiEGFR-BSA-PCL exhibited pronounced anti-tumoral effects on colorectal cancer. Peer-review This study evaluated the therapeutic effectiveness of 131 I-antiEGFR-BSA-PCL in the colorectal cancer mouse model and demonstrated the potential beneficial application of 131 I-antiEGFR-BSA-PCL for treating colorectal cancer. The manuscript is well written and properly conducted. REFERENCES 1 Fang M, Peng CW, Pang DW, Li Y. Quantum dots for cancer research: current status, remaining issues, and future perspectives. Cancer Biol Med 2012; 9: [PMID: DOI: /j.issn ] 2 Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, CA Cancer J Clin 2005; 55: [PMID: DOI: /canjclin ] 3 Gabizon A, Shmeeda H, Barenholz Y. Pharmacokinetics of pegylated liposomal Doxorubicin: review of animal and human studies. Clin Pharmacokinet 2003; 42: [PMID: DOI: / ] 4 Allen TM, Cullis PR. Drug delivery systems: entering the mainstream. Science 2004; 303: [PMID: DOI: /science ] 5 Mendelsohn J, Baselga J. The EGF receptor family as targets for cancer therapy. Oncogene 2000; 19: [PMID: DOI: /sj.onc ] 6 Messa C, Russo F, Caruso MG, Di Leo A. EGF, TGF-alpha, and EGF-R in human colorectal adenocarcinoma. Acta Oncol 1998; 37: [PMID: DOI: / ] 7 Ciardiello F, Tortora G. EGFR antagonists in cancer treatment. N Engl J Med 2008; 358: [PMID: DOI: /NEJMra ] 8 Yang J, Lim EK, Lee HJ, Park J, Lee SC, Lee K, Yoon HG, Suh JS, Huh YM, Haam S. Fluorescent magnetic nanohybrids as multimodal imaging agents for human epithelial cancer detection. Biomaterials 2008; 29: [PMID: DOI: /j.biomaterials ] 9 Nurwidya F, Murakami A, Takahashi F, Takahashi K. Molecular mechanisms contributing to resistance to tyrosine kinase-targeted therapy for non-small cell lung cancer. Cancer Biol Med 2012; 9: [PMID: DOI: /j.issn ] 10 Porebska I, Harlozińska A, Bojarowski T. Expression of the tyrosine kinase activity growth factor receptors (EGFR, ERB B2, ERB B3) in colorectal adenocarcinomas and adenomas. Tumour Biol 2000; 21: [PMID: ] 11 Koppe MJ, Bleichrodt RP, Soede AC, Verhofstad AA, Goldenberg DM, Oyen WJ, Boerman OC. Biodistribution and therapeutic efficacy of (125/131)I-, (186)Re-, (88/90)Y-, or (177)Lu-labeled monoclonal antibody MN-14 to carcinoembryonic antigen in mice with small peritoneal metastases of colorectal origin. J Nucl Med 2004; 45: [PMID: ] 12 Kao HW, Lin YY, Chen CC, Chi KH, Tien DC, Hsia CC, Lin MH, Wang HE. Evaluation of EGFR-targeted radioimmuno-goldnanoparticles as a theranostic agent in a tumor animal model. Bioorg Med Chem Lett 2013; 23: [PMID: DOI: /j.bmcl ] 13 Su CH, Sheu HS, Lin CY, Huang CC, Lo YW, Pu YC, Weng JC, Shieh DB, Chen JH, Yeh CS. Nanoshell magnetic resonance imaging contrast agents. J Am Chem Soc 2007; 129: [PMID: DOI: /ja ] 14 Liu Z, Dong C, Wang X, Wang H, Li W, Tan J, Chang J. Selfassembled biodegradable protein-polymer vesicle as a tumortargeted nanocarrier. ACS Appl Mater Interfaces 2014; 6: [PMID: DOI: /am404734c] 15 Ickenstein LM, Edwards K, Sjöberg S, Carlsson J, Gedda L. A novel 125I-labeled daunorubicin derivative for radionuclidebased cancer therapy. Nucl Med Biol 2006; 33: [PMID: ] 16 Li YC, Xu WY, Tan TZ, He S. 131I-recombinant human EGF has antitumor effects against MCF-7 human breast cancer xenografts with low levels of EGFR. Nucl Med Biol 2004; 31: [PMID: DOI: /j.nucmedbio ] 17 Shao X, Zhang H, Rajian JR, Chamberland DL, Sherman PS, Quesada CA, Koch AE, Kotov NA, Wang X. 125I-labeled gold nanorods for targeted imaging of inflammation. ACS Nano 2011; 5: [PMID: DOI: /nn203138t] 18 Lee YS, Bullard DE, Zalutsky MR, Coleman RE, Wikstrand CJ, Friedman HS, Colapinto EV, Bigner DD. Therapeutic efficacy of antiglioma mesenchymal extracellular matrix 131I-radiolabeled murine monoclonal antibody in a human glioma xenograft model. Cancer Res 1988; 48: [PMID: ] 19 Chang YJ, Chang CH, Chang TJ, Yu CY, Chen LC, Jan ML, Luo TY, Lee TW, Ting G. Biodistribution, pharmacokinetics and microspect/ct imaging of 188Re-bMEDA-liposome in a C26 murine colon carcinoma solid tumor animal model. Anticancer Res 2007; 27: [PMID: ] 20 Corbett TH, Griswold DP, Roberts BJ, Peckham JC, Schabel FM. Evaluation of single agents and combinations of chemotherapeutic agents in mouse colon carcinomas. Cancer 1977; 40: [PMID: DOI: / (197711)40:5] 3767 April 14, 2016 Volume 22 Issue 14
82 Li W et al. Radioiodine therapy of 131 I-labled-liposome in mouse colorectal cancer 21 Ting G, Chang CH, Wang HE, Lee TW. Nanotargeted radionuclides for cancer nuclear imaging and internal radiotherapy. J Biomed Biotechnol 2010; 2010: pii [PMID: DOI: /2010/953537] 22 Bao A, Goins B, Klipper R, Negrete G, Phillips WT. Direct 99mTc labeling of pegylated liposomal doxorubicin (Doxil) for pharmacokinetic and non-invasive imaging studies. J Pharmacol Exp Ther 2004; 308: [PMID: DOI: / jpet ] 23 Bao A, Goins B, Klipper R, Negrete G, Phillips WT. 186Reliposome labeling using 186Re-SNS/S complexes: in vitro stability, imaging, and biodistribution in rats. J Nucl Med 2003; 44: [PMID: ] 24 Lee N, Puri DR, Blanco AI, Chao KS. Intensity-modulated radiation therapy in head and neck cancers: an update. Head Neck 2007; 29: [PMID: DOI: /hed.20332] 25 Xia P, Fu KK, Wong GW, Akazawa C, Verhey LJ. Comparison of treatment plans involving intensity-modulated radiotherapy for nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys 2000; 48: [PMID: DOI: /S (00)00585-X] 26 Kirpotin DB, Drummond DC, Shao Y, Shalaby MR, Hong K, Nielsen UB, Marks JD, Benz CC, Park JW. Antibody targeting of longcirculating lipidic nanoparticles does not increase tumor localization but does increase internalization in animal models. Cancer Res 2006; 66: [PMID: DOI: / CAN ] 27 Bartlett DW, Su H, Hildebrandt IJ, Weber WA, Davis ME. Impact of tumor-specific targeting on the biodistribution and efficacy of sirna nanoparticles measured by multimodality in vivo imaging. Proc Natl Acad Sci USA 2007; 104: [PMID: DOI: /pnas ] 28 Chen LC, Chang CH, Yu CY, Chang YJ, Wu YH, Lee WC, Yeh CH, Lee TW, Ting G. Pharmacokinetics, micro-spect/ct imaging and therapeutic efficacy of (188)Re-DXR-liposome in C26 colon carcinoma ascites mice model. Nucl Med Biol 2008; 35: [PMID: DOI: /j.nucmedbio ] 29 Bao A, Phillips WT, Goins B, Zheng X, Sabour S, Natarajan M, Ross Woolley F, Zavaleta C, Otto RA. Potential use of drug carried-liposomes for cancer therapy via direct intratumoral injection. Int J Pharm 2006; 316: [PMID: DOI: /j.ijpharm ] 30 Bally MB, Masin D, Nayar R, Cullis PR, Mayer LD. Transfer of liposomal drug carriers from the blood to the peritoneal cavity of normal and ascitic tumor-bearing mice. Cancer Chemother Pharmacol 1994; 34: [PMID: DOI: / BF ] 31 Gabizon AA. Selective tumor localization and improved therapeutic index of anthracyclines encapsulated in long-circulating liposomes. Cancer Res 1992; 52: [PMID: ] 32 Wang SX, Bao A, Herrera SJ, Phillips WT, Goins B, Santoyo C, Miller FR, Otto RA. Intraoperative 186Re-liposome radionuclide therapy in a head and neck squamous cell carcinoma xenograft positive surgical margin model. Clin Cancer Res 2008; 14: [PMID: DOI: / CCR ] 33 Zhou C, Hao G, Thomas P, Liu J, Yu M, Sun S, Öz OK, Sun X, Zheng J. Near-infrared emitting radioactive gold nanoparticles with molecular pharmacokinetics. Angew Chem Int Ed Engl 2012; 51: [PMID: DOI: /anie ] 34 Wen S, Li K, Cai H, Chen Q, Shen M, Huang Y, Peng C, Hou W, Zhu M, Zhang G, Shi X. Multifunctional dendrimer-entrapped gold nanoparticles for dual mode CT/MR imaging applications. Biomaterials 2013; 34: [PMID: DOI: /j.biomaterials ] P- Reviewer: Meshikhes AW S- Editor: Gong ZM L- Editor: Wang TQ E- Editor: Ma S 3768 April 14, 2016 Volume 22 Issue 14
83 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Basic Study ORIGINAL ARTICLE Hypothalamic paraventricular nucleus stimulation reduces intestinal injury in rats with ulcerative colitis Quan-Jun Deng, Ding-Jing Deng, Jin Che, Hai-Rong Zhao, Jun-Jie Yu, Yong-Yu Lu Quan-Jun Deng, Department of Neurosurgery, General Hospital Affiliated to Tianjin Medical University, Tianjin , China Ding-Jing Deng, Jin Che, Hai-Rong Zhao, Department of gastroenterology, General Hospital Affiliated to Tianjin Medical University, Tianjin , China Jun-Jie Yu, Yong-Yu Lu, Department of cerebral surgery, people s Hospital of Haimen, Haimen , Jiangsu Province, China Author contributions: Deng Qj and Lu YY designed the research; Deng QJ, Deng DJ, Che J, Zhao HR, Lu YY and Yu JJ performed the research; Deng DJ, Che J, Zhao HR and Lu YY contributed new reagents/analytic tools; Deng QJ, Lu YY and Yu JJ analyzed the data; and Deng QJ and Lu YY wrote the paper. Institutional review board statement: The study was reviewed and approved by the Institutional Review Board of Haimen People s Hospital. Institutional animal care and use committee statement: All procedures involving animals were reviewed and approved by the Institutional Animal Care and Use Committee of the General Hospital Affiliated to Tianjin Medical University (IACUC protocol number: Shanghai Lab Animal Research Center, CP- GUIDE-IACUC-0458). Conflict-of-interest statement: We declare that there is no conflict of interest to disclose in this study. Data sharing statement: No additional data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Yong-yu Lu, Associate chief physician, Department of cerebral surgery, people s Hospital of Haimen, People s Road West, No. 253, Haimen , Jiangsu Province, China. luyongyu8@sina.com Telephone: Fax: Received: November 29, 2015 Peer-review started: November 30, 2015 First decision: December 16, 2015 Revised: January 11, 2016 Accepted: January 17, 2016 Article in press: January 19, 2016 Published online: April 14, 2016 Abstract AIM: To investigate the effect and mechanism of stimulation of the hypothalamic paraventricular nucleus with glutamate acid in rats with ulcerative colitis (UC). METHODS: The rats were anesthetized with 10% chloral hydrate via abdominal injection and treated with an equal volume of TNBS + 50% ethanol enema, injected into the upper section of the anus with the tail facing up. Colonic damage scores were calculated after injecting a certain dose of glutamic acid into the paraventricular nucleus (PVN), and the effect of the nucleus tractus solitarius (NTS) and vagus nerve in alleviating UC injury through chemical stimulation of the PVN was observed in rats. Expression changes of C-myc, Apaf-1, caspase-3, interleukin (IL)-6, and IL-17 during the protection against UC injury through chemical stimulation of the PVN in rats were detected by Western blot. Malondialdehyde (MDA) content and superoxide dismutase (SOD) activity in colon tissues of rats were measured by colorimetric methods. RESULTS: Chemical stimulation of the PVN significantly reduced UC in rats in a dose-dependent manner. The protective effects of the chemical stimulation 3769 April 14, 2016 Volume 22 Issue 14
84 Deng QJ et al. Hypothalamic PVN stimulation reduces intestinal injury of the PVN on rats with UC were eliminated after chemical damage to the PVN. After glutamate receptor antagonist kynurenic acid was injected into the PVN, the protective effects of the chemical stimulation of the PVN were eliminated in rats with UC. After AVP- Vl receptor antagonist ([Deamino-penl, val4, D-Arg8]- vasopressin) was injected into NTS or bilateral chemical damage to NTS, the protective effect of the chemical stimulation of PVN on UC was also eliminated. After chemical stimulation of the PVN, SOD activity increased, MDA content decreased, C-myc protein expression significantly increased, caspase-3 and Apaf-1 protein expression significantly decreased, and IL-6 and IL-17 expression decreased in colon tissues in rats with UC. CONCLUSION: Chemical stimulation of the hypothalamic PVN provides a protective effect against UC injury in rats. Hypothalamic PVN, NTS and vagus nerve play key roles in this process. Key words: Paraventricular nucleus; Nucleus tractus solitarius; Ulcerative colitis; Arginine vasopressin; 2,4,6-trinitrobenzene sulfonic acid The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: This study confirms that the chemical stimulation of the paraventricular nucleus with glutamic acid reduces intestinal injury in ulcerative colitis (UC). Furthermore, this study also discusses the possible regulatory mechanism of the central nervous system of rats with UC, so as to provide a theoretical basis for clinical treatment of UC. Deng QJ, Deng DJ, Che J, Zhao HR, Yu JJ, Lu YY. Hypothalamic paraventricular nucleus stimulation reduces intestinal injury in rats with ulcerative colitis. World J Gastroenterol 2016; 22(14): Available from: URL: com/ /full/v22/i14/3769.htm DOI: org/ /wjg.v22.i INTRODUCTION Ulcerative colitis (UC) is a common non-specific inflammatory bowel disease that easily recurs, has many complications and has a very poor prognosis [1]. At present, due to the influence of environmental, diet and other factors, UC has increasingly prevailed in the population, but its exact etiology and pathogenesis remain unclear [2,3]. A study carried out by Mascaraque et al [4] revealed that the central and peripheral nervous systems are involved in the regulation of UC. In addition, many studies have confirmed that the hypothalamic paraventricular nucleus (PVN) and nucleus tractus solitarius (NTS) may play an important role in regulating stress-induced gastric mucosal damage (SGMD) and gastric ischemia-reperfusion injury (GI-RI), and that the PVN and NTS may have participated in the regulatory role of the PVN in GI- RI [5-7]. However, the regulatory role of the PVN in UC, as well as its regulatory role in the treatment of UC, has been rarely reported. Therefore, in this study, we observed whether hypothalamic PVN stimulation could reduce intestinal injury in rats with UC through PVN chemical stimulation, chemical damage, injection of chemical antagonists and other methods, and preliminarily explored the related regulatory and molecular mechanisms. MATERIALS AND METHODS Reagents and equipment SPF-grade SD rats weighing g were purchased from the Shanghai Experimental Animal Center (Shanghai, China). Glutamic acid, kainic acid (KA), kynurenic acid (KYNA) and [Deamino-penl, val4, D-Arg8]-vasopressin (DPVDAV) were purchased from Sigma-Aldrich; 2,4,6-trinitrobenzene sulfonic acid (TNBS) was purchased from Gibco; anti-pcna antibody kit was purchased from Santa Cruz Biotechnology; rat interleukin-17 (IL-17) ELISA kit and BCA protein assay kit were purchased from Beyotime; C-myc polyclonal antibody and Apaf-1 polyclonal antibody were purchased from Invitrogen; the 680 automatic microplate reader and Western electrophoresis apparatus were purchased from Bio-Rad; the DYY- 6B nucleic acid electrophoresis apparatus was purchased from Nanjing Xianou Instrument Factory; the centrifuge was purchased from Eppendorf; and the optical biological microscope was purchased from Olympus. Experimental methods Preparation of the UC model: Rats were provided with water before establishing the model. After one day of fast, the animals were anesthetized with 10% chloral hydrate via abdominal injection and treated with an equal volume of TNBS + 50% ethanol enema, injected into the upper section of the anus with the tail facing up. The rats were maintained in an inverted position for 5 min. Three days after the successful establishment of the model, rats were sacrificed. Then, the brain and colon were removed and preserved for use. Colonic damage scoring: After the successful modeling of UC rats in each group, the colon was obtained and cut by careful incision with forceps, damage was carefully observed after the colon was rinsed, and scoring was performed according to the scoring criteria shown in Table 1, with the average score of each group as the final score of the group. Chemical stimulation and damage to the hypothalamic PVN: Glutamic acid and KA were 3770 April 14, 2016 Volume 22 Issue 14
85 Deng QJ et al. Hypothalamic PVN stimulation reduces intestinal injury Table 1 Colonic damage score scoring criteria Characteristic Score was induced and UC damage was observed. Control groups included a PVN group, a UC group and a vehicle group. There are eight rats in each group. Ulcer No ulcer 0 Punctate hyperemia, no ulcer 1 Ulcer, no hyperemia or bowel wall thickening 2 Ulcer with inflammation 3 Ulcer with two or more inflammations 4 The length of ulcer damage was greater than l cm 5 along the longitudinal axis of the colon The length of ulcer damage was greater than 2 cm 6-10 along the longitudinal axis of the colon, each additional 1 cm of the disease, score plus 1 Adhesions No adhesions 0 Slight adhesions 1 (the colon can easily be separated with other tissues) Severe adhesions 2 Diarrhea No diarrhea 0 Have diarrhea 1 Total score selected as PVN chemical stimuli and chemical damaging agents, and the glutamate receptor antagonist was KYNA, all of which were dissolved in 0.3 μl of 0.9% normal saline for use. For chemical stimulation group (PVN group), after stimulation of the PVN with 3, 6 or 12 μg of glutamic acid, UC was induced and colon injury scoring was performed. For PVN damage group (PVN + KA group), 0.3 μg of KA was injected into the PVN to induce PVN chemical damage. After 3 d, 12 μg of glutamic acid was injected again for hypothalamic PVN stimulation, then UC was induced and the UC injury scoring was performed. For glutamic acid antagonistic group (PVN + KYNA group): glutamic acid antagonist KYNA was injected into the PVN, 12 μg of glutamic acid was injected 10 min later for PVN stimulation, then UC was induced and the UC damage situation was observed. Control groups consist of a normal untreated group (normal group), a UC model group (UC alone group), and a vehicle group, in which the UC model was prepared by enema after 0.3 μl of 0.9% normal saline was microinjected into the cerebral nuclei. There are eight rats in each group. Chemical damage to the NTS and injection of the AVP-Vl receptor antagonist into the NTS: KA was selected to induce chemical damage to the NTS and the AVP-Vl receptor antagonist agent was DPVDAV, both of which were dissolved in 0.3 μl of 0.9% normal saline for use. In the NTS damage group (NTS + KA group), 0.3 μg of KA was used to induce NTS chemical damage. After 3 d, 12 μg of glutamic acid was used again for hypothalamic PVN stimulation, then UC was induced and the score conditions were observed. In AVP-Vl receptor antagonist group (NTS + DPVDAV group), AVP-Vl receptor antagonist DPVDAV was injected into the NTS. After 10 min, 12 μg of glutamic acid was injected again for PVN stimulation, then UC Determination of IL-6, IL-17 and C-myc, Apaf-1, caspase-3 protein expression in colon tissue of rats with UC by Western blot assay: Fifteen microliters of the test sample was mixed with 5 μl of 4 loading buffer and boiled for 10 min. Then, 10 μl of the same sample was placed onto a 12% SDS-PAGE gel for electrophoresis at a voltage of V. At the end of electrophoresis, the sample was transferred onto an NC membrane, blocked with 5% milk at room temperature for 2 h, and rinsed with TBST three times at 30-min intervals. Then, primary antibodies were successively added with the following dilutions: IL-6 at 1:1000, IL-17 at 1:1000, Apaf-1 at 1:500, C-myc at 1:600, caspase-3 at 1:750; and incubated overnight at 4. Subsequently, the samples were washed three times with TBST at 10-min intervals, selected alkaline phosphatase-labeled secondary antibodies, and incubated at room temperature for 2 h. After the samples were washed three times with TBST at 30-min intervals, wetted with coloured solution, and pictures were developed and photographed in an ECL developer. Detection of SOD activity and MDA content in colon tissue of rats with UC: SOD activity was measured in tissues of rats in each group. One hundred microliters of the supernatant and 100 μl of Reagent 7 were mixed. After 5 min, tissues were centrifuged (5000 r/min for 20 min) and the supernatant was obtained. For the control supernatant, the supernatant of tissue homogenate was replaced with normal saline; and other operations were the same. Control tubes and reaction tubes included: SOD control tube (500 μl of the agent μl of purified water), SOD measurement tube (500 μl of the agent μl of the sample), Cu-Zn SOD control tube (500 μl of the agent μl of the control supernatant), and Cu-Zn SOD measurement tube (500 μl of the agent μl of the supernatant of samples). Then, 100 μl of Reagents 2, 3 and 4 were added again and incubated for 1 h at 37. After adding the chromogenic reagent for 10 min, SOD activity was determined by colorimetric analysis and calculated in accordance with absorbance values. MDA content was determined from the same tissue homogenate supernatant selected in each group. Standard tube consisted of 200 μl of standard product + 3 ml of Reagent ml of Reagent 3; standard blank tube contained 200 μl ethanol + 3 ml of Reagent ml Reagent 3; measuring tube consisted of 200 μl of the sample + 3 ml of Reagent ml of Reagent 3; measuring blank tube contained 200 μl of the sample + 3 ml of Reagent ml of Reagent ml of acetic acid. After mixing, the tubes were placed in water bath at 95, and 3771 April 14, 2016 Volume 22 Issue 14
86 Deng QJ et al. Hypothalamic PVN stimulation reduces intestinal injury c e 8 a CDS 6 4 a c 2 0 Normal group UC group Vehicle group PVN (3 mg) PVN (6 mg) PVN (12 mg) PVN + KA group PVN + KYNA group Figure 1 colonic damage scores in colons of rats with ulcerative colitis in each group after glutamic acid stimulation and chemical damage to the paraventricular nucleus. a P < 0.05, PVN (12 μg) group vs each group; c P < 0.05, PVN (12 μg) group vs the PVN + KA group; e P < 0.05, PVN (12 μg) group vs the PVN + KYMA group. CDS: colonic damage score; PVN: paraventricular nucleus; KA: Kainic acid. centrifuged (5000 r/min, 20 min) after 1 h of cooling, the supernatant was obtained, and absorbance value was measured. MDA content was calculated according to the absorbance value of each tube. Statistical analysis: SPSS 19.0 software was used for statistical analyses. Quantitative data are expressed as mean ± sd. The t-test was carried out between two groups, and one-way analysis of variance (ANOVA) was used for multiple comparisons. Pearson s correlation analysis was employed for correlation analysis. P < 0.05 was considered statistically significant. RESULTS Influence of glutamic acid stimulation and chemical damage to the PVN on intestinal injury in rats After chemical stimulation of the PVN was induced with 3, 6 or 12 μg of glutamic acid, colonic damage scores (CDS) of rats were 7.25 ± 0.98, 5.34 ± 0.89 and 3.74 ± 0.94, respectively, which significantly decreased compared to the vehicle group (10.24 ± 1.02). As the amount of glutamic acid increased, CDS decreased significantly (P < 0.05). After KA was used to induce chemical damage to the PVN, 12 μg of glutamic acid was used again to induce chemical stimulation in rats, the CDS was ± 1.21, which significantly increased compared to simply using 12 μg of glutamic acid to induce chemical stimulation in rats (3.74 ± 0.94, P < 0.05). However, the difference was not statistically significant compared to rats in the UC group (9.86 ± 1.04, P > 0.05). In addition, after injecting glutamic acid antagonist KYNA into the PVN, chemical stimulation was carried out and the CDS was 9.87 ± 1.01, which significantly increased compared to simply using 12 μg of glutamic acid for chemical stimulation (3.74 ± 0.94, P < 0.05; Figure 1). Influence of chemical damage to the NTS and injection of AVP-Vl receptor antagonist into the NTS on alleviated UC injury in rats by glutamic acid stimulation of the hypothalamic PVN Three days after chemical damage to the NTS, 12 μg of glutamic acid was used again for the chemical stimulation of the hypothalamic PVN. CDS was ± 1.09, which significantly increased compared to simply using 12 μg of glutamic acid for chemical stimulation (3.74 ± 0.94, P < 0.05). Ten minutes after DPVDAV was injected into the NTS of rats, 12 μg of glutamic acid was injected again to stimulate the PVN. CDS in rats was 9.67 ± 1.05, which significantly increased compared to simply using 12 μg of glutamic acid for chemical stimulation (3.74 ± 0.94, P < 0.05). When comparing the CDS of the NTS chemical damage group and DPVDAV group with the UC group and vehicle group, the differences were not statistically significant (P > 0.05; Figure 2). Influence of stimulation of the PVN with glutamic acid on IL-6 and IL-17 contents in colon tissues in rats The contents of IL-6 and IL-17 in colon tissues were significantly increased in the UC group compared with the normal group, while the contents of IL-6 and IL-17 were significantly decreased in the 12-μg glutamic acid stimulation PVN group compared to the UC group and vehicle group (P < 0.05; Figure 3). Influence of stimulation of the PVN with glutamic acid on SOD activity and MDA content in colon tissue of rats SOD activity significantly decreased in colon tissues in the UC group compared with the normal group, while SOD activity was significantly higher in the 12-μg glutamic acid stimulation group compared with the UC group (P = 7.964, t = 0.001; P = , t = 0.002). MDA content was significantly increased in colon tissue 3772 April 14, 2016 Volume 22 Issue 14

 NTS + KA group NTS + DPVDAV group a P < 0.05, UC group vs the normal group; c P < 0.05, PVN (12 μg) group vs the UC group and vehicle group.")
87 Deng QJ et al. Hypothalamic PVN stimulation reduces intestinal injury a c Table 2 Superoxide dismutase activity and malondialdehyde content in colon tissue of rats with ulcerative colitis CDS Group SOD (U/mg) MDA (nmol/mg) Normal group ± ± 0.45 UC group ± 7.21 a 6.28 ± 0.94 a Vehicle group ± ± 0.83 PVN (12 μg) group ± c 3.13 ± 0.50 c 2 0 UC group Vehicle group PVN (12 mg) NTS + KA group NTS + DPVDAV group a P < 0.05, UC group vs the normal group; c P < 0.05, PVN (12 μg) group vs the UC group and vehicle group. PVN: Paraventricular nucleus; SOD: Superoxide dismutase; MDA: Malondialdehyde; UC: Ulcerative colitis. Normal group UC group PVN group Vehicle group Figure 2 Influence of chemical damage to the nucleus tractus solitarius and injection of AVP-Vl receptor antagonist into the nucleus tractus solitarius on alleviated ulcerative colitis injury in rats by stimulation of the hypothalamic paraventricular nucleus with glutamic acid. a P < 0.05, PVN (12 μg) group vs the NTS + KA group; c P < 0.05, PVN (12 μg) group vs the NTS + DPVDAV group. DPVDAV: damage in nucleus tractus solitarius and injection of AVP-Vl receptor antagonist; NTS: nucleus tractus solitaries; KA: Kainic acid; PVN: paraventricular nucleus. Normal group UC group PVN group Vehicle group C-myc Apaf-1 b-actin Caspase-3 IL-17 IL-6 b-actin Figure 3 interleukin-6 and interleukin-17 contents in colon tissue of rats with ulcerative colitis. in the UC group than in the normal group, while MDA content in the 12-μg glutamic acid chemical stimulation group was significantly decreased than in the UC group (P = , t = 0.010; P = 5.124, t = 0.007; Table 2). Influence of stimulation of the PVN with glutamic acid on C-myc, Apaf-1 and caspase-3 protein expression in colon tissues of rats Apaf-1 and caspase-3 protein expression levels were significantly higher in the UC group than in the normal group, while C-myc protein expression levels were significantly lower than the normal group (P < 0.05). After 12 μg of glutamic acid was used for stimulation in rats in the PVN group, Apaf-1 and caspase-3 protein expression levels were significantly decreased compared with the UC and vehicle groups, while C-myc protein expression levels were significantly increased compared with the UC and vehicle groups (P < 0.05; Figure 4). Figure 4 C-myc, Apaf-1 and caspase-3 protein expression in colon tissues of rats with ulcerative colitis. DISCUSSION UC is a common and complex gastrointestinal disease that often brings great suffering to patients [1]. At present, the exact etiology and pathogenesis of UC remain unclear. In this study, we investigated the chemical stimulation of rat hypothalamic PVN, as well as its role in UC in rats and its regulatory mechanisms. On the basis of the establishment of a UC rat model and the stimulation of the hypothalamic PVN with glutamic acid, we observed whether PVN stimulation could alleviate intestinal damage in rats with UC, and investigated related regulatory and molecular mechanisms, to provide a theoretical basis for clinical studies. Stimulation of the PVN with glutamic acid significantly reduces intestinal injury in rats with UC As one of the centers of visceral activity, the PVN can extensively regulate various gastrointestinal mucosal injuries and repair processes [8]. In this study, stimulation of the PVN with glutamic acid significantly reduced intestinal damage in rats with UC, and as the dose of glutamic acid increased, the scale of improvement correspondingly increased. This effect disappeared when the PVN was damaged before glutamic acid injection. This may be because the PVN 3773 April 14, 2016 Volume 22 Issue 14
88 Deng QJ et al. Hypothalamic PVN stimulation reduces intestinal injury is a central nervous system that plays a key part in the protection and repair of intestinal injuries in rats, and this effect may be limited to the center of the PVN and its related neurons and has nothing to do with its other parts or other neurons. The studies of A1-Ghoul WM and Mateos JM successively found that mrnas of two kinds of glutamate receptor subtypes (metabotropic glutamate and ionotropic) are closely associated with the PVN, which are only distributed in the PVN region [9,10]. In this study, glutamic acid receptor antagonist KYNA can block the stimulation of the PVN with glutamic acid for the protection and repair of intestinal injury in rats with UC. Therefore, we conclude that glutamic acid receptors at the molecular level possibly mediate PVN stimulation to alleviate this effect in intestinal injury in rats with UC. Effect of hypothalamic PVN for alleviating intestinal injury in rats with UC is mediated by the medulla oblongata NTS and outer peripheral vagal nerve Hypothalamic PVN has a wide range of projection capabilities, which can communicate with many functional areas in the brain by signals, and is most closely associated with the NTS [11]. In this study, stimulation of the PVN with glutamic acid for alleviating intestine injury in rats with UC can be blocked after using KA to damage the NTS, revealing that the NTS may play an important role in the regulation of the PVN in intestinal injury repair [12]. The research team of Hegart found that AVP neurons in the PVN have a direct fiber projection with other functional areas of the brain, and the NTS is one of these. A bidirectional fiber link can be formed between the NTS and PVN, because the NTS is rich in AVP-Vl receptors [13]. In this study, AVP-Vl receptor antagonist DPVDAV was injected into the NTS in order to investigate whether AVP-Vl receptors are involved in the regulation of the PVN in the intestinal repair of rats via the NTS. It was found that the effect of glutamic acid stimulation of the PVN for alleviating intestinal injury in rats with UC disappeared. After KA induced damage to the NTS, similar experimental results were obtained, which partly confirmed the key role that AVP-Vl receptors played. PVN stimulation regulates the intestinal repair possibly through anti-apoptotic effects, antioxidant effects, as well as the inhibition of inflammatory cytokines and other procedures UC can secrete large amounts of inflammatory cytokines in the body [14-16], in which TNF-α and IL-1β may play an extremely important role in the inflammatory process [17,18]. This study revealed that after glutamic acid stimulation, the hypothalamic PVN may cause TNF-α and IL-1β expression levels to significantly decrease in colon tissue. This may be because the stimulation of the PVN with glutamic acid can reduce inflammatory effects by inhibiting the expression of inflammatory cytokines, and thus, play a role in repairing damage. Increased oxygen free radicals can significantly injure body tissues. In order to eliminate such harm, the body can produce a free radical scavenger to scavenge oxygen free radicals. Therefore, the level of free radical scavenger activity can indirectly reflect the degree of injured body tissues, in which SOD is one of the most important members [19-22]. The study of the group of Talero E confirmed that UC can produce large amounts of oxygen free radicals such as reactive oxygen and nitrogen, which can cause great damage to the colonic mucosa [23-27]. In addition, an increase in oxygen free radicals can cause lipid peroxidation, resulting in increased MDA levels. Therefore, the level of MDA content may indirectly reflect the degree of cell damage. In this study, after PVN stimulation with glutamic acid, MDA content within the colonic mucosa significantly decreased in rats with UC, while SOD activity significantly increased. Perhaps, this is because of the regulatory role of the PVN after stimulation, in which the antioxidant capacity of colonic epithelial cells was enhanced so as to alleviate the injury. The injury degree of UC to the colon depends on the balance between colonic epithelial cell proliferation and apoptosis to some extent. If this balance is broken and apoptosis is more than proliferation, it can result in the exacerbation of intestinal injury, while when proliferation is more than apoptosis, it would likely alleviate UC disease. The studies of the groups of Kararmnolis DG and Limura M revealed that colonic epithelial injury is usually accompanied by C-myc, Apaf-1 and caspase-3 expression changes [28-31], in which C-myc protein can inhibit apoptosis and promote cell proliferation. On the contrary, Apaf-1 and caspase-3 proteins are closely associated with apoptosis, and their overexpression can inhibit C-myc and other anti-apoptotic effects, resulting in increased apoptosis and diminished proliferation capacity. In this study, when glutamic acid was used to stimulate the PVN, Apaf-1 and caspause-3 protein expression levels significantly decreased and C-myc protein expression levels significantly increased in rats with UC. This shows that PVN stimulation can reduce tissue damage by enhancing the anti-apoptotic ability of colonic epithelial cells. In summary, this study confirms that chemical stimulation of the PVN with glutamic acid can reduce intestinal injury in UC. Furthermore, this study also discussed the possible regulatory mechanism of the central nervous system of rats with UC, so as to provide a theoretical basis for clinical protection and the treatment of UC. COMMENTS Background Ulcerative colitis (UC) is a common non-specific inflammatory bowel disease 3774 April 14, 2016 Volume 22 Issue 14
89 Deng QJ et al. Hypothalamic PVN stimulation reduces intestinal injury that easily recurs, has many complications and has a very poor prognosis. At present, due to the influence of environmental, diet and other factors, UC has increasingly prevailed in the population, but its exact etiology and pathogenesis remain unclear. Research frontiers A study carried out by Mascaraque et al revealed that the central and peripheral nervous systems are involved in the regulation of UC. Innovations and breakthroughs The hypothalamic paraventricular nucleus (PVN) and nucleus tractus solitarius (NTS) may play an important role in regulating stress-induced gastric mucosal damage and gastric ischemia-reperfusion injury (GI-RI), and they may have participated in the regulatory role of PVN in GI-RI. However, the regulatory role of the PVN in UC, as well as its regulatory role for the treatment of UC, has been rarely reported. Applications In this study, the authors observed whether hypothalamic PVN stimulation could reduce intestinal injury in rats with UC through PVN chemical stimulation, chemical damage, injection of chemical antagonists and other methods, and preliminarily explored related regulatory and molecular mechanisms. Peer-review In this manuscript, the authors investigated the effect and mechanism of glutamate acid stimulation of the hypothalamic paraventricular nucleus in rats with UC. The study is well designed and the results are very interesting. REFERENCES 1 Pedersen J, LaCasse EC, Seidelin JB, Coskun M, Nielsen OH. Inhibitors of apoptosis (IAPs) regulate intestinal immunity and inflammatory bowel disease (IBD) inflammation. Trends Mol Med 2014; 20: [PMID: DOI: / j.molmed ] 2 Gothe F, Beigel F, Rust C, Hajji M, Koletzko S, Freudenberg F. Bile acid malabsorption assessed by 7 alpha-hydroxy-4-cholesten- 3-one in pediatric inflammatory bowel disease: correlation to clinical and laboratory findings. J Crohns Colitis 2014; 8: [PMID: DOI: /j.crohns ] 3 Xavier RJ, Podolsky DK. Unravelling the pathogenesis of inflammatory bowel disease. Nature 2007; 448: [PMID: DOI: /nature06005] 4 Mascaraque C, González R, Suárez MD, Zarzuelo A, Sánchez de Medina F, Martínez-Augustin O. Intestinal anti-inflammatory activity of apigenin K in two rat colitis models induced by trinitrobenzenesulfonic acid and dextran sulphate sodium. Br J Nutr 2015; 113: [PMID: DOI: /S ] 5 Li TT, Zhang JF, Fei SJ, Zhu SP, Zhu JZ, Qiao X, Liu ZB. Glutamate microinjection into the hypothalamic paraventricular nucleus attenuates ulcerative colitis in rats. Acta Pharmacol Sin 2014; 35: [PMID: DOI: /aps ] 6 Wang T, Zhou YT, Chen XN, Zhu AX, Wu BH. Remote ischemic postconditioning protects against gastric mucosal lesions in rats. World J Gastroenterol 2014; 20: [PMID: DOI: /wjg.v20.i ] 7 Bonamin F, Moraes TM, Dos Santos RC, Kushima H, Faria FM, Silva MA, Junior IV, Nogueira L, Bauab TM, Souza Brito AR, da Rocha LR, Hiruma-Lima CA. The effect of a minor constituent of essential oil from Citrus aurantium: the role of β-myrcene in preventing peptic ulcer disease. Chem Biol Interact 2014; 212: [PMID: DOI: /j.cbi ] 8 Radley JJ, Sawchenko PE. Evidence for involvement of a limbic paraventricular hypothalamic inhibitory network in hypothalamicpituitary-adrenal axis adaptations to repeated stress. J Comp Neurol 2015; 523: [PMID: DOI: /cne.23815] 9 Shi Z, Li B, Brooks VL. Role of the Paraventricular Nucleus of the Hypothalamus in the Sympathoexcitatory Effects of Leptin. Hypertension 2015; 66: [PMID: DOI: /HYPERTENSIONAHA ] 10 Samuelsson AM. New perspectives on the origin of hypertension; the role of the hypothalamic melanocortin system. Exp Physiol 2014; 99: [PMID: DOI: /expphysiol ] 11 Ong ZY, Alhadeff AL, Grill HJ. Medial nucleus tractus solitarius oxytocin receptor signaling and food intake control: the role of gastrointestinal satiation signal processing. Am J Physiol Regul Integr Comp Physiol 2015; 308: R800-R806 [PMID: DOI: /ajpregu ] 12 Gao L, Zhu T, Xie G, Lou X, Li S, Zhou Y, Deng Z, Chu D, Lou J, Du D. GABA(A) receptor overexpression in the lateral hypothalamic area attenuates gastric ischemia reperfusion injury in rats. Mol Med Rep 2015; 11: [PMID: DOI: /mmr ] 13 Huber MJ, Basu R, Cecchettini C, Cuadra AE, Chen QH, Shan Z. Activation of the (pro)renin receptor in the paraventricular nucleus increases sympathetic outflow in anesthetized rats. Am J Physiol Heart Circ Physiol 2015; 309: H880-H887 [PMID: DOI: /ajpheart ] 14 Hundorfean G, Neurath MF, Mudter J. Functional relevance of T helper 17 (Th17) cells and the IL-17 cytokine family in inflammatory bowel disease. Inflamm Bowel Dis 2012; 18: [PMID: DOI: /ibd.21677] 15 Imaeda H, Takahashi K, Fujimoto T, Kasumi E, Ban H, Bamba S, Sonoda H, Shimizu T, Fujiyama Y, Andoh A. Epithelial expression of interleukin-37b in inflammatory bowel disease. Clin Exp Immunol 2013; 172: [PMID: DOI: /cei.12061] 16 Pearl DS, Shah K, Whittaker MA, Nitch-Smith H, Brown JF, Shute JK, Trebble TM. Cytokine mucosal expression in ulcerative colitis, the relationship between cytokine release and disease activity. J Crohns Colitis 2013; 7: [PMID: DOI: /j.crohns ] 17 Rodríguez-Perálvarez ML, García-Sánchez V, Villar-Pastor CM, González R, Iglesias-Flores E, Muntane J, Gómez-Camacho F. Role of serum cytokine profile in ulcerative colitis assessment. Inflamm Bowel Dis 2012; 18: [PMID: DOI: /ibd.22865] 18 Lipinski S, Bremer L, Lammers T, Thieme F, Schreiber S, Rosenstiel P. Coagulation and inflammation. Molecular insights and diagnostic implications. Hamostaseologie 2011; 31: , 104 [PMID: DOI: /ha-1134] 19 Hayashi Y, Narumi K, Tsuji S, Tsubokawa T, Nakaya MA, Wakayama T, Zuka M, Ohshima T, Yamagishi M, Okada T. Impact of adrenomedullin on dextran sulfate sodium-induced inflammatory colitis in mice: insights from in vitro and in vivo experimental studies. Int J Colorectal Dis 2011; 26: [PMID: DOI: /s ] 20 Ballal SA, Veiga P, Fenn K, Michaud M, Kim JH, Gallini CA, Glickman JN, Quéré G, Garault P, Béal C, Derrien M, Courtin P, Kulakauskas S, Chapot-Chartier MP, van Hylckama Vlieg J, Garrett WS. Host lysozyme-mediated lysis of Lactococcus lactis facilitates delivery of colitis-attenuating superoxide dismutase to inflamed colons. Proc Natl Acad Sci USA 2015; 112: [PMID: DOI: /pnas ] 21 Wang C, Han Z. Ginkgo Biloba Extract Enhances Differentiation and Performance of Neural Stem Cells in Mouse Cochlea. Cell Mol Neurobiol 2015; 35: [PMID: DOI: / s z] 22 Grimstad T, Bjørndal B, Cacabelos D, Aasprong OG, Janssen EA, Omdal R, Svardal A, Hausken T, Bohov P, Portero-Otin M, Pamplona R, Berge RK. Dietary supplementation of krill oil attenuates inflammation and oxidative stress in experimental ulcerative colitis in rats. Scand J Gastroenterol 2012; 47: [PMID: DOI: / ] 23 Bank S, Skytt Andersen P, Burisch J, Pedersen N, Roug S, Galsgaard J, Ydegaard Turino S, Brodersen JB, Rashid S, Kaiser Rasmussen B, Avlund S, Bastholm Olesen T, Jürgen Hoffmann H, Kragh Thomsen M, Ostergaard Thomsen V, Frydenberg M, 3775 April 14, 2016 Volume 22 Issue 14
90 Deng QJ et al. Hypothalamic PVN stimulation reduces intestinal injury Andersen Nexø B, Sode J, Vogel U, Andersen V. Polymorphisms in the inflammatory pathway genes TLR2, TLR4, TLR9, LY96, NFKBIA, NFKB1, TNFA, TNFRSF1A, IL6R, IL10, IL23R, PTPN22, and PPARG are associated with susceptibility of inflammatory bowel disease in a Danish cohort. PLoS One 2014; 9: e98815 [PMID: DOI: /journal.pone ] 24 Büning C, von Kraft C, Hermsdorf M, Gentz E, Wirth EK, Valentini L, Haas V. Visceral Adipose Tissue in Patients with Crohn s Disease Correlates with Disease Activity, Inflammatory Markers, and Outcome. Inflamm Bowel Dis 2015; 21: [PMID: DOI: /MIB ] 25 Stallhofer J, Friedrich M, Konrad-Zerna A, Wetzke M, Lohse P, Glas J, Tillack-Schreiber C, Schnitzler F, Beigel F, Brand S. Lipocalin-2 Is a Disease Activity Marker in Inflammatory Bowel Disease Regulated by IL-17A, IL-22, and TNF-α and Modulated by IL23R Genotype Status. Inflamm Bowel Dis 2015; 21: [PMID: DOI: /MIB ] 26 Franzè E, Monteleone I, Cupi ML, Mancia P, Caprioli F, Marafini I, Colantoni A, Ortenzi A, Laudisi F, Sica G, Sileri P, Pallone F, Monteleone G. Interleukin-34 sustains inflammatory pathways in the gut. Clin Sci (Lond) 2015; 129: [PMID: DOI: /CS ] 27 Ramonaite R, Skieceviciene J, Kiudelis G, Jonaitis L, Tamelis A, Cizas P, Borutaite V, Kupcinskas L. Influence of NADPH oxidase on inflammatory response in primary intestinal epithelial cells in patients with ulcerative colitis. BMC Gastroenterol 2013; 13: 159 [PMID: DOI: / X ] 28 Leucht K, Caj M, Fried M, Rogler G, Hausmann M. Impaired removal of Vβ8(+) lymphocytes aggravates colitis in mice deficient for B cell lymphoma-2-interacting mediator of cell death (Bim). Clin Exp Immunol 2013; 173: [PMID: DOI: /cei.12137] 29 Zhao QJ, Yu YB, Zuo XL, Dong YY, Li YQ. Milk fat globuleepidermal growth factor 8 is decreased in intestinal epithelium of ulcerative colitis patients and thereby causes increased apoptosis and impaired wound healing. Mol Med 2012; 18: [PMID: DOI: /molmed ] 30 Schwarte LA, Schwartges I, Scheeren TW, Schober P, Picker O. The differential effects of recombinant brain natriuretic peptide, nitroglycerine and dihydralazine on systemic oxygen delivery and gastric mucosal microvascular oxygenation in dogs. Anaesthesia 2012; 67: [PMID: DOI: / j x] 31 Sanderson TH, Reynolds CA, Kumar R, Przyklenk K, Hüttemann M. Molecular mechanisms of ischemia-reperfusion injury in brain: pivotal role of the mitochondrial membrane potential in reactive oxygen species generation. Mol Neurobiol 2013; 47: 9-23 [PMID: DOI: /s z] P- Reviewer: Imai K, Shimizu Y, Sumi K S- Editor: Ma YJ L- Editor: Wang TQ E- Editor: Ma S 3776 April 14, 2016 Volume 22 Issue 14
91 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Case Control Study ORIGINAL ARTICLE Multi-locus genetic risk score predicts risk for Crohn s disease in Slovenian population Katarina Zupančič, Kristijan Skok, Katja Repnik, Rinse K Weersma, Uroš Potočnik, Pavel Skok Katarina Zupančič, Kristijan Skok, Katja Repnik, Uroš Potočnik, Center for Human Genetics and Pharmacogenomics, Medical Faculty of Maribor, University of Maribor, 2000 Maribor, Slovenia Rinse K Weersma, Department of Gastroenterology and Hepatology, University of Groningen and University Medical Center Groningen, 9700 Groningen, The Netherlands Pavel Skok, Department of Gastroenterology, University Medical Center, 2000 Maribor, Slovenia Pavel Skok, Slovenia and Medical Faculty of Maribor, University of Maribor, 2000 Maribor, Slovenia Author contributions: Zupančič K and Skok K contributed equally to this work; Zupančič K, Skok K and Potočnik U designed the research; Zupančič K, Skok K and Repnik K performed the research; Zupančič K, Skok K and Skok P analyzed the data; Weersma RK contributed new data and analytic methods; Zupančič K, Skok K, Potočnik U and Skok P wrote the paper; Potočnik U, Repnik K and Skok P revised the article. Institutional review board statement: The study was approved by the Slovenian National Committee for Medical Ethics (KME 80/10/ 07, 21p / 12/ 07 and 106/05/11). Informed consent statement: All patients gave informed consent. Conflict-of-interest statement: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. Data sharing statement: Technical appendix, statistical code, and dataset available from the corresponding author at pavel. skok@guest.arnes.si. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Pavel Skok, MD, PhD, Full Professor, Department of Gastroenterology, University Medical Center, Ljubljanska ulica 5, 2000 Maribor, Slovenia. pavel.skok@guest.arnes.si Telephone: Fax: Received: January 16, 2016 Peer-review started: January 18, 2016 First decision: February 18, 2016 Revised: March 1, 2016 Accepted: March 13, 2016 Article in press: March 14, 2016 Published online: April 14, 2016 Abstract AIM: To develop a risk model for Crohn s disease (CD) based on homogeneous population. METHODS: In our study were included 160 CD patients and 209 healthy individuals from Slovenia. The association study was performed for 112 single nucleotide polymorphisms (SNPs). We generated genetic risk scores (GRS) based on the number of risk alleles using weighted additive model. Discriminatory accuracy was measured by area under ROC curve (AUC). For risk evaluation, we divided individuals according to positive and negative likelihood ratios (LR) of a test, with LR > 5 for high risk group and LR < 0.20 for low risk group. RESULTS: The highest accuracy, AUC of 0.78 was achieved with GRS combining 33 SNPs with optimal sensitivity and specificity of 75.0% and 72.7%, respectively. Individuals with the highest risk (GRS > 3777 April 14, 2016 Volume 22 Issue 14
92 Zupančič K et al. Predictive risk score for Crohn patients 5.54) showed significantly increased odds of developing CD (OR = 26.65, 95%CI: ) compared to the individuals with the lowest risk (GRS < 4.57) which is a considerably greater risk captured than in one SNP with the highest effect size (OR = 3.24). When more than 33 SNPs were included in GRS, discriminatory ability was not improved significantly; AUC of all 74 SNPs was CONCLUSION: The authors proved the possibility of building accurate genetic risk score based on 33 risk variants on Slovenian CD patients which may serve as a screening tool in the targeted population. Key words: Inflammatory bowel disease; Crohn s disease; discriminatory accuracy; genetic risk score; Single nucleotide polymorphisms The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Genome wide association studies have provided a comprehensive catalogue of susceptibility inflammatory bowel disease (IBD) loci, which now present an important basis for genetic risk prediction. We aimed to develop an accurate Crohn s disease (CD) risk prediction model for the Slovenian cohort. The most optimal 33 SNPs model showed good discriminatory ability, which may be useful for risk stratification in targeted population (gastrointestinal disturbances, positive family history). Individuals in the highest risk group have 27-fold higher odds for CD risk compared to individuals in the lowest risk group. To the best of our knowledge, this is the first population specific genetic prediction based on recently established IBD loci. Zupančič K, Skok K, Repnik K, Weersma RK, Potočnik U, Skok P. Multi-locus genetic risk score predicts risk for Crohn s disease in Slovenian population. World J Gastroenterol 2016; 22(14): Available from: URL: com/ /full/v22/i14/3777.htm DOI: org/ /wjg.v22.i INTRODUCTION Crohn s disease (CD) is a multifactorial chronic inflammatory bowel disease (IBD) caused by dysregulated immune response to commensal intestinal microflora in genetically susceptible individuals [1]. CD can affect any segment of the gastrointestinal tract and has a relapsing-remitting course with various patterns of behavior [2,3]. Prevalence and incidence of CD increased significantly over the last decades in developed parts of the world and ranges from 136 to 319 per and from 6 to 29 per , respectively, indicating its emergence as a global disease [4]. Genome-wide association studies (GWASs) have provided valuable insight into the genetic architecture of CD, thus helping us better understand the mechanisms of innate immunity (NOD2), mucosal integrity (IBD5), autophagy (ATG16L1, IRGM), lymphocyte differentiation and proliferation (IL23R, STAT3) [5-7]. Recent meta-analysis of data from 15 existing GWASs and an independent genotype set obtained from DNA microarray (Immunochip) enrolled IBD cases and controls from International Inflammatory Bowel Diseases Genetic Consortium (IIBDGC) and identified 71 novel variants for a total of 163 IBD loci. Of these loci, 110 conferred risk to both IBD subtypes, whereas 30 were unique to CD [8]. Several studies have investigated risk prediction for CD [9-12]. In CD the strongest known association is with the NOD2 gene, which was for some time considered to be a possible candidate for genetic screening but ultimately has not been accepted [an area under ROC curve (AUC) of 0.56], because individual markers have small effect on risk and thus have poor predictive ability [13]. In addition, inclusion of only highly significant common variants with strong effect sizes (NOD2, IL23R, ATG16L1, IRGM) into a predictive model managed to improve predictive power but it was still insufficient for accurate prediction (AUC of 0.66) [10]. In recent studies, polygenic genetic risk scores (GRS) have been used to summarize riskassociated alleles, weighted by their effect sizes (odds ratios) among an assemble of markers that do not individually achieve significance in association study since it has been suggested that a higher number of included variants with weak to moderate effect sizes can explain larger proportion of heritability [5,14]. Recently established 163 IBD loci now provide an important basis for genetic risk prediction. Attempts have been made to develop accurate genetic risk profiles based on a large number of patients from several population heterogeneous cohorts that were enrolled in IIBDGC [15]. However, limited data exist on developing genetic risk profiles in a single genetically homogeneous population. We aimed to test the joint contribution of wellestablished susceptibility loci, obtained from custom designed single nucleotide polimorphism (SNP) genotyping chip Immunochip (ichip) [8], in order to construct accurate risk prediction for Slovenian CD patients. MATERIALS AND METHODS Cases and controls Study population consisted of 236 healthy individuals in the control group and 202 CD patients from the University Medical Center Ljubljana and Maribor as described previously [16]. All CD patients had reliable clinically and histopathologically confirmed disease. The study was approved by Slovenian National Committee for Medical Ethics (KME 80/10/07, 21p/12/07 and KME 106/05/11). Patients gave informed consent prior to inclusion in the study and the study was performed 3778 April 14, 2016 Volume 22 Issue 14
93 Zupančič K et al. Predictive risk score for Crohn patients in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki). SNP selection Genotyping data for cases and controls was obtained from the ichip, where Slovenian patients and controls were enrolled within the IIBDGC. Genotyping for initial 236 controls and 202 CD patients was performed with hybridization on ichip according to protocol (Illumina). Rigorous quality control of the study group (gender matching, call rate, family ties and genetic origin verification) and genotyping information [Hardy- Weinberg equilibrium (HWE)] was applied in PLINK v1.07 and R. Individuals with more than 10% missing genotypes were excluded. SNPs with a call rate below 90% were discarded from further analyses. We also excluded SNPs when the controls showed deviation from HWE with a P < in control group. The remaining 160 CD patients, 209 controls, and 112 SNPs from a total of 163 SNPs were included in further statistical analysis. Statistical analysis The case-control association analysis of allele frequencies was statistically assessed in SPSS 22.0 (IBM Corp., Armonk, NY) using Fischer exact test and χ 2. The results were presented as P-values, OR and 95%CI. We compared risk alleles and their frequencies to those in meta-analysis study by Jostins et al [8] and included only those SNPs from a total of 112 SNPs that showed association of risk allele with Slovenian CD patients risk allele. Statistical significant threshold (P-value) was at 0.05 and after Bonferroni correction for multiple testing. Genetic risk profiles construction We constructed GRS in an additive manner using a weighted approach. The number of risk alleles at each locus (2, 1, 0) was multiplied by their corresponding beta-coefficients of effects sizes [log(or)] and then summed up in GRS that each individual carried. In order to avoid bias we used ORs from recent metaanalysis by Jostins et al [8]. For optimal risk construction, we used a ranking P-values approach, starting with SNP with the lowest P-value and gradually adding one per one in GRS [17]. The most optimal GRS was then compared to GRS of the remaining SNPs, to GRS of marginally significant SNPs with highest OR and to GRS of all included SNPs. ROC with AUC were used to measure discriminatory accuracy at various GRS cut-offs (sensitivity/1- specificity). An area of an AUC < 0.7 represents poor discrimination; acceptable (fair) discrimination, and excellent discrimination [18]. Cut-off values for sensitivities, specificities, positive/negative predictive values and positive/negative likelihood ratios were computed in Medcalc Likelihood ratio (LR) describes how likely an affected person is going to have a disease compared to a healthy person with the same result according to a given test (positive or negative). A positive LR above 5 is considered to be a moderate evidence to confirm a disease, LR above 10 strongly confirms a disease, whereas a negative LR below 0.2 is considered moderate, and below 0.1 strong evidence to exclude disease. LR are powerful tools for GRS evaluation since they are not affected by a prevalence and with prior probability (prevalence) they present a basis for post-test probability (predictive value - PV) calculation [19]. Positive PV presents the probability of patient having a disease if the test is positive, while the opposite is true for a negative PV [20]. For post-test probabilities estimations, we used prevalence of disease 1.2/1000, since there are approximately CD patients in Slovenia. Statistical analysis of distribution (normal, nonparametric) of selected parameters (GRS, allele frequencies, OR, United States) between cases and controls, and between different GRS models was conducted with Shapiro-Wilk test in SPSS t-test or rank-sum test (Mann-Whitney) were used according to distribution. RESULTS Association analysis We found that risk alleles frequencies of 74 SNPs (66%) matched with those in the reference study by Jostins et al [8]. The risk alleles of remaining 38 SNPs were in the opposite direction and therefore we excluded them from further analysis (Supplement Table 1). This was to be expected since our case-control group was too small to achieve sufficient statistical power comparing to cases and controls enrolled in IIBDGC [8]. In present study, we initially confirmed 15 statistically significant associations (for dominant, recessive, allelic model) from a total of 74 SNPs; among these 15 significant associations, only 8 SNPs were statistically significant under allelic model (Supplement Table 1). None of them remained significant (P < ) after Bonferroni correction. Genetic risk profiles We used the ranking P-value method for GRS construction as described in the methods section. For individual SNPs, AUC ranged from 0.50 to 0.57 (median 0.53) for SNPs with the lowest effects sizes versus SNPs with the highest effect sizes, respectively, but the difference between these two most distant AUC values was not significant (P = 0.06). Significantly better (P < 10-4 ) discriminatory ability than in an individual marker was achieved when 8 nominally significant SNPs (P < 0.05) were included in a model with AUC of 0.69 (95%CI: ). Their ORs ranged from 1.42 to 3.24 (median 1.50). The most optimal GRS was achieved with 33 SNPs model with AUC of 0.78 (95%CI: ) and ORs ranging from 1.15 to 3779 April 14, 2016 Volume 22 Issue 14
94 Zupančič K et al. Predictive risk score for Crohn patients Table 1 Genetic risk profile based on the genetic risk score in 33 single nucleotide polymorphisms model GRS Sensitivity Specificity +LR -LR +PV -PV +PV 1 -PV 1 > % 19.62% % % 11.94% 98.95% > % 34.45% % 99.98% 13.63% 97.83% > % 72.73% % 99.96% 23.41% 96.32% > % 93.30% % 99.92% 37.14% 92.88% > % 99.04% % 99.89% 53.65% 90.83% > % 99.52% % 99.89% 59.13% 90.53% 1 PV-positive and negative predictive value for estimated prevalence of CD in targeted population with high risk (10%). LR-positive and negative likelihood ratio, PV-positive and negative predictive value for estimated prevalence of CD in Slovenian population (0.12%). GRS: Genetic risk scores; CD: Crohn s disease; LR: Likelihood ratios; PV: Predictive value AUC for different P -values thresholds 0.75 AUC SNP (P = 0.005) 8 SNPs (P < 0.05) 17 SNPs (P < 0.10) 29 SNPs (P < 0.20) 33 SNPs (P 0.26)* 34 SNPs (P < 0.30) 38 SNPs (P < 0.40) 43 SNPs (P < 0.50) 52 SNPs (P < 0.60) 55 SNPs (P < 0.70) 60 SNPs (P < 0.80) 68 SNPs (P < 0.90) 74 SNPs (P < 1.00) Figure 1 Area under curve for different P-values thresholds and corresponding numbers of included single nucleotide polymorphisms. The most optimal AUC was achieved with GRS of 33 risk alleles (AUC of 0.78) at P-value threshold of (marked with *). Adding 41 SNPs to GRS did not improve GRS significantly, however it presented needless background noise. AUC: Area under curve; GRS: Genetic risk scores; SNPs: Single nucleotide polymorphisms (median 1.32). It performed significantly better (P = ) than the 8 SNPs model, although the 8 SNPs model had higher ORs median (P = ). Interestingly, mean risk allele frequencies (RAF) of included SNPs did not differ significantly between 8 SNPs and 33 SNPs risk models (P = 0.110). When more than 33 SNPs were included in GRS (Figure 1), discriminatory ability was not improved significantly; AUC of all 74 SNPs was These additional SNPs present needless background noise. To confirm this, we also tested accuracy of the remaining 41 SNPs, which achieved poor performance with AUC of 0.58 (95%CI: ) and this value is similar to an accuracy of an individual SNP. The 41 SNPs model accuracy and median of ORs (ranging from 1.00 to 1.85; median 1.11) of SNPs were significantly lower than in the aforementioned 33 SNPs model (P < 10-4 ). RAF of the included SNPs did not differ significantly between these two models (P = 0.288). Evaluation of 33 SNPs genetic risk model We presented the applicability of GRS in context of pre-test (prevalence), LR, and corresponding post-test probability of target population for two different prior probabilities (general population, high-risk population) (Table 1). Due to the low CD prevalence (0.12%) only up to 1.5% of population would be correctly confirmed as diseased. On the contrary, high-risk individuals (positive family history, gastrointestinal disturbances) with estimated pre-test probability of 10% have up to 59.1% higher probabilities of having the disease if they test positive. To evaluate risk between individuals in our study, we divided them into three risk groups according to optimal positive and negative LRs at corresponding GRS cut-offs. LR are powerful tools for model evaluation, since they do not depend on prevalence (for further readings see Methods). The high-risk group included individuals who tested above GRS cut-off 5.54 (positive LR > 5.0). The intermediate group (grey zone) included individuals with GRS between 4.57 and 5.54 and the low risk group included individuals who tested below GRS cut-off 4.57 (negative LR < 0.20). The results showed that the odds of developing CD (OR = 26.65, 95%CI: ) were significantly increased in individuals in the highest risk group compared to individuals in the lowest risk group (Table 2). Since the majority of the tested individuals fall into the grey zone category (intermediate risk group) (Figure 2) it would be useful to further stratify 3780 April 14, 2016 Volume 22 Issue 14
95 Zupančič K et al. Predictive risk score for Crohn patients Table 2 Comparison of risk in different groups of individuals Group OR P value 95%CI High vs low risk < High vs intermediate risk 4.06 < Intermediate vs low risk 5.13 < High-risk group: GRS > 5.54; Intermediate risk group: 4.57 < GRS 5.54; low risk group: GRS GRS: Genetic risk scores. 40% 100 tested subjects 10 diseased subjects 90 healthy subjects 8 true positives 2 false negatives 65 true negatives 25 false positives Percentage of individuals 35% 30% 25% 20% 15% 10% 5% 0% < Genetic risk score these individuals. According to the best trade-off between sensitivity and specificity we can set GRS cut-off at 5.05 (sensitivity 75.0%, specificity 72.7%, +LR 2.45), where in high risk population 23.4% subjects will be identified as diseased if they are tested positive (Figure 3). Individuals, who test below the cut-off 5.05, have a high probability of 96.5% that they are not affected. Moderately better risk stratification (+LR > 5, high risk group) can be achieved by setting the threshold to GRS cut-off 5.54 with specificity of 93.3% but at expense of higher number of false negatives (sensitivity of 35.6%) (Figure 4). By setting the threshold even higher (GRS > 5.80) it is possible to yield positive LR greater than 10% and 53.7% individuals will be classified as diseased. More precise CD exclusion can be achieved with lower GRS cut-off (< 4.57), where we can rule out non-diseased individuals with a sensitivity of 93.12% and a negative PV of 97.8% but at an expense of having more false positives (specificity of 34.65%). DISCUSSION CD% CON% Figure 2 Distribution of Genetic risk scores in Crohn s disease and controls. GRS is normally distributed (Shapiro-Wilk, P > 0.05) in CD cases and controls. Cases have significantly higher GRS (5.32 ± 0.47) than controls (4.78 ± 0.53); P < CD: Crohn s disease; GRS: Genetic risk scores. In our study, we developed an accurate CD risk prediction model for Slovenian cohort. To the best of our knowledge, this is the first population specific genetic prediction based on recently established IBD loci. The most optimal 33 SNPs model showed Figure 3 Flow diagram for sensitivity (75%) and specificity (72.7%) in targeted population (Crohn s disease prevalence 10%). If we test 100 subjects and set the cut-off at 5.05, 32 of them will test positive (above cut-off), with post-test probability of disease approximately 24% (8/33). 100 tested subjects 10 diseased subjects 90 healthy subjects 4 true positives 6 false negatives 84 true negatives 6 false positives Figure 4 Flow diagram for sensitivity (35.6%) and specificity (93.3%) in targeted population (Crohn s disease prevalence 10%). If we test 100 subjects and set the cut-off at 5.54, 10 of them will test positive (above cut-off), with post-test probability of disease approximately 40% (4/10). good discriminatory ability (AUC of 0.78), which may be useful for risk stratification in targeted population. Individuals in the highest risk group (GRS > 5.54) have 27-fold higher OR for CD risk compared to individuals in the lowest risk group (GRS 4.57). This is considerably greater risk captured than in individual SNP with the highest effect size (IL23R, OR = 3.24). The highest discriminatory ability of individual SNPs yielded only 0.57 at best, which support findings from study by Jakobsdottir et al [10], that individual markers are poor classifiers even with replicated high effect sizes. According to literature, genetic risk prediction in CD using common risk loci ranges from AUC of 0.56 to 0.72 [10-12]. Recently it has been suggested that robust machine-learning techniques using large sample sizes and wider variant spectrum (including risk allele frequencies less than 0.05) in low linkage disequilibrium importantly improves risk prediction in CD to an AUC greater than 0.85 [15,17]. Theoretically, given its high heritability (not accounting the low prevalence of CD), it is possible to achieve AUC up to 0.98 if all CD risk loci have been identified and effect sizes are accurately measured [21,22]. However, these studies are technologically complex and are mostly based on 3781 April 14, 2016 Volume 22 Issue 14
96 Zupančič K et al. Predictive risk score for Crohn patients simulation data and/or require large and heterogeneous patients cohorts data which is not always available. In our study, in order to avoid methodologic complexity, we used a simplified P-value ranking approach to determine optimal number of SNPs, as already described in Methods [17]. Studies have shown that Europe is genetically and ethnically diverse. Genetic differentiation exists not only between the northwest and southeast part of the continent but also within these two distinct groups, creating indispensable inter-population differences [23,24]. In this case SNPs may serve as proxies for shared environments that can differ from population to population. This may be due to interference of different factors modifying genetic architecture (geographical placement, pollutants, adherence to particular diet, etc.) [25]. Therefore, population specific risk profiles may offer a more accurate risk estimation for the selected population, which was one of the main reasons why we included the small homogeneous Slovenian cohort [26]. A genetic risk model may be primarily useful for screening purposes in a population with higher prior probabilities of CD; prolonged gastrointestinal disturbances suggestive of CD (abdominal pain, diarrhea, weight loss) and/or positive family history to identify at-risk individuals for further more invasive diagnostic procedures. In addition to sufficiently high prevalence, a risk prediction model also needs to be sensitive and specific with considerably high positive and negative likelihood ratios and cost efficient (as few markers as possible) [19,20,27]. The prevalence of CD in patients with one affected first-degree relative ranges from 2.2% to 16.2% [28]. For Slovenia, there is currently no accurate data for family history in CD patients available, however it has been clinically estimated that around 10% of CD patients have one affected first-degree relative. In this case, positive post-test probability rises up to 59.1% compared to general population, where positive post-test probability due to low CD prevalence yields only 1.5% at best. According to our results, the most optimal cut-off was at GRS > 5.05 with sensitivity of 75.0% and specificity of 72.7%. By raising cut-off to a higher GRS > 5.54 it is possible to stratify at-risk individuals even more precisely with a specificity of 93.3% but at expense of lower sensitivity (35.6%) and therefore a higher number of false negatives. However, due to small number of individuals who test positive (Figure 4) it may be more costeffective and practical than setting cut-off to a lower GRS. For comparison, prostate-specific antigen test yields similar results with sensitivity and specificity of 20.5% and 93.6%, respectively and is widely used in screening for prostate cancer [29]. To compare risks between high and low risk group, GRS of individuals are usually divided into quartiles or quintiles. However, this approach may be too rigid and therefore may not present all true observations of the series [18]. We thereby propose a more suitable approach, by using test likelihood ratios, which are powerful tools for the GRS evaluation [19]. In our case we divided individuals into three groups according to moderate increase in likelihood of disease (+LR > 5.0; -LR < 0.20) because of a better trade-off between sensitivity and specificity (less false negatives). Individuals in the highest risk group had 27-fold higher OR for CD risk compared to individuals in the lowest risk group. Similar results with high OR between risk groups were presented in rheumatoid arthritis GRS study by Yarwood et al [27] (OR = 27.13), and in psoriasis GRS study by Yin et al [30] (OR = 28.20) but they used quintiles and quartiles, respectively. Since LR higher than 10 is largely conclusive for disease, in our case it is possible to yield even 55-fold higher OR for CD risk compared to individuals, but at expense of higher number of false negatives (sensitivity 10%). Our results also highlight the importance of testing published SNPs in population cohort before building models. For example, when all 112 SNP were included in the model we achieved an AUC of only 0.64, since risk alleles were labelled according to reference study by Jostins et al [8] and 38 were in the opposite directions than those in the reference study. It has been suggested that including a higher number of risk variants with weak to moderate effect sizes, that were not all significant in the association study, can improve risk prediction on account of explaining larger proportion of heritability [14,31]. Interestingly, when additional 41 SNPs with weak ORs were included to the model of 33 SNPs the discriminatory ability did not improve significantly. In our case, these SNPs actually present only a background noise and are therefore cost redundant. The discriminatory accuracy of 41 SNPs was in fact similar to an accuracy of an individual SNP, which represents a poor classifier (no better than a chance). Therefore, a cluster of higher numbers of non-significant variants with very weak effect sizes may also explain only a minor proportion of genetic variance in complex diseases (the same as individual SNP). Currently, 163 IBD loci accounts for 13.6% of total CD heritability [8]. Future discovery of rare variants with lower frequencies and high effect sizes through robust gene-mapping studies (nextgeneration sequencing) could lead to improvement of missing heritability and to more accurate genetic risk prediction [22,31]. A limitation of our study is a small number of CD patients and controls. Therefore, results may be biased due to over-fitting and should be validated on a larger case-control sample size. Furthermore, we analyzed only common risk loci from ichip, which were strongly confirmed on a large IIBDGC heterogeneous cohort thus balancing out possible inter-population genetic variations. It would be interesting to test, if other variants which have not reached genome-wide levels of significance could improve our population specific risk prediction. And lastly, we used additive model which does not account for possible gene-gene interactions. In conclusion, to the best of our knowledge, this is 3782 April 14, 2016 Volume 22 Issue 14
97 Zupančič K et al. Predictive risk score for Crohn patients the first population specific study developing predictive models after the 163 IBD SNPs have been discovered [8]. Population specific genetic models may offer more optimal risk stratification for selected population than ethnically and genetically diverse consortiums. In our study we presented real issues of small populations, a simpler methodology approach with ranking P-values and a comprehensible transition to clinical scenario. ACKNOWLEDGMENTS The authors thank Koder S, PhD, for part of the samples, which were used in the study. COMMENTS Background To date genome-wide association studies (GWAs) have identified more than 160 loci in the human genome that contribute to the development of inflammatory bowel disease (IBD). Multi-locus profiles of genetic risk can be used to translate discoveries from GWAs into tools for population health research, such as development of accurate risk profiles for genetic risk prediction. Research frontiers Attempts to develop reliable and accurate genetic risk profiles have been made on a large number of patients from several population heterogeneous cohorts. However, limited data exists on developing genetic risk profiles in a single genetically homogeneous population. Innovations and breakthroughs To the best of our knowledge, the authors performed one of the first population specific genetic prediction studies based on recently established IBD associated loci. their results suggest that it is possible to construct a genetic risk model with good discriminatory ability on a homogenous population cohort. The model may be useful for stratifying individuals at higher risk of developing Crohn s disease (CD). Applications The genetic risk model may serve as a screening tool in a targeted population with higher risk (gastrointestinal disturbances, positive family history) to develop disease. Similar studies may be performed for other smaller cohorts in order to further improve their population specific genetic risk prediction. Terminology Immunochip is an Illumina Infinium single-nucleotide polymorphism (SNP) microarray that includes momentarily approx., SNPs relevant to multiple different immune-mediated diseases including CD and ulcerative colitis. This chip provides a powerful tool for immunogenetics gene mapping. Peer-review The present work has originality. The research study on genetic risk predictor for CD using a reasonable number of SNPs has merits and the only shortcoming is sample size, which was very small. However, the sample population is homogeneous, thus attenuating the effects of the small sample size. The methodology used is adequate and the discussion is consistent. Therefore, the work deserves to be published. REFERENCES 1 Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis of inflammatory bowel disease. Nature 2011; 474: [PMID: DOI: /nature10209] 2 Ellinghaus D, Bethune J, Petersen BS, Franke A. The genetics of Crohn s disease and ulcerative colitis--status quo and beyond. Scand J Gastroenterol 2015; 50: [PMID: DOI: / ] 3 Dykes DM, Towbin AJ, Bonkowski E, Chalk C, Bezold R, Lake K, Kim MO, Heubi JE, Trapnell BC, Podberesky DJ, Denson LA. Increased prevalence of luminal narrowing and stricturing identified by enterography in pediatric Crohn s disease patients with elevated granulocyte-macrophage colony stimulating factor autoantibodies. Inflamm Bowel Dis 2013; 19: [PMID: DOI: /MIB.0b013e e0] 4 Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012; 142: e42; quiz e30 [PMID: DOI: /j.gastro ] 5 McGovern DP, Kugathasan S, Cho JH. Genetics of Inflammatory Bowel Diseases. Gastroenterology 2015; 149: e2 [PMID: DOI: /j.gastro ] 6 Van Limbergen J, Radford-Smith G, Satsangi J. Advances in IBD genetics. Nat Rev Gastroenterol Hepatol 2014; 11: [PMID: DOI: /nrgastro ] 7 Tsianos EV, Katsanos KH, Tsianos VE. Role of genetics in the diagnosis and prognosis of Crohn s disease. World J Gastroenterol 2011; 17: [PMID: DOI: /wjg.v17. i ] 8 Jostins L, Ripke S, Weersma RK, Duerr RH, McGovern DP, Hui KY, Lee JC, Schumm LP, Sharma Y, Anderson CA, Essers J, Mitrovic M, Ning K, Cleynen I, Theatre E, Spain SL, Raychaudhuri S, Goyette P, Wei Z, Abraham C, Achkar JP, Ahmad T, Amininejad L, Ananthakrishnan AN, Andersen V, Andrews JM, Baidoo L, Balschun T, Bampton PA, Bitton A, Boucher G, Brand S, Büning C, Cohain A, Cichon S, D Amato M, De Jong D, Devaney KL, Dubinsky M, Edwards C, Ellinghaus D, Ferguson LR, Franchimont D, Fransen K, Gearry R, Georges M, Gieger C, Glas J, Haritunians T, Hart A, Hawkey C, Hedl M, Hu X, Karlsen TH, Kupcinskas L, Kugathasan S, Latiano A, Laukens D, Lawrance IC, Lees CW, Louis E, Mahy G, Mansfield J, Morgan AR, Mowat C, Newman W, Palmieri O, Ponsioen CY, Potocnik U, Prescott NJ, Regueiro M, Rotter JI, Russell RK, Sanderson JD, Sans M, Satsangi J, Schreiber S, Simms LA, Sventoraityte J, Targan SR, Taylor KD, Tremelling M, Verspaget HW, De Vos M, Wijmenga C, Wilson DC, Winkelmann J, Xavier RJ, Zeissig S, Zhang B, Zhang CK, Zhao H, Silverberg MS, Annese V, Hakonarson H, Brant SR, Radford-Smith G, Mathew CG, Rioux JD, Schadt EE, Daly MJ, Franke A, Parkes M, Vermeire S, Barrett JC, Cho JH. Host-microbe interactions have shaped the genetic architecture of inflammatory bowel disease. Nature 2012; 491: [PMID: DOI: /nature11582] 9 Weersma RK, Stokkers PC, Cleynen I, Wolfkamp SC, Henckaerts L, Schreiber S, Dijkstra G, Franke A, Nolte IM, Rutgeerts P, Wijmenga C, Vermeire S. Confirmation of multiple Crohn s disease susceptibility loci in a large Dutch-Belgian cohort. Am J Gastroenterol 2009; 104: [PMID: DOI: / ajg ] 10 Jakobsdottir J, Gorin MB, Conley YP, Ferrell RE, Weeks DE. Interpretation of genetic association studies: markers with replicated highly significant odds ratios may be poor classifiers. PLoS Genet 2009; 5: e [PMID: DOI: /journal. pgen ] 11 Evans DM, Visscher PM, Wray NR. Harnessing the information contained within genome-wide association studies to improve individual prediction of complex disease risk. Hum Mol Genet 2009; 18: [PMID: DOI: /hmg/ddp295] 12 Kang J, Kugathasan S, Georges M, Zhao H, Cho JH; NIDDK IBD Genetics Consortium. Improved risk prediction for Crohn s disease with a multi-locus approach. Hum Mol Genet 2011; 20: [PMID: DOI: /hmg/ddr116] 13 Adler J, Rangwalla SC, Dwamena BA, Higgins PD. The prognostic power of the NOD2 genotype for complicated Crohn s disease: a meta-analysis. Am J Gastroenterol 2011; 106: April 14, 2016 Volume 22 Issue 14
98 Zupančič K et al. Predictive risk score for Crohn patients [PMID: DOI: /ajg ] 14 Dudbridge F. Power and predictive accuracy of polygenic risk scores. PLoS Genet 2013; 9: e [PMID: DOI: /journal.pgen ] 15 Wei Z, Wang W, Bradfield J, Li J, Cardinale C, Frackelton E, Kim C, Mentch F, Van Steen K, Visscher PM, Baldassano RN, Hakonarson H. Large sample size, wide variant spectrum, and advanced machine-learning technique boost risk prediction for inflammatory bowel disease. Am J Hum Genet 2013; 92: [PMID: DOI: /j.ajhg ] 16 Repnik K, Potočnik U. Haplotype in the IBD5 region is associated with refractory Crohn s disease in Slovenian patients and modulates expression of the SLC22A5 gene. J Gastroenterol 2011; 46: [PMID: DOI: /s ] 17 Wu J, Pfeiffer RM, Gail MH. Strategies for developing prediction models from genome-wide association studies. Genet Epidemiol 2013; 37: [PMID: DOI: /gepi.21762] 18 Hosmer JDW, Lemeshow S, Sturdivant RX. The Multiple Logistic Regression Model. Applied Logistic Regression: John Wiley & Sons, Inc., 2013: Grimes DA, Schulz KF. Refining clinical diagnosis with likelihood ratios. Lancet 2005; 365: [PMID: DOI: /s (05) ] 20 Lalkhen GA, McCluskey A. Clinical tests: sensitivity and specificity. Contin Educ Anaest Crit Care Pain 2008; 8: [DOI: /bjaceaccp/mkn041] 21 Jostins L, Barrett JC. Genetic risk prediction in complex disease. Hum Mol Genet 2011; 20: R182-R188 [PMID: DOI: /hmg/ddr378] 22 Liu JZ, Anderson CA. Genetic studies of Crohn s disease: past, present and future. Best Pract Res Clin Gastroenterol 2014; 28: [PMID: DOI: /j.bpg ] 23 Nelis M, Esko T, Mägi R, Zimprich F, Zimprich A, Toncheva D, Karachanak S, Piskácková T, Balascák I, Peltonen L, Jakkula E, Rehnström K, Lathrop M, Heath S, Galan P, Schreiber S, Meitinger T, Pfeufer A, Wichmann HE, Melegh B, Polgár N, Toniolo D, Gasparini P, D Adamo P, Klovins J, Nikitina-Zake L, Kucinskas V, Kasnauskiene J, Lubinski J, Debniak T, Limborska S, Khrunin A, Estivill X, Rabionet R, Marsal S, Julià A, Antonarakis SE, Deutsch S, Borel C, Attar H, Gagnebin M, Macek M, Krawczak M, Remm M, Metspalu A. Genetic structure of Europeans: a view from the North-East. PLoS One 2009; 4: e5472 [PMID: DOI: /journal.pone ] 24 Alesina AF, Easterly W, Devleeschauwer A, Kurlat S, Wacziarg RT. Fractionalization (June 2002). Harvard Institute Research Working Paper No Available from: URL: abstract= Abraham G, Inouye M. Genomic risk prediction of complex human disease and its clinical application. Curr Opin Genet Dev 2015; 33: [PMID: DOI: /j.gde ] 26 Golan D, Rosset S. Effective genetic-risk prediction using mixed models. Am J Hum Genet 2014; 95: [PMID: DOI: /j.ajhg ] 27 Yarwood A, Han B, Raychaudhuri S, Bowes J, Lunt M, Pappas DA, Kremer J, Greenberg JD, Plenge R, Worthington J, Barton A, Eyre S. A weighted genetic risk score using all known susceptibility variants to estimate rheumatoid arthritis risk. Ann Rheum Dis 2015; 74: [PMID: DOI: / annrheumdis ] 28 Ek WE, D Amato M, Halfvarson J. The history of genetics in inflammatory bowel disease. Ann Gastroenterol 2014; 27: [PMID: ] 29 Ankerst DP, Thompson IM. Sensitivity and specificity of prostatespecific antigen for prostate cancer detection with high rates of biopsy verification. Arch Ital Urol Androl 2006; 78: [PMID: ] 30 Yin X, Cheng H, Lin Y, Wineinger NE, Zhou F, Sheng Y, Yang C, Li P, Li F, Shen C, Yang S, Schork NJ, Zhang X. A weighted polygenic risk score using 14 known susceptibility variants to estimate risk and age onset of psoriasis in Han Chinese. PLoS One 2015; 10: e [PMID: DOI: /journal. pone ] 31 Eichler EE, Flint J, Gibson G, Kong A, Leal SM, Moore JH, Nadeau JH. Missing heritability and strategies for finding the underlying causes of complex disease. Nat Rev Genet 2010; 11: [PMID: DOI: /nrg2809] P- Reviewer: Goral V, Sipahi AM S- Editor: Gong ZM L- Editor: A E- Editor: Ma S 3784 April 14, 2016 Volume 22 Issue 14
99 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Retrospective Cohort Study ORIGINAL ARTICLE Characteristics and outcomes of chronic liver disease patients with acute deteriorated liver function by severity of underlying liver disease Yun Soo Hong, Dong Hyun Sinn, Geum-Youn Gwak, Juhee Cho, Danbee Kang, Yong-Han Paik, Moon Seok Choi, Joon Hyeok Lee, Kwang Cheol Koh, Seung Woon Paik Yun Soo Hong, Dong Hyun Sinn, Geum-Youn Gwak, Yong- Han Paik, Moon Seok Choi, Joon Hyeok Lee, Kwang Cheol Koh, Seung Woon Paik, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, South Korea Juhee Cho, Danbee Kang, Department of Health Sciences and Technology, SAIHST, Sungkyunkwan University, Seoul 06351, South Korea Juhee Cho, Deaprtment of Health, Behavior and Society and Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MA 21205, United States Author contributions: Sinn DH and Gwak GY designed this study; Hong YS, Cho J, Kang D statistical analysis; Hong YS, Sinn DH writing of the draft manuscript; Gwak GY, Paik YH, Choi MS, Lee JH, Koh KC and Paik SW collection data; Gwak GY, Paik YH, Choi MS, Lee JH, Koh KC and Paik SW critical revision of the manuscript; Hong YS and Sinn DH contributed equally to this work. Institutional review board statement: The study was reviewed and approved by the Institutional review board at Samsung Medical Center. Informed consent statement: Waived by the Institutional Review Board of Samsung Medical Center. Conflict-of-interest statement: All the authors have no conflict of interest related to the manuscript. Data sharing statement: The original anonymous dataset is available on request from the corresponding author at gy.gwak@ samsung.com Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Geum-Youn Gwak, MD, PhD, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-Gu, Seoul 06351, South Korea. gy.gwak@samsung.com Telephone: Fax: Received: December 10, 2015 Peer-review started: December 10, 2015 First decision: January 13, 2016 Revised: January 19, 2016 Accepted: February 20, 2016 Article in press: February 22, 2016 Published online: April 14, 2016 Abstract AIM: To analyze characteristics and outcome of patients with acute-on-chronic liver failure (ACLF) according to the severity of underlying liver disease. METHODS: One hundred and sixty-seven adult patients with chronic liver disease and acute deteriorated liver function, defined by jaundice and coagulopathy, were analyzed. Predisposition, type of injury, response, organ failure, and survival were analyzed and compared between patients with non-cirrhosis (type A), cirrhosis (type B) and cirrhosis with previous decompensation (type C). RESULTS: The predisposition was mostly hepatitis B in type A, while it was alcoholic liver disease in types 3785 April 14, 2016 Volume 22 Issue 14
100 Hong YS et al. ACLF subtype B and C. Injury was mostly hepatic in type A, but was non-hepatic in type C. Liver failure, defined by CLIF-SOFA, was more frequent in types A and B, and circulatory failure was more frequent in type C. The 30-d overall survival rate (85.3%, 81.1% and 83.7% for types A, B and C, respectively, P = 0.31) and the 30-d transplant-free survival rate (55.9%, 65.5% and 62.5% for types A, B and C, respectively P = 0.33) were not different by ACLF subtype, but 1-year overall survival rate were different (85.3%, 71.7% and 58.7% for types A, B and C, respectively, P = 0.02). CONCLUSION: There were clear differences in predisposition, type of injury, accompanying organ failure and long-term mortality according to spectrum of chronic liver disease, implying classifying subtype according to the severity of underlying liver disease is useful for defining, clarifying and comparing ACLF. Key words: Acute-on chronic liver failure; Classification; Injury; Organ failure; Survival The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Controversy exists over defining acute on chronic liver failure (ACLF). Recently, multimodal ACLF classification that classifies patients into chronic hepatitis, cirrhosis and cirrhosis with previous decompensation has been suggested. We found that the new ACLF classification has clear differences in predisposition, type of injury, accompanying organ failure and longterm outcome by subtype. ACLF patients showed similar high short-term mortality, especially without liver transplantation, according to the subtype, but showed clear difference in the long-term mortality, indicating that the subtyping of ACLF by severity of underlying liver disease is useful. Hong YS, Sinn DH, Gwak GY, Cho J, Kang D, Paik YH, Choi MS, Lee JH, Koh KC, Paik SW. Characteristics and outcomes of chronic liver disease patients with acute deteriorated liver function by severity of underlying liver disease. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Patients with either diagnosed or undiagnosed chronic liver disease occasionally present with an acute deterioration of liver function caused by direct or indirect insults to the liver. This event, in general, is termed acute-on-chronic liver failure (ACLF) [1]. However, because of varied etiology and manifestations, there has been a great heterogeneity in defining the disease and, in fact, a recent systematic review has found more than a dozen definitions for ACLF [2]. Among these, there are 2 mainstream definitions most widely used in clinical settings and research. The Asian Pacific Association for the Study of the Liver (APASL) consensus introduced an ACLF definition as an acute hepatic insult manifesting as jaundice (serum bilirubin 5 mg/dl) and coagulopathy (INR 1.5), complicated within 4 wk by ascites and/or encephalopathy in patients with previously diagnosed or undiagnosed chronic liver disease/cirrhosis, and is associated with a high 28-d mortality [3]. The European Association for the Study of the Liver-chronic liver failure (EASL-CLIF) Consortium defined ACLF as acute decompensation of cirrhosis in the form of one or more major complications of liver disease, including ascites, hepatic encephalopathy, gastrointestinal bleeding, and bacterial infection, associated with at least two organ failures with one being renal failure (serum creatinine 1.5 mg/dl) and high 28-d mortality of greater than 15% [4]. They share a common idea that ACLF is a spectrum of disease with varying severity, characterized by multiple organ failure and high mortality [5-8], with liver transplantation (LT) as the only definitive curative option [9-11]. However, the discordant details between the 2 definitions results in confusion rather than clarification of the situation. In specific, the 2 groups suggest different explanations for the duration of illness, severity of the underlying liver disease, and the type of precipitating events. However, these factors are what essentially define ACLF, because each factor determines the acuteness of event, chronicity of liver disease, and the type of insult, respectively. To embrace previously suggested definitions and better clarify this condition, Jalan et al [12] recently proposed a new definition and classification for ACLF. They defined ACLF as a syndrome in patients with chronic liver disease with or without previously diagnosed cirrhosis which is characterized by acute hepatic decompensation resulting in liver failure (jaundice and prolongation of the INR) and one or more extrahepatic organ failures that is associated with increased mortality within a period of 28 d and up to 3 mo from onset [12]. In their definition, they included any chronic liver disease, regardless of the presence of cirrhosis, and a wide range of precipitating events that could damage liver function either directly or indirectly. Patients with chronic liver disease but without cirrhotic features were categorized as type A. Type B ACLF was a group with previously well-compensated cirrhosis, while those with a history of jaundice and/or complications of portal hypertension were included in type C. However, they admitted that this is a working definition which is only to identify patients from whom to collect data to ultimately reach a validated definition. Therefore, the aims of this study were to investigate and compare clinical characteristics, including predisposition (etiologies of chronic liver disease), injury (precipitating events), response (manifestations), short and long-term outcomes according to spectrum 3786 April 14, 2016 Volume 22 Issue 14
101 Hong YS et al. ACLF subtype of chronic liver disease (non-cirrhosis, cirrhosis and cirrhosis with previous decompensation), thereby, to determine relevance of subtyping ACLF by severity of underlying disease for future practice and research. MATERIALS AND METHODS Study design and study population This is a retrospective cohort study conducted by using electronic medical records of ACLF patients who visited Samsung Medical Center between January 1, 2011 and June 30, We included patients 18 years or older and with deteriorated liver function, defined as jaundice (serum bilirubin 5 mg/dl) and coagulopathy (PT INR 1.5). A total of 268 patients were identified, and we excluded 101 patients due to the following reason: acute liver failure patients without underlying chronic liver disease (n = 91), patients with chronic hepatic decompensation (n = 9) (chronic liver failure without acute component), and patients who were on warfarin (n = 6). Chronic liver disease was defined when there was evidence of chronic hepatitis B virus (HBV) or hepatitis C virus (HCV) infection by reviewing serologic markers and history, history of significant alcohol intake, history of chronic abnormality in liver profiles with serologic evidence of autoimmune liver disease, and/or radiological evidence of cirrhosis. The final study sample includes 167 patients. The study was reviewed and approved by the Institutional Review Board of Samsung Medical Center. Because the study is based on the retrospective analysis of existing administrative and clinical data, the requirement of obtaining informed patient consent was waived by the Institutional Review Board of Samsung Medical Center. Patient records/information was anonymized and deidentified prior to analysis. Measurements Data on etiologies and severity of underlying liver disease at the time of diagnosis were evaluated. Acute precipitating events, major presenting complications and the presence of organ failure and systemic inflammatory response syndrome (SIRS) were assessed. Additionally, laboratory measurements including complete blood count (CBC), liver function tests, renal function tests, coagulation profile and culture tests were reviewed. Information on LT, mortality and cause of death was collected until a year after the enrollment. Predisposition and ACLF types Alcoholic liver disease (ALD), chronic hepatitis B, chronic hepatitis C, autoimmune hepatitis (AIH), Wilson s disease, biliary cirrhosis, Budd-Chiari syndrome, and cryptogenic liver cirrhosis were regarded as chronic liver diseases. Chronic liver disease and cirrhosis were confirmed by a thorough review of available previous medical records: biochemical analysis, ultrasonography, abdomen computed tomography (CT), and esophagogastroduodenoscopy (EGD). Cirrhosis was considered to be present if thrombocytopenia (platelet < /μl), splenomegaly, ascites (by cross sectional images), varices (by EGD, cross-sectional images, or history of variceal bleeding), and cirrhotic features of the liver (nodular surface or caudate lobe hypertrophy) in cross-sectional images were present [13]. When the findings were compatible with chronic liver disease without any features of liver cirrhosis, patients were designated type A. If patients had a previous history of jaundice and/or complications of portal hypertension such as variceal bleeding, ascites or hepatic encephalopathy, these patients were classified as type C of ACLF. Well-compensated liver cirrhosis patients were included in type B. Injury, responses and survival As possible injury, hepatic insults included reactivation of HBV, alcohol ingestion, superinfection by hepatitis A virus (HAV), toxic hepatitis, and AIH flare. Bacterial infection/sepsis, variceal bleeding, and non-variceal bleeding were regarded as extrahepatic insults. Alcohol consumption was considered as the most probable precipitating etiology when active alcohol consumption was documented within the last 4 wk and there was no other apparent cause of the acute event. Positive anti- HAV IgM by ELISA confirmed acute HAV infection. In addition, bacterial infection/sepsis was considered as an acute insult in case of definite evidence of infection, such as positive cultures of blood, ascites, urine and sputum and/or when clinically suspected. If patients had multiple injuries (e.g., HBV reactivation and variceal bleeding) and if it is difficult to differentiate an initial one, both of them were considered. Injury was categorized as unknown when all other possible causes were not matched. The Model for End-stage Liver Disease (MELD) score, SIRS, and organ failure were investigated [14]. The presence of each organ failure, as well as the number of organ failures was evaluated at the initial visit (baseline). Type of organ failure was categorized into none, hepatic/coagulation, and extrahepatic ± hepatic/coagulation. Extrahepatic organ failure was defined for renal, cerebral, circulatory and respiratory organ failure. Organ failure was defined according to the EASL-CLIF score [4]. The primary end-point was 30-d survival. Secondary end-point was 30-d transplant free survival, 1-year overall survival and 1-year transplant free survival. With transplant free survival, transplant was considered as end point (failure). Patient survival was assessed for 365 d after the initial visit. Patients who were lost to follow-up without reaching the end point were classified as censored cases. Statistical analysis Means ± SD were used for describing continuous outcomes, and analysis of variance was applied to 3787 April 14, 2016 Volume 22 Issue 14
102 Hong YS et al. ACLF subtype Table 1 Predisposition, injury and response according to the subtypes n (%) Type A (n = 34) Type B (n = 53) Type C (n = 80) P value Age (yr) c 51.9 ± ± ± Male 20 (58.8) 32 (60.4) 59 (73.8) Predisposition HBV c 21 (61.8) 19 (35.9) 28 (35.0) Alcohol ac 4 (11.8) 25 (47.2) 33 (41.3) HCV 0 (0.0) 0 (0.0) 6 (7.5) Autoimmune c 6 (17.7) 2 (3.8) 2 (2.5) Others 3 (8.8) 7 (13.2) 11 (13.8) Injury Hepatic ace 30 (88.2) 31 (58.5) 9 (11.3) < Extrahepatic ace 0 (0.0) 13 (24.5) 44 (55.0) < Unknown e 4 (11.8) 4 (7.6) 23 (28.8) Both (hepatic + extrahepatic) 0 (0.0) 5 (9.4) 4 (5.0) Response MELD score 29 ± ± ± SIRS 9 (26.5) 19 (35.9) 30 (37.5) Organ failures by CLIF-SOFA Type of organ failure None e 8 (23.5) 8 (15.1) 28 (35.0) Hepatic/coagulation ce 19 (55.9) 34 (64.2) 21 (26.3) Extrahepatic c 7 (20.6) 11 (20.8) 31 (38.8) Specific organ type Hepatic ce 26 (76.5) 42 (79.3) 28 (35.0) < Coagulation 10 (29.4) 11 (20.8) 21 (26.3) Renal 7 (20.6) 5 (9.4) 17 (21.3) Cerebral 2 (5.9) 4 (7.6) 11 (13.8) Circulatory ce 1 (2.9) 4 (7.6) 16 (20.0) Respiratory 2 (5.9) 1 (1.9) 4 (5.0) Number of organ failure None e 8 (23.5) 8 (15.1) 28 (35.0) One e 13 (38.2) 29 (54.7) 26 (32.5) (38.2) 16 (30.2) 26 (32.5) a P < 0.05 Type A vs B using Bonferroni s post hoc test; c P < 0.05 Type A vs C using Bonferroni s post hoc test; e P < 0.05 Type B vs C using Bonferroni s post hoc test. HBV: Hepatitis B virus; HCV: Hepatitis C virus; AIH: Autoimmune hepatitis; MELD: Model for end stage liver disease; SIRS: Systemic inflammatory response syndrome; CLIF-SOFA: Chronic liver failure-sequential organ failure assessment. compare the means of the different ACLF groups. In addition, Bonferroni s method was used as a posthoc test for group comparison. χ 2 test and Fisher s exact test were employed as needed for categorical variables. The Kaplan-Meier method was applied for estimating the survival rates, and the differences of the survival were compared using a log-rank test. We also obtained Bonferroni adjusted P-values to compensate multiple testing procedures. P-value of < 0.05 was considered statistically significant. RESULTS Predisposition, injury and response according to the ACLF types Comparison of baseline characteristics is shown in Table 1. The etiology of predisposing liver diseases was significantly different according to the ACLF types. Hepatitis B was the most common etiology in type A, while ALD was more common in type B and type C. AIH was more common in type A. Interestingly, except for unknown cases, all ACLF of type A were caused by injury directed at the liver. HBV flare was the most common precipitating event in type A. On the other hand, extrahepatic insults such as bacterial infection and bleeding episodes were more responsible for type C. Type B were in-between type A and type C. The specific injuries (precipitating events) are shown in Table 2. MELD score and SIRS at diagnosis were comparable among the types. In terms of organ failure, defined by the CLIF-SOFA system, the extrahepatic failure was more frequent in type C than type A, and hepatic/coagulation failure was more frequent in types A and B than type C. Outcomes according to the ACLF types At 30 d, the overall survival rate and the transplantfree survival rate were 83.2% and 61.1%, respectively. At 1 year, the overall survival rate and the transplantfree survival rate were 68.3% and 46.7%, respectively. The most common cause of death was infection (52.8%), followed by bleeding (20.8%). During the follow-up period, 44 patients (12, 16 and 16 in types A, B, and C, respectively) received LT. According to each ACLF type, the overall 30-d survival rate (85.3%, 81.1% and 83.7% for type A, B and C, respectively, P = 0.31; Figure 1A) and transplant-free survival rate at 30 d (55.9%, 65.5% 3788 April 14, 2016 Volume 22 Issue 14
103 Hong YS et al. ACLF subtype Table 2 Specific injury according to the acute on chronic liver failure type n (%) A 1.00 Type A Type B Type C P value HBV flare ace 17 (50.0) 11 (20.8) 4 (5.0) < Alcohol ae 3 (8.8) 19 (35.9) 6 (7.5) < HAV 3 (8.8) 1 (1.9) 1 (1.3) Toxin e 5 (14.7) 9 (17.0) 3 (3.8) AIH flare c 7 (20.6) 2 (3.8) 0 (0.0) < Infection ac 0 (0.0) 13 (24.5) 32 (40.0) < Varix bleeding 0 (0.0) 3 (5.7) 11 (13.8) Other bleeding 0 (0.0) 2 (3.8) 6 (7.5) Unknown e 4 (11.8) 4 (7.6) 23 (28.8) a P < 0.05, Type A vs B using Bonferroni s post hoc test; c P < 0.05 Type A vs C using Bonferroni s post hoc test; e P < 0.05 Type B vs C using Bonferroni s post hoc test. HBV: Hepatitis B virus; HAV: Hepatitis A virus; AIH: Autoimmune hepatitis. and 62.5% for type A, B and C, respectively, P = 0.33; Figure 1B) were not different among the types. However, the overall 1-year survival was significantly higher in type A (85.3%), as compared to types B (71.7%) and C (58.7%) (P = 0.02; Figure 1A). All mortality occurred within 30 d in type A, but mortality continued to occur after 30 d in types B and C. Transplant-free survival rate at 1-year was also lower in type C, as compared to types A and B; but the difference was not statistically significant (52.9%, 51.7% and 34.8% for type A, B and C, respectively, P = 0.86; Figure 1B). Outcome according to the type of organ failure Among 167 patients, 49 patients (29.3%) had extrahepatic organ failures with or without hepatic/coagulation failure, 74 patients (44.3%) had hepatic/ coagulation failure, and 44 patients (26.3%) showed no organ failure defined by EASL-CLIF. The 30-d and 1-year overall survival rate was 55.9% and 51.6% for patients with extrahepatic organ failures, 79.6% and 67.4% for hepatic and/or coagulation organ failure, and 90.0% and 74.5% for patients without organ failure, respectively (Figure 2A). The 30-d and 1-year transplant free survival rate was 48.9% and 19.6% for patients with extrahepatic organ failures, 54.9% and 37.6% for hepatic and/or coagulation organ failure, and 78.7% and 56.7% for patients without organ failure (Figure 2B). Outcome according to the LT The 30-d and 1-year overall survival rate was 74.8% and 56.2% for patients without LT, while it was 95.9% and 83.5% for patients with LT. The 30-d survival rate was higher in patients with LT in all ACLF types, although the difference was statistically significant only in type C (Type A: 92.3% vs 80.0%, P = 0.37; Type B: 93.7% vs 76.7%, P = 0.14; type C: 100% vs 78.7%, P = 0.029) and 1-year survival rate (Type A: 92.3% vs 80.0%, P = 0.37; Type B: 80.2% vs 62.4%, P = 0.18; Type C: 80.0% vs 42.1%, P = 0.007) B Follow-up duration (d) DISCUSSION Type A Type B Type C Type A Type B Type C Follow-up duration (d) Figure 1 Survival according to newly proposed acute-on-chronic liver failure types. The short-term overall and transplant-free survival was not significantly different according to acute-on-chronic liver failure (ACLF) type, while long-term overall survival was significantly different. A: Overall; B: Transplant-free survival. ACLF, by in the simplest term, is abrupt hepatic decompensation in patients with chronic liver disease [12]. Moreover, ACLF is usually defined as a condition wherein patients are at significantly increased risk for mortality, with improvement in survival with LT [12]. There is controversy regarding what constitutes a chronic liver disease. APASL includes non-cirrhotic chronic liver disease/cirrhosis, but not decompensated cirrhosis to define chronic liver disease [3,15] whereas EASL-AASLD includes only cirrhosis, either compensated or decompensated [4], The newly proposed ACLF definition includes all spectrum of chronic liver disease and categorizes them as type A (non-cirrhotic), type B (cirrhosis), and type C (decompensated cirrhosis) [12]. The present study included all stages of chronic liver disease patients with acute deteriorated liver function, defined by jaundice (serum bilirubin 5 mg/dl) and coagulopathy (PT INR 1.5). All types of patients showed comparably high short-term mortality, and improved survival with LT. The overall survival was 3789 April 14, 2016 Volume 22 Issue 14
104 Hong YS et al. ACLF subtype A B None Hepatic failure Extrahepatic or combined None Hepatic failure Extrahepatic or combined Follow-up duration (d) Follow-up duration (d) Figure 2 Survival according to the types of organ failure defined by EASL-CLIF. Extrahepatic organ failure showed worst survival, but patients without organ failure also showed low transplant-free survival. A: Overall; B: Transplant-free survival. significantly better for patients who received LT, and the survival benefit by LT was most prominent in type C (1-year survival rate: 80.0% vs 42.1% for with and without LT, P = 0.007). Thus, our finding support that ACLF can be defined for all spectrum of chronic liver disease (i.e., non-cirrhotic to decompensated cirrhosis). ACLF, by definition, also implies acute insult that leads to acute deterioration of liver function [3]. For example, superimposed viral hepatitis in chronic liver disease is a well-known injury to put patients at higher risk for acute deterioration of liver function [16]. Bacterial infection or sepsis is also a major risk factor for adverse event in cirrhosis patients [17,18]. Acute insults that lead to ACLF can be categorized as hepatotrophic insult (viral hepatitis, alcohol, drug, autoimmune hepatitis, Wilson s disease, etc.) and non-hepatotrophic insults (infection, surgery, bleeding, etc.) [3]. Because ACLF is a potentially reversible disease [1], it is very important to identify acute insults, and have immediate intervention (e.g., antiviral therapy for hepatitis B, treatment for infection). Importantly, except for few causes where specific injury was uncertain, all type A injuries were hepatotrophic injury (Table 1). In contrast, type C mostly comprised non-hepatotrophic insults, although hepatotrophic insults were observed as well. Type B was in between type A and type C. Organ failure rate was similar in terms of renal, cerebral, coagulation and respiratory failure by ACLF type, but hepatic failure was less frequent and circulatory failure was more frequent in type C (Table 1). Higher rate of circulatory failure in decompensated cirrhosis could be explained by circulatory dysfunction observed in cirrhosis [19]. Differences in injury (precipitating insult) and response (organ failure rates) by ACLF types provide a rationale to categorize ACLF as type A, B and C, which is also helpful in searching potential injury and planning specific intervention in patients with ACLF. It is also noteworthy that type B and type C were still at risk for mortality after 30 d, leading to a decreased 1-year survival compared to type A. This also provides a rationale to categorize patients who experienced ACLF, as different long-term prognosis is expected. The presence of one or more extrahepatic organ failure was suggested to define ACLF in the newly proposed ACLF definition [12]. However, question remains whether extrahepatic organ failures are mandatory to define ACLF. ACLF, by its simplest meaning, does not include extrahepatic organ failures. The purpose of including extrahepatic organ failures in the ACLF definition is to define the population at high risk for mortality. Our data did indeed show extremely poor short-term survival for patients with extrahepatic organ failures defined by CLIF-SOFA (55.9% and 48.9% for overall and transplant free 30-d survival), and good short-term survival for patients without any organ failures defined by CLIF-SOFA (90.0% and 78.7% for overall and transplant free 30-d survival). This is consistent with previous findings that extrahepatic organ failures are an important factor for survival in ACLF [20]. The association between organ failure and poorer prognosis is supported by numerous studies [4,11,21-26]. However, patients with only hepatic/coagulation failure also showed high shortterm mortality (79.6% and 54.9% for 30-d overall and transplant-free survival). Furthermore, mortality rate exceeding 15% without LT (90.0% and 79.7% for 30-d overall and transplant-free survival) even for patients without any organ failures defined by CLIF- SOFA. Short-term mortality rate of 15% are used to define increased mortality in patients with ACLF [4]. In this sense, our findings suggest that patients without extrahepatic organ failures could be defined as ACLF as well, when they present with acutely deteriorated liver function, defined by jaundice and coagulopathy. It is likely that presence of extrahepatic organ failures may reflect severity of ACLF, however, it may not be a prerequisite for being defined as ACLF. In fact, the APASL definition does not require extrahepatic organ failures to define ACLF [3]. This study had some limitations. First, some of 3790 April 14, 2016 Volume 22 Issue 14
105 Hong YS et al. ACLF subtype information on precipitating events could not be obtained regardless of thorough review of medical records because of the retrospective study design. We defined acute deteriorated liver function by jaundice and coagulopathy, as suggested by APASL [15]. However, in the CANONIC study, acute development of large ascites, hepatic encephalopathy, gastrointestinal hemorrhage, bacterial infection or any combination of above, are used to define acute deteriorated liver function [4]. Thus, patients who do not fulfill APASL criteria for liver failure, but present with acute deteriorated liver function, defined in the CANONIC study, are beyond the scope of this study. Lastly, sample size was relatively small, requiring larger scale, prospective study. In conclusion, ACLF is a distinct syndrome that can be defined as acute deteriorated liver function, precipitated by either direct or indirect injury to the liver, resulting in high short-term mortality with LT as a curative option. The study showed that all spectrum of chronic liver patients with acute deteriorated liver function defined by jaundice (serum bilirubin 5 mg/dl) and coagulopathy (PT INR 1.5) can be defined as ACLF. The newly proposed ACLF classification was clinically relevant because different insults and response could be expected, which also suggest different pathophysiology, different management strategy, and different long-term outcome. This suggest that classifying ACLF subtype according to the severity of underlying liver disease is useful for defining, clarifying and comparing ACLF. COMMENTS Background There has been a great heterogeneity in defining the acute-on-chronic liver failure (ACLF). Recently, ACLF subtype according to the severity of underlying liver disease has been proposed. Research frontiers Retrospective cohort of chronic liver disease patients with acute deteriorated liver function were analyzed to see whether ACLF subtype is useful. Innovations and breakthroughs The study showed that all spectrum of chronic liver patients with acute deteriorated liver function defined by jaundice (serum bilirubin 5 mg/dl) and coagulopathy (PT INR 1.5) can be defined as ACLF. The newly proposed ACLF classification was clinically relevant because different insults and response could be expected, which suggest different pathophysiology, different management strategy, and different long-term outcome. Applications Classifying ACLF patients into ACLF subtype will better clarify this condition, and can be used in clinical practice. Terminology ACLF is a spectrum of disease with varying severity, characterized by multiple organ failure and high mortality. Peer-review This is an interesting and well-written paper addressing an important topic, i.e. the outcome of patients with acute-on-chronic liver disease based on cause of liver disease and precipitating factors of acute disease. REFERENCES 1 Jalan R, Gines P, Olson JC, Mookerjee RP, Moreau R, Garcia- Tsao G, Arroyo V, Kamath PS. Acute-on chronic liver failure. J Hepatol 2012; 57: [PMID: DOI: / j.jhep ] 2 Wlodzimirow KA, Eslami S, Abu-Hanna A, Nieuwoudt M, Chamuleau RA. A systematic review on prognostic indicators of acute on chronic liver failure and their predictive value for mortality. Liver Int 2013; 33: [PMID: DOI: / j x] 3 Sarin SK, Kedarisetty CK, Abbas Z, Amarapurkar D, Bihari C, Chan AC, Chawla YK, Dokmeci AK, Garg H, Ghazinyan H, Hamid S, Kim DJ, Komolmit P, Lata S, Lee GH, Lesmana LA, Mahtab M, Maiwall R, Moreau R, Ning Q, Pamecha V, Payawal DA, Rastogi A, Rahman S, Rela M, Saraya A, Samuel D, Saraswat V, Shah S, Shiha G, Sharma BC, Sharma MK, Sharma K, Butt AS, Tan SS, Vashishtha C, Wani ZA, Yuen MF, Yokosuka O. Acuteon-chronic liver failure: consensus recommendations of the Asian Pacific Association for the Study of the Liver (APASL) Hepatol Int 2014; 8: [PMID: DOI: / s ] 4 Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, Durand F, Gustot T, Saliba F, Domenicali M, Gerbes A, Wendon J, Alessandria C, Laleman W, Zeuzem S, Trebicka J, Bernardi M, Arroyo V; CANONIC Study Investigators of the EASL-CLIF Consortium. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013; 144: , 1437.e1-9 [PMID: DOI: /j.gastro ] 5 Katoonizadeh A, Laleman W, Verslype C, Wilmer A, Maleux G, Roskams T, Nevens F. Early features of acute-on-chronic alcoholic liver failure: a prospective cohort study. Gut 2010; 59: [PMID: DOI: /gut ] 6 Garg H, Kumar A, Garg V, Sharma P, Sharma BC, Sarin SK. Clinical profile and predictors of mortality in patients of acuteon-chronic liver failure. Dig Liver Dis 2012; 44: [PMID: DOI: /j.dld ] 7 Duseja A, Chawla YK, Dhiman RK, Kumar A, Choudhary N, Taneja S. Non-hepatic insults are common acute precipitants in patients with acute on chronic liver failure (ACLF). Dig Dis Sci 2010; 55: [PMID: DOI: /s ] 8 Pan HC, Jenq CC, Tsai MH, Fan PC, Chang CH, Chang MY, Tian YC, Hung CC, Fang JT, Yang CW, Chen YC. Scoring systems for 6-month mortality in critically ill cirrhotic patients: a prospective analysis of chronic liver failure - sequential organ failure assessment score (CLIF-SOFA). Aliment Pharmacol Ther 2014; 40: [PMID: DOI: /apt.12953] 9 Liu CL, Fan ST, Lo CM, Wei WI, Yong BH, Lai CL, Wong J. Live-donor liver transplantation for acute-on-chronic hepatitis B liver failure. Transplantation 2003; 76: [PMID: DOI: /01.tp e5] 10 Chan AC, Fan ST, Lo CM, Liu CL, Chan SC, Ng KK, Yong BH, Chiu A, Lam BK. Liver transplantation for acute-on-chronic liver failure. Hepatol Int 2009; 3: [PMID: DOI: /s ] 11 Finkenstedt A, Nachbaur K, Zoller H, Joannidis M, Pratschke J, Graziadei IW, Vogel W. Acute-on-chronic liver failure: excellent outcomes after liver transplantation but high mortality on the wait list. Liver Transpl 2013; 19: [PMID: DOI: /lt.23678] 12 Jalan R, Yurdaydin C, Bajaj JS, Acharya SK, Arroyo V, Lin HC, Gines P, Kim WR, Kamath PS. Toward an improved definition of acute-on-chronic liver failure. Gastroenterology 2014; 147: 4-10 [PMID: DOI: /j.gastro ] 13 Yang JD, Kim WR, Coelho R, Mettler TA, Benson JT, Sanderson SO, Therneau TM, Kim B, Roberts LR. Cirrhosis is present in 3791 April 14, 2016 Volume 22 Issue 14
106 Hong YS et al. ACLF subtype most patients with hepatitis B and hepatocellular carcinoma. Clin Gastroenterol Hepatol 2011; 9: [PMID: DOI: /j.cgh ] 14 Muckart DJ, Bhagwanjee S. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference definitions of the systemic inflammatory response syndrome and allied disorders in relation to critically injured patients. Crit Care Med 1997; 25: [PMID: DOI: / ] 15 Sarin SK, Kumar A, Almeida JA, Chawla YK, Fan ST, Garg H, de Silva HJ, Hamid SS, Jalan R, Komolmit P, Lau GK, Liu Q, Madan K, Mohamed R, Ning Q, Rahman S, Rastogi A, Riordan SM, Sakhuja P, Samuel D, Shah S, Sharma BC, Sharma P, Takikawa Y, Thapa BR, Wai CT, Yuen MF. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the study of the liver (APASL). Hepatol Int 2009; 3: [PMID: DOI: /s x] 16 El-Serag HB, Everhart JE. Diabetes increases the risk of acute hepatic failure. Gastroenterology 2002; 122: [PMID: DOI: /gast ] 17 Jha AK, Nijhawan S, Rai RR, Nepalia S, Jain P, Suchismita A. Etiology, clinical profile, and inhospital mortality of acute-on-chronic liver failure: a prospective study. Indian J Gastroenterol 2013; 32: [PMID: DOI: / s ] 18 Karvellas CJ, Pink F, McPhail M, Austin M, Auzinger G, Bernal W, Sizer E, Kutsogiannis DJ, Eltringham I, Wendon JA. Bacteremia, acute physiology and chronic health evaluation II and modified end stage liver disease are independent predictors of mortality in critically ill nontransplanted patients with acute on chronic liver failure. Crit Care Med 2010; 38: [PMID: DOI: /CCM.0b013e3181b42a1c] 19 Solà E, Ginès P. Renal and circulatory dysfunction in cirrhosis: current management and future perspectives. J Hepatol 2010; 53: [PMID: DOI: /j.jhep ] 20 Bajaj JS, O Leary JG, Reddy KR, Wong F, Biggins SW, Patton H, Fallon MB, Garcia-Tsao G, Maliakkal B, Malik R, Subramanian RM, Thacker LR, Kamath PS. Survival in infection-related acuteon-chronic liver failure is defined by extrahepatic organ failures. Hepatology 2014; 60: [PMID: DOI: / hep.27077] 21 Thabut D, Massard J, Gangloff A, Carbonell N, Francoz C, Nguyen-Khac E, Duhamel C, Lebrec D, Poynard T, Moreau R. Model for end-stage liver disease score and systemic inflammatory response are major prognostic factors in patients with cirrhosis and acute functional renal failure. Hepatology 2007; 46: [PMID: DOI: /hep.21920] 22 Thadhani R, Pascual M, Bonventre JV. Acute renal failure. N Engl J Med 1996; 334: [PMID: DOI: / nejm ] 23 Terra C, Guevara M, Torre A, Gilabert R, Fernández J, Martín- Llahí M, Baccaro ME, Navasa M, Bru C, Arroyo V, Rodés J, Ginès P. Renal failure in patients with cirrhosis and sepsis unrelated to spontaneous bacterial peritonitis: value of MELD score. Gastroenterology 2005; 129: [PMID: DOI: /j.gastro ] 24 Ginès P, Fernández J, Durand F, Saliba F. Management of critically-ill cirrhotic patients. J Hepatol 2012; 56 Suppl 1: S13-S24 [PMID: DOI: /s (12) ] 25 Cordoba J, Ventura-Cots M, Simón-Talero M, Amorós À, Pavesi M, Vilstrup H, Angeli P, Domenicali M, Ginés P, Bernardi M, Arroyo V. Characteristics, risk factors, and mortality of cirrhotic patients hospitalized for hepatic encephalopathy with and without acute-on-chronic liver failure (ACLF). J Hepatol 2014; 60: [PMID: DOI: /j.jhep ] 26 Yan H, Wu W, Yang Y, Wu Y, Yang Q, Shi Y. A novel integrated Model for End-Stage Liver Disease model predicts short-term prognosis of hepatitis B virus-related acute-on-chronic liver failure patients. Hepatol Res 2015; 45: [PMID: DOI: /hepr.12362] P- Reviewer: Higuera-de la Tijera MF, Tziomalos K S- Editor: Qi Y L- Editor: A E- Editor: Ma S 3792 April 14, 2016 Volume 22 Issue 14
107 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Retrospective Study Multicenter study of endoscopic preoperative biliary drainage for malignant distal biliary obstruction ORIGINAL ARTICLE Naoki Sasahira, Tsuyoshi Hamada, Osamu Togawa, Ryuichi Yamamoto, Tomohisa Iwai, Kiichi Tamada, Yoshiaki Kawaguchi, Kenji Shimura, Takero Koike, Yu Yoshida, Kazuya Sugimori, Shomei Ryozawa, Toshiharu Kakimoto, Ko Nishikawa, Katsuya Kitamura, Tsunao Imamura, Masafumi Mizuide, Nobuo Toda, Iruru Maetani, Yuji Sakai, Takao Itoi, Masatsugu Nagahama, Yousuke Nakai, Hiroyuki Isayama Naoki Sasahira, Department of Gastroenterology, JCHO Tokyo Takanawa Hospital, Tokyo , Japan Tsuyoshi Hamada, Yousuke Nakai, Hiroyuki Isayama, Department of Gastroenterology, Graduate School of Medicine, The University of Tokyo, Tokyo , Japan Osamu Togawa, Department of Gastroenterology, Saitama International Medical Center, Saitama Medical University, Saitama , Japan Ryuichi Yamamoto, Department of Gastroenterology and Hepatology, Saitama Medical University International Medical Center, Saitama , Japan Tomohisa Iwai, Department of Gastroenterology, Kitasato University, Kanagawa , Japan Kiichi Tamada, Department of Gastroenterology, Jichi Medical University, Tochigi , Japan Yoshiaki Kawaguchi, Department of Gastroenterology, Tokai University, Kanagawa , Japan Kenji Shimura, Department of Gastroenterology, Asahi General Hospital, Chiba , Japan Takero Koike, Department of Internal Medicine, Japanese Red Cross Ashikaga Hospital, Tochigi , Japan Yu Yoshida, Department of Gastroenterology, Kimitsu Central Hospital, Chiba , Japan Kazuya Sugimori, Department of Gastroenterology, Yokohama City University Medical Center, Kanagawa , Japan Shomei Ryozawa, Department of Gastroenterology, Showa University Northern Yokohama Hospital, Kanagawa , Japan Toshiharu Kakimoto, Department of Gastroenterology, Saitama City Hospital, Saitama , Japan Ko Nishikawa, Department of Gastroenterology, Ageo Central General Hospital, Saitama , Japan Katsuya Kitamura, Division of Gastroenterology, Department of Medicine, Showa University School of Medicine, Tokyo , Japan Tsunao Imamura, Department of Gastroenterology, Toranomon Hospital, Tokyo , Japan Masafumi Mizuide, Department of Gastroenterology, Gunma University, Gunma , Japan Nobuo Toda, Department of Gastroenterology, Mitsui Memorial Hospital, Tokyo , Japan Iruru Maetani, Division of Gastroenterology and Hepatology, Department of Internal Medicine, Toho University Ohashi Medical Center, Tokyo , Japan Yuji Sakai, Department of Gastroenterology, Chiba University, Chiba , Japan Takao Itoi, Department of Gastroenterology, Tokyo Medical University, Tokyo , Japan Masatsugu Nagahama, Department of Gastroenterology, Showa University Fujigaoka Hospital, Kanagawa , Japan Author contributions: Sasahira N, Tamada K, Kawaguchi Y, Shimura K, Sugimori K, Kakimoto T, Mizuide M, Maetani I, Sakai Y, Itoi T, Nagahama M and Isayama H designed the research; Sasahira N, Hamada T, Togawa O, Yamamoto R, Iwai T, Tamada K, Kawaguchi Y, Shimura K, Koike T, Yoshida Y, Sugimori K, Ryozawa S, Kakimoto T, Nishikawa K, Kitamura K, Imamura T, Mizuide M, Toda N, Maetani I, Sakai Y, Itoi T 3793 April 14, 2016 Volume 22 Issue 14
108 Sasahira N et al. Endoscopic preoperative biliary drainage and Nagahama M acquired the data; Sasahira N and Hamada T analyzed the data; Sasahira N, Hamada T and Nakai Y wrote the paper; Tamada K, Ryozawa S, Maetani I, Itoi T and Isayama H revised the manuscript critically for important intellectual content; Isayama H finally approved the article. Supported by the grant from the Japanese Foundation for Research and Promotion of Endoscopy, No Institutional review board statement: The study was reviewed and approved by the ethics committee at The University of Tokyo Hospital and at each participating hospital. Informed consent statement: Informed consent was not obtained from each participant because this was the retrospective study and all participants had completed the observation period at the initiation of the study. Instead of that, all participants were given the right to withdraw the use of the data. Both were approved by the institutional review board of each hospital. Conflict-of-interest statement: We have no financial relationships to disclose. Data sharing statement: No additional data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Hiroyuki Isayama, MD, PhD, Department of Gastroenterology, Graduate School of Medicine, The University of Tokyo, 7-3-1, Hongo, Bunkyo-Ku, Tokyo , Japan. isayama-tky@umin.ac.jp Telephone: Fax: Received: November 19, 2015 Peer-review started: November 23, 2015 First decision: December 11, 2015 Revised: January 3, 2016 Accepted: January 30, 2016 Article in press: January 30, 2016 Published online: April 14, 2016 Abstract AIM: To determine the optimal method of endoscopic preoperative biliary drainage for malignant distal biliary obstruction. METHODS: Multicenter retrospective study was conducted in patients who underwent plastic stent (PS) or nasobiliary catheter (NBC) placement for resectable malignant distal biliary obstruction followed by surgery between January 2010 and March Procedurerelated adverse events, stent/catheter dysfunction (occlusion or migration of PS/NBC, development of cholangitis, or other conditions that required repeat endoscopic biliary intervention), and jaundice resolution (bilirubin level < 3.0 mg/dl) were evaluated. Cumulative incidence of jaundice resolution and dysfunction of PS/NBC were estimated using competing risk analysis. Patient characteristics and preoperative biliary drainage were also evaluated for association with the time to jaundice resolution and PS/NBC dysfunction using competing risk regression analysis. RESULTS: In total, 419 patients were included in the study (PS, 253 and NBC, 166). Primary cancers included pancreatic cancer in 194 patients (46%), bile duct cancer in 172 (41%), gallbladder cancer in three (1%), and ampullary cancer in 50 (12%). The median serum total bilirubin was 7.8 mg/dl and 324 patients (77%) had 3.0 mg/dl. During the median time to surgery of 29 d [interquartile range (IQR), d]. PS/NBC dysfunction rate was 35% for PS and 18% for NBC [Subdistribution hazard ratio (SHR) = 4.76; 95%CI: , P < 0.001]; the pig-tailed tip was a risk factor for PS dysfunction. Jaundice resolution was achieved in 85% of patients and did not depend on the drainage method (PS or NBC). CONCLUSION: PS has insufficient patency for preoperative biliary drainage. Given the drawbacks of external drainage via NBC, an alternative method of internal drainage should be explored. Key words: endoscopic preoperative biliary drainage; malignant distal biliary obstruction; periampullary cancer; plastic stent; nasobiliary drainage The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: To determine the optimal method of endoscopic preoperative biliary drainage for malignant distal biliary obstruction, we conducted a multicenter retrospective study in 419 patients who underwent plastic stent (PS) or nasobiliary catheter (NBC) placement for resectable malignant distal biliary obstruction followed by surgery. The dysfunction rate for PS was significantly higher than that for NBC. Since the current limitations of nasobiliary catheter may not be overcome by a plastic stent, further studies may need to focus on the use of other stents that could remain patent for a longer period of time. Sasahira N, Hamada T, Togawa O, Yamamoto R, Iwai T, Tamada K, Kawaguchi Y, Shimura K, Koike T, Yoshida Y, Sugimori K, Ryozawa S, Kakimoto T, Nishikawa K, Kitamura K, Imamura T, Mizuide M, Toda N, Maetani I, Sakai Y, Itoi T, Nagahama M, Nakai Y, Isayama H. Multicenter study of endoscopic preoperative biliary drainage for malignant distal biliary obstruction. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: April 14, 2016 Volume 22 Issue 14
109 Sasahira N et al. Endoscopic preoperative biliary drainage INTRODUCTION Surgical resection is the only treatment option for cure in patients with periampullary cancers, including pancreatic and biliary tract cancers. In such patients, obstructive jaundice is often complicated. The efficacy of preoperative biliary drainage on improving periand postoperative outcomes for jaundice due to periampullary cancers is controversial [1-6] ; however, biliary drainage is widely incorporated into clinical practice in many centers as a procedure following diagnostic cholangiography combined with pathological confirmation of malignancy or for the prevention of jaundice progression when the waiting time to a major surgery is prolonged, especially in tertiary centers [7,8]. Endoscopic biliary drainage (EBD) is preferred over percutaneous transhepatic biliary drainage (PTBD) for preoperative management of malignant distal biliary obstruction, because PTBD is more invasive, imposed considerable patient discomfort [9,10], and more importantly, is frequently susceptible to catheter tract recurrence after surgery [11]. Although EBD is usually performed via plastic stent (PS) or nasobiliary catheter (NBC), NBC is unacceptable, especially in western countries, because of patient intolerance. However, NBC is considered advantageous in preventing reflux cholangitis and for early resolution of jaundice and is often employed in Japan. In this multicenter retrospective study entitled endoscopic preoperative biliary drainage (E-POD) study, we evaluated the outcomes of preoperative EBD using both PS and NBC and analyzed the risk factors for PS/NBC dysfunction. MATERIALS AND METHODS Patients In this study, data from 33 referral centers in Japan were consecutively collected. Patients who were diagnosed with distal biliary obstruction due to periampullary cancer and who underwent EBD via PS or NBC followed by surgical resection with curative intent between January 2010 and March 2012 were included. Patients who underwent initial drainage by PTBD or underwent surgery more than 100 d after initial EBD were excluded. This study was approved by the ethics committee at each hospital and was registered with UMIN-CTR (clinical trial registration number: UMIN ). Data collection Data on baseline patient characteristics, procedures of EBD, procedure-related adverse events, outcomes of PS/NBC, types of surgery, and survival were collected retrospectively. All data were made anonymous and were collected from a collaborative web-based database. Definitions Distal biliary obstruction was defined as biliary stricture located 2 cm downstream from the hilar bifurcation. Performance status was determined using the World Health Organization classification. Tumor invasion to the duodenum [12] was diagnosed on the basis of pathological findings of resected specimens. Dysfunction of PS/NBC was defined as occlusion or migration of PS/NBC, development of cholangitis, or suspected insufficient drainage that required repeat endoscopic biliary intervention. Occlusion or cholangitis included jaundice or re-elevation of liver enzyme with or without fever-up, and fever-up without other causes even if no elevation of liver enzyme. Insufficient drainage included persistent liver dysfunction or limited improvement of the elevated liver enzyme even though it is sometimes difficult to distinguish from other causes of liver dysfunction. Designed PS replacement was defined as NBC replacement with PS in patients without NBC dysfunction. Diagnostic reendoscopic retrograde cholangiopancreatography (re- ERCP) was defined as further endoscopic examination (e.g., confirmation of pathological diagnosis and reevaluation of biliary system) that was required without PS/NBC dysfunction. The jaundice was defined as 3.0 mg/dl by using the application with modifications of Child-Pugh classification for cirrhotic patients, which was clinically used as one of the indications for surgery. Jaundice resolution was defined as reduction of serum total bilirubin from a pre-drainage level of 3.0 mg/dl to < 3.0 mg/dl. The time to jaundice resolution and dysfunction of PS/NBC was defined as the interval between the initial EBD and each outcome. Procedurerelated adverse events were diagnosed and graded according to the American Society of Gastrointestinal Endoscopy lexicon s severity grading system [13]. Statistical analysis Results are expressed as numbers and percentages of patients or as medians and interquartile ranges (IQRs). Continuous variables were compared using Student s t-test or Wilcoxon s rank-sum test, as appropriate. Categorical variables were compared using the χ 2 or Fisher exact test, as appropriate. Cumulative incidence of jaundice resolution and dysfunction of PS/NBC were estimated using competing risk analysis [14] and were compared using the Gray s test [15]. During the analysis of the cumulative incidence of jaundice resolution, surgery prior to jaundice resolution was considered as a competing risk event. On the other hand, during the analysis of the cumulative incidence of PS/NBC dysfunction, surgery without PS/NBC dysfunction, PS/NBC removal at the time of diagnostic re-ercp, or designed PS replacement was considered as a competing risk event. Patient characteristics and preoperative biliary drainage were evaluated for association with the time to jaundice resolution and PS/NBC dysfunction using competing 3795 April 14, 2016 Volume 22 Issue 14
110 Sasahira N et al. Endoscopic preoperative biliary drainage Table 1 Characteristics of 419 patients who underwent endoscopic preoperative biliary drainage via plastic stent and nasobiliary catheter n (%) All patients (n = 419) PS (n = 253) NBC (n = 166) P value Sex, male 269 (64) 163 (64) 106 (64) Age (yr) 69 (63-75) 69 (62-75) 70 (63-76) Performance status, 0/1/2 331/81/7 (79/19/2) 201/50/2 (79/20/1) 130/31/5 (78/19/3) Primary cancer, pancreas/biliary tract/ampullary 194/175/50 (46/42/12) 133/91/29 (53/36/11) 61/84/21 (37/51/13) Primary tumor size (mm) 20 (15-30) 20 (14-28) 22 (18-30) Length of biliary stricture (mm) 16 (11-22) 15 (11-22) 17 (12-23) Diameter of proximal bile duct (mm) 15 (12-18) 15 (12-18) 14 (11-17) Involvement of intrapancreatic bile duct 354 (84) 221 (87) 133 (80) Tumor invasion into duodenum 213 (51) (53) 81 (51) Cholangitis on admission 64 (15) 34 (13) 30 (18) Total bilirubin (mg/dl) 7.8 ( ) 7.5 ( ) 8.6 ( ) Data were not obtained in nine patients. Data are expressed as numbers (%) or median (interquartile range). PS: plastic stent; NBC: nasobiliary catheter. risk regression analysis [16]. Factors with a P-value of < 0.20 in the univariate analysis were further analyzed in multivariate models. Subdistribution hazard ratios (SHRs) and 95%CIs were calculated for each factor. A P-value of < 0.05 was considered statistically significant. All analyses were performed using R software version (R Development Core Team) and its cmprsk package. RESULTS Patients In total, 425 consecutive patients who underwent preoperative EBD for resectable periampullary cancers were identified. Six patients with placement of metal stent in this setting were excluded from the analyses. The characteristics of 419 patients are summarized in Table 1 (Those in patients with pancreatic and biliary tract cancer were shown separately in Supplementary table 1a and b). Primary cancers included pancreatic cancer in 194 patients (46%), bile duct cancer in 172 (41%), gallbladder cancer in three (1%), and ampullary cancer in 50 (12%). Eighty-four patients (20%) had diabetes, three (1%) had liver cirrhosis, and three (1%) had dementia. Sixty-four patients (15%) had acute cholangitis at the initial drainage. The median serum total bilirubin was 7.8 mg/dl and 324 patients (77%) had 3.0 mg/dl. Two patients underwent neoadjuvant chemotherapy. The following surgeries were performed: pancreatoduodenectomy in 166 patients (39.6%), pylorus-preserving pancreatoduodenectomy in 142 (33.9%), subtotal stomachpreserving pancreatoduodenectomy in 90 (21.5%), choledochectomy in 10 (2.4%), total pancreatectomy in four (1.0%), and other surgeries in seven (1.7%). Cancer invasion of the duodenum was confirmed in the resected specimens obtained from 213 patients (51%). Procedures and procedure-related adverse events after initial EBD PS and NBC were placed in 253 (60%) and 166 (40%) patients, respectively. NBC was placed in 30 of 64 patients (47%) with acute cholangitis and in 136 of 355 patients (38%) without acute cholangitis. The procedure for initial EBD is shown in Table 2 (Those in patients with pancreatic and biliary tract cancer was shown separately in Supplementary table 2a and b). The diameters of PSs were 5 Fr in 18 patients (7%), 7 Fr in 150 (59%), and 8.5 Fr or 10 Fr in 85 (34%), whereas those of NBCs were 5 Fr or 6 Fr in 80 patients (48%), 7 Fr in 80 (48%), and 7.5 Fr in 6 (4%). An NBC with a diameter larger than 8.5 Fr was not commercially available; thus, the mean diameter of NBCs were significantly smaller than that of PSs (P < 0.001). Approximately two-thirds of PSs were straight tipped, whereas almost the same proportion of NBCs was pig-tail tipped. Endoscopic sphincterotomy (39%) or endoscopic papillary balloon dilation (3%) was performed before placement of PS/NBC. During the initial EBD procedure, biliary biopsy or brushing cytology examination was performed in 362 patients (86.4%), and 250 of them (69.1%) were found to be positive for cancer. There were no significant differences in the initial EBD procedures between pancreatic cancer and biliary tract cancer. PEP was noted in 40 patients (9.5%). The PEP rate was higher in patients with bile duct cancer than in those with pancreatic or ampullary cancer (12.0% vs 7.8%, P = 0.15), but it was not related to PS/NBC (10.3% vs 8.4%, P = 0.53), the PS/NBC diameter (9.7% in < 7.5 Fr vs 9.4% in > 7.5 Fr, P = 0.91), and necessity for sphincterotomy (7.3% vs 11.3%, P = 0.17). Outcomes of preoperative biliary drainage via PS and NBC The median time to surgery was 29 d (IQR, d). Figure 1 demonstrates the clinical course of the patients after the initial drainage. In the PS group, 111 of 253 patients (44%) underwent additional ERCP (23 for diagnostic re-ercp and 88 for PS dysfunction) and NBC was replaced in 32 of them. In the NBC group, 94 of 166 patients (57%) underwent designed PS replacement after a median of 8.4 d (IQR, 6-10 d). There were 41 patients (25%) who underwent 3796 April 14, 2016 Volume 22 Issue 14
111 Sasahira N et al. Endoscopic preoperative biliary drainage Table 2 Procedures, adverse events, and causes of dysfunction in patients who underwent preoperative plastic stent and nasobiliary catheter placement n (%) All patients (n = 419) PS (n = 253) NBC (n = 166) P value Procedures of the initial ERCP EST or EPBD 178 (43) 101 (40) 77 (46) Biopsy or brushing of the bile duct 362 (86) 214 (85) 148 (89) Positive for cancer 250 (60) 150 (59) 100 (60) Biliary stents/catheters placed Diameter 5-6/7-7.5/ Fr 98/236/85 (23/56/20) 18/150/85 (7/59/34) 80/86/0 (48/52/0) < Pig-tailed tip/straight tip 152/ /177 (29/71) 78/47 (62/38) < Placement of pancreatic stent 41 (10) 25 (10) 16 (10) Adverse events (other than cholangitis) Pancreatitis 40 (10) 26 (10) 14 (8) Mild/moderate/severe 30/10/0 Cholecystitis 4 (1) 2 (1) 2 (1) Others 4 (1) 2 (1) 2 (1) Stent/catheter dysfunction 118 (36) 88 (35) 30 (18) < Causes of PS/NBC dysfunction Occlusion or cholangitis (27) 16 (10) Insufficient drainage (6) 5 (3) Migration 10 5 (2) 5 (3) Inadvertent removal 4 NA 4 (2) NA Number of ERCPs 2 (1-2) 1 (1-1) 2 (1-2) < Data was not obtained in 43 patients. A part of data on tips of PS/NBC was missing. Occlusion or cholangitis included jaundice or re-elevation of liver enzyme with or without fever-up, and fever-up without other causes even if no elevation of liver enzyme; Insufficient drainage included persistent liver dysfunction or limited improvement of the elevated liver enzyme, which is sometimes difficult to distinguish from other causes of liver dysfunction. PS: plastic stent; NBC: nasobiliary catheter; ERCP: endoscopic retrograde cholangiopancreatography; EST: endoscopic sphincterotomy; EPBD: endoscopic papillary balloon dilation; NA: not applicable. 419 patients underwent endoscopic preoperative biliary drainage Surgery (n = 142) PS (n = 253) Surgery (n = 50) NBC (n = 166) Surgery (n = 75) Designed PS placement (n = 94) Diagnostic re-ercp (n = 23) PS dysfunction (n = 88) Diagnostic re-ercp (n = 8) NBC dysfunction (n = 14) Diagnostic re-ercp (n = 3) PS dysfunction (n = 16) PS (n = 79) NBC (n = 32) PS (n = 9) NBC (n = 13) PS (n = 11) NBC (n = 8) Figure 1 Flowchart of the clinical course of 419 patients who underwent preoperative biliary drainage via plastic stent and nasobiliary catheter followed by surgery. PS: plastic stent; NBC: nasobiliary catheter. additional ERCP (11 for diagnostic re-ercp, 14 for initial NBC dysfunction, and 16 for designed PS dysfunction). Risk factors for PS/NBC dysfunction Multivariate analysis showed that PS placement had a significantly higher risk for dysfunction than NBC 3797 April 14, 2016 Volume 22 Issue 14
112 Sasahira N et al. Endoscopic preoperative biliary drainage Table 3 Univariate and multivariate competing risks regression analyses to identify risk factors for dysfunction of plastic stent or nasobiliary catheter in 419 patients who underwent endoscopic preoperative biliary drainage Univariate analysis Multivariate analysis SHR (95%CI) P value SHR (95%CI) P value Sex, male 0.96 ( ) Age > 70 yr 1.06 ( ) Performance status ( ) ( ) Primary cancer Biliary tract Reference Reference Pancreas 1.61 ( ) ( ) Ampullary 0.89 ( ) ( ) Primary tumor size > 20 mm 0.90 ( ) Length of biliary stricture > 20 mm 1.04 ( ) Diameter of proximal bile duct > 15 mm 0.94 ( ) Tumor invasion into duodenum 1.10 ( ) Cholangitis on admission 0.77 ( ) Total bilirubin 8 mg/dl 1.16 ( ) Placement of PS 4.76 ( ) < ( ) < Diameter of biliary stent/catheter 5-6 Fr Reference Reference Fr 1.92 ( ) ( ) Fr 2.44 ( ) ( ) Pig-tailed tip 1.05 ( ) PS: plastic stent; NBC: nasobiliary catheter; SHR: subdistribution hazard ratio. Cumulative incidence of PS/NBC dysfunction (%) PS (n = 253) NBC (n = 166) t /d Number at risk PS NBC Figure 2 Cumulative incidences of plastic stent/nasobiliary catheter dysfunction. PS: plastic stent; NBC: nasobiliary catheter. placement (SHR = 4.76, 95%CI: , P < 0.001) (Table 3). Figure 2 illustrates the cumulative incidences of PS/NBC dysfunction. The cumulative incidences of PS vs NBC was 13% vs 5% at 10 d, 22% vs 7% at 20 d, and 30% vs 8% at 30 d. Table 4 shows the results of the analyses for identifying risk factors for PS dysfunction. Only the pig-tailed tip stent was an independent risk factor for PS dysfunction (SHR = 1.72, 95%CI: , P = 0.012); a larger diameter of PS did not decrease the risk for PS dysfunction. Jaundice resolution after preoperative biliary drainage Jaundice was resolved at the time of surgery in 275 of 324 patients (84.9%). The other 49 patients (15.1%) underwent surgery without resolution of jaundice after a median of 21 d (IQR, d) from the initial EBD. The prognostic factors for jaundice resolution are shown in Table 5. Placement of PS or NBC did not result in earlier resolution of jaundice, and only a high total bilirubin level (SHR = 0.43, 95%CI: , P < 0.001) was identified as the significant risk factor for jaundice resolution. DISCUSSION In this multicenter retrospective study of 419 patients who underwent preoperative EBD for malignant distal biliary obstruction, PS placement was a risk factor for PS/NBC dysfunction, whereas NBC placement was not, and the cumulative incidence of PS dysfunction increased almost linearly with time after the initial drainage. Preoperative biliary drainage in patients with distal biliary obstruction has been a major matter of debate for decades. Although randomized controlled trials and meta-analyses failed to demonstrate the effectiveness of routine preoperative biliary drainage, this procedure is still performed widely, particularly in symptomatic patients with an expected long waiting time who have complication such as cholangitis or intense pruritus or because of some other reasons. In the 33 hospitals that participated in the present study, most patients with jaundice underwent preoperative biliary drainage because a major surgery that lasts for 5-10 h cannot always be scheduled immediately after a diagnosis of cancer [17] and such drainage also allows time for further staging of primary cancer, physical work-up of comorbidities, and potentially, for 3798 April 14, 2016 Volume 22 Issue 14
113 Sasahira N et al. Endoscopic preoperative biliary drainage Table 4 Univariate and multivariate competing risk regression analyses to identify risk factors for plastic stent dysfunction in 253 patients who underwent endoscopic preoperative plastic stent placement Univariate analysis Multivariate analysis SHR (95%CI) P value SHR (95%CI) P value Sex, male 1.00 ( ) Age > 70 yr 1.15 ( ) Performance status ( ) Primary cancer Biliary tract Reference Pancreas 1.27 ( ) Ampullary 0.83 ( ) Primary tumor size > 20 mm 1.10 ( ) Length of biliary stricture > 20 mm 1.01 ( ) Diameter of proximal bile duct > 15 mm 0.85 ( ) Tumor invasion into duodenum 1.10 ( ) Cholangitis on admission 0.79 ( ) Total bilirubin 8 mg/dl 1.32 ( ) ( ) Diameter of biliary stent/catheter 5-6 Fr Reference Fr 0.76 ( ) Fr 0.67 ( ) Pig-tailed tip 1.73 ( ) ( ) PS: plastic stent; SHR: subdistribution hazard ratio. Table 5 Univariate and multivariate competing risks regression analyses to identify prognostic factors for jaundice resolution after endoscopic preoperative biliary drainage in 325 patients Univariate analysis Multivariate analysis SHR (95%CI) P value SHR (95%CI) P value Sex, male 0.90 ( ) Age 69 yr 1.01 ( ) Performance status ( ) Primary cancer Biliary tract Reference Pancreas 1.07 ( ) Ampullary 1.19 ( ) Primary tumor size > 20 mm 0.81 ( ) ( ) Length of biliary stricture > 20 mm 0.80 ( ) ( ) Diameter of proximal bile duct > 15 mm 0.78 ( ) ( ) Tumor invasion to duodenum 0.96 ( ) Cholangitis on admission 1.11 ( ) Total bilirubin 8 mg/dl 0.41 ( ) < ( ) < EST or EPBD 1.02 ( ) Diameter of biliary stent/catheter 5-6 Fr Reference Fr 0.96 ( ) Fr 0.97 ( ) Pig-tailed tip 1.05 ( ) Placement of NBC 0.83 ( ) ( ) In these competing risks regression analyses, jaundice resolution was set as the outcome and thus, a higher SHR indicated a higher probability of early resolution of jaundice. SHR: subdistribution hazard ratio; CI: confidence interval; EST: endoscopic sphincterotomy; EPBD: endoscopic papillary balloon dilation; NBC: nasobiliary catheter. neoadjuvant chemotherapy, which is increasingly utilized for pancreatic cancer. EBD is preferred over PTBD for preoperative drainage because it is less invasive and insusceptible to tumor seeding. During EBD, PSs are preferred over NBCs with regard to comfort, but the rate of PS dysfunction before surgery is reported to be as high as 34%-70% [18-20]. Although Sugiyama et al [20] demonstrated that the time to dysfunction of PS and NBC did not differ significantly in a retrospective study of 76 patients, the rate of PS dysfunction was significantly higher than that of NBC dysfunction in the present study. In the PS group, a pig-tailed PS was the only risk factor for stent dysfunction and PS with a larger diameter failed to prolong the time to stent dysfunction. Interestingly, although the cumulative incidences of PS/NBC dysfunction were quite similar within a week of the initial biliary drainage, the cumulative incidence of PS 3799 April 14, 2016 Volume 22 Issue 14
114 Sasahira N et al. Endoscopic preoperative biliary drainage dysfunction linearly increased thereafter, whereas that of NBC dysfunction almost plateaued. At 30 d after the initial EBD, which was almost the median time to surgery in the present cohort, the cumulative incidence of dysfunction reached as high as 30% in the PS group, whereas that in the NBC group remained at 8%. In this study, the PS dysfunction rate and median time to dysfunction of 14 d were similar to those reported in a prospective study by van der Gaag et al [4] (30% and 13 d, respectively). NBC has other advantages such as repetitions of bile cytology to confirm malignancy [21] and contrast medium injection for cholangiography to evaluate longitudinal tumor spreading, especially in patients with bile duct cancer. However, there are several obvious disadvantages. For example, external bile drainage by NBC may impair enterohepatic circulation of bile, potentially leading to deterioration of intestinal immunity and coagulopathy, and prolonged placement of NBC may impose discomfort in the pharynx. NBC followed by the replacement of PS is another option for preoperative drainage, although it requires additional ERCP. Longer patency of self-expandable metal stent (SEMS) compared with PS has been well-established in unresectable distal biliary obstruction [22,23] and recently, SEMS in the preoperative setting has been reported to be effective because of its longer patency and lower dysfunction rate (< 20%) [24-27]. Therefore, despite some potential disadvantages of SEMS, including cholecystitis [28], pancreatitis [29], and cost, SEMS is a promising device for preoperative biliary drainage and deserves further investigation. Considering that the ultimate endpoint of endoscopic preoperative biliary drainage for malignant distal biliary obstruction is overall survival rather than outcomes, the most appropriate method should be determined by a randomized controlled trial that compares PS, NBC, and SEMS, with the survival time set as the primary endpoint. We acknowledge some limitations of this study. First, it was based on a non-randomized retrospective design and did not evaluate surgical outcomes. A randomized controlled trial is required to draw a definite conclusion of the optimal endoscopic preoperative biliary drainage procedure for malignant distal biliary obstruction, surgical outcomes (R0 resection rate, rate of surgical adverse events, and ultimately, overall survival), length of hospitalization, and cost-effectiveness. Second, we included only patients who underwent EBD and subsequent surgery; some patients in whom surgery could not be performed because of unsuccessful biliary drainage may have been excluded. Third, various types of PSs and NBCs were used in the present study. In conclusion, PS was associated with a higher rate of cholangitis or occlusion compared with NBC. Because internal bile drainage is not susceptible to inherent disadvantages of external bile drainage, internal bile drainage via SEMS should be evaluated in a preoperative setting. ACKNOWLEDGMENTS We thank the following investigators and clinical research coordinators. Investigators of the study: Hiroshi Nitta, Department of Surgery, Fukaya Red Cross Hospital; Shigeaki Mizuno and Yuji Shiozawa, Department of Gastroenterology and Hepatology, Nihon University School of Medicine; Naminatsu Takahara, Department of Gastroenterology, Kanto Central Hospital; Saburo Matsubara, Department of Gastroenterology, Tokyo Metropolitan Police Hospital; Tadashi Ohshima, Department of Gastroenterology, Saitama Red Cross Hospital; Shigeru Iwase, Department of Gastroenterology, Fujisawa City Hospital; Satoshi Shimizu, Department of Hepatobiliary & Pancreatic Oncology, National Cancer Center Hospital East; Naotaka Maruoka, Department of Gastroenterology, Odawara Municipal Hospital; Hiroshi Yagioka, Department of Gastroenterology, JR Tokyo General Hospital; Shinichiro Sato, Department of Gastroenterology, Chiba-Nishi General Hospital; Yukiko Ito, Department of Gastroenterology, Japanese Red Cross Medical Center; Toshihiko Arizumi, Department of Gastroenterology, Mitsui Memorial Hospital; Hiroaki Shigoka, Division of Gastroenterology and Hepatology, Department of Internal Medicine, Toho University Ohashi Medical Center; Shujiro Tsuji, Department of Gastroenterology, Tokyo Medical University; Natsuyo Yamamoto, Hirofumi Kogure and Takashi Sasaki, Department of Gastroenterology, The University of Tokyo. Clinical study coordinators: Miyuki Tsuchida, Clinical Research Support Center, The University of Tokyo Hospital. The authors would like to thank Enago ( for the English language review. COMMENTS Background Although the efficacy of preoperative biliary drainage on improving periand postoperative outcomes for jaundice due to periampullary cancers is controversial, biliary drainage is widely incorporated into clinical practice in many centers as a procedure following diagnostic cholangiography combined with pathological confirmation of malignancy or for the prevention of jaundice progression when the waiting time to a major surgery is prolonged, especially in tertiary centers. Endoscopic biliary drainage is usually performed via plastic stent (PS) or nasobiliary catheter (NBC). NBC is unacceptable, especially in western countries, because of patient intolerance. However, NBC is considered advantageous in preventing reflux cholangitis and for early resolution of jaundice and is often employed in Japan. Research frontiers The results of this study contribute to clarifying the outcomes of preoperative EBD using both PS and NBC and the risk factors for PS/NBC dysfunction in the largest cohort. Innovations and breakthroughs At 30 d after the initial EBD, which was almost the median time to surgery in the present cohort, the cumulative incidence of dysfunction reached as high as 30% in the PS group, whereas that in the NBC group remained at 8%. The PS 3800 April 14, 2016 Volume 22 Issue 14
115 Sasahira N et al. Endoscopic preoperative biliary drainage dysfunction rate and median time to dysfunction of 14 d were similar to those reported in a prospective randomized study by van der Gaag et al (30% and 13 d, respectively). Applications As the NBC has an obvious disadvantages of imposing discomfort in the pharynx, NBC followed by the replacement of PS is one of the options for preoperative drainage, although it requires additional ERCP. Preoperative placement of self-expandable metal stent should be investigated instead of plastic stent. Terminology Endoscopic naso-biliary drainage: Naso-biliary drainage has some advantages such as repetitions of bile cytology to confirm malignancy and contrast medium injection for cholangiography to evaluate longitudinal tumor spreading, especially in patients with bile duct cancer. However, it has several obvious disadvantages; external bile drainage by NBC may impair enterohepatic circulation of bile, potentially leading to deterioration of intestinal immunity and coagulopathy, and prolonged placement of NBC may impose discomfort in the pharynx. Peer-review Authors studied superiority between PS and NBC for preoperative drainage in a retrospective setting. This attempt is clinically valuable and the study is wellorganized. Their results and conclusions are simple and reasonable. REFERENCES 1 Smith RC, Pooley M, George CR, Faithful GR. Preoperative percutaneous transhepatic internal drainage in obstructive jaundice: a randomized, controlled trial examining renal function. Surgery 1985; 97: [PMID: ] 2 Pitt HA, Gomes AS, Lois JF, Mann LL, Deutsch LS, Longmire WP. Does preoperative percutaneous biliary drainage reduce operative risk or increase hospital cost? Ann Surg 1985; 201: [PMID: DOI: / ] 3 Lai EC, Mok FP, Fan ST, Lo CM, Chu KM, Liu CL, Wong J. Preoperative endoscopic drainage for malignant obstructive jaundice. Br J Surg 1994; 81: [PMID: DOI: /bjs ] 4 van der Gaag NA, Rauws EA, van Eijck CH, Bruno MJ, van der Harst E, Kubben FJ, Gerritsen JJ, Greve JW, Gerhards MF, de Hingh IH, Klinkenbijl JH, Nio CY, de Castro SM, Busch OR, van Gulik TM, Bossuyt PM, Gouma DJ. Preoperative biliary drainage for cancer of the head of the pancreas. N Engl J Med 2010; 362: [PMID: DOI: /NEJMoa ] 5 Sewnath ME, Karsten TM, Prins MH, Rauws EJ, Obertop H, Gouma DJ. A meta-analysis on the efficacy of preoperative biliary drainage for tumors causing obstructive jaundice. Ann Surg 2002; 236: [PMID: DOI: / ] 6 Wang Q, Gurusamy KS, Lin H, Xie X, Wang C. Preoperative biliary drainage for obstructive jaundice. Cochrane Database Syst Rev 2008; (3): CD [PMID: DOI: / CD pub2] 7 Nagino M, Takada T, Miyazaki M, Miyakawa S, Tsukada K, Kondo S, Furuse J, Saito H, Tsuyuguchi T, Yoshikawa T, Ohta T, Kimura F, Ohta T, Yoshitomi H, Nozawa S, Yoshida M, Wada K, Amano H, Miura F. Preoperative biliary drainage for biliary tract and ampullary carcinomas. J Hepatobiliary Pancreat Surg 2008; 15: [PMID: DOI: /s ] 8 van der Gaag NA, Kloek JJ, de Castro SM, Busch OR, van Gulik TM, Gouma DJ. Preoperative biliary drainage in patients with obstructive jaundice: history and current status. J Gastrointest Surg 2009; 13: [PMID: DOI: / s ] 9 Mueller PR, van Sonnenberg E, Ferrucci JT. Percutaneous biliary drainage: technical and catheter-related problems in 200 procedures. AJR Am J Roentgenol 1982; 138: [PMID: DOI: /ajr ] 10 Choi SH, Gwon DI, Ko GY, Sung KB, Yoon HK, Shin JH, Kim JH, Kim J, Oh JY, Song HY. Hepatic arterial injuries in 3110 patients following percutaneous transhepatic biliary drainage. Radiology 2011; 261: [PMID: DOI: / radiol ] 11 Takahashi Y, Nagino M, Nishio H, Ebata T, Igami T, Nimura Y. Percutaneous transhepatic biliary drainage catheter tract recurrence in cholangiocarcinoma. Br J Surg 2010; 97: [PMID: DOI: /bjs.7228] 12 Hamada T, Isayama H, Nakai Y, Togawa O, Kogure H, Kawakubo K, Tsujino T, Sasahira N, Hirano K, Yamamoto N, Arizumi T, Ito Y, Matsubara S, Sasaki T, Yagioka H, Yashima Y, Mohri D, Miyabayashi K, Mizuno S, Nagano R, Takahara N, Toda N, Tada M, Omata M, Koike K. Duodenal invasion is a risk factor for the early dysfunction of biliary metal stents in unresectable pancreatic cancer. Gastrointest Endosc 2011; 74: [PMID: DOI: /j.gie ] 13 Cotton PB, Eisen GM, Aabakken L, Baron TH, Hutter MM, Jacobson BC, Mergener K, Nemcek A, Petersen BT, Petrini JL, Pike IM, Rabeneck L, Romagnuolo J, Vargo JJ. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc 2010; 71: [PMID: DOI: /j.gie ] 14 Tai BC, Machin D, White I, Gebski V. Competing risks analysis of patients with osteosarcoma: a comparison of four different approaches. Stat Med 2001; 20: [PMID: DOI: /sim.711] 15 Kawakubo K, Isayama H, Sasahira N, Kogure H, Miyabayashi K, Hirano K, Tada M, Koike K. Mucosal hyperplasia in an uncovered portion of partially covered metal stent. World J Gastrointest Endosc 2012; 4: [PMID: DOI: /wjge. v4.i9.432] 16 Kawakubo K, Isayama H, Nakai Y, Sasahira N, Kogure H, Sasaki T, Hirano K, Tada M, Koike K. Simultaneous Duodenal Metal Stent Placement and EUS-Guided Choledochoduodenostomy for Unresectable Pancreatic Cancer. Gut Liver 2012; 6: [PMID: DOI: /gnl ] 17 Baron TH, Kozarek RA. Preoperative biliary stents in pancreatic cancer--proceed with caution. N Engl J Med 2010; 362: [PMID: DOI: /NEJMe ] 18 Mullen JT, Lee JH, Gomez HF, Ross WA, Fukami N, Wolff RA, Abdalla EK, Vauthey JN, Lee JE, Pisters PW, Evans DB. Pancreaticoduodenectomy after placement of endobiliary metal stents. J Gastrointest Surg 2005; 9: ; discussion [PMID: DOI: /j.gassur ] 19 Boulay BR, Gardner TB, Gordon SR. Occlusion rate and complications of plastic biliary stent placement in patients undergoing neoadjuvant chemoradiotherapy for pancreatic cancer with malignant biliary obstruction. J Clin Gastroenterol 2010; 44: [ PMID: DOI: / MCG.0b013e3181d2ef06] 20 Sugiyama H, Tsuyuguchi T, Sakai Y, Nisikawa T, Miyazaki M, Yokosuka O. Preoperative drainage for distal biliary obstruction: endoscopic stenting or nasobiliary drainage? Hepatogastroenterology 2013; 60: [PMID: DOI: /hge12621] 21 Yagioka H, Hirano K, Isayama H, Tsujino T, Sasahira N, Nagano R, Hamada T, Miyabayashi K, Ito Y, Mohri D, Kawakubo K, Kogure H, Sasaki T, Tada M, Koike K. Clinical significance of bile cytology via an endoscopic nasobiliary drainage tube for pathological diagnosis of malignant biliary strictures. J Hepatobiliary Pancreat Sci 2011; 18: [PMID: DOI: /s x] 22 Davids PH, Groen AK, Rauws EA, Tytgat GN, Huibregtse K. Randomised trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet 1992; 340: [PMID: DOI: / (9 2) ] 3801 April 14, 2016 Volume 22 Issue 14
116 Sasahira N et al. Endoscopic preoperative biliary drainage 23 Isayama H, Yasuda I, Ryozawa S, Maguchi H, Igarashi Y, Matsuyama Y, Katanuma A, Hasebe O, Irisawa A, Itoi T, Mukai H, Arisaka Y, Okushima K, Uno K, Kida M, Tamada K. Results of a Japanese multicenter, randomized trial of endoscopic stenting for non-resectable pancreatic head cancer (JM-test): Covered Wallstent versus DoubleLayer stent. Dig Endosc 2011; 23: [PMID: DOI: /j x] 24 Wasan SM, Ross WA, Staerkel GA, Lee JH. Use of expandable metallic biliary stents in resectable pancreatic cancer. Am J Gastroenterol 2005; 100: [PMID: DOI: /j x] 25 Singal AK, Ross WA, Guturu P, Varadhachary GR, Javle M, Jaganmohan SR, Raju RP, Fleming JB, Raju GS, Kuo YF, Lee JH. Self-expanding metal stents for biliary drainage in patients with resectable pancreatic cancer: single-center experience with 79 cases. Dig Dis Sci 2011; 56: [PMID: DOI: /s ] 26 Aadam AA, Evans DB, Khan A, Oh Y, Dua K. Efficacy and safety of self-expandable metal stents for biliary decompression in patients receiving neoadjuvant therapy for pancreatic cancer: a prospective study. Gastrointest Endosc 2012; 76: [PMID: DOI: /j.gie ] 27 Cavell LK, Allen PJ, Vinoya C, Eaton AA, Gonen M, Gerdes H, Mendelsohn RB, D Angelica MI, Kingham TP, Fong Y, Dematteo R, Jarnagin WR, Kurtz RC, Schattner MA. Biliary self-expandable metal stents do not adversely affect pancreaticoduodenectomy. Am J Gastroenterol 2013; 108: [PMID: DOI: /ajg ] 28 Isayama H, Kawabe T, Nakai Y, Tsujino T, Sasahira N, Yamamoto N, Arizumi T, Togawa O, Matsubara S, Ito Y, Sasaki T, Hirano K, Toda N, Komatsu Y, Tada M, Yoshida H, Omata M. Cholecystitis after metallic stent placement in patients with malignant distal biliary obstruction. Clin Gastroenterol Hepatol 2006; 4: [PMID: DOI: /j.cgh ] 29 Kawakubo K, Isayama H, Nakai Y, Togawa O, Sasahira N, Kogure H, Sasaki T, Matsubara S, Yamamoto N, Hirano K, Tsujino T, Toda N, Tada M, Omata M, Koike K. Risk factors for pancreatitis following transpapillary self-expandable metal stent placement. Surg Endosc 2012; 26: [PMID: DOI: /s ] P- Reviewer: Fujisawa T, Ogura T S- Editor: Gong ZM L- Editor: A E- Editor: Zhang DN 3802 April 14, 2016 Volume 22 Issue 14
117 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Retrospective Study ORIGINAL ARTICLE High-dose hepatitis B immunoglobulin therapy in hepatocellular carcinoma with hepatitis B virus-dna/ hepatitis B e antigen-positive patients after living donor liver transplantation Eung Chang Lee, Seong Hoon Kim, Seung Duk Lee, Hyeongmin Park, Soon-Ae Lee, Sang-Jae Park Eung Chang Lee, Seong Hoon Kim, Seung Duk Lee, Hyeongmin Park, Soon-Ae Lee, Sang-Jae Park, Center for Liver Cancer, National Cancer Center, Goyang-si, Gyeonggi-do , South Korea Author contributions: Lee EC, Kim SH, Lee SD, Park H, Lee SA and Park SJ designed the research; Lee EC, Lee SD, Park H performed the research and analyzed the data; Lee EC wrote the paper; Kim SH supervised the study and revised the paper. Institutional review board statement: This study was approved by the Institutional Review Board of National Cancer Center, Republic of Korea. Informed consent statement: We obtained a waiver of informed consent with the Institutional Review Board of our center. Conflict-of-interest statement: No conflicts of interest were declared for all authors. Data sharing statement: Technical appendix, statistical code, and dataset available from the corresponding author at kshlj@ ncc.re.kr. No additional data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Seong Hoon Kim, MD, PhD, Center for Liver Cancer, National Cancer Center, 323 Ilsan-ro, Ilsandonggu, Goyang-si, Gyeonggi-do , South Korea. kshlj@ncc.re.kr Telephone: Fax: Received: November 9, 2015 Peer-review started: November 10, 2015 First decision: November 27, 2015 Revised: December 13, 2015 Accepted: January 9, 2016 Article in press: January 11, 2016 Published online: April 14, 2016 Abstract AIM: To investigate the impact of high-dose hepatitis B immunoglobulin (HBIG) on hepatocellular carcinoma (HCC) and hepatitis B virus (HBV) recurrence and overall survival after living donor liver transplantation (LDLT). METHODS: We investigated 168 patients who underwent LDLT due to HCC, and who were HBV-DNA/ hepatitis B e antigen (HBeAg) -positive, from January 2008 to December After assessing whether the patients met the Milan criteria, they were assigned to the low-dose HBIG group and high-dose HBIG group. Using the propensity score 1:1 matching method, 38 and 18 pairs were defined as adhering to and not adhering to the Milan criteria. For each pair, HCC recurrence, HBV recurrence and overall survival were analyzed by the Kaplan-Meier method and the log rank test according to the HBIG dose. RESULTS: Among those who met the Milan criteria, the 6-mo, 1-year, and 3-year HCC recurrence-free survival rates were 88.9%, 83.2%, and 83.2% in the low-dose HBIG group and 97.2%, 97.2%, and 97.2% in the high-dose HBIG group, respectively (P = 0.042) April 14, 2016 Volume 22 Issue 14
118 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation In contrast, among those who did not meet the Milan criteria, HCC recurrence did not differ according to the HBIG dose (P = 0.937). Moreover, HBV recurrence and overall survival did not differ according to the HBIG dose among those who met (P = and 0.190, respectively) and did not meet (P = and 0.987, respectively) the Milan criteria. CONCLUSION: High-dose HBIG therapy can reduce HCC recurrence in HBV-DNA/HBeAg-positive patients after LDLT. Key words: Hepatitis B immune globulin; Hepatocellular carcinoma; Hepatitis B virus-dna; Liver transplantation; Hepatitis B e antigen The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: This is a single center analysis of the effects of high-dose hepatitis B immunoglobulin (HBIG) therapy on the recurrence of hepatocellular carcinoma and hepatitis B in hepatitis B virus (HBV)-DNA/hepatitis B e antigen (HBeAg)-positive patients after LDLT. High-dose HBIG therapy can be helpful in improving hepatocellular carcinoma recurrence-free survival in HBV-DNA/HBeAg-positive recipients who met the Milan criteria. In contrast, high-dose HBIG therapy was not effective in improving HCC recurrence-free survival in HBV-DNA/HBeAg-positive recipients who did not meet the Milan criteria. Recurrence of hepatitis B and overall survival were not affected by the HBIG dose in HBV- DNA/HBeAg-positive recipients regardless of the Milan status. Lee EC, Kim SH, Lee SD, Park H, Lee SA, Park SJ. High-dose hepatitis B immunoglobulin therapy in hepatocellular carcinoma with hepatitis B virus-dna/hepatitis B e antigen-positive patients after living donor liver transplantation. World J Gastroenterol 2016; 22(14): Available from: URL: wjgnet.com/ /full/v22/i14/3803.htm DOI: org/ /wjg.v22.i INTRODUCTION Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer. Approximately people are annually diagnosed with HCC worldwide. This condition usually develops in patients with cirrhosis, and is common in areas with a high prevalence of infection with hepatitis B virus (HBV) and hepatitis C virus, such as Africa and East Asia [1]. In South Korea, HCC is the fifth most common cancer, and the HBV is its most important risk factor for HCC, accounting for approximately 70% of all HCC cases [2]. Despite the available therapeutic treatment of HCC, such as liver transplantation and resection, tumor recurrence remains problematic. The HCC recurrence rate after orthotopic liver transplantation (OLT) reportedly ranges from 15% to 20%, whereas the survival rate among patients with recurrent HCC is reportedly 22% within 5 years [3-5]. The results of liver transplantation have markedly improved as a result of the rapid evolution of hepatitis B treatment strategies over the past decades. In 1991, Samuel et al [6] reported a HBV recurrence prevention rate of approximately 80% with hepatitis B immune globulin (HBIG) after liver transplantation. Since then, HBIG has become an important component of the prevention strategy for HBV. Despite the use of nucleos(t)ide analogues (NAs) such as lamivudine that have a superior efficacy, an increase in the hepatitis B recurrence rate was observed due to the emergence of HBV-DNA mutants in the long-term follow-up [7]. Subsequently, combination prophylaxis with HBIG and NAs became the standard method for HBV after OLT. It is well known that HBV induces HCC [8,9]. Some researchers have indicated that the viral replication status is a predictor of relapse after HCC surgery [10,11]. However, the relationship between the HBIG dose and HCC recurrence or overall survival rate after OLT has not yet been established. In the present study, we aimed to determine the effect of high-dose HBIG therapy on HCC recurrence, HBV recurrence, and overall survival in HBV-DNA/hepatitis B e antigen (HBeAg)-positive patients after living donor liver transplantation (LDLT). MATERIALS AND METHODS Patients From January 2008 to December 2013, 168 patients with HCC who were HBV-DNA/HBeAg-positive underwent LDLT at the National Cancer Center in the Republic of Korea. Those who have extrahepatic metastasis or obvious cases of major vascular incidents, such as portal vein or hepatic veins, have been excluded from the research. Patients with any other types of cancers in addition to HCC, severe cardiopulmonary comorbidity, active drug or alcohol abuse or active septic infections have also been excluded. The clinicopathologic variables of such patients, including age, sex, Child-Pugh score, alphafetoprotein (AFP) level, tumor number, largest tumor size, Edmondson-Steiner grade, major vessel (major branch of the hepatic vein/portal vein) invasion, microvascular invasion, bile duct invasion, and satellite nodule were analyzed. This study was approved by our Institutional Review Board. HBV prophylaxis Prior to May 2011, HBIG was administered to patients with HCC who were HBV-DNA/HBeAg-positive before OLT, as follows: IU of HBIG (Green Cross Corp., Seoul, South Korea) was administered daily for the first week, after which it was administrated weekly for April 14, 2016 Volume 22 Issue 14
119 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation mo. Thereafter, IU/L of HBIG was administered according to the serum hepatitis B surface antibody (anti-hbs) titer to maintain a titer of greater than 500 IU/L during the first year, and greater than 200 IU/L thereafter. After May 2011, IU of HBIG was administered daily for the first week, after which it was administered weekly for the rest of the month. Thereafter, IU of HBIG was administered monthly for 1 year, followed by administrations at varying doses to maintain a serum anti-hbs titer of > 200 IU/L. For patients who were taking an anti-viral agent before OLT, the same drug was administered. In other cases, entecavir (ETV) was administered following LDLT. Immunosuppression For induction therapy, 20 mg of basiliximab was administered on the operation day and on postoperative day 4. The immunosuppressive regimens consisted of a combination of tacrolimus, mycophenolate mofetil and corticosteroids after high-dose steroid administration during the operation. The initial target levels of tacrolimus ranged from 8 to 12 ng/ml, and mycophenolate mofetil was started with a dose of 1.5 g/d. The corticosteroid doses were reduced until they were discontinued over 6 mo after LDLT. Surveillance for HCC recurrence, HBV recurrence, and overall survival In each patient, post-transplantation follow-up was initially performed weekly after hospital discharge, and was then conducted bi-weekly or monthly, as clinically indicated. Biochemical tests were performed for assessing liver function, AFP levels, HBsAg levels, and anti-hbs titers at each visit. The serum HBV-DNA titer was also monitored regularly in all the patients for 1 year after LDLT. Thereafter, the patients were followed up for recurrence approximately every 2 or 3 mo for 1 year, and every 6 mo for the next 3 years. The definition of HBV recurrence was detectable HBsAg or HBV-DNA. HBsAg and HBeAg were measured via chemiluminescent microparticle immunoassay. The quantitative measurement of HBV-DNA was performed as follows. From January to April 2008, the serum HBV-DNA titers were monitored using the antibody capture solution hybridization HBV-DNA quantitative assay (Digene Hybrid Capture II Assay; Digene Corp., Beltsville, Md., United States), which had a lower detection limit of copies/ml [12]. Between May 2008 and April 2011, the COBAS AMPLICOR HBV MONITOR test (Roche Molecular Systems, Pleasanton, Calif., United States) was used, which had a lower detection limit of 2000 copies/ml [12]. After May 2011, the Abbott RealTime assays (Abbott Laboratories, Des Plaines, IL, United States) was used, which had a lower quantification limit of 70 copies/ml [13-16]. And imaging studies, including abdomen and chest computed tomography (CT), were also conducted every 3 or 6 mo. If HCC recurrence was suspected based on the results of these imaging tests, additional liver magnetic resonance imaging and positron-emissiontomographic-(pet)-ct imaging were performed. In case it was difficult to diagnose HCC recurrence through imaging tests, a biopsy was performed for confirmation. The maximum follow-up period was 5 years, and the censored data were observed until April In HCC patients who met the Milan criteria, the median follow-up periods of the low- and high-dose groups were 55.5 mo (range, mo) and 29.0 mo (range, mo), respectively. In the HCC patients who did not meet the Milan criteria, the median follow-up periods of the low- and high-dose groups were 18.4 mo (range, mo) and 11.4 mo (range, mo), respectively. Statistical analysis The baseline clinicopathologic variables were analyzed using the χ 2 test or Fisher's exact test for the categorical variables, and the Student's t-test or Mann- Whitney U test for the continuous variables, depending on the normality of the distribution. The patients were randomly matched into 1:1 pairs using calipers of width equal to 0.1 of the standard deviation of the logit of the propensity score, without replacement. The following served as contributors to the propensity score: age, sex, Child-Pugh score, AFP level, tumor number, largest tumor size, Edmondson-Steiner grade, major vessel (major branch of the hepatic vein/portal vein) invasion, microvascular invasion, bile duct invasion, and satellite nodule [17-21]. Overall, 38 and 18 pairs were identified as adhering to the Milan criteria and not adhering to these criteria, respectively. The pairs were compared using the McNemar test for the binominal categorical variables, and the paired t-test or Wilcoxon signed rank test for the continuous variables, depending on the normality of the distribution. HCC recurrence and overall survival were analyzed in accordance with the HBIG dose using the Kaplan- Meier method, and the survival curves were compared using the log-rank test. A P value of less than 0.05 was considered statistically significant. All calculations were made using the SPSS 22.0 statistical software package and R (IBM, Inc., Chicago, IL). The statistical methods of this study were reviewed by the Biometric Research Branch, Research Institute and Hospital, National Cancer Center, Republic of Korea. RESULTS Baseline characteristics A total of 168 patients with HCC who were HBV-DNA/ HBeAg-positive underwent LDLT at the National Cancer Center in the Republic of Korea between January 2008 and December Of these patients, April 14, 2016 Volume 22 Issue 14
120 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation Table 1 Baseline characteristics of all patients Characteristic Met the Milan criteria (n = 109) Did not meet the Milan criteria (n = 59) Low-dose HBIG High-dose HBIG P value Low-dose HBIG High-dose HBIG P value (n = 62) (n = 47) (n = 33) (n = 26) Age (yr) 53.8 ± ± ± ± Sex (male/female) 49/13 35/ /3 21/ Child-Pugh score 7 (5-13) 5 (5-12) (5-13) 6 (5-13) AFP (ng/ml) 18.8 ( ) 13.3 ( ) ( ) ( ) Number of tumors 1 (1-3) 1 (1-3) (1-8) 1 (1-5) Largest tumor size (cm) 2.2 ( ) 2.2 ( ) ( ) 4.9 ( ) Edmond-Steiner grade (Ⅰ,Ⅱ/Ⅲ,Ⅳ) 26/36 21/ /25 2/ Major vessel invasion 62/0 47/0 N/A 26/7 17/ (absent/present) Microvascular invasion 42/17 [3] 30/ /22 6/ (absent/present) Bile duct invasion (absent/present) 61/1 42/ /2 23/ Satellite nodule (absent/present) 46/15 [1] 37/ /19 11/ Values are presented as number/number, mean ± SD or median (range). Numbers in parentheses are missing value. AFP: Alpha-fetoprotein; N/A: Not applicable. HCC patients met the Milan criteria, whereas 59 HCC patients did not meet the Milan criteria. Of the HCC patients who met the Milan criteria (n = 109), 62 were included in the low-dose HBIG group, whereas 47 were included in the high-dose HBIG group. Although a significant difference in the Child-Pugh score (P = 0.002) was observed between the groups, none of the other clinicopathologic factors showed significant differences. Of the HCC patients who did not meet the Milan criteria (n = 59), 33 were included in the low-dose HBIG group, whereas 26 were included in the high-dose HBIG group. Except for AFP (P = 0.049), none of the other variables showed significant differences between the groups (Table 1). HCC recurrence, HBV recurrence, and overall survival before propensity matching Among the HCC patients who met the Milan criteria (n = 109), the 6-mo, 1-year, and 3-year HCC recurrencefree survival rates in the low-dose HBIG group (n = 62) were 96.6%, 87.9%, and 82.2%, whereas those in the high-dose HBIG group (n = 47) were 95.6% for all (P = 0.038; Figure 1A). The 6-mo, 1-year, and 3-year HBV recurrence-free rates in the low-dose HBIG group (n = 62) were 100.0%, 98.1%, and 95.8%, whereas those in the high-dose HBIG group (n = 47) were 95.6% for all (P = 0.622; Figure 1C). The 6-mo, 1-year, and 3-year overall survival rates in the lowdose HBIG group (n = 62) were 96.8%, 91.4%, and 76.7%, whereas those in the high-dose HBIG group (n = 47) were 95.7%, 95.7%, and 92.1%, respectively (P = 0.048; Figure 2A). Among the HCC patients who did not meet the Milan criteria (n = 59), the 6-mo, 1-year, and 3-year HCC recurrence-free survival rates in the low-dose HBIG group (n = 33) were 87.3%, 67.9%, and 45.0%, whereas those in the high-dose HBIG group (n = 26) were 76.9%, 53.8%, and 42.0%, respectively (P = 0.436; Figure 1B). The 6-mo, 1-year, and 3-year HBV recurrence-free survival rates in the low-dose HBIG group (n = 33) were 96.6%, 92.7%, and 82.6%, whereas those in the high-dose HBIG group (n = 26) were 92.3%, 82.0%, and 75.2%, respectively (P = 0.334; Figure 1D). No significant difference in overall survival was noted between the groups (P = 0.965; Figure 2B). HCC recurrence, HBV recurrence, and overall survival of the propensity-matched groups Using propensity matching, 38 pairs were found to have met the Milan criteria, whereas 18 pairs were found to have not met the Milan criteria. None of the variables in any of these pairs were found to significantly differ between the low- and high-dose HBIG groups (Table 2). Among the patients who met the Milan criteria (n = 38), the 6-mo, 1-year, and 3-year HCC recurrencefree survival rates in the low-dose HBIG group (n = 38) were 88.9%, 83.2%, and 83.2%, whereas those in the high-dose HBIG group (n = 38) were 97.2%, 97.2%, and 97.2%, respectively (P = 0.042; Figure 3A). There was no significant difference between the groups in terms of HBV recurrence-free survival rates (P = 0.317; Figure 3C). The 6-mo, 1-year, and 3-year overall survival rates of the low-dose HBIG group (n = 38) were 94.4%, 79.3%, and 76.2%, whereas those in the high-dose HBIG group (n = 38) were 94.7%, 94.7%, and 90.6%, respectively (P = 0.190; Figure 4A). Among the 18 pairs of patients who did not meet the Milan criteria, no significant differences in the HCC recurrence-free survival rates (P = 0.937; Figure 3B), HBV recurrence-free survival rates (P = 0.350; Figure 3D), and overall survival rate (P = 0.987; Figure 4B) 3806 April 14, 2016 Volume 22 Issue 14
121 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation A 1.0 High-dose HBIG B 1.0 HCC recurrence-free survival P = Low-dose HBIG HCC recurrence-free survival P = Low-dose HBIG High-dose HBIG t /mo t /mo C 1.0 Low-dose HBIG D 1.0 High-dose HBIG Low-dose HBIG HBV recurrence-free survival P = HBV recurrence-free survival P = High-dose HBIG t /mo t /mo Figure 1 Hepatocellular carcinoma recurrence-free survival rate of the low-dose hepatitis B immunoglobulin group and high-dose hepatitis B immunoglobulin group before adjustment with propensity scores among hepatocellular carcinoma patients who met the Milan criteria (A) and did not meet the Milan criteria (B); hepatitis B recurrence-free survival rate of the low-dose hepatitis B immunoglobulin group group and high-dose hepatitis B immunoglobulin group group before adjustment with propensity scores among hepatocellular carcinoma patients who met the Milan criteria (C) and did not meet the Milan criteria (D). HBIG: Hepatitis B Immunoglobulin; HBV: Hepatitis B virus; HCC: Hepatocellular carcinoma. A 1.0 High-dose HBIG B Overall survival Low-dose HBIG Overall survival High-dose HBIG Low-dose HBIG 0.2 P = P = t /mo t /mo Figure 2 Overall survival rate of the low-dose hepatitis B immunoglobulin group and high-dose hepatitis B Immunoglobulin group before adjustment with propensity scores among hepatocellular carcinoma patients who met the Milan criteria (A) and did not meet the Milan criteria (B). HBIG: Hepatitis B Immunoglobulin April 14, 2016 Volume 22 Issue 14
122 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation Table 2 Baseline characteristics of propensity-matched patients with low- and high-dose hepatitis B Immunoglobulin who met and did not meet the Milan criteria Characteristic Met the Milan criteria (38 pairs) Did not meet the Milan criteria (18 pairs) Low-dose HBIG High-dose HBIG P value Low-dose HBIG High-dose HBIG P value (n = 38) (n = 38) (n = 18) (n = 18) Age (yr) 52.7 ± ± ± ± Sex (male/female) 32/6 29/ /2 16/ Child-Pugh score 6 (5-12) 6 (5-12) (5-13) 6 (5-13) AFP (ng/ml) 22.6 ( ) 15.3 ( ) ( ) ( ) Number of tumors 1 (1-3) 1 (1-3) (1-5) 1 (1-5) Largest tumor size (cm) 2.2 ( ) 2.1 ( ) ( ) 4.9 ( ) Edmond-Steiner grade (Ⅰ, Ⅱ/Ⅲ, Ⅳ) 17/21 17/ /14 2/ Major vessel invasion (absent/present) 38/0 38/0 N/A 12/6 13/ Microvascular invasion (absent/present) 23/15 26/ /13 4/ Bile duct invasion (absent/present) 37/1 37/ /2 16/ Satellite nodule (absent/present) 26/12 29/ /12 5/ Values are presented as number/number, mean ± SD or median (range). AFP: Alpha-fetoprotein; N/A: Not applicable. A 1.0 High-dose HBIG B 1.0 HCC recurrence-free survival P = Low-dose HBIG HCC recurrence-free survival P = High-dose HBIG Low-dose HBIG t /mo t /mo C HBV recurrence-free survival P = Low-dose HBIG High-dose HBIG D HBV recurrence-free survival P = Low-dose HBIG High-dose HBIG t /mo t /mo Figure 3 Hepatocellular carcinoma recurrence-free survival rate of the low-dose hepatitis B immunoglobulin group and high-dose hepatitis B immunoglobulin group after adjustment with propensity scores among hepatocellular carcinoma patients who met the Milan criteria (A) and did not meet the Milan criteria (B); hepatitis B recurrence-free survival rate of the low-dose hepatitis B immunoglobulin group group and high-dose hepatitis B immunoglobulin group group after adjustment with propensity scores among hepatocellular carcinoma patients who met the Milan criteria (C) and did not meet the Milan criteria (D). HBIG: Hepatitis B Immunoglobulin; HBV: Hepatitis B virus; HCC: Hepatocellular carcinoma April 14, 2016 Volume 22 Issue 14
123 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation A 1.0 High-dose HBIG B Low-dose HBIG 0.8 Overall survival Overall survival High-dose HBIG Low-dose HBIG 0.2 P = P = t /mo t /mo Figure 4 Overall survival rate of the low-dose hepatocellular carcinoma group and high-dose hepatocellular carcinoma group after adjustment with propensity scores among hepatocellular carcinoma patients who met the Milan criteria (A) and did not meet the Milan criteria (B). HBIG: Hepatitis B Immunoglobulin. were noted between the groups. DISCUSSION The presence of HBV-DNA in the serum is a reliable marker of active HBV replication, and the presence of HBeAg and the absence of the HBe antibody usually indicate active HBV replication and high infectiousness. Some studies indicated that the pre-olt viral replicative status of the study subjects was a predictor of postoperative HCC recurrence [10,11]. Considering that HBV has been known to induce HCC [8,9,22], if the HBV recurrence rate decreased in the high-dose HBIG group, the reason for the HCC recurrence decrease might be clearly explained in our study. However, the outcome of the present study indicated that HBV recurrence did not significantly differ according to the HBIG dose among both HCC patients who met and did not meet the Milan criteria (P = and 0.350, respectively). Meanwhile, there were some reports that occult hepatitis B infection (OBI) could induce HCC [23-25]. OBI is defined as the presence of low levels of HBV-DNA in the serum, the cells of the lymphatic (immune) system, and/or the hepatic tissue in patients with serological markers of a previous infection [hepatitis B core antibody (anti-hbc)- and/or anti-hbs-positive] and without any serum HBsAg. Real-time polymerase chain reaction (RT-PCR), which is a currently used HBV- DNA quantification method, has a lower quantification limit of 70 copies/ml [13-16]. In comparison, the previous-generation HBV-DNA quantification methods for measuring HBV-DNA, such as the hybrid capture assay and branched-dna (bdna) assay, have much lower sensitivity [12]. In other words, the HBV-DNA titer level was undetectable in the past, it is now enough to define it as OBI as the development of the HBV-DNA quantification methods. Accordingly, HCC recurrence may develop not only in the OBI cases but also in subclinical HBV infection cases wherein the HBV-DNA is undetectable at the present time, as only a small amount of material (e.g., the X protein of HBV [9,26,27] ) produced by the virus may be needed to mediate or re-trigger the cancer. Therefore, in this study, HCC recurrence may have reduced as high-dose HBIG was more efficient for inhibiting the course induced by HBV, as compared to low-dose HBIG. However, only minimal information is available on the manner in which HBIG protects the transplanted liver against HBV reinfection. Virus reproduction begins when the virion comes in contact with a suitable host cell. HBIG may protect naive hepatocytes against infection by the HBV virion by blocking a putative HBV receptor [28]. Alternatively, HBIG may neutralize the circulating virions through immune precipitation and immune complex formation, or may trigger an antibody-dependent cell-mediated cytotoxicity response, resulting in target cell lysis [28,29]. Furthermore, HBIG has been reported to bind to hepatocytes and to interact with HBsAg within cells [30]. Regardless of the mechanism, clear evidence has been obtained for a dose-dependent response to HBIG treatment [31-33]. However, further studies may be required to clarify the several proposed mechanisms and to support the outcomes of this study. Another interesting aspect was that no significant difference was observed in HCC recurrence according to the HBIG dose among the HCC patients who did not meet the Milan criteria (P = 0.937; Figure 3B). In these patients, HCC recurrence may have been caused by circulating tumor cells [34] instead of being mediated or promoted by HBV, as is frequently noted in the recurrence of cancer in other organs. This trend may be associated with the fact that the Milan criteria 3809 April 14, 2016 Volume 22 Issue 14
124 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation includes major vessel invasion, along with tumor size and number, as indications for OLT. In this study, we did not observe any difference in the HBV recurrence according to the HBIG dose in those who met (P = 0.317; Figure 3C) and did not meet (P = 0.350; Figure 3D) the Milan criteria. Most of the patients were taking NAs before LDLT, whereas the other patients received ETV after LDLT. Combination therapy of low-dose HBIG and NAs is efficient and successful for preventing HBV recurrence after OLT, which has been proved several times [35-37]. As seen from our results, we believe that high-dose HBIG may not be essential for suppressing the HBV recurrence itself, but rather there may be a risk for HBsAg escape mutations, as reported in previous studies [38-41]. This study has certain limitations that are inherent to a non-randomized and retrospective study. Another limitation is that the effect of the pre-olt HBV-DNA titer on patient matching was not sufficiently clarified. As reported in previous studies, the pre-olt HBV-DNA titer is one of the risk factor for HCC and HBV recurrence after liver transplantation or liver resection [10,22,42]. In the present study, the effect of the pre-olt HBV-DNA titer on group matching was not directly reflected as three different quantification methods were used during the study period, including the hybrid capture assay, HBV bdna signal amplification assay, and RT-PCR. Among these methods, RT-PCR is the most sensitive, and has the lowest detection limit [12-14]. Accordingly, if the measurement were done via RT-PCR in the patients who were HBeAg- and hybrid-capture-assay- or bdnaassay-negative, HBV-DNA-positive results might have been observed. However, RT-PCR was not used in our institution before May The follow-up period of the high-dose HBIG group was shorter than that of the low-dose HBIG group. Among the patients who met the Milan criteria, the median follow-up periods of the low- and high-hbigdose groups were 55.5 mo (range, mo) and 29.0 mo (range, mo), respectively. Among those who did not meet the Milan criteria, the median follow-up periods of the low- and high-hbig-dose groups were 18.4 mo (range, mo) and 11.4 mo (range, mo), respectively. High-dose HBIG was administered to the HCC patients with HBV-DNA/HBeAgpositive since May 2011; hence, the follow-up period of the high-dose HBIG group might not be sufficient to completely support the findings of this study. In conclusion, high-dose HBIG therapy was confirmed to reduce HCC recurrence in patients who met the Milan criteria and who were HBV-DNA/HBeAgpositive after LDLT; to our knowledge, this is the first time such a finding has been reported. However, further prospective studies are required to confirm these results, and the optimal dose of HBIG therapy after LDLT should be reconsidered. COMMENTS Background In Asia, hepatocellular carcinoma (HCC) is one of the most common cancer. The hepatitis B virus (HBV) infection is endemic in most parts of Asia and chronic HBV infection was classified as group 1 carcinogens of HCC by the World Health Organization. The major prognostic factors in HBV-related HCC patients after orthotropic liver transplantation (OLT) are HBV and HCC recurrence. Research frontiers For HBV prophylaxis following OLT, combination therapy of hepatitis B immunoglobulin (HBIG) and nucleos(t)ide analogues were used in most centers. In HCC patients who showed high infectiousness with HBV-DNA/ hepatitis B e antigen (HBeAg) -positive, a protocol that applies a higher dose of HBIG after OLT is commonly used for HBV prophylaxis. However, no previous studies regarding the effect of HBIG doses on HCC recurrence and overall survival in patients with high infectiousness after OLT was reported. Innovations and breakthroughs The results showed that high-dose HBIG therapy can improve HCC recurrencefree survival of patients with HCC who were HBV-DNA/HBeAg-positive after OLT. Applications Authors suggest that high-dose HBIG can be effective therapy in HCC with HBV-DNA/HBeAg-positive patients after OLT. Terminology HBIG is a sterile solution of purified gamma globulin containing anti-hbs. It is prepared from plasma donated by healthy, screened donors with high titers of anti-hbs. It is used to prevent hepatitis B from occurring again in hepatitis B surface antigen-positive patients who have had OLT. Peer-review The strength of this study is that it is the first study regarding the effect of HBIG doses on HCC recurrence and overall survival in patients with high infectiousness after OLT. They conclude that a high-dose HBIG reduce HCC recurrence in patients with HCC who were HBV-DNA/HBeAg-positive after OLT. The paper is well written and of highly clinical implications. REFERENCES 1 El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology 2007; 132: [PMID: DOI: /j.gastro ] 2 Song IH, Kim KS. Current status of liver diseases in Korea: hepatocellular carcinoma. Korean J Hepatol 2009; 15 Suppl 6: S50-S59 [PMID: DOI: /kjhep S6.S50] 3 Roayaie S, Schwartz JD, Sung MW, Emre SH, Miller CM, Gondolesi GE, Krieger NR, Schwartz ME. Recurrence of hepatocellular carcinoma after liver transplant: patterns and prognosis. Liver Transpl 2004; 10: [PMID: DOI: / lt.20128] 4 Regalia E, Fassati LR, Valente U, Pulvirenti A, Damilano I, Dardano G, Montalto F, Coppa J, Mazzaferro V. Pattern and management of recurrent hepatocellular carcinoma after liver transplantation. J Hepatobiliary Pancreat Surg 1998; 5: [PMID: DOI: /PL ] 5 Welker MW, Bechstein WO, Zeuzem S, Trojan J. Recurrent hepatocellular carcinoma after liver transplantation - an emerging clinical challenge. Transpl Int 2013; 26: [PMID: DOI: /j x] 6 Samuel D, Bismuth A, Mathieu D, Arulnaden JL, Reynes M, 3810 April 14, 2016 Volume 22 Issue 14
125 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation Benhamou JP, Brechot C, Bismuth H. Passive immunoprophylaxis after liver transplantation in HBsAg-positive patients. Lancet 1991; 337: [PMID: DOI: / (91) ] 7 Perrillo R, Rakela J, Dienstag J, Levy G, Martin P, Wright T, Caldwell S, Schiff E, Gish R, Villeneuve JP, Farr G, Anschuetz G, Crowther L, Brown N. Multicenter study of lamivudine therapy for hepatitis B after liver transplantation. Lamivudine Transplant Group. Hepatology 1999; 29: [PMID: DOI: /hep ] 8 Beasley RP, Hwang LY, Lin CC, Chien CS. Hepatocellular carcinoma and hepatitis B virus. A prospective study of men in Taiwan. Lancet 1981; 2: [PMID: DOI: /S (81) ] 9 Kew MC. Hepatitis viruses and hepatocellular carcinoma. Res Virol 1998; 149: [PMID: DOI: / S (99) ] 10 Hung IF, Poon RT, Lai CL, Fung J, Fan ST, Yuen MF. Recurrence of hepatitis B-related hepatocellular carcinoma is associated with high viral load at the time of resection. Am J Gastroenterol 2008; 103: [PMID: DOI: / j x] 11 Wu JC, Huang YH, Chau GY, Su CW, Lai CR, Lee PC, Huo TI, Sheen IJ, Lee SD, Lui WY. Risk factors for early and late recurrence in hepatitis B-related hepatocellular carcinoma. J Hepatol 2009; 51: [PMID: DOI: / j.jhep ] 12 Ho SK, Chan TM, Cheng IK, Lai KN. Comparison of the secondgeneration digene hybrid capture assay with the branched-dna assay for measurement of hepatitis B virus DNA in serum. J Clin Microbiol 1999; 37: [PMID: ] 13 Allice T, Cerutti F, Pittaluga F, Varetto S, Gabella S, Marzano A, Franchello A, Colucci G, Ghisetti V. COBAS AmpliPrep-COBAS TaqMan hepatitis B virus (HBV) test: a novel automated realtime PCR assay for quantification of HBV DNA in plasma. J Clin Microbiol 2007; 45: [PMID: DOI: / JCM ] 14 Daniel HD, Fletcher JG, Chandy GM, Abraham P. Quantitation of hepatitis B virus DNA in plasma using a sensitive cost-effective in-house real-time PCR assay. Indian J Med Microbiol 2009; 27: [PMID: DOI: / ] 15 Ciotti M, Marcuccilli F, Guenci T, Prignano MG, Perno CF. Evaluation of the Abbott RealTime HBV DNA assay and comparison to the Cobas AmpliPrep/Cobas TaqMan 48 assay in monitoring patients with chronic cases of hepatitis B. J Clin Microbiol 2008; 46: [PMID: DOI: / JCM ] 16 Thibault V, Pichoud C, Mullen C, Rhoads J, Smith JB, Bitbol A, Thamm S, Zoulim F. Characterization of a new sensitive PCR assay for quantification of viral DNA isolated from patients with hepatitis B virus infections. J Clin Microbiol 2007; 45: [PMID: DOI: /JCM ] 17 Schlitt HJ, Neipp M, Weimann A, Oldhafer KJ, Schmoll E, Boeker K, Nashan B, Kubicka S, Maschek H, Tusch G, Raab R, Ringe B, Manns MP, Pichlmayr R. Recurrence patterns of hepatocellular and fibrolamellar carcinoma after liver transplantation. J Clin Oncol 1999; 17: [PMID: ] 18 Steinmüller T, Seehofer D, Rayes N, Müller AR, Settmacher U, Jonas S, Neuhaus R, Berg T, Hopf U, Neuhaus P. Increasing applicability of liver transplantation for patients with hepatitis B-related liver disease. Hepatology 2002; 35: [PMID: DOI: /jhep ] 19 Ben-Ari Z, Daudi N, Klein A, Sulkes J, Papo O, Mor E, Samra Z, Gadba R, Shouval D, Tur-Kaspa R. Genotypic and phenotypic resistance: longitudinal and sequential analysis of hepatitis B virus polymerase mutations in patients with lamivudine resistance after liver transplantation. Am J Gastroenterol 2003; 98: [PMID: DOI: /j x] 20 Yi NJ, Suh KS, Cho JY, Kwon CH, Lee KW, Joh JW, Lee SK, Kim SI, Lee KU. Recurrence of hepatitis B is associated with cumulative corticosteroid dose and chemotherapy against hepatocellular carcinoma recurrence after liver transplantation. Liver Transpl 2007; 13: [PMID: DOI: / lt.21043] 21 Faria LC, Gigou M, Roque-Afonso AM, Sebagh M, Roche B, Fallot G, Ferrari TC, Guettier C, Dussaix E, Castaing D, Brechot C, Samuel D. Hepatocellular carcinoma is associated with an increased risk of hepatitis B virus recurrence after liver transplantation. Gastroenterology 2008; 134: ; quiz 2155 [PMID: DOI: /j.gastro ] 22 Yasunaka T, Takaki A, Yagi T, Iwasaki Y, Sadamori H, Koike K, Hirohata S, Tatsukawa M, Kawai D, Shiraha H, Miyake Y, Ikeda F, Kobashi H, Matsuda H, Shinoura S, Yoshida R, Satoh D, Utsumi M, Onishi T, Yamamoto K. Serum hepatitis B virus DNA before liver transplantation correlates with HBV reinfection rate even under successful low-dose hepatitis B immunoglobulin prophylaxis. Hepatol Int 2011; 5: [PMID: DOI: / s z] 23 Zobeiri M. Occult hepatitis B: clinical viewpoint and management. Hepat Res Treat 2013; 2013: [PMID: DOI: /2013/259148] 24 Hollinger FB, Sood G. Occult hepatitis B virus infection: a covert operation. J Viral Hepat 2010; 17: 1-15 [PMID: DOI: /j x] 25 Ghisetti V, Marzano A, Zamboni F, Barbui A, Franchello A, Gaia S, Marchiaro G, Salizzoni M, Rizzetto M. Occult hepatitis B virus infection in HBsAg negative patients undergoing liver transplantation: clinical significance. Liver Transpl 2004; 10: [PMID: DOI: /lt.20093] 26 Yang HI, Lu SN, Liaw YF, You SL, Sun CA, Wang LY, Hsiao CK, Chen PJ, Chen DS, Chen CJ. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N Engl J Med 2002; 347: [PMID: DOI: /NEJMoa013215] 27 Murakami Y, Saigo K, Takashima H, Minami M, Okanoue T, Bréchot C, Paterlini-Bréchot P. Large scaled analysis of hepatitis B virus (HBV) DNA integration in HBV related hepatocellular carcinomas. Gut 2005; 54: [PMID: DOI: /gut ] 28 Shouval D, Samuel D. Hepatitis B immune globulin to prevent hepatitis B virus graft reinfection following liver transplantation: a concise review. Hepatology 2000; 32: [PMID: DOI: /jhep ] 29 Sawyer RG, McGory RW, Gaffey MJ, McCullough CC, Shephard BL, Houlgrave CW, Ryan TS, Kuhns M, McNamara A, Caldwell SH, Abdulkareem A, Pruett TL. Improved clinical outcomes with liver transplantation for hepatitis B-induced chronic liver failure using passive immunization. Ann Surg 1998; 227: [PMID: DOI: / ] 30 Schilling R, Ijaz S, Davidoff M, Lee JY, Locarnini S, Williams R, Naoumov NV. Endocytosis of hepatitis B immune globulin into hepatocytes inhibits the secretion of hepatitis B virus surface antigen and virions. J Virol 2003; 77: [PMID: DOI: /JVI ] 31 Samuel D, Muller R, Alexander G, Fassati L, Ducot B, Benhamou JP, Bismuth H. Liver transplantation in European patients with the hepatitis B surface antigen. N Engl J Med 1993; 329: [PMID: DOI: /NEJM ] 32 Beasley RP, Hwang LY, Stevens CE, Lin CC, Hsieh FJ, Wang KY, Sun TS, Szmuness W. Efficacy of hepatitis B immune globulin for prevention of perinatal transmission of the hepatitis B virus carrier state: final report of a randomized double-blind, placebocontrolled trial. Hepatology 1983; 3: [PMID: DOI: /hep ] 33 Committee for Proprietary Medicinal Products. Core SPC for human plasma derived hepatitis-b immunoglobulin for intravenous use (CPMP/BPWG/4027/02). London, UK: The European Agency for the Evaluation of Medicinal Products, Gupta GP, Massagué J. Cancer metastasis: building a framework. Cell 2006; 127: [PMID: DOI: / j.cell ] 3811 April 14, 2016 Volume 22 Issue 14
126 Lee EC et al. Hepatitis B immunoglobulin after liver transplantation 35 Takaki A, Yagi T, Yamamoto K. Safe and cost-effective control of post-transplantation recurrence of hepatitis B. Hepatol Res 2015; 45: [PMID: DOI: /hepr.12368] 36 Lo CM, Fan ST, Liu CL, Lai CL, Wong J. Prophylaxis and treatment of recurrent hepatitis B after liver transplantation. Transplantation 2003; 75: S41-S44 [PMID: ] 37 Lok AS. Prevention of recurrent hepatitis B post-liver transplantation. Liver Transpl 2002; 8: S67-S73 [PMID: ] 38 Cooreman MP, Leroux-Roels G, Paulij WP. Vaccine- and hepatitis B immune globulin-induced escape mutations of hepatitis B virus surface antigen. J Biomed Sci 2001; 8: [PMID: DOI: /BF ] 39 Sheldon J, Soriano V. Hepatitis B virus escape mutants induced by antiviral therapy. J Antimicrob Chemother 2008; 61: [PMID: DOI: /jac/dkn014] 40 Ijaz S, Torre F, Tedder RS, Williams R, Naoumov NV. Novel immunoassay for the detection of hepatitis B surface escape mutants and its application in liver transplant recipients. J Med Virol 2001; 63: [PMID: DOI: / (200103)63] 41 Protzer-Knolle U, Naumann U, Bartenschlager R, Berg T, Hopf U, Meyer zum Büschenfelde KH, Neuhaus P, Gerken G. Hepatitis B virus with antigenically altered hepatitis B surface antigen is selected by high-dose hepatitis B immune globulin after liver transplantation. Hepatology 1998; 27: [PMID: DOI: /hep ] 42 Saab S, Yeganeh M, Nguyen K, Durazo F, Han S, Yersiz H, Farmer DG, Goldstein LI, Tong MJ, Busuttil RW. Recurrence of hepatocellular carcinoma and hepatitis B reinfection in hepatitis B surface antigen-positive patients after liver transplantation. Liver Transpl 2009; 15: [PMID: DOI: / lt.21882] P- Reviewer: Kin T, Taheri S S- Editor: Qi Y L- Editor: A E- Editor: Ma S 3812 April 14, 2016 Volume 22 Issue 14
127 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Retrospective Study ORIGINAL ARTICLE Vascularizing lymph node dissection for advanced gastric cancer: A single-institution experience Fang-Hai Han, Sheng-Ning Zhou, Hong-Ming Li, Yu-Long He, Wen-Hua Zhan Fang-Hai Han, Sheng-Ning Zhou, Hong-Ming Li, Department of Gastrointestinal Surgery, Sun Yat-sen Memorial Hospital of Sun Yat-sen University, Guangzhou , Guangdong Province, China Yu-Long He, Wen-Hua Zhan, Department of Gastrointestinal- Pancreatic Surgery, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou , Guangdong Province, China Author contributions: Han FH and Zhou SN contributed equally to this work; Han FH and Zhou SN designed the research; Zhan WH, He YL and Han FH performed the research; Li HM contributed new reagents or analytic tools; Zhou SN analyzed the data; Han FH and Zhou SN wrote the paper. Institutional review board statement: The study was reviewed and approved by the Ethics Committee of Sun Yat-sen Memorial Hospital. Informed consent statement: All study participants, or their legal guardian, provided verbal informed consent. Conflict-of-interest statement: The authors declare no conflict of interest. Data sharing statement: No additional data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Wen-Hua Zhan, PhD, Department of Gastrointestinal-Pancreatic Surgery, the First Affiliated Hospital of Sun Yat-sen University, No. 58 Zhongshan Erlu, Guangzhou , Guangdong Province, China. wh_zhan@126.com Telephone: Received: October 11, 2015 Peer-review started: October 12, 2015 First decision: December 11, 2015 Revised: December 17, 2015 Accepted: January 17, 2016 Article in press: January 18, 2016 Published online: April 14, 2016 Abstract AIM: To compare the short- and long-term outcomes of vascularizing lymph node dissection (VLND) and nonvascularizing lymph node dissection (NVLND) from a single institution. METHODS: Data of 315 patients with advanced gastric cancer who underwent standard D2 lymphadenectomy with curative intent was collected between January 1994 and December One hundred and fifty-two patients received VLND while 163 patients received NVLND. Short- and long-term clinical outcomes were compared between the two groups. RESULTS: The median followed-up time was 82 mo. The rate of postoperative complications in the VLND group was 13.2%, while that in the NVLND group was 11.7% (P = 0.686). The overall 5-year survival rate was 64% in the VLND group and 59% in the NVLND group (P = 0.047). When subgroup analyses were performed according to Bormann type, type of differentiation and lymph node status, survival benefit was demonstrated in patients with Bormann type Ⅲ or Ⅳ (59% vs 50%, P = 0.032), undifferentiated type (63% vs 49%, P = 0.021) or presence of lymph node metastasis (53% vs 38%, P = 0.010) in the VLND group. CONCLUSION: D2 VLND in advanced gastric cancer treatment allows survival benefit with acceptable morbidity and mortality. VLND for patients with potentially curable advanced gastric cancer is feasible 3813 April 14, 2016 Volume 22 Issue 14
128 Han FH et al. VLND for gastric cancer and safe when performed by a well-trained surgical team. Key words: Gastric cancer; Vascularizing lymph node dissection; Non-vascularizing lymph node dissection; Clinical outcome The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: This study investigates the short- and longterm outcomes of vascularizing lymph node dissection (VLND) and non-vascularizing lymph node dissection (NVLND) from a single institution. The overall 5-year survival rate was 64% in the VLND group and 59% in the NVLND group (P = 0.047). We draw a conclusion that VLND with D2 lymphadenectomy has overall survival benefit for patients with advanced gastric cancer without significant operative complications and mortality if performed by a well-trained and experienced surgical team. If undifferentiated adenocarcinoma is confirmed by endoscopic biopsy preoperatively or macroscopically enlarged regional lymph nodes are found intraoperatively in advanced gastric cancer, VLND with D2 lymphadenectomy may be a considerable alternative. Han FH, Zhou SN, Li HM, He YL, Zhan WH. Vascularizing lymph node dissection for advanced gastric cancer: A singleinstitution experience. World J Gastroenterol 2016; 22(14): Available from: URL: com/ /full/v22/i14/3813.htm DOI: org/ /wjg.v22.i INTRODUCTION Gastric cancer (GC) is the third leading cause of cancer-related deaths in China [1]. Although current therapeutic practice includes neoadjuvant and adjuvant chemotherapy or radiotherapy into the treatment protocol [2], curative gastrectomy with radical lymphadenectomy is the only curative therapy for gastric cancer. An Italian multicenter randomized controlled trial [3,4] showed that subtotal and total gastrectomies, with second-level lymphadenectomy, had similar postoperative complication rate and survival probability, provided that the surgical margin of the resection fell in healthy tissue. The 10-year and the 15-year survival outcomes of Dutch gastric cancer trial showed that D2 dissection may be of benefit, especially for patients with N2 disease [5,6]. A Taiwanese single-institution trial (No. ClinicalTrials.gov NCT ) showed [7] that D3 dissection showed better survival outcome for gastric cancer patients compared with D1 lymphadenectomy if performed by experienced surgeons. Japanese MRCT showed [8] that more extended resection (D2+ para-aortic lymph node dissection) cannot provide survival benefit in curable gastric cancer patients when compared with D2 lymph node dissection alone. Nowadays in China, the majority (about 90%) of gastric cancer patients are diagnosed in advanced stages. Hence, D2 dissection has become the standard procedure for advanced gastric cancer. Numerous studies have shown that surgical specialization and experience as well as surgery volume may contribute to differences in outcomes; the morbidity and mortality vary among different surgeons and in different hospitals [9-11]. However, it has not been reported whether different lymph node dissection techniques would affect the outcome of gastric cancer. Two methods have been applied to dissect the lymph nodes around the artery; one was classified as vascularizing lymph node dissection (VLND) where the dissection is carried out along the plane between the artery adventitia and the vascular sheath, and the other is non-vascularizing lymph node dissection (NVLND) in which the lymph nodes are retrieved outside the vascular sheath with the vascular sheath preserved. So far no randomized controlled trial has been found on the comparison of the two methods. VLND has been performed in our department since the early 1990s. Data of all the patients were collected in the gastric cancer database of our department. The postoperative follow-up data were also included. The present study therefore investigated the long- and short-term clinical outcomes of VLND and NVLND from a single institution. MATERIALS AND METHODS This study was approved by Ethics Committee of Sun Yat-sen Memorial Hospital, Sun Yat-sen University. All patients provided verbal informed consent prior to study enrollment, because all study participants were out of hospital and we contacted them by telephone, message, , etc. Patients Three hundred and fifteen patients with primary GC who underwent radical gastrectomy with D2 lymph node dissection in the Department of Gastrointestinal Surgery, the Affiliated Hospital of Sun Yat-sen University between 1994 and 2006 were studied. Among these patients, 152 received VLND, and 163 received NVLND. Eligibility In this study, the inclusion criteria before surgical procedure were as follows: (1) histologically proven primary gastric cancer; (2) potentially curable by radial gastrectomy with D2 lymphadenectomy [Japanese Gastric Cancer Association (JGCA) guidelines]; (3) physical tolerance to radical operation; (4) age younger than 75 years; (5) no neoadjuvant chemotherapy or radiotherapy before surgery; (6) no concomitant other cancer; and (7) no previous gastrectomy April 14, 2016 Volume 22 Issue 14


129 Han FH et al. VLND for gastric cancer 367 patients were eligible A B 367 had elective gastrectomy 52 were excluded according to intraoperative findings 41 early cancer 4 esophageal involvement 5 para-aortic lymph node enlargement 2 liver metastatic nodules 315 patients were analyzed Figure 2 Vascularizing (A) and non-vascularizing lymph node dissection (B). Yellow lines indicate the dissection planes around the vessels. 152 in VLND group 163 in NVLND group Figure 1 Eligibility and exclusion. VLND: Vascularizing lymph node dissection; NVLND: Non-vascularizing lymph node dissection. Exclusion criteria Exclusion criteria were as follows (intraoperative findings): (1) early gastric cancer (T0 or T1); (2) enlarged lymph nodes were found around paraaortic or the hepatoduodenal ligament regions; (3) esophageal involvement; and (4) distant metastasis. Three hundred and sixty-seven patients met the inclusion criteria, and 52 of them were excluded because they did not meet the exclusion criteria as Figure 1 shows: 41 cases were found with early gastric cancer, 4 cases were found with esophageal involvement, 5 cases were found with para-aortic lymph nodes enlargement and 2 cases were found with liver metastatic nodules intraoperatively. Finally, data of 315 cases underwent statistic analysis (152 cases in the VLND group and 163 cases in the NVLND group). Surgery Lymph node dissection was standardized according to the JGCA Guidelines [12]. All patients underwent radical gastrectomy with D2 lymph node resection for curative intent. The stomach, lesser omentum, greater omentum, anterior leaf of transverse mesocolon, capsula pancreatis and lymph nodes were included in the resection. When proximal gastrectomies were performed, Nos. 1, 2, 3a, 4sa, 4sb, 7, 8a, 9, and 11p lymph nodes were removed. A total gastrectomy included the dissection of Nos. 1, 2, 3, 4, 5, 6, 7, 8a, 9, 10, 11p, 11d, and 12a lymph nodes. For distal gastrectomy, Nos. 1, 3, 4sb, 4d, 5, 6, 7, 8a, 9, 10, 11p and 12a lymph nodes were removed. At least 15 lymph nodes were retrieved and examined. After the surgery, perigastric lymph nodes were dissected immediately and sent for histopathological examination. Tumors were staged according to the latest version of the pathologic classification of the Union for International Cancer Control (UICC). When the cases underwent VLND, the vascular sheath of the artery and the dense fibrous tissue were peeled to expose the tunica adventitia. The loose layer between the vascular sheath and the tunica adventitia was accessed, and the lymph nodes around the artery together with the vascular sheath could be dissected promptly and easily (Figure 2A). In this way, all the anatomic structures in the upper abdominal floor were skeletonized, so that at the end of the procedure the surgical field resembled that seen in an anatomic atlas (Figure 3). As for NVLND, however, dissection was performed outside the vascular sheath, leaving the vascular sheath unopened (Figure 2B). Quality control The standard procedure was set up by Zhan WH. All surgeons had completed at least 20 gastrectomies with VLND and 20 gastrectomies with NVLND independently before the beginning of this study (Before January 1994). The UICC TNM staging system was used [13]. Follow-up and statistical analysis The median followed-up time was 82 mo (83 mo in the VLND group and 80 mo in the NVLND group, P = 0.475). Assessments were performed in a followup program every 3 mo during the first 3 years after surgery, then every 6 mo during the next 2 years, and annually thereafter until the patient s death. Statistical analyses were performed with software SPSS 16.0 G for Windows. The clinical and pathological variables were compared using the Fisher s exact test and Wilcoxon test, and P < 0.05 was considered statistically significant. The primary endpoints were recurrence free survival and overall survival. Comparisons were made by the log-rank test when using the Kaplan- Meier method. RESULTS Three hundred and sixty-seven patients met the inclusion criteria, and 52 of them were excluded April 14, 2016 Volume 22 Issue 14

 and 35.9% were female (113/315). The mean ages of the VLND and NVLND groups were 55.")

130 Han FH et al. VLND for gastric cancer A Op. date: 3 July , F, 30 y Table 1 Clinicopathological characteristics of patients Group VLND NVLND P value B C 16a1 CA 16a2 No16b1 SMA No16b2 Figure 3 Surgical field of a case that underwent partial D2 gastrectomy with vascularizing lymph node dissection. Finally, data of 315 cases were analyzed (152 cases in the VLND group and 163 cases in the NVLND group). Among the 315 patients with gastric cancer who underwent standard D2 lymphadenectomy, 64.1% were male (202/315) and 35.9% were female (113/315). The mean ages of the VLND and NVLND groups were ± years and ± years, respectively. The clinicopathological characteristics of all patients are showed in Table 1. No statistical difference was found between the two groups in terms of sex, age, macroscopic histological type, tumor site or size. No significant differences were demonstrated in operative procedures or postoperative pathological parameters either. The number of harvested lymph nodes was ± in the VLND group and ± in the NVLND group (P = 0.307). The number of involved lymph nodes in the VLND and NVLND groups were 4.41 and 5.30, respectively (P = 0.717). Total gastrectomy No. of cases Sex Male Female Age (yr), mean ± SD ± ± Tumor location Upper stomach Middle stomach Lower stomach Whole stomach 3 5 Tumor size (cm), mean ± SD 4.59 ± ± Bormann type Ⅰ or Ⅱ Ⅲ or Ⅳ Postoperative stay (d) Blood transfusion Absent Present Mean operation time ± ± Gastrectomy Total Subtotal Type of reconstruction Roux-en-Y Billroth Ⅰ 7 9 Billroth Ⅱ Pathological classification and differentiation Differentiated Undifferentiated Retrieved nodes, mean ± SD ± ± Metastatic nodes, mean ± SD 4.41 ± ± pt stage T T T T pn stage N N N N VLND: Vascularizing lymph node dissection; NVLND: Non-vascularizing lymph node dissection. was performed in 58 patients who underwent VLND and in 76 patients who underwent NVLND. The median operation time was ± min in the VLND group and ± min in the NVLND group, and there was no significant difference between the two groups (P = 0.931). Morbidity and mortality No significant difference was observed in postoperative complications between the VLND and NVLND groups (13.2% vs 11.7%, P = 0.686). Table 2 lists all the postoperative complications. As shown, intraabdominal infection, pulmonary complications, ileus, catheter-related infection and abdominal hemorrhage were the most common complications. There were no deaths during hospital stay April 14, 2016 Volume 22 Issue 14
131 Han FH et al. VLND for gastric cancer Table 2 Postoperative complications after gastrectomy Complication VLND NVLND P value Anastomotic leakage 1 1 Duodenal stump leak 1 2 Biliary fistula 2 0 Pancreatic fistula 1 0 Ileus 2 4 Lymphorrhea 2 0 Abdominal hemorrhage 3 1 Intra-abdominal infection 3 5 Pulmonary complications 3 4 Catheter-related infection 2 2 Total VLND: Vascularizing lymph node dissection; NVLND: Non-vascularizing lymph node dissection. Overall survival The overall 5-year survival rate was 64% in the VLND group and 59% in the NVLND group (log-rank test P = 0.047; Figure 4A). Survival by Bormann type Among patients with Bormann type Ⅰ or Ⅱ cancer, the overall 5-year survival rate was 81% in the VLND group and 79% in the NVLND group (log-rank test, P = 0.902). However, a significant difference was found between the two groups among patients with Bormann type Ⅲ or Ⅳ cancer. The overall 5-year survival rates of the VLND and NVLND groups were 59% and 50%, respectively (log-rank test, P = 0.032; Figure 4B). Survival by type of differentiation For differentiated GC, the overall 5-year survival rate was 81% for the VLND group and 79% for the NVLND group (log-rank test, P = 0.282). For patients with undifferentiated GC, however, VLND could improve the overall 5-year survival rate by more than 10% (63% for the VLND group vs 49% for the NVLND group, logrank test, P = 0.021; Figure 4C). Survival by status of lymph node metastasis Among patients without lymph node metastasis, no significant difference was found between the two groups. The overall 5-year survival rate was 86% in the VLND group and 82% in the NVLND group (log-rank test, P = 0.222). However, the overall 5-year survival rate was 53% in the VLND group and 38% in the VLND group among patients with regional lymph node metastasis, thus a significant difference was observed (log-rank test, P = 0.010; Figure 4D). DISCUSSION Long-term clinical outcomes of GC were variable according to several published studies [14-16], which can be affected by the physical condition, tumor growth, treatment protocol, and the scrutiny of pathological assessment. The results of the surgical treatment will differ if the patient is old, obese, or with co-morbid conditions such as diabetes and cardiovascular illness. The knowledge, skill and experience of the surgical team, the extent of lymph node dissection, pathological sampling and pathological diagnosis all affect the pathological staging [17-20]. The extent as well as the technique of nodal clearance is of significant influence on surgical quality of lymph node dissection [21-24]. However, the prognostic impact of different lymph node dissection techniques has not been reported in the literature. In our study, the impact of different lymph node dissection techniques on the short- and long-term clinical outcomes in patients with advanced gastric cancer who underwent radical operation was investigated on the basis of strict surgical quality control. In this setting, the application of VLND to advanced gastric cancer requires a surgical team who has rich experience in radical gastrectomy, familiarity with vascular surgery technique and a good understanding of anatomical structure. The surgical learning period for VLND extends to at least 20 cases. When NVLND was employed, the lymph nodes in the upper abdominal floor were removed leaving the vascular sheath intact and unopened. Our hospital has a high volume of GC surgery in China. Radical gastrectomy with D2 lymphadenectomy has commonly been carried out here. All involved surgeons in our department were experienced and had accomplished at least 20 gastrectomies with VLND and 20 gastrectomies with NVLND independently before the study. The standard procedure was set up and all surgeons did both VLND and NVLND. Hence, there were no deaths for postoperative complications in both groups, although the overall morbidity rate was slightly higher in the VLND group than in the NVLND group (13.2% vs 11.7%, P = 0.686). When complications were considered independently, no complication could reach a statistically significant difference between the two groups. The limitation of this study may be as follows: (1) the vascular sheath and the soft tissue between the vascular sheath and the tunica adventitia may be involved in some patients with advanced gastric cancer, thus VLND could reach better regional control. However, the lack of pathological data which can provide evidence of metastasis makes it less compelling; and (2) all the surgical procedures in our study were performed by several experienced surgeons in a single institution. Some more prospective randomized controlled trials are needed to support our results. In conclusion, the short- and long-term clinical outcomes of VLND and NVLND were studied and reported in a single institution. Data from our study demonstrated that VLND with D2 lymphadenectomy has overall survival benefit for patients with advanced gastric cancer without significant operative complications and mortality if performed by a well-trained and experienced surgical team. If undifferentiated adenocarcinoma 3817 April 14, 2016 Volume 22 Issue 14
132 Han FH et al. VLND for gastric cancer A Cum survival VLND n = 152 NVLND n = months after operation B 1.0 Borrmann Ⅰ or Ⅱ 1.0 Borrmann Ⅲ or Ⅳ Cum survival Cum survival VLND 0.2 VLND NVLND NVLND months after operation months after operation C 1.0 Differentiated 1.0 Undifferentiated Cum survival Cum survival VLND 0.2 VLND NVLND NVLND D months after operation Lymph node (-) months after operation Lymph node (+) Cum survival Cum survival VLND 0.2 VLND NVLND NVLND months after operation months after operation Figure 4 Survival analysis. A: Overall survival of VLND and NVLND groups; B: Survival according to Bormann type; C: Survival according to type of differentiation; D: Survival according to lymph node status. VLND: Vascularizing lymph node dissection; NVLND: Non-vascularizing lymph node dissection April 14, 2016 Volume 22 Issue 14
133 Han FH et al. VLND for gastric cancer is confirmed by endoscopic biopsy preoperatively or macroscopically enlarged regional lymph nodes are found intraoperatively in advanced gastric cancer, VLND with D2 lymphadenectomy may be a considerable alternative. COMMENTS Background Gastric cancer is the third leading cause of cancer-related deaths in China. Nowadays in China, the majority (about 90%) of gastric cancer patients are diagnosed in advanced stages. Hence, D2 dissection has become the standard procedure for advanced gastric cancer. However, it has not been reported whether different lymph node dissection techniques would affect the outcome of gastric cancer. Two methods have been applied to dissect the lymph nodes around the artery, and one was classified as vascularizing lymph node dissection (VLND) where the dissection is carried out along the plane between the artery adventitia and the vascular sheath. Non-vascularizing lymph node dissection (NVLND) is a technique in which the lymph nodes are retrieved outside the vascular sheath with the vascular sheath preserved. So far no randomized controlled trial has been found on the comparison of the two methods from a single institution. Research frontiers The appropriate degree of curative lymph node dissection remains controversial between Western and Eastern countries. There is still ambiguity in comparison between laparoscopic and open operation for gastric cancer. Innovations and breakthroughs It has not been reported whether different lymph node dissection techniques would affect the outcome of gastric cancer. This study found that D2 VLND in advanced gastric cancer treatment allows survival benefit and acceptable mortality and morbidity. Applications VLND with D2 lymphadenectomy has overall survival benefit for patients with advanced gastric cancer if performed by a well-trained and experienced surgical team. In radical operation for advanced gastric cancer, VLND with D2 lymphadenectomy may be a considerable alternative. Terminology VLND: Lymph nodes around the vessels, as well as the vascular sheath of the artery and the dense fibrous tissue are peeled to expose the tunica adventitia. Peer-review The authors investigated the short- and long-term outcomes of VLND and NVLND. They show that D2 VLND in advanced gastric cancer treatment allows survival benefit and acceptable morbidity and mortality. They emphasize that if undifferentiated adenocarcinoma is confirmed by endoscopic biopsy preoperatively or macroscopically enlarged regional lymph nodes are found intraoperatively in advanced gastric cancer, VLND with D2 lymphadenectomy would be a considerable alternative. Their findings are interesting and useful for the future treatment of advanced gastric cancer. REFERENCES 1 IARC GLOBOCAN 2008: Cancer Incidence, Mortality and Prevalence Worldwide. Available from: URL: fr 2 Lacueva J, Gallego J, Díaz-González JA. Updating controversies on the multidisciplinary management of gastric cancer. Clin Transl Oncol 2010; 12: [PMID: DOI: / s ] 3 Bozzetti F, Marubini E, Bonfanti G, Miceli R, Piano C, Gennari L. Subtotal versus total gastrectomy for gastric cancer: five-year survival rates in a multicenter randomized Italian trial. Italian Gastrointestinal Tumor Study Group. Ann Surg 1999; 230: [PMID: DOI: / ] 4 Bozzetti F, Marubini E, Bonfanti G, Miceli R, Piano C, Crose N, Gennari L. Total versus subtotal gastrectomy: surgical morbidity and mortality rates in a multicenter Italian randomized trial. The Italian Gastrointestinal Tumor Study Group. Ann Surg 1997; 226: [PMID: DOI: / ] 5 Hartgrink HH, van de Velde CJ, Putter H, Bonenkamp JJ, Klein Kranenbarg E, Songun I, Welvaart K, van Krieken JH, Meijer S, Plukker JT, van Elk PJ, Obertop H, Gouma DJ, van Lanschot JJ, Taat CW, de Graaf PW, von Meyenfeldt MF, Tilanus H, Sasako M. Extended lymph node dissection for gastric cancer: who may benefit? Final results of the randomized Dutch gastric cancer group trial. J Clin Oncol 2004; 22: [PMID: DOI: /JCO ] 6 Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol 2010; 11: [PMID: DOI: /S (10)70070-X] 7 Wu CW, Hsiung CA, Lo SS, Hsieh MC, Chen JH, Li AF, Lui WY, Whang-Peng J. Nodal dissection for patients with gastric cancer: a randomised controlled trial. Lancet Oncol 2006; 7: [PMID: DOI: /S (06) ] 8 Sasako M, Sano T, Yamamoto S, Kurokawa Y, Nashimoto A, Kurita A, Hiratsuka M, Tsujinaka T, Kinoshita T, Arai K, Yamamura Y, Okajima K. D2 lymphadenectomy alone or with para-aortic nodal dissection for gastric cancer. N Engl J Med 2008; 359: [PMID: DOI: /NEJMoa ] 9 Sasako M. Clinical trials of surgical treatment of malignant diseases. Int J Clin Oncol 2005; 10: [PMID: DOI: /s ] 10 Peeters KC, van de Velde CJ. Surgical quality assurance in breast, gastric and rectal cancer. J Surg Oncol 2003; 84: [PMID: DOI: /jso.10312] 11 Hartgrink HH, van de Velde CJ. Status of extended lymph node dissection: locoregional control is the only way to survive gastric cancer. J Surg Oncol 2005; 90: [PMID: DOI: /jso.20222] 12 Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma - 2nd English Edition - Gastric Cancer 1998; 1: [PMID: DOI: /PL ] 13 Page DL, Fleming ID, Fritz A. AJCC Cancer Staging Manual. 6th ed. Philadelphia: Lippincott-Raven, Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL, Batista I, Welch HG, Wennberg DE. Hospital volume and surgical mortality in the United States. N Engl J Med 2002; 346: [PMID: DOI: /NEJMsa012337] 15 Birkmeyer JD, Sun Y, Wong SL, Stukel TA. Hospital volume and late survival after cancer surgery. Ann Surg 2007; 245: [PMID: DOI: /01.sla dd] 16 Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume and operative mortality in the United States. N Engl J Med 2003; 349: [PMID: DOI: /NEJMsa035205] 17 Lee JH, Ryu KW, Lee JH, Park SR, Kim CG, Kook MC, Nam BH, Kim YW, Bae JM. Learning curve for total gastrectomy with D2 lymph node dissection: cumulative sum analysis for qualified surgery. Ann Surg Oncol 2006; 13: [PMID: DOI: /s ] 18 Weitz J, Koch M, Friess H, Büchler MW. Impact of volume and specialization for cancer surgery. Dig Surg 2004; 21: [PMID: DOI: / ] 19 Chowdhury MM, Dagash H, Pierro A. A systematic review of the impact of volume of surgery and specialization on patient outcome. Br J Surg 2007; 94: [PMID: DOI: / bjs.5714] 20 Kim JP. Surgical results in gastric cancer. Semin Surg Oncol 1999; 3819 April 14, 2016 Volume 22 Issue 14
134 Han FH et al. VLND for gastric cancer 17: [PMID: DOI: /(SICI) ( )17:2<132::AID-SSU8>3.0.CO;2-E] 21 Harrison LE, Choe JK, Goldstein M, Meridian A, Kim SH, Clarke K. Prognostic significance of immunohistochemical micrometastases in node negative gastric cancer patients. J Surg Oncol 2000; 73: [PMID: DOI: /(SICI) (200003)73:3<153::AID-JSO8>3.0.CO;2-4] 22 Cai J, Ikeguchi M, Maeta M, Kaibara N. Micrometastasis in lymph nodes and microinvasion of the muscularis propria in primary lesions of submucosal gastric cancer. Surgery 2000; 127: [PMID: DOI: /msy ] 23 Takeuchi H, Kitagawa Y. Is lymphadenectomy a predictor or savior for patients with gastric cancer? Ann Surg Oncol 2010; 17: [PMID: DOI: /s ] 24 Nakajima T. Gastric cancer treatment guidelines in Japan. Gastric Cancer 2002; 5: 1-5 [PMID: DOI: /s ] P- Reviewer: Ando T S- Editor: Yu J L- Editor: Wang TQ E- Editor: Ma S 3820 April 14, 2016 Volume 22 Issue 14
135 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Retrospective Study ORIGINAL ARTICLE Early enteral nutrition vs parenteral nutrition following pancreaticoduodenectomy: experience from a single center Jian-Wen Lu, Chang Liu, Zhao-Qing Du, Xue-Min Liu, Yi Lv, Xu-Feng Zhang Jian-Wen Lu, Chang Liu, Zhao-Qing Du, Yi Lv, Xu-Feng Zhang, Department of Hepatobiliary Surgery and Institute of Advanced Surgical Technology and Engineering, the First Affiliated Hospital of Xi an Jiaotong University, Xi an , Shaanxi Province, China Jian-Wen Lu, Chang Liu, Zhao-Qing Du, Yi Lv, Xu-Feng Zhang, Shaanxi Provincial Regenerative Medicine and Surgical Engineering Research Center, Xi an , Shaanxi Province, China Xue-Min Liu, Department of Health Statistics, the First Affiliated Hospital of Xi an Jiaotong University, Xi an , Shaanxi Province, China Author contributions: Lu JW, Lv Y and Zhang XF contributed equally to this work; Zhang XF and Lv Y conceived and designed the experiments; Lu JW, Liu C and Yin GZ performed the experiments; Lu JW, Liu XM and Du ZQ analyzed the data; Lu JW and Liu XM contributed reagents/materials/analysis tools; Lu JW, Lv Y and Zhang XF wrote the paper. Supported by the National Natural Science Foundation, No ; New-Star Young Scientists Program of Shaanxi Province, No. 2014kjxx-30; and the Fundamental Research Funds for the Central Universities. Institutional review board statement: The study was reviewed and approved by the First Affiliated Hospital of Xi an Jiaotong University Institutional Review Board. Informed consent statement: Informed written consent was provided by each participant or the participant s legal guardian prior to enrollment in the study. Conflict-of-interest statement: The authors have declared that no competing interests exist. Data sharing statement: Technical appendix, statistical code, and dataset available from the corresponding author at the following address: xfzhang125@126.com. The participants gave informed consent for data sharing. No additional data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Xu-feng Zhang, MD, PhD, Department of Hepatobiliary Surgery and Institute of Advanced Surgical Technology and Engineering, the First Affiliated Hospital of Xi an Jiaotong University, Xi an , Shaanxi Province, China. xfzhang125@126.com Telephone: Fax: Received: August 30, 2015 Peer-review started: September 1, 2015 First decision: September 29, 2015 Revised: October 22, 2015 Accepted: December 30, 2015 Article in press: December 30, 2015 Published online: April 14, 2016 Abstract AIM: To analyze and compare postoperative morbidity between patients receiving total parenteral nutrition (TPN) and early enteral nutrition supplemented with parenteral nutrition (EEN + PN). METHODS: three hundred and forty patients receiving pancreaticoduodenectomy (PD) from 2009 to 2013 at our center were enrolled retrospectively. Patients were divided into two groups depending on postoperative nutrition support scheme: an EEN + PN group (n = 87) and a TPN group (n = 253). Demographic characteristics, comorbidities, preoperative biochemical 3821 April 14, 2016 Volume 22 Issue 14
136 Lu JW et al. Efficacy comparison of post-pancreaticoduodenectomy nutrition modes parameters, pathological diagnosis, intraoperative information, and postoperative complications of the two groups were analyzed. RESULTS: The two groups did not differ in demographic characteristics, preoperative comorbidities, preoperative biochemical parameters or pathological findings (p > 0.05 for all). However, patients with EEN + PN following PD had a higher incidence of delayed gastric emptying (16.1% vs 6.7%, p = 0.016), pulmonary infection (10.3% vs 3.6%, p = 0.024), and probably intraperitoneal infection (18.4% vs 10.3%, p = 0.059), which might account for their longer nasogastric tube retention time (9 d vs 5 d, p = 0.006), postoperative hospital stay (25 d vs 20 d, p = 0.055) and higher hospitalization expenses (USD10397 vs USD8663.9, p = 0.008), compared to those with TPN. CONCLUSION: Our study suggests that TPN might be safe and sufficient for patient recovery after PD. Postoperative EEN should only be performed scrupulously and selectively. Key words: Pancreaticoduodenectomy; Postoperative complications; Enteral nutrition; Parenteral nutrition; Delayed gastric emptying The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Although most studies have shown that early enteral nutrition (EEN) seems to be superior to total parenteral nutrition (TPN) in postoperative outcomes, the optimal nutritional support route choice after pancreaticoduodenectomy (PD) remains debatable. In this retrospective study, we investigated postoperative outcomes between patients undergoing TPN and EEN + PN after PD. The results demonstrated that the EEN + PN group had an increased morbidity of delayed gastric emptying and pulmonary infection, which might account for longer nasogastric tube retention time, postoperative hospital stay and higher hospitalization expenses. In our opinion, EEN should only be performed cautiously and selectively. operatively, many candidates for PD are in a state of disease/comorbidities-associated malnutrition; aggravating this situation, surgery causes disorganization of the digestive arrhythmic and absorptive functions, leading to worsening postoperative indigestion and malabsorption, which accounts for the high morbidity rate of PD-related complications [2], and this is combined with the difficulty of the nil per os period during the first days after surgery. Hence, appropriate nutritional therapy is of great significance for postoperative rehabilitation following PD. Nutrition support strategies have undergone tremendous evolution in the decades following the first application of total parenteral nutrition (TPN) in postoperative patients [3]. Recent studies have elaborated that early enteral nutrition (EEN) could improve immune capability, maintain intestinal barrier function, and potentially moderate metabolic stress reactions caused by surgical intervention, thereby reducing the incidence of postoperative complications [4-8]. Moreover, EEN is thought to be a more reliable and economic solution for postoperative nutritional support compared with parenteral nutrition (PN) [6,7]. Currently, this is the mainstream view. Some studies, however, have claimed that EEN is insignificant or even negative in decreasing complication morbidity rates after abdominal surgery [9-17] ; thus, the role of EN remains debatable. On the other hand, with improvements in central venous catheter care and progress in energy supply (isocaloric or hypocaloric formulas), PN-associated morbidity has significantly decreased in high-volume centers. Because decided evidence in respect of the first-rank nutrition strategy following PD remains absent, feeding route decision relies prevailingly on the surgeon s subjective perspective. The objective of our research was to compare the incidence of postoperative complications between patients undergoing TPN and EEN by placing a nasojejunal catheter combined with additional PN [considering the universally recognized adverse effects of total enteral nutrition (TEN) such as diarrhoea, abdominal tympany, and abdominalgia]. Lu JW, Liu C, Du ZQ, Liu XM, Lv Y, Zhang XF. Early enteral nutrition vs parenteral nutrition following pancreaticoduodenectomy: Experience from a single center. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Since its introduction by Whipple in 1935, pancreaticoduodenectomy (PD) has been considered an irreplaceable treatment choice for carcinoma of the periampullary region and some benign lesions [1]. Pre- MATERIALS AND METHODS Patient selection From February 2009 to January 2013, patients receiving classic PD and Child s reconstruction were retrospectively enrolled in this study at Xi an Jiaotong University First Affiliated Hospital. Exclusion criteria included preoperative ongoing infection, inflammatory bowel disease, severe renal insufficiency and history of previous gastrointestinal surgery. In order to avoid the interference of variable PD patterns, patients subjected to pylorus-preserving PD, total PD, or Roux-en-Y choledochojejunostomy were also excluded. Finally, 340 patients undergoing PD were enrolled in this study. Data including patients demographic characteristics, 3822 April 14, 2016 Volume 22 Issue 14
137 Lu JW et al. Efficacy comparison of post-pancreaticoduodenectomy nutrition modes laboratory results, pathological diagnosis of resected lesions, intraoperative information and postoperative complications were registered on specific forms. The study was reviewed and approved by the First Affiliated Hospital of Xi an Jiaotong University ethics committee. Surgical procedures All operations were performed by six experienced senior surgeons. 87 and 253 cases received EEN + PN and only TPN, respectively. Preoperatively, nurses introduced a nasojejunal nutrition tube (NJT) [10/F, Nutricia Pharmaceutical (Wuxi) Co., China] through the nasal cavity, together with a nasogastric tube (NGT) [10/F, Nutricia Pharmaceutical (Wuxi) Co., China]. The decision to place an intraoperative jejunum feeding tube was more frequently determined by the surgeon s discretion rather than the patient s preoperative status. Child s procedures were standardized, with pancreatojejunostomy performed initially, and pancreatic duct stent was used as occasion demands. Interrupted jejunal muscularis serosapancreas sutures were made at the outer layer. Endto-side cholangioenterostomy was performed cm distal to the pancreatojejunal anastomotic stoma, and gastrojejunostomy cm distal to the cholangioenteral anastomosis. The NJT was then positioned cm distal to the gastrointestinal anastomosis by surgeons, and attached to the nose wing with surgical silk thread (4-0) and tape. Before abdominal closure, two rubber drainage tubes were routinely placed into the abdominal cavity (behind the pancreatojejunal and cholangioenteral anastomosis, respectively), with their external openings linked to anti-reflux negative-pressure drainage bags. Postoperative management Barring special circumstances (such as serious complications or comorbidities in need of strict monitoring), patients remained in the ICU for the first postoperative h. Unless sustained antibiotic treatment was necessary (like for severe sepsis, etc.), prophylactic antibiotics were discontinued after the first h. Both groups began parenteral nutrition through a central venous catheter on the first postoperative day. Then, the EEN + PN group was administered enteral nutrition through the NJT from the second day after surgery, with an initial volume of 500 ml (1 Kcal/ml, protein 4.5 g/100 ml, carbohydrate 14.3 g/100 ml, lipid 2.8 g/100 ml). The total calories and protein intake for both groups were maintained at Kcal/(kg d) and g/(kg d), respectively. The initial delivery rate was 30 ml/h, increasing gradually to normal intake in 48 h depending on patients condition. Once the patient had passed flatus, the nasogastric tube was clipped and an oral liquid diet was gradually started, beginning with small volumes. The volume of liquid diet via NJT or TPN was gradually decreased once the patient could tolerate oral intake, and was finally discontinued once the patient could eat regularly, followed by removal of the nasogastric tube and NJT. If the patient experienced abdominal distension, nausea or vomiting, the nasogastric tube was re-aspirated and the feeding was slowed or stopped temporarily. The character and volume of the abdominal drainage fluid were observed twice a day, and the drainage fluid amylase was examined if a pancreatic fistula was suspected. Routine ultrasound was used to detect any fluids in the abdominal cavity before removal of the drainage tubes. Postoperative morbidity The definition and classification of delayed gastric emptying (DGE) were based on International Study Group of Pancreatic Surgery (ISGPS) recommendations as follows: Grade A, demanding an NGT intubation or reinsertion between postoperative day (POD) 4 and POD 7 or intolerance to a solid diet by POD 7; Grade B, demanding an NGT intubation or reinsertion between POD 8 and POD 14 or intolerance to a solid diet by POD 14; and Grade C, demanding an NGT intubation or reinsertion after POD 14 or intolerance to a solid diet by POD 21 [18]. The definition of pancreatic fistula was based on ISGPS criteria as calculable intraperitoneal drainage volume on or after POD3 with concentration of amylase at least 3 times the serum normal upper limit [19,20]. Definition of bile leakage was based on the International Study Group of Liver Surgery as a bilirubin content of the drainage fluid 3 times or greater than the serum content on or after POD3 or requiring imaging or surgical treatment arising from choleperitonitis or bile collections [21]. Statistical analysis Quantitative variables are presented as the mean ± SE or median, and percentages for qualitative variables. The Mann-Whitney U test or Student s t-test was applied for quantitative variables, and the χ 2 test or Fisher s exact test for qualitative variables. Statistical analyses were completed with SPSS 21.0 software (Chicago, IL, United States). P-values less than 0.05 were defined statistically significant. RESULTS Patient characteristics Table 1 shows the comparison of patients demographic characteristics, comorbidities, and preoperative serum biochemical levels between the two groups. There were no significant differences in all the baseline characteristics between the two groups. Pathological variables The postoperative pathological diagnosis results of the two groups are shown in Table 2. Pancreatic adenocar April 14, 2016 Volume 22 Issue 14
138 Lu JW et al. Efficacy comparison of post-pancreaticoduodenectomy nutrition modes Table 1 General characteristics, comorbidities, and preoperative lab tests n (%) EEN + PN (n = 87) TPN (n = 253) P value Sex (male) 43 (49.4) 155 (61.3) Age (yr) 58 ± ± Smoking pack-years ( 20) 11 (12.6) 27 (10.7) Alcoholic abuse 8 (9.2) 41 (16.2) BMI 25.8 ± ± Body weight loss (n) > 10% 27 (31.0) 86 (34.0) Comorbidities CAD 5 (5.7) 14 (5.5) Hypertension 16 (18.4) 43 (17.0) Diabetes mellitus 9 (10.3) 25 (9.9) COPD 3 (7.0) 14 (5.5) ASA classification 3 53 (60.9) 149 (58.9) Hemoglobin (g/l) ± ± Leukocytes ( 10 9 /L) 7.0 ± ± Platelet ( 10 9 /L) ± ± Total bilirubin (μmol/l) ± ± Alanine aminotransferase ± ± (U/L) Aspartate aminotransferase ± ± (U/L) Albumin (ng/ml) 43.7 ± ± Prothrombin time (s) 12.6 ± ± Fibronectin 4.5 ± ± Carcinoembryonic antigen 12.8 ± ± (U/mL) CA-125 (U/mL) 22.6 ± ± CA19-9 (U/mL) ± ± BMI: Body mass index; EEN: Early postoperative enteral nutrition; PN: Parenteral nutrition; TPN: Total parenteral nutrition; CAD: Coronary atherosclerotic heart disease; COPD: Chronic obstructive pulmonary diseases; ASA: The American Society of Anesthesiologists. cinoma, bile duct adenocarcinoma and duodenal/ampullary adenocarcinoma were the top three common pathological patterns, accounting for 91.9% in the EEN + PN group and 88.7% in the TPN group. No significant differences existed in pathological types between the two groups (P > 0.05 for all). Operation details and postoperative recovery Table 3 shows the details of intraoperative information and postoperative recovery. There were no differences between the two groups in maximum tumor diameter, pancreatic/bile duct diameter, intraoperative bleeding volume, proportion of retrocolic choledochojejunostomy or combined vascular resection. However, the nasogastric tube retention time in the EEN + PN group was significantly longer (9 ± 0.2 d vs 5 ± 0.1 d, P = 0.006). The overall and postoperative hospitalization time in the EEN + PN group tended to be longer than those of the TPN group, although these were not significantly different (32 ± 2 d vs 27 ± 1 d, p = 0.074; and 25 ± 2 d vs 20 ± 1 d, p = 0.055). Finally, the results showed that the total costs were significantly higher in the EEN + PN group (USD ± vs USD ± 239.2, P = 0.008). Table 2 Pathological diagnosis of the primary disease n (%) Pathology EEN + PN (n = 87) TPN (n = 253) P value Pancreatic 24 (27.6) 82 (32.4) adenocarcinoma Bile duct adenocarcinoma 29 (33.3) 76 (30.0) Duodenal/ampullary 27 (31.0) 64 (25.3) adenocarcinoma Neuroendocrine tumor 2 (2.3) 4 (1.6) Pancreatic 1 (1.1) 5 (2.0) pseudopapillary tumor Cystic pancreatic tumor 1 (1.1) 3 (1.2) Chronic pancreatitis/ pancreatolithiasis 3 (3.4) 19 (7.5) EEN: Early postoperative enteral nutrition; PN: Parenteral nutrition; TPN: Total parenteral nutrition. Table 3 Intraoperative findings and postoperative presentation n (%) EEN + PN (n = 87) TPN (n = 253) P value Diameter of pancreatic duct 0.7 ± ± (cm) Diameter of bile duct (cm) 1.8 ± ± Tumor max-diameter (cm) 3.7 ± ± Retrocolic 85 (97.7) 227 (89.7) choledochojejunostomy Combined vascular resection 2 (2.3) 10 (4.3) Intraoperative bleeding 753 ± ± volume (ml) Intraoperative blood 15 (17.2) 69 (27.3) transfusion Duration of surgery (min) ± ± Nasogastric tube retention (d) 9 ± ± Hospital stay (d) 32 ± 2 27 ± Postoperative hospital stay (d) 25 ± 2 20 ± Total cost (US dollars) ± ± EEN: Early postoperative enteral nutrition; PN: Parenteral nutrition; TPN: Total parenteral nutrition. Postoperative complications Table 4 presents postoperative complications. The morbidity of pulmonary infection and DGE was significantly higher in the EEN + PN group (10.3% vs 3.6%, P = and 16.1% vs 6.7%, P = 0.016, respectively). In addition, the incidence of abdominal cavity infection seemed to be higher in the EEN + PN group (18.4% vs 10.3%, P = 0.059). No significant differences were shown in other surgery-related complications, involving bile leakage, pancreatic fistula, intraperitoneal bleeding, gastrointestinal bleeding, pulmonary embolism, chylous leakage or wound infection (P > 0.05 for all). Four of 87 (4.6%) patients in the EEN + PN group underwent unplanned second operation for intraperitoneal hemorrhage (1 case), severe choleperitonitis (2 cases) and intraperitoneal bleeding combined with severe bile leakage (1 case), 3824 April 14, 2016 Volume 22 Issue 14
139 Lu JW et al. Efficacy comparison of post-pancreaticoduodenectomy nutrition modes Table 4 Postoperative complications n (%) and eventually, 2 of these patients died of multiple organ dysfunction syndrome (MODS). Seven of 253 (2.8%) patients in the TPN group underwent unexpected reoperation due to intraperitoneal bleeding (3 cases), severe bile leakage (2 cases), complicated anastomotic failure (1 case) and wound dehiscence (1 case), and 4 of these patients died from MODS and serious systemic infection. There were no significant differences in the incidence of unplanned reoperation or in-hospital mortality (P = and P = 0.204, respectively). Moreover, 28 (32.2%) patients in the EEN + PN group developed EN-related complications, including abdominal distention (17 cases), abdominal cramps (15 cases), vomiting (10 cases) and diarrhea (9 cases), most of which were attenuated by decreasing the enteral feeding infusion speed or by administering prokinetic agents, and no discontinued enteral feeding occurred in these patients. DISCUSSION EEN + PN (n = 87) TPN (n = 253) P value Bile leakage 7 (8.0) 12 (4.7) Pancreatic fistulas 13 (14.9) 27 (10.7) Intraperitoneal infection 16 (18.4) 26 (10.3) Intraperitoneal bleeding 1 (1.1) 10 (4.0) Gastrointestinal bleeding 4 (4.6) 11 (4.3) Pulmonary infection 9 (10.3) 9 (3.6) Pulmonary embolism 0 1 (0.4) Chylous leakage 1 (1.1) 3 (1.2) Wound infection 8 (9.2) 23 (9.1) Delayed gastric emptying 14 (16.1) 17 (6.7) Grade B 9 (10.3) 11 (4.3) Grade C 5 (5.7) 6 (2.4) Unplanned reoperation 4 (4.6) 7 (2.8) In-hospital death 2 (2.3) 4 (1.6) EN-related complications 28 (32.2) - Abdominal distention 17 (19.5) - Abdominal cramps 15 (17.2) - Vomiting 10 (11.5) - Diarrhea 9 (10.3) - EEN: Early postoperative enteral nutrition; PN: Parenteral nutrition; TPN: Total parenteral nutrition. Despite the fact that mortality following PD at many pancreatic centers has decreased to less than 4%, the incidence rate of postoperative complications remains high, ranging from 34% to 50% [12,22]. Considering the fact that preoperatively most patients undergoing PD have significant weight loss or even cachexia due to anorexia and malabsorption, and considering the postoperative deficient oral intake duration as long as 10 d [23], nutritional debilitation might greatly contribute to the high rate of complications, making perioperative appropriate nutrition therapy necessary. Nutritional therapy has evolved over decades. Parenteral nutrition, which initially prevailed and was preferred, was replaced by enteral feeding in the early 1990s. Hyperalimentation evolved into iso- or even hypoalimentation, and standard formulas were superseded by individually optimized ones, such as immunonutrition. Nutritional feeding strategies have switched from having a role as a primary provider of basic substrates into a sustainer of optimal postoperative metabolic and immune status [24]. Nevertheless, there remains no agreement in studies concerning the optimal postoperative PD feeding strategy, so the ideal nutrition support mode remains controversial. Enteral feeding after PD is proposed applied routinely by European nutritional guidelines [25], however not for American guidelines [26]. Few research studies have evaluated the efficacy and complications related to the nutrition pathway (EEN + PN vs TPN) of the feeding strategies on postoperative recovery following standard PD procedures. In the present study, nasojejunal feeding tube placement was performed as the best enteral nutrition pathway, because any unnecessary enterotomy is a potential source of cumbersome complications. Whether to implement EEN + PN or TPN depended on the surgeon s preference instead of the patient s condition. There was no difference in patients general features, preoperative comorbidities existing before surgery, or general conditions between the EEN + PN and TPN groups, thus making the potential selection bias negligible. Moreover, the current series results suggested a homogeneous histological pattern, lesion condition, surgical technique, postoperative management, and most complications. Based on our study, patients with EEN + PN following PD had a higher incidence of DGE, pulmonary infection, and probably intraperitoneal infection, which might account for longer nasogastric tube retention time, longer hospital stay and higher hospitalization expenses, compared to administration of TPN. DGE was originally described as gastroparesis following pylorus-preserving PD. DGE is not lethal, but invariably prolongs the hospital stay duration significantly and increases hospital costs. According to the ISGPS classification, grade A DGE was not taken into account in our study due to our postoperative protocol for preserving NGT for 3-7 d until NGT became uncomfortable and the patient tolerated a liquid diet intake. Our results indicated that postoperative grades B and C DGE occurrence rate was 9.1%. Whether added EEN would consequentially lower postoperative DGE following PD remains unascertained. In our study, patients dealt with EEN + PN had an increased DGE incidence than those in the TPN group (16.1% vs 6.7%, P = 0.016). Some studies have stated that EEN (solely or combined with PN) was related to a less DGE occurrence, lower cost and shorter length of hospital stay compared with TPN [4,5,7,24,25,27-31]. One theoretical explanation for lower DGE morbidity is that NJT or feeding liquids stimulates gastrointestinal peristalsis [32,33]. However, some other studies, including 3825 April 14, 2016 Volume 22 Issue 14
140 Lu JW et al. Efficacy comparison of post-pancreaticoduodenectomy nutrition modes ours, have yielded opposite results. The proper mechanisms might be that intraduodenal (or enteral) transfusion of enteral nutrition solution inhibits gastric motility through numerous enterogastric feedback pathways including increased cholecystokinin release, which suppresses gastric emptying in a dosedependent manner [34-41]. This theory was further demonstrated by a later clinical research study of EN-DGE. Several studies have elucidated the theory of the gut adaptation to nutritional ingestion and reduced negative feedback on gastric peristalsis [42-44], making early oral intake encouragement after surgery indispensable, especially for patients suffering from anorexia nervosa [45,46]. Furthermore, from our perspective, the lack of universally validated EN normalization for the indication, the optimal timing, even the components, dose and concentration of enteral nutrient solution corresponding with different postoperative recovery periods made the EEN + PN feeding strategies in our center unsuitable for many patients. Another interesting result was a more frequent occurrence of pulmonary infection in the EEN + PN group than the TPN group (10.3% vs 3.6%, respectively, P = 0.024). Seven of nine patients diagnosed with pneumonia in the EEN + PN group had a prior history of vomiting, which could be exacerbated by DGE-vomiting or NJT placementrelated presumed pulmonary aspiration [47]. Moreover, impaired respiratory mechanics and postoperative mobility attributed to immediate postoperative jejunal feeding [48] might also play a significant role in the incidence of pneumonia following PD. Many clinicians have favored changes in nutritional strategies due to the insufficiency of evidence-based data. Some scholars have expressed their dissent concerning enteral feeding, arguing that compared with TPN, immediate postoperative EN failed to lower the postoperative morbidity rate [9-11,34,48,49]. In contrast, it might be associated with an increased incidence of DGE [34] and the development of chyle leakage [13], impaired respiratory mechanics and postoperative mobility [48]. Worse still, a number of cases of small bowel necrosis have occurred during enteral feeding after PD [14,17]. Furthermore, it was acknowledged that postoperative EEN tended to trigger complications such as diarrhoea, abdominal tympany, and abdominalgia, which were named EN-related complications [6,7]. In the present study, 28 of 87 (32.2%) patients with EEN + PN developed these complications. These complications were principally due to edema induced by digestive inadaptation to the colloid osmotic pressure between the adtevak and the gut cavity, and decreased motility of the gastrointestinal system after surgery [9,10,24,50]. CONCLUSION In this retrospective controlled series, postoperative EEN + PN following PD was associated with an increased incidence of DGE and pneumonia, prolonged nasogastric tube retention and increased hospitalization expenses. Regardless of the mainstream view that postoperative EN has many desirable effects, clinical practitioners should be highly vigilant and aware of its harmful impacts, such as DGE and aspiration-related pneumonia. Discreet catheter care combined with an isocaloric nutrition supply of the TPN might neutralize the superiority of EN. Postoperative EN should only be performed scrupulously and selectively (such as for patients with a severe malnourished status). However, due to the restriction of this single center retrospective study, a sequence of RCTs should be implemented to evaluate the impact of EN on the postoperative morbidity rate and the optimal timing and dose according to a variable postoperative recovery period. ACKNOWLEDGMENTS The authors would like to thank all the members from Xi an Jiaotong University Advanced Surgical Technology and Engineering Institute, for their contribution to the discussion of the study. COMMENTS Background Complications-related morbidity remains high after pancreaticoduodenectomy (PD), and this could be partly attributed to nutritional debilitation. An ideal nutrition support strategy remains controversial, and research evaluating the efficacy of early enteral nutrition accompanied by parenteral nutrition (EEN + PN) vs total parenteral nutrition (TPN) on postoperative recovery after PD is lacking. Research frontiers Although most studies have shown that EEN seems to be superior to TPN in enhancing immunocompetence, preserving intestinal structure and function, and attenuating dissimilatory stress reactions, some studies have demonstrated that EEN failed to lower the postoperative morbidity rate, and was even associated with an increased incidence of delayed gastric emptying (DGE) and chyle leakage, and impaired respiratory mechanics and postoperative mobility. Moreover, EN-related digestive symptoms (such as diarrhoea, abdominal tympany, and abdominalgia) could have a bad impact on caloric intake and might cause interrupted EN. Innovations and breakthroughs This study investigated the postoperative outcomes between patients undergoing TPN and EEN + PN after PD. The results suggest that EEN + PN is associated with a higher incidence of DGE and pulmonary infection morbidity, which might account for the longer nasogastric tube retention time, longer postoperative hospital stay and higher hospitalization expenses. In authors opinion, EEN should only be performed cautiously and selectively. Applications The results show that EEN + PN was associated with higher DGE and pulmonary infection morbidity, which might account for longer nasogastric tube retention time, longer postoperative hospital stay and higher hospitalization expenses. The conclusion is a wake-up call for surgeons to apply EEN cautiously and selectively following PD. Peer-review Well prepared and conducted retrospective study of postoperative nutrition and 3826 April 14, 2016 Volume 22 Issue 14
141 Lu JW et al. Efficacy comparison of post-pancreaticoduodenectomy nutrition modes energy management. Although it is controversial, this study well demonstrates that EEN + PN may have more postoperative complications compared with TPN after PD. Almost certainly, this effort will initiate controversy and launch prospective studies to evaluate the conclusions. This study is a good start to remind surgeons to pay more attention to postoperative management. REFERENCES 1 Whipple AO, Parsons WB, Mullins CR. Treatment of Carcinoma of the Ampulla of Vater. Ann Surg 1935; 102: [PMID: ] 2 Gouma DJ, van Geenen RC, van Gulik TM, de Haan RJ, de Wit LT, Busch OR, Obertop H. Rates of complications and death after pancreaticoduodenectomy: risk factors and the impact of hospital volume. Ann Surg 2000; 232: [PMID: DOI: / ] 3 Dudrick SJ, Wilmore DW, Vars HM, Rhoads JE. Long-term total parenteral nutrition with growth, development, and positive nitrogen balance. Surgery 1968; 64: [PMID: ] 4 Rayar M, Sulpice L, Meunier B, Boudjema K. Enteral nutrition reduces delayed gastric emptying after standard pancreaticoduodenectomy with child reconstruction. J Gastrointest Surg 2012; 16: [PMID: DOI: /s x] 5 Park JS, Chung HK, Hwang HK, Kim JK, Yoon DS. Postoperative nutritional effects of early enteral feeding compared with total parental nutrition in pancreaticoduodectomy patients: a prosepective, randomized study. J Korean Med Sci 2012; 27: [PMID: DOI: /jkms ] 6 Yang H, Feng Y, Sun X, Teitelbaum DH. Enteral versus parenteral nutrition: effect on intestinal barrier function. Ann N Y Acad Sci 2009; 1165: [PMID: DOI: /j x] 7 Baradi H, Walsh RM, Henderson JM, Vogt D, Popovich M. Postoperative jejunal feeding and outcome of pancreaticoduodenectomy. J Gastrointest Surg 2004; 8: [PMID: DOI: / j.gassur ] 8 Feng Y, Ralls MW, Xiao W, Miyasaka E, Herman RS, Teitelbaum DH. Loss of enteral nutrition in a mouse model results in intestinal epithelial barrier dysfunction. Ann N Y Acad Sci 2012; 1258: [PMID: DOI: /j x] 9 Padussis JC, Zani S, Blazer DG, Tyler DS, Pappas TN, Scarborough JE. Feeding jejunostomy during Whipple is associated with increased morbidity. J Surg Res 2014; 187: [PMID: DOI: /j.jss ] 10 Gerritsen A, Besselink MG, Gouma DJ, Steenhagen E, Borel Rinkes IH, Molenaar IQ. Systematic review of five feeding routes after pancreatoduodenectomy. Br J Surg 2013; 100: ; discussion 599 [PMID: DOI: /bjs.9049] 11 Gerritsen A, Besselink MG, Cieslak KP, Vriens MR, Steenhagen E, van Hillegersberg R, Borel Rinkes IH, Molenaar IQ. Efficacy and complications of nasojejunal, jejunostomy and parenteral feeding after pancreaticoduodenectomy. J Gastrointest Surg 2012; 16: [PMID: DOI: /s ] 12 Zhang XF, Yin GZ, Liu QG, Liu XM, Wang B, Yu L, Liu SN, Cui HY, Lv Y. Does Braun enteroenterostomy reduce delayed gastric emptying after pancreaticoduodenectomy? Medicine (Baltimore) 2014; 93: e48 [PMID: DOI: / MD ] 13 Malik HZ, Crozier J, Murray L, Carter R. Chyle leakage and early enteral feeding following pancreatico-duodenectomy: management options. Dig Surg 2007; 24: [PMID: DOI: / ] 14 Thaler K, Garreau J, Hansen PD. Non-occlusive small bowel necrosis during enteral feeding after pancreaticoduodenectomy. Dig Surg 2005; 22: [PMID: DOI: / ] 15 Peter JV, Moran JL, Phillips-Hughes J. A metaanalysis of treatment outcomes of early enteral versus early parenteral nutrition in hospitalized patients. Crit Care Med 2005; 33: ; discussion [PMID: DOI: /01. Ccm C0] 16 Takeuchi H, Miyata H, Gotoh M, Kitagawa Y, Baba H, Kimura W, Tomita N, Nakagoe T, Shimada M, Sugihara K, Mori M. A risk model for esophagectomy using data of 5354 patients included in a Japanese nationwide web-based database. Ann Surg 2014; 260: [PMID: DOI: / SLA ] 17 Jorba R, Fabregat J, Borobia FG, Torras J, Poves I, Jaurrieta E. Small bowel necrosis in association with early postoperative enteral feeding after pancreatic resection. Surgery 2000; 128: [PMID: DOI: /msy ] 18 Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr MG, Traverso LW, Yeo CJ, Büchler MW. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007; 142: [PMID: DOI: /j.surg ] 19 Bassi C, Falconi M, Molinari E, Salvia R, Butturini G, Sartori N, Mantovani W, Pederzoli P. Reconstruction by pancreaticojejunostomy versus pancreaticogastrostomy following pancreatectomy: results of a comparative study. Ann Surg 2005; 242: , discussion [PMID: DOI: /01. sla d] 20 Tan WJ, Kow AW, Liau KH. Moving towards the New International Study Group for Pancreatic Surgery (ISGPS) definitions in pancreaticoduodenectomy: a comparison between the old and new. HPB (Oxford) 2011; 13: [PMID: DOI: /j x] 21 Koch M, Garden OJ, Padbury R, Rahbari NN, Adam R, Capussotti L, Fan ST, Yokoyama Y, Crawford M, Makuuchi M, Christophi C, Banting S, Brooke-Smith M, Usatoff V, Nagino M, Maddern G, Hugh TJ, Vauthey JN, Greig P, Rees M, Nimura Y, Figueras J, DeMatteo RP, Büchler MW, Weitz J. Bile leakage after hepatobiliary and pancreatic surgery: a definition and grading of severity by the International Study Group of Liver Surgery. Surgery 2011; 149: [PMID: DOI: / j.surg ] 22 Kimura W, Miyata H, Gotoh M, Hirai I, Kenjo A, Kitagawa Y, Shimada M, Baba H, Tomita N, Nakagoe T, Sugihara K, Mori M. A pancreaticoduodenectomy risk model derived from 8575 cases from a national single-race population (Japanese) using a webbased data entry system: the 30-day and in-hospital mortality rates for pancreaticoduodenectomy. Ann Surg 2014; 259: [PMID: DOI: /SLA ] 23 Howard L, Ashley C. Nutrition in the perioperative patient. Annu Rev Nutr 2003; 23: [PMID: ] 24 Klek S, Sierzega M, Szybinski P, Szczepanek K, Scislo L, Walewska E, Kulig J. Perioperative nutrition in malnourished surgical cancer patients - a prospective, randomized, controlled clinical trial. Clin Nutr 2011; 30: [PMID: DOI: /j.clnu ] 25 Lassen K, Coolsen MM, Slim K, Carli F, de Aguilar-Nascimento JE, Schäfer M, Parks RW, Fearon KC, Lobo DN, Demartines N, Braga M, Ljungqvist O, Dejong CH. Guidelines for perioperative care for pancreaticoduodenectomy: Enhanced Recovery After Surgery (ERAS ) Society recommendations. Clin Nutr 2012; 31: [PMID: DOI: /j.clnu ] 26 Druyan ME, Compher C, Boullata JI, Braunschweig CL, George DE, Simpser E, Worthington PA. Clinical Guidelines For the Use of Parenteral and Enteral Nutrition in Adult and Pediatric Patients: applying the GRADE system to development of A.S.P.E.N. clinical guidelines. JPEN J Parenter Enteral Nutr 2012; 36: [PMID: DOI: / ] 27 Zhu XH, Wu YF, Qiu YD, Jiang CP, Ding YT. Effect of early enteral combined with parenteral nutrition in patients undergoing pancreaticoduodenectomy. World J Gastroenterol 2013; 19: [PMID: DOI: /wjg.v19.i ] 28 Liu C, Du Z, Lou C, Wu C, Yuan Q, Wang J, Shu G, Wang Y. Enteral nutrition is superior to total parenteral nutrition for pancreatic 3827 April 14, 2016 Volume 22 Issue 14
142 Lu JW et al. Efficacy comparison of post-pancreaticoduodenectomy nutrition modes cancer patients who underwent pancreaticoduodenectomy. Asia Pac J Clin Nutr 2011; 20: [PMID: ] 29 Yermilov I, Jain S, Sekeris E, Bentrem DJ, Hines OJ, Reber HA, Ko CY, Tomlinson JS. Utilization of parenteral nutrition following pancreaticoduodenectomy: is routine jejunostomy tube placement warranted? Dig Dis Sci 2009; 54: [PMID: DOI: /s ] 30 Okabayashi T, Kobayashi M, Nishimori I, Sugimoto T, Akimori T, Namikawa T, Okamoto K, Onishi S, Araki K. Benefits of early postoperative jejunal feeding in patients undergoing duodenohemipancreatectomy. World J Gastroenterol 2006; 12: [PMID: DOI: /wjg.v12.i1.89] 31 Gianotti L, Braga M, Gentilini O, Balzano G, Zerbi A, Di Carlo V. Artificial nutrition after pancreaticoduodenectomy. Pancreas 2000; 21: [PMID: DOI: / ] 32 Dong K, Yu XJ, Li B, Wen EG, Xiong W, Guan QL. Advances in mechanisms of postsurgical gastroparesis syndrome and its diagnosis and treatment. Chin J Dig Dis 2006; 7: [PMID: DOI: /j x] 33 Hallay J, Micskei C, Fülesdi B, Kovács G, Szentkereszty Z, Takács I, Sipka S, Bodolay E, Sápy P. Use of three lumen catheter facilitates bowel movement after pancreato-duodenectomy. Hepatogastroenterology 2008; 55: [PMID: ] 34 Martignoni ME, Friess H, Sell F, Ricken L, Shrikhande S, Kulli C, Büchler MW. Enteral nutrition prolongs delayed gastric emptying in patients after Whipple resection. Am J Surg 2000; 180: [PMID: DOI: /S (00) ] 35 van Berge Henegouwen MI, Akkermans LM, van Gulik TM, Masclee AA, Moojen TM, Obertop H, Gouma DJ. Prospective, randomized trial on the effect of cyclic versus continuous enteral nutrition on postoperative gastric function after pylorus-preserving pancreatoduodenectomy. Ann Surg 1997; 226: ; discussion [PMID: DOI: / ] 36 van Berge Henegouwen MI, van Gulik TM, Moojen TM, Boeckxstaens GE, Gouma DJ. Gastrointestinal motility after pancreatoduodenectomy. Scand J Gastroenterol Suppl 1998; 225: [PMID: DOI: / ] 37 Heddle R, Fone D, Dent J, Horowitz M. Stimulation of pyloric motility by intraduodenal dextrose in normal subjects. Gut 1988; 29: [PMID: DOI: /gut ] 38 Heddle R, Collins PJ, Dent J, Horowitz M, Read NW, Chatterton B, Houghton LA. Motor mechanisms associated with slowing of the gastric emptying of a solid meal by an intraduodenal lipid infusion. J Gastroenterol Hepatol 1989; 4: [PMID: DOI: /j tb01741.x] 39 Heddle R, Dent J, Read NW, Houghton LA, Toouli J, Horowitz M, Maddern GJ, Downton J. Antropyloroduodenal motor responses to intraduodenal lipid infusion in healthy volunteers. Am J Physiol 1988; 254: G671-G679 [PMID: ] 40 Debas HT, Farooq O, Grossman MI. Inhibition of gastric emptying is a physiological action of cholecystokinin. Gastroenterology 1975; 68: [PMID: ] 41 Kleibeuker JH, Beekhuis H, Jansen JB, Piers DA, Lamers CB. Cholecystokinin is a physiological hormonal mediator of fat-induced inhibition of gastric emptying in man. Eur J Clin Invest 1988; 18: [PMID: DOI: /j tb x] 42 Edelbroek M, Horowitz M, Fraser R, Wishart J, Morris H, Dent J, Akkermans L. Adaptive changes in the pyloric motor response to intraduodenal dextrose in normal subjects. Gastroenterology 1992; 103: [PMID: ] 43 Cunningham KM, Horowitz M, Read NW. The effect of shortterm dietary supplementation with glucose on gastric emptying in humans. Br J Nutr 1991; 65: [PMID: DOI: /BJN ] 44 Cunningham KM, Daly J, Horowitz M, Read NW. Gastrointestinal adaptation to diets of differing fat composition in human volunteers. Gut 1991; 32: [PMID: DOI: / Gut ] 45 Rigaud D, Bedig G, Merrouche M, Vulpillat M, Bonfils S, Apfelbaum M. Delayed gastric emptying in anorexia nervosa is improved by completion of a renutrition program. Dig Dis Sci 1988; 33: [PMID: DOI: /BF ] 46 Robinson PH, Clarke M, Barrett J. Determinants of delayed gastric emptying in anorexia nervosa and bulimia nervosa. Gut 1988; 29: [PMID: DOI: /Gut ] 47 Bullock TK, Waltrip TJ, Price SA, Galandiuk S. A retrospective study of nosocomial pneumonia in postoperative patients shows a higher mortality rate in patients receiving nasogastric tube feeding. Am Surg 2004; 70: [PMID: ] 48 Watters JM, Kirkpatrick SM, Norris SB, Shamji FM, Wells GA. Immediate postoperative enteral feeding results in impaired respiratory mechanics and decreased mobility. Ann Surg 1997; 226: ; discussion [PMID: DOI: / ] 49 Heslin MJ, Latkany L, Leung D, Brooks AD, Hochwald SN, Pisters PW, Shike M, Brennan MF. A prospective, randomized trial of early enteral feeding after resection of upper gastrointestinal malignancy. Ann Surg 1997; 226: ; discussion [PMID: DOI: / ] 50 Woodcock NP, Zeigler D, Palmer MD, Buckley P, Mitchell CJ, MacFie J. Enteral versus parenteral nutrition: a pragmatic study. Nutrition 2001; 17: 1-12 [PMID: DOI: / S (00) ] P- Reviewer: Bradley EL, Peng B S- Editor: Gong ZM L- Editor: Wang TQ E- Editor: Ma S 3828 April 14, 2016 Volume 22 Issue 14
143 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Retrospective Study ORIGINAL ARTICLE Oncogenic Wnt3a expression as an estimable prognostic marker for hepatocellular carcinoma Liu-Hong Pan, Min Yao, Yin Cai, Juan-Juan Gu, Xu-Li Yang, Li Wang, Deng-Fu Yao Liu-Hong Pan, Deng-Fu Yao, Research Center of Clinical Medicine, Affiliated Hospital of Nantong University, Nantong , Jiangsu Province, China Min Yao, Departments of Immunology, Medical College of Nantong University, Nantong , Jiangsu Province, China Li Wang, Medical Informatics, Medical College of Nantong University, Nantong , Jiangsu Province, China Yin Cai, Juan-Juan Gu, Xu-Li Yang, Department of Oncology, Affiliated Hospital of Nantong University, Nantong , Jiangsu Province, China Author contributions: Pan LH, Yao M contributed equally to this work; Pan LH, Yao M and Wang L designed and performed the research; Cai Y, Gu JJ and Yang XL contributed new reagents/ analytic tools; Pan LH and Yao M analyzed the data; Pan LH, Yao M and Yao DF wrote the paper; Yao DF is the guarantor; all authors have read and approved the final version to be published. Supported by the International S&T Cooperation Program, No. 2013DFA32150 of China. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Deng-Fu Yao, MD, PhD, Professor, Research Center of Clinical Medicine, Affiliated Hospital of Nantong University, No. 20 West Temple Road, Nantong , Jiangsu Province, China. yaodf@ahnmc.com Telephone: Fax: Received: November 1, 2015 Peer-review started: November 6, 2015 First decision: December 11, 2015 Revised: January 6, 2016 Accepted: January 17, 2016 Article in press: January 18, 2016 Published online: April 14, 2016 Abstract AIM: To investigate member 3a of Wingless-type MMTV integration site family (Wnt3a) expression in cancerous and surrounding tissues and the relationship between clinicopathologic features of hepatocellular carcinoma (HCC) and Wnt3a expression. METHODS: Wnt3a expression and cellular distribution and clinicopathologic characteristics in cancerous tissue and matched surrounding tissues were analyzed in 80 HCC patients from January 2006 to August 2008 by tissue microarrays and immunohistochemistry. The overall and disease-free survival rates were estimated using the Kaplan-Meier method and compared with the log-rank test. The prognostic analysis was carried out with univariate and multivariate Cox regressions models. RESULTS: The incidence of oncogenic Wnt3a expression in the cancerous group was up to 96.25% (77 of 80), which was significantly higher (χ 2 = , P < 0.001) than that in the surrounding group (46.25%, 37 of 80). Brown Wnt3a staining gradually increased with clinical staging that showed very strong staining in advanced HCC. The clinicopathologic features of high Wnt3a expression in HCC were related to poorlydifferentiated grade (χ 2 = , P < 0.001), liver cirrhosis (χ 2 = 8.467, P < 0.004), hepatitis B virus (HBV) infection (χ 2 = , P < 0.001), higher tumor-nodemetastasis stage (χ 2 = , P < 0.001), and 5-year survival rate (χ 2 = , P < 0.001). CONCLUSION: Oncogenic Wnt3a expression asso April 14, 2016 Volume 22 Issue 14
144 Pan LH et al. Wnt3a in HCC ciated with HBV infection and cirrhotic liver might be an independent prognostic factor for HCC. Key words: Hepatocellular carcinoma; Prognosis; Wnt3a; Wnt/β-catenin signal; Tissue microarrays; Immunohistochemistry The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Protein expression of member 3a of Winglesstype MMTV integration site family (Wnt3a) was shown to be increased progressively in hepatocarcinogenesis. Oncogenic Wnt3a expression associated with HBV infection and cirrhotic liver might be an independent prognostic factor for hepatocellular carcinoma (HCC). Survival analysis showed that HCC patients with high Wnt3a expression had a significantly shorter survival time compared with those low or no Wnt3a expression. Pan LH, Yao M, Cai Y, Gu JJ, Yang XL, Wang L, Yao DF. Oncogenic Wnt3a expression as an estimable prognostic marker for hepatocellular carcinoma. World J Gastroenterol 2016; 22(14): Available from: URL: com/ /full/v22/i14/3829.htm DOI: org/ /wjg.v22.i INTRODUCTION Hepatocellular carcinoma (HCC) is one of the most common and rapidly fatal malignancies worldwide [1,2]. It develops mostly in cirrhotic livers, and risk factors include chronic persistent infection by the hepatitis B viruses (HBV) and C viruses (HCV) as well as nonviral liver diseases [3,4]. HCC is a highly chemo-resistant cancer with no effective systemic or well-established adjuvant therapies, and prognosis remains poor because of its high recurrence [5,6]. Hepatic resection or transplantation is the only potential curative treatment for HCC patients [7,8]. Unfortunately, the molecular mechanisms of hepatocarcinogenesis remain poorly understood. Recently, abnormal expression of some key molecules in the Wingless (Wnt)/β-Catenin pathway was associated with the development and progression of HCC [9,10]. The Wnt proteins are secreted glycoproteins that regulate multiple cellular events, such as cell proliferation, differentiation, and apoptosis through β-catenin- dependent canonical and β-cateninindependent non-canonical pathways, and play an important role in HCC prognosis [11,12]. The member 3a of Wnt-type MMTV integration site family (Wnt3a) is a canonical Wnt ligand [13,14]. Its gene is located on human 17 chromosome (17q21) and has been regarded as an activator of the canonical Wnt signaling pathway, inducing β-catenin accumulation and activating the canonical Wnt signaling pathway [13]. Studies on human Wnt3a have focused primarily on its key role in human malignancy, and its high expression in many kinds of tumors was correlated with a worse outcome [15-17]. However, limited data are available on the relationship between Wnt3a and HCC, and its prognostic value remains to be explored. The objective of the current study, therefore, was to investigate alterations in the expression of oncogenic Wnt3a in cancerous tissues and to explore its clinical utility as a novel molecular marker for HCC prognosis. MATERIALS AND METHODS Liver specimen Human liver cancer and surrounding tissues in this study were obtained from 80 HCC patients who underwent operations between January 2006 and August 2008 at the Affiliated Hospital of Nantong University, Jiangsu Province, China. The tissues were immediately frozen in liquid nitrogen and kept at -80 until required. The patient cohort inclusion and exclusion criteria included: (1) accurate pathologic diagnosis of primary HCC; (2) complete clinicopathologic and follow-up data; and (3) previously untreated, with surgery as the first treatment. Thus, analysis of the data would reflect the actual impact of tumor biology on the clinical outcome. This study was approved by the Ethics Committee permission (No. TDFY ) of the Affiliated Hospital of Nantong University, and all patients signed informed consent. The related important clinical information of each patient was collected from their medical records. Clinical data of HCC patients The patient characteristics are listed in Table 1. The patient population consisted of 62 males and 18 females, with a median age of 51 years (range: 35-74). The sizes of tumors were 44 cases with > 5 cm and 36 with < 5 cm. α-fetoprotein (AFP) levels were 28 cases with 400 ng/ml and 52 with < 400 ng/ml. The tumor number was 64 cases with single and 16 with multiple. Tumor differentiation was graded using the Edmondson grading system [18] with 5 well-, 41 middle-, and 34 poor- differentiation. Tumor staging was 36 cases (45%, 36 of 80) at Ⅰ and Ⅱ and 44 cases (55%, 44 of 80) at Ⅲ and Ⅳ based on the 6 th edition of the tumor-node-metastasis (TNM) classification of the International Union against Cancer (IUAC). The incidence of hepatitis B surface antigen (HBsAg) was 81.25% (65 of 80) in these HCC tissues, and 63.75% (51 of 80) had a history of liver cirrhosis. All patients had regular follow-up. The follow-up period was defined as the duration from the date of the operation to the date of either death or the last followup. The last follow-up was October Overall survival (OS) was evaluated by the duration between the dates of surgery and death. During the follow-up period, a total of 48 patients died. Pathologic examination and HCC diagnosis Histopathologic examination of the livers with 3830 April 14, 2016 Volume 22 Issue 14
145 Pan LH et al. Wnt3a in HCC Table 1 Clinical characteristics of hepatocellular carcinoma patients Parameter Age (yr) median (range) 51 (35-74) Gender Male 62 Female 18 Differentiation Poor 34 Moderate 41 Well 5 Tumor number Single 64 Multiple 16 Liver cirrhosis Absent 29 Present 51 HBV infection Absent 15 Present 65 Periportal embolus Absent 9 Present 71 AFP (ng/ml) < TNM staging Ⅰ-Ⅱ 36 Ⅲ-Ⅳ 44 Five-year survival Yes 32 No 48 HBV: Hepatitis B virus; AFP: α-fetoprotein; TNM: Tumor-node-metastasis. hematoxylin and eosin (HE) staining showed that all cancerous tissues were accurate pathologic diagnosis of HCC according to the World Health Organization criteria. HCC diagnosis was confirmed according to the criteria set by the Chinese National Collaborative Cancer Research Group [18]. Tissue microarrays All HCC tissues were stained by HE staining and reviewed by two histopathologists. Representative areas free from necrotic and hemorrhagic materials were marked in paraffin blocks. Tissue cores (2.0 mm) were taken from each representative tumor tissue and peritumoral tissue to construct the tissue microarray (TMA) slides. Immunohistochemistry The TMA slides used for immunohistochemistry (IHC) were deparaffinized, and peroxidase was quenched with methanol and 3% H2O2 for 15 min. For antigen retrieval, the sections were boiled under pressure in citrate buffer (ph 6.0) for 3 min. After that, the tissues were incubated for 120 min with primary mouse anti- Wnt3a (ab81614; Abcam, United Kingdom) at 1:50 dilution. Following washing with phosphate buffered saline (PBS), the sections were incubated with n horseradish peroxidase conjugated goat anti-mouse IgG (A21010; Abcam, Cambridge, United Kingdom) for 15 min at 1:5000 dilution and washed again with PBS. The sections were incubated in diaminobenzidine solution, counterstained with hematoxylin, dehydrated in ethanol, cleared in xylene, and cover-slipped. For the negative control reactions, PBS was used instead of the primary antibody. Evaluation of the IHC findings The results of IHC staining were assessed by two independent pathologists without knowledge of the clinicopathologic features. The percentages for Wnt3a-positive cells were scored as follows: 0 (0%), 1 (1%-33%), 2 (34%-66%), and 3 (67%-100%). Staining intensity was stratified into four categories: 0 (negative), 1 (weakly), 2 (moderate), and 3 (strongly). The sum of the percentage and intensity score was defined as the IHC staining score. According to above criterion, the HCC tissues with Wnt3a expression were divided into two groups: low with 0-2 scores and high 3-6 scores. The higher score for positive percentages and staining intensity was taken as the final score when there was a difference between duplicate tissue scores. Statistical analysis Statistical analysis was carried out by using SPSS software (version 20.0, Armonk, NY, United States). The difference between HCC and para-cancerous groups was analyzed by χ 2 test. Quantitative variables were analyzed by Mann-Whitney U test (Z). The relationship between Wnt3a expression and clinicopathological factors was analyzed by χ 2 test. Survival curves were calculated using the Kaplan- Meier method and compared by the log-rank test. Factors shown to be of prognostic significance in the univariate models were evaluated in a multivariable Cox regression model. For all tests, the significance level for statistical analysis was set at P < RESULTS Hepatic Wnt3a expression in cancerous and surrounding tissues The over-expression of hepatic Wnt3a and its cellular distribution in cancerous or surrounding tissues analyzed by immunohistochemistry with human anti- Wnt3a antibodies are shown in Figure 1. Positive Wnt3a staining, identified as brown particles, was distributed in the cytosol and the membrane of hepatocytes or only a few cell nuclei. The incidence of hepatic Wnt3a expression in cancerous tissues (96.25%, 77 of 80) was significantly higher (χ 2 = , P < 0.001) than that in surrounding tissues (46.25%, 37 of 80). Liver Wnt3a staining and its expression frequency in cancerous or surrounding tissues are shown in Table 2. The liver Wnt3a staining scores were significantly 3831 April 14, 2016 Volume 22 Issue 14

 tissues; C and D: Light staining of Wnt3a in surrounding tissue.")
146 Pan LH et al. Wnt3a in HCC A B HCC C D Para-HCC Figure 1 Analysis of hepatic Wnt3a expression and its cellular distribution by immunohistochemistry. The expression of hepatic Wnt3a was analyzed on tissue microarrays by immunohistochemistry with the primary mouse anti-human Wnt3a antibody. The positive Wnt3a expression with brown staining particles was distributed in the cytosol and membrane of hepatocytes and only a few cell nuclei. A and B: Strong straining of Wnt3a in hepatocellular carcinoma (HCC) tissues; C and D: Light staining of Wnt3a in surrounding tissue. A and C: Original magnification 400; B and D: Original magnification 400. Table 2 Incidence of liver Wnt3a expression and its scores with staining strength in cancerous and surrounding tissues Group n Wnt3a χ 2 P value Wnt3a strength Z value P value Neg. Pos HCC < < Para-can Compared with the para-cancerous group. HCC: Hepatocellular carcinoma; Para-can: Para-cancerous tissues; Neg.: Negative Wnt3a expression; Pos.: Positive Wnt3a expression. different (Z = 8.144, P < 0.001) between cancerous tissues and surrounding tissues, with strong expression (3-6 scores) in 71.25% (57 of 80) of cancerous tissues and low or no expression (0-2 scores) in 86.25% (69 of 80) of surrounding tissues. Relationship between Wnt3a expression and HCC staging The relationship between hepatic Wnt3a expression and clinical staging of HCC is shown in Figure 2. According to the IUAC clinical staging criteria of HCC patients, there were nine cases at staging Ⅰ (11.25%, 9 of 80), 27 at Ⅱ (33.75%, 27 of 80), 38 at Ⅲ (47.5%, 38 of 80), and six at Ⅳ (7.5%, 6 of 80) among 80 cancerous tissues. The incidences of high or low Wnt3a expression in HCC tissues were 22.2% (two of nine) or 77.8% (seven of nine) at Ⅰ staging, 51.9% (14 of 27) or 48.1% (13 of 27) at Ⅱ staging, 94.7% (36 of 38) or 5.3% (two of 38) at Ⅲ staging, and 83.3% (five of six) or 16.7% (one of six) at Ⅳ staging, respectively. Brown Wnt3a expression was gradually increased in different clinical stages, with very strong staining at the advanced stage. Clinicopathologic characteristic of Wnt3a expression The correlation between Wnt3a levels and the clinicopathological parameters of 80 HCC patients is shown in Table 3. High Wnt3a expression was associated with poorly-differentiated grade (P < 0.001), liver cirrhosis (P = 0.004), HBV infection (P < 0.001), and higher TNM stage (P < 0.001). By contrast, there were no significant associations between hepatic Wnt3a expression and other clinicopathological features, such as HCC patients gender or age, tumor number, circulating AFP level, and periportal cancer embolus April 14, 2016 Volume 22 Issue 14

147 Pan LH et al. Wnt3a in HCC Clinical stage Para-HCC Ⅰ Ⅱ Ⅲ Ⅳ A1 A2 A3 A4 A5 200 B1 B2 B3 B4 B5 400 Figure 2 Expression of hepatic Wnt3a at different hepatocellular carcinoma stages. A1 and B1: Low or no Wnt3a expression in the para-cancerous tissues. A2-A5 and B2-B5: The brown staining of Wnt3a gradually increases in cancerous tissues from stage Ⅰ to Ⅳ. A1-A5: Original magnification 200; B1-B5: Original magnification 400. Table 3 Clinicopathological characteristics of high Wnt3a expression in 80 hepatocellular carcinoma patients Groups Patients, n % of total Wnt3a high expression, n % of total χ 2 P value Differentiation < Poor Moderate Well Tumor number Single Multiple Liver cirrhosis Absent Present HBV infection < Absent Present Periportal embolus Absent Present AFP (ng/ml) < TNM staging < Ⅰ-Ⅱ Ⅲ-Ⅳ Five-year survival < Yes No HBV: Hepatitis B virus; AFP: α-fetoprotein; TNM: Tumor-node-metastasis. High Wnt3a expression with shorter survival in HCC As expected, the overexpression of hepatic Wnt3a showed a significant relationship with 5-year survival of the 80 HCC patients (P < 0.001). Meanwhile, certain HCC clinical prognostic factors, such as liver cirrhosis (P = 0.035) and HBV infection (P = 0.029), also showed a statistically significant correlation with 5-year survival rate based on Cox regression univariate analysis (Table 4). All these factors were enrolled in a multivariable analysis. High Wnt3a expression (P < 0.001), liver 3833 April 14, 2016 Volume 22 Issue 14
148 Pan LH et al. Wnt3a in HCC Table 4 Univariate and multivariable analysis of prognostic factors in hepatocellular carcinoma for 5-year survival Variable Univariate analysis Multivariable analysis Age (yr) HR P > z 95%CI HR P > z 95%CI 60 vs > Gender Male vs female Differentiation Low vs high Tumor number Single vs multiple Liver cirrhosis Absent vs present HBV infection Absent vs present Periportal embolus Absent vs present AFP (ng/ml) < 400 vs TNM staging Ⅰ-Ⅱ vs Ⅲ-Ⅳ Wnt3a expression Low vs high < < HBV: Hepatitis B virus; AFP: α-fetoprotein; TNM: Tumor-node-metastasis Kaplan-Meier survival estimates, by WNT3a High expression of WNT3a Low and no expression of WNT3a Analysis time (mo) Figure 3 Overall survival curves of 80 hepatocellular carcinoma patients. The Wnt3a expression curves were calculated by the Kaplan-Meier method. Survival curves of 80 hepatocellular carcinoma patients were made according to cancerous tissues expressing a low or high level of Wnt3a (log-rank test, P < 0.001). The green line is the high Wnt3a group; and the blue line is the low or without Wnt3a group. cirrhosis (P = 0.033), and HBV infection (P = 0.010) were all identified as independent predictive factors for poor HCC outcome. The Kaplan-Meier survival curves (Figure 3) demonstrated that HCC patients with high Wnt3a expression had a significantly shorter survival time compared to those with low or no Wnt3a expression. DISCUSSION HCC is one of the most frequently occurring tumors worldwide [19]. Accumulating data have indicated that the Wnt/β-catenin pathway is associated with tumor progression by interacting with microenvironment and oncogenesis [20,21], and high expression of Wnt3a in different kinds of tumors was related to worse outcome [12]. Wnt3a is an important regulator of HCC cell growth in vitro, and induction of Wnt3a activates the canonical Wnt pathway after binding with sulfatase 2 and glypican-3 and increases cell proliferation in nude mouse xenografts in vivo [22,23]. However, limited data was available until now on the relationship between Wnt3a expression and HCC prognosis. In this present study, therefore, the alterations of oncogenic Wnt3a expression in cancerous tissues were investigated, and it was confirmed that Wnt3a may be a useful biomarker for HCC prognosis Recent advances have shown that, apart from autocrine stimulation by growth factors and the dysregulation of different growth regulatory pathways, the Wnt/β-catenin pathway is frequently involved in hepatocarcinogenesis [24,25]. Growing evidence has highlighted the key molecules of the Wnt/β-catenin pathway in the control of HCC suppressors, growth, invasiveness, and curability [26-28]. Wnt3a expression in a large array of HCC tissues demonstrated that HCC tissues exhibited unique immunostaining patterns and that the staining was positively correlated with the clinical stage. The incidence of oncogenic Wnt3a expression in the cancerous group was significantly higher than that in the surrounding tissue group. Brown 3834 April 14, 2016 Volume 22 Issue 14
149 Pan LH et al. Wnt3a in HCC Wnt3a staining was gradually increased with clinical staging and showed very strong staining in advanced HCC, indicating that hepatic Wnt3a expression might be related to HCC progression. The management of advanced HCC is entering a new era of molecular targeting therapy, which is of particular significance for HCC because of the lack of effective systemic therapies for HCC. Although the clinical significance of Wnt3a expression in tissue has been demonstrated in different human malignancies [13,14,16], little data until now was available on the relationship between Wnt3a expression and HCC. In this study, the clinicopathologic features of high Wnt3a expression in HCC were reported and associated with the poorly-differentiated grade, liver cirrhosis, HBV infection, higher TNM stage, and a relatively shorter survival time. Furthermore, univariate and multivariate analyses suggested that high Wnt3a expression in HCC patients might be an independent prognostic indicator, like the factors liver cirrhosis and HBV infection [29,30]. There are some possible limitations associated with this study. We evaluated a relatively small number of patients, and the study design was retrospective. In addition, this study is limited by the inclusion of only patients with resectable tumors. It is possible that these findings pertain only to those patients who have undergone resection. A larger prospective study examining Wnt3a expression is necessary to validate further the usefulness of this system. Inhibiting Wnt3a overexpression may prevent invasive progression and metastatic relapse, which would improve the prognosis and quality of life for HCC patients after hepatic resection. Targeting the Wnt3a pathway may be a therapeutic strategy for HCC that could be used in combination with conventional chemotherapy or radiotherapy. Wnt3a may play an important role in promoting HCC progression and metastasis. In conclusion, to the best of our knowledge, this is the first report to investigate cancerous Wnt3a expression and to indicate that it may be a novel prognostic marker for HCC. Multiple key factors along the Wnt/β-catenin signaling cascade likely represent potential diagnosis, prognosis, or therapeutic targets as well [31,32]. Here, the findings are promising, and the initial evidence confirmed that Wnt3a is one of the key molecules in the Wnt/β-catenin pathway. Future studies should clarify the molecular mechanisms of the upregulation of oncogenic Wnt3a expression and its important role in hepatocarcinogenesis [33,34]. ACKNOWLEDGMENTS The authors thank Dr. T. FitzGibbon for comments on earlier drafts of the manuscript. COMMENTS Background Hepatocellular carcinoma (HCC) is one of the most common and rapidly fatal malignancies worldwide. The oncogene member 3a of Wingless-type MMTV integration site family (Wnt3a) is located on chromosome 17q21 and has been regarded as an activator of the canonical Wnt signaling pathway. Some studies on human Wnt3a have focused primarily on its key role in human malignancy and its high expression in many kinds of tumors. However, little data is available regarding HCC, and the prognostic value of Wnt3a remains to be explored. Research frontiers Recently, Pan et al found that higher levels of circulating Wnt3a expression (over 800 ng/l) were present in 92.5% HCC patients, and this elevation was significantly related to α-fetoprotein (AFP) level, liver cirrhosis, hepatitis B virus (HBV) infection, poor differentiation, tumor node metastasis, and extra-hepatic metastasis. Wnt3a level in HCC was obviously higher than that in any other group of benign liver diseases, except for 5.67% cirrhosis cases, suggesting that Wnt3a expression was associated with tumor progression and that it may be a novel specific biomarker for diagnosis and differentiation of HCC. Innovations and breakthroughs Some studies on human Wnt3a have focused primarily on its key role in human malignancy, and its high expression in many kinds of tumors was correlated with a worse outcome. The present data showed that the clinicopathologic features of high Wnt3a expression in HCC were related to poorly-differentiated grade, liver cirrhosis, HBV infection, higher tumor-node-metastasis (TNM) stage, and 5-year survival rate, indicating that oncogenic Wnt3a expression associated with HBV infection and cirrhotic liver might be an independent prognostic factor for HCC. Applications The authors report for the first time that Wnt3a expression is a novel prognostic marker for HCC. Multiple key factors along the Wnt/β-catenin signaling cascade may also represent potential diagnosis, prognosis, or therapeutic targets. The present findings are promising, and the initial evidence confirmed that Wnt3a is a key molecule in the Wnt/β-catenin pathway and further studies should clarify the molecular mechanisms of the upregulation of oncogenic Wnt3a expression and its important role in hepatocarcinogenesis. Terminology Key molecules in the Wnt/β-catenin signaling pathway have been recognized to play an important role in HCC. These molecules regulate multiple cellular events through the β-catenin-dependent canonical pathway, such as Wnt1, Wnt2, Wnt3, Wnt3a, Wnt8a, Wnt8b, Wnt10a, and Wnt10b, characterized by the stabilization and subsequent nuclear transport of β-catenin, which result in the activation of transcriptional responses; and the β-catenin-independent noncanonical pathway, including Wnt4, Wnt5a, Wnt5b, Wnt6, ont7a, Wnt7b, and Wnt11, with more diverse and several different signaling modes that regulate cell behavior. Peer-review This research study is well presented, and the reviewers enjoyed reading the article, despite its limitations as a retrospective study. The main discovery by the authors will likely generate further interest in the use of Wnt3a as a molecular biomarker in HCC. REFERENCES 1 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011; 61: [PMID: DOI: /caac.20107] 2 Ringelhan M, O Connor T, Protzer U, Heikenwalder M. The direct and indirect roles of HBV in liver cancer: prospective markers for HCC screening and potential therapeutic targets. J Pathol 2015; 235: [PMID: DOI: /path.4434] 3 Bruix J, Gores GJ, Mazzaferro V. Hepatocellular carcinoma: clinical frontiers and perspectives. Gut 2014; 63: [PMID: ] 4 El-Serag HB. Hepatocellular carcinoma. N Engl J Med 2011; 365: [PMID: DOI: /NEJMra ] 3835 April 14, 2016 Volume 22 Issue 14
150 Pan LH et al. Wnt3a in HCC 5 Maluccio M, Covey A. Recent progress in understanding, diagnosing, and treating hepatocellular carcinoma. CA Cancer J Clin 2012; 62: [PMID: DOI: / caac.21161] 6 Wang L, Yao M, Dong Z, Zhang Y, Yao D. Circulating specific biomarkers in diagnosis of hepatocellular carcinoma and its metastasis monitoring. Tumour Biol 2014; 35: 9-20 [PMID: DOI: /s ] 7 Yao M, Wang L, Qiu L, Qian Q, Yao D. Encouraging micrornabased Therapeutic Strategies for Hepatocellular Carcinoma. Anticancer Agents Med Chem 2015; 15: [PMID: DOI: / ] 8 Pez F, Lopez A, Kim M, Wands JR, Caron de Fromentel C, Merle P. Wnt signaling and hepatocarcinogenesis: molecular targets for the development of innovative anticancer drugs. J Hepatol 2013; 59: [PMID: DOI: /j.jhep ] 9 Rogacki K, Kasprzak A, Stępiński A. Alterations of Wnt/β-catenin signaling pathway in hepatocellular carcinomas associated with hepatitis C virus. Pol J Pathol 2015; 66: 9-21 [PMID: DOI: /pjp ] 10 Gao C, Xiao G, Hu J. Regulation of Wnt/β-catenin signaling by posttranslational modifications. Cell Biosci 2014; 4: 13 [PMID: DOI: / ] 11 Willert K, Nusse R. Wnt proteins. Cold Spring Harb Perspect Biol 2012; 4: a [PMID: DOI: /cshperspect. a007864] 12 Neth P, Ciccarella M, Egea V, Hoelters J, Jochum M, Ries C. Wnt signaling regulates the invasion capacity of human mesenchymal stem cells. Stem Cells 2006; 24: [PMID: DOI: /stemcells ] 13 Nalesso G, Sherwood J, Bertrand J, Pap T, Ramachandran M, De Bari C, Pitzalis C, Dell accio F. WNT-3A modulates articular chondrocyte phenotype by activating both canonical and noncanonical pathways. J Cell Biol 2011; 193: [PMID: DOI: /jcb ] 14 Kaur N, Chettiar S, Rathod S, Rath P, Muzumdar D, Shaikh ML, Shiras A. Wnt3a mediated activation of Wnt/β-catenin signaling promotes tumor progression in glioblastoma. Mol Cell Neurosci 2013; 54: [PMID: DOI: /j.mcn ] 15 Lamb R, Ablett MP, Spence K, Landberg G, Sims AH, Clarke RB. Wnt pathway activity in breast cancer sub-types and stem-like cells. PLoS One 2013; 8: e67811 [PMID: DOI: / journal.pone ] 16 Verras M, Brown J, Li X, Nusse R, Sun Z. Wnt3a growth factor induces androgen receptor-mediated transcription and enhances cell growth in human prostate cancer cells. Cancer Res 2004; 64: [PMID: DOI: / CAN ] 17 Gao Q, Qiu SJ, Fan J, Zhou J, Wang XY, Xiao YS, Xu Y, Li YW, Tang ZY. Intratumoral balance of regulatory and cytotoxic T cells is associated with prognosis of hepatocellular carcinoma after resection. J Clin Oncol 2007; 25: [PMID: DOI: /JCO ] 18 Ministry of Health of the People's Republic of China. [Updated standards for the diagnosis and treatment of primary liver cancer]. Zhonghua Ganzangbing Zazhi 2012; 20: [PMID: ] 19 Yao M, Wang L, Yao Y, Gu HB, Yao DF. Biomarker-based MicroRNA Therapeutic Strategies for Hepatocellular Carcinoma. J Clin Transl Hepatol 2014; 2: [PMID: DOI: /JCTH ] 20 Wei Y, Shen N, Wang Z, Yang G, Yi B, Yang N, Qiu Y, Lu J. Sorafenib sensitizes hepatocellular carcinoma cell to cisplatin via suppression of Wnt/β-catenin signaling. Mol Cell Biochem 2013; 381: [PMID: DOI: /s ] 21 Zhang Q, Bai X, Chen W, Ma T, Hu Q, Liang C, Xie S, Chen C, Hu L, Xu S, Liang T. Wnt/β-catenin signaling enhances hypoxiainduced epithelial-mesenchymal transition in hepatocellular carcinoma via crosstalk with hif-1α signaling. Carcinogenesis 2013; 34: [PMID: DOI: /carcin/bgt027] 22 Lai JP, Oseini AM, Moser CD, Yu C, Elsawa SF, Hu C, Nakamura I, Han T, Aderca I, Isomoto H, Garrity-Park MM, Shire AM, Li J, Sanderson SO, Adjei AA, Fernandez-Zapico ME, Roberts LR. The oncogenic effect of sulfatase 2 in human hepatocellular carcinoma is mediated in part by glypican 3-dependent Wnt activation. Hepatology 2010; 52: [PMID: DOI: / hep.23848] 23 Yang T, Cai SY, Zhang J, Lu JH, Lin C, Zhai J, Wu MC, Shen F. Krüppel-like factor 8 is a new Wnt/beta-catenin signaling target gene and regulator in hepatocellular carcinoma. PLoS One 2012; 7: e39668 [PMID: DOI: /journal.pone ] 24 Zhang S, Li J, He F, Wang XM. Abnormal nuclear expression of Pygopus-2 in human primary hepatocellular carcinoma correlates with a poor prognosis. Histopathology 2015; 67: [PMID: ] 25 Song K, Wu J, Jiang C. Dysregulation of signaling pathways and putative biomarkers in liver cancer stem cells (Review). Oncol Rep 2013; 29: 3-12 [PMID: DOI: /or ] 26 Jiang L, Yang YD, Fu L, Xu W, Liu D, Liang Q, Zhang X, Xu L, Guan XY, Wu B, Sung JJ, Yu J. CLDN3 inhibits cancer aggressiveness via Wnt-EMT signaling and is a potential prognostic biomarker for hepatocellular carcinoma. Oncotarget 2014; 5: [PMID: DOI: /oncotarget] 27 Lu LC, Shao YY, Lee YH, Hsieh MS, Hsiao CH, Lin HH, Kao HF, Ma YY, Yen FC, Cheng AL, Hsu CH. β-catenin (CTNNB1) mutations are not associated with prognosis in advanced hepatocellular carcinoma. Oncology 2014; 87: [PMID: DOI: / ] 28 Yao M, Pan LH, Yao DF. Glypican-3 as a specific biomarker for hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int 2015; 14: [PMID: DOI: /S (15) ] 29 Chen J, Liu J, Jin R, Shen J, Liang Y, Ma R, Lin H, Liang X, Yu H, Cai X. Cytoplasmic and/or nuclear expression of β-catenin correlate with poor prognosis and unfavorable clinicopathological factors in hepatocellular carcinoma: a meta-analysis. PLoS One 2014; 9: e [PMID: DOI: /journal.pone ] 30 Guan CN, Chen XM, Lou HQ, Liao XH, Chen BY, Zhang PW. Clinical significance of axin and β-catenin protein expression in primary hepatocellular carcinomas. Asian Pac J Cancer Prev 2012; 13: [PMID: ] 31 Ma L, Ji L, Yu Y, Wang J. Novel molecular targets for diagnosis and treatment of hepatocellular carcinoma. Discov Med 2015; 19: 7-14 [PMID: ] 32 Lee MA, Park JH, Rhyu SY, Oh ST, Kang WK, Kim HN. Wnt3a expression is associated with MMP-9 expression in primary tumor and metastatic site in recurrent or stage IV colorectal cancer. BMC Cancer 2014; 14: 125 [PMID: DOI: / ] 33 Pinyol R, Nault JC, Quetglas IM, Zucman-Rossi J, Llovet JM. Molecular profiling of liver tumors: classification and clinical translation for decision making. Semin Liver Dis 2014; 34: [PMID: DOI: /s ] 34 Guerrieri F, Belloni L, Pediconi N, Levrero M. Molecular mechanisms of HBV-associated hepatocarcinogenesis. Semin Liver Dis 2013; 33: [PMID: DOI: / s ] P- Reviewer: Koh PS S- Editor: Yu J L- Editor: Filipodia E- Editor: Liu XM 3836 April 14, 2016 Volume 22 Issue 14
151 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Clinical Trials Study ORIGINAL ARTICLE Endoscopic management of unresectable malignant gastroduodenal obstruction with a nitinol uncovered metal stent: a prospective Japanese multicenter study Reina Sasaki, Yuji Sakai, Toshio Tsuyuguchi, Takao Nishikawa, Tatsuya Fujimoto, Shigeru Mikami, Harutoshi Sugiyama, Osamu Yokosuka Reina Sasaki, Yuji Sakai, Toshio Tsuyuguchi, Takao Nishikawa, Harutoshi Sugiyama, Osamu Yokosuka, Department of Gastroenterology and Nephrology, Graduate School of Medicine, Chiba University, Chiba , Japan Tatsuya Fujimoto, Department of Gastroenterology, Kimitsu Chuo Hospital, Chiba , Japan Shigeru Mikami, Department of Gastroenterology, Kikkoman General Hospital, Chiba , Japan Author contributions: Sasaki R contributed to collection, organization, analysis, and interpretation of data, and drafting of the manuscript; Sakai Y contributed to conception and design of the study; Tsuyuguchi T final approvaled the manuscript; Nishikawa T critical revision of technical content; Fujimoto T, Mikami S, Sugiyama H and Yokosuka O contributed to collection and organization of data. Institutional review board statement: This study was conducted under approval our ethical committee. Clinical trial registration statement: Medical Information Network Clinical Trial Registry (ID: UMIN ). Informed consent statement: All the treatment procedures were performed after obtaining the informed consent in writing from the patients. Conflict-of-interest statement: The authors have no other disclosures. Data sharing statement: I share data in the group of us. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Yuji Sakai, MD, Department of Gastroenterology and Nephrology, Graduate School of Medicine, Chiba University, Inohana, Chuo-ku, Chiba , Japan. sakai4754@yahoo.co.jp Telephone: Fax: Received: January 23, 2016 Peer-review started: January 23, 2016 First decision: February 18, 2016 Revised: February 25, 2016 Accepted: March 14, 2016 Article in press: March 14, 2016 Published online: April 14, 2016 Abstract AIM: to determine the safety and efficacy of endoscopic duodenal stent placement in patients with malignant gastric outlet obstruction. METHODS: This prospective, observational, multicenter study included 39 consecutive patients with malignant gastric outlet obstruction. All patients underwent endoscopic placement of a nitinol, uncovered, selfexpandable metal stent. The primary outcome was clinical success at 2 wk after stent placement that was defined as improvement in the Gastric Outlet Obstruction Scoring System score relative to the baseline. RESULTS: Technical success was achieved in all duodenal stent procedures. Procedure-related complications occurred in 4 patients (10.3%) in the form of mild pneumonitis. No other morbidities or mortalities 3837 April 14, 2016 Volume 22 Issue 14
152 Sasaki R et al. Multicenter study of duodenal stent were observed. The clinical success rate was 92.3%. The mean survival period after stent placement was 103 d. The mean period of stent patency was 149 d and the patency remained acceptable for the survival period. Stent dysfunction occurred in 3 patients (7.7%) on account of tumor growth. CONCLUSION: Endoscopic management using duodenal stents for patients with incurable malignant gastric outlet obstruction is safe and improved patients quality of life. Key words: Duodenal stenosis; Gastrointestinal stent; Gastric stenosis; Malignant tumors; Metallic stent The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Endoscopic management using duodenal stents for patients with incurable malignant gastric outlet obstruction is safe and improved patients quality of life. Sasaki R, Sakai Y, Tsuyuguchi T, Nishikawa T, Fujimoto T, Mikami S, Sugiyama H, Yokosuka O. Endoscopic management of unresectable malignant gastroduodenal obstruction with a nitinol uncovered metal stent: A prospective Japanese multicenter study. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Approximately 15%-20% of patients with various types of gastrointestinal malignancies, such as gastric cancer or pancreatic cancer, develop gastric outlet obstruction (GOO) during the end stage of their disease [1]. GOO causes nausea, vomiting, and abdominal discomfort, which diminish quality of life [2]. The primary aim of palliation for these patients is relief of obstructionrelated symptoms. Traditionally, GOO was treated using open surgical bypass; however this procedure has been reported to be associated with considerable morbidity and mortality [3]. Recently, endoscopic placement of self-expandable metal stents has emerged as an alternative, minimally invasive treatment in cases of malignant GOO. The reported technical success rates have ranged from 94% to 100%, and the clinical success rates have ranged from 84% to 97% [4-10]. Furthermore, stent placement allows faster resumption of food intake, usually tolerated the day after stent placement, and involves a shorter hospital stay than surgical gastrojejunostomy (GJ) [4,11,12]. Previously stent placement involved use of an over-the-wire technique under fluoroscopy. However, recent advances in devices technology have led to stent placement using a through-the-scope technique. The former technique takes much longer to perform, and the placement procedure is complicated and difficult [13]. The objective of this prospective single-arm observation study was to determine the safety and efficacy of endoscopic duodenal stent placement in patients with malignant GOO, including postoperative recurrence. MATERIALS AND METHODS Patients This was a prospective, observational, multicenter study of consecutive patients with malignant GOO, including postoperative recurrence, who were referred to 3 hospitals in Japan (1 university hospital and 2 referral hospitals) for palliative treatment from April 2011 to June Surgery was contraindicated in these patients, either because the lesion was not resectable or because the patients had advanced metastatic disease. Patients who had symptoms of GOO and a Gastric Outlet Obstruction Scoring System (GOOSS) [14] score (0 = no oral intake, 1 = liquid diet, 2 = soft solid diet, 3 = low residue or normal diet) of 2 were considered for inclusion in this study. Exclusion criteria included age < 20 years; obstruction in the proximal stomach, distal small intestine, or colon; previous treatment with metal stent for the same site; and contraindications for endoscopic therapy. The study protocol was approved by the Institutional Review Boards of the Ethics Committees at each hospital and registered with the University Hospital Medical Information Network Clinical Trials Registry (ID: UMIN ). Written informed consent was obtained from all patients. Procedures The WallFlex duodenal stent (Boston Scientific Japan, Tokyo, Japan) was used to treat all patients in this study. A nitinol, uncovered, self-expandable metal stent, available in lengths of 6, 9, and 12 cm, with a body diameter of 22 mm and a flare diameter of 27 mm at the proximal and distal ends, was used. The stent delivery system had a diameter of 10 Fr and allowed stent placement through the scope. If patients were suspected of having biliary obstruction, biliary drainage by insertion of a selfexpandable metal stent was endoscopically performed in advance or concurrent with duodenal stent placement. Duodenal stent placement was performed with the patient under conscious sedation. A forward-viewing gastrointestinal endoscope (Olympus CF-H260AI; Olympus Medical Systems, Tokyo, Japan) or a lateralviewing duodenoscope (Olympus TJF-260V; Olympus Medical Systems) with a working channel diameter of 3.7 mm was used depending on the site of the stricture. The oral side of the stricture was confirmed by direct endoscopic observation, and the length and shape of 3838 April 14, 2016 Volume 22 Issue 14
; B: A self-expandable metal stent was")
153 Sasaki R et al. Multicenter study of duodenal stent A B C D E F G H I Figure 1 Case of hepatocellular carcinoma. A: Cholangiogram showing a biliary stricture caused by primary tumor and lymph node metastasis in the right hepatic duct and middle bile duct (arrow heads); B: A self-expandable metal stent was inserted endoscopically; C, D: Coronal sections of contrast-enhanced computed tomography images show duodenal invasion of lymph node metastasis (arrow heads); E: Endoscopic view showing the oral side of the stricture at the superior duodenal angle; F: Injection of contrast material demonstrates a stricture in the second duodenal segment (arrow heads); G, H: A nitinol metal stent was placed in the shape of the character C from the stomach pylorus to the third duodenal segment (G: Endoscopic view; H: X-ray); I: X-ray image taken 1 wk later shows sufficient expansion and stability of the duodenal stent. the stricture was assessed fluoroscopically (Figure 1). A catheter and a guidewire were passed through the stricture and the guidewire was used to position the stent delivery system into the stricture. A stent length of 2 cm longer than the stricture was selected. The stent was deployed under continuous endoscopic and fluoroscopic control. All procedures were performed by therapeutic endoscopists who performed more than 100 endoscopic procedures per year. Outcome and definitions The primary outcome measure of this study was clinical success at 2 wk after stent placement. Clinical success was defined as improvement in the GOOSS score relative to the baseline score. Secondary outcomes included technical success, improvement in the World Health Organization (WHO) performance score, procedure-related complications, overall survival, and stent patency, which was defined as the time period between stent placement and stent dysfunction. Technical success was defined as successful stent placement and deployment at the site of stricture. The 2010 American Society for Gastrointestinal Endoscopy consensus criteria were used to define and grade complications [15]. Data collection The following data were collected before stent placement: age, sex, medical history, malignant GOO type, clinical stage of cancer according to the TNM 3839 April 14, 2016 Volume 22 Issue 14
154 Sasaki R et al. Multicenter study of duodenal stent Table 1 Baseline patients and stricture characteristics n (%) Age, yr, mean ± SD (range) 69.2 ± 13.3 (35-90) Sex (M/F) 25/14 Primary malignancy, Gastric cancer 1 (43.6) Pancreatic cancer 1 (41.0) Duodenal carcinoma 2 (5.1) Extrahepatic cholangiocarcinoma 1 (2.6) Intrahepatic cholangiocarcinoma 1 (2.6) Ampullary carcinoma 1 (2.6) Hepatocellular carcinoma (lymph node metastasis) 1 (2.6) Clinical stage of cancer 1 Stage Ⅲ 2 16 (41.0) Stage Ⅳ 3 23 (59.0) Altered gastrointestinal anatomy Gastroduodenostomy after Billroth Ⅰ gastrectomy 3 (7.7) Gastrojejunostomy after Billroth Ⅱ gastrectomy 1 (2.6) Gastrojejunostomy after pancreatoduodenectomy 1 (2.6) Gastrojejunostomy for surgical bypass 1 (2.6) Location of stricture Distal stomach 16 (41.0) Duodenal bulb 4 (10.3) Second duodenal segment 4 (10.3) Second/third duodenal segment 4 (10.3) Third duodenal segment 5 (12.8) Anastmosis site (gastrostomy) 6 (15.4) Stricture length, mm, mean ± SD (range) 42.6 ± 19.8 (15-93) GOOSS score before stent placement 0-no oral intake 16 (41.0) 1-liquid diet 18 (46.2) 2-soft solid diet 5 (12.8) 3-low residue or normal diet 0 WHO perfomance score 0-fully active 7 (17.9) 1-cannot carry out heavy physical work 8 (20.5) 2-up and about > 50% of the day 13 (33.3) 3-up and about < 50% of the day 9 (23.1) 4-bed or chair bound all day 2 (5.1) 1 TNM classification system (ref.); 2 Including stage ⅢB and ⅢC of gastric cancer; 3 Including stage ⅣA of intrahepatic cholangiocarcinoma and hepatocellular carcinoma. GOOSS: Gastric outlet obstruction scoring system; WHO: World Health Organization. classification system [16], obstruction site, GOOSS score, and WHO performance score. After stent placement, follow-up data were obtained during inpatient clinic visits when the patient was still hospitalized or during outpatient clinic visits. GOOSS scores and WHO performance scores were collected at 2 wk. The following data were collected until patient death or 18 mo postprocedure: procedure-related complications, additional therapy (chemotherapy, radiotherapy), and stent dysfunction. We confirmed stent dysfunction in a gastrointestinal contrast study and by endoscopy when GOO symptoms recurred. Statistical analysis The sample size was calculated on the basis of clinical success after stent placement. Previous reported data indicated that the clinical success rate was approximately 90% [4-10]. Consequently, we estimated that 35 patients would be required to assess the duodenal stent clinical success rate with a confidence interval of 95%, a power of 80%, and a margin of error of 10%. Furthermore, we estimated that as many as 40 patients would be required to account for possible loss of patients during follow-up. Continuous variables were expressed as the mean, median, standard deviation, standard error, and interquartile range, whereas categorical variables were expressed as counts and percentages. The Wilcoxon signed-rank test was used to assess improvements in the GOOSS score and WHO performance score relative to the baseline scores. Kaplan-Meier analysis was used to calculate overall survival and stent patency. SAS version 9.3 (SAS Institute, Cary, NC, United States) was used to perform all statistical analyses. The significance level was set to P < RESULTS Baseline characteristics A total of 39 patients [25 men, 14 women; age (mean ± SD): 69.2 ± 13.3 years] underwent duodenal stent placement between April 2011 and June The patient characteristics are summarized in Table 1. Of the included patients, 17 (43.6%) were diagnosed as having gastric cancer. The remaining patients had pancreatic cancer (16 patients, 41.0%), duodenal cancer (2 patients, 5.1%), extrahepatic cholangiocarcinoma (1 patient, 2.6%), intrahepatic cholangiocarcinoma (1 patient, 2.6%), ampullary carcinoma (1 patient, 2.6%), and hepatocellular carcinoma (1 patient, 2.6%). A pathological diagnosis of malignancy was made for 31 patients (79.5%). Six patients (15.4%) with altered gastrointestinal anatomy had strictures in the surgical anastomosis. Sixteen patients (41.0%) had stricture in the distal stomach, whereas 17 patients (43.6%) had strictures in the duodenum. Before stent placement, 16 (41.0%), 18 (46.2%), 5 (12.8%), and 0 (0%) patients had GOOSS scores of 0, 1, 2, and 3, respectively. Procedural details Technical success was achieved in 39 patients (100%). The duodenal stent was placed at the oral side of the papilla in 23 patients (59.0%), on the papilla in 6 patients (15.4%), and at the anal side of the papilla in 10 patients (25.6%). Procedure-related complications occurred in 4 patients (10.3%) in the form of mild pneumonitis. No other morbidities or mortalities were observed. Clinical success Clinical success was achieved in 36 of the 39 patients (92.3%). There was no increase/decrease in the GOOSS score for 3 patients (Figure 2A). The GOOSS scores for these patients were 0, 1, and 2, respectively. Oral intake inability in a patient whose GOOSS score remained 0 was caused by progression of a peritoneal carcinomatosis. At inclusion, the mean GOOSS score 3840 April 14, 2016 Volume 22 Issue 14
155 Sasaki R et al. Multicenter study of duodenal stent A Frequency B Mean GOOSS score ± 2 SE ± Difference in GOOSS score from baseline Table 2 Procedure details and study outcomes n (%) Technical success 39 (100) Relationship of the papilla and stent placement site Oral side of the papilla 23 (59.0) On the papilla 6 (15.4) Anal side of the papilla 10 (25.6) Procedure related complication Aspiration pneumonitis 4 (10.3) Bleeding 0 0 Perforation 0 0 Cholangitis 0 0 Motality disorder 0 0 Clinical success 36 (92.3) Additional treatment of malignancy after stent placement Chemotherapy 15 (38.5) Chemoradiation 1 (2.6) Survival after stent placement, d Median (IQR) 50.0 ( ) mean ± SE ± 18.2 Stent patency, d Median Not available mean ± SE (7.2) Stent dysfunction Stent ingrowth 2 (5.1) Stent overgrowth 1 (2.6) Stent compression 0 Stent migration 0 Food impaction Baseline After 14 d IQR: Interquartile range. Figure 2 Differences between the Gastric Outlet Obstruction Scoring System score at baseline and at 14 d after stent placement are shown (A) and the mean Gastric Outlet Obstruction Scoring System scores at baseline and after 14 d are shown (B). P-value of the Wilcoxon signed-rank test comparison was < GOOSS: Gastric Outlet Obstruction Scoring System. was 0.69 (Figure 2B). After 14 d of duodenal stent placement, the mean GOOSS score significantly improved to 2.21 (P < ). On the other hand, there was no significant difference in the WHO performance score before and after duodenal stenting (mean, 1.77 vs 1.95, P = 0.57). Survival After duodenal stenting, 15 patients (38.5%) received chemotherapy as an additional treatment of malignancy, and 1 patient (2.6%) received chemoradiation. Thirty-eight patients died during and 1 was alive at the end of the follow-up period. The median survival period of the 39 patients was 50 d, and the mean period was 103 d (Table 2). Four patients survived > 200 d, 2 survived > 300 d, 1 survived > 400 d, and 1 survived > 500 d. Stent patency During the follow-up period, 3 patients (7.7%) experienced stent dysfunction, which was caused by tumor growth in all 3 patients. No patient had stent migration (Table 2). The mean period of stent patency was 149 d (Figure 3). Stent patency was > 200 d in 2 patients, > 300 d in 2 patients, > 400 d in 1 patient, and > 500 d in 1 patient. All 6 patients with altered gastrointestinal anatomy died without recurrence of GOO symptoms, and the maximum period of stent patency was 77 d. All 3 patients with stent dysfunction underwent reintervention involving stent-in-stent placement of the duodenal stent, and all of them died without experiencing recurrent stent dysfunction. The stent patency periods after reintervention were 41, 73, and 88 d, respectively. DISCUSSION We prospectively evaluated outcomes of endoscopic management using a nitinol metal stent in patients with malignant GOO. In this study, the clinical success rate was 92.3%. Recent prospective multicenter studies have reported similar clinical success rates ranging from 85% to 91% [17-21]. Our study showed that the stent patency period was acceptable for the patient survival period. Endoscopic stent placement or surgical GJ are commonly used palliative treatments for malignant GOO. It has been reported that patients who have undergone stent placement require a shorter time to achieve oral intake and a shorter hospital stay than those who have undergone surgical GJ [4,11,12]. In a previous study, better physical health scores were obtained 1 mo after stent placement than 3841 April 14, 2016 Volume 22 Issue 14
156 Sasaki R et al. Multicenter study of duodenal stent Stent patency t /d Figure 3 Kaplan-Meier curve showing stent patency. after laparoscopic GJ [22], whereas fewer recurrent obstructive symptoms were associated with surgical GJ than with stent placement. The SUSTENT study results suggest that GJ should be primarily considered for patients with an expected survival of 2 mo and that stent placement should be primarily considered for patients with a shorter anticipated survival [23]. However, in this study, some patients, even those with unresectable malignancies, survived longer after chemotherapy. Moreover, long-term stent patencies were also observed. Further investigation to determine if duodenal stenting should be performed in patients with prognoses expected to be 2 mo is necessary. The major late complication associated with duodenal stents was obstruction, which was caused by tumor ingrowth or overgrowth. However, reintervention for obstructed duodenal stents is noninvasive and effective [24]. In addition, in this study, reintervention to correct an obstructed duodenal stent was technically and clinically successful. Patients at the end stage of cancer do not tolerate invasive procedures, and their life expectancy is relatively short; thus, stent placement is preferred for such patients. In a previous report of uncovered stents for malignant GOO, approximately 19% of patients had tumor ingrowths [25]. If the origin of obstructive malignancies was intraluminal, such as gastric cancer and duodenal cancer, then tumor ingrowth was often induced by uncovered stents. Extraluminal malignancies have a low risk of causing tumor ingrowth [26,27]. In a prospective cohort study [9] and a randomized controlled trial [10] of covered vs uncovered metal stents for malignant GOO, there were no differences in the clinical success rate and stent patency but there was a difference in the pattern of late stent failure. In addition, stent migration occurred more frequently for covered stents than for uncovered stents, and restenosis caused by tumor ingrowth occurred more frequently for uncovered stents [9,10]. Similarly, in the present study using uncovered metal stents, there was no stent migration, and only stent dysfunction due to tumor growth was observed. The currently available duodenal stents are the braided nitinol metal type [8,17,18,20]. Some studies have examined radial force as an expanding force and axial force as a force for recovery to a straight position for various structures and materials in biliary [28] and esophageal [29] metal stents but not in duodenal stents. In esophageal stents, braided nitinol metal stents were reported to have a lower radial force and a higher axial force than non-braided stents [29]. Because the axial force decreases with an increase in stent length [28], kinking and intestinal damage may be prevented by selecting a long stent in the duodenum (Figure 1). Duodenal stents of various structures and materials should be examined to reduce stent dysfunction. There were some limitations in the present study because we did not conduct a comparative investigation. First, we did not compare metal stent types, such as covered vs uncovered metal stents, the structure and material used, or the stent length. Second, stent placement techniques, such as the over-the-wire technique under fluoroscopy and the through-the-scope technique, were not compared. Third, we did not compare endoscopic stenting for malignant GOO with other endoscopic management approaches, such as endoscopic GJ. Van Hooft et al [30] reported a prospective multicenter study of endoscopic GJ that used a magnetic anastomotic device and transanastomotic deployment of stents. In an animal study, Itoi et al [31] reported an endoscopic ultrasonography-guided GJ technique using a doubleballoon enteric tube and a bilateral reflected metal stent. Stent dysfunction may be less likely to occur in routes that avoid the malignant obstruction section than in routes that include the malignant obstruction section. A randomized controlled trial of endoscopic duodenal stenting vs endoscopic GJ for malignant GOO is required. In conclusion, this prospective multicenter study showed that placement of a nitinol, uncovered, selfexpandable metal stent in patients with incurable malignant GOO was safe and improved their quality of life. ACKNOWLEDGMENTS The authors thank Rintaro Mikata, Shin Yasui, Kiyofumi Ishii, Sadahiro Itoh, Hiroshi Ohyama, Dai Sakamoto, Yuto Watanabe, Masato Nakamura, Ryousaku Azemoto, Yu Yoshida, and Toru Wakamatsu for their contributions in the collection of data. COMMENTS Background Gastric outlet obstruction (GOO) was treated using open surgical bypass; however this procedure has been reported to be associated with considerable morbidity and mortality. Recently, endoscopic placement of self-expandable metal stents has emerged as an alternative, minimally invasive treatment in 3842 April 14, 2016 Volume 22 Issue 14
157 Sasaki R et al. Multicenter study of duodenal stent cases of malignant GOO. Research frontiers Patients of GOO underwent endoscopic placement of a nitinol, uncovered, selfexpandable metal stent. The primary outcome was clinical success at 2 wk after stent placement that was defined as improvement in the Gastric Outlet Obstruction Scoring System (GOOSS) score relative to the baseline. Innovations and breakthroughs Endoscopic stent placement or surgical gastrojejunostomy (GJ) are commonly used palliative treatments for malignant GOO. This study showed that the stent patency period was acceptable for the patient survival period. At inclusion, the mean GOOSS score was After 14 d of duodenal stent placement, the mean GOOSS score significantly improved to 2.21 (P < ). Endoscopic management using duodenal stents for patients with incurable malignant gastric outlet obstruction is safe and improved patients quality of life. Applications Surgery was contraindicated in these patients, either because the lesion was not resectable or because the patients had advanced metastatic disease. Terminology Endoscopic management using duodenal stents for patients with incurable malignant gastric outlet obstruction is safe and improved patients quality of life. Peer-review The reviewed paper is very well organized, performed, and written research on actual topic. This article is very interesting and innovating and deserves publication. REFERENCES 1 Lillemoe KD, Cameron JL, Hardacre JM, Sohn TA, Sauter PK, Coleman J, Pitt HA, Yeo CJ. Is prophylactic gastrojejunostomy indicated for unresectable periampullary cancer? A prospective randomized trial. Ann Surg 1999; 230: discussion [PMID: ] 2 Monson JR, Donohue JH, McIlrath DC, Farnell MB, Ilstrup DM. Total gastrectomy for advanced cancer. A worthwhile palliative procedure. Cancer 1991; 68: [PMID: ] 3 Bozzetti F, Bonfanti G, Audisio RA, Doci R, Dossena G, Gennari L, Andreola S. Prognosis of patients after palliative surgical procedures for carcinoma of the stomach. Surg Gynecol Obstet 1987; 164: [PMID: ] 4 Jeurnink SM, van Eijck CH, Steyerberg EW, Kuipers EJ, Siersema PD. Stent versus gastrojejunostomy for the palliation of gastric outlet obstruction: a systematic review. BMC Gastroenterol 2007; 7: 18 [PMID: ] 5 Kim JH, Song HY, Shin JH, Choi E, Kim TW, Jung HY, Lee GH, Lee SK, Kim MH, Ryu MH, Kang YK, Kim BS, Yook JH. Metallic stent placement in the palliative treatment of malignant gastroduodenal obstructions: prospective evaluation of results and factors influencing outcome in 213 patients. Gastrointest Endosc 2007; 66: [PMID: ] 6 Mutignani M, Tringali A, Shah SG, Perri V, Familiari P, Iacopini F, Spada C, Costamagna G. Combined endoscopic stent insertion in malignant biliary and duodenal obstruction. Endoscopy 2007; 39: [PMID: ] 7 Graber I, Dumas R, Filoche B, Boyer J, Coumaros D, Lamouliatte H, Legoux JL, Napoléon B, Ponchon T. The efficacy and safety of duodenal stenting: a prospective multicenter study. Endoscopy 2007; 39: [PMID: ] 8 van Hooft JE, Uitdehaag MJ, Bruno MJ, Timmer R, Siersema PD, Dijkgraaf MG, Fockens P. Efficacy and safety of the new WallFlex enteral stent in palliative treatment of malignant gastric outlet obstruction (DUOFLEX study): a prospective multicenter study. Gastrointest Endosc 2009; 69: [PMID: DOI: /gie ] 9 Lee KM, Choi SJ, Shin SJ, Hwang JC, Lim SG, Jung JY, Yoo BM, Cho SW, Kim JH. Palliative treatment of malignant gastroduodenal obstruction with metallic stent: prospective comparison of covered and uncovered stents. Scand J Gastroenterol 2009; 44: [PMID: DOI: / ] 10 Kim CG, Choi IJ, Lee JY, Cho SJ, Park SR, Lee JH, Ryu KW, Kim YW, Park YI. Covered versus uncovered self-expandable metallic stents for palliation of malignant pyloric obstruction in gastric cancer patients: a randomized, prospective study. Gastrointest Endosc 2010; 72: [PMID: DOI: / gie ] 11 Hosono S, Ohtani H, Arimoto Y, Kanamiya Y. Endoscopic stenting versus surgical gastroenterostomy for palliation of malignant gastroduodenal obstruction: a meta-analysis. J Gastroenterol 2007; 42: [PMID: ] 12 Ly J, O Grady G, Mittal A, Plank L, Windsor JA. A systematic review of methods to palliate malignant gastric outlet obstruction. Surg Endosc 2010; 24: [PMID: DOI: / s ] 13 Maetani I, Ukita T, Nambu T, Shigoka H, Omuta S, Endo T, Takahashi K. Comparison of ultraflex and niti-s stents for palliation of unresectable malignant gastroduodenal obstruction. Dig Endosc 2010; 22: [PMID: DOI: /j x] 14 Adler DG, Baron TH. Endoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients. Am J Gastroenterol 2002; 97: [PMID: ] 15 Cotton PB, Eisen GM, Aabakken L, Baron TH, Hutter MM, Jacobson BC, Mergener K, Nemcek A, Petersen BT, Petrini JL, Pike IM, Rabeneck L, Romagnuolo J, Vargo JJ. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc 2010; 71: [PMID: DOI: /j.gie ] 16 Paleri V, Mehanna H, Wight RG. TNM classification of malignant tumours 7th edition: what s new for head and neck? Clin Otolaryngol 2010; 35: [PMID: ] 17 van Hooft JE, van Montfoort ML, Jeurnink SM, Bruno MJ, Dijkgraaf MG, Siersema PD, Fockens P. Safety and efficacy of a new non-foreshortening nitinol stent in malignant gastric outlet obstruction (DUONITI study): a prospective, multicenter study. Endoscopy 2011; 43: [PMID: DOI: / s ] 18 Kim YW, Choi CW, Kang DH, Kim HW, Chung CU, Kim DU, Park SB, Park KT, Kim S, Jeung EJ, Bae YM. A double-layered (comvi) self-expandable metal stent for malignant gastroduodenal obstruction: a prospective multicenter study. Dig Dis Sci 2011; 56: [PMID: DOI: /s ] 19 Costamagna G, Tringali A, Spicak J, Mutignani M, Shaw J, Roy A, Johnsson E, De Moura EG, Cheng S, Ponchon T, Bittinger M, Messmann H, Neuhaus H, Schumacher B, Laugier R, Saarnio J, Ariqueta FI. Treatment of malignant gastroduodenal obstruction with a nitinol self-expanding metal stent: an international prospective multicentre registry. Dig Liver Dis 2012; 44: [PMID: DOI: /j.dld ] 20 van den Berg MW, Haijtink S, Fockens P, Vleggaar FP, Dijkgraaf MG, Siersema PD, van Hooft JE. First data on the Evolution duodenal stent for palliation of malignant gastric outlet obstruction (DUOLUTION study): a prospective multicenter study. Endoscopy 2013; 45: [PMID: DOI: / s ] 21 Tringali A, Didden P, Repici A, Spaander M, Bourke MJ, Williams SJ, Spicak J, Drastich P, Mutignani M, Perri V, Roy A, Johnston K, Costamagna G. Endoscopic treatment of malignant gastric and duodenal strictures: a prospective, multicenter study. Gastrointest Endosc 2014; 79: [PMID: DOI: / j.gie ] 22 Mehta S, Hindmarsh A, Cheong E, Cockburn J, Saada J, Tighe R, Lewis MP, Rhodes M. Prospective randomized trial of laparoscopic gastrojejunostomy versus duodenal stenting for malignant gastric 3843 April 14, 2016 Volume 22 Issue 14

158 Sasaki R et al. Multicenter study of duodenal stent outflow obstruction. Surg Endosc 2006; 20: [PMID: ] 23 Jeurnink SM, Steyerberg EW, van Hooft JE, van Eijck CH, Schwartz MP, Vleggaar FP, Kuipers EJ, Siersema PD. Surgical gastrojejunostomy or endoscopic stent placement for the palliation of malignant gastric outlet obstruction (SUSTENT study): a multicenter randomized trial. Gastrointest Endosc 2010; 71: [PMID: DOI: /j.gie ] 24 Park JC, Park JJ, Cheoi K, Chung H, Lee H, Shin SK, Lee SK, Lee YC. Clinical outcomes of secondary stent-in-stent selfexpanding metal stent placement for primary stent malfunction in malignant gastric outlet obstruction. Dig Liver Dis 2012; 44: [PMID: DOI: /j.dld ] 25 Nassif T, Prat F, Meduri B, Fritsch J, Choury AD, Dumont JL, Auroux J, Desaint B, Boboc B, Ponsot P, Cervoni JP. Endoscopic palliation of malignant gastric outlet obstruction using selfexpandable metallic stents: results of a multicenter study. Endoscopy 2003; 35: [PMID: ] 26 Telford JJ, Carr-Locke DL, Baron TH, Tringali A, Parsons WG, Gabbrielli A, Costamagna G. Palliation of patients with malignant gastric outlet obstruction with the enteral Wallstent: outcomes from a multicenter study. Gastrointest Endosc 2004; 60: [PMID: ] 27 Kim GH, Kang DH, Lee DH, Heo J, Song GA, Cho M, Yang US. Which types of stent, uncovered or covered, should be used in gastric outlet obstructions? Scand J Gastroenterol 2004; 39: [PMID: ] 28 Isayama H, Nakai Y, Toyokawa Y, Togawa O, Gon C, Ito Y, Yashima Y, Yagioka H, Kogure H, Sasaki T, Arizumi T, Matsubara S, Yamamoto N, Sasahira N, Hirano K, Tsujino T, Toda N, Tada M, Kawabe T, Omata M. Measurement of radial and axial forces of biliary self-expandable metallic stents. Gastrointest Endosc 2009; 70: [PMID: DOI: /j.gie ] 29 Hirdes MM, Vleggaar FP, de Beule M, Siersema PD. In vitro evaluation of the radial and axial force of self-expanding esophageal stents. Endoscopy 2013; 45: [PMID: DOI: /s ] 30 van Hooft JE, Vleggaar FP, Le Moine O, Bizzotto A, Voermans RP, Costamagna G, Devière J, Siersema PD, Fockens P. Endoscopic magnetic gastroenteric anastomosis for palliation of malignant gastric outlet obstruction: a prospective multicenter study. Gastrointest Endosc 2010; 72: [PMID: DOI: /j.gie ] 31 Itoi T, Itokawa F, Uraoka T, Gotoda T, Horii J, Goto O, Moriyasu F, Moon JH, Kitagawa Y, Yahagi N. Novel EUS-guided gastrojejunostomy technique using a new double-balloon enteric tube and lumen-apposing metal stent (with videos). Gastrointest Endosc 2013; 78: [PMID: DOI: /j.gie ] P- Reviewer: Shiryajev YN S- Editor: Ma YJ L- Editor: A E- Editor: Ma S 3844 April 14, 2016 Volume 22 Issue 14
159 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Observational Study ORIGINAL ARTICLE Autofluorescence imaging endoscopy can distinguish non-erosive reflux disease from functional heartburn: A pilot study Xi Luo, Xiao-xu Guo, Wei-feng Wang, Li-hua Peng, Yun-sheng Yang, Noriya Uedo Xi Luo, Xiao-Xu Guo, Wei-Feng Wang, Li-Hua Peng, Yun- Sheng Yang, Department of Gastroenterology and Hepatology, Chinese PLA General Hospital, Beijing , China Noriya Uedo, Department of Gastrointestinal Oncology, Osaka Medical Center for Cancer and Cardiovascular Diseases, Osaka , Japan Author contributions: Luo X and Guo XX contributed equally to this work. Luo X, Guo XX, Wang WF and Peng LH performed the research; Luo X and Guo XX analyzed the data and wrote the paper; Wang WF designed the research; Yang YY and Uedo N critically reviewed the article. Institutional review board statement: The study was reviewed and approved by the Ethics Committee of Chinese PLA General Hospital Institutional Review Board. Informed consent statement: All study participants, or their legal guardian, provided informed written consent prior to study enrollment. Clinical trial registration statement: This study is registered at =Search. The registration identification number is NCT Conflict-of-interest statement: The authors disclose no conflicts of interest. Data sharing statement: Technical appendix, statistical code, and dataset available from the corresponding author at wangwf301@hotmail.com. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Wei-feng Wang, MD, Department of Gastroenterology and Hepatology, Chinese PLA General Hospital, 28 Fuxing Road, Beijing , China. wangwf301@hotmail.com Telephone: Fax: Received: December 18, 2015 Peer-review started: December 22, 2015 First decision: January 13, 2016 Revised: February 9, 2016 Accepted: March 1, 2016 Article in press: March 2, 2016 Published online: April 14, 2016 Abstract AIM: To investigate whether autofluorescence imaging (AFI) endoscopy can distinguish non-erosive reflux disease (NERD) from functional heartburn (FH). METHODS: In this prospective observational trial, 127 patients presenting with typical reflux symptoms for > 6 mo were screened. All the participants underwent endoscopy, during which white light imaging (WLI) was followed by AFI. Finally 84 patients with normal esophageal appearance on WLI were enrolled. It was defined as being suggestive of NERD if one or more longitudinal purple lines longer than one centimeter were visualized in the distal part of the esophagus during AFI endoscopy. Ambulatory 24-h multichannel intraluminal impedance and ph monitoring was also performed. After standard proton-pump inhibitor (PPI) tests, subjects were divided into an NERD group and an FH group and the diagnostic performance of AFI endoscopy to differentiate NERD from FH was evaluated. RESULTS: Of 84 endoscopy-negative patients, April 14, 2016 Volume 22 Issue 14
160 Luo X et al. AFI distinguishes NERD from FH (42.9%) had a normal ph/impedance test. Of these, 26 patients with favorable responses to PPI tests were classified as having NERD. Finally 10 patients were diagnosed with FH and the others with NERD. Altogether, 68 (81.0%) of the 84 patients were positive on AFI endoscopy. In the NERD group, there were 67 (90.5%) patients with abnormal esophageal findings on AFI endoscopy while only 1 (10%) patient was positive on AFI endoscopy in the FH group. The sensitivity and specificity of AFI in differentiating NERD from FH were 90.5% (95%CI: 81.5%-96.1%) and 90.0% (95%CI: 55.5%-99.7%), respectively. Meanwhile, the accuracy, positive predictive value and negative predictive value of AFI in differentiating between NERD and FH were 90.5% (95%CI: 84.2%-96.8%), 98.5% (95%CI: 92.1%-99.9%) and 56.3% (95%CI: 30.0%-80.2%), respectively. CONCLUSION: Autofluorescence imaging may serve as a complementary method in evaluating patients with NERD and FH. Key words: Gastroesophageal reflux disease; White light imaging; Non-erosive reflux disease; Functional heartburn; Autofluorescence imaging; Ambulatory 24-h ph/impedance monitoring; Endoscopy; Esophagitis The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: To date, few efforts have been put on the application of autofluorescence imaging (AFI) endoscopy in patients with non-malignant conditions such as gastrointestinal reflux disease (GERD). Our data showed that endoscopic features on AFI can distinguish non-erosive reflux disease (NERD) from functional heartburn (FH). Its real-time characteristics and simple endoscopic criteria may enhance the use of AFI as a complementary tool in the differentiation of NERD and FH. We believe that these findings have important implications for future research on the application of AFI endoscopy in patients with GERD. Luo X, Guo XX, Wang WF, Peng LH, Yang YS, Uedo N. Autofluorescence imaging endoscopy can distinguish non-erosive reflux disease from functional heartburn: A pilot study. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Functional heartburn (FH) and non-erosive reflux disease (NERD) share common manifestations, including the presence of reflux symptoms and the absence of esophageal abnormalities on conventional endoscopy. These common manifestations make it difficult to distinguish between FH and NERD without invasive diagnostic tests [1,2]. Autofluorescence imaging (AFI) is capable of identifying indistinct mucosal lesions [3,4] invisible on conventional endoscopy. Trimodal endoscopy, which combines AFI with white light imaging (WLI) and narrow band imaging, has been used to screen for early stage gastrointestinal cancer. Recently, AFI endoscopy was shown to be useful in predicting acid reflux [5]. As is known to all, NERD is characterized etiologically by pathologic reflux, whereas FH is not. Whether AFI endoscopy is capable of differentiating NERD from FH has not yet been determined. This study aimed to investigate the diagnostic performance of AFI video endoscopy to distinguish NERD from FH in patients with typical reflux symptoms but no mucosal breaks in the esophagus on WLI. MATERIALS AND METHODS Study subjects The study protocol was approved by the Ethics Committee of Chinese PLA General Hospital and conformed to the principles of the Declaration of Helsinki. This trial has been registered at ClinicalTrials. gov (ID: NCT ). Written informed consent was obtained before each participant was enrolled. In this prospective observational trial, consecutive patients with typical heartburn and/or regurgitation for > 6 mo were screened in Chinese PLA General Hospital between 2012 and 2014 (Figure 1). All patients underwent gastroscopy with both WLI and AFI functioning. Ambulatory impedance and ph monitoring was also performed. All participants were subsequently assessed by standard proton-pump inhibitor (PPI) tests. Patients with any symptom suggestive of esophageal motility disorders other than gastroesophageal reflux disease (GERD) were assessed by esophageal manometry. Patients aged years and with negative esophageal findings on WLI were eligible for this study. Patients would not be included if they had any known esophageal disease, including esophagitis or Barrett s esophagus; gastric or duodenal ulcer (except scarring); a previous history of thoracic or upper gastrointestinal (GI) surgery; clinically significant heart, lung, liver, or kidney disease; or pregnancy. Esophagogastroduodenoscopy Before endoscopic examination, antisecretory therapy, including PPIs and histamine-2 receptor antagonists, was discontinued for no less than 1 mo. Oral antacid was allowed as rescue medication during wash-out period. Gastroscopy was performed using a FQ260Z endoscope (Olympus Inc., Tokyo, Japan), equipped with multiple charged coupled devices for both highdefinition WLI and AFI. During endoscopic examination, the upper GI tract was carefully visualized using WLI, with the presence of a normal or abnormal esophagus 3846 April 14, 2016 Volume 22 Issue 14
161 Luo X et al. AFI distinguishes NERD from FH Assessed for eligibility (n = 127) Table 1 Demographics and clinical features Excluded (n = 13) for a previous history of upper gastrointestinal surgery, chronic liver or renal disease, refusal to ph-metry Characteristic Patients (n = 84) Mean age (yr) 49.0 ± 12.6 Gender (male:female) 39:45 BMI (kg/m 2 ) 24.1 ± 3.7 Endoscopy (AFI + WLI) ph/impedance monitoring Inclusion (n = 84) Excluded (n = 27) for erosive esophagitis, Barrett s esophagus, peptic ulcer, upper gastrointestinal neoplasm Excluded (n = 3) for intolerance to ph-metry Figure 1 Flow diagram illustrating patients enrolled in the present study. AFI: Autofluorescence imaging; WLI: White light imaging. documented. The video endoscope was subsequently switched to AFI mode and the esophagus again examined. It was defined as being suggestive of NERD if one or more longitudinal purple lines longer than one centimeter were visualized in the distal part of the esophagus during AFI endoscopy. Ambulatory ph and impedance monitoring Ambulatory 24-h multichannel intraluminal impedance and ph monitoring was performed using the routine protocol of our department [5]. Briefly, a catheter (Sierra Scientific Instruments Inc., Los Angeles, CA, United States) was inserted transnasally and the ph sensor was sited 5 cm above the lower esophageal sphincter (LES) with the impedance recording segments positioned at 3, 5, 7, 9, 15 and 17 cm above the upper border of the LES. The catheter was connected to a data storage device programmed by an AccuTrac ph-z System (Sierra Scientific Instruments Inc, Los Angeles, CA, United States). Patients were asked to record a diary of their symptoms and activity, including the time of rising in the morning, times in the supine position and meal times, as well as the onset of symptoms. AccuView analysis software (Sierra Scientific Instruments Inc, Los Angeles, CA, United States) was used to identify acid and non-acid episodes. Symptom association probability (SAP) and symptom index (SI) were assessed to determine the relationship of symptoms with acid, weakly acid or weakly alkaline reflux during monitoring. A positive ph/impedance test was defined as (1) acid exposure time more than 4.2% of monitoring time; (2) SAP 95%; or (3) SI > Data are expressed as mean ± SD. BMI: Body mass index. 50% [6,7]. Diagnosis of NERD and FH A diagnosis of NERD was reached when the endoscopynegative patients presented a positive ph/impedance or PPI test [8,9]. Consistent with Rome Ⅲ criteria [8], patients with normal esophageal findings on WLI were diagnosed with FH if they had normal ph/impedance monitoring results and negative PPI tests. Statistical analysis Data are expressed as mean and standard deviation. The subjects were divided into an NERD group and an FH group. The diagnostic performance of AFI for differentiating NERD from FH was calculated, using the sensitivity, specificity, accuracy, positive predictive value and negative predictive value with 95%CI. SPSS software (SPSS version 11.5, Chicago, IL, United States) was applied for statistical analyses. The diagnostic performance of different measures was evaluated using the McNemar test. RESULTS Demographic features Of the 127 consecutive patients with typical reflux symptoms screened for this study, 43 were excluded due to a previous history of upper gastrointestinal surgery, erosive esophagitis, Barrett s esophagus, peptic ulcer, upper gastrointestinal neoplasm, chronic liver or renal disease, or intolerance to ph-metry. Finally, 84 patients with negative esophageal findings on WLI were enrolled; their demographic and clinical characteristics are shown in Table 1. Yield of ph/impedance monitoring and PPI test Of 84 eligible participants, 48 (57.1%) were positive on ph/impedance tests (Figure 2), suggesting a diagnosis of NERD. Of 36 patients (42.9%) with normal ph/ impedance results, 26 benefitted from PPI tests and were classified as having NERD and the remaining 10 patients were classified as having FH. Diagnostic value of AFI endoscopy Altogether, 68 (81.0%) of the 84 patients were positive on AFI endoscopy (Figure 3) and the others were negative (Figure 4). Of 74 patients diagnosed with NERD, 67 had abnormal AFI findings (Table 2), giving this test a sensitivity of 90.5% (95%CI: 3847 April 14, 2016 Volume 22 Issue 14


162 Luo X et al. AFI distinguishes NERD from FH FH 11.9% A 31.0% 57.1% NERD ph/impedance test+ B ph//impedance test- and PPI+ ph//impedance test- and PPI- Figure 2 Categorization of patients by means of ph/impedance and proton-pump inhibitor test. PPI: Proton-pump inhibitor; FH: Functional heartburn; NERD: Non-erosive reflux disease. A Figure 4 Images in a patient with functional heartburn. A: A normal appearance of esophageal mucosa on WLI; B: A normal esophagus on AFI. AFI: Autofluorescence imaging; WLI: White light imaging. B Table 2 Results of autofluorescence imaging endoscopy in the differential diagnosis between non-erosive reflux disease and functional heartburn AFI NERD FH Total Positive Negative Total McNemar test, P = AFI: Autofluorescence imaging; NERD: Nonerosive reflux disease; FH: Functional heartburn. Figure 3 Images in a patient with non-erosive reflux disease. A: A normal appearance of esophageal mucosa on WLI; B: Longitudinal purple lines on AFI. AFI: Autofluorescence imaging; WLI: White light imaging. 81.5%-96.1%) and a specificity of 90.0% (95%CI: 55.5%-99.7%). Meanwhile, the accuracy, positive predictive value and negative predictive value of AFI in differentiating between NERD and FH were 90.5% (95%CI: 84.2%-96.8%), 98.5% (95%CI: 92.1%-99.9%) and 56.3% (95%CI: 30.0%-80.2%), respectively. DISCUSSION In the present study, patients with typical reflux symptoms were investigated using AFI endoscopy as well as 24-h ph and impedance tests. Our results showed that AFI was able to identify differences in endoscopic features between NERD and FH. Thus, AFI endoscopy may have potential in distinguishing between these two diseases. AFI, which was incorporated into a Tri-modal Imaging Endoscope system, has been increasingly used in the assessment of Barrett s esophagus [10-12] and the appearance of purple areas on a green background indicates the neoplastic changes that occur in Barrett s esophagus. Changes in coloration of the gastrointestinal tract revealed by AFI, however, do not represent 3848 April 14, 2016 Volume 22 Issue 14
163 Luo X et al. AFI distinguishes NERD from FH one type of neoplasia-specific manifestations, as AFI cannot identify the direct features of gastrointestinal neoplasms, such as loss of micro-architecture regularity and/or disruption of normal capillary patterns in the superficial layer of lesions. It was found that changes in tissue components, regardless of whether they are caused by neoplasia or inflammation, alter the density of autofluorescence emitted from lesions [13-15]. These findings suggest that AFI may also be useful to evaluate diseases caused by inflammation, such as esophagitis [5]. Differentiating NERD from FH remains challenging [8], as both disorders share similar clinical manifestations, such as reflux symptoms and normal esophageal appearance on traditional endoscopy. The responsiveness to PPI tests is diagnostic of GERD and excludes the possibility of FH, but the converse is not necessarily true because the response rate of NERD to PPI therapy was reported to be low, around 37%-73% [16-18]. These findings indicate that more than one quarter of patients with NERD are refractory to PPIs, making it difficult to distinguish between NERD and FH. Routine methods of evaluating patients with persistent reflux symptoms after PPI tests include esophagogastroduodenoscopy and esophageal ph monitoring. Various new techniques have been introduced, including esophageal histopathological analysis and esophageal impedance monitoring, in order to improve the clinical management of patients suspicious for NERD and FH. This study describes a new method using AFI to differentiate between NERD and FH. The presence of purple lines in the distal esophagus on AFI, which are indistinct on standard endoscopy, is considered diagnostic of GERD, including erosive esophagitis and NERD. Moreover, the endoscopic features identified by AFI were found to correlate with pathologic reflux [5]. GERD is characteristic of reflux from the stomach to the esophagus, but no reflux underlies FH. Therefore positive findings on AFI may help distinguish NERD from FH. Our results showed the diagnostic value of AFI in distinguishing between NERD and FH was promising, with a sensitivity of 90.5% and a specificity of 90%. These findings were comparable to results obtained with other new diagnostic modalities, such as identification of microscopic esophagitis and analysis of esophageal baseline impedance [19,20]. Microscopic esophagitis, which is considered a histological marker of both erosive esophagitis and NERD [21,22], can be observed in the distal esophagus of almost all patients with erosive esophagitis and in 70%-76% of those with NERD [21,23]. Recently, it was reported that histological evaluation of biopsy specimens from the distal esophagus of patients with reflux symptoms to show the presence or absence of microscopic esophagitis was capable of differentiating NERD from FH, with a sensitivity of 74% and an accuracy of 79% [19]. Also, change in baseline impedance was found to be a marker of pathological reflux, which can distinguish NERD from FH with a sensitivity of 78% and a specificity of 71% [20]. In addition, prolonged wireless esophageal ph monitoring was found to have a higher sensitivity in identifying NERD than 24-h ph monitoring. Nearly one-third of patients who fulfilled the Rome Ⅲ criteria for FH were found to have NERD after esophageal ph monitoring for > 48 h [24]. Although symptom-based approaches are favored in the initial diagnosis of GERD, endoscopic examination is always recommended for patients who do not respond to PPI tests, and patients suspicious for Barrett s esophagus [9,25]. AFI may improve the diagnostic yield of dysplasia or early stage malignancy in the esophagus. Recent studies showed both second and third generation AFI systems were more effective than first generation systems in detecting early neoplastic lesions [26-29]. Our findings suggest that, in addition to neoplastic disease, AFI may also be helpful in the diagnosis of NERD. Its advantages, including real-time evaluation and simple diagnostic criteria, imply that AFI may serve as a complementary method in differentiating NERD from FH. As stated above, other new diagnostic methods, such as prolonged wireless esophageal ph monitoring [24] and identification of microscopic esophagitis [22], may also be useful in distinguishing between NERD and FH. However, esophageal impedance and wireless ph monitoring cannot be performed simultaneously [24], reducing the ability to diagnose non-acid reflux [30]. In addition, microscopic esophagitis has shown limitations in identifying NERD, as nearly 20% of patients with NERD showed no evidence of microscopic esophagitis [22]. As none of the above diagnostic modalities is perfect, how to choose these methods is needed to be optimized for patients with suspicion of NERD or FH. One limitation of this study is the lack of esophageal biopsies. Microscopic esophagitis in the distal esophagus due to reflux may change tissue components, such as collagen and other fluorescent substances [31], attenuating AFI. However, we had no histopathological evidence to support this hypothesis, suggesting the need for further studies combining endoscopic and histopathological methods. Another limitation was that repeated AFI was not performed after PPI treatment in patients positive on AFI. It is unclear whether standard PPI treatment reverses abnormal findings on AFI. Previous data showed that treatment with omeprazole for 6 mo completely restored dilated intercellular spaces [32], which are considered characteristic of microscopic esophagitis in NERD [22]. It implied that positive AFI findings are likely to diminish after PPI therapy. Further studies are needed to clarify the duration of PPI treatment required to reverse positive AFI findings. In summary, this prospective observational study showed that endoscopic features on AFI can distinguish NERD from FH. Its real-time characteristics and simple endoscopic criteria may enhance the use of AFI as a complementary tool in the differentiation of NERD and FH April 14, 2016 Volume 22 Issue 14
164 Luo X et al. AFI distinguishes NERD from FH ACKNOWLEDGMENTS The authors would like to thank professor Enqiang Linghu, Wen Li, Ying-di Liu, Gang Sun and Qi-yang Huang for their support. We are also grateful to Jie Zhang, Xiao-xiao Wang, Jie Ai from GI Endoscopy Center and GI Motility Center for technical assistance. COMMENTS Background It is difficult to differentiate between functional heartburn (FH) and non-erosive reflux disease (NERD) endoscopically. Autofluorescence imaging (AFI) was recently shown to reveal indistinct mucosal lesions invisible on conventional endoscopy. Moreover, endoscopy with AFI was shown to predict acid reflux in patients with gastroesophageal reflux disease (GERD). NERD is characterized etiologically by the presence of pathologic reflux, while FH is not. This study aimed to assess whether AFI endoscopy could distinguish NERD from FH. Research frontiers Reflux symptoms are common in the general population. GERD (including NERD) and FH may underlie these symptoms. In order to differentiate NERD from FH, esophagogastroduodenoscopy, esophageal ph monitoring and protonpump inhibitor (PPI) test are often needed. Presently, various new techniques have been introduced, including esophageal histopathological analysis and esophageal impedance monitoring, in order to improve the clinical management of patients suspicious for NERD and FH. Innovations and breakthroughs To date, few efforts have been put on the application of AFI endoscopy in patients with GERD. In this pilot study, the authors found that endoscopic features on AFI can distinguish NERD from FH. Applications This study suggested that AFI may serve as a complementary tool in the differentiation of NERD from FH. It provided a new method to improve the clinical management of patients with reflux symptoms. Terminology AFI is a kind of digital imaging technique that detects autofluorescence that is emitted in response to light by endogenous fluorophores and cannot be observed by conventional endoscopy. NERD is a distinct pattern of GERD. It is caused by the reflux of gastric contents into the esophagus, but no mucosal damage is found at conventional endoscopy. FH is defined as retrosternal burning in the absence of GERD or other factors that can be detected in an objective manner. Peer-review The authors did an excellent job of assessing afi endoscopy for its utility in the evaluation of nerd vs fh. The flow diagram explaining patient recruitment and exclusions is extremely helpful and the color images are exceptionally well done, and very instructive. REFERENCES 1 Savarino E, Zentilin P, Savarino V. NERD: an umbrella term including heterogeneous subpopulations. Nat Rev Gastroenterol Hepatol 2013; 10: [PMID: DOI: / nrgastro ] 2 Savarino E, Marabotto E, Zentilin P, Frazzoni M, Sammito G, Bonfanti D, Sconfienza L, Assandri L, Gemignani L, Malesci A, Savarino V. The added value of impedance-ph monitoring to Rome III criteria in distinguishing functional heartburn from non-erosive reflux disease. Dig Liver Dis 2011; 43: [PMID: DOI: /j.dld ] 3 Song LM, Banerjee S, Desilets D, Diehl DL, Farraye FA, Kaul V, Kethu SR, Kwon RS, Mamula P, Pedrosa MC, Rodriguez SA, Tierney WM. Autofluorescence imaging. Gastrointest Endosc 2011; 73: [PMID: DOI: /j.gie ] 4 Uedo N, Iishi H, Tatsuta M, Yamada T, Ogiyama H, Imanaka K, Sugimoto N, Higashino K, Ishihara R, Narahara H, Ishiguro S. A novel videoendoscopy system by using autofluorescence and reflectance imaging for diagnosis of esophagogastric cancers. Gastrointest Endosc 2005; 62: [PMID: DOI: /j.gie ] 5 Wang W, Uedo N, Yang Y, Peng L, Bai D, Lu Z, Fan K, Wang J, Wang X, Zhao Y, Yu Z. Autofluorescence imaging endoscopy for predicting acid reflux in patients with gastroesophageal reflux disease. J Gastroenterol Hepatol 2014; 29: [PMID: DOI: /jgh.12566] 6 Weusten BL, Roelofs JM, Akkermans LM, Van Berge-Henegouwen GP, Smout AJ. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal ph data. Gastroenterology 1994; 107: [PMID: ] 7 Savarino E, Tutuian R, Zentilin P, Dulbecco P, Pohl D, Marabotto E, Parodi A, Sammito G, Gemignani L, Bodini G, Savarino V. Characteristics of reflux episodes and symptom association in patients with erosive esophagitis and nonerosive reflux disease: study using combined impedance-ph off therapy. Am J Gastroenterol 2010; 105: [PMID: DOI: / ajg ] 8 Galmiche JP, Clouse RE, Bálint A, Cook IJ, Kahrilas PJ, Paterson WG, Smout AJ. Functional esophageal disorders. Gastroenterology 2006; 130: [PMID: DOI: / j.gastro ] 9 Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013; 108: ; quiz 329 [PMID: DOI: /ajg ] 10 Kara MA, Peters FP, Ten Kate FJ, Van Deventer SJ, Fockens P, Bergman JJ. Endoscopic video autofluorescence imaging may improve the detection of early neoplasia in patients with Barrett s esophagus. Gastrointest Endosc 2005; 61: [PMID: DOI: /S (04) ] 11 Curvers WL, Alvarez Herrero L, Wallace MB, Wong Kee Song LM, Ragunath K, Wolfsen HC, Prasad GA, Wang KK, Subramanian V, Weusten BL, Ten Kate FJ, Bergman JJ. Endoscopic tri-modal imaging is more effective than standard endoscopy in identifying early-stage neoplasia in Barrett s esophagus. Gastroenterology 2010; 139: [PMID: DOI: /j.gastro ] 12 Curvers WL, Singh R, Song LM, Wolfsen HC, Ragunath K, Wang K, Wallace MB, Fockens P, Bergman JJ. Endoscopic tri-modal imaging for detection of early neoplasia in Barrett s oesophagus: a multi-centre feasibility study using high-resolution endoscopy, autofluorescence imaging and narrow band imaging incorporated in one endoscopy system. Gut 2008; 57: [PMID: DOI: /gut ] 13 van den Broek FJ, Fockens P, van Eeden S, Reitsma JB, Hardwick JC, Stokkers PC, Dekker E. Endoscopic tri-modal imaging for surveillance in ulcerative colitis: randomised comparison of highresolution endoscopy and autofluorescence imaging for neoplasia detection; and evaluation of narrow-band imaging for classification of lesions. Gut 2008; 57: [PMID: DOI: /gut ] 14 Moriichi K, Fujiya M, Ijiri M, Tanaka K, Sakatani A, Dokoshi T, Fujibayashi S, Ando K, Nomura Y, Ueno N, Kashima S, Gotoh T, Sasajima J, Inaba Y, Ito T, Tanabe H, Saitoh Y, Kohgo Y. Quantification of autofluorescence imaging can accurately and objectively assess the severity of ulcerative colitis. Int J Colorectal Dis 2015; 30: [PMID: DOI: / s ] 15 Osada T, Arakawa A, Sakamoto N, Ueyama H, Shibuya T, Ogihara T, Yao T, Watanabe S. Autofluorescence imaging endoscopy for identification and assessment of inflammatory ulcerative colitis April 14, 2016 Volume 22 Issue 14
165 Luo X et al. AFI distinguishes NERD from FH World J Gastroenterol 2011; 17: [PMID: DOI: /wjg.v17.i ] 16 Chey WD. Erosive esophagitis and NERD: Can we really classify patients with heartburn by endoscopic findings? Clin Gastroenterol Hepatol 2004; 2: [PMID: DOI: / S (04) ] 17 Dean BB, Gano AD, Knight K, Ofman JJ, Fass R. Effectiveness of proton pump inhibitors in nonerosive reflux disease. Clin Gastroenterol Hepatol 2004; 2: [PMID: DOI: /S (04) ] 18 Weijenborg PW, Cremonini F, Smout AJ, Bredenoord AJ. PPI therapy is equally effective in well-defined non-erosive reflux disease and in reflux esophagitis: a meta-analysis. Neurogastroenterol Motil 2012; 24: , e350 [PMID: DOI: /j x] 19 Savarino E, Zentilin P, Mastracci L, Dulbecco P, Marabotto E, Gemignani L, Bruzzone L, de Bortoli N, Frigo AC, Fiocca R, Savarino V. Microscopic esophagitis distinguishes patients with non-erosive reflux disease from those with functional heartburn. J Gastroenterol 2013; 48: [PMID: DOI: / s ] 20 Kandulski A, Weigt J, Caro C, Jechorek D, Wex T, Malfertheiner P. Esophageal intraluminal baseline impedance differentiates gastroesophageal reflux disease from functional heartburn. Clin Gastroenterol Hepatol 2015; 13: [PMID: DOI: /j.cgh ] 21 Zentilin P, Savarino V, Mastracci L, Spaggiari P, Dulbecco P, Ceppa P, Savarino E, Parodi A, Mansi C, Fiocca R. Reassessment of the diagnostic value of histology in patients with GERD, using multiple biopsy sites and an appropriate control group. Am J Gastroenterol 2005; 100: [PMID: DOI: /j x] 22 Fiocca R, Mastracci L, Riddell R, Takubo K, Vieth M, Yerian L, Sharma P, Fernström P, Ruth M. Development of consensus guidelines for the histologic recognition of microscopic esophagitis in patients with gastroesophageal reflux disease: the Esohisto project. Hum Pathol 2010; 41: [PMID: DOI: /j.humpath ] 23 Mastracci L, Spaggiari P, Grillo F, Zentilin P, Dulbecco P, Ceppa P, Baccini P, Mansi C, Savarino V, Fiocca R. Microscopic esophagitis in gastro-esophageal reflux disease: individual lesions, biopsy sampling, and clinical correlations. Virchows Arch 2009; 454: [PMID: DOI: /s ] 24 Penagini R, Sweis R, Mauro A, Domingues G, Vales A, Sifrim D. Inconsistency in the Diagnosis of Functional Heartburn: Usefulness of Prolonged Wireless ph Monitoring in Patients With Proton Pump Inhibitor Refractory Gastroesophageal Reflux Disease. J Neurogastroenterol Motil 2015; 21: [PMID: DOI: /jnm14075] 25 Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol 2006; 101: ; quiz 1943 [PMID: DOI: / j x] 26 Tamai N, Saito S, Aihara H, Kato T, Tajiri H. Evaluation of the effectiveness of color intensity analysis using a second-generation autofluorescence imaging system for diminutive colorectal polyp differentiation. Dig Endosc 2014; 26 Suppl 2: [PMID: DOI: /den.12246] 27 Tamai N, Takeuchi Y, Tajiri H. Second-generation autofluorescence imaging for colorectal neoplasia. Dig Endosc 2015; 27 Suppl 1: 46 [PMID: DOI: /den.12417] 28 Ide D, Tamai N, Inomata H, Ohya TR, Aihara H, Saito S, Kato T, Tajiri H. Visualization of colorectal neoplasia by a secondgeneration autofluorescence imaging system. Scand J Gastroenterol 2013; 48: [PMID: DOI: / ] 29 Boerwinkel DF, Holz JA, Aalders MC, Visser M, Meijer SL, Van Berge Henegouwen MI, Weusten BL, Bergman JJ. Thirdgeneration autofluorescence endoscopy for the detection of early neoplasia in Barrett s esophagus: a pilot study. Dis Esophagus 2014; 27: [PMID: DOI: /dote.12094] 30 Tutuian R, Vela MF, Shay SS, Castell DO. Multichannel intraluminal impedance in esophageal function testing and gastroesophageal reflux monitoring. J Clin Gastroenterol 2003; 37: [PMID: ] 31 Wang TD, Triadafilopoulos G. Autofluorescence imaging: have we finally seen the light? Gastrointest Endosc 2005; 61: [PMID: DOI: /S (05) ] 32 Calabrese C, Bortolotti M, Fabbri A, Areni A, Cenacchi G, Scialpi C, Miglioli M, Di Febo G. Reversibility of GERD ultrastructural alterations and relief of symptoms after omeprazole treatment. Am J Gastroenterol 2005; 100: [PMID: DOI: /j x] P- Reviewer: Dumitrascu DL, Parker W, Savarino E S- Editor: Gong ZM L- Editor: Wang TQ E- Editor: Ma S 3851 April 14, 2016 Volume 22 Issue 14
166 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. ORIGINAL ARTICLE Observational Study Integrin αvβ6 and matrix metalloproteinase 9 correlate with survival in gastric cancer Pei-Long Lian, Zhao Liu, Guang-Yun Yang, Rui Zhao, Zhao-Yang Zhang, Yue-Guang Chen, Zhuo-Nan Zhuang, Ke-Sen Xu Pei-Long Lian, Rui Zhao, Zhao-Yang Zhang, Yue-Guang Chen, Ke-Sen Xu, Department of Hepatobiliary Surgery, Qilu Hospital, Shandong University, Jinan , Shandong Province, China Zhao Liu, Department of Hepatobiliary and Pancreatic Surgery, Jinan Central Hospital Affiliated to Shandong University, Jinan , Shandong Province, China Guang-Yun Yang, Department of Hepatobiliary Surgery, Chinese People s Liberation Army General Hospital, Beijing , China Zhuo-Nan Zhuang, Department of General Surgery, Beijing Tsinghua Changgung Hospital Medical Center, Tsinghua University, Beijing , China Author contributions: Lian PL designed the research, drafted and revised the paper; Liu Z, Yang GY, Zhao R performed the research; Zhang ZY, Chen YG, Zhuang ZN searched the literature and analyzed the data; Xu KS revised the paper, approved the final version. Supported by China Postdoctoral Science Foundation funded Project, No and ; and the Natural Science Foundation of China, No Institutional review board statement: The study was reviewed and approved by QiLu Hospital Institutional Review Board. Informed consent statement: All study participants, or their legal guardian, provided informed written consent prior to study enrollment. Conflict-of-interest statement: We declare that there are no conflicts of interest to disclose. Data sharing statement: No additional data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Ke-Sen Xu, PhD, Professor, Department of Hepatobiliary Surgery, Qilu Hospital, Shandong University, 107 Wenhuaxi Road, Jinan , Shandong Province, China. xukesen0519@163.com Telephone: Fax: Received: December 6, 2015 Peer-review started: December 7, 2015 First decision: December 31, 2015 Revised: January 11, 2016 Accepted: February 20, 2016 Article in press: February 22, 2016 Published online: April 14, 2016 Abstract AIM: To investigate the expression of integrin αvβ6 and matrix metalloproteinase 9 (MMP-9), their association with prognostic factors and to assess their predictive role in gastric cancer patients. METHODS: Immunohistochemistry was used to determine the expressions of integrin αvβ6 and MMP-9 in 126 specimens from patients with primary gastric carcinoma. Associations between immunohistochemical staining and various clinic pathologic variables of tissue specimens were evaluated by the χ 2 test and Fisher s exact test. Expression correlation of αvβ6 and MMP-9 was assessed using bivariate correlation analysis. The patients were followed-up every 3 mo in the first two years and at least every 6 mo afterwards, with a median follow-up of 56 mo (ranging from 2 mo to 94 mo) April 14, 2016 Volume 22 Issue 14
167 Lian PL et al. Role of integrin αvβ6 and MMP-9 in GC patients Four different combinations of αvβ6 and MMP-9 levels (that is, both markers positive, both markers negative, αvβ6 positive with MMP-9 negative, and αvβ6 negative with MMP-9 positive) were evaluated for their relative effect on survival. The difference in survival curves was evaluated with a log-rank test. Survival analysis was conducted using the Kaplan-Meier survival and Cox proportional hazards model analysis. RESULTS: The expressions of integrin αvβ6 and MMP-9 were investigated in 126 cases, among which 34.92% were positive for αvβ6 expression, and 42.06% for MMP-9 expression. The expression of αvβ6 was associated with Lauren type, differentiation, N stage, and TNM stage (the P values were 0.006, 0.038, 0.016, and 0.002, respectively). While MMP-9 expression was associated with differentiation, T stage, N stage, and TNM stage (the P values were 0.039, 0.014, 0.033, and 0.008, respectively). The positive correlation between αvβ6 and MMP-9 in gastric cancer was confirmed by a correlation analysis. The Kaplan-Meier survival analysis showed that patients with expression of αvβ6 or MMP-9 alone died earlier than those with negative expression and that patients who were both αvβ6 and MMP-9 positive had a shorter overall survival than those with the opposite pattern (both αvβ6 and MMP-9 negative) (P = 0.000). A Cox model indicated that positive expression of αvβ6 and MMP-9, diffuse Lauren type, as well as a senior grade of N stage, M stage, and TNM stage were predictors of a poor prognosis in univariate analysis. Only αvβ6 and MMP-9 retained their significance when adjustments were made for other known prognostic factors in multivariate analysis (RR = 2.632, P = and RR = 1.813, P = 0.007). CONCLUSION: The expression of αvβ6 and MMP-9 are closely correlated, and the combinational pattern of αvβ6 and MMP-9 can serve as a more effective prognostic index for gastric cancer patients. Key words: Gastric cancer; Integrin αvβ6; Prognosis; Matrix metalloproteinase 9; Survival The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Both integrin αvβ6 and matrix metalloproteinase 9 (MMP-9) play an important role in the development and progression of cancer. However, the combined effect of the two proteins in gastric cancer is not yet clear. We would like to draw attention to this aspect. In the present study, we demonstrated that the expression of αvβ6 and MMP-9 are closely correlated, and the combinational pattern of αvβ6 and MMP-9 can serve as a more effective prognostic index for gastric cancer patients. Lian PL, Liu Z, Yang GY, Zhao R, Zhang ZY, Chen YG, Zhuang ZN, Xu KS. Integrin αvβ6 and matrix metalloproteinase 9 correlate with survival in gastric cancer. World J Gastroenterol 2016; 22(14): Available from: URL: wjgnet.com/ /full/v22/i14/3852.htm DOI: org/ /wjg.v22.i INTRODUCTION Gastric cancer is the fourth most common cancer world-wide and accounts for approximately cases annually, with more than half of these cases occurring in East Asia. Gastric cancer also ranks as the second leading cause of cancer-related death [1]. Clinical management of gastric cancer is, to some extent, based on the availability of markers that are predictive of prognosis and alterations commonly present in gastric cancer have the potential to serve such a purpose. Integrin αvβ6 is a member of the integrin family and is expressed in epithelial cells only, with fibronectin (FN) as its major ligand. The expression of αvβ6 is rare and can hardly be detected in normal epithelial cells [2], but increases substantially in response to injury and/ or inflammation and in epithelial tumors [3]. Previous studies have shown that the de novo expression of integrin αvβ6 is involved in the pathogenic processes of gastrointestinal malignancies, including cell adhesion, proliferation, apoptosis, and matrix metalloproteinase (MMPs) secretion [4-6]. Similar to the integrin family, members of the MMP family, including MMP-9, have been implicated in tumor invasion and metastasis, which are characterized by a zinc atom at the active site and classified according to homologies in sequence and substrate affinity [7]. MMP-9 has been confirmed to be associated with the malignant behavior of tumors or the eventual clinical outcome of patients afflicted with the disease and has a unique ability to degrade type Ⅳ collagen, which is a major component of the basement membrane [8]. Our prior research has suggested that αvβ6 integrin is an independent prognostic indicator of gastric cancer [9]. Since that initial report, limited work has been conducted to highlight the predictive value of αvβ6 in gastrointestinal cancers, until the research of Peng et al [10] on colorectal cancer. The fact that no index alone can be simply explicable in terms of its effect on cancer prognosis prompted us to focus on the combined analysis of both αvβ6 and MMP-9. In the present study, we undertook an immunohistochemical analysis of αvβ6 and MMP-9 expression in gastric cancer. Their correlation with clinical characteristics and prognosis was assessed to determine whether the combinational pattern of αvβ6 and MMP-9 expression could be used as a more effective prognostic index for gastric cancer patients after curative surgery. MATERIALS AND METHODS Antibodies and reagents The mouse monoclonal integrin αvβ6 antibody 6.2A1 (1:500, Biogen, Cambridge, MA, United States) [9] and 3853 April 14, 2016 Volume 22 Issue 14
168 Lian PL et al. Role of integrin αvβ6 and MMP-9 in GC patients rabbit polyclonal MMP-9 antibody ab38898 (1:100, Abcam, Cambridge, MA, United States) [11] were used for integrin αvβ6 and MMP-9 immunohistochemical staining, respectively. Specificity of the two staining patterns was confirmed by the use of irrelevant control antibodies. Immunohistochemistry Immunohistochemistry was performed on 5 micrometer sections of the formalin-fixed, paraffin-embedded routine sections, and tissue microarray (TMA) analysis using antibodies against αvβ6 (6.2A1) and MMP-9 (ab38898) was applied. The sections were deparaffinized and hydrated, and the heat induced epitope retrieval was performed with Borg decloaking high ph buffer in the Biocare decloaking chamber. Subsequently, endogenous peroxidase activity was blocked with 3% hydrogen peroxide, and then the slides were incubated first with an avidin-biotin kit, followed by incubations with the αvβ6 primary antibody (1:500) and the MMP-9 primary antibody (1:100) overnight at 4, streptavidin-horseradish peroxidase, and betazoid diaminobenzidine for color development. Negative controls were prepared by using the identical concentration of mouse immunoglobulin IgG1 (Dako). The next day, biotinylated anti-mouse IgG and anti-rabbit IgG (1:200) were applied to the slides, which were subsequently treated using horseradish peroxidase (HRP)-labelled streptoantibiotin (Dako) for 15 min. Finally, all the slides were counterstained with Dako hematoxylin, rinsed with water, and then dehydrated with alcohol and xylene, and cover-slipped. Appropriate controls were included. All incubations were conducted at room temperature. Assessment of α vβ 6 and MMP-9 scoring in the tissue sections Assessment of the two proteins staining was evaluated independently by two pathologists who were blinded to the patients clinical outcome. Disagreements were resolved by discussion in a meeting to obtain the final results. The staining stratification was established based on two scores: (1) the proportion score representing the fraction of positive staining cells (0, 0%; 1, < 20%; 2, 20%-50%; 3, 51%-75%; and 4, > 75%, respectively); and (2) the intensity of the staining (0, no staining; 1, weak staining, pale brown; 2, moderate staining, brown; and 3, strong staining, dark brown, respectively). Such assessment allows for a semi-quantitative estimate of the expression levels of protein in the tissue section. The two scores were added, and the final definition of every section was obtained. Finally, tumors with a final score of < 2 were designated as negative, and > 2 as positive, in both αvβ6 and MMP-9 expression. Patients and follow-up A series of consecutive specimens from tumors of 126 primary gastric cancer patients, with curative resection, were obtained from the Department of Pathology, Qilu Hospital, Shandong University (Jinan, China), from January 2007 to June 2010 and were formalin-fixed and paraffin-embedded. All of the specimens were procured before any adjuvant treatment and after the informed consent from the patients, with the approval of the Ethics Committee of Qilu Hospital. According to our protocol, all patients were followed up every 3 mo in the first two years and at least every 6 mo afterwards, until June 2015, with a median followup of 56 mo (ranging from 2 mo to 94 mo). They were examined by regular abdomen ultrasonography or computed tomography (CT), monitoring the relapse of the disease. Observations were censored at either the last follow-up date or the terminal date of the follow-up if death had not occurred. Statistical analysis Statistical analyses were performed with SPSS Associations between immunohistochemical staining and clinicopathologic variables of tissue specimens were evaluated by the χ 2 test and Fisher s exact test. Expression correlation of αvβ6 and MMP-9 was assessed using bivariate correlation analysis. The difference in survival curves was evaluated with a logrank test. Survival analysis was conducted using the Kaplan-Meier survival and Cox proportional hazards model analysis. A value of P < 0.05 was considered to be statistically significant. RESULTS Expression of α vβ 6 and MMP-9 and the association with clinical factors We characterized the expression of αvβ6 and MMP-9 by immunohistochemical staining in gastric cancer from 126 patients (Figure 1), aged from 27 to 81. Of these, 44 (34.92%) were positive for αvβ6 expression, with 82 (65.08%) being negative. For MMP-9, 53 (42.06%) patients were positive for expression, and 73 (57.93%) were negative. As in our clinical correlation studies, the immunohistochemical analysis was conducted without knowledge of any clinical information regarding prognostic outcome. Levels of the two proteins expression were compared with tumor characteristics and risk factors (Table 1). The following analysis showed that Lauren type, differentiation, N stage, and TNM stage were associated with αvβ6 expression (the P values were 0.006, 0.038, 0.016, and 0.002, respectively). Regarding MMP-9 expression, statistically significant differences existed in differentiation, T stage, N stage, and TNM stage (the P values were 0.039, 0.014, 0.033, and 0.008, respectively). No evidence of a significant association was observed between alteration of αvβ6 or MMP-9 expression and other characteristics or risk factors April 14, 2016 Volume 22 Issue 14
169 Lian PL et al. Role of integrin αvβ6 and MMP-9 in GC patients Table 1 Expression of integrin αvβ6 and MMP-9 and patient characteristics Characteristic No. αvβ6 P value MMP-9 P value Negative Positive Negative Positive Age (yr) < > Gender Male Female Location Upper Middle Lower Lauren type Intestinal Diffuse Differentiation Well Moderate Poor T stage T T T T N stage N N N N M stage M M TNM stage I II III IV MMP-9: Matrix metalloproteinase 9. Table 2 Expression correlation of integrin αvβ6 and MMP-9 αvβ6 expression MMP-9 expression Total Negative Positive Negative Positive Total MMP-9: Matrix metalloproteinase 9. Role of both α vβ 6 and MMP-9 in cancer-related survival The Kaplan-Meier plot (Figure 2A and B) showed that patients with positive αvβ6 expression had a much shorter survival time than the negative cases (P = 0.000), consistent with our previous study [9]. The same tendency was present in MMP-9 positive expression cases (P = 0.000). The expression of αvβ6 and MMP-9 were closely correlated in gastric cancers (r = 0.286, P = 0.001) (Table 2), which indicated that the combined analysis of the two proteins may be more helpful in predicting the survival for this disease. A striking stratification of mortality risk was observed when four different combinations of αvβ6 and MMP-9 levels (that is, both markers positive, both markers negative, αvβ6 positive with MMP-9 negative, and αvβ6 negative with MMP-9 positive) were evaluated for their relative effect on survival. Kaplan-Meier plots showed that patients who were both αvβ6 and MMP-9 positive died earlier (26.45 ± 5.54) than the other three groups (53.40 ± 5.90, ± 6.86, and ± 4.87, respectively; P = 0.000). The greatest difference in survival was found between patients with both markers being positive and those with the opposite pattern (both markers negative) (Figure 2C). Univariate and multivariate analysis for prognosis of patients with gastric cancer Sufficient clinical follow-up data were obtained from all 126 patients, allowing for evaluation of the association between protein alteration and prognostic outcome. Of these, 69 (54.8%) cases were confirmed as cancerrelated deaths within 5 years of prognosis and 57 (45.2%) were censored, as the follow-up survey was 3855 April 14, 2016 Volume 22 Issue 14

170 Lian PL et al. Role of integrin αvβ6 and MMP-9 in GC patients A B C D Figure 1 Comparison of immunohistochemical staining of αvβ6 and MMP-9 in the same gastric cancer specimen evaluated with formalin-fixed, paraffinembedded tissue (streptavidin-peroxidase method; original magnification 400). Positive αvβ6 expression was detected predominantly in the cell membrane, and matrix metalloproteinase 9 (MMP-9) mainly exhibited a cytoplasmic immunostaining in tumor cells. A: Positive αvβ6 expression; B: Negative αvβ6 expression; C: Positive MMP-9 expression; D: Negative MMP-9 expression. discontinued or patients were alive beyond 60 mo or died of reasons other than this disease. We estimated the relative risks (RR) (both univariate and multivariate) of dying and 95%CI, using the Cox proportional hazard model (Table 3). The Cox model indicated that positive expressions of αvβ6 and MMP-9, diffuse Lauren as well as high grades of N, M, and TNM stages were predictors of a poor prognosis in the univariate analysis. Then, the variables with statistical values of P < 0.05 were chosen for multivariate analysis, and only αvβ6 and MMP-9 retained their significance after adjustments for other known prognostic factors, which revealed that positive expression of αvβ6 and MMP-9 were unfavorable independent prognostic factors (P = and P = 0.007, respectively) and superior to all other known prognostic factors. DISCUSSION Molecular markers associated with distinct clinical outcomes have been identified in gastric cancer, laying the groundwork for improved clinical management through more personalized medicine. Despite improvements during the past years, the prognostic outcome of gastric cancer remains unsatisfactory. Molecular investigation of cancerous pathogenesis would contribute to the treatment of patients with gastric cancer [12], which suggests that the current molecular research is far from sufficient. Considerable evidence now exists that alteration in the expression of αvβ6 or MMP-9 may serve as an important pathogenic event for some human malignancies. We have previously shown that αvβ6 is an independent prognostic indicator in gastric cancer [9] and simultaneously extended its pathogenic role to mediating the potential for colon cancer cells to colonize in and metastasize to the liver [13]. When it came to MMP-9, a number of studies have been published on its prognostic value in human cancers. High expression of MMP-9 was found to be associated with lymph node metastasis and a higher tumor stage in breast cancer [14,15]. Moreover, MMP-9 is also implicated in the progression of esophageal squamous cell carcinoma [16]. Meanwhile, MMP-9 status represents a novel prognostic factor in evaluation of colorectal cancer [17], especially in combination with the membrane-anchored MMP regulator RECK [18]. As to the prognostic role of MMP-9 in gastric cancer, a consensus has not been reached in previous reports [19-23]. Given the variable natural history and heterogeneity of gastric cancer, conflicting studies published to date suffer from a similar problem: the interference from neoadjuvant chemotherapy, which was recently confirmed [24,25]. To exclude the possibility of chemotherapy interfering with the two proteins predictive role in gastric cancer, only patients who had not received neoadjuvant chemotherapy were enrolled April 14, 2016 Volume 22 Issue 14
171 Lian PL et al. Role of integrin αvβ6 and MMP-9 in GC patients A Table 3 Univariate and multivariate analyses comparing overall survival to prognostic factors in 126 gastric cancer patients Cumulative survival rate avb6 (-) (n = 82) avb6 (+) (n = 44) Factors Univariate analysis Multivariate analysis Relative risk (95%CI) Age (yr) < 60 1 > ( ) P value Relative risk (95%CI) P value B P = t/mo Gender Female 1 Male ( ) Location Upper 1 Middle/Lower ( ) Cumulative survival rate MMP-9 (-) (n = 73) MMP-9 (+) (n = 53) Lauren type Intestinal 1 Diffuse ( ) Differentiation Well 1 Moderate/Poor ( ) ( ) T stage T1 1 1 T ( ) ( ) P = N stage N0 1 1 C t/mo N ( ) ( ) M stage M0 1 1 M ( ) ( ) Cumulative survival rate avb6 (-)/MMP-9 (-) (n = 56) avb6 (+)/MMP-9 (-) (n = 17) avb6 (-)/MMP-9 (+) (n = 26) TNM stage I 1 1 II-IV ( ) < ( ) αvβ6 Negative 1 1 Positive ( ) < ( ) MMP-9 Negative P = avb6 (+)/MMP-9 (+) (n = 27) Positive ( ) ( ) t/mo MMP-9: Matrix metalloproteinase 9. Figure 2 Kaplan-Meier plots show the association of survival and expression of integrin αvβ6 and MMP-9 in all gastric cancer patients tested. A: Positive expression of αvβ6 was associated with decreased survival (P = 0.000); B: The same tendency was present in matrix metalloproteinase 9 (MMP-9) positive expression cases (P = 0.000); C: When αvβ6 and MMP-9 alterations were analyzed together, patients with both αvβ6 and MMP-9 positive expression experienced the highest mortality of the four groups (P = 0.000). In the present study, the expression of integrin αvβ6 and MMP-9 in 126 gastric cancer specimens was investigated, which showed a 34.92% incidence of αvβ6 expression, concordant with previously published positive rates of 36.7% in gastric cancer [9], as well as a 42.06% incidence of MMP-9 expression. Subsequently, a positive correlation between the two proteins was confirmed, and each of them was associated with a poor prognosis in gastric cancer. When comparing different combinational expression patterns in the Kaplan-Meier survival analysis, patients who were both αvβ6 and MMP-9 positive suffered a higher mortality rate than the other three expression states, especially in comparison to the opposite pattern. Furthermore, a Cox model indicated that positive expression of αvβ6 and MMP-9, diffuse Lauren type, as well as a higher grade of N, M, and TNM stage were 3857 April 14, 2016 Volume 22 Issue 14
172 Lian PL et al. Role of integrin αvβ6 and MMP-9 in GC patients predictors of a poor prognosis in univariate analysis. Only αvβ6 and MMP-9 retained their significance when adjustments were made for other known prognostic factors in multivariate analysis. Based on these data, we proposed that the concomitant expression of αvβ6 and MMP-9 in gastric cancer could serve as a more effective independent predictor to determine early relapse, metastases and prognosis in gastric cancer patients. As an exploratory attempt, this paper intends to provide some enlightenment for the clinical management of gastric cancer patients in the future. We have previously confirmed a direct linkage between ERK2 and the cytoplasmic domain of β6, as well as the binding domain for ERK2 within the cytoplasmic tail of the β6-integrin subunit [26,27], through which integrin αvβ6 transmitted a growth enhancing signal to cancer cells. Previous studies have shown that the expression of MMP-9 has a direct correlation to integrin αvβ6 [5,28]. Thus, a signaling pathway mediated by ERK2 between αvβ6 and MMP-9 was theoretically supposed to exist to play a key role in the biological behavior and/or clinical outcome of human gastric cancer. In summary, we concur with Zhang et al [22] that αvβ6 should be a focus of attention for diagnosis and therapy in human gastric cancers; our current findings extend this idea to the combination of αvβ6 and MMP-9. The expression of αvβ6 and MMP-9 are closely correlated, and the combinational pattern of αvβ6 and MMP-9 can serve as a more effective prognostic index for gastric cancer patients. However, further research is necessary to identify the signaling pathway between αvβ6 and MMP-9 as an important target for gastric cancer therapy. COMMENTS Background Both integrin αvβ6 and matrix metalloproteinase 9 (MMP-9) play an important role in the development and progression of cancer. However, the combined effect of the two proteins in gastric cancer is not yet clear. The fact that no index alone can be simply explicable in terms of its effect on cancer prognosis prompted us to focus on the combined analysis of both αvβ6 and MMP-9. Research frontiers The prior research by the authors suggested that αvβ6 integrin is an independent prognostic indicator of gastric cancer. Since that initial report, limited work has been conducted to highlight the predictive value of αvβ6 in gastrointestinal cancers, until the research of Peng et al on colorectal cancer. Innovations and breakthroughs The combinational pattern of αvβ6 and MMP-9 expression was demonstrated to be more effective than αvβ6 alone in prognosis of gastric cancer. Applications The combinational detection of αvβ6 and MMP-9 expression could be used as a more effective prognostic index for gastric cancer patients after curative surgery. Terminology Integrin αvβ6 is a member of the integrin family and is expressed in epithelial cells only, but increases substantially in response to injury and/or inflammation and in epithelial tumors. Peer-review In the present study, the authors undertook an immunohistochemical analysis of αvβ6 and MMP-9 expression in gastric cancer. The correlation with clinical characteristics and prognosis was assessed to determine whether the combinational pattern of αvβ6 and MMP-9 expression could be used as a more effective prognostic index for gastric cancer patients after curative surgery. Over all, this is an interesting manuscript about the expression of integrin αvβ6 and MMP-9 in gastric cancer patients. REFERENCES 1 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011; 61: [PMID: DOI: /caac.20107] 2 Breuss JM, Gillett N, Lu L, Sheppard D, Pytela R. Restricted distribution of integrin beta 6 mrna in primate epithelial tissues. J Histochem Cytochem 1993; 41: [PMID: DOI: / ] 3 Breuss JM, Gallo J, DeLisser HM, Klimanskaya IV, Folkesson HG, Pittet JF, Nishimura SL, Aldape K, Landers DV, Carpenter W. Expression of the beta 6 integrin subunit in development, neoplasia and tissue repair suggests a role in epithelial remodeling. J Cell Sci 1995; 108 (Pt 6): [PMID: ] 4 Niu J, Gu X, Turton J, Meldrum C, Howard EW, Agrez M. Integrinmediated signalling of gelatinase B secretion in colon cancer cells. Biochem Biophys Res Commun 1998; 249: [PMID: DOI: /bbrc ] 5 Agrez M, Gu X, Turton J, Meldrum C, Niu J, Antalis T, Howard EW. The alpha v beta 6 integrin induces gelatinase B secretion in colon cancer cells. Int J Cancer 1999; 81: [PMID: ] 6 Zhao R, Liu XQ, Wu XP, Liu YF, Zhang ZY, Yang GY, Guo S, Niu J, Wang JY, Xu KS. Vascular endothelial growth factor (VEGF) enhances gastric carcinoma invasiveness via integrin alpha(v)beta6. Cancer Lett 2010; 287: [PMID: DOI: / j.canlet ] 7 Nagase H, Woessner JF. Matrix metalloproteinases. J Biol Chem 1999; 274: [PMID: DOI: /jbc ] 8 Nelson AR, Fingleton B, Rothenberg ML, Matrisian LM. Matrix metalloproteinases: biologic activity and clinical implications. J Clin Oncol 2000; 18: [PMID: ] 9 Zhang ZY, Xu KS, Wang JS, Yang GY, Wang W, Wang JY, Niu WB, Liu EY, Mi YT, Niu J. Integrin alphanvbeta6 acts as a prognostic indicator in gastric carcinoma. Clin Oncol (R Coll Radiol) 2008; 20: [PMID: DOI: /j.clon ] 10 Peng C, Gao H, Niu Z, Wang B, Tan Z, Niu W, Liu E, Wang J, Sun J, Shahbaz M, Agrez M, Niu J. Integrin αvβ6 and transcriptional factor Ets-1 act as prognostic indicators in colorectal cancer. Cell Biosci 2014; 4: 53 [PMID: DOI: / ] 11 Li XS, Xu Q, Fu XY, Luo WS. ALDH1A1 overexpression is associated with the progression and prognosis in gastric cancer. BMC Cancer 2014; 14: 705 [PMID: DOI: / ] 12 Niu Z, Wang J, Muhammad S, Niu W, Liu E, Peng C, Liang B, Sun Q, Obo S, He Z, Liu S, Zou X, Niu J. Protein expression of eif4e and integrin αvβ6 in colon cancer can predict clinical significance, reveal their correlation and imply possible mechanism of interaction. Cell Biosci 2014; 4: 23 [PMID: DOI: / ] 13 Yang GY, Xu KS, Pan ZQ, Zhang ZY, Mi YT, Wang JS, Chen R, Niu J. Integrin alpha v beta 6 mediates the potential for colon cancer cells to colonize in and metastasize to the liver. Cancer Sci 2008; 99: [PMID: DOI: /j x] 14 Wu ZS, Wu Q, Yang JH, Wang HQ, Ding XD, Yang F, Xu XC. Prognostic significance of MMP-9 and TIMP-1 serum and tissue expression in breast cancer. Int J Cancer 2008; 122: [PMID: DOI: /ijc.23337] 15 Vizoso FJ, González LO, Corte MD, Rodríguez JC, Vázquez J, Lamelas ML, Junquera S, Merino AM, García-Muñiz JL. Study 3858 April 14, 2016 Volume 22 Issue 14

173 Lian PL et al. Role of integrin αvβ6 and MMP-9 in GC patients of matrix metalloproteinases and their inhibitors in breast cancer. Br J Cancer 2007; 96: [PMID: DOI: / sj.bjc ] 16 Yamamoto H, Vinitketkumnuen A, Adachi Y, Taniguchi H, Hirata T, Miyamoto N, Nosho K, Imsumran A, Fujita M, Hosokawa M, Hinoda Y, Imai K. Association of matrilysin-2 (MMP-26) expression with tumor progression and activation of MMP-9 in esophageal squamous cell carcinoma. Carcinogenesis 2004; 25: [PMID: DOI: /carcin/bgh270] 17 Cho YB, Lee WY, Song SY, Shin HJ, Yun SH, Chun HK. Matrix metalloproteinase-9 activity is associated with poor prognosis in T3-T4 node-negative colorectal cancer. Hum Pathol 2007; 38: [PMID: DOI: /j.humpath ] 18 Takeuchi T, Hisanaga M, Nagao M, Ikeda N, Fujii H, Koyama F, Mukogawa T, Matsumoto H, Kondo S, Takahashi C, Noda M, Nakajima Y. The membrane-anchored matrix metalloproteinase (MMP) regulator RECK in combination with MMP-9 serves as an informative prognostic indicator for colorectal cancer. Clin Cancer Res 2004; 10: [PMID: DOI: / CCR ] 19 Fanelli MF, Chinen LT, Begnami MD, Costa WL, Fregnami JH, Soares FA, Montagnini AL. The influence of transforming growth factor-α, cyclooxygenase-2, matrix metalloproteinase (MMP)-7, MMP-9 and CXCR4 proteins involved in epithelial-mesenchymal transition on overall survival of patients with gastric cancer. Histopathology 2012; 61: [PMID: DOI: / j x] 20 Sun WH, Sun YL, Fang RN, Shao Y, Xu HC, Xue QP, Ding GX, Cheng YL. Expression of cyclooxygenase-2 and matrix metalloproteinase-9 in gastric carcinoma and its correlation with angiogenesis. Jpn J Clin Oncol 2005; 35: [PMID: DOI: /jjco/hyi196] 21 Chu D, Zhang Z, Li Y, Zheng J, Dong G, Wang W, Ji G. Matrix metalloproteinase-9 is associated with disease-free survival and overall survival in patients with gastric cancer. Int J Cancer 2011; 129: [PMID: DOI: /ijc.25734] 22 Zhang S, Li L, Lin JY, Lin H. Imbalance between expression of matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 in invasiveness and metastasis of human gastric carcinoma. World J Gastroenterol 2003; 9: [PMID: DOI: / wjg.v9.i5.899] 23 Mrena J, Wiksten JP, Nordling S, Kokkola A, Ristimäki A, Haglund C. MMP-2 but not MMP-9 associated with COX-2 and survival in gastric cancer. J Clin Pathol 2006; 59: [PMID: DOI: /jcp ] 24 Manu KA, Shanmugam MK, Ramachandran L, Li F, Fong CW, Kumar AP, Tan P, Sethi G. First evidence that γ-tocotrienol inhibits the growth of human gastric cancer and chemosensitizes it to capecitabine in a xenograft mouse model through the modulation of NF-κB pathway. Clin Cancer Res 2012; 18: [PMID: DOI: / CCR ] 25 Liu S, Wang J, Niu W, Liu E, Wang J, Peng C, Lin P, Wang B, Khan AQ, Gao H, Liang B, Shahbaz M, Niu J. The β6-integrin-erk/map kinase pathway contributes to chemo resistance in colon cancer. Cancer Lett 2013; 328: [PMID: DOI: / j.canlet ] 26 Ahmed N, Niu J, Dorahy DJ, Gu X, Andrews S, Meldrum CJ, Scott RJ, Baker MS, Macreadie IG, Agrez MV. Direct integrin alphavbeta6-erk binding: implications for tumour growth. Oncogene 2002; 21: [PMID: DOI: /sj/onc/ ] 27 Wang B, Wang W, Niu W, Liu E, Liu X, Wang J, Peng C, Liu S, Xu L, Wang L, Niu J. SDF-1/CXCR4 axis promotes directional migration of colorectal cancer cells through upregulation of integrin αvβ6. Carcinogenesis 2014; 35: [PMID: DOI: / carcin/bgt331] 28 Scott KA, Arnott CH, Robinson SC, Moore RJ, Thompson RG, Marshall JF, Balkwill FR. TNF-alpha regulates epithelial expression of MMP-9 and integrin alphavbeta6 during tumour promotion. A role for TNF-alpha in keratinocyte migration? Oncogene 2004; 23: [PMID: DOI: /sj.onc ] P- Reviewer: Azoulay L, Sharma P, Zea N S- Editor: Yu J L- Editor: A E- Editor: Wang CH 3859 April 14, 2016 Volume 22 Issue 14
174 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. Prospective Study ORIGINAL ARTICLE Cost-effectiveness of Crohn s disease post-operative care Emily K Wright, Michael A Kamm, Peter Dr Cruz, Amy L Hamilton, Kathryn J Ritchie, Sally J Bell, Steven J Brown, William R Connell, Paul V Desmond, Danny Liew Emily K Wright, Michael A Kamm, Peter Dr Cruz, Amy L Hamilton, Kathryn J Ritchie, Sally J Bell, Steven J Brown, William R Connell, Paul V Desmond, Department of Gastroenterology, St Vincent s Hospital, University of Melbourne, Fitzroy VIC 3065, Melbourne, Australia Michael A Kamm, Imperial College, London SW7 2AZ, United Kingdom Danny Liew, Melbourne EpiCentre, University of Melbourne and Melbourne Health, Parkville VIC 3010, Melbourne, Australia Author contributions: Wright EK, Kamm MA and DeCruz P study concept and design; acquisition of data, analysis, data interpretation; drafting of the manuscript, critical revision of the manuscript for important intellectual content, statistical analysis; Hamilton AL acquisition of data, analysis and interpretation of data, drafting of the manuscript; Ritchie K acquisition and monitoring of data; Liew D analysis and interpretation of data, drafting of the manuscript; statistical analysis; Bell SJ, Brown SJ, Connell WR and Desmond PV acquisition of data and critical review of manuscript. Institutional review board statement: This study is a sub study of the Post-Operative Crohn s Endoscopic Recurrence (POCER) study which was approved by the Human Research Ethics Committee of St Vincent s Hospital Research Governance Unit (HREC-A 077/09). Clinical trial registration statement: This study is a sub study of the Post-Operative Endoscopic Recurrence (POCER) study which was registered and approved at Clinicaltrial.gov. Number NCT Informed consent statement: All study participants provided informed written consent prior to study enrolment. Conflict-of-interest statement: No potential conflicts of interest relevant to this article were reported. Data sharing statement: No additional data are available. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Michael A Kamm, Professor, Department of Gastroenterology, St Vincent s Hospital, University of Melbourne, Victoria Parade, Fitzroy VIC 3065, Melbourne, Australia. mkamm@unimelb.edu.au Telephone: Fax: Received: November 15, 2015 Peer-review started: November 16, 2015 First decision: December 11, 2015 Revised: December 22, 2015 Accepted: January 30, 2016 Article in press: January 31, 2016 Published online: April 14, 2016 Abstract AIM: To define the cost-effectiveness of strategies, including endoscopy and immunosuppression, to prevent endoscopic recurrence of Crohn s disease following intestinal resection. METHODS: In the POCER study patients undergoing intestinal resection were treated with post-operative drug therapy. Two thirds were randomized to active care (6 mo colonoscopy and drug intensification for endoscopic recurrence) and one third to drug therapy without early endoscopy. Colonoscopy at 18 mo and faecal calprotectin (FC) measurement were used to assess disease recurrence. Administrative data, chart review and patient questionnaires were collected prospectively over 18 mo. RESULTS: Sixty patients (active care n = 43, standard 3860 April 14, 2016 Volume 22 Issue 14
175 Wright EK et al. CD post-operative care care n = 17) were included from one health service. Median total health care cost was $6440 per patient. Active care cost $4824 more than standard care over 18 mo. Medication accounted for 78% of total cost, of which 90% was for adalimumab. Median health care cost was higher for those with endoscopic recurrence compared to those in remission [$26347 (IQR ) vs $2729 (IQR ), P < 0.001]. FC to select patients for colonoscopy could reduce cost by $1010 per patient over 18 mo. Active care was associated with 18% decreased endoscopic recurrence, costing $861 for each recurrence prevented. CONCLUSION: Post-operative management strategies are associated with high cost, primarily medication related. Calprotectin use reduces costs. The long term cost-benefit of these strategies remains to be evaluated. Key words: Crohn s disease; Post-operative; Health economics; Health care cost; Biologics The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: The health care costs of a proactive diseaseprevention post-operative Crohn s disease strategy are substantial. Much of this cost relates to drug therapy (biologics). Active care involving endoscopic monitoring for disease recurrence, costs more than symptombased monitoring. The occurrence of endoscopic recurrence increases costs significantly, related largely to drug therapy. Faecal calprotectin to monitor for disease recurrence can substantially decrease postoperative costs. Wright EK, Kamm MA, Dr Cruz P, Hamilton AL, Ritchie KJ, Bell SJ, Brown SJ, Connell WR, Desmond PV, Liew D. Costeffectiveness of Crohn s disease post-operative care. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Crohn s disease is a chronic, relapsing, progressive inflammatory disorder of the gastrointestinal tract. Annual direct medical costs are high, estimated at $4466 US dollars per patient per year [1], and exceed those required for the care of patients with ulcerative colitis. Costs are higher among those with active, severe, stricturing and/or penetrating disease and those requiring hospitalization, surgery, or therapy with glucocorticoids, immunosuppressives or biologic therapy [1-7]. Seventy percent of patients with Crohn s disease need an intestinal resection at some time [8-11]. Within one year of surgery, subclinical endoscopic recurrence occurs at the anastomosis in 90% of patients, symp- tomatic clinical recurrence occurs in 30%, and 5% of patients undergo further surgical intervention [12-14]. Seventy percent of patients who have had an operation will ultimately require further surgery [8,15]. Treatment with thiopurines and/or anti-tumor necrosis factor (TNF) agents has been associated with a reduction in endoscopic recurrence [16-19]. Thiopurines are associated with significant cost savings when used for the treatment of inflammatory bowel disease, especially when used with pharmacogenetic testing of thiopurine s-methyltransferase and metabolite monitoring [20,21]. Anti-TNF drugs in Crohn s disease are clinically effective [22,23]. But their cost-effectiveness has not been established with certainty. These agents reduce the costly complications of Crohn s disease such as surgery and hospitalization, especially in the short term [24] and appear to be cost-effective when disease is severe or active [25-27]. However, the cost-effectiveness of long term maintenance treatment with infliximab or adalimumab is not known [25,28] although costs with adalimumab are less than those associated with infliximab therapy largely because of reduced infusion centre costs [29]. When considering the cost-effectiveness of drug strategies for the prevention of post-operative clinical recurrence, Ananthakrishnan et al [30] found that antibiotics were the most cost-effective option. They found that immediate therapy with infliximab postoperatively was not cost-effective, even in patients at high risk of early recurrence, although could be costeffective if reserved for patients with early endoscopic recurrence at 6 mo. Doherty and colleagues [31] found that compared to no prophylactic treatment, prophylactic post-operative thiopurine therapy was the most cost-effective up to 1 year post-operatively, but at 5 years, mesalazine treatment was most favourable. However, endoscopic recurrence was not a factor in the primary model of these studies. While these studies have examined the costeffectiveness of prophylactic drug treatments postoperatively, there has been no detailed analysis to date of the cost-effectiveness of management strategies following intestinal resection, which include early endoscopic assessment, tailored drug therapy according to risk of recurrence, and the presence or absence of early endoscopic recurrence. The Post-Operative Crohn s Endoscopic Recurrence (POCER) study compared strategies to prevent endoscopic recurrence, taking into account risk of recurrence, efficacy of different drug regimens, and assessment of the benefit of endoscopic monitoring and treatment intensification providing a strategy for management of Crohn s disease after intestinal resection [17]. This study also evaluated the efficacy of faecal calprotectin testing to detect early recurrent disease [32]. In a subset of patients from the POCER study, we aimed to undertake a detailed health care utilization and cost analysis to estimate health care costs associated with post-operative Crohn s disease 3861 April 14, 2016 Volume 22 Issue 14
176 Wright EK et al. CD post-operative care care and to estimate the cost-effectiveness of one management strategy over another. MATERIALS AND METHODS Clinical post-operative recurrence study The POCER study [1] was a prospective randomized control trial which assessed the efficacy of postoperative endoscopic assessment and treatment step-up for early mucosal recurrence. Patients were stratified according to risk of recurrence. Smokers, patients with perforating disease, or patients with 1 previous resections were classified as high-risk ; all others low-risk. All patients underwent resection of all macroscopic disease and then received 3 mo of metronidazole. High-risk patients also received daily azathioprine (2 mg/kg per day) or 6-mercaptopurine (1.5 mg/kg per day). High-risk patients intolerant of thiopurine received adalimumab induction (160 mg/80 mg) and then 40 mg two-weekly. Low-risk patients received no further medication. Patients were randomly assigned in a 2:1 ratio to colonoscopy at 6 mo (active care) or no colonoscopy (standard care). For endoscopic recurrence (Rutgeerts score i2) at 6 mo, patients stepped-up to thiopurine, fortnightly adalimumab with thiopurine, or weekly adalimumab. The primary end-point was endoscopic recurrence at 18 mo. Endoscopic remission was defined as Rutgeert s score i0 or i1 (i0 = no lesions, i1 = mild small superficial anastomotic lesions), and recurrence defined as i2, i3 or i4 (moderate to severe lesions). One hundred and seventy four patients were included at 17 hospitals in Australia and New Zealand. One hundred and one of 122 patients randomized to endoscopic intervention (6 mo colonoscopy) were highrisk, compared to 44 of 56 in the standard care arm (Figure 1). Key findings from the POCER study were: (1) treatment according to clinical risk of recurrence, with early colonoscopy and treatment step-up for recurrence, was better than conventional drug therapy alone for prevention of postoperative Crohn's disease recurrence; and (2) selective immune suppression, adjusted for early recurrence, rather than routine use, led to disease control in most patients. The study showed that while clinical risk factors, including smoking, could predict recurrence, patients at low risk of recurrence also benefited from monitoring and that early remission did not preclude the need for ongoing monitoring. The present study comprised the subset of 60 patients from the POCER study with complete health care utilization and costing data, and complete postoperative follow-up for 6 mo or more. These patients post-operative care had been undertaken in one health service, St Vincent s Hospital Melbourne (SVHM), ensuring complete and consistent data capture. A minimum of 6 mo follow-up was chosen for patient inclusion, as this was the first endoscopic assessment point for patients in the study. Endoscopic visual assessment for disease recurrence At ileo-colonoscopy, mucosal recurrence at the anastomosis and neo-terminal ileum was assessed according to the Rutgeerts score [13] by the endoscopist, who was aware of the patient s treatment. At the 6 and 18 mo colonoscopies, endoscopic remission was defined as Rutgeerts score i0 (no lesions) or i1 ( 5 aphthous lesions) and recurrence as i2 (> 5 aphthous lesions or larger lesions confined to anastomosis), i3 (diffuse ileitis), or i4 (diffuse inflammation with large ulcers and/or narrowing) [13]. Health economic assessment Patients completed health care utilization and work productivity questionnaires pre-operatively (baseline) and at 1, 2, 4, 6, 7, 8, 10, 12, 15 and 18 mo postoperatively. The data extracted is shown in Table 1. Costs were stratified into the following categories: all drugs, adalimumab, inpatient care, in-hospital procedures (colonoscopy and iron infusion), emergency department attendances, specialist outpatient visits, outpatient allied health visits, primary care visits, outpatient medical imaging and pathology investigations. Hospital cost data were derived from administrative databases maintained by the Clinical Costing Unit at SVHM, which routinely tracks all services provided to individual inpatients and assigns relevant service costs. Services comprise specific individualized items such as medical imaging, pharmacy, pathology, and surgical procedures, including operating room time, as well as more general care, such as time spent as an in-patient and consultation by medical, nursing, and allied health staff. This method of costing is known as the bottomup approach [33]. Outpatient health care resource costs were estimated by multiplying episodes of care by unit costs. Episodes of care were derived from questionnaire data. Unit costs for medications and medical services were based on the Australian Medical Services Schedule [34] and Pharmaceutical Benefits Schedule [35] respectively. All costs were from the perspective of the Australian public healthcare system, which funds the majority of healthcare in Australia. Therefore, cost estimates excluded any patient contribution. All cost data were considered in Australian dollars (AUD). Faecal calprotectin measurement Faecal calprotectin (FC) was measured by a quantitative enzyme immunoassay (fcal TM, Bühlmann, Schonenbuch, Switzerland) as per manufacturer s instructions, without knowledge of patient data. Concentrations were expressed as μg/g of stool. FC measurement was performed at baseline (pre-operatively) and at 6, April 14, 2016 Volume 22 Issue 14
177 Wright EK et al. CD post-operative care Patients Screened and Consented n = 212 Surgery Ineligible after surgery n = 28 Stratification n = 184 High risk n = 153 One or more of: Previous surgery Penetrating disease Smoker Low risk n = 31 No risk factors Randomization n = 184 Did not receive allocated treatment n = 6 Active care n = 128 Standard care n = 56 Did not receive allocated treatment n = 4 High risk n = 101 Low risk n = 21 High risk n = 44 High risk n = 8 Withdrew prior to 6 mo n = Administrative reasons 6 Symptom recurrence 2 Comorbidity Colonoscopy at 6 mo n = 104 Withdrew between 0 and 18 mo n = 19 9 Symptom recurrence 5 Comorbidity 5 Administrative reasons Rutgeerts score i0 or i1 No change in therapy Rutgeerts score i2-i4 Step-up therapy Withdrew between 6 and 18 mo n = 19 8 Administrative reasons 7 Symptom recurrence 4 Comorbidity Primary endpoint Colonoscopy at 18 mo n = 118 Figure 1 Consort diagram: The POCER Study April 14, 2016 Volume 22 Issue 14
178 Wright EK et al. CD post-operative care Table 1 Health care utilization data extracted for health economic assessment Health care utilization data extracted for health economic assessment Number and type of consultations with gastroenterologists or other medical specialists for reasons related to Crohn s disease. Visits to primary care providers (general practitioners). Visits to allied health care providers Investigations related to Crohn s disease Visits to the emergency department Hospital admissions < 1 d (day procedures) Hospital admission 1 d Current prescription medicine use related to Crohn s disease and 18 mo post-operatively. Statistical analysis As costs were not normally distributed, medians and interquartile ranges of costs were calculated. A 2-tailed Mann-Whitney U Test was used to assess for statistically significant differences in costs between groups. Data were analysed using SPSS Statistics for Windows, Version 22.0 (Armonk NY: IBM Corp.). RESULTS Of the 174 patients (median age 38, 55% female) enrolled in the POCER study, 60 (median age 37, 60% female) were included in this analysis. Demographic and disease characteristics of the entire POCER cohort and the health-economic sub-cohort are shown in Table 2. Of the 60 patients, 43 (72%) were in the active care arm and 17 (28%) in the standard care arm. Average length of follow up for all patients was 17 mo, and was not different between standard and active care arms. Cost of post-operative care Median total healthcare cost per patient of post-operative care was AUD $6440 (IQR ). Medications were the highest single cost driver, responsible for 78% of the total cost, of which adalimumab constituted 90%. Day procedures (colonoscopy) constituted 10% of the healthcare cost, followed by inpatient admissions, outpatient specialist consultations and pathology at 6%, 2% and 2%, respectively. Detailed cost breakdowns can be seen in Figure 2. We have previously shown that by measuring FC post-operatively, the need for colonoscopy can be reduced by 47%. When used at 6 and 18 mo to select appropriate patients for colonoscopy, this would have reduced the cost of post-operative care by $1010 over 18 mo based on average colonoscopy costs from our cohort. Active vs standard care arms Median healthcare cost was non-statistically significantly higher in the active vs standard care arms [$8045 (IQR Table 2 Demographics n (%) Health economic sub-group Entire POCER study cohort n = 60 n = 174 P value n (male) 24 (40) 78 (45) Age > 40 yr 24 (40) 68 (39) Age, median Age at diagnosis 16 yr 4 (7) 19 (11) yr 49 (81) 134 (77) > 40 yr 7 (12) 21 (12) Duration of Crohn's disease 29 (48) 60 (34) yr Disease location at surgery: Ileum only (L1) 33 (55) 95 (55) Colon only (L2) 3 (5) 11 (6) Ileum and colon (L3) 21 (35) 68 (39) Disease phenotype at surgery: B1 (Inflammatory) 5 (8) 17 (10) B2 (Stricture) 18 (30) 62 (36) B3 (Penetrating) 37 (62) 95 (55) Indication for surgery: Failure of drug therapy 12 (20) 38 (22) Obstruction 14 (23) 50 (29) Perforation 34 (57) 86 (49) Number of prior surgical resections 0 47 (78) 124 (71) (15) 33 (19) (2) 9 (5) or more 3 (5) 8 (5) Active smoker 22 (37) 54 (31) Immediate post-operative baseline drug therapy Metronidazole alone 9 (15) 29 (17) Thiopurine 39 (65) 101 (58) Adalimumab 12 (20) 44 (25) CDAI > (67) 113 (65) CDAI > (50) 90 (52) ) vs $3221 (IQR ), P = 0.125], Figure 3A. Medications were the biggest cost items in both the active and standard care arms (both 78% of total), with adalimumab making up 90% of these costs in both arms. Median medication costs per patient were non-statistically significantly higher in those in the active vs standard care arm [$3286 (IQR ) vs $891 (IQR ), P = 0.80]. As colonoscopy at 6 mo was mandated for those in the active care arm, median day procedure (colonoscopy) costs were higher per patient in this group when compared to those in the standard care arm $1710 (IQR ) vs $694 ( ), P = Detailed costing breakdowns are shown in Figure 2. Cost of endoscopic recurrence Within the 43 active care patients, the median healthcare cost was higher in those who had endoscopic recurrence at 6 mo (n = 12) compared to those in remission (n = 31) [$26347 (IQR ) vs $2729 (IQR ), P < 0.001], Figure 3C. Most of this cost difference was accounted for by the increased need for medications among those with endoscopic 3864 April 14, 2016 Volume 22 Issue 14
179 Wright EK et al. CD post-operative care recurrence [$24038 (IQR ) vs $533 (IQR ), P < 0.001]. Medications contribute more to the total healthcare cost of patients with endoscopic recurrence compared to those in remission (95% vs 67%). In the entire POCER study, treatment in the active care compared to standard care arms was associated with an 18% reduction in the risk of endoscopic recurrence (NNT 5.6) [17]. Hence on average, $861 was spent over 18 mo to prevent each endoscopic recurrence. Cost-effectiveness of faecal calprotectin to identify suitability for colonoscopy We have previously shown that routine FC testing for asymptomatic patients post-operatively, with colonoscopy reserved for those with a FC > 100 µg/g, could reduce the rate of post-operative colonoscopy by 47% [32]. When used at 6 and 18 mo to select patients for colonoscopy, measurement of FC would have reduced the cost of post-operative care by $1010 over 18 mo based on average colonoscopy costs from our cohort and the cost of FC testing. DISCUSSION Medication Inpatient admission Day procedure (Colonoscopy) Emergency department Outpatient specialist Outpatient allied health Primary care Medical imaging Pathology Figure 2 Distribution of costs in post-operative Crohn s disease in this cohort. This cost analysis of structured post-operative care after intestinal resection in Crohn s disease has identified a number of findings. First, healthcare costs are substantial, with much of the cost relating to drug therapy. Secondly, active care involving endoscopic monitoring for disease recurrence, costs more than symptom-based monitoring. Thirdly, the occurrence of endoscopic recurrence increases costs significantly, related largely to drug therapy. Lastly, the use of FC to monitor for disease recurrence, a proven strategy, can substantially decrease post-operative costs. The severity of endoscopic recurrence has been shown previously to predict the subsequent development of clinical recurrence and the need for surgery [14]. The costs inherent in this strategy of monitoring and treating-to-target to maintain mucosal healing are predicated on the assumption that in the longer A B Cost per patient (1000 AUD) Total medication cost per patient (1000 AUD) C Cost per Patient (1000 AUD) Standard care Standard care Endoscopic remission P = Randomisation arm P = 0.80 Randomisation arm P < Active care Active care Endoscopic recurrence Post operative disease behaviour Figure 3 Active vs standard care arms. Total cost of care (A) and medication cost (B) in post-operative Crohn s disease in the standard versus active care arms. Total cost of care over twelve months for patients with endoscopic remission versus recurrence (C). Boxes indicate the median and 25 th and 75 th percentiles, whiskers indicate calculated maximum and minimum with circles indicating outliers. term, disease recurrence, the development of disease complications, and the need for further surgery are reduced. Potential cost savings by way of a reduction in future surgery and a reduction in the subsequent development of short gut syndrome (a rare but catastrophic complication of repeated intestinal resections 3865 April 14, 2016 Volume 22 Issue 14
180 Wright EK et al. CD post-operative care in Crohn s disease) are significant. In the POCER cohort, the median cost of the inpatient admission for intestinal resection was $15662 (IQR ), the annual cost of care per patients with short gut syndrome have been estimated as being between $ and $ per year [36]. However, longer term data are still needed to evaluate the cost of prolonged anti-tnf therapy and reduced interventions compared with less monitoring and drug therapy with a likely increased rate of intervention. While recent trials have demonstrated the efficacy [16,18,37], and explored the cost-effectiveness [30,31], of some drug therapies in preventing post-operative Crohn s disease recurrence, the cost of anti-tnf therapy and of an integrated package of care have not been evaluated. The healthcare costs of these resource-intensive strategies must be considered if these approaches are to be widely recommended. To our knowledge, this is the first study to describe healthcare cost profiles in the management of postoperative Crohn s disease. The post-operative period is completely different to treating known active disease outside of a surgical episode, the latter being clinically obvious and treatment essential. Post-operatively, patients are usually clinically well, as reflected in improved Crohn s Disease Severity Index (CDAI) and quality of life scores [38]. For the patient and the treating physician, this changed focus from treating active disease to disease prevention requires its own health and cost-benefit analysis and justification. The major limitation of this study is the small study size which included a sub-set of patients enrolled in the POCER study. The POCER study demonstrated the efficacy of risktailored prophylactic drug therapy, early colonoscopy and treatment step-up in the event of endoscopic recurrence, for the prevention of post-operative recurrence [17]. The active care arm of the POCER study cost a median of $8045 per patient, with the cost of drug therapy exceeding the cost of colonoscopy, hospital admissions and specialist appointments. An alternative strategy involves the routine use of anti- TNF therapy for all patients at high-risk of recurrence, without inherent monitoring for recurrence and drug adjustment; the recent PREVENT study evaluated the efficacy of infliximab in this setting [39]. Such routine use of anti-tnf therapy would be more expensive in the short-term, but the longer term costs-benefits are unknown. The significant proportion of healthcare costs attributable to adalimumab therapy in our study reflects recent studies that illustrate the change in cost profiles in inflammatory bowel disease management as a consequence of anti-tnf use. Anti-TNF drugs come at a considerable cost and have been found to increase the overall cost for patients with Crohn s disease. Adalimumab is more cost-effective than infliximab because of the absence of incidental costs associated with the administration of infliximab including infusion centre admission and nursing care [40-42]. A recent cost-of-illness study by van der Valk et al [6] demonstrated that the cost of anti-tnf therapy for treatment of inflammatory bowel disease makes up the majority of health care cost, in excess of surgery and hospitalisation. Among Crohn s disease patients in that study, medication costs accounted for 71% of total healthcare costs, of which 64% was related to anti- TNF therapy. Hospitalisation and surgery accounted for only 19% and less than 1%, respectively. In our study, similar to the study by van der Valk et al [6], outpatient specialist and general practitioner care accounted for small proportions of the total healthcare cost, at 3.7% and less than 1%, respectively. Australian data reflects similar trends in healthcare costs, with medications being the main cost driver in the care of patients with Crohn s disease [43]. The introduction of biosimilar anti-tnf drugs, and a general trend towards lower drug pricing, may result in lower drug costs in the medium term [44]. Healthcare spending on biologics is predicted to fall between 10 and 50% in Europe and the United States following the introduction of biosimilar drugs [45-47]. Cost-effectiveness of the tested strategy may therefore change. This study has identified the main costs associated with a proactive disease-prevention post-operative Crohn s disease strategy. It provides the financial basis for current management and the planning of future strategies. ACKNOWLEDGMENTS Maura McSweeney, Clinical Costing Analyst, Decisions Support Unit, St Vincent s Public Hospital Melbourne. AbbVie, Gutsy Group, Gandel Philanthropy, Angior Foundation and Crohn s Colitis Australia and The National Health and Medical Research Council provided research support. COMMENTS Background Healthcare costs for Crohn s disease are high. Active disease, surgery, hospitalisations and anti-tnf use are the key costs. Precent of 70 patients with Crohn s disease require at least one surgical resection, and of these most develop disease recurrence. Post-operative strategies to prevent disease recurrence, which include endoscopic assessment and patienttailored prophylactic drug therapy, are therefore desirable. However, the costeffectiveness of such strategies is unknown. Research frontiers Post-operative management for patients with Crohn s disease has been an area of intense interest over recent years. Randomised studies have sought to define optimal drug therapy and monitoring algorithms. Anti-TNF drugs have consistently been found to be superior to other drugs in the prevention of recurrent Crohn s disease. Anti-TNF drugs however come at a considerable expense to the health care system. This study is part of the Post-Operative Crohn s Endoscopic Recurrence (POCER) platform of studies which has successfully defined the management of patients with Crohn s disease following intestinal resection. Results from the POCER study have radically altered treatment algorithms and our understanding of drug therapy in the prevention of post-operative recurrence of Crohn s disease. The POCER study has 3866 April 14, 2016 Volume 22 Issue 14
181 Wright EK et al. CD post-operative care demonstrated that in patients at high risk of recurrence after curative surgery for Crohn s disease, adalimumab (an anti-tnfα drug) prevents recurrent mucosal disease in most patients, and is superior to thiopurines. A strategy for the post-operative management of these patients has also been determined with treatment according to risk of recurrence, with 6 mo colonoscopy and treatment step-up for endoscopic recurrence, being significantly superior to optimal drug therapy alone, in preventing postoperative recurrence of Crohn s disease. Selective potent immune suppression, adjusted if needed on the basis of colonoscopy, rather than its use in all high risk patients, was shown to lead to effective disease control in a majority of patients. The study described in this manuscript describes the health care costs involved in delivering this treatment and monitoring strategy compared to those required for the provision of standard post-operative care. Innovations and breakthroughs Post-operative strategies to prevent disease recurrence after intestinal resection are associated with high healthcare costs, the majority of which is medication driven. Endoscopic recurrence when compared to remission is associated with significantly higher healthcare costs. The POCER strategy, as illustrated in the active care arm of this study, is based on risk-related medication, monitoring for early disease recurrence, and treatment intensification when needed. It is associated with a reduction in post-operative endoscopic recurrence without a significantly greater cost than standard care. Applications Strategies that prevent endoscopic recurrence may therefore be associated with substantial healthcare savings downstream, making the POCER algorithm a potentially cost effective strategy. Further, using FC to select patients appropriate for colonoscopy reduces costs significantly. Peer-review This manuscript by Wright et al is the first study to describe healthcare cost profiles in the management of post-operative Crohn s disease. The manuscript is well written, it is certainly interesting for the readers of the journal, and I believe that could be accepted for publication. REFERENCES 1 Feagan BG, Vreeland MG, Larson LR, Bala MV. Annual cost of care for Crohn s disease: a payor perspective. Am J Gastroenterol 2000; 95: [PMID: DOI: /j x] 2 Longobardi T, Bernstein CN. Health care resource utilization in inflammatory bowel disease. Clin Gastroenterol Hepatol 2006; 4: [PMID: DOI: /j.cgh ] 3 Cohen RD, Larson LR, Roth JM, Becker RV, Mummert LL. The cost of hospitalization in Crohn s disease. Am J Gastroenterol 2000; 95: [PMID: DOI: /j x] 4 Silverstein MD, Loftus EV, Sandborn WJ, Tremaine WJ, Feagan BG, Nietert PJ, Harmsen WS, Zinsmeister AR. Clinical course and costs of care for Crohn s disease: Markov model analysis of a population-based cohort. Gastroenterology 1999; 117: [PMID: DOI: /S (99) ] 5 Bassi A, Dodd S, Williamson P, Bodger K. Cost of illness of inflammatory bowel disease in the UK: a single centre retrospective study. Gut 2004; 53: [PMID: DOI: / gut ] 6 van der Valk ME, Mangen MJ, Leenders M, Dijkstra G, van Bodegraven AA, Fidder HH, de Jong DJ, Pierik M, van der Woude CJ, Romberg-Camps MJ, Clemens CH, Jansen JM, Mahmmod N, van de Meeberg PC, van der Meulen-de Jong AE, Ponsioen CY, Bolwerk CJ, Vermeijden JR, Siersema PD, van Oijen MG, Oldenburg B. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-tnfα therapy: results from the COIN study. Gut 2014; 63: [PMID: DOI: /gutjnl ] 7 Odes S, Vardi H, Friger M, Wolters F, Hoie O, Moum B, Bernklev T, Yona H, Russel M, Munkholm P, Langholz E, Riis L, Politi P, Bondini P, Tsianos E, Katsanos K, Clofent J, Vermeire S, Freitas J, Mouzas I, Limonard C, O Morain C, Monteiro E, Fornaciari G, Vatn M, Stockbrugger R. Effect of phenotype on health care costs in Crohn s disease: A European study using the Montreal classification. J Crohns Colitis 2007; 1: [PMID: DOI: /j.crohns ] 8 Bernell O, Lapidus A, Hellers G. Risk factors for surgery and postoperative recurrence in Crohn s disease. Ann Surg 2000; 231: [PMID: DOI: / ] 9 Binder V, Hendriksen C, Kreiner S. Prognosis in Crohn s disease- -based on results from a regional patient group from the county of Copenhagen. Gut 1985; 26: [PMID: DOI: /gut ] 10 Cosnes J, Nion-Larmurier I, Beaugerie L, Afchain P, Tiret E, Gendre JP. Impact of the increasing use of immunosuppressants in Crohn s disease on the need for intestinal surgery. Gut 2005; 54: [PMID: DOI: /gut ] 11 Peyrin-Biroulet L, Harmsen WS, Tremaine WJ, Zinsmeister AR, Sandborn WJ, Loftus EV. Surgery in a population-based cohort of Crohn s disease from Olmsted County, Minnesota ( ). Am J Gastroenterol 2012; 107: [PMID: DOI: /ajg ] 12 Olaison G, Smedh K, Sjödahl R. Natural course of Crohn s disease after ileocolic resection: endoscopically visualised ileal ulcers preceding symptoms. Gut 1992; 33: [PMID: DOI: /gut ] 13 Rutgeerts P, Geboes K, Vantrappen G, Kerremans R, Coenegrachts JL, Coremans G. Natural history of recurrent Crohn s disease at the ileocolonic anastomosis after curative surgery. Gut 1984; 25: [PMID: DOI: /gut ] 14 Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohn s disease. Gastroenterology 1990; 99: [PMID: ] 15 Landsend E, Johnson E, Johannessen HO, Carlsen E. Long-term outcome after intestinal resection for Crohn s disease. Scand J Gastroenterol 2006; 41: [PMID: DOI: / ] 16 Regueiro M, Schraut W, Baidoo L, Kip KE, Sepulveda AR, Pesci M, Harrison J, Plevy SE. Infliximab prevents Crohn s disease recurrence after ileal resection. Gastroenterology 2009; 136: e1; quiz 716 [PMID: DOI: / j.gastro ] 17 De Cruz P, Kamm MA, Hamilton AL, Ritchie KJ, Krejany EO, Gorelik A, Liew D, Prideaux L, Lawrance IC, Andrews JM, Bampton PA, Gibson PR, Sparrow M, Leong RW, Florin TH, Gearry RB, Radford-Smith G, Macrae FA, Debinski H, Selby W, Kronborg I, Johnston MJ, Woods R, Elliott PR, Bell SJ, Brown SJ, Connell WR, Desmond PV. Crohn s disease management after intestinal resection: a randomised trial. Lancet 2015; 385: [PMID: DOI: /S (14) ] 18 Regueiro M, Kip KE, Baidoo L, Swoger JM, Schraut W. Postoperative therapy with infliximab prevents long-term Crohn s disease recurrence. Clin Gastroenterol Hepatol 2014; 12: e1 [PMID: ] 19 Doherty G, Bennett G, Patil S, Cheifetz A, Moss AC. Interventions for prevention of post-operative recurrence of Crohn s disease. Cochrane Database Syst Rev 2009; (4): CD [PMID: DOI: / cd pub2] 20 Priest VL, Begg EJ, Gardiner SJ, Frampton CM, Gearry RB, Barclay ML, Clark DW, Hansen P. Pharmacoeconomic analyses of azathioprine, methotrexate and prospective pharmacogenetic testing for the management of inflammatory bowel disease. Pharmacoeconomics 2006; 24: [PMID: DOI: / ] 21 Dubinsky MC, Reyes E, Ofman J, Chiou CF, Wade S, Sandborn WJ. A cost-effectiveness analysis of alternative disease management strategies in patients with Crohn s disease treated with azathioprine or 6-mercaptopurine. Am J Gastroenterol 2005; 100: [PMID: DOI: /j x] 3867 April 14, 2016 Volume 22 Issue 14
182 Wright EK et al. CD post-operative care 22 Present DH, Rutgeerts P, Targan S, Hanauer SB, Mayer L, van Hogezand RA, Podolsky DK, Sands BE, Braakman T, DeWoody KL, Schaible TF, van Deventer SJ. Infliximab for the treatment of fistulas in patients with Crohn s disease. N Engl J Med 1999; 340: [PMID: DOI: / NEJM ] 23 Hanauer SB, Sandborn WJ, Rutgeerts P, Fedorak RN, Lukas M, MacIntosh D, Panaccione R, Wolf D, Pollack P. Human antitumor necrosis factor monoclonal antibody (adalimumab) in Crohn s disease: the CLASSIC-I trial. Gastroenterology 2006; 130: ; quiz 591 [PMID: DOI: / j.gastro ] 24 Feagan BG, Panaccione R, Sandborn WJ, D Haens GR, Schreiber S, Rutgeerts PJ, Loftus EV, Lomax KG, Yu AP, Wu EQ, Chao J, Mulani P. Effects of adalimumab therapy on incidence of hospitalization and surgery in Crohn s disease: results from the CHARM study. Gastroenterology 2008; 135: [PMID: DOI: /j.gastro ] 25 Bodger K, Kikuchi T, Hughes D. Cost-effectiveness of biological therapy for Crohn s disease: Markov cohort analyses incorporating United Kingdom patient-level cost data. Aliment Pharmacol Ther 2009; 30: [PMID: DOI: / j x] 26 Loftus EV, Johnson SJ, Yu AP, Wu EQ, Chao J, Mulani PM. Cost-effectiveness of adalimumab for the maintenance of remission in patients with Crohn s disease. Eur J Gastroenterol Hepatol 2009; 21: [PMID: DOI: / MEG.0b013e32832a8d71] 27 Lindsay J, Punekar YS, Morris J, Chung-Faye G. Healtheconomic analysis: cost-effectiveness of scheduled maintenance treatment with infliximab for Crohn s disease--modelling outcomes in active luminal and fistulizing disease in adults. Aliment Pharmacol Ther 2008; 28: [PMID: DOI: / j x] 28 Jaisson-Hot I, Flourié B, Descos L, Colin C. Management for severe Crohn s disease: a lifetime cost-utility analysis. Int J Technol Assess Health Care 2004; 20: [PMID: DOI: /S ] 29 Dretzke J, Edlin R, Round J, Connock M, Hulme C, Czeczot J, Fry-Smith A, McCabe C, Meads C. A systematic review and economic evaluation of the use of tumour necrosis factor-alpha (TNF-α) inhibitors, adalimumab and infliximab, for Crohn s disease. Health Technol Assess 2011; 15: [PMID: DOI: /hta15060] 30 Ananthakrishnan AN, Hur C, Juillerat P, Korzenik JR. Strategies for the prevention of postoperative recurrence in Crohn s disease: results of a decision analysis. Am J Gastroenterol 2011; 106: [PMID: DOI: /ajg ] 31 Doherty GA, Miksad RA, Cheifetz AS, Moss AC. Comparative cost-effectiveness of strategies to prevent postoperative clinical recurrence of Crohn s disease. Inflamm Bowel Dis 2012; 18: [PMID: DOI: /ibd.21904] 32 Wright EK, Kamm MA, De Cruz P, Hamilton AL, Ritchie KJ, Krejany EO, Leach S, Gorelik A, Liew D, Prideaux L, Lawrance IC, Andrews JM, Bampton PA, Jakobovits SL, Florin TH, Gibson PR, Debinski H, Macrae FA, Samuel D, Kronborg I, Radford-Smith G, Selby W, Johnston MJ, Woods R, Elliott PR, Bell SJ, Brown SJ, Connell WR, Day AS, Desmond PV, Gearry RB. Measurement of fecal calprotectin improves monitoring and detection of recurrence of Crohn s disease after surgery. Gastroenterology 2015; 148: e1 [PMID: ] 33 Dowsey MM, Liew D, Choong PF. Economic burden of obesity in primary total knee arthroplasty. Arthritis Care Res (Hoboken) 2011; 63: [PMID: DOI: /acr.20563] 34 MBS Online. Medicare Benefits Schedule Available from: URL: 35 The Pharmaceutical Benefits Scheme Available from: URL: 36 Schalamon J, Mayr JM, Höllwarth ME. Mortality and economics in short bowel syndrome. Best Pract Res Clin Gastroenterol 2003; 17: [PMID: DOI: /S (03) ] 37 Rutgeerts P, Hiele M, Geboes K, Peeters M, Penninckx F, Aerts R, Kerremans R. Controlled trial of metronidazole treatment for prevention of Crohn s recurrence after ileal resection. Gastroenterology 1995; 108: [PMID: ] 38 Wright EK, Kamm MA, De Cruz P, Hamilton AL, Ritchie KJ, Krejany EO, Gorelik A, Liew D, Prideaux L, Lawrance IC, Andrews JM, Bampton PA, Sparrow MP, Florin TH, Gibson PR, Debinski H, Gearry RB, Macrae FA, Leong RW, Kronborg I, Radford-Smith G, Selby W, Johnston MJ, Woods R, Elliott PR, Bell SJ, Brown SJ, Connell WR, Desmond PV. Effect of intestinal resection on quality of life in Crohn s disease. J Crohns Colitis 2015; 9: [PMID: DOI: /ecco-jcc/jjv058] 39 Regueiro M, Feagan BG, Zou B, Johanns J, Blank M, Chevrier M, Plevy SE, Popp J, Cornillie F, Lukas M, Danese S, Gionchetti P, Molenda MR, Hanauer SB, Reinisch W, Sandborn W, Sorrentino D, Rutgeerts PJ. Infliximab for prevention of recurrence of postsurgical Crohn s disease following ileocolonic resection: A randomized placebo-controlled study. Gastroenterology 2015; 148 (Suppl 1): S-141 [DOI: /S (15) ] 40 Saro C, da la Coba C, Casado MA, Morales JM, Otero B. Resource use in patients with Crohn s disease treated with infliximab. Aliment Pharmacol Ther 2007; 26: [PMID: DOI: /j x] 41 Rudakova AV. [Cost-effectiveness of tumor necrosis factor in Crohn s disease]. Eksp Klin Gastroenterol 2012; (5): [PMID: ] 42 Yu AP, Johnson S, Wang ST, Atanasov P, Tang J, Wu E, Chao J, Mulani PM. Cost utility of adalimumab versus infliximab maintenance therapies in the United States for moderately to severely active Crohn s disease. Pharmacoeconomics 2009; 27: [PMID: DOI: / ] 43 Niewiadomski O, Studd C, Hair C, Wilson J, McNeill J, Knight R, Prewett E, Dabkowski P, Dowling D, Alexander S, Allen B, Tacey M, Connell W, Desmond P, Bell S. Health Care Cost Analysis in a Population-based Inception Cohort of Inflammatory Bowel Disease Patients in the First Year of Diagnosis. J Crohns Colitis 2015; 9: [PMID: DOI: /ecco-jcc/jjv117] 44 Danese S, Gomollon F. ECCO position statement: the use of biosimilar medicines in the treatment of inflammatory bowel disease (IBD). J Crohns Colitis 2013; 7: [PMID: DOI: /j.crohns ] 45 Haustein R, de Millas C, Hoer A, Haussler B. Saving money in the European healthcare systems with biosimilars. GaBI J 2012; 1: [DOI: /gabij ] 46 Shapiro RJ, Singh K, Mukim M. The potential American market for generic biological treatments and the associated cost savings Available from: URL: _GenericBiologicsStudy.pdf 47 Mulcahy AW, Predmore Z, Mattke S. The cost savings potential of biosimilar drugs in the United States, Available from: URL: P- Reviewer: Caboclo JLF, Rocha R, Trifan A S- Editor: Qi Y L- Editor: A E- Editor: Ma S 3868 April 14, 2016 Volume 22 Issue 14
183 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. CASE REPORT Ileo-right hemi-colonic cervical pull-up on a non-supercharged ileocolic arterial pedicle: A technical and case report Andreas RR Weiss, Christina Hackl, Yorick Soeder, Hans J Schlitt, Marc-H Dahlke Andreas RR Weiss, Christina Hackl, Yorick Soeder, Hans J Schlitt, Marc-H Dahlke, Department of Surgery, University Medical Center Regensburg, Regensburg, Germany Author contributions: Weiss ARR drafted and wrote the manuscript; Hackl C, Soeder Y and Dahlke MH drafted and critically revised the manuscript; Schlitt HJ critically revised the manuscript. Institutional review board statement: This case report was exempt from the Institutional Review Board standards at the University Medical Center Regensburg. Informed consent statement: The patient involved in this study gave his written informed consent authorizing use and disclosure of his protected health information. Conflict-of-interest statement: All the authors have no conflicts of interests to declare. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Andreas RR Weiss, MD, Department of Surgery, University Medical Center Regensburg, Franz-Josef- Strauß-Allee 11, Regensburg, Germany. andreas1.weiss@ukr.de Telephone: Fax: Received: December 12, 2015 Peer-review started: December 12, 2015 First decision: December 21, 2015 Revised: January 4, 2016 Accepted: January 30, 2016 Article in press: January 30, 2016 Published online: April 14, 2016 Abstract Esophageal reconstruction can be challenging when stomach and colon are not anatomically intact and their use as esophageal substitutes is therefore limited. Innovative individual approaches are then necessary to restore the intestinal passage. We describe a technique in which a short stump of the right hemicolon and 25 cm of ileum on a long, non-supercharged, fully mobilized ileocolic arterial pedicle were used for esophageal reconstruction to the neck. In this case, a 65 year-old male patient had accidentally indigested hydrochloric acid which caused necrosis of his upper digestive tract. An emergency esophagectomy, gastrectomy, duodenectomy, pancreatectomy and splenectomy had been performed in an outside hospital. A cervical esophagostomy and a biliodigestive anastomosis had been created and a jejunal catheter for enteral feeding had been placed. After the patient had recovered, a reconstruction of his food passage via the left and transverse colon failed for technical reasons due to an intraoperative necrotic demarcation of the colon. Our team then faced the situation that only a short stump of the right hemi-colon was left in situ when the patient was referred to our center. After intensified nutritional therapy, we reconstructed this patient s food passage with the right hemicolonapproach described herein. After treatment of a postoperative pneumonia, the patient was discharged from hospital on the 26 th postoperative day in a good clinical condition on an oral-only diet. In conclusion, individual approaches for long-segment reconstruction of the esophagus can be technically feasible in experienced hands. They do not always require arterial supercharging or free intestinal transplantation April 14, 2016 Volume 22 Issue 14
184 Weiss ARR et al. Ileo-right hemi-colonic cervical pull-up Key words: Esophageal cancer; Esophageal trauma; Esophageal reconstruction; Gastric pull-up; Colonic interposition The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Esophageal reconstructions are more challenging than usual when the stomach and the colon are not available as substitutes for esophageal replacement. In this case, hydrochloric acid had caused severe caustic injuries to the upper digestive tract requiring esophagectomy, gastrectomy, duodenectomy, pancreatectomy and splenectomy in a 65-year-old patient. The initial reconstruction failed, leaving only a short stump of the right hemicolon in situ. We then reconstructed the intestinal passage utilizing this short part of the right hemicolon and 25 cm of ileum on a long, non-supercharged, fully mobilized ileocolic arterial pedicle. Weiss ARR, Hackl C, Soeder Y, Schlitt HJ, Dahlke MH. Ileoright hemi-colonic cervical pull-up on a non-supercharged ileocolic arterial pedicle: A technical and case report. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Malignant tumors of the esophagus and the esophagogastric junction, as well as caustic injuries and perforations are among the prime indications for resections of the esophagus. All esophagogastric resections with reconstruction are associated with significant morbidity and mortality. A gastric tube is preferably used to reconstruct the food passage after esophagectomy as it usally comes along with a reliable blood supply and only one single anastomosis is necessary for reconstruction. The situation becomes more difficult when the stomach is not available for reconstruction. In these cases, either a pedicled colonic or jejunal interposition or a free jejunal graft can be used. Pedicled interposition grafts always come along with limitations of the blood supply. This is especially relevant towards the oral part of the graft, which - if insufficient - can lead to anastomotic leakage or, in the worst case, to partial or complete necrosis of the pull-up. Necrotic complications then frequently lead to life threatening secondary problems. Recently published studies demonstrate the benefit of additional arterial and venous supercharging, which may improve the blood supply of the graft or pull-up and can therefore reduce the incidence of graft loss and anastomotic leakage [1-4]. When the initial reconstruction fails and a salvage operation with limited intestinal resources for recon- struction has to be planned, the situation can be further complicated. This case report introduces an individual approach of a secondary reconstruction of the food passage with an ileo-right hemi-colonic cervical pull-up on a non-supercharged ileocolic arterial pedicle after a first colonic reconstruction had failed. CASE REPORT A 65-year-old male patient had accidentally indigested hydrochloric acid which caused a necrosis of his upper digestive tract. In an emergency surgery, an esophagectomy, gastrectomy, duodenectomy, pancreatectomy and splenectomy were performed (Figure 1A and B). At the end of this first operation, a cervical esophagostomy and a choledocho-jejunostomy were created. Furthermore, a jejunal catheter for enteral feeding was inserted. One month later, an exploratory laparotomy was performed due to a massive pneumoperitoneum and suspected bowel perforation diagnosed in a routine chest X-ray after the placement of a central venous catheter. During surgery, pneumatosis coli without perforation were detected, most likely based on an antibiotic-associated colitis (C. difficile toxin negative). Colon resection was renounced due to missing clinical symptoms and a planned esophageal reconstruction via a colonic interposition. Instead, a protective loop ileostomy was formed and reversed three months later. After the patient had recovered, five months after the first surgery, a reconstruction of the food passage with a colonic pull-up using the transverse and descending colon was attempted. The reconstruction failed due to an intraoperative ischemic demarcation of the colon, leaving only a short oral part of the ascending colon and approximately 40 cm of the descending colon in situ (Figure 1C, D and E). The colonic remnants were connected via a colo-colonic anastomosis. Eight months after the first surgery, the patient contacted our team seeking alternative reconstruction options for his intestinal passage. In the meantime, the patient was in a poor nutritional condition (BMI 16.1) and was fed exclusively via the jejunal catheter. The patient was admitted to our surgical ward for an intensified nutritional therapy to improve his body weight and constitution. Furthermore, an angiography of the patient s mesenteric arteries was performed, which revealed a sufficient blood supply of the remaining right hemicolon and the terminal ileum via the ileocolic artery (Figure 2). Fortunately, the ileocolic artery formed a tight loop with the terminal jejunal branch of the superior mesenteric artery, which was used later as described below. The patient was discharged from hospital for further home-based nutritional therapy and readmitted for surgery two months later. After readmission, the patient s food passage was reconstructed via a retrosternal ileo-right hemi April 14, 2016 Volume 22 Issue 14

185 Weiss ARR et al. Ileo-right hemi-colonic cervical pull-up A B C D E F G H Figure 1 Secondary reconstruction with an ileo-right hemi-colonic cervical pull-up on a non-supercharged ileocolic arterial pedicle. A, B: Before and after emergency esophagectomy, gastrectomy, duodenectomy and pancreatectomy due to a caustic injury with hydrochloric acid; C, D: Esophageal reconstruction with transverse and descending colon fails due to ischemic demarcation consecutive resection of transverse and descending colon including the distal part of the ascending colon; E: A short stump of the right hemi-colon and approximately 40 cm of descending colon were left in situ, connected via a colo-colonic anastomosis; F: Esophageal reconstruction with an ileo-right hemi-colonic cervical pull-up on a non-supercharged ileocolic arterial pedicle in an isoperistaltic direction; G: Situation 9 mo after reconstruction: The cecal part of the pulled-up graft had moved downwards from the thoracic cavity into the abdomen and largely dilated, causing recurrent episodes of bowel obstruction; H: Final result: The ileocecal region was resected and an ileo-jejunostomy was formed. Ileocolic artery Terminal branch of SMA Figure 2 Arteriographic examination of the superior mesenteric artery. The ileocolic artery forms a tight loop with the terminal jejunal branch of the superior mesenteric artery. colonic cervical pull-up on a non-supercharged ileocolic arterial pedicle. During surgery, the ileocecal region and the remaining ascending colon were mobilized and the ileum was transected about 25 cm proximal to Bauhin s valve. The ileocolic artery was fully mobilized to its origin from the superior mesenteric artery by meticulous micro-preparation and then dissected to use the full length of both branches of the artery. After a sufficient blood supply of the pedicled graft was ensured, the ileum was pulled up to the neck retrosternally and anastomosed end-to-side in an iso-peristaltic fashion to the esophageal stump with a tension-free running manual suture. To achieve this position, the ileocolic artery was turned upwards to a 180 angle. The stump of the ascending colon was then anastomosed end-to-side to the proximal end of the jejunum. Finally, the neo-terminal ileum was anastomosed to the stump of the remaining descending colon (Figure 1F). The following day, a scheduled second look laparotomy was performed to confirm a sufficient blood supply of the interposition graft. During the postoperative course on the intensive care unit the patient developed severe pneumonia, which was treated with antibiotics, chest tubes and intensified respiratory and positioning therapy. After further stabilization, the patient could be transferred to the general ward on the 13 th postoperative day. Stepwise return to a normal diet was well tolerated. A contrast X-ray swallow showed a smooth passage of a soft bolus. The patient was discharged from hospital in a good clinical condition on the 26 th postoperative day on an oral-only diet. During the following months, the patient suffered from episodes of dysphagia, recurrent nausea and air 3871 April 14, 2016 Volume 22 Issue 14

186 Weiss ARR et al. Ileo-right hemi-colonic cervical pull-up Figure 3 Largely dilated cecum in the upper abdomen. The cecal part of the interposition graft had moved downwards from the thoracic cavity into the abdomen with consecutive massive dilatation causing bowel obstruction. regurgitation. Additional work-up showed significant dilatation of the pulled-up cecum so that another operation became necessary. Intraoperative assessment revealed that the cecal part of the pulled-up pedicled graft had moved downwards significantly (likely due to gravital challenge in an upright position) from the thoracic cavity through the diaphragm into the abdomen. The cecum was massively dilated and seen as the cause for dysphagia and bowel obstruction as the distal anastomosis was kinked (Figures 3 and 1G). Hence, the ileocecal region was resected and an ileo-jejunostomy was created (Figure 1H). No further complications occurred in the postoperative course and the patient was discharged from hospital on the 12 th postoperative day. A few months later, the patient complained about new symptoms of dysphagia, which were due to a stenosis of the ileo-jejunostomy. The stenosis could successfully be dilated by endoscopic balloon dilatation. Similar symptoms reappeared, this time due to intraabdominal and retrosternal adhesions that were removed in yet another reoperation via a re-laparotomy and a lower partial sternotomy. During the whole treatment episode at our hospital, the patient had regular appointments with our nutritional experts who adjusted his diet to his special needs (including the substitution of pancreatic enzymes and vitamins). In the last outpatient follow-up examination 32 mo after reconstruction, the patient s bodyweight was still below average (BMI 17.5) but stable under oralonly food intake without the need for additional enteral or parenteral nutrition and no symptoms of dysphagia (see timeline, Figure 4). He lives an independent life. DISCUSSION In selected cases where the stomach cannot be used for reconstruction of the enteric passageway after esophagectomy, several techniques have been described: pedicled colonic grafts have the advantage that longer conduits can be formed to reconstruct the passage up to the neck when compared to pedicled jejunal grafts. On the downside, colonic enterobacteria pose a higher risk for pulmonary complications in the postoperative course and stenoses and graft redundancy are more frequent in colonic than in jejunal interpositions [1,5,6]. Pedicled jejunal grafts are limited in length due to the shorter mesenteric arcades [7]. Moreover, the diameter of the jejunum is usually more congruent to the diameter of the esophagus and jejunal grafts fit easier through the thoracic inlet in case of retrosternal pull-up. Other advantages of jejunal grafts are a better food transit due to the physiologic peristalsis of the jejunum and a lower risk for intrinsic disease such as hemorrhage or the development of graft carcinoma [8]. All grafts to restore the intestinal continuity after near-total esophagectomy need to be moved up to the cervical esophagus without major tension. This is usually more difficult for jejunal than for colonic grafts and becomes the more complicated the longer the distance to the esophageal stump is. Tension to the anastomosis regularly results in an insufficient blood supply of the graft and can lead to anastomotic leakage or graft necrosis, the most feared complications of these procedures. Thus, supercharging techniques have been introduced using additional arterial and venous anastomoses to vessels located in the neck or chest regions. Several studies demonstrated the benefit of this approach showing that it can improve blood supply to the graft and consequently reduce the incidence of graft necrosis and anastomotic leakage [1-4,7,9]. Since the introduction of the supercharging technique, pedicled jejunal grafts with these anastomoses have become more relevant in the reconstruction of esophageal defects and some authors prefer the jejunum instead of the colon for these purposes [1,7]. However, supercharging is technically challenging and requires microvascular anastomoses, which come along with another array of possible vascular complications. In case of limited esophageal defects, free jenunal or colonic grafts are an alternative with good postoperative results [10-13]. Right hemi-colonic pull-ups can also be used for esophageal replacement when long enough [14]. In our case, only a short stump of the right hemi-colon was left. Hence, a far longer segment of the terminal ileum had to be chosen to gain enough length for a pull-up to the neck. Accomplishing this without arterial supercharging would have been inconceivable without a previous angiography of the mesenteric arteries with meticulous planning on how to gain maximum length out of it. Using the full length of the ileocolic artery finally made this pull-up possible in the reported case. We thus suggest that preoperative angiography of the mesenteric vessels 3872 April 14, 2016 Volume 22 Issue 14
187 Weiss ARR et al. Ileo-right hemi-colonic cervical pull-up 05/2012 Initial operation 1 06/2012 Formation of a loop ileostomy due to pneumatosis coli 09/2012 Reversal of loop ileostomy 10/2012 Reconstruction with transverse and descending colon fails 04/2013 Secondary reconstruction with ileo-right hemi-colonic cervical pull-up 01/2014 Colon redundancy, resection of the cecal part of the pulled-up graft 06/2014 Endoscopic balloon dilatation of a stenosis of the ileojejunostomy 10/2014 Re-operation with removal of intraabdominal and retrosternal adhesions Figure 4 Timeline. 1 Initial operation: Indigestion of hydrochloric acid with consecutive esophagectomy, gastrectomy, duodenectomy, pancreatectomy and splenectomy. Creation of a cervical esophagostomy, a choledo-jejunostomy and placement of a jejunal catheter. should be regularly used to ensure a reliable blood supply of the graft and therefore reduce the incidence of graft necrosis and anastomotic leakage [15]. Long-segment esophageal reconstructions without the stomach are demanding and need individual planning of the experienced surgeon and his team. Such reconstructions do not always require arterial supercharging. To prevent graft loss and anastomotic leakage due to insufficient blood supply, preoperative angiography with thorough planning of the expected circulatory situation and vessel length can be recommended. Individual approaches for esophageal reconstructions can then be feasible and restore quality of life. ACKNOWLEDGMENTS The authors would like to thank Dieter Pirner for the design of Figures 1 and 4. COMMENTS Case characteristics A 65-year-old patient with caustic injury requiring emergency esophagectomy, gastrectomy, duodenectomy, pancreatectomy and splenectomy. Clinical diagnosis Inability of oral food intake due to discontinuity resection of the esophagus and failed reconstruction with left and transverse colon. Laboratory diagnosis Signs of malnutrition with hypoalbuminemia and vitamin B12 deficiency. Imaging diagnosis Angiography of the superior mesenteric artery reveals blood supply of the ileocecal region with the formation of a tight loop between the ileocolic artery and the terminal jejunal branch of the superior mesenteric artery. Treatment Secondary reconstruction of the food passage with ileo-right hemi-colonic cervical pull-up after the initial reconstruction with left and transverse colon failed, followed by resection of the cecal part of the pulled-up graft due to colon redundancy, endoscopic balloon dilatation of a stenosis of the ileo-jejunostomy and re-operation with removal of retrosternal and intraabdominal adhesions. Related reports A preoperative angiography of the mesenteric arteries might show different or new aspects of possible esophageal substitutes. Term explanation Pedicled grafts remain connected to their original blood supply and are therefore limited in length. Supercharging describes a method to improve the blood supply of a pedicled graft by adding an additional blood supply via microvascular anastomoses to local vessels in the area of application. Experiences and lessons Esophageal reconstructions are still associated with a high morbidity and mortality. In complicated cases with limited intestinal resources, individual approaches can be feasible to restore the patient s quality of life. Peer-review This is a very good clinical case report with an interesting topic. REFERENCES 1 Blackmon SH, Correa AM, Skoracki R, Chevray PM, Kim MP, Mehran RJ, Rice DC, Roth JA, Swisher SG, Vaporciyan AA, Yu P, Walsh GL, Hofstetter WL. Supercharged pedicled jejunal interposition for esophageal replacement: a 10-year experience. Ann Thorac Surg 2012; 94: ; discussion [PMID: DOI: /j.athoracsur ] 2 Fujita H, Yamana H, Sueyoshi S, Shima I, Fujii T, Shirouzu K, Inoue Y, Kiyokawa K, Tanabe HY, Tai Y, Inutsuka H. Impact on outcome of additional microvascular anastomosis--supercharge- -on colon interposition for esophageal replacement: comparative and multivariate analysis. World J Surg 1997; 21: [PMID: DOI: /s ] 3 Kesler KA, Pillai ST, Birdas TJ, Rieger KM, Okereke IC, Ceppa D, Socas J, Starnes SL. Supercharged isoperistaltic colon interposition for long-segment esophageal reconstruction. Ann Thorac Surg 2013; 95: ; discussion [PMID: DOI: /j.athoracsur ] 4 Sekido M, Yamamoto Y, Minakawa H, Sasaki S, Furukawa H, Sugihara T, Nohira K, Yajima K, Shintomi Y, Okushiba S, Kato H, Hosokawa M. Use of the supercharge technique in esophageal and pharyngeal reconstruction to augment microvascular blood flow. Surgery 2003; 134: [PMID: DOI: /S (03) ] 3873 April 14, 2016 Volume 22 Issue 14
188 Weiss ARR et al. Ileo-right hemi-colonic cervical pull-up 5 Chirica M, Veyrie N, Munoz-Bongrand N, Zohar S, Halimi B, Celerier M, Cattan P, Sarfati E. Late morbidity after colon interposition for corrosive esophageal injury: risk factors, management, and outcome. A 20-years experience. Ann Surg 2010; 252: [PMID: DOI: /SLA.0b013e3181e8fd40] 6 Greene CL, DeMeester SR, Augustin F, Worrell SG, Oh DS, Hagen JA, DeMeester TR. Long-term quality of life and alimentary satisfaction after esophagectomy with colon interposition. Ann Thorac Surg 2014; 98: ; discussion [PMID: ] 7 Doki Y, Okada K, Miyata H, Yamasaki M, Fujiwara Y, Takiguchi S, Yasuda T, Hirao T, Nagano H, Monden M. Long-term and shortterm evaluation of esophageal reconstruction using the colon or the jejunum in esophageal cancer patients after gastrectomy. Dis Esophagus 2008; 21: [PMID: DOI: / j x] 8 Jeyasingham K, Lerut T, Belsey RH. Revisional surgery after colon interposition for benign oesophageal disease. Dis Esophagus 1999; 12: 7-9 [PMID: DOI: /j x] 9 Poh M, Selber JC, Skoracki R, Walsh GL, Yu P. Technical challenges of total esophageal reconstruction using a supercharged jejunal flap. Ann Surg 2011; 253: [PMID: DOI: /SLA.0b013e318217e875] 10 Hackl C, Popp FC, Ehehalt K, Dendl LM, Benseler V, Renner P, Loss M, Dolderer J, Prantl L, Kühnel T, Schlitt HJ, Dahlke MH. Retrograde stapling of a free cervical jejunal interposition graft: a technical innovation and case report. BMC Surg 2014; 14: 78 [PMID: ] 11 Okumura Y, Mori K, Yamagata Y, Fukuda T, Wada I, Shimizu N, Nomura S, Iida T, Mihara M, Seto Y. Two-stage operation for thoracic esophageal cancer: esophagectomy and subsequent reconstruction by a free jejunal flap. Surg Today 2014; 44: [PMID: DOI: /s ] 12 Shirakawa Y, Naomoto Y, Noma K, Ono R, Nobuhisa T, Kobayashi M, Fujiwara T, Noguchi H, Ohkawa T, Yamatsuji T, Haisa M, Matsuoka J, Gunduz M, Tanaka N. Free jejunal graft for hypopharyngeal and esophageal reconstruction. Langenbecks Arch Surg 2004; 389: [PMID: DOI: /s z] 13 Noguchi T, Uchida Y, Hashimoto T, Wada S, Takeno S, Suzuki M. Reconstruction of the cervical esophagus using a free transverse colonic graft: report of a case with upper esophageal web and carcinoma. Dis Esophagus 2003; 16: [PMID: DOI: /j x] 14 Hamai Y, Hihara J, Emi M, Aoki Y, Okada M. Esophageal reconstruction using the terminal ileum and right colon in esophageal cancer surgery. Surg Today 2012; 42: [PMID: DOI: /s ] 15 Predescu D, Popa B, Gheorghe M, Predescu I, Jinescu G, Boeriu M, Constantinoiu S. The vascularization pattern of the colon and surgical decision in esophageal reconstruction with colon. A selective SMA and IMA arteriographic study. Chirurgia (Bucur) 2013; 108: [PMID: ] P- Reviewer: Can G, Majbar MA S- Editor: Qi Y L- Editor: A E- Editor: Ma S 3874 April 14, 2016 Volume 22 Issue 14
189 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. rare cause of odynophagia: giant esophageal ulcer CASE REPORT Massimiliano Veroux, Giuseppe Aprile, Francesca F Amore, Daniela Corona, Alessia Giaquinta, Pierfrancesco Veroux Massimiliano Veroux, Daniela Corona, Alessia Giaquinta, Pierfrancesco Veroux, the Vascular Surgery and Organ Transplant Unit, Department of Medical and Surgical Sciences and Advanced Technologies, University Hospital of Catania, Catania, Italy Giuseppe Aprile, Endoscopy Unit, Department of Surgical Specialties, University Hospital of Catania, Catania, Italy Francesca F Amore, Pathology Unit, Department of Medical and Surgical Sciences and Advanced Technologies, University Hospital of Catania, Catania, Italy Author contributions: Veroux M and Veroux P designed the report; Aprile G performed the endoscopic procedures; Amore FF performed the histological analysis and immunohistochemical studies; Corona D and Giaquinta A collected the patient s clinical data; Veroux M analyzed the data and wrote the paper. Supported by Italian Ministry of Health, No. PE ; and University of Catania, No. FIR Institutional review board statement: This case report was exempt from the Institutional Review Board standards at University of Catania. Informed consent statement: The patient involved in this study gave her written informed consent authorizing use and disclosure of her protected health information. Conflict-of-interest statement: all the authors have no conflicts of interest to disclose. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Massimiliano Veroux, MD, PhD, FEBS, Associate Professor of Surgery, the Vascular Surgery and Organ Transplant Unit, Department of Medical and Surgical Sciences and Advanced Technologies, University Hospital of Catania, Via Santa Sofia, 84, Catania, Italy. veroux@unict.it Telephone: Fax: Received: August 28, 2015 Peer-review started: August 31, 2015 First decision: September 29, 2015 Revised: October 22, 2015 Accepted: December 12, 2015 Article in press: December 14, 2015 Published online: April 14, 2016 Abstract Gastrointestinal complications are a frequent cause of morbidity after transplantation and may affect up to 40% of kidney transplant recipients. Here we report a rare case of idiopathic giant esophageal ulcer in a kidney transplant recipient. A 37-year-old female presented with a one-week history of odynophagia and weight loss. Upon admission, the patient presented cold sores, and a quantitative cytomegalovirus polymerase chain reaction was positive (10 5 copies/ml). An upper endoscopy demonstrated the presence of a giant ulcer. Serological test and tissue biopsies were unable to demonstrate an infectious origin of the ulcer. Immunosuppression was reduced and everolimus was introduced. An empirical i.v. therapy with acyclovir was started, resulting in a dramatic improvement in symptoms and complete healing of the ulcer. Only two cases of idiopathic giant esophageal ulcer in kidney transplant recipients have been reported in the literature; in both cases, steroid therapy was successful without recurrence of symptoms or endoscopic findings. However, this report suggests that correction of immune imbalance is mandatory to treat such a rare complication. Key words: Acyclovir; Gastrointestinal complications; Kidney transplantation; Endoscopy; Steroid; Idiopathic 3875 April 14, 2016 Volume 22 Issue 14

190 Veroux M et al. Giant esophageal ulcer The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: gastrointestinal complications after kidney transplantation are common and may be associated to an increased risk of serious post-transplant morbidity. Giant esophageal ulcers are very rare and the diagnosis of causality is often delayed. This case illustrates the clinical management of an idiopathic giant ulcer, suggesting the possible role of innate immunity imbalance in the pathogenesis of this rare clinical finding. Veroux M, Aprile G, Amore FF, Corona D, Giaquinta A, Veroux P. Rare cause of odynophagia: Giant esophageal ulcer. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION Gastrointestinal (GI) complications are a frequent cause of morbidity after transplantation and may affect up to 40% of kidney transplant recipients [1-3]. Although most patients present with mild symptoms, such as diarrhea, peptic ulcer and oral lesions, these complications may be severe in approximately 10% of patients and may be associated with a doubled risk of graft loss and patient death [1,2]. Idiopathic giant esophageal ulcers in immunocompromised patients have been described more commonly in patients with acquired immunodeficiency syndrome (AIDS) [4,5]. In this report, we present a rare case of idiopathic giant esophageal ulcer in a kidney transplant patient, responding to acyclovir therapy and reduction of immunosuppression. CASE REPORT A 37-year-old female presented with a 1-wk history of severe odynophagia and epigastric pain, worsening after food intake. She had received a deceased donor kidney transplantation 6 mo prior, and the immunosuppressive regimen consisted of tacrolimus, mycophenolic acid and prednisone. Upon admission, the patient presented cold sores, the leucocytes were 1300/mm 3, and a quantitative cytomegalovirus (CMV) polymerase chain reaction (PCR) was positive (10 5 copies/ml). Graft functionality was slightly impaired (Serum creatinine, 2.1 mg/dl). Intravenous ganciclovir therapy (250 mg daily) was immediately started combined with oral acyclovir; mycophenolic acid was discontinued; and tacrolimus was replaced with everolimus, without any beneficial effects. The patient was unable to swallow solid food and lost 8 kg. Upper endoscopy was performed, showing a large ulcer in the distal esophagus measuring 40 mm in diameter (Figure 1). Endoscopic biopsies Figure 1 Upper endoscopy showing a giant ulcer of the distal esophagus (arrows). showed acute inflammation without any viral particles, but with positivity to Candida species (PASD stain) (Figure 2). Her symptoms failed to resolve after two weeks of total parental nutrition, high dose omeprazole (80 mg daily) and fluconazole (200 mg daily). Repeat endoscopy revealed only a slight improvement of the ulcer. Histological examination of biopsy and cytology material for fungal or viral infection was negative, and histochemical studies for CMV, herpes simplex virus (HSV) and adenoviruses were negative and CMV-DNA PCR was negative. Intravenous/empiric therapy with acyclovir (900 mg daily) was started. Her symptoms dramatically improved over 48 h and completely resolved within 10 d, with concomitant partial weight gain (4 kg), and normal leucocytes count (5240/mm 3 ). Repeat endoscopy 10 d after acyclovir treatment revealed near complete resolution of the ulcer (Figure 3). The patient continued oral valganciclovir and acyclovir therapies, without recurrence of symptoms six months after diagnosis and with excellent graft function. DISCUSSION Candida esophagitis is the most common esophageal disorder in renal transplant recipients, and usually occurs in leukopenic or over-immunosuppressed patients within six months after transplantation [1,2]. In most cases, candida esophagitis is associated with candidal stomatitis and epiglottitis. In general, candida esophagitis presents with odynophagia, but endoscopic findings are characteristic with multiple small plaques in the upper or mid esophagus. Other causes of esophagitis include CMV or herpes simplex infection. The typical appearance of herpetic esophagitis is represented by multiple vesicular lesions with or without ulcers along the entire esophagus [2]. However, the endoscopic manifestation of herpetic esophagitis may be similar to that of CMV esophagitis, such that diagnosis should be confirmed by cytology, histological examination and viral cultures. Idiopathic giant ulcers are rarely observed and are 3876 April 14, 2016 Volume 22 Issue 14

![(PAS-positive) (arrow). Figure 3 Endoscopy demonstrated the near complete healing of the ulcer. more commonly encountered in patients with HIV infection [4,5].](/docs-images/92/109922872/images/191-1.jpg "HIV has been observed in ulcer tissue, suggesting that HIV itself could be the direct cause of these lesions [6].")
191 Veroux M et al. Giant esophageal ulcer 200 mm Figure 2 Histopathological examination of ulcer showed esophagitis with ulceration and underlying granulation tissue, with many bacterial colonies and fungal spores (PAS-positive) (arrow). Figure 3 Endoscopy demonstrated the near complete healing of the ulcer. more commonly encountered in patients with HIV infection [4,5]. HIV has been observed in ulcer tissue, suggesting that HIV itself could be the direct cause of these lesions [6]. However, it can also be detected in esophageal biopsies from patients with Candida, CMV and HSV esophagitis [5]. Our report and other previous cases [7,8] provide clinical evidence that idiopathic giant esophageal ulcer can occur in the absence of HIV infection, and favor a defect of immunity rather than a virus etiology in the pathogenesis of idiopathic esophageal ulceration [5]. In our report, although the clinical context of the patient suggested a potential CMV-related ulcer, there was no evidence of viral cytopathology as assessed from routine histological or immunohistochemical studies. Furthermore, our patient was on high dose ganciclovir and did not demonstrate any clinical beneficial effect on odynophagia and weight loss because the patient continued to be unable to swallow solid food. Histological finding of fungal infection was most likely related to a direct contamination of the ulcer because there was no evidence of candida stomatitis or characteristic endoscopic lesions in the esophagus. Moreover, the ulcer failed to improve after a high dose of fluconazole. Histopathological features cannot distinguish idiopathic ulceration from gastroesophageal reflux disease, but the patient presented no endoscopic appearance to suggest reflux disease and her symptoms and esophageal ulceration failed to improve to high dose omeprazole and total parental nutrition. Although the clinical finding of cold sores and the dramatic temporal response to highdose acyclovir therapy may suggest a herpetic origin for the giant ulcer, we were unable to demonstrate the presence of viral particles using histological or immunohistochemical studies, and routine serological tests for HSV were negative. There have only been two reports of idiopathic giant esophageal ulcer in kidney transplant recipients [6,7], and both patients were previously subjected to overimmunosuppression to prevent acute rejection episodes. In both cases, steroid therapy was successful without recurrence of symptoms or endoscopic findings. The response to idiopathic esophageal ulcer to steroids is clearly documented in AIDS, with a clinical remission observed in more than 90% of cases [9]. The prednisone regimen consists of 40 mg/d, tapering 10 mg/wk for a 1-mo treatment course. The relapse rate for esophageal ulcers in AIDS treated with steroids is approximately 40%, but retreatment is usually successful. Leucopenia has been shown to be involved in the pathogenesis of giant ulcer in a kidney transplant recipient [7] as a result of overimmunosuppression. Our report provides the first clinical experience that a combination of reduction in immunosuppression and high-dose of acyclovir may result in a normalization of leucopenia and correction of immune imbalance, leading to rapid healing of the ulcer and a resolution of symptoms. In conclusion, giant esophageal ulcers are uncommon in kidney transplant recipients and the diagnosis of causality is often delayed. Treatment is often empirical and the aggressive nature of the disease may result in erroneous treatment decision, leading to higher patient morbidity. The correction of the immune imbalance found in these patients plays a key role in the management of giant esophageal ulcer April 14, 2016 Volume 22 Issue 14
192 Veroux M et al. Giant esophageal ulcer COMMENTS Case characteristics A 37-year-old kidney transplant recipient presented with a 1-wk history of severe odynophagia and epigastric pain, which worsened after food intake. Clinical diagnosis Cold sores, odynophagia and an inability to swallow solid food. Differential diagnosis Candida esophagitis, cytomegalovirus (CMV) or herpes simplex virus esophagitis, esophageal cancer, and gastric cancer. Laboratory diagnosis Leucocytes 1300/mm 3, and quantitative CMV-DNA polymerase chain reaction positive (10 5 copies/ml). Slight increase in serum creatinine (2.1 mg/dl). Imaging diagnosis Upper endoscopy showed a large ulcer in the distal esophagus measuring 40 mm in diameter. Pathological diagnosis Acute esophageal inflammation without any viral particles, but with positivity to Candida species. Treatment Reduction of immunosuppression and intravenous/empiric therapy with acyclovir. Related reports Idiopathic giant esophageal ulcer is very uncommon in kidney transplant recipients and it is usually related to over-immunosuppression. Treatment with high-dose steroids might result in complete healing of the ulcer. Term explanation Giant idiopathic esophageal ulcer is a rare complication of an immunosuppressed patient, which is related to a defect in immunity rather than a virus etiology in its pathogenesis. Experiences and lessons Giant idiopathic esophageal ulcer may be commonly confused for a neoplastic lesion of the esophagus. Treatment is often empirical, but correction of the immune imbalance is mandatory. Peer-review This is an interesting case report. Farrell et al reported previously the first case of giant esophageal ulceration responsive to steroids in an immunosuppressed human immunodeficiency virus negative patient. It s well written and acceptable for publication. REFERENCES 1 Ponticelli C, Passerini P. Gastrointestinal complications in renal transplant recipients. Transpl Int 2005; 18: [PMID: DOI: /j x] 2 Gautam A. Gastrointestinal complications following transplantation. Surg Clin North Am 2006; 86: , vii [PMID: DOI: /j.suc ] 3 Veroux M, Grosso G, Ekser B, Corona D, Giaquinta A, Veroux P. Impact of conversion to a once daily tacrolimus-based regimen in kidney transplant recipients with gastrointestinal complications. Transplantation 2012; 93: [PMID: DOI: /TP.0b013e318248ca90] 4 Dragean CA, Bogdan I, Azzouzzi K, Goncette L. Giant idiopathic ulcer of esophagus in the context of acquired immunodeficiency syndrome (AIDS). JBR-BTR 2013; 96: [PMID: DOI: /jbr-btr.212] 5 Siegmund B, Moos V, Loddenkemper C, Wahnschaffe U, Engelmann E, Zeitz M, Schneider T. Esophageal giant ulcer in primary human immunodeficiency virus infection is associated with an infiltration of activated T cells. Scand J Gastroenterol 2007; 42: [PMID: DOI: / ] 6 Wilcox CM, Zaki SR, Coffield LM, Greer PW, Schwartz DA. Evaluation of idiopathic esophageal ulceration for human immunodeficiency virus. Mod Pathol 1995; 8: [PMID: ] 7 Farrell JJ, Cosimi AB, Chung RT. Idiopathic giant esophageal ulcers in a renal transplant patient responsive to steroid therapy. Transplantation 2000; 70: [PMID: ] 8 van Boekel GA, Volbeda M, van den Hoogen MW, Hilbrands LB, Berden JH. Idiopathic giant oesophageal ulcer and leucopoenia after renal transplantation. Neth J Med 2012; 70: [PMID: ] 9 Wilcox CM, Schwartz DA, Clark WS. Esophageal ulceration in human immunodeficiency virus infection. Causes, response to therapy, and long-term outcome. Ann Intern Med 1995; 123: [PMID: DOI: / ] P- Reviewer: Tarnawski A S- Editor: Gong ZM L- Editor: A E- Editor: Ma S 3878 April 14, 2016 Volume 22 Issue 14
193 Submit a Manuscript: Help Desk: DOI: /wjg.v22.i World J Gastroenterol 2016 April 14; 22(14): ISSN (print) ISSN (online) 2016 Baishideng Publishing Group Inc. All rights reserved. CASE REPORT Case of metachronous bilateral isolated adrenal metastasis from colorectal adenocarcinoma and review of the literature Yu-yi Liu, Zhi-hui Chen, Er-tao Zhai, Jie Yang, Jian-bo Xu, Shi-rong Cai, Wu Song Yu-yi Liu, Zhi-hui Chen, Er-tao Zhai, Jie Yang, Jian-bo Xu, Shi-rong Cai, Wu Song, Department of Gastrointestinal Surgery, the First Affiliated Hospital, Sun Yat-sen University, Guangzhou , Guangdong Province, China Author contributions: Liu YY and Song W designed the report; Chen ZH, Zhai ET and Yang J collected the patient s clinical data; Xu JB, Cai SR and Liu YY analyzed the data and wrote the paper. Supported by grants from The Natural Science Foundation of Guangdong, No. S Institutional review board statement: The study was reviewed and approved by the First Affiliated hospital, Sun Yat-sen University Review Board. Informed consent statement: All study participants, or their legal guardian, provided informed written consent prior to study enrollment. Conflict-of-interest statement: The authors declare no conflict of interest. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: licenses/by-nc/4.0/ Correspondence to: Dr. Wu Song, Department of Gastrointestinal Surgery, the First Affiliated Hospital, Sun Yat-sen University, Zhongshan Second Road 58, Guangzhou , Guangdong Province, China. songwu@mail.sysu.edu.cn Telephone: Fax: Received: August 26, 2015 Peer-review started: August 27, 2015 First decision: September 29, 2015 Revised: October 14, 2015 Accepted: December 30, 2015 Article in press: December 30, 2015 Published online: April 14, 2016 Abstract Rarely has a solitary, metachronous bilateral adrenal metastasis of colorectal cancer been reported. We depict a 41-year-old man who underwent sigmoid colon cancer radical surgery followed by adjuvant chemotherapy for a locally ulcerative sigmoid adenocarcinoma with metachronous bilateral adrenal metastasis revealed by a computed tomography scan. Histopathological examination showed adenocarcinoma, compatible with metastasis from the rectal cancer. The level of serum carcinoembryonic antigen had indicative significance for the presence of adrenal metastasis in the reported series. We performed a literature analysis related to this pathological characteristic and attach importance to consistent, vigilant radiological surveillance of the adrenal glands in the patients follow up for colorectal cancer with or without subsequent adrenal metastasis. Key words: adrenal gland; bilateral; Colorectal cancer; metastasis; metachronous The Author(s) Published by Baishideng Publishing Group Inc. All rights reserved. Core tip: Very rarely are patients with a solitary adrenal metastasis from colorectal cancer, especially coupled with metachronous contralateral adrenal metastasis, identified. The case report not only covers a rare case of metachronous bilateral isolated adrenal metastasis from colorectal adenocarcinoma but also summarizes and discusses relevant mechanisms and therapies of this type of disease reported previously in the literature April 14, 2016 Volume 22 Issue 14
: 3879-3884 Available from: URL: http://www.")
194 Liu YY et al. Adrenal metastasis from colorectal adenocarcinoma Liu YY, Chen ZH, Zhai ET, Yang J, Xu JB, Cai SR, Song W. Case of metachronous bilateral isolated adrenal metastasis from colorectal adenocarcinoma and review of the literature. World J Gastroenterol 2016; 22(14): Available from: URL: DOI: INTRODUCTION The most common primary sites of adrenal metastatic tumors are lung, breast, and kidney, while adrenal metastases from colorectal cancer are not rare findings based on autopsy reports. However, the presence of isolated adrenal metastases from colorectal cancer was quite rare, especially when they are bilateral. We herein report a case of solitary bilateral adrenal metastasis from rectal carcinoma and review the relevant literature. CASE REPORT A 41-year-old man had a sigmoid tumor, as demonstrated by sigmoidoscopy, that was confirmed as an adenocarcinoma by subsequent biopsies. Computed tomography (CT) of the abdomen and pelvis showed no evidence of metastatic disease. A radical resection of the sigmoid colon carcinoma was performed. Histology identified a moderately differentiated ulcerative adenocarcinoma with negative surgical resection margins. The stage was pt4n2m0 (LN: 5/12) according to Tumor, Node, Metastases His postoperative serum carcinoembryonic antigen (CEA) was reduced to 2.05 μg/l (within the normal limit). Systemic chemotherapy was initiated after surgery. The patient underwent seven cycles (XELOX) with good clinical and biological tolerance. Eleven months after the completion of the adjuvant chemotherapy, thoracoabdominopelvic CT scan revealed a heterogeneous mass in the right adrenal gland, with no evidence of metastasis elsewhere (Figure 1). A total colonoscopy showed no sign of local recurrence. General blood tests, including adrenal hormones, were normal, but his serum CEA was increased markedly up to μg/l. Since chest and abdominal CT scans showed no sign of other metastatic diseases, a resection of the right adrenal neoplasm was performed without complication 18 mo following initial surgery. On macroscopic examination, the tumor, which was 80 mm 65 mm 45 mm in size, consisted of a white, solid mass with central necrosis (Figure 2a). Histopathological findings showed an atypical duct that was comprised of high columnar epithelium with necrosis within it (Figure 2b). The adrenal tumor was considered a metastasis from the sigmoid colon cancer based on comparative analysis of histopathological findings of previous sigmoid colon cancer and those of Figure 1 Abdominal enhanced computed tomography revealed a low density mass in the right adrenal gland. the adrenal tumor. Chemotherapy (XELOX) was taken back. The patient received one cycle, and his general health was good when his serum CEA was μg/l. Four months later, surveillance CT identified a left adrenal nodule (Figure 3a) and absence of the previous right adrenal mass, coupled with an expansion of the left kidney and proximal ureter. Left ureteral stent implantation was performed followed by a FOLFIRI chemotherapy regimen that was adopted for the first time. Serum CEA at this time was elevated to μg/l. The patient received four cycles of FOLFIRI with good clinical and biological tolerance. Three months after the completion of the adjuvant chemotherapy, suspicious nodules were noted in the right lung by chest radiography. Meanwhile, thoracoabdominopelvic CT scan revealed that the size of the left adrenal nodule was almost the same as previously measured (Figure 3b). In addition, imaging studies showed local recurrence at the site of the resected sigmoid and expansion to the left kidney and proximal ureter combined with mild atrophy of the left kidney. Serum CEA of the patient was μg/l. Seven months following removal of the right adrenal mass, an exploratory laparotomy, including neoplasm resection of the left adrenal, was performed. A 50 mm 35 mm 30 mm adrenal mass containing several white nodules was confirmed by histology as a moderately differentiated adenocarcinoma, compatible with the previous resected mass specimen of the right adrenal (Figure 4). DISCUSSION The incidence of adrenal metastases of primary malignancies is not rare. The most common primary sites of adrenal metastatic tumors are lung, breast, and kidney. However, adrenal metastases from colorectal carcinomas are less frequent (Table 1). The incidence of adrenal metastases from any primary carcinoma ranges from 8.6% to 27.0%, while that 3880 April 14, 2016 Volume 22 Issue 14

 of the abdomen shows a left adrenal mass; B: CT evaluation showed response of the adrenal metastases after chemotherapy.")

195 Liu YY et al. Adrenal metastasis from colorectal adenocarcinoma A B Figure 2 Adrenal tumor. A: Macroscopic findings of the adrenal lesion showed a solid tumor with necrosis; B: Microscopic findings of the adrenal tumor showed moderately differentiated adenocarcinoma that resembles the primary sigmoid lesion that had been resected. This indicated that the metastasis was from the sigmoid carcinoma. A B Figure 3 Computed tomography image. A: Computed tomography (CT) of the abdomen shows a left adrenal mass; B: CT evaluation showed response of the adrenal metastases after chemotherapy. Figure 4 Pathological findings of the left adrenal tumor showed moderately differentiated adenocarcinoma, compatible with metastasis from the rectal carcinoma. from a colorectal malignant lesion ranges between 1.9% and 17.4% [1]. However, this incidence may be underestimated because of the adrenal mass being mistaken for a lombo-aortic node [1]. A previous study reported that of 47 patients (17%) who received an adrenalectomy for metastatic cancers, eight patients adrenal metastases were derived from colorectal cancer [2]. Moreover, another study addressing fine needle aspiration of adrenal masses showed that five of 39 adrenal metastatic malignancies cases (12.8%) originated from colorectal cancer [3]. Lam et al [4] described the prevalence of colorectal cancer in adrenal metastases in both autopsy and biopsy series. Around 5% of metastases were from large intestinal primary sites in an Asian series [4]. In spite of a discrepancy within the reported literature, it is conceivable that the incidence of adrenal metastases from colorectal carcinomas is not rare. Several studies 3881 April 14, 2016 Volume 22 Issue 14
196 Liu YY et al. Adrenal metastasis from colorectal adenocarcinoma Table 1 Reported adrenal metastasis from colorectal carcinoma Ref. No. of adrenal metastasis from colorectal carcinoma Total No. of adrenal metastasis Percentage Cedermark et al [1] % Kim et al [24] % Lo et al [7] % Moreno-Elola et al [8] 1 1 Katayama et al [5] 1 1 Watatani et al [9] 3 3 Candel et al [3] % Wade et al [2] % have demonstrated that the vast majority of autopsies with adrenal metastases also involved metastases of multiple other sites. It is acknowledged that the spread of adrenal metastases occurs via the arterial, portal venous, or lymphatic routes. Generally, hematogenous spread is considered the major route of primary carcinoma metastasis to the adrenal. Katayama et al [5] described a plausible route of hematogenous metastasis from the primary site via the lungs to the adrenals. Although the lung metastasis in our patient was not detected until after the left adrenal metastasis, it is possible that a silent lung metastasis had gradually occurred when the adrenal metastasis was detected. In general, adrenal metastasis is thought to indicate widespread disease; and, hence, patients with a solitary adrenal metastasis from colorectal carcinoma are rare, especially coupled with metachronous contralateral adrenal metastasis, according to our review of the literature [5-10]. Serum CEA is thought to be essential in predicting the presence of adrenal metastasis in the postoperative period of colorectal cancer [5,9,10]. As in our patient, serum CEA levels indicated the presence of adrenal metastases in the reported series, which was confirmed by the imaging findings. Therefore, early detection and resection of the adrenal metastasis based on regular follow-up could improve the prognosis to some extent despite systemic diseases. In addition, attention should be paid to the occurrence of adrenal metastasis series after a relatively long-term course. However, there have been multiple cases in which serum CEA level remains within the normal range in spite of an occurrence of adrenal metastasis [11-13]. Therefore, a variety of modalities combined with serum CEA levels should be applied to accurately detect the status of colorectal cancer. The past several years have witnessed a substantial improvement in the detection of clinically quiescent adrenal masses owing to the common use of imaging modalities such as CT, positron emission tomography (PET) CT, and magnetic resonance imaging (MRI). Among various radiological studies used to assess adrenal metastases, CT and ultrasonography are prevalently preferred due to their wide applicability and non-invasive nature [14]. On CT, our patient displayed low density of the adrenal gland, consistent with adrenal masses in other reports [3,15,16]. CT scan allows for diagnosis of the adrenal masses with accuracy to sub-centimetric lesions. However, it fails to distinguish between primary lesions, incidentalomas, or secondary lesions. Percutaneous fine needle-biopsy was, therefore, proposed for the differential diagnosis by attaining histological confirmation [17]. This procedure was not performed on our patient since the CT characteristics and the story of the disease were sufficient to support the diagnosis of adrenal metastases. MRI is also an effective procedure for appraising the tumors in adrenal glands. It plays a significant role in distinguishing between adenoma, carcinoma, and metastasis in cases of adrenal incidentaloma. On the other hand, it allows for identification of the functional nature of the adrenal mass when an adrenal incidentaloma is found [18,19]. The emergence of PET-CT for detection and surveillance has allowed for more accurate specifics of adrenal metastases, with better characterizations of the metabolic activities. This approach permits choosing an adapted treatment and avoiding a useless laparotomy in cases of generalized metastases [20,21]. Adrenal metastasis from colorectal malignancy is not uncommon in autopsy series. Therefore, adrenal metastasis should be tested in the follow-up of colorectal cancer patients who undergo an initial surgery, even though the lung and liver are the primary metastatic sites. For early detection of adrenal metastasis, measuring of serum CEA and imaging examination, such as ultrasonography and CT, should be done routinely. Although it is generally thought that an adrenal metastasis is part of a widespread metastasis [8,22,23], the secondary adrenal gland lesions may be involved in the lung metastases and even neoplastic invasion of other organs without negative effect on the prognosis [24]. A resection of the involved adrenal gland is supposed to contribute to a good prognosis when a separate adrenal metastasis is found [8-10]. Therefore, it is essential to make allowance for the possibility of adrenal metastasis from colorectal cancer, especially a delayed contralateral adrenal metastasis when unilateral adrenal was implicated, during follow-up after the primary operation. Our patient is currently in stable condition, and further surveillance is needed because this case has been observed for only half a year. In conclusion, it is suggested in this case that separate, metachronous metastases in bilateral adrenal glands may not achieve desired results through chemotherapy alone but surgical resection and continual follow-up as well. A number of cases of similar adrenal metastasis are needed to elucidate this issue April 14, 2016 Volume 22 Issue 14
197 Liu YY et al. Adrenal metastasis from colorectal adenocarcinoma COMMENTS Case characteristics A 41-year-old man presented with metachronous bilateral adrenal metastases with a history of sigmoid tumor resection and chemotherapy. Clinical diagnosis Bilateral adrenal metastases from sigmoid tumor. Differential diagnosis Pheochromocytoma and adrenocortical carcinoma Laboratory diagnosis All of the laboratory results were within the normal ranges, with the exception of a fluctuant carcinoembryonic antigen level. Imaging diagnosis Abdominal computed tomography demonstrated heterogeneous masses in bilateral adrenal glands heterochronously. Pathological diagnosis Bilateral adrenal tumors were confirmed as a metastasis from the sigmoid colon cancer through comparative analysis of histopathological findings of previous sigmoid colon cancers and those of the adrenal tumors. Treatment Resection of bilateral adrenal tumor with chemotherapy. Experiences and lessons This report presents a rare case of metachronous bilateral adrenal metastases from colorectal cancer and improves our understanding of this disease process. Peer-review This rare case indicates that resection of the involved adrenal gland improves prognosis when a separate adrenal metastasis is found. Additionally, it is essential to consider the possibility of adrenal metastasis from colorectal cancer during follow-up after the primary operation. REFERENCES 1 Murakami S, Terakado M, Hashimoto T, Tsuji Y, Okubo K, Hirayama R. Adrenal metastasis from rectal cancer: report of a case. Surg Today 2003; 33: [PMID: DOI: /s ] 2 Wade TP, Longo WE, Virgo KS, Johnson FE. A comparison of adrenalectomy with other resections for metastatic cancers. Am J Surg 1998; 175: [PMID: DOI: /S (97)00281-X] 3 Candel AG, Gattuso P, Reyes CV, Prinz RA, Castelli MJ. Fineneedle aspiration biopsy of adrenal masses in patients with extraadrenal malignancy. Surgery 1993; 114: ; discussion [PMID: ] 4 Lam KY, Lo CY. Metastatic tumours of the adrenal glands: a 30-year experience in a teaching hospital. Clin Endocrinol (Oxf) 2002; 56: [PMID: DOI: /j x] 5 Katayama A, Mafune K, Makuuchi M. Adrenalectomy for solitary adrenal metastasis from colorectal carcinoma. Jpn J Clin Oncol 2000; 30: [PMID: DOI: /jjco/hyd104] 6 Omoigui NA, Cave WT, Chang AY. Adrenal insufficiency. A rare initial sign of metastatic colon carcinoma. J Clin Gastroenterol 1987; 9: [PMID: DOI: / ] 7 Lo CY, van Heerden JA, Soreide JA, Grant CS, Thompson GB, Lloyd RV, Harmsen WS. Adrenalectomy for metastatic disease to the adrenal glands. Br J Surg 1996; 83: [PMID: DOI: /bjs ] 8 Moreno-Elola A, Moreno-Gonzalez E, Alonso-Casado O, Meneu-Diaz JC, García-García I, Abradelo-Usera M. Exceptional bilateral adrenalectomy after secondaries from colorectal cancer. Hepatogastroenterology 2004; 51: [PMID: ] 9 Watatani M, Ooshima M, Wada T, Terashita H, Matsuda T, Shindo K, Yasutomi M. Adrenal metastasis from carcinoma of the colon and rectum: a report of three cases. Surg Today 1993; 23: [PMID: DOI: /BF ] 10 Fujita K, Kameyama S, Kawamura M. Surgically removed adrenal metastasis from cancer of the rectum. Report of a case. Dis Colon Rectum 1988; 31: [PMID: DOI: / BF ] 11 Thrumurthy SG, Jadav AM, Pitt M, Dobson M, Hearn A, Scott NA, Susnerwala SS. Metachronous bilateral adrenal metastases following curative treatment for colorectal carcinoma. Ann R Coll Surg Engl 2011; 93: e96-e98 [PMID: DOI: / X591134] 12 Jabir H, Tawfiq N, Moukhlissi M, Akssim M, Guensi A, Kadiri B, Bouchbika Z, Taleb A, Benchekroun N, Jouhadi H, Sahraoui S, Zamiati S, Benider A. Metachronous bilateral isolated adrenal metastasis from rectal adenocarcinoma: a case report. Case Rep Gastrointest Med 2014; 2014: [PMID: DOI: /2014/516403] 13 Capaldi M, Ricci G, Bertolini R, Alessandroni L, Di Castro A, Saraco E, Guiducci A, Tersigni R. Colon cancer adrenal metastasis: case report and review of the literature. G Chir 2011; 32: [PMID: ] 14 Francis IR, Smid A, Gross MD, Shapiro B, Naylor B, Glazer GM. Adrenal masses in oncologic patients: functional and morphologic evaluation. Radiology 1988; 166: [PMID: DOI: /radiology ] 15 Chezmar JL, Robbins SM, Nelson RC, Steinberg HV, Torres WE, Bernardino ME. Adrenal masses: characterization with T1- weighted MR imaging. Radiology 1988; 166: [PMID: DOI: /radiology ] 16 Brunt LM, Moley JF. Adrenal incidentaloma. World J Surg 2001; 25: [PMID: DOI: /s ] 17 Terzolo M, Ali A, Osella G, Mazza E. Prevalence of adrenal carcinoma among incidentally discovered adrenal masses. A retrospective study from 1989 to Gruppo Piemontese Incidentalomi Surrenalici. Arch Surg 1997; 132: [PMID: DOI: /archsurg ] 18 Sheeler LR, Myers JH, Eversman JJ, Taylor HC. Adrenal insufficiency secondary to carcinoma metastatic to the adrenal gland. Cancer 1983; 52: [PMID: DOI: / ( )52:7<1312::AID-CNCR >3.0.CO;2-O] 19 Chong S, Lee KS, Kim HY, Kim YK, Kim BT, Chung MJ, Yi CA, Kwon GY. Integrated PET-CT for the characterization of adrenal gland lesions in cancer patients: diagnostic efficacy and interpretation pitfalls. Radiographics 2006; 26: ; discussion [PMID: DOI: / rg ] 20 Votrubova J, Belohlavek O, Jaruskova M, Oliverius M, Lohynska R, Trskova K, Sedlackova E, Lipska L, Stahalova V. The role of FDG-PET/CT in the detection of recurrent colorectal cancer. Eur J Nucl Med Mol Imaging 2006; 33: [PMID: DOI: /s z] 21 Wade TP, Virgo KS, Li MJ, Callander PW, Longo WE, Johnson FE. Outcomes after detection of metastatic carcinoma of the colon and rectum in a national hospital system. J Am Coll Surg 1996; 182: [PMID: ] 22 Berge T, Ekelund G, Mellner C, Pihl B, Wenckert A. Carcinoma of the colon and rectum in a defined population. An epidemiological, clinical and postmortem investigation of colorectal carcinoma and coexisting benign polyps in Malmö, Sweden. Acta Chir Scand Suppl 1973; 438: 1-86 [PMID: ] 23 Cedermark BJ, Blumenson LE, Pickren JW, Holyoke DE, Elias EG. Ths significance of metastases to the adrenal glands in 3883 April 14, 2016 Volume 22 Issue 14
198 Liu YY et al. Adrenal metastasis from colorectal adenocarcinoma adenocarcinoma of the colon and rectum. Surg Gynecol Obstet 1977; 144: [PMID: ] 24 Kim SH, Brennan MF, Russo P, Burt ME, Coit DG. The role of surgery in the treatment of clinically isolated adrenal metastasis. Cancer 1998; 82: [PMID: DOI: /(SICI) ( )82:2<395::AID-CNCR20>3.3.CO;2-E] P- Reviewer: Lam AK S- Editor: Gong ZM L- Editor: Filipodia E- Editor: Ma S 3884 April 14, 2016 Volume 22 Issue 14


199 Published by Baishideng Publishing Group Inc 8226 Regency Drive, Pleasanton, CA 94588, USA Telephone: Fax: Help Desk: I S S N Baishideng Publishing Group Inc. All rights reserved.
Genome-wide association study of esophageal squamous cell carcinoma in Chinese subjects identifies susceptibility loci at PLCE1 and C20orf54
 CORRECTION NOTICE Nat. Genet. 42, 759 763 (2010); published online 22 August 2010; corrected online 27 August 2014 Genome-wide association study of esophageal squamous cell carcinoma in Chinese subjects
CORRECTION NOTICE Nat. Genet. 42, 759 763 (2010); published online 22 August 2010; corrected online 27 August 2014 Genome-wide association study of esophageal squamous cell carcinoma in Chinese subjects
Members of The Chinese Medicine Council of Hong Kong, Chinese Medicine Practitioners Board, Chinese Medicines Board and its Committees
 Members of The Chinese Medicine Council of Hong Kong, Chinese Medicine Practitioners Board, Chinese Medicines Board and its Committees and of the Chinese Medicine Council of Hong Kong (e) (f) (g) a chairman;
Members of The Chinese Medicine Council of Hong Kong, Chinese Medicine Practitioners Board, Chinese Medicines Board and its Committees and of the Chinese Medicine Council of Hong Kong (e) (f) (g) a chairman;
EMPEROR'S COLLEGE MTOM COURSE SYLLABUS HERB FORMULAE II
 COURSE DESCRIPTION The second of three courses in the Herb Formulae series. Categories covered in Formulae II include the Tonify Qi and Blood, Regulate Qi, Invigorate the Blood, Stop Bleeding, Stabilize
COURSE DESCRIPTION The second of three courses in the Herb Formulae series. Categories covered in Formulae II include the Tonify Qi and Blood, Regulate Qi, Invigorate the Blood, Stop Bleeding, Stabilize
EMPEROR'S COLLEGE MTOM COURSE SYLLABUS HERB FORMULAE I
 COURSE DESCRIPTION The first of three courses in the Herb Formulae series. These courses can be taken in any order. The Herb Formulae series analyzes the functions, ingredients, and properties of approximately
COURSE DESCRIPTION The first of three courses in the Herb Formulae series. These courses can be taken in any order. The Herb Formulae series analyzes the functions, ingredients, and properties of approximately
Root & Branch Bulk Formula List
 An asterisk * indicates the inclusion of 1 or more granule versions of an herb because of limited availability on the American herbal market. These products are usually animal in nature like E Jiao, Shui
An asterisk * indicates the inclusion of 1 or more granule versions of an herb because of limited availability on the American herbal market. These products are usually animal in nature like E Jiao, Shui
Appendix 5 Members of the Chinese Medicine Council of Hong. Kong, Chinese Medicine Practitioners Board, Chinese
 Appendix 5 Members of the Chinese Medicine Council of Hong Kong, Chinese Medicine Practitioners Board, Chinese Medicines Board and its Committees and of the Chinese Medicine Council of Hong Kong a chairman;
Appendix 5 Members of the Chinese Medicine Council of Hong Kong, Chinese Medicine Practitioners Board, Chinese Medicines Board and its Committees and of the Chinese Medicine Council of Hong Kong a chairman;
Liu Jing and Liu Jing Diagnosis System in Classical TCM Discussions of Six Divisions or Six Confirmations Diagnosis System in Classical TCM Texts
 Liu Jing and Liu Jing Diagnosis System in Classical TCM Discussions of Six Divisions or Six Confirmations Diagnosis System in Classical TCM Texts Liu Jing Bian Zheng system had developed about 1800 years
Liu Jing and Liu Jing Diagnosis System in Classical TCM Discussions of Six Divisions or Six Confirmations Diagnosis System in Classical TCM Texts Liu Jing Bian Zheng system had developed about 1800 years
Preliminary Agenda. 9:55-10:20 How to overcome TKI resistance? James Chih-Hsin Yang 10:20-10:40 Discussion All 10:40-10:55 Coffee break
 Preliminary Agenda November 7, 2018 14:00-17:00 Registration and check in Satellite Symposia with Dinner 17:00-18:30 Jiangsu Hengrui Medicine Co., Ltd 17:00-18:30 Satellite Symposia with Dinner 17:00-18:30
Preliminary Agenda November 7, 2018 14:00-17:00 Registration and check in Satellite Symposia with Dinner 17:00-18:30 Jiangsu Hengrui Medicine Co., Ltd 17:00-18:30 Satellite Symposia with Dinner 17:00-18:30
World Journal of Gastrointestinal Pharmacology and Therapeutics
 ISSN 2150-5349 (online) World Journal of Gastrointestinal Pharmacology and Therapeutics World J Gastrointest Pharmacol Ther 2017 November 6; 8(4): 193-209 Published by Baishideng Publishing Group Inc Contents
ISSN 2150-5349 (online) World Journal of Gastrointestinal Pharmacology and Therapeutics World J Gastrointest Pharmacol Ther 2017 November 6; 8(4): 193-209 Published by Baishideng Publishing Group Inc Contents
Journal of Chinese Medicine. Vol.20, No.1, Vol.20, No.3,
 163 Journal of Chinese Medicine Vol.20, No.1,2 1-96 Vol.20, No.3,4 97-162 ~ - 145 45-135 21 117 79-19 137-135 ~ - 137 65 87-65 - 145-65 - 153-79 - 153-87 47-137 - 65-87 - 47-145 - 145-47 - 19 164 153 HT7
163 Journal of Chinese Medicine Vol.20, No.1,2 1-96 Vol.20, No.3,4 97-162 ~ - 145 45-135 21 117 79-19 137-135 ~ - 137 65 87-65 - 145-65 - 153-79 - 153-87 47-137 - 65-87 - 47-145 - 145-47 - 19 164 153 HT7
The 1 st Congress of Asian Society of Cardiovascular Imaging
 The 1 st Congress of Asian Society of Cardiovascular Imaging April 27 (Friday) ~ April 28 (Saturday), 2007 Asan Medical Center, Seoul, Korea Number of Participants : 545 Participants from 26 Countries
The 1 st Congress of Asian Society of Cardiovascular Imaging April 27 (Friday) ~ April 28 (Saturday), 2007 Asan Medical Center, Seoul, Korea Number of Participants : 545 Participants from 26 Countries
Index : Bridging Asia to the World- A New Era for Psychiatric Treatment
 1 Index : 2 3 Mood disorders President Tung-Ping Su Honorary president Shigeto Yamawaki Division of Psychiatry, Faculty of Medicine, National Yang-Ming University Department of Psychiatry and Neurosciences,
1 Index : 2 3 Mood disorders President Tung-Ping Su Honorary president Shigeto Yamawaki Division of Psychiatry, Faculty of Medicine, National Yang-Ming University Department of Psychiatry and Neurosciences,
Agenda of the 5 th Hong Kong International Oncology Symposium
 Day 1 Program of the 5 th HKIOS (10 th November 2018) Venue: The Hong Kong Science Park Time Name of Speaker Name of Presentation Topic Affiliations of the Speaker 08:40 08:50 Joseph Siu Kie AU Welcome
Day 1 Program of the 5 th HKIOS (10 th November 2018) Venue: The Hong Kong Science Park Time Name of Speaker Name of Presentation Topic Affiliations of the Speaker 08:40 08:50 Joseph Siu Kie AU Welcome
Name List of Scout of the Year
 Name List of Scout of the Year Name Sex Section Group Year of Award 1. Jimmy TONG Chun-kuen M Cub Scout 14 th Hong Kong Group 1987 2. YIP Chi-kwong M Scout 98 th Kowloon Group 1987 3. Wilfred MAK Wai-fung
Name List of Scout of the Year Name Sex Section Group Year of Award 1. Jimmy TONG Chun-kuen M Cub Scout 14 th Hong Kong Group 1987 2. YIP Chi-kwong M Scout 98 th Kowloon Group 1987 3. Wilfred MAK Wai-fung
Current Issues of Chronic Hepatitis B
 June 22 (Fri), 2018 Postgraduate Course (I) Current Issues of Chronic Hepatitis B Room 201 13:20-15:00 Wan-Long Chuang (Kaohsiung)/ Han-Chieh Lin () 13:20-13:45 PG-1 Experience from HCV Cure Chen-Hua Liu
June 22 (Fri), 2018 Postgraduate Course (I) Current Issues of Chronic Hepatitis B Room 201 13:20-15:00 Wan-Long Chuang (Kaohsiung)/ Han-Chieh Lin () 13:20-13:45 PG-1 Experience from HCV Cure Chen-Hua Liu
Undetectable = Untransmittable. Mariah Wilberg Communications Specialist
 Undetectable = Untransmittable Mariah Wilberg Communications Specialist Undetectable=Untransmittable PLWH who get and stay undetectable have effectively no risk of transmitting HIV to their sex partners
Undetectable = Untransmittable Mariah Wilberg Communications Specialist Undetectable=Untransmittable PLWH who get and stay undetectable have effectively no risk of transmitting HIV to their sex partners
Terms and Conditions. VISA Global Customer Assistance Services
 Terms and Conditions VISA Global Customer Assistance Services Visa Global Customer Assistance Services (VGCAS) 1 The Visa Global Customer Assistance Services are co-ordinated by the Global Assistance Centre
Terms and Conditions VISA Global Customer Assistance Services Visa Global Customer Assistance Services (VGCAS) 1 The Visa Global Customer Assistance Services are co-ordinated by the Global Assistance Centre
National & International Lectures
 2005-2008 National & International Lectures 6/24/05 ECFS Crete, Greece Mucoid Psuedomonas aeruginosa Infection, Antibiotic Resistance, and Lung Disease Progression in Children with Cystic Fibrosis 9/30/05
2005-2008 National & International Lectures 6/24/05 ECFS Crete, Greece Mucoid Psuedomonas aeruginosa Infection, Antibiotic Resistance, and Lung Disease Progression in Children with Cystic Fibrosis 9/30/05
Name List of Scout of the Year
 Name List of Scout of the Year Name Sex Section Group Year of Award 1. Jimmy TONG Chun-kuen M Cub Scout 14 th Hong Kong Group 1987 2. YIP Chi-kwong M Scout 98 th Kowloon Group 1987 3. Wilfred MAK Wai-fung
Name List of Scout of the Year Name Sex Section Group Year of Award 1. Jimmy TONG Chun-kuen M Cub Scout 14 th Hong Kong Group 1987 2. YIP Chi-kwong M Scout 98 th Kowloon Group 1987 3. Wilfred MAK Wai-fung
Welcome Message. We look forward to seeing you in Nanjing in Welcome to Nanjing! Sincerely yours,
 Welcome Message On behalf of the organising committee, it gives us immense pleasure to invite you to participate in the 6th ISMAAR World Congress on Mild Approaches in Assisted Reproduction, which will
Welcome Message On behalf of the organising committee, it gives us immense pleasure to invite you to participate in the 6th ISMAAR World Congress on Mild Approaches in Assisted Reproduction, which will
Seasonal and geographical dispersal regularity of airborne pollens in China LI Quan-sheng, JIANG Sheng-xue, LI Xin-ze, ZHU Xiao-ming, WEI Qing-yu *
 Med J Chin PLA, Vol. 42, No. 11, November 1, 2017 951 [] [ ] [ ] R562.25[ ] A[] 0177-7402(2017)11-0951-05 [DOI] 10.11855/j.issn.0577-7402.2017.11.03 Seasonal and geographical dispersal regularity of airborne
Med J Chin PLA, Vol. 42, No. 11, November 1, 2017 951 [] [ ] [ ] R562.25[ ] A[] 0177-7402(2017)11-0951-05 [DOI] 10.11855/j.issn.0577-7402.2017.11.03 Seasonal and geographical dispersal regularity of airborne
FOUNDATIONS, ACUPUNCTURE, CHINESE HERBAL MEDICINE, BIO-MEDICINE. Stage Four Review
 ICAOM LEARNING PROFICIENCY EXAMINATION FOUNDATIONS, ACUPUNCTURE, CHINESE HERBAL MEDICINE, BIO-MEDICINE Review and know the following: Stage Four Review 1. Familiar with the disease or symptom of the following
ICAOM LEARNING PROFICIENCY EXAMINATION FOUNDATIONS, ACUPUNCTURE, CHINESE HERBAL MEDICINE, BIO-MEDICINE Review and know the following: Stage Four Review 1. Familiar with the disease or symptom of the following
EU Market Situation for Poultry. Committee for the Common Organisation of the Agricultural Markets 20 April 2017
 EU Market Situation for Poultry Committee for the Common Organisation of the Agricultural Markets 2 April 217 -9.% -11.% -5.% -.1% -.7% -2.2% 3.% 1.7% 1.2%.8%.6%.%.%.% 7.9% 7.% 6.4% 6.2% 6.% 5.5% 5.3%
EU Market Situation for Poultry Committee for the Common Organisation of the Agricultural Markets 2 April 217 -9.% -11.% -5.% -.1% -.7% -2.2% 3.% 1.7% 1.2%.8%.6%.%.%.% 7.9% 7.% 6.4% 6.2% 6.% 5.5% 5.3%
World Journal of Hepatology
 ISSN 1948-5182 (online) World Journal of Hepatology World J Hepatol 2017 July 18; 9(20): 867-906 Published by Baishideng Publishing Group Inc Contents Three issues per month Volume 9 Number 20 July 18,
ISSN 1948-5182 (online) World Journal of Hepatology World J Hepatol 2017 July 18; 9(20): 867-906 Published by Baishideng Publishing Group Inc Contents Three issues per month Volume 9 Number 20 July 18,
Edited by Annamária Kis with the cooperation of Dr. Gábor Papp, Prof. Ekkehart Tillmanns, Dr. Tamás G. Weiszburg
 2 nd Report of the IMA Archive Edited by Annamária Kis with the cooperation of Dr. Gábor Papp, Prof. Ekkehart Tillmanns, Dr. Tamás G. Weiszburg 1 st Business Meeting 2 nd European Mineralogical Conference,
2 nd Report of the IMA Archive Edited by Annamária Kis with the cooperation of Dr. Gábor Papp, Prof. Ekkehart Tillmanns, Dr. Tamás G. Weiszburg 1 st Business Meeting 2 nd European Mineralogical Conference,
Prostate Disease A Pass By TANG QIAN LI ZHU BIAN
 Prostate Disease A Pass By TANG QIAN LI ZHU BIAN Oxytocin and the Human Prostate in Health and - and PSA is then able to pass into the proliferation within the normal prostate. 4.4. Oxytocin and prostate
Prostate Disease A Pass By TANG QIAN LI ZHU BIAN Oxytocin and the Human Prostate in Health and - and PSA is then able to pass into the proliferation within the normal prostate. 4.4. Oxytocin and prostate
Recommended composition of influenza virus vaccines for use in the 2007 influenza season
 Recommended composition of influenza virus vaccines for use in the 2007 influenza season September 2006 This recommendation relates to the composition of vaccines for the forthcoming winter in the southern
Recommended composition of influenza virus vaccines for use in the 2007 influenza season September 2006 This recommendation relates to the composition of vaccines for the forthcoming winter in the southern
Translational Lung Cancer Research, the 7 th AME Journal indexed in SCIE
 News Translational Lung Cancer Research, the 7 th AME Journal indexed in SCIE Editorial Office Editorial Office of Translational Lung Cancer Research, AME Publishing Company, Hong Kong, China Correspondence
News Translational Lung Cancer Research, the 7 th AME Journal indexed in SCIE Editorial Office Editorial Office of Translational Lung Cancer Research, AME Publishing Company, Hong Kong, China Correspondence
TGH Annual Report (2016) Editorial Office
 Editorial Office") TGH Annual Report (2016) Editorial Office tgh@amegroups.com Outline of the Report 1.Basic Information 2.Editor-in-Chief 3.Message from the EIC 4.Distribution of Editorial Board Members 5.Number of Published
TGH Annual Report (2016) Editorial Office tgh@amegroups.com Outline of the Report 1.Basic Information 2.Editor-in-Chief 3.Message from the EIC 4.Distribution of Editorial Board Members 5.Number of Published
Emily J. Hadgkiss, 1 George A. Jelinek, 1,2 Tracey J. Weiland, 1,3 Naresh G. Pereira, 4 Claudia H. Marck, 1 and Dania M.
 Neurology Research International Volume 2013, Article ID 129417, 5 pages http://dx.doi.org/10.1155/2013/129417 Erratum Erratum to Methodology of an International Study of People with Multiple Sclerosis
Neurology Research International Volume 2013, Article ID 129417, 5 pages http://dx.doi.org/10.1155/2013/129417 Erratum Erratum to Methodology of an International Study of People with Multiple Sclerosis
Sperm donation Oocyte donation. Hong Kong þ Guideline þ þ Hungary þ þ þ þ Israel þ þ þ þ Italy þ þ þ. Germany þ þ þ þ Greece þ þ þ þ
 CHAPTER 8: Donation Although there has been a reduction in the use of donor sperm because of ICSI and the impact of the removal of anonymity in some countries (1), sperm donation is still used and has
CHAPTER 8: Donation Although there has been a reduction in the use of donor sperm because of ICSI and the impact of the removal of anonymity in some countries (1), sperm donation is still used and has
Cancer incidence and patient survival rates among the residents in the Pudong New Area of Shanghai between 2002 and 2006
 Chinese Journal of Cancer Original Article Cancer incidence and patient survival rates among the residents in the Pudong New Area of Shanghai between 2002 and 2006 Xiao-Pan Li 1, Guang-Wen Cao 2, Qiao
Chinese Journal of Cancer Original Article Cancer incidence and patient survival rates among the residents in the Pudong New Area of Shanghai between 2002 and 2006 Xiao-Pan Li 1, Guang-Wen Cao 2, Qiao
WELLNESS COACHING. Wellness & Personal Fitness Solution Providers
 WELLNESS COACHING Wellness & Personal Fitness Solution Providers Introducing Ourselves... We are Personal Wellness Coaches 2 We help people look and feel better by: - Educating on proper nutrition (80%)
WELLNESS COACHING Wellness & Personal Fitness Solution Providers Introducing Ourselves... We are Personal Wellness Coaches 2 We help people look and feel better by: - Educating on proper nutrition (80%)
Hepatitis C Virus Disease
 Hepatitis C Virus Disease Emilio Jirillo Editor Hepatitis C Virus Disease Immunobiology and Clinical Applications Editor Emilio Jirillo University of Bari and National Institute for Digestive Disease Castellana
Hepatitis C Virus Disease Emilio Jirillo Editor Hepatitis C Virus Disease Immunobiology and Clinical Applications Editor Emilio Jirillo University of Bari and National Institute for Digestive Disease Castellana
CORRELATION BETWEEN SURVIVIN OVEREXPRESSION AND CLINICO-PATHOLOGICAL FEATURES OF INVASIVE CERVICAL CANCER: A META-ANALYSIS
 Acta Medica Mediterranea, 2018, 34: 1091 CORRELATION BETWEEN SURVIVIN OVEREXPRESSION AND CLINICO-PATHOLOGICAL FEATURES OF INVASIVE CERVICAL CANCER: A META-ANALYSIS HUI-RONG LI 1, JI-LI BAI 2*, RUI XU 2,
Acta Medica Mediterranea, 2018, 34: 1091 CORRELATION BETWEEN SURVIVIN OVEREXPRESSION AND CLINICO-PATHOLOGICAL FEATURES OF INVASIVE CERVICAL CANCER: A META-ANALYSIS HUI-RONG LI 1, JI-LI BAI 2*, RUI XU 2,
2011 International Conference of Inflammation, Cancer and Metabolic Disorders Program
 Friday, November 4 th, 2011 09:00-09:30 Registration 09:30-09:40 Welcome & Opening Remarks Kenneth K. Wu, M.D., Ph.D. Fu-Tong Liu, M.D., Ph.D. Plenary Lecture I Chair: Kenneth K. Wu, M.D., Ph.D. 09:40-10:40
Friday, November 4 th, 2011 09:00-09:30 Registration 09:30-09:40 Welcome & Opening Remarks Kenneth K. Wu, M.D., Ph.D. Fu-Tong Liu, M.D., Ph.D. Plenary Lecture I Chair: Kenneth K. Wu, M.D., Ph.D. 09:40-10:40
Global EHS Resource Center
 Global EHS Resource Center Understand environmental and workplace safety requirements that affect your global operations. 800.372.1033 bna.com/gelw Global EHS Resource Center This comprehensive research
Global EHS Resource Center Understand environmental and workplace safety requirements that affect your global operations. 800.372.1033 bna.com/gelw Global EHS Resource Center This comprehensive research
Main developments in past 24 hours
 ECDC DAILY UPDATE Pandemic (H1N1) 2009 Update 02 October 2009, 09:00 hours CEST Main developments in past 24 hours Weekly Influenza Surveillance Overview to be published today; Media highlights and Eurosurveillance
ECDC DAILY UPDATE Pandemic (H1N1) 2009 Update 02 October 2009, 09:00 hours CEST Main developments in past 24 hours Weekly Influenza Surveillance Overview to be published today; Media highlights and Eurosurveillance
HBSN Annual Report (2016) Editorial Office
 Editorial Office") HBSN Annual Report (2016) Editorial Office editor@thehbsn.org Basic Information Open-access Peer-reviewed Published Bi-monthly 2012: Launched in Dec. 2014: Indexed in PubMed/PMC 2016: Indexed in ESCI New
HBSN Annual Report (2016) Editorial Office editor@thehbsn.org Basic Information Open-access Peer-reviewed Published Bi-monthly 2012: Launched in Dec. 2014: Indexed in PubMed/PMC 2016: Indexed in ESCI New
ESPEN-LLL. Schedule of Live courses for Wroclaw, Poland,
 ESPEN-LLL Schedule of Live courses for 2016 Wroclaw, Poland, 09. 01. 2016 (Responsible: K. Matysiak-Luśnia, email: mi_anest@op.pl) - Approach to oral and enteral nutrition - Approach to parenteral nutrition
ESPEN-LLL Schedule of Live courses for 2016 Wroclaw, Poland, 09. 01. 2016 (Responsible: K. Matysiak-Luśnia, email: mi_anest@op.pl) - Approach to oral and enteral nutrition - Approach to parenteral nutrition
REGIONAL OFFICE FOR THE WESTERN PACIFIC BUREAU REGIONAL DU PACIFIQUE OCCIDENTAL
 W O R L D H E A L T H ORGANIZATION ORGANISATIONS MONDIALE DE LA SANTE REGIONAL OFFICE FOR THE WESTERN PACIFIC BUREAU REGIONAL DU PACIFIQUE OCCIDENTAL EXPERTS' CONSULTATION MEETING WPR/DHS/EMT(2)/2010/IB/2
W O R L D H E A L T H ORGANIZATION ORGANISATIONS MONDIALE DE LA SANTE REGIONAL OFFICE FOR THE WESTERN PACIFIC BUREAU REGIONAL DU PACIFIQUE OCCIDENTAL EXPERTS' CONSULTATION MEETING WPR/DHS/EMT(2)/2010/IB/2
Gastrointestinal Oncology
 2 nd MD ANDERSON INTERNATIONAL MEETING IN Gastrointestinal Oncology CURRENT PRACTICE AND CONTROVERSIES in the Era of Personalized Medicine e Madrid, 13 th -15 th November, 2019 SCIENTIFIC PROGRAM Meeting
2 nd MD ANDERSON INTERNATIONAL MEETING IN Gastrointestinal Oncology CURRENT PRACTICE AND CONTROVERSIES in the Era of Personalized Medicine e Madrid, 13 th -15 th November, 2019 SCIENTIFIC PROGRAM Meeting
Medical Radiology. Diagnostic Imaging
 Medical Radiology Diagnostic Imaging Series editors Hans-Ulrich Kauczor Hedvig Hricak Michael Knauth Editorial board Andy Adam, London Fred Avni, Brussels Richard L. Baron, Chicago Carlo Bartolozzi, Pisa
Medical Radiology Diagnostic Imaging Series editors Hans-Ulrich Kauczor Hedvig Hricak Michael Knauth Editorial board Andy Adam, London Fred Avni, Brussels Richard L. Baron, Chicago Carlo Bartolozzi, Pisa
Country Length Discount Travel Period Anguilla All 20% off 08/24/11 12/15/11 Antigua All 20% off 08/24/11 12/15/11 Argentina All 20% off 08/24/11
 Country Length Discount Travel Period Anguilla All 20% off 08/24/11 12/15/11 Antigua All 20% off 08/24/11 12/15/11 Argentina All 20% off 08/24/11 12/15/11 Aruba All 20% off 08/24/11 12/15/11 Australia
Country Length Discount Travel Period Anguilla All 20% off 08/24/11 12/15/11 Antigua All 20% off 08/24/11 12/15/11 Argentina All 20% off 08/24/11 12/15/11 Aruba All 20% off 08/24/11 12/15/11 Australia
C 22. Calming LV, tranquilizing internal wind (13) LV yang. Shi Jue Ming ** Properties: Salty, mild cold LV. Actions: Suppress LV yang, clear eye heat
 LV yang. Shi Jue Ming ** Properties: Salty, mild cold LV. Actions: Suppress LV yang, clear eye heat") C 22. Calming LV, tranquilizing internal wind (13) LV yang Shi Jue Ming ** Zhen Zhu Mu * (Long Gu -)*** Mu Li *** Dai Zhe Shi ** Bai Ji Li/Ci Ji Li Wind/spasm Gou Teng ** Tian Ma *** Di Long ** Quan Xie
C 22. Calming LV, tranquilizing internal wind (13) LV yang Shi Jue Ming ** Zhen Zhu Mu * (Long Gu -)*** Mu Li *** Dai Zhe Shi ** Bai Ji Li/Ci Ji Li Wind/spasm Gou Teng ** Tian Ma *** Di Long ** Quan Xie
Researches on Fermentation Engineering of Polysaccharide of
 13 1 Vol13 No1 1 2009 2 Life Science Research Feb 2009 1a 1b, 2, 1 416000 2 416000 3 410300 : (Cordyceps militaris), :, 6% 1% 25, ; 6% 1% 22, : ; ; ; ; ; : TQ92 : A : 1007-7847(2009)01-0065-06 Researches
13 1 Vol13 No1 1 2009 2 Life Science Research Feb 2009 1a 1b, 2, 1 416000 2 416000 3 410300 : (Cordyceps militaris), :, 6% 1% 25, ; 6% 1% 22, : ; ; ; ; ; : TQ92 : A : 1007-7847(2009)01-0065-06 Researches
17:00 17:45 Meet-the-Professor Immuno-Oncology Fan Yang, Beijing, Christoph Zielinski, Vienna
 8 th Chinese German Lung Cancer Forum Dresden, Germany, September 8-10, 2016 Precision oncology in lung cancer Thursday, September 8, 2016 17:00 17:45 Meet-the-Professor Immuno-Oncology Fan Yang, Beijing,
8 th Chinese German Lung Cancer Forum Dresden, Germany, September 8-10, 2016 Precision oncology in lung cancer Thursday, September 8, 2016 17:00 17:45 Meet-the-Professor Immuno-Oncology Fan Yang, Beijing,
CURRICULUM VITAE. Name: PoTsung Chen, Ph.D.
 CURRICULUM VITAE Name: PoTsung Chen, Ph.D. #1 University Rd, Dept. of Architecture, NCKU Tainan, Taiwan, 701 Tel:886-6-252-1019 Fax:886-6-281-0380 Email:potsung@mail.ncku.edu.tw (1)Personal Information:
CURRICULUM VITAE Name: PoTsung Chen, Ph.D. #1 University Rd, Dept. of Architecture, NCKU Tainan, Taiwan, 701 Tel:886-6-252-1019 Fax:886-6-281-0380 Email:potsung@mail.ncku.edu.tw (1)Personal Information:
World Connections Committee (WCC) Report
 Report") World Connections Committee (WCC) Report 06 Co-Dependents Anonymous Service Conference Countries Where CoDA Exists This report reflects the World Connections Committee (WCC) support of the growth and development
World Connections Committee (WCC) Report 06 Co-Dependents Anonymous Service Conference Countries Where CoDA Exists This report reflects the World Connections Committee (WCC) support of the growth and development
51. DETACHMENT COURSE with International Faculty at the 2007 SYMPOSIUM OF THE KOREAN RETINA SOCIETY. Seoul, Korea, June 23 24, 2007 PROGRAM
 DEPARTMENTS OF OPHTHALMOLOGY MANNHEIM, WEILL CORNELL MEDICAL COLLEGE NEW YORK PROGRAM 51. DETACHMENT COURSE with International Faculty at the 2007 SYMPOSIUM OF THE KOREAN RETINA SOCIETY Seoul, Korea, June
DEPARTMENTS OF OPHTHALMOLOGY MANNHEIM, WEILL CORNELL MEDICAL COLLEGE NEW YORK PROGRAM 51. DETACHMENT COURSE with International Faculty at the 2007 SYMPOSIUM OF THE KOREAN RETINA SOCIETY Seoul, Korea, June
Tobacco: World Markets and Trade
 United States Department of Agriculture Foreign Agricultural Service Circular Series FT -09-05 Sep. 2005 List of Tables Tobacco: World Markets and Trade Table 2 U.S. Tobacco Trade: 2004-2005 Table 3 Unmanufactured
United States Department of Agriculture Foreign Agricultural Service Circular Series FT -09-05 Sep. 2005 List of Tables Tobacco: World Markets and Trade Table 2 U.S. Tobacco Trade: 2004-2005 Table 3 Unmanufactured
Residual Cancer. May 3-5, International Symposium. on Minimal. Le Corum. > Preliminary. Program MONTPELLIER, FRANCE
 International Symposium th on Minimal Residual Cancer > Preliminary Program May 3-5, 2018 Le Corum MONTPELLIER, FRANCE Organizers: www.ismrc2018.com > Committee & Speakers > Welcome to Montpellier Scientific
International Symposium th on Minimal Residual Cancer > Preliminary Program May 3-5, 2018 Le Corum MONTPELLIER, FRANCE Organizers: www.ismrc2018.com > Committee & Speakers > Welcome to Montpellier Scientific
Single Herbs III / Quiz I
 Single Herbs III / Quiz I 1. What herb is good to generate fluids? A. Ren Shen C. Xi Yang Shen B. Tai Zi Shen D. All the Shens 2. What herb is best for Qi collapse? A. Huang Qi C. Dang Shen B. Ren Shen
Single Herbs III / Quiz I 1. What herb is good to generate fluids? A. Ren Shen C. Xi Yang Shen B. Tai Zi Shen D. All the Shens 2. What herb is best for Qi collapse? A. Huang Qi C. Dang Shen B. Ren Shen
Founding Editorial Board Meeting of the JGO. Date & Time: November 14 th (Sat) 2015, 6:30~7:30AM Venue: Crystal Ballroom (2F) Lotte Hotel, Seoul
 2015, 6:30~7:30AM Venue: Crystal Ballroom (2F) Lotte Hotel, Seoul") Founding Editorial Board Meeting of the JGO Date & Time: November 14 th (Sat) 2015, 6:30~7:30AM Venue: Crystal Ballroom (2F) Lotte Hotel, Seoul Objective of this meeting Share the current status of the
Founding Editorial Board Meeting of the JGO Date & Time: November 14 th (Sat) 2015, 6:30~7:30AM Venue: Crystal Ballroom (2F) Lotte Hotel, Seoul Objective of this meeting Share the current status of the
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2017 September 28; 23(36): 6549-6746 Published by Baishideng Publishing Group Inc Editorial Board
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2017 September 28; 23(36): 6549-6746 Published by Baishideng Publishing Group Inc Editorial Board
SEPI: Past, Present, and Future. Carol R. Glass The Catholic University of America Washington, DC, USA
 SEPI: Past, Present, and Future Carol R. Glass The Catholic University of America Washington, DC, USA Carol s thoughts I m not a founding member but involved for almost 30 years will share some of my first
SEPI: Past, Present, and Future Carol R. Glass The Catholic University of America Washington, DC, USA Carol s thoughts I m not a founding member but involved for almost 30 years will share some of my first
- Network for Excellence in Health Innovation
 Real-world evidence is evidence from any and all sources of data that may contribute to more effective health care, including health care best tailored to the needs of individual patients. - Network for
Real-world evidence is evidence from any and all sources of data that may contribute to more effective health care, including health care best tailored to the needs of individual patients. - Network for
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 January 21; 22(3): 895-1330 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 January 21; 22(3): 895-1330 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
Hyun Kee Kim, M.S. Curriculum Vitae
 Hyun Kee Kim, M.S. Curriculum Vitae August, 2012 Ⅰ. Personal Information Address - Office. Researcher Molecular Genetic Laboratory, Research Institute of Medical Science, College of Medicine, The Catholic
Hyun Kee Kim, M.S. Curriculum Vitae August, 2012 Ⅰ. Personal Information Address - Office. Researcher Molecular Genetic Laboratory, Research Institute of Medical Science, College of Medicine, The Catholic
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 September 28; 22(36): 8067-8246 Published by Baishideng Publishing Group Inc Editorial Board
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 September 28; 22(36): 8067-8246 Published by Baishideng Publishing Group Inc Editorial Board
Incidence And Mortality Trend of Cervical Cancer in 11 Cancer Registries of China
 10 Chin J Cancer Res 23(1):10-14, 2011 www.springerlink.com Original Article And Trend of Cervical Cancer in 11 Cancer Registries of China Tao Lei 1, Wei-min Mao 1*, Tong-hai Lei 1, Li-qiong Dai 1, Luo
10 Chin J Cancer Res 23(1):10-14, 2011 www.springerlink.com Original Article And Trend of Cervical Cancer in 11 Cancer Registries of China Tao Lei 1, Wei-min Mao 1*, Tong-hai Lei 1, Li-qiong Dai 1, Luo
Version Practitioner Guide
 Version 1.0 2017 Practitioner Guide KAMWO MERIDIAN HERBS The oldest herbal dispensary & supplier of professional, natural health products on the East Coast. With thousands of options for your practice
Version 1.0 2017 Practitioner Guide KAMWO MERIDIAN HERBS The oldest herbal dispensary & supplier of professional, natural health products on the East Coast. With thousands of options for your practice
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 June 14; 22(22): 5137-5300 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 June 14; 22(22): 5137-5300 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
THURSDAY, 9 JUNE 2016
 COMMITTEE Dr. Peter Vorwald. Fundación Jiménez Díaz. Madrid. Dr. Gabriel Salcedo. Fundación Jiménez Díaz. Madrid. Dra. María Posada. Fundación Jiménez Díaz. Madrid. Dr. Damián García Olmo. Grupo Quirón
COMMITTEE Dr. Peter Vorwald. Fundación Jiménez Díaz. Madrid. Dr. Gabriel Salcedo. Fundación Jiménez Díaz. Madrid. Dra. María Posada. Fundación Jiménez Díaz. Madrid. Dr. Damián García Olmo. Grupo Quirón
Kwun Tong Government Secondary School 34th Annual Swimming Gala ( ) Master Participant List for All Events. 25m FREE STYLE (Boy C)
 Master Participant List for All Events. 25m FREE STYLE (Boy C)") File: MasterLane.dbf Heats Day Kwun Tong Government Secondary School 34th Annual Swimming Gala (2017-2018) Master Participant List for All Events Event No. (1) 25m FREE STYLE (Boy C) 1 YIP CHEUK YUEN 2A(36)
File: MasterLane.dbf Heats Day Kwun Tong Government Secondary School 34th Annual Swimming Gala (2017-2018) Master Participant List for All Events Event No. (1) 25m FREE STYLE (Boy C) 1 YIP CHEUK YUEN 2A(36)
Scientific publications in critical care medicine journals from East Asia: A 10-year survey of the literature
 Open Access Original Article Scientific publications in critical care medicine journals from East Asia: A 10-year survey of the literature Zhenyu Cao 1, Chongyang Ou 2, Hongfei Teng 3, Xiguang Liu 4, Hongxin
Open Access Original Article Scientific publications in critical care medicine journals from East Asia: A 10-year survey of the literature Zhenyu Cao 1, Chongyang Ou 2, Hongfei Teng 3, Xiguang Liu 4, Hongxin
MSCI GLOBAL MARKET ACCESSIBILITY REVIEW JUNE Competitive landscape
 DEVELOPED MARKETS Americas Canada USA Austria Belgium Denmark Finland France Germany Ireland Israel Italy Netherlands Investor qualification requirement ++ ++ ++ ++ ++ ++ ++ ++ ++ ++ ++ ++ Foreign ownership
DEVELOPED MARKETS Americas Canada USA Austria Belgium Denmark Finland France Germany Ireland Israel Italy Netherlands Investor qualification requirement ++ ++ ++ ++ ++ ++ ++ ++ ++ ++ ++ ++ Foreign ownership
Appendix F: Test-Curriculum Matching Analysis
 Appendix F: Test-Curriculum Matching Analysis TIMSS went to great lengths to ensure that comparisons of student achievement across countries would be as fair and equitable as possible. The TIMSS 2015 Assessment
Appendix F: Test-Curriculum Matching Analysis TIMSS went to great lengths to ensure that comparisons of student achievement across countries would be as fair and equitable as possible. The TIMSS 2015 Assessment
Evidence-based Research Methods for Chinese Medicine
 Evidence-based Research Methods for Chinese Medicine Siu-wai Leung Hao Hu Editors Evidence-based Research Methods for Chinese Medicine 123 Editors Siu-wai Leung Institute of Chinese Medical Sciences University
Evidence-based Research Methods for Chinese Medicine Siu-wai Leung Hao Hu Editors Evidence-based Research Methods for Chinese Medicine 123 Editors Siu-wai Leung Institute of Chinese Medical Sciences University
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2017 August 7; 23(29): 5257-5450 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2017 August 7; 23(29): 5257-5450 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2017 March 7; 23(9): 1513-1734 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2017 March 7; 23(9): 1513-1734 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2015 May 28; 21(20): 6097-6426 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2015 May 28; 21(20): 6097-6426 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 September 21; 22(35): 7857-8066 Published by Baishideng Publishing Group Inc Editorial Board
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 September 21; 22(35): 7857-8066 Published by Baishideng Publishing Group Inc Editorial Board
ACTA PHYSIOLOGICA SINICA
 Acta Physiologica Sinica, Volume 63, Contents (1 6) 619 ACTA PHYSIOLOGICA SINICA (Continuing The Chinese Journal of Physiology Started in 1927) VOLUME 63 CONTENTS (1 6) No. 1 INVITED REVIEW Neuronal signaling
Acta Physiologica Sinica, Volume 63, Contents (1 6) 619 ACTA PHYSIOLOGICA SINICA (Continuing The Chinese Journal of Physiology Started in 1927) VOLUME 63 CONTENTS (1 6) No. 1 INVITED REVIEW Neuronal signaling
4-1 Dyspnea (Chuan, 喘 )
") 4-1 Dyspnea (Chuan, 喘 ) Concept Breathing with difficulty (open wide mouth, raise shoulders) Etiology and pathogenesis Climatic factors Phlegm fluid Emotion Chronic diseases Exertion Over sex Diagnosis
4-1 Dyspnea (Chuan, 喘 ) Concept Breathing with difficulty (open wide mouth, raise shoulders) Etiology and pathogenesis Climatic factors Phlegm fluid Emotion Chronic diseases Exertion Over sex Diagnosis
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2014 June 21; 20(23): 7079-7524 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2014 June 21; 20(23): 7079-7524 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
Nasopharyngeal carcinoma incidence and mortality in China in 2010
 Chinese Journal of Cancer Original Article Nasopharyngeal carcinoma incidence and mortality in China in 2010 Kuang-Rong Wei 1, Rong-Shou Zheng 2, Si-Wei Zhang 2, Zhi-Heng Liang 1, Zhi-Xiong Ou 1 and Wan-Qing
Chinese Journal of Cancer Original Article Nasopharyngeal carcinoma incidence and mortality in China in 2010 Kuang-Rong Wei 1, Rong-Shou Zheng 2, Si-Wei Zhang 2, Zhi-Heng Liang 1, Zhi-Xiong Ou 1 and Wan-Qing
Programme. TTS New Key Opinion Leader Meeting Thursday September 21 st Arrivals and Dinner at the Hotel. Friday September 22 nd
 TTS New Key Opinion Leader Meeting 2006 Programme Thursday September 21 st Arrivals and Dinner at the Hotel After dinner approx 9.00pm Pioneers in Transplantation Professor Josep Ma Caralps Heart transplantation
TTS New Key Opinion Leader Meeting 2006 Programme Thursday September 21 st Arrivals and Dinner at the Hotel After dinner approx 9.00pm Pioneers in Transplantation Professor Josep Ma Caralps Heart transplantation
2018 National Oncologists Workforce Study OCTOBER 2018
 2018 National Oncologists Workforce Study OCTOBER 2018 Introduction Providers have long cautioned that the U.S. healthcare system is facing imminent physician shortages across many different specialties.
2018 National Oncologists Workforce Study OCTOBER 2018 Introduction Providers have long cautioned that the U.S. healthcare system is facing imminent physician shortages across many different specialties.
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 May 28; 22(20): 4789-4962 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 May 28; 22(20): 4789-4962 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
Chang Gung Medical Journal
 Vol. 32 No. 6 November-December 2009 Chang Gung Medical Journal CONTENTS IN BRIEF REVIEW ARTICLES 589 Mitochondrial Dysfunction and Biogenesis in the Pathogenesis of Parkinson s Disease Tsu-Kung Lin, MD,
Vol. 32 No. 6 November-December 2009 Chang Gung Medical Journal CONTENTS IN BRIEF REVIEW ARTICLES 589 Mitochondrial Dysfunction and Biogenesis in the Pathogenesis of Parkinson s Disease Tsu-Kung Lin, MD,
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2017 January 7; 23(1): 1-190 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2017 January 7; 23(1): 1-190 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 February 21; 22(7): 2159-2402 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2016 February 21; 22(7): 2159-2402 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2015 November 14; 21(42): 11887-12210 Published by Baishideng Publishing Group Inc Editorial Board
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2015 November 14; 21(42): 11887-12210 Published by Baishideng Publishing Group Inc Editorial Board
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2014 April 7; 20(13): 3391-3718 www.wjgnet.com Editorial Board 2014-2017 The World Journal of Gastroenterology
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2014 April 7; 20(13): 3391-3718 www.wjgnet.com Editorial Board 2014-2017 The World Journal of Gastroenterology
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES
 SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2014 April 21; 20(15): 4115-4466 www.wjgnet.com Editorial Board 2014-2017 The World Journal of Gastroenterology
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2014 April 21; 20(15): 4115-4466 www.wjgnet.com Editorial Board 2014-2017 The World Journal of Gastroenterology
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2014 April 14; 20(14): 3719-4114 www.wjgnet.com Editorial Board 2014-2017 The World Journal of Gastroenterology
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2014 April 14; 20(14): 3719-4114 www.wjgnet.com Editorial Board 2014-2017 The World Journal of Gastroenterology
LYON. FRANCE NOVEMBER / 2013 TRANSLATIONAL RESEARCH IN CHRONIC VIRAL HEPATITIS - BRIDGING BASIC SCIENCE AND CLINICAL RESEARCH
 LYON. FRANCE NOVEMBER 29-30 / 2013 TRANSLATIONAL RESEARCH IN CHRONIC VIRAL HEPATITIS - BRIDGING BASIC SCIENCE https://events.easl.eu/eventportal/ Information/MLYON2013/HOME.aspx Abstract submission deadline:
LYON. FRANCE NOVEMBER 29-30 / 2013 TRANSLATIONAL RESEARCH IN CHRONIC VIRAL HEPATITIS - BRIDGING BASIC SCIENCE https://events.easl.eu/eventportal/ Information/MLYON2013/HOME.aspx Abstract submission deadline:
Contents. Foreword Qian Chen Shu-Xun Hou Stephan M. Perren L. K. Hung xiii Preface. Part I Cell Culture and Molecular Biology 1
 Foreword Qian Chen v Shu-Xun Hou ix Stephan M. Perren xi L. K. Hung xiii Preface xv List of Contributors xxvii Part I Cell Culture and Molecular Biology 1 Chapter 1 DNA Microarray 3 Xiao-Ling Zhang and
Foreword Qian Chen v Shu-Xun Hou ix Stephan M. Perren xi L. K. Hung xiii Preface xv List of Contributors xxvii Part I Cell Culture and Molecular Biology 1 Chapter 1 DNA Microarray 3 Xiao-Ling Zhang and
Liu et al., Afr J Tradit Complement Altern Med. (2013) 10(4):78-82
 10(4):78-82") 78 A COMPARATIVE STUDY OF ANTI-GASTRIC CANCER ACTIVITY BETWEEN AQUEOUS EXTRACT AND ETHANOL EXTRACT OF FOLIUM CORDYLINES FRUTICOSAE Shaojun Liu 1, Dongbo Cao 2, Zhiming Xiao 1, Fen Liu 1, Xiaoyan Wang 1,
78 A COMPARATIVE STUDY OF ANTI-GASTRIC CANCER ACTIVITY BETWEEN AQUEOUS EXTRACT AND ETHANOL EXTRACT OF FOLIUM CORDYLINES FRUTICOSAE Shaojun Liu 1, Dongbo Cao 2, Zhiming Xiao 1, Fen Liu 1, Xiaoyan Wang 1,
Course: Formulas 1 Date: December 2, 2009 Class #: 10. Function in Formula. Disperse stagnation
 Course: Formulas 1 Date: December 2, 2009 Class #: 10 Xi Jiao Di Huang Tang : o Clear Heat toxins o o Disperse stagnation : o Heat in the blood Xi jiao Sheng di Shao yao Mu dan pi Clear Heart heat Nourish
Course: Formulas 1 Date: December 2, 2009 Class #: 10 Xi Jiao Di Huang Tang : o Clear Heat toxins o o Disperse stagnation : o Heat in the blood Xi jiao Sheng di Shao yao Mu dan pi Clear Heart heat Nourish
A continuous Educational Programme from Basic Immunology to Clinical Neuroimmunology PROFILE 2017
 A continuous Educational Programme from Basic Immunology to Clinical Neuroimmunology PROFILE 2017 ABOUT US Gianvito Martino (for the Scientific Committee) It is a pleasure to introduce this new, exciting
A continuous Educational Programme from Basic Immunology to Clinical Neuroimmunology PROFILE 2017 ABOUT US Gianvito Martino (for the Scientific Committee) It is a pleasure to introduce this new, exciting
Update on Biology and Clinical Impact of Occult Hepatitis B Virus Infection
 Update on Biology and Clinical Impact of Occult Hepatitis B Virus Infection Taormina-MeSSINA-Italy October 1 st 2 nd 2018 1 Update on Biology and Clinical Impact of Occult Hepatitis B Virus Infection Taormina-MeSSINA-Italy
Update on Biology and Clinical Impact of Occult Hepatitis B Virus Infection Taormina-MeSSINA-Italy October 1 st 2 nd 2018 1 Update on Biology and Clinical Impact of Occult Hepatitis B Virus Infection Taormina-MeSSINA-Italy
ratio in patients treated by sorafenib alone decreased after treatment (P<0.05), while CD 8
, while CD 8") Int J Clin Exp Med 2016;9(2):4625-4629 www.ijcem.com /ISSN:1940-5901/IJCEM0015836 Original Article Effect of sorafenib combined with CIK cell treatment on immunity and adverse events in patients with late-stage
Int J Clin Exp Med 2016;9(2):4625-4629 www.ijcem.com /ISSN:1940-5901/IJCEM0015836 Original Article Effect of sorafenib combined with CIK cell treatment on immunity and adverse events in patients with late-stage
211 Coronary Heart Disease How To Do By WU NING HAN DING ZHU BIAN READ ONLINE
 211 Coronary Heart Disease How To Do By WU NING HAN DING ZHU BIAN READ ONLINE Jian-Hua Li Di Xie Wen-Yan Lai Jia-Yi Wu Ping with non-st elevation acute coronary syndrome referred for Yang Hui Fan Hong-Li
211 Coronary Heart Disease How To Do By WU NING HAN DING ZHU BIAN READ ONLINE Jian-Hua Li Di Xie Wen-Yan Lai Jia-Yi Wu Ping with non-st elevation acute coronary syndrome referred for Yang Hui Fan Hong-Li
ICMART. International Council of Medical Acupuncture and Related Techniques
 ICMART International Council of Medical Acupuncture and Related Techniques Headquarters Louisenstrasse 15-17 / Loewengasse 1 61348 Bad Homburg Germany tel +49 6172 21038 fax +49 6172 599800 www.icmart.org
ICMART International Council of Medical Acupuncture and Related Techniques Headquarters Louisenstrasse 15-17 / Loewengasse 1 61348 Bad Homburg Germany tel +49 6172 21038 fax +49 6172 599800 www.icmart.org
Supportive Cancer Care with Chinese Medicine
 Supportive Cancer Care with Chinese Medicine William C.S. Cho Editor Supportive Cancer Care with Chinese Medicine 123 Editor Dr. William Chi-Shing Cho Department Clinical Oncology Queen Elizabeth Hospital
Supportive Cancer Care with Chinese Medicine William C.S. Cho Editor Supportive Cancer Care with Chinese Medicine 123 Editor Dr. William Chi-Shing Cho Department Clinical Oncology Queen Elizabeth Hospital
World Journal of Gastroenterology
 ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2015 May 7; 21(17): 5115-5444 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017
ISSN 1007-9327 (print) ISSN 2219-2840 (online) World Journal of Gastroenterology World J Gastroenterol 2015 May 7; 21(17): 5115-5444 Published by Baishideng Publishing Group Inc Editorial Board 2014-2017