The malignant colorectal polyp
|
|
|
- Alfred Richards
- 5 years ago
- Views:
Transcription

1 The malignant colorectal polyp Dr Ian Brown Envoi Pathology Envoi data reproduced from J Clin Path 2015 article
2 Definition Adenocarcinoma found in an endoscopically resected polypoidal tumour Submucosal invasive tumour in a pre existing adenoma (conventional or serrated) Polypoidal carcinoma ( intramucosal adenocarcinoma)
3 Importance Detection is increasing NBCSP A quality marker for pathology practice standards Surgery versus conservative Patient risk and economic benefit
4 What do we know? 1) RISK Resection specimens LN metastasis in 7-9% (Envoi - 8.0%) * most important Residual adenocarcinoma at polypectomy site 5% Residual adenoma at polypectomy site 5-10% Overall rate of residual disease = 10-15% All specimens 50-60% of endoscopic MCP are followed by resection Overall risk of LN mets all MCP = 4% Overall risk of residual disease all MCP = 7-10% (Envoi =8.7%)
5 What do we know? 2) CLINICAL Males (55-60%) Mean age years 3/4 are in rectum or sigmoid Sessile: pedunculated 6:4 (Envoi) to 4:1 (Ueno) when assessed by pathologist 1:2 when assessed by endoscopist MCP may be small 25% 10mm 1.7% 5mm
6 What do we know? 3) RISK FACTORS predict: LN mets, residual disease in wall, overall tumour specific survival 2 groups: 1) Qualitative 2) Quantitative Differentiation, vascular invasion, margin status etc Tumour size - Depth of invasion, tumour width, Haggitt, Kikuchi etc Tumour size is the most important risk factor
7 What are we trying to do? Cost benefit analysis for surgery Costs Risk of surgery morbidity and mortality Economic cost of unnecessary surgery ( sunk cost = tumour may already have metastasized beyond bowel wall or patient might die of another condition before the benefit of surgery accrues) Benefits Remove residual disease that might latter directly cause morbidity or mortality
8 What are the issues? 1) Risk of residual disease for MCP is overstated Risk criteria Degree of Risk Resection margin < 1mm 4 Resection margin 1-2mm 1 Pedunculated Haggitt level 4 4 Sessile: Kikuchi 2 2 Sessile: Kikuchi 3 4 Poor differentiation 3 Mucinous tumour 1 Tumour budding 1 Lymphovascular invasion 2 Total score % risk of residual cancer 0 <3% 1 <5% % % 4 >20% Williams JG, Pullan RD, Hill J et al. (2013). Management of the malignant colorectal polyp: ACPGBI position statement. Colorectal Dis Suppl. 2:1-38.
9 What are the issues? 1) Risk of residual disease for MCP is overstated Number of risk factors Nodal involvement Ueno Envoi 0 0.7% 2% % 8.2% % 12.2% Risk factors = poor differentiation, lymphovascular invasion and tumour budding Ueno et al Gastroenterology 2004;127: * half the MCP in this study were treated by primary surgical resection
10 What are the issues? 1) Risk of residual disease for MCP is overstated T stage N+ stage proportion (%) Rectal cancer Colon cancer All untreated CRC Envoi T1 10.2% 4.3% 6.3% T2 22.3% 19.0% 15.0% T % 38.5% 46.2% World J Gastroenterol Nov 14; 16(42):
11 What are the issues? 2) Risk of surgical resection is overstated Quoted figures (overall) mortality 2-5 % morbidity 30 % Anastomotic leak 1-4% Local colorectal surgeons are much better than this
 Risk for primary colonoscopic resection Munich polypectomy study (Endoscopy 2005;37:1116-1122) Major complication")
12 What are the issues? 3) Risk for primary colonoscopic resection Munich polypectomy study (Endoscopy 2005;37: ) Major complication rate = death, perforation, bleeding BSG audit perforation %, bleeding %, readmission 0.14%
13 SEER data What are the issues? 4) The 5 year survival for stage III colorectal carcinoma is quite good and is getting better! Stage 5-year Relative Survival Rate Colon vs Rectum I 92% vs 87% IIA 87% vs 80% IIB 63% vs 49% IIIA 89% vs 84% IIIB 69% vs 78% IIIC 53% vs 51% IV 11% vs 12%
14 Further treatment decision 1) Patient factors Age Co-morbidities Genetic syndrome (eg Lynch, FAP) Cancer phobia
15 Further treatment decision 2) Pathological factors 1) Qualitative 2) Quantitative Differentiation, vascular invasion, margin status etc Size of invasive tumour
16 Further treatment decision 3) Gastroenterologist/surgeon* Feeling on adequacy of endoscopic resection Personality Experience EMR/ESD (gastroenterologist) vs laparoscopic resection (colorectal surgeon) Knowledge!!! Recommendations for surgical resection: (from Nivatvongs S. Surg Clin N Am 2002;82: ) A. Lesions in colon a) Pedunculated Haggitt level 4 with invasion into distal third of submucosa, or pedunculated lesions with lymphovascular invasion b) Sessile lesions removed with margin <2 mm c) Sessile lesions removed piecemeal d) Sessile lesions with depth of invasion into distal third of submucosa (Sm3) e) Sessile lesions with lymphovascular invasion B. Lesions in middle third and upper third rectum Same as lesions in colon C. Lesions in distal third rectum a) Pedunculated Haggitt level 4 with invasion into distal third of submucosa, or pedunculated lesions with lymphovascular invasion b) All sessile lesions
17 Bottom line Better pathological risk assessment Better endoscopic resection Better surgical outcomes Better oncological therapy if a LN met is missed?? imaging techniques to detect LN met NBCSP = smaller malignant polyps The risk benefit data is changing All we can control is the pathology input
18 Pathological factors
19 Quantitative factors (Tumour size/depth of invasion)
20 1) Haggitt levels Depth of invasion CIS or Intramucosal Haggitt et al Gastroenterology 1985;89:328-36
21 1) Haggitt levels Haggitt paper Gastroenterology 1985;89: cases (50% were level 0) 70 (54%) pedunculated; 42 sessile, indeterminate 17 51% underwent resection; 35% of all cases were primary resections Lymphatic invasion - 2 cases Venous invasion 0 cases 8 (6.2%) adverse outcome = LN mets in 4 (but not known in 3 cases who died); death from disease in 5
22 1) Haggitt levels 8/64 (12.5%) submucosal invasive carcinoma (levels 1-4) had an adverse outcome (LN mets/tumour related death). These were: Levels 0-2 = 0 cases (0%) Level 3 = 1 case (12.5%) Level 4 = 7 cases (87.5%)** (2 were pedunculated, 6 were sessile) Level 4 is the significant factor 7/28 polyps were level 4 = PPV for adverse behaviour = 25%?How many level 4 were pedunculated
23 1) Haggitt levels Problems: 1) 59 non pedunculated polyps were by definition level 4 (6 had adverse outcome = 10%) 2) 70 pedunculated polyps? how many level 4 invasion (2 adverse) Data from paper suggests PPV of risk for pedunculated Level 4 > sessile level 4 (but data is incomplete)
24 1) Haggitt levels 3) Difficult to apply in practice poor orientation Piecemeal specimen Pedunculated vs sessile Levels 1 vs 2 and 2 vs 3 4) Over interpretation by surgeons 5) Small series, not contemporary
25 Envoi data Less pedunculated polyps than reported in clinical series (43% vs 66%) Pedunculated Haggitt level 4 = nil Haggitt level 3 = 14% 2 (12.5%) had LN mets (one was pt3 at resection) 1 other case had residual adenocarcinoma in lymphatics Haggitt level 2 = 19% 1 (5.9%) had LN mets; large mucinous LVI Haggitt level 1 = 10% no LN mets
26 2) Kikuchi/Kudo levels Sessile polyps LN metastasis risk Nascimbeni R et al Dis Colon Rectum 2002;45: % (0% in contemporary studies) 8% 23% Kikuchi R et al Dis Colon Rectum 1995;38: Kudo S. Endoscopy 1993;25: Overall pt1 6-12%
27 2) Kikuchi/Kudo levels Problems: 1. Fragmented specimen Invasion <0.3mm = Kikuchi sm1 Mid submucosal venous plexus is good surrogate for sm2 2. Muscularis mucosae destroyed by tumour and/or extensive tumour ulceration 3. Full thickness of submucosa is not included in standard endoscopic resection specimens (need ESD) 4. Not applicable to pedunculated polyps
28 3) Tumour size - measured Width and Depth (surrogate of tumour volume) of invasive carcinoma The most important prognostic feature now confirmed in multiple studies Y1 or Y2 depends on intactness of MM LN metastasis risk Width <2mm = 0% Depth <0.5mm = 0% Width <4mm = 2.5% Depth <2mm = 3.9% Width 4mm = 18.2% Depth 2mm = 17.1% Ueno et al Gastroenterology 2004;127: pt1 adenocarcinoma (mostly in a pre-existing polyp) Width 4mm and/or Depth 2mm predict LN metastasis
29 3) Katajima depth modification for pedunculated polyps Useful when sessile polyp is ulcerated or muscularis mucosae is destroyed Correlates tumour size in pedunculated polyps to sessile polyps Pedunculated Allows 2mm for this distance No lymph metastases if: 1) Pedunculated <3mm 2) Sessile <1mm Sessile 1 Sessile 2 J Gastroenterol 2004;39(6):534-43; WJG 2010;16(25):

30 4) Current Japanese criteria* Japanese society for cancer of the colon and rectum Kawachi et al Mod Path 2015
31 Tumour size - measured Problems: 1) Poor orientation (levels might help) 2) Fragmented specimen Often one or two pieces contain the majority of the carcinoma Can give a minimum size which often exceeds 2mm depth or 4mm width 3) Muscularis mucosae destroyed - Measure full thickness of adenocarcinoma 4) Sessile vs pedunculated - if no definite stalk measure as per sessile polyp
32 Tumour size - measured Envoi data Size LN mets No LN mets Odds ratio P value Width of invasion >4mm 91.7% 51.5% ( ) Depth of invasion >2mm 83.3% 48.0% 5.41 ( ) 0.02 Size <1mm depth or <2mm width = 0% LN mets
33 Qualitative factors
34 1) Poor tumour differentiation Poor differentiation Envoi (N=239) 18.4% (all CRC = 20%) Pooled analysis (Hassan et al N=1400) Ueno et al (N = 292) Butte (N=143) Kawachi Mod path 2015 (N=805) 7.2% 26.7% 11.9% 32.2% Wide variation in frequency Poor interobserver agreement Kappa % Cooper et al Gastroenterology. 1995;108: ; 0.14 Terris et al Mod Path 2012;25(2)182A Studies are moving toward the concept of tumour grade rather than differentiation Requires MMR status
35 1) Poor tumour differentiation Residual disease Metastasis Mortality % (average) 18% 23% 15% Odds ratio - Hassan 2 4 9** %/Odds ratio - Ueno 29%/3 (multivariate) Hassan et al Dis Colon Rectum 2005;48: Ueno et al Gastroenterology 2004;127: Consistently associated with adverse outcome in all studies Probably because we all agree on the significant high grade lesions
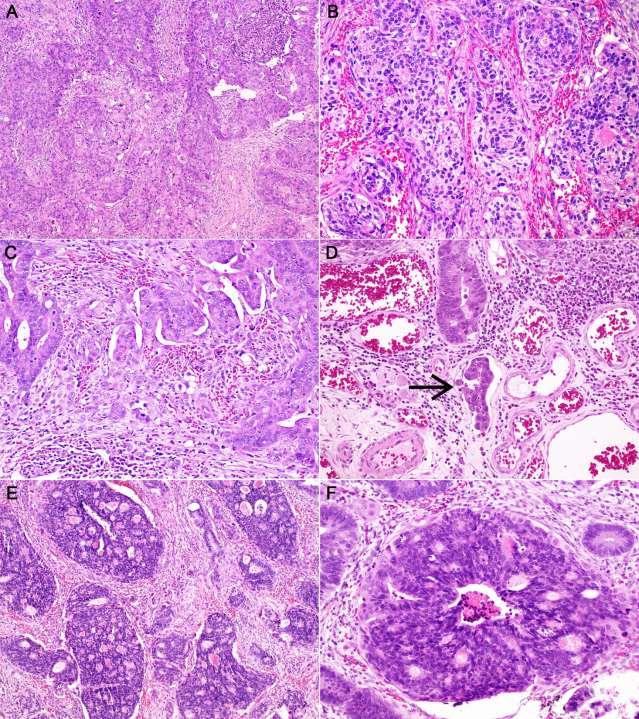
36 1) Poor tumour differentiation Poor differentiation in any part of tumour but particularly at invasive edge some studies require 50% of adenocarcinoma to be poorly differentiated Patterns: o o o o o o o <50% gland lumina Mucinous (MLH-1 def) Signet ring Tumour buds with >5 cells (poorly differentiated clusters) Cribriform comedo Undifferentiated carcinoma (?neuroendocrine) NOT true tumour budding (<5 cells)
37


38 Cribriform and mucinous Large buds focal dedifferentiation poorly differentiated clusters

39 Beware!!! Neuroendocrine very high risk of metastatic diseae
40 2) Margin of resection positive variously defined o In diathermy artefact o 1 HP field o <1mm o <2mm from margin deep margin Ueno et al Gastroenterology 2004;127: only involvement of diathermy artefact is significant 1 mm clearance Butte et al Dis Colon Rectum 2012;55: General agreement that 2mm is definitely clear

41 > 2mm - clear POSITIVE
42 2) Margin of resection - Risk: Too high Ueno = 12.5%; Envoi 12%, Butte 11.2% (INTACT polyps) Residual disease Metastasis Mortality % (average) 30% 7% 8% Odds ratio 15** 1 6 Hassan et al Dis Colon Rectum 2005;48: Interobserver agreement good 86-93% - positive margin = inadequate treatment NOT a risk for metastatic disease
43 2) Margin of resection Positive margin 33% (using all definitions) Envoi Diathermy involvement 27.2% no residual disease if clearance >0.1mm above diathermy artefact Positive margin = 12% risk of residual disease (adenoma or adenocarcinoma) at site of polypectomy
44 3) Vascular invasion Lymphatic or venous invasion Wide range of detection 0-57% (average 18%) Envoi LI = 23% VI = 9%, Butte = 18.2%, Ueno = 30%, Kawachi = 32% PPV for LN mets is low (5-30%) Only 7.3% of Envoi cases with LI had LN mets; 30% in Ueno, 19.2% in Butte NPV for LN mets may also be poor 50% in Butte; 67% at Envoi, 9% in Kawachi (resections) had LN mets despite no lymphatic invasion seen Has lead to inaccuracy/uncertainty in the significance of this prognostic factor


45 Sometimes easy!!


46 Often subtle need to look carefully



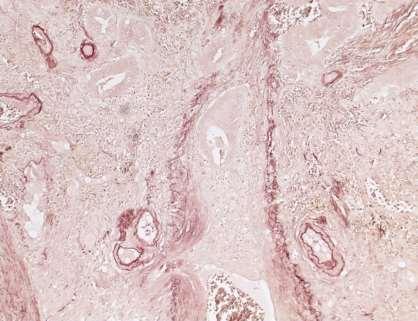
47 Orcein stain excellent for venous invasion detection

48
49 3) Vascular invasion Too high! Residual disease Metastasis Mortality % (average) 18% 35%(LN)/5% (H) 3% Odds ratio - Hassan 1 7/2** 1.5 %/Odds ratio - Ueno 31%/3 (multivariate) Hassan et al Dis Colon Rectum 2005;48: Ueno et al Gastroenterology 2004;127: usually associated with another adverse prognostic factor Vascular invasion does not add to risk when other adverse factors are already present Interobserver agreement is poor/moderate 37-77%
50 4) Tumour budding Identified as a significant prognostic factor in several papers Ueno et al Gastroenterology 2004;127: Tateishi et al Mod Path 2010;1:1-5 Sohn et al J Clin Pathol 2007;60: Katajima et al J Gastroenterol 2004;39: Yasuda et al Dis Colon Rectum 2007;50: Choi et al Dis Colon Rectum 2009; 52: Kawachi et al Mod Path 2015*** Uniform definition lacking range from any budding to strict definitions
51 Tumour budding Japanese criteria Budding/sprouting was counted in a field measuring 0.95mm 2 using a 20 objective lens and 10 ocular lens and classified as grade 1 (0 4 foci in the field), grade 2 (5 9 foci), or grade 3 ( 10 foci) Only grade 2/3 is significant high grade Kawachi et al = no cases with high grade budding metastasized if invasive ca was <1mm deep US criteria 10 buds = high grade
52 Tumour budding Problems: 1) Reproducibility Apparently high (AJSP 2015) But lots more buds if you use keratin 2) Field area of 0.95mm 2 = diameter 1.1mm so polyps <1mm are not reliably assessed and in the polyps reliably assessed it is probably not helpful to prognostication


53
54 4) Tumour budding Present in ~ 20-30% - however, bias to resection specimens in all studies (Envoi 29% - any) Risk Kawachi Odds ratio 3.14 Prognostic relevance in malignant polyps treated only by endoscopy is still not established Perhaps tumour budding and poorly differentiated clusters should be merged into high grade
55 5) Polyp morphology Pedunculated vs sessile Sessile polyps have overall mortality 8 x that of pedunculated polyps Reason why sessile is worse = increased adverse factors are usually present: poor differentiation vascular invasion positive resection margin**
56 5) Polyp morphology - Overall increased risk for sessile polyps - Risk for sessile polyp Vs pedunculated polyp pooled analysis* Residual/recurrent disease Metastasis Mortality % (average) - S 11%/6% 10%(LN)/4% (H) 5% % (average) - P 3%/0.5% 10%(LN)/1% (H) 0.5% Odds ratio - Hassan 4 1/4 10 Hassan et al Dis Colon Rectum 2005;48: *approximation (multivariate)? not an independent risk for LN metastasis However, most (85%) of sessile polyps had surgery
57 5) Polyp morphology Kawachi paper slight increased risk for sessile polyps but 80% of their polyps were sessile Envoi no difference Problem what is sessile and what is pedunculated? Japanese series 80% sessile Western meta-analysis 35% sessile Pedunculated = presence of definite stalk
58 6) Rectal location Rectal location, in particular, the distal 1/3 of rectum is an adverse factor for: 1. LN metastases (up to 1/3) 2. Recurrent/Residual disease (5-28%) Haggitt et al Gastroenterology 1985;89: Nascimbeni R et al Dis Colon Rectum 2002;45: Nivatvongs S. Surg Clin N Am 2002;82: Butte et al Dis Colon Rectum 2012;55: Reason is not clear from the literature Problem = surgery is ULAR or APR
59 6) Others Cribriform pattern adverse in Ueno paper Lymphatic density Kaneko et al Dis Colon Rectum 2006;50:1-9 Various IHC markers Matrix metalloproteinase expression, p53, p27 Misaki et al Hirano et al Carcinomatous destruction of muscularis mucosae vs retained muscularis mucosae Tateishi et al Mod Path 2010;1:1-5 LN met rate destroyed 16% preserved - 2% Polypoid carcinoma
60 Pathological risk assessment
61 Risk factors are additive Ueno et al Gastroenterology 2004;127: Adverse Qualitative 1. Poor differentiation 2. Vascular invasion (L or V) 3. Tumour budding (NOT margin involvement) N o Factors LN met risk 0 0.7%* % % * 7% micrometastasis rate Adverse Quantitive 1. Width 4mm 2. Depth 2mm 3. Haggitt level 3/4 Adverse Quantitive + Adverse Qualitative = did not change the LN metastasis risk
62 Risk factors are additive Envoi data Numbers of Ueno s 3 risk p value Poor differentiation, p value Poor differentiation, p value risk factors factors cribriform pattern and cribriform pattern and invasive depth >2mm invasive width >4mm None 3/149 (2.0%) /97 (0%) < /91 (1.1%) < /49 (8.2%) 5/112 (4.5%) 3/116 (2.6%) 2 or 3 5/41 (12.2%) 7/30 (23.3%) 8/32 (25.0%)

63 Risk factors are not equal Kawachi et al Mod Path 2015
64 How should we approach the MCP?
65 Size as per Japanese <1mm deep and <2mm wide 1-2mm deep or 2-4mm wide >2mm deep or >4mm wide lymph node risk = 0% (no matter what other factors are present) Lymph node risk = 0-5% (other adverse factors may additive to 10%) Lymph node risk = 5-10% (other adverse factors additive to %) Adverse factor risk: Poor differentiation > tumour budding > LVI > rectal site Margin involvement = 10-15% risk of residual adenoma or adenocarcinoma at polypectomy site The haematogenous metastasis rate is <1-2% (with adverse risk factors)
66 Piecemeal specimen Measure size of largest piece of invasive adenocarcinoma If >2mm deep and >4mm wide then adverse Other factors add to the risk If <1mm deep and <2mm wide and only in one piece no risk Margin status requires endoscopic determination
67 Pathology report Site Size (as per Japanese) Depth of invasion (mm) Width of invasion (mm) Haggitt ± Kikuchi/Kudo level (optional) Differentiation/grade (based on least differentiated area) Tumour budding (high level) Lymphatic invasion Venous invasion Margin status Clearance (carcinoma to margin - deep/circumferential): Mismatch repair IHC: Adjacent adenoma type (if present): Comment..
68 Intramucosal adenocarcinoma Tis in TNM Vienna classification (Japan/Europe) Just high grade dysplasia (HGD) in USA Increasingly encountering invasive adenocarcinoma with extension into a thickened reduplicated muscularis mucosae but not through this layer HGD does not seem appropriate but?any metastatic risk



69
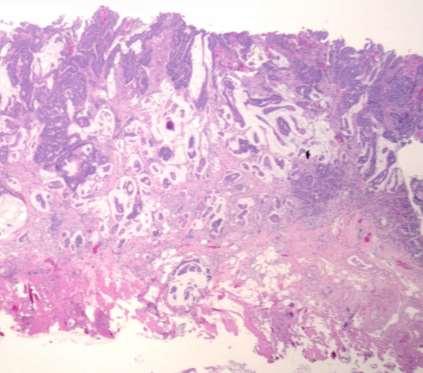
70 Pseudoinvasion 2-10% pedunculated polyps Left colon (sigmoid) Prolapse of dysplastic mucosa into submucosa following polyp torsion Note: can be associated with true invasive carcinoma Distinction from invasive carcinoma 1. Architecture 2. Stromal change 3. Cytology


71 Pseudoinvasion - architecture Narrow gap in muscularis mucosae Tanazawa et al Pathology International. 2003;53: Rounded appearance to focus Rounded appearance of glands within focus
72 Pseudoinvasion - stroma Lamina propria surrounds glands Dense fibrosis (not desmoplasia) Smooth muscle hypertrophy (and fibromuscular ) Haemosiderin Chronic inflamation Extravasated mucin No epithelium or epithelium at edge not epithelium floating in mucin pools


73 Pseudoinvasion


74 Pseudoinvasion Invasive carcinoma



75 Pseudoinvasion Invasive carcinoma Vs

76 Pseudoinvasion - cytology Same as in overlying mucosa Pseudoinvasion of non dysplastic normal epithelium If it looks like invasive carcinoma it probably is!
77 Pseudoinvasion - other p53 negative MMP-1 and Stromelysin-3 - negative Usually does not matter if we get it wrong since pseudoinvasive focus is clear of margin, vascular invasion negative and not poorly differentiated
78
79 References Coverlizza S et al. Colorectal adenomas containing invasive carcinoma, pathological assessment of lymph node metastasis. Cancer 1989;64: Hassan C, et al. Histologic risk factors and clinical outcome in colorectal malignant polyp: a pooleddata analysis. Dis Colon Rectum 2005;48: Kyzer S et al. The care of patients with colorectal polyps that contain invasive adenocarcinoma. Endoscopic polypectomy or colectomy? Cancer 1992;70: Seitz U et al. Is Endoscopic polypectomy an adequate therapy for malignant colorectal adenomas? Presentation of 114 patients and review of the literature. Dis Colon Rectum 2004;47: Geraghty JM et al.(1991) Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy. Gut 1991;32: Haggitt RC et al. Prognostic factors in colorectal carcinomas arising in adenomas: implications for lesions removed by endoscopic polypectomy. Gastroenterology 1985;89: Morson BC, et al. Histopathology and prognosis of malignant colorectal polyps treated by endoscopic polypectomy. Gut 1984;25: Cooper HS et al. Pathology of the malignant colorectal polyp. Hum Pathol 1998;29:15 26 Komuta K et al. Interobserver variability in the pathological assessment of malignant polyps. Br J Surg 2004;91: Cooper HS et al. Endoscopically removed malignant colorectal polyps: clinicopathologic correlations. Gastroenterology 1995;108: Volk EE et al. Management and outcome of patients with invasive carcinoma arising in colorectal polyps. Gastroenterology 1995;109: Netzer P et al. Risk factor assessment of endoscopically removed malignant colorectal polyps. Gut 1998;43:
80 References Hackelsberger et al. Endoscopic polypectomy and management of colorectal adenomas with invasive carcinoma. Endoscopy 1995;27: Christie JP. Malignant colon polyps cure by colonoscopy or colectomy? Am J Gastroenterol 1984;79: Hermanek P et al. Early (microinvasive) colorectal carcinoma. Pathology, diagnosis, surgical treatment. Int J Colorectal Dis 1986;1:79 84 Sukuki T et al. Risk of lymph node and distant metastases in patients with early invasive colorectal cancer classified as Haggitt s level 4 invasion. Dis Colon Rectum 2001;46: Nivatvongs S et al. The risk of lymph node metastasis in colorectal polyps with invasive adenocarcinoma. Dis Colon Rectum 1991;34: Wilcox GM et al. Early invasive carcinoma in colonic polyps. A review of the literature with emphasis on the assessment of the risk of metastasis. Cancer 1986;57: Chapman MAS et al. Management and outcome of patients with malignant colonic polyp identified from the Nottingham Colo-Rectal Screening Study. Col Rect Dis 2000;2:8 12 Jones L et al. Patient management after endoscopic removal of the cancerous colon adenoma. Ann Surg 1987; 205: Pollard CW et al. The fate of patients following polypectomy alone for polyps containing invasive carcinoma. Dis Colon Rectum 1992;35: Timmcke AE et al. Long-term survival after treatment of malignant colonic polyps. Dis Colon Rectum 1997;40: Haboubi NY et al. Clinicopathological management of the patient with a malignant colorectal adenoma. Col Rect Dis 2000;2:2 7 Tominaga K et al. Dis Colon Rectum 2005; 48: Nascimbeni R et al Dis Colon Rectum 2002;45: Nivatvongs S. Surg Clin N Am 2002;82:
81 References Ueno et al Gastroenterology 2004;127: Tateishi et al Mod Path 2010;1:1-5 Sohn et al J Clin Pathol 2007;60: Katajima et al J Gastroenterol 2004;39: Yasuda et al Dis Colon Rectum 2007;50: Choi et al Dis Colon Rectum 2009; 52: Butte et al Dis Colon Rectum 2012;55: Benizri et al Int J Colorectal Dis 2012 (prepublication)
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
BC CRC Update Malignant Polyp Who Needs Surgery
 BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Formula One Study. Assessment criteria of pathological parameters. Ver.2. UK Japan Joint Study for Risk Factors of Lymph Node
 APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications
 Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Malignant colorectal polyps: venous invasion and
 774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Modern colonoscopy allows for both diagnosis and treatment
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:662 667 CLINICAL PATHOLOGY The Malignant Colon Polyp: Diagnosis and Therapeutic Recommendations MARIE E. ROBERT Department of Pathology, Yale University
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:662 667 CLINICAL PATHOLOGY The Malignant Colon Polyp: Diagnosis and Therapeutic Recommendations MARIE E. ROBERT Department of Pathology, Yale University
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE RISK OF RESIDUAL CANCER AND LYMPH NODE METASTASIS
 253SJS102210.1177/1457496913482253S. E. Steigen, et al.adenomas with adenocarcinomas and risk factors Scandinavian Journal of Surgery 102: 90 95, 2013 ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE
253SJS102210.1177/1457496913482253S. E. Steigen, et al.adenomas with adenocarcinomas and risk factors Scandinavian Journal of Surgery 102: 90 95, 2013 ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
05/07/2018. What colorectal cancer screening is all about. Not so simple pathology: issues from the screening programme
 Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
The Paris classification of colonic lesions
 The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
Short and longterm outcomes after endoscopic resection of malignant polyps.
 Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Malignant colonic adenomas. Therapeutic criteria. Long-term results of therapy in a series of 42 patients in our healthcare area
 1130-0108/2009/101/12/830-836 REVISTA ESPAÑOLA DE ENFERMEDADES DIGESTIVAS Copyright 2009 ARÁN EDICIONES, S. L. REV ESP ENFERM DIG (Madrid) Vol. 101. N. 12, pp. 830-836, 2009 ORIGINAL PAPERS Malignant colonic
1130-0108/2009/101/12/830-836 REVISTA ESPAÑOLA DE ENFERMEDADES DIGESTIVAS Copyright 2009 ARÁN EDICIONES, S. L. REV ESP ENFERM DIG (Madrid) Vol. 101. N. 12, pp. 830-836, 2009 ORIGINAL PAPERS Malignant colonic
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER?
 CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Treatment Strategy for Non-curative Resection of Early Gastric Cancer. Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea
 Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School
 Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
How to treat early gastric cancer? Endoscopy
 How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
polyps of the colon and rectum
 J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Histopathologic risk factors for lymph node metastasis in patients with T1 colorectal cancer
 ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 https://doi.org/10.4174/astr.2017.93.5.266 Annals of Surgical Treatment and Research Histopathologic risk factors for lymph node metastasis in patients
ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 https://doi.org/10.4174/astr.2017.93.5.266 Annals of Surgical Treatment and Research Histopathologic risk factors for lymph node metastasis in patients
European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition
 SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations
 Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
The Kamal Ishak Lecture. The pathology of bowel cancer screening
 The Kamal Ishak Lecture The pathology of bowel cancer screening Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November
The Kamal Ishak Lecture The pathology of bowel cancer screening Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November
A Comparative Study of Rectal and Colonic Carcinoma: Demographic, Pathologic and TNM Staging Analysis
 Journal of the Egyptian Nat. Cancer Inst., Vol. 18, 3, September: 2-263, 2006 A Comparative Study of Rectal and ic Carcinoma: Demographic, Pathologic and TNM Staging Analysis TAREK N. EL-BOLKAINY, M.D.;
Journal of the Egyptian Nat. Cancer Inst., Vol. 18, 3, September: 2-263, 2006 A Comparative Study of Rectal and ic Carcinoma: Demographic, Pathologic and TNM Staging Analysis TAREK N. EL-BOLKAINY, M.D.;
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Do any benign polyps require an operation?
 Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
IN THE DEVELOPMENT and progression of colorectal
 Digestive Endoscopy 2014; 26 (Suppl. 2): 73 77 doi: 10.1111/den.12276 Treatment strategy of diminutive colorectal polyp
Digestive Endoscopy 2014; 26 (Suppl. 2): 73 77 doi: 10.1111/den.12276 Treatment strategy of diminutive colorectal polyp
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications. Andres A. Roma, MD Cleveland Clinic
 Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Management of malignant colon polyps: Current status and controversies
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v20.i43.16178 World J Gastroenterol 2014 November 21; 20(43): 16178-16183 ISSN 1007-9327
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v20.i43.16178 World J Gastroenterol 2014 November 21; 20(43): 16178-16183 ISSN 1007-9327
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Overview. Collecting Cancer Data: Colon 11/5/2009. Collecting Cancer Data: NAACCR Webinar Series 1. Agenda NAACCR WEBINAR SERIES
 Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
High risk stage II colon cancer
 High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay
 1 Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay Abstract: The estate of a 60 year old male alleged negligence against a gastroenterologist in failing to properly evaluate
1 Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay Abstract: The estate of a 60 year old male alleged negligence against a gastroenterologist in failing to properly evaluate
S rectal polyps that show atypia, adenocarcinoma,
 HOW RELIABLE IS BIOPSY OF RECTAL POLYPS? A Clinical and Morphological Study of 107 Cases C. ALEXANDER HELLWIG, M.D., AND EDGARD BARBOSA. nr.d. OME OVERLY cautious pathologists call all S rectal polyps
HOW RELIABLE IS BIOPSY OF RECTAL POLYPS? A Clinical and Morphological Study of 107 Cases C. ALEXANDER HELLWIG, M.D., AND EDGARD BARBOSA. nr.d. OME OVERLY cautious pathologists call all S rectal polyps
Factors for Endoscopic Submucosal Dissection in Early Colorectal Neoplasms: A Single Center Clinical Experience in China
 ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
M. Azzam Kayasseh,Dubai,UAE
 Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Please Silence Your Cell Phones. Thank You
 Please Silence Your Cell Phones Thank You TUMOR BUDDING IN PRE OPERATIVE BIOPSIES AND RESECTIONS Alessandro Lugli, MD Institute of Pathology and Translational Research Unit (TRU) University of Bern Bern,
Please Silence Your Cell Phones Thank You TUMOR BUDDING IN PRE OPERATIVE BIOPSIES AND RESECTIONS Alessandro Lugli, MD Institute of Pathology and Translational Research Unit (TRU) University of Bern Bern,
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Colonic adenomas-a colonoscopy survey
 Gut, 1979, 20, 240-245 Colonic adenomas-a colonoscopy survey P. E. GILLESPIE, T. J. CHAMBERS, K. W. CHAN, F. DORONZO, B. C. MORSON, AND C. B. WILLIAMS From St Mark's Hospital, City Road, London SUMMARY
Gut, 1979, 20, 240-245 Colonic adenomas-a colonoscopy survey P. E. GILLESPIE, T. J. CHAMBERS, K. W. CHAN, F. DORONZO, B. C. MORSON, AND C. B. WILLIAMS From St Mark's Hospital, City Road, London SUMMARY
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer
 498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
What Pathology can tell us in the approach of localized colorectal cancer
 What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and