Hormonal Manipulations in CRPC. NW Clarke Professor of Urological Oncology Manchester UK
|
|
|
- Brett Ramsey
- 5 years ago
- Views:
Transcription
1 Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK
2 Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component C Bicalutamide stopped
3 Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component C Bicalutamide stopped
4 Traditional Hormonal Therapies for CRPC Addition of Anti-androgens Addition of anti-androgen n PSA response 50% decline (%) Median duration (months) Bicalutamide 150 mg/day NA Bicalutamide 150 mg/day NA Bicalutamide 200 mg/day Nilutamide 200 or 300 mg/day Nilutamide 150 or 300 mg/day Bicalutamide 80 mg/day or flutamide 375 mg/day Median OS (months) 15* NA NA NA NA NM None have been shown to significantly improve overall survival 1. Kucuk et al. Urology 2001;58: Joyce et al. J Urol 1998;159: Scher et al. J Clin Oncol 1997;15: Kassouf et al. J Urol 2003;169: Desai et al. Urology 2001;58: Suzuki et al. J Urol 2008;180:921 7.
5 Traditional Hormonal Therapies for CRPC Corticosteroids / oestrogens Corticosteroids n PSA response 50% decline (%) Median duration (months) Hydrocortisone 40 mg/day Hydrocortisone 40 mg/day Prednisone 10 mg/day Prednisone 20 mg/day Dexamethasone (0.5 mg/day) Oestrogens DES 1 mg/day NA DES 3 mg/day Transdermal oestradiol 0.6 mg/day Median OS (months) NA 12.6* NM* 11.9* NA NM NA NA None have been shown to improve overall survival significantly Kelly et al. J Clin Oncol 1995;. Kantoff J Clin Oncol 1999; Tannock. J Clin Oncol Sternberg et al. Oncology 2005 Venkitaraman et al. BJU Int 2007 Smith. Urology Oh et al. J Clin Oncol Dawson et al. Cancer 2000.
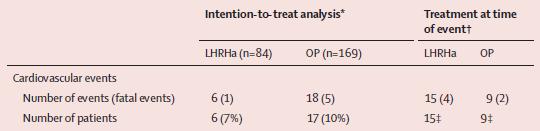
6 N=270 CV Event Rate 20% TTP for DAiS (8.6 months) was significantly longer DA (4.5 months p<0,001)


7 Lancet Oncology Vol 14 April 2013
8 Evolving treatment in CRPC Hormone sensitive mcrpc asymptomatic disease (failed ADT) mcrpc mildly symptomatic disease mcrpc symptomatic pre-chemo C he m o mcrpc post-chemo Hormone therapy Sipuleucel-T Abiraterone Abiraterone Docetaxel Cabazitaxel Enzalutamide Approved for use by FDA/EMA Approved for use by FDA Positive Phase III data Radium 223 PLUS supportive care (e.g. denosumab/bisphosphonates/β-emitters)
9 Ongoing Phase III Trials in Metastatic CRPC Asymptomatic mcrpc (failed ADT) Mildly symptomatic mcrpc mcrpc symptomatic pre-chemo C he m o mcrpc post-chemo Ipilimumab vs. placebo Cabazitaxel vs. Docetaxel (FIRSTANA) Cabozantinib vs. prednisone (COMET-1) PROSTVAC-V/F ± GM-CSF vs. placebo (PROSPECT) Tasquinimod vs. placebo Dasatinib vs. placebo (+ docetaxel, both arms) (READY*) Enzalutamide vs. placebo (PREVAIL) Cabozantinib vs. mitoxantrone + prednisone (COMET-2) Cabazitaxel 20 mg/m² vs. 25 mg/m² (PROSELICA) Custirsen ± docetaxel + prednisone (SYNERGY) Ipilimumab vs. placebo following RT Orteronel vs. placebo Orteronel vs. placebo


 n=755")
 de Bono JS, et al.")
10 Cytotoxic Chemotherapy: Docetaxel and Cabazitaxel in CRPC Phase 3, randomized, open-label trial of cabazitaxel + prednisone versus mitoxantrone + prednisone in mcrpc previously treated with docetaxel Primary endpoint: OS Secondary endpoints: PSA response, PSA progression, tumour response (RECIST), pain response 25 mg/m 2 cabazitaxel IV every 3 weeks + prednisone 10 mg QD (n=378) n=755 mcrpc progression after Docetaxel 1:1 12 mg/m 2 mitoxantrone IV every 3 weeks + prednisone 10 mg QD (n=377) de Bono JS, et al. Lancet 2010;376:
 Docetaxel is initiated: 8 cycles 75 mg/m 2 + prednisone 5 mg bid Response after 6 cycles: PSA 256")
11 Standard Treatment of CRPC Post 2005 (? in 2013) Docetaxel is initiated: 8 cycles 75 mg/m 2 + prednisone 5 mg bid Response after 6 cycles: PSA 256 to 162 ng/ml, small decrease on LN 8 cycles of docetaxel 75 mg/m 2
12 Standard Treatment of CRPC Post 2005 Treatment with docetaxel is stopped after 9 cycles due to PSA progression, Grade 3 fatigue and multiple lymph node metastases This was followed by a more rapid PSA progression Multiple lymph nodes metastases 99m TC BS Docetaxel



13 Standard Treatment of CRPC Post 2005 Treatment with docetaxel is stopped after 9 cycles due to PSA progression, Grade 3 fatigue and multiple lymph node metastases This was followed by a more rapid PSA progression Multiple lymph nodes metastases 99m TC BS Docetaxel









14 Novel Androgenic Approaches in CRPC LHRH agonists LH ACTH Androstenedione Ligand-dependent Receptor tyrosine kinase Ligand-independent 4 Ligand-independent activation of AR 1 2 Alternate ligands 6 Coactivators Corepressors Nuclear localisation Transcription 5 7 AR splice variants Nucleus Cytoplasm
15 Standard Treatment of CRPC in 2013 / 2014 Abiraterone Docetaxel AFFIRM: A Multinational Phase 3, Randomized, Double-Blind, Placebo-Controlled Efficacy and Safety Study of Oral MDV3100 in Patients With Progressive Castration-Resistant Prostate Cancer Previously Treated With Docetaxel-Based Chemotherapy (NCT )
16 Standard Treatment of CRPC in 2013 / 2014 PSA progression Patient asymptomatic Hb 10.5 mg/dl from 12.5 mg/dl Abiraterone Docetaxel
17 Standard Treatment of CRPC in 2013 / 2014 PSA progression Patient is now moderately symptomatic in cervical spine (treated by paracetamol and piroxicam) Hb 10.5 mg/dl from 12.5 mg/dl Abiraterone Docetaxel
18 Standard Treatment of CRPC in 2013 / 2014 Increase cervical pain with neurological symptoms in both arms, urinary retention Abiraterone Docetaxel Enzalutamide
19 Standard Treatment of CRPC in 2013 / 2014 Increase cervical pain with neurological symptoms in both arms, urinary retention Abiraterone Enzalutamide Docetaxel Enzalutamide Abiraterone
20 Problems and Uncertainties in CRPC Who gets the drugs Who gives the drugs? What is the optimal sequencing and combination What about poor performance status patients Who pays the bill.?
21 Problems and Uncertainties in CRPC Who gets the drugs Who gives the drugs? What is the optimal sequencing and combination What about poor performance status patients Who pays the bill.?
22 prevention Survival Palliation What Are the Aims and Expectations Chemotherapy Hormones Radiotherapy Radionuclide Non-metastatic PSA increasing Metastatic Asymptomatic Metastatic Symptomatic (bone pain)
23 prevention Survival Palliation What Are the Aims and Expectations Chemotherapy Hormones Radiotherapy Radionuclide Chemotherapy Hormones Radiotherapy Radionuclide Non-metastatic PSA increasing Metastatic Asymptomatic Metastatic Symptomatic (bone pain)
24 prevention Survival Palliation What Are the Aims and Expectations Chemotherapy Hormones Radiotherapy Radionuclide Chemotherapy Hormones Radiotherapy Radionuclide Chemotherapy Hormones Radiotherapy Radionuclide Non-metastatic PSA increasing Metastatic Asymptomatic Metastatic Symptomatic (bone pain)
25 prevention Survival Palliation What Are the Aims and Expectations? Chemotherapy Non-metastatic PSA increasing Metastatic Asymptomatic Metastatic Symptomatic (bone pain)
26 prevention Survival Palliation What Are the Aims and Expectations? Chemotherapy Non-metastatic PSA increasing Metastatic Asymptomatic Metastatic Symptomatic (bone pain)
27 prevention Survival Palliation What Are the Aims and Expectations? Non-metastatic PSA increasing Metastatic Asymptomatic Metastatic Symptomatic (bone pain)
28 prevention Survival Palliation What Are the Aims and Expectations? Non-metastatic PSA increasing Metastatic Asymptomatic Metastatic Symptomatic (bone pain)
29 prevention Survival Palliation What Are the Aims and Expectations Palliate symptoms Improve survival? Prevent onset and complications of bone metastases? Non-metastatic PSA increasing Metastatic Asymptomatic Metastatic Symptomatic (bone pain)
30 Cumulative incidence Older Men Have a Higher Risk of Dying Due to PCa Cumulative incidence of PCa-related death <75 Years from prostate cancer diagnosis Skosyrev E et al. Cancer 2012;118:

31 Treatment Should be Adapted to Health Status Fit Vulnerable Frail No serious co-morbidity (CIRS-G rating: 0 2) Functionally independent No malnutrition years (50% ) and years (25%) Uncontrolled co-morbidity Dependent in at least one IADL Risk of malnutrition Reversible through geriatric intervention Two or more uncontrolled co- morbidities Dependent in one or more IADL Severe malnutrition Too sick Terminal illness Bedridden Major co-morbidities Cognitive impairments Same treatment as younger patients Geriatric intervention => Standard treatment Geriatric intervention => Adapted treatment (or palliation) Only palliative treatment Standard Treatment Geriatric Intervention Droz JP et al. Crit Rev Oncol Hematol 2010;73:61 91 Droz JP et al. BJU Int 2010;106:462 9
32 What Do We Combine in CRPC? Advances in the understanding of mcrpc have led to the development of new agents with diverse mechanisms of action: Second-generation taxanes Androgen-lowering agents AR signalling inhibitors Radiopharmaceuticals Bone Protective Agents Tyrosine kinase inhibitors Others Hou X, Flaig TW. Adv Urol 2012;2012;978531; Fizazi K, et al. Ann Oncol 2012;23(Suppl. 10):x264 7.
33 Figure 2 Overall survival HR=hazard ratio. AA=abiraterone acetate. P=prednisone. Karim Fizazi, Howard I Scher, Arturo Molina, Christopher J Logothetis, Kim N Chi, Robert J Jones, John N St... Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study The Lancet Oncology null 2012 null
34 The Lancet Oncology null 2012 null
35 The Affirm Study MDV3100 Placebo Median OS (months) Hazard ratio 0.63 P value < NEJM Sept 2012
36 Orteronel (TAK-700): Clinical Studies Phase 1/2 study in metastatic CRPC: Phase 2 results Percent change from baseline in PSA at 24 weeks by patient Bars with darker shading marked X indicate patients who received prior ketoconazole At 24 weeks, 36 patients (64% of evaluable, 38% of intent-to-treat population) had PSA decreases of 50% (PSA50) Agus DB, et al. ASCO 2011, Chicago, IL, USA; Abstract 4531
37 Orteronel (TAK-700) Registration Study C21005: mcrpc Following Docetaxel Failure Patients 1,083 patients, progressive, mcrpc Failed 1 or 2 chemotherapy regimens, one of which contained docetaxel Orteronel po BID Prednisone po BID Placebo po BID Prednisone po BID Efficacy Endpoints Primary: OS Secondary: PSA response Pain response rpfs rpfs = radiographic progression-free survival accessed June 2011
38 Phase III PREVAIL Trial: Study Design CRPC R 1:1 MDV mg daily Placebo Co-primary endpoints: overall survival and progression-free survival Secondary endpoints: time to first SRE; time to start of chemotherapy Key inclusion criteria: No prior treatment with cytotoxic chemotherapy Asymptomatic or mildly symptomatic Estimated primary completion date September 2014 Clinicaltrials.gov identifier # NCT
39 Updated Interim Analysis (55% OS) of COU-AA-302, a Randomized Phase 3 Study of Abiraterone Acetate in Metastatic Castration-Resistant Prostate Cancer Patients Without Prior Chemotherapy Dana Rathkopf,1 Matthew R Smith,2 Johann S. de Bono,3 Christopher Logothetis,4 Neal D. Shore,5 Paul de Souza,6 Karim Fizazi,7 Peter F.A. Mulders,8 Paul Mainwaring,9 John D. Hainsworth,10 Tomasz M. Beer,11 Scott North,12 Yves Fradet,13 Tom Griffin,14 Youn C. Park,15 Thian Kheoh,14 Eric J. Small,16 Howard I. Scher,1,17 Arturo Molina,14 Charles J. Ryan18 on behalf of the COU-AA-302 Investigators Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)
40 Subjects Without Progression or Death (%) Abiraterone and Time to rpfs Abiraterone (median, mos): 16.5 Prednisone (median, mos): 8.3 HR (95% CI): 0.53 ( ) p Value: < Abiraterone Prednisone Months From Randomization Abiraterone Prednisone Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)
41 Subjects Without Death (%) Abiraterone and Overall Survival 100 Abiraterone (median, mos): 35.3 Prednisone (median, mos): 30.1 HR (95% CI): 0.79 ( ) p Value a : Abiraterone Prednisone Months From Randomization Abiraterone Prednisone Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)
42 Subsequent Therapy After Abiraterone Abiraterone (n = 419) n (%) Prednisone (n = 482) n (%) No. with selected subsequent therapy for mcrpc a 274 (65) 347 (72) Docetaxel 239 (57) 304 (63) Cabazitaxel 60 (14) 70 (15) Ketoconazole 39 (9) 63 (13) Abiraterone b 38 (9) 78 (16) Sipuleucel-T 33 (8) 28 (6) Rathkopf et al. ASCO GU 2013; Abstract 5
43 Safety Profile Abiraterone (n = 542) % Prednisone (n = 540) % Adverse event All grades Grades 3/4 All grades Grades 3/4 Fatigue Fluid retention Hypokalemia Hypertension Hyperglycemia Weight gain Cardiac disorders ALT increased AST increased Rathkopf et al. ASCO GU 2013; Abstract 5
44 COU-AA-302 Updated Interim Analysis: Summary 8.2 months rpfs improvement (16.5 vs 8.3 months) 5.2 months OS improvement (35.3 vs 30.1 months) 9.7 months delay chemotherapy (26.5 vs 16.8 months) Delayed time to opiate use (NR vs 23.7 months) Improved QoL Tolerated treatment with longer exposure Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)
45 Problems and Uncertainties in CRPC Who gets the drugs Who gives the drugs? What is the optimal sequencing and combination What about poor performance status patients Who pays the bill.?
46 Chemotherapy or Hormonal Treatment First?
47 When Should Chemotherapy be Started? Not all men are suitable for chemotherapy Both QoL and pain can be improved by chemotherapy Men with minimal symptoms had prolonged survival Berthold, D. R. et al. J Clin Oncol; 26:
48 Should Docetaxel Responders be Re-Treated Re-Treatments of Initial Responders 59% Response to 1 st Line 90% Response to 2 nd Line 71% Response to 3 rd Line Duration of Response Weeks N Sepsis st Line /4.2 2 nd Line /5.2 % 3 rd Line Ansari et al GU ASCO 2009 # 185
49 Survival (%) TROPIC results: Efficacy Median follow-up: 12.8 months Median OS: Cabazitaxel 15.1 months Mitoxantrone 12.7 months HR=0.70 (95% CI: ); p< % reduction in risk of death Mitoxantrone Cabazitaxel Months Mitoxantrone (n) Cabazitaxel (n) CI=confidence interval; HR=hazard ratio. de Bono JS, et al. Lancet 2010;376:
50 Novel Androgen Receptor Signalling Should all patients receive this routinely as the first 2 nd line agent How do we decide whether to give chemotherapy 1 st or 2 nd How will regulation affect sequencing?
51 Novel Androgen Receptor Signalling Should all patients receive this routinely as the first 2 nd line agent How do we decide whether to give chemotherapy 1 st or 2 nd How will regulation affect sequencing?
52 Docetaxel in Chemotherapy-naive Patients after Abiraterone Failure N = 35 TAX (Docetaxel q3w) Phase I-II 2 (Abiraterone Docetaxel) PSA decrease 50% 45% 26% Time to PSA progression (median) Overall survival (median) 7.7 mo 4.6 mo 18.9 mo 12.5 mo Docetaxel after AA failure maybe not as effective as docetaxel 1 st line 1. Tannock IF et al. N Engl J Med 2004;351: Mezynski J et al. Ann Oncol 2012;epub ahead of print.
53 Androgen Receptor Inhibition After Chemotherapy COU-AA (Abiraterone vs Placebo) AFFIRM 2 (Enzalutamide vs Placebo) OS after 1 prior line chemotherapy OS after 2 prior lines chemotherapy 17.1 vs 11.7 mo NR vs 14.2 mo 14.2 vs 10.4 mo 15.9 vs 12.3 mo Abiraterone and enzalutamide both effective after 2 lines of chemotherapy 1. Fizazi K et al. Lancet Oncol Scher H et al. N Engl J Med 2012;367:

54 Cumulative survival Sequence after Docetaxel Failure Abiraterone Median OS 8 months Cabazitaxel Median OS 18 months Docetaxel Cabazitaxel Docetaxel Abiraterone Months (Treatment start) Malik Z et al. J Clin Oncol 2012;30 (Suppl):abstract e15135
55 Problems and Uncertainties in CRPC Who gets the drugs Who gives the drugs? What is the optimal sequencing and combination What about poor performance status patients Who pays the bill.?
56 The Lancet Oncology null 2012 null
57 Survival (%) ECOG Status 100 OS: ECOG status (0-1 vs 2) AA ECOG months AA ECOG months 40 Placebo ECOG 2 7 months Placebo ECOG months Time to Death (Months) Scher et al. J Clin Oncol 2011; 25 (suppl 7); Abstract 4 (oral presentation)
58 Survival (%) Survival (%) Prior Chemotherapy OS: 1 prior line of chemotherapy OS: 2 prior lines of chemotherapy AA 15.4 months 80 AA 14.0 months Placebo 11.5 months 20 Placebo 10.3 months Time to Death (Months) Time to Death (Months) de Bono et al. Ann Oncol 2010; 21 (10 suppl 8): Abstract LBA5 (oral presentation) Scher et al. J Clin Oncol 2011; 25 (suppl 7): Abstract 4 (oral presentation)
59 Survival (%) Survival (%) Pain Status OS: Pain (0-3 [absent]) OS: Pain (4-10 [present]) AA 16.2 months 80 AA 12.6 months Placebo 13 months 20 Placebo 8.9 months Time to Death (Months) Time to Death (Months) *Brief Pain Inventory scale Scher et al. J Clin Oncol 2011; 25 (suppl 7); Abstract 4 (oral presentation)
60 Problems and Uncertainties in CRPC Who gets the drugs Who gives the drugs? What is the optimal sequencing and combination What about poor performance status patients Who pays the bill.?
61 Costs 2930 / Month ($4640) 46,800-50,000 / QALY Initially rejected by NICE: Too Costly Accepted June 2012 after Renegotiation of the price
62 Costs 2930 / Month ($4640) 46,800-50,000 / QALY Initially rejected by NICE: Too Costly Accepted June 2012 after Renegotiation of the price
63 Costs
64 Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Until 2004, CRPC was consistently a rapidly lethal disease.
 Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Group Sequential Design: Uses and Abuses
 Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC
 Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc
 SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Management of castrate resistant disease; after first line hormone therapy fails
 Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Evolution or revolution in the treatment of prostate cancer
 Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC
 Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
- La Terapia Farmacologica -
 XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer?
 Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Advanced Prostate Cancer. Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options
 Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
SUMMARY. 3. Emerging understanding of mechanisms of resistance to current treatments
 SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Evolution of Chemotherapy for. Cancer
 Evolution of Chemotherapy for Hormone Refractory Prostate t Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology Princess Margaret Hospital and University of Toronto In 1985, two
Evolution of Chemotherapy for Hormone Refractory Prostate t Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology Princess Margaret Hospital and University of Toronto In 1985, two
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Anti-Androgen Therapies for Prostate Cancer: A Focused Review
 Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223
 SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T
 Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater
Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
8/31/ ) Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases
 Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases") Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Navigating Prostate Cancer Therapy. Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA
 Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER
 INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER Daniel George, MD Professor of Medicine and Surgery Director of Genitourinary Oncology Program Duke Cancer Institute 1 Disclosures Consultant:
INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER Daniel George, MD Professor of Medicine and Surgery Director of Genitourinary Oncology Program Duke Cancer Institute 1 Disclosures Consultant:
Published on The YODA Project (
 Principal Investigator First Name: David Last Name: Lorente Degree: MD Primary Affiliation: Medical Oncology Service, Hospital Provincial de Castellón E-mail: lorente.davest@gmail.com Phone number: +34
Principal Investigator First Name: David Last Name: Lorente Degree: MD Primary Affiliation: Medical Oncology Service, Hospital Provincial de Castellón E-mail: lorente.davest@gmail.com Phone number: +34
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS
 UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE. Daan De Maeseneer, Medisch Oncoloog
 PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
Perspective on endocrine and chemotherapy agents. Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Michiel H.F. Poorthuis*, Robin W.M. Vernooij*, R. Jeroen A. van Moorselaar and Theo M. de Reijke
 First-line non-cytotoxic therapy in chemotherapynaive patients with metastatic castration-resistant prostate cancer: a systematic review of 10 randomised clinical trials Michiel H.F. Poorthuis*, Robin
First-line non-cytotoxic therapy in chemotherapynaive patients with metastatic castration-resistant prostate cancer: a systematic review of 10 randomised clinical trials Michiel H.F. Poorthuis*, Robin
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Con$nuing Care for Your Pa$ents with Metasta$c CRPC
 27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Please consider the following information on ZYTIGA (abiraterone acetate). ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017
. ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017") Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
To treat or not to treat: When to treat! A case presentation
 To treat or not to treat: When to treat! A case presentation Filip Ameye, MD,Phd Universitary Hospitals Leuven, Belgium Departement of Urology Prostate Center A case presentation Pt. 76 y. Mild LUTS (07/1999)
To treat or not to treat: When to treat! A case presentation Filip Ameye, MD,Phd Universitary Hospitals Leuven, Belgium Departement of Urology Prostate Center A case presentation Pt. 76 y. Mild LUTS (07/1999)
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
What will change for men with advanced prostate cancer in the next 24 months? ESO Observatory: Perspective on endocrine and chemotherapy agents
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Board Review 2017: Prostate Cancer. Dana Rathkopf, MD Associate Attending
 Board Review 2017: Prostate Cancer Dana Rathkopf, MD Associate Attending www.mskcc.org The Paradox of Prostate Cancer High prevalence in the general population: over diagnosis of clinically insignificant
Board Review 2017: Prostate Cancer Dana Rathkopf, MD Associate Attending www.mskcc.org The Paradox of Prostate Cancer High prevalence in the general population: over diagnosis of clinically insignificant
SIMPOSIO. Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico
 SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Patients Living Longer: The Promise of Newer Therapies
 Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
Management Options in Advanced Prostate Cancer: What is the Role for Sipuleucel-T?
 Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Castrate resistant prostate cancer: the future of anti-androgens.
 Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer?
 Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer. Michal Mego
 National Cancer Institute, Slovakia Translational Research Unit Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer Michal Mego 2 nd Department of Oncology, Faculty
National Cancer Institute, Slovakia Translational Research Unit Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer Michal Mego 2 nd Department of Oncology, Faculty
January Abiraterone pre-docetaxel for patients with asymptomatic or minimally symptomatic metastatic castration resistant prostate cancer
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone pre-docetaxel for asymptomatic/minimally symptomatic metastatic castration resistant prostate cancer Abiraterone pre-docetaxel for patients with asymptomatic
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone pre-docetaxel for asymptomatic/minimally symptomatic metastatic castration resistant prostate cancer Abiraterone pre-docetaxel for patients with asymptomatic
abiraterone acetate, 250mg tablets (Zytiga ) SMC No. (873/13) Janssen-Cilag Ltd
 SMC No. (873/13) Janssen-Cilag Ltd") abiraterone acetate, 250mg tablets (Zytiga ) SMC No. (873/13) Janssen-Cilag Ltd 09 January 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
abiraterone acetate, 250mg tablets (Zytiga ) SMC No. (873/13) Janssen-Cilag Ltd 09 January 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
American Urological Association (AUA) Guideline
 Guideline") 1 Approved by the AUA Board of Directors May 2018 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2018 by the American Urological
1 Approved by the AUA Board of Directors May 2018 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2018 by the American Urological
Present and Future Perspectives in Treatment of mcrpc Patients
 Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
New Treatment Options for Prostate Cancer
 New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT
![Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT](/thumbs/71/65630457.jpg "Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT") Evolution of Treatment Options for Patients with and Bone Metastases Trials of Treatments for Castration-Resistant Prostrate Cancer Mentioned in This Review Bisphosphonates (Zometa) 4 mg IV 8 mg IV ( to
Evolution of Treatment Options for Patients with and Bone Metastases Trials of Treatments for Castration-Resistant Prostrate Cancer Mentioned in This Review Bisphosphonates (Zometa) 4 mg IV 8 mg IV ( to
Economic Evaluation of cabazitaxel (Jevtana ) for the treatment of patients with hormone-refractory metastatic prostate cancer previously treated
 for the treatment of patients with hormone-refractory metastatic prostate cancer previously treated") Economic Evaluation of cabazitaxel (Jevtana ) for the treatment of patients with hormone-refractory metastatic prostate cancer previously treated with docetaxel-containing treatment regimen. March 2012
Economic Evaluation of cabazitaxel (Jevtana ) for the treatment of patients with hormone-refractory metastatic prostate cancer previously treated with docetaxel-containing treatment regimen. March 2012
SUPPLEMENTARY APPENDIX. COU-AA-301 enrolled men with pathologically confirmed mcrpc who had received previous
 SUPPLEMENTARY APPENDIX Methods Subjects COUAA30 enrolled men with pathologically confirmed mcrpc who had received previous treatment with docetaxel chemotherapy and had documented PSA progression according
SUPPLEMENTARY APPENDIX Methods Subjects COUAA30 enrolled men with pathologically confirmed mcrpc who had received previous treatment with docetaxel chemotherapy and had documented PSA progression according
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
Metastatic castrate-resistant prostate cancer: Toward a chronic disease
 Metastatic castrate-resistant prostate cancer: Toward a chronic disease Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France General recommendations in CRPC Check serum Testosterone (should
Metastatic castrate-resistant prostate cancer: Toward a chronic disease Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France General recommendations in CRPC Check serum Testosterone (should
mcrpc in 2016 How to decide the optimal treatment? N. Mottet
 mcrpc in 2016 How to decide the optimal treatment? N. Mottet Disclosures Conflict of interest Chairman EAU PCa guidelines..... Therefore I'm 100% biased Castrate-resistant prostate cancer (CRPC) Definition
mcrpc in 2016 How to decide the optimal treatment? N. Mottet Disclosures Conflict of interest Chairman EAU PCa guidelines..... Therefore I'm 100% biased Castrate-resistant prostate cancer (CRPC) Definition
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD
 Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD The University of Athens Medical School Dept of Clinical Therapeutics Prostate Cancer Evolution Chemotherapy
Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD The University of Athens Medical School Dept of Clinical Therapeutics Prostate Cancer Evolution Chemotherapy
Advances in Chemotherapy for Castration Resistant Prostate Cancer
 Advances in Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Director, Genitourinary Oncology Co Director, Signal Transduction Program Yale Comprehensive Cancer Center Sequencing
Advances in Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Director, Genitourinary Oncology Co Director, Signal Transduction Program Yale Comprehensive Cancer Center Sequencing
POSITIVE CHMP OPINION FOR XTANDI (ENZALUTAMIDE) IN ADVANCED PROSTATE CANCER 1
 IN ADVANCED PROSTATE CANCER 1") POSITIVE CHMP OPINION FOR XTANDI (ENZALUTAMIDE) IN ADVANCED PROSTATE CANCER 1 Enzalutamide recommended for approval in the European Union (EU) for the treatment of adult men with metastatic castration-resistant
POSITIVE CHMP OPINION FOR XTANDI (ENZALUTAMIDE) IN ADVANCED PROSTATE CANCER 1 Enzalutamide recommended for approval in the European Union (EU) for the treatment of adult men with metastatic castration-resistant
Principal Investigator. General Information. Conflict of Interest Published on The YODA Project (http://yoda.yale.edu)
") Principal Investigator First Name: Antonio Last Name: Finelli Degree: MD, MSc, FRCSC Primary Affiliation: Princess Margaret Cancer Centre E-mail: antonio.finelli@uhn.ca Phone number: 416-946-4501 x2851
Principal Investigator First Name: Antonio Last Name: Finelli Degree: MD, MSc, FRCSC Primary Affiliation: Princess Margaret Cancer Centre E-mail: antonio.finelli@uhn.ca Phone number: 416-946-4501 x2851
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
Sequencing treatment for metastatic prostate cancer
 11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
ESMO SUMMIT AFRICA Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit
 ESMO SUMMIT AFRICA 2018 Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche Merck Lilly 14 years of
ESMO SUMMIT AFRICA 2018 Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche Merck Lilly 14 years of
Challenges in the sequencing of therapies for the management of metastatic castrationresistant
 See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/261569460 Challenges in the sequencing of therapies for the management of metastatic castrationresistant
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/261569460 Challenges in the sequencing of therapies for the management of metastatic castrationresistant
HHS Public Access Author manuscript Prostate Cancer Prostatic Dis. Author manuscript; available in PMC 2015 December 01.
 Prospective Evaluation of Low-Dose Ketoconazole Plus Hydrocortisone (HC) in Docetaxel Pre-treated Castration- Resistant Prostate Cancer (CRPC) Patients Ernest N. Lo, M.D. 1, Laurel A. Beckett, Ph.D. 1,
Prospective Evaluation of Low-Dose Ketoconazole Plus Hydrocortisone (HC) in Docetaxel Pre-treated Castration- Resistant Prostate Cancer (CRPC) Patients Ernest N. Lo, M.D. 1, Laurel A. Beckett, Ph.D. 1,
What s New in Advanced Disease (CRPC)?
?") What s New in Advanced Disease (castration resistant prostate cancer = CRC)? Matthew Rettig, MD Associate rofessor Department of Medicine Division of Hematology-Oncology Department of Urology Medical Director,
What s New in Advanced Disease (castration resistant prostate cancer = CRC)? Matthew Rettig, MD Associate rofessor Department of Medicine Division of Hematology-Oncology Department of Urology Medical Director,
*For reprints and all correspondence: Nobuaki Matsubara, Kashiwanoha, Kashiwa, Chiba , Japan.
 Japanese Journal of Clinical Oncology, 2015, 45(8) 774 779 doi: 10.1093/jjco/hyv070 Advance Access Publication Date: 15 May 2015 Original Article Original Article A multicenter retrospective analysis of
Japanese Journal of Clinical Oncology, 2015, 45(8) 774 779 doi: 10.1093/jjco/hyv070 Advance Access Publication Date: 15 May 2015 Original Article Original Article A multicenter retrospective analysis of
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION
 FINAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
Two late stage clinical programs
 Safe harbor This presentation and our remarks based upon it, including responses to questions made during and following the presentation, may include forward-looking statements. Such statements are subject
Safe harbor This presentation and our remarks based upon it, including responses to questions made during and following the presentation, may include forward-looking statements. Such statements are subject