Barrett s s Dysplasia
|
|
|
- Blaise Price
- 5 years ago
- Views:
Transcription
1 Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation
2 Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia Dysplasia Adenocarcinoma
3 Dysplasia Definition Neoplastic epithelium confined within the basement membrane of the gland within which it arose
4 Grading System for Dysplasia Negative Indefinite Positive Low-grade High-grade grade Modified from IBD/DMSG Hum Pathol 1983 Pathol 1983;14:831

5

6

7

8

9

10

11

12

13
14

15

16
17

18
19 Intramucosal Adenocarcinoma Single cell lamina propria invasion Sheets of malignant cells Abortive angulated glands Never ending gland pattern

20

21

22

23
24 Invasive Adenocarcinoma Unequivocal desmoplasia Indicates at least submucosal invasion

25
26 Dysplasia: Problems Sampling Distinction from reactive change Observer variation Natural history incompletely understood

27 Distribution of Dysplasia

28 Biopsy Protocol
29 Seattle Protocol? Safe 4 quadrant bxs every 2 cm 1 cm (HGD) May not detect superficial carcinoma 10 of 29 CCF pts with Seattle protocol lacking visible lesions had higher grade neoplasia on resection specimen 9 of 29 HGD bx Intra-mucosal CA 1 of 29 HGD bx Sub-mucosal CA Plesec T, et al. USCAP 2006
30 Dysplasia: Problems Sampling Distinction from reactive change Observer variation Natural history incompletely understood

31

32
33 Dysplasia: Problems Sampling Distinction from reactive change Observer variation Natural history incompletely understood
34

35

36 Spectrum of Dysplasia
37 Interobserver Agreement: Dysplasia in Barrett s s Esophagus Diagnosis Kappa Statistic Agreement HGD/CA 0.65 Substantial LGD 0.32 Fair Indefinite 0.15 Poor Negative 0.58 Moderate From: Montgomery E, et al. Hum Pathol 32:368-78; 2001

38
39 Squamous Overgrowth Healing biopsy sites Proton pump inhibitors Ablative therapies Photodynamic therapy (PDT) Endoscopic mucosal resection (EMR) Cryotherapy Argon Plasma Coagulation (APC) Heater probe

40

41

42
43 Two Main Problems In Barrett s s Pathology Over diagnosis of Barrett s esophagus Over diagnosis of high-grade grade dysplasia in Barrett s esophagus
44 Inaccuracy in the Diagnosis of Barrett s s with HGD PDT multi-center trial for Barrett s s with HGD 485 patients with HGD screened Review original slides Repeat protocol study endoscopy 4 quad q2cm 248 with confirmed HGD (51%) 193 patients overdiagnosed as Barrett s s with HGD (40%)
45 Reinterpretation of Barrett s s with High-Grade Dysplasia 193 Over-Diagnosed as HGD Reinterpretations No. Percent Gastric only 18 9% Barrett s s negative 35 18% Barrett s s indefinite 61 32% Barrett s s LGD 79 41% Yearsley M, et al., USCAP 2006
46 Over Diagnosis of HGD in Barrett s s Esophagus NOT atypia limited to basal glands NOT reactive gastric cardiac- type mucosa NOT inflammatory reactive change Sampling error
47 NOT Baseline Glandular Atypia

48 NOT Reactive Gastric Mucosa

49 NOT Inflammatory Atypia
50 Misdiagnosis of HGD in Barrett s s Esophagus Under utilization of loss of nuclear polarity as most objective criterion Morphologic spectrum without precise definable boundaries Accuracy is experience and volume dependent


51 Loss of Nuclear Polarity to Distinguish Low and High-Grade Dysplasia
52 ACG GUIDELINES High-grade grade dysplasia in Barrett s esophagus should be confirmed by an expert GI pathologist Sampliner RE. Am J Gastroenterol : 97; 2002
53 Dysplasia: Problems Sampling Distinction from reactive change Observer variation Natural history incompletely understood
54 Progression to Cancer Based on Diagnosis at First Visit Proportion Free of Cancer p = Time on Study (years) Metaplasia (n=78) Indefinite (n=36) Low-grade (n=20) High-grade grade (n=48)
55 Progression to Cancer Based on Prevalent or Incident HGD Proportion Free of Cancer Incident HGD (n=21) Prevalent HGD (n=55) p = Time Since First Diagnosis of HGD (years)
56 High Grade Dysplasia Management Options Surveillance Ablation (e.g.pdt) Surgery
57 Can we tell BAD from WORSE? HGD IMC SMC Shaheen NJ. Gastroenterology 2003; 125:260-1
58 Results Dx Overall kappa Individual kappa P 95% CI 0.30 < Poor HGD 0.47 < Moderate HGD- MAD 0.21 < Poor IMC 0.30 < Poor SMC 0.17 < Poor
59 Can we tell BAD from WORSE? Lack of agreement above HGD Management based on accurate distinction between HGD, IMC and SMC in biopsies is questionable
60 Summary-1 Grading of Dysplasia Problems with dysplasia Sampling Observer variation Natural history: prevalent vs. incident
61 Summary-2 Overdiagnosis of HGD Baseline atypia of metaplasia Reactive cardia Inflammatory change Loss of nuclear polarity HGD management broadening but ddx from cancer difficult
62 BARRETT S DYSPLASIA RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY COMPANION MEETING UNITED STATES AND CANADIAN ACADEMY OF PATHOLOGY ANNUAL MEETING, FEBRUARY 2006, ATLANTA, GA by Mary P. Bronner, M.D. Director of Gastrointestinal Pathology Section Head of Morphologic Molecular Pathology Cleveland Clinic Foundation Cleveland, OH
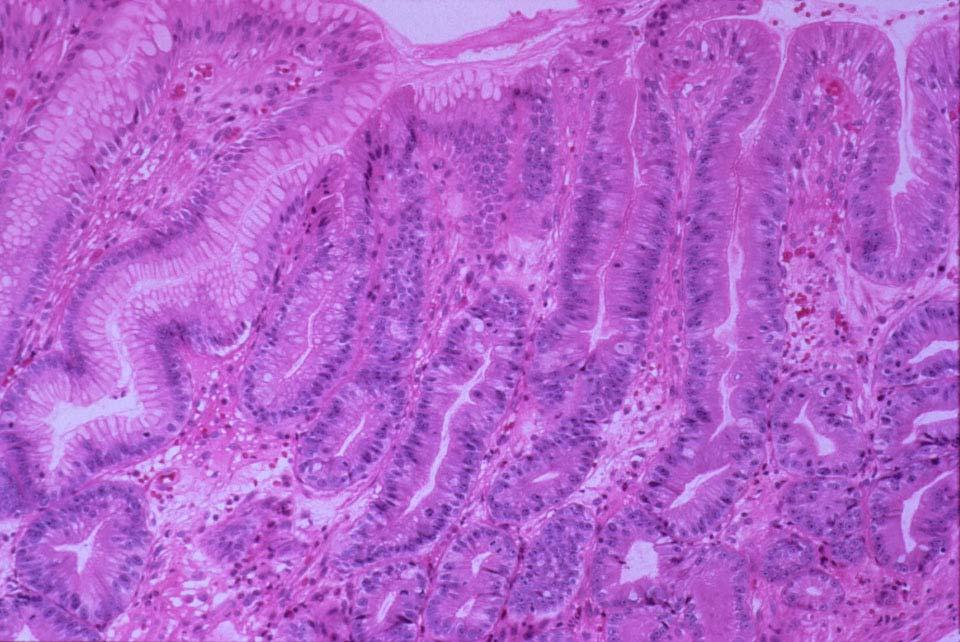
63 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 2 Barrett s Dysplasia by M. Bronner, M.D. BARRETT S DYSPLASIA Barrett s esophagus predisposes to the development of esophageal adenocarcinoma but the frequency with which it does so is not well established 1,2. Part of the difficulty in defining the cancer risk is that the prevalence of Barrett s esophagus itself is not well documented. Barrett s esophagus is present in about 10 to 12% of patients with symptomatic gastroesophageal reflux disease (GERD) who undergo endoscopy, 1 but autopsy data suggests that its true frequency may be as much as 20 times higher. 3 The reported prevalence of adenocarcinoma in Barrett s esophagus averages about 10%, i.e., at the time the initial diagnosis of Barrett s esophagus is made, about 10% of patients will have adenocarcinoma. 1 The estimated incidence of adenocarcinoma in Barrett s esophagus ranges from 1 in 52 to 1 in 441 patient years, representing an increased risk of 30 to 127- fold, which is higher than the risk of lung cancer from smoking. 1 Adenocarcinoma of the esophagus appears to be limited to patients who have metaplastic epithelium. The length of the endoscopically visible columnar-lined segment does not seem to have a practical influence on cancer risk, as patients with even very short segments may develop cancer. 4,5 Cancer arises in Barrett s esophagus through a multi-step sequence of events that is initiated by chronic GERD, leading to metaplasia, then dysplasia, and finally adenocarcinoma. Definitions and Characteristics of Dysplasia Dysplasia is defined as neoplastic epithelium that remains confined within the basement membrane of the epithelium within which it arises. 6 When the dysplastic epithelium proliferates to form a mass, the term adenoma may be applied, but this is uncommon in Barrett s esophagus 7 and has no independent relevance in comparison to non-polypoid dysplasia. Barrett s dysplasia is recognized histologically by a combination of architectural and cytologic abnormalities. Slightly more baseline cytoarchitectural atypia develops in the absence of dysplasia directly at the SCJ. Dysplastic glands may retain their normal configuration, but more often have irregular, crowded or even grossly distorted architecture. The glands are usually lined by cells with enlarged, irregular, hyperchromatic, crowded and stratified nuclei. In other examples, the nuclei are large, hyperchromatic and contain large nucleoli, but lack the crowding and stratification mentioned above. In all cases, the cytologic features extend from the glands onto the epithelial surface and this is perhaps the single most important criterion in the diagnosis of dysplasia. For purposes of clinical utility, dysplasia in Barrett s esophagus is subdivided into lowgrade and high-grade categories. When no features of dysplasia are observed, the diagnosis of negative for dysplasia is rendered, and when the findings are uncertain, the category of indefinite for dysplasia is assigned. This grading scheme is directly analogous to that for dysplasia complicating idiopathic inflammatory bowel disease. 1,6,8 The criteria are as follows: Negative for dysplasia: The glandular architecture and cellular morphology are free of neoplastic alterations, but may contain reactive or regenerative change in relation to inflammatory damage. The glandular architecture is orderly and not crowded. The regenerative basal glands in Barrett s intestinalized mucosa characteristically display cytologic atypia that is negative for dysplasia. This basal atypia includes nuclear enlargement, pleomorphism, outline irregularity, hyperchromasia and stratification, and is the baseline atypia of metaplastic epithelium that is negative for dysplasia. It may be particularly striking in comparison to frequently admixed mucinous gastric glands that are usually quite bland. Basal glandular atypia matures completely to the surface in epithelium that is negative for dysplasia. Surface maturation refers to the nuclei becoming smaller (less than twice the size of stromal nuclei and usually much less), less darkly staining, smoothly contoured, uniform, and non-stratified, as the cells extend from the basal glands and onto the mucosal surface. Care must be taken to not over interpret tangential sectioning artifact as surface nuclear stratification. Nuclear uniformity and
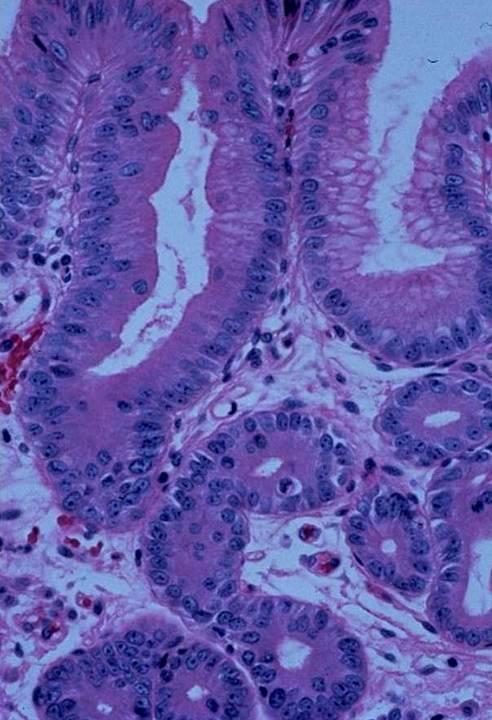
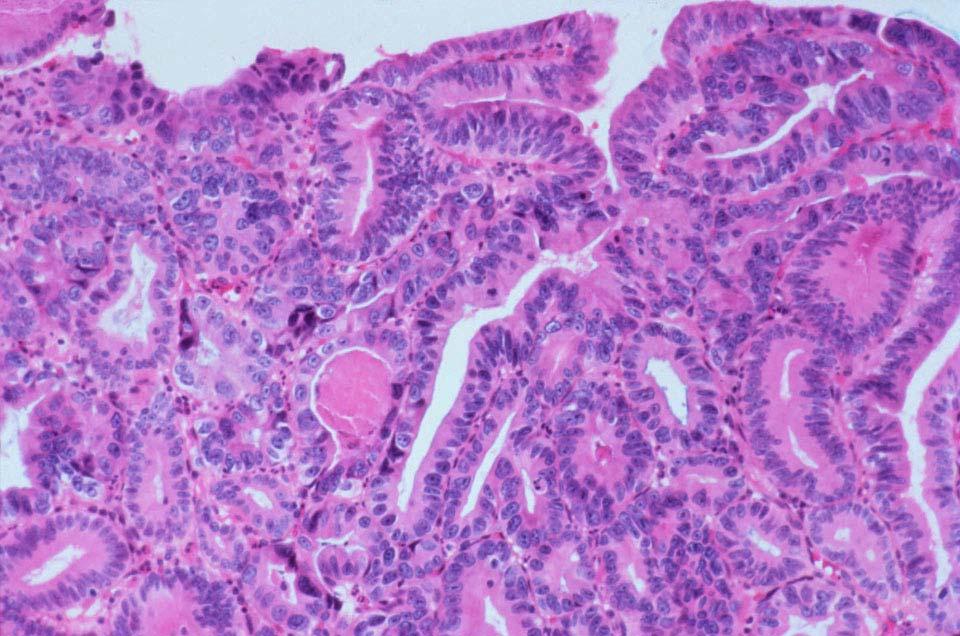
64 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 3 Barrett s Dysplasia by M. Bronner, M.D. coexisting cytoplasmic elongation usually accompany tangential sectioning artifact and can be helpful diagnostic clues. Reactive cytologic alterations, in the presence of active inflammation, are also part of the spectrum of negative for dysplasia, as long as the cytologic changes still mature to the surface of the biopsy and the glandular architecture is intact. Reactive inflammatory change often produces a more open chromatin structure and some degree of cytoplasmic mucin depletion. Regenerative cytoarchitectural alterations are also classified as negative for dysplasia. Regenerative change consists of a surface monolayer of cells, covering eroded or ulcerated mucosa that is usually devoid of glands or shows gland loss with replacement by granulation tissue. The surface regenerative cells may have variably atypical and even bizarre nuclei but in general they maintain a characteristic monolayer growth pattern and the cells generally have abundant cytoplasm. Indefinite for dysplasia: The glandular architecture is intact or may exhibit mild crowding or mild loss of parallel architecture. The cytologic changes may be mildly abnormal as the cells extend onto the surface. In the presence of pronounced inflammation or erosion/ulceration, the cells may be markedly atypical and lack surface maturation altogether. Numerous mitotic figures may be present. Marked crypt atypia that matures to the surface and mild atypia that mostly matures to the surface also fall into the indefinite for dysplasia category. Biopsies without intact surface to permit assessment of maturation to the surface may also be categorized as indefinite for dysplasia. The highly variable and problematic changes in this category are further discussed below. Low-grade dysplasia: The crypt architecture is relatively preserved, and distortion, if present, is generally mild to moderate at the most. A villiform surface configuration may be present. The nuclei exhibit some combination of stratification, enlargement, hyperchromasia, pleomorphism and crowding. Abnormal mitotic figures may be present in the upper portion of the crypt, but in general mitotic figures are not very helpful. Goblet cell mucin is often diminished and may be absent. So called dystrophic goblet cells may be seen in which the mucin vacuole is located on the basal, rather than luminal side of the nucleus. The cytologic changes extend from the base of the crypts onto the surface epithelium. Nuclear polarity is preserved, whereby the long axes of the nuclei remain perpendicular to the basement membrane. Maintenance of nuclear polarity is the most important and most objective criteria to differentiate low and high-grade dysplasia. High-grade dysplasia: Distortion of crypt architecture is usually present and may be marked and consists of some combination of branching and lateral budding of crypts, marked glandular crowding, villiform surface configuration, or intraglandular bridging of epithelium to form a cribriform pattern or back-to-back gland patterns. Nuclear abnormalities are present as in low-grade dysplasia, but in addition, there is more marked nuclear enlargement, more irregularity of nuclear membranes, and more hyperchromasia. These features are unfortunately subjective, because they are continuous variables for which precise cutoffs cannot be established. Loss of nuclear polarity, however, is the most objective criterion to differentiate low and highgrade dysplasia. For this criterion, the long axes of the nuclei no longer remain perpendicular to the basement membrane. Loss of nuclear polarity also refers to the loss of an orderly arrangement of nuclei and the lack of orientation of nuclei to each other. The nuclei vary markedly in size, shape and staining characteristics. Cytoplasmic mucin is usually diminished or absent and dystrophic goblet cells (see above) may be present. It should be noted that a small percentage of dysplasias, both low and high-grade may retain cytoplasmic mucin. The cytologic changes extend from the base of the crypts onto the surface epithelium. Due to the major
65 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 4 Barrett s Dysplasia by M. Bronner, M.D. consequences of a diagnosis of high-grade dysplasia, this author believes it should not be established without 100% certainty on the part of the pathologist. Additional general comments on the grading of dysplasia: Criteria applying to all grades of dysplasia are that biopsies that stand out as significantly different from others, such as those with mucin loss or hypermucinous change, dystrophic goblet cells and/or endocrine cell hyperplasia, or varying architecture or cytology, tend to associate with dysplasia. In the case of discrepancy between cytology and architecture, cytology generally determines the grade. The one exception to this is when architecture is extremely abnormal. Dilated glands with necrotic luminal debris a feature of markedly abnormal architecture that could in some cases determine a designation of high-grade dysplasia despite less abnormal cytology. In the presence of severe inflammation with or without erosion/ulceration, assignment of unequivocal dysplasia is done only in rare circumstances. In general, all of the cytologic alterations of neoplasia may be mimicked by inflammatory change, whereas architectural changes may be somewhat more helpful in this differential diagnosis. Nonetheless, the overwhelming majority of ulcerated/eroded biopsies with cytoarchitectual alterations suggesting neoplasia should be classified as indefinite for dysplasia with commentary that they could be neoplastic. In such situations, the patient should be rebiopsied after aggressive medical management to induce remission of obscuring inflammation. Problems in the Diagnosis of Dysplasia Sampling: Mapping studies of esophagectomy specimens containing adenocarcinoma that was not endoscopically visible show that dysplasia involves a highly variable amount of esophageal mucosa surrounding the invasive carcinoma. 9 The dysplastic mucosa may occupy most or the entire esophagus or it may be quite limited in extent. 10 Thus, the endoscopist must thoroughly sample the mucosa in order to avoid missing small areas of dysplasia or carcinoma. Four-quadrant, well-oriented jumbo biopsies taken at 2 cm intervals or less throughout the length of the Barrett s segment are recommended, combined with additional biopsies of any endoscopic lesions. 11 Shortening of the interval to every 1 cm, based on mathematical modeling without prospective validation, has been suggested for patients with high-grade dysplasia who are maintained in endoscopic surveillance. 13 Adherence to this or similar protocols has shown excellent correlation between the pre-operative endoscopic diagnosis and the final diagnosis in the resected specimen by the Seattle group Prospective application of the Seattle protocol at the Cleveland Clinic has not reproduced such favorable results, as presented at this USCAP meeting, and suggests that the Seattle protocol may still miss cancer in HGD patients. 12 Despite rigorous pre-operative biopsy sampling using the Seattle protocol, a more advanced lesion was found in up to 34.5% (10 of 29 patients) of cases in resection specimens with BE superficial adenocarcinoma, including both intramucosal and submucosal cancers. This calls into question the safety of continued surveillance for HGD without an endoscopically visible lesion. Baseline Glandular Atypia of Barrett s Metaplastic Epithelium: Metaplastic Barrett s epithelium that is negative for dysplasia consistently shows nuclear atypism when viewed in contrast to gastric epithelium. This is particularly true of the deepest metaplastic glands closest to the muscularis mucosae. This deep glandular nuclear atypia includes enlargement, hyperchromatism, crowding, irregular nuclear contours, and prominence of nucleoli and stratification. These changes may be marked and because of this may be confused with dysplasia. However, they are usually separable from dysplasia because they are confined to the deep glands, while the upper portions show less abnormality or are normal; this feature is best recognized in well-oriented biopsy specimens and is termed maturation to the surface. Thus, the
66 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 5 Barrett s Dysplasia by M. Bronner, M.D. diagnosis of dysplasia should be made with great caution, if ever, when the changes do not involve the mucosal surface. Variations of Indefinite for Dysplasia: When there is doubt as to the significance of the epithelial abnormalities in a biopsy, the diagnosis of indefinite for dysplasia should be made. Clinicians have the impression that there is only one type of indefinite for dysplasia. This is understandable because the diagnostic terminology in written pathology reports is always the same. In reality there may be hundreds or even thousands of variations on the cytoarchitectural changes in Barrett s epithelium in this category. Pathologists strive to classify the vast array of alterations in this category into this single and utterly limited designation of indefinite for dysplasia. Understandably, this situation leads to inter and intra-observer diagnostic variability, which is highest in the indefinite category in the grading schema of Barrett s esophagus. 8 Fortunately, the distinction between indefinite and low-grade dysplasia has no clinical significance for both categories are followed the same way, namely continued periodic careful surveillance. The differentiation of Barrett s dysplasia from reactive or regenerative change caused by inflammation is difficult, and at times impossible. Reactive changes in biopsies from the edges of ulcers may be indistinguishable from dysplasia. In cases with marked inflammation or ulceration, the atypia may be so severe that not only is dysplasia in contention, but even carcinoma may be suspected. This is the first and most concerning type of change that is classified as indefinite for dysplasia. If inflammation or ulceration is present, repeat biopsies after intensive medical antireflux therapy will often show resolution of the abnormalities. Cases with reactive inflammatory change that are milder and are probably negative for dysplasia form the second major type of change that is classified as indefinite for dysplasia. The cytologic abnormalities do not entirely mature onto the surface, however, so that the diagnosis of indefinite for dysplasia is still warranted. The third major category of change that may be classified as indefinite for dysplasia is that of cytoarchitectural abnormalities in uninflamed Barrett s epithelium that is not negative for dysplasia, but yet is insufficient for a diagnosis of low-grade dysplasia. A common issue is that the cytologic alterations mature partially but incompletely as the cells extend onto the surface of the biopsy. These are alterations that presumably are on the pathway of neoplastic progression, but have not yet crossed the threshold for low-grade dysplasia. Mechanical issues are one final category that may be diagnosed at indefinite for dysplasia, such as when the biopsy surface is denuded or the biopsy is maloriented and the surface is otherwise unavailable for evaluation. Variability in the Diagnosis of Dysplasia: Because the epithelial abnormalities in dysplasia form a continuous morphologic spectrum, from relatively mild atypia to overt dysplasia, the boundaries between the grades cannot be sharply defined. Thus, observer variation exists in the diagnosis and grading of dysplasia, particularly at the indefinite/low-grade interface. 8 For this reason, the categories of indefinite for dysplasia and low-grade dysplasia are combined in most endoscopic protocols for practical clinical management purposes. Fortunately, at high end of the spectrum, namely high-grade dysplasia and intramucosal carcinoma, where the diagnosis may lead to invasive therapy, there is excellent agreement by GI pathologists within and between observers. Similarly, there is good reliability for the diagnosis of negative for dysplasia as well 8, which is also very important when one considers that more than 90% of biopsies in Barrett s esophagus should be negative. Of great concern, is the recently documented lack of reproducibility beyond a diagnosis of high-grade dysplasia, that is regarding GI pathologists ability to distinguish high-grade dysplasia from intramucosal or submucosally invasive adenocarcinoma. 14 In a recent study from
67 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 6 Barrett s Dysplasia by M. Bronner, M.D. the GI pathologists at the Cleveland Clinic Foundation with its high volume Barrett s practice, 168 preoperative biopsies that were at least high-grade dysplasia (Table 1) were reviewed. Observer variability was poor in general for distinguishing high-grade dysplasia from adenocarcinoma in biopsies. This calls into question clinical management practices based on pathologists being able to differentiate these high end diagnoses accurately. TABLE 1. OBSERVER VARIABILITY IN BARRETT S BIOPSIES WITH AT LEAST HIGH-GRADE DYSPLASIA Diagnosis Overall Kappa P-value 95% CI Interpretation Kappa ALL 0.30 < Poor HGD* 0.47 < Moderate HGD-MAD** 0.21 < Poor IMC^ 0.30 < Poor SMC # 0.17 < Poor *HGD=high-grade dysplasia; **HGD-MAD=high-grade dysplasia with marked architectural distortion such that intramucosal carcinoma cannot be excluded; ^IMC=intramucosal adenocarcinoma; # SMC=submucosally invasive adenocarcinoma Thus, the problem of observer variability for diagnosing negative for dysplasia through high-grade dysplasia, at least for experienced GI pathologists, has probably been overstated in the literature. 13 Inter- and intra-observer diagnostic concordance can be excellent to outstanding through this part of the neoplastic spectrum. The caveat of course is that pathologists should see a high and continual volume of Barrett s biopsies to achieve this level of reproducibility. This is an important and probably critical factor in the accuracy of dysplasia grading in Barrett s esophagus. Nonetheless, histopathologic diagnosis can be highly reliable and accurate, especially regarding negative for dysplasia and high-grade dysplasia, the aspects of the spectrum where diagnostic management decisions are most important. Expanding management options that now go beyond esophagectomy to include continued surveillance, ablative therapies and endoscopic mucosal resection (EMR), make differentiating high-grade dysplasia from carcinoma increasingly important. Unfortunately, even experienced GI pathologists in a high volume practice have poor reproducibility at this diagnostic task (Table 1). 14 Similarly, sampling error remains a major problem at the high end of the spectrum as well, even if the Seattle protocol is used. 12 Over Diagnosis of High-Grade Dysplasia in Barrett s Esophagus: Barrett s esophagus with high-grade dysplasia is a serious condition prone to over diagnosis by pathologists. Documentation of the magnitude of the problem of the over diagnosis of high-grade dysplasia is also provided by a multi-institutional and international trial of photodynamic therapy in 208 patients with high-grade dysplasia in Barrett s esophagus. Prior to study enrollment, all potential patients carried a biopsy diagnosis from their local hospital of Barrett s esophagus with highgrade dysplasia. In order to identify the 208 patients with Barrett s with high-grade dysplasia who were ultimately randomized into the trial, at total of 485 patients had to be screened (Table 4-1). There were an incredible 193 or 40% of patients who were thought to have high-grade dysplasia but ultimately had lower grades or no Barrett s at all. 15 This was discovered by a rigorous endoscopic and pathologic screening biopsy protocol. The screening included review of the original pathology thought to have high-grade dysplasia by the referring pathologists, and a new protocol endoscopy by one of the trial investigators. This included 4-quadrant jumbo biopsies every 2 cm, beginning in the proximal gastric fundus, through the LES region and the
68 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 7 Barrett s Dysplasia by M. Bronner, M.D. entire visible columnar pink mucosa within the tubular esophagus to the proximally displaced Z- line and squamous mucosa. The 193 (40%) patients who had been over-diagnosed with highgrade dysplasia had a variety of pathologies (Table 2), as interpreted by the three study pathologists at the University of Washington. 15 Inter-rater agreement per endoscopy for highgrade dysplasia, carcinoma and Barrett s esophagus was 88%, 96% and 99%, respectively. Intrarater agreement for high-grade dysplasia was 94% (95% CI 86,97) with a kappa statistic of 0.85 (near perfect). TABLE 2: REINTERPRETATION OF HIGH-GRADE DYSPLASIA IN BARRETT S ESOPHAGUS IN 193 OF 485 PATIENTS SCREENED FOR AN ABLATION THERAPY TRIAL Reinterpreted Diagnoses No. % Gastric only 18 9% Barrett s negative 35 18% Barrett s indefinite for dysplasia 61 32% Barrett s low-grade dysplasia 79 41% TOTAL % As shown in Table 2, many of the patients (18 or 9%) who failed to qualify for the trial did not even have Barrett s esophagus, much less Barrett s esophagus with high-grade dysplasia. These and the rest of a total 193 patients with less than Barrett s with high-grade dysplasia were all facing esophagectomy. This underscores the problem of the over diagnosis not only of Barrett s esophagus itself, but also Barrett s with high-grade dysplasia. One of the more frequent problems in the over diagnosis of high-grade dysplasia in Barrett s esophagus is the misinterpretation of cardiac-type mucosa with reactive change. Such reactive change frequently develops in gastric mucosa in response to gastroesophageal reflux and gastritis involving the lower esophageal region and hiatal hernias. This is a particularly unfortunate misinterpretation, as it not only renders a false positive diagnosis of Barrett s, with all of its attendant problems, but it may even precipitate unnecessary esophagectomy. The reasons for this error are at least 2-fold. First, damaged cardiac-type mucosa tends to develop reactive mucin depletion. Mucin depletion is also common in dysplastic Barrett s epithelium. Thus, both tend to lack goblet cells or much mucin in the remaining columnar epithelial cells, so that this potential differentiating cytoplasmic feature becomes confounding. Second, reactive cardiac-type mucosa may have marked cytologic atypia. The atypia of benign reactive gastric mucosa may in fact be worse than neoplastic atypia. Based on these issues, it is no surprise that reactive cardiac-type mucosa may be histologically treacherous and difficult to differentiate from Barrett s dysplastic epithelium. A useful criterion to distinguish reactive cardiac-type mucosa from Barrett s dysplasia involves the deeper glands. The deeper glands in reactive gastric mucosa tend to retain most and commonly all of their mucin. Further, the mucinous cells within the deep glands (and the surface for that matter) involve the entire gland or crypt in a linear continuous fashion, rather than as scattered goblet cells typical of metaplastic mucosa. The basal glands of cardiac or fundic-type mucosa are characteristically not mitotically active because the regenerative zone in these epithelia resides in the more superficial foveolar neck region, generally located in the upper midregion of gastric-type mucosa, rather than within the deep glandular compartment. Parietal cells
69 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 8 Barrett s Dysplasia by M. Bronner, M.D. also indicate gastric-type mucosa. Reactive cardiac-type mucosa may also retain some surface mucin in the form of markedly shortened but back-to-back foveolar mucin caps over the biopsy surfaces. These features in combination with bland mitotically inactive mucinous glands, that may be diffusely positive for Alcian blue at ph 2.5, are the best criteria for recognizing reactive cardiac-type mucosa and distinguishing it from Barrett s mucosa with dysplasia. Dysplastic Barrett s epithelium typically also shows loss of goblet cell mucin, but the glandular compartment is characteristically more atypical than the surface. This is in sharp contrast to the opposite pattern in reactive cardiac-type mucosa, where the glands tend to be very bland and the surface markedly atypical, as described above. Thus the bottom-heavy versus topheavy pattern of atypia may be very helpful in distinguishing these two diagnoses. Mitotic activity is also highest in the regenerative glandular compartment of Barrett s metaplastic epithelium, akin to the regenerative compartment of intestinal epithelium elsewhere in the GI tract. This is quite different from the regenerative mitotic region of cardiac-type mucosa, located in the mid or neck region. The cytologic atypia in reactive cardiac-type mucosa tends to be uniform across all of the affected nuclei, whereas dysplastic Barrett s nuclei tend to show more pleomorphism. Reactive cardiac-type nuclei usually are not as hyperchromatic as dysplastic Barrett s epithelium, but this often depends on the type of fixative and processing used and is therefore a somewhat less reliable criterion. As in all areas of diagnostic pathology, it is not always possible to distinguish reactive cardiac-type mucosa from Barrett s with dysplasia. In such cases, a diagnosis of atypical glandular epithelium of uncertain type with alterations indefinite for dysplasia can be made, along with the request for additional biopsies following aggressive medical management to attempt to eliminate any obscuring reactive change. Baseline Atypia in Barrett s Regenerative Glands: Another issue of great importance in the over diagnosis of dysplasia in Barrett s esophagus is that Barrett s metaplastic epithelium has a baseline and characteristic glandular atypia that is negative for dysplasia. 64 This is especially true when the metaplastic glands are viewed in comparison with the frequently admixed non-metaplastic cardiac or fundic glands. The pathologist needs to see enough cases of metaplastic Barrett s epithelium to gain an appreciation for the spectrum of this baseline glandular atypia that is negative for dysplasia. The major distinguishing factor between this and dysplastic Barrett s epithelium is maturation to the surface. This feature cannot be over emphasized. High-Grade Dysplasia versus Carcinoma: When high-grade dysplasia develops, architectural distortion may reach a point at which the diagnosis of carcinoma is impossible to exclude with certainty on the basis of superficial biopsy samples. This occurs when glands grow in a cribriform or dense back-to-back pattern or when dilated glands with luminal necrotic debris are present. High-grade dysplasia in the setting of an ulcer is another significant risk factor for carcinoma. In such cases, a diagnosis along the lines of high-grade dysplasia with marked distortion of glandular architecture, invasive adenocarcinoma cannot be excluded is appropriate. When numerous individual invasive cells, or sheets of malignant cells, or angulated infiltrative and abortive glands or the never-ending-gland pattern is seen to infiltrate the lamina propria, a diagnosis of intramucosal adenocarcinoma can be made. If a well-defined desmoplastic stroma with infiltrating malignant glands can be identified and separated from inflammatory stromal change, which can be very difficult at times, the diagnosis of at least submucosal invasive adenocarcinoma can be made. While the diagnostic categories of high-grade dysplasia and intramucosal adenocarcinoma are easily defined on the printed page, distinction in practice can be quite
70 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 9 Barrett s Dysplasia by M. Bronner, M.D. challenging, especially in endoscopic biopsies. Now that a few groups have published natural history data on dysplasia in Barrett s esophagus, and have shown that continued endoscopic surveillance may be a somewhat safe option for patients with high-grade dysplasia (see below), the precise distinction between high-grade dysplasia and intramucosal carcinoma is becoming ever more important. Inter- and intra-observer variability data did not exist regarding this distinction from mucosal biopsy material until the recent study at the Cleveland Clinic Foundation (Table 1 above). Unfortunately, these data document that accurate distinction of high-grade dysplasia from adenocarcinoma may not be possible based on mucosal biopsy morphology. Brush Cytology Brush cytology may not be as sensitive or specific as histology in detecting Barrett s neoplastic epithelium. Although thought to be useful in detecting dysplasia in several studies, 16,17 others have found that its addition to histology increased the cost but not the diagnostic yield for dysplasia or cancer. 18 The use of brush cytology to diagnose Barrett s esophagus via nonendoscopic screening techniques may have more utility. 19 Flow Cytometry DNA content flow cytometry has been extensively evaluated in the study of neoplastic progression in patients with Barrett s esophagus. The prevalence of DNA aneuploidy and /or increased 4N (G2/tetraploid) and S-phase fractions all increase with increasing histologic grade. 13 DNA aneuploidy can be detected in paraffin embedded mucosal biopsy specimens, and may help determine the significance of epithelial alterations in negative, indefinite and even possibly the low-grade dysplastic biopsy categories. 11,13 It appears to be adjunctive, but experts in this field do not recommend that it replace histology. 13 Once the histologic diagnosis of highgrade dysplasia has been made, DNA flow cytometry adds no additional prognostic information. The late Dr. Rodger Haggitt notes additional insights into neoplastic progression that are afforded by DNA flow cytometry in his excellent review on Barrett s esophagus. 1 Specific Genetic Abnormalities in Barrett s Esophagus Although many genetic abnormalities have been documented in Barrett s esophagus, these tend to correlate with advancing histologic grades of neoplastic progression. However, to date, long-term, prospective studies are virtually non-existent to determine the potential clinical utility of these markers. No genetic marker has yet been shown to be a better predictor of cancer than histologic neoplastic progression, and in particular, high-grade dysplasia. 1 Reproducibility studies regarding genetic biomarkers of cancer risk are also limited to non-existent, and ease of extrapolation of these methods to routine use remains unknown. There has never been to date, to the knowledge of this author, a single patient who was referred for esophagectomy or any other high-risk therapy, for anything other than a histologic diagnosis of high-grade dysplasia or cancer in Barrett s esophagus. This may and hopefully will change in the future, but the current standard of care continues to rely upon histology. Significance and Management of Barrett s Dysplasia Management of the patient with dysplasia complicating Barrett s esophagus presents a difficult task. Until very recently, insufficient numbers of patients with dysplasia had been followed for a long enough period and using adequate numbers of biopsies to achieve a high degree of diagnostic confidence, to determine the natural history of dysplasia in Barrett s esophagus. Two large cohorts of patients with Barrett s esophagus have been followed extensively using similar rigorous high-density surveillance biopsy protocols. One program is at the Hines VA Hospital in Chicago, 20 and the other is at the University of Washington in Seattle. 13
71 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 10 Barrett s Dysplasia by M. Bronner, M.D. At the Hines VA program, 20 a total of 1,099 patients were followed with Barrett s esophagus over a 20-year period. Of these, 79 (7.2%) patients had high-grade dysplasia, of which 34 had prevalent high-grade dysplasia (present at the first endoscopy) and 45 had incident high-grade dysplasia (detected during surveillance and therefore probably earlier in its natural history). Of the 75 who remained without detectable cancer during the first year of intensive biopsy surveillance, only 12 patients (16%) developed cancer over a mean of 7.3 years of surveillance. Further, 11 of the 12 who were compliant with the surveillance protocol were considered cured of their early cancers by surgical or ablative therapy. These findings support that high-grade dysplasia does not inexorably and rapidly progress to cancer, as previously feared. This previous unsubstantiated fear drove the standard of care over the past several decades that high-grade dysplasia was an indication for esophagectomy. The Hines VA data supports that it is much safer than previously thought to follow these patients, albeit with great vigilance. In the 15-year prospective longitudinal study at the University of Washington, 13 a total of 327 patients were evaluated by rigorous surveillance endoscopy for progression from their baseline alterations, as interpreted by the late Dr. Rodger Haggitt. Median surveillance intervals were 24.4 months for baseline negative histology, 18.2 months for indefinite histology, 15.7 months for low-grade dysplasia, and 4.6 months for high-grade dysplasia. Overall mean and medium follow-up periods were 3.9 and 2.4 years, respectively. Overall, a total of 42 patients developed cancer and 35 of these developed it within 5 years of their first endoscopy. No patient with negative, indefinite or low-grade dysplasia with normal flow cytometric studies developed cancer within 5 years; this patient group comprised two-thirds of the entire cohort. This indicates that surveillance intervals could be lengthened to 5 years for this majority subset, using the intensive Seattle surveillance protocol, including baseline intensive biopsies and flow cytometry with expert preparation and interpretation of both. The benefits of extending the surveillance interval are manifold. No biomarkers were more powerful or diagnostically significant than the histologic detection of neoplastic progression and high-grade dysplasia in particular, which had a 5-year cancer incidence of 59%. Detailed information on the cancers that developed in this surveillance protocol and their curability were not provided by Reid and colleagues. TABLE 3. NATURAL HISTORY OF BARRETT S NEOPLASTIC PROGRESSION: FROM THE SEATTLE COHORT AND DR. RODGER HAGGITT
72 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 11 Barrett s Dysplasia by M. Bronner, M.D. The above graphs derive from the Seattle cohort (Table 3), and like the Hines VA data, show that lesions less than high-grade dysplasia (metaplasia, indefinite, and low-grade dysplasia) have a very low rate of progression over even greater than 10 years of follow-up, if they do so at all. The right hand graph above also shows that even high-grade dysplasia itself, as diagnosed by the late Dr. Rodger Haggitt, does not inexorably progress to cancer. In fact, one can increase the margin of safety if continued surveillance is performed for incident rather than prevalent highgrade dysplasia as shown. Specifically, incident high-grade dysplasia is discovered after the patient has been under surveillance with adequate biopsy sampling for some period of time. As shown, this type of high-grade dysplasia has only an ~20% progression rate to cancer after 6 years of follow-up. This is undoubtedly because incident high-grade dysplasia is diagnosed closer to the time at which it actually begins, and is therefore much more likely to be early in its progression. Prevalent high-grade dysplasia, on the other hand, is diagnosed at the patient s first endoscopy, when they are symptomatic in some way, and has therefore been present for an unknown and likely much longer period of time than incident high-grade dysplasia. Prevalent high-grade dysplasia would thus be expected to have a higher rate of progression to cancer, as it is further along in its neoplastic pathway than incident disease. Based on these natural history data, we finally are beginning to form a rational basis for patient management. Especially in the setting of a patient who may be a poor surgical candidate, and in one who has incident high-grade dysplasia, continued intensive surveillance is now a more acceptable option. The reproducibility of the discussed Seattle and Chicago data, and the non-trivial issue of the transportability of this type of intensive surveillance from research settings into practice both remain serious and important caveats at this time, however. Squamous Overgrowth Successful antireflux therapy can eliminate or reduce the intensity of reactive changes secondary to inflammation that may be misinterpreted as dysplasia. Successful medical or surgical antireflux therapy may also be associated with some downward migration of the SCJ and with the development of squamous islands within the Barrett s segment; however, complete regression of all Barrett s epithelium rarely occurs. Prior biopsy sites, proton pump inhibitor therapy and ablative therapies are also associated with the development of squamous islands. Such squamous overgrowth may cause an underestimation of the endoscopic extent of Barrett s mucosa, as metaplastic epithelium may persist beneath squamous re-epithelialized areas in Barrett s esophagus. 21,22 The magnitude of this problem remains unknown. The grading of dysplasia in metaplastic epithelium beneath squamous overgrowth remains uncharted territory. This author approaches it as follows: bland epithelium can be classified as negative for dysplasia and severely crowded and cytologically severely atypical glands with loss of nuclear polarity can be recognized as high-grade dysplasia or invasive carcinoma. However, because of the squamous overgrowth, maturation to the mucosal surface cannot be ascertained, so that the distinction between low-grade dysplasia and indefinite cannot be reliably made. This author classifies biopsies in this part of the spectrum beneath squamous mucosa all as indefinite for dysplasia. High-Grade Dysplasia as a Marker for Unsampled Carcinoma When high-grade dysplasia is detected for the first time in a patient with Barrett s esophagus, early re-endoscopy with multiple biopsies should be done to rule out a coexisting early carcinoma. 9,20 Extensive sampling of the mucosa is essential, as early carcinomas may not be recognizable to the endoscopist. Accordingly, it has been recommended based on mathematical data modeling that the sampling interval be increased to 4 biopsies every 1 cm throughout the Barrett s segment in patients with high-grade dysplasia. Because high-grade
73 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 12 Barrett s Dysplasia by M. Bronner, M.D. dysplasia is rare in unselected patients with Barrett s esophagus, and because most pathologists therefore do not have the opportunity to study many examples of it, the general pathologist would be wise to seek a second opinion regarding the diagnosis of high-grade dysplasia before surgery is undertaken. The patient with early carcinoma, either intramucosal or submucosa and who has a reasonable estimated operative risk is a candidate for esophagectomy because these lesions have a low, but significant potential to metastasize (5% for intramucosal ca and 10-20% for submucosal invasion have positive nodes). 23 Resection of early carcinoma provides the best opportunity for cure. 20,24,25 In patients with an endoscopic diagnosis of high-grade dysplasia, but not carcinoma, and who undergo esophagectomy, a relatively high prevalence of carcinoma in resected specimens has been reported. 25 This has lead to the conclusion that high-grade dysplasia is a marker for coexisting adenocarcinoma, but this conclusion has been based on small numbers of patients, many of whom already had advanced prevalent disease. When thorough endoscopic biopsy sampling is carried out according to the protocol outlined above, biopsies have been said to accurately determine whether or not a clinically unsuspected carcinoma accompanies the dysplasia. 9,20 Following such a policy has produced a high cure rate for early adenocarcinoma in Barrett s esophagus, but at the same time, avoids esophagectomy in patients with high-grade dysplasia who may never develop carcinoma (as many as ~41-84% based on the University of WA and Hines VA data). 9,20 However, given the intensity of the biopsy protocols mentioned above, it is uncertain whether this information can be extrapolated to other centers. In fact, preliminary data presented at this meeting from the Cleveland Clinic suggests that the Seattle protocol may not be as safe as has been stated, in that 10 of 29 patients without endoscopically visible lesions and high-grade dysplasia on preoperative biopsy sampled by the Seattle 1cm interval protocol have more advanced pathology (intramucosal and submucosal carcinomas) at resection. 12 Endoscopic Ablative Therapy in Barrett s Esophagus Non-surgical methods for the treatment of patients with high-grade dysplasia are being explored, and with very promising results. These include photodynamic therapy, multipolar electrocoagulation, heater probe, and argon plasma coagulation Photodynamic therapy (PDT), has now completed a phase III FDA controlled 2 year trial of 208 patients for the treatment of Barrett s with high-grade dysplasia. 26,30,31 Interim results demonstrate that after a mean follow-up of two years (out of a total follow-up of 5 years now under analysis), 77% had complete ablation of all of their high-grade dysplasia relative to 39% in the omeprazole only control arm with continued surveillance (p<0.006). Further, PDT patients had a greater than 1.5- fold reduction in cancer development, compared to controls without PDT under identical surveillance and selection conditions. 30,31 BARRETT S DYSPLASIA REFERENCES 1. Haggitt RC. Barrett s esophagus, dysplasia and adenocarcinoma. Hum Pathol 27: , Antonioli DA, Wang HH. Morphology of Barrett s esophagus and Barrett s-associated dysplasia and adenocarcinoma. Gastroenterol Clin N Am 26: , Cameron AJ, Zinsmeister AR, Ballard DJ, et al. Prevalence of columnar-lined (Barrett ) esophagus: comparison of population-based and autopsy findings. Gastroenterology 99: , Sharma P, Morales TG, Sampliner RE. Short segment Barrett s esophagus the need for standardization of the definition and of endoscopic criteria. Am J Gastroenterol 93:
74 USCAP Atlanta 2006, Haggitt GIPS Companion Meeting Page 13 Barrett s Dysplasia by M. Bronner, M.D. 5. Nobukawa B, Abraham SC, Gill J, Heitmiller RF, et al. Clinicopathologic and molecular analysis of highgrade dysplasia and early adenocarcinoma in short- versus long-segment Barrett esophagus. Hum Pathol 32: , Riddell RH, Goldman H, Ransohoff DF, et al. Dysplasia in inflammatory bowel disease: standardized classification with provisional clinical applications. Hum Pathol 14: , Lee RG. Adenomas arising in Barrett s esophagus. Am J Clin Pathol 85: , Montgomery E, Bronner MP, Goldblum JR, et al: Reproducibility of the diagnosis of dysplasia in Barrett esophagus (BE): A reaffirmation. Hum Pathol 32:368-78, Levine DS, Haggitt RC, Blount PL, et al. A systematic endoscopic biopsy protocol can differentiate highgrade dysplasia from early adenocarcinoma in Barrett s esophagus. Gastroenterology 105:40-50, Cameron AJ, Carpenter HA. Barrett s esophagus, high-grade dysplasia, and early adenocarcinoma: A pathological study. Am J Gastroenterol 92: , Reid BJ, Blount PL, Rubin CE, et al. Predictors of progression to malignancy in Barrett s esophagus: endoscopic, histologic and flow cytometric follow-up of a cohort. Gastroenterology 102: , Plesec TP, Kariv R, Mendelin JE, Bennett AE, Castilla E, Henricks WH, Schoenfield L, Skacel M, Yerian LM, Oldenburgh M, Falk GW, Rice TW, Bronner MP, Goldblum JR. Does an Intensive Pre-Resection Biopsy Miss Significant Lesions in Barrett s Esophagus? USCAP abstract, Atlanta Reid BJ, Levine DS, Longton G, et al. Predictors of progression to cancer in Barrett's esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets. Am J Gastroenterol 95: , Mendelin JE, Bennett AE, Castilla E, Henricks WH, Schoenfield L, Skacel M, Yerian LM, Rice TW, Rybicki LA, Bronner MP, Goldblum JR. Interobserver agreement in the evaluation of pre-resection biopsies with at least high-grade dysplasia (HGD) in 163 Barrett s esophagus (BE) patients. Mod Pathol 18 (S-1): 112A, Yearsley MM, Haggitt RC, Taylor SL, Overholt BF, Depot M, Emond MJ, Bronner MP. Reinterpretation of high-grade dysplasia in Barretts esophagus: A multicneter international phase III trial in 485 patients. USCAP abstract, Atlanta Wang HH, Sovie S, Zeroogian JM, et al. Value of cytology in detecting intestinal metaplasia and associated dysplasia at the gastroesophageal junction. Hum Pathol 28: , Geisinger KR, Teot LA, Richter JE. A comparative cytopathologic and histologic study of atypia, dysplasia and adenocarcinoma in Barrett s esophagus. Cancer 69:8-16, Alexander JA, Jones SM, Smith CJ, et al. Usefulness of cytopathology and histology in the evaluation of Barrett s esophagus in a community hospital. Gastrointest Endosc 46: , Rader AE, Faigel DO, Ditomasso J, Magaret N, Burm M, Fennerty MB. Cytologic screening for Barrett s esophagus using a prototype flexible mesh catheter. Diag Dis Sci 46: , Schnell TG, Sontag SJ, Chejfec G, et al. Long-term nonsurgical management of Barrett's esophagus with high-grade dysplasia. Gastroenterology 120: , Sharma P, Morales TG, Bhattacharyya A, et al. Squamous islands in Barrett s esophagus: what lies underneath? Am J Gastroenterol 93: , Biddlestone LR, Barham CP, Wilkinson SP, et al. The histopathology of treated Barrett s esophagus. Am J Surg Pathol 22: , Paraf F, Fléjou J-F, Pignon J-P, et al. Surgical pathology of adenocarcinoma arising in Barrett s esophagus: Analysis of 67 cases. Am J Surg Pathol 19: , Rusch VW, Levine DS, Haggitt RC, et al. The management of high-grade dysplasia and early cancer in Barrett s esophagus. Cancer 74: , Rice TW, Falk GW, Achkar E, et al. Surgical management of high-grade dysplasia in Barrett's esophagus. Am J Gastroenterol 88: , Overholt BF. Evaluating treatments of Barrett's esophagus that shows high-grade dysplasia. Am J Manag Care 6(16 Suppl):S Review, 2000.
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Division of Anatomic Pathology & Molecular Oncology, University of Utah and ARUP Laboratories, Huntsman Cancer Institute, Salt Lake City, UT, USA
 REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, by Am. Coll. of Gastroenterology ISSN /02/$22.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
One of the more common specimens encountered by
 Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Burning Issues in the Esophagus
 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
The presence of intestinal-type goblet cells (ITGCs) in
 in") Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL
 THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Part 1. A pragmatic approach to common problems in esophageal biopsy pathology
 Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following
Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful in characterizing esophageal location
 Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Diagnosis and grading of dysplasia in Barrett s oesophagus ... J Clin Pathol 2006;59: doi: /jcp
 1029 MY APPROACH Diagnosis and grading of dysplasia in Barrett s oesophagus R D Odze... This review focuses on the pathological features of dysplasia in Barrett s oesophagus. Two categorisation schemes
1029 MY APPROACH Diagnosis and grading of dysplasia in Barrett s oesophagus R D Odze... This review focuses on the pathological features of dysplasia in Barrett s oesophagus. Two categorisation schemes
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations
 Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
The normal esophagus is lined with squamous epithelium.
 .. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
.. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus. Original Policy Date
 MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
The increasing incidence of esophageal adenocarcinoma
 GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Case in discussion. Common diagnostic problems in gallbladder pathology 62, F
 Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
chapter 4. The effect of oncogenic HPV on transformation zone epithelium
 chapter 4. The effect of oncogenic HPV on transformation zone epithelium CHAPTER 1 All squamous cervical cancer (and probably all cervical adenocarcinoma) is associated with oncogenic HPV, and the absence
chapter 4. The effect of oncogenic HPV on transformation zone epithelium CHAPTER 1 All squamous cervical cancer (and probably all cervical adenocarcinoma) is associated with oncogenic HPV, and the absence
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)
 - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)") SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
During the past 30 years, the incidence of esophageal ORIGINAL ARTICLES
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:38 43 ORIGINAL ARTICLES Optical Coherence Tomography to Identify Intramucosal Carcinoma and High-Grade Dysplasia in Barrett s Esophagus JOHN A. EVANS,* JOHN
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:38 43 ORIGINAL ARTICLES Optical Coherence Tomography to Identify Intramucosal Carcinoma and High-Grade Dysplasia in Barrett s Esophagus JOHN A. EVANS,* JOHN
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Chapter 12: Training in Pathology. DDSEP Chapter 13: Question 19
 DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Barrett s Esophagus and Barrett s-associated Neoplasia: Etiology and Pathologic Features
 Barrett s Esophagus and Barrett s-associated Neoplasia: Etiology and Pathologic Features Domenico Coppola, MD, and Richard C. Karl, MD Enhancement of molecular markers and cytology may improve outcomes
Barrett s Esophagus and Barrett s-associated Neoplasia: Etiology and Pathologic Features Domenico Coppola, MD, and Richard C. Karl, MD Enhancement of molecular markers and cytology may improve outcomes
ATLAS OF HEAD AND NECK PATHOLOGY METAPLASIA
 Metaplasia is the conversion of one adult differentiated cell type to another. Generally it is the result of persistent cellular trauma and serves as a protective mechanism. Thus anteriorly along the nasal
Metaplasia is the conversion of one adult differentiated cell type to another. Generally it is the result of persistent cellular trauma and serves as a protective mechanism. Thus anteriorly along the nasal
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Cytology Report Format
 Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
DIGESTIVE TRACT ESOPHAGUS
 DIGESTIVE TRACT From the lower esophagus to the lower rectum four fundamental layers comprise the wall of the digestive tube: mucosa, submucosa, muscularis propria (externa), and adventitia or serosa (see
DIGESTIVE TRACT From the lower esophagus to the lower rectum four fundamental layers comprise the wall of the digestive tube: mucosa, submucosa, muscularis propria (externa), and adventitia or serosa (see
Normal Morphology. Anatomic Considerations. Normal Urothelial Histology and Cytology
 1 Normal Morphology Anatomic Considerations The urinary tract can be divided into three regions: the kidney; the calyces, pelves and ureters (upper collecting system or upper tract); and the bladder and
1 Normal Morphology Anatomic Considerations The urinary tract can be divided into three regions: the kidney; the calyces, pelves and ureters (upper collecting system or upper tract); and the bladder and