CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
|
|
|
- Annice Garrison
- 6 years ago
- Views:
Transcription


1 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D
2 ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually associated with severe acute upper abdominal pain and elevated blood levels of pancreatic enzymes
3 ETIOLOGY Biliary tract disease Alcoholism Drugs Infection Hypertriglyceridemia ERCP Pancreatic duct abnormalities CBD abnormalities Scorpion sting Surgery Vascular disease Trauma Hyperparathyroidism Hypercalcemia Renal transplant. Hereditary pancreatitis Uncertain causes
4 PATHOGENESIS In biliary tract disease Temporary impaction of a gallstone in the sphincter of Oddi before it passes into the duodenum. Obstruction of the pancreatic duct in the absence of biliary reflux can produce pancreatitis, suggesting that increased ductal pressure triggers pancreatitis.
5 PATHOGENESIS Alcohol intake Alcohol intake > 100 g/day for several years may cause the protein of pancreatic enzymes to precipitate within small pancreatic ductules. In time, protein plugs accumulate, inducing additional histologic abnormalities. Because of premature activation of pancreatic enzymes
6 PATHOLOGY EDEMA - NECROSIS - HEMORRHAGE Tissue necrosis is caused by activation of pancreatic enzymes, including trypsin and phospholipase A2. Hemorrhage is caused by activation of pancreatic enzymes, including pancreatic elastase, which dissolves elastic fibers of blood vessels.
7 HYPOVOLEMIA AND SHOCK Pancreatic exudate containing toxins and activated pancreatic enzymes permeates the retroperitoneum and at times the peritoneal cavity, inducing a chemical burn and increasing the permeability of blood vessels. This causes extravasation of large amounts of protein-rich fluid from the systemic circulation into third spaces, producing hypovolemia and shock.
8 HYPOTENSION AND ARDS On entering the systemic circulation, these activated enzymes and toxins increase capillary permeability throughout the body and may reduce peripheral vascular tone, thereby intensifying hypotension. Circulating activated enzymes may damage tissue directly

9 CLINICAL FEATURES Abdominal pain Nausea Vomiting Restlessness Agitation Shock Coma
10 ABDOMINAL PAIN Acute in the epigastrium at the onset, and may be right upper quadrant, diffuse, or, infrequently, confined to the left side relieved on bending forward. The pain of pancreatitis can last for days. Its onset is rapid, but not as abrupt as that with a perforated viscus, is band-like radiation to the back. The abdominal pain is typically accompanied by nausea and vomiting, restlessness, and agitation.
11 PHYSICAL EXAMINATION
12 PHYSICAL EXAMINATION Fever Tachycardia Hypotension Dyspnea Shallow respirations Epigastric tenderness Guarding Abdominal distention Hypoactive bowel sounds Shock Coma Jaundice
13 OTHER SIGNS Grey-Turner's sign Ecchymotic discoloration in the flank Cullen's sign Ecchymotic discoloration in the periumbilical region Epigastric Mass due to pseudocyst formation Subcutaneous Nodular Fat Necrosis, 0.5 to 2 cm tender red nodules, are usually located over the distal extremities but may occur elsewhere, Thrombophlebitis in the legs Polyarthritis

14 GREY-TURNER'S SIGN

15

16

17 CULLEN S SIGN

18 CULLEN S SIGN

19 FAT NECROSIS

20 THROMBOPHLEBITIS
21 FINDINGS INDICATIVE OF UNDERLYING DISORDERS Hepatomegaly in alcoholic pancreatitis Xanthomas in hyperlipidemic pancreatitis Parotid swelling associated with mumps

22 JAUNDICE
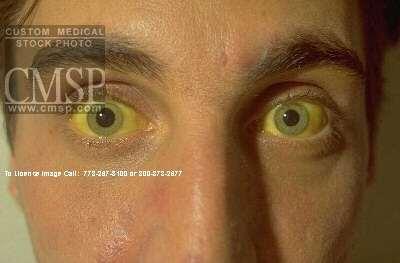
23 JAUNDICE
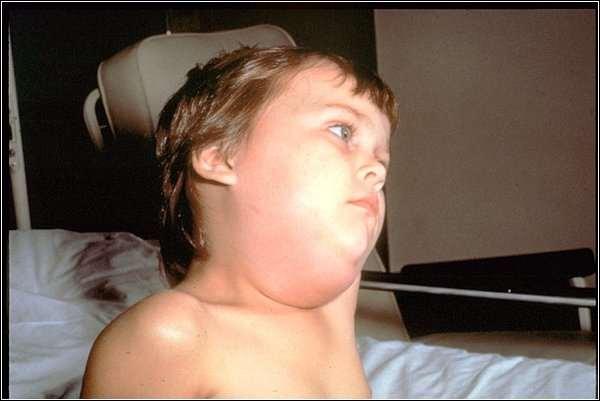
24 MUMPS


25 MUMPS


26 ERUPTIVE XANTHOMA
27 DIFFERENTIAL DIAGNOSIS Perforated duodenal ulcer Mesenteric infarction Strangulating intestinal obstruction Ectopic pregnancy Dissecting aneurysm Biliary colic Appendicitis Diverticulitis Inferior wall MI Hematoma of abdominal muscles or spleen.
28 LABORATORY DIAGNOSIS PANCREATIC ENZYMES Serum amylase Urine amylase Serum lipase
29 SERUM AMYLASE It rises within 6 to 12 hours of onset Its half-life is 10 hours In uncomplicated attacks, serum amylase is usually elevated for three to five days It is usually more than three times the upper limit of normal.
30 LIMITATIONS OF SERUM AMYLASE 1. May be normal or minimally elevated in patients with fatal pancreatitis or those who have a mild attack 2. May remain normal if destruction of acinar tissue happened during previous episode 3. May remain normal if there is coexisting hypertriglyceridemia 4. Increased in other disorders
31 URINE AMYLASE Hyperamylasuria occurs in acute pancreatitis Amylase-to-creatinine clearance ratio (ACCR), increases to approximately 10% Moderate renal insufficiency interferes with accuracy and specificity of the ACCR. Urinary amylase excretion is not increased in macroamylasemia.
32 SERUM LIPASE The sensitivity for the diagnosis of acute pancreatitis is between 85 and 100% Lipase elevations occur earlier and last longer than amylase elevations. The combination of enzymes does not improve diagnostic accuracy.
33 LABORATORY DIAGNOSIS The WBC count increases to 12,000 to 20,000/mL Hct may increase to as high as 50 to 55 Hyperglycemia may occur Serum Ca concentration falls as early as the first day because of the formation of Ca soaps secondary to excess generation of free fatty acids Serum bilirubin increases in 15 to 25% of patients
34 RADIOLOGIC FEATURES Abdominal plain film Normal Sentinel Loop: Localized ileus of a segment of small intestine Colon cutoff sign: a paucity of air in the colon distal to the splenic flexure due to functional spasm of the descending colon Generalized ileus may occur in severe disease
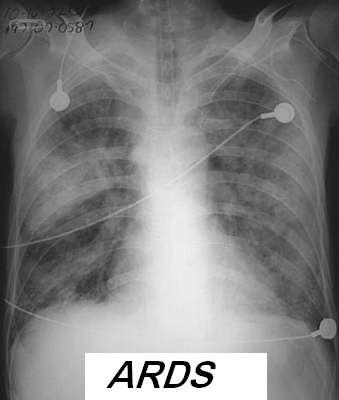
35 CHEST FILM Approximately one-third of patients will have abnormalities Elevation of a hemidiaphragm Pleural effusions Basal atelectasis Pulmonary infiltrates ARDS
36
37 ABDOMINAL ULTRASOUND The classic ultrasonographic image of acute pancreatitis is a diffusely enlarged, hypoechoic pancreas It can detect gallstones in the gallbladder A less frequent pattern is the presence of focal hypoechoic areas 25 to 35 percent of patients have bowel gas that may obscure the pancreas.

38

39
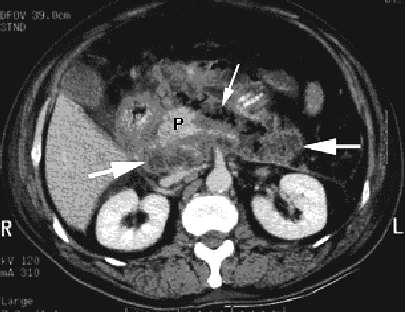
40 CT SCAN The most important imaging test for the diagnosis of acute pancreatitis and its intraabdominal complications. Patients who do not improve with initial conservative therapy or who are suspected of having complications should undergo CT scan to identify any areas of pancreatic necrosis CT or US guided needle aspiration can differentiate between sterile and infected pancreatic necrosis or a pseudocyst.
41 RANSON'S PROGNOSTIC SIGNS At Admission 1. Age > 55 yr 2. Serum glucose > 200 mg/dl 3. Serum LDH > 350 IU/L 4. AST > 250 U 5. WBC count > 16,000/mL. 48 H After Admission 1. Hct decrease > 10% 2. BUN rise > 5 mg/dl 3. Serum Ca < 8 mg/dl 4. PaO2 < 60 mm Hg 5. Base deficit > 4 meq/l 6. Estimated fluid sequestration > 6 L.

42 RANSON'S PROGNOSTIC SIGNS Mortality increases with the number of positive signs If fewer than three signs are positive, the mortality rate is < 5% If three or four are positive, it is 15 to 20% If 5 positive criteria the mortality rate is 100%
43 PROGNOSIS Pancreatitis associated with necrosis and hemorrhage has a mortality rate > 10 to 50%. If CT shows only mild pancreatic edema, the prognosis is excellent A markedly swollen pancreas denotes a more severe prognosis, especially when extravasation of fluid
44 COMPLICATIONS Death Shock Sepsis Renal failure ARDS Pancreatic abscess Pancreatic necrosis Pancreatic pseudocysts
45 PANCREATIC ABSCESS
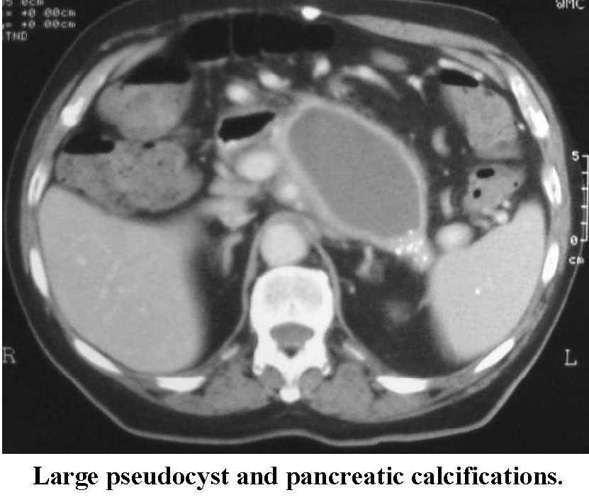
46 PSEUDOCYSTS Collections of fluid escaped from the pancreatic ductal tree disrupted by acute inflammation and/or obstructed by stricture or stone,lacking an epithelial lining.
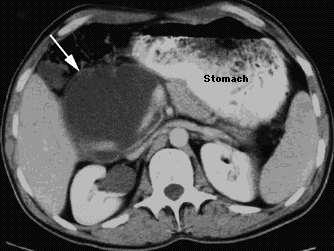
47 PSEUDOCYST
48
49 PSEUDOCYSTS More common in alcoholic than biliary pancreatitis (15 vs 3%) Occur in upto 20% of acute pancreatitis >50% resolve spontaneously within 4-6 wks 1. Infection 11% Complications 2. Haemorrhage into cyst(30-60% mortality) 3. Spontaneous rupture 4. Obstruction of duodenum 5. Obstruction of CBD
50 MANAGEMENT Fluid replacement Oxygenation Minimising pancreatic secretion Nutritional support Antibiotics Metabolic complications
51 TREATMENT Mild Edematous Pancreatitis Pain treated with meperidine NPO until manifestations of acute inflammation subside IV fluids Insertion of a nasogastric tube

52 INDICATIONS FOR ICU ADMISION Hypotension Oliguria Hypoxemia Hemoconcentration
53 TREATMENT Severe Acute Pancreatitis Pain should be treated with meperidine Fasting is maintained for 2 wk and possibly 3 to 4 wk. Nasogastric tube usually counteracts vomiting and intestinal ileus H2 blockers Fluid resuscitation 6 to 8 L/day Blood Transfusion CVP line or Swan-Ganz catheter
54 TREATMENT Severe Acute Pancreatitis Hyperglycemia treated with Insuline Hypocalcemia generally is not treated Hypoxia treated with Oxygen Renal failure should be treated by IV fluids if there is prerenal azotemia Antibiotic use is controversial Peritoneal lavage remains controversial TPN initiated within the first few days
55 SURGICAL INTERVENTION during the first several days 1. Severe blunt or penetrating trauma 2. Uncontrolled biliary sepsis 3. Poor response to supportive treatment 4. Clinical deterioration 5. Progression of organ failure 6. Peritonitis 7. Inability to distinguish acute pancreatitis from a surgical emergency

56 THANK YOU Raed Abu Sham a, M.D
Caring for the Patient with Acute Pancreatitis. Disclosure. Objectives
 Caring for the Patient with Acute Pancreatitis Bruce D. Askey, MS, ANP-BC Associate Lecturer Fitzgerald Health Education North Andover, MA Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology
Caring for the Patient with Acute Pancreatitis Bruce D. Askey, MS, ANP-BC Associate Lecturer Fitzgerald Health Education North Andover, MA Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology
Emergency Surgery Course Graz, March ACUTE PANCREATITIS. Carlos Mesquita Coimbra
 ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
Multi modality Imaging in Acute Pancreatitis. Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009
 Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland
 pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
PATHOLOGY MCQs. The Pancreas
 PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance of Gillian Lieberman, MD
 Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Acute Pancreatitis:
 American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Adv Pathophysiology Unit 9: GI Page 1 of 10
 Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
DISEASES OF THE PANCREAS
 V DISEASES OF THE PANCREAS Peter Draganov, m.d. Chris E. Forsmark, m.d., f.a.c.p. Definitions of Disease Presentations acute and chronic pancreatitis Acute pancreatitis has traditionally been defined as
V DISEASES OF THE PANCREAS Peter Draganov, m.d. Chris E. Forsmark, m.d., f.a.c.p. Definitions of Disease Presentations acute and chronic pancreatitis Acute pancreatitis has traditionally been defined as
Acute pancreatitis Case reports. Clinical problems. Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4)
 Surgical treatment of AP? (P 3 & 4)") Case reports Clinical problems Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4) Case reports Case 1 Case 1 Patient KD History M, 63 y Obesity BMI 30.3 kg/m 2 Gallbladder stones No concomitant
Case reports Clinical problems Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4) Case reports Case 1 Case 1 Patient KD History M, 63 y Obesity BMI 30.3 kg/m 2 Gallbladder stones No concomitant
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/27/2011 Radiology Quiz of the Week # 35 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/27/2011 Radiology Quiz of the Week # 35 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
A Patient with Severe Pancreatitis Successfully Treated by. Takaya Tanaka, Kenji Suzuki, Nobuaki Matsuo, Fumihiro Nozu,
 A Patient with Severe Pancreatitis Successfully Treated by Continuous Peritoneal Dialysis Takaya Tanaka, Kenji Suzuki, Nobuaki Matsuo, Fumihiro Nozu, Kazunobu Yamagami and Naoshi Takeyama Emergency Care
A Patient with Severe Pancreatitis Successfully Treated by Continuous Peritoneal Dialysis Takaya Tanaka, Kenji Suzuki, Nobuaki Matsuo, Fumihiro Nozu, Kazunobu Yamagami and Naoshi Takeyama Emergency Care
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Assessment of Severity in Acute Pancreatitis: Use of Prognostic Factors
 Qasim O. Al-Qasabi, FRCS(I); Mohammed K. Alam, MS, FRCS(Ed); Mohammed M. Haque, FRCS(Ed), FRCS(Glas); Mohammed I. Sebayel, FRCS(Glas); Saad Al-Faqih, FRCS(Glas); Abdullah Al-Kraida, FRCS(Ed) From the Department
Qasim O. Al-Qasabi, FRCS(I); Mohammed K. Alam, MS, FRCS(Ed); Mohammed M. Haque, FRCS(Ed), FRCS(Glas); Mohammed I. Sebayel, FRCS(Glas); Saad Al-Faqih, FRCS(Glas); Abdullah Al-Kraida, FRCS(Ed) From the Department
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram
 Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
Endoscopic Management of Acute Pancreatitis. Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018
 Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
General data. Age: 31 y/o Gender: male Occupation: electronic worker Admission: 92/10/27~92/11/07, total 11 days
 General data Age: 31 y/o Gender: male Occupation: electronic worker Admission: 92/10/27~92/11/07, total 11 days Chief Complaint Abdominal pain and vomiting since this morning (92/10/27) Brief Illness 1
General data Age: 31 y/o Gender: male Occupation: electronic worker Admission: 92/10/27~92/11/07, total 11 days Chief Complaint Abdominal pain and vomiting since this morning (92/10/27) Brief Illness 1
Acute Pancreatitis: Role of Imaging Modalities
 International Journal of Interdisciplinary and Multidisciplinary Studies (IJIMS), 2015, Vol 2, No.9,109-114. 109 Available online at http://www.ijims.com ISSN: 2348 0343 Abstract Acute Pancreatitis: Role
International Journal of Interdisciplinary and Multidisciplinary Studies (IJIMS), 2015, Vol 2, No.9,109-114. 109 Available online at http://www.ijims.com ISSN: 2348 0343 Abstract Acute Pancreatitis: Role
Diseases of exocrine pancreas
 Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Exocrine functions: secretion of digestive enzymes (eg. lipase, amylase,
 Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
Disorders of the Liver, Gallbladder and Pancreas
 Disorders of the Liver, Gallbladder and Pancreas Objectives: Disorders of the liver Disorders of the gall bladder Disorders of the pancreas Part 1: Disorders of the Liver 1 Jaundice: is a manifestation
Disorders of the Liver, Gallbladder and Pancreas Objectives: Disorders of the liver Disorders of the gall bladder Disorders of the pancreas Part 1: Disorders of the Liver 1 Jaundice: is a manifestation
The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012
 The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012 Darra D. Kingsley, MD Associate Professor, Surgery, University of New Mexico School of Medicine Associate Chief of Staff,
The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012 Darra D. Kingsley, MD Associate Professor, Surgery, University of New Mexico School of Medicine Associate Chief of Staff,
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
SASKATCHEWAN REGISTERED NURSES ASSOCIATION. RNs WITH ADDITIONAL AUTHORIZED PRACTICE CLINICAL DECISION TOOL AUGUST 2017
 DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Gastric ulcer Duodenal ulcer Pancreatitis Ileus. Barbora Konečná
 Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Comprehensive Study of Acute Pancreatitis (Diagnosis, Disease Course, and Clinical Management): A Retrospective and Prospective Study
: A Retrospective and Prospective Study") Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/449 Comprehensive Study of Acute Pancreatitis (Diagnosis, Disease Course, and Clinical Management): A Retrospective
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/449 Comprehensive Study of Acute Pancreatitis (Diagnosis, Disease Course, and Clinical Management): A Retrospective
Summary of the Home Health Prospective Payment System Final Rule FY 2014
 Summary of the Home Health Prospective Payment System Final Rule FY 2014 Medicare and Medicaid Programs; Home Health Prospective Payment System Rate Update for CY 2014, Home Health Quality Reporting Requirements,
Summary of the Home Health Prospective Payment System Final Rule FY 2014 Medicare and Medicaid Programs; Home Health Prospective Payment System Rate Update for CY 2014, Home Health Quality Reporting Requirements,
Introduction to Evidence Based Medicine:
 Introduction to Evidence Based Medicine: General Abdominal Examination o Inspection Cullen s sign and Grey Turner s sign are indications of intraperitoneal or retroperitoneal hemorrhage. Traditionally,
Introduction to Evidence Based Medicine: General Abdominal Examination o Inspection Cullen s sign and Grey Turner s sign are indications of intraperitoneal or retroperitoneal hemorrhage. Traditionally,
In The Name of God. Advanced Concept of Nursing- II UNIT- V Advance Nursing Management of GIT diseases. Cholecystitis.
 In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI) Advanced Concept of Nursing- II UNIT- V Advance Nursing Management of GIT diseases. Cholecystitis. Shahzad Bashir RN, BScN, DCHN,MScN
In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI) Advanced Concept of Nursing- II UNIT- V Advance Nursing Management of GIT diseases. Cholecystitis. Shahzad Bashir RN, BScN, DCHN,MScN
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Anaesthesia. Update in. Acute Pancreatitis - A Clinical Overiew. Chris Langrish Correspondence
 Update in Anaesthesia Acute Pancreatitis - A Clinical Overiew Chris Langrish Correspondence Email: chrislangrish@blueyonder.co.uk INTRODUCTION Acute pancreatitis is characterized by upper abdominal pain
Update in Anaesthesia Acute Pancreatitis - A Clinical Overiew Chris Langrish Correspondence Email: chrislangrish@blueyonder.co.uk INTRODUCTION Acute pancreatitis is characterized by upper abdominal pain
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
KIDNEY FAILURE. What causes kidney failure People who are most at risk for kidney failure usually have one or more of the following causes:
 KIDNEY FAILURE Your kidneys are a pair of organs located toward your lower back. One kidney is on each side of your spine. They filter your blood and remove toxins from your body. Your kidneys send toxins
KIDNEY FAILURE Your kidneys are a pair of organs located toward your lower back. One kidney is on each side of your spine. They filter your blood and remove toxins from your body. Your kidneys send toxins
U Nordic Forum - Trauma & Emergency Radiology. Lecture Objectives. MDCT in Acute Pancreatitis. Acute Pancreatitis: Etiologies
 Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Laboratory tests in emergency medicine. Dr O Kiabilua Block SA 13 Department of Chemical Pathology University of Pretoria
 Laboratory tests in emergency medicine Dr O Kiabilua Block SA 13 Department of Chemical Pathology University of Pretoria Acute abdomen The diagnosis depends : The clinical examination, Experience of the
Laboratory tests in emergency medicine Dr O Kiabilua Block SA 13 Department of Chemical Pathology University of Pretoria Acute abdomen The diagnosis depends : The clinical examination, Experience of the
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Role of Imaging Methods in Diagnosis of Acute Pancreatitis. Válek V. Radiologická klinika, FN Brno a LF MU v Brně
 Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Gastrointestinal & Genitourinary Emergencies. Lesson Goal. Learning Objectives 9/10/2012
 Gastrointestinal & Genitourinary Emergencies Lesson Goal Recognize, assess & provide care to patients with abdominal cavity injuries Learning Objectives Discuss different causes of nontraumatic abdominal
Gastrointestinal & Genitourinary Emergencies Lesson Goal Recognize, assess & provide care to patients with abdominal cavity injuries Learning Objectives Discuss different causes of nontraumatic abdominal
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Chapter 18 - Gastrointestinal & Urologic Emergencies
 1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
Evidence Process for Abdominal Pain Guideline Research 11/16/2017. Guideline Review using ADAPTE method and AGREE II instrument 11/16/2017
 Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Role of imaging in the evaluation of the acute abdomen
 Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
Chapter 45 3/2/2017. Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder
 Chapter 45 Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights
Chapter 45 Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
Cholelithiasis & cholecystitis
 1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Imaging Criteria (CT findings) Inflammatory changes localized to appendix +/- appendiceal dilation +/- contrast non-filling
 Inflammatory changes localized to appendix +/- appendiceal dilation +/- contrast non-filling") Table 1. Data Dictionaries for Grading System for EGS Conditions A. Acute Appendicitis I Description Acutely inflamed appendix, intact Gangrenous appendix, intact Perforated appendix with local contamination
Table 1. Data Dictionaries for Grading System for EGS Conditions A. Acute Appendicitis I Description Acutely inflamed appendix, intact Gangrenous appendix, intact Perforated appendix with local contamination
Causes of abdominal pain Doctors in the ED spend lots of time and money diagnosing abdominal pain. They still often do not know the exact cause
 1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
Imaging of common diseases of hepatobiliary and GI system
 Imaging of common diseases of hepatobiliary and GI system Natthaporn Tanpowpong, M.D. Diagnostic radiology Faculty of Medicine, Chulalongkorn University Normal plain radiograph A = Common bile duct
Imaging of common diseases of hepatobiliary and GI system Natthaporn Tanpowpong, M.D. Diagnostic radiology Faculty of Medicine, Chulalongkorn University Normal plain radiograph A = Common bile duct
Chapter 24 - Abdominal_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Acute Pancreatitis. What is the Pancreas? What does it do? What is acute pancreatitis? What causes acute pancreatitis? What symptoms do you get?
 In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Acute Pancreatitis www.corecharity.org.uk What is the Pancreas? What does it do? What is acute pancreatitis? What causes
In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Acute Pancreatitis www.corecharity.org.uk What is the Pancreas? What does it do? What is acute pancreatitis? What causes
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Joint Trust Management of Acute Severe Pancreatitis in Adults
 A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Comparison of Different Scoring System in Predicting the Severity and Prognosis of Acute Pancreatitis
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 5 Ver. 3 (May. 2018), PP 56-60 www.iosrjournals.org Comparison of Different Scoring System
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 5 Ver. 3 (May. 2018), PP 56-60 www.iosrjournals.org Comparison of Different Scoring System
Definitions. You & Your New Transplant ` 38
 Definitions Acute Short, relatively severe Analgesic Pain medicine Anemia A low number of red blood cells Anesthetic Medication that dulls sensation in order to reduce pain Acute Tubular Necrosis (ATN)
Definitions Acute Short, relatively severe Analgesic Pain medicine Anemia A low number of red blood cells Anesthetic Medication that dulls sensation in order to reduce pain Acute Tubular Necrosis (ATN)
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
5. Which component of the duodenal contents entering the stomach causes the most severe changes to gastric mucosa:
 Gastro-intestinal disorders 1. Which are the most common causes of chronic gastritis? 1. Toxic substances 2. Chronic stress 3. Alimentary factors 4. Endogenous noxious stimuli 5. Genetic factors 2. Chronic
Gastro-intestinal disorders 1. Which are the most common causes of chronic gastritis? 1. Toxic substances 2. Chronic stress 3. Alimentary factors 4. Endogenous noxious stimuli 5. Genetic factors 2. Chronic
Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas)
 (see also: biliary/pancreatic folios => pancreas)") Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas) Physiology ductal system produces bicarb, high carbonic anhydrase secretin primary stimulus duodenal enterokinase activates trypsin
Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas) Physiology ductal system produces bicarb, high carbonic anhydrase secretin primary stimulus duodenal enterokinase activates trypsin
Abdominal ultrasound:
 Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Bile composition. Pathophysiology of Gallstone Formation and Pancreatitis. Bile
 Bile composition Pathophysiology of Gallstone Formation and Pancreatitis Robert F. Schwabe rfs2102@columbia.edu Phospholipids Miscellaneous (Pigment, Protein) (Lecithin) Bile Salts 0.7% 4% H 2 0 1% 12%
Bile composition Pathophysiology of Gallstone Formation and Pancreatitis Robert F. Schwabe rfs2102@columbia.edu Phospholipids Miscellaneous (Pigment, Protein) (Lecithin) Bile Salts 0.7% 4% H 2 0 1% 12%
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil
 Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Cardiac Pathology & Rehabilitation
 Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll