Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer?
|
|
|
- Noel Henry
- 6 years ago
- Views:
Transcription


1 Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
2 Disclosure Participation to advisory boards/honorarium for: Amgen, Astellas, Astrazeneca, Bayer, Clovis, Curevac, Essa, Genentech, Janssen, MSD, Orion, Sanofi




3 Androgen Receptor is still expressed in CRPC Xenograft model of MDA PCa 2b prostate cancer cells in SCID mice Prostate cancer in intact animal After castration Castration-resistant Androgen Receptor Navone N and Fizazi K, unpublished data
4 Targeting the AR pathway Adrenals Abiraterone Orteronel Galeterone ODM-204 Androgen Receptor inhibitors: -Bicalutamide -Enzalutamide -ODM-201 -ARN 509 -Galeterone -ODM-204 -EPI drugs DNA Testosterone/ Other androgens Cell division Testis Castration (alhrh or Surg.) Autocrine secretion Abiraterone Orteronel Galeterone ODM-204
5 Survival (%) Proportion of Overall Survival 4 new active drugs in 4 years for post-docetaxel CRPC! Cabazitaxel, De Bono J, Lancet 2010 Abiraterone, Fizazi K, Lancet Oncol MTX+PRED CBZ+PRED Time (months) Enzalutamide, Scher HI, NEJM Placebo: 13.6 months (95% CI: ) Duration of overall survival (months) Enzalutamide: 18.4 months (95% CI: 17.3 NYR) % Radium-223, Parker J, NEJM Placebo Median OS 11.3 mo Radium-223 Median OS 14.9 mo

6 b Abiraterone: CYP17 blockade inhibits androgen synthesis
7 Abiraterone post-chemotherapy: COU-301 Patients Progressive mcrpc patients (N = 1195) Failed 1 or 2 chemotherapy regimens R A N D O M I Z E D 2:1 AA 1000 mg daily Prednisone 5 mg BID n = 797 Placebo daily Prednisone 5 mg BID n = 398 Efficacy end points Primary end point: Overall survival (25% improvement; HR=0.8) Secondary end points: TTPP rpfs PSA response Stratification by: Performance status 0-1 vs 2 Worst pain BPI short form; 0-3 (absent) vs 4-10 (present) Prior chemotherapy 1 vs 2 Type of progression PSA only vs radiographic (with or without PSA) de Bono JS, et al. N Engl J Med, 2011
8 COU-301: Abiraterone prolongs survival in post-docetaxel mcrpc patients Fizazi K, et al. Lancet Oncol. 2012;13:
9 Abiraterone-Prednisone: Adverse events of special interest All Grades AA (n=791) Grades 3/4 All Grades Placebo (n=394) Grades 3/4 Fluid retention 31% 2% 22% 1% Hypokalemia 17% 3% 8% 1% Hypertension 10% 1% 8% <1% Cardiac disorders a 13% 3% 11% 2% LFT abnormalities 10% 3% 8% 3% Fizazi K, et al. Lancet Oncol.2012;13: de Bono et al. N Engl J Med 2011; 346:
10 Randomisation 1:1 Abiraterone in asymptomatic mcrpc: the COU-302 Phase III study Co-primary endpoints Patients Progressive chemonaïve mcrpc Asymptomatic or mildly symptomatic Abiraterone acetate + prednisone (n = 546) Placebo + prednisone (n = 542) Radiographic progression-free survival Overall survival Secondary Time to opiate use (cancerrelated pain) Time to initiation of chemotherapy Time to ECOG-PS deterioration Time to PSA progression Stratification by ECOG performance status 0 vs. 1 Ryan C, et al. American Society of Clinical Oncology Congress 2012; Abstract LBA4518.
11 Overall Survival (%) COU-302: Abiraterone in docetaxel-naïve CRPC patients Radiographic progression-free survival (rpfs) Overall survival (Final analysis) HR 0.43 (95% CI: ; P < ) HR (95% CI): 0.81 ( ) p Value: Abiraterone, 34.7 mos AA + P PL + P Abiraterone acetate Control Prednisone, 30.3 mos Abiraterone acetate Placebo Time to Death (Months) Ryan C, et al. N Engl J Med 2013 Ryan C et al., Lancet Oncol 2015

12 Cou-302: Safety Profile Abiraterone (n = 542) % Prednisone (n = 540) % All Grades Grade 3/4 All Grades Grade 3/4 Fluid retention/edema Hypokalemia Hypertension Cardiac disorders Atrial fibrillation ALT increased AST increased ALT, alanine aminotransferase; AST, aspartate aminotransferase September 2014, Madrid, Spain esmo.org
 Placebo per qd (n = 399) * 1 docetaxel (glucocorticoids were allowed but not required) Recruitment in 156 centres from 15 countries across 5 continents between September 2009 and")
13 AFFIRM: Enzalutamide in mcrpc patients post-chemotherapy AFFIRM is a phase III randomised, double-blind, placebo-controlled trial mcrpc 1 2 prior chemotherapy regimens* (n = 1,199) R 2:1 Enzalutamide 160 mg qd (n = 800) Placebo per qd (n = 399) * 1 docetaxel (glucocorticoids were allowed but not required) Recruitment in 156 centres from 15 countries across 5 continents between September 2009 and November 2010 Scher HI et al. N Engl J Med 2012; 367(13): mcrpc, metastatic castrate-resistant prostate cancer; qd, once per day; R, randomisation
14 Survival (%) AFFIRM: Overall survival HR = 0.63 (95%CI: ); p< % reduction in risk of death Enzalutamide: 18.4 months (95% CI: 17.3 NYR) Placebo: 13.6 months (95% CI: ) 4.8 month difference in median overall survival N o at risk: Enzalutamide, n = Placebo, n = Duration of overall survival (months) Scher HI et al. N Engl J Med 2012; 367(13): CI, confidence interval; HR, hazard ratio; NYR, not yet reached
15 AFFIRM: Summary of adverse events Adverse events, n (%) Total events (all grades) Enzalutamide (n = 800) Placebo (n = 399) Grade 3 events Enzalutamide (n = 800) Placebo (n = 399) 1 Adverse event 785 (98) 390 (98) 362 (45) 212 (53) Any serious adverse event 268 (34) 154 (39) 227 (28) 134 (34) Discontinuation due to adverse event 61 (8) 39 (10) 37 (5) 28 (7) Adverse event leading to death 23 (3) 14 (4) 23 (3) 14 (4) Adverse events of interest, n (%) Fatigue 269 (34) 116 (29) 50 (6) 29 (7) Cardiac disorder (any) 49 (6) 30 (8) 7 (1) 8 (2) Myocardial infarction 2 (<1) 2 (<1) 2 (<1) 2 (<1) LFT abnormality* 8 (1) 6 (2) 3 (<1) 3 (<1) Seizure 5 (<1) 0 5 (<1) 0 LFT, liver function test *abnormalities on LFT included hyperbilirubinaemia and increased levels of aspartate aminotransferase or alanine aminotransferase The adverse event reporting period for the Enzalutamide group was more than twice that for the placebo group Scher HI et al. N Engl J Med 2012; 367(13):
 832 Placebo 801 305 79 128 34 5 1 0 20 5 0 0 0 Beer T,")
16 Radiographic Progression-Free Survival (%) Prevail: Enzalutamide in docetaxel-naïve mcrpc patients 100 Hazard Ratio: (95% CI: 0.15,0.23) P < Enzalutamide Placebo Radiographic Progression-Free Survival (Months) 832 Placebo Beer T, N Engl J Med 2014; 371:
17 Prevail: safety of Enzalutamide pre-docetaxel Enzalutamide (n=871) All Grades (%) Grade 3 events (%) Placebo (n=844) Enzalutamide (n=871) Placebo (n=844) Fatigue Back pain Constipation Arthralgia Cardiac AEs Hypertension ALT increased Seizure
18 Comparison between 302 & PREVAIL Overall Study Design COU-AA-302 PREVAIL Number of pts 1,088 1,717 Conditions Treatment Primary endpoints Secondary endpoints Design Locations Progressive chemo-naïve mcrpc Asymptomatic/mildly symptom No visceral mets AA+ Prednisone Prednisone rpfs OS Time to opiate use Time to initiation of chemotherapy Time to ECOG-PS deterioration TTPP multicenter, randomized, doubleblind, placebo-controlled 151 sites in 12 countries (USA EU Australia Canada) Progressive chemo-naïve mcrpc Asymptomatic/mildly symptom Visceral mets allowed ENZA (Steroid is allowed) Placebo (Steroid is allowed) rpfs OS Time to initiation of chemotherapy Time to 1st SRE multicenter, randomized, doubleblind, placebo-controlled 207 sites in 22 countries (USA EU Australia Canada Asia including Japan ) Stratification ECOG PS 0 vs. 1

19 Short response to ADT predicts poor response to Enzalutamide (post-docetaxel) PSA decrease 50% PFS 8% 58% P<0.001 TTCRPC Loriot Y et al., Eur J Cancer 2015
20 Treatment decision making in CRPC: several obvious situations History of seizure Enzalutamide Visceral metastases Radium-223 Patient too old/sick Taxanes Contra-indication to steroids (severe diabetes, etc) Abiraterone
21 Drug-drug interactions with enzalutamide Enzalutamide = powerful CYP3A4 inducer and a moderate CYP2C9 and CYP2C19 inducer: Avoid Cabazitaxel, Be careful with many drugs (zolpidem, fentanyl, clopidrogel, lovastatin, triazolam, amiodarone, etc) CYP2C8 induces Enzalutamide metabolism into its active metabolite and its elimination: Avoid CYP2C8 inhibitors (gemfibrozil) and inducers (rifampicine) Avoid any drug that increases the risk of seizure (anti-depressors, neuroleptics, tramadol)
22 Drug-drug interactions with abiraterone Abiraterone = CYP 2C8 inducer (ex: pioglitazone, anti-diabetes: AUC increased x 1.5) Abiraterone= CYP 2D6 inhibitor (ex: dextromethorphan: AUC is increased x 3, thioridazine=melleril) Abiraterone is a substrate of CYP 3A4: theoretically, be careful with strong CYP3A4 inducers (rifampicine). No effect of ketoconazole
23 How to best treat mcrpc? Earlier treatment? Sequential treatments? Combinations? Personalized treatments?
24 How to best treat mcrpc? Ealier treatment Sequential treatments Combinations Personalized treatments
25 Who Dies of Prostate Cancer? Upfront localized cancer 44% of deaths Metastases Death De novo metastases 56% of deaths Patrikidou A. Prostate Cancer Prostatic Dis. 2014;17:



26 Randomization 1:1 LATITUDE: study design Randomized, double-blind, active-controlled, multicentre, phase 3 study Patients de novo mhnpc Meets at least 2 of 3 highrisk criteria Gleason score 8 Presence of 3 lesions on bone scan Presence of measurable visceral lesion ADT + abiraterone Abiraterone 1000 mg QD + Prednisone 1,000 mg 5 q.d. mg QD + ADT + prednisone 5 mg q.d. Placebo 1000 mg QD + Placebo 5 mg QD + ADT ADT + placebos q.d. Efficacy endpoints Primary: Primary OS endpoints rpfs OS Secondary: rpfs Time to next skeletalrelated event Time to PSA progression mhnpc, metastatic hormone naive prostate cancer; q.d., once daily; rpfs, radiographic progression-free survival. Fizazi K, N Engl J Med 2017; 377:
27 LATITUDE: Abiraterone in mcspc 38% risk reduction of death 53% risk reduction of progression/death Overall survival rate at 3 years: ADT + AA + P: 66% ADT + placebos: 49% Median follow-up: 30.4 months Fizazi K, N Engl J Med 2017; 377:
28 EMA approval
29 Stampede Abiraterone James ND, N Engl J Med 2017
30 LATITUDE: Prespecified Secondary and Exploratory End Points ADT+AA+P (n = 597) ADT+place bos (n = 602) Hazard Ratio (95% CI) P Value* Secondary end points Time to pain progression mo NR ( ) < Time to PSA progression mo ( ) < Time to next symptomatic skeletal event mo NR NR 0.70 ( ) Time to chemotherapy mo NR ( ) < Time to subsequent prostate cancer therapy mo NR ( ) < Exploratory end point Patients with a PSA response (decline 50% from baseline) % ( ) * < Fizazi K, N Engl J Med 2017; 377:
31 Patients without worst fatigue progression (%) Mean change from baseline in worst fatigue score (BFI) Addition of Abiraterone to ADT significantly improved fatigue: PROs from LATITUDE 35% Risk Reduction for Worst Fatigue Progression Mean Change From Baseline Differed from Cycle 5 Onward ADT + AAP, NR 0.2 Worse 60 ADT + Placebos, NR HR 0.65 (95% CI, ) P = Better Patients at risk ADT + AAP Months Cycle* ADT + Placebos ADT + AAP ADT + Placebos *1 cycle = 28 days. PRO, patient reported outcomes. Chi K, et al. Data presented at ESMO 2017 (abstract 7830).
32 An indirect comparison to determine the relative efficacy of Abiraterone vs Docetaxel in mhspc Posterior Density: OS - Main Analysis Posterior Density: rpfs - Main Analysis HR (95% CrI): 0.85 (0.63, 1.14) P (HR < 1) = 86.7% HR (95% CrI): 0.71 (0.49, 1.02) P (HR < 1) = 96.8% Analyses suggest that ADT + AAP has greater reduction in risk of progression and death vs ADT + Doc CrI, credible interval; P, Bayesian probabilities. Feyerabend S, et al. Data presented at ESMO 2017 (abstr 803P).
33 Abiraterone or docetaxel? Direct comparison from STAMPEDE Favours SOC+AAP Favours SOC+DocP Head-to-head data in 566 pts (Nov-2011 to Mar-2013) Failure-free survival Progression-free survival Metastatic progression-free survival Strong evidence favouring AAP Weak evidence favouring AAP Symptomatic skeletal events Cause-specific survival Overall survival No good evidence of a difference Proportionately different time spent in each disease state Hazard ratio Toxicity profiles quite different and well known Sydes M, et al. Data presented at ESMO (abstract LBA31).
34 PEACE-1: European Phase III Trial in de novo Metastatic Prostate Cancer (revised design) SOC Patients with newly diagnosed (castration-naïve) metastatic CaP 1156 pts planned R A N D O M I Z E D SOC + Abiraterone 1000 mg Prednisone 5 mg BID SOC + Local radiotherapy Co-primary endpoints: OS and PFS (HR: 0.75) SOC + Local radiotherapy + Abiraterone-Pred Standard of Care (SOC)= Androgen deprivation therapy (ADT) +/- docetaxel (Stratification) ClinicalTrials.gov. Identifier: NCT Study sponsor: Unicancer

 until")
35 ENZAMET Screening Randomisation 1:1 Enzalutamide 160mg/daily + LHRHA (or orchidectomy) until progression Eligibility Metastatic prostate cancer Starting 1 st line ADT Adequate organ function Stratification Comorbidities Volume of disease Study site Bone anti-resorptive therapy Use of early docetaxel Non-steroidal anti-androgen + LHRHA (or orchidectomy) until progression
36 Who Dies of Prostate Cancer? Upfront localized cancer 44% of deaths Metastases Death De novo metastases Patrikidou A. Prostate Cancer Prostatic Dis. 2014;17:
37 Phase III trials in M0 CRPC Atrasentan (n=941) Zibotentan (n=1421) Denosumab (n=1432) Miller K, Prostate Cancer Prostatic Dis 2013; 16: Nelson JB, Cancer 2008; 113: Smith MR, Lancet 2012; 379: 39-46

38 PROSPER Trial Design: Enzalutamide in M0 CRPC Hussain M et al. ASCO Poster TPS5094

39 AR targeting works!
 Antagonism WT AR IC50 (nm)")
 8 25 600 No CYP inhibition or")


40 ODM-201 has a unique profile enzalutamide 19%* ODM main metabolite 3% ** ARN %* Compound AR affinity Ki (nm) Antagonism WT AR IC50 (nm) Proliferation VCaP IC50 (nm) enzalutamide ARN ODM ORM (main metabolite) No CYP inhibition or induction with therapeutic doses Fizazi K et al., ECC2013 poster E *Refs. Clegg et al, Cancer Research 2012; Forster at al, Prostate 2011 ** Rat autoradiography (QWBA confirms brain/plasma ratio of 14C-ODM-201 related radioactivity was , indicating negligible penetration to the brain
: PSA response")


41 ODM-201 and ARN-509 (AR inhibitors): PSA response ARN-509 ODM-201 No chemotherapy Chemotherapy Smith MR et al. ASCO GU 2013, Abstract # LBA 7 Fizazi K, Lancet Oncol 2014; 15:
42 How to best treat mcrpc? Earlier treatment Sequential treatments Combinations Personalized treatments
43 Should We Keep Using Old Hormonal Manipulations Before Using Next-generation AR-Targeting Drugs?

")



44 TERRAIN Study Design Patient population 375 men with progressive mcrpc Asymptomatic/mild ly symptomatic Chemotherapy naive No requirement for steroids TERRAIN trial: NCT R A N D O M I Z E D 1:1 ENZA 160 mg/day n = 184 BIC 50 mg/day n = 191 Primary endpoint Progression-free survival (PFS) Radiographic progression (central review) Skeletal-related event Change in new antineoplastic therapy Death Statistical design The final analysis was planned at 220 progression events with 85% power to detect a target hazard ratio of 0.67 (assuming a median PFS of 9 months vs 6 months 1 ) The data cutoff date was 19 October 2014, with 240 events for the primary efficacy endpoint Secondary endpoints PSA response Time to PSA progression Shore ND, Lancet Oncol 2016; 17:
45 Patients without PFS event (%) Progression-Free Survival in TERRAIN ENZA Patients at risk BIC Patients at risk Median (95% CI): 5.8 months (4.8, 8.1) Median (95% CI): 15.7 months (11.5, 19.4) Time (months) ENZA BIC Hazard ratio (95% CI): 0.44 (0.34, 0.57); P < Shore ND, Lancet Oncol 2016; 17:
46 Percentage Change in PSA from Baseline PSA Response by Week 13 with ENZA or BICA ENZA BIC BICA ENZA PSA response: 21% Observations PSA response: 82% Shore ND, Lancet Oncol 2016; 17:
47 STRIVE trial: Enzalutamide vs Bicalutamide in early CRPC n=396 pts (M0=139; M1=257 Composite PFS: HR= 0.24 (95% CI, 0.18 to 0.32; P <.001) Median PFS: 19.4 months Enza vs 5.7 months Bica Penson DP, J Clin Oncol 2016; 34:
48 Patients without degradation (%) Terrain: Quality of life Patients at risk : Enzalutamide Bicalutamide Time to QoL deterioration (FACT-P) Time (months) Bicalutamide : Median = 8.5 mo (IC95% : ) Enzalutamide : Median = 13.8 mo (IC95% : ) HR=0.64 (IC95% : ) ; p= Shore N. et al, Lancet Oncol 2016; 17:
49 CRPC progressing on abiraterone or enzalutamide: How to treat?
50 Cross-resistance between abiraterone and enzalutamide Author ENZ ABI Year published N pts Duration of 2 nd treatment PSA 50% Median PFS Loriot et al mo 8% 2.7 mo Noonan et al wks 3% 3.6 mo ABI ENZ Schrader et al mo 29% - Badrising et al mo 21% - Bianchini et al mo 23% - Schmid et al mo 10% - Brasso et al mo 18% - Zhang T et al. Expert Opin Pharmacotherap 2014;16:1-9
51 Réduction maximale du PSA (%) Docetaxel post-abiraterone (COU-302) PSA response rate=47% TTP: 7.6 months Flaig T, ASCO GU 2016 De Bono J, Eur Urol 2016

52 Cabazitaxel post-abiraterone (and post-docetaxel) n=79 pts PSA response>30%: 62% PSA response>50%: 35% PFS: 4.4 mo OS: 11 mo In vitro: Caba active against both enza-s and enza-r cells PSA response Al Nakouzi N, Eur Urol 2015; 68:
53 A proposed decision tree for metastatic CRPC Majority of patients (If drug availaible) mcrpc - Cancer progression - Testo<0.50 ng/ml (2017) Abiraterone or Enzalutamide Patients who experience progression after a short ADT period Progression: Docetaxel (Switch to Enza?) (Radium-223?) Docetaxel Progression: Cabazitaxel Radium-223 Denosumab (or ZA), Vit D/Calcium, Supp. care Progression: consider: Cabazitaxel Abiraterone Enzalutamide Radium-223 mcrpc patient initially treated with ADT + Docetaxel??? Fizazi K, Eur J Cancer 2016; 66:
54 Decrease Increase PSA response for CRPC pts treated with docetaxel according to primary treatment for M1 Decrease Increase Best PSA variation (%) during the treatment (n= 80) Best PSA variation (%) during the treatment (n= 29) Docetaxel for CRPC if upfront ADT alone Docetaxel for CRPC if upfront ADT+Doce Lavaud P, Eur Urol 2017
55 PSA response for CRPC pts treated with abiraterone/enzalutamide when treated upfront with ADT+Docetaxel for M1 Best PSA variation (%) during the treatment (n= 15) 100 Decrease Increase Lavaud P, Eur Urol 2017
56 How to best treat mcrpc? Earlier treatment Sequential treatments Combinations Personalized treatments
57 Combining drug X to docetaxel: a failing strategy so far Doc + Oblimersen Doc + DN-101 Doc + Bevacizumab Doc + VEGF-Trap Doc + Lenalidomide Doc + Atrasentan Doc + Zibotentan Doc + GVAX Doc + Dasatinib Doc + Custirsen Negative Phase III trials
58 PSA change (%) PSA Change (%) Abiraterone + Enzalutamide Phase I-II trial PSA 50 decline in 78% 30% Redunction: of patients 87%(52/60) (47 out of 60) PSA 90 decline in 50% Redunction: of patients 77%(46/60) (30 out of 60) 90% Redunction: 47%(28/60) PSA 0.1 ng/ml in 13% of patients (8 out of 60) Exploratory: association of lack of PSA decline with resistance (p=0.008) Efstathiou E, ASCO 2014
59 Current combination strategies (ongoing Phase III) Abiraterone + Enzalutamide (US) Abiraterone + ARN-509 (ACIS) Abiraterone + Radium-223 (ERA) Enzalutamide + Radium-223 (PEACE-3)
60 How to best treat mcrpc? Earlier treatment Sequential treatments Combinations Personalized treatment
61 Success stories of Personalized Medicine Breast cancer: Trastuzumab in HER2 + tumors (Slamon, N Engl J Med 2001, 344: ) Colo-rectal cancer: Cetuximab in K-ras wt tumors (Karapetis CS, N Engl J Med 2008; 359: ) Wild type K-ras Mutated K-ras Non-small cell lung cancer: Crizotinib in Alk+ tumors (Shaw AT, ESMO 2012, Abstr 2862) PFS Crizotinib Chemotherapy
62 AR splice variants Nuclear localization domain N-Terminal Domain DNA binding domain Ligand Binding domain AR splice variants (V7) Splice variant -> AR constitutively active (no need for androgens)
63 PSA change, % * * * * CTCs: AR-V7 is a promising predictor of treatment response Abiraterone Enzalutamide Taxanes PSA response rate: AR-V7 positive: 0% (95% CI: 0-46%) AR-V7 negative: 68.0% (95% CI: 46-85%) P= AR-V7 positive * * * AR-V7 negative PSA response rate: AR-V7 positive: 0% (95% CI: 0-26%) AR-V7 negative: 52.6% (95% CI: 29-76%) P= Docetaxel, n=30 Cabazitaxel, n=7 PSA response rate: AR-V7 positive: 41% (95% CI: 18-67%) AR-V7 negative: 65% (95% CI: 41-85%) P=0.19 Antonarakis ES et al. N Engl J Med 2014;371: ; Antonarakis ES et al. JAMA Oncol 2015; 1:582-91
 Romanel A, Science Trans")
64 AR gains and mutations are associated with primary resistance to next generation AR axis targeted agents (Abiraterone) Romanel A, Science Trans Med 2015

65 Association between AR aberrations (cfdna) and PFS on Enzalutamide Wyatt AW, JAMA Oncol 2016

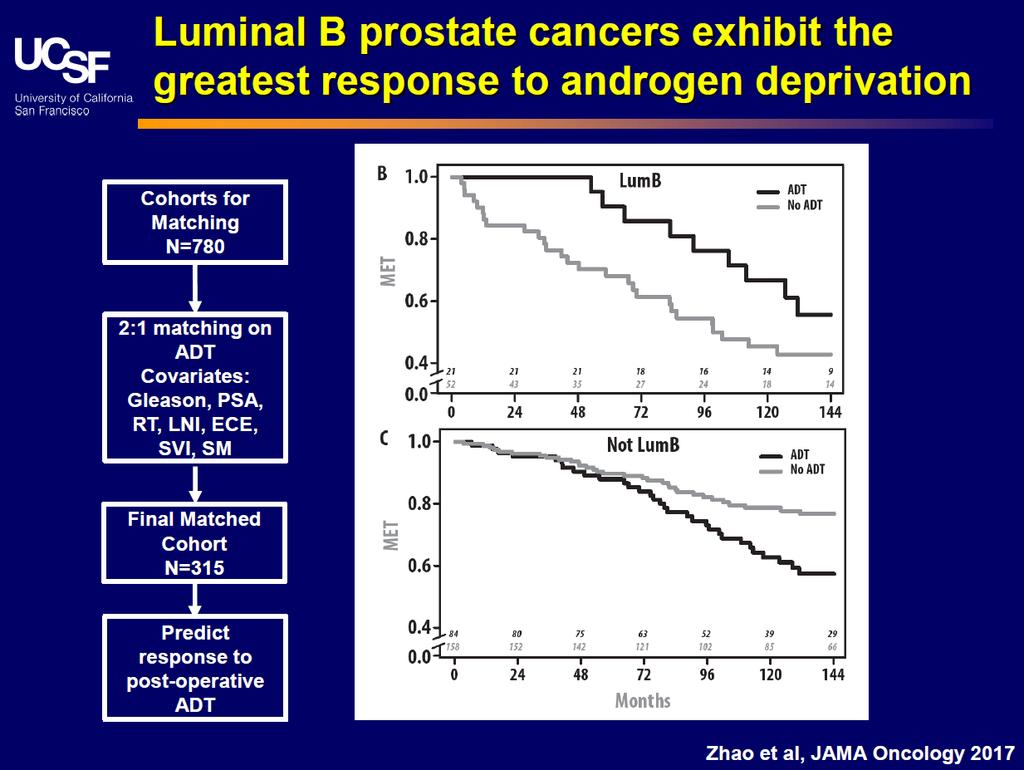
66 Zhao et al., JAMA Oncol 2017
67
68 Conclusion Sequential treatment still routinely used for CRPC, combination remains experimental The field is changing in 2017: M1 CSPC: Abiraterone M0 CRPC: Enzalutamide Cross-resistance between Abi and Enza (20% responders) but Taxanes still active after abi/enza Biomarkers clearly emerging
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer?
 Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Perspective on endocrine and chemotherapy agents. Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
What will change for men with advanced prostate cancer in the next 24 months? ESO Observatory: Perspective on endocrine and chemotherapy agents
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering
 > Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
> Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC
 Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Metastatic castrate-resistant prostate cancer: Toward a chronic disease
 Metastatic castrate-resistant prostate cancer: Toward a chronic disease Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France General recommendations in CRPC Check serum Testosterone (should
Metastatic castrate-resistant prostate cancer: Toward a chronic disease Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France General recommendations in CRPC Check serum Testosterone (should
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Until 2004, CRPC was consistently a rapidly lethal disease.
 Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
 Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Chemioterapia: quando e a chi? Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Chemioterapia: quando e a chi? Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
ESMO SUMMIT AFRICA Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit
 ESMO SUMMIT AFRICA 2018 Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche Merck Lilly 14 years of
ESMO SUMMIT AFRICA 2018 Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche Merck Lilly 14 years of
Institut Gustave Roussy, University of Paris Sud, Villejuif, France. Queen Elizabeth Hospital, Birmingham, United Kingdom
 An open-label, phase I/II safety, pharmacokinetic, and proof-of concept study of ODM-201 in patients with progressive metastatic castration-resistant prostate cancer (CRPC) K Fizazi 1, P Bono 2, R J Jones
An open-label, phase I/II safety, pharmacokinetic, and proof-of concept study of ODM-201 in patients with progressive metastatic castration-resistant prostate cancer (CRPC) K Fizazi 1, P Bono 2, R J Jones
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC
 Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Group Sequential Design: Uses and Abuses
 Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Evolution or revolution in the treatment of prostate cancer
 Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
8/31/ ) Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases
 Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases") Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
ESMO SUMMIT MIDDLE EAST 2018
 ESMO SUMMIT MIDDLE EAST 2018 14 Years of progress in Prostate Cancer Standards of Care and new targets Name Ronald de Wit 6-7 April 2018, Dubai, UAE CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche
ESMO SUMMIT MIDDLE EAST 2018 14 Years of progress in Prostate Cancer Standards of Care and new targets Name Ronald de Wit 6-7 April 2018, Dubai, UAE CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Hormonal Manipulations in CRPC. NW Clarke Professor of Urological Oncology Manchester UK
 Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
Advanced Prostate Cancer. Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options
 Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Non metastatic castrate-resistant prostate cancer (M0 CRPC) Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France") Non metastatic castrate-resistant prostate cancer (M0 CRPC) Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium for: Amgen, Astellas,
Non metastatic castrate-resistant prostate cancer (M0 CRPC) Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium for: Amgen, Astellas,
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi?
 ADT e Terapia ormonale: quando e a chi?") Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi? Paolo Andrea Zucali Dipartimento di Oncologia HUMANITAS CANCER CENTER Rozzano - Milano AGENDA Literature
Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi? Paolo Andrea Zucali Dipartimento di Oncologia HUMANITAS CANCER CENTER Rozzano - Milano AGENDA Literature
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS
 UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Management of castrate resistant disease; after first line hormone therapy fails
 Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE
 NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE S.S. Oncologia Medica Genitourinaria Outline 1. Clinical case 2. Chemotherapy
NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE S.S. Oncologia Medica Genitourinaria Outline 1. Clinical case 2. Chemotherapy
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer. Michal Mego
 National Cancer Institute, Slovakia Translational Research Unit Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer Michal Mego 2 nd Department of Oncology, Faculty
National Cancer Institute, Slovakia Translational Research Unit Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer Michal Mego 2 nd Department of Oncology, Faculty
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
mcrpc in 2016 How to decide the optimal treatment? N. Mottet
 mcrpc in 2016 How to decide the optimal treatment? N. Mottet Disclosures Conflict of interest Chairman EAU PCa guidelines..... Therefore I'm 100% biased Castrate-resistant prostate cancer (CRPC) Definition
mcrpc in 2016 How to decide the optimal treatment? N. Mottet Disclosures Conflict of interest Chairman EAU PCa guidelines..... Therefore I'm 100% biased Castrate-resistant prostate cancer (CRPC) Definition
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Castrate-resistant prostate cancer: Bone-targeted agents. Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Castrate-resistant prostate cancer: Bone-targeted agents Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for: Amgen, Astellas,
Castrate-resistant prostate cancer: Bone-targeted agents Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for: Amgen, Astellas,
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
Please consider the following information on ZYTIGA (abiraterone acetate). ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017
. ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017") Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
- La Terapia Farmacologica -
 XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
Anti-Androgen Therapies for Prostate Cancer: A Focused Review
 Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Management of chronic pre-existing or treatment-emergent adverse events of the other systemic therapies. Michael J. Morris, MD
 Management of chronic pre-existing or treatment-emergent adverse events of the other systemic therapies Michael J. Morris, MD www.mskcc.org Disclosures Research funding (institutional contracts): Sanofi
Management of chronic pre-existing or treatment-emergent adverse events of the other systemic therapies Michael J. Morris, MD www.mskcc.org Disclosures Research funding (institutional contracts): Sanofi
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
SUMMARY. 3. Emerging understanding of mechanisms of resistance to current treatments
 SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
 Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors The Treatment Plan for Patients With Advanced Prostate Cancer: Where Do
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors The Treatment Plan for Patients With Advanced Prostate Cancer: Where Do
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Bone-targeted therapies for prostate cancer in Institut Gustave Roussy Villejuif, France
 Bone-targeted therapies for prostate cancer in 2012 Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards or speaker for: Amgen, Astellas-Medivation,
Bone-targeted therapies for prostate cancer in 2012 Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards or speaker for: Amgen, Astellas-Medivation,
SEQUENCING IN METASTATIC PROSTATE CANCER TREATMENT
 SEQUENCING IN METASTATIC PROSTATE CANCER TREATMENT Eleni Maragkouli, Medical Oncologist Oncology Department The University of Thessaly, Medical School University Hospital of Larissa, Greece Tumour volume
SEQUENCING IN METASTATIC PROSTATE CANCER TREATMENT Eleni Maragkouli, Medical Oncologist Oncology Department The University of Thessaly, Medical School University Hospital of Larissa, Greece Tumour volume
Present and Future Perspectives in Treatment of mcrpc Patients
 Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
ADVANCES IN METASTATIC HORMONE-SENSITIVE PROSTATE CANCER. ALICIA K. MORGANS, MD, MPH Associate Professor of Medicine Northwestern University, USA
 ADVANCES IN METASTATIC HORMONE-SENSITIVE PROSTATE CANCER ALICIA K. MORGANS, MD, MPH Associate Professor of Medicine Northwestern University, USA MAY 2018 DISCLAIMER Please note: The views expressed within
ADVANCES IN METASTATIC HORMONE-SENSITIVE PROSTATE CANCER ALICIA K. MORGANS, MD, MPH Associate Professor of Medicine Northwestern University, USA MAY 2018 DISCLAIMER Please note: The views expressed within
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
Developmental Therapeutics for Genitourinary Malignancies
 Developmental Therapeutics for Genitourinary Malignancies Russell Szmulewitz, MD April 2018 Disclosure Information 23 rd Annual Developmental Therapeutics Symposium Name of Speaker I have the following
Developmental Therapeutics for Genitourinary Malignancies Russell Szmulewitz, MD April 2018 Disclosure Information 23 rd Annual Developmental Therapeutics Symposium Name of Speaker I have the following
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc
 SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE
 mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE. Daan De Maeseneer, Medisch Oncoloog
 PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Dr. Tia Higano University of Washington Seattle, USA
 AN UPDATE ON THE TREATMENT OF PATIENTS WITH mcrpc WITH RA-223 PLUS AAP Dr. Tia Higano University of Washington Seattle, USA AAP, Abiraterone Acetate and Prednisone/Prednisolone; mcrpc, metastatic Castration-Resistant
AN UPDATE ON THE TREATMENT OF PATIENTS WITH mcrpc WITH RA-223 PLUS AAP Dr. Tia Higano University of Washington Seattle, USA AAP, Abiraterone Acetate and Prednisone/Prednisolone; mcrpc, metastatic Castration-Resistant
Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena
 Il Trattamento della Malattia CRPC metastatica Terapie Radiometaboliche Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena AIOM: Gestione ottimale del Paziente con Carcinoma della
Il Trattamento della Malattia CRPC metastatica Terapie Radiometaboliche Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena AIOM: Gestione ottimale del Paziente con Carcinoma della
Published on The YODA Project (
 Principal Investigator First Name: David Last Name: Lorente Degree: MD Primary Affiliation: Medical Oncology Service, Hospital Provincial de Castellón E-mail: lorente.davest@gmail.com Phone number: +34
Principal Investigator First Name: David Last Name: Lorente Degree: MD Primary Affiliation: Medical Oncology Service, Hospital Provincial de Castellón E-mail: lorente.davest@gmail.com Phone number: +34
Sergio Bracarda MD, Medical Oncology, Dept. Of Oncology Az. Ospedaliera S. Maria, Terni; Italy. Milano, 2 marzo 2019
 Sergio Bracarda MD, Medical Oncology, Dept. Of Oncology Az. Ospedaliera S. Maria, Terni; Italy Milano, 2 marzo 2019 My Disclosure Adv. Board Member for: Pfizer, BMS, Novartis, MSD, Roche, Genentech, Astellas,
Sergio Bracarda MD, Medical Oncology, Dept. Of Oncology Az. Ospedaliera S. Maria, Terni; Italy Milano, 2 marzo 2019 My Disclosure Adv. Board Member for: Pfizer, BMS, Novartis, MSD, Roche, Genentech, Astellas,
Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy).
.") Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
SIMPOSIO. Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico
 SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
Sequencing treatment for metastatic prostate cancer
 11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
 Prostata: Oral Communications Emerging strategies and controversial topics in advanced prostate cancer Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
Prostata: Oral Communications Emerging strategies and controversial topics in advanced prostate cancer Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223
 SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
Convegno Nazionale AIOM Giovani 2016: News in Oncology. Daniele Alesini. Istituto Nazionale dei Tumori Regina Elena
 Convegno Nazionale AIOM Giovani 2016: News in Oncology Daniele Alesini Istituto Nazionale dei Tumori Regina Elena Something Old Something New Something Borrowed Something Blue DOCETAXEL: BACK AND FORTH
Convegno Nazionale AIOM Giovani 2016: News in Oncology Daniele Alesini Istituto Nazionale dei Tumori Regina Elena Something Old Something New Something Borrowed Something Blue DOCETAXEL: BACK AND FORTH
Ongoing trials that might change the standard of care in mcrpc
 Ongoing trials that might change the standard of care in mcrpc Igor Tsaur University Medicine Mainz COI Off-label use of drugs, devices, or other agents: none Data from IRB-approved human research is presented:
Ongoing trials that might change the standard of care in mcrpc Igor Tsaur University Medicine Mainz COI Off-label use of drugs, devices, or other agents: none Data from IRB-approved human research is presented:
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Navigating Prostate Cancer Therapy. Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA
 Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Review of the Stampede Results. Charles Ryan MD University of California San Francisco
 Review of the Stampede Results Charles Ryan MD University of California San Francisco Se#ng and hypothesis Se
Review of the Stampede Results Charles Ryan MD University of California San Francisco Se#ng and hypothesis Se
Cancer de la prostate: best of 2016
 Cancer de la prostate: best of 2016 Dr Christophe Massard GR2016, 3 DEC 2016 Disclosure Participation to advisory boards, speaker or investigator for: Amgen, Astellas, Astra Zeneca, Bayer, Celgene, Genentech,
Cancer de la prostate: best of 2016 Dr Christophe Massard GR2016, 3 DEC 2016 Disclosure Participation to advisory boards, speaker or investigator for: Amgen, Astellas, Astra Zeneca, Bayer, Celgene, Genentech,
LATITUDE and other coordinates in quality of life of prostate cancer patients
 Editorial LATITUDE and other coordinates in quality of life of prostate cancer patients Maria Lucia Reale 1,2, Consuelo Buttigliero 1,2, Marcello Tucci 1,2, Rosario F. Di Stefano 1,2, Francesca Vignani
Editorial LATITUDE and other coordinates in quality of life of prostate cancer patients Maria Lucia Reale 1,2, Consuelo Buttigliero 1,2, Marcello Tucci 1,2, Rosario F. Di Stefano 1,2, Francesca Vignani
Michiel H.F. Poorthuis*, Robin W.M. Vernooij*, R. Jeroen A. van Moorselaar and Theo M. de Reijke
 First-line non-cytotoxic therapy in chemotherapynaive patients with metastatic castration-resistant prostate cancer: a systematic review of 10 randomised clinical trials Michiel H.F. Poorthuis*, Robin
First-line non-cytotoxic therapy in chemotherapynaive patients with metastatic castration-resistant prostate cancer: a systematic review of 10 randomised clinical trials Michiel H.F. Poorthuis*, Robin
R&D Presentation for Investors after FY2016
 R&D Presentation for Investors after FY2016 Disclaimer This presentation contains forward-looking statements which involve risks and uncertainty factors. These statements are not based on historical facts
R&D Presentation for Investors after FY2016 Disclaimer This presentation contains forward-looking statements which involve risks and uncertainty factors. These statements are not based on historical facts
Targeting the Androgen Receptor in Prostate Cancer. Raoul S. Concepcion, MD,FACS FDUS/Colorado Springs August 2017
 Targeting the Androgen Receptor in Prostate Cancer Raoul S. Concepcion, MD,FACS FDUS/Colorado Springs August 2017 Consultant: GHI, CUSP, Tolmar, Integra Connect, Cellay, AZ Speakers Bureau: Dendreon, Astellas,
Targeting the Androgen Receptor in Prostate Cancer Raoul S. Concepcion, MD,FACS FDUS/Colorado Springs August 2017 Consultant: GHI, CUSP, Tolmar, Integra Connect, Cellay, AZ Speakers Bureau: Dendreon, Astellas,
STAMPEDE trial (MRC PR08): Arm J overview. Enzalutamide and abiraterone comparison and trial update
: Arm J overview. Enzalutamide and abiraterone comparison and trial update") STAMPEDE trial (MRC PR08): Arm J overview Enzalutamide and abiraterone comparison and trial update Arm J Hypotheses and rationale STAMPEDE: Hypothesis Will addition of enzalutamide and abiraterone to standard-of-care
STAMPEDE trial (MRC PR08): Arm J overview Enzalutamide and abiraterone comparison and trial update Arm J Hypotheses and rationale STAMPEDE: Hypothesis Will addition of enzalutamide and abiraterone to standard-of-care
Evolution of Chemotherapy for. Cancer
 Evolution of Chemotherapy for Hormone Refractory Prostate t Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology Princess Margaret Hospital and University of Toronto In 1985, two
Evolution of Chemotherapy for Hormone Refractory Prostate t Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology Princess Margaret Hospital and University of Toronto In 1985, two
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most