Morning Report. Allison Haden, MD October 1, 2002
|
|
|
- Prosper Ford
- 5 years ago
- Views:
Transcription
1 Morning Report Allison Haden, MD October 1, 2002
2 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious, no blood constant diffuse abdominal pain, worse with eating in the LUQ + weight loss, unable to quantify symptoms less severe with liquids
3 Family says: Worse in last 2 weeks symptoms going on for about 1 year h/o heavy ETOH, none in several months due to illness weight loss of greater than 40 pounds abdominal pain very severe and limiting po intake
4 ROS: Diffuse mild weakness normal BM s but only one every 3 days no fevers, chills no abdominal distension or increasing girth no CP, SOB, LE edema
5 Past Medical History Colon CA dx d 1993 s/p partial colectomy, reanastamosis, XRT, CTX COPD h/o heavy ETOH, no sz s or DT s chronic pancreatitis presumably due to ETOH, not hospitalized in last 3 years, but several hospitalizations in past ALLERGY- iodine causing hives
6 PMH (cont d.) Social: Lives in Clinton by himself. Retired TV repair man on disability. Widower since py h/o tobacco, currently 2ppd Denies ETOH in several months, but h/o several fifths and at least a six pack per day denies other drug use
7 PMH (cont d) Family hx: mother died at 60 w/breast CA, father died in 80 s from CAD/CHF
8 Physical Exam Cachectic, temporal wasting, NAD CV: RRR, no m/r/g Lungs: CTAB Abd: soft, voluntary guarding, no rebound, diffuse tenderness, no HSM, hypoactive BS,? ascites Ext: no c/c/e Neuro: nonfocal
9 Labs: WBC 9.9, HCT 32.8, plt 435, chem 7 WNL, Tbili 0.5, AST 38, ALT 29, AP 166, GGT 167, lipase 330, alb 1.4, PT 13.3, PTT 30.2, TSH 2.7 Diagnostic studies performed

10

11
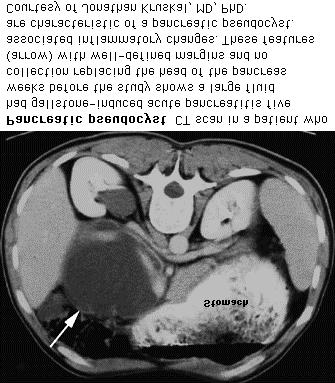
12 CT Scan Abdomen and Pelvis Liver w/low attenuation c/w steatosis, no focal lesions, diffuse abdominal ascites, and cholelithiasis poorly enhancing, atrophic pancreas, scattered calcifications pancreatic fluid collections: 3.9x3.4cm in head, 5x3cm in tail, and 12x7cm adjacent to LL of liver w/adjacent 5x8cm exerting mass effect on stomach and duodenum

13

14
15 EGD/Colonoscopy Small amount of debris in stomach large extrinsic bulge along greater curvature of stomach creating a partial gastric outlet obstruction several <1cm sessile polyps and widely patent left colon anastamosis
16 Pancreatic Pseudocysts Definition: pancreatitis or ductal leakage resulting in a collection of pancreatic enzymes encased by reactive granulation tissue in or around the pancreas walls are adjacent structures (stomach, colon, omentum, pancreas) and lining is granulation tissue (not epithelium)

17
18 Etiology: after acute pancreatitis: 10% of cases, formed from liquefaction of necrotic pancreatic and peripancreatic tissue which may communicate with the pancreatic duct or cause gross leakage of enzymes chronic pancreatitis (usually ETOH) causing chronic ductal obstruction from sticture or protein plugs which increases intraductal pressure inducing leakage blunt or penetrating trauma disrupting the pancreatic duct
19
20 Symptoms mostly asymptomatic pain, duodenal or biliary obstruction, vascular occlusion, fistula formation infection and abscess formation pseudoaneurysm from digestion of adjacent vessel causing GI bleed or bleed into pancreatic duct (hemosuccus pancreaticus) pancreatic ascites or pleural effusion
21 Diagnosis usually by US or CT, fluid will have high amylase levels Watch out for neoplasm: concern for if no h/o pancreatitis or trauma, no inflammatory changes on CT, or septated cysts pseudoaneuysm: in 10% of cases, risk of fatal hemorrhage with endoscopic drainage, must undergo embolization (coils or gel foam), concern for if unexplained GI bleed or HCT drop or sudden pseudocyst expansion
22 Classic surgical teaching: Bradley, et al. Am J Surg, wks, rare resolution and 50% complication rate 13 wks no resolution, and high complication rate recommended resection at 6 wks more recent studies have shown that expectant management has low complication rate if no significant abdominal pain, early complications, or continued enlargement of the cyst Vitas, et al. Surgery, 1992
23 Drainage Options Surgical internal drainage: CG, CD, CJ or resection of tail +/- splenectomy. Morbidity 15%, mortality <5%, and recurrence 10%, complication of external pancreatic fistulas Percutaneous catheter drainage: as effective as surgery, +/- octreotide, complication of tract infection
24 Endoscopy: ECG, ECD, ERCP % resolve, complications of bleeding, perforation, infection, and recurrence (6-18%.) Minimal mortality. EUS and FNA becoming more popular to differentiate neoplasm from pseudocyst and find spot for drainage. Severe pancreatic necrosis on CT is deterrent to endoscopy as seems to have higher risk of infectious complications
25 Pancreatic abscess requires operative debridement and drainage. May use endoscopic drainage if poor operative candidate. Generally recommend transpapillary stenting if cyst is solitary and small (<6cm), and transmural drainage if pancreatic duct is obstructed or if >6cm
26 Summary Pancreatic pseudocysts are often asymptomatic, but can have a wide range of presentations Complications can be life-threatening, but chances of happening decrease significantly with time Reserve intervention to those w/sx s and have not had resolution over time
27 References Bradley, et al. The natural history of pancreatic pseudocysts. Am J Surg 1979; 137:135. O malley, et al. Pancreatic pseudocysts: Cause, theapy, and results. Am J Surg 1985; 150:680. Vitas, et al. Selective management of pancreatic psuedocyts. Surgery 1992; 111:123. Yeo, et al. The natural history of pancreatic pseudocysts documented by CT. Surg Gynecol 1990; 170:411. Up to Date Online version
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies. Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels
 PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels 1. Diagnosis. 2. Multidisciplinary approach. 3. Therapeutic planning. 4. How? 5. Follow-up
PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels 1. Diagnosis. 2. Multidisciplinary approach. 3. Therapeutic planning. 4. How? 5. Follow-up
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
U Nordic Forum - Trauma & Emergency Radiology. Lecture Objectives. MDCT in Acute Pancreatitis. Acute Pancreatitis: Etiologies
 Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
GI Grand Rounds. A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards
 GI Grand Rounds A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards PMH Aug 25, 1992 4 year old male presents to a pediatric gastroenterologist for primary complaint of anorexia, intermittent abdominal
GI Grand Rounds A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards PMH Aug 25, 1992 4 year old male presents to a pediatric gastroenterologist for primary complaint of anorexia, intermittent abdominal
Chronic Pancreatitis. Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture
 Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
53 year old Female with Hypoglycemia. Colleen Flynn, MD April 5, 2012
 53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
The Influence of Pancreatic Ductal Anatomy on the Complications of Pancreatitis. William H. Nealon M.D.
 The Influence of Pancreatic Ductal Anatomy on the Complications of Pancreatitis William H. Nealon M.D. Students and Trainees: Guide to Creativity, Productivity and Innovation in a Clinical Career Choose
The Influence of Pancreatic Ductal Anatomy on the Complications of Pancreatitis William H. Nealon M.D. Students and Trainees: Guide to Creativity, Productivity and Innovation in a Clinical Career Choose
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD
 Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those
Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Treatment of chronic calcific pancreatitis endoscopy versus surgery
 Treatment of chronic calcific pancreatitis endoscopy versus surgery 35 - year old ladypresented to LPC Mumbai with intermittent abdominal pain. Pain was intermittent, colicky, more in epigastrium and periumbilical
Treatment of chronic calcific pancreatitis endoscopy versus surgery 35 - year old ladypresented to LPC Mumbai with intermittent abdominal pain. Pain was intermittent, colicky, more in epigastrium and periumbilical
Multi modality Imaging in Acute Pancreatitis. Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009
 Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Case Presentation: Mr. S
 Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Cecal Volvulus: Case Presentation and Review of CT Findings
 August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report
 Chin J Radiol 2003; 28: 347-351 347 Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report HSIN-YI LAI YUNG-FANG CHEN HSEIN-JAR CHIANG WU-CHUNG SHEN Department
Chin J Radiol 2003; 28: 347-351 347 Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report HSIN-YI LAI YUNG-FANG CHEN HSEIN-JAR CHIANG WU-CHUNG SHEN Department
Case Presentation. PMH: HTN, BPH, strabismus PSH: appendectomy Medications: norvasc, tamsulosin NKDA SH/FH: negative
 Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Evolving Gallstone Ileus. SUNY Downstate Case Conference January 12, 2012
 Evolving Gallstone Ileus SUNY Downstate Case Conference January 12, 2012 Initial Presentation HPI: 90 yo F c 1wk h/o abdominal pain and N/V. Denied F/C. Passing flatus/bm. PMH: DM, HTN, CAD. PSH: C-sections
Evolving Gallstone Ileus SUNY Downstate Case Conference January 12, 2012 Initial Presentation HPI: 90 yo F c 1wk h/o abdominal pain and N/V. Denied F/C. Passing flatus/bm. PMH: DM, HTN, CAD. PSH: C-sections
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
and Transmural Drainage
 HPB Surgery, 2000, Vol. 11, pp. 333-338 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
HPB Surgery, 2000, Vol. 11, pp. 333-338 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Endoscopic Management of Acute Pancreatitis. Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018
 Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
Spontaneous Regression of Pancreatic. Pseudocyst Mimicking a Submucosal. Tumor of the Stomach with Upper. Gastrointestinal Bleeding.
 2006 17 128-132 Spontaneous Regression of Pancreatic Pseudocyst Mimicking a Submucosal Tumor of the Stomach with Upper Gastrointestinal Bleeding Report of a Case Kuo-Chih Tseng, Yu-Hsi Hsieh, Chang-An
2006 17 128-132 Spontaneous Regression of Pancreatic Pseudocyst Mimicking a Submucosal Tumor of the Stomach with Upper Gastrointestinal Bleeding Report of a Case Kuo-Chih Tseng, Yu-Hsi Hsieh, Chang-An
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
SOD (Sphincter of Oddi Dysfunction)
") SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram
 Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Background. RUQ Ultrasound Normal, Recommend Clinical Correlation. Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial
 RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Cystic liver lesion and eosinophilia
 November, 2005 Cystic liver lesion and eosinophilia Jakob Begun, Harvard medical School Year III Patient Presentation 55 year old Cape Verde female presented to her PCP with 6 month history of variable
November, 2005 Cystic liver lesion and eosinophilia Jakob Begun, Harvard medical School Year III Patient Presentation 55 year old Cape Verde female presented to her PCP with 6 month history of variable
Acute Pancreatitis: Role of Imaging Modalities
 International Journal of Interdisciplinary and Multidisciplinary Studies (IJIMS), 2015, Vol 2, No.9,109-114. 109 Available online at http://www.ijims.com ISSN: 2348 0343 Abstract Acute Pancreatitis: Role
International Journal of Interdisciplinary and Multidisciplinary Studies (IJIMS), 2015, Vol 2, No.9,109-114. 109 Available online at http://www.ijims.com ISSN: 2348 0343 Abstract Acute Pancreatitis: Role
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Chronic Pancreatitis
 Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Chronic Pancreatitis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun,
Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Chronic Pancreatitis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun,
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Frank Burton Memorial Update on Pancreato-biliary Cancers
 Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance of Gillian Lieberman, MD
 Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
What Is Pancreatitis?
 What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
M. Ellrichmann; C. Jürgensen; A. Arlt; A. Fritscher-Ravens
 Randomized multicenter study on pancreatic duct stenting in disrupted or obstructed ducts in context with endoscopic treatment of pancreatic pseudocysts. M. Ellrichmann; C. Jürgensen; A. Arlt; A. Fritscher-Ravens
Randomized multicenter study on pancreatic duct stenting in disrupted or obstructed ducts in context with endoscopic treatment of pancreatic pseudocysts. M. Ellrichmann; C. Jürgensen; A. Arlt; A. Fritscher-Ravens
Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pritesh Mutha, MD, MPH
 Virginia Commonwealth University Fellow Presentations Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pit Pritesh hm Mutha, MD, MPH Benign Esophageal Stricture Sanjay
Virginia Commonwealth University Fellow Presentations Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pit Pritesh hm Mutha, MD, MPH Benign Esophageal Stricture Sanjay
Overview. Doumit S. BouHaidar, MD ACG/VGS/ODSGNA Regional Postgraduate Course Copyright American College of Gastroenterology 1
 Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
An unusual source of right upper quadrant pain
 Originally Posted: Month, 00, 20xx An unusual source of right upper quadrant pain Resident(s): Ashish R. Vyas MD (PGY-V), Dominic T. Semaan M.D., J.D. (PGY-V) Attending(s): Dr. Denis Lincoln Program/Dept(s):
Originally Posted: Month, 00, 20xx An unusual source of right upper quadrant pain Resident(s): Ashish R. Vyas MD (PGY-V), Dominic T. Semaan M.D., J.D. (PGY-V) Attending(s): Dr. Denis Lincoln Program/Dept(s):
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Endoscopic pancreatic necrosectomy in 2017
 Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Title. region. Author(s) Citation Surgery, 145(3), pp ; Issue Date
 Citation Surgery, 145(3), pp ; Issue Date") NAOSITE: Nagasaki University's Ac Title Author(s) Huge pancreatic pseudocyst migratin region. Tajima, Yoshitsugu; Mishima, Takehi Taiichiro; Adachi, Tomohiko; Tsuneo Citation Surgery, 145(3), pp.341-342;
NAOSITE: Nagasaki University's Ac Title Author(s) Huge pancreatic pseudocyst migratin region. Tajima, Yoshitsugu; Mishima, Takehi Taiichiro; Adachi, Tomohiko; Tsuneo Citation Surgery, 145(3), pp.341-342;
Gastric ulcer Duodenal ulcer Pancreatitis Ileus. Barbora Konečná
 Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland
 pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
Original Article. Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome
 Tropical Gastroenterology 2015;36(1):31 35 Original Article Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome Surinder S Rana 1, Vishal Sharma 1, Deepak
Tropical Gastroenterology 2015;36(1):31 35 Original Article Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome Surinder S Rana 1, Vishal Sharma 1, Deepak
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Acute Pancreatitis:
 American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
Gastrectomy procedure and its complications: Findings at TC multi-detector 64 row.
 Gastrectomy procedure and its complications: Findings at TC multi-detector 64 row. Poster No.: C-2184 Congress: ECR 2012 Type: Educational Exhibit Authors: M. M. Mendigana Ramos, A. Burguete, A. Sáez de
Gastrectomy procedure and its complications: Findings at TC multi-detector 64 row. Poster No.: C-2184 Congress: ECR 2012 Type: Educational Exhibit Authors: M. M. Mendigana Ramos, A. Burguete, A. Sáez de
2017 Chicago CAPA meeting Case Discussion
 2017 Chicago CAPA meeting Case Discussion Case 1 (Presented by Haiyan Chen) 25 yo M, h/o melanoma diagnosed 2 months ago before presenting severe abdominal pain Left colon biopsy, low power Left colon
2017 Chicago CAPA meeting Case Discussion Case 1 (Presented by Haiyan Chen) 25 yo M, h/o melanoma diagnosed 2 months ago before presenting severe abdominal pain Left colon biopsy, low power Left colon
EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018
 EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018 Please respond to the following items on a scale from 5 (highest) to 1 (lowest). The
EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018 Please respond to the following items on a scale from 5 (highest) to 1 (lowest). The
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Prof. (DR.) MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet
 MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet") Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
Douglas G. Adler MD. ACG Regional Postgraduate Course - Nashville, TN Copyright 2013 American College of Gastroenterology
 Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Non Operative Management of Perforated Duodenal Ulcers. Rabih Nemr M.D. Kings County Hospital Sept 2006
 Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
X-rays. Dr Will Dooley
 X-rays Dr Will Dooley Plan Chest X-Rays Abdominal X-Rays Exam approach Presentation skills EMQ EMQ- answers Chest X-Ray - Systematic Approach D R Details RIP Image Quality +/- OBVIOUS ABNORMALITY A B C
X-rays Dr Will Dooley Plan Chest X-Rays Abdominal X-Rays Exam approach Presentation skills EMQ EMQ- answers Chest X-Ray - Systematic Approach D R Details RIP Image Quality +/- OBVIOUS ABNORMALITY A B C
Does it matter what we drain?
 Endoscopic Management of Pancreatic Fluid Collections Shyam Varadarajulu, MD Medical Director Center for Interventional Endoscopy Florida Hospital, Orlando Does it matter what we drain? Makes all the difference!
Endoscopic Management of Pancreatic Fluid Collections Shyam Varadarajulu, MD Medical Director Center for Interventional Endoscopy Florida Hospital, Orlando Does it matter what we drain? Makes all the difference!
Patient Information. Age: 8 y/o Sex: Female. Date of Admission: Date of Discharge:
 Patient Information Age: 8 y/o Sex: Female Date of Admission: 92-10-08 Date of Discharge: 92-10-18 Chief Complaint Severe admominal pain and vomiting with dysuria since last afternoon Present Illness Lower
Patient Information Age: 8 y/o Sex: Female Date of Admission: 92-10-08 Date of Discharge: 92-10-18 Chief Complaint Severe admominal pain and vomiting with dysuria since last afternoon Present Illness Lower
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Pseudo Pancreatic Cyst Causing Portal Hypertension Dr. B. Ananda Rama Rao 1, Dr. Mohd Raheemuddinkhan 2,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Pseudo Pancreatic Cyst Causing Portal Hypertension Dr. B. Ananda Rama Rao 1, Dr. Mohd Raheemuddinkhan 2,
Citywide Infectious Disease Conference. March 27 th, 2018
 Citywide Infectious Disease Conference March 27 th, 2018 Citywide Show and Tell Case 1 Summary 60 s year old Puerto Rican born man SCC of Esophagus, treated with radiation and chemotherapy and then esophageal
Citywide Infectious Disease Conference March 27 th, 2018 Citywide Show and Tell Case 1 Summary 60 s year old Puerto Rican born man SCC of Esophagus, treated with radiation and chemotherapy and then esophageal