Hernia Advisory Panel. Ethicon, Johnson & Johnson. Funding
|
|
|
- Curtis Perry
- 5 years ago
- Views:
Transcription

1 Acute Abdomen Andreas M Kluftinger MD FRCSC Kelowna General Hospital
2 Disclosure Hernia Advisory Panel Ethicon, Johnson & Johnson Funding nil, zilch, zippo, nada, zero
3 Objectives Understand the Pathophysiology and Etiology of the acute abdomen Approch to acute abdomen in rural practice Case presentations
4 Stedman's Medical Dictionary 27th Edition any serious acute intra-abdominal condition attended by pain, tenderness, and muscular rigidity, and for which emergency surgery must be considered. "
5 Acute Abdominal Pain 5-10 % of ER visits Complex black box Delays in diagnosis i can increase morbidity Excessive consultations (+/- transport) and imaging can be costly and tax resources. Primary assessment and triage are key
6 History & Physical Onset, nature, duration, location, radiation Aggravating and relieving factors Associated GI or GU symptoms Past history (Surg and Med) Review of Systems Full physical exam
7 Stereotypes of Pain Onset and Associated Pathology Sudden S onset Rapid R onset Gradual G d l onset (full pain in seconds) (initial sensation to (hours) full pain over minutes or hours) Perforated ulcer Mesenteric infarction Ruptured abdominal aortic aneurysm Ruptured ectopic pregnancy Ovarian torsion or ruptured cyst Pulmonary embolism Acute myocardial infarction Strangulated hernia Volvulus Intussusception Acute pancreatitis Biliary colic Diverticulitis Ureteral and renal colic Appendicitis Strangulated hernia Chronic pancreatitis Peptic ulcer disease Inflammatory bowel disease Mesenteric lymphadenitis Cystitis and urinary retention Salpingitis and prostatitis


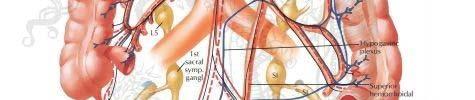

8 Abdominal Innervation
9 Simplified in Thirds Embryologic Structures Nerves Arteries Pain Location Foregut Esophagus, stomach,3/4 duod,liver, gb panc Thoracic splanchnics, vagus Coeliac Epigastrium Midgut ¼ duod to Thoracic SMA Periumbilical splenic flexure splanchnics, vagus Hindgut Left colon, Pelvic IMA Hypogastrium rectum, GU tract splanchnics, lesser thoracic splanchnics
10 Possible Causes of Pain by Location Location of Pain Right upper quadrant (liver, kidney, gallbladder) Right lower quadrant (ascending colon, appendix, ovary, fallopian tube) Left upper quadrant (pancreas, spleen, kidney) Left lower quadrant (sigmoid and descending colon, ovary, fallopian tube) Midline or periumbilical Flank Front to back Suprapubic or lower abdominal Associated Diseases Acute cholecystitis, biliary colic, acute hepatitis, duodenal ulcer, right lower lobe pneumonia Appendicitis, cecal diverticulitis, ectopic pregnancy, tubo-ovarian ovarian abcess, ruptured ovarian cyst, ovarian torsion Gastritis, acute pancreatitis, splenic pathology, left lower lobe pneumonia Diverticulitis, ectopic pregnancy, tubo-ovarian abcess, ruptured ovarian cyst, ovarian torsion Appendicitis (early), gastroenteritis, mesenteric lymphadenitis, myocardial ischemia or infarction, pacreatitis Abdominal aortic aneurysm, renal colic, pyelonephritis Acute pancreatitis, ruptured abdominal aortic aneurysm, retrocecal appendicitis, posterior duodenal ulcer Ectopic pregnancy, mittelschmerz, ruptured ovarian cyst, pelvic inflammatory disease, endometriosis, urinary tract infection
11 Sign Finding Association Cullen's sign Grey Turner s sign Bluish periumbilical discoloration Bluish flank discoloration Retroperitoneal hemorrhage pancreatitis, abdominal aortic aneurysm rupture) Kehr's sign Severe left shoulder pain Splenic rupture Ectopic pregnancy McBurney's sign Tenderness located 2/3 distance from Appendicitis ASIS to umbilicus on right side Murphy's sign Iliopsoas sign Obturator's sign Abrupt interruption of inspiration on palpation of right upper quadrant Hyperextension of right hip causing abdominal pain Internal rotation of flexed right hip causing abdominal pain Acute cholecystitis Appendicitis Appendicitis Chandelier sign Manipulation of cervix causes patient Pelvic inflammatory to lift buttocks off table disease Rovsing's sign Right lower quadrant pain with palpation of the left lower quadrant Appendicitis
12 Referred Pain Structure Irritated Diaphragmatic Ureteral Cardiac pain Appendix Location of Referred Pain Supraclavicular area (Kehr's sign) Hypogastrium, groin, inner thigh Epigastrum, jaw, shoulder Periumbilical via T10 nerve Duodenum Umbilical l region via greater thoracic splanchnic nerve Hiatal hernia Pancreas or gallbladder Gallbladder and bile duct Epigastrum via T7 and T8 nerves Epigastrum Epigastric pain that wraps around to the scapula
13 Imaging for Appendicitis
14 Imaging g Accuracy in Appendicitis iti Modality Sensitivity Specificity Pos PredValue Neg Pred Value Plain Film 10% 90% Ultrasound 85-90% 92-96% 95% 80-90% CT 95-97% 95% 97% % MRI 93% 91% 92% 100%
15 Laboratory in Appendicitis Test Sensitivity Neg Pred Value 1. WBC > % 2. Neutrophils >75% 78% 94% 3. C reactive protein 93-96% 96% % % % (81% in children)
16 Urinalysis in Appendicitis 30% of appendicitis patients have some urinary syptoms 14% have >10 WBC/hpf 18% have > 3 RBC/hpf
17 Imaging in Pregnancy Ultrasound Safest Useful for fetal assessment (dates, viability, placenta, amniotic fluid) NPV for appendicitis 80-90% PPV for appendicitis 95%
18 Imaging in Pregnancy Procedure Chest radiograph (2 views) Abdominal film (single view) Intravenous pyelography Hip film (single view) Mammography Barium enema or small bowel series CT (computed tomography) scan head or chest CT scan abdomen and lumbar spine CT pelvimetry Fetal Exposure mrad 100 mrad >1 rad* 200 mrad 7-20 mrad 2-4 rad <1 rad 3.5 rad 250 mrad No evidence of teratogenesis or fetal loss if cumulative dose < 5 rads
19 Early pregnancy Acute Abdomen Caused by Pregnancy Ruptured ectopic pregnancy Septic abortion with peritonitis Acute urinary retention due to retroverted gravid uterus Torsion of the pregnant uterus Later pregnancy Red degeneration of myoma Torsion of pedunculated myoma Placental abruption, Placenta percreta HELLP (hemolysis, elevated liver function, and low platelets) syndrome Spontaneous rupture of the liver Uterine rupture Chorioamnionitis
20 Conditions Associated with Acute pyelonephritis Acute cystitis Pregnancy Acute cholecystitis Acute fatty liver of pregnancy Rupture of rectus abdominis muscle
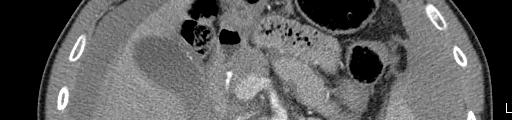
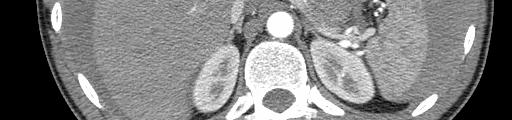
21 Case #1 68 male, 48 hrs RLQ pain Quick onset, in RLQ No nausea or anorexia No urinary syptoms PHx: GERD, dyslipidemia Tender RLQ and flank with peritonism WBC 9.2 Urine clear

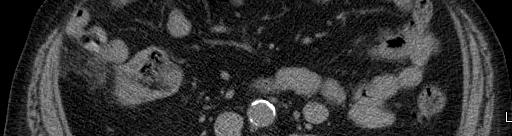


22 CT abdomen
23 Case #2 BW 41 yo electrician collapsed at home with chest, abd pain CPR by family, EHS to KGH PHx: appe Meds: ASA Exam: BP 60 sys, HR 100 RR 16 Chest clear Abdomen tender, acute
24 Investigations Hb 108 WBC 8.9 Plts 256 Hep panel normal Lipase 43 ECG normal Trop < 0.1

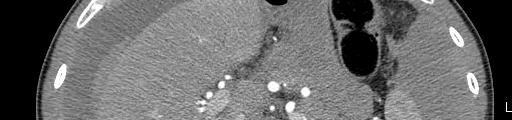

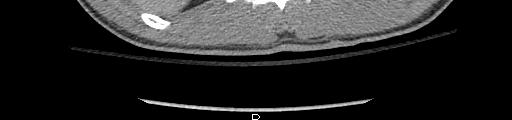
25 CT with Aorta Protocol
26 Laparotomy 3 litres blood intact liver, spleen, viscera blood from lesser sac rupured splenic artery aneurysm at hilum splenectomy, distal pancreatectomy 4 units FP, 6 units RBC Recovery uneventful





27
Gastrointestinal & Genitourinary Emergencies. Lesson Goal. Learning Objectives 9/10/2012
 Gastrointestinal & Genitourinary Emergencies Lesson Goal Recognize, assess & provide care to patients with abdominal cavity injuries Learning Objectives Discuss different causes of nontraumatic abdominal
Gastrointestinal & Genitourinary Emergencies Lesson Goal Recognize, assess & provide care to patients with abdominal cavity injuries Learning Objectives Discuss different causes of nontraumatic abdominal
: Abdominal Emergencies
 INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Surgical Education Series
 Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012
 The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012 Darra D. Kingsley, MD Associate Professor, Surgery, University of New Mexico School of Medicine Associate Chief of Staff,
The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012 Darra D. Kingsley, MD Associate Professor, Surgery, University of New Mexico School of Medicine Associate Chief of Staff,
Chapter 24 - Abdominal_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Causes of abdominal pain Doctors in the ED spend lots of time and money diagnosing abdominal pain. They still often do not know the exact cause
 1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Abdominal & scrotal pain
 Abdominal & scrotal pain Junior Teach Emergency Department 1 Created by SR Bruijns 03/11/2010 Objectives Understanding of, and emergency management of Acute abdominal pain Undifferentiated abdominal pain
Abdominal & scrotal pain Junior Teach Emergency Department 1 Created by SR Bruijns 03/11/2010 Objectives Understanding of, and emergency management of Acute abdominal pain Undifferentiated abdominal pain
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
USMLE and COMLEX II. CE / CK Review. General Surgery. 1. Northwestern Medical Review
 USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Role of imaging in the evaluation of the acute abdomen
 Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
Anatomy: Know Your Abdomen
 Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Abdo Pain rules & regulations. Mark Hartnell 2010
 Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Always keep it in the differential
 Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Problem. A 34-year. year-old woman admitted for control of diabetes develops acute abdominal pain that increases in severity over several hours.
 Immediate Questions Problem. A 34-year year-old woman admitted for control of diabetes develops acute abdominal pain that increases in severity over several hours. A. What are the patient's vital signs?
Immediate Questions Problem. A 34-year year-old woman admitted for control of diabetes develops acute abdominal pain that increases in severity over several hours. A. What are the patient's vital signs?
Left abdominal pain with back pain
 Search Search Left abdominal pain with back pain Lower left abdominal pain and lower back pain in women - Possible causes of chronic but worsening lower left abdominal pain with simultaneous low back pain?
Search Search Left abdominal pain with back pain Lower left abdominal pain and lower back pain in women - Possible causes of chronic but worsening lower left abdominal pain with simultaneous low back pain?
Appendicitis USG vs CT
 Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
Abdominal radiology 腹部放射線學
 Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Anatomy of the Large Intestine
 Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
PARAMEDIC RESOURCE MANUAL
 .. ONTARIO BASE HOSPITAL GROUP PARAMEDIC RESOURCE MANUAL THE ABDOMEN SECTION EIGHT Version 1.1 2010 Update PARAMEDIC RESOURCE MANUAL OJECTIVES: THE ABDOMEN The objectives indicate what you should know,
.. ONTARIO BASE HOSPITAL GROUP PARAMEDIC RESOURCE MANUAL THE ABDOMEN SECTION EIGHT Version 1.1 2010 Update PARAMEDIC RESOURCE MANUAL OJECTIVES: THE ABDOMEN The objectives indicate what you should know,
Exploring Anatomy: the Human Abdomen
 Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Chapter Goal. Learning Objectives 9/12/2012. Chapter 29. Nontraumatic Abdominal Injuries
 Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Introduction to Evidence Based Medicine:
 Introduction to Evidence Based Medicine: General Abdominal Examination o Inspection Cullen s sign and Grey Turner s sign are indications of intraperitoneal or retroperitoneal hemorrhage. Traditionally,
Introduction to Evidence Based Medicine: General Abdominal Examination o Inspection Cullen s sign and Grey Turner s sign are indications of intraperitoneal or retroperitoneal hemorrhage. Traditionally,
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera.
 Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera. Layers of the peritoneum: 1. Outer Layer ( Parietal Peritoneum) : lines
Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera. Layers of the peritoneum: 1. Outer Layer ( Parietal Peritoneum) : lines
UNIVERSITY DEVELOPMENT CENTER. Course Specification 2015/2016 For the Anatomy (first year) Medicine Anatomy and Embryology Department 29/12/2015
 Medicine Anatomy and Embryology Department 29/12/2015") Course Specification 2015/2016 For the Anatomy (first year) Faculty : Department : Medicine Anatomy and Embryology Department Course Specification: Programme (s) on which the course is given : M.B.B.Ch
Course Specification 2015/2016 For the Anatomy (first year) Faculty : Department : Medicine Anatomy and Embryology Department Course Specification: Programme (s) on which the course is given : M.B.B.Ch
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
Chapter 43 - Acute Abdomen
 Use of this content is subject to the Terms and Conditions of the MD Consult web site. Townsend: Sabiston Textbook of Surgery, 17th ed., Copyright 2004 Elsevier 1219 Chapter 43 - Acute Abdomen R. Scott
Use of this content is subject to the Terms and Conditions of the MD Consult web site. Townsend: Sabiston Textbook of Surgery, 17th ed., Copyright 2004 Elsevier 1219 Chapter 43 - Acute Abdomen R. Scott
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution,
 SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution, derivatives 4. Hindgut- limits, evolution, derivatives
SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution, derivatives 4. Hindgut- limits, evolution, derivatives
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 16, 2015
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
Right Iliac Fossa Pain
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Right Iliac Fossa Pain Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Right Iliac Fossa Pain Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Gastrointestinal Tract. Anatomy of GI Tract. Anatomy of GI Tract. (Effective February 2007) (1%-5%)
 (1%-5%)") Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
In the name ofgod. Abdomen 3. Dr. Zahiri
 In the name ofgod Abdomen 3 Dr. Zahiri Peritoneum Peritoneum It is the serous membrane(a type of loose connective tissue and is covered by mesothelium) that lines the abdominal cavity. Extensions of the
In the name ofgod Abdomen 3 Dr. Zahiri Peritoneum Peritoneum It is the serous membrane(a type of loose connective tissue and is covered by mesothelium) that lines the abdominal cavity. Extensions of the
Body Regions Review. Anatomical Position. Anatomical Planes. Supine versus Prone 9/9/2009
 Body Regions Review The fundamental divisions of the human body Christine Sparks Anatomy / Physiology I Sept. 9, 2009 Anatomical Position Universal terms are used to describe the body accurately and result
Body Regions Review The fundamental divisions of the human body Christine Sparks Anatomy / Physiology I Sept. 9, 2009 Anatomical Position Universal terms are used to describe the body accurately and result
Chapter 18 - Gastrointestinal & Urologic Emergencies
 1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Ultrasound ICD-10-CM
 Ultrasound ICD-10-CM Clinical Documentation Guides Brought to you by www.codingstrategies.com The Resource for Physician and Outpatient Coding, Compliance & ICD-10-CM OTHER CLINICAL DOCUMENTATION GUIDES
Ultrasound ICD-10-CM Clinical Documentation Guides Brought to you by www.codingstrategies.com The Resource for Physician and Outpatient Coding, Compliance & ICD-10-CM OTHER CLINICAL DOCUMENTATION GUIDES
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
Midgut. Over its entire length the midgut is supplied by the superior mesenteric artery
 Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
- GI and GU are the main sources of AP, but AP can come from extra- and intraabdominal
 Abdominal Pain Karima Sajadi Based on Chapter 27 in Rosen s Emergency Medicine Common CC in ED, but presents lot of challenges for the pts and docs (pts have hard time conveying the nature and quality
Abdominal Pain Karima Sajadi Based on Chapter 27 in Rosen s Emergency Medicine Common CC in ED, but presents lot of challenges for the pts and docs (pts have hard time conveying the nature and quality
1 Right & left Hepatic ducts Gastric Impression of spleen
 Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
CLASS 1. PATHOLOGY 3. PATHOLOGY 5. PATHOLOGY 7. PATHOLOGY 1. CELL BIOLOGY/PHYSIO
 WEEK 1 Time/Date Monday, July 16 Tuesday, July 17 Wednesday, July 18 Thursday, July 19 Friday, July 20 1. PATHOLOGY 3. PATHOLOGY 5. PATHOLOGY 7. PATHOLOGY 1. CELL BIOLOGY/PHYSIO SDL: Diseases of the Oral
WEEK 1 Time/Date Monday, July 16 Tuesday, July 17 Wednesday, July 18 Thursday, July 19 Friday, July 20 1. PATHOLOGY 3. PATHOLOGY 5. PATHOLOGY 7. PATHOLOGY 1. CELL BIOLOGY/PHYSIO SDL: Diseases of the Oral
U Lecture Objectives. U Nordic Forum Trauma & Emergency Radiology. Bowel obstruction. U Bowel Obstruction: Etiologies
 Nordic Forum Trauma & Emergency Radiology Lecture Objectives Bowel Obstruction To illustrate the spectrum of acute obstruction of the small and the large bowel To explain how these bowel obstructions may
Nordic Forum Trauma & Emergency Radiology Lecture Objectives Bowel Obstruction To illustrate the spectrum of acute obstruction of the small and the large bowel To explain how these bowel obstructions may
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Preview from Notesale.co.uk Page 1 of 34
 Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Evidence Process for Abdominal Pain Guideline Research 11/16/2017. Guideline Review using ADAPTE method and AGREE II instrument 11/16/2017
 Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Abdominal Exam. Winter Quarter Adapted from previous years by Amanda Kocoloski, OMS IV
 Abdominal Exam Winter Quarter 2010 Adapted from previous years by Amanda Kocoloski, OMS IV Agenda ó History ó Anatomy ó Physical ó Prac4ce cases ó 2 gastrointes4nal complaints ó Work on incorpora4ng GI
Abdominal Exam Winter Quarter 2010 Adapted from previous years by Amanda Kocoloski, OMS IV Agenda ó History ó Anatomy ó Physical ó Prac4ce cases ó 2 gastrointes4nal complaints ó Work on incorpora4ng GI
Radiology of the abdomen Lecture -1-
 Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Arteriovenostomy for renal dialysis 39.27, 39.42
 Surgery categories NHSN Surgery codes (Reference: NHSN Operative Procedure Category Mappings to ICD-9-CM Codes, October 2010 www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf) Operative aortic aneurysm
Surgery categories NHSN Surgery codes (Reference: NHSN Operative Procedure Category Mappings to ICD-9-CM Codes, October 2010 www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf) Operative aortic aneurysm
Diagnostic Laparoscopy
 Department of Obstetrics and Gynecology, Chang Gung Memorial Hospital at ChiaYi 嘉義長庚紀念醫院婦產科 Clinical Guideline Diagnostic Laparoscopy By Dr. CJ Tseng Diagnostic laparoscopy is a minimally invasive surgical
Department of Obstetrics and Gynecology, Chang Gung Memorial Hospital at ChiaYi 嘉義長庚紀念醫院婦產科 Clinical Guideline Diagnostic Laparoscopy By Dr. CJ Tseng Diagnostic laparoscopy is a minimally invasive surgical
Clinical, Diagnostic, and Operative Correlation of Acute Abdomen
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/163 Clinical, Diagnostic, and Operative Correlation of Acute Abdomen Madipeddi Venkanna 1, Doolam Srinivas 2, Budida
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/163 Clinical, Diagnostic, and Operative Correlation of Acute Abdomen Madipeddi Venkanna 1, Doolam Srinivas 2, Budida
USMLE Step 1 Problem Drill 17: Gastrointestinal System
 USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
Measuring What Students Know: Writing Effective MCQ Questions
 Measuring What Students Know: Writing Effective MCQ Questions 1 What Can Student Assessments Do? Communicate important content and skills Provide basis for grading, passing, graduation Identify students
Measuring What Students Know: Writing Effective MCQ Questions 1 What Can Student Assessments Do? Communicate important content and skills Provide basis for grading, passing, graduation Identify students
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Cecal Volvulus: Case Presentation and Review of CT Findings
 August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
ANATOMY OF THE SMALL & LARGE INTESTINES. Semester 1, 2011 A. Mwakikunga
 ANATOMY OF THE SMALL & LARGE INTESTINES Semester 1, 2011 A. Mwakikunga LEARNING OBJECTIVES 1. List the parts and anatomical regions of the small and large intestines 2. State anatomical relations of the
ANATOMY OF THE SMALL & LARGE INTESTINES Semester 1, 2011 A. Mwakikunga LEARNING OBJECTIVES 1. List the parts and anatomical regions of the small and large intestines 2. State anatomical relations of the
By Junaid Asghar M Med, FAFP Consultant Adult Emergency Medicine. King Faisal Specialist Hospital & Research Centre- Riyadh- KSA
 By Junaid Asghar M Med, FAFP Consultant Adult Emergency Medicine King Faisal Specialist Hospital & Research Centre- Riyadh- KSA Case No 1 A VIP patient brings his 21 years son in EM with the complaints
By Junaid Asghar M Med, FAFP Consultant Adult Emergency Medicine King Faisal Specialist Hospital & Research Centre- Riyadh- KSA Case No 1 A VIP patient brings his 21 years son in EM with the complaints
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
GI Grand Rounds. A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards
 GI Grand Rounds A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards PMH Aug 25, 1992 4 year old male presents to a pediatric gastroenterologist for primary complaint of anorexia, intermittent abdominal
GI Grand Rounds A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards PMH Aug 25, 1992 4 year old male presents to a pediatric gastroenterologist for primary complaint of anorexia, intermittent abdominal
ABy Susan Simmons Holcomb, ARNP-BC, PhD
 cute bdomen: ABy Susan Simmons Holcomb, ARNP-BC, PhD So many things some life-threatening can cause abdominal pain. Here s how to capture the clues quickly and accurately. Determining the cause of abdominal
cute bdomen: ABy Susan Simmons Holcomb, ARNP-BC, PhD So many things some life-threatening can cause abdominal pain. Here s how to capture the clues quickly and accurately. Determining the cause of abdominal
Mousa Salah. Dr. Mohammad Al. Mohtasib. 1 P a g e
 8 Mousa Salah Dr. Mohammad Al. Mohtasib 1 P a g e In the previous lecture we talked about the peritoneum, and we said that the peritonium is a serous sac, and it consists of two layers, visceral and parietal.
8 Mousa Salah Dr. Mohammad Al. Mohtasib 1 P a g e In the previous lecture we talked about the peritoneum, and we said that the peritonium is a serous sac, and it consists of two layers, visceral and parietal.
What is Laparoscopy All About?
 Disclaimer This movie is an educational resource only and should not be used to manage surgical health. All decisions about the management of Laparoscopy must be made in conjunction with your Physician
Disclaimer This movie is an educational resource only and should not be used to manage surgical health. All decisions about the management of Laparoscopy must be made in conjunction with your Physician
SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module
 SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module Dawn Daniels Tucson Medical Center January 2016 PURPOSE This SAEMS Standing Order Training Module has been developed to serve as a template for
SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module Dawn Daniels Tucson Medical Center January 2016 PURPOSE This SAEMS Standing Order Training Module has been developed to serve as a template for
Appendicitis. I. Background & Significance: Algorithm Definitions 1. CASE
 I. Background & Significance: Appendicitis Appendicitis is one of the most common acquired surgical conditions of childhood. Diagnosis of appendicitis remains difficult. Much work has been done on validation
I. Background & Significance: Appendicitis Appendicitis is one of the most common acquired surgical conditions of childhood. Diagnosis of appendicitis remains difficult. Much work has been done on validation
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 17, 2014
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 17, 2014 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 17, 2014 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
Abdominal Examination Benchmarks
 Abdominal Examination Benchmarks Preparation and Positioning: Stand on the right side of the patient. The patient should be supine and double draped so only the abdomen is exposed o To relax the abdominal
Abdominal Examination Benchmarks Preparation and Positioning: Stand on the right side of the patient. The patient should be supine and double draped so only the abdomen is exposed o To relax the abdominal
RADPrimer Curriculum Breast Topics Covered Basic Intermediate 225
 Breast Anatomy & Normal Variants 11 Breast Imaging Modalities 13 BI RADS Lexicon 3 Mammography: Masses 9 Mammography: Calcifications 17 Mammography: Additional Findings 8 Ultrasound Features 10 Ultrasound
Breast Anatomy & Normal Variants 11 Breast Imaging Modalities 13 BI RADS Lexicon 3 Mammography: Masses 9 Mammography: Calcifications 17 Mammography: Additional Findings 8 Ultrasound Features 10 Ultrasound
Role of Ultrasound in Acute Non Traumatic Abdominal Emergencies
 ORIGINALARTICLE Role of Ultrasound in Acute Non Traumatic Abdominal Emergencies Kamlesh Gupta, Ramesh Chander, Arvinder Singh, Sohan Singh, Sandeep Singh Abstract The current study was undertaken to access
ORIGINALARTICLE Role of Ultrasound in Acute Non Traumatic Abdominal Emergencies Kamlesh Gupta, Ramesh Chander, Arvinder Singh, Sohan Singh, Sandeep Singh Abstract The current study was undertaken to access
GASTROINTESTINAL SYSTEM
 GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
BIOE221. Session 6. Abdominal Examination. Bioscience Department. Endeavour College of Natural Health endeavour.edu.au
 BIOE221 Session 6 Abdominal Examination Bioscience Department Examination of the Abdomen Session objectives Understand the organs / structures that are present in the abdominal cavity Understand the importance
BIOE221 Session 6 Abdominal Examination Bioscience Department Examination of the Abdomen Session objectives Understand the organs / structures that are present in the abdominal cavity Understand the importance
The peritoneum. Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website:
 Website:") The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
Clinical Anatomy of the Biliary Apparatus: Relations & Variations
 Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 27 March 2007 Lawrence M. Witmer, PhD Professor of Anatomy Department
Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 27 March 2007 Lawrence M. Witmer, PhD Professor of Anatomy Department
Accessory Glands of Digestive System
 Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
physical therapy assessment of abdominal pain
 physical therapy assessment of abdominal pain abdominal landmarks anatomy in the RUQ anatomy in the LUQ anatomy of the RLQ anatomy of the LLQ problem based history (OLDCART) abdominal pain nausea and vomiting
physical therapy assessment of abdominal pain abdominal landmarks anatomy in the RUQ anatomy in the LUQ anatomy of the RLQ anatomy of the LLQ problem based history (OLDCART) abdominal pain nausea and vomiting
Chapter 2 Lower Abdominal Pain/Suprapubic Pain
 Chapter 2 Lower Abdominal Pain/Suprapubic Pain Paolo Gontero and Bruno Frea Abstract The term lower abdomen refers to the portion of abdomen below the umbilicus in which three topographic regions can be
Chapter 2 Lower Abdominal Pain/Suprapubic Pain Paolo Gontero and Bruno Frea Abstract The term lower abdomen refers to the portion of abdomen below the umbilicus in which three topographic regions can be
Paediatric surgical emergencies. Mani Thyagarajan BWCH
 Paediatric surgical emergencies Mani Thyagarajan BWCH General points Always discuss Call consultant for help ASAP CT scan is a bad modality in paediatrics Ultrasound? Intussusception? Renal colic? UTI
Paediatric surgical emergencies Mani Thyagarajan BWCH General points Always discuss Call consultant for help ASAP CT scan is a bad modality in paediatrics Ultrasound? Intussusception? Renal colic? UTI
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Bushra Arafa Zayed & Hanan Jamal. - Dana AF
 - 10 - Bushra Arafa Zayed & Hanan Jamal - Dana AF - Mohammad Al Muhtaseb Notes: This sheet was written in the same order as the slides, and everything in the slides is mentioned in this sheet. Pictures
- 10 - Bushra Arafa Zayed & Hanan Jamal - Dana AF - Mohammad Al Muhtaseb Notes: This sheet was written in the same order as the slides, and everything in the slides is mentioned in this sheet. Pictures
OVARIES URETER FALLOPIAN TUBES BLADDER UROGENITAL OPENINGS (BOTH SEXES) PENIS VAGINA UTERUS
 PENIS VAGINA UTERUS") URETER OVARIES FALLOPIAN TUBES BLADDER UROGENITAL OPENINGS (BOTH SEXES) PENIS VAGINA UTERUS REPRODUCTIVE PRODUCE FEMALE HORMONES EXCRETORY FROM KIDNEY TO BLADDER EXCRETORY STORES URINE REPRODUCTIVE TRANSPORTS
URETER OVARIES FALLOPIAN TUBES BLADDER UROGENITAL OPENINGS (BOTH SEXES) PENIS VAGINA UTERUS REPRODUCTIVE PRODUCE FEMALE HORMONES EXCRETORY FROM KIDNEY TO BLADDER EXCRETORY STORES URINE REPRODUCTIVE TRANSPORTS
In any operation. Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications.
 In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for