Jejunostomy after oesophagectomy, how and why I do it
|
|
|
- Gwenda Horn
- 6 years ago
- Views:
Transcription
1 Jejunostomy after oesophagectomy, how and why I do it Graeme Couper. Consultant Oesophago-gastric Surgeon, The Royal Infirmary of Edinburgh BAPEN Conference nd & 3rd November Harrogate International Centre
2 Oesophageal Cancer. 8 th most common adult malignancy. Rapidly increasing incidence. Median survival 9 months. 5-year survival 10-15% following curative resection.
3 Number of Deaths. Deaths From Upper GI Malignancy in Scotland Between Oesophageal Male. Oesopageal Female Gastric Male Gastric Female Year
4 Changing pattern of Oesophageal Cancer. Study Period % Adenocarcinoma. Ellis % Applequist % Malik % Sons % Yang % Wang % Orringer %
5 Implications. More advanced stage at presentation. Younger population. Lower response rates than squamous cell carcinoma to neo-adjuvant/adjuvant treatment.
6 Pre-op. Peri-op. Post-op. Why nutritional support? Review of literature and unit experience in Edinburgh.
7 Personal results. 50 consecutive patients undergoing oesophagectomy. Notes available for minimally invasive. 27 Ivor Lewis. 35% (17/48) had pre op chemo.
8 Pre-operative concerns. Pre-operative chemotherapy. Based on OEO2 trial demonstrating survival advantage. 2-year 43% vs 34% 5-year 23% vs 17%
9 Weight. Weight changes during pre-operative chemotherapy
10 ESPEN guidelines on TPN. Braga et. al. Clin Nutrition Pre-op TPN in well-nourished or mildly undernourished patients is associated with either no benefit or with increased morbidity. Post-op nutrition should be via the enteral route or a combination of enteral and supplementary parenteral feeding in the first instance.
11 TPN vs Enteral nutrition. Moore et. al. Ann Surg Meta analysis of 8 trials comparing TPN and TEN. high-risk surgical patients have reduced septic morbidity rates with TEN compared with those receiving TPN
12 Pre-op nutrition. Gianotti et. al. Gastroenterology pts undergoing surgery for GI cancer randomised. Infections Hospital Stay Pre-op only 13% 11.6 days Pre + Peri-op 15.8% 12.2 days No Supplement. 30.4% 14.0 days
13 Newcastle Trial. 300 patients undergoing upper GI resection randomised to: A.Omega-3 fatty acid preparation. 7 days pre and post op. B. Standard feed. 7 days pre and post op. C. Standard post op feed. No difference in: morbidity mortality antibiotic usage hospital stay immune function

14
15 Pre-operative concerns. Presence of dysphagia. (23/48) 48% of patients dysphagia to solids. All are assessed at initial clinic by dietician. Those with weight loss or swallowing difficulties are prescribed oral supplements. None required fine-bore feeding. Few if any patients are admitted for surgery in a malnourished state.
16 Peri-operative. Does early post-operative feeding reduce morbidity and mortality?
17 Early post op nutrition. Heslin et. al. Ann Surg pts undergoing Upper GI surgery randomised to early post-op feeding with immune-enhancing formula or IV crystalloid. No difference in number of minor, major or infective complications. Not beneficial and should not be routine.
18 Early post op nutrition. Waters et. al. Ann Surg pts undergoing Upper GI surgery randomised to early post-op feeding or no feeding for 6 days. Feeding group had impaired respiratory mechanics and impaired post-op mobility. Immediate post-op enteral feeding should not be routine in well nourished patients at low risk of nutrition related complications.
19 Post operative. Main indications for nutritional support. Major Complication rate 30-66%. Long-term nutritional difficulties.
20 Weight Loss (Kg) Weight Change in Patients Undergoing Oesophagectomy Pre op 4 Weeks 6 Months
21 At 6 months only 8% of patients have regained their pre-operative weight.
22 Post op Complications. 23/48 (48%) patients had complication. 10 pneumonia. 5 anastomotic leak. 8 other.
23 Weight (Kg) Weight changes in patients with post-op complications Pre op 2 weeks 6months Time
24 Weight )Kg) Weight changes in patients without post-op complications Pre op 2 weeks 6months Time
25 Weight loss and Complications. Complication Group Average weight loss at 6 months postoesophagectomy 9.7Kg ( ) No Complication Group Average weight loss at 6 months postoesophagectomy 6.7Kg ( )
26 Weight loss and Survival. 34/48 (71%) of patients were alive and disease-free at 2 years. 13/14 (93%) had node positive disease. 10/14 (71%) had received pre-op chemo.
27 Weight(Kg) Weight Changes in Patients with Recurrent Disease within 24 months Pre op 2 weeks 6months Time
28 Weight(Kg) Weight Changes in Patients Without Recurrent Disease at 24 months Pre op 2 weeks 6months Time
29 Weight loss and Survival. Early Recurrence Group Average weight loss at 6 months postoesophagectomy 7.8Kg ( ) No Recurrence Group Average weight loss at 6 months postoesophagectomy 7.6Kg ( )
30 Why feeding jejunostomy? Alternatives. Fine-bore feeding. Uncomfortable. Blockage. Displacement. TPN. Expensive. Line complications. Unsuitable for home use.
31 Feeding jejunostomy in Oesophageal surgery. Reference Year Study design Patient No. Complication rate (%) Brandmair 1988 RCT Gerndt 1994 Retrospective Wakefield 1995 Retrospective Mercer 1996 RCT Yagi 1999 Retrospective 78 4 Date 2004 Retrospective Han-Geurts 2004 RCT Han-Geurts 2007 RCT
32 Post-op feeding. Length of feeding tube insertion. Patients with complications: Median 11.5 weeks (4-32 weeks): Patients without complications: Median 8 weeks (1-32 weeks).
33 Tube complications. 6/48 (12.5%) had minor complications. 4 fell out at 9 wks, 12 wks, 6 months and 7 months. 1 pulled out at 7 days. 1 infection at 4 weeks. No tube required replacement or reoperation.

34 Which feeding jejunostomy tube? Alternatives. T-tube. Large diameter. High leak rate. Difficult to unblock. Foley catheter. Large diameter. High leak rate. Difficult to unblock.
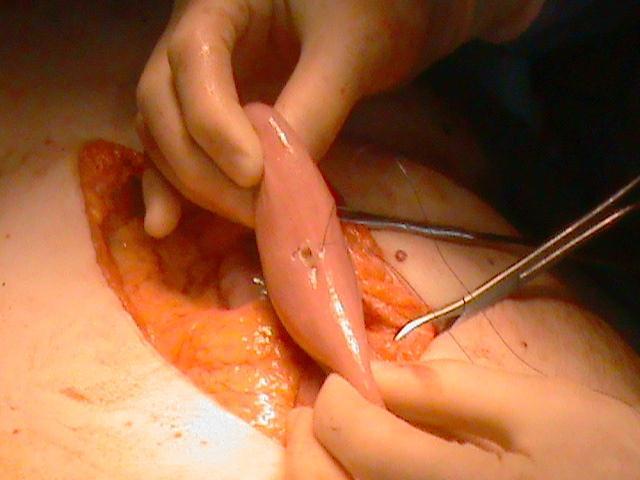
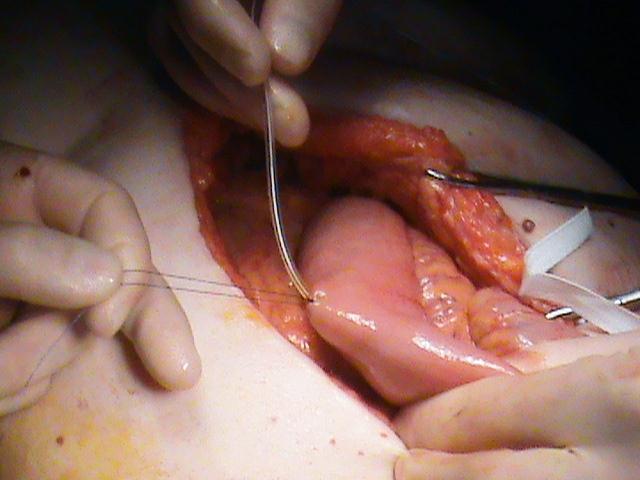
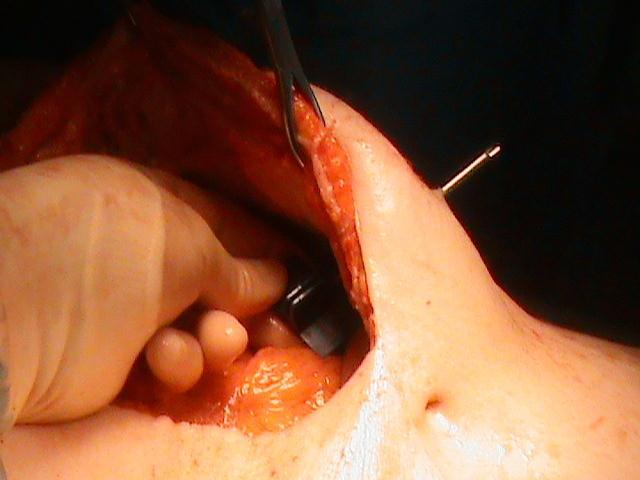
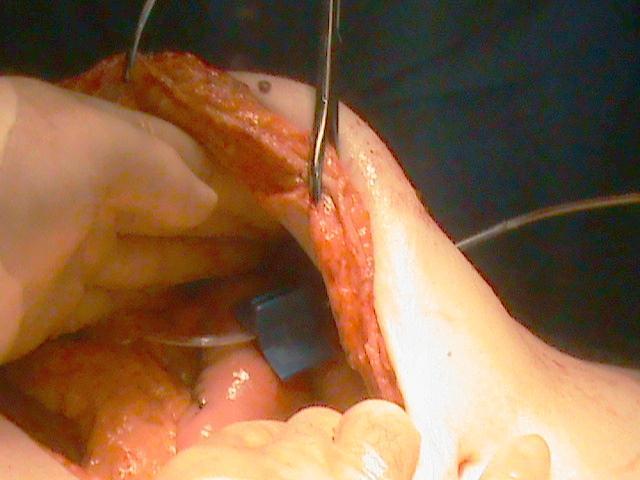
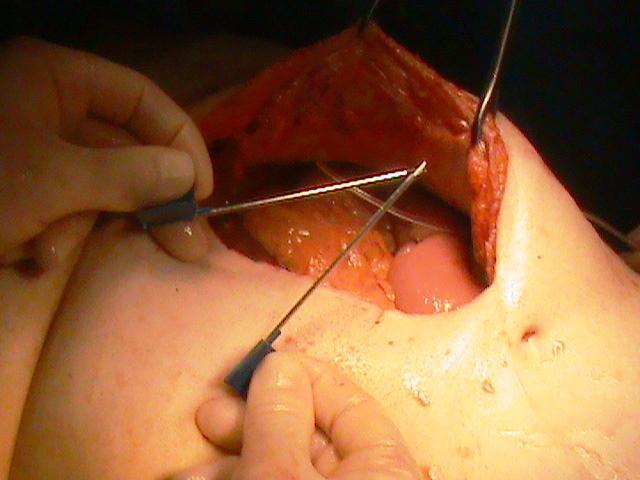
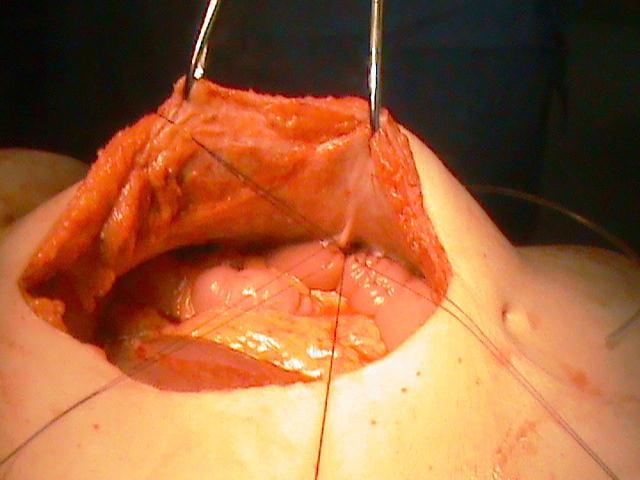
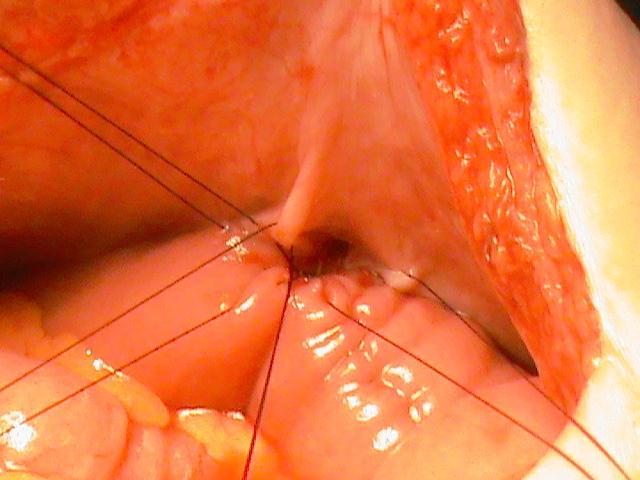
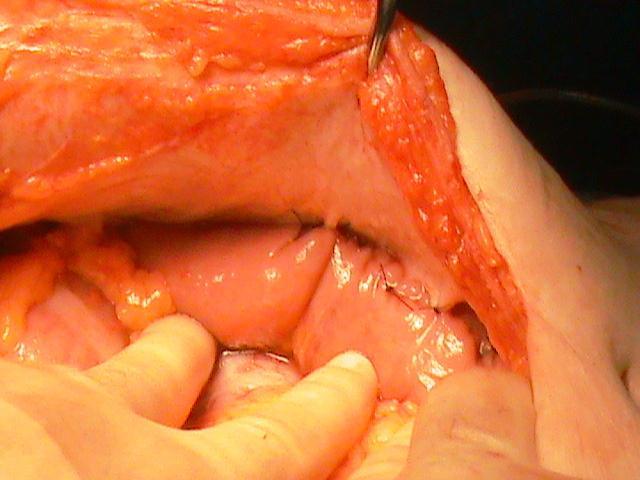
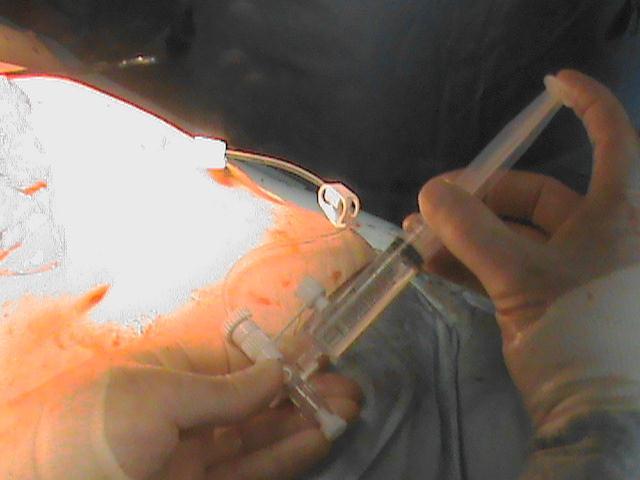
35 FREKA SURGICAL JEJUNOSTOMY SET Indications For early post-operative long-term intra-jejunal nutrition after laparotomy or laparoscopy. Contraindications Ileus Immune suppression Peritonitis Acute Abdomen Sepsis Ascites Blood clotting disorders Severe general wound healing disorders Peritoneal carcinoma Crohn s disease Ulcerative Colitis

36 FREKA SURGICAL JEJUNOSTOMY SET

37

38

39


40
41

42
43
44
45
46
47
48
49
50
51 Conclusions. All patients with oesophageal cancer need ongoing dietary assessment from time of diagnosis to discharge or death. The main indication for feeding is to maintain nutrition in patients with postoperative complications or those with prolonged poor oral intake. Feeding is best achieved using a Freka jejunostomy.
52
Nutritional Support in the Perioperative Period
 Nutritional Support in the Perioperative Period Topic 17 Module 17.3 Nutritional Support in the Perioperative Period Ken Fearon Learning Objectives Understand the principles behind nutritional care for
Nutritional Support in the Perioperative Period Topic 17 Module 17.3 Nutritional Support in the Perioperative Period Ken Fearon Learning Objectives Understand the principles behind nutritional care for
APPLYING ENHANCED RECOVERY PRINCIPLES: EARLY TESTING IN UPPER GI CANCER
 APPLYING ENHANCED RECOVERY PRINCIPLES: EARLY TESTING IN UPPER GI CANCER William Allum Consultant Surgeon, Royal Marsden NHS Foundation Trust ? POSSIBLE Major procedure Painful Anastomotic complications
APPLYING ENHANCED RECOVERY PRINCIPLES: EARLY TESTING IN UPPER GI CANCER William Allum Consultant Surgeon, Royal Marsden NHS Foundation Trust ? POSSIBLE Major procedure Painful Anastomotic complications
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
FTS Oesophagectomy: minimal research to date 3,4
 Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings?
 Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Stellenwert der prä- und postoperativen Sicht des Chirurgen
 Interdisziplinäre Chirurgie Stellenwert der prä- und postoperativen Ernährung Sicht des Chirurgen Kantonsspital Luzern 24.11.2005 Prof. L. Krähenbühl Chirurgische Klinik Hôpital Cantonal Fribourg Problems
Interdisziplinäre Chirurgie Stellenwert der prä- und postoperativen Ernährung Sicht des Chirurgen Kantonsspital Luzern 24.11.2005 Prof. L. Krähenbühl Chirurgische Klinik Hôpital Cantonal Fribourg Problems
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT
 BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor
 Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand?
 MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
ESPEN Congress Florence 2008
 ESPEN Congress Florence 2008 Interactive Case Discussion Nutrition multimodal support of an adult with oesophageal cancer Roberto Biffi (Italy) EUROPEAN INSTITUTE OF ONCOLOGY Nutrition multimodal support
ESPEN Congress Florence 2008 Interactive Case Discussion Nutrition multimodal support of an adult with oesophageal cancer Roberto Biffi (Italy) EUROPEAN INSTITUTE OF ONCOLOGY Nutrition multimodal support
DATA REPORT. August 2014
 AUDIT DATA REPORT August 2014 Prepared for the Australian and New Zealand Gastric and Oesophageal Surgical Association by the Royal Australasian College of Surgeons 199 Ward St, North Adelaide, SA 5006
AUDIT DATA REPORT August 2014 Prepared for the Australian and New Zealand Gastric and Oesophageal Surgical Association by the Royal Australasian College of Surgeons 199 Ward St, North Adelaide, SA 5006
Malnutrition: An independent Risk Factor for Postoperative Complications
 Malnutrition: An independent Risk Factor for Postoperative Complications Bryan P. Hooks, D.O. University of Pittsburgh-Horizon June 24, 2017 Orthopedic Surgeon-Adult Reconstruction Disclosures: None Objectives:
Malnutrition: An independent Risk Factor for Postoperative Complications Bryan P. Hooks, D.O. University of Pittsburgh-Horizon June 24, 2017 Orthopedic Surgeon-Adult Reconstruction Disclosures: None Objectives:
ESPEN Congress Copenhagen 2016
 ESPEN Congress Copenhagen 2016 ESPEN GUIDELINES SURGERY A. Weimann (DE) ESPEN Guideline Clinical Nutrition in Surgery Conflicts of interest Speaker `s honoraria: Baxter Germany Berlin Chemie B. Braun Melsungen
ESPEN Congress Copenhagen 2016 ESPEN GUIDELINES SURGERY A. Weimann (DE) ESPEN Guideline Clinical Nutrition in Surgery Conflicts of interest Speaker `s honoraria: Baxter Germany Berlin Chemie B. Braun Melsungen
Adult Trauma Feeding Access Guideline
 Adult Trauma Feeding Access Guideline Background: Enteral feeding access mode (NGT, NDT, PEG, PEG-J, Jejunostomy tube) dependent upon patient characteristics. Enteral feeding management guidelines aim
Adult Trauma Feeding Access Guideline Background: Enteral feeding access mode (NGT, NDT, PEG, PEG-J, Jejunostomy tube) dependent upon patient characteristics. Enteral feeding management guidelines aim
Nutritional intervention in hospitalised paediatric patients. Dr Y.K.Amdekar
 Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
NICE guideline Published: 24 January 2018 nice.org.uk/guidance/ng83
 Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
IMMUNONUTRITION AND GI SURGERY (UPPER AND LOWER) STUDIES COMPENDIUM
 STUDIES COMPENDIUM") IMMUNONUTRITION AND GI SURGERY (UPPER AND LOWER) Colorectal or gastric cancer Xu 2006 (WJS;30:1284-1289) RCT to determine the effect of preoperative immunonutrition on nutritional status, immunity, and
IMMUNONUTRITION AND GI SURGERY (UPPER AND LOWER) Colorectal or gastric cancer Xu 2006 (WJS;30:1284-1289) RCT to determine the effect of preoperative immunonutrition on nutritional status, immunity, and
Parenteral Nutrition in IBD: Any indication?
 Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
Minimally Invasive Esophagectomy
 Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil
 Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
ERAS. Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic
 ERAS Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic Outline Definition Justification Ileus Pain Outline Specifics Data BMC Data Worldwide Data Implementation What is ERAS? AKA Fast-track
ERAS Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic Outline Definition Justification Ileus Pain Outline Specifics Data BMC Data Worldwide Data Implementation What is ERAS? AKA Fast-track
The 1 st Oesophago gastric Cancer Centers Meeting for The Anglia Cancer Network
 The 1 st Oesophago gastric Cancer Centers Meeting for The Anglia Cancer Network Date: Sept 28 th 2012 Venue: The Bedford Lodge Hotel Attendees: NORFOLK & NORWICH Mr Ed Cheong (UGI Cancer Lead) Dr Ben Simpson
The 1 st Oesophago gastric Cancer Centers Meeting for The Anglia Cancer Network Date: Sept 28 th 2012 Venue: The Bedford Lodge Hotel Attendees: NORFOLK & NORWICH Mr Ed Cheong (UGI Cancer Lead) Dr Ben Simpson
How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective. Aravind Suppiah; Sarah K.
 How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective Aravind Suppiah; Sarah K. Thompson ANZGOSA database Commenced 2010; 1469 cases (2002 2014)
How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective Aravind Suppiah; Sarah K. Thompson ANZGOSA database Commenced 2010; 1469 cases (2002 2014)
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Diet what helps? Lindsey Allan Macmillan Oncology Dietitian Royal Surrey County Hospital, Guildford
 Diet what helps? Lindsey Allan Macmillan Oncology Dietitian Royal Surrey County Hospital, Guildford Diet and cancer Diet and cancer Nutrition research Lack of funding RCTs Low quality Small sample sizes
Diet what helps? Lindsey Allan Macmillan Oncology Dietitian Royal Surrey County Hospital, Guildford Diet and cancer Diet and cancer Nutrition research Lack of funding RCTs Low quality Small sample sizes
Subtotal and Total Gastrectomy
 DR ADEEB MAJID MBBS, MS, FRACS, ANZHPBA FELLOWSHIP GENERAL, HEPATOBILIARY AND PANCREATIC SURGEON CALVARY MATER HOSPITAL NEWCASTLE Information for patients and carers Subtotal and Total Gastrectomy Introduction
DR ADEEB MAJID MBBS, MS, FRACS, ANZHPBA FELLOWSHIP GENERAL, HEPATOBILIARY AND PANCREATIC SURGEON CALVARY MATER HOSPITAL NEWCASTLE Information for patients and carers Subtotal and Total Gastrectomy Introduction
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Nutrition Support. John Cha Department of Surgery DHMC/UCHSC
 Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
Home Enteral Nutrition: What happens after discharge? Niamh Maher Senior Dietitian HSE Dublin North East
 Home Enteral Nutrition: What happens after discharge? Niamh Maher Senior Dietitian HSE Dublin North East Nutrition Support Study Day April 25 th 2012 Home enteral nutrition (HEN) Enteral tube feeding is
Home Enteral Nutrition: What happens after discharge? Niamh Maher Senior Dietitian HSE Dublin North East Nutrition Support Study Day April 25 th 2012 Home enteral nutrition (HEN) Enteral tube feeding is
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers
 WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
Surgical strategies in esophageal cancer
 Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
ESPEN GUIDELINES. on clinical nutrition and hydration in geriatrics
 ESPEN GUIDELINES on clinical nutrition and hydration in geriatrics SUMMARY Malnutrition and dehydration are widespread in older people, and obesity is an increasing problem. A range of effective interventions
ESPEN GUIDELINES on clinical nutrition and hydration in geriatrics SUMMARY Malnutrition and dehydration are widespread in older people, and obesity is an increasing problem. A range of effective interventions
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Enhanced Recovery after Surgery - A Colorectal Perspective. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Enhanced Recovery after Surgery - A Colorectal Perspective R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus resolves Opioid
Enhanced Recovery after Surgery - A Colorectal Perspective R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus resolves Opioid
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
10/3/2012. Pediatric Parenteral Nutrition A Comprehensive Review
 Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SMALL BOWEL 7-Nov-2016 DEVELOPED BY: Graham Cullingford,
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SMALL BOWEL 7-Nov-2016 DEVELOPED BY: Graham Cullingford,
Paraoesophageal Hernia
 Paraoesophageal Hernia Grand Round Adam Cichowitz Surgical Registrar Paraoesophageal Hernia Type of hiatal hernia Transdiaphragmatic migration of abdominal content gastric fundus gastric body pylorus colon
Paraoesophageal Hernia Grand Round Adam Cichowitz Surgical Registrar Paraoesophageal Hernia Type of hiatal hernia Transdiaphragmatic migration of abdominal content gastric fundus gastric body pylorus colon
Wali R Johnson et. al. / International Journal of New Technologies in Science and Engineering Vol. 2, Issue 4, October 2015, ISSN
 Enteral Feeding via Percutaneous Endoscopic Gastrojejunostomy(PEGJ) Tubes Decreases Risk of Aspiration and Tube Dislodgement Related Complications Compared to PEGs. Wali R Johnson, MSIV, L Ray Matthews,
Enteral Feeding via Percutaneous Endoscopic Gastrojejunostomy(PEGJ) Tubes Decreases Risk of Aspiration and Tube Dislodgement Related Complications Compared to PEGs. Wali R Johnson, MSIV, L Ray Matthews,
ESPEN Congress Brussels Stenting of the esophagus and small bowel. Jean-Marc Dumonceau
 ESPEN Congress Brussels 2005 Stenting of the esophagus and small bowel Jean-Marc Dumonceau Stenting of the esophagus and small bowel Jean-Marc Dumonceau, Div. of Gastroenterology Geneva, Switzerland Indication:
ESPEN Congress Brussels 2005 Stenting of the esophagus and small bowel Jean-Marc Dumonceau Stenting of the esophagus and small bowel Jean-Marc Dumonceau, Div. of Gastroenterology Geneva, Switzerland Indication:
7/31/2015. Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice. Objectives. Enhanced Recovery Society
 Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice Margaret Odhner MS, ANP-BC, COCN Kim Meacham, MSN FNP-C, CWON Objectives 1. Describe the Enhanced Recover After Surgery (ERAS) pathway.
Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice Margaret Odhner MS, ANP-BC, COCN Kim Meacham, MSN FNP-C, CWON Objectives 1. Describe the Enhanced Recover After Surgery (ERAS) pathway.
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer
 Complex Thoracoscopic Resections for Locally Advanced Lung Cancer Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery,
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery,
Preoperative Biliary Drainage Among Patients With Resectable Hepatobiliary Malignancy: Does Technique Matter?
 Preoperative Biliary Drainage Among Patients With Resectable Hepatobiliary Malignancy: Does Technique Matter? Q. Lina Hu, MD; Jason B. Liu, MD, MS; Ryan J. Ellis, MD, MS; Jessica Y. Liu, MD, MS; Anthony
Preoperative Biliary Drainage Among Patients With Resectable Hepatobiliary Malignancy: Does Technique Matter? Q. Lina Hu, MD; Jason B. Liu, MD, MS; Ryan J. Ellis, MD, MS; Jessica Y. Liu, MD, MS; Anthony
OESOPHAGO-GASTRIC CANCER 2016
 SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT OESOPHAGO-GASTRIC CANCER 2016 COMPARATIVE AUDIT REPORT Mr Peter Lamb SCAN Lead Upper GI Cancer Clinician Dr Jonathan Fletcher, Consultant Physician,
SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT OESOPHAGO-GASTRIC CANCER 2016 COMPARATIVE AUDIT REPORT Mr Peter Lamb SCAN Lead Upper GI Cancer Clinician Dr Jonathan Fletcher, Consultant Physician,
Complication of Percutaneous Endoscopic Gastrostomy
 Complication of Percutaneous Endoscopic Gastrostomy Tube Ogori N. Kalu MD Morbidity & Mortality Conference General Surgery Service Kings County Hospital Center ACGME Core Competencies 1. Medical knowledge
Complication of Percutaneous Endoscopic Gastrostomy Tube Ogori N. Kalu MD Morbidity & Mortality Conference General Surgery Service Kings County Hospital Center ACGME Core Competencies 1. Medical knowledge
Definition and Types of Intestinal Failure
 Definition and Types of Intestinal Failure Jeremy Nightingale Consultant Gastroenterologist St Mark s Hospital Intestinal Failure - Definitions Reduction in functioning gut mass below the minimum amount
Definition and Types of Intestinal Failure Jeremy Nightingale Consultant Gastroenterologist St Mark s Hospital Intestinal Failure - Definitions Reduction in functioning gut mass below the minimum amount
Nutritional Issues. Perioperative Nutritional Interventions. A challenging case you are likely familiar with
 Perioperative Nutritional Interventions Lygia Stewart MD, John Maa MD, and Annette Romani RD UCSF Post-Graduate Course Nutritional Issues Who needs nutritional supplementation? Oral, feeding tube, or TPN?
Perioperative Nutritional Interventions Lygia Stewart MD, John Maa MD, and Annette Romani RD UCSF Post-Graduate Course Nutritional Issues Who needs nutritional supplementation? Oral, feeding tube, or TPN?
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
Postoperative complications and weight loss following jejunostomy tube feeding after total gastrectomy for advanced adenocarcinomas
 Original Article Postoperative complications and weight loss following jejunostomy tube feeding after total gastrectomy for advanced adenocarcinomas Hylke J.F. Brenkman 1, Stéphanie V.S. Roelen 1, Elles
Original Article Postoperative complications and weight loss following jejunostomy tube feeding after total gastrectomy for advanced adenocarcinomas Hylke J.F. Brenkman 1, Stéphanie V.S. Roelen 1, Elles
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Laparoscopic Colorectal Surgery
 Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Total Parenteral Nutrition and Enteral Nutrition in the Home. Original Policy Date 12:2013
 MP 1.02.01 Total Parenteral Nutrition and Enteral Nutrition in the Home Medical Policy Section Durable Medical Equipment Issue Original Policy Date Last Review Status/Date Return to Medical Policy Index
MP 1.02.01 Total Parenteral Nutrition and Enteral Nutrition in the Home Medical Policy Section Durable Medical Equipment Issue Original Policy Date Last Review Status/Date Return to Medical Policy Index
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness
 Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
A video demonstration of the Li s anastomosis the key part of the non-tube no fasting fast track program for resectable esophageal carcinoma
 Surgical Technique A video demonstration of the the key part of the non-tube no fasting fast track program for resectable esophageal carcinoma Yan Zheng*, Yin Li*, Zongfei Wang, Haibo Sun, Ruixiang Zhang
Surgical Technique A video demonstration of the the key part of the non-tube no fasting fast track program for resectable esophageal carcinoma Yan Zheng*, Yin Li*, Zongfei Wang, Haibo Sun, Ruixiang Zhang
Providing Optimal Nutritional Support on the ICU common problems and practical solutions. Pete Turner Specialist Nutritional Support Dietitian
 Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
ESOPHAGEAL CANCER. Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds
 ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery
 Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery Zhobin Moghadamyeghaneh MD 1, Michael J. Stamos MD 1 1 Department of Surgery, University of California, Irvine Nothing to
Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery Zhobin Moghadamyeghaneh MD 1, Michael J. Stamos MD 1 1 Department of Surgery, University of California, Irvine Nothing to
A 16 yr old boy with aggressive ca esophagus. DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health
 A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
Short and longterm outcomes after endoscopic resection of malignant polyps.
 Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Dr Candice Silverman MBBS (HONS) FRACS General & Laparoscopic Surgeon
 FRACS General & Laparoscopic Surgeon") Dr Candice Silverman MBBS (HONS) FRACS General & Laparoscopic Surgeon Core Specialist Group Suite 5G, John Flynn Medical Centre 42 Inland Drive TUGUN QLD 4224 Tel: 07 5598 0955 Write questions or notes
Dr Candice Silverman MBBS (HONS) FRACS General & Laparoscopic Surgeon Core Specialist Group Suite 5G, John Flynn Medical Centre 42 Inland Drive TUGUN QLD 4224 Tel: 07 5598 0955 Write questions or notes
Critical illness or major surgery usually results in
 : Improving Outcomes in Multiple Trauma and Gastrointestinal Cancer Resection Rex O. Brown, PharmD, FCCP, BCNSP ABSTRACT Immune-enhancing diets are nutritionally complete enteral nutrition formulations
: Improving Outcomes in Multiple Trauma and Gastrointestinal Cancer Resection Rex O. Brown, PharmD, FCCP, BCNSP ABSTRACT Immune-enhancing diets are nutritionally complete enteral nutrition formulations
Early Postoperative 24-Hour Continuous Jejunostomy Feeding in Esophagectomy Patients
 Case Report Clin Nutr Res 2014;3:69-73 pissn 2287-3732 eissn 2287-3740 Early Postoperative 24-Hour Continuous Jejunostomy Feeding in Esophagectomy Patients Jeong Hyun Lim 1, Dal Lae Ju 1, Yoohwa Hwang
Case Report Clin Nutr Res 2014;3:69-73 pissn 2287-3732 eissn 2287-3740 Early Postoperative 24-Hour Continuous Jejunostomy Feeding in Esophagectomy Patients Jeong Hyun Lim 1, Dal Lae Ju 1, Yoohwa Hwang
Cost Benefit Analysis of T Tube Feeding Jejunostomy
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 11 Ver. IV (November. 2016), PP 23-27 www.iosrjournals.org Cost Benefit Analysis of T Tube
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 11 Ver. IV (November. 2016), PP 23-27 www.iosrjournals.org Cost Benefit Analysis of T Tube
Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs.
 Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern
Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
General introduction and outline of thesis
 General introduction and outline of thesis General introduction and outline of thesis 11 GENERAL INTRODUCTION AND OUTLINE OF THESIS The incidence of esophageal cancer is increasing in the western world.
General introduction and outline of thesis General introduction and outline of thesis 11 GENERAL INTRODUCTION AND OUTLINE OF THESIS The incidence of esophageal cancer is increasing in the western world.
Early enteral nutrition in the major trauma patient requiring intensive care: An overview of the evidence.
 Early enteral nutrition in the major trauma patient requiring intensive care: An overview of the evidence. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern Clinical School Intensive Care
Early enteral nutrition in the major trauma patient requiring intensive care: An overview of the evidence. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern Clinical School Intensive Care
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
DGEM Guidelines Enteral Nutrition
 ESPEN Congress Cannes 2003 Organised by the Israel Society for Clinical Nutrition Education and Clinical Practice Programme Session: Nutritional Guidelines: ESPEN and other Societies German Society of
ESPEN Congress Cannes 2003 Organised by the Israel Society for Clinical Nutrition Education and Clinical Practice Programme Session: Nutritional Guidelines: ESPEN and other Societies German Society of
Appropriateness of the Use of Parenteral Nutrition in a Local Tertiary-Care Hospital
 494 Original Article Appropriateness of the Use of Parenteral Nutrition in a Local Tertiary-Care Hospital SL Chan, 1 BSc (Pharm), W Luman, 2 MB ChB, MD, FRCP Abstract Introduction: Parenteral nutrition
494 Original Article Appropriateness of the Use of Parenteral Nutrition in a Local Tertiary-Care Hospital SL Chan, 1 BSc (Pharm), W Luman, 2 MB ChB, MD, FRCP Abstract Introduction: Parenteral nutrition
Lymph node audit on Ivor-Lewis Oesophagogastrectomy specimens - November 2013 to October 2014.
 Lymph node audit on Ivor-Lewis Oesophagogastrectomy specimens - November 2013 to October 2014. Paul Malcolm, Speciality Doctor, Department of Cellular and Anatomical Pathology, Derriford Hospital, Plymouth.
Lymph node audit on Ivor-Lewis Oesophagogastrectomy specimens - November 2013 to October 2014. Paul Malcolm, Speciality Doctor, Department of Cellular and Anatomical Pathology, Derriford Hospital, Plymouth.
Operational Efficiency in Colon Surgery Enhanced Recovery Pathways: 23 hour laparoscopic colectomy
 Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
The impact of adhesions on operations and postoperative recovery in colon cancer surgery
 The American Journal of Surgery (2013) -, - - The impact of adhesions on operations and postoperative recovery in colon cancer surgery Ramzi Amri, M.Sc., Hannah C. den Boon, B.Sc., Liliana G. Bordeianou,
The American Journal of Surgery (2013) -, - - The impact of adhesions on operations and postoperative recovery in colon cancer surgery Ramzi Amri, M.Sc., Hannah C. den Boon, B.Sc., Liliana G. Bordeianou,
Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic Surgery for Colorectal Disease
 ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
T3 NSCLC: Chest Wall, Diaphragm, Mediastinum
 for T3 NSCLC: Chest Wall, Diaphragm, Mediastinum AATS Postgraduate Course April 29, 2012 Thomas A. D Amico MD Professor of Surgery, Chief of Thoracic Surgery Duke University Health System Disclosure No
for T3 NSCLC: Chest Wall, Diaphragm, Mediastinum AATS Postgraduate Course April 29, 2012 Thomas A. D Amico MD Professor of Surgery, Chief of Thoracic Surgery Duke University Health System Disclosure No
Stage 1 esophageal cancer survival rate
 Stage 1 esophageal cancer survival rate Search Below are the five-year survival rates for esophageal cancer patients treated by SCCA compared to patients who were treated for esophageal. Stage I Esophageal
Stage 1 esophageal cancer survival rate Search Below are the five-year survival rates for esophageal cancer patients treated by SCCA compared to patients who were treated for esophageal. Stage I Esophageal
The CREST Trial. Funded by Cancer Research UK and developed by the National Cancer Research Institute
 The CREST Trial A randomised phase III study of stenting as a bridge to surgery in obstructing colorectal cancer. Results of the UK ColoRectal Endoscopic Stenting Trial (CREST). Funded by Cancer Research
The CREST Trial A randomised phase III study of stenting as a bridge to surgery in obstructing colorectal cancer. Results of the UK ColoRectal Endoscopic Stenting Trial (CREST). Funded by Cancer Research
Nutrition care plan for surgical patients. Objectives
 Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
ANICOLAU.RO. Enhanced Recovery after Colorectal Surgery. Irina Grecu, Alexandru E. Nicolau, Olle Ljungqvist*
 Enhanced Recovery after Colorectal Surgery Irina Grecu, Alexandru E. Nicolau, Olle Ljungqvist* Clinical Emergency Hospital of Bucharest, Romania *Karolinska Institute, Stockholm, Sweden ERAS - Enhanced
Enhanced Recovery after Colorectal Surgery Irina Grecu, Alexandru E. Nicolau, Olle Ljungqvist* Clinical Emergency Hospital of Bucharest, Romania *Karolinska Institute, Stockholm, Sweden ERAS - Enhanced
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies
 Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Advances in Bioscience and Clinical Medicine ISSN:
 Advances in Bioscience and Clinical Medicine ISSN: 2203-1413 www.abcmed.aiac.org.au Original Paper Comparison between the Effects of Early and Late Nourishing by Jejunal Feeding in Patients with Esophageal
Advances in Bioscience and Clinical Medicine ISSN: 2203-1413 www.abcmed.aiac.org.au Original Paper Comparison between the Effects of Early and Late Nourishing by Jejunal Feeding in Patients with Esophageal
Case discussion. Anastomotic leakage. intern superviser
 Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Multimodality therapy for esophageal cancer: should nutritional support be included? Federico Bozzetti. ESMO SYMPOSIUM Zurich March 2009
 Multimodality therapy for esophageal cancer: should nutritional support be included? Federico Bozzetti ESMO SYMPOSIUM Zurich 20-21 March 2009 TOPICS Nutritional status: obesity and weight loss (WL) Metabolic
Multimodality therapy for esophageal cancer: should nutritional support be included? Federico Bozzetti ESMO SYMPOSIUM Zurich 20-21 March 2009 TOPICS Nutritional status: obesity and weight loss (WL) Metabolic
Enteral Feeding Access: Your BFF or Frenemy?
 Enteral Feeding Access: Your BFF or Frenemy? Elizabeth Hood, APN/CPNP The Ann and Robert H. Lurie Children s Hospital of Chicago Chicago, IL Disclosure Information No disclosures to report Objectives The
Enteral Feeding Access: Your BFF or Frenemy? Elizabeth Hood, APN/CPNP The Ann and Robert H. Lurie Children s Hospital of Chicago Chicago, IL Disclosure Information No disclosures to report Objectives The
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies
 HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
Having a Sleeve Gastrectomy
 University Teaching Trust Having a Sleeve Gastrectomy Hope Building Upper G.I. / Bariatrics 0161 206 5062 All Rights Reserved 2016. Document for issue as handout. This booklet aims to describe: l What
University Teaching Trust Having a Sleeve Gastrectomy Hope Building Upper G.I. / Bariatrics 0161 206 5062 All Rights Reserved 2016. Document for issue as handout. This booklet aims to describe: l What
[No conflicts of interest]
![[No conflicts of interest]](/thumbs/86/94144068.jpg "[No conflicts of interest]") [No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
[No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme