Interventional Techniques for Cancer Pain Management
|
|
|
- Tyrone Wade
- 5 years ago
- Views:
Transcription
1 Interventional Techniques for Cancer Pain Management Musa M. Aner, MD Director, Cancer Pain Service Arnold Pain Management Center Beth Israel Deaconess Medical Center
2 Disclosure No financial or industry relationships to disclose. Off-label use of drugs will be discussed.
3 Objectives Evaluation of pain in cancer patients Review the indications of interventional pain techniques in cancer patients Discuss different modalities of interventional pain management
4 Incidence of Cancer Pain Up to 70% of patients with advanced cancer report pain: Tumor related (67%) - Direct invasion of the tumor into nerves, bones, soft tissue, ligaments, and fascia Treatment related (23%) - Surgery related - Radiation related bone necrosis, myelopathy and plexopathies - Chemotherapy related mucositis, peripheral neuropathies, and aseptic bone necrosis Unrelated to cancer (10%)
5 Neuropathic pain Types of Pain Described as burning, shooting, electric-like Results from damage or altered function of a nerve Caused by tumor invasion to any areas of the nerves Brachial plexus invasion due to breast cancer Tumor compression of nerves/spinal cord Nociceptive / Visceral pain Described as a dull ache, throbbing or sharp pain Transmitted by nociceptors responsive to high-intensity mechanical, thermal, and chemical stimuli Tumor expansion inside viscera, soft tissue or bone Frequently occurs with metastasis to the bone common progression of breast, prostate and lung cancers
6 Cancer Pain Prevalent and multifactorial Severe and chronic in 67% of patients with advanced disease 46% of dying patients are inadequately treated for their pain, as reported by family members. Close to 80% of cancer patients in pain are well managed by the 3-Step Ladder Model 15-20% of patients with inadequate pain control Bruera, E. et al. Opioid rotation in patients with cancer pain. A retrospective comparison of dose ratios between methadone, hydromorphone, and morphine. Cancer 1996,78:

7
8 4th Step- Beyond WHO Ladder Neuroaxial Techniques - Epidural / Intrathecal Infusion Therapy Neurolytic Techniques - Chemical - Cryoablation - Radiofrequency Neuromodulation Techniques - Spinal Cord and Peripheral Nerve Stimulation Vertebroplasty / Kyphoplasty Lamer, T. Treatment of Cancer-Related Pain: When Orally Administered Medications Fail. Mayo Clinic Proceedings, 1994,69:
9 Indications (I) Intractable pain despite high doses of opioids with adjuvants Persistent VAS>5 Neuropathic nature Refractory after opioid rotation (minimum 2 different opioids) Opioid induced hyperalgesia Pain amenable to interventional therapy Anatomical and clinical correlation
10 Indications(II) Uncontrolled side effects due to high dose systemic opioid therapy Fatigue More prevalent than pain in patients with metastatic cancer Depressed level of consciousness/ Sedation Dose-limiting problems Constipation Nausea Delirium/ Confusion Respiratory depression
 Sepsis Infection at injection/procedure site Tumor invasion at injection/procedure site Skin breakdown at")
11 Contraindications Coagulopathy INR >1.3 Thrombocytopenia < 100K (?) Sepsis Infection at injection/procedure site Tumor invasion at injection/procedure site Skin breakdown at injection/procedure site Patient refusal Poor access to treatment
12 Neuroaxial Techniques Advantages: Targeted therapy- NMDA & opioid reseptors, Ca +2 channels Decreased systemic medication Decreased toxicity Disadvantages: Invasive Risk for complications Specialized treatments Rauck RL et al. Long-term intrathecal opioid therapy with a patient activated, implanted delivery system for the treatment of cancer pain. J Pain 2003; 4:
13 Neuroaxial Techniques Reduced Dose : Pain control with reduced side effects 300 mg oral morphine: 10 mg epidural morphine 300 mg oral morphine: 1 mg intrathecal morphine
14 Epidural Infusion Therapy Anatomy Pros Reduced risk of respiratory depression and motor block Cons 80-90% of drug is systemically absorbed Possible dural fibrosis can occlude catheter Greater dose requirement Increased risk of infection with long-term use Mostly used as a trial method prior to implantation Consider if life expectancy < 3 months
15 Intrathecal Infusion Therapy Anatomy Pros Lower drug dose Faster onset of analgesia Lower incidence of side effects Longer interval between refills Cons Potential CSF leakage leading to spinal headache Increased risk of meningeal infection or neural injury Intrathecal granulomas Levy, R. Implanted Drug Delivery Systems for Control of Chronic Pain. Ch. 19 of Neurosurgical Management of Pain. New York, NY: Springer-Verlag;1997.

16
17 Intrathecal Drugs Morphine Action site: Substantia gelatinosa Dorsal Horn Dose dependent analgesia- mu receptor The ONLY opioid approved by the FDA for IT use Effective in nociceptive pain Adverse effects Somnolence, weight gain, nightmares, vomiting, itching, constipation, respiratory depression, decreased libido Granuloma formation mg/day
18 Intrathecal Drugs Hydromorphone Semisynthetic hydrogenated ketone of morphine More potent and faster- acting due to greater lipophilic properties Mu receptor (primary), delta and k-opioid receptors Smaller spinal distribution than Morphine- Less SE Granuloma formation (?) 1 case report Equianalgesic dose: 20% of IT Morphine dose Effective in nociceptive pain Johansen MJ et al. Pain Med 2004,5:14-25.
19 Intrathecal Drugs Bupivacaine Improvement in quality of pain relief Synergism to opioids Effective at the site of the catheter tip Nociceptive and neuropathic pain Stable with Morphine+Clonidine or Hydromorphone+Clonidine for 90 days at 37 C
20 Intrathecal Drugs Clonidine Selective alpha-2-adrenergic agonist Lipophilic Approved by the FDA for epidural use Dose-dependent anti-hypersensitivity to mechanical stimuli in a rat model of neuropathic pain Stable with Hydromorphone SE: Reduced MAP & HR
21 Intrathecal Drugs Ziconotide (SNX-111) A nonopioid analgesic and a voltage sensitive, N-type Calcium channel blocker Potent synthetic neuroactive peptide isolated from the venom of a marine snail SE: Elevated creatine kinase levels, sedation, somnolence, nausea, headache, neuropsychiatric symptoms, ataxia, gait disturbance, double vision Neuropathic agent Staats et al. Intrathecal ziconotide in the treatmet of refractory pain in patients with cancer or AIDS. JAMA 2004;291:63-70.
22 Intrathecal Drugs Line 1 Morphine/ Hydromorphone/ Ziconotide/ Fentanyl Line 2 Morphine/ Hydromorphone/ Fentanyl + Bupivacaine Morphine/Hydromorphone/ Fentanyl + Ziconotide Line 3 Opioid + Clonidine Deer, TK et al. Polyanalgesic consensus conference 2012: Recommendations for the management of pain by intrathecal drug delivery. Report of an interdisciplinary expert panel. Neuromodulation 2012, 15:

23 Implantable Drug Delivery Systems (IDDS) Hockey-puck sized Attached to a catheter Programmable Reservoir 20 or 40 ml Internalized Low maintenance Costly, yet cost effective
24 Efficacy of IDDS Cancer Pain Trial 2002 by Smith TJ et al Clinical trial of efficacy of Intrathecal Drug Delivery System (IDDS) plus comprehensive medical management (CMM) vs. CMM alone for patients with refractory cancer pain Randomized Prospective International (5 countries) Multi-center (21 centers) Smith TJ et al. Randomized clinical trial of an implantable drug delivery system compared with comprehensive medical management for refractory cancer pain: impact on pain, drug-related toxicity, and survival. J. Clin. Oncol & 2005.
25 At the end of 4 weeks: Efficacy of IDDS CMM+IDDS group reported: Significant decrease in fatigue Elevated level of consciousness Pain reduction (VAS) 39.1% for CMM, 51.5% for IDDS Toxicity 17.1% for CMM, 50.3% for IDDS (p=0.004) At 6 months: (incidental finding) 54% of IDDS patients alive versus 37% of CMM patients
26 Outcomes Improved clinical success Reduced pain scores Relieved most toxicity of pain control drugs Increased survival for duration of 6 month trial Pain control = Increased survival
27 Neurolysis Intentional injury to a nerve or group of nerves Chemical (alcohol or phenol) Thermal (heat- radiofrequency) Surgical Cryogenic (freezing) Predominantly neuronal axonal damage; cell body is preserved
28 Chemical Neurolysis Pros: Targeted relief Usually single shot Cons: Effective for 3-6 months at most Risk of neuritis, neurologic deficit, damage to non-neural tissue or nontargeted neural structures Incomplete pain relief


29 Cryoablation
30 Neurolytic Blockade and Corresponding Anatomic Structures Stellate Ganglion Head and neck Gasserian Ganglion Face/mouth, trigeminal distribution Thoracic sympathetic chain Upper extremities, thorax, esophagus, lungs Celiac plexus Pancreas, stomach, transverse colon Lumbar sympathetic chain Lower extremities, ureters, kidneys, testes Hypogastric plexus Uterus, ovaries, bladder, prostate, descending and sigmoid colon Ganglion impar Perineum, rectum,anus, vagina, urethra, vulva
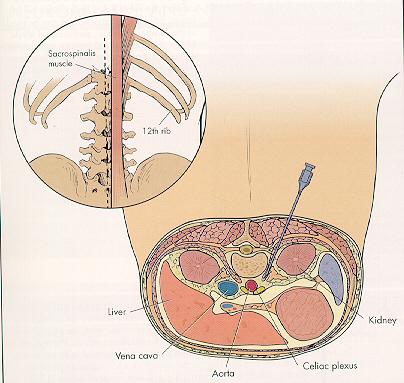
31 Celiac Plexus Block and Neurolysis First descibed by Kappis in 1919 One of the most useful and effective neurolytic blocks Pancreatic, primary intraabdominal and hepatic metastatic tumors Network of neuronal ganglia under the diaphragmatic crus in the retroperitoneal space, anterolateral to the aorta Greater, lesser and least splanchnic nerves (sympathetic rami from T5-T12) and superior mesenteric ganglion
32 Celiac Plexus Block and Neurolysis Anatomy Sympathetic fibers from the splanchnic nerves, vagal parasympathetic fibers and visceral afferent fibers Function Nociceptive transmission innervating the pancreas, liver, gallbladder, stomach, spleen, kidneys, intestines and adrenals

33
34 Celiac Plexus Block and Neurolysis Percutaneous Techniques (need fluoroscopic or CT guidance) Transcrural Approach Two needle Retrocrural Approach Two needle splanchnic Transaortic Approach Single needle through the aorta Anterior Approach Single needle w/ CT or US guidance Endoscopic US Guided Technique
35 Celiac Plexus Block and Neurolysis Complications: Hypotension - transient Diarrhea - transient Hematuria from renal injury Pain at the site of injection Pneumothorax Impotence Paraplegia (1%) -Ischemia of anterior spinal cord due to vasospasm or mechanical injury to the Artery of Adamkiewicz
36 Celiac Plexus Block and Neurolysis Efficacy: RCT of 24 patients show decreased use of analgesics in the group that received NCPB A meta-analysis of NCPB for pancreatic and other intraabdominal cancer pain demonstrates 90% of the patients reported partial to complete relief at 3 months, while 70-90% patients had partial to complete relief at the time of death Moore JC, Adler DG. Celiac Plexus Neurolysis for Pain Relief in Pancreatic Cancer. The Journal of Supportive Oncology 2009, 7:3,
37

38


39


40 Splanchnic Nerve RFL Bilateral Thoracic Splanchnic Nerve Radiofrequency Thermocoagulation for the Management of End-Stage Pancreatic Abdominal Cancer Pain Papadopoulos et al. Pain Physician 2013; 16: Retrospective study of 35 patients at the end of life followed for 6 months Sustained pain relief from 8.9/10 to 3-4/10 Improved QOL and decreased opioid consumption
41 Anatomy Superior Hypogastric Block and Neurolysis The sympathetic trunk from T10-L2 and the parasympathetic fibers from S2-S4 create neuronal network at the anterior projection of the sacral promontorium at L5-S1 level Located retroperitoneally in the subserous fascia of the common iliac bifurcation Function Sensory information from the bladder, rectum, prostate, testes, vagina, uterus, ovaries and descending and sigmoid colon
42 Superior Hypogastric Block and Neurolysis Percutaneous techniques: Initially described by Plancarte in 1990 for the treatment of pelvic cancer pain Requires fluoroscopic or CT guidance Posterior Approach: Two needle technique Transdiscal Approach: Through L5-S1 disc space Anterior Approach: Single needle technique


43

44

45

46
47 Superior Hypogastric Block and Neurolysis Complications: Hypotension Pain at injection tract Bladder puncture Retroperitoneal hematoma L5- S1 nerve root injury Disciitis (1-4%)
48 Superior Hypogastric Block and Efficacy: A trial of 227 patients Neurolysis 72% reported effective pain relief with reduction of opioid consumption At 6 months, 69% had continued pain relief Plancarte, R. Et al. Neurolytic superior hypogastric plexus block for chronic pelvic pain associated with cancer. Reg. Anesth. 1997, 22: Only one RCT comparing opiod therapy with neurolytic SHP found decreased pain intensity, opioid consumption and increased quality of life de Oliveira,R. et al. The effects of early or late neurolytic sympathetic plexus block on the management of abdominal or pelvic cancer pain. Pain 2004, 110:
49 Ganglion Impar Block and Neurolysis First described by Plancarte in 1990 for the treatment of intractable perineal pain Primary indications are perineal pain due to anal or rectal cancer Anatomy: Located anterior to the lower portion of the first cocygeal body Termination of the paravertebral sympathetic chains
50 Function: Ganglion Impar Block and Neurolysis Contains visceral afferent fibers that innervate the perineum, distal part of the rectum, anus, distal urethra, distal third of the vagina and vulva Techniques: Anococcygeal Approach Trans-Sacrococcygeal Approach Intercoccygeal Approach Coccygeal Transverse Approach
51 Ganglion Impar Block and Neurolysis Complications: Rectal perforation Sacral nerve root injury Epidural injection Bowel or bladder dysfunction Efficacy: Two prospective studies with good efficacy One study using RF lesioning with 50% decrease in pain scores

52
53 Conclusion The need and responsibility to treat pain Communication between disciplines to establish treatment goals Risk / Benefit ratio Patient preference Vigilance Multimodal therapy To cure sometimes, to relieve often, to comfort always Anonymous
Interventional Techniques for Cancer Pain Management
 Interventional Techniques for Cancer Pain Management Musa M. Aner, MD Director, Cancer Pain Service Arnold - Warfield Pain Center Beth Israel Deaconess Medical Center Boston, MA Disclosure No financial
Interventional Techniques for Cancer Pain Management Musa M. Aner, MD Director, Cancer Pain Service Arnold - Warfield Pain Center Beth Israel Deaconess Medical Center Boston, MA Disclosure No financial
nerve blocks in the diagnosis and therapy of visceral disease
 Visceral Pain nerve blocks in the diagnosis and therapy of visceral disease Guy Hans, MD, PhD Dept. of Anesthesiology, Multidisciplinary Pain Center Visceral Pain? Type of nociceptive pain (although often
Visceral Pain nerve blocks in the diagnosis and therapy of visceral disease Guy Hans, MD, PhD Dept. of Anesthesiology, Multidisciplinary Pain Center Visceral Pain? Type of nociceptive pain (although often
14RC1-PERRUCHOUD Interventional management of cancer pain
 14RC1-PERRUCHOUD Interventional management of cancer pain Christophe Perruchoud Department of Anaesthesiology and Pain Management, University Hospital Centre and University of Lausanne, Lausanne Background
14RC1-PERRUCHOUD Interventional management of cancer pain Christophe Perruchoud Department of Anaesthesiology and Pain Management, University Hospital Centre and University of Lausanne, Lausanne Background
Celiac plexus block. Dr.Kasturi Bhagawati Asst.professor Dept. of Emergency Medicine & Critical care.
 Celiac plexus block Dr.Kasturi Bhagawati Asst.professor Dept. of Emergency Medicine & Critical care. Introduction A celiac plexus block is an injection of local anesthetic into or around the celiac plexus
Celiac plexus block Dr.Kasturi Bhagawati Asst.professor Dept. of Emergency Medicine & Critical care. Introduction A celiac plexus block is an injection of local anesthetic into or around the celiac plexus
SYMPATHETIC BLOCKS AND THEIR ROLE IN MANAGEMENT AND DIAGNOSIS OF CHRONIC PAIN SYNDROMES
 SYMPATHETIC BLOCKS AND THEIR ROLE IN MANAGEMENT AND DIAGNOSIS OF CHRONIC PAIN SYNDROMES Overview Eugene Mitchell, MD Activity of the sympathetic efferents and their role in the pathology of chronic pain
SYMPATHETIC BLOCKS AND THEIR ROLE IN MANAGEMENT AND DIAGNOSIS OF CHRONIC PAIN SYNDROMES Overview Eugene Mitchell, MD Activity of the sympathetic efferents and their role in the pathology of chronic pain
Types of blocks. Clinical considerations 8/11/2009. Let s Discuss Sympathetic Blocks. Stellate Celiac plexis Lumbar sympathetic Hypogastric
 Let s Discuss Sympathetic Blocks Janette Elliott, RN-BC, MSN, AOCN ASPMN 19 th Annual Conference September 2009 Types of blocks Stellate Celiac plexis Lumbar sympathetic Hypogastric Clinical considerations
Let s Discuss Sympathetic Blocks Janette Elliott, RN-BC, MSN, AOCN ASPMN 19 th Annual Conference September 2009 Types of blocks Stellate Celiac plexis Lumbar sympathetic Hypogastric Clinical considerations
Dr P.W.Buczkowski. Consultant in Anaesthesia & Pain Medicine. Royal Derby Hospital
 Dr P.W.Buczkowski Consultant in Anaesthesia & Pain Medicine Royal Derby Hospital INTERVENTIONAL PAIN MANAGEMENT III Neuroaxial Drug Delivery KYIV May 2010 Dr J Azzopardi MD FRCA FFPMANZCA FFPMRCA Consultant
Dr P.W.Buczkowski Consultant in Anaesthesia & Pain Medicine Royal Derby Hospital INTERVENTIONAL PAIN MANAGEMENT III Neuroaxial Drug Delivery KYIV May 2010 Dr J Azzopardi MD FRCA FFPMANZCA FFPMRCA Consultant
Pain Management Clinic ISIC
 Pain Management Clinic ISIC Let us rebuild a pain free life Pain is one of the commonest symptoms in patients attending OPDs of various hospitals and clinics. Chronic pain is any pain that has persisted
Pain Management Clinic ISIC Let us rebuild a pain free life Pain is one of the commonest symptoms in patients attending OPDs of various hospitals and clinics. Chronic pain is any pain that has persisted
Fig Glossopharyngeal nerve transmits signals to medulla oblongata. Integrating center. Receptor. Baroreceptors sense increased blood pressure
 Fig. 5. Integrating center Glossopharyngeal nerve transmits signals to medulla oblongata Receptor 3 Vagus nerve transmits inhibitory signals to cardiac pacemaker Baroreceptors sense increased blood pressure
Fig. 5. Integrating center Glossopharyngeal nerve transmits signals to medulla oblongata Receptor 3 Vagus nerve transmits inhibitory signals to cardiac pacemaker Baroreceptors sense increased blood pressure
Chapter 15: The Autonomic Nervous System. Copyright 2009, John Wiley & Sons, Inc.
 Chapter 15: The Autonomic Nervous System Comparison of Somatic and Autonomic Nervous Systems Comparison of Somatic and Autonomic Nervous Systems Anatomy of Autonomic Motor Pathways Preganglionic neuron
Chapter 15: The Autonomic Nervous System Comparison of Somatic and Autonomic Nervous Systems Comparison of Somatic and Autonomic Nervous Systems Anatomy of Autonomic Motor Pathways Preganglionic neuron
Non-Pharmacological Management of Pain. Anesthetic interventions Neurosurgical interventions Cognitive behavioral therapy Physical Therapies
 Non-Pharmacological Management of Pain Anesthetic interventions Neurosurgical interventions Cognitive behavioral therapy Physical Therapies Practice Pharmacotherapy treats majority of pain(90%). Occasionally
Non-Pharmacological Management of Pain Anesthetic interventions Neurosurgical interventions Cognitive behavioral therapy Physical Therapies Practice Pharmacotherapy treats majority of pain(90%). Occasionally
CELIAC PLEXUS NEUROLYSIS WITH REPEATED AMMONIUM SULPHATE INJECTION FOR THE TREATMENT OF CHRONIC NON- CANCER ABDOMINAL PAIN UNDER CT SCAN GUIDANCE
 CELIAC PLEXUS NEUROLYSIS WITH REPEATED AMMONIUM SULPHATE INJECTION FOR THE TREATMENT OF CHRONIC NON- CANCER ABDOMINAL PAIN UNDER CT SCAN GUIDANCE By Eshaq AlShaqaq Clinical fellow Introduction Celiac Plexus
CELIAC PLEXUS NEUROLYSIS WITH REPEATED AMMONIUM SULPHATE INJECTION FOR THE TREATMENT OF CHRONIC NON- CANCER ABDOMINAL PAIN UNDER CT SCAN GUIDANCE By Eshaq AlShaqaq Clinical fellow Introduction Celiac Plexus
Organisation of the nervous system
 Chapter1 Organisation of the nervous system 1. Subdivisions of the nervous system The nervous system is divided: i) Structurally The central nervous system (CNS) composed of the brain and spinal cord.
Chapter1 Organisation of the nervous system 1. Subdivisions of the nervous system The nervous system is divided: i) Structurally The central nervous system (CNS) composed of the brain and spinal cord.
ALTERNATIVAS A LA ADMINISTRACION: OPIOIDES IT
 ALTERNATIVAS A LA ADMINISTRACION: OPIOIDES IT Oscar A. de Leon-Casasola, MD Professor of Anesthesiology and Medicine Senior Vice-Chair Dept. of Anesthesiology, The Jacobs School of Medicine Chief, Pain
ALTERNATIVAS A LA ADMINISTRACION: OPIOIDES IT Oscar A. de Leon-Casasola, MD Professor of Anesthesiology and Medicine Senior Vice-Chair Dept. of Anesthesiology, The Jacobs School of Medicine Chief, Pain
Sympathetic Nervous System
 Sympathetic Nervous System Lecture Objectives Review the subdivisions of the nervous system. Review the general arrangement and compare the sympathetic and parasympathetic parts. Describe the following
Sympathetic Nervous System Lecture Objectives Review the subdivisions of the nervous system. Review the general arrangement and compare the sympathetic and parasympathetic parts. Describe the following
The Nervous System: Autonomic Nervous System
 17 The Nervous System: Autonomic Nervous System PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction The autonomic nervous system functions
17 The Nervous System: Autonomic Nervous System PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction The autonomic nervous system functions
Chapter 16. APR Enhanced Lecture Slides
 Chapter 16 APR Enhanced Lecture Slides See separate PowerPoint slides for all figures and tables pre-inserted into PowerPoint without notes and animations. Copyright The McGraw-Hill Companies, Inc. Permission
Chapter 16 APR Enhanced Lecture Slides See separate PowerPoint slides for all figures and tables pre-inserted into PowerPoint without notes and animations. Copyright The McGraw-Hill Companies, Inc. Permission
The Nervous System: Autonomic Nervous System Pearson Education, Inc.
 17 The Nervous System: Autonomic Nervous System Introduction The autonomic nervous system: Functions outside of our conscious awareness Makes routine adjustments in our body s systems The autonomic nervous
17 The Nervous System: Autonomic Nervous System Introduction The autonomic nervous system: Functions outside of our conscious awareness Makes routine adjustments in our body s systems The autonomic nervous
ANATOMY & PHYSIOLOGY - CLUTCH CH THE AUTONOMIC NERVOUS SYSTEM.
 !! www.clutchprep.com ANATOMY & PHYSIOLOGY - CLUTCH CONCEPT: THE AUTONOMIC NERVOUS SYSTEM: DIVISIONS AND STRUCTURE The Autonomic Nervous System and its Divisions: Autonomic Nervous System (ANS) controls
!! www.clutchprep.com ANATOMY & PHYSIOLOGY - CLUTCH CONCEPT: THE AUTONOMIC NERVOUS SYSTEM: DIVISIONS AND STRUCTURE The Autonomic Nervous System and its Divisions: Autonomic Nervous System (ANS) controls
Cancer Pain Management Pharmacological Treatment and Beyond. Marie Aouad-Maroun MD Professor Department of Anesthesiology
 Cancer Pain Management Pharmacological Treatment and Beyond Marie Aouad-Maroun MD Professor Department of Anesthesiology Palliative and End-of-Life Care Master Class October 18-19, 2013 Pain in cancer
Cancer Pain Management Pharmacological Treatment and Beyond Marie Aouad-Maroun MD Professor Department of Anesthesiology Palliative and End-of-Life Care Master Class October 18-19, 2013 Pain in cancer
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Interventional Pain
 Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Interventional Pain Goals GOALS AND OBJECTIVES The ACGME recognizes that interventional pain medicine
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Interventional Pain Goals GOALS AND OBJECTIVES The ACGME recognizes that interventional pain medicine
Human Anatomy. Autonomic Nervous System
 Human Anatomy Autonomic Nervous System 1 Autonomic Nervous System ANS complex system of nerves controls involuntary actions. Works with the somatic nervous system (SNS) regulates body organs maintains
Human Anatomy Autonomic Nervous System 1 Autonomic Nervous System ANS complex system of nerves controls involuntary actions. Works with the somatic nervous system (SNS) regulates body organs maintains
Dana Alrafaiah. - Amani Nofal. - Ahmad Alsalman. 1 P a g e
 - 2 - Dana Alrafaiah - Amani Nofal - Ahmad Alsalman 1 P a g e This lecture will discuss five topics as follows: 1- Arrangement of pelvic viscera. 2- Muscles of Pelvis. 3- Blood Supply of pelvis. 4- Nerve
- 2 - Dana Alrafaiah - Amani Nofal - Ahmad Alsalman 1 P a g e This lecture will discuss five topics as follows: 1- Arrangement of pelvic viscera. 2- Muscles of Pelvis. 3- Blood Supply of pelvis. 4- Nerve
Group of students. - Rawan almujabili د. محمد المحتسب - 1 P a g e
 - 14 - Group of students - Rawan almujabili د. محمد المحتسب - 1 P a g e Nerves of the posterior abdominal wall The spinal cord gives off spinal nerves between the vertebrae. In the abdomen, through the
- 14 - Group of students - Rawan almujabili د. محمد المحتسب - 1 P a g e Nerves of the posterior abdominal wall The spinal cord gives off spinal nerves between the vertebrae. In the abdomen, through the
ParasymPathetic Nervous system. Done by : Zaid Al-Ghnaneem
 ParasymPathetic Nervous system Done by : Zaid Al-Ghnaneem In this lecture we are going to discuss Parasympathetic, in the last lecture we took sympathetic and one of the objectives of last lecture was
ParasymPathetic Nervous system Done by : Zaid Al-Ghnaneem In this lecture we are going to discuss Parasympathetic, in the last lecture we took sympathetic and one of the objectives of last lecture was
[ANATOMY #12] April 28, 2013
![[ANATOMY #12] April 28, 2013](/thumbs/86/93473883.jpg "[ANATOMY #12] April 28, 2013") Sympathetic chain : Sympathetic chain is each of the pair of ganglionated longitudinal cords of the sympathetic nervous system; extend from level of atlas (base of skull) till coccyx. It is paravertebral
Sympathetic chain : Sympathetic chain is each of the pair of ganglionated longitudinal cords of the sympathetic nervous system; extend from level of atlas (base of skull) till coccyx. It is paravertebral
Nerves on the Posterior Abdominal Wall
 Nerves on the Posterior Abdominal Wall Lumbar Plexus The lumbar plexus, which is one of the main nervous pathways supplying the lower limb, is formed in the psoasmuscle from the anterior ramiof the upper
Nerves on the Posterior Abdominal Wall Lumbar Plexus The lumbar plexus, which is one of the main nervous pathways supplying the lower limb, is formed in the psoasmuscle from the anterior ramiof the upper
Computed tomography versus fluoroscopy guidance in celiac plexus neurolysis for treatment of upper abdominal malignant pain
 Computed tomography versus fluoroscopy guidance in celiac plexus neurolysis for treatment of upper abdominal malignant pain Thesis Submitted for the partial fulfillment of MD Degree in anesthesiology and
Computed tomography versus fluoroscopy guidance in celiac plexus neurolysis for treatment of upper abdominal malignant pain Thesis Submitted for the partial fulfillment of MD Degree in anesthesiology and
Human Anatomy & Physiology
 PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 14 Annie Leibovitz/Contact Press Images 2013 Pearson Education,
PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 14 Annie Leibovitz/Contact Press Images 2013 Pearson Education,
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test
 Analgesia Community Nurses Competency Test") Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
HBA 531 THE BODY. Trunk Examination September 30, What is the effect of the parasympathetic nervous system on: (2.5)
") HBA 531 THE BODY Trunk Examination September 30, 2013 Name: 1. What is the effect of the parasympathetic nervous system on: (2.5) a) Heart rate b) Male reproductive function c) Pylorus d) Internal anal
HBA 531 THE BODY Trunk Examination September 30, 2013 Name: 1. What is the effect of the parasympathetic nervous system on: (2.5) a) Heart rate b) Male reproductive function c) Pylorus d) Internal anal
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Preview from Notesale.co.uk Page 1 of 34
 Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
INTERVENTIONAL PAIN MANAGEMENT UPDATE
 INTERVENTIONAL PAIN MANAGEMENT UPDATE Orlando G. Florete Jr.,M.D. Director, Institute of Pain Management Director, Florida Institute of Medical Research Jacksonville, FL HIPPOCRATIC OATH I I will prescribe
INTERVENTIONAL PAIN MANAGEMENT UPDATE Orlando G. Florete Jr.,M.D. Director, Institute of Pain Management Director, Florida Institute of Medical Research Jacksonville, FL HIPPOCRATIC OATH I I will prescribe
I. Autonomic Nervous System (ANS) A. Dual Innervation B. Autonomic Motor Pathway 1. Preganglionic Neuron a. Preganglionic Fibers (Axons) (1)
 A. Dual Innervation B. Autonomic Motor Pathway 1. Preganglionic Neuron a. Preganglionic Fibers (Axons) (1)") I. Autonomic Nervous System (ANS) A. Dual Innervation B. Autonomic Motor Pathway 1. Preganglionic Neuron a. Preganglionic Fibers (Axons) (1) Acetylcholine - ACh 2. Ganglion (Ganglia) 3. Ganglionic Neuron
I. Autonomic Nervous System (ANS) A. Dual Innervation B. Autonomic Motor Pathway 1. Preganglionic Neuron a. Preganglionic Fibers (Axons) (1) Acetylcholine - ACh 2. Ganglion (Ganglia) 3. Ganglionic Neuron
2018 ASC FINAL Payment Rates
 20526 20550 20551 20552 20553 20600 20605 20610 22510 22511 22513 22514 62263 62264 62268 62269 62270 62272 62273 Injection, therapeutic tendon sheath, ligament injection Tendon origin/insertion injection
20526 20550 20551 20552 20553 20600 20605 20610 22510 22511 22513 22514 62263 62264 62268 62269 62270 62272 62273 Injection, therapeutic tendon sheath, ligament injection Tendon origin/insertion injection
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management
 Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Pathogenesis of Chronic Pelvic Pain
 Pathogenesis of Chronic Pelvic Pain Yong-Chul Kim Department of anesthesia and pain medicine, Seoul National University College of Medicine 1 Overview Anatomy Nerve innervation CPP by pathology CPP by
Pathogenesis of Chronic Pelvic Pain Yong-Chul Kim Department of anesthesia and pain medicine, Seoul National University College of Medicine 1 Overview Anatomy Nerve innervation CPP by pathology CPP by
Chp. 16: AUTONOMIC N.S. (In Review: Peripheral N. S.)
") Chp. 16: AUTONOMIC N.S. (In Review: Peripheral N. S.) Peripheral nerves contain both motor and sensory neurons Among the motor neurons, some of these are somatic and innervate skeletal muscles while some
Chp. 16: AUTONOMIC N.S. (In Review: Peripheral N. S.) Peripheral nerves contain both motor and sensory neurons Among the motor neurons, some of these are somatic and innervate skeletal muscles while some
Part 1. Copyright 2011 Pearson Education, Inc. Copyright 2011 Pearson Education, Inc. Stimulatory
 PowerPoint Lecture Slides prepared by Leslie Hendon University of Alabama, Birmingham C H A P T E R 15 Part 1 The Autonomic Nervous System and Visceral Sensory Neurons The ANS and Visceral Sensory Neurons
PowerPoint Lecture Slides prepared by Leslie Hendon University of Alabama, Birmingham C H A P T E R 15 Part 1 The Autonomic Nervous System and Visceral Sensory Neurons The ANS and Visceral Sensory Neurons
4/8/2015. Autonomic Nervous System (ANS) Learn and Understand: Divisions of the ANS. Sympathetic division Parasympathetic division Dual innervation
 Learn and Understand: Divisions of the ANS. Sympathetic division Parasympathetic division Dual innervation") Autonomic Nervous System (ANS) Learn and Understand: Divisions of the ANS Sympathetic division Parasympathetic division Dual innervation ~ All visceral organs served by both divisions, usually cause opposite
Autonomic Nervous System (ANS) Learn and Understand: Divisions of the ANS Sympathetic division Parasympathetic division Dual innervation ~ All visceral organs served by both divisions, usually cause opposite
cardiac plexus is continuous with the coronary and no named branches pain from the heart and lungs
 Nerves of the Thoracic Region Nerve Source Branches Motor Sensory Notes cardiac plexus cardiac brs. of the vagus n. and cervical ; thoracic l nn. the heart and lungs cardiac, cervical cardiac, vagal vagus
Nerves of the Thoracic Region Nerve Source Branches Motor Sensory Notes cardiac plexus cardiac brs. of the vagus n. and cervical ; thoracic l nn. the heart and lungs cardiac, cervical cardiac, vagal vagus
A New Technique for Superior Hypogastric Plexus Block: The Posteromedian Transdiscal Approach
 Tohoku J. Exp. Med., 2005, A New 206, Transdiscal 277-281Approach for Hypogastric Plexus Block 277 A New Technique for Superior Hypogastric Plexus Block: The Posteromedian Transdiscal Approach Case Report
Tohoku J. Exp. Med., 2005, A New 206, Transdiscal 277-281Approach for Hypogastric Plexus Block 277 A New Technique for Superior Hypogastric Plexus Block: The Posteromedian Transdiscal Approach Case Report
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Autonomic Nervous System DR JAMILA EL MEDANY
 Autonomic Nervous System DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: Define the autonomic nervous system. Describe the structure of autonomic nervous system Trace
Autonomic Nervous System DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: Define the autonomic nervous system. Describe the structure of autonomic nervous system Trace
2019 ASC FINAL Payment Rates
 20526 20550 20551 20552 20553 20600 20605 20610 22510 22511 22513 22514 22869 27279 62263 62264 62268 62269 62270 Injection, therapeutic tendon sheath, ligament injection Tendon origin/insertion injection
20526 20550 20551 20552 20553 20600 20605 20610 22510 22511 22513 22514 22869 27279 62263 62264 62268 62269 62270 Injection, therapeutic tendon sheath, ligament injection Tendon origin/insertion injection
Tymaa Al-zaben & Amin Al-ajalouni
 Done by: Tymaa Al-zaben & Amin Al-ajalouni ** Hello SERTONIN! SLIDE 3 note:: the slide included within the sheet but make sure back to slide for pictures The Autonomic Nervous System Function : Regulate
Done by: Tymaa Al-zaben & Amin Al-ajalouni ** Hello SERTONIN! SLIDE 3 note:: the slide included within the sheet but make sure back to slide for pictures The Autonomic Nervous System Function : Regulate
Autonomic Nervous System. Ms. DS Pillay Room 2P24
 Autonomic Nervous System Ms. DS Pillay Room 2P24 OVERVIEW OF THE NERVOUS SYSTEM NERVOUS SYSTEM CNS PNS BRAIN SPINAL CORD SOMATIC ANS SYMPATHEIC PARASYMPATHEIC LOCATION OF GANGLIA IN THE ANS Short post-ganglionic
Autonomic Nervous System Ms. DS Pillay Room 2P24 OVERVIEW OF THE NERVOUS SYSTEM NERVOUS SYSTEM CNS PNS BRAIN SPINAL CORD SOMATIC ANS SYMPATHEIC PARASYMPATHEIC LOCATION OF GANGLIA IN THE ANS Short post-ganglionic
Interventional Pain. Judith Dunipace MD Board certified in Anesthesiology, Pain Management and Hospice and Palliative Care
 Interventional Pain Judith Dunipace MD Board certified in Anesthesiology, Pain Management and Hospice and Palliative Care IASP Definition of Pain Pain is an unpleasant sensory or emotional experience associated
Interventional Pain Judith Dunipace MD Board certified in Anesthesiology, Pain Management and Hospice and Palliative Care IASP Definition of Pain Pain is an unpleasant sensory or emotional experience associated
Biology 218 Human Anatomy
 Chapter 20 Adapted form Tortora 10 th ed. LECTURE OUTLINE A. Introduction (p. 632) 1. The autonomic nervous system (ANS) regulates the activity of smooth muscle, cardiac muscle, and certain glands. 2.
Chapter 20 Adapted form Tortora 10 th ed. LECTURE OUTLINE A. Introduction (p. 632) 1. The autonomic nervous system (ANS) regulates the activity of smooth muscle, cardiac muscle, and certain glands. 2.
2019 ASC Proposed Payment Rates
 20526 20550 20551 20552 20553 20600 20605 20610 22510 22511 22513 22514 22869 27279 62263 62264 62268 62269 62270 Injection, therapeutic tendon sheath, ligament injection Tendon origin/insertion injection
20526 20550 20551 20552 20553 20600 20605 20610 22510 22511 22513 22514 22869 27279 62263 62264 62268 62269 62270 Injection, therapeutic tendon sheath, ligament injection Tendon origin/insertion injection
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 17, 2014
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 17, 2014 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 17, 2014 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
Inferior Pelvic Border
 Pelvis + Perineum Pelvic Cavity Enclosed by bony, ligamentous and muscular wall Contains the urinary bladder, ureters, pelvic genital organs, rectum, blood vessels, lymphatics and nerves Pelvic inlet (superior
Pelvis + Perineum Pelvic Cavity Enclosed by bony, ligamentous and muscular wall Contains the urinary bladder, ureters, pelvic genital organs, rectum, blood vessels, lymphatics and nerves Pelvic inlet (superior
01/07/2018 MANAGEMENT OF RECTAL TENESMUS PRESENTATION OUTLINE
 MANAGEMENT OF RECTAL TENESMUS Dr. Áine Ní Laoire The Oxford Advanced Pain & Symptom Management Course Nottingham 27 th June 2018 PRESENTATION OUTLINE Definition A Clinical Case Epidemiology Pathophysiology
MANAGEMENT OF RECTAL TENESMUS Dr. Áine Ní Laoire The Oxford Advanced Pain & Symptom Management Course Nottingham 27 th June 2018 PRESENTATION OUTLINE Definition A Clinical Case Epidemiology Pathophysiology
4/9/2019. Autonomic Nervous System (ANS)
") Autonomic Nervous System (ANS) Learn and Understand: What appears to be two separate systems actually work together to maintain homeostasis under varying conditions. Receptors on the membranes of ANS effectors
Autonomic Nervous System (ANS) Learn and Understand: What appears to be two separate systems actually work together to maintain homeostasis under varying conditions. Receptors on the membranes of ANS effectors
Management of Neuropathic pain
 Management of Neuropathic pain Ravi Parekodi Consultant in Anaesthetics and Pain Management 08/04/2014 Ref: BJA July2013, Map of Medicine2013, Pain Physician 2007, IASP 2012, Nice guideline 2013 Aims Highlight
Management of Neuropathic pain Ravi Parekodi Consultant in Anaesthetics and Pain Management 08/04/2014 Ref: BJA July2013, Map of Medicine2013, Pain Physician 2007, IASP 2012, Nice guideline 2013 Aims Highlight
Human Anatomy Key Points Unit 1/ Study Guide
 Human Anatomy Key Points Unit 1/ Study Guide I. Anatomy and Physiology a. Anatomy 1. Means cutting apart (dissection) 2. Study of the body and the relationships of its parts to each other. 3. Dissection
Human Anatomy Key Points Unit 1/ Study Guide I. Anatomy and Physiology a. Anatomy 1. Means cutting apart (dissection) 2. Study of the body and the relationships of its parts to each other. 3. Dissection
Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat.
 Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Cancer Pain. Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center
 Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
The Role of the Neuromodulation in Management of Chronic Pain
 The Role of the Neuromodulation in Management of Chronic Pain Adnan Al-Kaisy, MB ChB, FRCA, FFPMRCA, FIPP Clinical Lead of the Pain Management & Neuromodulation Centre Guy s & St Thomas Hospital, London,
The Role of the Neuromodulation in Management of Chronic Pain Adnan Al-Kaisy, MB ChB, FRCA, FFPMRCA, FIPP Clinical Lead of the Pain Management & Neuromodulation Centre Guy s & St Thomas Hospital, London,
PAIN MANAGEMENT IN UROLOGY
 24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
Review Polyanalgesic Consensus Charles Brooker Royal North Shore Hospital
 Review Polyanalgesic Consensus 2007 Charles Brooker Royal North Shore Hospital cbrooker@med.usyd.edu.au Article review Polyanalgesic Consensus Conference 2007 Recommendations for the management of Pain
Review Polyanalgesic Consensus 2007 Charles Brooker Royal North Shore Hospital cbrooker@med.usyd.edu.au Article review Polyanalgesic Consensus Conference 2007 Recommendations for the management of Pain
CHAPTER 15 LECTURE OUTLINE
 CHAPTER 15 LECTURE OUTLINE I. INTRODUCTION A. The autonomic nervous system (ANS) regulates the activity of smooth muscle, cardiac muscle, and certain glands. B. Operation of the ANS to maintain homeostasis,
CHAPTER 15 LECTURE OUTLINE I. INTRODUCTION A. The autonomic nervous system (ANS) regulates the activity of smooth muscle, cardiac muscle, and certain glands. B. Operation of the ANS to maintain homeostasis,
Current evidence in acute pain management. Jeremy Cashman
 Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
Chapter 16. Sense of Pain
 Chapter 16 Sense of Pain Pain Discomfort caused by tissue injury or noxious stimulation, and typically leading to evasive action important /// helps to protect us lost of pain in diabetes mellitus = diabetic
Chapter 16 Sense of Pain Pain Discomfort caused by tissue injury or noxious stimulation, and typically leading to evasive action important /// helps to protect us lost of pain in diabetes mellitus = diabetic
Basic Body Structure
 Basic Body Structure The Cell All life consists of microscopic living structures called cells. They perform various functions throughout the body. All cells are similar in structure, but not identical.
Basic Body Structure The Cell All life consists of microscopic living structures called cells. They perform various functions throughout the body. All cells are similar in structure, but not identical.
Anatomy. Contents Brain (Questions)
") Anatomy 12 Contents 12.1 Brain (Questions).................................................... 683 12.2 Head and Neck (Questions)............................................. 685 12.3 Thorax (Questions)...................................................
Anatomy 12 Contents 12.1 Brain (Questions).................................................... 683 12.2 Head and Neck (Questions)............................................. 685 12.3 Thorax (Questions)...................................................
44th Annual CME Conference for Physician Assistants. Alexander Bautista, MD Assistant Professor Anesthesiology and Pain Medicine
 44th Annual CME Conference for Physician Assistants Alexander Bautista, MD Assistant Professor Anesthesiology and Pain Medicine Fifth Vital Sign: 15 years later Opioid Epidemic Relevant Disclosure and
44th Annual CME Conference for Physician Assistants Alexander Bautista, MD Assistant Professor Anesthesiology and Pain Medicine Fifth Vital Sign: 15 years later Opioid Epidemic Relevant Disclosure and
ICD-9-CM Diagnosis Code options
 ICD-9-CM Diagnosis Code options Diagnosis codes are used by both physicians and facilities to document the indication for the procedure. Intrathecal drug delivery is directed at managing chronic, intractable
ICD-9-CM Diagnosis Code options Diagnosis codes are used by both physicians and facilities to document the indication for the procedure. Intrathecal drug delivery is directed at managing chronic, intractable
Divisions of ANS. Divisions of ANS 2 Divisions dualing innervate most organs. Autonomic Nervous System (Chapter 9)
") Autonomic Nervous System (Chapter 9) Autonomic Nervous System (ANS) general properties anatomy Autonomic Effects on Target Organs Subs of Nervous System Central nervous system Brain Spinal cord Peripheral
Autonomic Nervous System (Chapter 9) Autonomic Nervous System (ANS) general properties anatomy Autonomic Effects on Target Organs Subs of Nervous System Central nervous system Brain Spinal cord Peripheral
Regional Anesthesia. Fatiş Altındaş Dept. of Anesthesiology
 Regional Anesthesia Fatiş Altındaş Dept. of Anesthesiology Regional anesthesia - Definition Renders a specific area of the body, e.g. foot, arm, lower extremities insensating to stimulus of surgery or
Regional Anesthesia Fatiş Altındaş Dept. of Anesthesiology Regional anesthesia - Definition Renders a specific area of the body, e.g. foot, arm, lower extremities insensating to stimulus of surgery or
Chapter 14 Autonomic Nervous System
 Chapter 14 Autonomic Nervous System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Why This Matters Understanding the autonomic
Chapter 14 Autonomic Nervous System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Why This Matters Understanding the autonomic
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 16, 2015
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
Chapter 16. Autonomic nervous system. AP2 Chapter 16: ANS
 Chapter 16 Autonomic nervous system AP2 Chapter 16: ANS 1 Quick Review Nervous System Central Nervous System Peripheral Nervous System Sensory Division Motor Division Somatic Nervous System Autonomic Nervous
Chapter 16 Autonomic nervous system AP2 Chapter 16: ANS 1 Quick Review Nervous System Central Nervous System Peripheral Nervous System Sensory Division Motor Division Somatic Nervous System Autonomic Nervous
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress REDUCING THE PAIN FACTOR AN UPDATE ON PERI-OPERATIVE ANALGESIA Sandra Forysth, BVSc DipACVA Institute of Veterinary,
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress REDUCING THE PAIN FACTOR AN UPDATE ON PERI-OPERATIVE ANALGESIA Sandra Forysth, BVSc DipACVA Institute of Veterinary,
Pain teaching. Muhammad Laklouk
 Pain teaching Muhammad Laklouk Definition Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage. Sensory (discriminatiory)
Pain teaching Muhammad Laklouk Definition Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage. Sensory (discriminatiory)
AUTONOMIC NERVOUS SYSTEM PART I: SPINAL CORD
 AUTONOMIC NERVOUS SYSTEM PART I: SPINAL CORD How is the organization of the autonomic nervous system different from that of the somatic nervous system? Peripheral Nervous System Divisions Somatic Nervous
AUTONOMIC NERVOUS SYSTEM PART I: SPINAL CORD How is the organization of the autonomic nervous system different from that of the somatic nervous system? Peripheral Nervous System Divisions Somatic Nervous
Discussion Points 10/17/16. Spine Pain is Ubiquitous. Interventional Pain Management
 Interventional Pain Management Blake Christensen, D.O. Fellowship Trained Interventional Pain Management Board Eligible in Anesthesiology and Interventional Pain Management Oklahoma Interventional Pain
Interventional Pain Management Blake Christensen, D.O. Fellowship Trained Interventional Pain Management Board Eligible in Anesthesiology and Interventional Pain Management Oklahoma Interventional Pain
NERVOUS SYSTEM ANATOMY
 INTRODUCTION to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science
INTRODUCTION to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science
NERVOUS SYSTEM ANATOMY
 NTRODUCTON to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science Engineering
NTRODUCTON to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science Engineering
INDEX. Cancerpain alcohol neurolysis for, 5, 20, 53-54
 INDEX Alcohol advantages of, 54 celiac plexus block with, 19-20, 165 chemical hypophysectomy with, 20 complications and side effects of, 18, 19, 45-46, 54-55 contraindications for, 54 doses with, 52 drug
INDEX Alcohol advantages of, 54 celiac plexus block with, 19-20, 165 chemical hypophysectomy with, 20 complications and side effects of, 18, 19, 45-46, 54-55 contraindications for, 54 doses with, 52 drug
PERCUTANEOUS FACET JOINT DENERVATION
 Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-95 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-95 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Transsacrococcygeal Approach to Ganglion Impar Block for Management Of Chronic Perineal Pain: A Prospective Observational Study
 Pain Physician 2007; 10:661-666 ISSN 1533-3159 Prospective Evaluation Transsacrococcygeal Approach to Ganglion Impar Block for Management Of Chronic Perineal Pain: A Prospective Observational Study Gokul
Pain Physician 2007; 10:661-666 ISSN 1533-3159 Prospective Evaluation Transsacrococcygeal Approach to Ganglion Impar Block for Management Of Chronic Perineal Pain: A Prospective Observational Study Gokul
IN PRESS. Case Report. A Challenging Case of Ganglion Impar Block in a Patient with. Kevin Wong, DO and Brian R. Monroe, MD
 Case Report Interventional Pain Management Reports Volume 1, Number 1, pp71-77 2017, American Society of Interventional Pain Physicians A Challenging Case of Ganglion Impar Block in a Patient with Coccygeal
Case Report Interventional Pain Management Reports Volume 1, Number 1, pp71-77 2017, American Society of Interventional Pain Physicians A Challenging Case of Ganglion Impar Block in a Patient with Coccygeal
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution,
 SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution, derivatives 4. Hindgut- limits, evolution, derivatives
SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution, derivatives 4. Hindgut- limits, evolution, derivatives
Anatomy: Know Your Abdomen
 Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Neuropathic Pain. Scott Magnuson, MD Pain Management of North Idaho, PLLC
 Neuropathic Pain Scott Magnuson, MD Pain Management of North Idaho, PLLC Pain is our friend "An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described
Neuropathic Pain Scott Magnuson, MD Pain Management of North Idaho, PLLC Pain is our friend "An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described
A New Technique for Inferior Hypogastric Plexus Block: A Coccygeal Transverse Approach
 Case Report Korean J Pain 2012 January; Vol. 25, No. 1: 38-42 pissn 2005-9159 eissn 2093-0569 http://dx.doi.org/10.3344/kjp.2012.25.1.38 A New Technique for Inferior Hypogastric Plexus Block: A Coccygeal
Case Report Korean J Pain 2012 January; Vol. 25, No. 1: 38-42 pissn 2005-9159 eissn 2093-0569 http://dx.doi.org/10.3344/kjp.2012.25.1.38 A New Technique for Inferior Hypogastric Plexus Block: A Coccygeal
ISPUB.COM. Lumbar Sympathectomy by Laser Technique. S Kantha, B Kantha METHODS AND MATERIALS
 ISPUB.COM The Internet Journal of Minimally Invasive Spinal Technology Volume 1 Number 2 Lumbar Sympathectomy by Laser Technique S Kantha, B Kantha Citation S Kantha, B Kantha. Lumbar Sympathectomy by
ISPUB.COM The Internet Journal of Minimally Invasive Spinal Technology Volume 1 Number 2 Lumbar Sympathectomy by Laser Technique S Kantha, B Kantha Citation S Kantha, B Kantha. Lumbar Sympathectomy by
THE SACRAL PARASYMPATHETIC INNERVATION OF THE COLON
 THE SACRAL PARASYMPATHETIC INNERVATION OF THE COLON RUSSELL T. WOODBURNE Department of Anatomy, University of Michigan Hedical School, Ann Arbofi TWO FIGURES Autonomic nerves distribute by a variety of
THE SACRAL PARASYMPATHETIC INNERVATION OF THE COLON RUSSELL T. WOODBURNE Department of Anatomy, University of Michigan Hedical School, Ann Arbofi TWO FIGURES Autonomic nerves distribute by a variety of
Y A L E S C H O O L O F M E D I C I N E. This is a CME accredited activity. The presenters and there are no conflicts of interest.
 This is a CME accredited activity. The presenters and there are no conflicts of interest. Pain in Pancreatic Cancer More than 50% of patients with pancreatic cancer suffer from abdominal and back pain
This is a CME accredited activity. The presenters and there are no conflicts of interest. Pain in Pancreatic Cancer More than 50% of patients with pancreatic cancer suffer from abdominal and back pain
Introduction to The Autonomic Nervous System. Sympathetic VS Parasympathetic Divisions. Adrenergic and Cholinergic Fibers. ANS Neurotransmitters
 Chapter 15 Introduction to The Autonomic Nervous System Sympathetic VS Parasympathetic Divisions Adrenergic and Cholinergic Fibers ANS Neurotransmitters Autonomic Nervous System Portion of the nervous
Chapter 15 Introduction to The Autonomic Nervous System Sympathetic VS Parasympathetic Divisions Adrenergic and Cholinergic Fibers ANS Neurotransmitters Autonomic Nervous System Portion of the nervous
Epidural Analgesia in Labor - Whats s New
 Epidural Analgesia in Labor - Whats s New Wichelewski Josef 821 Selective neural blockade has many clinical applications in medicine but nowhere has its use been so well accepted than in the field of Obstetrics.
Epidural Analgesia in Labor - Whats s New Wichelewski Josef 821 Selective neural blockade has many clinical applications in medicine but nowhere has its use been so well accepted than in the field of Obstetrics.
The Human Body: An Overview of Anatomy. Anatomy. Physiology. Anatomy - Study of internal and external body structures
 C H A P T E R 1 The Human Body: An Orientation An Overview of Anatomy Anatomy The study of the structure of the human body Physiology The study of body function Anatomy - Study of internal and external
C H A P T E R 1 The Human Body: An Orientation An Overview of Anatomy Anatomy The study of the structure of the human body Physiology The study of body function Anatomy - Study of internal and external