PERIPHERAL NEUROPATHIES
|
|
|
- Nickolas Rodgers
- 5 years ago
- Views:
Transcription



1 PERIPHERAL NEUROPATHIES DIAGNOSIS AND TREATMENT Stefanie Geisler, MD Assistant Professor Neuromuscular Division Department of Neurology Washington University Saint Louis
2 Financial disclosures Funding: NIH Thompson Family Foundation ICTS Inventor on patent to use SARM1 dominant-negative to block axonal degeneration
3 Goals How to clinically stratify to determine who would benefit from specialty consultation How to treat symptoms of painful peripheral neuropathy
4 Patient 1 58 yo man USOH until 3 years ago: tingling in toes bilaterally and increased slowly involving more parts of his feet over the next two years About 6 months ago: Gait slower Fell in the yard, because of ankle rolling Current symptoms: Tingling to mid-shin bilaterally Gait difficulties Mild balance problems Negative for symptoms in arms/hands, pain, autonomic symptoms, weight changes
5 Patient 1 PMH: HTN, anxiety SH: used to smoke 1 PPD for 20 yrs, stopped in 1999; drinks alcohol occasionally, no recreational drugs; no toxin exposure FH: mother: lung cancer, sister breast cancer Examination: Normal VS Normal general exam
6 Patient 1 Normal cranial nerves Motor: Muscle bulk normal normal tone Right Left Deltoid 5/5 5/5 Biceps 5/5 5/5 Triceps 5/5 5/5 Wrist extension 5/5 5/5 Hand muscles 5/5 5/5 Iliopsoas 5/5 5/5 Quadriceps 5/5 5/5 Hamstrings 5/5 5/5 Tibialis anterior 4/5 4/5 Gastrocnemius 5/5 5/5 Toe extension 4/5 4/5
7 Patient 1 Sensation: Light touch: intact Pinprick: cannot feel PP on the right to his mid-foot afterwards pinprick gradient; cannot feel PP on the left at the toes, afterwards gradient Vibration: Right Left Toe 0/8 trace ankle 6/8 3/8 knee 6/8 4.5/8 Coordination (Finger-Nose-Finger, Heel-Knee-Shin, Romberg): intact
8 Patient 1 Reflexes: Right Left Biceps Triceps Brachioradial Patella Ankle absent absent Gait: was able to get up on his toes briefly, could not walk on heels, could not tandem
9 Patient 1 Summary: 58 year old man with 3 year history of tingling and 6 mo history of gait abnormalities and imbalance. On neurological examination, he has severely reduced vibration sense distally, a pin prick gradient in his legs, absent ankle reflexes and distal weakness of his feet. Clinical diagnosis: Sensorimotor peripheral polyneuropathy
10 Overview Peripheral Neuropathy Anatomy Symptoms Diagnosis Symptomatic treatment
11 Peripheral Neuropathy Estimated 20 million people in USA alone suffer from peripheral neuropathy

12 Peripheral nervous system - Anatomy Motor Sensory

13 Autonomic Peripheral nervous system
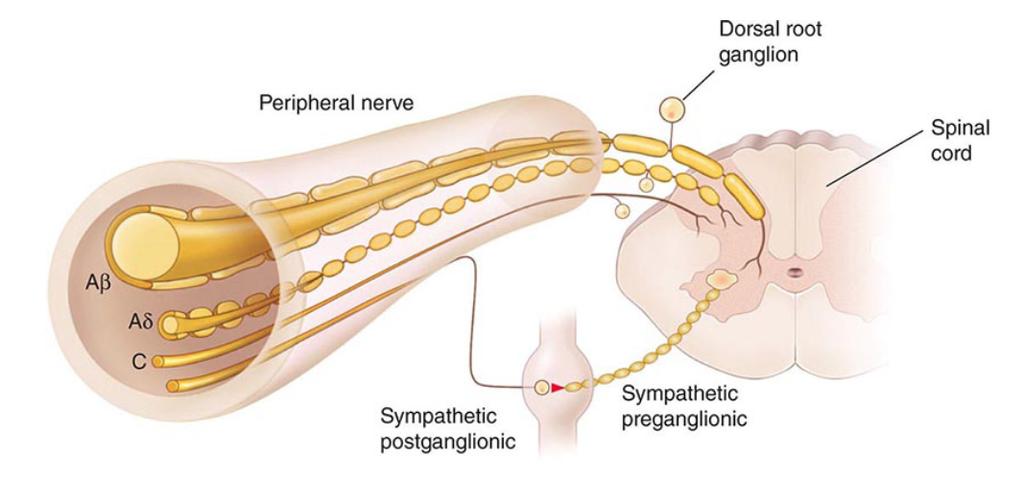
14 Peripheral Nerve
15 Peripheral Nerve Fiber Type CV m/s Neuro exam A alpha A beta Muscle afferent, efferent; Sensory Muscle afferent; Sensory Muscle reflexes Light touch Vibration Proprioception A gamma 40 Muscle efferent; Sensory A delta 20 Free nerve endings of touch and pressure Nociceptors Cold thermoceptors Preganglionic autonomic function C fibers 2 Nociceptors Warmth receptors Postganglionic autonomic function Pain Light touch Temperature Pain Light touch temperature Pin prick Temperature
16 Length dependent sensorimotor peripheral neuropathies - 74% to 82% of cases are length dependent, sensory predominant - At least 1/3 idiopathic - Progress slowly - Unlikely to cause severe physical disability
17 Length-dependent sensorimotor peripheral neuropathy Characteristics: From distal to proximal: Feet first, when leg symptoms approach knee, hand involvement Ascending Symmetric Slowly progressive Sensory symptoms usually precede motor weakness




18 Symptoms: Length-dependent sensorimotor peripheral neuropathy A) Positive symptoms Tingling Abnormal sensation Pain burning, lanciating Allodynia B) Negative symptoms Numbness
19 Length-dependent sensorimotor peripheral neuropathy Imbalance Distal muscle weakness (tripping, falling, difficulties opening bottles, turning door knobs) Autonomic symptoms: Dry eyes/mouth Constipation/diarrhea Early satiety Lightheadedness/orthostasis Erectile dysfunction Urinary incontinence Abnormalities in sweating (hyper/hypohidrosis)
20 Peripheral Sensorimotor Neuropathy Stratifying Length dependent Length independent Multifocal Red flags: Significant weakness Length independent (symptoms in hands first or hands and feet at same time) Multifocal Prominent autonomic symptoms (e.g., anhidrosis)
21 Examination - Cranial nerves - Motor: tone strength: especially distally - Sensation: - light touch, vibration, proprioception - Pin prick, temperature - Romberg - Reflexes - Gait
22 Stratifying - Specialty consultation - Multifocal neuropathy (hand drop and foot drop) - Pure motor or autonomic symptoms - Severe or diffuse sensory neuropathies causing gait ataxia and proprioceptive dysfunction - Acute onset - Fast progressive - Clinical uncertainty
23 Length dependent sensorimotor peripheral neuropathy Causes: Diabetes mellitus Chemotherapy Dysproteinemia HIV Metabolic Endocrine Toxins Small vessel disease alcohol
 - Serum and urine immunofixation (10%) Others: -CBC, CMP, TSH, ESR Rare: - Lyme, Celiac (anti tissue transglutaminase), copper (bariatric surgery), Vitamin E, toxic")
24 -Highest yield serological testing: - Screen for diabetes melllitus (11%) - Vitamin B12 with methylmalonic acid (3.6%) - Serum and urine immunofixation (10%) Others: -CBC, CMP, TSH, ESR Rare: - Lyme, Celiac (anti tissue transglutaminase), copper (bariatric surgery), Vitamin E, toxic (heavy metals), autoimmune (ANA, ANCA, ENA, cryoglobulin)
25 Evaluation Nerve conduction studies/emg Confirm diagnosis Localize Affected modalities (sensory/motor) Axonal/demyelinating Severity Decrease of SNAP amplitude first (sural, superficial peroneal), followed by reduced CMAP amplitude
26 Length-dependent sensorimotor peripheral neuropathy - Nerve conduction studies/emg Decrease of sensory nerve action potential (SNAP) amplitude first (sural, superficial peroneal), followed by reduced compound muscle action potential (CMAP) amplitude Nerve conduction velocity can be normal or mildly slowed (>70% LLN) EMG with signs of distal denervation (foot muscles)
27 Nerve conduction velocity Axon loss
28 Nerve conduction velocity Axon loss
29 Nerve conduction velocity Axon loss
30 Nerve conduction velocity Axon loss
31 Length-dependent sensorimotor peripheral neuropathy Symptomatic management Foot care, properly fitted footwear, monitor feet Neuropathic pain (burning, pins and needles, electrical, allodynia): Gabapentin 300 mg PO TID; max: 3600 mg/day Pregabalin (Lyrica) 75 mg PO BID; max: 300 mg PO BID Tricyclic antidepressants: Amitriptyline 100 mg PO qpm; max: 150 mg/d Nortriptyline Duloxetine (Cymbalta) 60 mg PO daily Venlafaxine (Effexor) Topicals: Lidocaine (5%) cream or ointment
32 Patient 1 Laboratory testing: Serum IF: IgG kappa monoclonal protein, free kappa light chain monoclonal protein Low IgG, IgA, IgM levels Kappa free light chain: 242 ( ); kappa/lambda ratio: ( ) No lytic lesions on skeletal survey Bone Marrow biopsy: Diagnosis: Multiple Myeloma
33 66 yo man Patient 2 USOH until 6 months ago (Octoboer) could walk about 2 miles, was physically active End of October: Numbness around his left ankle 2-3 weeks later numbness 3 fingers L hand 3 weeks later right ankle numbness and L foot weakness Increasingly balance problems, starts to walk with a cane 2 weeks later difficulties getting up from his seated position Noticed muscles in lower legs were gone, had great difficulties walking, started to use a walker for walking Over time, numbness increased to his calves One month ago: weakness in his hands (difficulties cutting food eating, handwriting)
34 Stratification 1. Is it a length dependent neuropathy? 2. Is it symmetrical? 3. Red flags?
35 Patient 2 PMH: HTN, GERD Meds: NC SH: does not drink alcohol, no drugs, no toxin exposure FH: PD and dementia
36 Patient 2 Exam VS nml, General exam nml Neuro: CN normal Motor: Normal tone
37 Patient 2 Exam Right Left deltoids 5/5 5/5 biceps 5/5 5/5 triceps 5/5 5/5 wrist extension 5/5 5/5 FDI 4/5 4/5 APB 5/5 4/5 iliopsoas 5/5 5/5 quadriceps 5/5 5/5 hamstrings 5/5 5/5 tibialis anterior 2/5 2/5 gastrocnemius 4-/5 5-/5 foot eversion 0/5 0/5 foot inversion 0/5 0/5
38 Patient 2 Exam Sensation: Light touch: intact Pinprick: intact Proprioception intact on the right, moderately impaired on the left Vibration sense: Right Left Toes trace 1/8 Ankle 2/8 1/8 Knee 5/8 5/8 Finger 5/8 5/8 Elbow 5.5/8 7/8
39 Patient 2 - Exam Coordination: No Romberg testing possible Reflexes Right Left Biceps 0 1+ Triceps 0 0 Brachioradial 0 0 Patella 0 0 Ankle 0 0
40 Patient 2 - Exam Gait: Requires a walker to walk High steppage gait
41 Patient 2 - Summary Six month history of progressive, asymmetrical, distal predominant weakness and numbness On neurological examination he has severe weakness in his feet and mild to moderate weakness in his hands. In addition he has decreased reflexes throughout and decreased vibration sense with no changes in pinprick sensation
42 Patient 2 Differential diagnosis? What to do next diagnostically?
43 Patient 2 - NCS/EMG Absent tibial and peroneal CMAPs Absent sural, median and ulnar SNAPs Conduction velocities: between 19.9 to 35.6 m/s
44 Patient 2 - NCS/EMG Absent tibial and peroneal CMAPs Absent sural, median and ulnar SNAPs Conduction velocities: between 19.9 to 35.6 m/s Diagnosis: acquired, mixed axonal and demyelinating sensorimotor peripheral neuropathy.
45 Chronic inflammatory demyelinating plyradiculopathy (CIDP) Symptoms and signs of neuropathy progressive for at least 2 months Progressive, symmetric proximal and distal weakness of arms and legs (increasing difficulty rising from a chair, going upstairs, opening jars Sensory-motor Exam: Particularly large fiber modalities involved (vibration) Hypo or areflexia (4 limbs) Sensory ataxia, gait imbalance
46 Chronic inflammatory demyelinating plyradiculopathy (CIDP) Can be pure sensory (MAG) Cranial neuropathy Mild facial weakness Ophthalmoparesis Dysarthria Dysphagia Hearing loss vertigo
47 CIDP electrophysiological testing 3 out of 4 criteria must be met: Reduction in conduction velocity in two or more motor nerves: <80% of lower limit of normal if amplitude is >80% of LLN <70% of lower limit of normal if amplitude is <80% of LLN (generally <30 m/s in legs, and <36 m/s in arms) Conduction block Prolonged distal latencies Absent F waves in two or more nerves
48 CIDP Laboratory Features CSF: Mandatory: normal cell count (<10), supportive: elevated protein (>45 mg/dl) 80-95% of patients Up 25% monoclonal gammopathy MRI: enhancement of nerve roots
49 Medical conditions associated with CIDP HIV DM Inflammatory bowel disease MGUS Paraneoplastic POEMS Lymphoma Small cell carcinoma of the lung Carcinoma of pancreas, colon BM and organ transplantation
50 Progressive proximal, distal or both paresis and reduced tendon reflexes Duration <2 months Duration > 2 months Ephys may be normal first 1-2 weeks Ephys for signs of demyelination Lsb, including CSF Other family members with similar symtpoms Ephys and CSF criteria fulfilled and no evidence of another cause of PNP Ephys and supportive CSF criteria fulfilled Guillain-Barre- Syndrome Start treatment for CIDP Signs of demyelination in sural nerve biopsy Consider hereditary neuorpathy
51 CIDP - Treatment Corticosteroids Oral or IV IV: 1000 mg/day Solu-Medrol IV for 3-5 days 1000 mg IV weekly for 1-2 months, then slowly down-titrate IVIG 2g/kg over 2-5 days (e.g., 0.4 g/kg/d) 1g/kg q 2 weeks to 6 weeks Referral to Neurology Plasma exchange Immune modulators
52 Patient 3 67 yo woman with DM and diabetes-associated neuorpathy Noticed sudden onset of numbness of digits 4 and 5 of right hand Over next two months numbness increased Weakness and atrophy ulnar 3 months later tripping over her left toes Left wrist drop and numbness One week later acute onset left foot drop
53 Stratification Length dependent? Symmetric?
54 Patient 3 Exam: asymmetric weakness: hand right(0/5) > left 4/5) Foot: left (0/5) > right (5/5) Decreased sensation to PP, LT entire right hand, thereafter normal Patchy decrease of all modalities L arm, and both legs DTRs: 2+ upper extremities and patella, absent ankle reflexes
55 Red flags Patient 3
56 Patient 3 Further testing: Positive ANCA Vasculitis on skin biopsy Immune features on biopsy of posterior cutaneous radial nerve Diagnosis: Mononeuritis multiplex Treatment: IV steroids and Azathioprine Outcome: got strength back in feet (5/5), walks unaided; full strength left hand, weakness right thumb
57 Patient 4 47 yo man in his USOH until 5 yrs ago Avid runner Decreased sweating while running (none over legs and his socks remain dry) Overheating while running core body temperature up to 101F Other symptoms: Dry eyes (Restasis) Dry mouth (chews gum) Constipation and diarrhea Early satiety No numbness, tingling, weakness
58 Patient 4 Normal VS, normal general exam Normal cranial nerves Normal motor exam Sensation: Intact to LT, PP, vibration Coordination: intact Gait normal
59 Autonomic testing: RR interval Sympathetic skin response Sweat test Skin biopsy
60 Patient 4 Sweat test abnormal in patchy distribution Decreased intra-epidermal nerve fibers Diagnosis: Autonomic neuropathy
61 Autonomic neuropathy Diabetes mellitus Hereditary Amyloidosis (+weakness) GBS (+weakness) Paraneoplastic Idiopathic Immune mediated
62 Patient 4 Despite extensive and repeated work-up no cause identified Treatment with steroids and IVIG was unsuccessful Symptomatic treatment
63 Summary Length-dependent, symmetric sensorimotor peripheral neuropathy typically slowly progressive Unlikely to cause severe physical disability Highest yield laboratory testing: DM, VitB12 (with MMA), serum immunofixation Red flags (referral to Neurology) Weakness Asymmetry Length independent/multifocal Rapidly progressive Severe sensory Clinical uncertainty
64 Stefanie Geisler, MD Neuromuscular Division Washington University Saint Louis Phone: (314) Fax: (314)
A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017
 A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017 Disclosures Research support from Cytokinetics, Inc Catalyst, Inc Editorial fees from UptoDate. Objectives Describe
A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017 Disclosures Research support from Cytokinetics, Inc Catalyst, Inc Editorial fees from UptoDate. Objectives Describe
A Tale of Five Demyelinating Neuropathies
 Objectives A Tale of Five Demyelinating Neuropathies Tahseen Mozaffar, MD FAAN Professor and Vice Chair of Neurology Director, UC Irvine-MDA ALS and Neuromuscular Center Director, Neurology Residency Training
Objectives A Tale of Five Demyelinating Neuropathies Tahseen Mozaffar, MD FAAN Professor and Vice Chair of Neurology Director, UC Irvine-MDA ALS and Neuromuscular Center Director, Neurology Residency Training
The Internist s Approach to Neuropathy
 The Internist s Approach to Neuropathy VOLKAN GRANIT, MD, MSC ASSISTANT PROFESSOR OF NEUROLOGY NEUROMUSCU LAR DIVISION UNIVERSITY OF MIAMI, MILLER SCHOOL OF MEDICINE RELEVANT DECLARATIONS Financial disclosures:
The Internist s Approach to Neuropathy VOLKAN GRANIT, MD, MSC ASSISTANT PROFESSOR OF NEUROLOGY NEUROMUSCU LAR DIVISION UNIVERSITY OF MIAMI, MILLER SCHOOL OF MEDICINE RELEVANT DECLARATIONS Financial disclosures:
Evaluation of Peripheral Neuropathy. Evaluation of Peripheral Neuropathy - Introduction
 Evaluation of Peripheral Neuropathy Chris Edwards, MD Ochsner Neurology, Main Campus Evaluation of Peripheral Neuropathy - Introduction A very common complaint in the clinic Presentation is variable Multiple
Evaluation of Peripheral Neuropathy Chris Edwards, MD Ochsner Neurology, Main Campus Evaluation of Peripheral Neuropathy - Introduction A very common complaint in the clinic Presentation is variable Multiple
CIDP + MMN - how to diagnose and treat. Dr Hadi Manji
 CIDP + MMN - how to diagnose and treat Dr Hadi Manji Outline Introduction CIDP Diagnosis Clinical features MRI Nerve conduction tests Lumbar puncture Nerve biopsy Treatment IV Ig Steroids Plasma Exchnage
CIDP + MMN - how to diagnose and treat Dr Hadi Manji Outline Introduction CIDP Diagnosis Clinical features MRI Nerve conduction tests Lumbar puncture Nerve biopsy Treatment IV Ig Steroids Plasma Exchnage
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
A/Professor Arun Aggarwal Balmain Hospital
 A/Professor Arun Aggarwal Balmain Hospital Nerve Conduction Studies Test to evaluate the function of motor / sensory nerves Evaluate Paraesthesia (numbness, tingling, burning) Weakness of arms and legs
A/Professor Arun Aggarwal Balmain Hospital Nerve Conduction Studies Test to evaluate the function of motor / sensory nerves Evaluate Paraesthesia (numbness, tingling, burning) Weakness of arms and legs
Peripheral Neuropathy. Dr James Stevens Consultant Neurologist Southmead Hospital, Bristol
 Dr James Stevens Consultant Neurologist Southmead Hospital, Bristol Declaration of interests Aims and objectives A 57 year old textile worker reports pins and needles in her hands, following a fall at
Dr James Stevens Consultant Neurologist Southmead Hospital, Bristol Declaration of interests Aims and objectives A 57 year old textile worker reports pins and needles in her hands, following a fall at
Differential Diagnosis of Neuropathies and Compression. Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre
 Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Peripheral Neuropathies
 Peripheral Neuropathies ELBA Y. GERENA MALDONADO, MD ACTING ASSISTANT PROFESSOR UNIVERSITY OF WASHINGTON MEDICAL CENTER Objectives Definition Neurophysiology Evaluation of polyneuropathies Cases Summary
Peripheral Neuropathies ELBA Y. GERENA MALDONADO, MD ACTING ASSISTANT PROFESSOR UNIVERSITY OF WASHINGTON MEDICAL CENTER Objectives Definition Neurophysiology Evaluation of polyneuropathies Cases Summary
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists
 & electromyography (EMG) for non-neurologists") Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Some observations we are making
 Some observations we are making The audience is very smart and they know how to diagnose a neuropathy. There is a standard workup that all patients seem to get: B12, folate, RPR, TSH prior to them being
Some observations we are making The audience is very smart and they know how to diagnose a neuropathy. There is a standard workup that all patients seem to get: B12, folate, RPR, TSH prior to them being
Jonathan Katz, MD CPMC
 Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC First, a bit of background Classic CIDP--TREATABLE MADSAM/Asymmetric Neuropathy Chronic Length Dependent Neuropathy-
Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC First, a bit of background Classic CIDP--TREATABLE MADSAM/Asymmetric Neuropathy Chronic Length Dependent Neuropathy-
ACUTE AND CHRONIC NEUROPATHIES
 ACUTE AND CHRONIC NEUROPATHIES American College of Osteopathic Internists Internal Medicine Board Review Course 2018 April 25-29, 2018 Marriott Chicago Downtown Chicago, Illinois Scott Spradlin D.O.,FACP,FACOI
ACUTE AND CHRONIC NEUROPATHIES American College of Osteopathic Internists Internal Medicine Board Review Course 2018 April 25-29, 2018 Marriott Chicago Downtown Chicago, Illinois Scott Spradlin D.O.,FACP,FACOI
Nerve Conduction Studies and EMG
 Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
DISCLOSURES. UCSF Continuing Medical Education Neuropathy Pearls. Overview. Neuropathy terminology. Topics to be covered:
 UCSF Continuing Medical Education DISCLOSURES Nothing to Disclose Laura K. Rosow, MD Overview Topics to be covered: Neuropathy definitions, terminology Evaluation of the patient with neuropathy History
UCSF Continuing Medical Education DISCLOSURES Nothing to Disclose Laura K. Rosow, MD Overview Topics to be covered: Neuropathy definitions, terminology Evaluation of the patient with neuropathy History
Doc, DO I Have Neuropathy?
 Doc, DO I Have Neuropathy? Stanley Jones P. Iyadurai, MSc, PhD, MD Assistant Professor of Neurology Neuromuscular Division, Department of Neurology The Ohio State University Wexner Medical Center Case
Doc, DO I Have Neuropathy? Stanley Jones P. Iyadurai, MSc, PhD, MD Assistant Professor of Neurology Neuromuscular Division, Department of Neurology The Ohio State University Wexner Medical Center Case
Immune Mediated Neuropathies
 Immune Mediated Neuropathies Hernan Gatuslao, M.D. Assistant Professor Department of Neurology Virginia Commonwealth University School of Medicine AIDP and CIDP Acute inflammatory demyelinating polyneuropathy
Immune Mediated Neuropathies Hernan Gatuslao, M.D. Assistant Professor Department of Neurology Virginia Commonwealth University School of Medicine AIDP and CIDP Acute inflammatory demyelinating polyneuropathy
Painful Diabetic Neuropathy Effective Management. Ketan Dhatariya Consultant in Diabetes NNUH
 Painful Diabetic Neuropathy Effective Management Ketan Dhatariya Consultant in Diabetes NNUH Neuropathic Pain Prevalence varies between 10 and 90% depending on classification Accounts for 50-75% of non-traumatic
Painful Diabetic Neuropathy Effective Management Ketan Dhatariya Consultant in Diabetes NNUH Neuropathic Pain Prevalence varies between 10 and 90% depending on classification Accounts for 50-75% of non-traumatic
Making sense of Nerve conduction & EMG
 Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Nerve Site Latency ms Amplitude mv Distance mm Conduction Velocity m/s
 Clinical Electrophysiology Instructions and Sample Reports NCS/EMG REPORT Date: August 2007 Reason for Electrophysiologic Referral: Bilateral upper extremity pain and numbness. History: 59 year-old female
Clinical Electrophysiology Instructions and Sample Reports NCS/EMG REPORT Date: August 2007 Reason for Electrophysiologic Referral: Bilateral upper extremity pain and numbness. History: 59 year-old female
Table 1: Nerve Conduction Studies (summarised)
") Table 1: Nerve Conduction Studies (summarised) Sensory nerve conduction 1 week* 3 months Superficial radial sensory Normal, symmetric SNAP and CV No change Median to digit II Normal, symmetric SNAP and
Table 1: Nerve Conduction Studies (summarised) Sensory nerve conduction 1 week* 3 months Superficial radial sensory Normal, symmetric SNAP and CV No change Median to digit II Normal, symmetric SNAP and
Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype Five Years after Initial Diagnosis
 Case Reports in Neurological Medicine Volume 2013, Article ID 356157, 4 pages http://dx.doi.org/10.1155/2013/356157 Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype
Case Reports in Neurological Medicine Volume 2013, Article ID 356157, 4 pages http://dx.doi.org/10.1155/2013/356157 Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype
Doctor, I have dizzy feet! Evaluation of patients with suspected neuropathy
 Doctor, I have dizzy feet! Evaluation of patients with suspected neuropathy Causes of chronic polyneuropathy Signs and symptoms Large fiber modalities Ataxia esp. in the dark Are you ok in the shower
Doctor, I have dizzy feet! Evaluation of patients with suspected neuropathy Causes of chronic polyneuropathy Signs and symptoms Large fiber modalities Ataxia esp. in the dark Are you ok in the shower
Peripheral neuropathy (PN)
") Peripheral neuropathy (PN) damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic:
Peripheral neuropathy (PN) damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic:
sensory nerves, motor nerves, autonomic nerves
 damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: long term, begins subtly
damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: long term, begins subtly
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
DIAGNOSIS OF DIABETIC NEUROPATHY
 DIAGNOSIS OF DIABETIC NEUROPATHY Dept of PM&R, College of Medicine, Korea University Dong Hwee Kim Electrodiagnosis ANS Clinical Measures QST DIAGRAM OF CASUAL PATHWAYS TO FOOT ULCERATION Rathur & Boulton.
DIAGNOSIS OF DIABETIC NEUROPATHY Dept of PM&R, College of Medicine, Korea University Dong Hwee Kim Electrodiagnosis ANS Clinical Measures QST DIAGRAM OF CASUAL PATHWAYS TO FOOT ULCERATION Rathur & Boulton.
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
Electrodiagnostics for Back & Neck Pain. Steven Andersen, MD Providence Physiatry Clinic
 Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
peripheral neuropathy peripheral neuropathy neuropathy peripheral neuropathy neuropathic foot heel Bilateral foot pain Bilateral heel pain bilateral
 Peripheral neuropathy (PN) is damage to or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health. The 2018 edition of ICD-10-CM G62.9. Auditory
Peripheral neuropathy (PN) is damage to or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health. The 2018 edition of ICD-10-CM G62.9. Auditory
Evaluation of Tingling and Numbness in the Upper Extremities
 Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of
 Peripheral Nervous System Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of non-insulin dependent diabetes
Peripheral Nervous System Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of non-insulin dependent diabetes
Disclosures. Objectives. Clinical Scenario. Four Common Neurological Problems: An Update for /25/2009. None
 Four Common Neurological Problems: An Update for 2009 Disclosures Vanja Douglas, M.D. Clinical Instructor UCSF Department of Neurology, Neurohospitalist Program None Objectives Learn an approach to the
Four Common Neurological Problems: An Update for 2009 Disclosures Vanja Douglas, M.D. Clinical Instructor UCSF Department of Neurology, Neurohospitalist Program None Objectives Learn an approach to the
For convenience values outside the normal range are bolded. Normal values for the specified patient are stated below the tables.
 Case tudy 8 or convenience values outside the normal range are bolded. Normal values for the specified patient are stated below the tables. History: 60 year-ol man with a history of left hand weakness
Case tudy 8 or convenience values outside the normal range are bolded. Normal values for the specified patient are stated below the tables. History: 60 year-ol man with a history of left hand weakness
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Assistant Professor, Department of Neurology Divisions of Neurovascular and Behavioral Neurology University of California San Francisco
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Assistant Professor, Department of Neurology Divisions of Neurovascular and Behavioral Neurology University of California San Francisco
Index. Note: Page numbers of article titles are in boldface type.
 Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases
 Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Diabetic Neuropathy. Nicholas J. Silvestri, M.D.
 Diabetic Neuropathy Nicholas J. Silvestri, M.D. Types of Neuropathies Associated with Diabetes Mellitus p Chronic distal sensorimotor polyneuropathy p Focal compression neuropathies p Autonomic neuropathy
Diabetic Neuropathy Nicholas J. Silvestri, M.D. Types of Neuropathies Associated with Diabetes Mellitus p Chronic distal sensorimotor polyneuropathy p Focal compression neuropathies p Autonomic neuropathy
Symptomatic pain treatments (carbamazepine and gabapentin) were tried and had only a transient and incomplete effect on the severe pain syndrome.
 were tried and had only a transient and incomplete effect on the severe pain syndrome.") Laurencin 1 Appendix e-1 Supplementary Material: Clinical observations Patient 1 (48-year-old man) This patient, who was without a notable medical history, presented with thoracic pain and cough, which
Laurencin 1 Appendix e-1 Supplementary Material: Clinical observations Patient 1 (48-year-old man) This patient, who was without a notable medical history, presented with thoracic pain and cough, which
Case Example. Nerve Entrapments in the Lower limb
 Nerve Entrapments in the Lower limb February, 2013 William S. Pease, M.D. Ernest W. Johnson Professor of PM&R Case Example CC: Right ankle dorsiflexion weakness with minimal paresthesias HPI: 87 year-old
Nerve Entrapments in the Lower limb February, 2013 William S. Pease, M.D. Ernest W. Johnson Professor of PM&R Case Example CC: Right ankle dorsiflexion weakness with minimal paresthesias HPI: 87 year-old
Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM. Andrzej Sladkowski
 Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM Andrzej Sladkowski Potential causes of weakness in the ICU-1 Muscle disease Critical illness myopathy Inflammatory myopathy Hypokalemic
Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM Andrzej Sladkowski Potential causes of weakness in the ICU-1 Muscle disease Critical illness myopathy Inflammatory myopathy Hypokalemic
Electrodiagnostic studies comprising of electromyography (EMG) and nerve
 and nerve") INTRODUCTION AND TERMINOLOGY Electrodiagnostic studies comprising of electromyography (EMG) and nerve conduction studies (NCS) are well-established objective methods for the diagnosis, quantification and
INTRODUCTION AND TERMINOLOGY Electrodiagnostic studies comprising of electromyography (EMG) and nerve conduction studies (NCS) are well-established objective methods for the diagnosis, quantification and
Patogenesi e terapia della Neuropatia Motoria Multifocale
 26 Settembre 2014 Patogenesi e terapia della Neuropatia Motoria Multifocale Francesca Gallia Neurologia 2, Ist. Clin. Humanitas Rozzano, Milano Multifocal Motor Neuropathy Rare disorder characterized by:
26 Settembre 2014 Patogenesi e terapia della Neuropatia Motoria Multifocale Francesca Gallia Neurologia 2, Ist. Clin. Humanitas Rozzano, Milano Multifocal Motor Neuropathy Rare disorder characterized by:
Ahmed Abbas, Mark Cook, Liong Hiew Fu, Alistair Lewthwaite, Colin Shirley, Yusuf A. Rajabally
 2016, Elsevier. Licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International http://creativecommons.org/licenses/by-nc-nd/4.0/ Accepted Manuscript A case of POEMS mimicking
2016, Elsevier. Licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International http://creativecommons.org/licenses/by-nc-nd/4.0/ Accepted Manuscript A case of POEMS mimicking
Clinical Aspects of Peripheral Nerve and Muscle Disease. Roy Weller Clinical Neurosciences University of Southampton School of Medicine
 Clinical Aspects of Peripheral Nerve and Muscle Disease Roy Weller Clinical Neurosciences University of Southampton School of Medicine Normal Nerves 1. Anterior Horn Cell 2. Dorsal root ganglion cell 3.
Clinical Aspects of Peripheral Nerve and Muscle Disease Roy Weller Clinical Neurosciences University of Southampton School of Medicine Normal Nerves 1. Anterior Horn Cell 2. Dorsal root ganglion cell 3.
The High-Yield Neurologic Examination
 The High-Yield Neurologic Examination S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director, Neurohospitalist
The High-Yield Neurologic Examination S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director, Neurohospitalist
BRAIN STEM CASE HISTORIES CASE HISTORY VII
 463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment
 Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment 7 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, HW Van Es, LH Van den Berg Annals of Neurology 2000;
Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment 7 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, HW Van Es, LH Van den Berg Annals of Neurology 2000;
Disclosure. Entrapment Neuropathies - Overview. Common mononeuropathy sites. Definitions. Common mononeuropathy sites. Common mononeuropathy sites
 Disclosure Entrapment Neuropathies - Overview I receive compensation from Wiley- Blackwell publishers for my work as Editor-in-Chief of Muscle & Nerve Lawrence H. Phillips, II, MD Definitions Mononeuropathy:
Disclosure Entrapment Neuropathies - Overview I receive compensation from Wiley- Blackwell publishers for my work as Editor-in-Chief of Muscle & Nerve Lawrence H. Phillips, II, MD Definitions Mononeuropathy:
Clinical and electrophysiologic features of childhood Guillain-Barré syndrome in Northeast China
 Journal of the Formosan Medical Association (2014) 113, 634e639 Available online at www.sciencedirect.com journal homepage: www.jfma-online.com ORIGINAL ARTICLE Clinical and electrophysiologic features
Journal of the Formosan Medical Association (2014) 113, 634e639 Available online at www.sciencedirect.com journal homepage: www.jfma-online.com ORIGINAL ARTICLE Clinical and electrophysiologic features
Neuro Exam Explained
 Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
PMH: No medications; Immunizations UTD No hospitalizations or surgeries Speech Delay. Birth Hx: 24 WGA, NICU x6 months
 HPI: 6 months of weakness and parathesias- originally in both feet x 2-3 months, then resolved. Now with parathesias and weakness in fingers x 1 week. Seen by podiatrist and given custom in-soles 1 month
HPI: 6 months of weakness and parathesias- originally in both feet x 2-3 months, then resolved. Now with parathesias and weakness in fingers x 1 week. Seen by podiatrist and given custom in-soles 1 month
Index. Clin Podiatr Med Surg 23 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Clin Podiatr Med Surg 23 (2006) 667 672 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, electromyography of, in tarsal tunnel syndrome, 537 539 Abductor
Clin Podiatr Med Surg 23 (2006) 667 672 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, electromyography of, in tarsal tunnel syndrome, 537 539 Abductor
How to Do the EDSS. Stephen S. Kamin, MD New Jersey Medical School
 How to Do the EDSS Stephen S. Kamin, MD New Jersey Medical School John F. Kurtzke, MD 1926-2015 EDSS Expanded Disability Status Scale Devised by John Kurtzke in the 1960s and modified in the 1980s EDSS
How to Do the EDSS Stephen S. Kamin, MD New Jersey Medical School John F. Kurtzke, MD 1926-2015 EDSS Expanded Disability Status Scale Devised by John Kurtzke in the 1960s and modified in the 1980s EDSS
Cesarean section for breech presentation. Jonathan H. Waters, M.D.
 Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
Neurological Examination
 Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY?
 Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY? D iabetic neuropathy is actually a group of nerve diseases. All of these disorders affect the peripheral nerves, that is, the nerves that are outside the
Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY? D iabetic neuropathy is actually a group of nerve diseases. All of these disorders affect the peripheral nerves, that is, the nerves that are outside the
This is a repository copy of Anti-MAG negative distal acquired demyelinating symmetric neuropathy in association with a neuroendocrine tumor..
 This is a repository copy of Anti-MAG negative distal acquired demyelinating symmetric neuropathy in association with a neuroendocrine tumor.. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk//
This is a repository copy of Anti-MAG negative distal acquired demyelinating symmetric neuropathy in association with a neuroendocrine tumor.. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk//
A Practical Approach to Peripheral Neuropathy
 A Practical Approach to Peripheral Neuropathy Michelle L. Mauermann M.D. Associate Professor of Neurology Mayo Clinic, Rochester MN 2017 MFMER slide-1 Disclosures None 2017 MFMER slide-2 Learning Objectives
A Practical Approach to Peripheral Neuropathy Michelle L. Mauermann M.D. Associate Professor of Neurology Mayo Clinic, Rochester MN 2017 MFMER slide-1 Disclosures None 2017 MFMER slide-2 Learning Objectives
A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL
 A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL CASE HISTORY Nine year old male child Second born Born
A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL CASE HISTORY Nine year old male child Second born Born
Motor, Reflex, Coordination and Sensory Screening Examination
 Motor, Reflex, Coordination and Sensory Screening Examination K. Jeffrey Miller, DC, DABCO Miller 2002 2002-2012 K Jeffrey Miller DC DABCO Motor Function Neurological Testing Handedness Right or Left Handed
Motor, Reflex, Coordination and Sensory Screening Examination K. Jeffrey Miller, DC, DABCO Miller 2002 2002-2012 K Jeffrey Miller DC DABCO Motor Function Neurological Testing Handedness Right or Left Handed
Distal chronic spinal muscular atrophy involving the hands
 Journal ofneurology, Neurosurgery, and Psychiatry, 1978, 41, 653-658 Distal chronic spinal muscular atrophy involving the hands D. J. O'SULLIVAN AND J. G. McLEOD From St Vincent's Hospital, and Department
Journal ofneurology, Neurosurgery, and Psychiatry, 1978, 41, 653-658 Distal chronic spinal muscular atrophy involving the hands D. J. O'SULLIVAN AND J. G. McLEOD From St Vincent's Hospital, and Department
A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T
 A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T Guillain-Barre Acute inflammatory demyelinating polyneuropathy Highly diverse presentation, course, outcome Miller-Fisher:
A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T Guillain-Barre Acute inflammatory demyelinating polyneuropathy Highly diverse presentation, course, outcome Miller-Fisher:
A Case of Vascular MCI
 A Case of Vascular MCI Charles DeCarli, MD Victor and Genevieve Orsi Chair in Alzheimer s Research Director Alzheimer s Disease Center University of California at Davis Initial Evaluation 78 y.o. Rt. Handed
A Case of Vascular MCI Charles DeCarli, MD Victor and Genevieve Orsi Chair in Alzheimer s Research Director Alzheimer s Disease Center University of California at Davis Initial Evaluation 78 y.o. Rt. Handed
Four Common Neurological Problems: An Update for Vanja Douglas, M.D. Clinical Instructor UCSF Department of Neurology, Neurohospitalist Program
 Four Common Neurological Problems: An Update for 2009 Vanja Douglas, M.D. Clinical Instructor UCSF Department of Neurology, Neurohospitalist Program Disclosures None Objectives Learn an approach to the
Four Common Neurological Problems: An Update for 2009 Vanja Douglas, M.D. Clinical Instructor UCSF Department of Neurology, Neurohospitalist Program Disclosures None Objectives Learn an approach to the
Severe Chronic Inflammatory Demyelinating Polyneuropathy Ameliorated following High-dose (3 g/kg) Intravenous Immunoglobulin Therapy
 Intravenous Immunoglobulin Therapy") doi: 10.2169/internalmedicine.1723-18 http://internmed.jp CASE REPORT Severe Chronic Inflammatory Demyelinating Polyneuropathy Ameliorated following High-dose (3 g/kg) Intravenous Immunoglobulin Therapy
doi: 10.2169/internalmedicine.1723-18 http://internmed.jp CASE REPORT Severe Chronic Inflammatory Demyelinating Polyneuropathy Ameliorated following High-dose (3 g/kg) Intravenous Immunoglobulin Therapy
PERIPHERAL NERVE WORKUP FORM (PNW)
") PERIPHERAL NERVE WORKUP FORM (PNW) The Peripheral Nerve Workup Form (PNW) has to be filled out at the time a new patient is enrolled into the PNRR study. Only testing conducted within 36 months of visit
PERIPHERAL NERVE WORKUP FORM (PNW) The Peripheral Nerve Workup Form (PNW) has to be filled out at the time a new patient is enrolled into the PNRR study. Only testing conducted within 36 months of visit
Cancer Rehabilitation New Patient Intake Form
 _ I. Personal Information Date of Birth Age: Home Address: Home Phone: Cell Phone: Office Phone: Fax: E-Mail: II. Chief Complaint Please describe the major problem that brings you in today: Who referred
_ I. Personal Information Date of Birth Age: Home Address: Home Phone: Cell Phone: Office Phone: Fax: E-Mail: II. Chief Complaint Please describe the major problem that brings you in today: Who referred
FootHuggers Comfort Socks have been found to help people suffering with: Peripheral Neuropathy
 FootHuggers Comfort Socks have been found to help people suffering with: Peripheral Neuropathy Peripheral Neuropathy - Peripheral neuropathy is a term used to describe disorders of your peripheral nervous
FootHuggers Comfort Socks have been found to help people suffering with: Peripheral Neuropathy Peripheral Neuropathy - Peripheral neuropathy is a term used to describe disorders of your peripheral nervous
Wartenberg s migrant sensory neuritis: a prospective follow-up study
 J Neurol (2010) 257:1344 1348 DOI 10.1007/s00415-010-5530-7 ORIGINAL COMMUNICATION Wartenberg s migrant sensory neuritis: a prospective follow-up study Abraham C. J. Stork Marjon F. G. van der Meulen W.-Ludo
J Neurol (2010) 257:1344 1348 DOI 10.1007/s00415-010-5530-7 ORIGINAL COMMUNICATION Wartenberg s migrant sensory neuritis: a prospective follow-up study Abraham C. J. Stork Marjon F. G. van der Meulen W.-Ludo
An Illustrated Guide For Peripheral Nerve Examination. Bedside Teaching for 2 nd year medical Students
 An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
Treatment of multifocal motor neuropathy with interferon-β1a
 Treatment of multifocal motor neuropathy with interferon-β1a 12 MMN RM Van den Berg-Vos, LH Van den Berg, H Franssen, PA Van Doorn, ISJ Martina, JHJ Wokke Adapted from Neurology 2000; 54: 1518-1521. Chapter
Treatment of multifocal motor neuropathy with interferon-β1a 12 MMN RM Van den Berg-Vos, LH Van den Berg, H Franssen, PA Van Doorn, ISJ Martina, JHJ Wokke Adapted from Neurology 2000; 54: 1518-1521. Chapter
Differentialdianosis to CRPS Departmentdoctor Bo Biering-Sørensen, Pain Clinic, Neurological Department
 Differentialdianosis to CRPS Departmentdoctor Bo Biering-Sørensen, Pain Clinic, Neurological Department Dato (Sidehoved/fod) Case 1 36 year old man other ethnically background than Danish 2006 Left foot
Differentialdianosis to CRPS Departmentdoctor Bo Biering-Sørensen, Pain Clinic, Neurological Department Dato (Sidehoved/fod) Case 1 36 year old man other ethnically background than Danish 2006 Left foot
Neurophysiological Diagnosis of Birth Brachial Plexus Palsy. Dr Grace Ng Department of Paed PMH
 Neurophysiological Diagnosis of Birth Brachial Plexus Palsy Dr Grace Ng Department of Paed PMH Brachial Plexus Anatomy Brachial Plexus Cords Medial cord: motor and sensory conduction for median and ulnar
Neurophysiological Diagnosis of Birth Brachial Plexus Palsy Dr Grace Ng Department of Paed PMH Brachial Plexus Anatomy Brachial Plexus Cords Medial cord: motor and sensory conduction for median and ulnar
Comparison of Sudomotor and Sensory Nerve Testing in Painful Sensory Neuropathies
 138 Original Article Comparison of Sudomotor and Sensory Nerve Testing in Painful Sensory Neuropathies James M. Killian, MD,* Shane Smyth, MD,* Rudy Guerra, PhD, Ishan Adhikari, MD,* and Yadollah Harati,
138 Original Article Comparison of Sudomotor and Sensory Nerve Testing in Painful Sensory Neuropathies James M. Killian, MD,* Shane Smyth, MD,* Rudy Guerra, PhD, Ishan Adhikari, MD,* and Yadollah Harati,
Radiculopathy and Polyneuropathy
 Objectives Radiculopathy and Polyneuropathy Jeffrey W. Ralph, MD Jeffrey.Ralph@ucsf.edu UCSF Department of Neurology Advances in Internal Medicine May 24 and June 28, 2012 Radiculopathy Anatomy & Signs
Objectives Radiculopathy and Polyneuropathy Jeffrey W. Ralph, MD Jeffrey.Ralph@ucsf.edu UCSF Department of Neurology Advances in Internal Medicine May 24 and June 28, 2012 Radiculopathy Anatomy & Signs
Supplementary Online Content
 Supplementary Online Content Stevens O, Claeys KG, Poesen K, Veroniek S, Van Damme P. Diagnostic challenges and clinical characteristics of hepatitis E virus associated Guillain- Barré syndrome. JAMA Neurol.
Supplementary Online Content Stevens O, Claeys KG, Poesen K, Veroniek S, Van Damme P. Diagnostic challenges and clinical characteristics of hepatitis E virus associated Guillain- Barré syndrome. JAMA Neurol.
Kim Chong Hwa MD,PhD Sejong general hospital, Division of endocrine & metabolism
 Kim Chong Hwa MD,PhD Sejong general hospital, Division of endocrine & metabolism st1 Classification and definition of diabetic neuropathies Painful diabetic peripheral neuropathy Diabetic autonomic neuropathy
Kim Chong Hwa MD,PhD Sejong general hospital, Division of endocrine & metabolism st1 Classification and definition of diabetic neuropathies Painful diabetic peripheral neuropathy Diabetic autonomic neuropathy
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Journal of Ayurveda and Pharmaceutical Chemistry
 International Journal of Ayurveda and Pharmaceutical Chemistry Volume 7 Issue 2 2017 www.ijapc.com Managed by Green m RESEARCH ARTICLE www.ijapc.com e-issn 2350-0204 Role of an Advanced Diagnostic Technique
International Journal of Ayurveda and Pharmaceutical Chemistry Volume 7 Issue 2 2017 www.ijapc.com Managed by Green m RESEARCH ARTICLE www.ijapc.com e-issn 2350-0204 Role of an Advanced Diagnostic Technique
November 16-18, 2017 Hotel Monteleone New Orleans, LA. Provided by
 November 16-18, 2017 Hotel Monteleone New Orleans, LA Provided by Diabetic Neuropathy: A Global and Growing Problem John D. England, MD Louisiana State University Health Sciences Center School of Medicine
November 16-18, 2017 Hotel Monteleone New Orleans, LA Provided by Diabetic Neuropathy: A Global and Growing Problem John D. England, MD Louisiana State University Health Sciences Center School of Medicine
Is Small-Fiber Neuropathy Killing You?
 Is Small-Fiber Neuropathy Killing You? Presented By: Dr. Greg Fors, DC, DIBCN Board-certified Neurologist (IBCN) Author of the Best-Selling Why We Hurt Maybe Its Small Fiber Sensory NEUROPATHY! Do you
Is Small-Fiber Neuropathy Killing You? Presented By: Dr. Greg Fors, DC, DIBCN Board-certified Neurologist (IBCN) Author of the Best-Selling Why We Hurt Maybe Its Small Fiber Sensory NEUROPATHY! Do you
Peripheral Nerve Disorders - P a g e 1. Introduction
 Peripheral Nerve Disorders - P a g e 1 Introduction The peripheral nerves connect the central nervous system (the brain and the spinal cord) to the periphery (the sensory receptors and muscles). An illness
Peripheral Nerve Disorders - P a g e 1 Introduction The peripheral nerves connect the central nervous system (the brain and the spinal cord) to the periphery (the sensory receptors and muscles). An illness
Gait Disorders. Nicholas J. Silvestri, MD
 Gait Disorders Nicholas J. Silvestri, MD Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Learning Objectives Explain the normal development of gait Describe various gait
Gait Disorders Nicholas J. Silvestri, MD Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Learning Objectives Explain the normal development of gait Describe various gait
Peripheral Neuropathies
 Peripheral Neuropathies Natalie H. Strand, MD Disclosure Nothing to disclose 1 Learning Objectives Describe the pathophysiology of peripheral neuropathies Review the anatomy of the nervous system Describe
Peripheral Neuropathies Natalie H. Strand, MD Disclosure Nothing to disclose 1 Learning Objectives Describe the pathophysiology of peripheral neuropathies Review the anatomy of the nervous system Describe
AN INTERESTING CASE OF PROGRESSIVE QUADRIPARESIS DR SHILPA
 AN INTERESTING CASE OF PROGRESSIVE QUADRIPARESIS DR SHILPA CASE: A 50yr old female, homemaker, hailing from Mandya, Chief complaints 1. Weakness of left upper limb since 9months. 2. Weakness of right upper
AN INTERESTING CASE OF PROGRESSIVE QUADRIPARESIS DR SHILPA CASE: A 50yr old female, homemaker, hailing from Mandya, Chief complaints 1. Weakness of left upper limb since 9months. 2. Weakness of right upper
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
AII-type: Select the most appropriate answer
 AII-type: Select the most appropriate answer ( )1. Choose one best answer for the following pathologic pictures. A. choroid cyst B. choroid papilloma C. pontine glioma D. ependymoma E. metastatic tumor
AII-type: Select the most appropriate answer ( )1. Choose one best answer for the following pathologic pictures. A. choroid cyst B. choroid papilloma C. pontine glioma D. ependymoma E. metastatic tumor
Slide 1. Slide 2. Slide 3. Intro to Physical Therapy for Neuromuscular Conditions. PT Evaluation. PT Evaluation
 Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Balgrist Symposium zum Diabetischen Fuss. Der Charcot-Fuss Oktober diabetic neuropathies. symptoms. signs. sensory disorders.
 symptoms sensory disorders spontaneous paraesthesia tingling burning by touch, pressure dysaesthesia sign pain continuous boring cutting drawing paroxysmal lancinating neuralgiform causalgic fluctuating,
symptoms sensory disorders spontaneous paraesthesia tingling burning by touch, pressure dysaesthesia sign pain continuous boring cutting drawing paroxysmal lancinating neuralgiform causalgic fluctuating,
MOLLOY COLLEGE THE BARBARA H. HAGAN SCHOOL OF NURSING NURSE PRACTITIONER PROGRAMS. Study Guide for the Basic Physical Assessment Exam
 THE BARBARA H. HAGAN SCHOOL OF NURSING S Study Guide for the Basic Physical Assessment Exam Questions will be based on following chapters in, Bickley, L.S. (2016). (12 th ed). Bates guide to physical examination
THE BARBARA H. HAGAN SCHOOL OF NURSING S Study Guide for the Basic Physical Assessment Exam Questions will be based on following chapters in, Bickley, L.S. (2016). (12 th ed). Bates guide to physical examination
FILED: NEW YORK COUNTY CLERK 04/12/ :57 PM INDEX NO /2011 NYSCEF DOC. NO RECEIVED NYSCEF: 04/12/2018
 ' NYNeurological.- 't Associates, P.C. e 3He e a David Dc vld Snyder, M.D. Emilio Oribe, M.D., F.A.C.P Tonya FOtiml, M.D. Yvonne Zoharckis, M,b. www.nynapc.com July 3, 2017 Sabatini 4 Associates 237 West
' NYNeurological.- 't Associates, P.C. e 3He e a David Dc vld Snyder, M.D. Emilio Oribe, M.D., F.A.C.P Tonya FOtiml, M.D. Yvonne Zoharckis, M,b. www.nynapc.com July 3, 2017 Sabatini 4 Associates 237 West
Original Research Article
 NERVE CONDUCTION STUDY IN CHILDREN WITH INSULIN DEPENDENT DIABETES MELLITUS Hannah John, Sahila M 2 Senior Resident, Department of Physiology, Government Medical College, Trivandrum, Kerala, India. 2Professor,
NERVE CONDUCTION STUDY IN CHILDREN WITH INSULIN DEPENDENT DIABETES MELLITUS Hannah John, Sahila M 2 Senior Resident, Department of Physiology, Government Medical College, Trivandrum, Kerala, India. 2Professor,
NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES
 NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES Endorsed by the following organizations - October 2000: American Academy of Neurology Association of University Professors of Neurology American Neurological
NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES Endorsed by the following organizations - October 2000: American Academy of Neurology Association of University Professors of Neurology American Neurological
Update: Plasmapheresis in Neurologic Disorders
 Update: Plasmapheresis in Neurologic Disorders Case Presentation A 62-year-old, right-hand-dominant male presented to the emergency department with a 3-day history of progressive weakness. Initially he
Update: Plasmapheresis in Neurologic Disorders Case Presentation A 62-year-old, right-hand-dominant male presented to the emergency department with a 3-day history of progressive weakness. Initially he
Power Line to your Line to your Circuit Line to the station neighborhood house breaker living room. Outlet lamp Lamp with socket, Light bulb
 IMC 606 Neuroscience and Behavior Module Dr. Margaret Paroski Analysis of Sensory Lesions You walk into your living room and turn on the lamp. But no light comes on. What would you do? You would probably
IMC 606 Neuroscience and Behavior Module Dr. Margaret Paroski Analysis of Sensory Lesions You walk into your living room and turn on the lamp. But no light comes on. What would you do? You would probably
Motor and sensory nerve conduction studies
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Hands-on Course 2 Assessment of peripheral nerves function and structure in suspected peripheral neuropathies
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Hands-on Course 2 Assessment of peripheral nerves function and structure in suspected peripheral neuropathies