Management of Lower Limb Ulcers. D. NAIK MBChB FRACS DDU
|
|
|
- Curtis Horace O’Neal’
- 5 years ago
- Views:
Transcription
1 Management of Lower Limb Ulcers D. NAIK MBChB FRACS DDU
2 Ulcer A defect in the epithelium
3 A failure to heal Ulcer
4 Aetiology of Leg Ulcers Venous insufficiency Macrovascular arterial insufficiency Infectious conditions Vasculitis/Microvascular insufficiency Malignancy Excessive pressure Lymphoedema Collagen vascular disorders Haemotologic abnormalities D Naik MBchB FRACS DDU [Vascular]
5 Venous Ulcers Gaiter area Mild pain Venous ooze Shallow,irregular shape,round edges Granulating base Surrounding inflammation Stasis dermatitis D Naik MBchB FRACS DDU [Vascular]

6 D Naik MBchB FRACS DDU [Vascular]

7
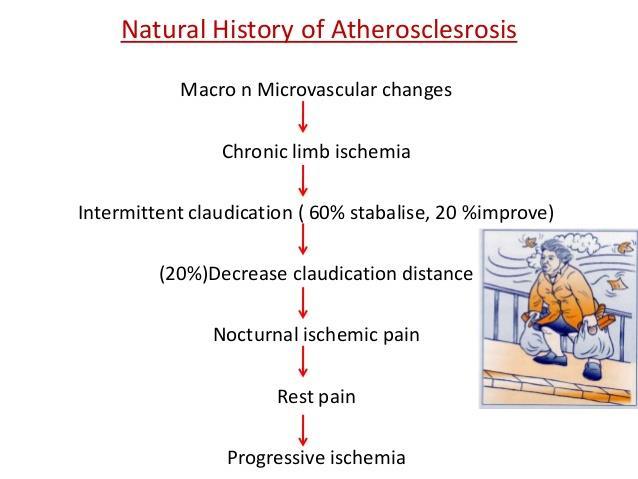
8 Macrovascular arterial Atherosclerosis Posttraumatic Embolic Acute or chronic thrombosis
9 Ischaemic Ulcers Occur distally and over bony prominences Severe pain Little or no bleeding Irregular edge Poor granulation tissue Absent surrounding inflammation Trophic changes Absent pulses and low ABI D Naik MBchB FRACS DDU [Vascular]

10
11 Vasculitis/Microvascular arterial insufficiency Diabetes microangiopathy Hypertensive microangiopathy Thromboangitis obliterans Raynauds disorder

12

13
14 Infectious conditions Bacterial Fungal Mycobacterial Treponemal/spirochaetal
15 Malignancy Basal cell carcinoma Squamous cell carcinoma Malignant melanoma Kaposi s sarcoma Lymphoma Mycosis fungoides

16 Marjolin s ulcer
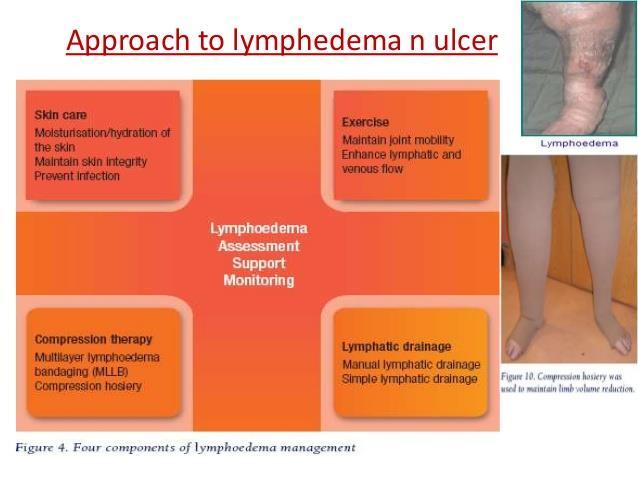
17 Lymphatic obstruction /lymphoedema Venolymphatic disease Primary or secondary lymphatic insufficiency Lymphangiosarcoma

18
19 Haemotologic abnormalities Sickle cell anaemia Polycythaemia Dysproteinaemia
20 Collagen vascular disorders SLE Scleroderma Polyarteritis nodosa Wegeners granulomatosis
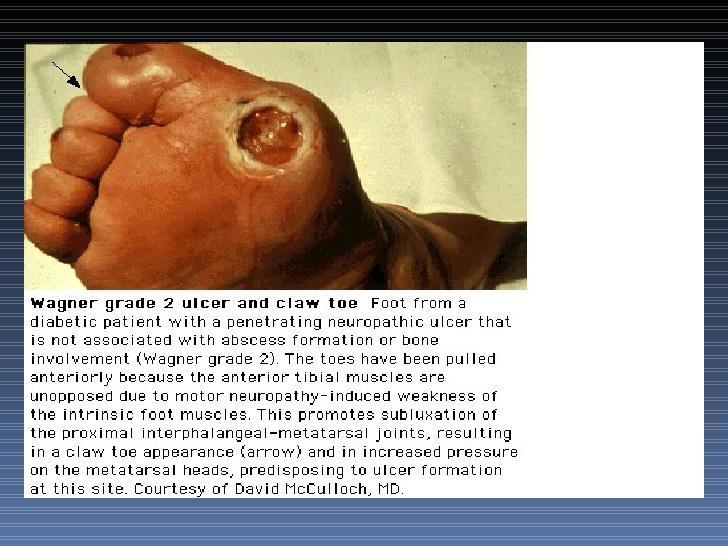
21 Excessive pressure Diabetic neuropathy Alcoholic neuropathy Decubitus ulcer Postoperative deformity Bone spurs
22 Neuropathic Ulcers Under calluses or pressure points Painless Bleeding maybe brisk Punched out,with deep sinus Surrounding inflammation Demonstrable neuropathy D Naik MBchB FRACS DDU [Vascular]
23

24 D Naik MBchB FRACS DDU [Vascular]
25 Management of ulcers History Physical examination Ankle brachial index Blood tests Xrays Vascular investigations Biopsy Management of the underlying condition
26 History Varicose veins Deep venous thrombosis Claudication Rest pain Diabetes Injury Arthritis
27
28
29 Clinical Examination Oedema Surrounding skin Site Pain Ulcer Pulses Stigmata of venous disease Doppler indices D Naik MBchB FRACS DDU [Vascular]

30

31
32

33

34
35 Complications Bleeding Eczema Superficial thrombophlebitis Ulceration Deep vein thrombosis D Naik MBchB FRACS DDU [Vascular]
36 Epidemiology of Venous Ulcers 0.06 and 1% Rising prevalence in elderly Peak prevalence age 70 years F:M ratio 3:1 D Naik MBchB FRACS DDU [Vascular]
37 Risk factors for Venous Ulceration Venous insufficiency Previous DVT Chronic skin changes Local trauma Aggravation by co-existing conditions D Naik MBchB FRACS DDU [Vascular]

38
39
40 Macrovascular Changes Ambulatory venous hypertension
41 Microvascular Changes Pericapillary fibrin deposition Localised microvascular ischaemia White cell adhaerence White cell activation Activity of inflammatory mediators D Naik MBchB FRACS DDU [Vascular]
42 Management of Venous Ulcers General measures Adjuvant pharmacotherapy Compression Dressings Sclerotherapy Endovenous interventions Surgery D Naik MBchB FRACS DDU [Vascular]

43

44
45 Management-General Measures Address needs of the patient as a whole Consider lifestyle,mobility,occupation,nutrition Elevation of legs Prop bed up by 10-15% D Naik MBchB FRACS DDU [Vascular]
46
47 Management - Dressings Choice is a matter of clinical judgement Insufficient clinical trials to allow recommendation D Naik MBchB FRACS DDU [Vascular]
48 The Ideal Dressing Reduce ulcer pain Allow excess exudate to escape Be non-allergenic Easy to change without discomfort Leave no dressing residue Inexpensive Easy to apply D Naik MBchB FRACS DDU [Vascular]
49 Management-Compression Ambulant patients need bandages or stockings mm Hg at ankle Graduated Sustained compression D Naik MBchB FRACS DDU [Vascular]
50 Ideal Compression Bandaging System Gradient of pressure Even pressure over anatomical contours Maintains pressure Remains in position Complements dressing functions Non-irritant and non-allergenic Comfortable Washable D Naik MBchB FRACS DDU [Vascular]
51 Management- Adjuvant Pharmacotherapy Only in addition to compression Agents include :fibrinolytic agents fibrinolysis-enhancing hydroxyrutosides pentoxifylline prostaglandin E systemic antibiotics diuretics D Naik MBchB FRACS DDU [Vascular]
52 Venous Ulceration 50-70% of venous ulceration is secondary to primary varicose veins and is curable with relatively simple venous interventions D Naik MBchB FRACS DDU [Vascular]

53 D Naik MBchB FRACS DDU [Vascular]

54 D Naik MBchB FRACS DDU [Vascular]

55
56 Epidemiology Disease of Western civilisation 10-20% men and 67% of adult women have physically identifiable varicosities Varicose veins range from venectasia or telangiectasia to protuberant tortuous varicosities D Naik MBchB FRACS DDU [Vascular]
57 Primary Varicose Veins Great Saphenous Small Saphenous Perforator veins D Naik MBchB FRACS DDU [Vascular]
58 Secondary Varicose Veins A-V fistula Deep venous obstruction D Naik MBchB FRACS DDU [Vascular]
59 Investigation Duplex scan Venography CT venography D Naik MBchB FRACS DDU [Vascular]
60 Duplex Scanning Combination of ultrasound and Doppler Operator dependent Significantly improved our understanding and management of varicose veins Relatively cheap and non-invasive Mandatory prior to any major intervention D Naik MBchB FRACS DDU [Vascular]

61 D Naik MBchB FRACS DDU [Vascular]

62
63 Management Conservative Sclerotherapy Non-surgical saphenous ablation Chemical Radiofrequency Laser Surgery D Naik MBchB FRACS DDU [Vascular]
64 Conservative treatment Weight loss Exercise Compression hosiery D Naik MBchB FRACS DDU [Vascular]
65 Local Sclerotherapy Simple office procedure Good results in appropriately selected patients May buy time Cheapest option D Naik MBchB FRACS DDU [Vascular]
66 Endovevous intervention Now the gold standard for varicose vein treatment Includes UGS and endovenous ablation Minimally invasive therefore lower threshold for intervention No general anaesthetic therefore suitable for high risk patients Day case local procedures Lower cost
67 Ultrasound Guided Sclerotherapy [UGS] Minimally invasive Poor results in large axial veins Good option in selected patients Systemic effects of sclerosants unknown May require multiple treatments Phlebitis and brown staining an issue Poor long-term results in large axial D Naik MBchB FRACS DDU [Vascular]

68 D Naik MBchB FRACS DDU [Vascular]

69 D Naik MBchB FRACS DDU [Vascular]
70 Endovenous Laser Therapy First described by Bone in 1999 Diode laser forms steam bubbles in blood leading to endothelial damage,coagulative necrosis and thrombotic occlusion of vein Requires tumescent anaesthesia Deals with saphenous trunks only Requires adjunctive procedures for varices Early results favourable Day procedure D Naik MBchB FRACS DDU [Vascular]

71 D Naik MBchB FRACS DDU [Vascular]
72 Radiofrequency Ablation First described by Goldman in 2000 Heat generated by radiofrequency probe causes local heating of vein wall Requires tumescent anaesthesia Deals with saphenous trunks only Requires adjunctive procedures for varices Day procedure D Naik MBchB FRACS DDU [Vascular]
73 Management Surgical Therapy Varicose vein surgery Valvuloplasty Venous cuffs Venous bypass SSG Flaps D Naik MBchB FRACS DDU [Vascular]
74 Surgery Excellent results if performed well Requires anaesthesia,cuts and more recovery Neovascularisation in less than 7% Cutaneous nerve injury and leg swelling are issues Good long-term results Everything treated in one hit Good option in patients with very large varices D Naik MBchB FRACS DDU [Vascular]

75 D Naik MBchB FRACS DDU [Vascular]

76 D Naik MBchB FRACS DDU [Vascular]

77 D Naik MBchB FRACS DDU [Vascular]
78 Complications of Venous Interventions Complicatio ns EVLT RFA SURGERY Bruising Pain Parathesia Phlebitis Haemotom a Burns Infection D Naik MBchB FRACS DDU [Vascular]
79 Management of Varicose Veins UGS EVLT/RF SURGERY Invasion Cost Discomfort Recovery Recurrence +++?? + D Naik MBchB FRACS DDU [Vascular]
80

81
82 There has been a paradigm shift in the management of superficial venous insufficiency with most cases treated with an endovenous approach

83

84
85 Äetiology of Arterial Occlusive Disease Atherosclerosis Emboli Arterial dissection Arteritis Aneurysms Arterial trauma Entrapment syndromes Adventitial cystic disease Vascular tumours D Naik MBchB FRACS DDU [Vascular]

86
87
88
89 Epidemiology of PAD Affects 12-14% of the general population Affects upto 20% of patients over 75 Coexistent coronary artery disease and cerebrovascular disease are highly prevalent in patients with PAD D Naik MBchB FRACS DDU [Vascular]
90 History Location Duration Progress Distance Time for relief Associated rest pain D Naik MBchB FRACS DDU [Vascular]
91 Rest pain Pain felt in the distal forefoot which is exacerbated by elevation
92 Examination Arterial palpation Bruits Pallor Rubor Temperature Tissue loss Integumentary changes ABI D Naik MBchB FRACS DDU [Vascular]

93
94 Management of Arterial Ulcers Duplex scanning Arteriography Angioplasty/stent Vascular reconstruction Debridement Skin grafting D Naik MBchB FRACS DDU [Vascular]

95
96 Interpreting Doppler Readings >1 Normal arterial flow 0.9 Mild degree of arterial involvement 0.8 Lowest level at which compression can be safely applied 0.7 Significant arterial disease is present and full compression should not be used 0.5 Limb is at risk and urgent vascular opinion should be sought D Naik MBchB FRACS DDU [Vascular]
97 Non-invasive Vascular Tests Exercise ABI Toe pressures Pressure studies Duplex scanning Ultrasound Doppler Spectral analysis D Naik MBchB FRACS DDU [Vascular]
98 ABI Right Leg Left Leg Exe rcis e Per iod Rest Minutes Post Exercise D Naik MBchB FRACS DDU [Vascular]

99 D Naik MBchB FRACS DDU [Vascular]
100 Invasive studies CT angiography MR angiography Digital subtraction angiography D Naik MBchB FRACS DDU [Vascular]

101

102

103

104
105 Best Medical Therapy Smoking Antiplatelet therapy Hypertension Diabetes Hyperlipidaemia Statin Cilastozol,Trental Exercise D Naik MBchB FRACS DDU [Vascular]
106 Our Approach We favour an endovascular first policy
107 Endovascular Treatment Angioplasty Stenting Atherectomy Thombolysis D Naik MBchB FRACS DDU [Vascular]

108 D Naik MBchB FRACS DDU [Vascular]
109 Angioplasty Best in big arteries with short stenoses Results below inguinal ligament best in focal lesions Short occlusions Myointimal hyperplasia affects results Greater role in high risk patients Improved technology with drug eluting balloons D Naik MBchB FRACS DDU [Vascular]

110

111 D Naik MBchB FRACS DDU [Vascular]

112
113 Stenting Good long term results in iliac arteries Results below the inguinal ligament less durable Stent fracture an issue in mobile arteries Myointimal hyperplasia and in stent restenosis affect durability Improved technology resulting in better outcomes in high risk patients Drug eluting and biodegradable stents on the horizon D Naik MBchB FRACS DDU [Vascular]

114
115 Surgical Treatment Aortoiliofemoral interventions Femoropopliteal reconstructions Distal arterial reconstruction Sympathectomy Amputation D Naik MBchB FRACS DDU [Vascular]
116 Surgical outcomes Improved outcomes with better peri-operative care and surgical techniques Operative mortality about 2-3 % Synthetic grafts work well in the aorta and iliacs but autologous grafts preferred below the infrainguinal ligament 5 year patency rates about 70-80% and limb salvage rates 80-90% Appropriate work up prior to surgery essential D Naik MBchB FRACS DDU [Vascular]
117 Endovascular or Surgery? BASIL trial Life expectancy greater than 2 years limb salvage greater and mortality lower in surgery patients Role of stenting still undefined but long-term patency and cost effectiveness remain an issue D Naik MBchB FRACS DDU [Vascular]

118 D Naik MBchB FRACS DDU [Vascular]

119 D Naik MBchB FRACS DDU [Vascular]

120 D Naik MBchB FRACS DDU [Vascular]

121 D Naik MBchB FRACS DDU [Vascular]

122 D Naik MBchB FRACS DDU [Vascular]

123 D Naik MBchB FRACS DDU [Vascular]

124 D Naik MBchB FRACS DDU [Vascular]

125 D Naik MBchB FRACS DDU [Vascular]

126 D Naik MBchB FRACS DDU [Vascular]

127 D Naik MBchB FRACS DDU [Vascular]

128 D Naik MBchB FRACS DDU [Vascular]

129 D Naik MBchB FRACS DDU [Vascular]

130 D Naik MBchB FRACS DDU [Vascular]
131

132

133
134
135
136

137

138

139

140
141
142 Ulcers When to refer Pain Infection Absent pulses ABI < 0.8 Refractory ulcers Cellulitis Deteriorating ulcers D Naik MBchB FRACS DDU [Vascular]
143 Conclusion Aetiology of lower limb ulcers is often multifactorial Management of leg ulcers should include an assessment and management of aetiological factors Current management of vascular patients involves tailoring intervention according to the clinical and risk profile of the patient As less invasive management options are available for intervention consideration of early specialist referral is appropriate

144
Management of Lower Limb Ulcers. D. NAIK MBChB FRACS DDU
 Management of Lower Limb Ulcers D. NAIK MBChB FRACS DDU Ulcer A defect in the epithelium Ulcer A failure to heal Aetiology of Leg Ulcers Arterial Venous Neuropathic Vasculitic Infectious Neoplastic Lymphoedema
Management of Lower Limb Ulcers D. NAIK MBChB FRACS DDU Ulcer A defect in the epithelium Ulcer A failure to heal Aetiology of Leg Ulcers Arterial Venous Neuropathic Vasculitic Infectious Neoplastic Lymphoedema
How to manage leg ulcers in the elderly
 How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT
 VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
Chronic Venous Insufficiency Compression and Beyond
 Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
ULCERS 1/12/ million diabetics in the US (2012) Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years
 Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years") Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Priorities Forum Statement
 Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Venous Insufficiency Ulcers. Patient Assessment: Superficial varicosities. Evidence of healed ulcers. Dermatitis. Normal ABI.
 Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
The role of ultrasound duplex in endovenous procedures
 The role of ultrasound duplex in endovenous procedures Neophytos A. Zambas MD, PhD Vascular Surgeon Polyclinic Ygia, Limassol, Cyprus ΚΕΑΕΧ ΚΥΠΡΙΑΚΗ ΕΤΑΙΡΕΙΑ ΑΓΓΕΙΑΚΗΣ ΚΑΙ ΕΝΔΑΓΓΕΙΑΚΗΣ ΧΕΙΡΟΥΡΓΙΚΗΣ Pre
The role of ultrasound duplex in endovenous procedures Neophytos A. Zambas MD, PhD Vascular Surgeon Polyclinic Ygia, Limassol, Cyprus ΚΕΑΕΧ ΚΥΠΡΙΑΚΗ ΕΤΑΙΡΕΙΑ ΑΓΓΕΙΑΚΗΣ ΚΑΙ ΕΝΔΑΓΓΕΙΑΚΗΣ ΧΕΙΡΟΥΡΓΙΚΗΣ Pre
Date: A. Venous Health History Form. Patient please complete questions Primary Care Physician:
 E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
TREATMENT OPTIONS FOR CHRONIC VENOUS INSUFFICIENCY
 TREATMENT OPTIONS FOR CHRONIC VENOUS INSUFFICIENCY TL LUK Consultant Vascular Surgeon Sarawak General Hospital HKL Vascular Conference 19/06/2013 PREVALENCE OF LOWER LIMB VENOUS DISEASE Affects half of
TREATMENT OPTIONS FOR CHRONIC VENOUS INSUFFICIENCY TL LUK Consultant Vascular Surgeon Sarawak General Hospital HKL Vascular Conference 19/06/2013 PREVALENCE OF LOWER LIMB VENOUS DISEASE Affects half of
OHTAC Recommendation. Endovascular Laser Treatment for Varicose Veins. Presented to the Ontario Health Technology Advisory Committee in November 2009
 OHTAC Recommendation Endovascular Laser Treatment for Varicose Veins Presented to the Ontario Health Technology Advisory Committee in November 2009 April 2010 Issue Background The Ontario Health Technology
OHTAC Recommendation Endovascular Laser Treatment for Varicose Veins Presented to the Ontario Health Technology Advisory Committee in November 2009 April 2010 Issue Background The Ontario Health Technology
New Guideline in venous ulcer treatment: dressing, medication, intervention
 New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
Vein Disease Treatment
 MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
Will it heal? How to assess the probability of wound healing
 Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY
 RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
PROVIDER POLICIES & PROCEDURES
 PROVIDER POLICIES & PROCEDURES TREATMENT OF VARICOSE VEINS OF THE LOWER EXTREMITIES STAB PHLEBECTOMY AND SCLEROTHERAPY TREATMENT The primary purpose of this document is to assist providers enrolled in
PROVIDER POLICIES & PROCEDURES TREATMENT OF VARICOSE VEINS OF THE LOWER EXTREMITIES STAB PHLEBECTOMY AND SCLEROTHERAPY TREATMENT The primary purpose of this document is to assist providers enrolled in
The Use of Adjunctive Venography and Endovascular Manoeuvres In The Treatment of Saphenous Vein Insufficiency. A Prospective, Multi-centre Study
 The Use of Adjunctive Venography and Endovascular Manoeuvres In The Treatment of Saphenous Vein Insufficiency A Prospective, Multi-centre Study Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor
The Use of Adjunctive Venography and Endovascular Manoeuvres In The Treatment of Saphenous Vein Insufficiency A Prospective, Multi-centre Study Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor
PRODIGY Quick Reference Guide
 PRODIGY Quick Venous leg ulcer infected How do I assess a venous leg ulcer? Chronic venous insufficiency and venous hypertension result from damage to the valves in the veins of the leg and inadequate
PRODIGY Quick Venous leg ulcer infected How do I assess a venous leg ulcer? Chronic venous insufficiency and venous hypertension result from damage to the valves in the veins of the leg and inadequate
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Objectives. Abdominal Aortic Aneuryms 11/16/2017. The Vascular Patient: Diagnosis and Conservative Treatment
 The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
All WALES LYMPHOEDEMA GUIDANCE:
 All WALES LYMPHOEDEMA GUIDANCE: Lymphoedema Vascular Assessment Policy (Toe Brachial Pressure Index / TBPI) April 2013 Created by the All Wales Lymphoedema Service Leads 1 Background The presence of peripheral
All WALES LYMPHOEDEMA GUIDANCE: Lymphoedema Vascular Assessment Policy (Toe Brachial Pressure Index / TBPI) April 2013 Created by the All Wales Lymphoedema Service Leads 1 Background The presence of peripheral
Peripheral Arterial Disease Extremity
 Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Leg ulcer assessment and management
 Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Features compression after open and endovascular operation in vascular malformation
 Features compression after open and endovascular operation in vascular malformation Sapelkin Sergey Institute of Surgery named A.V. Vishnevsky, Moscow, Russia 21.10.2017 CIRC Meeting, Grassau AV-malformations:
Features compression after open and endovascular operation in vascular malformation Sapelkin Sergey Institute of Surgery named A.V. Vishnevsky, Moscow, Russia 21.10.2017 CIRC Meeting, Grassau AV-malformations:
BC Vascular Surgery Day
 BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Date: A. Venous Health History Form. Patient please complete questions Primary Care Physician:
 E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
Vascular surgery is a specialty that deals with diseases of the vascular system (i.e. arteries, veins
 Vascular Surgery Vascular surgery is a specialty that deals with diseases of the vascular system (i.e. arteries, veins and lymphatics). These are managed by medical therapy, interventional procedures,
Vascular Surgery Vascular surgery is a specialty that deals with diseases of the vascular system (i.e. arteries, veins and lymphatics). These are managed by medical therapy, interventional procedures,
COMMISSIONING POLICY
 Ref No. 1a7.5 COMMISSIONING POLICY Surgery for venous disease of the leg (Varicosities of the Long Saphenous Vein) April 2011 CONTENTS Section Page Summary 2 1. Background 2 2. Criteria for eligibility
Ref No. 1a7.5 COMMISSIONING POLICY Surgery for venous disease of the leg (Varicosities of the Long Saphenous Vein) April 2011 CONTENTS Section Page Summary 2 1. Background 2 2. Criteria for eligibility
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Role of free tissue transfer in management of chronic venous ulcer
 Original Article Role of free tissue transfer in management of chronic venous ulcer K. Murali Mohan Reddy, D. Mukunda Reddy Department of Plastic Surgery, Nizams Institute of Medical Sciences, India. Address
Original Article Role of free tissue transfer in management of chronic venous ulcer K. Murali Mohan Reddy, D. Mukunda Reddy Department of Plastic Surgery, Nizams Institute of Medical Sciences, India. Address
Starting with deep venous treatment
 Starting with deep venous treatment Carsten Arnoldussen, MD Interventional Radiologist Maastricht University Medical Centre, Maastricht VieCuri Medical Centre, Venlo The Netherlands Background Maastricht
Starting with deep venous treatment Carsten Arnoldussen, MD Interventional Radiologist Maastricht University Medical Centre, Maastricht VieCuri Medical Centre, Venlo The Netherlands Background Maastricht
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease
 Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Identification and recommended management of leg ulcers Jill Robson RGN and Gerard Stansby MA, MChir, FRCS
 Identification and recommended management of leg ulcers Jill Robson RGN and Gerard Stansby MA, MChir, FRCS thickened skin, lipodermatosclerosis skin stained haemosiderin shallow ulcer irregular shape Our
Identification and recommended management of leg ulcers Jill Robson RGN and Gerard Stansby MA, MChir, FRCS thickened skin, lipodermatosclerosis skin stained haemosiderin shallow ulcer irregular shape Our
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Wound Classification. Overview
 Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Current Management of Varicose Veins
 Current Management of Varicose Veins Michael J. Heidenreich, MD St. Joseph Mercy Hospital Ann Arbor, MI March 23, 2013 Nothing to disclose History Prevalence Anatomy Risk factors Clinical manifestations
Current Management of Varicose Veins Michael J. Heidenreich, MD St. Joseph Mercy Hospital Ann Arbor, MI March 23, 2013 Nothing to disclose History Prevalence Anatomy Risk factors Clinical manifestations
Varicose veins. Information for patients Sheffield Vascular Institute
 Varicose veins Information for patients Sheffield Vascular Institute You have been diagnosed as having varicose veins. This leaflet explains more about varicose veins and answers some of the most frequently
Varicose veins Information for patients Sheffield Vascular Institute You have been diagnosed as having varicose veins. This leaflet explains more about varicose veins and answers some of the most frequently
Varicose Vein Surgery
 What are varicose veins? Varicose veins are enlarged and twisted veins in your leg. Varicose veins are common, affecting up to 3 in 10 people. Varicose veins tend to run in families and are made worse
What are varicose veins? Varicose veins are enlarged and twisted veins in your leg. Varicose veins are common, affecting up to 3 in 10 people. Varicose veins tend to run in families and are made worse
Patient Brochure. Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland. PK Rev. 0 05/17
 Patient Brochure Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland PK1411100 Rev. 0 05/17 LIFESTREAM Patient Brochure If you or a member of your family has been diagnosed with
Patient Brochure Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland PK1411100 Rev. 0 05/17 LIFESTREAM Patient Brochure If you or a member of your family has been diagnosed with
Physician s Vascular Interpretation Examination Content Outline
 Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
National Vascular Registry
 National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Policy Number: MP.066.MH Last Review Date: 11/08/2018 Effective Date: 01/01/2019
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers the treatment of Varicose
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers the treatment of Varicose
When general causes such as cardiac or renal failure and hypoproteinaemia (which tend to affect both legs) have
 have") Part One: Assessment and Diagnosis THE REDISTRIBUTION OF FLUID FROM THE ARTERIAL END OF THE CAPILLARY TO THE VENOUS END (STARLING'S LAW) IS THE MECHANISM UNDERLYING ALMOST ALL CASES OF LIMB OEDEMA. This
Part One: Assessment and Diagnosis THE REDISTRIBUTION OF FLUID FROM THE ARTERIAL END OF THE CAPILLARY TO THE VENOUS END (STARLING'S LAW) IS THE MECHANISM UNDERLYING ALMOST ALL CASES OF LIMB OEDEMA. This
How varicose veins occur
 Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Reality TV Managing patients in the real world. Wounds UK Harrogate 2009
 Reality TV Managing patients in the real world Wounds UK Harrogate 2009 Reality TV Managing patients in the real world Brenda M King Nurse Consultant Tissue Viability Sheffield PCT Harrogate 2009 Familiar
Reality TV Managing patients in the real world Wounds UK Harrogate 2009 Reality TV Managing patients in the real world Brenda M King Nurse Consultant Tissue Viability Sheffield PCT Harrogate 2009 Familiar
Additional Information S-55
 Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Introduction to Saphenous Vein Ablations: When/Why/How?
 John Ligush, MD SMJH Vascular and Vein Center Introduction to Saphenous Vein Ablations: When/Why/How? Saphenous Vein Ablations: When/Why/How? Venous disease is easy Treatment is straightforward The patients
John Ligush, MD SMJH Vascular and Vein Center Introduction to Saphenous Vein Ablations: When/Why/How? Saphenous Vein Ablations: When/Why/How? Venous disease is easy Treatment is straightforward The patients
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI
 Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Boca Raton Regional Hospital Grand Rounds September 13, 2016
 Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Criteria For Medicare Members. Kaiser Foundation Health Plan of Washington
 Clinical Review Criteria Treatment of Varicose Veins Radiofrequency Catheter Closure Sclerotherapy Surgical Stripping Trivex System for Outpatient Varicose Vein Surgery VenaSeal Closure System VNUS Closure
Clinical Review Criteria Treatment of Varicose Veins Radiofrequency Catheter Closure Sclerotherapy Surgical Stripping Trivex System for Outpatient Varicose Vein Surgery VenaSeal Closure System VNUS Closure
Chronic Iliocaval Venous Occlusive Disease
 none Chronic Iliocaval Venous Occlusive Disease David Rigberg, M.D. Clinical Professor of Surgery Division of Vascular Surgery University of California Los Angeles Chronic Venous Occlusive Disease Chronic
none Chronic Iliocaval Venous Occlusive Disease David Rigberg, M.D. Clinical Professor of Surgery Division of Vascular Surgery University of California Los Angeles Chronic Venous Occlusive Disease Chronic
Arterial & Venous Ulcers. A Comprehensive Review Assessment & Management
 Arterial & Venous Ulcers A Comprehensive Review Assessment & Management 1 Objectives Understand Arterial & Venous disease Understand the etiology of lower extremities ulcers Understand assessment of lower
Arterial & Venous Ulcers A Comprehensive Review Assessment & Management 1 Objectives Understand Arterial & Venous disease Understand the etiology of lower extremities ulcers Understand assessment of lower
High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC
 High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC A new paradigm? Foot ulceration 101 Assessing Perfusion a new challenge Pressure
High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC A new paradigm? Foot ulceration 101 Assessing Perfusion a new challenge Pressure
Disclosures. What is a Specialty Vein Clinic? Prevalence of Venous Disease. Management of Venous Disease: an evidence based approach.
 Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
SVS AVF Clinical Practice Guidelines Venous Ulcer
 Venous Ulcer SVS AVF Venous Ulcer Clinical Practice Guidelines Task Force Multispecialty committee members Thomas F. O Donnell, Jr., MD (Chair), Marc A. Passman, MD (Vice Chair), William A. Marston, MD,
Venous Ulcer SVS AVF Venous Ulcer Clinical Practice Guidelines Task Force Multispecialty committee members Thomas F. O Donnell, Jr., MD (Chair), Marc A. Passman, MD (Vice Chair), William A. Marston, MD,
Prevention and Management of Leg Ulcers
 EWMA Educational Development Programme Curriculum Development Project Education Module: Prevention and Management of Leg Ulcers Latest revision: October 2015 ABOUT THE EWMA EDUCATIONAL DEVELOPMENT PROGRAMME
EWMA Educational Development Programme Curriculum Development Project Education Module: Prevention and Management of Leg Ulcers Latest revision: October 2015 ABOUT THE EWMA EDUCATIONAL DEVELOPMENT PROGRAMME
Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Promoting best practice in leg ulcer management
 Promoting best practice in leg ulcer management Sylvie Hampton MA BSc (Hons) DpSN RGN Independent Tissue Viability Consultant Nurse Leg Ulcers - What are the causes? Chronic leg ulcers are defined as those
Promoting best practice in leg ulcer management Sylvie Hampton MA BSc (Hons) DpSN RGN Independent Tissue Viability Consultant Nurse Leg Ulcers - What are the causes? Chronic leg ulcers are defined as those
Venous Leg Ulcers. Care for Patients in All Settings
 Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Lower Limb Venous Ultrasound. Colin P. Griffin MSc, BSc (Hons)
") Lower Limb Venous Ultrasound Colin P. Griffin MSc, BSc (Hons) Peripheral Vessels Lower Limb Peripheral Vessels Lower Limb Venous Deep System Common Iliac External/Internal Iliac Common Femoral Femoral
Lower Limb Venous Ultrasound Colin P. Griffin MSc, BSc (Hons) Peripheral Vessels Lower Limb Peripheral Vessels Lower Limb Venous Deep System Common Iliac External/Internal Iliac Common Femoral Femoral
Case study: A targeted approach to healing complex wounds using the geko device.
 Case study: A targeted approach to healing complex wounds using the geko device. Authors: Mr Sameh Dimitri Consultant Vascular and Endovascular Surgeon MSc FRCS (Eng Edin) Nikki Pavey Physiotherapist at
Case study: A targeted approach to healing complex wounds using the geko device. Authors: Mr Sameh Dimitri Consultant Vascular and Endovascular Surgeon MSc FRCS (Eng Edin) Nikki Pavey Physiotherapist at
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists
 EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
Lower Extremity Arterial Disease
 Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
AWMA MODULE ACCREDITATION. Module Three: Assessment and Management of Lower Leg Ulceration
 AWMA MODULE ACCREDITATION Module Three: Assessment and Management of Lower Leg Ulceration Introduction - The Australian Wound Management Association Education & Professional Development Sub Committee-(AWMA
AWMA MODULE ACCREDITATION Module Three: Assessment and Management of Lower Leg Ulceration Introduction - The Australian Wound Management Association Education & Professional Development Sub Committee-(AWMA
Case 1. Your diagnosis
 Case 1 44-year-old midwife presented with intermittent pins and needles in the little and ring fingers with blanching. Symptoms were exacerbated by cold exposure. Your diagnosis Diagnosis Hypothenar syndrome
Case 1 44-year-old midwife presented with intermittent pins and needles in the little and ring fingers with blanching. Symptoms were exacerbated by cold exposure. Your diagnosis Diagnosis Hypothenar syndrome
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Indications: following: embolization. artery that has diseases 5. The evaluation. of suspected. such entities. a cold hand. biopsy
 Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Appendix D: Leg Ulcer Assessment Form
 Nursing Best Practice Guideline Appendix D: Ulcer Assessment Form Person Completing Assessment: Date: Client Name: Caf # CM# VON ID #: District CCAC ID # Address Telephone Home: Work: Date of Birth Y/M/D:
Nursing Best Practice Guideline Appendix D: Ulcer Assessment Form Person Completing Assessment: Date: Client Name: Caf # CM# VON ID #: District CCAC ID # Address Telephone Home: Work: Date of Birth Y/M/D:
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2)
") Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
A A U
 PVD Venous AUC Rating Sheet 2nd Round 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Median I NI MADM Rating Agree Disagree Upper Extremity Venous Evaluation Table 1. Venous Duplex of the Upper Extremities for Patency
PVD Venous AUC Rating Sheet 2nd Round 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Median I NI MADM Rating Agree Disagree Upper Extremity Venous Evaluation Table 1. Venous Duplex of the Upper Extremities for Patency
STEPHAN MOSTOWY BSc, MD, FRCS (C) Endovascular/Vascular Surgeon Kelowna General Hospital
 Endovascular/Vascular Surgeon Kelowna General Hospital") STEPHAN MOSTOWY BSc, MD, FRCS (C) Endovascular/Vascular Surgeon Kelowna General Hospital Faculty/Presenter Disclosure Faculty: Dr. Stephan Mostowy Relationships with financial sponsors: NONE From head
STEPHAN MOSTOWY BSc, MD, FRCS (C) Endovascular/Vascular Surgeon Kelowna General Hospital Faculty/Presenter Disclosure Faculty: Dr. Stephan Mostowy Relationships with financial sponsors: NONE From head
Dr Peter Chapman-Smith
 Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Medicare C/D Medical Coverage Policy
 Varicose Vein Treatment Medicare C/D Medical Coverage Policy Origination Date: June 1, 1993 Review Date: February 15, 2017 Next Review: February, 2019 DESCRIPTION OF PROCEDURE OR SERVICE Varicose veins
Varicose Vein Treatment Medicare C/D Medical Coverage Policy Origination Date: June 1, 1993 Review Date: February 15, 2017 Next Review: February, 2019 DESCRIPTION OF PROCEDURE OR SERVICE Varicose veins
DISORDERS OF VENOUS SYSTEM
 DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
Morbidity Audit and Logbook Tool SNOMED Board Reporting Terms for SET and IMG Vascular Surgery AMPUTATION AORTA
 SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN.
 to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN.") How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN Surgeon Dr G Mark Malouf Sydney Australia Following History and Physical examination
How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN Surgeon Dr G Mark Malouf Sydney Australia Following History and Physical examination
UC SF. Disclosures. Vascular Assessment of the Diabetic Foot. What are the best predictors of wound healing? None. Non-Invasive Vascular Studies
 Disclosures Vascular Assessment of the Diabetic Foot What are the best predictors of wound healing? None Shant Vartanian MD Assistant Professor of Vascular Surgery UCSF Vascular Symposium April 20, 2013
Disclosures Vascular Assessment of the Diabetic Foot What are the best predictors of wound healing? None Shant Vartanian MD Assistant Professor of Vascular Surgery UCSF Vascular Symposium April 20, 2013
Venous Disease and Leg Ulcers. Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL
 Venous Disease and Leg Ulcers Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL Disclosures Stocks Endoshape Sapheon Medical Advisory Board BTG, Boston Scientific Venous Leg Ulcer Most common
Venous Disease and Leg Ulcers Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL Disclosures Stocks Endoshape Sapheon Medical Advisory Board BTG, Boston Scientific Venous Leg Ulcer Most common
Conflict of Interest. None
 Conflict of Interest None American Venous Forum Guidelines on Superficial Venous Disease TOP 10 GUIDELINES 10. We recommend using the CEAP classification to describe chronic venous disorders. (GRADE 1B)
Conflict of Interest None American Venous Forum Guidelines on Superficial Venous Disease TOP 10 GUIDELINES 10. We recommend using the CEAP classification to describe chronic venous disorders. (GRADE 1B)
National Clinical Conference 2018 Baltimore, MD
 National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
2018 ACOI Internal Medicine Board Review. Peripheral Vascular Disease. Robert Bender, DO, FACOI, FACC
 2018 ACOI Internal Medicine Board Review Peripheral Vascular Disease Robert Bender, DO, FACOI, FACC Peripheral Vascular Disease (PVD) Arteriosclerosis Obliterans (ASO) Aneurysmal Disease Acute Arterial
2018 ACOI Internal Medicine Board Review Peripheral Vascular Disease Robert Bender, DO, FACOI, FACC Peripheral Vascular Disease (PVD) Arteriosclerosis Obliterans (ASO) Aneurysmal Disease Acute Arterial
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
GUIDELINES FOR THE MEASUREMENT OF ANKLE BRACHIAL PRESSURE INDEX USING DOPPLER ULTRASOUND
 GUIDELINES FOR THE MEASUREMENT OF ANKLE BRACHIAL PRESSURE INDEX USING DOPPLER ULTRASOUND AIM To provide evidence based principles for the measurement of Ankle Brachial Pressure Index (ABPI) using a BACKGROUND/EVIDENCE
GUIDELINES FOR THE MEASUREMENT OF ANKLE BRACHIAL PRESSURE INDEX USING DOPPLER ULTRASOUND AIM To provide evidence based principles for the measurement of Ankle Brachial Pressure Index (ABPI) using a BACKGROUND/EVIDENCE
Peripheral Vascular Disease
 Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Imaging for Peripheral Vascular Disease
 Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Endothermal Ablation for Venous Insufficiency. Dr. S. Kundu Medical Director The Vein Institute of Toronto
 Endothermal Ablation for Venous Insufficiency Dr. S. Kundu Medical Director The Vein Institute of Toronto Objective: remove the GSV from the circulation 1. Surgical - HL & stripping 2. Chemical sclerotherapy
Endothermal Ablation for Venous Insufficiency Dr. S. Kundu Medical Director The Vein Institute of Toronto Objective: remove the GSV from the circulation 1. Surgical - HL & stripping 2. Chemical sclerotherapy