Immunohistochemistry in prostate pathology: Recent Advances
|
|
|
- Eugene Tate
- 5 years ago
- Views:
Transcription
1 Immunohistochemistry in prostate pathology: Recent Advances Jae Y. Ro, M.D., Ph.D. Weill Medical College of Cornell University, Methodist Hospital, and UT MD Anderson Cancer Center, Houston, TX Yonsei and Ewha University College of Medicine, Seoul, Korea November 9, 2013


2 Do your BeST! November 9, 2013
3 Do your BeST! B represents Basic. e (effort) S represents Study. T represents Think. E represents Enjoy.
4 1) Basic 2) Study 3) Think 4) Enjoy Contents
5 1. Basic Prostate anatomy Prostate histology Immunohistochemistry Your limitation Get second opinion (Consultation. Communication and Collaboration)

6

7
8 Disease of Prostate P. Zone (70%) T. Zone (5-10) C. Zone (20) CA (70%) CA (25%) CA (<5%) PIN BPH AAH BCH CCCH SA
9
10
11
12

13
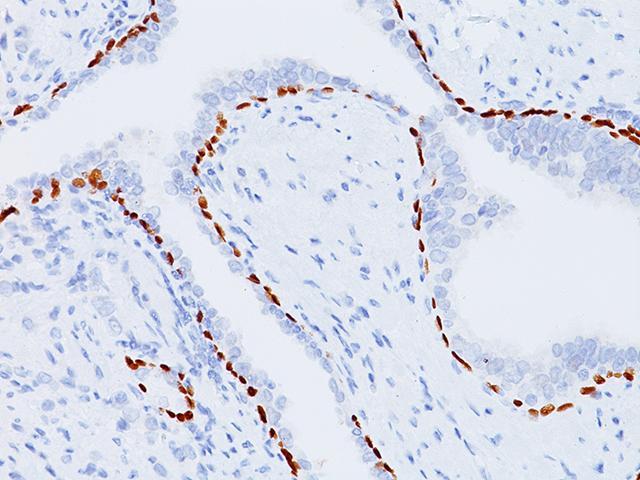
14 Basal cell markers P63 cancer cells aberrantly +: AJSP 2008;32: High molecular cytokeratin (34βE12) cancer cells aberrantly +: AJSP 2008;32: CK5/6 P63 combined with 34βE12 or CK5/6

15

16
17 Markers for Prostate Cancer Alpha-methyl-CoA-Recemase (AMACR) ERG (TMPRSS2-ERG fusion) Cocktailes of AMACR and Basal cell markers AMACR + P63 AMACR +HMWCK + p63 (PIN4) Other markers PAX2 and PAX8/MUC6 (Seminal vesicle) Ki-67 (MIB-1) NKX3.1, human glandular kallikrein 2 (hk2), propsa, Ep-CAM, Ataxia-telangiectasia Mutated

18

19 PIN4 cocktail (AMACR, P63, HMCK)

20 Erg

21

22
23 2. Study Immunohistochemistry Prostate cancer Cancer mimickers ASAP Intraductal cribriform lesions DD between prostate cancer vs. non-prostate cancer Prognosis/predictive markers



24


25 You have to look for 3 things! In any specimens Small glands Medium/Large glands with atypia Stromal abnormalities

26

27

28
29 Diagnostic Approach Lesions Small glands Cytologic change Stromal change PIN vs. Intraductal ca other? Infl Stromal lesion carcinoma Ca. mimickers

30
31 Prostate Carcinoma Well-diff. and poorly diff. adenocarcinoma well-diff. adenocarcinoma - For screening: three Too s (too small, too crowded, and too clear) - For confirmation: nuclear enlargement, prominent nucleoli and lack of basal cells poorly diff. adenoca - Uniformity, p. nucleolus, no or low mitoses


32

33

34

35

36

37

38

39 PIN4: p63+hmck+amacr


40

41 Erg

42 P63 expression in prostate ca. Am J Surg Pathol 2013;37: However, HMWCK negative

43
44 Cancer Mimickers Small gland pattern Large and cribriform pattern Solid and non-glandular pattern
45
46

47

48


49

50

51

52

53

54 HMWCK

55 P63

56 SMA
57 SA vs. carcinoma SA Carcinoma Stroma Cellular No stromal reaction Spindle Desmoplasia Basal cells + - Thick BM + - P. nucleoli -/+ + Cryst/mucin +/- + Borders Circum Infiltrative Location TZ PZ
58 Other small glands Normal structures and metaplasia Seminal vesicles/ejaculatory ducts, Cowper s glands, Atrophy Basal cell hyperplasia Clear cell cribriform hyperplasia Nephrogenic adenoma Mesonephric hyperplasia Verumontanum mucosal gland hyperplasia

59


60 MUC6

61 PAX8

62

63

64
65


66

67

68

69


70


71
72 Prostate Ca and Mimickers Pca SV NA Others PSA, PAP, PSMA + - CD AR + + ER, PR -/+ - AMACR + - Erg + - HMCK, CK5/6, p PAX2, PAX /+ -/ /

73



74

75 Idiopathic granulomatous prostatitis
76 Atypical small acinar proliferation (ASAP) Size: 1) small number of acini in focus of concern 2) small focus size, average 0.4 mm in greatest dimension 3) lesion breakage at core tip Histology: 1) lack of clear histologic detail 2) distortion of acini 3) lack of convincing malignant features 4) clustered growth pattern mimicking benign process such as AAH or atrophy 5) loss of the focus of concern in deeper 6) focal positive HMWCK or negative racemase 7) presence of PIN raising the possibility of tangential cutting Inflammation: 1) overdiagnosis of reactive changes or atrophy 2) reactive atypia with nuclear and nucleolar enlargement

77

78

79

80

81

82

83

84

85

86 AMACR expression in ASAP c > s cancer; USCAP abstract 2011, #982
 in ASAP USCAP")
87 TMPRSS2:ERG fusion (erg immunostain) in ASAP USCAP abstract 2011, #826
88 ASAP ASAP is a valid diagnostic category Clinical significance: predictive value for cancer on repeat biopsy ASAP predicts cancer : 34% to 60% Repeat biopsy and close clinical follow up

89
90 Precancerous Lesions PIN: Architecturally normal, but cytologically abnormal AAH: Architecturally abnormal, but cytologically normal

91

92

93

94

95
96 Diagnostic Criteria of PIN Low-grade High-Grade PIN (PIN 1) (PIN 2 & 3) Patterns Crowding, More Changes, stratification, 4 patterns T, MP, irregular spacing crib, flat Nuclei Sl. enlarged, Enlarged, less size variation size variation Chromatin Normal Increased Nucleoli Rarely Occ. to freq. prominent prominent

97

98 Architectural patterns of PIN: Bostwick and Amin Hum Pathol 24:298, 1993

99

100

101
102 Intraductal carcinoma

103

104

105

106

107
108 Intraductal carcinoma (IDC-P) McNeal & Yemoto, AJSP 1996;20:802 Guo and Epstein, 2006, Mod Pathol 19:1528 Epithelial cells filling large ducts/acinar with preservation of basal cells 1) Solid or dense cribriform pattern 2) Loose cribriform or micropapillary with marked cellular atypia (6 normal or larger) or presence of comedonecrosis Shah et al, 2010, AJSP, 34:470 (ACLs) > 6 glands with cribriform hyperplastic epithelium with pleomorphic nuclei, nucleomegaly and complex architecture (necrosis, solid architecture, or branching): > 1mm

109
110 Atypical cribriform lesions

111

112

113 IDC-P

114 IDC-P, solid pattern

115 IDC-P, micropapillary & necrosis
116 Intraductal Carcinoma Ductal spread of high grade cancer? May be a possible lesion?
117 Our data (not published yet) Of 901 radical prostatectomy specimens ( ) 141 regular type IDC-P cases and 14 precursor-like IDC-P cases (3 IDC-P without coexisting invasive cancer and 11 predominant IDC-P with foci of invasive carcinoma) at least a subset of IDC-P precursor lesion of invasive carcinoma.
118
119
120 Prostatic Duct Ca with Endometrioid Features First described in 1967 by Melicow and Pachter Because of histologic similarity to endometrial ca, reported that it originated from Mullerian remnant (prostatic utricle) Estrogen Rx or orchiectomy was considered contraindicated Melicow and Tannenbaum reported 6 pts. All stage B, no orchiectomy, no hormone: survival excellent in 3 pts (less than 1 year follow-up)
121 Prostatic Duct Ca with Endometrioid Features Zaloudek et al: PAP positivity in tumor cells; tumor cells resemble prostate than endometrial carcinoma by EM Young and Lagios: orchiectomy produced tumor regression and clinical improvement Bostwick et al (13 cases), Epstein et al (10 cases) and Ro et al (35 cases) Those studies demonstrated that this tumor is prostatic origin and behavior is more aggressive than previously thought
122 Prostatic Duct Carcinoma Clinical presentation is similar to usual prostatic adenocarcinoma May be exophytic into urethra producing a papillary lesion visible cystoscopically May present earlier with hematuria or obstruction and can be diagnosed in TURP specimen Have lower levels of serum PSA elevation than usual adenocarcinoma Metastatic pattern is similar to usual prostatic adenocarcinoma
123 Prostatic Duct Carcinoma Exuberant papillary pattern (type A) Predominantly intraductal component (type B) Types A and B coexist in half of cases Single to stratified tall columnar epithelium Tumor cell have basally located nuclei, prominent nucleoli and abundant eosinophilic cytoplasm

124

125

126

127

128

129
130 Prostatic Duct Carcinoma Association with microacinar ca in half of cases Grade of microacinar ca is generally low grade: Gleason s score 6 PSA and PAP positive: CEA may be positive (CK 20 may be positive) Electron microscopy: prostatic secretory cells with no endometrial feature

131
132 Prostatic Duct Carcinoma Treatment & Prognosis: Radical prostatectomy, hormone, castration and/or radiation Hormonal response: unpredictable 5 year survival rate: 30% Median survival time: 46.3%
133 Prostatic Duct Carcinoma Christensen et al studies in radical prostatectomy (15 cases) - clinical stage B Compared c acinar ca of similar stage Ductal ca were larger and occupied larger portion of the glands Advanced final pathologic stage and higher short-term failure than acinar ca
134 Prostatic Duct Carcinoma Differential diagnosis PDC Cribriform ca PIN Cell type Columnar Cuboidal Columnar Stratified Maturation Lumina Slit-like Punched-out Complex round lumina Fibrovas core Comedo Nec Periurethral/TZ + -/+ -/+ TURP + -/+ -/+

135

136

137
138 Prostatic Duct Carcinoma McNeal et al raised question on the entity of ductal carcinoma: may be ductal spread of acinar ca Grade matched ductal ca and acinar ca demonstrated higher mitotic no. and proliferative activity in ductal ca
139 Prostatic Duct Carcinoma Summary: Patients frequently presented with obstruction/hematuria Carcinoma of ductal origin Role of hormone/orchiectomy is still uncertain Its biologic behavior is more aggressive than previously thought
140 PIN-like (Intraductal-like) Prostatic Duct Carcinoma Hammed and Humphrey: Mod Pathol(2006) 19, Tavora and Epstein: Am J Surg Pathol (2008)32, PIN-like prostatic ductal carcinoma Variant? Need more studies
141 PIN-like prostatic Duct Carcinoma Gleason pattern 3 No basal cells, AMACR freq + 6 of 9 RP cases associated with GS 6 carcinoma and small volume tumor up to 1.2 cm3 Only one had EPE DD from HGPIN and conventional ductal carcinoma


142
143 Large Cribriform Gland Lesions Lesions No cytologic atypia Cytologic atypia Basal cells + _ CCCH PIN vs. Intraductal ca*** Ductal-endometrioid ***: > 6 glands, > 1mm, branching contour, dense cribriform/solid, comedonecrosis, pleomorphism

144

145

146

147

148

149


150

151

152
153 High grade prostatic carcinoma vs. Non-prostatic carcinoma Prostate Non-prostate N. monotony + - Nucleolus prominent variable Mitoses rare frequent




154

155 SL

156

157

158
159 High grade Undiff Ca prostate urothelial PSA/PAP/PSMA + - AMACR/NKX HMCK -/+ (6-10%) + Uroplakin - + (65-100%) Thrombomodulin - + (49-69%) P63 -/+ (-18%) + (70-75%) CD57 + -/+ (- 17%) S100p - + (78-86%) GATA - + (67%)

160 PSA P501S PSMA

161 NKX3.1. ppsa Am J Surg Pathol 2007;31:

162 PSA P501S PSMA NKA3.1


163 HMCK P63 Throm


164 S100P Am J Surg Pathol 2007;31:

165 AJSP 2012;36: UC Pca UC GATA Throm Uroplakin
166 3. Think Diagnostic accuracy Prognostic/predictive factors Stage Grade (Gleason score) Non-anatomic factors (e.g., PSA) Keep 3 Cs practice (communication, consultation, collaboration)
167 3. Think! Prognostic factors - Category I (well supported): ptnm stage, Gleason grade, margin status (serum PSA) - Category II (extensively studied but not well established): volume (intraglandular extent), tumor subtype - Category III (currently studying): vascular invasion, perineural invasion

168
169 Other prognostic markers The Ki-67 cell proliferation index p53 bcl-2 immunostaining Anti-PSMA and p27 Erg immunostaining INPP4B, and PTEN genes Claudin-4 and claudin-5 DNA ploidy analysis


170 Anti- PSMA Anti- PSMA mrna Am J Clin Pathol 2003;120(Suppl 1):S85-S100

171 p27 Am J Clin Pathol 2003;120(Suppl 1):S85-S100

172 Erg stain Int Urol Nephrol 2013;45:
173 Br J Cancer February 16; 102(4):
174 Cancer Res January 15; 71(2): inositol polyphosphate 4-phosphatase type II (INPP4B) Phosphatase and tensin homolog (PTEN)
175 Prostate Cancer TX T0 T1 clinically inapparent tumor (not palpable, not visible) T1a < 5% of tissue resected; T1b > 5% T1c tumor identified by needle biopsy (elevated PSA) T2 Tumor confined within prostate T2a involve ½ of one lobe or less T2b more than ½ of one lobe T2c both lobes T3 tumor extends through capsule, T3a extracapsular, bladder neck extension (uni, bilateral) T3b tumor invades seminal vesicle (s) T4 Rectum, ext sphincter, levator muscle, pelvic wall No pathologic T1 classification
176 Regional Lymph Nodes (N) pnx pn0 pn1 Regional nodes not sampled No positive regional nodes Metastases in regional node(s) Distant Metastasis (M) MX No more MX in 7 th edition (AJCC, 2009) M0 No distant metastasis M1 Distant metastasis M1a Non-regional lymph node(s) M1b Bone(s) M1c Other site(s) with or without bone disease
177 Anatomic stage/prognostic groups Group 1 Group IIA T1a-c T2a T1-2a T1a-c T1a-c T2a T2b T2b Group IIB T2c T1-2 T1-2 N0 N0 N0 N0 N0 N0 N0 N0 N0 N0 N0 Group III T3a-b N0 Group IV T4 Any T Any T N0 N1 Any N M0 PSA<10 M0 PSA<10 M) PSA X M0 PSA<20 M0 PSA<20 M0 PSA<20 M0 PSA<20 M0 PSA X M0 any PSA M0 PSA>20 M0 any PSA G< 6 G< 6 G X G7 G< 6 G< 7 G< 7 G X Any G Any G G>8 M0 any PSA Any G M0 any PSA Any G M0 any PSA Any G M1 any PSA Any G


178 Original, 1977 Revision, 2005 New Revision, 2010,2011, cribriform, 4 or 5
179 4. Enjoy Joy and Fun Enjoy what you are doing!




180
181 Take Home Message Basic: Study: Diagnosis DD between prostate vs. non-prostate Prognosis/predictive markers Think: how to report pathologic findings, prognostic factors (stage and grade, PSA) Enjoy: joy and fun

182 Thank you for your attention! Urological pathologists
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA
 PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
Pathology of the Prostate. PathoBasic Tatjana Vlajnic
 Pathology of the Prostate PathoBasic 24.01.17 Tatjana Vlajnic Overview Adenocarcinoma of the prostate Grading Special variants Mimickers of prostate adenocarcinoma Atrophy Inflammatory conditions Granulomatous
Pathology of the Prostate PathoBasic 24.01.17 Tatjana Vlajnic Overview Adenocarcinoma of the prostate Grading Special variants Mimickers of prostate adenocarcinoma Atrophy Inflammatory conditions Granulomatous
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
Macro- and microacinar proliferations of the prostate
 Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
3/23/2017. Significant Changes in Prostate Cancer Classification, Grading, Staging and Reporting. Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Prostatic ductal adenocarcinoma is a subtype of
 ORIGINAL ARTICLE High-grade Prostatic Intraepithelial Neoplasialike Ductal Adenocarcinoma of the Prostate: A Clinicopathologic Study of 28 Cases Fabio Tavora, MD* and Jonathan I. Epstein, MD*w z Abstract:
ORIGINAL ARTICLE High-grade Prostatic Intraepithelial Neoplasialike Ductal Adenocarcinoma of the Prostate: A Clinicopathologic Study of 28 Cases Fabio Tavora, MD* and Jonathan I. Epstein, MD*w z Abstract:
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
5/21/2018. Difficulty in Underdiagnosing Prostate Cancer. Diagnosis of Prostate Cancer. Evaluation of Prostate Cancer and Atypical on Needle Biopsy
 Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE. Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT
 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
Diagnosis, pathology and prognosis including variant pathology
 PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA
 Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA Learners Objectives u Latest changes per ISUP 2014 that impact
Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA Learners Objectives u Latest changes per ISUP 2014 that impact
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Some prostatic diseases
 Some prostatic diseases Benign Prostatic Hyperplasia (Nodular Hyperplasia) Extremely common Present in a significant number of men by the age of 40 & its frequency rises progressively with age, reaching
Some prostatic diseases Benign Prostatic Hyperplasia (Nodular Hyperplasia) Extremely common Present in a significant number of men by the age of 40 & its frequency rises progressively with age, reaching
Prostate Immunohistochemistry. Literature Interpretation: Caveats. Must be aware of staining pattern of antibody in the relevant tissue
 IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
Prognostic factors of genitourinary tumors: Do we have to care?
 Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Uropathology January Jon Oxley
 Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a product in my presentation.
 Prostate t Cancer MR Report Disclosure Information Vikas Kundra, M.D, Ph.D. I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a g product
Prostate t Cancer MR Report Disclosure Information Vikas Kundra, M.D, Ph.D. I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a g product
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Metachronous anterior urethral metastasis of prostatic ductal adenocarcinoma
 http://dx.doi.org/10.7180/kmj.2016.31.1.66 KMJ Case Report Metachronous anterior urethral metastasis of prostatic ductal adenocarcinoma Jeong Hyun Oh 1, Taek Sang Kim 1, Hyun Yul Rhew 1, Bong Kwon Chun
http://dx.doi.org/10.7180/kmj.2016.31.1.66 KMJ Case Report Metachronous anterior urethral metastasis of prostatic ductal adenocarcinoma Jeong Hyun Oh 1, Taek Sang Kim 1, Hyun Yul Rhew 1, Bong Kwon Chun
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
S1.04 PRINCIPAL CLINICIAN G1.01 COMMENTS S2.01 SPECIMEN LABELLED AS G2.01 *SPECIMEN DIMENSIONS (PROSTATE) S2.03 *SEMINAL VESICLES
 S2.03 *SEMINAL VESICLES") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Intraductal Carcinoma of the Prostate
 Intraductal Carcinoma of the Prostate Morphologic Features, Differential Diagnoses, Significance, and Reporting Practices The differential diagnosis for atypical cribriform lesions of the prostate has
Intraductal Carcinoma of the Prostate Morphologic Features, Differential Diagnoses, Significance, and Reporting Practices The differential diagnosis for atypical cribriform lesions of the prostate has
Unknown Slides Conference
 Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Clinicopathological Features of Prostate Ductal Carcinoma: Matching Analysis and Comparison with Prostate Acinar Carcinoma
 ORIGINAL ARTICLE Oncology & Hematology http://dx.doi.org/0.3346/jkms.205.30.4.385 J Korean Med Sci 205; 30: 385-389 Clinicopathological Features of Prostate Ductal Carcinoma: Matching Analysis and Comparison
ORIGINAL ARTICLE Oncology & Hematology http://dx.doi.org/0.3346/jkms.205.30.4.385 J Korean Med Sci 205; 30: 385-389 Clinicopathological Features of Prostate Ductal Carcinoma: Matching Analysis and Comparison
1 NORMAL HISTOLOGY AND METAPLASIAS
 1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
Outline (1) Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer
 Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer") Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Although current American Cancer Society guidelines
 ORIGINAL ARTICLE Diffuse Adenosis of the Peripheral Zone in Prostate Needle Biopsy and Prostatectomy Specimens Tamara L. Lotan, MD* and Jonathan I. Epstein, MD*w z Abstract: We have observed a group of
ORIGINAL ARTICLE Diffuse Adenosis of the Peripheral Zone in Prostate Needle Biopsy and Prostatectomy Specimens Tamara L. Lotan, MD* and Jonathan I. Epstein, MD*w z Abstract: We have observed a group of
Metastatic Ductal Adenocarcinoma of the Prostate Cytologic Features and Clinical Findings
 Anatomic Pathology / FNA OF METASTATIC PROSTATIC DUCTAL ADENOCARCINOMA Metastatic Ductal Adenocarcinoma of the Prostate Cytologic Features and Clinical Findings Yun Gong, MD, Nancy Caraway, MD, John Stewart,
Anatomic Pathology / FNA OF METASTATIC PROSTATIC DUCTAL ADENOCARCINOMA Metastatic Ductal Adenocarcinoma of the Prostate Cytologic Features and Clinical Findings Yun Gong, MD, Nancy Caraway, MD, John Stewart,
Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD
 Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology,
Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology,
Mucin-producing urothelial-type adenocarcinoma of prostate: report of two cases of a rare and diagnostically challenging entity
 & 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Mucin-producing urothelial-type adenocarcinoma of prostate: report of two cases of a rare and diagnostically challenging
& 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Mucin-producing urothelial-type adenocarcinoma of prostate: report of two cases of a rare and diagnostically challenging
Grading Prostate Cancer: Recent Changes and Refinements
 USPSTF: 2012 Report on serum PSA Screening Recommendation rating of D Reduced screening, Reduced biopsies, reduced incidence Refinements currently occurring in 2017. WHY? Grading Prostate Cancer: Recent
USPSTF: 2012 Report on serum PSA Screening Recommendation rating of D Reduced screening, Reduced biopsies, reduced incidence Refinements currently occurring in 2017. WHY? Grading Prostate Cancer: Recent
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Although partial atrophy is one of the most common
 ORIGINAL ARTICLE Partial Atrophy on Prostate Needle Biopsy Cores: A Morphologic and Immunohistochemical Study Wenle Wang, MD, PhD,* Xinlai Sun, MD,w and Jonathan I. Epstein, MD*zy Abstract: Partial atrophy
ORIGINAL ARTICLE Partial Atrophy on Prostate Needle Biopsy Cores: A Morphologic and Immunohistochemical Study Wenle Wang, MD, PhD,* Xinlai Sun, MD,w and Jonathan I. Epstein, MD*zy Abstract: Partial atrophy
Proliferative Epithelial lesions of the Breast. Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London
 Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
ISPUB.COM. Interpretation Of Prostatic Biopsies: A Review. A Chitale, S Khubchandani INTRODUCTION NON-NEOPLASTIC LESIONS GRADING: GLEASON'S SCORE
 ISPUB.COM The Internet Journal of Urology Volume 3 Number 1 A Chitale, S Khubchandani Citation A Chitale, S Khubchandani.. The Internet Journal of Urology. 2004 Volume 3 Number 1. Abstract The incidence
ISPUB.COM The Internet Journal of Urology Volume 3 Number 1 A Chitale, S Khubchandani Citation A Chitale, S Khubchandani.. The Internet Journal of Urology. 2004 Volume 3 Number 1. Abstract The incidence
TOPICS FOR DISCUSSION
 INTERNATIONAL SOCIETY OF UROLOGIC PATHOLOGY PATHOLOGIC STAGING OF SELECT UROLOGIC MALIGNANCIES Mahul B. Amin, MD Professor and Chairman Pathology and Laboratory Medicine Cedars-Sinai Medical Center Los
INTERNATIONAL SOCIETY OF UROLOGIC PATHOLOGY PATHOLOGIC STAGING OF SELECT UROLOGIC MALIGNANCIES Mahul B. Amin, MD Professor and Chairman Pathology and Laboratory Medicine Cedars-Sinai Medical Center Los
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma
 Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Objective. Atypical/Atypia. Atypical Glandular Lesions of the Prostate 12/27/2011
 Atypical Glandular Lesions of the Prostate V.O.Speights,Jr.,D.O. Scott and White Memorial Hospital Texas A & M Health Science Center January 13,2012 Objective To identify histological abnormalities in
Atypical Glandular Lesions of the Prostate V.O.Speights,Jr.,D.O. Scott and White Memorial Hospital Texas A & M Health Science Center January 13,2012 Objective To identify histological abnormalities in
Ductal adenocarcinoma of the prostate: A clinicopathological study
 20 B. SATHESAN, S. A. S. GOONEWARDENA, H. W. D. ANURUDDHIKA AND M. V. C. DE SILVA Sri Lanka Journal of Urology, 2008, 9, 20-24 Original Article Ductal adenocarcinoma of the prostate: A clinicopathological
20 B. SATHESAN, S. A. S. GOONEWARDENA, H. W. D. ANURUDDHIKA AND M. V. C. DE SILVA Sri Lanka Journal of Urology, 2008, 9, 20-24 Original Article Ductal adenocarcinoma of the prostate: A clinicopathological
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseudocapsule
 GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Supplemental Information
 Supplemental Information Prediction of Prostate Cancer Recurrence using Quantitative Phase Imaging Shamira Sridharan 1, Virgilia Macias 2, Krishnarao Tangella 3, André Kajdacsy-Balla 2 and Gabriel Popescu
Supplemental Information Prediction of Prostate Cancer Recurrence using Quantitative Phase Imaging Shamira Sridharan 1, Virgilia Macias 2, Krishnarao Tangella 3, André Kajdacsy-Balla 2 and Gabriel Popescu
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Demystifying Endometrial Hyperplasia
 Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
ROLE OF PROSTATIC BASAL CELL MARKER IN DIAGNOSIS OF PROSTATIC LESIONS
 Original Research Article Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 ROLE OF PROSTATIC BASAL CELL MARKER IN DIAGNOSIS OF PROSTATIC LESIONS SUBATHRA K* Department of pathology,
Original Research Article Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 ROLE OF PROSTATIC BASAL CELL MARKER IN DIAGNOSIS OF PROSTATIC LESIONS SUBATHRA K* Department of pathology,
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Low grade urothelial carcinoma mimicking basal cell hyperplasia and transitional metaplasia in needle prostate biopsy
 ORIGINAL ARTICLE Vol. 42 (2): 247-252, March - April, 2016 doi: 10.1590/S1677-5538.IBJU.2014.0512 Low grade urothelial carcinoma mimicking basal cell hyperplasia and transitional metaplasia in needle prostate
ORIGINAL ARTICLE Vol. 42 (2): 247-252, March - April, 2016 doi: 10.1590/S1677-5538.IBJU.2014.0512 Low grade urothelial carcinoma mimicking basal cell hyperplasia and transitional metaplasia in needle prostate
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Columnar Cell Lesions
 Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Prostate Overview Quiz
 Prostate Overview Quiz 1. The path report reads: Gleason 3 + 4 = 7. The Gleason s score is a. 3 b. 4 c. 7 d. None of the above 2. The path report reads: Moderately differentiated adenocarcinoma of the
Prostate Overview Quiz 1. The path report reads: Gleason 3 + 4 = 7. The Gleason s score is a. 3 b. 4 c. 7 d. None of the above 2. The path report reads: Moderately differentiated adenocarcinoma of the
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency
 Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseud
 GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
P rare and, therefore, their histopathologic
 PROSTATIC ADENOCARCINOMA OF DUCTAL ORIGIN VOLKER E. DUBE, MD,+ GEORGE M. FARROW, AND LAURENCE F. GREENE, MD+ MD+ Clinical and histopathologic features of prostatic ductal adenocarcinomas have been incompletely
PROSTATIC ADENOCARCINOMA OF DUCTAL ORIGIN VOLKER E. DUBE, MD,+ GEORGE M. FARROW, AND LAURENCE F. GREENE, MD+ MD+ Clinical and histopathologic features of prostatic ductal adenocarcinomas have been incompletely
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Update on Bladder Cancer: What s New in the 2016 WHO Classification of Bladder Tumors and 8 th Edition of AJCC Staging Manual
 Update on Bladder Cancer: What s New in the 2016 WHO Classification of Bladder Tumors and 8 th Edition of AJCC Staging Manual Rajal B. Shah, M.D. Director, Urologic Pathology SHAHR6@ccf.org @rajalbshah
Update on Bladder Cancer: What s New in the 2016 WHO Classification of Bladder Tumors and 8 th Edition of AJCC Staging Manual Rajal B. Shah, M.D. Director, Urologic Pathology SHAHR6@ccf.org @rajalbshah
OMPRN Pathology Matters Meeting 2017
 OMPRN Pathology Matters Meeting 2017 Pathology of Aggressive Prostate Cancer Intraductal Carcinoma and Cribriform Carcinoma Dr. Michelle Downes, Staff Urologic Pathologist Sunnybrook Health Sciences Centre,
OMPRN Pathology Matters Meeting 2017 Pathology of Aggressive Prostate Cancer Intraductal Carcinoma and Cribriform Carcinoma Dr. Michelle Downes, Staff Urologic Pathologist Sunnybrook Health Sciences Centre,
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
!! 2 to 3% of All New Visceral Cancers.!! Peak Incidence is 6th Decade!! M:F = 2:1
 !! Kathleen M. O Toole, M.D.!! 2 to 3% of All New Visceral Cancers!! Peak Incidence is 6th Decade!! M:F = 2:1!! Grossly is a Bright Yellow, Necrotic Mass with a Pseudocapsule 1 !!Conventional RCC! Clear
!! Kathleen M. O Toole, M.D.!! 2 to 3% of All New Visceral Cancers!! Peak Incidence is 6th Decade!! M:F = 2:1!! Grossly is a Bright Yellow, Necrotic Mass with a Pseudocapsule 1 !!Conventional RCC! Clear
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel