Pancreatic Pathology. Janak A. Parikh, MD, MSHS, FACS Clinical Teaching Faculty St. John Providence Hospital
|
|
|
- Sarah Gibson
- 5 years ago
- Views:
Transcription
1 Pancreatic Pathology Janak A. Parikh, MD, MSHS, FACS Clinical Teaching Faculty St. John Providence Hospital
2 Determination of resectability A 68 year old female presents with a biopsy proven adenoca of the pancreas. A staging CT scan demonstrates a 3 cm hypodense mass in the head of the pancreas with no evidence of extrapancreatic disease. There is evidence of abutment (< 30 O involvement) along the superior mesenteric vein-portal vein confluence. The celiac axis, superior mesenteric artery, and common hepatic artery are uninvolved.
3 Question The most appropriate management for this patient is: A. Endoscopic placement of a metal biliary stent B. Referral for neoadjuvant chemotherapy C. Surgical exploration with palliative biliary and gastric bypass D. Surgical exploration with pancreaticoduodenectomy E. Surgical exploration with total pancreatectomy
4 Answer The most appropriate management for this patient is: A. Endoscopic placement of a metal biliary stent B. Referral for neoadjuvant chemotherapy C. Surgical exploration with palliative biliary and gastric bypass D. Surgical exploration with pancreaticoduodenectomy E. Surgical exploration with total pancreatectomy



5 Pancreatic Cancer 45,000 new cases in 2013 Fourth leading cause of cancer death in the United States Only 10-15% of patients resectable Five year survival 20% for resected patients Five year survival 3% for all stages
 Resectable no evidence of")



6 CT Resectability-Classification Metastatic evidence of metastatic spread (typically to the liver, peritoneum or lung) Resectable no evidence of extra-pancreatic disease patent SMV/PV Normal tissue plane between tumor and the celiac, CHA, or the SMA. Borderline resectable patent SMV/PV, or short segment occlusion if reconstructable evidence of tumor abutment (< 180 degree or 50% vessel circumference) against celiac, CHA, or SMA Locally advanced SMV/PV occlusion with no option for reconstruction arterial encasement (> 180 degree or 50% vessel circumference) of celiac, CHA, or SMA
7 Management of severe gallstone pancreatitis 47 year old female presents with epigastric abdominal pain, vomiting and fevers Serum amylase is 4000 IU/ml, Tbili 2.6 mg/dl, AST 400 IU/L, ALT 450 U/L, and Alk Phos 720 U/L On admission she has four Ranson s criteria Ultrasound reveals multiple small gallstones and an 11 mm common bile duct.
8 Question The most appropriate management for this patient is: A. Endoscopic retrograde cholangiography and endoscopic sphincterotomy within 48 hours of admission B. Endoscopic retrograde cholangiography and endoscopic sphincterotomy prior to discharge C. Laparoscopic cholecystectomy and intraoperative cholangiography within 48 hours of admission D. Laparoscopic cholecystectomy and intraoperative cholangiography before discharge E. Open cholecystectomy and common bile duct exploration before discharge
9 Answer The most appropriate management for this patient is: A. Endoscopic retrograde cholangiography and endoscopic sphincterotomy within 48 hours of admission B. Endoscopic retrograde cholangiography and endoscopic sphincterotomy prior to discharge C. Laparoscopic cholecystectomy and intraoperative cholangiography within 48 hours of admission D. Laparoscopic cholecystectomy and intraoperative cholangiography before discharge E. Open cholecystectomy and common bile duct exploration before discharge
 GSP responsible for 40-50%% of all cases of acute pancreatitis")

10 Gallstone Pancreatitis Acute pancreatitis 240,000/yr (40 cases/100,000) Necrotizing pancreatitis 15-20% (mortality: 15 20%) GSP responsible for 40-50%% of all cases of acute pancreatitis Pathogenesis related to transient obstruction of pancreatic duct Gallstones recovered in stool of 85% of patients with GSP vs. 10% of patients with symptomatic cholelithiasis Jemal, et al. CA 2007; 57: 47







11 2 Phases: Pathogenesis of Acute Pancreatitis Day 0-14 = SIRS cytokine mediated organ dysfunction Day 15 on = resolution vs. infection of pancreatic necrosis Zymogen activation Generation of inflammatory mediators Ischemia Systemic inflammatory response Multi-organ failure Insult Inflammation Ischemia Necrosis Apoptosis Werner et al. Gut 2005; 54:426-36
12 % Mortality Severity Scoring Systems in Acute Pancreatitis 20% will have severe disease Clinical scoring systems to predict severity Ranson s criteria Glasgow criteria APACHE-II Balthazar CT Grade A-E A: Normal B: Enlargement (edema) C: Abnl gland + peripanc inflam D: Fluid collection in 1 loc On admission or diagnosis Age White blood cell count Blood glucose LDH SGOT During initial 48 h Hematocrit decrease Blood urea nitrogen increase Serum calcium level Arterial po 2 Base deficit Fluid sequestration E: 2 or more fluid collections/gas adjacent to pancreas Acute pancreatitis Alcohol-induced Biliary > 55 years > 16000/mm 3 > 200 mg/dl > 350 U/I > 250 U/I > 10 % > 5 mg/dl > 8 mg/dl > 60 mm Hg > 4 meq/i > 6 I > 70 years > 18000/mm 3 > 220 mg/dl > 400 U/I > 250 U/I > 10 % > 2 mg/dl > 8 mg/dl > 5 meq/i > 4 I 0 to 2 3 to 5 6 to 8 9 to 11 Score
13 Randomized trials of early ERCP for gallstone pancreatitis Author Yr N ERCP Comp Mortality Timing ERCP Control ERCP Controls Neoptolemos Fan <72 hrs 24* < 24 hrs 0* Nowak < 24 hrs 17* 36 2* 13 Folsch <72 hrs Acosta < 48 hrs 29* Oria <72 hrs * Significantly different vs controls



14 Management of Gallstone Pancreatitis Patients with severe gallstone pancreatitis who fail to improve substantially during the initial 24 hour period should be considered for urgent endoscopic ERCP and endoscopic biliary sphincterotomy Patients with mild GSP should undergo cholecystectomy during the initial hospitalization If the gallbladder not removed risk of recurrent pancreatitis - 90% 3 months recurrence - 50%
15 Pancreatic Pseudocyst 50 year old male with diabetes and a past history of heavy alcohol use (none in the past year) presents with a 6 week history of left upper quadrant abdominal pain and fullness CT shows calcifications throughout the pancreas, a non dilated pancreatic duct in the head In the tail of the pancreas there is a 8 cm pseudocyst bulging against the transverse mesocolon associated with a dilated pancreatic duct (8 mm)
16 Question The most appropriate management for this patient is: A. Percutaneous cyst drainage B. Endoscopic cyst gastrostomy C. Surgical cyst gastrostomy D. Surgical Roux en Y pancreatic cyst jejunostomy E. Distal pancreatectomy and splenectomy
17 Answer The most appropriate management for this patient is: A. Percutaneous cyst drainage B. Endoscopic cyst gastrostomy C. Surgical cyst gastrostomy D. Surgical Roux en Y pancreatic cyst jejunostomy E. Distal pancreatectomy and splenectomy
18 Pancreatic Pseudocyst A fluid collection contained within a well-defined capsule of fibrous or granulation tissue or a combination of both Does not possess an epithelial lining Persists > 4 weeks Etiology Acute Pancreatitis Chronic pancreatitis Pancreatic trauma Pancreatic neoplasm

19 Natural History of Pseudocyst ~50% resolve spontaneously Size Nearly all <4cm resolve spontaneously >6cm 60-80% persist, necessitate intervention Cause Traumatic, chronic pancreatitis <10% resolve Duration - Less likely to resolve if persist > 6-8 weeks

20 Complications Infection GI obstruction Perforation Hemorrhage Recent hemorrhage Pseudoaneurysm Thrombosis Pseudoaneurysm
 Complications Suspicion of malignancy Intervention Percutaneous drainage Endoscopic drainage Surgical")
21 Pancreatic Pseudocyst Indications for drainage Presence of symptoms (> 6 wks) Enlargement of pseudocyst ( > 6 cm) Complications Suspicion of malignancy Intervention Percutaneous drainage Endoscopic drainage Surgical drainage


22 Operative Therapy Cystgastrostomy for cysts adhered to posterior wall of stomach Cystduodenostomy cysts in head and uncinate process of pancreas Cystjejunostomy via Roux-en Y limb, for cysts adhered elsewhere i.e. to transverse mesocolon
23 Management of IPMN A 67 year old male with acute onset right lower quadrant abdominal pain undergoes a CT scan for presumed appendicitis. An incidental 2 cm cyst is identified in the tail of the pancreas. Endoscopic ultrasound reveals a unilocular cyst, no evidence of mural nodularity, and a non dilated main pancreatic duct. Cyst aspiration reveals a cyst fluid amylase of 200,000 U/L and a cyst fluid CEA level of 400 ng/ml.
24 Question The most appropriate management for this patient is: A. Distal pancreatectomy and splenectomy B. Pancreatic cyst enucleation C. Endoscopic alcohol cyst ablation D. Endoscopic retrograde cholangiopancreatography E. Surveillance with MRI/MRCP in six months
25 Answer The most appropriate management for this patient is: A. Distal pancreatectomy and splenectomy B. Pancreatic cyst enucleation C. Endoscopic alcohol cyst ablation D. Endoscopic retrograde cholangiopancreatography E. Surveillance with MRI/MRCP in six months
26 Cystic Pancreatic Neoplasms TYPES OF CYSTIC NEOPLASMS Benign Premalignant Malignant Pseudocyst Serous Cystadenoma (SCN) Solid Pseudopapillary Neoplasm (SPN) Main Duct IPMN (MD-IPMN) Mucinous Cystic Neoplasm (MCN) Branch-Duct IPMN (BD-IPMN) Main Duct IPMN (MD-IPMN) Mucinous Cystic Neoplasm (MCN) Branch-Duct IPMN (BD-IPMN) Cystic Neuroendocrine (PNET)


27 Cystic Pancreatic Neoplasms SEROUS CYSTADENOMA


28 Cystic Pancreatic Neoplasms SOLID PSEUDOPAPILLARY NEOPLASM


29 Cystic Pancreatic Neoplasms MUCINOUS CYSTIC NEOPLASM

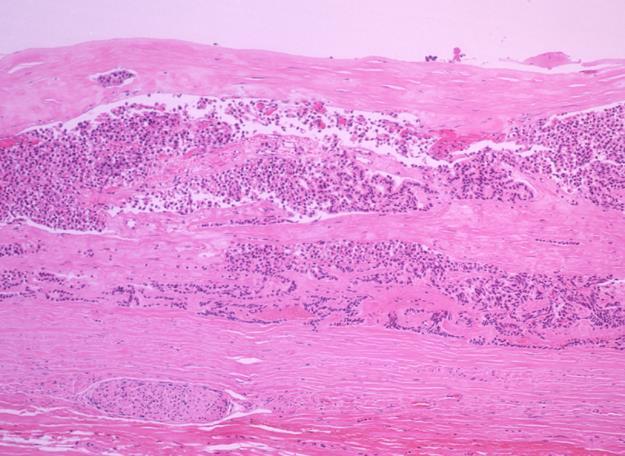
30 Cystic Pancreatic Neoplasms NEUROENDOCRINE TUMOR




31 Cystic Pancreatic Neoplasms INTRADUCTAL PAPILLARY MUCINOUS NEOPLAMS CT Head CT Body Gross Pathology Microscopic Path
32 MAKING A DIAGNOSIS
33 Cystic Pancreatic Neoplasms OBTAIN A THOROUGH HISTORY Symptoms Pain Pancreatic insufficiency New onset diabetes History of pancreatitis Family history of pancreatic cancer
34 Cystic Pancreatic Neoplasms IS THEIR PANCREATIC DUCTAL COMMUNICATION? Dilated main duct or side-branch on CT/MR MRI/MRCP* EUS Cyst fluid aspirate for amylase ERCP Yes DDx=Pseudocyst, IPMN No DDX=SCN, MCN
35 Cystic Pancreatic Neoplasms DISTINGUISH BETWEEN MUCINOUS VS. NON-MUCINOUS EUS-guided FNA for: Mucin CEA (>200) ERCP: mucin extruding from ampulla Yes DDx=MCN, IPMN No DDx=Pseudocyst, SCN
36 Cystic Pancreatic Neoplasms WHO NEEDS AN EUS? All cysts >=1cm to look for high-risk stigmata or worrisome features High-risk stigmata : MPD>=10mm or enhancing solid component Worrisome features : Cyst>=3cm, MPD5-9mm, non-enhancing solid component, thickened or enhancing cyst wall, abrupt change in MPD caliber with distal atrophy, lymphadenopathy
37 Cystic Pancreatic Neoplasms WHO NEEDS AN EUS? Diagnostic uncertainty Cyst fluid analysis for mucin, CEA, amylase Characterizing risk of malignancy Cyst fluid analysis for molecular markers (investigational)
38 WHAT TO DO NOW? WHEN TO OPERATE
39 % Patients Symptomatic SYMPTOMS & CYST PATHOLOGY *p<0.05 vs Benign * * 0 Benign Premalignant Malignant

40 AGE & CYST PATHOLOGY % Patients >70yrs *p<0.02 vs Benign & Premalignant Benign Premalignant Malignant *
41 Cystic Pancreatic Neoplasms PSEUDOCYSTS, SCN, SPN Pseudocysts: Treat if symptomatic (pain, mass effect, infected) Operation: Internal drainage SCN: Treat if symptomatic (pain, mass effect) in good risk patient Operation: Can enucleate if away from MPD; otherwise resection based on location
42 International Consensus Guidelines Worrisome Features MPD 5-9mm Cyst >3cm Thickened-enhanced cyst wall High-Risk Stigmata MPD>=10mm Enhancing solid component Non-enhancing mural nodule Abrupt change in MPD caliber w/ distal atrophy LAD
43 Cystic Pancreatic Neoplasms MCN, IPMN 2012 Consensus guidelines MCN and MD-IPMN: Should all be formally resected in appropriate surgical candidates BD-IPMN: Resect if high-risk stigmata present Consider resection for worrisome features
44 % Invasive or Malignant IPMN INCIDENCE OF MALIGNANCY/ INVASION BY DUCT INVOLVEMENT 60% * 50% 40% Malignant, *P<0.001 Invasive, **P= % 30% 20% 19% ** 28% 10% 14% 0% Branch DUCT INVOLVEMENT Main
45 % Invasive or Malignant IPMN INCIDENCE OF MALIGNANT/ INVASIVE 60% BRANCH DUCT BY SIZE 50% 40% Malignant, P= NS Invasive, P= NS 30% 20% 10% 17% 17% 20% 13% 19% 14% 0% <10mm 10mm-30mm >30mm Size (ICG Category)

46 % Incidence Mural Nodules 60% MURAL NODULE INCIDENCE : BRANCH DUCT IPMN 50% 40% 30% Mural Nodule * 33% * P= * 28% 20% 10% 7% 7% 0% Adenoma Borderline CIS Invasive Grade of Dysplasia
47 PREDICTORS OF MALIGNANCY MULTIVARIATE ANALYSIS MALIGNANT OR P Main Duct IPMN RADIOGRAPHIC Mural nodule 4.3 <0.01 INVASIVE Main Duct IPMN MALIGNANT OR P Mural nodule OVERALL Cytopathology INVASIVE Mural nodule 4.3 <0.04 Male Gender 3.6 <0.002 Cytopathology 4.3 <0.04
48 Cystic Pancreatic Neoplasms IPMN SUMMARY IPMNs occur in elderly pts, M>F Progression to invasive cancer 5-10 yrs Surgery can be performed safely 50-70% noninvasive, % survival 30-50% invasive, 40-60% survival 10-20% of noninvasive tumors recur 45-65% of invasive tumors recur

49 Cystic Pancreatic Neoplasms IPMN CONCLUSIONS IPMNs offer a unique opportunity to prevent or treat a less virulent form of pancreatic cancer Surgical resection should be recommended even in fit elderly patients Total pancreatectomy is not routinely recommended Careful follow-up is necessary after resection
50 Cystic Pancreatic Neoplasms WHEN TO OPERATE Older fit patients malignancy Symptomatic pts premalig or malig Increasing in size premalig or malig Younger asymptomatic cost effective
51 Cystic Pancreatic Neoplasms WHAT OPERATION Benign and premalignant Enucleation Segmental resection Laparoscopic resection Splenic preservation Main duct IPMN and malignant Resection - negative margins Palliative bypasses
52 Preoperative localization of insulinoma 45 year old male with acute onset of mental status changes Labs reveal a serum glucose of 30 mg/dl Fasting Proinsulin and C-peptide are elevated CT scan of the abdomen demonstrates no lesions in the pancreas
53 Question The most appropriate management for this patient is: A. magnetic resonance pancreatography B. octreotide scan C. ERCP D. EUS E. Arteriography with selective venous sampling
54 Answer The most appropriate management for this patient is: A. magnetic resonance pancreatography B. octreotide scan C. ERCP D. EUS E. Arteriography with selective venous sampling
55 Pancreatic Endocrine Tumors Incidence = 1 in 100,000; 2500 new cases each year in US Adeno:PEN 125:1 Second most common source of isolated liver metastases after colorectal cancer Secrete biologically active substances resulting in disabling symptoms Sporadic or association with MEN1
56 PNET: Insulinoma Sx: hypoglycemia (fasting <45), neuroglycopenic symptoms, relief of symptoms with glucose (Whipple s triad); obesity (wt gain) Weakness Diaphoresis Shaking Blurry vision Speech disturbances Confusion
57 PNET: Insulinoma Diagnosis Elevated serum insulin glucose ratio (ratio>0.3) Elevated C-peptide > hour fasting test Admission and glucose monitoring every 2 hours Insulin levels when glucose<50mg/dl Sensitivity: 75% at 24hrs, 90% at 48hrs, 98% at 72hrs Insulin >5 in setting of hypoglycemia highly suggestive WU: NO octreotide scan; CT/MRI/EUS Even distribution in pancreas (head/body/tail) Can hide in duodenum, splenic hilum, gastrocolic ligament 10% malignant, 10% multiple tumors, 10% MEN 1
 scanning EUS - 85%sensitivity EUS especially useful for detection of small NETs (< 2.")
58 PNET: Insulinoma Tend to be small tumors (<2 cm) Usually are solitarysolitary Benign (>90%) Uniformly distributed throughout pancreas Pre-operative localization difficult CT, US, and MRI have a <50% sensitivity Don t light up with (octreotide) scanning EUS - 85%sensitivity EUS especially useful for detection of small NETs (< 2.5 cm) missed by other imaging studies Arteriography with selective venous sampling has sensitivity in the 80%-90% range but is an invasive
59 PNET: Gastrinoma Sx: Diarrhea (improved with NGT), refractory ulcers or ulcers in unusual locations Dx: Serum gastrin >1000, Secretin stimulation test (gastrin increase >200) WU: Octreotide scan is best, CT/MR/EUS Tx: Resection, most in gastrinoma triangle (CD, panc neck/body, D2/D3) Located in duodenum in up to 60% 25% associated with MEN I (usually duodenum and multiple)
60 PNET: Gastrinoma Causes of hypergastrinemia High acid ZES (gastrinoma) GOO G-cell hyperplasia Retained antrum Low acid H2 blocker/ppi Atrophic gastritis Pernicious anemia Vitiligo Achlorhydria ESRD Vagotomy
61 PNET: Somatostatinoma Sx: Steatorrhea, Cl, gallstones, DM Dx: Somatostatin level pg/dL (14mol/L fasting) WU: Octreotide, CT/MR/EUS Tx: Resection Nearly all are malignant NOT associated with MEN1, but associated with pheochromocytoma and von Recklinghausen s (NF1)
62 Can be associated with MEN1 (10%) PNET: VIPoma Sx: watery diarrhea (persists despite fasting or NGT), K Cl (WDHA) Dx: elevated serum VIP ( ) WU: Octrotide scan, CT/MR, 10% can be extrapancreatic Tx: Resection 75% found in body/tail pancreas 50% malignant
63 PNET: Glucagonoma Sx: Necrolytic migratory erythema (dematitis), DM, anemia Dx: Glucagon , glucagonoma syndrome: 4Ds (DM, dermatits, DVT, depression) WU: Octreotide scan, CT/MR/EUS Tx: Resection Most found in body/tail of pancreas Nearly all are malignant
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
Pancreatic Cysts. Darius C. Desai, MD FACS St. Luke s University Health Network
 Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Outline. Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines
 Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines") Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Index (SIRS), 158, 173
, 158, 173") Index A Acute pancreatitis surgery abdominal compartment syndrome, 188 adjuvant treatment, 194 anterior approach, 175 antibiotic prophylaxis, 166 167, 197 Atlanta classification, 181 classification of
Index A Acute pancreatitis surgery abdominal compartment syndrome, 188 adjuvant treatment, 194 anterior approach, 175 antibiotic prophylaxis, 166 167, 197 Atlanta classification, 181 classification of
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Citation American Journal of Surgery, 196(5)
") NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Laparoscopic & Robotic Surgery in Pancreas Disease
 2007 년도대한췌담도학회추계학술대회 Session IV: Recent Updates in Pancreatobiliary Diseases Laparoscopic & Robotic Surgery in Pancreas Disease Department of Surgery, Yonsei University College of Medicine, Korea Woo-Jung
2007 년도대한췌담도학회추계학술대회 Session IV: Recent Updates in Pancreatobiliary Diseases Laparoscopic & Robotic Surgery in Pancreas Disease Department of Surgery, Yonsei University College of Medicine, Korea Woo-Jung
Neuro-endocrine and pancreatic non-adenocarcinomas. Marc Engelbrecht, AMC, Amsterdam
 Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Assistant Professor: Dr.Samer Al-Sawalhi (M.R.C.S.I)(M.D)
(M.D)") Assistant Professor: Dr.Samer Al-Sawalhi (M.R.C.S.I)(M.D) The incidence of pancreatic ca is 10:100000 population per year *The disease is a disease of ageing. Male=Female *Approximately 80-90%
Assistant Professor: Dr.Samer Al-Sawalhi (M.R.C.S.I)(M.D) The incidence of pancreatic ca is 10:100000 population per year *The disease is a disease of ageing. Male=Female *Approximately 80-90%
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Diagnosis abnormal morphology and /or abnormal biochemistry
 Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS
 Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Cystic pancreatic lesions A proposal for a network approach. Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth
 Cystic pancreatic lesions A proposal for a network approach Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth Aims Brief overview of cystic pancreatic lesions International
Cystic pancreatic lesions A proposal for a network approach Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth Aims Brief overview of cystic pancreatic lesions International
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
X-ray Corner. Imaging of The Pancreas. Pantongrag-Brown L
 X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
Intraductal Papillary Mucinous Neoplasm of Pancreas
 Review Article Intraductal Papillary Mucinous Neoplasm of Pancreas Norman Oneil Machado, Hani al Qadhi, Khalifa al Wahibi Department of Surgery, Sultan Qaboos University Hospital, Muscat, Oman Abstract
Review Article Intraductal Papillary Mucinous Neoplasm of Pancreas Norman Oneil Machado, Hani al Qadhi, Khalifa al Wahibi Department of Surgery, Sultan Qaboos University Hospital, Muscat, Oman Abstract
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Case Presentation. PMH: HTN, BPH, strabismus PSH: appendectomy Medications: norvasc, tamsulosin NKDA SH/FH: negative
 Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
Cystic Pancreatic Lesions: Approach to Diagnosis
 Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
6 th August 2018 Day 1 - Gallbladder & Bile duct Topic
 Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Update on Surgical Management of NETs
 Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts
 Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Video Microscopy Tutorial 19
 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Pancreatic Cystic Neoplasms: Guidelines and beyond
 Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment
 Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
General Surgery PURPLE SERVICE MUHC-RVH Site
 Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas)
 (see also: biliary/pancreatic folios => pancreas)") Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas) Physiology ductal system produces bicarb, high carbonic anhydrase secretin primary stimulus duodenal enterokinase activates trypsin
Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas) Physiology ductal system produces bicarb, high carbonic anhydrase secretin primary stimulus duodenal enterokinase activates trypsin
SOLID PANCREATIC NEOPLASMS
 SOLID PANCREAIC NEOPLASMS SCBMR, Annual Meeting October 6-10, 2012 Boston, MA Isaac R Francis, M.B; B.S. University of Michigan Ann Arbor, Michigan Over 43,000 estimated cases in US in 2010 Over 36,000
SOLID PANCREAIC NEOPLASMS SCBMR, Annual Meeting October 6-10, 2012 Boston, MA Isaac R Francis, M.B; B.S. University of Michigan Ann Arbor, Michigan Over 43,000 estimated cases in US in 2010 Over 36,000
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Morning Report. Allison Haden, MD October 1, 2002
 Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review
 Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
Endoscopic Ultrasonography Clinical Impact. Giancarlo Caletti. Gastroenterologia Università di Bologna. Caletti
 Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
LIVER. Question 1 ~ Anatomy. Answer 1 ~ Anatomy 1/5/2018. SEMCME Board Review January 11-12, 2017
 SEMCME Board Review January 11-12, 2017 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
SEMCME Board Review January 11-12, 2017 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
Surgical Treatment of Hepatobiliary and Splenic Disorders
 SEMCME Board Review January 10-11, 2019 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
SEMCME Board Review January 10-11, 2019 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Cystic Disease of the Liver Work Up and Management. Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center
 Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Pancreatic cysts: etiology, diagnosis and management
 Cent. Eur. J. Med. 9(1) 2014 92-107 DOI: 10.2478/s11536-013-0244-8 Central European Journal of Medicine Pancreatic cysts: etiology, diagnosis and management Review Article Beata Jabłońska* Department of
Cent. Eur. J. Med. 9(1) 2014 92-107 DOI: 10.2478/s11536-013-0244-8 Central European Journal of Medicine Pancreatic cysts: etiology, diagnosis and management Review Article Beata Jabłońska* Department of
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Research Article The Changing Spectrum of Surgically Treated Cystic Neoplasms of the Pancreas
 HPB Surgery Volume 2015, Article ID 791704, 7 pages http://dx.doi.org/10.1155/2015/791704 Research Article The Changing Spectrum of Surgically Treated Cystic Neoplasms of the Pancreas Jennifer K. Plichta,
HPB Surgery Volume 2015, Article ID 791704, 7 pages http://dx.doi.org/10.1155/2015/791704 Research Article The Changing Spectrum of Surgically Treated Cystic Neoplasms of the Pancreas Jennifer K. Plichta,
Yoshitsugu; Kanematsu, Takashi; Kur
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation Laparoscopic Middle Pancreatectomy Surgery Kitasato, Amane; Adachi, Tomohiko; Yoshitsugu; Kanematsu, Takashi; Kur Hepato-Gastroenterology, 59(120),
NAOSITE: Nagasaki University's Ac Title Author(s) Citation Laparoscopic Middle Pancreatectomy Surgery Kitasato, Amane; Adachi, Tomohiko; Yoshitsugu; Kanematsu, Takashi; Kur Hepato-Gastroenterology, 59(120),
Chronic Pancreatitis. Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture
 Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Genetics of Pancreatic Cancer. October 6, If you experience technical difficulty during the presentation:
 Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
PATHOLOGY MCQs. The Pancreas
 PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma