The Subzygomatic Triangle: Rapid, minimally invasive identification of the masseteric nerve for facial ACCEPTED
|
|
|
- Ariel Norman
- 6 years ago
- Views:
Transcription
1 Plastic and Reconstructive Surgery Advance Online Article DOI: /PRS.0b013e318290f6dc The Subzygomatic Triangle: Rapid, minimally invasive identification of the masseteric nerve for facial reanimation Ryan M. Collar MD Assistant Professor Division of Facial Plastic and Reconstructive Surgery Department of Otolaryngology Head and Neck Surgery University of Cincinnati College of Medicine Cincinnati, OH Patrick J. Byrne MD Associate Professor Division of Facial Plastic and Reconstructive Surgery Department of Otolaryngology Head and Neck Surgery Johns Hopkins School of Medicine Baltimore, MD Kofi D. O. Boahene MD Associate Professor Division of Facial Plastic and Reconstructive Surgery Department of Otolaryngology Head and Neck Surgery Johns Hopkins School of Medicine Baltimore, MD Level of Evidence: IV
2 Corresponding Author Ryan M. Collar 7576 Wellness Way, Suite 309 West Chester, OH (p) (f)
3 The authors have no commercial associations or financial disclosures with regard to this manuscript. There was no internal or external funding involved in the study. The cadavers were donated for use by the Johns Hopkins School Medicine. The only device utilized during the study was a standard facial nerve monitor. Our institution utilizes the NIM Nerve Monitoring System from Medtronic USA.
4 Abstract Background: The masseteric nerve is a valuable donor nerve in the management of facial paralysis, however its location is less familiar to surgeons because this motor nerve is not commonly exposed in other head and neck procedures. Current techniques for masseteric nerve identification rely on physical measurements from surface or bony landmarks that may be unpredictable across patient age, ethnicity and size. We sought to identify a rapid and minimally invasive technique based on surgical anatomy independent of intra-operative physical measurements. Methods: A two phase fresh frozen cadaver study was performed followed by a clinical application that included 11 consecutive patients undergoing facial reanimation procedures between May 2012 and October Results: Ten cadavers were dissected and 11 clinical applications are reported. In all dissections the masseteric nerve was identified through the newly described Subzygomatic Triangle. This triangle is formed by the zygomatic arch superiorly, the temporomandibular joint posteriorly, and the frontal branch of the facial nerve inferiorly and anteriorly. This finding was consistent across patient ages (8-49 years) and ethnicities. Through using the short scar, minimal dissection approach described in the study, average time to nerve identification was 10.2 minutes during the clinical application. Conclusion: The subzygomatic triangle is a consistent anatomic landmark for rapid, reliable and minimally invasive identification of the masseteric nerve. The use of the subzygomatic triangle obviates the need for extensive dissection and surgeon reliance upon soft tissue measurements that may vary between patients of different size, gender or ethnicity.
5 Introduction The masseteric nerve is a valuable source for new neural input in the management of facial paralysis. In patients with reversible facial paralysis, the location of masseteric nerve provides the potential for a tension free anastomosis to the main trunk or peripheral branches of the facial nerve without the need for an interposition graft. In patients with irreversible facial paralysis, the masseteric nerve can adequately power transplanted free functional muscle flaps in a single stage reanimation procedure. In both cases, the masseteric nerve may be completely mobilized and transposed for an end-to-end neurorrhaphy without functional complications. 1,2,3,4,5,6 The masseteric nerve is not routinely identified in common head and neck operations. As such, surgeons generally have little clinical experience with masseteric nerve anatomy. Although the nerve s skull base anatomy and ramification pattern in the masseter muscle has been well described, few reports depict clinically applicable data for identifying the nerve during facial reanimation procedures. 7,8 A very recent report describes the masseteric nerve location through a series of average measurements from the tragus and the zygomatic arch 9. Although a valuable contribution to the literature, this masseteric nerve identification schema is reliant on physical measurements from surface or bony landmarks that may be unpredictable when considering the age, gender, ethnicity, size and general anatomic variability of a given patient. As the masseteric nerve is a valuable asset to the facial reanimation surgeon, and because identifying the masseteric nerve is an uncommon exercise, we set out to identify a reliable means of masseteric nerve identification that does not rely upon soft tissue measurements and that is applicable to all patients. Additionally we sought to create an identification technique that is both rapid and minimally invasive.
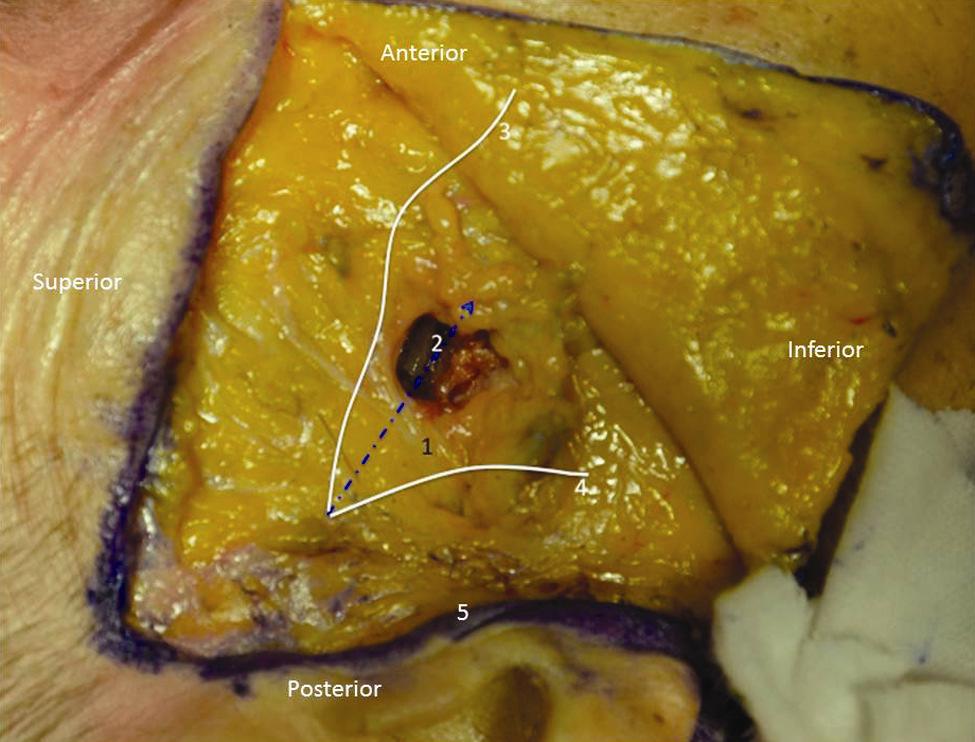
6 Methods Specimens Ten fresh frozen cadaver heads were obtained from the Johns Hopkins Department of Anatomy. The specific cause of death for the cadavers was not known to the surgical team, however there was no history of head and neck surgery or trauma in any specimen. The age of death was also not known, but all cadavers were adult specimens. The set of cadavers included Caucasian (six specimens), African American (three specimens), and Asian (one specimen) ethnicities. Surgeons The dissections were performed by the senior author (K.O.B), the first author (R.M.C), and an Otolaryngology Head and Neck Surgery senior resident at our institution. All masseteric nerve transfers were performed under the supervision of the senior author (K.O.B.). Design To reliably identify the masseter nerve for clinical application in facial reanimation, we designed a two phase cadaveric dissection study on 10 fresh frozen head specimens. Cadavers 1-5 In the first five fresh frozen cadaver heads, wide dissection with generous masseteric nerve exposure was performed. The location and course of the masseteric nerve was delineated relative to the adjacent bony anatomic landmarks the temporomandibular joint, sigmoid notch, zygomatic arch, and malar eminence. The masseteric nerve location relative to the main trunk and the frontal branch of the facial nerve was also recorded. The depth of the masseteric nerve within the masseter muscle was measured. Photographs were taken to document our findings. (Figure 1). Based on observations made from these wide dissections, we developed a strategy to rapidly and reliably identify the masseteric nerve through a minimally invasive approach using a novel anatomic triangle.
7 Cadavers 6-10 In fresh frozen cadaver heads six through 10, the masseteric nerve was identified through a limited minimally invasive dissection based on a novel anatomic triangle identified during dissection of cadavers one through five. The time to identification was noted. Clinical Application The newly developed rapid, minimal dissection approach to the masseteric nerve was applied to 11 consecutive patients undergoing facial reanimation procedures between May 2012 and October Time to nerve identification defined as the duration of dissection between SMAS flap elevation and identification of the masseter nerve confirmed by direct visualization and stimulation of the nerve was measured. Results Cadavers 1-5 In all cadavers undergoing broad dissection the nerve was identified within the substance of the masseter muscle. In each specimen, the nerve was found to reliably bisect what we have defined as the Subzygomatic Triangle. This triangle is formed by the inferior border of the zygomatic arch superiorly, a vertical line through the anterior border of the temporomandibular joint posteriorly, and the frontal branch of the facial nerve inferiorly and anteriorly (Figure 1 and 2). The masseteric nerve followed a line that begins at the angle of the subzygomatic triangle that is formed by the temporomandibular joint and zygomatic arch, and crosses the midpoint of the triangle base formed by frontal branch of the facial nerve (Figures 1-2). This relationship was consistent in all specimens.
8 Within the masseter muscle itself, the nerve was located in the deep muscle belly below a white fibrous fascia. The nerve was between 10mm and 15mm deep to the parotidomasseteric fascia. At this location, a dominant branch was identified. The dominant branch of masseter nerve coursed obliquely within the substance of the muscle for approximately 2 to 3 cm in an anterior-posterior direction before branching out. Cadavers 6-10 Based on the nerve s relationship, we designed an approach for rapid identification with minimal incision and dissection that we applied to cadavers six through ten. A modified mini-facelift type incision was created with an extension into the temporal hair tuft. The vertical incision extended in the preauricular crease with a retrotragal component and stopped just superior to the ear lobule. A subcutaneous flap was elevated from the zygomatic arch superiorly to the level of the lobule inferiorly. A short SMAS flap was elevated and the course of the frontal branch of the facial nerve was outlined. A marking pen was used to ink boundaries of subzygomatic triangle and the line of bisection along which the masseteric nerve travels as described above. The nerve was then easily identified along its inked course within the subzygomatic triangle after minimal blunt dissection within the substance of masseter muscle. Clinical Application We applied the subzygomatic triangle as a means of identifying the masseteric nerve in 11 consecutive patients undergoing facial reanimation between May 2012 and October Patient ages ranged from 8 to 49 and the series included Caucasian, Hispanic, Middle Eastern, Asian and African American patients (Table 1). The cases included masseteric nerve to buccal branch neurorrhaphies, masseteric nerve to facial nerve main trunk neurroraphies, and a masseteric nerve to obturator nerve neurorrhaphy for a single staged gracillis free functional flap.
9 The procedures were performed with a facial nerve monitor in place in those patients with partial facial paralysis. Neuromuscular blocking agents were avoided beyond the induction period for intubation. Local anesthetic agents were not employed limiting soft tissue infiltration to vasocontricting agents only, using a 1:100,000 epinephrine solution. To outline the subzygomatic triangle, the inferior border of the zygomatic arch was outlined. This was joined by a vertical line through the anterior border of the temporomandibular joint. The location of temporomandibular joint was accurately identified by palpating the sigmoid notch or manually opening and closing the mandible. The anticipated course of the frontal branch of the facial nerve over the zygomatic arch completed the subzygomatic triangle. Following skin flap elevation, a separate limited short SMAS flap was performed to expose the parotid fascia. The frontal branch of the facial nerve was easily identified using blunt dissection. The frontal branch was traced retrograde to the main facial nerve trunk when nerve anastomosis at that level was planned. Similarly, blunt dissection through the parotidomasseteric fascia was employed to identify the buccal branches when they are the target for nerve grafting. With the facial nerve branches safely retracted, blunt dissection was carried out within the subzygomatic triangle into the substance of the masseter muscle. At the base of the subzygomatic triangle, the nerve was identified along a line bisecting the angle formed by the temporomandibular joint and zygomatic arch, as described above (Figure 3). We found that careful bipolar cautery through the masseter muscle fibers to the depth of the nerve with intermittent nerve stimulation allowed safe and nearly bloodless dissection. With this approach, the masseteric nerve was identified for the 11 clinical cases at a mean of 10.2 minutes (Table 1). Once identified, the masseter nerve was traced inferiorly approximately 2 to 3 cm until it arborized. It was then divided and transposed toward its target nerve. In all cases tension free neurorrhaphy was performed without interposition grafting. In addition, the limited incision and exposure was adequate for identifying the masseter and facial nerves and for neurorrhaphy under microscopic magnification. There were no significant cases of post-operative trismus.
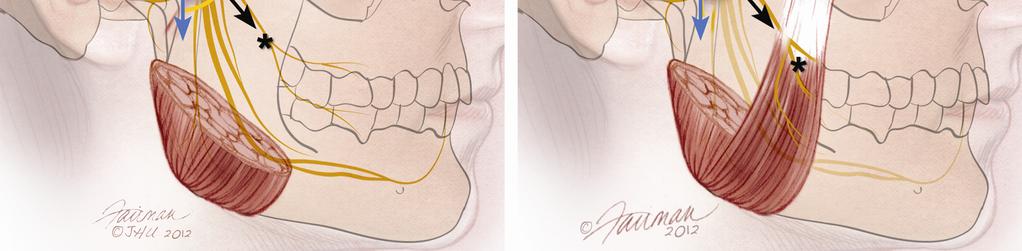
10 Discussion This study describes a novel anatomic triangle that reliably predicts masseteric nerve location without reliance on measurements from soft tissue and bony landmarks. The subzygomatic triangle predicted the location of the masseteric nerve in ten consecutive cadaveric dissections, and 11 patients of all age groups undergoing a myriad of facial reanimation procedures, with a mean time to masseteric nerve identification of 10.2 minutes. Anatomic Considerations The masseteric nerve is a motor branch of the third division of the trigeminal nerve. The mandibular nerve exits the skull base through the foramen ovale, and the masseteric nerve leaves the mandibular nerve shortly after its entrance into the infratemporal fossa. The masseteric nerve is the largest motor branch of the trigeminal nerve averaging 2mm in diameter 7. It passes superior to the lateral pterygoid muscle and exits the infratemporal fossa through the mandibular notch, also called the sigmoid notch, accompanied by the masseteric artery. There are approximately one to five branches of the nerve at the entrance into the masseter muscle with one dominant branch 10. The subzygomatic triangle overlies the entrance of the masseteric nerve from the infratemporal fossa into the masseter muscle and outlines a limited and condensed area within which the nerve can be identified without the need for extensive exposure and muscle fiber dissection. The probability of finding this small sized nerve is greatly enhanced when dissection is confined to this defined triangle as compared to an expanded field requiring more muscle fiber dissection. One can visualize the nerve traveling retrograde within the masseter muscle as if funneling to the base of the subzygomatic triangle from its broad inconsistent ramified state in the substance of the muscle toward its narrow consistent location as it exits the muscle toward the infratemporal fossa and ultimately the foramen ovale (Figure 2A-B). The optimized efficiency and reliability in locating the masseteric nerve within subzygomatic triangle is supported by our cadaver dissection series and clinical application.
11 Efficient, Consistent, and Minimally Invasive During the clinical application of the study, the average time to masseteric nerve identification was 10.2 minutes. Although the stuwas not designed to specifically compare efficiency in the clinical setting before and after introduction of the new approach, our overall case times for masseteric nerve transfer were markedly reduced with the implementation of this approach (data not reported). Notably we successfully applied this approach to both adult and pediatric patients. The relationship of the masseteric nerve to the subzygomatic triangle was consistent across age, gender and ethnicities. Finally, the approach required only a modified short scar facelift incision ending at the level of the lobule and minimal soft tissue dissection. Because the nerve is identified superiorly at the subzygomatic triangle, there is no need to extend the incision anteriorly into the neck nor extend the dissection broadly over the parotid and masseter muscle unless otherwise indicated for the procedure. Since disruption of the parotid is minimal no volume loss or sialoceles were encountered in this clinical series. Study Strength This study describes a novel anatomic triangle that reliably predicts the location of the masseteric nerve without the need for surgeon reliance upon soft tissue measurements. Previous publications addressing the location on the masseter nerve have relied heavily on surface measurements. While surface measurements are a useful guide, they do not account for the variability in facial shapes and head size that may vary with ethnicity and age particularly when considering children. Facial measurements also do not provide a palpable landmark that can serve as a constant reference point during the dissection. Our cadaver dissection series and group of patients undergoing facial reanimation procedures included a child, men and women aged 8 to 49 of multiple ethnic backgrounds. The masseteric nerve s simple anatomic relationship to the subzygomatic triangle was consistent in all cases.
12 Study weakness This cadaver study and case series represents a relatively small number of dissections. A larger sample size would provide additional support for the relationship we identified in twenty-one consecutive dissections. A potential confounder to the nerve identification efficiency we report is the practice effect, or learning effect. Due to repeating the task alone in the lab, one s ability to complete the task with greater efficiency may be enhanced. To the contrary, in the clinical application component of our study, a board eligible Otolaryngology Head and Neck Surgeon without past involvement in our cadaver dissections, nor previous clinical experience with masseteric nerve identification, was able to independently identify the nerve using the subzygomatic triangle principles with comparable efficiency. Conclusion The subzygomatic triangle, defined as the triangle formed by the temporomandibular joint, zygomatic arch, and frontal branch of the facial nerve, is a reliable anatomic landmark for rapid, reliable and minimally invasive identification of the masseteric nerve. The use of the subzygomatic triangle obviates the need for extensive dissection and surgeon reliance upon soft tissue measurements that may vary between patients of different size, gender or ethnicity.
13 1 Spira M. Anastomosis of masseteric nerve to lower division of facial nerve for correction of lower facial paralysis. Preliminary report. Plast Reconstr Surg. 1978;61(3): Bermudez LE, Nieto LE. Masseteric-facial nerve anastomosis: case report. J Reconstr Microsurg. 2004; Jan(1): Faria JC, Scopel GP, Ferreira MC. Facial reanimation with masseteric nerve: babysitter or permanent procedure? Preliminary results. Ann Plast Surg. 2010;Jan(1): Sforza C, Frigerio A, Mapelli A, Mandelli F, Sidequersky FV, Colombo V, Ferrario VF, Biglioli F. Facial movement before and after masseteric-facial nerves anastomosis: A three-dimensional optoelectronic pilot study. J Craniomaxillofac Surg. 2012; Jul(5): Biglioli F, Frigerio A, Colombo V, Colletti G, Rabbiosi D, Mortini P, Dalla Toffola E, Lozza A, Brusati R. Masseteric-facial nerve anastomosis for early facial reanimation. J Craniomaxillofac Surg. 2012;Feb(2): Coombs CJ, Ek EW, Wu T, Cleland H, Leung MK. Masseteric-facial nerve coaptation--an alternative technique for facial nerve reinnervation. J Plast Reconstr Aesthet Surg. 2009;Dec(12): Fournier HD, Denis F, Papon X, Hentati N, Mercier P. An anatomical study of the motor distribution of the mandibular nerve for a masseteric-facial anastomosis to restore facial function. Surg Radiol Anat. 1997;19(4): Brenner E, Schoeller T. Masseteric nerve: a possible donor for facial nerve anastomosis? Clin Anat. 1998;11(6): Borschel GH, Kawamura DH, Kasukurthi R, Hunter DA, Zuker RM, Woo AS. The motor nerve to the masseter muscle: an anatomic and histomorphometric study to facilitate its use in facial reanimation. J Plast Reconstr Aesthet Surg. 2012;65(3): Brenner E, Schoeller T. Masseteric nerve: a possible donor for facial nerve anastomosis? Clin Anat. 1998;11(6):
14 Figure Legend Figure 1: Representative from cadaver one though five, with wide dissection allowing masseteric nerve exposure. 1: Frontal branch of facial nerve; 2: Course of masseteric nerve bisecting the base of the subzygomatic triangle; 3: Zygomatic arch; 4: Temporomandibular joint; 5: pre-auricular incision. Figure 2A-B: Illustrations of the subzygomatic triangle demonstrating the masseteric nerve at its location within the subzygomatic triangle. Note the nerve is identified near the apex of the triangle. Yellow A = frontal branch of facial n; Blue B = temporomandibular joint; red C = Zygomatic Arch; black asterisk = masseteric nerve Figure 3A-C: A) Preoperative markings showing the palpated zygomatic arch, temporomandibular joint, and anticipated course of the frontal branch of the facial nerve marked with ink; the subzygomatic triangle is indicated by dashed lines. B) Intraoperative photograph showing the subzygomatic triange delinieated by the temporomandibular joint (1), the zygomatic arch (2), and the frontal branch of the facial nerve (3). The yellow nerve loop extends deep the masseteric nerve deep in the dissection (4). Note that it bisects the base of the subzygomatic triangle. C) Post operative appearance showing minimally invasive incisions.
15 Table Legend Table 1: Patient data from Clinical Application phase of the study, including age, gender, ethnicity, and time to masseteric nerve identification.
16 Age Gender Ethnicity Time to Nerve Identification 49 M African American F Caucasian F Caucasian F Caucasian 7 19 F Caucasian 8 8 M Hispanic M African American F Asian F Hispanic M Caucasian F Middle Eastern 9 Copyright American Society of Plastic Surgeons. All rights reserved.
17

18 TE D EP C C A


19 TE D EP C C A
be very thin and variable. Facial nerve branches that exit the parotid gland are deep to the SMAS.
 The Superficial musculoaponeurotic system (SMAS) fascia is a fanlike fascia that envelops the face and provides a suspensory sheet which distributes forces of facial expression.. The SMAS is continuous
The Superficial musculoaponeurotic system (SMAS) fascia is a fanlike fascia that envelops the face and provides a suspensory sheet which distributes forces of facial expression.. The SMAS is continuous
STEP 1 INCISION AND ELEVATION OF SKIN FLAP STEP 3 SEPARATE PAROTID GLAND FROM SCM STEP 2 IDENTIFICATON OF GREAT AURICULAR NERVE
 STEP 1 INCISION AND ELEVATION OF SKIN FLAP Create a modified Blair Figure 1 or facelift incision. Figure 2 Raise a superficial cervico-fascial flap between the Superficial Musculo Aponeurotic System (SMAS)
STEP 1 INCISION AND ELEVATION OF SKIN FLAP Create a modified Blair Figure 1 or facelift incision. Figure 2 Raise a superficial cervico-fascial flap between the Superficial Musculo Aponeurotic System (SMAS)
Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :
![Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :](/thumbs/88/115294566.jpg "Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :") Lec [5] / Temporal fossa : Borders of the Temporal Fossa: Superior: Superior temporal line. Inferior: gap between zygomatic arch and infratemporal crest of sphenoid bone. Anterior: Frontal process of the
Lec [5] / Temporal fossa : Borders of the Temporal Fossa: Superior: Superior temporal line. Inferior: gap between zygomatic arch and infratemporal crest of sphenoid bone. Anterior: Frontal process of the
3. The Jaw and Related Structures
 Overview and objectives of this dissection 3. The Jaw and Related Structures The goal of this dissection is to observe the muscles of jaw raising. You will also have the opportunity to observe several
Overview and objectives of this dissection 3. The Jaw and Related Structures The goal of this dissection is to observe the muscles of jaw raising. You will also have the opportunity to observe several
Parotid Gland, Temporomandibular Joint and Infratemporal Fossa
 M1 - Anatomy Parotid Gland, Temporomandibular Joint and Infratemporal Fossa Jeff Dupree Sanger 9-057 jldupree@vcu.edu Parotid gland: wraps around the mandible positioned between the mandible and the sphenoid
M1 - Anatomy Parotid Gland, Temporomandibular Joint and Infratemporal Fossa Jeff Dupree Sanger 9-057 jldupree@vcu.edu Parotid gland: wraps around the mandible positioned between the mandible and the sphenoid
Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus
 Outline of content Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus Boundary Content Communication Mandibular division of trigeminal
Outline of content Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus Boundary Content Communication Mandibular division of trigeminal
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
Temporal region. temporal & infratemporal fossae. Zhou Hong Ying Dept. of Anatomy
 Temporal region temporal & infratemporal fossae Zhou Hong Ying Dept. of Anatomy Temporal region is divided by zygomatic arch into temporal & infratemporal fossae. Temporal Fossa Infratemporal fossa Temporal
Temporal region temporal & infratemporal fossae Zhou Hong Ying Dept. of Anatomy Temporal region is divided by zygomatic arch into temporal & infratemporal fossae. Temporal Fossa Infratemporal fossa Temporal
The Skull and Temporomandibular joint II Prof. Abdulameer Al-Nuaimi. E. mail:
 The Skull and Temporomandibular joint II Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Temporal fossa The temporal fossa is a depression on the temporal
The Skull and Temporomandibular joint II Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Temporal fossa The temporal fossa is a depression on the temporal
Anatomical Landmarks to Avoid Injury to the Great Auricular Nerve During Rhytidectomy
 Facial Surgery Anatomical Landmarks to Avoid Injury to the Great Auricular Nerve During Rhytidectomy Todd Lefkowitz, MD; Ron Hazani, MD; Saeed Chowdhry, MD; Josh Elston, BS; Michael J. Yaremchuk, MD; and
Facial Surgery Anatomical Landmarks to Avoid Injury to the Great Auricular Nerve During Rhytidectomy Todd Lefkowitz, MD; Ron Hazani, MD; Saeed Chowdhry, MD; Josh Elston, BS; Michael J. Yaremchuk, MD; and
Infratemporal fossa: Tikrit University college of Dentistry Dr.Ban I.S. head & neck Anatomy 2 nd y.
 Infratemporal fossa: This is a space lying beneath the base of the skull between the lateral wall of the pharynx and the ramus of the mandible. It is also referred to as the parapharyngeal or lateral pharyngeal
Infratemporal fossa: This is a space lying beneath the base of the skull between the lateral wall of the pharynx and the ramus of the mandible. It is also referred to as the parapharyngeal or lateral pharyngeal
Dr.Ban I.S. head & neck anatomy 2 nd y. جامعة تكريت كلية طب االسنان املرحلة الثانية أ.م.د. بان امساعيل صديق 6102/6102
 جامعة تكريت كلية طب االسنان التشريح مادة املرحلة الثانية أ.م.د. بان امساعيل صديق 6102/6102 Parotid region The part of the face in front of the ear and below the zygomatic arch is the parotid region. The
جامعة تكريت كلية طب االسنان التشريح مادة املرحلة الثانية أ.م.د. بان امساعيل صديق 6102/6102 Parotid region The part of the face in front of the ear and below the zygomatic arch is the parotid region. The
Lec [8]: Mandibular nerve:
![Lec [8]: Mandibular nerve:](/thumbs/94/121295776.jpg "Lec [8]: Mandibular nerve:") Lec [8]: Mandibular nerve: The mandibular branch from the trigeminal ganglion lies in the middle cranial fossa lateral to the cavernous sinus. With the motor root of the trigeminal nerve [motor roots lies
Lec [8]: Mandibular nerve: The mandibular branch from the trigeminal ganglion lies in the middle cranial fossa lateral to the cavernous sinus. With the motor root of the trigeminal nerve [motor roots lies
PTERYGOPALATINE FOSSA
 PTERYGOPALATINE FOSSA Outline Anatomical Structure and Boundaries Foramina and Communications with other spaces and cavities Contents Pterygopalatine Ganglion Especial emphasis on certain arteries and
PTERYGOPALATINE FOSSA Outline Anatomical Structure and Boundaries Foramina and Communications with other spaces and cavities Contents Pterygopalatine Ganglion Especial emphasis on certain arteries and
Use of Modified Retro-mandibular subparotid approach for treatment of Condylar fracture: a Technical note
 Original article: Use of Modified Retro-mandibular subparotid approach for treatment of Condylar fracture: a Technical note 1 DR.Sonal Anchlia, 2 DR.BIPIN.S.SADHWANI, 3 DR.ROHIT KUMAR, 4 Dr.Vipul 1Assistant
Original article: Use of Modified Retro-mandibular subparotid approach for treatment of Condylar fracture: a Technical note 1 DR.Sonal Anchlia, 2 DR.BIPIN.S.SADHWANI, 3 DR.ROHIT KUMAR, 4 Dr.Vipul 1Assistant
For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER
 GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
THIEME. Scalp and Superficial Temporal Region
 CHAPTER 2 Scalp and Superficial Temporal Region Scalp Learning Objectives At the end of the dissection of the scalp, you should be able to identify, understand and correlate the clinical aspects: Layers
CHAPTER 2 Scalp and Superficial Temporal Region Scalp Learning Objectives At the end of the dissection of the scalp, you should be able to identify, understand and correlate the clinical aspects: Layers
Trigeminal Nerve Worksheets, Distributions Page 1
 Trigeminal Nerve Worksheet #1 Distribution by Nerve Dr. Darren Hoffmann Dental Gross Anatomy, Spring 2013 We have drawn out each of the branches of CN V in lecture and you have an idea now for their basic
Trigeminal Nerve Worksheet #1 Distribution by Nerve Dr. Darren Hoffmann Dental Gross Anatomy, Spring 2013 We have drawn out each of the branches of CN V in lecture and you have an idea now for their basic
Anatomical Landmarks for Safe Elevation of the Deep Inferior Epigastric Perforator Flap: A Cadaveric Study
 Anatomical Landmarks for Safe Elevation of the Deep Inferior Epigastric Perforator Flap: A Cadaveric Study Saeed Chowdhry, MD, Ron Hazani, MD, Philip Collis, BS, and Bradon J. Wilhelmi, MD University of
Anatomical Landmarks for Safe Elevation of the Deep Inferior Epigastric Perforator Flap: A Cadaveric Study Saeed Chowdhry, MD, Ron Hazani, MD, Philip Collis, BS, and Bradon J. Wilhelmi, MD University of
Temporomandibular Joint. Dr Noman ullah wazir
 Temporomandibular Joint Dr Noman ullah wazir Type of Joint TMJ is a Synovial joint between : The condylar head of the mandible. The mandibular fossa of squamous part of temporal bone. The joint cavity
Temporomandibular Joint Dr Noman ullah wazir Type of Joint TMJ is a Synovial joint between : The condylar head of the mandible. The mandibular fossa of squamous part of temporal bone. The joint cavity
Tikrit University College of Dentistry Dr.Ban I.S. head & neck anatomy 2 nd y.
 Lec [3]/The scalp The scalp extends from the supraorbital margins anteriorly to the nuchal lines at the back of the skull and down to the temporal lines at the sides. The forehead, from eyebrows to hairline,
Lec [3]/The scalp The scalp extends from the supraorbital margins anteriorly to the nuchal lines at the back of the skull and down to the temporal lines at the sides. The forehead, from eyebrows to hairline,
Anatomic Relations Summary. Done by: Sohayyla Yasin Dababseh
 Anatomic Relations Summary Done by: Sohayyla Yasin Dababseh Anatomic Relations Lecture 1 Part-1 - The medial wall of the nose is the septum. - The vestibule lies directly inside the nostrils (Nares). -
Anatomic Relations Summary Done by: Sohayyla Yasin Dababseh Anatomic Relations Lecture 1 Part-1 - The medial wall of the nose is the septum. - The vestibule lies directly inside the nostrils (Nares). -
Surgical Correction of Crow s Feet Deformity With Radiofrequency Current
 INTERNATIONAL CONTRIBUTION Oculoplastic Surgery Surgical Correction of Crow s Feet Deformity With Radiofrequency Current Min-Hee Ryu, MD; David Kahng, MD; and Yongho Shin, MD, PhD Aesthetic Surgery Journal
INTERNATIONAL CONTRIBUTION Oculoplastic Surgery Surgical Correction of Crow s Feet Deformity With Radiofrequency Current Min-Hee Ryu, MD; David Kahng, MD; and Yongho Shin, MD, PhD Aesthetic Surgery Journal
cally, a distinct superior crease of the forehead marks this spot. The hairline and
 4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
Bones Ethmoid bone Inferior nasal concha Lacrimal bone Maxilla Nasal bone Palatine bone Vomer Zygomatic bone Mandible
 splanchnocranium - Consists of part of skull that is derived from branchial arches - The facial bones are the bones of the anterior and lower human skull Bones Ethmoid bone Inferior nasal concha Lacrimal
splanchnocranium - Consists of part of skull that is derived from branchial arches - The facial bones are the bones of the anterior and lower human skull Bones Ethmoid bone Inferior nasal concha Lacrimal
Parotid Gland. Parotid Gland. Largest of 3 paired salivary glands (submandibular; sublingual) Ramus of Mandible. Medial pterygoid.
 Ramus of Mandible. Medial pterygoid.") Parotid region Parotid Gland Largest of 3 paired salivary glands (submandibular; sublingual) Ramus of Mandible Medial pterygoid Cross section of mandible Masseter D S SCM Parotid Gland Mastoid Process
Parotid region Parotid Gland Largest of 3 paired salivary glands (submandibular; sublingual) Ramus of Mandible Medial pterygoid Cross section of mandible Masseter D S SCM Parotid Gland Mastoid Process
Mohammad Hisham Al-Mohtaseb. Lina Mansour. Reyad Jabiri. 0 P a g e
 2 Mohammad Hisham Al-Mohtaseb Lina Mansour Reyad Jabiri 0 P a g e This is only correction for the last year sheet according to our record. If you already studied this sheet just read the yellow notes which
2 Mohammad Hisham Al-Mohtaseb Lina Mansour Reyad Jabiri 0 P a g e This is only correction for the last year sheet according to our record. If you already studied this sheet just read the yellow notes which
Techniques of local anesthesia in the mandible
 Techniques of local anesthesia in the mandible The technique of choice for anesthesia of the mandible is the block injection and this is attributed to the absence of the advantages which are present in
Techniques of local anesthesia in the mandible The technique of choice for anesthesia of the mandible is the block injection and this is attributed to the absence of the advantages which are present in
jamafacialplasticsurgery.com JAMA Facial Plastic Surgery September/October 2014 Volume 16, Number 5 359
 Research Case Report/Case Series Salvage Procedures fter Failed Facial Reanimation Surgery Using the Masseteric Nerve as the Motor Nerve for Free Functional Gracilis Muscle Transfer Steffen U. Eisenhardt,
Research Case Report/Case Series Salvage Procedures fter Failed Facial Reanimation Surgery Using the Masseteric Nerve as the Motor Nerve for Free Functional Gracilis Muscle Transfer Steffen U. Eisenhardt,
ANTERIOR CERVICAL TRIANGLE (Fig. 2.1 )
") 2 Neck Anatomy ANTERIOR CERVICAL TRIANGLE (Fig. 2.1 ) The boundaries are: Lateral: sternocleidomastoid muscle Superior: inferior border of the mandible Medial: anterior midline of the neck This large triangle
2 Neck Anatomy ANTERIOR CERVICAL TRIANGLE (Fig. 2.1 ) The boundaries are: Lateral: sternocleidomastoid muscle Superior: inferior border of the mandible Medial: anterior midline of the neck This large triangle
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
THE ANGULAR TRACT: AN ANATOMICAL
 British Journal of Oral Surgery (1981) 19, 116-120 0 The British Association of Oral Surgeons 0007-117X/81/00170116$02.00 THE ANGULAR TRACT: AN ANATOMICAL OF SURGICAL SIGNIFICANCE STRUCTURE HAITHEM A.
British Journal of Oral Surgery (1981) 19, 116-120 0 The British Association of Oral Surgeons 0007-117X/81/00170116$02.00 THE ANGULAR TRACT: AN ANATOMICAL OF SURGICAL SIGNIFICANCE STRUCTURE HAITHEM A.
An Algorithm to Guide Recipient Vessel Selection in Cases of Free Functional Muscle Transfer for Facial Reanimation
 An Algorithm to Guide Recipient Vessel Selection in Cases of Free Functional Muscle Transfer for Facial Reanimation Original Article Francis P Henry, Jonathan I Leckenby, Daniel P Butler, Adriaan O Grobbelaar
An Algorithm to Guide Recipient Vessel Selection in Cases of Free Functional Muscle Transfer for Facial Reanimation Original Article Francis P Henry, Jonathan I Leckenby, Daniel P Butler, Adriaan O Grobbelaar
Cranial Nerve VII - Facial Nerve. The facial nerve has 3 main components with distinct functions
 Cranial Nerve VII - Facial Nerve The facial nerve has 3 main components with distinct functions Somatic motor efferent Supplies the muscles of facial expression; posterior belly of digastric muscle; stylohyoid,
Cranial Nerve VII - Facial Nerve The facial nerve has 3 main components with distinct functions Somatic motor efferent Supplies the muscles of facial expression; posterior belly of digastric muscle; stylohyoid,
Peripheral Extracranial Neurostimulation for the treatment of Primary Headache and Migraine:
 Chapter 19 Peripheral Extracranial Neurostimulation for the treatment of Primary Headache and Migraine: Introduction 1) The occipital nerve is involved in pain syndromes originating from nerve trauma,
Chapter 19 Peripheral Extracranial Neurostimulation for the treatment of Primary Headache and Migraine: Introduction 1) The occipital nerve is involved in pain syndromes originating from nerve trauma,
3-Deep fascia: is absent (except over the parotid gland & buccopharngeal fascia covering the buccinator muscle)
") The Face 1-Skin of the Face The skin of the face is: Elastic Vascular (bleed profusely however heal rapidly) Rich in sweat and sebaceous glands (can cause acne in adults) It is connected to the underlying
The Face 1-Skin of the Face The skin of the face is: Elastic Vascular (bleed profusely however heal rapidly) Rich in sweat and sebaceous glands (can cause acne in adults) It is connected to the underlying
Anatomical Study of Pectoral Nerves and its Implications in Surgery
 DOI: 10.7860/JCDR/2014/8631.4545 Anatomy Section Original Article Anatomical Study of Pectoral Nerves and its Implications in Surgery Prakash KG 1, Saniya K 2 ABSTRACT Introduction: This anatomical study
DOI: 10.7860/JCDR/2014/8631.4545 Anatomy Section Original Article Anatomical Study of Pectoral Nerves and its Implications in Surgery Prakash KG 1, Saniya K 2 ABSTRACT Introduction: This anatomical study
Skull-2. Norma Basalis Interna Norma Basalis Externa. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Skull-2 Norma Basalis Interna Norma Basalis Externa Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the
Skull-2 Norma Basalis Interna Norma Basalis Externa Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the
Maxilla, ORBIT and infratemporal fossa. Neophytos C Demetriades MD, DDS, MSc Associate professor European University of Cyprus School of Medicine
 Maxilla, ORBIT and infratemporal fossa Neophytos C Demetriades MD, DDS, MSc Associate professor European University of Cyprus School of Medicine MAXILLA Superior, middle, and inferior meatus Frontal sinus
Maxilla, ORBIT and infratemporal fossa Neophytos C Demetriades MD, DDS, MSc Associate professor European University of Cyprus School of Medicine MAXILLA Superior, middle, and inferior meatus Frontal sinus
Pichayen Duangthongpon MD*, Chaiwit Thanapaisal MD*, Amnat Kitkhuandee MD*, Kowit Chaiciwamongkol MD**, Vilaiwan Morthong MD**
 The Relationships between Asterion, the Transverse-Sigmoid Junction, the Superior Nuchal Line and the Transverse Sinus in Thai Cadavers: Surgical Relevance Pichayen Duangthongpon MD*, Chaiwit Thanapaisal
The Relationships between Asterion, the Transverse-Sigmoid Junction, the Superior Nuchal Line and the Transverse Sinus in Thai Cadavers: Surgical Relevance Pichayen Duangthongpon MD*, Chaiwit Thanapaisal
The Neck the lower margin of the mandible above the suprasternal notch and the upper border of the clavicle
 The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The SCALP. Prof. Dr. Muhammad Imran Qureshi
 The SCALP By Prof. Dr. Muhammad Imran Qureshi The SCALP includes FIVE layers external to the Calvaria. These are: S: Skin & Superficial Fascia C: Connective Tissue A: Aponeurosis (Epicranial) L: Loose
The SCALP By Prof. Dr. Muhammad Imran Qureshi The SCALP includes FIVE layers external to the Calvaria. These are: S: Skin & Superficial Fascia C: Connective Tissue A: Aponeurosis (Epicranial) L: Loose
The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR.
 The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR Made of A-AURICLE B-EXTERNAL AUDITORY MEATUS A-AURICLE It consists
The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR Made of A-AURICLE B-EXTERNAL AUDITORY MEATUS A-AURICLE It consists
SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions. 4 May 2012
 SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions 4 May 2012 1. With regard to the muscles of the neck: a. the platysma muscle is supplied by the accessory nerve. b. the stylohyoid muscle is supplied by
SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions 4 May 2012 1. With regard to the muscles of the neck: a. the platysma muscle is supplied by the accessory nerve. b. the stylohyoid muscle is supplied by
Head and Face Anatomy
 Head and Face Anatomy Epicranial region The Scalp The soft tissue that covers the vault of skull. Extends from supraorbital margin to superior nuchal line. Layers of the scalp S C A L P = skin = connective
Head and Face Anatomy Epicranial region The Scalp The soft tissue that covers the vault of skull. Extends from supraorbital margin to superior nuchal line. Layers of the scalp S C A L P = skin = connective
Muscles of mastication [part 1]
![Muscles of mastication [part 1]](/thumbs/76/73586850.jpg "Muscles of mastication [part 1]") Muscles of mastication [part 1] In this lecture well have the muscles of mastication, neuromuscular function, and its relationship to the occlusion morphology. The fourth determinant of occlusion is the
Muscles of mastication [part 1] In this lecture well have the muscles of mastication, neuromuscular function, and its relationship to the occlusion morphology. The fourth determinant of occlusion is the
EndoBlade Soft Tissue Release System
 Surgical Technique Endoscopic Gastroc Recession Endoscopic Plantar Fascia Release EndoBlade Soft Tissue Release System Endoscopic Gastroc Recession Arthrex has developed a comprehensive, completely disposable
Surgical Technique Endoscopic Gastroc Recession Endoscopic Plantar Fascia Release EndoBlade Soft Tissue Release System Endoscopic Gastroc Recession Arthrex has developed a comprehensive, completely disposable
Facial palsy is a well-known pathological condition. Masseteric facial nerve neurorrhaphy: results of a case series
 clinical article J Neurosurg 126:312 318, 2017 Masseteric facial nerve neurorrhaphy: results of a case series Federico Biglioli, MD, 1 Valeria Colombo, MD, 1 Dimitri Rabbiosi, MD, 1 Filippo Tarabbia, MD,
clinical article J Neurosurg 126:312 318, 2017 Masseteric facial nerve neurorrhaphy: results of a case series Federico Biglioli, MD, 1 Valeria Colombo, MD, 1 Dimitri Rabbiosi, MD, 1 Filippo Tarabbia, MD,
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Surgical Anatomy Relevant to the Transpalpebral Subperiosteal Elevation of the Midface
 Surgical Anatomy Relevant to the Transpalpebral Subperiosteal Elevation of the Midface Gaby Doumit, MD, Msc, Bahar Bassiri Gharb, MD, PhD, Antonio Rampazzo, MD, PhD, Jennifer McBride, PhD, Francis Papay,
Surgical Anatomy Relevant to the Transpalpebral Subperiosteal Elevation of the Midface Gaby Doumit, MD, Msc, Bahar Bassiri Gharb, MD, PhD, Antonio Rampazzo, MD, PhD, Jennifer McBride, PhD, Francis Papay,
Face. Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face
 Face Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face The muscle of facial expression (include the muscle of the face and the scalp). All are derived
Face Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face The muscle of facial expression (include the muscle of the face and the scalp). All are derived
Tips and Tricks in Ventral Skull Base Dissection Narayanan Janakiram, Dharambir S. Sethi, Onkar K. Deshmukh, and Arvindh K.
 05 Tips and Tricks in Ventral Skull Base Dissection Narayanan Janakiram, Dharambir S. Sethi, Onkar K. Deshmukh, and Arvindh K. Gananathan Introduction...75 General Principles...76 Tips and Tricks in Ventral
05 Tips and Tricks in Ventral Skull Base Dissection Narayanan Janakiram, Dharambir S. Sethi, Onkar K. Deshmukh, and Arvindh K. Gananathan Introduction...75 General Principles...76 Tips and Tricks in Ventral
Upper arch. 1Prosthodontics. Dr.Bassam Ali Al-Turaihi. Basic anatomy & & landmark of denture & mouth
 1Prosthodontics Lecture 2 Dr.Bassam Ali Al-Turaihi Basic anatomy & & landmark of denture & mouth Upper arch Palatine process of maxilla: it form the anterior three quarter of the hard palate. Horizontal
1Prosthodontics Lecture 2 Dr.Bassam Ali Al-Turaihi Basic anatomy & & landmark of denture & mouth Upper arch Palatine process of maxilla: it form the anterior three quarter of the hard palate. Horizontal
Dr. Sami Zaqout Faculty of Medicine IUG
 Auricle External Ear External auditory meatus The Ear Middle Ear (Tympanic Cavity) Auditory ossicles Internal Ear (Labyrinth) Bony labyrinth Membranous labyrinth External Ear Auricle External auditory
Auricle External Ear External auditory meatus The Ear Middle Ear (Tympanic Cavity) Auditory ossicles Internal Ear (Labyrinth) Bony labyrinth Membranous labyrinth External Ear Auricle External auditory
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Intrapetrous Internal Carotid Artery
 James C. Andrews, M.D., Neil A. Martin, M.D., Keith Black, M.D., Vincent F Honrubia, M.D., and Donald P Becker, M.D. Midd le Cranial Fossa Transtemporal Approach to the Intrapetrous Internal Carotid Artery
James C. Andrews, M.D., Neil A. Martin, M.D., Keith Black, M.D., Vincent F Honrubia, M.D., and Donald P Becker, M.D. Midd le Cranial Fossa Transtemporal Approach to the Intrapetrous Internal Carotid Artery
Neck-2. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Medical Journal of the Volume 20 Islamic Republic of Iran Number 3 Fall 1385 November Original Articles
 Medical Journal of the Volume 0 Islamic Republic of Iran Number 3 Fall 38 November 00 Original Articles ANATOMY OF THE SUPERFICIAL INFERIOR EPIGASTRIC ARTERY FLAP MAHDI FATHI, M.D., EBRAHIM HATAMIPOUR,
Medical Journal of the Volume 0 Islamic Republic of Iran Number 3 Fall 38 November 00 Original Articles ANATOMY OF THE SUPERFICIAL INFERIOR EPIGASTRIC ARTERY FLAP MAHDI FATHI, M.D., EBRAHIM HATAMIPOUR,
The External Anatomy of the Lungs. Prof Oluwadiya KS
 The External Anatomy of the Lungs Prof Oluwadiya KS www.oluwadiya.com Introduction The lungs are the vital organs of respiration Their main function is to oxygenate the blood by bringing inspired air into
The External Anatomy of the Lungs Prof Oluwadiya KS www.oluwadiya.com Introduction The lungs are the vital organs of respiration Their main function is to oxygenate the blood by bringing inspired air into
Lya Crichlow, MD Lutheran Medical Center November 21, 2008
 Lya Crichlow, MD Lutheran Medical Center November 21, 2008 Case Presentation 64 year old male presented with a painless mass posterior to the right angle of the mandible for 3 months PMHx HTN COPD BPH
Lya Crichlow, MD Lutheran Medical Center November 21, 2008 Case Presentation 64 year old male presented with a painless mass posterior to the right angle of the mandible for 3 months PMHx HTN COPD BPH
Tympanic Bulla Temporal Bone. Digastric Muscle. Masseter Muscle
 Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Trigeminal Nerve Anatomy. Dr. Mohamed Rahil Ali
 Trigeminal Nerve Anatomy Dr. Mohamed Rahil Ali Trigeminal nerve Largest cranial nerve Mixed nerve Small motor root and large sensory root Motor root Nucleus of motor root present in the pons and medulla
Trigeminal Nerve Anatomy Dr. Mohamed Rahil Ali Trigeminal nerve Largest cranial nerve Mixed nerve Small motor root and large sensory root Motor root Nucleus of motor root present in the pons and medulla
Small access postaural parotidectomy: an analysis of techniques, feasibility and safety
 Eur Arch Otorhinolaryngol (2016) 273:1879 1883 DOI 10.1007/s00405-015-3691-9 HEAD AND NECK Small access postaural parotidectomy: an analysis of techniques, feasibility and safety Anthony Po-Wing Yuen 1
Eur Arch Otorhinolaryngol (2016) 273:1879 1883 DOI 10.1007/s00405-015-3691-9 HEAD AND NECK Small access postaural parotidectomy: an analysis of techniques, feasibility and safety Anthony Po-Wing Yuen 1
Prevertebral Region, Pharynx and Soft Palate
 Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
Conventional radiograph verses CT for evaluation of sagittal fracture of mandibular condyle
 Case Report: Conventional radiograph verses CT for evaluation of sagittal fracture of mandibular condyle Dr Anjali Wadhwa, Dr Gaurav Shah, Dr Shweta Sharma, Dr Anand Bhatnagar, Dr Pallavi Malaviya NIMS
Case Report: Conventional radiograph verses CT for evaluation of sagittal fracture of mandibular condyle Dr Anjali Wadhwa, Dr Gaurav Shah, Dr Shweta Sharma, Dr Anand Bhatnagar, Dr Pallavi Malaviya NIMS
Trigeminal Nerve (V)
") Trigeminal Nerve (V) Lecture Objectives Discuss briefly how the face is developed. Follow up the course of trigeminal nerve from its point of central connections, exit and down to its target areas. Describe
Trigeminal Nerve (V) Lecture Objectives Discuss briefly how the face is developed. Follow up the course of trigeminal nerve from its point of central connections, exit and down to its target areas. Describe
THE SURGICAL ANATOMY OF THE CERVICAL DISTRIBUTION OF THE FACIAL NERVE. Biology and Anatomy, University of Shefield
 British Journal of Oral Surgery (1981), 19, 171-179 @ The British Association of Oral Surgeons 0007-117X/81/00260171$02.00 THE SURGICAL ANATOMY OF THE CERVICAL DISTRIBUTION OF THE FACIAL NERVE HAITHEM
British Journal of Oral Surgery (1981), 19, 171-179 @ The British Association of Oral Surgeons 0007-117X/81/00260171$02.00 THE SURGICAL ANATOMY OF THE CERVICAL DISTRIBUTION OF THE FACIAL NERVE HAITHEM
T HE visual field changes that accompany
 J. Neurosurg. / Volume 31 / September, 1969 The Arterial Supply of the Human Optic Chiasm RICHARD BERGLAND, M.D.,* AND BRONSON S. RAY, M.D. Department of Surgery (Neurosurgery), New York Hospital-Cornell
J. Neurosurg. / Volume 31 / September, 1969 The Arterial Supply of the Human Optic Chiasm RICHARD BERGLAND, M.D.,* AND BRONSON S. RAY, M.D. Department of Surgery (Neurosurgery), New York Hospital-Cornell
Oral cavity landmarks
 By: Dr. Ahmed Rabah Oral cavity landmarks The knowledge of oral anatomy and physiology will help the operator and provides enough landmarks to act as positive guide during denture construction. This subject
By: Dr. Ahmed Rabah Oral cavity landmarks The knowledge of oral anatomy and physiology will help the operator and provides enough landmarks to act as positive guide during denture construction. This subject
Surgical Anatomy of the Lower Face: The Premasseter Space, the Jowl, and the Labiomandibular Fold
 Aesth Plast Surg (2008) 32:185 195 DOI 10.1007/s00266-007-9060-3 ORIGINAL ARTICLE Surgical Anatomy of the Lower Face: The Premasseter Space, the Jowl, and the Labiomandibular Fold Bryan C. Mendelson Æ
Aesth Plast Surg (2008) 32:185 195 DOI 10.1007/s00266-007-9060-3 ORIGINAL ARTICLE Surgical Anatomy of the Lower Face: The Premasseter Space, the Jowl, and the Labiomandibular Fold Bryan C. Mendelson Æ
ISPUB.COM. Cutting Burr Otoplasty. D Wynne, N Balaji INTRODUCTION ANATOMY CUTTING BURR TECHNIQUE
 ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 7 Number 1 D Wynne, N Balaji Citation D Wynne, N Balaji.. The Internet Journal of Otorhinolaryngology. 2006 Volume 7 Number 1. Abstract Prominent
ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 7 Number 1 D Wynne, N Balaji Citation D Wynne, N Balaji.. The Internet Journal of Otorhinolaryngology. 2006 Volume 7 Number 1. Abstract Prominent
Clinical Study Open Reduction of Subcondylar Fractures Using a New Retractor
 Plastic Surgery International Volume 2011, Article ID 421245, 5 pages doi:10.1155/2011/421245 Clinical Study Open Reduction of Subcondylar Fractures Using a New Retractor Akira Sugamata, 1 Naoki Yoshizawa,
Plastic Surgery International Volume 2011, Article ID 421245, 5 pages doi:10.1155/2011/421245 Clinical Study Open Reduction of Subcondylar Fractures Using a New Retractor Akira Sugamata, 1 Naoki Yoshizawa,
Spinal nerves and cervical plexus Prof. Abdulameer Al Nuaimi. E mail: a.al E. mail:
 Spinal nerves and cervical plexus Prof. Abdulameer Al Nuaimi E mail: a.al nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Branches of ophthalmic artery Muscles of face A spinal nerve Spinal
Spinal nerves and cervical plexus Prof. Abdulameer Al Nuaimi E mail: a.al nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Branches of ophthalmic artery Muscles of face A spinal nerve Spinal
Tracing the Cranial Nerves Osteologically
 CN I II III IV V 1 Supra-orbital ethmoidal nn. Ext. nasal V 2 Tracing the Cranial Nerves Osteologically Nucleus of Origin Olfactory tracts of frontal lobe of cerebrum Optic tracts from optic chiasma and
CN I II III IV V 1 Supra-orbital ethmoidal nn. Ext. nasal V 2 Tracing the Cranial Nerves Osteologically Nucleus of Origin Olfactory tracts of frontal lobe of cerebrum Optic tracts from optic chiasma and
Dr. Sami Zaqout, IUG Medical School
 The skull The skull is composed of several separate bones united at immobile joints called sutures. Exceptions? Frontal bone Occipital bone Vault Cranium Sphenoid bone Zygomatic bones Base Ethmoid bone
The skull The skull is composed of several separate bones united at immobile joints called sutures. Exceptions? Frontal bone Occipital bone Vault Cranium Sphenoid bone Zygomatic bones Base Ethmoid bone
The Melbourne Temporomandibular Total Joint Replacement System
 The Melbourne Temporomandibular Total Joint Replacement System Device Description: The Melbourne TMJ Total Joint Replacement System is used to reconstruct a damaged or diseased temporomandibular joint
The Melbourne Temporomandibular Total Joint Replacement System Device Description: The Melbourne TMJ Total Joint Replacement System is used to reconstruct a damaged or diseased temporomandibular joint
Temple and Postauricular Dissection in Face and Neck Lift Surgery
 Temple and Postauricular Dissection in Face and Neck Lift Surgery Topic Joo Heon Lee 1, Tae Suk Oh 2, Sung Wan Park 3, Jae Hoon Kim 3, Tanvaa Tansatit 4 1 Area88 Plastic Surgery Clinic, Seoul; 2 Department
Temple and Postauricular Dissection in Face and Neck Lift Surgery Topic Joo Heon Lee 1, Tae Suk Oh 2, Sung Wan Park 3, Jae Hoon Kim 3, Tanvaa Tansatit 4 1 Area88 Plastic Surgery Clinic, Seoul; 2 Department
Research Article Length and Geometric Patterns of the Greater Palatine Canal Observed in Cone Beam Computed Tomography
 International Dentistry Volume 2010, Article ID 292753, 6 pages doi:10.1155/2010/292753 Research Article Length and Geometric Patterns of the Greater Palatine Canal Observed in Cone Beam Computed Tomography
International Dentistry Volume 2010, Article ID 292753, 6 pages doi:10.1155/2010/292753 Research Article Length and Geometric Patterns of the Greater Palatine Canal Observed in Cone Beam Computed Tomography
Deposited on: 13 December 2010
 Ng, Z.Y., Fogg, Q., and Shoaib, T. (2010) Where to find facial artery perforators: a reference point. Journal of Plastic, Reconstructive & Aesthetic Surgery, 63 (12). pp. 2046-2051. ISSN 1748-6815. http://eprints.gla.ac.uk/45921/
Ng, Z.Y., Fogg, Q., and Shoaib, T. (2010) Where to find facial artery perforators: a reference point. Journal of Plastic, Reconstructive & Aesthetic Surgery, 63 (12). pp. 2046-2051. ISSN 1748-6815. http://eprints.gla.ac.uk/45921/
CHAPTER 11 FACIAL PARALYSIS. Shailesh Agarwal, MD and Arash Momeni, MD
 CHAPTER 11 FACIAL PARALYSIS Shailesh Agarwal, MD and Arash Momeni, MD The facial nerve innervates a total of 23 paired muscles and the orbicularis oris muscle. The majority of muscles innervated by the
CHAPTER 11 FACIAL PARALYSIS Shailesh Agarwal, MD and Arash Momeni, MD The facial nerve innervates a total of 23 paired muscles and the orbicularis oris muscle. The majority of muscles innervated by the
A Cadaveric Anatomical Study of the Levator Aponeurosis and Whitnall s Ligament
 접수번호 : 2008-087 Korean Journal of Ophthalmology 2009;23:183-187 ISSN : 1011-8942 DOI : 10.3341/kjo.2009.23.3.183 A Cadaveric Anatomical Study of the Levator Aponeurosis and Whitnall s Ligament Han Woong
접수번호 : 2008-087 Korean Journal of Ophthalmology 2009;23:183-187 ISSN : 1011-8942 DOI : 10.3341/kjo.2009.23.3.183 A Cadaveric Anatomical Study of the Levator Aponeurosis and Whitnall s Ligament Han Woong
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Anterior triangle of neck
 Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
CHAPTER 17 FACIAL AESTHETIC SURGERY. Christopher C. Surek, DO and Mohammed S. Alghoul, MD. I. BROW LIFT (Figures 1 and 2)
") CHAPTER 17 FACIAL AESTHETIC SURGERY Christopher C. Surek, DO and Mohammed S. Alghoul, MD I. BROW LIFT (Figures 1 and 2) A. Open Coronal Brow Lift Technique 1. Coronal incision is made in the hair-bearing
CHAPTER 17 FACIAL AESTHETIC SURGERY Christopher C. Surek, DO and Mohammed S. Alghoul, MD I. BROW LIFT (Figures 1 and 2) A. Open Coronal Brow Lift Technique 1. Coronal incision is made in the hair-bearing
EXTRACRANIAL MENINGIOMA PRESENTING AS INFRATEMPORAL FOSSA MASS: A CASE SERIES
 Case Series EXTRACRANIAL MENINGIOMA PRESENTING AS INFRATEMPORAL FOSSA MASS: A CASE SERIES Sunil Mathew * 1, Reddy Ravikanth 2, Vijaykishan B 3. ABSTRACT Extradural meningioma occurs as extracranial extension
Case Series EXTRACRANIAL MENINGIOMA PRESENTING AS INFRATEMPORAL FOSSA MASS: A CASE SERIES Sunil Mathew * 1, Reddy Ravikanth 2, Vijaykishan B 3. ABSTRACT Extradural meningioma occurs as extracranial extension
Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes
 DOI 10.1186/s40064-016-1714-7 RESEARCH Open Access Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes Chi Sun Yoon and Kyu Nam
DOI 10.1186/s40064-016-1714-7 RESEARCH Open Access Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes Chi Sun Yoon and Kyu Nam
Report of Ankylosis of the Temporomandibular Joint: Treatment with a Temporalis Muscle Flap and Augmentation Genioplasty
 Report of Ankylosis of the Temporomandibular Joint: Treatment with a Temporalis Muscle Flap and Augmentation Genioplasty Abstract A case of true bilateral ankylosis of the temporomandibular joint (TMJ)
Report of Ankylosis of the Temporomandibular Joint: Treatment with a Temporalis Muscle Flap and Augmentation Genioplasty Abstract A case of true bilateral ankylosis of the temporomandibular joint (TMJ)
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi
 Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
The Visible Ear Simulator Dissection Manual.
 The Visible Ear Simulator Dissection Manual. Stereoscopic Tutorialized Version 3.1, August 2017 Peter Trier Mikkelsen, the Alexandra Institute A/S, Aarhus, Denmark Mads Sølvsten Sørensen & Steven Andersen,
The Visible Ear Simulator Dissection Manual. Stereoscopic Tutorialized Version 3.1, August 2017 Peter Trier Mikkelsen, the Alexandra Institute A/S, Aarhus, Denmark Mads Sølvsten Sørensen & Steven Andersen,
Omran Saeed. Luma Taweel. Mohammad Almohtaseb. 1 P a g e
 2 Omran Saeed Luma Taweel Mohammad Almohtaseb 1 P a g e I didn t include all the photos in this sheet in order to keep it as small as possible so if you need more clarification please refer to slides In
2 Omran Saeed Luma Taweel Mohammad Almohtaseb 1 P a g e I didn t include all the photos in this sheet in order to keep it as small as possible so if you need more clarification please refer to slides In
Mandibular and Maxillary Anesthesia
 Mandibular and Maxillary Anesthesia Uses of the Conduction Technique JACK H. SELTSAM, D.D.S., M.D., Los Angeles THE ARMAMENTARIUM of a surgeon who operates on the head and neck should include the ability
Mandibular and Maxillary Anesthesia Uses of the Conduction Technique JACK H. SELTSAM, D.D.S., M.D., Los Angeles THE ARMAMENTARIUM of a surgeon who operates on the head and neck should include the ability
Original article Journal of International Medicine and Dentistry 2014; 1 (1): 10-18
: 10-18") Original article JOURNAL OF INTERNATIONAL MEDICINE AND DENTISTRY To search..to know...to share ISSN 2350-045X Study of variations in medial sural cutaneous nerve, lateral sural cutaneous nerve and peroneal
Original article JOURNAL OF INTERNATIONAL MEDICINE AND DENTISTRY To search..to know...to share ISSN 2350-045X Study of variations in medial sural cutaneous nerve, lateral sural cutaneous nerve and peroneal
THE MAXILLARY ARTERY IS THE
 ORIGINAL ARTICLE Anatomical Variability of the Maxillary Artery Findings From 100 Asian Cadaveric Dissections Jin Kook Kim, MD; Jae Hoon Cho, MD; Yeo-Jin Lee, MD; Chang-Hoon Kim, MD; Jung Ho Bae, MD; Jeung-Gweon
ORIGINAL ARTICLE Anatomical Variability of the Maxillary Artery Findings From 100 Asian Cadaveric Dissections Jin Kook Kim, MD; Jae Hoon Cho, MD; Yeo-Jin Lee, MD; Chang-Hoon Kim, MD; Jung Ho Bae, MD; Jeung-Gweon
An Isolated, Giant Infratemporal Fossa Schwannoma: Removal By Transmandibular Transpterygoid Approach
 ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 5 Number 2 An Isolated, Giant Infratemporal Fossa Schwannoma: Removal By Transmandibular Transpterygoid Rijuneeta, P Kumar Parida, V Mshesha,
ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 5 Number 2 An Isolated, Giant Infratemporal Fossa Schwannoma: Removal By Transmandibular Transpterygoid Rijuneeta, P Kumar Parida, V Mshesha,
The study of arterial anastomoses in the region of the alveolar process and the anterior maxilla wall in foetuses
 O R I G I N A L A R T I C L E Folia Morphol. Vol. 68, No. 2, pp. 65 69 Copyright 2009 Via Medica ISSN 0015 5659 www.fm.viamedica.pl The study of arterial anastomoses in the region of the alveolar process
O R I G I N A L A R T I C L E Folia Morphol. Vol. 68, No. 2, pp. 65 69 Copyright 2009 Via Medica ISSN 0015 5659 www.fm.viamedica.pl The study of arterial anastomoses in the region of the alveolar process