Diabetes-related complications: screening and treatment
|
|
|
- Frederica Sharp
- 5 years ago
- Views:
Transcription
 Denis Daneman University of Toronto The Hospital for Sick")
1 Diabetes-related complications: screening and treatment (focus on diabetic nephropathy) Denis Daneman University of Toronto The Hospital for Sick Children
2 Declared Conflicts of Interest Hvidore International Childhood Diabetes Study Group funded by NovoNordisk Pfizer Ltd. UK supplying medications and placebo for AdDIT
3 Pathogenesis of Complications Chronic hyperglycemia Hemodynamic alterations Advanced Glycation End Products (AGEs) Polyol pathway derangements Protein Kinase C (PKC) activation Growth factors and cytokines
4 Metabolic Pathway High Glucose AGEs, polyols, GLUTs, GAG Hemodynamic Pathway Ang ll (RAS), ET, VP, NEP, PG, TXA2 Growth factors and cytokines (GH/IGF-l, TGF-β, CTGF, VEGF, PDGF) Intracellular signalling molecules (PKC-α, PKC-β, NF-κB, MAPK) Structural EC matrix accumulation Functional Albuminuria Reduced GFR DIABETIC NEPHROPATHY Modified from Fukami et al, 2005
5 Metabolic Pathway High Glucose AGEs, polyols, GLUTs, GAG Dyslipidemia Hemodynamic Pathway Ang ll (RAS), ET, VP, NEP, PG, TXA2 Growth factors and cytokines (GH/IGF-l, TGF-β, CTGF, VEGF, PDGF) Intracellular signalling molecules (PKC-α, PKC-β, NF-κB, MAPK) Structural EC matrix accumulation Functional Albuminuria Reduced GFR DIABETIC NEPHROPATHY Modified from Fukami et al, 2005
6 Trajectories of DN AER Macroalbuminuria/ frank proteinuria Microalbuminuria d. persistent c. intermittent Onset First decade Second decade b. a. Duration of Diabetes
7 Risk factors: Modifiers and modifiables*: Early onset and long duration Glycemic control******** - metabolic memory Hypertension*** Family history candidate genes Autonomic neuropathy, retinopathy Smoking** Hyperlipidemia** - IR/Metabolic syndrome Diet* - protein intake, BMI* Exercise** Psychosocial dysfunction* (Cameron et al, Diab Care )
8 Age (years) CDA 2003: Glycemic Targets A1C target children and adolescents Preprandial glucose target (mmol/l) Considerations < 5 9% Extreme caution required to avoid severe hypoglycemia because of the risk of cognitive impairment in this age group % Targets should be graduated to the child s age % 6% Appropriate for most patients Consider for patients in whom it can be achieved safely.
9 Age (years) CDA 2003: Glycemic Targets A1C target children and adolescents Preprandial glucose target (mmol/l) Considerations < 5 9% 2008 <8.5% Extreme caution required to avoid severe hypoglycemia because of the risk of cognitive impairment in this age group Under intense debate: hyper vs hypo!! % Targets should be graduated to the child s age % 6% Appropriate for most patients Consider for patients in whom it can be achieved safely.
10
11 Hvidore Study Group 2005: Institutional correlates of outcomes Centre differences significant but weak relationships with: Availability of a 24 hr hotline Clear (and lower) targets for glucose and A1c Frequency of visits with MD (inverse relationship with DNE/MHP) Balanced approach to parental involvement avoidance of extremes of neglect and over-dependence
12 Candidate genes: ACE gene: Boright et al (Diabetes 2005; 54: DCCT cohort) I/I confers lower risk for persisent MA and severe DN; also homozygosity for common TIC haplotype SOD 1/splicing factor serine alanine 15 variants from the DCCT/EDIC cohort 3q locus (3q23-q24) Moczulski (Diabetes 1998; 47:1164-9):?near AT1 (ang II type 1 receptor) Christiskov (DRCP 2004; 66:79-86): confirmed Moczulski Vionnet (Diabetes 2006; 55: ): 3q analysis:?dn associated with a variant in the promoter region of adiponectin gene Osterholm (KI 2007; 71:140-5): 3q likely has locus for DN susceptibility
13 Data from 2007: mass screening FSX (Farsenoid X receptor nuclear hormone receptor superfamily) Jiang (Diabetes 2007, epub): FXR agonists modulate DN in animal model VEGF-A: Lindenmeyer (JASN 2007; 18: ): paradoxical findings ENTPD1: Friedman (Diabetes 2007; 56:2371-9): novel vascular protective factor in glomerular inflammation/thromboregulation Carnosinase (18q); ELMO1(7p14): Iyengar (Sem Nephr 2007; 27:208-22): preliminary data from genome-wide scans in large-scale studies 7q, 10p and 18q: Iyengar (Diabetes 2007;56: ) FIND Study 6p; 7q: Kankova (Diabetologia 2007; 50:990-9): SNP approach TGFB1 type 1 & 2 receptors: McKnight (BMC Med Genet 2007; 23:5) do not influence DN
14 Critical questions: How do we diagnose early complications, esp. diabetic nephropathy? Is early identification of at risk youth possible? Are there effective primary preventions or secondary interventions? Do we blithely follow the adult data? Exciting therapeutic agents in the pipeline
15 How do we diagnose early diabetic nephropathy?: Diagnostic levels of microalbuminuria are: Arbitrary: AER >15/20/30 µg/min; ACR? Based on prediction models in adults c1980s Not based on nondiabetic normal ranges: <7.2 or <7.5 µg/min (= 3 SDS above nondiabetic mean) ORPS database suggests trajectory within normal range
16 Predictive value of MA for development of DN: Early studies
17

18 HR of Regression
19 Conclusions1: Microalbuminuria remains best predictor for progression of DN in adults BUT at a lower level Data not shown MA is an independent risk factor for CVD In adults, presence of MA indicates need for therapy (ACEi/ARB +/- statin) Case for intervention during adolescence: Based on limited data and declining rates of MA Extrapolated from adult data
20 ACEi in Adults: A Caveat Fiociello et al (Krolewski s group at Joslin). Determinants of progression from MA to Proteinuria in patients who have T1D and are treated with ACEi. Clin J AM Soc Nephrol 2: , Cohort of 373 with MA during 2 yr baseline fllwd X10 yr Patients treated with ACEi had higher BP, higher UAE, and longer duration of T1D
21 Fiociello2 Progression from MA to Proteinuria common: 6.3/100 person-years Determinants/predictors of progression: Poor glycemic control Elevated serum cholesterol
22 Fiociello3 Person-yr Progress to Prot (n) HbA1c <8.6% Inc rate (/100 pt-yr) P < % >9.6% Cholesterol < >
23 Incidence Rate per 100 p.yr No. of Predictors/determinants: HbA1c & Cholesterol
24 Should we screen for microalbuminuria prepuberty? How frequent is MA prepuberty? Lawson (1996, Toronto); Riihimaa (2000, Finland): Olsen (2004, Denmark): 0 Joner (1992, Norway): only 1/41 < 13 yrs Schultz et al (1999-, ORPS): Used ACR cut-offs of >3.5 & 4 for boys & girls respectively At 5 yr, 63/514 = 12.8% had MA NB: 21 regressed, 22 persisted and 20 no f/up Age at diagnosis: 5-11 appearance of MA after puberty onset <5 6 developed MA prepuberty but 3/3 with f/up regressed More rapid rate of MA increase in puberty cf prepuberty (80 vs 26%)
25 MA prepuberty an-other view Moore & Shield (2000, MIDAC) Used low ACR cut-off (>2) 5/131 (3.8%) of prepubertal children with MA Jones (Liverpool, 1998) Used 2.5 cut-off 13/34 (39%) prepuberty with persistent MA Donaghue (Sydney, 1997) 5/64 (8%) prepubertal children with AER >7.5 µg/min Only 1 >15 Also: Janner (Berne, 1994) Persistent MA linked to early puberty NB: Wessex Diabetes Nephropathy Project (2001) suggested ACR cut-offs of <4.5 and <5.2 mg/mmol Cr in males and females respectively.
26 Effect of pubertal duration on prevalence of MA & kidney volume: (Lawson, Sochett et al, Diabetes 1996) STAGE Prepuberty Pubertal Postpub N Age (yr, SD) * A1c (%) T1DM duration Insulin (u/kg) * MA (%) >15<200 on 2/3 Kidney volume (/BSA) * *
27 MA in Adolescents: % of adolescents with persistent MA >15-20 µg/min after 5-8 yr Older studies: 7-27% Newer studies: 2-4% limited long-term studies - ORPS
28 DN in 27,805 children, adolescents and adults with T1D. Raile et al, Diabetes Care 30: , 2007 By 40 yr duration, 24.5% MA, <10% Macro/ESRD 26,605 = normal 919 = MA 78 = MacroAlbuminuria 203 = ESRD Determinants: Diabetes duration; A1c, LDL cholesterol; BP; male sex Childhood onset = protective young age at diagnosis reduced risk of MA corrected for duration & other independent covariates
29 Summary of 6 studies: Studies 6 % (range) Subjects 1443 MA initial (7-27) Regressors (31-65) Persistents (35-69) Follow-up 3-10 yr
30 Predictors of Regression/ Progression Shield: A1c, AER, age Rudberg: A1c, AER, age Gorman: A1c, AER Bojestig: A1c Schultz: A1c, females, age at diagnosis Steinke: Biopsy: inc GBM width and GFR NB: in these studies, neither disease duration nor clinic BP significantly contributed to MA status at follow-up
31 Does puberty initiate/accelerate DN? White, Krolewski, Kostraba: prepuberty contributes little to diabetes-related complications But many studies do not support this view: some retinopathy, microalbuminuria in prepubertal children? Some changes prepuberty, e.g. kidney size, GFR DCCT data affected by overall duration Important risk factors in adolescence: Deteriorating metabolic control Insulin resistance of puberty Changes in the GH/IGF-l axis
32 Control and Complications: Linear vs. Threshold effect?
33
34
35 ORPS Database: Kaplan-Meier survival estimates for the risk of developing MA based on tertiles of albumin excretion phenotype (at yrs-corrected for gender, age at diagnosis, diabetes duration). RR 1.96 RR 4.03 Dunger et al. Diab Med 24:131-6,2007
36 Kaplan-Meier survival estimates for the risk of developing MA based on average HbA1c levels /> 9%. RR 0.26 Dunger et al. Diab Med 24:131-6,2007
37 Risk of developing MA comparing Group [1] subjects with an albumin excretion phenotype in upper tertile or in the middle tertile with HbA1c >9%: Group [2] - albumin excretion phenotype in the lowest tertile or in the middle tertile with an HbA1c 9%. RR 5.69 Dunger et al. Diab Med 24:131-6,2007
38 Conclusions2: Persistent microalbuminuria in the prepubertal years is sufficiently uncommon and likely to regress thereby making its routine screening costineffective Diabetic nephropathy risk prepuberty most closely linked to metabolic control and genetic risk
39 Conclusions3: From ORPS Prediction models for progression of DN possible using early ACR determinations adjusting for Age, gender, disease duration Glycemic exposure A1c In contrast to adults, few studies of intervention during adolescence DCCT glycemic intervention ACEi Cook (1990), Rudberg (1990), Yuksel (1998)
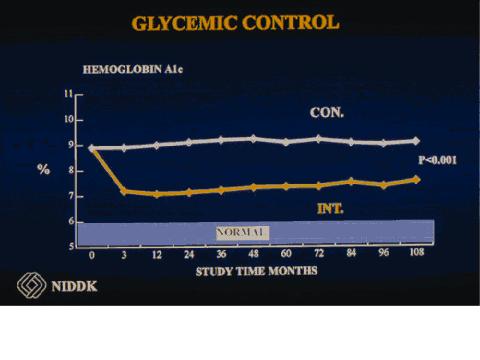
40 Lessons from the DCCT/EDIC Follow-up of DCCT cohort in EDIC since 1993: Glycemic Control METABOLIC MEMORY Search for complication susceptibility genes Novel analysis of data

41

42

43
44
45 Copyright restrictions may apply. JAMA 2003;290: Prevalence and Cumulative Incidence of Microalbuminuria
46 Prevalence and Incidence of Albuminuria JAMA 2003;290: Copyright restrictions may apply.

47 Prevalence of Hypertension at Each Year of the EDIC Study Writing Team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Res Group, JAMA 2003;290: Copyright restrictions may apply. JAMA 2003;290:
48 Metabolic Memory The group treated intensively in the DCCT continues to maintain an advantage over the conventional treatment group >8 years later despite similar A1c levels (~8%) Metabolic memory may dissipate with time in adolescent cohort parallel cumulative incidence Concept that long periods of poor control prime the system for ongoing complication risk (Engerman in dogs in 1980s)
49 Metabolic Memory: Progression of incipient diabetic retinopathy during good glycemic control. Engerman and Kern, Diabetes dogs randomly divided into nondiabetic and 3 diabetic groups: poor control for 5 yr good control for 5 yr poor control for 2.5 yr followed by good control for 2.5 yr Retinal lesions developed during 60 mo of poor control but inhibited if good control was begun within 2 mo In group 3, retinopathy was absent/equivocal at 2.5 yr of poor control BUT, was found to develop subsequently despite good glycemic control
50
51 Investigational targets for diabetic nephropathy Target 1: insulin resistance: PTP-1B inhibitors GSK-3 inhibitors Target 2: AGE accumulation: AGE formation inhibitors AGE crosslink breakers Soluble RAGE Target 3: Oxidative stress: Polyol pathway inhibitors Antioxidants RAS blockers GLUT inhibitors Target 5: Others: Glycosaminoglycans Vasopressin antagonists HMG-CoA reductase inhibitors Target 4: Fibrogenesis: RAS blockers Endothelin antagonists NEP inhibitors Cyclooxygenase -2 inhibitors Prostacycline analogue TXA-2 antagonists TGF-β antagonists CTGF antagonists VEGF antagonists PDGF antagonists *GH/IGF-1 inhibitors* PKC inhibitors NF-κB inhibitors MAPK inhibitors Modified from Fukami et al, 2005
52 Interventions in Adolescents: Step 1: Improve glycemia From diagnosis: A1c tracking DCCT suggests: Metabolic memory:?application to pubertal group Advantage of intensive insulin therapy Don t forget psychosocial factors! Step 2: If MA persistent/progressive, consider medication therapy ACEi/ARB/combination Addition of HMG Co-A reductase inhibitor may: Decrease MA Lower cardiovascular risk
53 What sort of RCT? Primary prevention: Introduction of renoprotection prior to identification of MA Problem: would need to treat enormous numbers for long time to show benefit in relatively few Secondary intervention: Renoprotection at first sign of risk: pma vs ORPS criteria Need: large scale screening and trajectory to identify at risk Choice of intervention: ACEi/ARB/combo + statin vs other Tertiary intervention: Treat advanced DN: fortunately too few in adolescence
54 AdDIT (UK, Australia, Canada) Secondary intervention: Eligibility according to ORPS criteria Large scale screening and trajectory to identify at risk yr olds treat through puberty?renoprotection Choice of intervention: Treatment Placebo ACEi Placebo ACEi Placebo Placebo Statin Statin
55 What about RASS? Primary prevention: Introduction of renoprotection prior to identification of MA year olds Biopsy pre and 5 yr post RCT Placebo vs ACEi/ARB No histologic advantage from so-called renoprotection at 5 yr (Mauer, ADA 2008)?significance of these results?
56 Take Home Messages Current treatment philosophy in T1D is informed by the outcomes of the DCCT/ EDIC Hyperglycemia is the single most important modifiable risk factor for the onset and/or progression of the micro- and macrovascular complications of T1D starting at disease onset. Tracking A1c from diagnosis most important indicator of risk trajectory But do not forget potentially important role of hyperlipidemia
57 Hypothesis since 1995: GLYCEMIA Obesity GLYCEMIA BP regulation Smoking Lipids/CV risk Diet Obesity/IR/MS Exercise prepuberty puberty GLYCEMIA Systemic Hypertension Smoking Lipids/CV risk factors Diet Obesity/IR/metabolic syndrome Exercise adulthood
58 Accumulating burden Glycemia Good start Risk factors: smoking, obesity, BP, lipids, genes Adolescent amplification Surveillance Psychosocial indicators In childhood, A1c = best indicator of DN risk
59 Acknowledgements SickKids: Etienne Sochett Jenny Cook (Couper) (Adelaide), Margaret Lawson (Ottawa), Beth Cummings (Halifax) Diabetes Team AdDIT: David Dunger (Cambridge), Tim Jones (Perth) Hvidore International Study Group Funders: JDRF/Diabetes UK/CDA/ Mclaughlin Chair
Adolescent renal and cardiovascular disease protection in type 1 diabetes AdDIT Study
 Keystone, Colorado, July 2013 Practical Ways to Achieve Targets in Diabetes Care Adolescent renal and cardiovascular disease protection in type 1 diabetes AdDIT Study Professor David Dunger Department
Keystone, Colorado, July 2013 Practical Ways to Achieve Targets in Diabetes Care Adolescent renal and cardiovascular disease protection in type 1 diabetes AdDIT Study Professor David Dunger Department
Microvascular Disease in Type 1 Diabetes
 Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Kidney Disease: Update. GKA Master Class. Istanbul 2011
 Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Managing patients with renal disease
 Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
The metabolic memory. Antonio Ceriello
 The metabolic memory Antonio Ceriello : DCCT/EDIC - Long-term Microvascular Risk Reduction in Type 1 Diabetes A1C 12% 10% Intensive Retinopathy progression (incidence) Conventional 0.5 0.4 0.3 62% risk
The metabolic memory Antonio Ceriello : DCCT/EDIC - Long-term Microvascular Risk Reduction in Type 1 Diabetes A1C 12% 10% Intensive Retinopathy progression (incidence) Conventional 0.5 0.4 0.3 62% risk
Lecture 19 Summary Gestational Diabetes and Complications of Diabetes. Gestational diabetes;
 Lecture 19 Summary Gestational Diabetes and Complications of Diabetes Gestational diabetes; - Type of diabetes that only develops during pregnancy Usually diagnosed in late pregnancy Causes high blood
Lecture 19 Summary Gestational Diabetes and Complications of Diabetes Gestational diabetes; - Type of diabetes that only develops during pregnancy Usually diagnosed in late pregnancy Causes high blood
Uric acid and CKD. Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George
 Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Microvascular Complications in Diabetes:
 Microvascular Complications in Diabetes: Perspectives on Glycemic Control to Prevent Microvascular Complications Discussion Outline: Glycemia and Microvascular Compliations Clinical Trials - A Brief History
Microvascular Complications in Diabetes: Perspectives on Glycemic Control to Prevent Microvascular Complications Discussion Outline: Glycemia and Microvascular Compliations Clinical Trials - A Brief History
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Nephropathy in Type 1 Diabetes: Can One Identity the Patients at Risk?
 Nephropathy in Type 1 Diabetes: Can One Identity the Patients at Risk? Pierre Lefèbvre University of Liège, Belgium Cuba, November 2007 Nephropathy in Type 1 Diabetes It has been known for years that the
Nephropathy in Type 1 Diabetes: Can One Identity the Patients at Risk? Pierre Lefèbvre University of Liège, Belgium Cuba, November 2007 Nephropathy in Type 1 Diabetes It has been known for years that the
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions
 Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Nephropathy
 Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
DIABETES MEASURES GROUP OVERVIEW
 2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes Mellitus: Evaluation and Care Management
 Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes and Kidney Disease. Kris Bentley Renal Nurse practitioner 2018
 Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
1.6 > < ESRD. < >2.0 ESRD Serum creatinine mg/dl
 HMG-CoA Reductase Inhibitors and Renal Function Vito M. Campese, MD Professor of Medicine, Physiology and Biophysics Chief, Division of Nephrology and Hypertension Center Keck School of Medicine, USC Los
HMG-CoA Reductase Inhibitors and Renal Function Vito M. Campese, MD Professor of Medicine, Physiology and Biophysics Chief, Division of Nephrology and Hypertension Center Keck School of Medicine, USC Los
For more information about how to cite these materials visit
 Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Supplementary Online Content
 Supplementary Online Content Afkarian M, Zelnick L, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. doi:10.1001/jama.2016.10924 emethods efigure
Supplementary Online Content Afkarian M, Zelnick L, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. doi:10.1001/jama.2016.10924 emethods efigure
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
DCCT Diabetes Control & Complications Trial
 DCCT Diabetes Control & Complications Trial A. Vinik MD, PhD, FCP, MACP, FACE, Καθηγητής και Αντιπρόεδρος για την Έρευνα, Ιατρική Σχολή Ανατολικής Βιρτζίνια, Κέντρο Ενδοκρινολογικών και Μεταβολικών Νοσημάτων,
DCCT Diabetes Control & Complications Trial A. Vinik MD, PhD, FCP, MACP, FACE, Καθηγητής και Αντιπρόεδρος για την Έρευνα, Ιατρική Σχολή Ανατολικής Βιρτζίνια, Κέντρο Ενδοκρινολογικών και Μεταβολικών Νοσημάτων,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Kidney and heart: dangerous liaisons. Luis M. RUILOPE (Madrid, Spain)
") Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
The CARI Guidelines Caring for Australians with Renal Impairment. Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy
 Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
ACCORD, ADVANCE & VADT. Now what do I do in my practice?
 ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
Do All Prepubertal Years of Diabetes Duration Contribute Equally to Diabetes Complications?
 Pathophysiology/Complications O R I G I N A L A R T I C L E Do All Prepubertal Years of Diabetes Duration Contribute Equally to Diabetes Complications? KIM C. DONAGHUE, FRACP, PHD 1,2 JAN M. FAIRCHILD,
Pathophysiology/Complications O R I G I N A L A R T I C L E Do All Prepubertal Years of Diabetes Duration Contribute Equally to Diabetes Complications? KIM C. DONAGHUE, FRACP, PHD 1,2 JAN M. FAIRCHILD,
Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη
 Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη Κωνσταντίνος Τζιόμαλος Επίκουρος Καθηγητής Παθολογίας Α Προπαιδευτική Παθολογική Κλινική, Νοσοκομείο
Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη Κωνσταντίνος Τζιόμαλος Επίκουρος Καθηγητής Παθολογίας Α Προπαιδευτική Παθολογική Κλινική, Νοσοκομείο
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
23-Jun-15. Albuminuria Renal and Cardiovascular Consequences A history of progress since ,490,000. Kidney Center, UMC Groningen
 Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Prevention of complications: are we winning or losing the battle. Naveed Sattar Professor of Metabolic Medicine
 Prevention of complications: are we winning or losing the battle Naveed Sattar Professor of Metabolic Medicine Duality of Interest Declaration Consultant or speaker for: Amgen, AstraZeneca, Boehringer
Prevention of complications: are we winning or losing the battle Naveed Sattar Professor of Metabolic Medicine Duality of Interest Declaration Consultant or speaker for: Amgen, AstraZeneca, Boehringer
CARDIO-RENAL SYNDROME
 CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CORRELATION BETWEEN SERUM LIPID PROFILE AND ALBUMINURIA IN NORMOTENSIVE DIABETIC SUBJECTS Dr.Abhijit Basu 1*, Dr J.S. Jhala 2
 Original research article International Journal of Medical Science and Education pissn- 2348 4438 eissn-2349-3208 CORRELATION BETWEEN SERUM LIPID PROFILE AND ALBUMINURIA IN NORMOTENSIVE DIABETIC SUBJECTS
Original research article International Journal of Medical Science and Education pissn- 2348 4438 eissn-2349-3208 CORRELATION BETWEEN SERUM LIPID PROFILE AND ALBUMINURIA IN NORMOTENSIVE DIABETIC SUBJECTS
INTRODUCTION. In this study we examined the
 GLYCEMIC CONTROL PREDICTS DIABETIC EXTRARENAL MICROVASCULAR COMPLICATIONS BUT NOT RENAL SURVIVAL IN PATIENTS WITH MODERATE TO SEVERE CHRONIC KIDNEY DISEASE Background: Control of blood pressure (BP) and
GLYCEMIC CONTROL PREDICTS DIABETIC EXTRARENAL MICROVASCULAR COMPLICATIONS BUT NOT RENAL SURVIVAL IN PATIENTS WITH MODERATE TO SEVERE CHRONIC KIDNEY DISEASE Background: Control of blood pressure (BP) and
Prevention and management of chronic kidney disease in type 2 diabetes
 162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes mellitus is a complex of syndromes characterized metabolically by hyperglycemia and altered glucose metabolism, and associated
 Diabetes mellitus is a complex of syndromes characterized metabolically by hyperglycemia and altered glucose metabolism, and associated pathologically with specific microvascular and macrovascular complications.
Diabetes mellitus is a complex of syndromes characterized metabolically by hyperglycemia and altered glucose metabolism, and associated pathologically with specific microvascular and macrovascular complications.
Invited Revie W. Diabetic nephropathy: the modulating influence of glucose on transforming factor D production
 Histol Histopathol (1 998) 13: 565-574 Histology and Histopathology Invited Revie W Diabetic nephropathy: the modulating influence of glucose on transforming factor D production A.O. Phillips lnstitute
Histol Histopathol (1 998) 13: 565-574 Histology and Histopathology Invited Revie W Diabetic nephropathy: the modulating influence of glucose on transforming factor D production A.O. Phillips lnstitute
1995 The Diabetes Control and Complications Trial: Implications for Children and Adolescents
 ADS Position Statements 1995 The Diabetes Control and Complications Trial: Implications for Children and Adolescents Jennifer Couper, Timothy Jones, Kim Donaghue, Caroline Clarke, Michael Thomsett, Martin
ADS Position Statements 1995 The Diabetes Control and Complications Trial: Implications for Children and Adolescents Jennifer Couper, Timothy Jones, Kim Donaghue, Caroline Clarke, Michael Thomsett, Martin
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
A Fork in the Road: Navigating Through New Terrain
 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
CLINICIAN INTERVIEW A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY. Interview with Ralph Rabkin, MD
 A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
Update on Diabetes. Ketan Dhatariya. Why it s Not Just About Glucose Lowering Any More. Consultant in Diabetes NNUH
 Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Type 2 Diabetes. Treat to: limit complications maintain quality of life Improve survival
 Type 2 Diabetes Treat to: limit complications maintain quality of life Improve survival 1 Criteria for the diagnosis of diabetes 1. HbA1C 6.5% (rounded to 50mmol/mol). 2. FPG 7.0 mmol/l. 3. 2-h plasma
Type 2 Diabetes Treat to: limit complications maintain quality of life Improve survival 1 Criteria for the diagnosis of diabetes 1. HbA1C 6.5% (rounded to 50mmol/mol). 2. FPG 7.0 mmol/l. 3. 2-h plasma
Type 2 Diabetes in Adolescents
 Type 2 Diabetes in Adolescents Disclosures Paid consultant, Eli Lilly, Inc, Pediatric Type 2 Diabetes Clinical Trials Outline The burden of diabetes Treatment and Prevention Youth Diabetes Prevention Clinic
Type 2 Diabetes in Adolescents Disclosures Paid consultant, Eli Lilly, Inc, Pediatric Type 2 Diabetes Clinical Trials Outline The burden of diabetes Treatment and Prevention Youth Diabetes Prevention Clinic
JOSHUA K. KAYIMA INTERLINKING CARDIOVASCULAR DISEASE, CHRONIC KIDNEY DISEASE, AND OBESITY
 INTERLINKING CARDIOVASCULAR DISEASE, CHRONIC KIDNEY DISEASE, AND OBESITY JOSHUA K. KAYIMA ASSOCIATE PROFESSOR DEPT. OF CLINICAL MEDICINE AND THERAPEUTICS UNIVERSITY OF NAIROBI Introduction According to
INTERLINKING CARDIOVASCULAR DISEASE, CHRONIC KIDNEY DISEASE, AND OBESITY JOSHUA K. KAYIMA ASSOCIATE PROFESSOR DEPT. OF CLINICAL MEDICINE AND THERAPEUTICS UNIVERSITY OF NAIROBI Introduction According to
Clinical therapeutic strategies for early stage of diabetic kidney disease
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4239/wjd.v5.i3.342 World J Diabetes 2014 June 15; 5(3): 342-356 ISSN 1948-9358 (online) 2014
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4239/wjd.v5.i3.342 World J Diabetes 2014 June 15; 5(3): 342-356 ISSN 1948-9358 (online) 2014
Diabetic & Complications. Dr. A K Viswanath Consultant Diabetologist
 Diabetic & Complications Dr. A K Viswanath Consultant Diabetologist Outline Challenges in diabetes How do we fare? Diabetes complications Improving outcomes in diabetes Types of Diabetes Type-1 DM Genetic
Diabetic & Complications Dr. A K Viswanath Consultant Diabetologist Outline Challenges in diabetes How do we fare? Diabetes complications Improving outcomes in diabetes Types of Diabetes Type-1 DM Genetic
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care
 Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
International Journal of Diabetes & its Complications
 Research Article ISSN 253-8895 Research Article International Journal of Diabetes & its Complications Microalbuminuria in Children and Adolescents with Type 1 Diabetes Mellitus: Prevalence and Predictive
Research Article ISSN 253-8895 Research Article International Journal of Diabetes & its Complications Microalbuminuria in Children and Adolescents with Type 1 Diabetes Mellitus: Prevalence and Predictive
Modified version focused on CCNC Quality Measures and Feedback Processes
 Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
The Effect of Glycemic Exposure on the Risk of Microvascular Complications in the Diabetes Control and Complications Trial -- Revisited
 Diabetes Publish Ahead of Print, published online January 25, 2008 The Effect of Glycemic Exposure on the Risk of Microvascular Complications in the Diabetes Control and Complications Trial -- Revisited
Diabetes Publish Ahead of Print, published online January 25, 2008 The Effect of Glycemic Exposure on the Risk of Microvascular Complications in the Diabetes Control and Complications Trial -- Revisited
Cardiovascular Diabetology. Open Access ORIGINAL INVESTIGATION. C. R. L. Cardoso 1, N. C. Leite 1, C. B. M. Moram 2 and G. F.
 https://doi.org/10.1186/s12933-018-0677-0 Cardiovascular Diabetology ORIGINAL INVESTIGATION Open Access Long term visit to visit glycemic variability as predictor of micro and macrovascular complications
https://doi.org/10.1186/s12933-018-0677-0 Cardiovascular Diabetology ORIGINAL INVESTIGATION Open Access Long term visit to visit glycemic variability as predictor of micro and macrovascular complications
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes is a chronic illness that requires
 P O S I T I O N S T A T E M E N T Standards of Medical Care for Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Diabetes is a chronic illness that requires continuing medical care and patient
P O S I T I O N S T A T E M E N T Standards of Medical Care for Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Diabetes is a chronic illness that requires continuing medical care and patient
Diabetes: Staying Two Steps Ahead. The prevalence of diabetes is increasing. What causes Type 2 diabetes?
 Focus on CME at the University of University Manitoba of Manitoba : Staying Two Steps Ahead By Shagufta Khan, MD; and Liam J. Murphy, MD The prevalence of diabetes is increasing worldwide and will double
Focus on CME at the University of University Manitoba of Manitoba : Staying Two Steps Ahead By Shagufta Khan, MD; and Liam J. Murphy, MD The prevalence of diabetes is increasing worldwide and will double
Cumulative Kidney Complication Risk by 50 Years of Type 1 Diabetes: The Effects of Sex, Age, and Calendar Year at Onset
 Diabetes Care 1 Cumulative Kidney Complication Risk by 50 Years of Type 1 Diabetes: The Effects of Sex, Age, and Calendar Year at Onset Tina Costacou and Trevor J. Orchard https://doi.org/10.2337/dc17-1118
Diabetes Care 1 Cumulative Kidney Complication Risk by 50 Years of Type 1 Diabetes: The Effects of Sex, Age, and Calendar Year at Onset Tina Costacou and Trevor J. Orchard https://doi.org/10.2337/dc17-1118
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Pathology of endocrine pancreas. By: Shifaa Alqa qa
 Pathology of endocrine pancreas By: Shifaa Alqa qa major cell types: Beta ----- insulin Alpha ----- glucagon Delta ----- somatostatin PP (pancreatic polypeptide) cells ------ VIP DIABETES MELLITUS Normal
Pathology of endocrine pancreas By: Shifaa Alqa qa major cell types: Beta ----- insulin Alpha ----- glucagon Delta ----- somatostatin PP (pancreatic polypeptide) cells ------ VIP DIABETES MELLITUS Normal
Glycemic Control and Diabetic Complications
 Glycemic Control and Diabetic Complications SUZANNE STROWIG, RN, MSN PHIUP RASKIN, MD The relationship between glycemic control and diabetic complications remains unclear. Epidemiological studies reveal
Glycemic Control and Diabetic Complications SUZANNE STROWIG, RN, MSN PHIUP RASKIN, MD The relationship between glycemic control and diabetic complications remains unclear. Epidemiological studies reveal
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Discordance in risk factors for the progression of diabetic retinopathy and diabetic nephropathy in patients with type 2 diabetes mellitus
 Discordance in risk factors for the progression of diabetic retinopathy and diabetic nephropathy in patients with type 2 diabetes mellitus Ki-Ho Song*, Jee-Sun Jeong, Mee Kyoung Kim, Hyuk-Sang Kwon, Ki-Hyun
Discordance in risk factors for the progression of diabetic retinopathy and diabetic nephropathy in patients with type 2 diabetes mellitus Ki-Ho Song*, Jee-Sun Jeong, Mee Kyoung Kim, Hyuk-Sang Kwon, Ki-Hyun
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Microvascular and macrovascular complications in children and adolescents
 ISPAD Clinical Practice Consensus Guidelines 2018 Microvascular and macrovascular complications in children and adolescents Kim C Donaghue a,b, Loredana Marcovecchio c, R Paul Wadwa d, Emily Y Chew e,
ISPAD Clinical Practice Consensus Guidelines 2018 Microvascular and macrovascular complications in children and adolescents Kim C Donaghue a,b, Loredana Marcovecchio c, R Paul Wadwa d, Emily Y Chew e,
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
CV Risk Management in Diabetes Mellitus
 CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES
 RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D.
 Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Micro- and macroalbuminuria are
 Epidemiology/Health Services Research O R I G I N A L A R T I C L E Diabetic Nephropathy in 27,805 Children, Adolescents, and Adults With Type 1 Diabetes Effect of diabetes duration, A1C, hypertension,
Epidemiology/Health Services Research O R I G I N A L A R T I C L E Diabetic Nephropathy in 27,805 Children, Adolescents, and Adults With Type 1 Diabetes Effect of diabetes duration, A1C, hypertension,
Summary of Recommendation Statements Kidney International Supplements (2013) 3, 5 14; doi: /kisup
 3, 5 14; doi: /kisup") http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of