Novel Therapies in Melanoma the Immunotherapy Approach
|
|
|
- Augustine Brooks
- 6 years ago
- Views:
Transcription
1 2018 AAD Annual Meeting, San Diego, CA Novel Therapies in Melanoma the Immunotherapy Approach Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion & Melanoma Program Physician Leader, Cancer Care Program in Cutaneous Oncology Stanford University Medical Center & Cancer Institute VA Palo Alto Health Care System

2 DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Susan M. Swetter, MD F002 Novel Therapies for Cutaneous Malignancies: What s New and What s Ahead DISCLOSURES I do not have any relevant relationships with industry.
3 Metastatic Melanoma (AJCC Stage IV) Distant skin, nodal, visceral, skeletal, or brain metastasis Before 2011, survival had not changed appreciably over the prior 30+ years Median survival in 2010: 6-9 months; in 2016: months! Approved agents for unresectable stage III and stage IV melanoma: DTIC: RR 6%-8%, no long-term survival benefit High dose bolus IL-2: 5-7% durable remission, highly toxic Ipilimumab (CTLA-4 Ab), Vemurafenib (BRAFi) Dabrafenib (BRAFi), Trametinib (MEKi) ; Combination dab/tram Pembrolizumab (PD-1 Ab) 2014; Nivolumab (PD-1 Ab) 2015 Vemurafenib/Cobemetinib (BRAF/MEKi combo); ipi/nivo combination; and Talimogene laherparepvec (T-VEC) 2015 Atezolizumab (PD-L1 Ab) under investigation

4 Where we came from High-dose IL-2 An Era of Futility: Korn et al. J Clin Oncol 2009 DTIC Courtesy of Ryan Sullivan, MD

5 Overall Survival After Checkpoint Blockade Percent Alive nivolumab + ipilimumab PD-1 pathway blockade ipilimumab Years





6 During the Era of Futility - 2 fundamental and translatable discoveries occurred Sullivan and Flaherty. Clin Cancer Res Sullivan et al. ASCO Ed Book Melanoma TCGA. Cell 2015





7 Systemic Therapy for Metastatic Melanoma The therapeutic landscape for metastatic melanoma is rapidly changing with the recent development of novel agents which have demonstrated better efficacy than traditional chemotherapy NCCN guidelines, Melanoma
8 Changing Melanoma Treatment Landscape DTIC High-dose IL-2 Vemurafenib (V) Ipilimumab Dabafenib (D), Trametinib (T) D + T Binimetinib, Encorafenib Cobimetinib + Vem Nivolumab TVEC Pembrolizumab Ipi + Nivo Median survival 2016: mos! Courtesy of Ryan Sullivan, MD
9 Systemic Therapy for Metastatic Melanoma Targeted therapy BRAF inhibitors dabrafenib vemurafenib MEK inhibitors trametinib cobimetinib Immunotherapy Anti CTLA-4 ipilimumab Anti PD-1 pembrolizumab nivolumab Immune-mediated dermatitis often responds to topical corticosteroids. For immune-mediated dermatitis that does not respond, or for patients who have a history of immune-mediated skin disorders such as psoriasis or autoimmune blistering disease, consider referral to a dermatologist or provider experienced in the diagnosis and management of cutaneous manifestations of immunotherapy. Regular dermatologic evaluation and referral to a dermatologist or provider experienced in the diagnosis and management of cutaneous manifestations of targeted therapy is recommended. National Comprehensive Cancer Network, 2017, Melanoma,

10 Grading of Dermatologic Adverse Events Common Terminology Criteria for Adverse Events (CTCAE), Version 4.0 Adverse event: any abnormal clinical finding temporally associated with the use of therapy; causality is not required Grade: refers to the severity of the AE In general, (*specific parameters according to organ system involved): Grade 1: Mild; asymptomatic or mild symptoms; clinical or diagnostic observations only; intervention not indicated. Grade 2: Moderate; minimal, local or noninvasive intervention indicated; limiting age-appropriate instrumental ADL (preparing meals, shopping for groceries or clothes, using the telephone, managing money, etc.). Grade 3: Severe or medically significant but not immediately lifethreatening; hospitalization or prolongation of hospitalization indicated; disabling; limiting self care ADL (bathing, dressing and undressing, feeding self, using the toilet, taking medications, and not bedridden). (May result in holding the drug). Grade 4: Life-threatening consequences; urgent intervention indicated. Grade 5: Death related to AE.
11 Key Developments in Melanoma Immunotherapy Occurred in Tandem with Targeted Therapy Approaches Inhibition of Immune Checkpoints: -Creation of blocking antibodies against: -CTLA-4 -PD-1 -PD-L1 Immunotherapy BRAF-Targeted Therapy Takes the breaks off the immune system Sullivan and Flaherty. Clin Cancer Res. 2015
12 Why do we have negative immune checkpoints? Cancer immune inhibitory molecules (CTLA-4, PD-1, PD-L1/L2) These negative signals: Maintain immune tolerance Protect tissues from damage by immune response Turn down immune response after elimination of microbes Tumors and microbes exploit these inhibitory signals to prevent immune eradication
13 Ipilimumab Monoclonal antibody against cytotoxic T lymphocyte antigen-4 (CTLA-4) Increased T-cell activation and cytokine secretion FDA approved March 2011 for treatment of metastatic melanoma First agent to demonstrate increased overall survival compared to dacarbazine Substantial risk of immune-related reactions (60% in pivotal trial), including deaths skin (pruritus, rash) and gastrointestinal tract (diarrhea/colitis) side effects most frequently reported, endocrinopathies are permanent Hodi FS et al. NEJM. 2010;363:711
14 Ipilimumab (ipi) first novel immunotherapy agent to show prolonged survival in melanoma Hodi et al. NEJM 2010 Robert et al. NEJM 2011 Sullivan and Flaherty. Clin Cancer Res Hodi et al. ECCO 2014
 (64%) skin (pruritus, rash) and gastrointestinal tract (diarrhea/colitis) side effects most frequently")
15 Systemic Therapy for Advanced or Metastatic Melanoma: ipilimumab Targeted therapy BRAF inhibitors dabrafenib vemurefenib MEK inhibitors trametinib cobimetinib Immunotherapy Anti CTLA-4 ipilimumab Anti PD-1 pembrolizumab nivolumab Substantial risk of immune-related adverse events (iraes) (64%) skin (pruritus, rash) and gastrointestinal tract (diarrhea/colitis) side effects most frequently reported Dermatologic events manifest earlier in treatment than other iraes Gen include: nonspecific rash, pruritus, and vitiligo Lacouture M et al. JAAD 2014; Hodi S et al. NEJM. 2010
16 Ipilimumab related morbilliform dermatitis 24.3% incidence all-grade rash reticular, erythematous, edematous, maculopapular may be pronounced around nevi, suggesting inflammatory response toward melanocytes +/- pruritus +/- peripheral eosinophilia median time to onset of 3-4 weeks (range up to 17.3 weeks should be followed) Shorter time to onset than GI, liver, or endocrine system symptoms Lacouture M et al. JAAD 2014
17 Ipilimumab related morbilliform dermatitis 24.3% incidence all-grade rash reticular, erythematous, edematous, maculopapular may be pronounced around nevi, suggesting inflammatory response toward melanocytes +/- pruritus +/- peripheral eosinophilia histology nonspecific median time to onset of 3-4 weeks (range up to 17.3 weeks should be followed) Shorter time to onset than GI, liver, or endocrine system symptoms Lacouture M et al. JAAD 2014;71:161-9.



18 Ipilimumab related morbilliform dermatitis Lacouture M et al. JAAD 2014;71:161-9.


19 Ipilimumab related pruritus ~30% incidence negative impact on quality of life not necessarily accompanied by visible rash Lacouture M et al. JAAD 2014

20 Ipilimumab related vitiligo-like melanomaassociated hypopigmentation (MAH) asymptomatic possibly portends prognostic favorability Management: sun protection, camouflage, make-up/cover-up Courtesy: Bernice Kwong, MD
 - Overall survival same in patients with iraes, including skin reactions, compared with those without an iraes -")
21 Does treatment of iraes affect outcome? Study of nearly 300 pts on ipi: - 85% developed immune-related adverse events (iraes) - Overall survival same in patients with iraes, including skin reactions, compared with those without an iraes - No difference in survival between patients requiring corticosteroids and those not requiring immunosuppressive therapy for treatment of iraes Horvat TZ et al. J Clin Oncol 2015; 33:3193.
22 Pembrolizumab/Nivolumab Monoclonal antibody that binds to the PD-1 (programmed cell death-1) receptor Blocks interaction of PD-1 with its ligands: PD-L1 and PD-L2 Releases PD-1 pathway-mediated inhibition of the immune system to increase antitumor immune response FDA approved pembro in September 2014 for patients with unresectable or metastatic melanoma and disease progression following ipilimumab and, if BRAF-mutant, a BRAF inhibitor Approved as 1 st line monotherapy in 2015 >80% of patients alive at 2 yrs

23 Anti-PD1 therapy is better than chemo after ipi Ribas et al. Lancet Oncol 2015 Nivolumab Chemo Sullivan and Flaherty. Clin Cancer Res Weber et al. Lancet Oncol 2015 Nivolumab showed OS benefit compared to chemotherapy - even after ipilimumab failure
24 Front-line anti-pd1 therapy better than chemo & ipi Robert et al. NEJM 2014 Sullivan and Flaherty. Clin Cancer Res Robert et al. NEJM 2015
 receptor Anti PD-1 related cutaneous adverse events (49%) Includes nonspecific rash, vitiligo, lichenoid dermatitis,")
25 Anti PD-1 antibodies (aka PD-1 inhibitors) Targeted therapy BRAF inhibitors dabrafenib vemurefenib MEK inhibitors trametinib cobimetinib Immunotherapy Anti CTLA-4 ipilimumab Anti PD-1 pembrolizumab nivolumab Monoclonal antibodies that bind to the PD-1 (programmed cell death-1) receptor Anti PD-1 related cutaneous adverse events (49%) Includes nonspecific rash, vitiligo, lichenoid dermatitis, bullous pemphigoid, psoriasiform dermatitis, 9% grade 3-4 delayed reactions (immunotherapy requires more time to induce immune responses) cutaneous AEs associated with significantly longer progressionfree survival Hwang et al. J Am Acad Dermatol. 2016;74: e1; Brahmer et al NEJM 2012; Nishimura, 2011, Cell. Sanlorenzo et al JAMA Dermatol. 2015
26 PD-1 inhibitors: Breakthrough in Melanoma Treatment Pembrolizumab - superior to ipilimumab for unresectable advanced melanoma (global KEYNOTE-006 trial) Nivolumab and Pembrolizumab are equivalent in efficacy Higher expression of PD-L1 associated with improved response Most responses partial but DURABLE! ~60% maintain disease control in absence of a complete response (CR) Requires ongoing tx every 2-3 wks (maybe), more tolerable than ipi Bottom line: Melanoma patients are living longer and better with these new treatments Side effect management and survivorship issues need to be addressed



:45-51.")
27 Anti PD-1 antibody therapy related vitiligo 11-25% incidence time to onset: days (median 126 days) immune-mediated destruction through recognition of melanomaassociated antigens shared by normal melanocytes and melanoma cells Management: sun protection Courtesy: Silvina Pugliese, MD Hua C, et al. JAMA Dermatol. 2016;152(1): Courtesy: Silvina Pugliese, MD
 in those who developed vitiligo (71%) vs those who didn t (28%) Hua et al. JAMA Dermatol. 2016152:45-51. Freeman-Keller. et al. Clin Cancer Res.")
28 Development of vitiligo associated with improved outcome - 67 patients, 25% developed vitiligo - All vitiligo patients alive at 441 days - Higher objective response (complete or partial) in those who developed vitiligo (71%) vs those who didn t (28%) Hua et al. JAMA Dermatol : Freeman-Keller. et al. Clin Cancer Res. 2016;2:

29 Anti PD-1/PD-L1 related lichenoid dermatitis 75% with pruritus Variable time of onset (mean 4 mos) delayed compared to ipi Variable clinical presentation (even in same patient) Pathology strikingly consistent: lichenoid infiltrate with more spongiosis and epidermal necrosis than LP Gen responds to topical steroids Shi et al JAMA Dermatol Schaberg K et al. J Cutan Pathol. 2016;43(4):



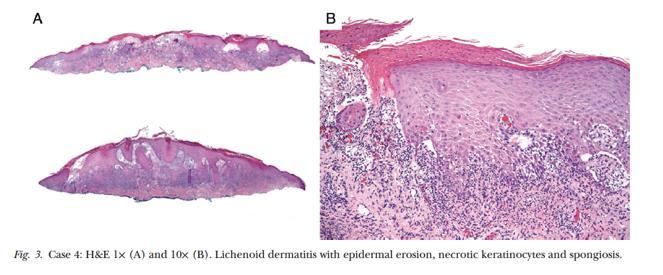


30 Anti-PD1/PD-L1 related lichenoid dermatitis Management: topical steroids (under occlusion) Courtesy: Stanford Dermatopathology and




31 Anti-PD1/PD-L1 related lichenoid mucositis Management: dexamethasone elixir swish/spit; clobetasol ointment to vulva Courtesy: Stanford Dermatopathology and






32 Delayed lichenoid dermatitis after discontinuation of anti-pd-1 therapy Courtesy: Bernice Kwong, MD

33 Management: topical steroids under occlusion when severe Courtesy: Bernice Kwong, MD presentation 36 hours later after triamcinolone 0.1% ointment with sauna suit occlusion; asymptomatic






34 Severity of lichenoid dermatitis may worsen over time 8/2015; more widespread, severe pruritus 9/ % BSA Wolf s isotopic response Initial solitary lesion 7 weeks after first infusion (8/2014) 12/2014: exquisitely pruritic, more lesions Courtesy: Bernice Kwong, MD



35 Anti PD-1 antibody therapy related psoriasiform dermatitis Ohtsuka M et al. JAMA Dermatol. 2015
36 Anti PD-1 immunotherapy related autoimmune blistering disease Can present up to 18 months after starting therapy may persist for several months after discontinuation of the agent May not present with vesicles/bullae Courtesy: Stanford Dermatopathology Carlos G, et al. Melanoma Res 2015; Hwang SJ et al. Melanoma Res 2016 ; Naidoo J et al. Cancer Immunol Res 2016






37 Carlos G, et al. Melanoma Res 2015; Hwang SJ et al. Melanoma Res 2016 ; Naidoo J et al. Cancer Immunol Res 2016 Anti PD-1 immunotherapy related autoimmune blistering disease Management: doxycycline, nicotinamide, topical steroids under occlusion, treatment of secondary infection, systemic steroids, IVIG, methotrexate, tocilizumab, omalizumab (similar to BP) Courtesy: Stanford Dermatopathology
38 Dual anti-pd1/anti-ctla4 (nivo + ipi) therapy is associated with high RR Wolchok et al. NEJM 2013 Sullivan and Flaherty. Clin Cancer Res. 2015
39 Checkmate Combination: ipi + nivo is associated with increased toxicity Safety Summary at 3 years Patients Reporting Event, % NIVO + IPI (N=313) NIVO (N=313) IPI (N=311) Any Grade Grade 3 4 Any Grade Grade 3 4 Any Grade Grade 3 4 Treatment-related adverse event (AE) 96% 59% 86% 21% 86% 28% Treatment-related AE leading to discontinuation 39% 30% 12% 8% 16% 14% Treatment-related death* *Two reported in the NIVO group (neutropenia) and one in the IPI group (colonic performation) 2 deaths in NIVO/IPI (cardiac insufficiency/autoimmune myocarditis and liver necrosis). Wolchok JD et al. NEJM 2017; Larkin J et al. NEJM 2015;373:23.





40 Combo immunotherapy & BRAF inhibitor: Drug-induced hypersensitivity
41 Talimogene Laherparavec (T-VEC) Andtbacka RT et al. J Clin Oncol 2015:33: Viral oncolytic immunotherapy Newer approach to treating certain melanomas (cutaneous, in-transit, nodal mets) in the outpatient clinical setting based on herpes simplex virus type 1 administered via intra-tumoral injection to in-transit or nodal mets induces viral lysis of melanoma cells, followed by stimulation of a tumorspecific immune response risk of spread to people in close contact with the patient following administration, vulnerable populations or through accidental exposure Specific bio-safety procedures and processes are required
42 Comparison of systemic therapy for advanced * melanoma Treatment RR PFS (med) OS (med/2-yr) Single-agent BRAFi 50% 6-8 mo 18.7 mo / ~40% Combo BRAFi & MEKi (1 st line) 65-70% 9-12 mo 25 mo / ~50+% Ipilimumab (IPI) 10% 2-3 mo 36 mo / 34%** (20% 5 yr survival) Anti-PD1 Ab (1 st line) (NIVO or PEMBRO) Combo IPI & NIVO (1 st line) 25-45% ~6 mo 36 mo /52%** ~60% mo 36 mo /58%** * Unresectable Stage III or Stage IV melanoma **Wolchok JD et al. NEJM 2017
43 Other Novel Immunotherapies and Combinations Bench (or early trials) PD-L1 blockers: VERY PROMISING Monotherapy Combined with targeted or other checkpoint inhibitors Inhibitors of negative regulators in tumor microenvironment Indoleamine dioxygenase inhibitor Inhibitors of suppressive cells like certain myeloid cells and Treg cells Immune costimulation 4-1BB- or OX-40 or CD40L agonistic Ab GM-CSF with checkpoint blockers Vaccines? still very challenging Bedside (later trials) CTLA-4 Ab +/- bevacizumab CTLA-4 Ab + PD-1 Ab +/- GM-CSF Other γc cytokines IL-15 + PD-1 blockade IL-7 + various adoptive T cell Rxs CTLA-4 Ab and/or PD-1 Ab plus radiotherapy (abscopal effect) or T-vec Enhancers of ADCC Lesional, regional delivery Viral immunomodulatory genes Cytokines, DC activators Systemically toxic checkpoint inhibitor like ipilimumab Courtesy of Kim Margolin, MD

44 trametinib vemurafenib ipilimumab dabrafenib Conclusion dabrafenib/ trametinib pembrolizumab nivolumab nivolumab/ ipilimumab cobimetinib/ vemurafenib March 2011 August 2011 May 2013 January September FDA approval date December 2014 September 2015 November 2015 Therapeutic landscape for metastatic melanoma continues to rapidly change with development of novel, targeted- and immuno-therapies that demonstrate better efficacy and less toxicity overall HOWEVER, skin toxicity is common! Critical for dermatologists to work with oncologists to recognize and manage these toxicities: improve patient quality of life prevent unnecessary dose reduction or discontinuation of medication
What You Need to Know about Advanced Melanoma Therapies Targeted Approaches
 2018 AAD Annual Meeting, San Diego, CA What You Need to Know about Advanced Melanoma Therapies Targeted Approaches Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion & Melanoma
2018 AAD Annual Meeting, San Diego, CA What You Need to Know about Advanced Melanoma Therapies Targeted Approaches Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion & Melanoma
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Skin Deep Into Toxicities of Cancer Therapies. Mario E Lacouture MD Member, Memorial Hospital Director, Oncodermatology Program New York, NY
 Skin Deep Into Toxicities of Cancer Therapies Mario E Lacouture MD Member, Memorial Hospital Director, Oncodermatology Program New York, NY Targeting the Immune System in Cancer. Sharma et al, Nat Rev
Skin Deep Into Toxicities of Cancer Therapies Mario E Lacouture MD Member, Memorial Hospital Director, Oncodermatology Program New York, NY Targeting the Immune System in Cancer. Sharma et al, Nat Rev
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
What's New in Oncodermatopathology: Immunotherapy Reactions
 What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
TAO-Cancer Toxicity Management: Cutaneous Toxicities of Immunotherapies
 TAO-Cancer Toxicity Management: Cutaneous Toxicities of Immunotherapies Mario E Lacouture MD Director, Oncodermatology Program Attending, Dermatology www. MSKCC.org Dermatologic Care With Immunotherapies
TAO-Cancer Toxicity Management: Cutaneous Toxicities of Immunotherapies Mario E Lacouture MD Director, Oncodermatology Program Attending, Dermatology www. MSKCC.org Dermatologic Care With Immunotherapies
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Update on Melanoma Treatment. Tara C Mitchell, MD
 Update on Melanoma Treatment Tara C Mitchell, MD Overview Immune therapy update Targeted therapy update New concepts in treating melanoma What is the immune system? A complex network of protective cells
Update on Melanoma Treatment Tara C Mitchell, MD Overview Immune therapy update Targeted therapy update New concepts in treating melanoma What is the immune system? A complex network of protective cells
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Basic Principles of Tumor Immunotherapy. Ryan J. Sullivan, M.D. Massachusetts General Hospital Cancer Center Boston, MA
 Basic Principles of Tumor Immunotherapy Ryan J. Sullivan, M.D. Massachusetts General Hospital Cancer Center Boston, MA Disclosures Consulting Fees: Biodesix, Novartis Pharmaceuticals Other: Boehringer
Basic Principles of Tumor Immunotherapy Ryan J. Sullivan, M.D. Massachusetts General Hospital Cancer Center Boston, MA Disclosures Consulting Fees: Biodesix, Novartis Pharmaceuticals Other: Boehringer
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
ONCOS-102 in melanoma Dr. Alexander Shoushtari. 4. ONCOS-102 in mesothelioma 5. Summary & closing
 ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Immune-Related Adverse Events: Dermatologic
 Immune-Related Adverse Events: Dermatologic Mario E Lacouture, MD Director, Oncodermatology Program Attending, Dermatology Dermatology Service, Department of Medicine lacoutum@mskcc.org Disclosures Research
Immune-Related Adverse Events: Dermatologic Mario E Lacouture, MD Director, Oncodermatology Program Attending, Dermatology Dermatology Service, Department of Medicine lacoutum@mskcc.org Disclosures Research
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Immunoterapia e melanoma maligno metastatico: siamo partiti da li. Vanna Chiarion Sileni Istituto Oncologico Veneto
 Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Toxicity of Systemic Melanoma Therapies. Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney
 Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy
 New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
Nursing Perspective on iraes: Patient Education, Monitoring and Management
 Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
New Therapeutic Approaches to Malignant Melanoma
 2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
2/16/2018. The Immune System and Cancer. Fatal Melanoma Transferred in a Donated Kidney 16 years after Melanoma Surgery
 C007: Immunology of Melanoma: Mechanisms of Immune Therapies Delphine J. Lee, MD, PhD Chief and Program Director, Dermatology, Harbor UCLA Medical Center Principal Investigator, Los Angeles Biomedical
C007: Immunology of Melanoma: Mechanisms of Immune Therapies Delphine J. Lee, MD, PhD Chief and Program Director, Dermatology, Harbor UCLA Medical Center Principal Investigator, Los Angeles Biomedical
2/19/2018. The Immune System and Cancer. Fatal Melanoma Transferred in a Donated Kidney 16 years after Melanoma Surgery
 F141: Advanced Melanoma: Mechanisms of Immune Therapies beyond Checkpoint blockade Delphine J. Lee, MD, PhD Chief and Program Director, Dermatology, Harbor UCLA Medical Center Principal Investigator, Los
F141: Advanced Melanoma: Mechanisms of Immune Therapies beyond Checkpoint blockade Delphine J. Lee, MD, PhD Chief and Program Director, Dermatology, Harbor UCLA Medical Center Principal Investigator, Los
Cancer Immunotherapy: Promises and Challenges. Disclosures
 Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Combination Approaches in Melanoma: A Balancing Act
 Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Adverse effects of Immunotherapy. Asha Nayak M.D
 Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Melanoma in Focus: Update on Novel Therapy, Emerging Agents, and Optimizing Patient Care Presentation 1
 Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Melanoma- Fighting the Dark Side
 Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS
 MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS John B.A.G. Haanen MD PhD CONTENT OF THIS PRESENTATION General aspects of immune related adverse events related to immune checkpoint
MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS John B.A.G. Haanen MD PhD CONTENT OF THIS PRESENTATION General aspects of immune related adverse events related to immune checkpoint
Oncology and surgery Yolanda Gilaberte. Hospital Universitario Miguel Servet, Zaragoza
 Oncology and surgery Yolanda Gilaberte. Hospital Universitario Miguel Servet, Zaragoza Dermatologic adverse events of oncologic drugs Grading of Dermatologic Adverse Events (ver 5.0) 5 grades: mild, moderate,
Oncology and surgery Yolanda Gilaberte. Hospital Universitario Miguel Servet, Zaragoza Dermatologic adverse events of oncologic drugs Grading of Dermatologic Adverse Events (ver 5.0) 5 grades: mild, moderate,
Locally Advanced and Metastatic Melanoma. Relevant disclosures 6/23/2018. What is the median survival of metastatic melanoma? Abel D.
 Locally Advanced and Metastatic Melanoma Abel D. Jarell, MD, FAAD Adjunct Dartmouth School of Medicine, Hanover, NH Northeast Dermatology Associates, Portsmouth, NH Relevant disclosures What is the median
Locally Advanced and Metastatic Melanoma Abel D. Jarell, MD, FAAD Adjunct Dartmouth School of Medicine, Hanover, NH Northeast Dermatology Associates, Portsmouth, NH Relevant disclosures What is the median
Emerging Trends & Strategies in the Treatment & Management of Metastatic Melanoma. Evan J. Lipson, MD
 Emerging Trends & Strategies in the Treatment & Management of Metastatic Melanoma Evan J. Lipson, MD Johns Hopkins University School of Medicine Sidney Kimmel Comprehensive Cancer Center April 25, 2014
Emerging Trends & Strategies in the Treatment & Management of Metastatic Melanoma Evan J. Lipson, MD Johns Hopkins University School of Medicine Sidney Kimmel Comprehensive Cancer Center April 25, 2014
Talimogene Laherparepvec (T-VEC) at the SCCA: an update
 at the SCCA: an update") Talimogene Laherparepvec (T-VEC) at the SCCA: an update Jennifer M. Gardner, MD Assistant Professor, Division of Dermatology University of Washington jen1110@uw.edu Northwest Melanoma Symposium: Science
Talimogene Laherparepvec (T-VEC) at the SCCA: an update Jennifer M. Gardner, MD Assistant Professor, Division of Dermatology University of Washington jen1110@uw.edu Northwest Melanoma Symposium: Science
Significance. Outline and Objectives. S007 Systemic Therapies for Medical Oncology
 S007 Systemic Therapies for Medical Oncology Anisha B. Patel, M.D. Assistant Professor, Dermatology UT MD Anderson Cancer Center UT Health Science Center Houston Safety considerations Outline and Objectives
S007 Systemic Therapies for Medical Oncology Anisha B. Patel, M.D. Assistant Professor, Dermatology UT MD Anderson Cancer Center UT Health Science Center Houston Safety considerations Outline and Objectives
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies. Michael A. Curran, Ph.D.
 Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies Michael A. Curran, Ph.D. MD Anderson Cancer Center Department of Immunology Disclosures I have research
Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies Michael A. Curran, Ph.D. MD Anderson Cancer Center Department of Immunology Disclosures I have research
9/22/2016. Introduction / Goals. What is Cancer? Pharmacologic Strategies to Treat Cancer. Immune System Modulation
 Immunomodulatory Therapies in Cancer Treatment Bill O Hara, PharmD, BCPS, BCOP Advanced Practice Pharmacist, Oncology/BMT Thomas Jefferson University Hospital Introduction / Goals What is Cancer? How can
Immunomodulatory Therapies in Cancer Treatment Bill O Hara, PharmD, BCPS, BCOP Advanced Practice Pharmacist, Oncology/BMT Thomas Jefferson University Hospital Introduction / Goals What is Cancer? How can
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Principles and Application of Immunotherapy for Cancer: Advanced Melanoma
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
New treatments in melanoma
 New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
Melanoma 10/12/18 Justin J. Baker, M.D.
 Objectives Review Incidence Risk Factors for Development Detection 10/12/18 Justin J. Baker, M.D. Treatment of Surgery Medicine Radiation What is Incidence Cancer of Melanocytes Melanocytes are normal
Objectives Review Incidence Risk Factors for Development Detection 10/12/18 Justin J. Baker, M.D. Treatment of Surgery Medicine Radiation What is Incidence Cancer of Melanocytes Melanocytes are normal
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Cytokines: Interferons, Interleukins and Beyond. Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center
 Cytokines: Interferons, Interleukins and Beyond Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center Disclosures Advisory Boards: Bristol-Myers Squibb,Amgen, Novartis, Alkermes, Infinity,
Cytokines: Interferons, Interleukins and Beyond Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center Disclosures Advisory Boards: Bristol-Myers Squibb,Amgen, Novartis, Alkermes, Infinity,
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
DISCLOSURES. Roche/MSD-Merck/Celgene: Research Funding
 DISCLOSURES Roche/MSD-Merck/Celgene: Research Funding Roche/Celgene/AstraZeneca/Amgen/MSD/Novartis/Sanofi- Aventis/Pierre Fabré: Advisory Board or Consultant No conflict of interest with respect to this
DISCLOSURES Roche/MSD-Merck/Celgene: Research Funding Roche/Celgene/AstraZeneca/Amgen/MSD/Novartis/Sanofi- Aventis/Pierre Fabré: Advisory Board or Consultant No conflict of interest with respect to this
Complications of Immunotherapy
 Complications of Immunotherapy Sarah Norskog, PharmD, BCOP Oncology Pharmacy Specialist University of Colorado Hospital Disclosures I have no relevant financial relationships with commercial interests
Complications of Immunotherapy Sarah Norskog, PharmD, BCOP Oncology Pharmacy Specialist University of Colorado Hospital Disclosures I have no relevant financial relationships with commercial interests
MELANOMA: THE BEST OF THE YEAR Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone
 MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY
 ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
TOXICITY RELATED TO IO IN LUNG CANCER
 TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico
TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico
Current State of Immunotherapy for Metastatic Melanoma
 Current State of Immunotherapy for Metastatic Melanoma Background: The Duval County Medical Society (DCMS) is proud to provide its members with free continuing medical education (CME) opportunities in
Current State of Immunotherapy for Metastatic Melanoma Background: The Duval County Medical Society (DCMS) is proud to provide its members with free continuing medical education (CME) opportunities in
Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy
 due to Cancer Immunotherapy") Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy Philip Mease MD Director, Rheumatology Clinical Research, Swedish- Providence St. Joseph Health Clinical Professor, University of Washington
Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy Philip Mease MD Director, Rheumatology Clinical Research, Swedish- Providence St. Joseph Health Clinical Professor, University of Washington
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
Melanoma: Early Detection and Therapeutic Progress
 Melanoma: Early Detection and Therapeutic Progress David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Surgery Thanks to my collaborators, mentors and patients May 19, 2017 Disclosures:
Melanoma: Early Detection and Therapeutic Progress David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Surgery Thanks to my collaborators, mentors and patients May 19, 2017 Disclosures:
Melanoma: The poster child for immunotherapy Jason J. Luke, M.D., F.A.C.P.
 Melanoma: The poster child for immunotherapy Jason J. Luke, M.D., F.A.C.P. SITC Immunotherapy CME - June 23 rd, 2016 Disclosures Consultancy: Amgen Array Research Grant Support to Institution: Bristol
Melanoma: The poster child for immunotherapy Jason J. Luke, M.D., F.A.C.P. SITC Immunotherapy CME - June 23 rd, 2016 Disclosures Consultancy: Amgen Array Research Grant Support to Institution: Bristol
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD
 Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER. Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia
 IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
Metastasectomy for Melanoma What s the Evidence and When Do We Stop?
 Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
CANCER IMMUNOTHERAPY. Pocket Guide
 CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
Exploring Immunotherapies: Beyond Checkpoint Inhibitors
 Exploring Immunotherapies: Beyond Checkpoint Inhibitors Authored by: Jennifer Dolan Fox, PhD VirtualScopics (Now part of BioTelemetry Research) jennifer_fox@virtualscopics.com +1 585 249 6231 Introduction
Exploring Immunotherapies: Beyond Checkpoint Inhibitors Authored by: Jennifer Dolan Fox, PhD VirtualScopics (Now part of BioTelemetry Research) jennifer_fox@virtualscopics.com +1 585 249 6231 Introduction
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
WHAT S HOT IN MELANOMA CNS METASTASES?
 WHAT S HOT IN MELANOMA CNS METASTASES? GIUSEPPE MINNITI, MD, PHD Radiation Unit, UPMC, Hillman Cancer Center, San Pietro Hospital, Rome, and IRCCS Neuromed, Pozzilli (IS), Italy Marseille, September 21-22,
WHAT S HOT IN MELANOMA CNS METASTASES? GIUSEPPE MINNITI, MD, PHD Radiation Unit, UPMC, Hillman Cancer Center, San Pietro Hospital, Rome, and IRCCS Neuromed, Pozzilli (IS), Italy Marseille, September 21-22,
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Update on Targeted Therapy in Melanoma
 Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Cutaneous melanoma: new developments for 2018
 Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Pembrolizumab: First in Class for Treatment of Metastatic Melanoma
 Section Editors: Christopher J. Campen and Beth Eaby-Sandy Pembrolizumab: First in Class for Treatment of Metastatic Melanoma CARRIE BARNHART, PharmD From Billings Clinic Cancer Center, Billings, Montana
Section Editors: Christopher J. Campen and Beth Eaby-Sandy Pembrolizumab: First in Class for Treatment of Metastatic Melanoma CARRIE BARNHART, PharmD From Billings Clinic Cancer Center, Billings, Montana
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Melanoma Immunotherapy. Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management
 Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Systemic implications of Melanoma. Melanoma 2/4/2018. Cancer USA Epidemiology: Incidence and Mortality. Skin Cancer USA
 Systemic implications of Melanoma Darrell S. Rigel, MD MS Clinical Professor of Dermatology New York University Medical Center New York, New York DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Darrell
Systemic implications of Melanoma Darrell S. Rigel, MD MS Clinical Professor of Dermatology New York University Medical Center New York, New York DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Darrell
IMMUNOTARGET THERAPY: ASPETTI GENERALI
 IMMUNOTARGET THERAPY: ASPETTI GENERALI Alessandro Minisini Dipartimento di Oncologia Azienda Ospedaliero Universitaria Udine Verona, 19 settembre 2015 HALLMARKS OF CANCER Douglas Hanahan, Robert A. Weinberg,
IMMUNOTARGET THERAPY: ASPETTI GENERALI Alessandro Minisini Dipartimento di Oncologia Azienda Ospedaliero Universitaria Udine Verona, 19 settembre 2015 HALLMARKS OF CANCER Douglas Hanahan, Robert A. Weinberg,