Part 1. A pragmatic approach to common problems in esophageal biopsy pathology
|
|
|
- Leslie Leonard
- 5 years ago
- Views:
Transcription


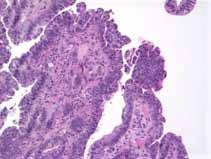
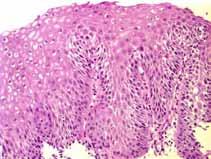
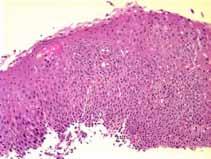
1 Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following biopsies are taken from the distal esophagus of a 57 year old man who has a history of Barrett s esophagus. He had a diagnosis of indefinite for dysplasia made one year ago. Surface epithelium not as concerning Collection of crowded tubules in deep mucosa 1
2 What is your diagnosis? How sure are you? Why is dysplasia in the setting of Barrett s esophagus our most common consultation case? Dysplastic mucosa has no reliable endoscopic features. Mucosal elevation Flat mucosa 2

3 The consequences of a diagnosis of dysplasia are significant. More frequent endoscopy A surgical procedure While some specimens with dysplasia are very common... Colorectal adenoma Surveillance biopsies of Barrett s mucosa are less common specimens So we have fewer opportunities to define our thresholds, and fewer chances to see follow up. 3
4 The features of dysplasia and regeneration may be only subtly different, making the distinction maddeningly difficult! It would be great if we could define precancerous epithelium by its molecular changes, but until this is practical on a day to day basis we must make morphologic diagnoses! Terminology for dysplasia Two grades: Low grade High grade Indefinite for dysplasia introduced at the same time as 2-grade system for cases that are not clearly dysplastic, nor clearly regenerative. 4

5 Management recommendations for Barrett s are based on this 2-grade system. Diagnosis Management Negative Indefinite for dysplasia Low grade dysplasia Moderate dysplasia High grade dysplasia Follow up at routine interval Follow up at shortened interval Confirmation by expert Follow up at shortened interval Confirmation by expert Resection or Ablative therapy or Follow up at very short interval What are the histologic features we use to diagnose dysplasia? Cytologic abnormalities Nuclear enlargement, hyperchromasia, pleomorphism Increased mitoses, especially near or at surface Loss of cytoplasmic maturation, including decrease or loss in mucin 5


6 Architectural abnormalities Nuclear stratification, loss of polarity Complex arrangements, crowded tubules Abnormal surface villiform rather than flat Low Grade Dysplasia Mild, or no architectural abnormalities Nuclear stratification usually not full thickness of epithelium Polarity retained These features involve the surface, not just the epithelium deep in the mucosa. What are the criteria for high grade dysplasia? Worse than low grade dysplasia! How much worse? 6


7 High Grade Dysplasia Architectural abnormalities, often marked Nuclear stratification and cytologic abnormalities more marked than low grade, loss of polarity What are the criteria for indefinite for dysplasia? Probably not definable Published criteria include: Marked nuclear abnormalities in deep mucosa, with surface that matures or mostly matures Biopsies with disturbing cytologic/architectural abnormalities, but with significant inflammation or lack of evaluable surface 7


8 Journals and textbooks make these criteria seem straightforward. Are these images good examples of low and high grade dysplasia? Do most of your biopsies look like this? Practice Parameters Committee of the American College of Gastroenterology: An expert pathologist should confirm the interpretation of low and high-grade dysplasia. The most common type of GI consultation case handled at UM is the Barrett s biopsy sent for diagnosis/confirmation and grading of dysplasia. 8

9 Starting in late 2003, we began recording our votes on Barrett s and colitic dysplasia cases. Also, in cases of adenomas with a question of invasive carcinoma or not. Over ~18 months we voted on 432 biopsies from 332 cases. The consult diagnoses were different from those of the submitting pathologist 66% of the time. In 45% of cases the different diagnoses would indicate different management. Diagnosis Management Negative Indefinite for dysplasia Low grade dysplasia High grade dysplasia Carcinoma Follow up at routine interval Follow up at shortened interval Confirmation by expert, Follow up at shortened interval Confirmation by expert Resection or Ablative therapy or Follow up at very short interval Resect, either endoscopically or open, possible neoadjuvant Rx 9
10 What happens to the cases diagnosed as high grade dysplasia and sent for confirmation? HGD 3% Neg 29% Indef/LGD 35% HGD 25% Susp for CA 8% CA So, maybe the recommendation to have diagnoses of high grade dysplasia reviewed is appropriate? What happens with other diagnoses that we reviewed? Contributors diagnosis Negative Negative Indefinite/ Low grade High grade/ suspicious for carcinoma Carcinoma 76% 15% 6% 3% Indefinite/ Low grade 22% 50% 27% <1% High grade/ suspicious for carcinoma Carcinoma U of Michigan consultant diagnosis <2% 24% 56% 19% % 86% 10
11 How much did the 3 consultants agree? All three agreed: 46% 2 of 3 agreed: 46% No agreement: 8% What do we agree on the most? Negative 84% Indefinite 34% Low grade 23% At least low grade 23% High grade 50% Suspicious for CA 52% Carcinoma 74% How much did our disagreements involve management difference? 33% of all biopsies 10% between Neg and Indef/LG 15% between Indef/LG and HG 8% between HG and Carcinoma 11
12 Summary: The consultation diagnosis significantly differs from the contributed diagnosis 45% of the time. There is significant disagreement among the consultants 33% of the time. Who is right? The contributing pathologist? Appelman? Greenson? McKenna? Who Knows? Some of our internal differences were between suspicious for carcinoma and carcinoma. Does this matter? 12
13 HGD in Barrett s as a marker for Carcinoma Literature tells us that 30-50% of Barrett s patients with HGD on biopsy will have carcinoma in esophagectomy. Yet, when patients with HGD are followed closely with repeat endoscopy and biopsy, only 8-10% develop carcinoma on follow up. At Michigan 127 Esophagectomies resected for biopsy diagnoses of HGD or HGD/susp for ca 69 of the biopsies were reviewed and reclassified Neg LGD HGD Susp for CA CA In our cases at Michigan: Only one of 21 HGD biopsies had CA in the resection, 4.8% Much different than the 30-50% that we read in the literature! 13


14 In our cases at Michigan: 72% of those we classified as suspicious for carcinoma had carcinoma in the resection 74% of those we classified as carcinoma had carcinoma in the resection Thus, a diagnosis of suspicious for carcinoma is the same as an outright diagnosis of carcinoma in our practice! What do we use to diagnose a Barrett s biopsy as suspicious for carcinoma? First, What are the criteria to diagnose carcinoma in Barrett s mucosa? Carcinoma invading the submucosa elicits a characteristic desmoplastic stromal reaction 14

15 Intramucosal carcinoma definition: carcinoma cells extending beyond basement membrane into lamina propria How does one recognize carcinoma cells extending beyond the basement membrane? Criteria used by those who studied intramucosal carcinoma in Barrett s Syncytial growth pattern Abortive microglands Small clusters of epithelial cells infiltrating lamina propria between glands Irregularly shaped tubules Solid nests of neoplasm Interobserver agreement on this diagnosis is not great (kappa ~ 0.5) Downs-Kelly E, et al. Am J Gastroenterol 2008;103: Syncytial/ solid growth pattern? 15




16 Abortive microglands???? Small clusters of epithelial cells infiltrating lamina propria between glands Irregularly shaped, atypical tubules infiltrating between benign-looking tubules Irregularly shaped, atypical tubules with infiltrative pattern 16

17 Solid/cribriform pattern Riddell OESO, 1998 The only criterion for the confident diagnosis of invasive carcinoma in the lamina propria is the pathologist s own subjective and personal interpretation that invasion may or may not be present. Greenson: I know it when I see it What features did we use to classify a biopsy as suspicious for carcinoma? Many are similar to those used to diagnose intramucosal carcinoma Cribriform architecture of tubules Dilated tubules containing necrotic debris Extensive neutrophilic infiltrate in highly dysplastic epithelium Squamous epithelial invasion by tubules 17
18 18
19 19

20 Cribriform architecture of tubules Dilated tubules containing necrotic debris Extensive neutrophilic infiltrate in highly dysplastic epithelium Squamous epithelial invasion by tubules When one of these features was present in the biopsy, there was carcinoma in the subsequent resection in 40% of cases. When 2 or more were present, the rate was >80%! Zhu et al. AJCP 2009;132: Let s look at some of these cases.. 20

21 10307c 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma All three consultants called Negative Why negative? Slightly enlarged nuclei at base, maturation at surface c 21

22 10307d 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma 2 consultants called indefinite 1 called low grade 22


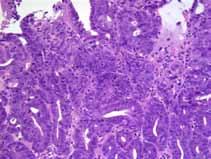
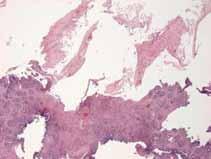
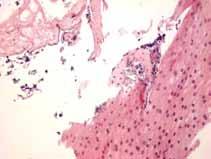
23 The question of whether this is low grade dysplasia depends on your interpretation of the surface epithelium Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia Carcinoma All 3 consultants called this carcinoma. 23

24 Very complex architecture Small nests of cells that seem to invading lamina propria


25 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma Two consultants called this at least low grade. 1 called it high grade. One of us thought surface nuclear abnormalities were sufficient for high grade; Two didn t think the architecture was complex enough. The previous photos were from the 179 biopsies we all voted on. Some of the sections and stains are less than ideal. Perhaps I didn t choose the microscopic fields that the others would have The next set of photos are ones for which the votes were placed on the IMAGE, rather than the glass slide. 25


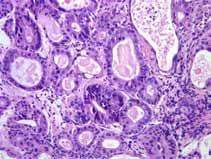
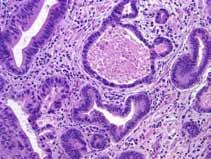
26 1 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma Two consultants called high grade I said suspicious for carcinoma 1 Nuclear abnormalities and architecture sufficiently abnormal for high grade. Tubule with necrotic debris raised concern for carcinoma. 26

27 4 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma 4 Two consultants called high grade I said at least low grade 4 The one who stuck with at least low grade did so because he didn t think the architectural abnormalities were sufficiently complex. 27

28 5 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma Two consultants called it low grade I said at least low grade 5 This focus must have looked like it was approaching high grade to one of us. At least all agreed that it was dysplastic. 28

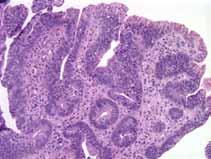
29 6 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma Two consultants called it indefinite 1 said low grade 6 The surface looks abnormal and that bothered all of us, but there is not much else here. One thought that was enough. 29
30 8 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma All three consultants called it low grade 8 Finally! Something we can all agree on! 30
31 9 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma All three consultants called it high grade No problem here very atypical, disorganized, architecturally complex. 9 31

32 11 1. Negative 2. Low grade dysplasia 3. At least low grade dysplasia 4. High grade dysplasia 5. Suspicious for carcinoma 6. Indefinite for dysplasia 7. Carcinoma Two consultants called it negative 1 said indefinite 11 And here, I included this as one we could all agree on as negative! Just goes to show you 32
33 What does that go to show us? Histologic criteria for low and high grade dysplasia have been defined, and you can read about them and see lovely pictures in any GI pathology text. Presumably these criteria are based on what is known about follow up and outcome for these type of epithelia. We also find that: Applying the criteria to real life cases is difficult, and reproducibility is poor. Consultants (at least 3 we know) disagree with submitting pathologists more than half of the time, and with each other about a third of the time. These same consultants change more low grade outside diagnoses to high grade than the converse. How many of your diagnoses matched at least one of ours? Remember.we all agreed only 46% of the time! 33
34 Until something better comes along We must all do the best we can with our histologic diagnoses Adjust our thresholds to our colleagues, especially those who have more experience with follow up of cases and are therefore more expert. Until something better comes along Accept that fact that we cannot agree much of the time, and that disagreeing does not in itself make anyone wrong. Case #2 These esophageal biopsies were obtained from a 14 year old boy who complains of dysphagia. 34

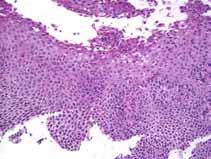
35 Upper esophagus 35

36 Distal esophagus 36
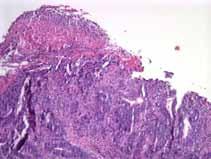
37 What is your diagnosis? Sure looks like a case of eosinophilic esophagitis! How specific are you able to be in your report? What terminology do you use? Eosinophilic esophagitis is an increasingly prevalent and recognized esophageal disease, and attempts to diagnose this disease result in many of our esophageal biopsies. First reported in the 1970 s with scattered case reports over the next two decades. Dramatic rise in patients diagnosed with EoE and publications concerning EoE since mid 1990 s. Now known to be a worldwide disease. The classic patient with EoE is young, more likely male, more likely Caucasian, but.. EoE can occur in people of any age, gender, or ethnicity. 37
38 The clinical presentation tends to be different in young children than in adults. Failure to thrive Vomiting Nausea Regurgitation Epigastric or chest pain Dysphagia/food impaction Nausea, vomiting Heartburn A personal and family history of atopic disorders (asthma, eczema, allergic rhinitis is present in more than half of patients. Many studies suggest that food allergy is the cause of most cases of EoE. Removal of dietary antigens with an elemental diet improves symptoms and histology in 98% of patients. Results of allergy testing are good at guiding effective dietary therapy, via elimination diets. However, there is likely a role for aeroallergens in some patients, as well. Maybe because some environmental allergens cross react with food allergens (grass and wheat)? Dietary therapy alone, however, does not work in many patients. Dietary modification is not easy, and can be costly (elemental formulas). Corticosteroids, either systemic or swallowed are often effective. A combined approach, using dietary therapy, swallowed corticosteroids, and proton pump inhibitors has been found to be effective in >90% of patients, but many patients relapse. Experimental studies of IL-5 blockers are showing promise. (IL-5 involved in recruitment, proliferation and survival of eosinophils.) 38
39 The diagnosis depends on recognizing suggestive symptoms and performing upper endoscopy with biopsy. Some patients have endoscopic abnormalities and some do not, so biopsies are required for the diagnosis. At least a third of patients have normal appearance. Rings White exudates Not everyone with these findings has EoE! Furrows Narrow caliber The diagnostic histologic findings are patchy, so the diagnostic sensitivity of biopsies increases with the number of biopsies. At least four biopsies from each the upper and lower esophagus are recommended. 39


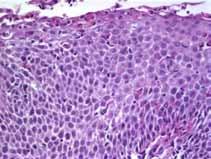
40 The classic histologic appearance of EoE intraepithelial eosinophilia superficial layering of eosinophils eosinophil microabscesses basal zone hyperplasia increased lymphocytes and mast cells Huge numbers of eosinophils, eosinophil microabscesses, superficial layering of eosinophils Some of the eosinophils are degranulated. 40



41 Basal zone hyperplasia It is hard to see the lymphocytes and mast cells in the background, but they are there! Lamina propria fibrosis shows up in a deep biopsy or resection. 41

42 Reflux esophagitis also has eosinophils, but usually far fewer that EoE, although there is overlap. Fortunately, Reflux E almost always has < 5-10 eos/hpf, and EoE usually has more than 20, like Reflux esophagitis Eosinophilic esophagitis The pathologic diagnosis of EoE has been evolving, but has involved mostly the quantitation of the intraepithelial eosinophils. An AGA consensus statement in 2007 (Furuta, et al, Gastroenterol 133: ) defined EoE as requiring greater than or equal to 15 intraepithelial eosinophils/hpf in one or more biopsies, and the absence of GERD based on ph monitoring and the lack of response to PPI. Based on that recommendation, here is how we have been signing out any esophageal biopsy with eosinophils: Esophagitis with eosinophils, maximum count of per HPF 42
43 A recent updated consensus document (2011) upholds the 15 eosinophils/hpf criterion, but adds the following statement: Pathologists should report all abnormalities associated with EoE, such as the peak eosinophil value (obtained from the area with the highest density of eosinophils), eosinophilic microabscesses, surface layering of eosinophils, extracellular eosinophil granules, basal cell hyperplasia, dilated intercellular spaces, and lamina propria fibrosis. Liacouras, et al. J Allergy Clin Immunol July, 2011 Now what should we do? What do you do? Eosinophilic esophagitis is a recognized clinicopathologic entity, in which pathologists play a pivotal role in diagnosis. At the very least, it is incumbent upon us to give a count of the maximum concentration of eosinophils. You will have to work with your gastroenterologists to see what else, if anything, they require. 43
44 Case 3 56 year old woman with multiple medical problems, on multiple medications She presents with chest pain and dysphagia, and undergoes upper endoscopy as part of the evaluation. Endoscopic findings: White plaques or membranes present in mid- and distal esophagus. Biopsies and brushings obtained. Requisition says, R/O Candida 44


45 Squamous mucosa and strips of detached surface epithelial cells Detached layer of necrotic superficial epithelium No fungus The intact squamous mucosa has a sharply delineated superficial layer of squamous cells with eosinophilic cytoplasm and pyknotic nuclei. 45

46 What is this? Sloughing esophagitis A small group of cases (4) was described in abstract form. Patients had endoscopic membranes, detached superficial necrotic epithelium, and tended to be debilitated patients. Moore RJ, et al. Sloughing esophagitis: a distinct histologic and endoscopic entity. Mod Pathol 1999;12:81A 24 cases of sloughing esophagitis at UM: Compared with a group of 34 controls, Sloughing esophagitis patients were significantly more likely to: Be older (median age of 53.5 vs. 43.5) Taking multiple prescription medications, especially CNS depressants and medications known to injure the esophagus (Fe, ASA, KCl, etc.) Be chronically debilitated, bedridden, on home O 2, have metastatic cancer, have an organ transplant, be on immunosuppressive therapy have died in the interval between the biopsy and the study, mean time to death 120 days Have a history of peptic ulcer disease 46
47 Sloughing Control Age or more medications 77% 32% CNS depressants 65% 32% Drugs assoc w esoph 55% 18% injury (Fe, ASA, KCl) Peptic ulcers 55% 24% Renal insuff 16% 0 GERD sx 45% 74% 24 cases of sloughing esophagitis at the University of Michigan: Compared with a group of 34 controls, Sloughing esophagitis patients were significantly LESS likely to: Have GERD There was no difference between SE patients and controls with respect to dysmotility disorders irritable bowel disease atherosclerotic valvular disease. 24 cases of sloughing esophagitis at the University of Michigan: Conclusions: Sloughing esophagitis is a unique endoscopic and histologic entity that occurs in debilitated patients and is associated with medications known to injure squamous mucosa. It is likely to be a direct toxic injury, rather than an ischemic injury. 47
 associated with the endoscopic finding of a back esophageal mucosa.")

48 Is there such a thing as ischemic esophageal injury? Necrotizing esophagitis: The Black Esophagus A rare condition characterized by upper gastrointestinal bleeding (life threatening) associated with the endoscopic finding of a back esophageal mucosa. No history of corrosive or toxic agent. This black mucosa is necrotic and hemorrhagic. Underlying conditions that are believed to predispose patients to an ischemic black esophagus include coronary and peripheral vascular diseases low flow states (e.g., shock) gastric volvulus or gastric-outlet obstruction Pancreatitis cancer acute fatty liver of pregnancy overwhelming infection severe hypothermia severe emesis hyperglycemia (particularly in diabetic ketoacidosis). The necrosis can progress to become full thickness with rupture and lead to death. 48

49 Other cases of sloughing esophagitis.. 49
50 Is sloughing esophagitis a rare condition? We come across a case or two per month. With awareness of the endoscopic appearance, which looks to the endoscopist like Candida and attention to the desquamated necrotic superficial squamous layers I suspect you will begin to recognize a case from time to time. Dr. Elizabeth Montgomery Department of Pathology, Johns Hopkins: Our job is to make sure the patient gets appropriately waited on. In an attempt to follow Dr. Montgomery s advice, these are the questions I am always asking myself: What is my role in making a diagnosis or guiding therapy? What does the provider need to know? What information should I leave out because it is confusing or potentially misleading? What new entities are emerging that I can help gastroenterologists recognize? 50

51 51
Eosinophilic Esophagitis (EoE)
") Eosinophilic Esophagitis (EoE) 01.06.2016 EoE: immune-mediated disorder food or environmental antigens => Th2 inflammatory response. Key cytokines: IL-4, IL-5, and IL-13 stimulate the production of eotaxin-3
Eosinophilic Esophagitis (EoE) 01.06.2016 EoE: immune-mediated disorder food or environmental antigens => Th2 inflammatory response. Key cytokines: IL-4, IL-5, and IL-13 stimulate the production of eotaxin-3
Eosinophilic Esophagitis. Kristine J. Krueger M.D. June 2014
 Eosinophilic Esophagitis Kristine J. Krueger M.D. June 2014 A Most Interesting Patient 36 year old self employed tree surgeon with long standing history of intermittent dysphagia and atypical GERD, NOT
Eosinophilic Esophagitis Kristine J. Krueger M.D. June 2014 A Most Interesting Patient 36 year old self employed tree surgeon with long standing history of intermittent dysphagia and atypical GERD, NOT
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Disclosure. Learning Objectives 4/25/2014. I have no disclosures
 Alka Goyal MD Division of Pediatric Gastroenterology Hepatology and Nutrition Children s Hospital of Pittsburgh of UPMC Disclosure I have no disclosures Learning Objectives Diagnosis of Eosinophilic Esophagitis
Alka Goyal MD Division of Pediatric Gastroenterology Hepatology and Nutrition Children s Hospital of Pittsburgh of UPMC Disclosure I have no disclosures Learning Objectives Diagnosis of Eosinophilic Esophagitis
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations
 Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
When Food Keeps Getting Stuck: Recognizing and Understanding Eosinophilic Esophagitis in Children
 When Food Keeps Getting Stuck: Recognizing and Understanding Eosinophilic Esophagitis in Children Jenifer R. Lightdale, MD, MPH, FASGE Division Chief, Pediatric Gastroenterology UMass Memorial Children
When Food Keeps Getting Stuck: Recognizing and Understanding Eosinophilic Esophagitis in Children Jenifer R. Lightdale, MD, MPH, FASGE Division Chief, Pediatric Gastroenterology UMass Memorial Children
ACG Clinical Guideline: Evidenced Based Approach to the Diagnosis and Management of Esophageal Eosinophilia and Eosinophilic Esophagitis (EoE)
") ACG Clinical Guideline: Evidenced Based Approach to the Diagnosis and Management of Esophageal Eosinophilia and Eosinophilic Esophagitis (EoE) Evan S. Dellon, MD, MPH, 1,6 Nirmala Gonsalves, MD, 2,6 Ikuo
ACG Clinical Guideline: Evidenced Based Approach to the Diagnosis and Management of Esophageal Eosinophilia and Eosinophilic Esophagitis (EoE) Evan S. Dellon, MD, MPH, 1,6 Nirmala Gonsalves, MD, 2,6 Ikuo
Learning Objectives. Disclaimer 9/8/2015. Jean Marie Osborne MS, RN, ANP-C
 Jean Marie Osborne MS, RN, ANP-C Learning Objectives 1. Understand the pathophysiologic process of EoE. 2. Dietary indiscretions 3. Management None to report Disclaimer 1 History EoE as an allergic disease
Jean Marie Osborne MS, RN, ANP-C Learning Objectives 1. Understand the pathophysiologic process of EoE. 2. Dietary indiscretions 3. Management None to report Disclaimer 1 History EoE as an allergic disease
A Chronic or Recurring Pattern of Esophagitis Resembling Allergic Contact Dermatitis
 Anatomic Pathology / Lymphocytic Esophagitis Lymphocytic Esophagitis A Chronic or Recurring Pattern of Esophagitis Resembling Allergic Contact Dermatitis Julianne K. Purdy, MD, Henry D. Appelman, MD, Christopher
Anatomic Pathology / Lymphocytic Esophagitis Lymphocytic Esophagitis A Chronic or Recurring Pattern of Esophagitis Resembling Allergic Contact Dermatitis Julianne K. Purdy, MD, Henry D. Appelman, MD, Christopher
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Eosinophilic Esophagitis: The New Kid on the Block
 6/9/215 Eosinophilic Esophagitis: The New Kid on the Block Consultant: Takeda Disclosures Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal
6/9/215 Eosinophilic Esophagitis: The New Kid on the Block Consultant: Takeda Disclosures Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal
Esophageal Eosinophilia and Eosinophilic Esophagitis. Bible Class 09. Mai 2018
 Esophageal Eosinophilia and Eosinophilic Esophagitis Bible Class 09. Mai 2018 61 yo male No upper-gi symptoms Gastroscopy vor bariatric Operation Lesion: Papilloma Histology of the surrounding mucosa:
Esophageal Eosinophilia and Eosinophilic Esophagitis Bible Class 09. Mai 2018 61 yo male No upper-gi symptoms Gastroscopy vor bariatric Operation Lesion: Papilloma Histology of the surrounding mucosa:
Eosinophilic Oesophagitis Bruce McLain Consultant Paediatric Gastroenterologist University Hospital North Tees
 Eosinophilic Oesophagitis Bruce McLain Consultant Paediatric Gastroenterologist University Hospital North Tees Eosinophilic oesophagitis Outline Definition Incidence and prevalence Pathology Presentation
Eosinophilic Oesophagitis Bruce McLain Consultant Paediatric Gastroenterologist University Hospital North Tees Eosinophilic oesophagitis Outline Definition Incidence and prevalence Pathology Presentation
Rings in the esophagus are not always eosinophilic esophagitis: Case series of ring forming lymphocytic esophagitis and review of the literature
 Rings in the esophagus are not always eosinophilic esophagitis: Case series of ring forming lymphocytic esophagitis and review of the literature Authors Julia L. Pleet 1,SofiaTaboada 2, Arvind Rishi 2,
Rings in the esophagus are not always eosinophilic esophagitis: Case series of ring forming lymphocytic esophagitis and review of the literature Authors Julia L. Pleet 1,SofiaTaboada 2, Arvind Rishi 2,
Eosinophilic Esophagitis. Another Reason Not to Swallow
 Eosinophilic Esophagitis Another Reason Not to Swallow Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Eosinophilic Esophagitis Another Reason Not to Swallow Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Faculty Disclosures Research Support Consultant
 Faculty Disclosures Research Support Shire clinical area: eosinophilic esophagitis Regeneron clinical area: eosinophilic esophagitis Allakos clinical area: eosinophilic gastritis Consultant Shire clinical
Faculty Disclosures Research Support Shire clinical area: eosinophilic esophagitis Regeneron clinical area: eosinophilic esophagitis Allakos clinical area: eosinophilic gastritis Consultant Shire clinical
CS05 NEW DEVELOPMENTS IN GASTROINTESTINAL PATHOLOGY-GIPS FUNNY FORMS OF ESOPHAGITIS: BEYOND GERD AND EOSINOPHILIC ESOPHAGITIS
 CS05 NEW DEVELOPMENTS IN GASTROINTESTINAL PATHOLOGY-GIPS FUNNY FORMS OF ESOPHAGITIS: BEYOND GERD AND EOSINOPHILIC ESOPHAGITIS Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Weill
CS05 NEW DEVELOPMENTS IN GASTROINTESTINAL PATHOLOGY-GIPS FUNNY FORMS OF ESOPHAGITIS: BEYOND GERD AND EOSINOPHILIC ESOPHAGITIS Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Weill
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
What is Eosinophilic Esophagitis (EoE)?
?") EOSINOPHILIC ESOPHAGITIS What is Eosinophilic Esophagitis (EoE)? Eosinophilic esophagitis (EoE) is an illness found in the esophagus (the tube that links your mouth and stomach). EoE is the result of an
EOSINOPHILIC ESOPHAGITIS What is Eosinophilic Esophagitis (EoE)? Eosinophilic esophagitis (EoE) is an illness found in the esophagus (the tube that links your mouth and stomach). EoE is the result of an
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Objectives. Disclosures. Eosinophilic Esophagitis and Nutritional Consequences. Food Allergy In Schools
 Eosinophilic Esophagitis and Nutritional Consequences Douglas T. Johnston, DO, FACAAI, FAAAAI Assistant Professor of Internal Medicine / Allergy & Immunology Edward Via College of Osteopathic Medicine
Eosinophilic Esophagitis and Nutritional Consequences Douglas T. Johnston, DO, FACAAI, FAAAAI Assistant Professor of Internal Medicine / Allergy & Immunology Edward Via College of Osteopathic Medicine
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Eosinophilic esophagitis. Kathleen Boynton MD University of Utah Gastroenterology Division
 Eosinophilic esophagitis Kathleen Boynton MD University of Utah Gastroenterology Division Financial disclosures: Janssen Genetech UCB All for research support Learning Objectives To identify the clinical
Eosinophilic esophagitis Kathleen Boynton MD University of Utah Gastroenterology Division Financial disclosures: Janssen Genetech UCB All for research support Learning Objectives To identify the clinical
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT.
 PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
Case discussions. Case 1
 Case discussions Arzu Ensari 12 year old teen Case 1 Progressive cough and dysphagia following flu-like symptoms Family history of asthma Erythema in lower oesophagus 1 40 eos/hpf 2 What is Eosinophilic
Case discussions Arzu Ensari 12 year old teen Case 1 Progressive cough and dysphagia following flu-like symptoms Family history of asthma Erythema in lower oesophagus 1 40 eos/hpf 2 What is Eosinophilic
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
Eosinophilic oesophagitis
 Eosinophilic oesophagitis Food Allergy (Allergic food hypersensitivity) Mike Levin Paediatric Allergy Red Cross Hospital UCT IgE mediated Mixed Non IgE mediated Disease Mechanisms in EGID Rothenberg, JACI,
Eosinophilic oesophagitis Food Allergy (Allergic food hypersensitivity) Mike Levin Paediatric Allergy Red Cross Hospital UCT IgE mediated Mixed Non IgE mediated Disease Mechanisms in EGID Rothenberg, JACI,
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Burning Issues in the Esophagus
 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Webinar Presenter: Marijn J. Warners, MD, PhD. Department Gastroenterology & Hepatology, Academic Medical Center, Amsterdam
 Efficacy of Amino Acid-based diet on Histologic Remission and Restoring Esophageal Mucosal Integrity in Adult Patients with Eosinophilic Esophagitis (EoE) Dr. Marijn Warners June 23, 2016 Webinar Presenter:
Efficacy of Amino Acid-based diet on Histologic Remission and Restoring Esophageal Mucosal Integrity in Adult Patients with Eosinophilic Esophagitis (EoE) Dr. Marijn Warners June 23, 2016 Webinar Presenter:
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM
 Eosinophilic Esophagitis: Are We There Yet? Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Learning Objectives Understand current definition
Eosinophilic Esophagitis: Are We There Yet? Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Learning Objectives Understand current definition
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
One of the more common specimens encountered by
 Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
pissn: eissn: Journal of Neurogastroenterology and Motility
 JNM J Neurogastroenterol Motil, Vol. 24 No. 2 April, 2018 pissn: 2093-0879 eissn: 2093-0887 https://doi.org/10.5056/jnm17047 Original Article Diagnostic Trends and Clinical Characteristics of Eosinophilic
JNM J Neurogastroenterol Motil, Vol. 24 No. 2 April, 2018 pissn: 2093-0879 eissn: 2093-0887 https://doi.org/10.5056/jnm17047 Original Article Diagnostic Trends and Clinical Characteristics of Eosinophilic
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
What Is Barrett s Esophagus?
 What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
What is Eosinophilic Esophagitis, how is it treated, and will it go away?
 Panelists What is Eosinophilic Esophagitis, how is it treated, and will it go away? Bradley A. Becker, M.D. Professor of Pediatrics and Internal Medicine Division of Allergy and Immunology Saint Louis
Panelists What is Eosinophilic Esophagitis, how is it treated, and will it go away? Bradley A. Becker, M.D. Professor of Pediatrics and Internal Medicine Division of Allergy and Immunology Saint Louis
Kids Like to Break the Rules: Gastrointestinal Pathology in Children
 Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Eosinophilic Esophagitis: Extraesophageal Manifestations
 Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Eosinophilic Esophagitis No Relevant Disclosures
 Eosinophilic Esophagitis No Relevant Disclosures Rabindra R Watson, MD Assistant Clinical Professor of Medicine Director, Career Development in Advanced Endoscopy Division of Digestive Diseases David Geffen
Eosinophilic Esophagitis No Relevant Disclosures Rabindra R Watson, MD Assistant Clinical Professor of Medicine Director, Career Development in Advanced Endoscopy Division of Digestive Diseases David Geffen
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1. January 06, 2012
 PATHOLOGY LAB #1. January 06, 2012") MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Complex EoE patients. EoE is complicated
 Complex EoE patients ACG Annual Meeting 10/17/2016 Evan S. Dellon, MD, MPH Center for Esophageal Diseases And Swallowing EoE is complicated Page 1 of 21 Overview 4 complex cases EoE non-response a diagnostic
Complex EoE patients ACG Annual Meeting 10/17/2016 Evan S. Dellon, MD, MPH Center for Esophageal Diseases And Swallowing EoE is complicated Page 1 of 21 Overview 4 complex cases EoE non-response a diagnostic
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, by Am. Coll. of Gastroenterology ISSN /02/$22.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
Barrett s s Dysplasia
 Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease
 GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL
 THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Eosinophilic Esophagitis in Children and Adults
 Journal of Pediatric Gastroenterology and Nutrition 37:S23 S28 November/December 2003 Lippincott Williams & Wilkins, Inc., Philadelphia Eosinophilic Esophagitis in Children and Adults Chris A. Liacouras
Journal of Pediatric Gastroenterology and Nutrition 37:S23 S28 November/December 2003 Lippincott Williams & Wilkins, Inc., Philadelphia Eosinophilic Esophagitis in Children and Adults Chris A. Liacouras
Premalignant lesions may expose to a promoting. factor & may be induced to undergo malignant. Carcinoma in situ displays the cytologic features of
 بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
MVST BOD & NST PART IB Thurs. 2 nd & Fri. 3 rd March 2017 Pathology Practical Class 23
 MVST BOD & NST PART IB Thurs. 2 nd & Fri. 3 rd March 2017 Pathology Practical Class 23 Neoplasia I Neoplasia I: Benign and malignant neoplasms in glandular epithelium and mesenchyme 1.0. Aims 1. To understand
MVST BOD & NST PART IB Thurs. 2 nd & Fri. 3 rd March 2017 Pathology Practical Class 23 Neoplasia I Neoplasia I: Benign and malignant neoplasms in glandular epithelium and mesenchyme 1.0. Aims 1. To understand
How I Handle Mast Cells in GI Biopsies
 How I Handle Mast Cells in GI Biopsies Dora Lam-Himlin, MD Rodger C. Haggitt Gastrointestinal Pathology Society Forum United States and Canadian Academy of Pathologists Seattle, Washington, March 12, 2016
How I Handle Mast Cells in GI Biopsies Dora Lam-Himlin, MD Rodger C. Haggitt Gastrointestinal Pathology Society Forum United States and Canadian Academy of Pathologists Seattle, Washington, March 12, 2016
Supplementary Methods: Omalizumab Trial This double-blind, randomized, placebo-controlled trial was conducted at the University of Utah Hospital and
 Supplementary Methods: Omalizumab Trial This double-blind, randomized, placebo-controlled trial was conducted at the University of Utah Hospital and Primary Children s Hospital, Salt Lake City, UT, both
Supplementary Methods: Omalizumab Trial This double-blind, randomized, placebo-controlled trial was conducted at the University of Utah Hospital and Primary Children s Hospital, Salt Lake City, UT, both
Chapter 12: Training in Pathology. DDSEP Chapter 13: Question 19
 DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance