|
|
|
- Chastity Maxwell
- 6 years ago
- Views:
Transcription
1 Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009
2 Questions The T and N status of esophageal carcinoma is most accurately assessed by? A. Upper gastrointestinal series B. Computed tomographic scan of the chest with double contrast C. Endoscopic ultrasound (EUS) D. Positron emission i tomography (PET scan) E. Magnetic resonance imaging (MRI)
3 Questions Which of the following statements about the incidence, location, and type of esophageal cancer is TRUE? A. The overall rate is decreasing B. Proximal squamous cell lesions are increasing C. Proximal adenocarcinomas are increasing D. Distal adenocarcinomas are increasing E. Distal squamous cell cancers are decreasing
4 Questions When mobilizing the stomach in an esophagectomy, which h vessel is preserved? A. Left gastric artery B. Short gastric arteries C. Left gastroepiploic artery D. Right gastroepiploic i artery
5 Questions In a patient without metastatic disease who completes neoadjuvant chemotherapy and radiation therapy, the 5-yr survival after complete resection would be? A. 5% B. 10% C. 35% D. 50% E. 75%
6 Questions Substantial mortality from anastomotic leakage A. Transthoracic (Ivor Lewis) esophagectomy B. Transhiatal esophagectomy C. Both D. Neither
7 History & Physical 48 yo female c/o dysphagia since 5/2008, primarily solid foods then progressing to liquids w/100 lb wt loss over 10 months. Pt c/o post-prandial p vomiting. PMH: htn, DM, asthma PSH/ FHx: denies SocHx: 1 ½ ppw x30yrs; occ etoh 3-4/wk Physical Exam: No significant findings






8 EGD 10/14/2008
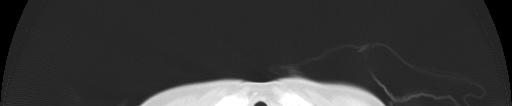
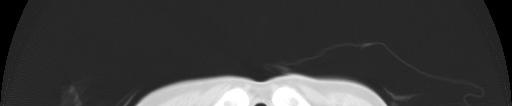
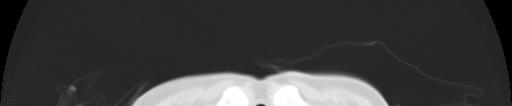
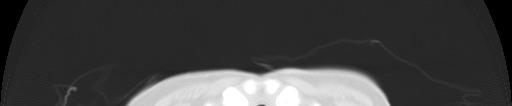
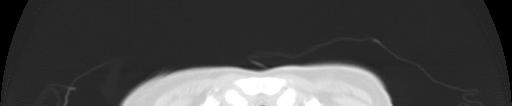
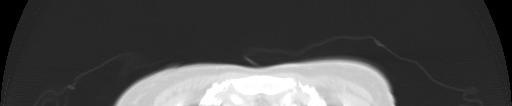
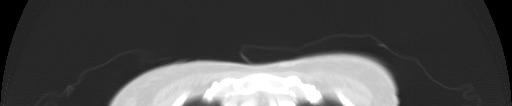
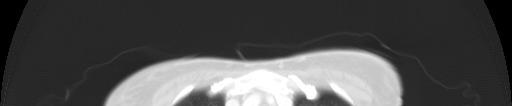
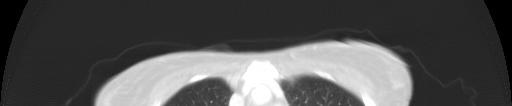
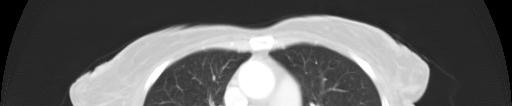
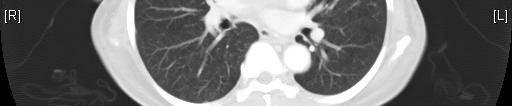

9 Esophageal CA CT Scan ¾ CT chest/abd/pelvis 10/15/2008 mass midesophagus w/proximal arch & extending to low pulmonary vein (4.2x2.7cm)




10 Esophagogram g


11 Studies Bronchoscopy 10/16/2008 Whitish lesion post tracheal wall above carina, histo neg ENT laryngoscopy No vocal cord paralysis/involvement PET scan Neg
 Eh Echo EF 60%, nl LVSF & wall motion, PAP 34, mild MR/TR Stress echo peak stress")
12 Cardiopulmonary Function PFTs 10/17/2008 FEV (64%); FEV 1 /FVC 77%; DLCO 17.9 (78%) Eh Echo EF 60%, nl LVSF & wall motion, PAP 34, mild MR/TR Stress echo peak stress EF 75%
13 EUS 10/27/2009 Friable tumor 70% circumference upper 1/3 esophagus w/ulcerated narrowing & severe obstruction T3 Nx Mx




14 Chemotherapy & XRT Radiation 11/17/ /19/ cgy to esophagus & supraclavicular region Chemotherapy Cisplatin & 5-FU Sx improved Re-gained 50 lbs w/appetite simulants
15 Laboratory work-up MCV 89 RDW13.3 TP 6.6 Alb 3.33 Tbili 0.2 Dbili 0 AST 43 ALT 30 AP 84 AMY 52 Lip 91 CEA 2.3
16 Operative Report 2/10/2009 Exploratory laparotomy, gastric mobilization, pyloromyotomy, feeding jejunostomy Esophagoscopy Right thoracotomy, esophagectomy w/esophagogastric anastomosis Time IVF PRBCS EBL UO 13.5 hrs 11.5 L 2 Units 700 ml 1200 ml








17 Ivor Lewis Esophagectomy
18 Gross Specimen


19 Celiac Node Metastatic moderately well differentiated keratinizing Squamous cell CA


20 Esophagus Moderately well 30mm proximal margin differentiated keratinizing Squamous cell CA Invades esophageal wall Extends to adventitia 6 neg LN T3 N1 M0 G2




21 Hospital Course POD#2 Extubated in SICU 2U PRBCs Tube feeds started POD#7 Esophagogram neg POD#9 D/C home
22 Esophageal Cancer
23 Introduction Incidence increasing 4% of all cancers dx d each year Overall poor rate of survival Adenocarcinoma has risen 6x over last quarter century Squamous cell carcinoma Smoking & ETOH Adenocarcinoma Barrett s Esophagus Long-standing GERD

")
24 Presentation Dysphagia Endoscopy: Chronic GERD BE surveillance Bleeding (anemia or hematemesis) Chest or abd pain

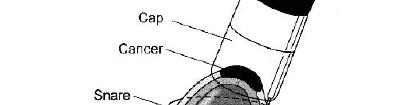

25 Diagnosis Confirm dx: Bx EsophagoGastroDuodenoscopy Endoscopic c US Endoscopic Mucosal Resection
26 Resectability Determine extent of dz Local, regional & systemic CT chest PET scan PET-CT CT PET Scan CT
27 Pre-operative Assessment Evaluate physiologic i status t Cardiac & pulmonary reserve PFTs Noninvasive cardiac stress eval Nutritional status
28 Priniciples of Esophagectomy Standard of care for non-metastatic esophageal CA 1º goal: complete (R 0 ) resection of tumor & surrounding lymph nodes Maximize opportunity for cure Minimize incidence of local recurrence Earlier lesions: more physiologic outcome Advanced locoregional dz w/good cardiopulmonary reserve: extended lymphadenctomy
29 Neoadjuvant Therapy Candidates for resection Neoadjuvant chemotherapy Concurrent radiation therapy Good performance status & bulky disease 20-30% rate of complete response Afterwards, re-stage w/barium swallow & CT Resection in 2-3 wks after Chemo/XRT
30 Different Surgical Approaches Transhiatal Blind dissection in chest Cervical esophagogastrostomy Ivor-Lewis Abdominal/thoracic dissection Intra-thoracic esophagogastrostomy En bloc esophagectomy Left thoracoabdominal Cervical esophagogastrostomy Minimally invasive Laparoscopic ± thoracoscopic
31 Transhiatal Esophagectomy
32 Ivor-Lewis Esophagectomy
33 En Bloc esophagectomy
34 Reconstruction Tubularized or whole Cl Colon stomach Unusable stomach Easiest Single anastomosis Enough length for neck Effective alimentary conduit Intestine Prior Surgery Extensive tumor Most complex Last resort
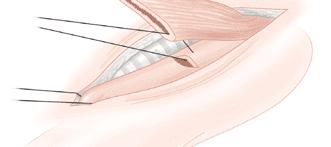
35 Division of Gastrohepatic Ligament & Mobilization of Distal Esophagus
36 Mobilization of Stomach & Duodenum
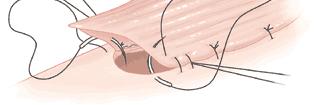
37 Pyloromyotomy & Feeding Jj Jejunostomy
38 Exposure & Mobilization of Esophagus
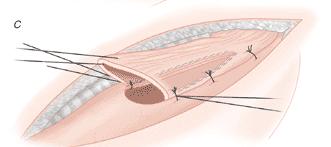
39 Excision & Removal Specimen


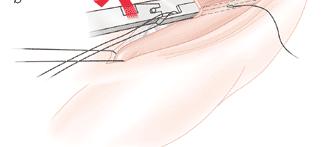
40 Esophagogastric Anastomosis
41 How to determine which procedure?
42 Tumor Depth
43 Nodal metastasis Exceedingly rare in CA limited to lamina propria Increases in incidence w/deeper penetration Recent analysis of 23 pts w/complete lymphadenctomy for intramucosal CA, 1020 LNs examined: 1 LN (0.09%) 09%) in 1 pt (4%) detected w/metastasis Lamina propria (0 of 13; 0%) Superficial muscularis mucosa (1 of 10; 10%) Hagan et al. Ann Surg. 2001; 234:520
44 Prevalence of nodal metastases & 5-yr Survival lb by depth of tumor penetration Hagan et al. Ann Surg. 2001; 234:520
45 AJCC Nodal Staging Regional lymph nodes (N) Nx cannot be assessed N0 No regional node metastasis N1 Regional node metastasis Distant metastasis (M) Mx cannot be assessed M0 No distant metastasis M1a Celiac or supraclavicular l node M1b Nonregional nodal metastasis or distant metastasis AJCC Esophageal Cancer
46 Proposed Modification of Nodal Status in AJCC Staging Retrospective study: 1027 pts ( ) Revised nodal status (3yr survival): Location (3yr survival): #LNs (3 yr survival): Nonregional: 0% (n=17) pn0: 0 nodes 63% (n=496) 0 nodes: 63% pn1: 1-3 nodes 32% (n=292) Regional: 24% (n=441) 1-3 nodes: 31% pn2: >3 nodes 14% (n=222) Celiac: 23% (n=73) >3 nodes: 13% pn3: nonregional nodes 0% (n=17) P< Location & #LNs independent predictors survival Revised: celiac nodes are regional & includes #LN Hofstetter et al. Ann Thor Surg. 2007; 84:365-75
47 Algorithm for Management of Esophageal CA




48 Algorithm for Management of Esophageal CA
49 Questions The T and N status of esophageal carcinoma is most accurately assessed by? A. Upper gastrointestinal series B. Computed tomographic scan of the chest with double contrast C. Endoscopic ultrasound (EUS) D. Positron emission i tomography (PET scan) E. Magnetic resonance imaging (MRI)
50 Questions Which of the following statements about the incidence, location, and type of esophageal cancer is TRUE? A. The overall rate is decreasing B. Proximal squamous cell lesions are increasing C. Proximal adenocarcinomas are increasing D. Distal adenocarcinomas are increasing E. Distal squamous cell cancers are decreasing
51 Questions In a patient without metastatic disease who completes neoadjuvant chemotherapy and radiation therapy, the 5-yr survival after complete resection would be? A. 5% B. 10% C. 35% D. 50% E. 75%
52 Questions When mobilizing the stomach in an esophagectomy, which h vessel is preserved? A. Left gastric artery B. Short gastric arteries C. Left gastroepiploic artery D. Right gastroepiploic i artery
53 Questions Substantial mortality from anastomotic leakage A. Transthoracic (Ivor Lewis) esophagectomy B. Transhiatal esophagectomy C. Both D. Neither





54 Esophagus Anatomy The esophagus is a muscular tube extending from the pharynx to the estomach. 4 segments Cervical esophagus From the inferior aspect of the cricoid cartilage to the thoracic inlet (suprasternal notch, ~18 cm from incisors) Thoracic esophagus Upper thoracic Thoracic inlet to level of tracheal bifurcation; cm. Mid thoracic Tracheal bifuraction midway to gastroesophageal junction; cm. Lower thoracic Midway between tracheal bifurcation and gastroesophageal junction to GE junction, including abdominal esophagus; cm. Abdominal Considered part of lower thoracic esophagus; cm.
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
 Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
RTC Dec Felicitas Koller and Eric Grogan
 RTC Dec 11 2009 Felicitas Koller and Eric Grogan Cancer Statistics, United States Number of patients 200000 150000 100000 50000 0 Lung Breast New Cases Deaths Esophageal Colorectal Prostate http://www.cancer.org/statistics
RTC Dec 11 2009 Felicitas Koller and Eric Grogan Cancer Statistics, United States Number of patients 200000 150000 100000 50000 0 Lung Breast New Cases Deaths Esophageal Colorectal Prostate http://www.cancer.org/statistics
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand?
 MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD
 Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006
 Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
AATS Focus on Thoracic Surgery: Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017?
 AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
A Proposed Strategy for Treatment of Superficial Carcinoma. in the Thoracic Esophagus Based on an Analysis. of Lymph Node Metastasis
 Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Minimally Invasive Esophagectomy
 American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
Esophageal Cancer. What is esophageal cancer?
 Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Surgical strategies in esophageal cancer
 Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Minimally Invasive Esophagectomy
 Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Esophageal cancer. What is esophageal cancer? Esophageal cancer is a disease in which malignant (cancer) cells form in the tissues of the esophagus.
 cells form in the tissues of the esophagus.") Esophageal Cancer Esophageal cancer What is esophageal cancer? What are risk factors? Signs and symptoms Tests for esophageal cancer Stages of esophageal cancer Treatment options What is esophageal cancer?
Esophageal Cancer Esophageal cancer What is esophageal cancer? What are risk factors? Signs and symptoms Tests for esophageal cancer Stages of esophageal cancer Treatment options What is esophageal cancer?
Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition
 22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Adenocarcinoma of gastro-esophageal junction - Case report
 Case Report denocarcinoma of gastro-esophageal junction - Case report nupsingh Dhakre 1*, Ibethoi Yengkhom 2, Harshin Nagori 1, nup Kurele 1, Shreedevi. Patel 3 1 2 nd year Resident, 2 3rd year Resident,
Case Report denocarcinoma of gastro-esophageal junction - Case report nupsingh Dhakre 1*, Ibethoi Yengkhom 2, Harshin Nagori 1, nup Kurele 1, Shreedevi. Patel 3 1 2 nd year Resident, 2 3rd year Resident,
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.
 Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.") Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Robotic Surgery for Esophageal Cancer
 Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Di Lu 1#, Xiguang Liu 1#, Mei Li 1#, Siyang Feng 1#, Xiaoying Dong 1, Xuezhou Yu 2, Hua Wu 1, Gang Xiong 1, Ruijun Cai 1, Guoxin Li 3, Kaican Cai 1
 Case Report Three-port mediastino-laparoscopic esophagectomy (TPMLE) for an 81-year-old female with early-staged esophageal cancer: a case report of combining single-port mediastinoscopic esophagectomy
Case Report Three-port mediastino-laparoscopic esophagectomy (TPMLE) for an 81-year-old female with early-staged esophageal cancer: a case report of combining single-port mediastinoscopic esophagectomy
Determining Resectability and Appropriate Surgery for Esophageal Cancer
 Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications
 and Clinicoradiologic Implications") Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Esophageal Cancer. Source: National Cancer Institute
 Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
ESOPHAGEAL CANCER. Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds
 ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
The present staging system for esophageal carcinoma
 Esophageal Carcinoma: Depth of Tumor Invasion Is Predictive of Regional Lymph Node Status Thomas W. Rice, MD, Gregory Zuccaro, Jr, MD, David J. Adelstein, MD, Lisa A. Rybicki, MS, Eugene H. Blackstone,
Esophageal Carcinoma: Depth of Tumor Invasion Is Predictive of Regional Lymph Node Status Thomas W. Rice, MD, Gregory Zuccaro, Jr, MD, David J. Adelstein, MD, Lisa A. Rybicki, MS, Eugene H. Blackstone,
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness
 Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Diagnosis and Preoperative Staging of Esophageal Cancer
 2 Diagnosis and Preoperative Staging of Esophageal Cancer ARNOLD J. MARKOWITZ, MD HANS GERDES, MD The clinical presentation of esophageal cancer in the United States and Europe has been changing, but unfortunately,
2 Diagnosis and Preoperative Staging of Esophageal Cancer ARNOLD J. MARKOWITZ, MD HANS GERDES, MD The clinical presentation of esophageal cancer in the United States and Europe has been changing, but unfortunately,
GASTRIC CANCER. Joyce Au SUNY Downstate Grand Rounds July 11, 2013
 GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
THORACIC SURGERY: Dysphagia. Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone. Thoracic Surgery Toronto East General Hospital
 THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Basic Principles of Esophageal Surgery. 1 Surgical Anatomy of the Esophagus... 3
 Contents Basic Principles of Esophageal Surgery 1 Surgical Anatomy of the Esophagus... 3 D. C. Broering, J. Walter, Z. Halata ] Topography of the esophagus... 3 ] Development of the esophagus... 4 ] Structure
Contents Basic Principles of Esophageal Surgery 1 Surgical Anatomy of the Esophagus... 3 D. C. Broering, J. Walter, Z. Halata ] Topography of the esophagus... 3 ] Development of the esophagus... 4 ] Structure
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
UCLA General Surgery Residency Program Rotation Educational Policy Goals and Objectives
 UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
 Rectal Cancer Sophia L Fu, MD SUNY Downstate Medical Center, Brooklyn, NY September 10, 2009 History 40 yo female w/rectal cancer treated w/chemo-xrt at Brookdale 11/08 who p/w rectal-vaginal fistula in
Rectal Cancer Sophia L Fu, MD SUNY Downstate Medical Center, Brooklyn, NY September 10, 2009 History 40 yo female w/rectal cancer treated w/chemo-xrt at Brookdale 11/08 who p/w rectal-vaginal fistula in
Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012
 Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012 Esophageal Leiomyoma Introduction Case presentation Operative video Discussion Esophageal Leiomyoma Benign tumors of the
Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012 Esophageal Leiomyoma Introduction Case presentation Operative video Discussion Esophageal Leiomyoma Benign tumors of the
Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node
 2012 66 5 417 421 Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node a b* a a a a a a a b ʼ 418 Horio et al. Acta Med. Okayama Vol.
2012 66 5 417 421 Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node a b* a a a a a a a b ʼ 418 Horio et al. Acta Med. Okayama Vol.
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Lymph node metastasis is one of the most important prognostic
 ORIGINAL ARTICLE Comparison of Survival and Recurrence Pattern Between Two-Field and Three-Field Lymph Node Dissections for Upper Thoracic Esophageal Squamous Cell Carcinoma Young Mog Shim, MD, Hong Kwan
ORIGINAL ARTICLE Comparison of Survival and Recurrence Pattern Between Two-Field and Three-Field Lymph Node Dissections for Upper Thoracic Esophageal Squamous Cell Carcinoma Young Mog Shim, MD, Hong Kwan
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Esophagus and Esophagogastric Junction
 Esophagus and Esophagogastric Junction 16 Thomas William Rice, David Kelsen, Eugene H. Blackstone, Hemant Ishwaran, Deepa T. Patil, Adam J. Bass, Jeremy J. Erasmus, Hans Gerdes, and Wayne L. Hofstetter
Esophagus and Esophagogastric Junction 16 Thomas William Rice, David Kelsen, Eugene H. Blackstone, Hemant Ishwaran, Deepa T. Patil, Adam J. Bass, Jeremy J. Erasmus, Hans Gerdes, and Wayne L. Hofstetter
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Robotic-assisted McKeown esophagectomy
 Case Report Page 1 of 8 Robotic-assisted McKeown esophagectomy Dingpei Han, Su Yang, Wei Guo, Runsen Jin, Yajie Zhang, Xingshi Chen, Han Wu, Hailei Du, Kai Chen, Jie Xiang, Hecheng Li Department of Thoracic
Case Report Page 1 of 8 Robotic-assisted McKeown esophagectomy Dingpei Han, Su Yang, Wei Guo, Runsen Jin, Yajie Zhang, Xingshi Chen, Han Wu, Hailei Du, Kai Chen, Jie Xiang, Hecheng Li Department of Thoracic
Slide 1. Slide 2. Slide 3 Pancreatic Cancer- Case #1. Endoscopic management of GI malignancy. Endoscopic approaches in GI malignancy- Agenda
 Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Oesophageal Cancer: The Image after Surgery
 Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard
 Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
Oesophageal Cancer: The Image after Surgery
 Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Laparoscopic and Thoracoscopic Ivor Lewis Esophagectomy With Colonic Interposition
 HOW TO DO IT Laparoscopic and Thoracoscopic Ivor Lewis Esophagectomy With Colonic Interposition Ninh T. Nguyen, MD, FACS, Marcelo Hinojosa, MD, Christine Fayad, BS, James Gray, BS, Zuri Murrell, MD, and
HOW TO DO IT Laparoscopic and Thoracoscopic Ivor Lewis Esophagectomy With Colonic Interposition Ninh T. Nguyen, MD, FACS, Marcelo Hinojosa, MD, Christine Fayad, BS, James Gray, BS, Zuri Murrell, MD, and
Kawahara, Katsunobu; Tomita, Masao. Citation Acta Medica Nagasakiensia. 1992, 37
 NAOSITE: Nagasaki University's Ac Title Author(s) TRANSHIATAL ESOPHAGECTOMY FOR CARCI THORACIC ESOPHAGUS Ayabe, Hiroyoshi; Tsuji, Hiroharu; Kawahara, Katsunobu; Tomita, Masao Citation Acta Medica Nagasakiensia.
NAOSITE: Nagasaki University's Ac Title Author(s) TRANSHIATAL ESOPHAGECTOMY FOR CARCI THORACIC ESOPHAGUS Ayabe, Hiroyoshi; Tsuji, Hiroharu; Kawahara, Katsunobu; Tomita, Masao Citation Acta Medica Nagasakiensia.
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion
 Clinical Case Discussion") Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Cancer of Esophagus and Esophagogastric Junction: Analysis of Results of 1,025 Resections after 5 to 20 Years
 Cancer of Esophagus and Esophagogastric Junction: Analysis of Results of 1,025 Resections after 5 to 20 Years Yun Kan Lu, M.D., Yueh Min Li, M.D., and Yue Zhi Gu, M.D. ABSTRACT Resection was carried out
Cancer of Esophagus and Esophagogastric Junction: Analysis of Results of 1,025 Resections after 5 to 20 Years Yun Kan Lu, M.D., Yueh Min Li, M.D., and Yue Zhi Gu, M.D. ABSTRACT Resection was carried out
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Imaging techniques in the diagnosis, staging and follow up of GI cancers. Moderators: Banke Agarwal, MD and Paul Schultz, MD
 Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Clinical Case Presentation. Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006
 Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da
 University of Groningen Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da IMPORTANT NOTE: You are advised
University of Groningen Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da IMPORTANT NOTE: You are advised
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these