Oral and Maxillofacial Surgeons and the seriously injured patient. Barts and The London NHS Trust
|
|
|
- Gavin Griffin
- 5 years ago
- Views:
Transcription
1 Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust

2 How do you assess this?
3 Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation & Arrest Haemorrhage Disability Exposure

4 Airway & Cervical spine
5 Emergency airways A attempt should be made at oro-tracheal intubation by an experienced senior anaethetist If this fails, needle crico-thyroidotomy is the next step, with jet insufflation. It will buy 30 to 40 mins. Another option is open crico-thyroidotomy with insertion of a size 6 ETT TRACHEOSTOMY HAS NO PLACE IN THE EMERGENCY ROOM (and is not in the ATLS protocol)

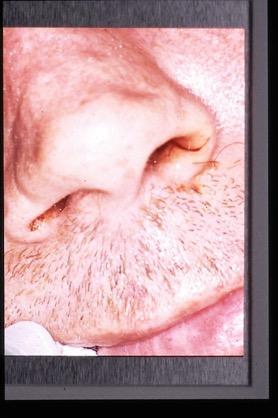
6 Acute airway embarrassment from GSW

7 Circulation & Control Bleeding
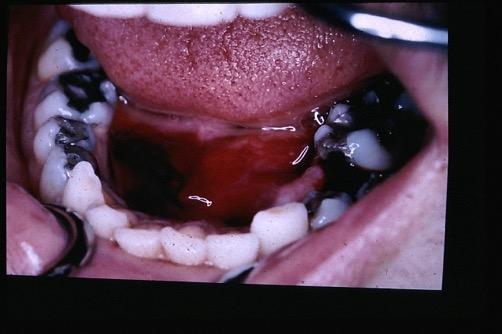
8 Controlling acute maxillofacial bleeding Midface fractures bleed profusely. Place a medium mouth prop on each side and insert an epistat into each nostril Inflate the posterior balloon with saline, tug back and then inflate the anterior one. If epistats are not available then pack the nose using posterior nasal packs.

9 Epistats

10 Nasal Packs

11 D for disability (neurological)
12 Secondary Survey A systematic examination of the entire body from head to toe. Carried out only once the primary survey has been completed and the resulting issues dealt with. A thorough Maxillofacial examination is part of the secondary survey, systematically examining all the facial structures to identify potential injuries. Document findings clearly.
13 Maxillofacial Secondary Survey LOOK for swelling, bruising, lacerations, or signs specific to facial bone fractures (e.g. subconjunctival haemorrhage or Battles sign. FEEL the entire facial skeleton by bilateral palpation to elicit crepitus or steps. If patient conscious test sensation. MOVE the maxilla and mandible to see if there is abnormal mobility indicative of a fracture e.g. lefort 2/3 EXAMINE the eyes for globe injury, visual acuity, pupils and orbit disruption.?ophthalmology. Auroscope for ears EXAMINE the oral cavity for signs of facial bone fractures, avulsed or fractured teeth and dental occlusion. Reassess once extubated

14 Skull Base Interface- CSF
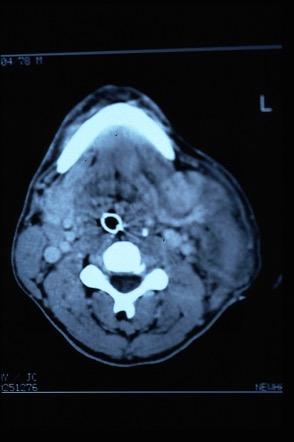
15 Imaging Seriously injured patients usually are going to the CT scanner for their brain, doing axial scans of the facial bones takes minimal extra time. Ask for 3D reformat. Conscious co-operative patients can have a facial bone series (OPG, PA jaws and single Occipitomental). Further imaging is carried out according to the specific injuries identified by the facial bone series or the clinical examination. Chest x-ray if unaccounted missing teeth


16 Maxillofacial Trauma
17 Soft Tissue Trauma


18 Consider the Anatomy..and the mechanism Facial nerve Parotid duct Vasculature Bones

19 Soft Tissue Trauma Immediate management Inspection Irrigation Debridement Haemostasis Closure and repair Tetanus & Antibiotics Know when to refer


20 Know when to refer

21 Suspect vascular injury
22 Beware penetrating neck wounds Size and Level of entry wound is unreliable. Do not explore depth with your finger! Anything deeper than platysma MUST be formally assessed. Obtain history from ambulance crew - type of weapon, amount of blood loss at scene, vital signs Haemodynamic status is important (pulse and BP) If unstable at scene and unstable in resus room - need exploration in main theatre with a vascular surgeon and on table angiogram facility If unstable at scene but stable in resus room - investgate further with CT angiogram If stable at scene and stable in resus - explore and close at leisure
23 Hard Tissue Trauma Mandible Central midface Lateral midface including orbit Dental trauma
24 Mandibular Fractures


25 Sites of Weakness

26 Pathognomonic Signs


27 Condylar Fracture
28 Central Midface Fractures

29 Nasal Bones
30 Nasoethmoid Telecanthus (>35mm) Blunting of canthal angle Loss of nasal bridge projection Upturned nasal tip Loss of almond shaped eye


31 Nasoethmoidal fractures

32 Best chance of correction is at the time of injury..
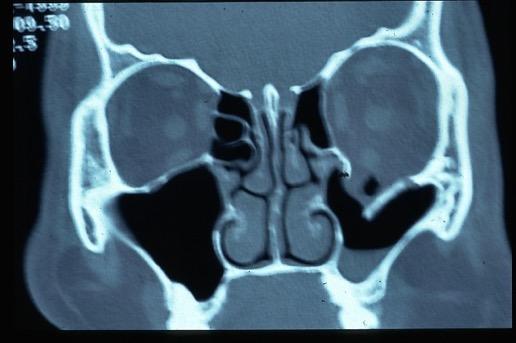
33 Orbital Fractures
34


35 Supra Orbital Fractures


36 Operative View
37 Maxillary & Midface Fractures

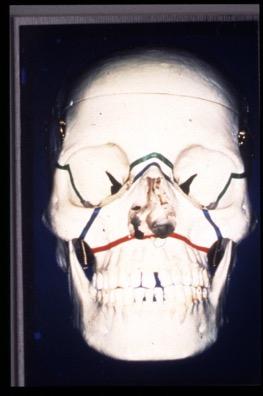
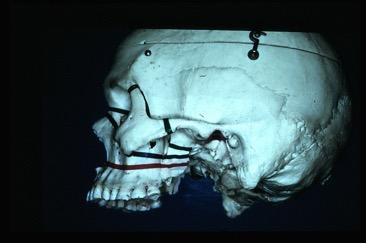
38 Le Fort fractures
39 Signs of Le Fort 2/3 injury Severe swelling/bruising (football) Subconjunctival haemorrhage and chemosis Diplopia and limitation of eye movements Panda eyes/battle sign/csf leaks = skull base Malocclusion and pathological movement of midface

40 Le Fort 2/3 fractures

41 Panda eyes


42 Le Fort II + Palatal Split
43 Lateral Midface


44 Zygomatic injury


45 Eye signs

46 Zygomatic Complex Fracture

47 Injured Anterior Teeth
48 Timing of definitive treatment Maxillofacial bleeding or loss of vision requires immediate intervention Non-brain injured patients can have definitive facial fracture treatment once swelling has reduced and investigations completed, usually first 2 days for mandibles, and 5-10 days for midface/orbit fractures Brain injured patients need combined care by Neurosurgeon, Maxillofacial Surgeon and Ophthalmic surgeon. Timing of Maxillofacial fracture fixation is a team decision, taking into account the risks of worsening the brain injury against the morbidity of leaving the fractures untreated. Try to fix mandible early, midface can wait 2 weeks, by which time the neurological picture will usually have cleared.
49 Thank you.
MAXILLOFACIAL TRAUMA. The on-call maxillofacial surgeons can be contacted through the switchboard at the Southern General Hospital
 MAXILLOFACIAL TRAUMA The on-call maxillofacial surgeons can be contacted through the switchboard at the Southern General Hospital Mandibular Injuries Mechanism of injury Assault, falls, RTA-Direct trauma
MAXILLOFACIAL TRAUMA The on-call maxillofacial surgeons can be contacted through the switchboard at the Southern General Hospital Mandibular Injuries Mechanism of injury Assault, falls, RTA-Direct trauma
15. Facial and dental injuries
 15. Facial and dental injuries Priorities in management Best practice is based on current APLS / ATLS guidelines. Maxillofacial injuries will often take a lower priority than other potentially life or
15. Facial and dental injuries Priorities in management Best practice is based on current APLS / ATLS guidelines. Maxillofacial injuries will often take a lower priority than other potentially life or
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
TRAUMA TO THE FACE AND MOUTH
 Dr.Yahya A. Ali 3/10/2012 F.I.C.M.S TRAUMA TO THE FACE AND MOUTH Bailey & Love s 25 th edition Injuries to the orofacial region are common, but the majority are relatively minor in nature. A few are major
Dr.Yahya A. Ali 3/10/2012 F.I.C.M.S TRAUMA TO THE FACE AND MOUTH Bailey & Love s 25 th edition Injuries to the orofacial region are common, but the majority are relatively minor in nature. A few are major
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery FACIAL FRACTURES
 Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Maxillofacial and Ocular Injuries
 Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma The face is vital to human appearance and function. Facial injuries can impair a patient
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma The face is vital to human appearance and function. Facial injuries can impair a patient
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Ears. Mouth. Jowls 6 Major Bones of the Face Nasal bone Two
 1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
CT of Maxillofacial Injuries
 CT of Maxillofacial Injuries Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology changes the diagnosis Technologic Evolution
CT of Maxillofacial Injuries Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology changes the diagnosis Technologic Evolution
MAXILLOFACIAL TRAUMATOLOGY Department of Maxillofacial Surgery Semmelweis University, Budapest. Dr. Huszár Tamás
 MAXILLOFACIAL TRAUMATOLOGY Department of Maxillofacial Surgery Semmelweis University, Budapest Dr. Huszár Tamás Maxillofacial injuries isolated maxillofacial injury multiple injuries polytrauma (injury
MAXILLOFACIAL TRAUMATOLOGY Department of Maxillofacial Surgery Semmelweis University, Budapest Dr. Huszár Tamás Maxillofacial injuries isolated maxillofacial injury multiple injuries polytrauma (injury
CT of Maxillofacial Fracture Patterns. CT of Maxillofacial Fracture Patterns
 CT of Maxillofacial Fracture Patterns CT of Maxillofacial Fracture Patterns Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology
CT of Maxillofacial Fracture Patterns CT of Maxillofacial Fracture Patterns Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology
Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line.
 Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line. After reading the article, the staff will be able to: Define facial trauma
Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line. After reading the article, the staff will be able to: Define facial trauma
Facial Trauma. Facial Trauma. Facial Trauma
 Facial Trauma Facial Trauma Brian Bast DMD, MD Department of Oral and Maxillofacial Surgery University of California, San Francisco School of Dentistry Brian Bast DMD, MD Department of Oral and Maxillofacial
Facial Trauma Facial Trauma Brian Bast DMD, MD Department of Oral and Maxillofacial Surgery University of California, San Francisco School of Dentistry Brian Bast DMD, MD Department of Oral and Maxillofacial
Injuries to the Head and Spine
 Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Epidemiology 3002). Epidemiology and Pathophysiology
. Epidemiology and Pathophysiology") Epidemiology Maxillofacial trauma or injuries are commonly encountered in the practice of emergency medicine and are presenting one of the most challenging problems to the attending surgeons or physicians
Epidemiology Maxillofacial trauma or injuries are commonly encountered in the practice of emergency medicine and are presenting one of the most challenging problems to the attending surgeons or physicians
Maxillofacial Injuries Practical Tips
 Saturday, October 29, 2016 Maxillofacial Injuries Practical Tips Suyash Mohan MD, PDCC THE ROOTS OF PENN RADIOLOGY RADIOLOGICAL Assistant Professor of Radiology Assistant Professor of Neurosurgery Neuroradiology
Saturday, October 29, 2016 Maxillofacial Injuries Practical Tips Suyash Mohan MD, PDCC THE ROOTS OF PENN RADIOLOGY RADIOLOGICAL Assistant Professor of Radiology Assistant Professor of Neurosurgery Neuroradiology
Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI. Monitor the vital signs. Monitor the vital signs. Complications of Facial Traumas.
 Complications of Facial Traumas 1) Immediate Complications 2) Late Complications Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI Assistant Professor Oral & Maxillofacial Surgeon Taibah University Monitor
Complications of Facial Traumas 1) Immediate Complications 2) Late Complications Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI Assistant Professor Oral & Maxillofacial Surgeon Taibah University Monitor
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions
 54 Questions") Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What is caused by overexerting or tearing of a muscle? p. 375 A.) Dislocation B.) Sprain C.) Fracture *D.)
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What is caused by overexerting or tearing of a muscle? p. 375 A.) Dislocation B.) Sprain C.) Fracture *D.)
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
MEDICAL CODING FOR FACIAL INJURIES & RECONSTRUCTION
 MEDICAL CODING FOR FACIAL INJURIES & RECONSTRUCTION Tirbod Fattahi, MD, DDS, FACS Chief & Associate Professor Division of Oral & Maxillofacial Surgery University of Florida Health Science Center, Jacksonville
MEDICAL CODING FOR FACIAL INJURIES & RECONSTRUCTION Tirbod Fattahi, MD, DDS, FACS Chief & Associate Professor Division of Oral & Maxillofacial Surgery University of Florida Health Science Center, Jacksonville
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Eyes, ears, teeth and everything in between
 Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Facial Trauma. Rural Emergency Services and Trauma Symposium 2008
 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Mitchell Stotland, MD Associate Professor of Surgery and Pediatrics Dartmouth-Hitchcock Medical Center Children s Hospital of Dartmouth
Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Mitchell Stotland, MD Associate Professor of Surgery and Pediatrics Dartmouth-Hitchcock Medical Center Children s Hospital of Dartmouth
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate
 Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
ISPUB.COM. GSW To The Face: "Hunting Camp" C Perry, B Phillips CASE REPORT
 ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 2 Number 2 C Perry, B Phillips Citation C Perry, B Phillips.. The Internet Journal of Rescue and Disaster Medicine. 2000 Volume 2 Number
ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 2 Number 2 C Perry, B Phillips Citation C Perry, B Phillips.. The Internet Journal of Rescue and Disaster Medicine. 2000 Volume 2 Number
The diagnostic value of Computed Tomography in evaluation of maxillofacial Trauma
 The diagnostic value of Computed Tomography in evaluation of maxillofacial Trauma Qais H. Muassa FICMS College of Dentistry, Babylon University Ibrahim S. Gataa, BDS, FICMS College of Dentistry, Sulaimania
The diagnostic value of Computed Tomography in evaluation of maxillofacial Trauma Qais H. Muassa FICMS College of Dentistry, Babylon University Ibrahim S. Gataa, BDS, FICMS College of Dentistry, Sulaimania
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
Case Report. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System.
 Case Report Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System
Case Report Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions
 54 Questions") Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What do injuries to the shoulder often produce? p. 393 *A.) Anterior dislocation B.) Superior dislocation
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What do injuries to the shoulder often produce? p. 393 *A.) Anterior dislocation B.) Superior dislocation
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
MRI masterfile Part 5 WM Heme Strokes.ppt 1
 Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September ISSN
 International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
Ocular Urgencies and Emergencies
 Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Provision of General Anesthesia Out of Hospital: Perspective from The Americas. Anthony Charles Caputo
 Provision of General Anesthesia Out of Hospital: Perspective from The Americas Anthony Charles Caputo Welcome!! A Little About Me President, Southwest Dental Anesthesia Services Past President, American
Provision of General Anesthesia Out of Hospital: Perspective from The Americas Anthony Charles Caputo Welcome!! A Little About Me President, Southwest Dental Anesthesia Services Past President, American
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
AXIAL SKELETON SKULL
 AXIAL SKELETON SKULL CRANIAL BONES (8 total flat bones w/ 2 paired) 1. Frontal forms forehead & upper portion of eyesocket (orbital) 2. Parietal paired bones; form superior & lateral walls of cranium 3.
AXIAL SKELETON SKULL CRANIAL BONES (8 total flat bones w/ 2 paired) 1. Frontal forms forehead & upper portion of eyesocket (orbital) 2. Parietal paired bones; form superior & lateral walls of cranium 3.
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Chapter 28. Objectives. Objectives 01/09/2013. Bleeding and Soft-Tissue Trauma
 Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Chapter 30 Putting It All Together for the Trauma Patient
 Chapter 30 Putting It All Together for the Trauma Patient Putting It All Together Balance need for prompt transport vs. treatment on scene. Select critical interventions to implement at scene of multipletrauma
Chapter 30 Putting It All Together for the Trauma Patient Putting It All Together Balance need for prompt transport vs. treatment on scene. Select critical interventions to implement at scene of multipletrauma
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Nasotracheal Intubation for Head and Neck Surgery
 Nasotracheal Intubation for Head and Neck Surgery Dr A J Cartwright Introduction History Anatomy Indications for Technique of Complications Contraindications Conclusions History First described in 1902
Nasotracheal Intubation for Head and Neck Surgery Dr A J Cartwright Introduction History Anatomy Indications for Technique of Complications Contraindications Conclusions History First described in 1902
MRI masterfile Part 5 WM Heme Strokes.ppt 2
 Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
ZYGOMATIC (MALAR) FRACTURES
 FRACTURES") b854_chapter-12.qxd 1/31/2011 9:40 AM Page 129 ZYGOMATIC (MALAR) FRACTURES CHAPTER 12 Anatomical articulations FZ Fronto-zygomatic ZT Zygomaticotemporal ZMB Zygomatico - maxillary buttress IO Infraorbital
b854_chapter-12.qxd 1/31/2011 9:40 AM Page 129 ZYGOMATIC (MALAR) FRACTURES CHAPTER 12 Anatomical articulations FZ Fronto-zygomatic ZT Zygomaticotemporal ZMB Zygomatico - maxillary buttress IO Infraorbital
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
Chapter 11: Maxillofacial Trauma
 The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 11: Maxillofacial Trauma Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN
The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 11: Maxillofacial Trauma Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN
Anatomy and Physiology. Bones, Sutures, Teeth, Processes and Foramina of the Human Skull
 Anatomy and Physiology Chapter 6 DRO Bones, Sutures, Teeth, Processes and Foramina of the Human Skull Name: Period: Bones of the Human Skull Bones of the Cranium: Frontal bone: forms the forehead and the
Anatomy and Physiology Chapter 6 DRO Bones, Sutures, Teeth, Processes and Foramina of the Human Skull Name: Period: Bones of the Human Skull Bones of the Cranium: Frontal bone: forms the forehead and the
68W COMBAT MEDIC POCKET GUIDE
 GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
Assessment and Management of Ocular Trauma. Disclosure I have no direct financial interests in today s subject matter. 3/25/2019. Normal Eye Anatomy
 Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Imaging Orbit/Periorbital Injury
 Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
Bundeswehrkrankenhaus Ulm Abteilung HNO Kopf-Halschirurgie
 Kai Johannes Lorenz and Klaus Effinger Department of Otorhinolaryngology, Head and Neck Surgery Department of Radiology and interventional Radiology German Armed Forces Hospital Incidence of hemorrhage
Kai Johannes Lorenz and Klaus Effinger Department of Otorhinolaryngology, Head and Neck Surgery Department of Radiology and interventional Radiology German Armed Forces Hospital Incidence of hemorrhage
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Assessment of the Trauma Patient
 CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions
 83 Questions") Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Dysmorphology. Sue White. Diagnostic Dysmorphology, Aase. Victorian Clinical Genetics Services
 Dysmorphology Sue White www.rch.unimelb.edu.au/nets/handbook Diagnostic Dysmorphology, Aase Dysmorphology Assessment Algorithm no Are the features familial? yes Recognised syndrome yes no AD/XL syndrome
Dysmorphology Sue White www.rch.unimelb.edu.au/nets/handbook Diagnostic Dysmorphology, Aase Dysmorphology Assessment Algorithm no Are the features familial? yes Recognised syndrome yes no AD/XL syndrome
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Clues of a Ruptured Globe
 Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Postnatal Growth. The study of growth in growing children is for two reasons : -For health and nutrition assessment
 Growth of The Soft Tissues Postnatal Growth Postnatal growth is defined as the first 20 years of growth after birth krogman 1972 The study of growth in growing children is for two reasons : -For health
Growth of The Soft Tissues Postnatal Growth Postnatal growth is defined as the first 20 years of growth after birth krogman 1972 The study of growth in growing children is for two reasons : -For health
Dr. Sami Zaqout, IUG Medical School
 The skull The skull is composed of several separate bones united at immobile joints called sutures. Exceptions? Frontal bone Occipital bone Vault Cranium Sphenoid bone Zygomatic bones Base Ethmoid bone
The skull The skull is composed of several separate bones united at immobile joints called sutures. Exceptions? Frontal bone Occipital bone Vault Cranium Sphenoid bone Zygomatic bones Base Ethmoid bone
Introduction. Topics. Seattle/King County EMT-B Class. EMS Online. Class schedule Message board Lecture presentations
 Seattle/King County EMT-B Class Introduction EMS Online http://www.emsonline.net/emtb Class schedule Message board Lecture presentations Topics Airway Management: Chapter 7 Patient Assessment: Chapter
Seattle/King County EMT-B Class Introduction EMS Online http://www.emsonline.net/emtb Class schedule Message board Lecture presentations Topics Airway Management: Chapter 7 Patient Assessment: Chapter
Senior Registrar, Maxillofacial and Oral Surgery Det~artment, Wythenshawe Hospital, Manchester
 SURGICAL EMPHYSEMA OF THE FACE, NECK, AND UPPER THORACIC WALL ASSOCIATED WITH FRACTURE OF THE FACIAL SKELETON By IAN H. HESLOP, M.B., B.S., B.D.S., F.D.S., R.C.S. Senior Registrar, Maxillofacial and Oral
SURGICAL EMPHYSEMA OF THE FACE, NECK, AND UPPER THORACIC WALL ASSOCIATED WITH FRACTURE OF THE FACIAL SKELETON By IAN H. HESLOP, M.B., B.S., B.D.S., F.D.S., R.C.S. Senior Registrar, Maxillofacial and Oral
IMPACTED CANINES. Unfortunately, this important tooth is the second most common tooth to be impacted after third molars
 IMPACTED CANINES After we talked about impacted third molars, today we ll discuss about maxillary impacted canines in upper dental arch, how to manage these cases as a dental surgeon. You will study about
IMPACTED CANINES After we talked about impacted third molars, today we ll discuss about maxillary impacted canines in upper dental arch, how to manage these cases as a dental surgeon. You will study about
Evaluation and Stabilization of the Athlete with Possible Spine Injury
 Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Structure Location Function
 Frontal Bone Cranium forms the forehead and roof of the orbits Occipital Bone Cranium forms posterior and inferior portions of the cranium Temporal Bone Cranium inferior to the parietal bone forms the
Frontal Bone Cranium forms the forehead and roof of the orbits Occipital Bone Cranium forms posterior and inferior portions of the cranium Temporal Bone Cranium inferior to the parietal bone forms the
Conventional radiograph verses CT for evaluation of sagittal fracture of mandibular condyle
 Case Report: Conventional radiograph verses CT for evaluation of sagittal fracture of mandibular condyle Dr Anjali Wadhwa, Dr Gaurav Shah, Dr Shweta Sharma, Dr Anand Bhatnagar, Dr Pallavi Malaviya NIMS
Case Report: Conventional radiograph verses CT for evaluation of sagittal fracture of mandibular condyle Dr Anjali Wadhwa, Dr Gaurav Shah, Dr Shweta Sharma, Dr Anand Bhatnagar, Dr Pallavi Malaviya NIMS
ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section. REVIEW SHEET Exercise 10 Axial Skeleton
 ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section REVIEW SHEET Exercise 10 Axial Skeleton 1 POINT EACH. THE SKULL MULTIPLE CHOICE 1. The major components of the axial skeleton include the 7. The
ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section REVIEW SHEET Exercise 10 Axial Skeleton 1 POINT EACH. THE SKULL MULTIPLE CHOICE 1. The major components of the axial skeleton include the 7. The
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. Railway accidents injured pedal cyclist
 Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Hockey New South Wales Head Injury Guidelines Effective November
 Hockey New South Wales Effective November 2011 1 Table of Contents Part 1: Guidelines Statement 3 Head Injuries 3 Two Types of Head Injuries 3 Symptoms of Head Injuries 3 Head Injury Notifications 3 Important
Hockey New South Wales Effective November 2011 1 Table of Contents Part 1: Guidelines Statement 3 Head Injuries 3 Two Types of Head Injuries 3 Symptoms of Head Injuries 3 Head Injury Notifications 3 Important
Stretching of the corners of the mouth that may lead to cracking or bruising.
 INFORMED CONSENT FOR REMOVAL OF CYST OR TUMOR Practice Administrator 9450 E Ironwood Square Dr. Scottsdale, AZ 85258 Phone: (480) 551-0581 Fax: (480) 551-0585 www.anewbeautifulyou.com Patient s Name Please
INFORMED CONSENT FOR REMOVAL OF CYST OR TUMOR Practice Administrator 9450 E Ironwood Square Dr. Scottsdale, AZ 85258 Phone: (480) 551-0581 Fax: (480) 551-0585 www.anewbeautifulyou.com Patient s Name Please
MANAGEMENT OF FRACTURE. Sudi maiteh (seminar 2 )
") MANAGEMENT OF FRACTURE Sudi maiteh (seminar 2 ) Management of fracture Subjects : _ general management of fractures & Orthopedic patient evaluation _ Closed and open fractures management (Conservative,
MANAGEMENT OF FRACTURE Sudi maiteh (seminar 2 ) Management of fracture Subjects : _ general management of fractures & Orthopedic patient evaluation _ Closed and open fractures management (Conservative,
Use of Modified Retro-mandibular subparotid approach for treatment of Condylar fracture: a Technical note
 Original article: Use of Modified Retro-mandibular subparotid approach for treatment of Condylar fracture: a Technical note 1 DR.Sonal Anchlia, 2 DR.BIPIN.S.SADHWANI, 3 DR.ROHIT KUMAR, 4 Dr.Vipul 1Assistant
Original article: Use of Modified Retro-mandibular subparotid approach for treatment of Condylar fracture: a Technical note 1 DR.Sonal Anchlia, 2 DR.BIPIN.S.SADHWANI, 3 DR.ROHIT KUMAR, 4 Dr.Vipul 1Assistant
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
Risky Extubation. Andy Higgs. Warrington Hospitals Cheshire UK
 Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Head and Neck Examination
 Head and Neck Examination Statement of Goals Understand and perform an examination of the head and neck. Learning Objectives Head Ears Nose Sinus A. Describe the anatomy of the head, including regions
Head and Neck Examination Statement of Goals Understand and perform an examination of the head and neck. Learning Objectives Head Ears Nose Sinus A. Describe the anatomy of the head, including regions
If you suspect airway problems, get a second opinion before you anaesthetise, not after!
 Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Head and Face Anatomy
 Head and Face Anatomy Epicranial region The Scalp The soft tissue that covers the vault of skull. Extends from supraorbital margin to superior nuchal line. Layers of the scalp S C A L P = skin = connective
Head and Face Anatomy Epicranial region The Scalp The soft tissue that covers the vault of skull. Extends from supraorbital margin to superior nuchal line. Layers of the scalp S C A L P = skin = connective