Melanoma- Fighting the Dark Side
|
|
|
- Adam Griffin
- 5 years ago
- Views:
Transcription

1 Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
2 Disclosures American Osteopathic College of Dermatology Anna C. Pavlick, BSN, MSc, DO, MBA I have the following financial relationships to disclose: Consultant for: BMS, Merck, Novartis Research Support (funds go to NYU); BMS, Merck, Novartis, Celldex, Millineum, Genentech, Roche I will investigational in clinical trials in my presentation. I will not discuss off label use.
3 Overview Overview of Cutaneous Metastatic Melanoma Targeted Therapies BRAF inhibitors MEK inhibitors Checkpoint Inhibitors CTLA4 inhibition PD1 inhibition Combination therapy Conjugated Monoclonal Antibodies
4 Melanoma Most deadly of all skin cancers If caught early, it is 95% curable One person dies from melanoma every hour Only cancer in the US that is rising 1 in 50 Americans will be diagnosed with melanoma Once you have one melanoma you are 10 times more likely to develop another melanoma Risk for melanoma doubles if you have had more than 5 sunburns One or more blistering sunburn as a child doubles melanoma risk Use of tanning beds dramatically increases melanoma risk
5 Metastatic Disease Less than 5% of all patients survived for 5 years with metastatic disease prior to 2011 With new therapies, approximately 25% of patients will survive metastatic disease. Disease response to therapy is approximately 75% 50% with metastatic disease develop brain metastases. 2 FDA approved therapies prior to 2011: Dacarbazine and Il-2-both with response rates between 6 and 15% and NO impact on overall survival ipilimumab and BRAF inhibitors FDA approved and changed overall survival.


6 Unprecedented Progress : Two Different Approaches Targeting MAP Kinase Pathway Immune Checkpoint Inhibitors
7 Targeted Therapies
8 Mutations in Melanoma BRAF NRAS MEK KIT GNAQ GNA11
9 BRAF Mutated in approximately 50% of melanoma Most common mutation is V600E Other mutations- V600 K (20%), V 600D, 601 Sensitivity to BRAF inhibitors to be defined Younger age, fewer markers of chronic sun damage, trunk primary, superficial spreading melanoma or nodular subtype. Perhaps worse overall survival

10 MAPK and PI3K Pathways RTK KIT mut 20% ~10-20% mucosal ~10-20% acral ~20-25% ~10% cutaneous ~9% mucosal ~9% acral ~50% Primarily cutaneous melanomas NRAS RAS mut P BRAF RAF mut P MEK PI3K P Akt P ERK P mtor Cell Responses








11 The Target: B-RAF Kinase RTK RAS ATP MEKi ATP Trametinib BRAF V600E Raf MEK ERK BRAFi Vemurafenib Dabrafenib Cellular Proliferation




12 2 nd Generation V600-Selective BRAF Inhibitors Vemurafenib Dabrafanib/GSK Day 1 Day 15 Pre Week 10 Flaherty NEJM, 2010 Long, ESMO, 2010 ORR Median PFS (Mos) OS at 6 Mos Vemurafenib 48.6% % DTIC 5.5% % Chapman, NEJM, 2011

13

14

15

16
17 Possible Adverse Effects of BRAFi Arthralgias Myalgias Rash Hepatotoxicity Hand/Foot Syndrome Pyrexia Photosensitivity New cutaneous skin cancers (SCC, Melanoma)

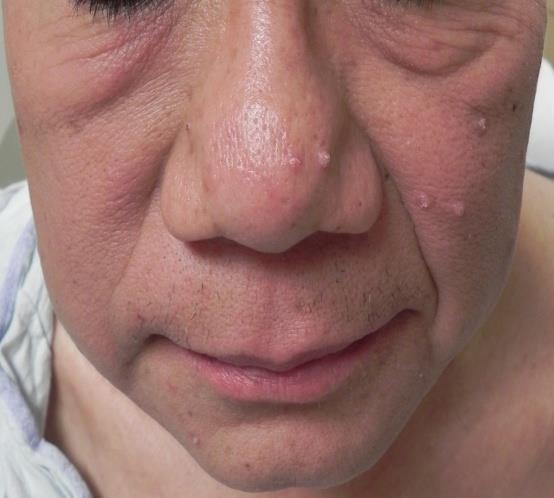


18 Skin Toxicities-BRAFi Plantar-palmar Hyperkeratoses Squamous Cell Carcinoma Verrucal Lesion



19 Diffuse Macular Rash From BRAF Inhibitor
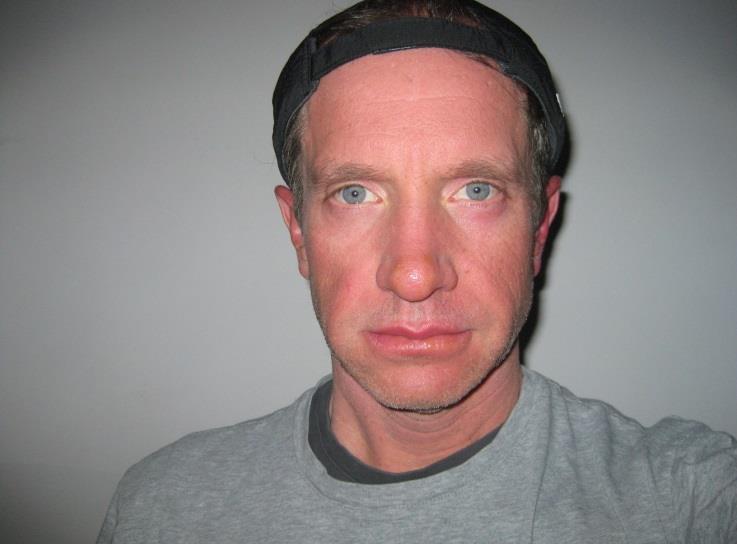
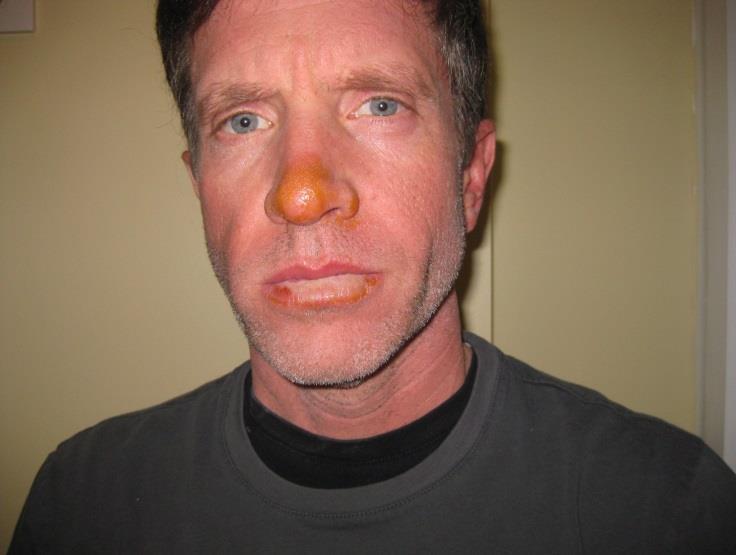
20 Photosensitivity Secondary to BRAF Inhibitors
21 BRAF/MEK Inhibition
22 Progression Progression-Free Survival Survival Mono = Dabrafenib monotherapy 150/1 = Dabrafenib (150 mg) plus trametinib (1 mg) 150/2 = Dabrafenib (150 mg) plus trametinib (2 mg) Flaherty KT et al. N Engl J Med 2012 Sept 29;[Epub ahead of print]
23
24 Maximum percent reduction from baseline measurement MEK, BRAF & BRAF/MEK combination (1 st line) Trametinib 2 mg QD Disease stage IIIC M1a M1b M1c Unknown Dabrafenib 150 mg BID Flaherty KT et al. NEJM Best confirmed response Progressive disease Stable disease Partial response Complete response Dabrafenib 150 mg BID/Trametinib 2 mg QD Long G et al. ESMO 2012

25 Rash on MEK Inhibitor

26 Erythematous Acneiform Rash Typical of MEK Inhibitors

27 Erythema Surrounding All Tattoos
28 Checkpoint Inhibitors
29 Anti-CTLA4 Monoclonal Antibodies for Melanoma Stimulate T cells to recognize cancer antigens and develop mechanisms for cell death- taking the brakes off the immune system Break tolerance of T cells to self antigens in order to permit anti-tumor response Potential side effects are autoimmune diseases
30 Ipilimumab Augments T-Cell Activation and Proliferation T-cell activation T-cell inhibition T-cell remains active T-cell T-cell T-cell CD28 CTLA-4 TCR CD28 TCR CTLA-4 TCR APC HLA CD80/ CD86 APC HLA CD80/ CD86 APC HLA CD80/ CD86 Ipilimumab blocks CTLA-4 Adapted from O Day et al. Plenary session presentation, abstract #4, ASCO 2010.
31 Antigen recognition by T cells activation T cell ab T cell antigen receptor (TCR) cytokines MHC Antigen presenting cell Antigen Processing
, dacarbazine, temozolomide, fotemustine, or carboplatin.")
32 Pivotal Phase 3 Study of Ipilimumab a Due to the inclusion of the gp100 peptide vaccine comparator, the study was restricted to patients with HLA-A2*0201 genotype. b All patients had been previously treated with one or more of the following: aldesleukin (IL-2), dacarbazine, temozolomide, fotemustine, or carboplatin. Primary Endpoint: Overall survival in ipilimumab + gp100 arm vs gp100 arm 14
33 Ipilimumab Overall Survival 1 Year OS = 46% 2 Year OS =24% ipilimumab + gp100 (A) ipilimumab alone (B) gp100 alone (C) Survival Rate 1 2 Years 3 4 ipilimumab + gp100 N=403 ipilimumab + placebo N=137 gp100 + placebo N=136 1 year 44% 46% 25% 2 year 22% 24% 14% Hodi et al NEJM 2010
 Dermatitis (43.5%) Panhypopituitary Hypophysitis (4%) Adrenal failure (1.")
34 Ipilimumab Toxicities Management: 1) Early Detection 2) Early Consult 3) Early Treatment (Steroids) Thyroiditis ( %) Dermatitis (43.5%) Panhypopituitary Hypophysitis (4%) Adrenal failure (1.5-3%) ALT/AST rise( 30%*) Hepatitis (4%) Colitis Diarrhea( 30%)

35 Immune-Mediated Side Effects: Time to Onset Time-to-onset data are not available for hepatitis, neuropathy, and other immune-mediated side effects 1. YERVOY package insert. Princeton, NJ: Bristol-Myers Squibb; Data on file. YERV
36 Nonconventional Kinetics Are Most Apparent With Pseudo-Progression Pseudo-progression may occur when T-cell infiltration causes tumors to flare or new lesions to appear upon imaging 1 Considerations when evaluating true progression vs pseudo-progression May indicate progression May indicate pseudo-progression Performance status Deterioration of performance Remains stable or improves Systemic symptoms Worsen May or may not improve Symptoms of tumor enlargement Tumor burden Baseline New lesions Present Increase Appear and increase in size May or may not be present Increase followed by response Appear then remain stable and/or subsequently respond Biopsy may reveal Evidence of tumor growth Evidence of T-cell infiltration 1. Wolchok JD, et al. Clin Cancer Res. 2009;15: ; 2. Topalian SL, et al. N Engl J Med. 2012;366: ; 3. Eisenhauer EA, et al. Eur J Cancer. 2009;45: ; 4. Chow LQ. Am Soc Clin Oncol Educ Book. 2013: ; 5. American Cancer Society. Lung Cancer. Accessed September 30, 2013.








37 Ipilimumab: Response After Tumor Volume Increase Screening Week 72 Durable & ongoing response without signs of IRAEs Week 12 Initial increase in total tumor burden (mwho PD) Week 16 Responding Courtesy of K. Harmankaya and S. Hodi


38 11/28/06 1/9/14


39 Tumorous nodule with melanin pigment (macrophages and lymphocytes; no melanocytes) Macrophages and lymphocytes are present, but no tumor cells


40 Skin Toxicity Ribas, A. et al. J Clin Oncol; 23:

41 Hair Depigmentation

42

43
44 Anti-PD1 Antibodies for Melanoma Immunotherapy for melanoma only available through clinical trials targets anti-programmed cell death 1 receptor. Targets PDL-1and 2 receptors on tumor cells. As a single agent approximately 30% of patients with metastatic melanoma respond. Less of a chance of side effects when compared to ipilimumab. Side effects include rash, itching, diarrhea and pneumonitis. Given by vein every 2-3 weeks depending on PD1 compound. May be even better if combined with ipilimumab, but toxicity is also increased.




45 Role of PD-1 Pathway in Tumor Immunity Recognition of tumor by T cell through MHC/antigen interaction mediates IFNγ release and PD-L1/2 up-regulation on tumor Priming and activation of T cells through MHC/antigen & CD28/B7 interactions with antigen-presenting cells IFNγ IFNγR MHC T-cell receptor T-cell receptor MHC Tumor cell PD-L1 PD-L2 PD-1 Shp-2 PI3K NFκB Other T cell Shp-2 CD28 PD-1 B7 PD-L1 Dendritic cell PD-1 PD-1 PD-L2 Sznol et al., ASCO, 2013 Nivolumab PD-1 Receptor Blocking Ab 45
46 Change in target lesions from baseline (%) Best Responses in All Evaluable Patients in Sequenced Cohorts -80 Patients Patients who had stable disease with prior ipilimumab treatment. Patients who had radiographic D. Wolchok, progression PhD with prior ipilimumab treatment.


47 Pembrolizumab (anti-pd1) Skin Rash
48 Dual Checkpoint Blockade



49 Blocking CTLA-4 and PD-1 Tumor Microenvironment Activation (cytokines, lysis, proliferation, migration to tumor) Dendritic cell MHC B7 TCR CD B7 CTLA anti-ctla-4 T cell CTLA-4 Blockade (ipilimumab) T cell TCR MHC PD-1 PD-L1 anti-pd-1 PD-1 PD-L2 anti-pd-1 PD-1 Blockade (nivolumab) Tumor cell
50 Phase II CA : Study Design Eligible patients with unresectable stage III or IV melanoma Treatment-naïve BRAF WT (N = 100) or MT (N = 50) Stratified by BRAF status R 2:1 NIVO 1 mg/kg + IPI 3 mg/kg Double-blind Placebo + IPI 3 mg/kg Q3Wx4 Q3Wx4 NIVO 3 mg/kg Placebo Q2W Q2W Treat until: disease progression a or unacceptable toxicity a Treatment beyond initial investigator-assessed RECIST v1.1- defined progression is permitted in patients experiencing clinical benefit and tolerating study therapy. Arm B patients have option to receive nivolumab monotherapy after progression. Upon confirmed progression and change of treatment, all patients are unblinded. MT = mutation; PFS = progression-free survival; Q3W = every 3 weeks; WT = wild type Primary endpoint: ORR in BRAF WT patients Secondary endpoints: PFS in BRAF WT patients ORR and PFS in BRAF MT patients Safety
51 Objective Response, Investigator-Assessed All Randomized Patients NIVO + IPI (N = 95) IPI (N = 47) ORR, % (95% CI) a 59 (48, 69) 11 (4, 23) P value for comparison < Best overall response, % b Complete response 22 0 Partial response Stable disease Progressive disease Unable to determine a (Complete response + partial response)/(all randomized patients); 95% CI based on Clopper and Pearson method b RECIST v1.1 CI = confidence interval


52 PD-1 Inhibition after Ipilimumab Progression 7/1/13 3/20/14
53 Probability of Progression-Free Survival PFS in All Randomized Patients Death or disease progression, n/n Median PFS, months (95% CI) HR (95% CI) NIVO + IPI (N=95) IPI (N=47) 42/95 32/47 NR 0.39 (0.25, 0.63) 3.0 ( ) NIVO + IPI (all randomized) IPI (all randomized) Number of Patients at Risk NIVO + IPI Progression-Free Survival (months) IPI monotherapy
54 Probability of Progression Free Survival PFS in Patient Subgroups: M1c Stage M1c stage subgroup Death or disease progression, n/n Median PFS, mo (95% CI) NIVO + IPI 22/ (4.1, NA) IPI monotherapy 14/ (2.7, 6.8) Nivolumab + Ipilimumab Ipilimumab Number of Patients at Risk Nivolumab + Ipilimumab Progression-Free Survival per Investigator (months) Ipilimumab
55 Patients Alive and Progression-Free (%) PFS in Patient Subgroups: BRAF V600 Mutation-positive BRAF V600 mutant subgroup Death or disease progression, n/n Median PFS, mo (95% CI) NIVO + IPI 12/ (2.8 NR) IPI monotherapy 7/ ( ) Nivolumab + Ipilimumab (N = 23) Ipilimumab (N = 10) Number of Patients at Risk Nivolumab + Ipilimumab Progression-Free Survival (months) Ipilimumab
56 Safety Summary Patients Reporting Event, % NIVO + IPI (N = 94) a IPI (N = 46) a Any Grade Grade 3 4 Any Grade Grade 3 4 Treatment-related AEs Age <65 years Age 65 years M1c disease Treatment-related AEs leading to discontinuation Treatment-related death 3 b 0 a Safety was evaluated in all patients who received at least one dose of study treatment b Associated with ventricular arrhythmia, pneumonitis, and pneumonia/hypercalcemia AEs = adverse events
57 Most Common Treatment-Related Select AEs Patients Reporting, % NIVO + IPI (N = 94) a IPI (N =46) a Any Grade Grade 3 4 Any Grade Grade 3 4 Gastrointestinal AEs Diarrhea Colitis Hepatic AEs ALT increased AST increased Pulmonary AEs Pneumonitis Renal AEs Creatinine increased Endocrine AEs Thyroid disorder Hypothyroidism Hypophysitis Skin AEs Rash Pruritus Apart from endocrinopathies, the majority (~80%) of treatment-related select AEs resolved when immune-modulating medications were utilized
58 Time to Onset of Grade 3/4 Treatment-related Select AEs in Patients Treated with Immune-modulating Medication Skin (n=8) 2.2 ( ) NIVO + IPI IPI Gastrointestinal (n=18) 6.9 ( ) Gastrointestinal (n=5) 5.7 ( ) Endocrine (n=5) Endocrine (n=2) Hepatic (n=12) Pulmonary (n=2) 9.4 ( ) 8.0 ( ) 12.1 ( ) 14.6 ( ) 29.0 ( ) Renal (n=1) Weeks Most grade 3/4 treatment-related select AEs occurred during the combination phase Circles represent median; bars signify ranges.
59 Conjugated Monoclonal Antibody Glembatumumab
 Originally identified by high throughput genomic screening technologies")
60 CR011-vcMMAE-Glembatumumab Fully human monoclonal IgG 2 antibody (CR011) conjugated to cytotoxic monomethyl auristatin-e (MMAE) MMAE is related to dolastatin, a marine-peptide derived tubulin inhibitor Enzyme-cleavable valine-citrulline linker Stable in the circulation Antibody targets glycoprotein NMB (GPNMB) Originally identified by high throughput genomic screening technologies Overexpressed in melanoma and other cancers
61 CR011-vcMMAE CR011-vcMMAE: Mechanism of Action MMAE vc Linker Cell membrane GPNMB Binding Cleavage Tubulin inhibition 1. CR011-vcMMAE binds to GPNMB on the surface of cancer cells 2. After internalization, the valine-citrulline linker is cleaved by endosomal enzymes 3. Free MMAE inhibits tubulin polymerization, leading to cell death




62 Presented at ASCO 2008 Immunohistochemical Staining of Patient Tumor Tissue for GPNMB Pt Pt CR011 antibody Control IgG 2 CR011 antibody Control IgG 2 Specific expression of GPNMB in patient tumor biopsies
63 CR011-vcMMAE: Phase I/II Study in Patients with Melanoma Patient Population: Unresectable Stage III or Stage IV melanoma Progressive disease at study entry Any prior cytokines or immunotherapy 1 prior cytotoxic regimen Stable brain metastases allowed Study Design: Phase I enrolls sequential cohorts of patients at increasing doses IV infusion once every 3 weeks (IV Q3W) Starting dose 0.03 mg/kg IV Q3W Phase II Simon 2-stage design Primary endpoint is response rate, n=32 Phase I Dose Escalation Establish MTD Phase II Study at MTD Simon Two Stage Design Primary Endpoint: Response Rate





64 Skin Rash from Glembatumumab
65 Conclusions: Metastatic melanoma is no longer an incurable, universally fatal disease. Immunotherapy has provided patients with long term, durable responses. Targeted therapy has provided a rapid mechanism for disease control in BRAF mutated patients. We have made dramatic strides in the treatment and long term control of melanoma, however, more work needs to be done to cure everyone. Participation in a clinical research trial remains the gold standard for patients with metastatic melanoma.
66 Acknowledgements: Thank you to all the patients who participated in our melanoma research trials and changed the outcome of this disease. Thank you to all the patient who agreed to having photos taken of their responses or toxicity, so that we could learn from them. Thank you to all of my referring physicians who trust their patients to my care Finally, thank you to my dedicated staff for their dedication to our patients and most importantly for putting up with me.
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
New Therapeutic Approaches to Malignant Melanoma
 2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Immunoterapia e melanoma maligno metastatico: siamo partiti da li. Vanna Chiarion Sileni Istituto Oncologico Veneto
 Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
Principles and Application of Immunotherapy for Cancer: Advanced Melanoma
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma
 and Binimetinib (MEK162) in Patients With Metastatic Melanoma") The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma Reinhard Dummer, 1 Keith Flaherty, 2 Richard Kefford, 3 Paolo A. Ascierto, 4 Laure Moutouh-de Parseval,
The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma Reinhard Dummer, 1 Keith Flaherty, 2 Richard Kefford, 3 Paolo A. Ascierto, 4 Laure Moutouh-de Parseval,
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
One Moment Please. Skin Cancer. Today s Webcast Friday, 09/09/11, Noon. David Carr, MD
 One Moment Please One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast Friday, 09/09/11, Noon 1 New Features Enlarge Slides Links Chapters Polling Use the email function to let
One Moment Please One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast Friday, 09/09/11, Noon 1 New Features Enlarge Slides Links Chapters Polling Use the email function to let
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Updates in Metastatic Melanoma
 SCSHP 214 Annual Meeting Updates in Metastatic Melanoma LeAnn B. orris, PharmD, BCPS, BCOP Assistant Professor South Carolina College of Pharmacy Background Estimated 76,69 new cases in 213 Increasing
SCSHP 214 Annual Meeting Updates in Metastatic Melanoma LeAnn B. orris, PharmD, BCPS, BCOP Assistant Professor South Carolina College of Pharmacy Background Estimated 76,69 new cases in 213 Increasing
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies
 Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies
 Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Update on Targeted Therapy in Melanoma
 Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Combination Approaches in Melanoma: A Balancing Act
 Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Response and resistance to BRAF inhibitors in melanoma
 Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
Melanoma: Early Detection and Therapeutic Progress
 Melanoma: Early Detection and Therapeutic Progress David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Surgery Thanks to my collaborators, mentors and patients May 19, 2017 Disclosures:
Melanoma: Early Detection and Therapeutic Progress David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Surgery Thanks to my collaborators, mentors and patients May 19, 2017 Disclosures:
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
presentation session & clinical Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania
 Melanoma: highlights from the oral presentation session & clinical science symposium at ASCO 2009 Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania Abstracts to be discussed
Melanoma: highlights from the oral presentation session & clinical science symposium at ASCO 2009 Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania Abstracts to be discussed
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
New treatments in melanoma
 New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
Normal RAS-RAF (MAPK) pathway signaling
 pathway signaling") BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial
: Results of a phase I trial") Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove)
") Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Nivolumab in Hodgkin Lymphoma
 Nivolumab in Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Chair, Lymphoma Group Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers Squibb Celldex Therapeutics Seattle
Nivolumab in Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Chair, Lymphoma Group Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers Squibb Celldex Therapeutics Seattle
Enlarge Slides. One Moment Please. Skin Cancer. Thomas Olencki, DO David Carr, MD. Today s Webcast Friday, 09/09/11, Noon
 New Features Enlarge Slides Links One Moment Please Chapters Polling Use the email function to let us know what you think One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast
New Features Enlarge Slides Links One Moment Please Chapters Polling Use the email function to let us know what you think One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma
 Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Modern therapy in oncology Metastatic melanoma
 Modern therapy in oncology Metastatic melanoma Anna Buda-Nowak Oncology Department; University Hospital in Cracow Melanoma Malignant skin neoplasm derived from neuroectodermal melanomatous cells. The incidence:
Modern therapy in oncology Metastatic melanoma Anna Buda-Nowak Oncology Department; University Hospital in Cracow Melanoma Malignant skin neoplasm derived from neuroectodermal melanomatous cells. The incidence:
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic
 Dabrafenib for treating unresectable, advanced or metastatic") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
Advances in Melanoma
 Advances in Melanoma The Blue, the Black and the Ugly 1 Outline History of Melanoma Why be concerned? Skin cancer updates What s old? What s new (and why are Skin Tumor Group med oncs excited again)? What
Advances in Melanoma The Blue, the Black and the Ugly 1 Outline History of Melanoma Why be concerned? Skin cancer updates What s old? What s new (and why are Skin Tumor Group med oncs excited again)? What
Interleukin-2 Single Agent and Combinations
 Interleukin-2 Single Agent and Combinations Michael K Wong MD PhD Norris Cancer Center University of Southern California mike.wong@med.usc.edu Disclosures Advisory Board Attendance Merck Bristol Myers
Interleukin-2 Single Agent and Combinations Michael K Wong MD PhD Norris Cancer Center University of Southern California mike.wong@med.usc.edu Disclosures Advisory Board Attendance Merck Bristol Myers
Melanoma in Focus: Update on Novel Therapy, Emerging Agents, and Optimizing Patient Care Presentation 1
 Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
A Phase 2 Study of Glembatumumab Vedotin, an Antibody Drug Conjugate Targeting gpnmb, in Advanced Melanoma
 A Phase 2 Study of Glembatumumab Vedotin, an Antibody Drug Conjugate Targeting gpnmb, in Advanced Melanoma Patrick A. Ott, MD, PhD 1, Anna C. Pavlick, DO 2, Douglas B. Johnson, MD 3, Lowell Hart, MD 4,
A Phase 2 Study of Glembatumumab Vedotin, an Antibody Drug Conjugate Targeting gpnmb, in Advanced Melanoma Patrick A. Ott, MD, PhD 1, Anna C. Pavlick, DO 2, Douglas B. Johnson, MD 3, Lowell Hart, MD 4,
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
BRAF Inhibitors in Metastatic disease. Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia
 Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use
 Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
 Overall Survival (OS) Analysis From an Expanded Access Program (EAP) of Nivolumab (NIVO) in Combination with Ipilimumab (IPI) in Patients with Advanced Melanoma (MEL) David Hogg, Paul B. Chapman, 2 Mario
Overall Survival (OS) Analysis From an Expanded Access Program (EAP) of Nivolumab (NIVO) in Combination with Ipilimumab (IPI) in Patients with Advanced Melanoma (MEL) David Hogg, Paul B. Chapman, 2 Mario
Evan J. Lipson, M.D.
 Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
BRAF Inhibition in Melanoma
 BRAF Inhibition in Melanoma New York City, Mar 22-23, 2013 Bartosz Chmielowski, MD, PhD Assistant Clinical Professor University of California Los Angeles Disclosures Speaker Bureau: BMS, Genentech, Prometheus
BRAF Inhibition in Melanoma New York City, Mar 22-23, 2013 Bartosz Chmielowski, MD, PhD Assistant Clinical Professor University of California Los Angeles Disclosures Speaker Bureau: BMS, Genentech, Prometheus
Array BioPharma Jefferies 2016 Global Healthcare Conference. June 9, 2016
 Array BioPharma Jefferies 216 Global Healthcare Conference June 9, 216 Safe Harbor Statement 2 Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Array BioPharma Jefferies 216 Global Healthcare Conference June 9, 216 Safe Harbor Statement 2 Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Name of Policy: Yervoy (Ipilimumab)
") Name of Policy: Yervoy (Ipilimumab) Policy #: 335 Latest Review Date: October 2013 Category: Pharmacology Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Yervoy (Ipilimumab) Policy #: 335 Latest Review Date: October 2013 Category: Pharmacology Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Pembrolizumab: First in Class for Treatment of Metastatic Melanoma
 Section Editors: Christopher J. Campen and Beth Eaby-Sandy Pembrolizumab: First in Class for Treatment of Metastatic Melanoma CARRIE BARNHART, PharmD From Billings Clinic Cancer Center, Billings, Montana
Section Editors: Christopher J. Campen and Beth Eaby-Sandy Pembrolizumab: First in Class for Treatment of Metastatic Melanoma CARRIE BARNHART, PharmD From Billings Clinic Cancer Center, Billings, Montana
Immunotherapy for the Treatment of Cancer
 Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Improving Immunotherapy for Melanoma
 Improving Immunotherapy for Melanoma David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/ Harvard Cancer Center Harvard Medical School Immunotherapy Improvement Model All patients All
Improving Immunotherapy for Melanoma David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/ Harvard Cancer Center Harvard Medical School Immunotherapy Improvement Model All patients All
 for patients with ECOG PS 0-1 as indicated in the CheckMate-067 trial. Upon reconsideration of the Initial Recommendation, perc noted PAG s feedback requesting guidance on extrapolating eligibility to
for patients with ECOG PS 0-1 as indicated in the CheckMate-067 trial. Upon reconsideration of the Initial Recommendation, perc noted PAG s feedback requesting guidance on extrapolating eligibility to
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment
 Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo
 U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo (nivolumab) in Patients with Previously Untreated Advanced Melanoma Application includes CheckMate -066,
U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo (nivolumab) in Patients with Previously Untreated Advanced Melanoma Application includes CheckMate -066,
Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy
 due to Cancer Immunotherapy") Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy Philip Mease MD Director, Rheumatology Clinical Research, Swedish- Providence St. Joseph Health Clinical Professor, University of Washington
Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy Philip Mease MD Director, Rheumatology Clinical Research, Swedish- Providence St. Joseph Health Clinical Professor, University of Washington
Ipilimumab ASCO Data Review and Discussion Webcast. Monday, June 2, 2008
 Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER. Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia
 IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
Immunotherapy: Toxicity Management. Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital
 Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
METRIC Study Key Eligibility Criteria
 The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro. Immune checkpoint inhibition in DLBCL
 Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
ONCOS-102 in melanoma Dr. Alexander Shoushtari. 4. ONCOS-102 in mesothelioma 5. Summary & closing
 ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology